-
8/19/2019 Med Onc Jnr Handbook
1/35
-
8/19/2019 Med Onc Jnr Handbook
2/35
2
Introduction:
Welcome to the department of medical oncology at the Townsville
Cancer Centre. By
the end of the term, you should be able to identify and manage
common side effects of
chemotherapy and radiotherapy in the land of general practice,
emergency
departments and rural hospitals and general medical wards. You
will also have some
understanding of treatment principles and aims of cancer therapy
for common
malignancies. This handbook is meant for the use of resident
medical officers and
basic physician trainees. It may also be useful to advanced
trainees in their first few
months of training.. We hope that this experience will give you
the skills to deal with
cancer patients with positive and empathetic approach.
If you are encountering emotional difficulties when dealing with
poor prognosis,
please talk to one of us earlier in the term to learn ways to
deal with it effectively.
Enjoy the medical oncology rotation.
Regards ,
Consultant Medical Oncologists.
-
8/19/2019 Med Onc Jnr Handbook
3/35
3
Table of contents:
1. Introduction of senior medical
staff-----------------------------------------------------4
2. Weekly time table of clinical and educational
activities-----------------------------4
3. Educational aims and Duties
------------------------------------------------------------5
4. Principles of management of patients on
chemotherapy:---------------------------6
Assessing fitness for
chemotherapy-------------------------------------------------------
6
Important practice points for common
drugs--------------------------------------- ---- 9
Antiemesis
----------------------------------------------------------------------------------
12
Febrile
neutropenia-------------------------------------------------------------------------
15
Extravasation-------------------------------------------------------------------------------
18
Premedications for selected drugs
------------------------------------------------------- 19
5. Medical
emergencies---------------------------------------------------------------------21
6. Summary of management of common
cancers:------------------------------------23
Anus-------------------------------------------------------------------------------------------
23
Bladder----------------------------------------------------------------------------------------
23
Breast------------------------------------------------------------------------------------------
24 Carcinoma of unknown
primary-----------------------------------------------------------
26
Cervix------------------------------------------------------------------------------------------
26
Colo
rectum-----------------------------------------------------------------------------------
26
GBM-------------------------------------------------------------------------------------------
28
Germ cell
tumours----------------------------------------------------------------------------
28
Head and
neck--------------------------------------------------------------------------------
30
Lung
cancer-----------------------------------------------------------------------------------
30
Melanoma-------------------------------------------------------------------------------------
31
Mesothelioma---------------------------------------------------------------------------------
31
Oesophagus------------------------------------------------------------------------------------
32
Ovary-------------------------------------------------------------------------------------------
33
Pancreas----------------------------------------------------------------------------------------
33
Prostate-----------------------------------------------------------------------------------------
34
Stomach and distal
oesophagus-------------------------------------------------------------
33
7. Symptom control
---------------------------------------------------------------------------
35
-
8/19/2019 Med Onc Jnr Handbook
4/35
4
Senior Medical Staff:
1. A/Prof Sabe Sabesan,BMBS( Flinders), FRACP,Director and
Senior Staff Specialist.Clinical Dean, Townsville Clinical
School.
2. Dr Suresh varma,MBBS,MD,DM, FRACP,Senior Staff Specialist and
adjunct senior lecturer.
3. Dr Abhishek Joshi,MBBS,MD,DM,ECMO,FRACP.Staff Specialist and
senior lecturer.
4. Dr Zulfiquer Otty, MBBS, MD,MRCP,FRACP,Staff specialist and
adjunct senior lecturer.
Weekly Timetable:
Time Mon Tues Wed Thurs Fri 0745 ‐0830 GI MDT
(0800 ‐0900) 4 Breast 1 MDT Gyne onc 2
( monthly) 0900 ‐1200 Clinics
SS, AJ Clinic SV
Clinic CM, SV
Clinic SS,CM
Clinic SV
1230 ‐1330 Grand rounds
Radiology meeting
1330 ‐ Clinic H&N clinic 4 Skin MDT
1400‐1500
clinic
Medonc
tutes Journal
Club
1500 ‐1600 Reg training 1600 ‐1700 Neuro MDT
monthly Lung MDT 4
1. pathology conference room, 2. NICU conference room, 3. onc
conferenceroom, 4. Oncology conference room.
2. Consultant ward rounds are 2-3 times a week and more often
for sick patients.
-
8/19/2019 Med Onc Jnr Handbook
5/35
5
Educational aims for this rotation:
1. Management of complications of chemotherapy
2. Familiarise with common chemotherapy regimens
3. Management of medical emergencies
4. Management of quality of life issues
5. Understanding of psychosocial issues related to cancer
patients- discussing prognosis, breaking bad news, family meetings
etc
6. Understanding of curative vs palliative intent therapy
7. Familiarise with the management of common malignancies
includingmultidisciplinary approach
Tasks:
1. Managing inpatients – routine inpatient care, ward
consultations, weekendroster ( it is the responsibility of the
registrars to do this roster).
Prior to consultant ward rounds, results should be available for
imagingstudies, histology and blood tests.
(For interns, all the procedures except IV cannulation need to
besupervised by registrars or consultants).
2. Review of day unit patients
3. Review of clinic patients
4. Phone consults from GPs, other staff and the patients
Day unit and clinic patient review:
1. To assess fitness for chemotherapy2. To assess symptoms and
side effects of treatment.3. To address new concerns4. To assess
for treatment response-
a. tumour markers b. scans- performed after 2-3 cycles,
5. To update chemotherapy scripts
-
8/19/2019 Med Onc Jnr Handbook
6/35
6
Principles of management of patients on chemotherapy
Assessing fitness for chemotherapyFitness for chemotherapy
depends on three factors:
performance status the type and severity of side effects from
previous cycles of chemotherapy (if
any) blood parameters Co-morbidities
If cure is the aim, it is usual to accept mild-to-moderate,
non-life-threateningtoxicities and continue treatment without
delaying or reducing the dosage tominimise side effects. However,
in patients with incurable metastatic disease wherequality of life
is paramount, dose delays or dose reductions are necessary.
Performance status
This is graded using the Eastern Cooperative Oncology Group
(ECOG) scale.
Grade ECOG performance status0 Fully active, able to carry on
all pre-disease performance without
restriction
1 Restricted in strenuous physical activity but able to carry
out work ofa light sedentary nature
2 Ambulatory and capable of all self-care but unable to carry
out anywork activities
3 Capable of only limited self-care, confined to bed or chair
more than50% of waking hours
4 Completely disabled, cannot carry on any self-care, totally
confinedto bed or chair
Usually, patients with ECOG grade > 2 are not fit for
chemotherapy. The exception is
chemotherapy-sensitive cancers such as lymphoma and small cell
lung cancers. Thedecision to offer chemotherapy must be
individualised depending upon factors likeage of the patient,
comorbidities, etc; For example, a young patient with
metastatic
breast cancer with poor performance status could still be
offered systemic treatments.Targeted agents and endocrine therapy
are usually tolerated better than chemotherapy.
Toxicity from previous cycles of chemotherapy :
Clinicians must assess whether a side effect is affecting
function or is life threatening:
First, determine the type and severity of side effects.
-
8/19/2019 Med Onc Jnr Handbook
7/35
7
For example, in patients with early breast cancers undergoing
taxane chemotherapy,mild peripheral neuropathy is acceptable.
However, in patients undergoingfluorouracil-based therapy, ongoing
or severe diarrhoea necessitates a dose delay anddose reduction of
subsequent cycles.
Mid-cycle neutropenic fever usually requires dose reduction of
the subsequent cycleunless the cancer is curable. If the cancer is
curable or a substantial duration ofremission is expected,
prophylactic colony stimulating factors such as
pegfilgrastim(neulasta) and/or antibiotics can reduce the risk of
opportunistic infection.
Next, determine the effects on important organs, such as:
Fertility. Discuss semen cryopreservation with men. There are no
proven useful procedures for women, however preservation of egg,
embryo and a piece ofovary is offered by some fertility groups.
Women who wish to discuss thisoption should be referred to a
fertility specialist.
Renal function, liver functions. Cardiac function. This may
affect the dosage of anthracyclines (check ejection
fraction before treatment begins and after every 2–3 cycles) and
trastuzumab(check ejection fraction before treatment begins and
every 3 months duringtherapy).
Toxicity is graded according to NCI common terminology criteria
for adverse events 1
1.Blood parameters:
(a) Requires haematological and non-haematological
parameters.For most regimens, a neutrophil count >1.5 x 10 9/L
and platelet count > 100 x 10 9/Lare needed for safe
administration of chemotherapy. For weekly Taxol, neutrophilcount
of >1.0 x 109/L and platelet count of >75 x 109/L is
acceptable.
Some regimens, like single agent bleomycin and vincristine, are
not myelotoxic andadministration is not affected by blood
counts.
Renal function is important for cisplatin and carboplatin and
liver function fordocetaxel. .Magnesium levels esp for
cisplatin.Calcium levels for denosumab.
Action- withhold treatment until recovery, then dose delay
and/or dosereduction.
(b) Pregnancy test: For women of child bearing potential, if
they are not sure ofpregnancy status, perform beta HCG before
initiating treatment.
-
8/19/2019 Med Onc Jnr Handbook
8/35
8
2:Non-haematological toxicity
( Also see the summary of common SEs for seleceted drugs in
page11)
a. Diarrhoea – mainly 5FU based, Irinotecan, Oxaliplatin,
Taxotereaction- low threshold for withholding therapy if diarrhoea
the day before
or moderate diarrhoea for longer than expected duration or
nocturnaldiarrhoea.
b. Mucositis/mouth care
c. EmesisAction-( see antiemetics) change class, add another
agent or dosereduction.
d. Skin Rash
e. Neuropathy- Cisplatin, Oxaliplatin, Taxanes, Vinca
alkaloidsdose delays or reduction if neuropathy persist or
interferes with function.
f. Autotoxicity- Cisplatin
g. Renal impairment- Cisplatin.Action- prior to most agents,
need to check creatinine especially if they arerenally
cleared.Carboplatin- dose adjusted based on creatinine.
h. Pulmonary toxixcity- bleomycin, methotrexate
3. physical examination-routine exam and mouth, central lines,
lymph nodes andsigns of recurrence and side effects.
When to s top cancer treatmentA decision to stop treatment
prematurely depends on the aim of the treatment.
For curable cancers, it is acceptable to continue treatment with
dose modifications.However, life threatening or severe dose
limiting toxicities usually necessitatecessation of treatment (eg.
moderate to severe peripheral neuropathy with taxanes
andoxaliplatin, severe enteritis from fluorouracil). Alternative
regimens are sometimesavailable.
If the cancer is incurable and the toxicities severely interfere
with the activities of
daily living, treatment may have to be stopped.
-
8/19/2019 Med Onc Jnr Handbook
9/35
9
Deteriorating performance status and organ function usually
require cessation oftreatment. Ongoing neutropenia or
thrombocytopenia typically means the patient isnot going to handle
further chemotherapy.
If the cancer is not responding to the therapy after 2–3 cycles,
cessation of the sametherapy is advised.In case of patients with
metastatic disease, palliative care team referral is done evenwhen
they are on active treatment , to improve symptom management and
supportivecare.
Important practice points for common drugs:
1. Adriamycin/ Epirubicin - look at cumulative dose, perform
cardiac function
every 2-3cycles.
2. Bleomycin - Lung function every 3 weeks.
3. Cisplatin - renal function, Mg levels, peripheral neuropathy,
hearing loss/tinnitus.
4. Carboplatin - adjust dose based on renal function.
Dose= AUC x (GFR+25).
5. 5-FU - diarrhoea. In severe cases, it can be life
threatening.
No diarrhoea on the day and the previous day of chemo.
If diarrhoea daily, consider dose reduction.
5FU could also cause coronary Artery spasm.
In severe 5FU enteritis, admission for bowel rest +/-TPN along
with aggressive
anti diarrhoeal and antibiotics may be required.
6. Gemcitabine - pneumonitis, peripheral edema.
7. Irinotecan - need to have normal bilirubin. diarrhoea,
flushing- acute symptoms
could settle with atropine with chemotherapy. For chronic
symptoms,
dose reduction is necessary.8. Taxol/ Paclitaxel - peripheral
neuropathy, flu like symptoms
9. Taxotere/Docetaxel - adequate liver function, peripheral
edema, neuropathy, rash.
10. Oxaliplatin - cold induced paresthesia( acceptable), but
signs of peripheral
neuropathy may be dose limiting. Laryngo spasm (cold
induced)
and bronchospasm are other acute side effects.
11. Cyclophosphamide/ Ifosfamide - renal function, hydration,
confusion from
encephalopathy.12. Xeloda - mucositis, hand foot syndrome, rash,
angina, diarrhoea.
-
8/19/2019 Med Onc Jnr Handbook
10/35
10
13. Herceptin - cardiac function every 3 months.
14. Erbitux - acneform rash. Presence of k-ras mutation is
associated with no
response from erbitux.
15. methotrexate - folinic acid rescue.
16. Caelyx/ Liposomal doxorubicin - rash, hand foot syndrome,
cardiac function.
17. Avastin - hypertension and proteinuria.18. Denosumab -
prolonged hypocalcaemia(require calcium suppliments).19.
Vemurafenib (b-raf inhibitor)- rash,squamous cell carcinomas of
skin.20. Zelodronic acid -renal function, hypocalcaemia, requires
dose reduction
for renal impairment. Need calcium suppliments
Alopecia- not with every drug.Common with breast, ovarian,
sarcoma, small cell, lung(Carbo/Taxol) cancer and
testicular regimens
COMMON CHEMOTHERAPY ABBREVIATIONSBREAST CANCERTAC : Docetaxel,
Adriamycin, CyclophosphamideFEC : 5Fluorouracil, Epirubicin,
CyclophosphamideAC : Adriamycin, Cyclophosphamide
COLO-RECTAL CANCER
FOLFOX : Oxaliplatin, Continious infusion 5Fluorouracil and
LeucovorinXELOX : Oxaliplatin, CapecitabineFOLFIRI : Irinotecan,
Continious infusion 5 Fluorouracil and LeucovirinXELIRI :
Irinotecan, Capecitabine
GASTRIC/LOWER OESOPHAGEALECF : Epirubicin, Cisplatin, 5
FluorouracilECX : Epirubicin, Cisplatin, CapecitabineEOX :
Epirubicin, Oxaliplatin, Capecitabine
HEAD AND NECK CANCER
TPF : Docetaxel, Cisplatin, 5 Flurouracil
TESTICULAR CANCERBEP : Bleomycin, Etoposide, CisplatinTIP :
Ifosfamide, Paclitaxel, Cisplatin
-
8/19/2019 Med Onc Jnr Handbook
11/35
11
Common side effects of oncology medications
Combinations are more likely to cause myelosuppression and
emesis than single agents.Myelosuppression Mucositis Enteritis
Alopecia Cardiac Renal Neuropathy
Anthracyclines ++ + ++ + Bleomycin Capecitabine ++ ++ angina
Carboplatin ++ +Cisplatin + ++ ++Cyclophosphamide + + + 5FU ++
++ angina Fotemustine ++ +Gemcitabine + + Irinotecan + ++ +
Oxaliplatin(combinedwith 5FU)
+ + ++ angina ++
Paclitaxel + ++ ++Taxotere/Docetaxel + + ++ ++ permetexed +
+
Monoclonal antibodies and small moleculesInfusionreaction
Anaphylaxis cardiac rash thyroid Proteinuria diarrh
Trastuzumab + + +Bevaczuzumab + + + Cetuximab + + ++Sunitinib ++
+ +
Erlotinib ++
-
8/19/2019 Med Onc Jnr Handbook
12/35
12
Chemotherapy related emesis :
Causes of nausea and vomiting in patients receiving
chemotherapy:1. Chemotherapy related
2. Other causes like gastro-oesophageal reflux disease or
medications likeopioids.
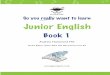
Pathways by which chemotherapeutic agents may produce anemetic
response 2
Chemotherapy-induced emesis results from stimulation of a
multistep reflex pathwaythat is controlled by the brain and
triggered by afferent impulses to the vomitingcenter from the
chemoreceptor trigger zone, gastrointestinal tract (by way of
vagalafferent fibers), and possibly, the cerebral cortex.
-
8/19/2019 Med Onc Jnr Handbook
13/35
13
Emetogenic potential of chemotherapy agents
High (>90%) Moderate (60-90% Moderate(30-60%)
Low(10-30%)
Minimal
Cisplatin>50mg/m2
Carboplatin Cyclophos60mg/m2 Doxorubicin20-60mg/m2
Caelyx Cetuximab
Epirubicin>90mg/m2 Epirubicin
-
8/19/2019 Med Onc Jnr Handbook
14/35
14
Antiemetics:
1. Neurokinin 1 receptor antagonist- Aprepitant (emend),
fosaprepitant
2. 5HT3 antagonists: ondansetron (zofran), granisetron &
palonosetron(aloxi)
3. Dopamine antagonists : 1.Phenothiazines- prochlorperazine, 2.
Benzamides:Metoclopromide. 3.butyrophenons-haloperidol
4. Glucocorticoids:- good for early and delayed nausea.
5. Anti histamines:Promethazine
6. Benzodiazepins: Lorazepam-good for anticipatory emesis
High emetogenic drugs and anthracycline containing regimens for
breast
cancer :3
Emend (Aprepitant)-
Day 1- 1 hour pre chemo 125 mg orally,day 2 and 3- 80 mg
daily.
Plus
Aloxi (Palonosetron) 250 mcg IV on Day 1 only or Zofran (
Ondansetron) 8mgbd for 2-3 days starting the night of
chemotherapy.
Plus
Dexamethasone- 8-12 mg IV pre-chemo and 8mg oral mane for 2-3
days.
NB- for patients who experience sudden decline in well being
when steroids arestopped, a weaning off regimen might be
useful.
Maxolon- 10 mg Q6H PRN.
NB- Zofran can be constipating- so warn pts about prevention of
constipation. Donot prescribe take-home zofran after Aloxi.
Moderately emetogenic drugs or combination of drugs:
Aloxi (Palonosetron) 250 mcg IV on day 1.Plus
Dexamethasone- 8 mg IV pre-chemo and 8mg oral mane 2-3 days
NB- for patients who experience sudden decline in well being
when steroids arestopped, a weaning off regimen might be
useful.
-
8/19/2019 Med Onc Jnr Handbook
15/35
15
Emend can be added to the above regimen if the patients
experience nausea &vomiting after moderately emetogenic
chemotherapy.
Maxolon- 10 mg Q6H PRN.
.
Mildly emetogenic drugs:
Usually maxolon premedication with maxolon 10 mg Q6H PRN would
be enough. Ifnausea not controlled with maxolon, might have to
treat it like moderate drugs afterexcluding other causes of nausea.
Eg- GORD.
If nausea persists, look for other causes.Addition of lorazepam
1 mg Q6H PRN useful esp for anxious patients
INFECTIONS
Neutropenic Fever 4, 5
It is a medical emergency. It is the responsibility of the MO to
ensure promptantibiotic administration.
With diarrhoea and neutropenia, even if afebrile, use the same
protocol.
Definitions
A single oral temperature of 38.3 0 A temperature ≥ 38 0 on two
occasions over 1 hour ANC ≤ 500 or less ≤ 1000/µl with predicted
rapid decline to less than 500/µl
Septic Work-Up
Physical examination
Blood cultures x 2 sets (venipuncture and indwelling venous
catheter if present),urine C&S, cultures from any suspected
sites, CXR .)
Treatment of Neutropenic Fever : 6 Antibiotics
Cefepime* IV 2 g BDor Piperacillin/ tazobactam (Tazocin) 4.5 gm
Q6-8 hourlyor Ceftazidime 2 gm 8 hourly.
In patients with hypersensitivity to pencillins, seek expert
advice.
-
8/19/2019 Med Onc Jnr Handbook
16/35
16
Modifications
Add Gentamycin 5-7 mg/kg/IV if patient is unstable or has
pneumoniaor in suspected gram-negative infection.
Add Vancomycin 1 g 12 hourly if clinically unstable, gram
positive bloodcultures before antibiotics, severe mucositis
present, already on Quinolone
prophylaxis, a catheter associated cellulitis or tunnel
infection, high prevalenceof Methicillin-resistant staph
aureus.
Metronidazole for abdominal symptoms or suspected C. difficile
infection.
Persistent neutropenic fever on D5 – add antifungal therapy
(Amphotericin B0.5mg/kg/day or Fluconazole 400mg/day)- But discuss
with consultants first.
Duration of Antibiotics (variable) Low risk patient (clinically
well, stable signs, no mucositis, ANC >100/µL, rising
ANC, afebrile within 3 days of starting antibiotics, negative
cultures) considerearly discharge on Day 4 on oral Ciprofloxacin
750mg BD for 5 days or ceaseantibiotics altogether when ANC
>500/µL
High risk patients who become afebrile within 3 days, should
continue parenteralantibiotics, targeted to the specific pathogen,
until resolution of neutropenia
Specific pathogens need to be treated according to therapeutic
guidelines
Patients with any of the following characteristics are
considered to be at high risk for seriouscomplications during
episodes of neutropenic fever:
Neutropenia (absolute neutrophil count 7 days*
Presence of any comorbid medical problems, including, but not
limited to:
Hemodynamic instability
Oral or gastrointestinal mucositis that interferes with
swallowing or causes severe diarrhea Gastrointestinal symptoms,
including abdominal pain, nausea and vomiting, or diarrhea
Neurologic or mental status changes of new onset
Intravascular catheter infection, especially catheter tunnel
infection
New pulmonary infiltrate or hypoxemia
Underlying chronic lung disease
Complex infection at the time of presentation
-
8/19/2019 Med Onc Jnr Handbook
17/35
17
Inpatient status at the time of development of fever
Uncontrolled or progressive cancer Δ
Evidence of hepatic insufficiency (defined as aminotransferase
levels >5 times normal values) orrenal insufficiency (defined as
a creatinine clearance of 1000 µL
Add Vancomycin 1 g 12 hourly
Re-evaluate on Day 5
Febrile Afebrile
Add Amphotericin B (1-1.5 mg/kg/day) or Continue antibiotics for
5 days
Fluconazole 400mg/day or until neutrophils >1000 µL
Consider non infective causes of fever
-
8/19/2019 Med Onc Jnr Handbook
18/35
18
Colony stimulating factors (GCSF) are generally not recommended
in managementof febrile neutropaenia, with some exceptions.
Catheter-related infections;
Catheter removal is recommended in addition to antibiotic
therapy for at least 14days. But if the infection is caused by
coagulase-negative staphylococci and isimportant to save the line,
catheter could be retained using systemic antibiotics.
EXTRAVASATION OF CHEMOTHERPAY DRUGS 7
If it does occur, proper documentation should include the time,
site of line insertion,
needle
size, estimated amount of extravasated drug, technique used to
manage the
extravasation, appearance of site, photograph, patients
comments, and notification of
physician.
Management
Stop infusion. Before removing cannula attempt to aspirate some
of extravasated
fluid. If antidote exists give it both IV through cannula and by
SC infiltration (see
table).
Intermittent local cooling is recommended, except for vinca
alkaloids (warming
packs). Rest and elevate the affected site for 48 hours.
Telephone contact daily and
assess need for plastic surgery.
-
8/19/2019 Med Onc Jnr Handbook
19/35
19
Antidotes for Ves icant and Irr it ant Dr ugs
Table 3
Chemotherapy agent Pharmacologicantidote
Nonpharmacologic Antidote
Method of Administration
Mechlorethamine
(nitrogen mustard)
Cisplatin (largeextravasation)
Sodium
thiosulfate
None Prepare 1/6 molar
solution: if 10%Na
thiosulfate solution, mix 4
mL with 6 mL sterile water
for injection.
Through existing IV line,
inject 2 mL for every 1 mg
extravasated. Inject SC if
needle is removed.
Vincristine
Vinblastine
Vindesine
Etoposide
Vinorelbine
Hyaluronidase Warm packs. 15-20
minutes at least four
times/day for the first 24-
48 hours and elevate
Prepare hyaluronidase,
150 units/mL with 1-3 mL
saline. Inject through
existing IV line, 1 mL for
each 1 mL infiltrated.
Inject SC if needle is
removed.
Doxorubicin
(Adriamycin)
Daunorubicin
Idarubicin
Mitomycin C
DMSO Ice packs Apply cold pad with
circulating ice water pack
or cryogel pack for 15-20
minutes at least four
times/day for first 24-48
hours. Some benefit of
99% dimethyl sulfoxide
(DMSO) 1-2 mL applied to
site every 6 hours.
Paclitaxel
Docetaxel
Hyaluronidase Ice packs As for Vinca alkaloids.
Premedications to prevent allergic reactionsPaclitaxel
Premedications
Recommended schedule:
- Dexamethasone 20 mg oral, 12 hours and 6 hours before
Paclitaxel (in practice
the night before and the morning of treatment).
- Promethazine 25 mg IV 30-60 minutes before therapy.
- Ranitidine 50 mg IV 30-60 minutes before therapy.
- Additional Dexamethasone IV as antiemetic depending if
Paclitaxel givenalone (4mg IV) or in combination with other
drugs.
-
8/19/2019 Med Onc Jnr Handbook
20/35
20
Modified regimen (in cases where the patient forgets to take
premedication, or 2 nd
and subsequent cycles where no hypersensitivity reaction
occurred with 1 st
treatment and steroids are not appropriate):
- Dexamethasone IV 20 mg 30 minutes before Paclitaxel.
- Promethazine IV 25 mg IV 30-60 minutes before therapy.
- Ranitidine 50 mg IV 30-60 minutes before therapy.
(Product Information, 2001)
(Markman M. J Clin Oncol 15(12): 3517, 1997.)
(Kintzel PE. Ann Pharmacother 35:1114-7, 2001.)
Modified schedule for weekly regimen (where steroids are not
appropriate):
1st Treatment - Dexamethasone 12 mg IV
- Promethazine 25mg IV
- Ranitidine 50mg IV
If no hypersensitivity reaction, subsequent treatments may be
given without
premedications.
(Quock J. Proc ASCO 18 abstr 635, 1999.)
Docetaxel Premedications
Recommended schedule for 3 weekly regimen:
- Dexamethasone 8mg BD oral x 6 doses (starting night before
treatment)
- Additional Dexamethasone IV as antiemetic depending if
Docetaxel used
alone (4mg IV) or in combination with other drugs.
(Product Information, 2001.)
Schedule for weekly regimen:
- Dexamethasone 8mg oral BD x 3 doses (starting night before
treatment)
(Jackisch C. Proc ASCO 19 abstr 417, 2000.)
-
8/19/2019 Med Onc Jnr Handbook
21/35
21
Monoclonal Antibodies
Trastuzumab (Herceptin) may cause fever and chills, chest
tightness and
tachycardia with 1 st infusion.
Rituximab (Mabthera) may cause asthenia, chills, bronchospasm,
hypotension,angioedema. Premedicate with Paracetamol 1 g QID,
Promethazine 25 mg IV
and Hydrocortisone 200 mg IV 30-60 minutes prior to drug.
Cetuximab requires phenergan 12.5mg or 25 mg prior to
infusion.
Medical Oncology Emergencies:Management of Neutropaenic fever is
discussed above.
Spinal Cord-compression
neurological symptoms and signs consistent with spinal cord
compression necessitates
1.urgent review and MRI of spine.2.Urgent neurosurgical and or
radiotherapy referral3. start Dexamethasone8mg IV stat , followed
by 16-24
mg daily in divided doses.
SVC Obstruction :
If the patient presents with stridor or respiratory compromise ,
emergency treatmentwith endovascular stent and Radiotherapy is
required.In other cases, a histological diagnosis is required prior
to initiating specifictreatment.
In chemotherapy-sensitive malignancies like small –cell lung
cancer, germ celltumour or lymphoma, systemic chemotherapy is
usually the treatment. In most othertum ours, including non-small
cell lung cancer, Radiotherapy is the
preferredtreatment.Endovascular stenting prived rapid relief of
symptoms.
Hypercalcemia:
Saline hydration.IV zolendronate.IV frusemide if fluid
overload.
Steroids useful in hypercalcaemia due to lymphoma.s/c
calcitonin.
-
8/19/2019 Med Onc Jnr Handbook
22/35
22
Infusion reactions and other acute reactions
Mild to moderate infusion reactions with no features of
anaphylaxis-IV hydrocortisone and phenergan. Stop infusion till
reaction subsides and restart at a
lower rate, with close monitoring.
Severe infusion reactions and anaphylaxis (hypotension,
angioedema,bronchospasm,generalised urticaria)- Resuscitaion with
epinephrine, hydrocortisone,phergan,ranitidine and fluids.DO NOT
RE-CHALLENGE.
Notes:
-
8/19/2019 Med Onc Jnr Handbook
23/35
23
Summary of management of common cancers: 8,9
This section outlines the principles behind the management of
common cancers.
For metastatic cancers, enrolment into a clinical trial is the
best treatmentoption.EviQ and NCCN guidelines offer up to date
practical guidelines for mostcancers.
Anal cancer-
Most cancers are treated with chemoradiation.*For chemo
radiation - mitomycin and 5FU.
Contraindication- ischaemic heart disease, severe diarhhoea.
*Metastasis - same regimen or cisplatin- 5FU.
Bladder- Non-muscle invasive disease is treated with surgery and
adjuvant intravesicaltherapies (eg. intravesical therapy with
BCG).
Muscle invasive disease is treated with surgery. Pre-op
chemotherapy improves
survival.
Inoperable disease may be managed with:
radiotherapy with or without radiosensitising chemotherapy
chemotherapy alone (platinum and gemcitabine), or palliative care
alone.
Metastatic disease is managed with above chemotherapy regimens
or palliative carealone.
Carbo AUC 5 or Cisplatin Day 1 and Gem 1000mg/m2 D1 and
Day8.
-
8/19/2019 Med Onc Jnr Handbook
24/35
24
Breast cancer-
Early breast cancers:
(Includes axillary node positive disease)
Mostly curative intent therapy.Post operative systemic treatment
depends on oestrogen and/ or progestogen receptorstatus, Her 2
status and prognosis ( risk of systemic relapse).
Prognosis- depends on prognostic factors.Size, age, grade,
axillary nodes, receptor status and lymphovascular invasion.
Low risk average High risksize 2 cmage
-
8/19/2019 Med Onc Jnr Handbook
25/35
25
In post-menopausal patients who are on treatment with tamoxifen,
switching to AIafter 2-3 years is recommended .5 additional years
of aromatase inhibitors after 5 years of tamoxifen improves
survivalin high-risk patients. 10 years of tamoxifen improves
survival compared to 5 years oftamoxifen.
For patients on AIs and documented osteopaenia (T score less
than 2.00), twice yearlyZometa decreases the rate of decline in
bone density. Thay are also encouraged totake regular calcium and
vitamin D tablets. Usually DEXA scans are done yearly totwo yearly.
Chemotherapy regimens -Lower risk average risk- r4 cycles of
Taxotere/Cyclophosphamide (TC), or 4x ACAverage risk- usually 6
cycles of anthracyclines (FAC)High risk- TAC x6 or FECx3 then
Taxoterex3 (PACS 01).Her 2 positive disease-Herceptin is combined
with Taxanes and not with anthracyclines because of
cardiactoxicity.In Her2 positive disease, a non-anthracycline
regimen ,TCarboH is an alternative 10
Neulasta- if cycles delayed because of neutropenia or had
neutropenic fever. PACS01 and TAC needs Neulasta day2 regardless of
neutropenia. All breast canceradjuvant regimens need Emend as well
as 5HT3 antagonist and dexamethasone forantiemetic prophylaxis.
Neoadjuvant chemotherapy:
Chemotherapy regimens are similar to adjuvant regimens. Assess
response clinicallyor by ultrasound.More effective in triple
negative or her 2 positive disease.
Post operative radiotherapy:
After lumpectomy, radiotherapy decreases local recurrence
rates.
After mastectomy, indications include:
close or positive margins >4 axillary nodes involved tumour
size >5 cm extensive lymphovascular invasion.
Radiotherapy is given after the chemotherapy is completed.
Locally advanced and inflammatory breast cancers
The cure rate is much lower than with early breast
cancers.Chemotherapy is given before surgery to reduce the size of
the primary and eradicate
micrometastases (see above for regimens).Radiotherapy is given
after surgery.
-
8/19/2019 Med Onc Jnr Handbook
26/35
26
Metastatic breast cancer-
• ER/PR positive bone only mets- hormones +/- Herceptin.•Bone
mets also benefit from monthly Bisphosphonates or Denosumab to
reduce pain,
skeletal events and hypercalcemia.•First line chemotherapy is
usually Taxanes or anthracyclines usually as single agentor with
cyclo. If the disease is aggressive and of high volume that
threatens survival,could offer triple agent combination like FEC or
TAC.•In Her 2 positive disease, Taxanes can be combined with
Herceptin as initialtreatment. Herceptin is continued as long as it
is effective. Once herceptin fails,lapatinib is second-line
anti-her 2 agent.•If there are metastases after adjuvant or 2 nd
line- Taxol/ Gemzar D1 and GemzarD8 on a 3 weekly cycle.•If
progression – Xeloda 900-1000mg/m2/ bd for 14 days.Other agents
include Caelyx, Taxotere and Vinorelbine.
Carcinoma unknown primary:
Poorly differentiated carcinoma with mediastinal or retro
peritoneal nodes esp inyoung people- could be germ cell.
Adenocarcinoma in the axilla - treat like breast.Adenocarcinoma
with peritoneal disease or liver mets in female - treat
likeovarian.Check CA 125.
Adenocarcinoma in males esp bone mets- could be prostate.
SCC -Nodal disease in the neck – treat like head and neck
cancer. Nodes in inguinal region—could be anal or vulval
primary.
Cervical cancer-
Early disease- surgery, locally advanced- chemoradiotherapy with
weekly cisplatin,
Metastatic- Platinum and 5FU.
Colon cancer-
*Stage 1 and stage 2 with no risk factors- surgery alone,
*Stage 2 with adverse features - possible benefit from
chemotherapy since the prognosis can be as bad as stage3.
-
8/19/2019 Med Onc Jnr Handbook
27/35
27
Adverse features- lympho vascular invasion, poorly
differentiated tumours,obstruction, perforation, invasion of other
organs.
5FU weekly at a dose of 500mg/m2 with leucovorin( 50 mg flat
dose).CI- unstable angina.
*Stage 3 -
FOLFOX using a Port-a-cath or XELOX .In patients who cannot
toleratecombination chemotherapy, Capecitabine (xeloda) is an
alternative.FOLFOX more effective than Xeloda. Difference is 7%
disease free survival.)
*Stage 4 ( includes rectal cancers)-
Consider resectability in selected patients: Those patients
would benefit from 3cycles of Oxaliplatin based regimen prior to
surgery then more chemotherapy.
Good performance, bilirubin
-
8/19/2019 Med Onc Jnr Handbook
28/35
28
GBM:Surgery is for resectable disease.For resected GBM,
Temazolamide with RT and 4 weeks later, 5days per month for 6months
improves survival.Temozolomide.
With RT- 75mg/m2/day M-F.After RT or on its own for palliation-
150-200 mg/m2/day for 5 days a month.
Check platelets in 2 weeks.
For recurrent Anaplastic astrocytoma- same as above.
Germ cell tumours-
Stage 1 -
Normally for stage 1 seminoma (make sure serum AFP normal)-
Single dose carboAUC 7, with neulasta. Check counts every week for
2 weeks post.Remember sperm banking. or wait and watch in selected
cases.
For stage 1 non seminoma - wait and watch (6 weekly markers and
3 monthly CTsfirst 2 years and later relax to 6 monthly scans and 3
monthly bloods for another 3years).or 2 cycles of BEP for patients
who are not reliable or who move around.
Stage 2 onwards-This includes patients with normal scans but
have the markers elevated fewweeks post orchidectomy.
Seminoma:
Stage 2 -
-
8/19/2019 Med Onc Jnr Handbook
29/35
29
Pre BEP treatment:
History of renal, auditory, neuropathy and vascular issues,Lung
function test- DLCO and lung volumes,Sperm banking( Semen
cryopreservation: In Townsville, this is performed by QFG),
ELFTS, FBC, LDH and markers.( Smoking to be
discouraged).Recurrent GCTs can still be cured by TIP or VIP
chemotherapy.
Prognostic groups:
Depend on site of primary, presence or absence of non pulmonary
visceral metastasisand marker level.
Seminoma:
Good prognosis Intermediate prognosisPrimary site any any
Presence of nonpulmonary metastasis
no yes
Markers( note- not AFP) any any
If Alfa Feto Protein is elevated, it is treated as non
seminoma.
Non Seminoma:
Good Intermediate PoorPrimary site Non mediastinal Non
mediastinal mediastinal
Non pulmonarymetastasis
no no yes
Markers
AFP 10000B HCG 50000LDH 10 x ULN
-
8/19/2019 Med Onc Jnr Handbook
30/35
30
Head and neck-
Resectable disease- Surgery.For high risk disease, post op
radiotherapy with chemotherapy improves survival.
Unresectable disease or organ preservation-
Induction chemotherapy followed by chemoradiotherapy.
Induction chemotherapy - 2 -3 cycles of TPF.Chemoradiotherapy -
weekly cisplatin 40mg/m2.
*If not fit for weekly cisplatin , abnormal renal function or
cardiac issues-Cetuximab (Erbitux) Loading dose 400mg/m2 one week
prior to RT and then weekly250mg/m2 weekly.
they need Phenergan 12.5mg or 25mg as premed.
Metastatic H&N cancer - (Cisplatin or Carboplatin) and
5FU.
Lung cancer-
Non Small Cell Lung cancers:
*Stage 1 to 3- Surgical resection offers the best chance of
cure.
For resected stage 1b, 2 or 3 -Adjuvant chemotherapy with
cisplatin/ vinorelbine x 4 cycles to improve survival infit and
-
8/19/2019 Med Onc Jnr Handbook
31/35
31
.In other patients with good performance status- consider
Cisplatin or Carboplatin /Gemcitabine( Day1 and Day 8).
Or Carboplatin/Taxol.
Once first line treatment fails- Permetexed (Alimta) 500mg/m2
every 3 weeks fornon-squamous histology And Docetaxel for squamous
cell carcinoma.( see under mesothelioma for Alimta precaution).
Once Alimta fails or cannot tolerate chemotherapy- EGFR TKI
Erlotinb (Tarceva) orIressa(Gefitinib) if there is mutation in EGFR
genes..Non metastatic pan coast tumours- chemoradiotherapy followed
by surgery.
Small cell lung cancer-
Limited stage -Cisplatin and etoposide x 4 cycles and radiation
as early as possible or Carboplatinand etoposide for 6 cycles and
radiation.At the end of the treatment, if no brain mets-
Prophylactic cranial irradiation to addanother 5% survival
benefit.
Extensive stage- Carboplatin and etoposide for 6 cycles. If
complete response that last for 6-12 months,could have re
treated.
Melanoma-
Stage 1 to 3- resection of the primary +/- sentinel node biopsy
and node dissection fornode positive disease.
For stage 3 disease- adjuvant Interferoncould offer a small
survival benefit . But hassignificant toxicity.Adjuvant
radiotherapy.
Stage4-
Resection of solitary metastasis could offer survival benefit,
even when they areon multiple organs.Unresectable disease:
Enrollment in clinical trials is the best approach.Check for B-raf
mutation . If B-raf mutated, consider targeted agents
likevemurafenib.
Chemotherapy; In fit patients even with brain mets-Fotemustine
100mg/m2/week for 3 weeks then rescan after a 4 week break.
If response and good tolerance without too much cytopenias-
100mg/m2 every 3weeks Fotemustine.
-
8/19/2019 Med Onc Jnr Handbook
32/35
32
Mesothelioma-
Surgical decortication can be useful in selected patients.
Otherwise, Carbo AUC 5 or Cisplatin and Alimta 500mg/m2 every 3
weeks.( Important- 1 week before Alimta- start VitB12 1000mcg IM
every 9 weeks and folicacid 0.5 mg daily until Alimta is
stopped.
Oesophagus:
SCC:
Curable:
Surgery or Chemo radiotherapy.
Chemoradiotherapy:
Cisplatin and 5FU. ( Cis 25mg/m2 daily x4 days, and 5FU 800
mg/m2/day x 4 daysvia CADD) week 1 and week 5 of RT.
Unfit- no chemo or Carbo/5FU. Carbo AUC 5.
Surgery:
Same chemotherapy for 3 cycles then Surgery.
Incurable:
Same chemotherapy for 2-3 cycles then reassess.
Adenocarcinoma:
Curable:ECF x3 then surgery then 3xECF.Incurable:EOX or ECX or
ECF.
-
8/19/2019 Med Onc Jnr Handbook
33/35
33
Ovarian cancer-( Epithelial ,not Carcino sarcoma or mixed
mullerian tumour)
Stage 1 - surgery, ( chemotherapy for rupture or positive
peritoneal washing)
Stage 2 onwards- debulking surgery, BSO/TAH
( In selected stage 4 this can be useful).Post debulking
surgery- Carbo AUC 5 and taxol 175mg/m2 every 3 weeks.If not so
fit- Carboplatin AUC 5 alone.
NB- patients who are unfit for surgery can be given chemotherapy
first and havesurgery later.Intraperitoneal chemotherapy is used in
selected stage3 disease, after optimumdebulking surgery.
If cancer returns 6 months after completeing Carbo or
carbo/Taxol, (this constitutes platinum sensitive relapse)- try
Carbo AUC 4 day 1 and Gem 1000mg/m2 day 1 andday 8.If less than 6
months ( platinum resistant relapse)- Caelyx 40mg/m2 every 4
weeks.
Pancreas-
Early disease-resection is the gold standard. Adjuvant
chemotherapy with 5FU or gemcitabine
offers survival benefit.
Metastatic -weekly Gemzar 1000mg/m2 for 7 weeks and 1 week off.
Then stage at the end of thisinduction. If response is confirmed, 3
weeks on 1 week off until progression or sideeffects limit.
Stomach/ adenocarcinoma of distal esophagus-
T1 and T2-Surgery alone.
T3 onwards for resectable disease:
Peri operative approach:MAGIC protocol - 3 x ECF → Surgery → 3
xECF.
Post operative approach:
Surgery → Mayo regimen 1 cycle( 5FU 425 mg/m2 and LV 50mg) → ( 4
weeks later)RT ( 5FU 400 mg/m2 and LV 50 mg- D1-D4 during week 1
and d1-3 during week 5)→ ( 4 weeks later) 2 cycles of Mayo.
Metastatic: EOX or ECX or ECF.
-
8/19/2019 Med Onc Jnr Handbook
34/35
34
Prostate-Treatment depends on disease stage and hormone
sensitivity.
Early stage disease is treated with surgery, radiotherapy (
external beam and/ or brachytherapy) or observation. Treatment
modality is individualised based on severalfactors: age and co
morbidities of the patient, serum PSA level, Gleeson score,clinical
stage and patient preference based on benefits and side effects of
therapy.
For example, a patient with clinically non apparent tumour with
Gleason score of
-
8/19/2019 Med Onc Jnr Handbook
35/35
Symptom controlDiscussion with palliative care is
helpful.However, basic principles are as follow:1. Pain ----always
find out the cause of the pain before prescribing analgesics
Total daily morphine requirement will guide to the required
daily slowrelease dose. When prescribing breakthrough---dose is 1/6
th of the daily dose. So, ifyou are increasing the daily dose,
break through need to increase as well. If oral intakeis
difficult—patches or infusional morphine are options.2. Dyspnoea
---again find out the cause, for cancer related
dyspnoea—morphinenebulised and anxiolytics could be helpful.
References:1. National cancer institute common toxicity criteria
( (CTCAE, version 4.03,
June 2010), National Institutes of Health, National Cancer
Institute .
http://ctep.cancer.gov .
2. Hesketh, P. J. (2008). "Chemotherapy-induced nausea and
vomiting." NewEngland Journal of Medicine 358 (23): 2482-2494.
3. Roila, F., J. Herrstedt, et al. (2010). "Guideline update for
MASCC and ESMOin the prevention of chemotherapy- and
radiotherapy-induced nausea andvomiting: results of the Perugia
consensus conference." Annals of Oncology21 Suppl 5 : v232-243.
4. Freifeld, A. G., E. J. Bow, et al. (2011). "Clinical practice
guideline for the useof antimicrobial agents in neutropenic
patients with cancer: 2010 Update bythe Infectious Diseases Society
of America." Clinical Infectious Diseases52 (4): 427-431.
5. National Comprehensive Cancer Network (NCCN) Clinical
PracticeGuidelines in Oncology. Prevention and treatment of
cancer-relatedinfections. Version 2.2011. www.nccn.org .
6. Therapeutic guidelines.
online-tg-org-au.cknservices.dotsec.com
7. Albanell & Boselga. sem oncol 27. 3:347-361, 2000
8. www.nccn.org.
9. www.eviq.org.au.
10. Slamon, D., W. Eiermann, et al. (2011). "Adjuvant
trastuzumab in HER2- positive breast cancer." New England Journal
of Medicine 365 (14): 1273-1283.