-
OtolaryngologyHead and Neck Surgery144(5) 662 675 American
Academy of OtolaryngologyHead and Neck Surgery Foundation
2011Reprints and permission:
sagepub.com/journalsPermissions.navDOI:
10.1177/0194599811399241http://otojournal.org
No sponsorships or competing interests have been disclosed for
this article.
Abstract
Background. Hearing loss associated with congenital
cyto-megalovirus (CMV) infection occurs in 0.2 to 0.6 per 1000
neonates.
Objective. The primary goal of this systemic review was to test
the following null hypotheses: (1) antiviral therapy has no impact
on congenital CMV-related sensorineural hearing loss and (2)
surgical therapy has no impact on congenital CMV-related
sensorineural hearing loss.
Data Sources. Computerized searches of MEDLINE and EMBASE
databases through September 2010 were performed, supplemented with
manual searches and inquiries to topic experts.
Review Methods. Studies were included based on review of 387
studies according to criteria developed a priori. Data extrac-tion
was performed by independent reviewers and focused on relevant
audiologic measurements, study designs, and potential
confounders.
Results. Criterion-meeting studies (n = 19) included a total of
446 participants. The largest randomized controlled trial (RCT)
suggested a significant protective effect of intravenous
ganciclovir against deterioration of hearing in neonates with
central nervous system manifestations of CMV infection. It also,
however, suggested a 3-fold increase in neutropenia. The second RCT
suggested that there may be no significant ben-efit of intravenous
ganciclovir for normal-hearing infants with asymptomatic congenital
CMV. Additional prospective and retrospective data evaluated the
impact of oral therapy and cochlear implantation in affected
patients.
Conclusion. Although results are mixed, the highest level of
evidence suggests that antiviral therapy confers a protective
benefit on neonates with hearing loss and symptomatic CMV. Cochlear
implantation can result in advancement of speech and language
skills, but there are mixed results compared with nonCMV-infected
patients.
Keywords
hearing loss, cytomegalovirus, antiviral, systematic review
Received November 16, 2010; revised January 4, 2011; accepted
January 13, 2011.
Congenital hearing loss is estimated to occur in 1 to 4 per 1000
live births in the United States.1,2 Congenital hearing loss may
result in developmental delay, lan-guage impairment, academic
deficiency, and lower perceived health status.3 Medical care for
children with hearing impair-ment has been estimated to cost 3
times that of normal-hearing children.3
Cytomegalovirus (CMV) is the most common congenital infection in
the United States, with the economic impact exceeding $2 billion in
this country alone.4-6 Data from cohorts followed in the United
States, Europe, and Canada suggest that congenital CMV occurs in 3
to 12 per 1000 newborns.5 Hearing loss is the most common
manifestation of congenital CMV infection, occurring in 15% to 65%
of affected patients.5 The hearing loss may manifest in infants
with or without cen-tral nervous system manifestation of CMV. It
may also occur at birth and be detectable during newborn hearing
screening, or it may occur years later. CMV-associated hearing loss
is estimated to occur in 0.2 to 0.6 per 1000 and may account for up
to 10% to 60% of congenital hearing loss.5
399241OTOXXX10.1177/0194599811399241Shin et alOtolaryngologyHead
and Neck Surgery The Author(s) 2010
Reprints and permission:sagepub.com/journalsPermissions.nav
1Department of Otology and Laryngology, Harvard Medical School,
Massachusetts Eye and Ear Infirmary, Boston, Massachusetts,
USA2Division of Head and Neck Surgery, Los Angeles Medical Center,
Southern California Permanente Medical Group, Los Angeles,
California, USA3Division of Pediatric Infectious Disease, Los
Angeles Medical Center, Southern California Permanente Medical
Group, Los Angeles, California, USA
Corresponding Author:Jennifer J. Shin, MD, SM, Division of Head
and Neck Surgery, Los Angeles Medical Center, Southern California
Permanente Medical Group, Los Angeles, California, USA, and
Department of Otology and Laryngology, Harvard Medical School,
Massachusetts Eye and Ear Infirmary, 243 Charles Street, Boston, MA
02114 Email: [email protected]
Medical and Surgical Interventions for Hearing Loss Associated
with Congenital Cytomegalovirus: A Systematic Review
Jennifer J. Shin, MD, SM1,2, Donald G. Keamy Jr, MD, MPH1 and
Evan A. Steinberg, MD3
Literature Review
at IMSS on May 26, 2015oto.sagepub.comDownloaded from
-
Shin et al 663
A variety of studies have been performed to assess the potential
impact of proposed therapies for hearing loss associ-ated with
congenital CMV, with mixed reports of efficacy. Proposed therapies
have the potential for serious adverse effects. Medical therapy may
result in neutropenia, thrombo-cytopenia, and liver dysfunction.
Surgical intervention intro-duces risks of facial nerve
dysfunction, cerebrospinal fluid leak, and wound problems. Thus, it
is critical to understand whether data suggest that intervention
confers a true benefit to affected patients. This systematic review
was therefore under-taken with the primary goal of testing the
following null hypotheses: (1) antiviral therapy (intravenous,
oral, or a com-bination) has no impact on congenital CMV-related
sensori-neural hearing loss and (2) surgical therapy has no impact
on congenital CMV-related sensorineural hearing loss. In addi-tion,
secondary inquiries were made into potential optimal therapies and
ages of intervention.
MethodsSearch StrategyA combination of computerized and manual
searches was performed to identify all relevant data. A
computerized PubMed search of MEDLINE ranging from 1966 to
September 2010 was performed. The medical subject headings
Cytomegalovirus and Cytomegalovirus Infections were exploded and
the articles collected into a first group. Next, articles mapping
to the subject headings Hearing Loss, Hearing Loss, Sensorineural,
Hearing Loss, High-Frequency, Hearing Loss, Unilateral, Hearing
Loss, Bilateral, Hearing Loss, Sudden, and Deafness were
exploded and collected into a second group. The 2 groups were
cross-referenced, yielding 180 articles. In addition, a PubMed
search from 1966 to September 2010 via the Endnote interface was
performed using keywords Cytomegalovirus and Hearing in all fields.
This search yielded 372 articles. A similar search was performed in
EMBASE through September 2010, cross-referencing the exploded
Emtree terms Cytomegalovirus or Hearing loss, which yielded 73
refer-ences. Reference lists for relevant narrative reviews and
crite-ria-meeting publications were searched manually for
additional studies. In addition, topic experts were contacted via
phone, email, or letter to determine if any additional stud-ies or
unpublished data could be identified. Studies were considered for
inclusion in the systematic review by 2 inde-pendent physicians.
The titles of all of the studies from these combined search methods
(n = 387) were evaluated according to the a priori
inclusion/exclusion criteria described below. This title evaluation
then yielded 134 potential abstracts, which were reviewed in more
detail according to the same criteria. Ultimately, 77 full articles
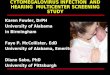
were evaluated against a priori criteria in detail (Figure 1).
Inclusion/Exclusion CriteriaThe articles identified by the
computerized and manual search strategy described above were
evaluated to identify those that met the following inclusion
criteria: (1) patients with congeni-tal CMV infection, (2)
intervention with medical (intravenous or oral) or surgical
therapy, (3) outcome measured in terms of hearing thresholds and
(4) hearing outcomes reported in com-parison to a control group or
in comparison to before treatment.
PubMed search of MEDLINE (n = 180)All fields search of MEDLINE
(n = 372)EMBASE search (n = 73)Manual search (n = 13)Field experts
(n = 6)
Citations initially identified*
Excluded based on a priori criteria (n = 253)
Included based on a priori criteria (n = 134)
Title search
Included based on a priori criteria (n = 77)
Excluded based on a priori criteria (n = 57)Abstract search
Inclusion in final analysis Included based on a priori criteria
(n = 19)
Excluded based on a priori criteria (n = 58)Complete article
search
Figure 1. Flow diagram showing the stages of identification of
studies for the systematic review.
at IMSS on May 26, 2015oto.sagepub.comDownloaded from
-
664 OtolaryngologyHead and Neck Surgery 144(5)
Congenital CMV infections were confirmed via urine, saliva, or
blood laboratory analysis of the affected infant. Hearing results
were quantified and described via auditory brainstem response (ABR)
or age-appropriate booth audiometry. Articles were excluded if (a)
no hearing results were reported, (b) hear-ing results were
reported only before or only after intervention but not both, (c)
hearing results were unclear relative to the timing of
intervention, (d) only maternal CMV status was analyzed, or (e)
only diagnostic measures for CMV were evaluated. Letters,
abstracts, and brief reports were included if sufficient
information was present to determine that the inclu-sion/exclusion
criteria were clearly met. This process yielded 19
criterion-meeting studies.
Data ExtractionData extraction was focused on items relevant to
the study results, potential sources of heterogeneity among those
results, and study identification (author, year of publication,
full reference citation). Extracted data included (1) the
num-ber/percentage with maintenance of hearing thresholds,
improvement in hearing thresholds, deterioration in hearing
thresholds; (2) the number of subjects in each group; (3) the P
value, confidence interval, standard error of the mean,
proportions, or descriptive statistics reported; and (4) the
follow-up time. Data collection also included multiple poten-tial
sources of heterogeneity among studies: (1) age at inter-vention,
(2) means of CMV diagnosis, (3) details of the medical (antiviral
type, dose, route of delivery, duration) or surgical intervention
regimen, (4) details of the control regi-men if applicable, (5)
audiologic criteria used for stratifica-tion of data, (6)
additional manifestations of CMV, (7) primary study endpoints, (8)
morbidity/complications of therapy, and (9) study design. Two
reviewers experienced in systematic reviews and clinical treatment
of CMV-affected infants evaluated the data independently using
standardized tables.
Quantitative Data AnalysisAn a priori plan was made to perform a
meta-analysis if the data were appropriate, meaning that study
designs, outcome measures, and follow-up periods were similar
enough. There proved, however, to be wide variation in study
design, audio-metric criteria, and reporting parameters, so a
quantitative meta-analysis was not performed.
ResultsStudy CharacteristicsThe 19 criterion-meeting studies
included a total of 446 par-ticipants, but some of these were lost
to follow-up, leaving 365 patients whose complete audiologic
results could be ana-lyzed. Studies evaluating medical therapy
included interven-tion with intravenous ganciclovir, oral
ganciclovir, oral valganciclovir, or a combination thereof. Studies
evaluating surgical intervention focused on cochlear implantation
for severe to profound sensorineural hearing loss associated with
congenital CMV. Study data and characteristics are described in
Tables 1 to 6.
Impact of Antiviral Therapy on HearingAmong studies assessing
the impact of antiviral therapy, there were 2 randomized controlled
trials (RCTs), 2 prospective cohort studies, 3 retrospective case
series, and 4 case reports (Tables 1-5).
Highest level of evidence. The larger randomized controlled
trial6 was conducted by the National Institute of Allergy and
Infectious Diseases Collaborative Antiviral Study Group. This RCT
evaluated neonates with symptomatic congenital CMV disease
involving the central nervous system. Hearing was assessed with ABR
at baseline, 6 months, and 12 months. Randomization effectively
balanced age, sex, race, prematu-rity, and multiple other potential
confounders between antivi-ral and control groups. Infants were
treated before 1 month of age with intravenous ganciclovir for 6
weeks. A placebo was not administered due to ethical concerns
associated with maintaining an intravenous catheter for 6 weeks in
a neonate, but the audiologist reviewing ABR results was masked to
the status of the treatment arm. Forty-two infants completed the
study; 100 were initially enrolled (58% attrition rate). A priori
power calculations were not described in detail, although an
initial plan to recruit 130 patients was described. The study was
terminated early by the data safety and monitoring board due to
favorable results in the interim analysis, as well as chal-lenges
in patient accrual and follow-up. The results suggested that 6
weeks of intravenous ganciclovir resulted in a signifi-cantly
improved prevention of deterioration of hearing in both the raw and
adjusted analyses (P < .01). While 41% of neo-nates in the
control group had worsened hearing at the 6-month follow-up, none
of the neonates who underwent ganciclovir therapy had hearing
deterioration. This significant decrease in risk persisted at the
12-month follow-up and regardless of whether a best ear or total
ear analysis was performed. There was, however, also a higher rate
of neutropenia in the ganci-clovir group (63% vs 21%, P <
.01).
The second, smaller RCT7 evaluated the impact of intrave-nous
ganciclovir on neonates 10 days of age with asymptom-atic
congenital CMV. Randomization effectively balanced confounders
between groups. All patients had normal hearing at the outset, and
18 of 23 completed the study. Hearing dete-rioration did not occur
in any of the infants treated with ganci-clovir, while 25% of those
in the control group had progressive hearing loss. The difference
was not statistically significant, although an a priori power
analysis was not reported. Neutropenia occurred in 2 (11.1%) of the
infants in the ganci-clovir group.
Treatment of symptomatic infants with intravenous ganciclovir
only. Multiple studies addressed the impact of treatment of infants
affected by symptomatic CMV disease with intrave-nous ganciclovir
only. The larger RCT6 discussed in detail above (see the Highest
Level of Evidence section) used intravenous ganciclovir 6
mg/kg/dose every 12 hours for 6 weeks and showed a significant
decrease in risk of progres-sion of hearing loss as compared with
no treatment. A pro-spective phase 2 cohort study8 utilized 6 weeks
of 8 or 12 mg/kg/d of intravenous ganciclovir for 6 weeks in
infants
-
665
Tabl
e 1.
Med
ical
Tre
atm
ent:
Ran
dom
ized
Con
trol
led
Tria
ls
Ref
eren
ce:
Kim
berl
in e
t al
(20
03)6
Lack
ner
et a
l (20
09)7
Leve
l (de
sign
):1
(ran
dom
ized
con
trol
led
tria
l)1
(ran
dom
ized
con
trol
led
tria
l)Sa
mpl
e si
zea :
42 p
atie
nts
(100
), 85
ear
s (2
00)
18 (
23)
patie
nts
Out
com
es
Best
Ear
A
sses
smen
tH
eari
ng
Impr
ovem
ent
Mai
nten
ance
of
Nor
mal
Hea
ring
Mai
nten
ance
of
Abn
orm
al H
eari
ngH
eari
ng
Det
erio
ratio
nH
eari
ng
Impr
ovem
ent
Mai
nten
ance
of
Nor
mal
Hea
ring
Mai
nten
ance
of
Abn
orm
al H
eari
ngH
eari
ng
Det
erio
ratio
n
Ant
ivir
al24
% (
n =
6/2
5)60
% (
n =
15/
25)
16%
(n
= 4
/25)
0% (
n =
0/2
5)0%
(n
= 0
/10)
100%
(n
= 1
0)0%
(n
= 0
/10)
0% (
n =
0/1
0)C
ontr
ol29
% (
n =
5/1
7)29
% (
n =
5/1
7)0%
(n
= 0
/17)
41%
(n
= 7
/17)
0% (
n =
0/8
)75
% (
n =
6/8
)0%
(n
= 0
/8)
25%
(n
= 2
/8)
P.0
5C
oncl
usio
nA
ntiv
iral
reg
imen
has
sig
nific
ant
effe
ct o
n pr
even
ting
dete
rior
atio
n of
hea
ring
in
adju
sted
and
una
djus
ted
anal
ysis
Tren
d to
war
d le
ss h
eari
ng d
eter
iora
tion
with
ant
ivir
al t
hera
py b
ut n
o si
gnifi
cant
di
ffere
nce
Follo
w-u
p tim
e6
mo,
1 y
Mea
n of
7.1
y (
SD, 2
.2; r
ange
, 3.2
-10.
3)
Stud
y D
esig
n
Incl
usio
n
crite
ria
Neo
nate
s (
1 m
o of
age
) w
ith s
ympt
omat
ic c
onge
nita
l CM
V d
isea
se in
volv
ing
the
CN
S, w
ith c
onfir
med
isol
atio
n of
CM
V fr
om a
uri
ne s
peci
men
. All
had
C
NS
dise
ase
such
as
(1)
mic
roce
phal
y, (2
) in
trac
rani
al c
alci
ficat
ions
, (3
) ab
norm
al C
SF fo
r ag
e, (
4) c
hori
oret
initi
s, an
d/or
(5)
hea
ring
def
icits
. Inf
ants
>
32 w
k ge
stat
ion,
>12
00 g
at
birt
h
Neo
nate
s
1.5
mg/
dL, H
IV, h
ydra
nenc
epha
lyM
icro
ceph
aly,
hydr
ocep
haly,
ven
tric
ulom
egal
y, ch
orio
retin
itis
or o
ther
oph
thal
mol
ogic
al
sym
ptom
s, he
pato
sple
nom
egal
y, th
rom
bocy
tope
nia,
neut
rope
nia,
anem
ia, j
aund
ice,
or
hear
ing
diso
rder
at
the
outs
etR
ando
miz
atio
n ef
fect
iven
ess
No
sign
ifica
nt d
iffer
ence
in a
ge, s
ex, r
ace,
pre
mat
urity
, ges
tatio
nal a
ge, w
eigh
t,
head
cir
cum
fere
nce,
abn
orm
al C
T o
r C
SF, A
LT, p
late
let
coun
t, bi
lirub
in,
sple
nom
egal
y, he
mal
omeg
aly,
base
line
ABR
, AN
C g
rade
No
sign
ifica
nt d
iffer
ence
in a
ge, s
ex, h
eari
ng a
t th
e ou
tset
Age
at
inte
rven
tion
1 m
o1
0 d
of li
fe
Mas
king
A s
ingl
e au
diol
ogis
t w
ho w
as m
aske
d to
ran
dom
izat
ion
revi
ewed
all
ABR
sN
ot r
epor
ted
Ant
ivir
al
regi
men
de
tails
Gan
cicl
ovir
6 m
g/kg
/dos
e IV
eve
ry 1
2 h
for
6 w
k; if
AN
C fe
ll be
low
50
0 ce
lls/m
m3 ,
ganc
iclo
vir
was
hel
d un
til a
ret
urn
to >
750
cells
/mm
3 , w
hen
it w
as r
esum
ed a
t th
e fu
ll do
se. I
f neu
trop
enia
rec
urre
d, t
he d
ose
was
de
crea
sed
by 5
0% u
ntil
the
AN
C r
ose
abov
e 50
0 ce
lls/m
m3 .
If ne
utro
peni
a pe
rsis
ted
at t
he 5
0% d
osag
e, g
anci
clov
ir w
as d
isco
ntin
ued
Gan
cicl
ovir
10
mg/
kg IV
for
21 d
ays.
If ne
utro
peni
a or
oth
er a
dver
se e
ffect
s oc
curr
ed,
the
dose
was
low
ered
to
5 m
g/kg
; the
rapy
was
sto
pped
if s
ide
effe
cts
did
not
reso
lve
Con
trol
reg
imen
de
tails
No
trea
tmen
t. A
pla
cebo
arm
was
not
use
d be
caus
e of
eth
ical
con
cern
s ov
er
mai
ntai
ning
intr
aven
ous
acce
ss fo
r 6
wk
No
trea
tmen
t
(con
tinue
d)
at IMSS on May 26, 2015oto.sagepub.comDownloaded from
-
666 Ref
eren
ce:
Kim
berl
in e
t al
(20
03)6
Lack
ner
et a
l (20
09)7
Leve
l (de
sign
):1
(ran
dom
ized
con
trol
led
tria
l)1
(ran
dom
ized
con
trol
led
tria
l)Sa
mpl
e si
zea :
42 p
atie
nts
(100
), 85
ear
s (2
00)
18 (
23)
patie
nts
Endp
oint
sT
he p
rim
ary
stud
y en
dpoi
nt w
as im
prov
emen
t by
1 g
rada
tion
in A
BR a
t th
e 6-
mo
follo
w-u
p (e
g, m
oder
ate
impa
irm
ent
impr
oved
to
mild
impa
irm
ent)
or
norm
al A
BR a
t bo
th t
ime
poin
ts. N
onpr
imar
y en
dpoi
nts:
thro
mbo
cyto
peni
a, he
patit
is, o
rgan
omeg
aly,
chor
iore
tiniti
s, ra
te o
f gro
wth
, dea
th.A
fter
the
thi
rd
inte
rim
ana
lysi
s, th
e D
SMB
reco
mm
ende
d ea
rly
term
inat
ion
base
d on
favo
rabl
e pr
elim
inar
y st
udy
resu
lts a
nd in
rec
ogni
tion
of c
halle
nges
in p
atie
nt a
ccru
al a
nd
follo
w-u
p
Hea
ring
loss
, alth
ough
chi
ldre
n w
ere
orig
inal
ly r
ando
miz
ed fo
r a
prev
ious
stu
dy. H
eari
ng
thre
shol
d w
as a
sses
sed
usin
g ea
r m
icro
scop
y, m
iddl
e-ea
r im
peda
nce
test
ing,
and
beha
vior
al o
bser
vatio
n au
diom
etry
unt
il 4
y of
age
; pur
e-to
ne a
udio
met
ry w
as u
sed
for
olde
r ch
ildre
n
Aud
iolo
gic
crite
ria
used
ABR
thr
esho
lds:
the
low
est
inte
nsity
leve
l at
whi
ch w
ave
V c
ould
be
dete
cted
and
re
plic
ated
. The
follo
win
g de
finiti
ons
wer
e us
ed: n
orm
al h
eari
ng, 0
to
20 d
B; m
ild
hear
ing
loss
, 21
to 4
5 dB
; mod
erat
e he
arin
g lo
ss, 4
6 to
70
dB; s
ever
e he
arin
g
loss
, >71
dB
Sens
orin
eura
l hea
ring
loss
was
def
ined
as
a m
edia
n se
nsor
ineu
ral d
ecre
ase
in h
eari
ng
of >
10 d
B he
arin
g lo
ss a
t lo
w (
125-
1000
Hz)
, mid
dle
(100
0-40
00 H
z), o
r hi
gh (
4000
-16
,000
Hz)
freq
uenc
ies
and
was
gra
ded
as m
ild (
25 t
o 40
dB
hear
ing
loss
), m
oder
ate
(41
to 6
5 dB
hea
ring
loss
), se
vere
(66
to
96 d
B he
arin
g lo
ss),
or p
rofo
und
(>96
db
hear
ing
loss
)Po
wer
Sam
ple
size
cal
cula
tions
pro
ject
ed 1
30 e
nrol
led
patie
nts
to p
rovi
de 1
00 e
valu
able
pa
tient
sN
ot r
epor
ted
Mor
bidi
ty/
com
plic
atio
ns63
% o
f gan
cicl
ovir
rec
ipie
nts
deve
lope
d gr
ade
3 or
4 n
eutr
open
ia, c
ompa
red
with
21
% o
f pat
ient
s in
the
con
trol
gro
up (
P
2.0
mg
Not
oth
erw
ise
spec
ified
Age
at
time
of
trea
tmen
t