Embed Size (px)
Citation preview

Maxillofacial TraumaMaxillofacial Trauma
Anthony G. Hillier, D.O.Anthony G. Hillier, D.O.
St. John West ShoreSt. John West Shore
Emergency Medicine ResidentEmergency Medicine Resident

Etiology and Incidence Etiology and Incidence
►Multisystem injury 20-50%Multisystem injury 20-50%►Nasal and mandibular fractures most Nasal and mandibular fractures most
common in community ED’scommon in community ED’s►Midface and zygomatic injuries most Midface and zygomatic injuries most
common in Trauma centerscommon in Trauma centers►25% of women with facial trauma 25% of women with facial trauma
result of domestic violenceresult of domestic violence► Incidence of concomitant cervical Incidence of concomitant cervical
spine injuries with facial fracturesspine injuries with facial fractures

Etiology and IncidenceEtiology and Incidence
►Older age, MVC and TBI-higher incidenceOlder age, MVC and TBI-higher incidence
►Facial fractures-a distracting injury?Facial fractures-a distracting injury?
►Carotid artery injuryCarotid artery injury
►Blindness may occur with facial fracturesBlindness may occur with facial fractures

Maxillofacial TraumaMaxillofacial Trauma

Emergency Management and Emergency Management and ResuscitationResuscitation
► AirwayAirway Most urgent complication-Airway compromiseMost urgent complication-Airway compromise Simple interventions firstSimple interventions first No mandible?No mandible?
► IntubationIntubation Avoid nasotracheal intubationAvoid nasotracheal intubation May not want RSIMay not want RSI
►BenzodiazepinesBenzodiazepines►KetamineKetamine►EtomidateEtomidate
Be Prepared and Be CreativeBe Prepared and Be Creative


Emergency Management and Emergency Management and ResuscitationResuscitation
►Airway Management OptionsAirway Management Options Awake intubationAwake intubation Laryngeal Mask AirwayLaryngeal Mask Airway Fiberoptic intubationFiberoptic intubation Lateral or semi-prone positionLateral or semi-prone position Percutaneous transtracheal jet ventilationPercutaneous transtracheal jet ventilation Retrograde intubationRetrograde intubation CricothyroidotomyCricothyroidotomy

Emergency Management and Emergency Management and ResuscitationResuscitation
►Hemorrhage ControlHemorrhage Control Rarely develop shock from facial bleeding Rarely develop shock from facial bleeding
alonealone Direct PressureDirect Pressure LeFort FracturesLeFort Fractures Nasal hemorrhage may require A&P packingNasal hemorrhage may require A&P packing
►HistoryHistory VisionVision Teeth alignmentTeeth alignment Abuse Abuse

Maxillofacial Trauma-Physical Maxillofacial Trauma-Physical ExamExam
► InspectionInspection Facial elongationFacial elongation
►High grade LeFort FractureHigh grade LeFort Fracture AsymmetryAsymmetry
►Deformities and cranial nerve injuryDeformities and cranial nerve injury
►PalpationPalpation TendernessTenderness Step offsStep offs Facial stabilityFacial stability
CrepitusCrepitus Subcutaneous airSubcutaneous air Cutaneous anesthesiaCutaneous anesthesia

Maxillofacial Trauma-Physical Maxillofacial Trauma-Physical ExamExam
► Periorbital and Periorbital and Orbital ExamOrbital Exam Perform earlyPerform early
Professional Lid Retractor

Maxillofacial Trauma-Physical Maxillofacial Trauma-Physical ExamExam
► Periorbital and Orbital ExamPeriorbital and Orbital Exam Look for exophthalmos or enophthalmosLook for exophthalmos or enophthalmos Pupil shapePupil shape HyphemaHyphema Visual acuityVisual acuity Entrapment signsEntrapment signs Raccoon signRaccoon sign
► Bimanual Palpation TestBimanual Palpation Test

Maxillofacial Trauma-Physical Maxillofacial Trauma-Physical ExamExam
►Penetrating InjuriesPenetrating Injuries Occult globe penetrationOccult globe penetration Eyelid lacerationsEyelid lacerations
►NoseNose Septal hematomaSeptal hematoma CSF RhinorrheaCSF Rhinorrhea
►EarsEars Subperichondral hematomaSubperichondral hematoma HemotympanumHemotympanum Battle signBattle sign

Maxillofacial Trauma-Physical Maxillofacial Trauma-Physical ExamExam
►Oral and Mandibular ExamOral and Mandibular Exam Mandible deviationMandible deviation Teeth malocclusionTeeth malocclusion ParesthesiaParesthesia Tongue Blade TestTongue Blade Test
►95% Sensitive95% Sensitive►65% Specific65% Specific

Maxillofacial Trauma-ImagingMaxillofacial Trauma-Imaging
►Head, chest and abdominal trauma Head, chest and abdominal trauma takes precedencetakes precedence
►PE detects up to 90% of fracturesPE detects up to 90% of fractures►Plain FilmsPlain Films►CTCT
Orbital fracturesOrbital fractures 3D images available3D images available

Maxillofacial Trauma-Specific Maxillofacial Trauma-Specific FracturesFractures
►Frontal Sinus/Bone FracturesFrontal Sinus/Bone Fractures Direct blowDirect blow Frequent intracranial injuriesFrequent intracranial injuries MucopyocelesMucopyoceles Consult with NS for treatment, disposition Consult with NS for treatment, disposition
and antibioticsand antibiotics►Nasoethmoidal-Orbital InjuriesNasoethmoidal-Orbital Injuries
Lacrimal apparatus disruptionLacrimal apparatus disruption Bimanual palpation if medial canthus painBimanual palpation if medial canthus pain CT faceCT face

Maxillofacial Trauma-Specific Maxillofacial Trauma-Specific FracturesFractures
►Orbital FracturesOrbital Fractures Usually through Usually through
floor or medial wallfloor or medial wall EnophthalmosEnophthalmos AnesthesiaAnesthesia DiplopiaDiplopia Infraorbital stepoff Infraorbital stepoff
deformitydeformity Subcutaneous Subcutaneous
emphysemaemphysema

Maxillofacial Trauma-Specific Maxillofacial Trauma-Specific FracturesFractures
► Orbital Fissure SyndromeOrbital Fissure Syndrome Fracture of the orbital canalFracture of the orbital canal
► Extraocular motor palsies and blindnessExtraocular motor palsies and blindness► If significant retrobulbar hemorrhage, may If significant retrobulbar hemorrhage, may
need cantholysis to save visionneed cantholysis to save vision
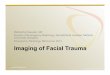
► Zygomatic FracturesZygomatic Fractures Tripod fractureTripod fracture
► Most seriousMost serious► Lateral subconjunctival hemorrhageLateral subconjunctival hemorrhage► Need ORIFNeed ORIF
Arch fractureArch fracture►Most commonMost common►Outpatient Outpatient
repairrepair

Tripod FractureTripod Fracture

Maxillofacial Trauma-Specific Maxillofacial Trauma-Specific FracturesFractures
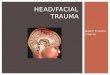
►Maxillary FracturesMaxillary Fractures High-energy injuryHigh-energy injury 100x gravity100x gravity MalocclusionMalocclusion Facial lengtheningFacial lengthening CSF rhinorrheaCSF rhinorrhea Periorbital ecchymosisPeriorbital ecchymosis

LeFort FracturesLeFort Fractures


Maxillofacial Trauma-Specific Maxillofacial Trauma-Specific Facial FracturesFacial Fractures
►Mandibular FracturesMandibular Fractures Second most common facial Second most common facial
fracturefracture Often multipleOften multiple MalocclusionMalocclusion Intraoral lacerationsIntraoral lacerations Sublingual ecchymosisSublingual ecchymosis Nerve injuryNerve injury
Plain filmsPlain films PanorexPanorex CTCT
Open FracturesOpen Fractures►Pen G or CleocinPen G or Cleocin

BodyBody 30-40 %30-40 %
AngleAngle 25-30 %25-30 %
CondyleCondyle 15-17 %15-17 %
SymphysisSymphysis 7-15 %7-15 %
RamusRamus 3-9 %3-9 %
AlveolarAlveolar 2-4 %2-4 %
Coronoid Coronoid ProcessProcess
1-2 %1-2 %

Questions?Questions?Thank You!Thank You!

Lecture QuestionsLecture Questions
1.1. What portion of the mandible is most What portion of the mandible is most commonly fractured?commonly fractured?
a.a. RamusRamus
b.b. Coronoid processCoronoid process
c.c. BodyBody
d.d. AngleAngle
e.e. SymphysisSymphysis

2.2. Orbital fractures can cause all of the Orbital fractures can cause all of the following except:following except:
a.a. BlindnessBlindness
b.b. Motor palsiesMotor palsies
c.c. Facial anesthesiaFacial anesthesia
d.d. EnophthalmosEnophthalmos
e.e. HyphemaHyphema

3.3. Which of the following is/are true Which of the following is/are true regarding maxillary fractures?regarding maxillary fractures?
a.a. Only minimal force necessaryOnly minimal force necessary
b.b. Rarely cause CSF rhinorrheaRarely cause CSF rhinorrhea
c.c. May cause facial lengtheningMay cause facial lengthening
d.d. Usually the only sustained injuryUsually the only sustained injury
e.e. All of the above are trueAll of the above are true

4.4. The best modality for diagnosing an The best modality for diagnosing an orbital or facial fractures isorbital or facial fractures is
a.a. Plain filmsPlain films
b.b. MRIMRI
c.c. CTCT
d.d. UltrasoundUltrasound
e.e. Osteopathic palpationOsteopathic palpation

5.5. Which statement below is correct?Which statement below is correct?a.a. Midface fractures usually have minimal Midface fractures usually have minimal
morbiditymorbidityb.b. The tongue blade test is quite sensitive The tongue blade test is quite sensitive
in assessing need for mandibular xraysin assessing need for mandibular xraysc.c. The bimanual nasal exam is crucial in The bimanual nasal exam is crucial in
possible medial orbital wall fracturepossible medial orbital wall fractured.d. Midface fracture is an indication for Midface fracture is an indication for
nasotracheal intubation and RSI is often nasotracheal intubation and RSI is often needed in these patientsneeded in these patients
c, e, c, c, bc, e, c, c, b