Embed Size (px)
Citation preview

Masseter muscle thickness, chewingefficiency and bite force in edentulouspatients with fixed and removableimplant-supported prostheses: a cross-sectional multicenter study
Frauke MullerMarta HernandezLinda GrutterLuis Aracil-KesslerDieter WeingartMartin Schimmel
Authors’ affiliations:Frauke Muller, Martin Schimmel, Division ofGerodontology and Removable Prosthodontics,University of Geneva, Geneva, SwitzerlandFrauke Muller, Department of Rehabilitation andGeriatrics, University Hospitals of Geneva, Thonex,SwitzerlandMarta Hernandez, Luis Aracil-Kessler, Department ofPeriodontology, Oral Surgery, Oral Medicine,University Complutense Madrid, Madrid, SpainMarta Hernandez, Dieter Weingart, Department ofMaxillofacial Surgery, Plastic Surgery and Centre ofOral Implantology, Katharinen Hospital, Stuttgart,GermanyLinda Grutter, Division of Fixed Prosthodontics andOcclusion, University of Geneva, Geneva, Switzerland
Corresponding author:Martin Schimmel, Dr Med Dent, MAS Oral BiolDivision of Gerodontology and RemovableProsthodonticsUniversity of Geneva19, Rue Barthelemy-MennCH-1205GenevaSwitzerlandTel.: þ 41 22 379 4060Fax: þ 41 22 379 4052e-mail: [email protected]
Key words: implant-supported fixed dental prostheses, implant-supported overdenture,
masseter muscle thickness, masticatory efficiency, maximum voluntary bite force, ultrasound
Abstract
Objectives: Edentulous patients may be restored with conventional dentures (C/C), implant-supported
overdentures (IOD) or implant-supported fixed dental prostheses (IFDP). Null-hypotheses: chewing
efficiency, maximum voluntary bite force (MBF) and masseter muscle thickness (MMT) are lower in
patients with C/IOD compared with the patients with bimaxillary IFDPs. Both groups perform better
than C/C and are inferior to fully dentate controls.
Material and methods: Ethical approval was obtained. For this multicenter cross-sectional study, 80
patients were recruited. Four groups of different dental states comprised of either implant-supported
prostheses (C/IOD and IFDP/IFDP) or served as control-groups (C/C and fully dentate D/D). Chewing
efficiency was assessed with a two-colour mixing ability test. MBF was measured bilaterally with a
force gauge. Two dimensional ultrasonography was used to measure MMT bilaterally.
Results: Chewing efficiency in C/IOD and IFDP/IFDP (difference NS) was better than in C/C, but not as
good as in D/D. MBF in C/IOD was lower than in IFDP/IFDP. Chewing efficiency and MBF were
significantly lower in IFDP/IFDP, who had experienced chipping or fracture of the prosthetic
superstructure. Median MMT of patients with implant-supported prostheses was between those with
C/C and fully dentate participants. There was no significant difference in MMT between C/IOD and
IFDP/IFDP.
Conclusion: Supporting complete prostheses with oral implants seems to have positive effects on the
thickness of the masseter muscle, maximum bite force as well as chewing efficiency. The type of
implant-supported prostheses may have an influence on the magnitude of the effect.
Compared with conventional complete dentures,
implant-supported overdentures (IOD) and im-
plant-supported fixed dental prostheses (IFDP)
seem to offer substantial psycho-social and func-
tional benefits to the edentulous individuals
(Feine et al. 1994a; Brennan et al. 2010). Once
all teeth are lost, the stabilization of the lower
denture with two implants placed in the inter-
foraminal region was recommended as treatment
of first choice (Thomason et al. 2009). The
improvements of orofacial functions with IOD
comprises of increased bite force (van der Bilt et
al. 2010a), larger chewing cycles, better coordi-
nation of the chewing sequence (Benzig et al.
1994) as well as improved masticatory efficiency
and ability (van Kampen et al. 2004). In addition,
they seem to provide better oral health-related
quality of life (Rashid et al. 2011) and might even
be more cost effective (Emami et al. 2009) than
conventional full dentures. Also, dental implants
seem to slow down the peri-implant alveolar
bone loss in the edentulous mandible and thus
show tertiary preventive properties (Behneke
1994).
The patient’s age and years of the edentulism
have a negative impact on the macro- and micro-
scopic structure of the chewing muscles (Raustia
et al. 1996). The cross-sectional area as well as
radiographic density of the masseter and medial
pterygoid muscle decrease with age and these
effects are significantly aggravated by edentulism
(Newton et al. 1993). In an animal model the
change from a hard to a soft texture diet reduced
the weight of the masseter muscle significantly.
Mice fed with a soft diet lost 19% of the muscle
weight within 1 week (Urushiyama et al. 2004).
Date:Accepted 31 March 2011
To cite this article:Muller F, Hernandez M, Grutter L, Aracil-Kessler L,Weingart D, Schimmel M. Masseter muscle thickness,chewing efficiency and bite force in edentulous patients withfixed and removable implant-supported prostheses: a cross-sectional multicenter study.Clin. Oral Impl. Res. 23, 2012 144–150doi: 10.1111/j.1600-0501.2011.02213.x
144 © 2011 John Wiley & Sons A/S
.;

These findings are particularly relevant for com-
plete denture wearers who often compensate the
lack of masticatory ability by changing to a softer
diet (Millwood & Heath 2000). The observed
atrophy of the muscle tissues in edentulous
patients with conventional complete dentures
may therefore be caused by a ‘‘de-training’’ effect.
Newton et al. (2004) have demonstrated that
overdentures supported by natural roots seem to
counteract atrophy of the jaw closing muscles.
For implant-supported dental prostheses evidence
on their effect on masticatory muscle atrophy
remains scarce (Schimmel et al. 2010). Also, it
remains unclear if IFDP provide better function
and show a superior effect on the macroscopic
structure of the jaw closing muscles than IOD
(Feine et al. 1994b). Such findings would under-
line the preventive value of placing fixed implant-
supported restorations rather than removable
IODs.
The aim of the study was to test the hypoth-
eses: Edentulous patients who were restored with
maxillary complete dentures and mandibular
IOD show lower masticatory efficiency (first
H0), lower maximum voluntary bite force
(MBF) (second H0) and reduced masseter muscle
thickness (MMT) (third H0) compared with pa-
tients with upper and lower IFDP.
Concerning these investigated parameters,
both implant-born reconstructions perform better
than controls with conventional complete den-
tures (fourth H0) and are inferior to volunteers
with a natural dentition (fifth H0).
Materials and methods
Approval was obtained from the ethics commit-
tees of the University Hospitals of Geneva,
Switzerland (Ref.: 08-162/Psy 08-020) and the
Medical Association of Baden-Wurttemberg,
Germany (Ref.: 2009-084-f-z). Written informed
consent was obtained before the experiments.
Subjects
For this multicenter cross-sectional study, 80
patients with similar age were recruited (four
sites: two clinics, two private practices). Inclu-
sion criteria comprised of edentulism and the
provision of maxillary complete dentures and
mandibular implant-supported overdentures (C/
IOD), upper and lower implant-supported fixed
dental prostheses (IFDP/IFDP) or conventional
complete dentures (C/C, first control-group) at
least 1 year before the experiments. Furthermore,
participants were selected to be similar in gender,
wearing period of the current prostheses and the
time of edentulism. The second control-group
(D/D) consisted of fully dentate participants.
Exclusion criteria were history of neuromuscular
disease, radiotherapy and clinically relevant TMJ
dysfunction.
Chewing efficiency
Chewing efficiency was evaluated with a pre-
viously described two-colour mixing ability test
(Schimmel et al. 2007). Commercially available
chewing gum in azure and pink colour (The Wrig-
ley Company Ltd, Plymouth, Devon, UK) served
as test food. The specimen (30 � 18 � 3mm) was
placed on the tongue and the participant was asked
to masticate the gum for 20 chewing cycles on his/
her preferred chewing side. It was then retrieved
from the oral cavity, placed into a transparent
plastic bag and flattened to a 1-mm-thick wafer.
The wafer was scanned with a flatbed scanner and
the images subsequently copied into a template of
fixed size. Using the ‘‘magic wand tool’’ and
‘‘histogram’’ function (Adobe Photoshop Elements
2.0, Adobe Systems Inc., San Jose, CA, USA) the
total number of pixels of unmixed azure colour was
evaluated and subsequently, the ratio of azure pixels
to the total pixels of the original template was
calculated (unmixed fraction [UF]).
UF shows characteristics of a logarithmic func-
tion (log10) on the base of chewing cycles and will
decrease for two reasons: a higher degree of colour
mixture (lower ratio of unmixed azure) and a
reduction in volume of the specimen due to
sweetener extraction (Schimmel et al. 2007,
2011). Both are measures for chewing efficiency
(Anastassiadou & Heath 2001; van der Bilt et al.
2010b); thus the smaller the UF, the higher is the
individual chewing efficiency.
MBF
The Occlusal Force-Meter GM 10s
(Nagano Keiki
Co. Ltd; 1-30-4 Higashimagome, Ohta-ku, To-
kyo, Japan) was utilized (Nakatsuka et al. 2006). It
is a digital force gauge with an 8.6-mm-thick bite
element. MBF was assessed bilaterally between
the upper and lower first molar. The participant
was asked to bite as hard as possible on the force
gauge, but to stop clenching when she/he started
feeling uncomfortable. The mean of six recordings
(3 � right, 3 � left) was used for analysis. Further-
more, participants with IFDP/IFDP were asked if
they had experienced a fracture of the framework
and/or chipping of the veneering material since
their prosthesis had been provided.
MMT
MMT was evaluated bilaterally with real time
ultrasound scanners (FALCO 100 [PieMedical,
Imaging BV, Maastricht, The Netherlands] or
MyLab25 [Esaote, Genova, Italy]) and linear array
transducers (6–8 or 4–13 MHz, respectively). The
two examiners (M. H., M. S.) had been calibrated
by the experienced operator, who had developed
the method (Kiliaridis & Kalebo 1991). The parti-
cipants sat upright with no head support. The
anterior border and subsequently the origin as
well as insertion of the masseter muscle were
palpated to locate the thickest part of the muscle
as site for the measurement. To avoid compression
of the muscle a generous amount of ultrasound
contact gel was applied to the probe (Kendall
Meditec, Mirandola (MO), Italy). The transducer
was oriented perpendicular to the mandibular ra-
mus to avoid oblique scanning, as this would result
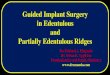
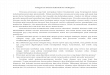
in artificially elevated readings (Fig. 1). The probe
was then tilted until the reflection of the bone was
depicted as a sharp white line. The thickest part of
the muscle close to the occlusal plane level was
measured (distance between ramus and fascia,
resolution of 0.1 mm). For MMT the mean of the
four readings in contracted muscle condition
(2 � right, 2 � left) was used for analysis. The
error of the method ranged from 0.2 to 0.4 mm
(Kiliaridis & Kalebo 1991; Botteron et al. 2009).
Statistical analysis
Categorical variables were compared using w2-
tests or Fisher’s exact test. A priori comparisons
Fig. 1. Example of an image of a masseter muscle obtained with ultrasonography. The distance between the thickest part of
the muscle between ramus mandibularis and muscle fascia (white arrow) in contracted muscle condition was used for
evaluation of masseter muscle thickness.
Muller et al �Masseter muscle thickness and bite force
© 2011 John Wiley & Sons A/S 145 | Clin. Oral Impl. Res. 23, 2012 / 144–150

between C/IOD and IFDP/IFDP were performed
using Mann–Whitney U-tests to assess the first,
second and third H0. Continuous data of all
investigated groups of different dental state were
then compared using Kruskal–Wallis tests to
investigate the fourth and fifth H0; post hoc tests
were performed with adjusted P-values for multi-
ple comparisons between groups (Siegel & Cas-
tellan 1988). Non-parametric 95% confidence
intervals (95% CI) for the difference between
medians of two groups C/IOD and IFDP/IFDP
(point estimate of shift: y¼pop2�pop1) was
computed using the Hodges–Lehmann estimates
of shift parameters. The level of significance for
type 1 errors was set at ao0.05. Hypothetical
sample size calculation was performed for type 2
errors with a power of 1�b40.9 using GnPower
3.1 (Faul et al. 2009). All statistical tests were
performed using Stata Statistical Software release
11 (Stata Corporation, College Station, TX,
USA). Figures were drawn with StatView for
Windows 5.0 (SAS Institute Inc., Carry, NC,
USA).
Results
Subjects
The four groups were not significantly different
regarding gender (P¼0.85, Fisher’s exact test),
time of edentulism (P¼0.557, Kruskall–Wallis)
and wearing period of the present prosthesis
(P¼0.334, Kruskall–Wallis) (Table 1). All pa-
tients were satisfied with their prostheses to the
degree that they did not actively seek dental
treatment.
In the C/IOD-group all participants wore max-
illary conventional complete dentures, six had
mandibular IOD with bar-attachments on four
implants, and further 14 presented with ball or
Locators
attachments on two implants. All IODs
were placed on Straumanns
implants (Basel,
Switzerland). The IFDP/IFDP-group comprised
one patient with 16 implants, 10 patients with
14 implants, six patients with 12 implants, one
patient with 13 implants, one patient with 10
implants and one patient with eight implants.
Seven patients presented with composite ve-
neered bridges and further 13 had ceramic-fused
metal prostheses. Of the 20 IFDP/IFDP patients,
13 were restored with single-unit prostheses,
whereas seven patients presented with three to
six unit restorations. Six patients had Nobel
Biocares
(Gothenburg, Sweden) and further 14
Straumanns
implants.
Chewing efficiency
Chewing efficiency as evaluated with the two-
colour mixing ability test was significantly dif-
ferent between the four groups (P¼0.0001, Krus-
kal–Wallis). The lowest chewing performance
was found in the conventional complete denture
control-group with the highest ratio of unmixed
colour and the highest efficiency in the fully
dentate control-group. The groups with im-
plant-supported restorations showed median
chewing efficiencies between the control-groups
(Fig. 2). No difference was found between C/IOD
and IFDP/IFDP (P¼0.339, Mann–Whitney,
y¼ �0.01055: 95% CI for y: [�0.0264,
0.0093]). In each of the groups with implant-
supported restorations C/IOD and IFDP/IFDP a
sample size of n¼536 (total n¼1072) would
have to be realized to demonstrate a significant
difference (a¼0.05, power¼0.9, m1¼0.05706,
m2¼0.0507, SD1¼0.028532, SD2¼0.035315,
n2/n1¼1). The dentate control-group (D/D)
showed a significantly better masticatory effi-
ciency than all other groups except for IFDP/
IFDP. The conventional complete denture wear-
ers chewed significantly less efficient than all
other groups (Fig. 3).
MBF
MBF was significantly different between groups
(P¼0.0001, Kruskal–Wallis). The lowest forces
were found in the C/C-group, the highest values
were measured in the D/D-group. The partici-
pants, who were restored with C/IOD, showed
significantly lower forces than those with IFDP/
IFDP (P¼0.0002, Mann–Whitney, y ¼118.165:
95% CI for y: [70.33, 196.84]). The IFDP/IFDP-
group showed a lower median MBF than the fully
dentate control-group, however, this difference
was not significant. The mean MBF in the C/C-
group was only 69.7% of the mean MBF in the
C/IOD-group, but again the difference was not
significant (Fig. 4).
Fracture experience in IFDP/IFDP and itsinfluence on UF and MBF
Of the 20 participants with IFDP/IFDP, 10 had
experienced a chipping of the veneering material
or fracture of the bridge framework of their
prosthetic superstructure during time in function.
The participants with such fracture occurrence
showed a significantly lower chewing efficiency
(with fracture: UF¼mean 0.074 � 0.035, with-
out fracture: UF¼mean 0.03 � 0.02, P¼0.004,
Mann–Whitney) as well as a significantly lower
MBF (with fracture: mean 176.4 � 112.57 N,
without fracture: mean 363.6 � 249.85 N,
P¼0.041, Mann–Whitney).
MMT
There was a significant difference in MMT be-
tween the four groups (P¼0.002, Kruskal–
Table 1. Descriptive of the study population: maxillary complete dentures and mandibular implant-supported overdentures (C/IOD), bimaxillary implant-supported fixed dental prostheses (IFDP/IFDP),complete full dentures (C/C), fully dentate (D/D)
C/IOD IFDP/IFDP C/C D/D
N 20 20 20 20Age (years � SD) 68.1 � 4.6 61.5 � 8.3 68.2 � 6.2 66.4 � 8Gender 9#, 11~ 8#, 12~ 6#, 14~ 8#, 12~Edentulous since (years � SD) 7.3 � 5.9 7.6 � 6.5 9 � 11.2 NAProstheses in function (years � SD) 4 � 2.6 3.89 � 2.1 3.3 � 3 NA
NA, not applicable.
0.001
0.01
0.1
10 5 10 20 30 50
log UF
Chewing cycles
C/CC/IODIFDP/IFDPD/D
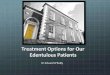
Fig. 2. Nomogram of 20 fully dentate, healthy, young adults: data taken from a previous study (Schimmel et al. 2007). The
unmixed fraction (UF) of azure colour follows an almost logarithmic function on the base of chewing cycles and is thus a
measure for chewing efficiency. A high UF correlates to a low chewing performance and vice versa. Complete denture wearers
(C/C: UF¼0.106 � 0.041, n¼20) showed the lowest and dentate participants (D/D: UF¼0.028 � 0.014, n¼20) the
highest chewing efficiency. Participants with maxillary complete dentures and mandibular implant-supported overdentures
(C/IOD: UF¼0.057 � 0.029, n¼20) were not different from participants with bimaxillary implant-supported fixed dental
prostheses (IFDP/IFDP: UF¼0.051 � 0.035, n¼20, P¼0.339, Mann–Whitney).
Muller et al �Masseter muscle thickness and bite force
146 | Clin. Oral Impl. Res. 23, 2012 / 144–150 © 2011 John Wiley & Sons A/S

Wallis). The thinnest masseter muscles were
found in the C/C-group, the thickest muscles
in the D/D-group. The results for MMT in the C/
IOD-group were statistically not different from
those in the IFDP/IFDP-group (P¼0.536, Mann–
Whitney, y¼0.3625002: 95% CI for y: [�1.075,
1.925]). To each group C/IOD and IFDP/IFDP a
sample size of n¼271 (total n¼542) would have
to be attributed in order to demonstrate a sig-
nificant difference (a¼0.05, power ¼0.9,
m1¼13.2875, m2¼13.9039, SD1¼2.07162,
SD2¼2.34623, n2/n1¼1). MMT in the two
groups with implant-supported dental prostheses
was higher than in the control-group of edentu-
lous participants with conventional full dentures,
nevertheless this result was not significant when
the P-value for significance was adjusted for
multiple comparisons between the groups (Krus-
kal–Wallis, adjusted P¼0.004). Furthermore,
MMT in the IFDP/IFDP-group were not signifi-
cantly different from those in the fully dentate
control-group (Fig. 5).
Discussion
The benefits of stabilizing complete dentures by
means of oral implants are largely documented
(Thomason et al. 2009). Fixed implant-supported
dental prostheses seem to be a valid treatment
option especially for younger patients, yet the
clinical effort and cost are considerably higher
(Feine et al. 1994a; Lambert et al. 2009). Little is
known if fixed restorations offer superior func-
tional and structural benefits to IOD (Brennan et
al. 2010, Carlsson & Lindquist 1994).
Chewing efficiency
As expected, study participants with conven-
tional full dentures showed the lowest chewing
efficiency and fully dentate ones the highest.
This result is intuitive and corresponds to evi-
dence from the literature (Manly & Braley 1950;
Ikebe et al. 2010). However, no difference be-
tween edentulous patients with C/IOD and
IFDP/IFDP was found. Statistically this may be
explained either by the absence of a difference or a
lack of power of the current study. As post hoc
power analyses are subject to controversial dis-
cussion (Thomas 1997) a hypothetical sample
size calculation, to avoid type II errors on the
basis of the current results, was performed. In
each implant-group a sample size of 536 partici-
pants would have to be included to demonstrate a
significant difference with a power of 90%. It can
thus be concluded that, if there were a difference,
it would be extremely small and of no clinical
relevance. The first null-hypothesis must there-
fore be rejected. Chewing with removable pros-
theses may be limited by a displacement or
loosening of the denture during unfavourable
loading or food getting caught underneath the
denture base. When the upper complete denture
and the posterior parts of the lower denture are
mucosa-born, chewing forces may be limited by
pain from the denture bearing tissues. Removable
denture wearers may further chew more cau-
tiously, as they may be aware that the denture
resin can fracture while chewing hard food-stuffs.
However, the total occlusal surface area is sig-
nificantly correlated with chewing efficiency
(Bourdiol & Mioche 2000); and removable den-
tures frequently replace the second molars and
restore the posterior denture teeth in their full
oro-vestibular dimension. The total occlusal sur-
face available for chewing may therefore be larger
in C/IOD than in patients with fixed reconstruc-
tions. These opposed effects may have finally
eliminated any differences in UF between C/IOD
and IFDP/IFDP participants in the present study.
Reports in the literature on the masticatory
efficiency of bimaxillary implant-supported pros-
theses are scarce. Carlsson and Lindquist com-
0
100
200
300
400
500
600
700
800
900
MB
F [
N]
[p<0.0001]
[p<0.0001]
[p=0.129]
[p<0.0001]
[p=0.0002*]
[p=0.181]
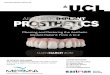
Fig. 4. Abbreviations as in Fig. 2. Box plot of maximum voluntary bite force measured in the four groups of participants.
(nMann–Whitney test for second H0, all other P-values: Kruskall–Wallis for multiple comparisons between groups, adjusted P-
value for significance: 0.004, each group n¼20, mean values with standard deviation below group descriptive.)
0
.02
.04
.06
.08
.1
.12
.14
.16
.18
.2
UF
[p=0.00006]
[p=0.0006]
[p=0.011]
[p<0.0001]
[p=0.339*]
[p=0.001]
C/IOD0.057±0.029
IFDP/IFDP0.051±0.035
C/C0.106±0.041
D/D0.028±0.014
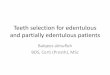
Fig. 3. Abbreviations as in Fig. 2. Box plot of unmixed fraction (UF), which is a measure for chewing efficiency. A high UF
correlates to a low chewing performance and vice versa. (nMann–Whitney test for first H0, all other P-values: Kruskall–Wallis
for multiple comparisons between groups, adjusted P-value for significance: 0.004, each group n¼20, mean values with
standard deviation below group descriptive.)
Muller et al �Masseter muscle thickness and bite force
© 2011 John Wiley & Sons A/S 147 | Clin. Oral Impl. Res. 23, 2012 / 144–150

pared in a 10 year follow-up study patients with
maxillary complete dentures/mandibular IFDP to
those with bimaxillary IFDP. In their study, no
difference in masticatory efficiency between
those two groups was found which is in agree-
ment with the results of the current study.
Interestingly, the subjective perception of masti-
catory function was significantly higher in pa-
tients with bimaxillary IFDP, so that the gain for
such treatment may mainly be psychological
(Carlsson & Lindquist 1994).
MBF
Albeit a similar chewing efficiency, in the pre-
sent study MBF was significantly lower in parti-
cipants with C/IOD than with IFDP/IFDP. Both
groups lack periodontal receptors in the surround-
ings of the dental implants and subsequently
projections on the primary sensory and motor
cortex (Abarca et al. 2006). But in contrast to the
fixed restorations the C/IOD provide a close
contact of the denture base with the underlying
mucosa. Previous experiments with complete
dentures showed, that a good retention of a lower
denture and thus an intimate contact between
the denture base and the denture bearing tissues
allows for a higher inter-occlusal tactile sensitiv-
ity than in edentulous patients with poor lower
denture retention (Muller et al. 1995). It is likely
that the quantity and/or quality of stimuli to the
mechanoreceptors in the mucosa account for this
finding. The higher MBF in patients restored
with IFDP/IFDP may therefore be related to a
reduced peripheral input, which is necessary to
tune muscle force during oral function. Harald-
son (1983) reported that the reduction of muscle
force during a chewing sequence along with the
softening of the food bolus was less in patients
with fixed implant-bridges than in dentate indi-
viduals. There seems to be unique activation
patterns of the jaw closing muscles in patients
with oral implants which implies a less graduated
contraction of the jaw closing muscles if biting is
performed on implant-supported prostheses
(Gartner et al. 2000). In the current study, the
fixed implant-supported dental restorations var-
ied with regard to the number of implants and
type of the superstructures used. This implies
differences in the total implant–bone contact
surface between the patients who might have
influenced the inter-occlusal perception and con-
sequently the fine motor control. If osseopercep-
tion is caused by vibration (Klineberg et al. 2005),
the different damping characteristics of the ve-
neering materials (ceramic/composite) would
have influenced the results.
Although in the current study MBF in patients
with C/IOD proved higher than patients with
conventional full dentures, the difference was not
significant which contrasts with previous find-
ings reported in the literature (van der Bilt et al.
2010a). This result may be related to the applied
measuring technique as MBF was assessed uni-
laterally with an 8.6-mm-thick gauge. The use of
thinner pressure sensitive foils would have re-
duced the gape and allowed for higher MBF in
both groups (Proschel et al. 2008). Higher forces
might have possibly accentuated a possible dif-
ference in MBF between the C/C and C/IOD
groups.
A further interesting finding is the discrepancy
in chewing efficiency and MBF between partici-
pants who experienced a fracture of their fixed
dental prostheses and those who did not. These
fractures may have resulted from an impaired
mechanosensation with IFDP/IFDP (Luraschi
2009) and consequently a poor motor control
(Trulsson & Gunne 1998). Another possible ex-
planation would be technical shortcomings of the
reconstructions as clear differences in fracture
prevalence had occurred between the different
centres. Thus particular attention should be
paid to technical execution and occlusion of
implant-supported prostheses. Patients might
have also lost confidence in the durability of
their IFDPs and consequently avoided applying
maximum forces when asked during the experi-
ments; a presumption confirmed qualitatively by
several participants with fracture experience.
MMT
In the current study, MMT was assessed with
ultrasound as described by Kiliaridis & Kalebo
(1991). The method shows only small errors (in
contracted muscle condition 0.2–0.4 mm), does
not use electromagnetic radiation like computed
tomography and does not necessitate supervision
and interpretation of a specialist radiologist. For
this multicenter study, which also included pa-
tients from private practice an added advantage
was the portability of the ultrasound equipment.
Although atrophy of the masseter and medial
pterygoid muscles related to age and edentulism
is well documented (Newton et al. 1993), there is
little evidence on the morphological effects of
dental prostheses on the masticatory muscles.
Newton et al. (2004) had demonstrated that the
retention of natural roots covered by overdentures
was associated with less atrophied chewing mus-
cles than in subjects with conventional full den-
tures. Schimmel et al. (2010) had described the
case of a patient who had regained MMTafter the
stabilization of the lower denture with two im-
plants. The current study demonstrated, with the
conceptual limitations of any cross-sectional
study, the positive structural effects of mastica-
tory muscles of implant placement in edentulous
patients. Because of the cross-sectional study
design, it remains unclear if the placing of im-
plants prevented atrophy of the masseter muscles
or if the patients regained muscle mass through
improved function.
Prolonged low activity of muscles will result in
atrophy both on a macroscopic and microscopic
level. Consequently, the cross-sectional area of
the masticatory muscles is reduced in edentulous
8
10
12
14
16
18
20
22
MM
T [
mm
]
C/IOD13.29±2.07
IFDP/IFDP13.90±2.35
C/C11.98±1.84
D/D15.05±2.68
[p=0.011]
[p=0.021]
[p=0.082]
[p<0.0001]
[p=0.536*]
[p=0.043]
Fig. 5. Abbreviations as in Fig. 2. Box plot of masseter muscle thickness measured in the four groups of different dental state.
(nMann–Whitney test for third H0, all other P-values: Kruskall–Wallis for multiple comparisons between groups, adjusted P-
value for significance: 0.004, each group n¼20, mean values with standard deviation below group descriptive.)
Muller et al �Masseter muscle thickness and bite force
148 | Clin. Oral Impl. Res. 23, 2012 / 144–150 © 2011 John Wiley & Sons A/S

patients compared with dentate subjects, regard-
less of their age (Newton et al. 1993), a finding
that was confirmed by the current study. Also,
the radiographic density of these muscles is
reduced after a long wearing time of conventional
full dentures (Raustia et al. 1996). On a micro-
scopic level ageing muscle tissue shows a de-
creased fibre diameter, a degenerated sarcoplasm
and a replacement of muscle fibres by fat and
connective tissue (Larsson 1995). Temporal mus-
cle type II fibres in denture wearers, who rate
their dentures as insufficient, are smaller than
the corresponding fibres in the dentate patients
(Ringqvist 1974). She suggested that the low
percentage and small size of these fibres in
denture wearers might be attributed to reduced
functional demands. The described studies may
only in part explain the age- and function-related
changes in the masticatory muscles. Findings
from other muscles may not apply to the chewing
muscles as their functioning, their embryo-ge-
netic origin and the fibre composition are unique
in the human body (Monemi et al. 1998).
Edentulous patients benefit from an improved
muscle activity by stabilizing the lower denture
with two implants, but there seems to be no
further improvement of these parameters by
providing bimaxillary IFDPs (Ferrario et al.
2004; Heckmann et al. 2009). The current study
confirmed these results on a morphological level.
The third null-hypothesis must be rejected, as
MMT between the two implant-groups was not
statistically different. Patients with implant-sup-
ported dental prostheses showed thicker masseter
muscles than edentulous patients with conven-
tional full dentures, although the result was no
longer significant when the statistical test was
corrected for multiple comparisons between
groups.
Summary and conclusion
Although the stabilization of conventional man-
dibular dentures with dental implants improves
chewing efficiency significantly, the effect might
not be improved further by providing edentulous
patients with bimaxillary implant-supported
fixed prostheses.
A fracture experience with the dental recon-
struction may limit the functional benefit.
In edentulous patients, supporting or stabiliz-
ing dental prostheses by placing oral implants
seems to have positive effects on the training
level and dimension of the masseter muscle.
The type of implant prostheses may have an
influence on the magnitude of the effect. The
functional advantages of implant reconstructions
and their tertiary preventive properties on the
masseter muscle should be considered in treat-
ment planning.
Acknowledgements: The study was
supported by the ITI Foundation (grant no.
552_2008). The contributions of Prof Dr Jean-
Pierre Bernard, Prof Dr Urs Belser and Dr
German Gallucci (University of Geneva,
Switzerland), Dr Manfred Imsand (Sion,
Switzerland), Dr Kamel Salem (Morges,
Switzerland), Leonard Brazzola (Lausanne,
Switzerland) and the staff of the Divisions of
fixed and removable Prosthodontics of the
University of Geneva to the clinical care and
recruitment of study participants is greatly
acknowledged. Furthermore the authors want
to express their gratitude to Priv. Doc. Dr
Francois R Herrmann, MPH (University
Hospitals of Geneva, Switzerland) for his help
with the statistical analysis. Thanks are also
due to Prof Dr Stavros Kiliaridis (University of
Geneva, Switzerland) for teaching the
ultrasound method and calibrating the two
examiners of the study.
References
Abarca, M., Van Steenberghe, D., Malevez, C. & Jacobs,
R. (2006) The neurophysiology of osseointegrated oral
implants. A clinically underestimated aspect. Journal
of Oral Rehabilitation 33: 161–169.
Anastassiadou, V. & Heath, M.R. (2001) The develop-
ment of a simple objective test of mastication suitable
for older people, using chewing gums. Gerodontology
18: 79–86.
Behneke, N. (1994) Klinische Erfahrungen mit enossa-
len Implantaten im zahnlosen Unterkiefer. Dr Med
Dent Habil Thesis, Johannes Gutenberg-University,
Mainz, Germany.
Benzig, U., Weber, H., Simonis, A. & Engel, E. (1994)
Changes in chewing patterns after implantation in the
edentulous mandible. The International Journal of
Oral & Maxillofacial Implants 9: 207–213.
Botteron, S., Verdebout, C.M., Jeannet, P.Y. & Kiliar-
idis, S. (2009) Orofacial dysfunction in Duchenne
muscular dystrophy. Archives of Oral Biology 54:
26–31.
Bourdiol, P. & Mioche, L. (2000) Correlations between
functional and occlusal tooth-surface areas and food
texture during natural chewing sequences in humans.
Archives of Oral Biology 45: 691–699.
Brennan, M., Houston, F., O’Sullivan, M. & O’Connell,
B. (2010) Patient satisfaction and oral health-related
quality of life outcomes of implant overdentures and
fixed complete dentures. The International Journal of
Oral & Maxillofacial Implants 25: 791–800.
Carlsson, G.E. & Lindquist, L.W. (1994) Ten-year long-
itudinal study of masticatory function in edentulous
patients treated with fixed complete dentures on
osseointegrated implants. International Journal of
Prosthodontics 7: 448–453.
Emami, E., Heydecke, G., Rompre, P.H., de Grand-
mont, P. & Feine, J.S. (2009) Impact of implant
support for mandibular dentures on satisfaction, oral
and general health-related quality of life: a meta-
analysis of randomized-controlled trials. Clinical
Oral Implants Research 20: 533–544.
Faul, F., Erdfelder, E., Buchner, A. & Lang, A.G. (2009)
Statistical power analyses using Gnpower 3.1: tests for
correlation and regression analyses. Behavior Re-
search Methods 41: 1149–1160.
Feine, J.S., de Grandmont, P., Boudrias, P., Brien, N.,
LaMarche, C., Tache, R. & Lund, J.P. (1994a)
Within-subject comparisons of implant-supported
mandibular prostheses: choice of prosthesis. Journal
of Dental Research 73: 1105–1111.
Feine, J.S., Maskawi, K., de Grandmont, P., Donohue,
W.B., Tanguay, R. & Lund, J.P. (1994b) Within-
subject comparisons of implant-supported mandibular
prostheses: evaluation of masticatory function. Jour-
nal of Dental Research 73: 1646–1656.
Ferrario, V.F., Tartaglia, G.M., Maglione, M., Simion,
M. & Sforza, C. (2004) Neuromuscular coordination
of masticatory muscles in subjects with two types of
implant-supported prostheses. Clinical Oral Im-
plants Research 15: 219–225.
Gartner, J.L., Mushimoto, K., Weber, H.P. & Nishi-
mura, I. (2000) Effect of osseointegrated implants
on the coordination of masticatory muscles: a
pilot study. Journal of Prosthetic Dentistry 84:
185–193.
Haraldson, T. (1983) Comparisons of chewing patterns
in patients with bridges supported on osseointegrated
implants and subjects with natural dentitions. Acta
Odontology Scandinavica 41: 203–208.
Heckmann, S.M., Heussinger, S., Linke, J.J., Graef, F.
& Proschel, P. (2009) Improvement and long-term
stability of neuromuscular adaptation in implant-
supported overdentures. Clinical Oral Implants Re-
search 20: 1200–1205.
Ikebe, K., Matsuda, K., Murai, S., Maeda, Y. & Nokubi,
T. (2010) Validation of the Eichner index in relation to
occlusal force and masticatory performance. Interna-
tional Journal of Prosthodontics 23: 521–524.
Kiliaridis, S. & Kalebo, P. (1991) Masseter muscle
thickness measured by ultrasonography and its rela-
tion to facial morphology. Journal of Dental Research
70: 1262–1265.
Klineberg, I., Calford, M.B., Dreher, B., Henry, P.,
Macefield, V., Miles, T., Rowe, M., Sessle, B. &
Trulsson, M. (2005) A consensus statement on osseo-
perception. Clinical and Experimental Pharmacology
and Physiology 32: 145–146.
Lambert, F.E., Weber, H.P., Susarla, S.M., Belser, U.C.
& Gallucci, G.O. (2009) Descriptive analysis
of implant and prosthodontic survival rates with
fixed implant-supported rehabilitations in the
edentulous maxilla. Journal of Periodontology 80:
1220–1230.
Larsson, L. (1995) Motor units: remodeling in
aged animals. The Journals of Gerontology Series A:
Biological Sciences and Medical Sciences 50:
91–95.
Muller et al �Masseter muscle thickness and bite force
© 2011 John Wiley & Sons A/S 149 | Clin. Oral Impl. Res. 23, 2012 / 144–150

Luraschi, J. (2009) Mechanosensation in totally edentu-
lous persons rehabilitated by means of implant-sup-
ported fixed dental prostheses. Dr Med Dent, Thesis,
University of Geneva, Geneva, Switzerland.
Manly, R.S & Braley, L. (1950) Masticatory perfor-
mance and efficiency. Journal of Dental Research
29: 448–462.
Millwood, J. & Heath, M.R. (2000) Food choice by older
people: the use of semi-structured interviews with
open and closed questions. Gerodontology 17: 25–32.
Monemi, M., Eriksson, P.O., Eriksson, A. & Thornell,
L.E. (1998) Adverse changes in fibre type composition
of the human masseter versus biceps brachii muscle
during aging. Journal of the Neurological Sciences
154: 35–48.
Muller, F., Link, I., Fuhr, K. & Utz, K.H. (1995) Studies
on adaptation to complete dentures. Part ii: oral
stereognosis and tactile sensibility. Journal of Oral
Rehabilitation 22: 759–767.
Nakatsuka, K., Usui, T., Masuda, Y., Rugh, J. &
Kurihara, S. (2006) Accuracy and repeatability of the
GM10 occlusal force-meter. Nihon Kyosei Shika
Gakkai Taikai Puroguramu, Shorokushu 65: 336.
Newton, J., Yemm, R., Abel, R. & Menhinick, S. (1993)
Changes in human jaw muscles with age and dental
state. Gerodontology 10: 16–22.
Newton, J.P., McManus, F.C. & Menhenick, S. (2004)
Jaw muscles in older overdenture patients. Gerodon-
tology 21: 37–42.
Proschel, P.A., Jamal, T. & Morneburg, T.R. (2008)
Motor control of jaw muscles in chewing and in
isometric biting with graded narrowing of jaw gape.
Journal of Oral Rehabilitation 35: 722–728.
Rashid, F., Awad, M.A., Thomason, J.M., Piovano, A.,
Spielberg, G.P., Scilingo, E., Mojon, P., Muller, F.,
Spielberg, M., Heydecke, G., Stoker, G., Wismeijer,
D., Allen, F. & Feine, J.S. (2011) The effectiveness of
2-implant overdentures – a pragmatic international
multicentre study. Journal of Oral Rehabilitation 38:
176–184.
Raustia, A.M., Salonen, M.A. & Pyhtinen, J. (1996)
Evaluation of masticatory muscles of edentulous
patients by computed tomography and electromyo-
graphy. Journal of Oral Rehabilitation 23: 11–16.
Ringqvist, M. (1974) A histochemical study of temporal
muscle fibers in denture wearers and subjects with
natural dentition. Scandinavian Journal of Dental
Research 82: 28–39.
Schimmel, M., Christou, P., Herrmann, F. & Muller, F.
(2007) A two-colour chewing gum test for mastica-
tory efficiency: development of different assessment
methods. Journal of Oral Rehabilitation 34: 671–
678.
Schimmel, M., Leemann, B., Herrmann, F.R., Kiliar-
idis, S., Schnider, A. & Muller, F. (2011) Masticatory
function and bite force in stroke patients. Journal of
Dental Research 90: 230–234.
Schimmel, M., Loup, A., Duvernay, E., Gaydarov, N.
& Muller, F. (2010) The effect of lower denture
abstention on masseter muscle thickness in a 97
year-old patient: a case report. International Journal
of Prosthodontics 23: 418–420.
Siegel, S. & Castellan, N.J. (1988) Nonparametric
Statistics for the Behavioral Sciences. Singapore:
McGraw-Hill.
Thomas, L. (1997) Retrospective power analysis. Con-
servation Biology 11: 276–280.
Thomason, J.M., Feine, J., Exley, C., Moynihan, P.,
Muller, F., Naert, I., Ellis, J.S., Barclay, C., Butter-
worth, C., Scott, B., Lynch, C., Stewardson, D.,
Smith, P., Welfare, R., Hyde, P. & McAndrew, R.
(2009) Mandibular two implant-supported overden-
tures as the first choice standard of care for edentulous
patients-the York consensus statement. British Den-
tal Journal 207: 185–186.
Trulsson, M. & Gunne, H.S. (1998) Food-holding
and -biting behavior in human subjects lacking
periodontal receptors. Journal of Dental Research
77: 574–582.
Urushiyama, T., Akutsu, S., Miyazaki, J., Fukui, T.,
Diekwisch, T. & Yamane, A. (2004) Change from a
hard to soft diet alters the expression of insulin-like
growth factors, their receptors, and binding proteins in
association with atrophy in adult mouse masseter
muscle. Cell and Tissue Research 315: 97–105.
van der Bilt, A., Burgers, M., van Kampen, F.M. &
Cune, M.S. (2010a) Mandibular implant-supported
overdentures and oral function. Clinical Oral Im-
plants Research 21: 1209–1213.
van der Bilt, A., Mojet, J., Tekamp, F.A. & Abbink, J.H.
(2010b) Comparing masticatory performance and
mixing ability. Journal of Oral Rehabilitation 37:
79–84.
van Kampen, F.M., van der Bilt, A., Cune, M.S.,
Fontijn-Tekamp, F.A. & Bosman, F. (2004) Mastica-
tory function with implant-supported overdentures.
Journal of Dental Research 83: 708–711.
Muller et al �Masseter muscle thickness and bite force
150 | Clin. Oral Impl. Res. 23, 2012 / 144–150 © 2011 John Wiley & Sons A/S