Embed Size (px)
Citation preview

Nachreiner 1
Matthew Nachreiner
Professor Konan
Economic Theory of Healthcare
13 December 2016
Public v. Private Health Exchange Models
Abstract
The research looks at the effectiveness and responses to the creation of public health
exchanges implemented as part of Affordable Care Act (ACA) to help control expenses and
make healthcare portable for individuals (not employer dependent). The Obama Administration
implemented ACA that allowed consumers to buy health insurance plans on a public health
exchange independent of their employer with government subsidies available for lower income
participants. In response some employers have moved to private health exchanges offered from
the private sector that operates on two platforms single carrier and multi-carrier. The goal of the
research is to show overall efficiency in terms of the consumer and producer for both types of
health exchanges. It has been concluded that the majority of public health exchange models are
inefficient for both the consumer and health insurance companies. There have been many
negative externalities due to Obamacare with only Cover California being the shining light. The
ACA needs serious reform and lawmakers should look at Cover California as a successful case
study for the public health exchange. The private health exchange has experienced significant
growth, but needs to provide information more efficiently and transparently to consumers in
order to meet and sustain growth rates. In addition, the private health exchange needs to aid
insurance companies to alter their business model to fit the exchange. It is important to note that
part of this research may be irrelevant in the upcoming years as Trump’s administration1 and
Republican dominated Congress has vowed to repeal or make major amends to ACA.
1 For example, Oscar Insurance Corp. built its business around on the ACA and finds itself expecting to fall short of
its 2017 projections due to the uncertainty of what the current administration (Trump and the Republicans) will do
for health reform. In 2014, 23 nonprofits cooperatives were tied to the ACA, now only 6 are offering plans in the
ACA marketplaces (Winkler and Mathews).

Nachreiner 2
Introduction
In 2012, the ACA was passed to address the following issues:
1. The Congressional Budget Office (CBO) estimated that 65 million Americans under the
age of 55 lacked health insurance (CBO)
2. Health care spending represented 17.9% of GDP – the highest in the industrialized world
(Folland 5).
3. The costs to families and employers doubled from 2001 to 2011 (Obamacare Facts).
4. The US ranks 24th in health outcomes among the 30 OECD countries despite the high
costs of care (National Research Council).
Public health exchanges were touted as a key component of the program by providing a
marketplace for all Americans to find affordable health insurance. At the time, many even
envisioned a point in the distant future where most insurance would move through a public
exchange.
Health exchanges emerged in the private sector in the 1980’s using computer networking
to integrate claims management, eligibility verification, and inter-carrier payments. They became
popular in some parts of the country with small and medium-sized companies because it allowed
them to offer more cost-effective insurance to their employees.
President Obama promoted the health insurance exchange concept as a key part of the
ACA. As part of the ACA, each state was required to develop a health exchange. If a state chose
not to develop an exchange, they would be required to use the federal exchange. For 2017, we
will have 16 state run exchanges and 34 exchanges run by the federal government or as a state-
federal government partnership (Obamacare Facts).
At the launch of the ACA, the CBO projected 21 million Americans would be using the
exchanges by 2016. For 2016, 13 million Americans will use the exchanges (“History and
Timeline of the Affordable Care Act (ACA)”). Also, three of the largest insurance carriers
Aetna, United Healthcare and Humana pulled out of the exchanges. ACA-supporters argue that
more people are employed than projected, and they are using private insurance plans. For those

Nachreiner 3
critical of ACA, they are arguing that the exchanges are ineffective. In addition, the costs on the
public exchange are expected to rise significantly in 2017 – a CNN report projected increases
between 16-25% after moderate increases of 2.5% in 2014 and 7.5% in 2015 (Jost).
Thesis:
In the Spring of 2010, President Obama mandated ACA (Affordable Healthcare Act) by
issuing Executive Order 13535 (The White House). As a result, the public health exchange was
created. To date, the public exchanges have primarily provided coverage to low income
Americans at a high cost, and private exchanges have emerged as a viable alternative. I believe
that we can build upon these developments and involve the insurance industry in the debate to
significantly improve the outcomes. The public health exchange needs to develop programs to
replicate Cover California throughout the country and continually improve the IT infrastructure.
The private health exchanges have become a solid platform that needs to transfer information
more efficiently and transparently to consumers in order to sustain and meet growth
expectations. Furthermore, I believe that the private health exchange needs to be more
accommodating to insurance companies to gain their commitment to the private exchanges. Also,
I recommend that federal subsidies be made available through private exchanges breaking the
subsidy monopoly of the public exchange. Finally, the insurance industry must be part of the
solution participating in exchanges and developing lower cost business models to serve this
market using examples from California insurance companies. Regardless of Trump’s
Administration impact, both health exchange models need to improve by learning from past
mistakes, involve insurers, while building upon their successes.
Public Health Exchange Model

Nachreiner 4
During the 2008 election, the general population was frustrated with soaring costs of
healthcare and stagnant wages leaving many uninsured or underinsured. Obama proposed a
mixed public-private group insurance to reform the infrastructure of the healthcare industry.
After winning the presidency, Obama passed the Affordable Care Act (ACA) as an Executive
Order in 2010 amidst controversy with Republicans. The ACA was aimed to cut down on the
costs of healthcare, increase the number of insured Americans, and quality of care. There were
many new important benefits, rights, and protections that were introduced within the ACA. The
creation of a public health exchange was offered as a centerpiece to the legislation to create an
avenue for coverage to more Americans and as a vehicle to lower costs with an intent to attract
employers and insurance carriers. The public exchange in each state was given a monopoly in
providing federally mandated insurance subsidies.
The Public Health Exchange Model has four potential different ways to operate, two on
federal and state level. The two state level public health exchange models serve as an active
purchaser and clearinghouse of policies. The active purchaser model is where the state “directly
negotiates with insurers over premiums, doctor networks, benefits and other aspects of plans sold
in the marketplace” (Kardish). The clearinghouse model “establishes basic criteria and allows
any plan that meets those benchmarks to be sold in the marketplace” (Kardish). The two federal
level public health exchange models are the federal partnership exchange and federally
facilitated exchange model. The federal partnership exchange model runs the web site where
individuals purchase insurance, but the state exercises some control over plan management or
consumer outreach. (Kardish). The federally facilitated exchange model “operates all major
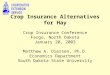
functions of the exchange” (Kardish). Figure 1 displays the types of exchanges active in each

Nachreiner 5
state. In addition, the two different state level health exchange models are differentiated in the
figure.
Figure 1 (Kaiser Family Foundation: 2013)
Negative Externalities (Poorly Executed IT Infrastructure and Majority of Insurance
Companies Leaving Market Leaving Little to No Competitions)
The Obama Administration encouraged states to develop their own homegrown public
exchanges with the intent that each state would be able to offer solutions specific to their local
environment. Many states decided to not create their own public health exchanges because of
political spite or difficulties associated with building complex technical infrastructure of an
exchange. And this proved true as the Obama Administration spent over $150 million in costs to
fix the initial version of the federal public health exchange (Baker). The IT infrastructure wasn’t

Nachreiner 6
ready for the scale of site traffic, but it was quickly fixed. And for the states that built
homegrown public health exchanges provided mixed results. For instance, Oregon decided to
build their own public health exchange, Cover Oregon and enlisted Oracle as a provider. The
plan was to open on Oct 1, 2013 coinciding with open enrollment for the entire nation. However,
consumers were left disappointed and upset because the website failed to work due to technology
problems. This left Oregon and its citizens in a bind to find a solution. Thus, Oregon decided to
hire and train officials to help its citizens manually sign up under ACA. To comply with the law,
Oregon made the decision to move Cover Oregon under the federal run public health exchange at
an estimated cost of $4-6 million (Manning). This created a large scale inefficiency in the State
of Oregon as many eligible enrollees were unable to sign up. After a lengthy trial due to lawsuits
between the state of Oregon2 and Oracle, it was decided that Oracle would pay the state of
Oregon $100 million (Manning). Across the US, we saw states bearing excessive costs to set up
the exchanges and individuals unable to obtain subsidized health care.
The public health exchange faces problems in many states that utilize the two federal-run
models. Insurance companies are taking heavy losses as they are forced to provide insurance for
high cost, unhealthy consumers as well as losing premiums for individuals who would rather pay
a penalty than a premium. In other words, the risk pool is heavily out of balance biased towards
riskier consumers that are more expensive to insure. As a result, the insurance company, Aetna,
has sustained $430 million of losses in these exchanges as of August 15, 2016 (Luhby).
Additionally, Aetna traditional products that target employers who focus on choice and demand
aren’t successful for this set of consumers in the public health exchange. Furthermore, only 15%
2 I worked for a free clinic that provided basic healthcare and gave referrals to the uninsured, gap-coverage,
underinsured, homeless, and undocumented workers in the summer of 2014 and 2015. I witnessed first-hand the
problems that the patients were encountering and saw that the website couldn’t handle a lot of traffic. To help our
patients get on Cover Oregon, we had to refer them to an official that would manually enroll them in the program.

Nachreiner 7
of insurance companies ran profitable individual division in 2015 according to McKinsey’s
Center for Health Reform (Luhby). These companies face a dilemma to either leave the market,
restrict their coverage to consumers leading to potential lawsuits, or raise their rates. Several of
the largest insurance companies such as United Health, Humana and Aetna have exited the
public exchanges. As a result, the market has significantly less competition which has led to
large increases in 2017 quoted rates on the public exchanges, and, in some cases, no insurance
options for some small counties. For example, Arizona represents the most extreme example,
where Pinal County has no insurance company selling on the exchange. This leaves the
consumer to switch insurance multiple times to attain any coverage, devote time to the searching
process, and choose from a limited pool of plans.
Model to Fix Problems
The most successful model for a public health exchange has been the active purchase
model. California’s public health exchange, Cover California, serves as a case study. Cover
California is unique in that it requires all health plans to be standardized, which means that all
plans must have the same benefits. The only difference between plans are premiums, drug
formularies (covered drug lists), and provider networks. Insurance carriers who fail to comply to
Cover California’s requirements are not allowed to engage in the exchange. Aggressive
negotiations between Cover California and carriers has led to a competitive market. In addition,
Cover California has implemented policies that quell the insurer concerns about profitability and
insuree concerns about limited care. For example, monthly prescription costs force the insuree to
reach their maximum out of pocket exposure quickly and insurer’s requests for rate increases are
approved by the state to avoid losses by the insurers. This causes significant inefficiency and
volatility in the market. Thus, Cover California has capped monthly prescription costs for plans

Nachreiner 8
that are in and out of the exchange to increase and stabilize the market. This helps quell both the
insuree and insurer’s concerns. Cover California’s strategy has led to 1.42 million enrollees in
2016 and projected 13.2% increase in enrollment for 2017 (Luhby).
In addition to a successful public exchange example, Molina Insurance (based in
California) illustrates how insurance providers can be profitable in the public exchange model.
By offering narrow networks of doctors, hospitals and providers and implementing rigorous
administrative cost controls, Molina is able to profitably provide low cost care while also
providing high service levels through case workers who proactively work with individuals on
prevention strategies. For example, Molina doesn’t allow its policy holders access to a
prestigious Los Angeles Hospital (Cedars-Sinai Medical Center) to help keep rates low (Luhby).
Molina is successful on the cases provided by the public exchange as it is closely related to their
core Medicaid business. Ironically, the decision by the large insurance providers to exit the
public exchanges will place an increasing burden on players like Molina as they are forced to
handle more high risk cases. Molina is preparing for the challenge and has raised rates to offset
the impact. Although margins are low, Molina remains confident that it will continue to be
profitable and grow through their low cost model (Luhby).
Private Health Exchange Model
Traditionally, employers delivered health benefits to its employees via defined benefits
model. Through this model, the employer would control the type of coverage that the employee
would receive. Thus, the majority of the financial burden and healthcare costs fell on the
employer. In addition, it was time consuming and an additional administration expense in finding
the cheapest, most effective benefit plan to offer to their employees.

Nachreiner 9
The ever-rising health expenditures have increased the costs incurred to the employers,
where it has altered their behavior. In order to minimize their costs, employers have opted to
delivering health benefits to is employees via defined contribution model. This model allows the
employer to “make cash contributions to savings accounts that employees use to purchase
insurance products of their choice. This model allows the company to cap its healthcare cost at a
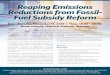
desired threshold, improving control of current expenses and future liabilities” (Kapur). Figure 2
demonstrates the different agents involved in the private health exchange. The private health
exchange platforms serve as an online marketplace for employees to browse through the
different health insurance plans. There are two type of private health exchange platforms: Single
Carrier and Multi-Carrier.
Figure 2 (Source: Kapur:2012)
Strategy & research surveyed 500 employers and 300 individuals concerning private exchanges.
The research is summarized below:

Nachreiner 10
80% of employers would prefer to purchase from a private exchange vs. a public
exchange due to design flexibility, customer service, and a wariness of government.
More than 50% would prefer a multi-carrier exchange
Employers favored a defined contribution plan yet less than 20% plan on moving to that
type of plan
Lower-income individuals gravitate towards the public exchanges to take advantage of
subsidies
Individuals want a “guided purchase experience” with plan and product recommendations
based on needs
Individuals expressed a strong desire for real-time administrative support which is not
available on public exchanges
Individuals did not have brand preferences for particular insurance providers (Kapur)
Single Carrier
The single carrier private health exchange platform is operated by an insurance carrier
that allows employees/employers to work with that one insurance carrier. For example, Blue
Cross/Blue Shield, most likely creates a group product for an employer. The single carrier model
is very similar to the current practice of employers providing coverage and administrative
support. With the single carrier model, the administrative burden is shifted to the insurance
provider. With a single carrier model, the employees are limited to the choices provided by the
single carrier (Kapur).
Multi-Carrier
The multi-carrier private health exchange platform is operated by a 3rd party that allows
employees/employers to browse through insurance products from many different insurance
carriers. Most of the products are individual and allows for personalization. For example, AON
Hewitt, essentially works as a middle man. They create the infrastructure for the exchange,
obtain insurance plans from many different carriers, and then work with employers to modify the
exchange to their employees. This model allows the employer to be passive in their involvement
and have relatively low administrative burden due to outsourcing their work to a 3rd party. As a

Nachreiner 11
result, the employers avoid devoting time to develop relationships with insurance companies and
analyzing the health plans. This helps streamline their operations (Kapur).
Relative Uncertainty for Consumers and Insurance Companies
Many employers prefer the private health exchange compared to the public health
exchange, but remain hesitant to engage in either the single or multiple carrier channels for a
multitude of reasons. As the private exchanges are relatively a new business model, employers
remain cautious because there is limited data regarding the efficiency and quality of the
exchanges. Furthermore, the different channels (single and multi-carrier) need to educate
employers on the operations and benefits of the private health exchange. As a result, the
employers have not fully embraced private exchanges due to concerns over competitiveness and
longevity. Finally, many employers are concerned about the future of health reform and prefer to
stay with status quo.
As with employers, insurance companies are still trying to come to terms with how the
private health exchange operates and how they fit into the model. The different channels have
forced these insurance companies to become business to consumer models as opposed to their
current business to business models. The insurance providers are especially nervous about the
multi-carrier exchanges as the insurance companies are trying to understand how outsourcing
their plans to a 3rd party platform will alter their profit margins. Furthermore, the multi-carrier
channel typically does not allow the insurance companies to have a direct relationship with
consumers and effectively limits their ability to cross-sell, up-sell, and retain customers. As a
result, the 3rd party will have the ability to control the sales and marketing process. For the single
carrier exchanges, insurance companies are coming to terms with increasing their customer
support to help consumers pick coverages/products. Due to increasing demand, the private health

Nachreiner 12
exchanges will force these insurance companies to engage in the exchange sooner or later. Figure
3 shows a decision making framework for insurance companies on how to enter the private
health exchange.
Figure 3 (Source Kapur:2012).
Summary and Conclusion
The public health exchanges were created when Affordable Care was mandated by
Executive Order in the Spring of 2010. Although the public exchanges have not realized initial
projections, they have provided more healthcare for lower income Americans and sparked
changes in the insurance industry that will bring more choices to consumers. As a positive
example, California has led the country. Cover California stands out as a clear best practice in
creating solutions for low cost healthcare and running public health exchanges. Another
important development is that private health exchanges have become increasingly popular and
bring important competition to the marketplace. To thrive, the private health exchanges will need
to develop marketing communication to educate employers and consumers on the benefits of the

Nachreiner 13
exchanges. The private health exchanges will also need to partner with insurance providers to
gain their participation. Finally, I am recommending that we bring the insurance industry into the
debate to help provide solutions. In particular, the insurance companies need to develop business
to consumer models and fully engage in the exchanges. In addition, ACA funds need to be set
aside to assist insurance carriers who have created viable low cost options that make quality
healthcare available to low income consumers and Medicaid participants.

Nachreiner 14
References/Bibliography
Alltucker , Ken, et al. "Rate hikes, new doctors: Obamacare exchanges open to angst." USA
Today, 1 Nov. 2016. www.usatoday.com/story/news/politics/2016/10/31/obamacare-
exchanges-open-amid-fears-rates-effect-enrollment/92913140/
Baker, Sam. "Obamacare Website Has Cost $840 Million." The Atlantic , 30 July 2014.
www.theatlantic.com/politics/archive/2014/07/obamacare-website-has-cost-840
-million/440478/.
CBO (Congressional Budget Office). Affordable Care Act. CBO, www.cbo.gov/topics/health-
care/affordable-care-act. Accessed 8 Dec. 2016.
Folland, Sherman, et al. The Economics of Health and Health Care. 7th, Pearson, 2013.
History and Timeline of the Affordable Care Act (ACA)." eHealth , 22 Sept. 2016.
resources.ehealthinsurance.com/affordable-care-act/history-timeline-affordable-care-act-
aca.
Jost, Timothy. "The truth about those rising health insurance premiums." CNN, 25 Oct. 2016.
www.cnn.com/2016/10/25/opinions/affordable-health-care-exchange-premiums-jost/.
Kaiser Family Foundation. "State Action Toward Creating Health Insurance Exchanges." 4 Jan.
2013, kff.org/.
Kapur, Akshay, et al. "Private Health Insurance Exchange ." PWC, 2012.
www.strategyand.pwc.com/media/file/Private-health-insurance-exchanges.pdf.
Kardish, Christ . "Which Health Exchanges Have the Lowest Premiums? ." Governing , 7 Jan.
2015, www.governing.com/topics/health-human-services/gov-health-exchange-lowest
-premiums.html.
Luhby, Tami. "Will Obamacare Survive As Insurers Pull Out?" CNN, 17 Aug. 2016.
money.cnn.com/2016/08/17/news/economy/obamacare-insurers/.
Manning, Jeff. "Oregon Settles Bitter Legal Fight With Oracle for $100 Million." The Oregonian
[Portland], 15 Sept. 2016.www.oregonlive.com/politics/index.ssf/2016/09/post_183.html.
National Research Council (US); Institute of Medicine (US); Woolf SH, Aron L, editors. U.S.
Health in International Perspective: Shorter Lives, Poorer Health. Washington (DC):
National Academies Press (US); 2013. Available from:
https://www.ncbi.nlm.nih.gov/books/NBK115854/ doi: 10.17226/13497
Norris, Louise . "California health insurance exchange / marketplace." Health Insurance
Government, 8 Oct. 2016, www.healthinsurance.org/california-state-health-insurance-
exchange/.

Nachreiner 15
Obamacare Facts . "State Health Insurance Exchange: State Run Exchanges."
obamacarefacts.com/state-health-insurance-exchange/. Accessed 6 Dec. 2016.
O'Donnell, Jayne , et al. "As Obamacare choices dwindle, feds face consumer, political
backlash." USA Today, 30 Aug. 2016.
www.usatoday.com/story/news/politics/2016/08/29/obamacare-choices-dwindle- feds-
face-consumer-political-backlash/89403698/.
OECD (2013), Health at a Glance: OECD Indicators, OECD Publishing.
http://dx.doi/10.1787/health_glance-20130en
The White House. "Executive Order 13535-- Patient Protection and Affordable Care Act's
Consistency with Longstanding Restrictions on the Use of Federal Funds for Abortion."
The White House (President Barack Obama), 24 Mar. 2010, www.whitehouse.gov/the-
press-office/executive-order-patient-protection-and-affordable-care-acts-consistency-
with-longst.
Winkler, Rolfe, and Ana Wilde Mathews. "Uncertainty for Insurer Started by Kushner's
Brother." WSJ [NYC], 22 Nov. 2016.