Embed Size (px)
Citation preview

5/21/2018
1
Hepatocellular Mass Lesions – weighty mattersJOHN HART, M.D.SURGICAL PATHOLOGY & HEPATOLOGY
UNIVERSITY OF CHICAGO MEDICAL [email protected]
Source: GLOBOCAN 2008 v2.0 http://globalcancermap.com/
Mass Lesions of the LiverCIRRHOTIC LIVER
• Focal fibrosis
• Macroregenerative nodule
• Dysplastic nodule
• Hepatocellular carcinoma (HCC)
• Cholangiocarcinoma
• (metastatic tumor)
NORMAL LIVER
• Metastatic tumor
• Focal nodular hyperplasia
• Hepatocellular adenoma
• Hepatocellular carcinoma
• Cholangiocarcinoma
• Combined HCC/cholangioCa
• Other (cystic) biliary tumors
• Angiomyolipoma
• Epithelioid hemangioendothelioma
• Other mesenchymal tumors
5/21/2018
2
Hepatocellular Carcinoma in Cirrhosis• High risk:
– Alcoholic steatohepatitis
– Hereditary hemochromatosis
– Chronic HCV hepatitis
– Chronic HBV hepatitis
• Intermediate risk:
– Non-alcoholic steatohepatitis
– Autoimmune hepatitis
– Alpha-1-antitrypsin deficiency
• Low risk:
– Wilson disease
– Primary biliary cirrhosis
– Primary sclerosing cholangitis
Diagnostic algorithm for HCC by the American Association for the Study of Liver Diseases (AASLD)
practice guidelines on the management of HCC in 2010 (Adopted from Bruix J et al).
72 year old male with alcoholic cirrhosis
and an increased serum AFP
2.0 cm mass with atypical imaging characteristics

5/21/2018
3
reticulin stain
5/21/2018
4
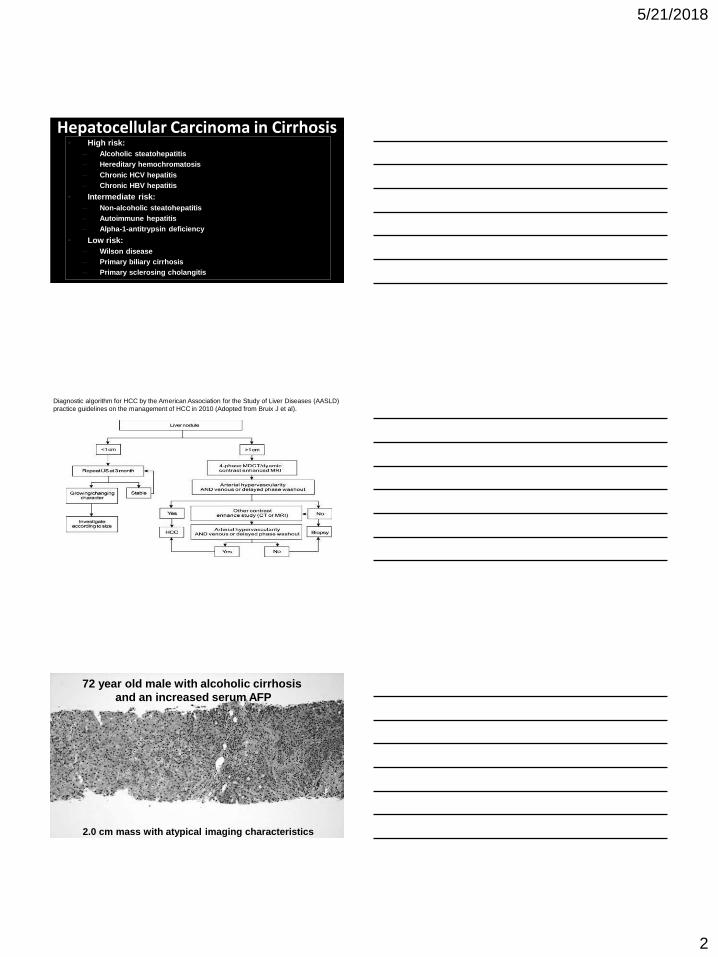
Hepatocellular Carcinoma – pseudoacinar type
Hepatocellular Carcinoma – pseudoacinar type
Hepatocellular Carcinoma – clear cell type
5/21/2018
5
Mass Lesions of the LiverCIRRHOTIC LIVER
• Focal fibrosis
• Macroregenerative nodule
• Dysplastic nodule
• Hepatocellular carcinoma
• Cholangiocarcinoma
• (metastatic tumor)
NORMAL LIVER
• Metastatic tumor
• Focal nodular hyperplasia
• Hepatocellular adenoma
• Hepatocellular carcinoma
• Cholangiocarcinoma
• Combined HCC/cholangioCa
• Other (cystic) biliary tumors
• Angiomyolipoma
• Epithelioid hemangioendothelioma
• Other mesenchymal tumors
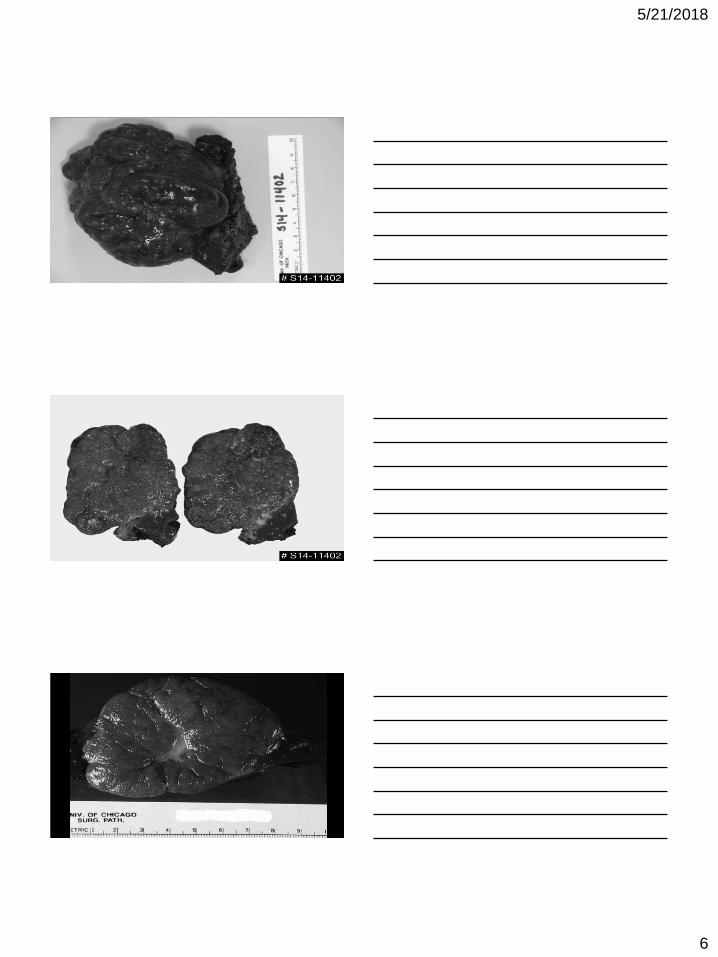
Focal Nodular HyperplasiaClinical Features
• Presentation:
– Asymptomatic if < 10 cm (majority)
– Abdominal pain, palpable mass
– Serum AFP level is NOT elevated
• Predisposing factors: None identified
• OCP may cause increase in size
• Central scar by CT or MRI:
– Also seen in fibrolamellar carcinoma
– Only present in larger lesions
• Can be multiple
• No malignant potential
5/21/2018
6
5/21/2018
7
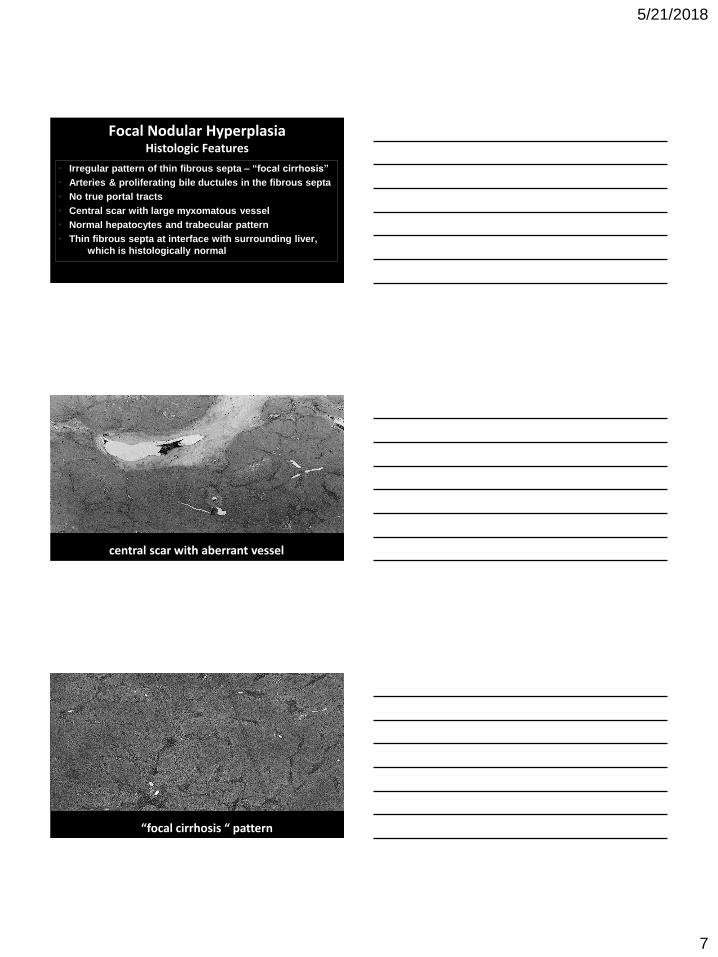
Focal Nodular HyperplasiaHistologic Features
• Irregular pattern of thin fibrous septa – “focal cirrhosis”
• Arteries & proliferating bile ductules in the fibrous septa
• No true portal tracts
• Central scar with large myxomatous vessel
• Normal hepatocytes and trabecular pattern
• Thin fibrous septa at interface with surrounding liver,
which is histologically normal
central scar with aberrant vessel
“focal cirrhosis “ pattern
5/21/2018
8
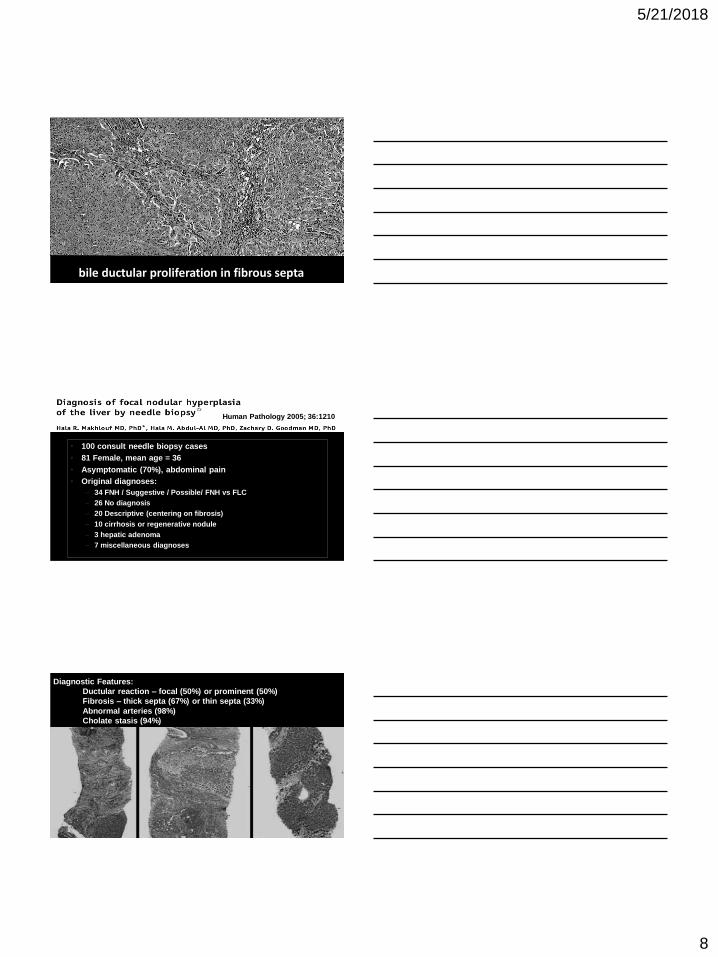
bile ductular proliferation in fibrous septa
• 100 consult needle biopsy cases
• 81 Female, mean age = 36
• Asymptomatic (70%), abdominal pain
• Original diagnoses:
– 34 FNH / Suggestive / Possible/ FNH vs FLC
– 26 No diagnosis
– 20 Descriptive (centering on fibrosis)
– 10 cirrhosis or regenerative nodule
– 3 hepatic adenoma
– 7 miscellaneous diagnoses
Human Pathology 2005; 36:1210
Human Pathology 2005; 36:1210-16.Diagnostic Features:
Ductular reaction – focal (50%) or prominent (50%)
Fibrosis – thick septa (67%) or thin septa (33%)
Abnormal arteries (98%)
Cholate stasis (94%)
5/21/2018
9
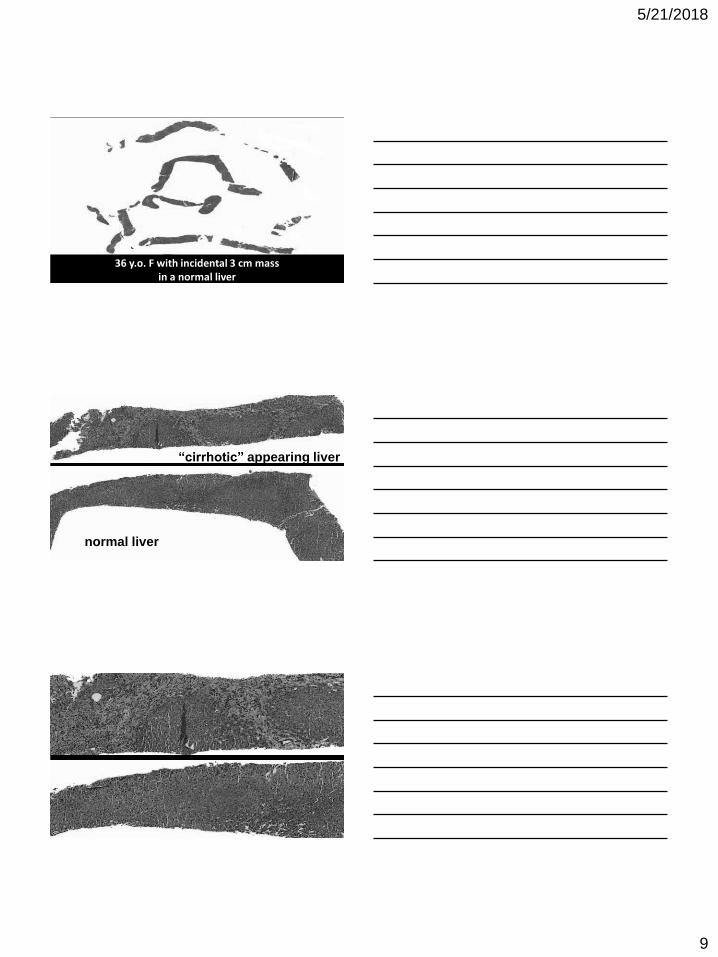
36 y.o. F with incidental 3 cm mass in a normal liver
normal liver
“cirrhotic” appearing liver
5/21/2018
10
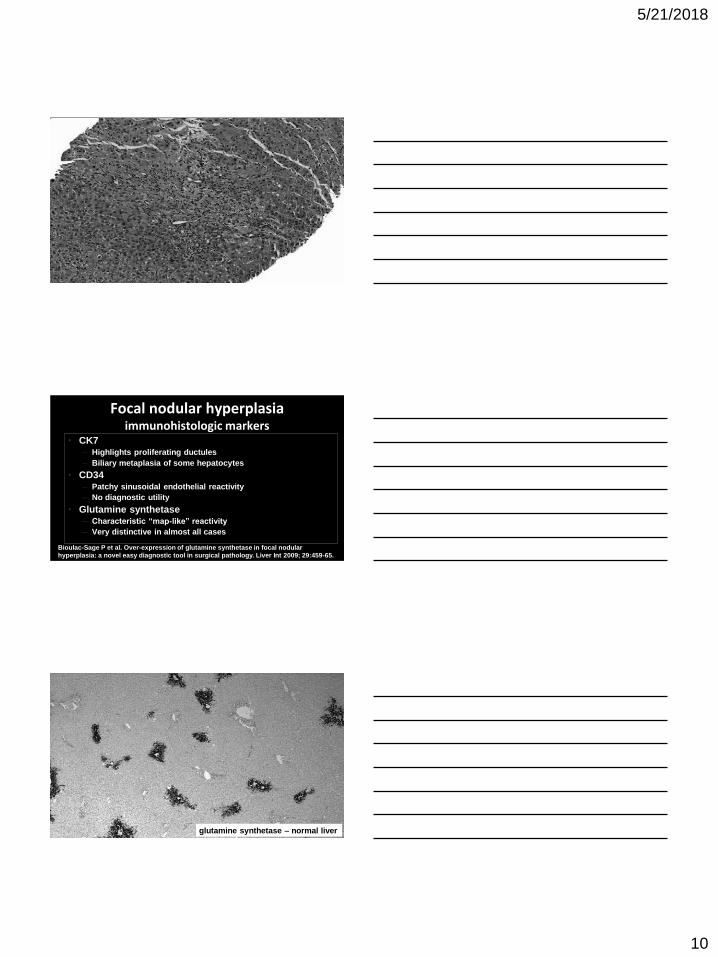
Focal nodular hyperplasiaimmunohistologic markers
• CK7– Highlights proliferating ductules
– Biliary metaplasia of some hepatocytes
• CD34– Patchy sinusoidal endothelial reactivity
– No diagnostic utility
• Glutamine synthetase– Characteristic “map-like” reactivity
– Very distinctive in almost all cases
Bioulac-Sage P et al. Over-expression of glutamine synthetase in focal nodular
hyperplasia: a novel easy diagnostic tool in surgical pathology. Liver Int 2009; 29:459-65.
glutamine synthetase – normal liver

5/21/2018
11
Focal nodular hyperplasia
Glutamine synthetase
Focal nodular hyperplasia

5/21/2018
12
Glutamine synthetase
Glutamine SynthetaseCONDITION STAINING PATTERN
Normal Distinct zone 3 perivenular cuff
Cirrhosis Patchy & weak periseptal
Focal nodular hyperplasia Strong map-like (geographic)
Hepatocellular adenoma Perivenular or weak & patchy or strong diffuse*
Hepatocellular carcinoma Perivenular or weak & patchy or strong diffuse*
Joseph NM, Ferrell LD, Jain D, Torbenson MS, Wu TT, Yeh MM, Kakar S.
Modern Pathol 2014; 27(1):62-72.
*beta-catenin activated
hepatocellular adenoma

5/21/2018
13
glutamine synthetase in hepatocellular adenoma
focal nodular hyperplasia
glutamine synthetase in focal nodular hyperplasia
5/21/2018
14
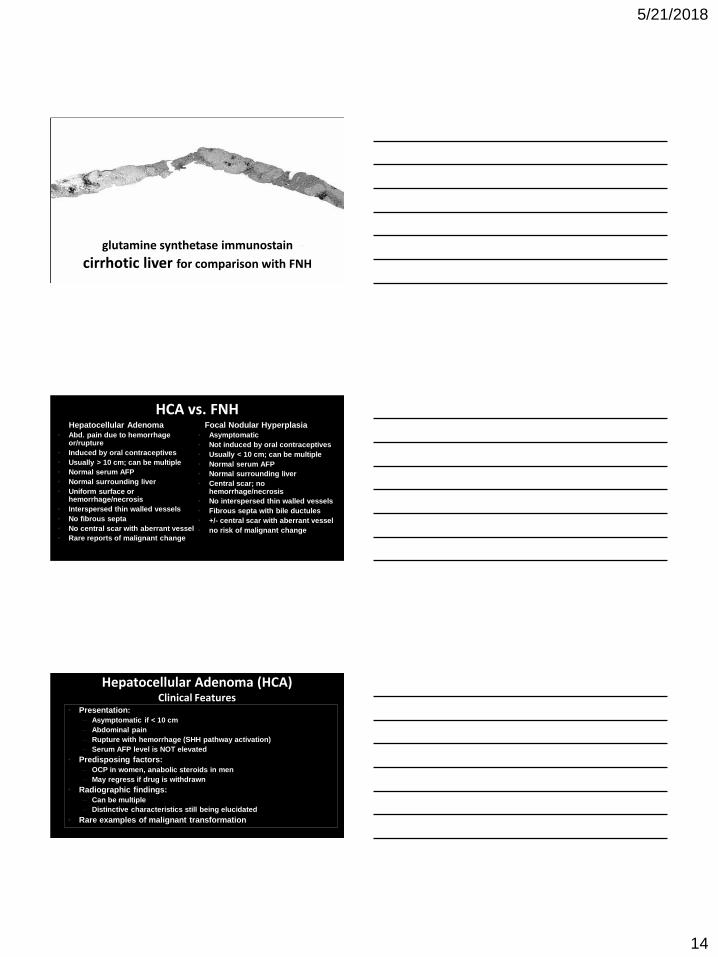
glutamine synthetase immunostain
cirrhotic liver for comparison with FNH
HCA vs. FNHHepatocellular Adenoma
• Abd. pain due to hemorrhage or/rupture
• Induced by oral contraceptives
• Usually > 10 cm; can be multiple
• Normal serum AFP
• Normal surrounding liver
• Uniform surface or hemorrhage/necrosis
• Interspersed thin walled vessels
• No fibrous septa
• No central scar with aberrant vessel
• Rare reports of malignant change
Focal Nodular Hyperplasia
• Asymptomatic
• Not induced by oral contraceptives
• Usually < 10 cm; can be multiple
• Normal serum AFP
• Normal surrounding liver
• Central scar; no hemorrhage/necrosis
• No interspersed thin walled vessels
• Fibrous septa with bile ductules
• +/- central scar with aberrant vessel
• no risk of malignant change
Hepatocellular Adenoma (HCA)Clinical Features
• Presentation:
– Asymptomatic if < 10 cm
– Abdominal pain
– Rupture with hemorrhage (SHH pathway activation)
– Serum AFP level is NOT elevated
• Predisposing factors:
– OCP in women, anabolic steroids in men
– May regress if drug is withdrawn
• Radiographic findings:
– Can be multiple
– Distinctive characteristics still being elucidated
• Rare examples of malignant transformation
5/21/2018
15
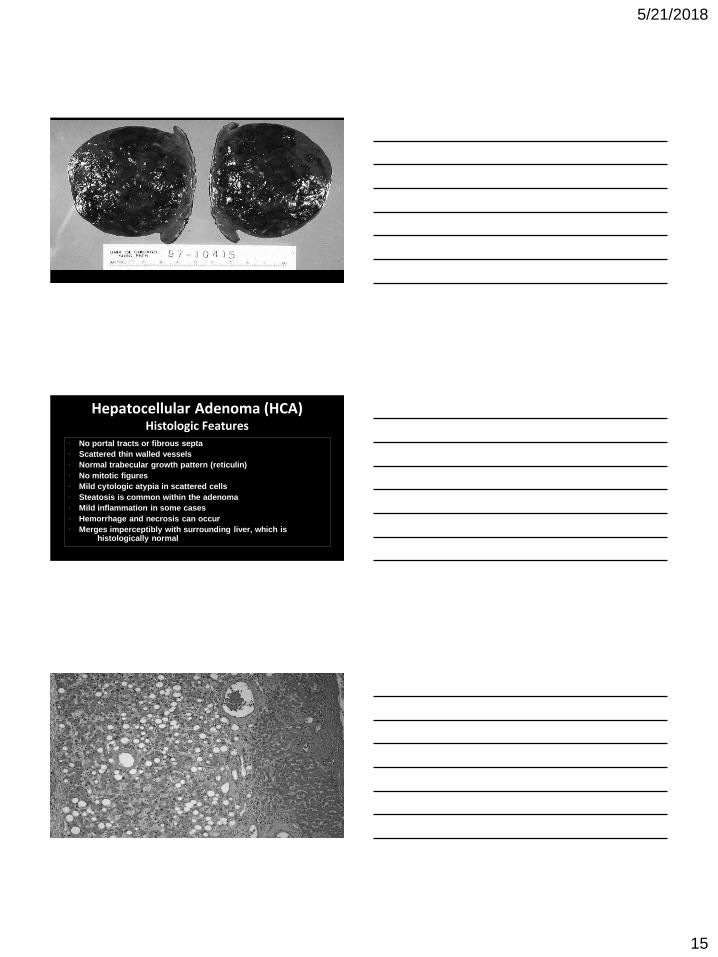
Hepatocellular Adenoma (HCA)Histologic Features
• No portal tracts or fibrous septa
• Scattered thin walled vessels
• Normal trabecular growth pattern (reticulin)
• No mitotic figures
• Mild cytologic atypia in scattered cells
• Steatosis is common within the adenoma
• Mild inflammation in some cases
• Hemorrhage and necrosis can occur
• Merges imperceptibly with surrounding liver, which is histologically normal

5/21/2018
16
reticulin stain

5/21/2018
17
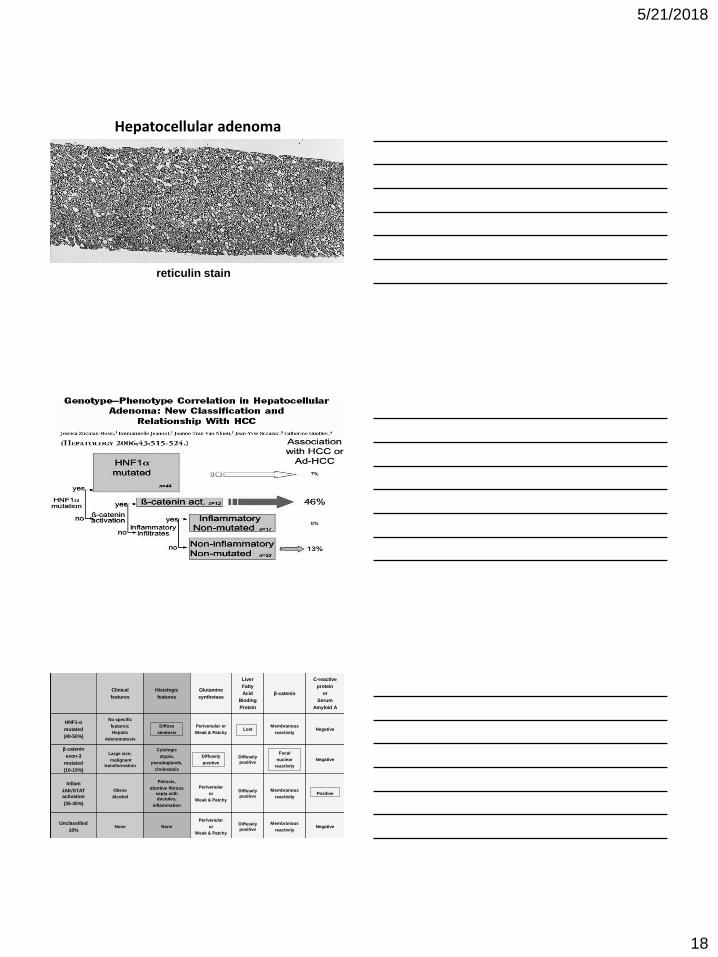
Hepatocellular adenoma
5/21/2018
18
Hepatocellular adenoma
reticulin stain
Clinical
features
Histologic
features
Glutamine
synthetase
Liver
Fatty
Acid
Binding
Protein
β-catenin
C-reactive
protein
or
Serum
Amyloid A
HNF1-α
mutated
(40-50%)
No specific
features;
Hepatic
Adenomatosis
Diffuse
steatosis
Perivenular or
Weak & PatchyLost
Membranous
reactivityNegative
β-catenin
exon-3
mutated
(10-15%)
Large size;
malignant
transformation
Cytologic
atypia,
pseudoglands,
cholestasis
Diffusely
positive
Diffusely
positive
Focal
nuclear
reactivity
Negative
Inflam
JAK/STAT
activation
(35-45%)
Obese
Alcohol
Peliosis,
abortive fibrous
septa with
ductules,
inflammation
Perivenular
or
Weak & Patchy
Diffusely
positive
Membranous
reactivityPositive
Unclassified
10%None None
Perivenular
or
Weak & Patchy
Diffusely
positive
Membranous
reactivityNegative

5/21/2018
19
HCA Normal
Liver Fatty Acid Binding Protein
HCA Normal
HFA mutated HCA (40-50%):
Obese women on OCP
No malignant potential
Loss of LFABP by immuno

5/21/2018
20
• 35 year old female presents with abdominal pain
• CT scan reveals a 6.5 cm liver mass; no central scar
• No history of chronic liver disease
• Serum AFP = < 5
• Resection performed
Clinical HistoryCase Courtesy of Dr. Benjamin Yan,
Medical College of Wisconsin
C12-1323
Inflammatory (telangiectatic) HCA

5/21/2018
21
reticulin stain
Peliosis

5/21/2018
22
inflammation
Abortive fibrous septa with ductules
HCA, inflammatory (telangiectatic) subtype
5/21/2018
23
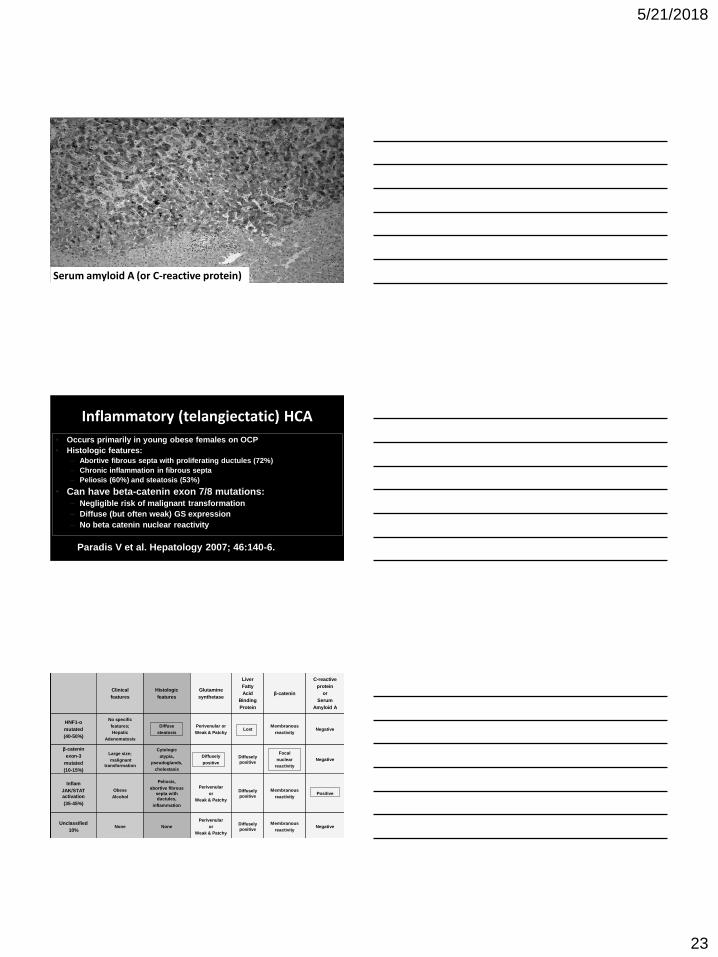
Serum amyloid A (or C-reactive protein)
Inflammatory (telangiectatic) HCA
• Occurs primarily in young obese females on OCP
• Histologic features:
– Abortive fibrous septa with proliferating ductules (72%)
– Chronic inflammation in fibrous septa
– Peliosis (60%) and steatosis (53%)
• Can have beta-catenin exon 7/8 mutations:– Negligible risk of malignant transformation
– Diffuse (but often weak) GS expression
– No beta catenin nuclear reactivity
Paradis V et al. Hepatology 2007; 46:140-6.
Clinical
features
Histologic
features
Glutamine
synthetase
Liver
Fatty
Acid
Binding
Protein
β-catenin
C-reactive
protein
or
Serum
Amyloid A
HNF1-α
mutated
(40-50%)
No specific
features;
Hepatic
Adenomatosis
Diffuse
steatosis
Perivenular or
Weak & PatchyLost
Membranous
reactivityNegative
β-catenin
exon-3
mutated
(10-15%)
Large size;
malignant
transformation
Cytologic
atypia,
pseudoglands,
cholestasis
Diffusely
positive
Diffusely
positive
Focal
nuclear
reactivity
Negative
Inflam
JAK/STAT
activation
(35-45%)
Obese
Alcohol
Peliosis,
abortive fibrous
septa with
ductules,
inflammation
Perivenular
or
Weak & Patchy
Diffusely
positive
Membranous
reactivityPositive
Unclassified
10%None None
Perivenular
or
Weak & Patchy
Diffusely
positive
Membranous
reactivityNegative
5/21/2018
24
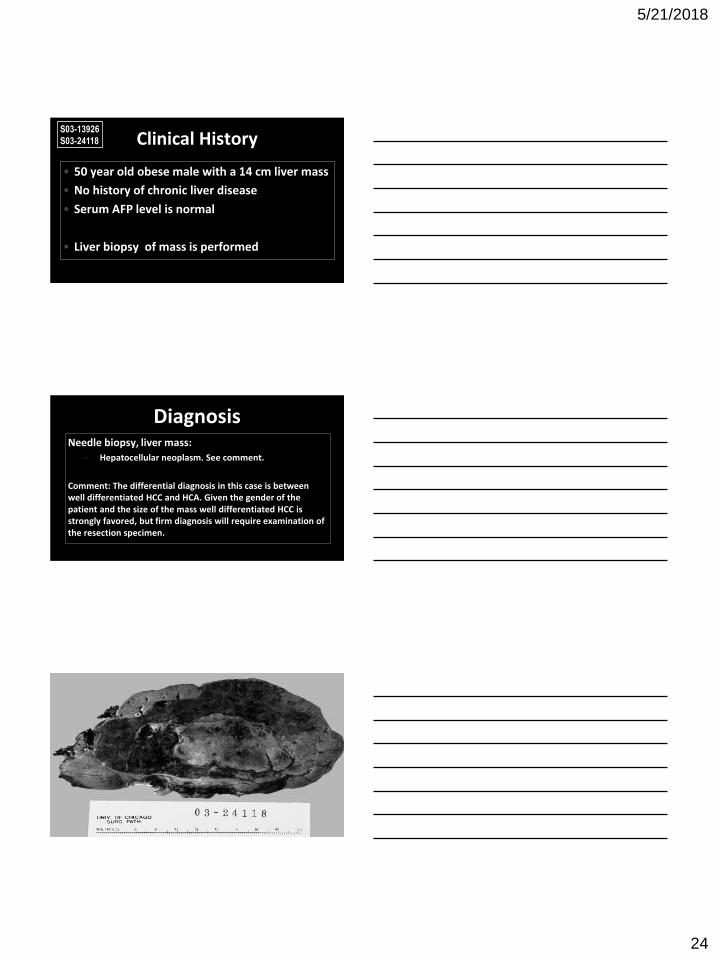
Clinical History
• 50 year old obese male with a 14 cm liver mass
• No history of chronic liver disease
• Serum AFP level is normal
• Liver biopsy of mass is performed
S03-13926
S03-24118
DiagnosisNeedle biopsy, liver mass:
– Hepatocellular neoplasm. See comment.
Comment: The differential diagnosis in this case is between well differentiated HCC and HCA. Given the gender of the patient and the size of the mass well differentiated HCC is strongly favored, but firm diagnosis will require examination of the resection specimen.

5/21/2018
25

5/21/2018
26
β-catenin
β-catenin

5/21/2018
27
glutamine synthetase – diffuse strong
Clinical
features
Histologic
features
Glutamine
synthetase
Liver
Fatty
Acid
Binding
Protein
β-catenin
C-reactive
protein
or
Serum
Amyloid A
HNF1-α
mutated
(40-50%)
No specific
features;
Hepatic
Adenomatosis
Diffuse
steatosis
Perivenular or
Weak & PatchyLost
Membranous
reactivityNegative
β-catenin
exon-3
mutated
(10-15%)
Large size;
malignant
transformation
Cytologic
atypia,
pseudoglands,
cholestasis
Diffusely
positive
Diffusely
positive
Focal
nuclear
reactivity
Negative
Inflam
JAK/STAT
activation
(35-45%)
Obese
Alcohol
Peliosis,
abortive fibrous
septa with
ductules,
inflammation
Perivenular
or
Weak & Patchy
Diffusely
positive
Membranous
reactivityPositive
Unclassified
10%None None
Perivenular
or
Weak & Patchy
Diffusely
positive
Membranous
reactivityNegative
HCA vs HCC• Worrisome features in an HCA:
– Large size (> 5 cm)
– Male gender
– Prominent nuclear pleomorphism
– β-catenin nuclear reactivity
– Diffuse glutamine synthetase reactivity
• Features for HCC:– Elevated serum AFP
– Mitoses, numerous isolated arterioles
– Loss of reticulin or clearly thickened trabeculae
– Stromal production by tumor cells
5/21/2018
28

5/21/2018
29
Hepatocellular Carcinoma Origin in “Normal Liver”
• Clinical Features:
– Abdominal pain and/or mass
– Constitutional symptoms
– Serum AFP elevated in only 1/3 of patients
– Search for occult chronic liver disease
• Histologic Features:
– No special histologic features (except for distinctive variants)
– Foci of dysplasia in surrounding liver
HCC in non-cirrhotic liver
Hepatocellular Carcinoma (HCC)Immunohistologic Profile
• pCEA – canalicular staining
• CD10 – canalicular staining
• HepPar1 – granular cytoplasmic staining
• MOC31 – no staining
• Cam 5.2 – cytoplasmic staining
• CD34 – increased in endothelial cells
• TTF-1 – cytoplasmic staining (Dako antibody)
• CK7, CK20, CK19 – negative???
• In situ hybridization for albumin mRNA (Mayo)
• [AFP – cytoplasmic staining]

5/21/2018
30
Bile production by tumor cells is diagnostic of hepatocellular origin
HepPar1• aka “hepatocyte”; “hepatocyte antigen”
• Developed at the University of Pittsburgh
• Staining characteristics:
– Reactive in > 80% of HCC
– Non-reactive in some poorly differentiated HCC
– Can be patchy (20%)
– Coarse cytoplasmic reactivity
– Can also be reactive in some gastric, pancreatic, gallbladder, and lung adenocarcinomas
• Also reactive in benign hepatocytes, FNH, adenoma, MRN, dysplastic nodule
HepPar-1 normal liver

5/21/2018
31
70 y.o. male with a 10 cm mass in non-cirrhotic liver
HepPar-1
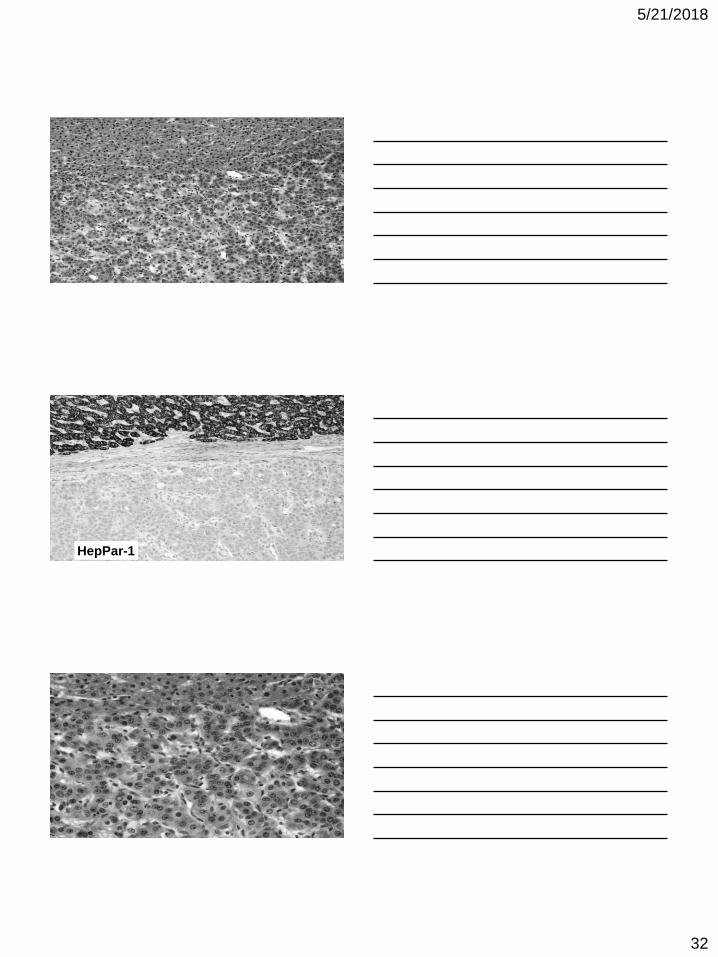
• 35 year old male with an 18 cm liver mass
• No history of chronic liver disease
• Non-cirrhotic liver
• Normal serum AFP level
5/21/2018
32
HepPar-1

5/21/2018
33
Synaptophysin
metastatic well differentiated neuroendocrine tumor
C15-1240 65 y.o. M with a 4 cm liver massNo history of liver diseaseSerum AFP level is normal
Normal liverTumor

5/21/2018
34
HepPar-1
PAX-8
metastatic renal cell carcinoma

5/21/2018
35
HepPar-1 False Positive Staining• Lung adenocarcinoma (~10%)
• Esophageal adenocarcinoma (~20%)
• Pancreatic adenocarcinoma (~10%)
• Duodenal (small bowel) adenocarcinoma (~25%)
• Liver (hepatocellular) carcinoma (~80%)
• Stomach (gastric) adenocarcinoma (> 40%)
• Gallbladder adenocarcinoma (~30%)
HepPar-1 False Positive Staining• Stomach (gastric) adenocarcinoma (> 40%)
• Lung adenocarcinoma (~10%)
• Pancreatic adenocarcinoma (~10%)
• Gallbladder adenocarcinoma (~30%)
• Esophageal adenocarcinoma (~20%)
• Duodenal (small bowel) adenocarcinoma (~25%)
• Liver (hepatocellular) carcinoma (~80%)
• 87 year old female undergoing cholecystectomy
• Liver mass in a non-cirrhotic liver
• No history of malignancy
C07-11895

5/21/2018
36
HepPar-1
5/21/2018
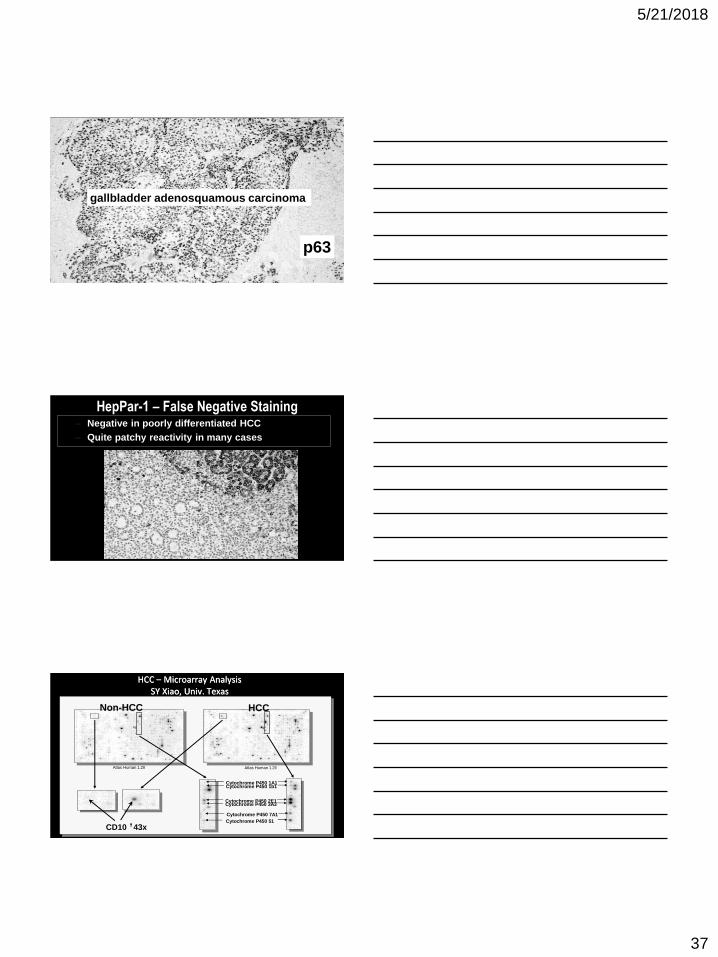
37
p63
gallbladder adenosquamous carcinoma
HepPar-1 – False Negative Staining– Negative in poorly differentiated HCC
– Quite patchy reactivity in many cases
HCC – Microarray AnalysisSY Xiao, Univ. Texas
Non-HCC HCC
Cytochrome P450 7A1
Cytochrome P450 3A3Cytochrome P450 2E1
Cytochrome P450 1A1Cytochrome P450 1b1
Cytochrome P450 51
CD10 43x
Atlas Human 1.2II Atlas Human 1.2II

5/21/2018
38
Canalicular CD10 in Normal Liver
Well differentiated HCC
pCEA CD10
72 y.o. male with an 8 cm mass in non-cirrhotic liver

5/21/2018
39
HepPar-1
CD 10
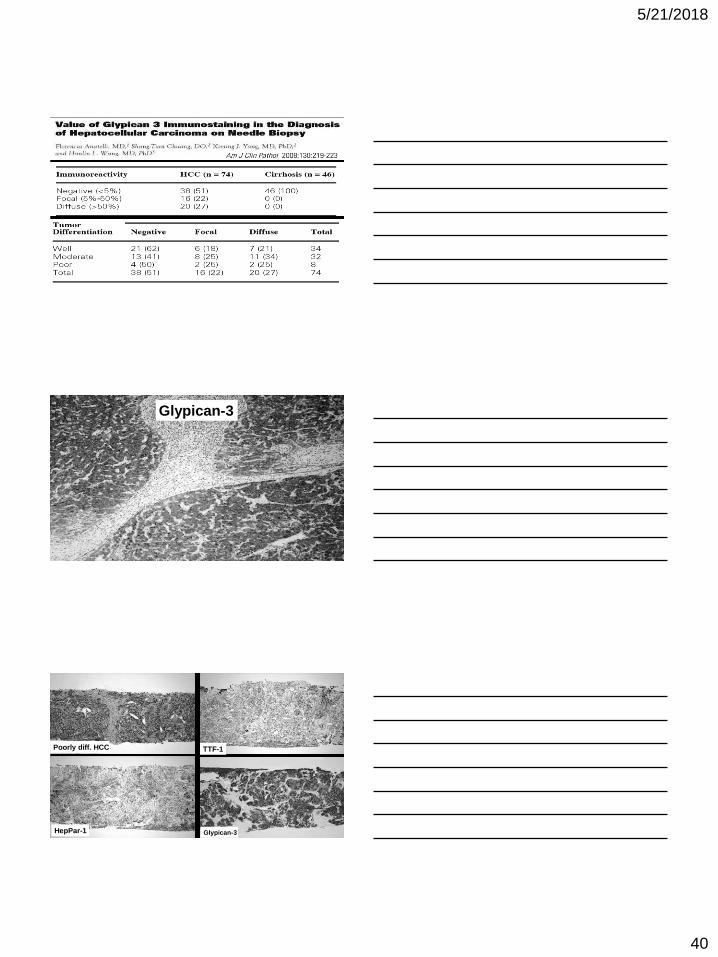
Glypican-3
• Cell surface heparin sulfate proteoglycan
• Oncofetal antigen expressed in embryonic kidney and liver
• Staining characteristics:
– Cytoplasmic reactivity; can be patchy
– Up-regulated in about 80% of HCC
– High rate of reactivity in poorly differentiated HCCs
– Also reactive in a small number of high grade DNs
– No reactivity in adenoma and FNH (& well diff HCC)
– Also reactive in Wilm’s tumor, melanoma and some ovarian carcinomas
• Small number of studies with small sample numbers
5/21/2018
40
Glypican-3
Glypican-3HepPar-1
TTF-1Poorly diff. HCC

5/21/2018
41
HepPar-1
Arg-1
UREA CYCLE
HepPar-1 Arg-1

5/21/2018
42
HepPar-1 Arginase-1

5/21/2018
43
Immunohistologic Stains for HCC
• Cam 5.2
• pCEA or CD10
• HepPar-1 or Arginase-1
• Glypican-3
• MOC-31 or mCEA (negative)
Immunohistologic Stains
for Masses in Non-Cirrhotic Liver
• Immunostains are not necessary in every case
• Polygonal cell tumors in the HCC differential diagnosis:
– Neuroendocrine (carcinoid) tumor - synaptophysin
– Melanoma – S-100, HMB-45, SOX10
– Hepatoid adenocarcinoma – Arginase-1, CDX2
– Angiomyolipoma, epithelioid type – HMB45
– Adrenocortical carcinoma – inhibin, calretinin
– Renal cell carcinoma – PAX-8
• In situ hybridization for albumin mRNA for poorly diff. tumors
• Much less useful stains: CD34, AFP, CK7, CK20