Embed Size (px)
Citation preview

MEASUREMENTSOF THE CIRCULATION IN CONSTRICTIVEPERICARDITIS BEFOREANDAFTER RESECTIONOF
THE PERICARDIUM1
By HAROLDJ. STEWART,GEORGEJ. HEUER, JOHNE. DEITRICK, NORMANF.CRANE, ROBERTF. WATSONAND CHARLESH. WHEELER
(From the New York Hospital, Departments of Medicine and Surgery, Cornell UniversityMedical College, New York City)
(Received for publication April 1, 1938)
Experience is showing that chronic constrictivepericarditis is not an uncommon syndrome. At-tention has been directed to it again in recentyears. Its recognition has been facilitated byWhite's (1) historical resume and analysis of itsclinical features. It is of therapeutic importanceto'recognize this syndrome for it is a cardiac af-fection that lends itself to surgical treatment asthe experience of Churchill (2), Beck and Gris-wold (3), Blalock (4), and of Stewart andHeuer (5), as well as others, has demonstrated.The clinical manifestations of this disease havebeen very well described; the pathological physiol-ogy of the circulation has not, however, beensufficiently explored.
In the last two and a half years, we have ob-served 9 patients suffering from chronic con-strictive pericarditis, and in six of these part ofthe pericardium has been resected by Dr. GeorgeJ. Heuer.2 In them, studies of the circulationhave been made before as well as after partialpericardiectomy. One clinical group does nothave the opportunity to see large numbers ofthese patients in a short time, and for this reasonthis paper records our studies of the circulationin this situation, together with a statement ofour experience with surgical treatment.
PLAN OF STUDY
All patients were admitted to the hospital and re-mained in bed. The daily fluid intake was limited to1200 cc., and the salt to 2.0 grams. A high protein dietwas given.
Studies of the circulation were made when the pa-tients first came under observation and before we in-
1 An abstract of these studies was read before theAssociation of American Physicians, Atlantic City, May5, 1937.
2 Since this paper went to press the pericardium wasresected from another patient, making seven cases inall (5).
stituted drug therapy. Diuretics were then administeredand studies were repeated, this time when they were inthe best state it was possible for them to attain. Re-section of the pericardium was then done. As soon afteroperation as the patients were able to participate, ob-servations were repeated, as well as later when changesin the clinical state occurred. The patients were dis-charged from the hospital free of excess fluid and fol-lowed in the Cardiac Outpatient Clinic, from whichthey were readmitted to the hospital at intervals forrepetition of the studies of the circulation.
METHODS
All observations were made in the morning while thepatients were in a basal metabolic state. Measurementsof the cardiac output were made by the acetylene method,three samples of gas being taken as first recommended byGrollman (6), and by Grollman, Friedman, Clark, andHarrison (7). During this measurement the patients weresitting in a steamer chair (angle 135 degrees). They weretrained beforehand to carry out the procedures. Whilethe patient was at rest, the cardiac rate was counted atintervals of five minutes. At the end of one-half hourthe acetylene-air-oxygen mixture was rebreathed. Threesamples of gas were taken during each rebreathing pe-riod for estimation of the arteriovenous oxygen differ-ence. The first sample was taken after rebreathing 10to 12 times in 20 seconds, the second after 2 to 3 breathsmore, and the third after 2 to 3 additional breaths. Allthree samples were usually obtained before the end of 30seconds. Samples were taken during expiration. Twoto three periods of rebreathing were carried out on eachpatient. Shortly afterward, the oxygen consumption wasmeasured with a Benedict-Roth spirometer. After ashort pause, the vital capacity was measured, and heightand weight recorded. In succession, sufficient time beingallowed between each procedure for the patient to returnto a basal metabolic state, an electrocardiogram wastaken, the arm to tongue circulation time recorded, thevenous pressure estimated, and the blood pressure meas-ured; finally an x-ray photograph of the heart wasmade at a distance of two meters.
The arm to tongue circulation time was estimated bythe use of decholin (8). Five cc. of a 20 per cent solu-tion were injected rapidly (1 to 2 seconds) through an18-gauge needle into an antecubital vein while the patientwas lying quietly in the supine position. This was re-
581

STEWART, HEUER, DEITRICK, CRANE, WATSONAND WHEELER
peated in one and one-half minutes after the response tothe first test had been elicited. The time was recordedfrom the beginning of the injection until the patientperceived the bitter taste.
The venous pressure was measured by the directmethod (9), using a large antecubital vein, the armbeing placed on a level with the right auricle. Normalpressures by this method range from 4.0 to 10.0 cm. ofsaline. The antecubital vein of one arm was reserved forthe injection of decholin and of the other arm for themeasurement of venous pressure. In subsequent meas-urements the vein was entered at the site first punctured.
X-ray photographs of the heart were taken with thepatient in the standing position, in full inspiration, at adistance of two meters.8 Measurements of the cardiacarea were carried out by the technique of Levy (10) andestimations of volume were made as recommended byBardeen (11). Special x-ray exposures in the anterio-posterior as well as in the lateral positions were takenfor the detection of calcification. Examination underthe fluoroscope was also carried out. In certain patientsphotographs of the eyegrounds were made for definitionof the vessels. Infra-red photographs of the patientswere taken to record the state of the peripheral veins.The patients assumed as nearly as possible exactly thesame position for each observation in order to assureuniformity from this point of view. In addition, eachprocedure in the observation was carried out by thesame investigator.
The six patients who were operated upon and in whomobservations were made both before and after partialpericardiectomy form the subject of this paper.
RESULTS
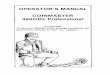
The data are recorded in Tables I and II andcertain of the data are summarized in Figure 1.
The arteriovenous oxygen difference beforeoperation was increased in all except one (Case6, 59.7), the range being from 71.5 to 88.6 cc.After operation when the patients were in theirbest state, it decreased in all patients and onlyone fell outside of the normal range, which wasthen 51.4 to 68.7 cc.
The cardiac output per minute and cardiac in-dex 4 were decreased in all except one patient(Case 6, 2.16 liters), the range of the index being1.35 to 1.82 liters. After operation it increasedand ranged between 1.80 to 2.72 liters, and wasbelow normal in only one (Case 4).
8 The authors are deeply indebted to the X-ray De-partment of the New York Hospital for their coopera-tion in this investigation.
4 Cardiac index = liters per square meter per minute.
The stroke volume was decreased and the rangewas from 20 to 42 cc. per beat. After operationit increased and ranged from 33 to 50 cc. per beat.
The venous pressure was elevated in every case,the range being 17.9 to 24.0 cm. After operationit fell and when the patients were in their beststate the range was 8.3 to 16.7 cm.
The arm to tongue circulation time ranged from13.5 to 29.8 seconds before operation; in short,it was prolonged. After operation the range was7.3 to 17.1 seconds when the patients were intheir best state.
There was no consistent behavior of the heartrate. In certain patients it was elevated beforeoperation and slowed afterward, and in othersthe reverse happened. The basal metabolic ratewas not altered significantly in this syndrome, norwas it changed by operation.
The vital capacity before operation was notlowered if the pleural cavities were free of fluid.In certain patients it decreased and in others itincreased after operation. Decrease after opera-tion was in part due to the flexible thoracic cageresulting from removal of the ribs.
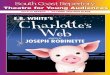
Infra-red photographs revealed marked disten-tion of and increase in the number and caliberof the venous channels before operation. Asimprovement occurred after operation there wasprogressive decrease in their number and caliber(Figure 2).
CLINICAL COURSEOF PATIENTS
After operation there were 3 trends: (1) Clini-cal improvement was rapid and striking, andassociated with this were changes toward normalof the measurements of the circulation (Tables Iand II, Figure 1). In two patients "cure" wasa matter of months (Cases 1 and 2). (2) Inone (Case 3), clinical improvement was slow andgradual, to cure in approximately 1 year afteroperation (Tables I and II); in her, the measure-ments of the circulation showed gradual changes.(3) Three patients improved gradually after op-eration; their condition has now become sta-tionary (Cases 4, 5, and 6). They are betterthan before the operation and are ambulatory,and there have been changes in the circulationtoward normal (Tables I and II).
582

...-II~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~
i3}~~~~~~~~~wC "-D e
CO I .00 00 = 1iC°i =°a000 14 449 °4 =0 °°°I
'.g11 941l$,#0;48--1 __
M!lPHa OCOO CD000 OCDQO;_ 0 0 CD o00 =0=00ooo oo aooo
%~~~~~~~~~~~~~~~~~~~~~+ +0 Cl + ++ + +0e
fl~~~~~~~~~~~~~C ..+++++ H+++CX
l | @. U t tww | | eos ~~~~~~4 |oB 3w>g-
t~~~~~~~~~~~~~~~~~~~~~+a+ + +=Cl §1°^v°4S s Zor ztot § too>¢ Zo O"t i ano""ono++*+ +
eef( CDDO +00+tJBz co=CD>0eS3S8tezceea 00008+0-e°es0>U°eoeeoS o
R|Swnog D £Xba <°4t4t41- |<439<9 ea c9¢9< |2 esS>z4¢pg|q3Cs>.X
^,I sooe bOro1bor°.t sou $SS ISe 9b; .4.IoEI.e9.t
ll~~~~~~~~~~~~~~~~cg§Io alCginaw~ ~ ~ ~ + ++++I++ ORt ! 0: Rci R.0 a0 -0
oo4.o.,to a 0 eq-wcoe.C* on- ++a +ioow-aoo I ++a ++
l t>xs| " ! j§ 80z-M!t;t-!! a £^ttSviti2zS [Zz£ai^ S>Cs40
11
ll
583CIRCULATION IN CONSTRICTIVE PERICARDITIS
ognd IPM.OPIBJICI I ++ oo+0 Hl I+++++ ++ ++++411 ++ ++ ++Ccoc 1++ ++++
ta04m.0.1 4
aIN;;!joqumu AjorM
9". pq!joqmu ono
" * r- i
4<AR(>b
;e OF
aco
a% ra1:4 .
o; 0z cc** Fb

juno poolq pwl q.He °" q4 Zo
3 s1 ++ +++1~~~~~+++ + +°°+*a ssw ~~~+-H o++ I ++ + -H44 -H
O" +0 0~~~~~~l++ ++ 0
RFMAD ++ +++I+ +°°tI ~~~~000D++ 1+0 0 000
J- - Cs -4 C
glodso-l~~~~~~C IR C!goE C!|
ooo%fo tee oaro WM,_
"'B, $H t.f¢ 0t 00 z
*noo | 0 X t! 2 0<~~~~o|q 80 to 0 0°ndtnoD | j l, i § Nt- C!" .1 IR .8R4~~~~~~~~~~~C V4.4_&Q Mfge:- O
=2&0 ~ gKAJ! isaX t3
584 STEWART., HEUER, DEITRICK, CRANE, WATSONAND WHEELER
..q4t
I._--
4I
en
C:
._
lar"5
co
* -I-
*4
4J0C
co
o
cd
to l
Coc:
A .8
g 0
r .
Cd'
++ +++ I++ + ++- +
le
LPi,
a
t-&acq
U* 1'IO.li.0.1IA;Az(.
zoo PUT!sa
gjoqu 1ip!RI
'Xoqm ow,

CIRCULATION IN CONSTRICTIVE PERICARDITIS 585
TABLE HI
Additional data relating to 6 cases of chronic constrictive pericarditis *
Casenu~~~nb!r;~~~Calcific- TnInitial; l)tDration Etlol tion of sincean lme of o Heart sie | orl- Fluoroscopy of heart Electrocardiogram R| ut |rram
History diaset cardlum tnumber
Cas 1 Before yars unk Vey small Prest Vey ma pulations S. R.A.D. QRSi, , sand Ti,t,, lowA B operation 6 onths L asp T2,, cove haped Ax shift28323 -_ _- _ _ _ _ _ _ _
After Larger Present Very good pulsatiom Axis ift 22. No other change Cured 1 yearopeation 9 montsCase 2 Before 1 year unk. Large 0 S1. of It. side, none of rt. side. No R.A.D. QRI,2,s, low ampl. T1,2 neg.W. M., operation 4 months downward st, dL It. hift Axis shift 0°Number -_ _- _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _
103699 After Smaller 0 Good pustions R.A.D. QR&.,ssfll lowampL T1,2, Cured 1 yearoperation iner. ampL Axis shift r 4 months
Cas 3 Before 4 monts tb. Si. elarged 0 Der. pulations of rt. sur. and rt. 81. R.A.D. QRS2.,t low ampL Ti,2,,A. ., operation vent. low ampL Axis shift 11°
91648 After Smaller 0 Exodlent pulsations No chae Axis ft 6r Cured 2 yeaoperation 2 months
Cas 4 Before 7 montbh unk. Large 0 No motion lowe Hof heart 81. hLA.D. QRSi,s.a low ampl. T1,2J. McC., operation oove shaped. Axis shft 11°Number -
128763 After No ohange In 0 Incr. motion but none of rt. vent. No axis deviation. Incr. ampl. of Improved 1 year,operation oee, but shape QR,A,.s. Axis ft 18° 3 months
changedCase 5 Before unk. Lae Prnt Der. pulsations of rt. aur. S1. R.A.D. QRS sIlow ampL Ti,,tP A operation diphado. Axie ift 35Nu-nr -
141257 After Not much Preset Iner. along It. but almost none of No ohange. Axis sft 30° Improved 1year,operation change rt. aur. and rt. vent. 6 months
Case 6 Before 6 years unk. Small Not en 81 pultions of It. vent. SL LA.D. QRSi,i.s low ampl. LowJ. 8, operation in x-ray amppL of Ta. Axs sift 0_Number169168 After Larger Present in Iner. pulstions SI. L.A.D. QRSi,,, d. iner. In anpL Improved 8 months
operation micro. secl.ne.I mp.A6 sit3of perid.T, incr.inampi. Axissh 30
* In this Table the following abbreviations are used:unk. = unknowntbc. = tuberculosissl. = slightIt., rt. = left, right, respectivelyincr., decr. = increased, decreased, respectivelyampl. = amplitudeneg. = negativeR.A.D., L.A.D. = right and left axis deviation respectivelyaur., vent. = auricle, ventricle, respectivelymicro. sec. of pericard. = microscopic sections of pericardium
t As estimated from evaluation of patients' history.As of March, 1938.
§ Edema of ankles was noted 10 years before admission. Symptoms were first noted 2 months before admission.
DISCUSSION
Our observations- show that chronic constric-tive pericarditis is characterized by decreased car-diac output per minute and per beat, rise in venous
pressure, slowing of the velocity of blood flow,and engorgment of the venous vascular bed.Fluoroscopic examination shows decreased con-traction of the heart chambers, and fixation ofthe heart may be observed. Clinical improvementafter operation was associated with changes inall these functions toward normal. There appearto be two essential defects in this syndrome,
namely, (1) obstruction to the entrance of bloodinto the chambers of the heart resulting in de-creased filling, and (2) interference with con-traction of the heart. There is evidence for thefirst in (a) the decreased dilatation of the heartin diastole under fluoroscopic examination and atoperation and (b) the observation at operationof the thickened pericardium which was not capa-ble of much distention and may have been cal-cified. (c) Infra-red photographs revealed dis-tention of the peripheral veins. (d) The elevatedvenous pressure is evidence that there is ample

STEWART, HEUER, DEITRICK, CRANE, WATSONAND WHEELER
A CURED B IMPROVED-- -5 . If - - - .. - -_ tIRIA
riP%3T bEFOfE ^FTER _ FIRST bEFORE AFTEROWERVEDOPERATION OPEPATIO" OWERVED. OPERATon OKRA'Fi"
. ~~~~~~~"CUREDW _ |10w9
3.C so T30
°0 '111a vlul110
75E~~~~~~~~~5
toC LEVEL
Mm,'5&50l -^
too 10
Data o -t 3pee
>' 50
K. 3r
1.00 11-00~~~~~IG1Daarltn o3 ains"ue" yoeain() n ipoe" yoeain()
blood available for the heart. With respect tocontraction, impairment is inferred from the (a)decreased extent of contraction on fluoroscopicexamination and at operation, as well as from(b) the examination of the thickened unyieldingpericardium incapable of much change duringcontraction. These two defects result in decreasein cardiac output, per beat and per minute, andpiling up of blood on the venous side, accountingfor increase in venous pressure and slowing ofthe velocity of blood flow. The heart may beunusually small or not much enlarged.5 Removalof the pericardium results in alteration of these
5The cardiac silhouette is made up of cardiac shadowplus the shadow of the thickened pericardium.
two defects, in short, in removing obstruction toblood entering the heart, allowing the heart tostretch in diastole, and increase in extent ofcontraction; these account for changes in the cir-culation which have been recorded after opera-tion. Parallel with improvement in circulationafter operation, clinical improvement occurs.
These observations with respect to cardiac out-put and venous pressure are in accord with thosereported by Burwell and his associates (12, 13),and by Beck and Cushing (14).
The delay in improvement of certain patientsafter operation may be due in part to dilatationof the region of the heart from which the peri-cardium has been resected, and in part to ob-
586

CIRCULATION IN CONSTRICTIVE PERICARDITIS
FIG. 2
Infra-red photographs of A.B. (Case 1), in whom operation was followed by" cure." Photograph A was made on May 20, 1936; B on June 29, 1936, 20 days afterpericardiectomy, and C on April 4, 1937, approximately 10 months after operation.Attention is directed to the decrease in venous channels, to the patient's growth anddevelopment, and to change in flare of the ribs with the elimination of the chronic ascitesfrom which the patient had suffered five and a half years.
struction not having been sufficiently relieved. Atoperation, the heart bulged through the windowwhich was made in the pericardium and unduestretching of this muscle may have resulted. Itmay require time for this muscle to regain " tone."
Three patients (Cases 2, 3, and 4) were ob-served from the stage of pericarditis with effu-sion through the stage of constriction. In them,signs of obstruction disappeared with absorptionof the pericardial fluid, but increased rapidlywhen formation of adhesions and constrictionbegan and was associated with rapid parallel risein venous pressure, and circulation time, and de-crease in cardiac output.
The use of digitalis appears to be contraindi-cated except under certain circumstances. Stew-art and his associates have shown that digitalisdecreases cardiac size (15, 16, 17) and increasesthe extent of ventricular contraction (18, 19, 20).
In the presence of constrictive pericarditis, thesize of the heart may already be restricted andthe cavities small, and further decrease in its sizemay not be beneficial but may increase the ob-struction. On the other hand, the heart is prob-ably contracting as fully as possible while it isattached to the unyielding thickened pericardium.One patient (Case 5) exhibiting auricular fibril-lation was under the influence of digitalis whenshe came under observation. Its use seemed es-sential to maintain a slow heart rate, and it didnot appear justifiable to withdraw the drug. Toone patient (Case 3), exhibiting normal sinusrhythmu, the drug was given after resection of thepericardium. In this instance, increase in cardiacoutput and fall in venous pressure occurred, ef-fects which were to be expected (15, 16, 17),(Table I.). Change in size of the heart couldnot be estimated because of the presence of fluid
587

STEWART, HEUER, DEITRICK, CRANE, WATSONAND WHEELER
in the right pleural cavity. Digitalis was givento another patient (Case" 2) exhibiting normalsinus rhythm. Wewere un'able to state the stageof the pericardiat4esion at the time of exhibitionof the drug; it was probably in the stage of ab-sorption of pericardial fluid and early formationof adhesions. The patient was taking theocalcinat the time the first observations were made(Table I). When the drug was discontinuedthere was rise in venous pressure, slowing ofcirculation time and decrease in cardiac output.When it was given again the venous pressure fell,the circulation-time decreased, and cardiac outputincreased, and all the measurements were in thenormal range. We were unable to evaluate theeffects of giving digitalis, 1.8 grams, on Sep-tember 29, 1935. The control measurements weremade 4 days beforehand and spontaneous changeswhich would invalidate the comparison may haveoccurred in the circulation in this interval. Theeffects of theocalcin can, however, be evaluatedand were similar to those already recorded byStewart and Cohn (15).
Case 6 calls for comment. Except for the ele-vated venous pressure, the measurements of the'circulation were in the normal ran'ge before op-eration. She improved before operation by medi-cal treatment and the use of drugs. She was ableapparently to maintain at rest in bed a normalcardiac output per minute and cardiac index andapproximately normal output per beat in spiteof the very thickened adherent pericardium. Op-eration resulted only in moderate clinical improve-ment, and the venous pressure fell to normal.Subtotal thyroidectomy had been performed onthis patient early in her illness 6 years before,when it was suspected that heart failure wascaused by hyperthyroidism. Whether this ac-counted for the deviation of the patient from thepattern of the other patients, we are unable tostate. The circulation was not maintained at theexpense of an elevated heart rate, nor was thereanemia (21). The plasma protein in this patientremained low although she was given a highprotein diet. Before operation, diuretics wereineffectual in this patient. After operation, how-ever, urine outputs of 5 liters a day resulted from2.0 cc. injections of mercupurin, and 16 kgm. ofweight were lost in 6 weeks (Table I).
The partition of the circulation time was studied
in 4 patients (Table III). The -arm to tonguecirculation time was measured by the use of de-cholin (D), the arm to lung time by the injectionof ether (E) (22), and the lung to respiratorycenter by the inhalation of carbon dioxide (C)(23). D minus E should approximate the valueof C, which was found to be the case when ob-servations sweye made (Table III). The ether
TABLE III
Data relating to partition of circulation time in 4 cases
Circulation tinme
Ve- LungPatient Date nous Arm to Arm to re- D-E
sure to lgun .t spira- shouldlin (D) Ether center. (C)E)C02(C)
cm. seconds seconds seconds secondsCase 2 Jan. 28, 1938 9.2 19.2 5.5 15.0 13.7Case 4 Jan. 29, 1938 18.8 21.5 13.5 9.5 8.0Case 5 Feb. 1, 1938 15.3 19.2 6.0 13.5 13.2Case 6 Feb. 28, 1938 15.5 21.4 8.3 12.0 13.1
arm to lun'g circulation time was in the normalrange in Cases 2, 5, and 6, and prolonged in Case4. The lung to respiratory center time was pro-longed in Cases 2, 5, and 6, and normal in Case 4.In short, no uniformity was apparen't.
The effect of pregnancy was observed in on'epatient (Case 3). Observations made on Novem-ber 30, 1937 (Table I) when she was 3 monthspregnant revealed increase in arteriovenous oxy-gen difference, decrease in cardiac output perminute and per beat, and in cardiac index, andlengthening of the circulation time, not only oncomparison of them with the measurements onMarch 18, 1937, before pregnancy occurred, butalso when restoration to normal was found onDecember 16, 1937, 13 days after therapeuticabortion.
SUMMARYAND CONCLUSION
Chronic constrictive pericarditis is usually as-sociated with decrease in cardiac output per min-ute and per beat, and decrease in the cardiacindex. The venous pressure is elevated and thecirculation time prolonged, and there is increasein size and caliber of the peripheral venous chan-nels. Rest in bed and medical therapy mayoccasion clinical improvement with disappearance
588

CIRCULATION IN CONSTRICTIVE PERICARDITIS
of the accumulations of fluid, and with changesof the circulation toward normal. After opera-tion in those cured, the measurements assumednormal limits and in those " improved " the meas-urements of the circulation approached normal.In this syndrome the symptoms and signs appearto be a consequence of the defects in circulationwhich the constricting pericardium occasions.These defects appear to be two: (1) obstructionto entrance of blood into the chambers of theheart and (2) interference with contraction andemptying of the heart. These result in (1) de-crease in cardiac output per minute and per beatand (2) piling up of blood on the venous side,which accounts for rise in venous pressure andslowing of the velocity of blood flow. Releasingthe heart and removing obstruction by resection ofpart of the pericardium results in return of thesefunctions toward or to normal levels.
BIBLIOGRAPHY
1. White, P. D., Chronic constrictive pericarditis (Pick'sdisease) treated by pericardial resection. Lancet,1935, 2, 539 and 597.
2. Churchill, E. D., Pericardial resection in chronicconstrictive pericarditis. Ann. Surg., 1936, 104,516.
3. Beck, C. S., and Griswold, R. A., Pericardiectomy inthe treatment of the Pick syndrome. Experi-mental and clinical observations. Arch. Surg.,1930, 21, 1064.
4. Blalock quoted by Burwell (13).5. Stewart, H. J., and Heuer, G. J., Chronic constrictive
pericarditis: Dynamics of the circulation and re-sults of surgical treatment. Arch. Int. Med. (Inpress).
6. Grollman, A., The Cardiac Output of Man in Healthand Disease. C. C. Thomas Co., Springfield, 1932,p. 73.
7. Grollman, A., Friedman, B., Clark, G., and Harrison,T. R., Studies in congestive heart failure. XXIII.A critical study of methods for determining thecardiac output in patients with cardiac disease.J. Clin. Invest., 1933, 12, 751.
8. Tarr, L., Oppenheimer, B. S., and Sager, R. V., Thecirculation time in various clinical conditions de-termined by the use of sodium dehydrocholate.Am. Heart J., 1933, 8, 766.
9. Taylor, F. A., Thomas, A. B., and Schleiter, H. G.,A direct method for the estimation of venous pres-sure. Proc. Soc. Exper. Biol. and Med., 1930,27, 867.
10. Levy, Robert L., The size of the heart in pneumonia.A teleoroentgenographic study, with observations
on the effect of digitalis therapy. Arch. Int. Med.,1923, 32, 359.
11. Bardeen, C. R., Determination of the size of theheart by means of the x-rays. Am. J. Anat.,1918, 23, 423.
12. Burwell, C. S., and Strayhorn, W. D., Concretiocordis. I. A clinical study, with observations onthe venous pressure and cardiac output. Arch.Surg., 1932, 24, 106.
13. Burwell, C. S., and Flickinger, D., Obstructive peri-carditis. Effect of resection of the pericardiumon the circulation of a patient with concretio cor-dis. Arch. Int. Med., 1935, 56, 250.
14. Beck, C. S., and Cushing, E. H., Circulatory stasis ofintrapericardial origin. The clinical and surgicalaspects of the Pick syndrome. J. A. M. A., 1934,102, 1543.
15. Stewart, Harold J., and Cohn, Alfred, E., Studieson the effect of the action of digitalis on theoutput of blood from the heart. III. Part I.The effect on the output in normal human hearts.Part II. The effect on the output of hearts inheart failure with congestion, in human beings.J. Clin. Invest., 1932, 11, 917.
16. Stewart, H. J., Crane, N. F., Deitrick, J. E., andThompson, W. P., Action of digitalis in com-pensated heart disease. Part I. In the presenceof regular sinus rhythm. Part II. In the pres-ence of auricular fibrillation. Arch. Int. Med. (Inpress).
17. Stewart, H. J., Deitrick, J. E., Crane, N. F., andWheeler, C. H., Action of digitalis in the uncom-pensated heart disease. Part I. In the presenceof regular sinus mechanism. Part II. In thepresence of auricular fibrillation. Arch. Int. Med.(In press).
18. Cohn, A. E., and Stewart, H. J., Evidence thatdigitalis influences contraction of the heart in man.J. Clin. Invest., 1924, 1, 97.
19. Cohn, A. E., and Stewart, H. J., The relation betweencardiac size and cardiac output per minute follow-ing the administration of digitalis in normal dogs.J. Clin. Invest., 1928, 6, 53.
20. Cohn, A. E., and Stewart, H. J., The relation betweencardiac size and cardiac output per minute follow-ing the administration of digitalis in dogs in whichthe heart is enlarged. J. Clin. Invest., 1928, 6, 79.
21. Stewart, H. J., Crane, N. F., and Deitrick, J. E.,Studies of the circulation in pernicious anemia.J. Clin. Invest., 1937, 16, 431.
22. Hitzig, W. M., The use of ether in measuring thecirculation time from the antecubital veins to thepulmonary capillaries. Am. Heart J., 1935, 10,1080.
23. Gubner, R., The use of CO, inhalation and of alpha-lobeline as tests of circulation time. Read beforethe Scientific Meeting of the New York HeartAssoc., New York Acad. Med., February 1st, 1938.
589