Embed Size (px)
Citation preview

1
Medical Informatics II
Zlatko TrajanoskiInstitute for Genomics and Bioinformatics
Graz University of Technologyhttp://genome.tugraz.at
Medical Informatics II
• Introduction• Mathematical Foundations
– Biostatistics– Probability theory
• Computational Methods– Classification Methods– Clustering Methods– Hidden Markov Models
• Data and Data Management– LIMS– Standards– Data Integration– Electronic Patient Record– eHealth
2
Introduction
“Adjective” problem of the field:
• Medical Informatics• Bioinformatics• Biomedical Informatics• Biomedical Computing• Health Care Informatics• Public Health Informatics• Clinical Informatics• eHealth• Telemedicine• ….

3
IntroductionThe term biomedical computing ...is non-descriptive and neutral, implying only that computers are employed for some purpose in biology or medicine...We define medical informatics as the … scientific field that deals with the storage, retrieval, and optimal use of biomedical information, data, and knowledge for problem solving and decision making.
Shortliffe, E.H., Perreault, L.E., Wiederhold, G., and Fagan, L.M. (eds.) (1990). Medical Informatics: Computer Applications in Health Care and Biomedicine, Menlo Park: Addison-Wesley.
…medical informatics is a field of study concerned with the broad issues in the management and use of biomedical information, including medical computing and the study of the nature of medical information.
Shortliffe, E.H., Perreault, L.E., Wiederhold, G., and Fagan, L.M. (eds.) (2001). Medical Informatics: Computer Applications in Health Care and Biomedicine, 2nd Edition. New York: Springer-Verlag
storage, retrieval, and optimal use of biomedical information, data, and knowledge for problem solving, decision making, and research
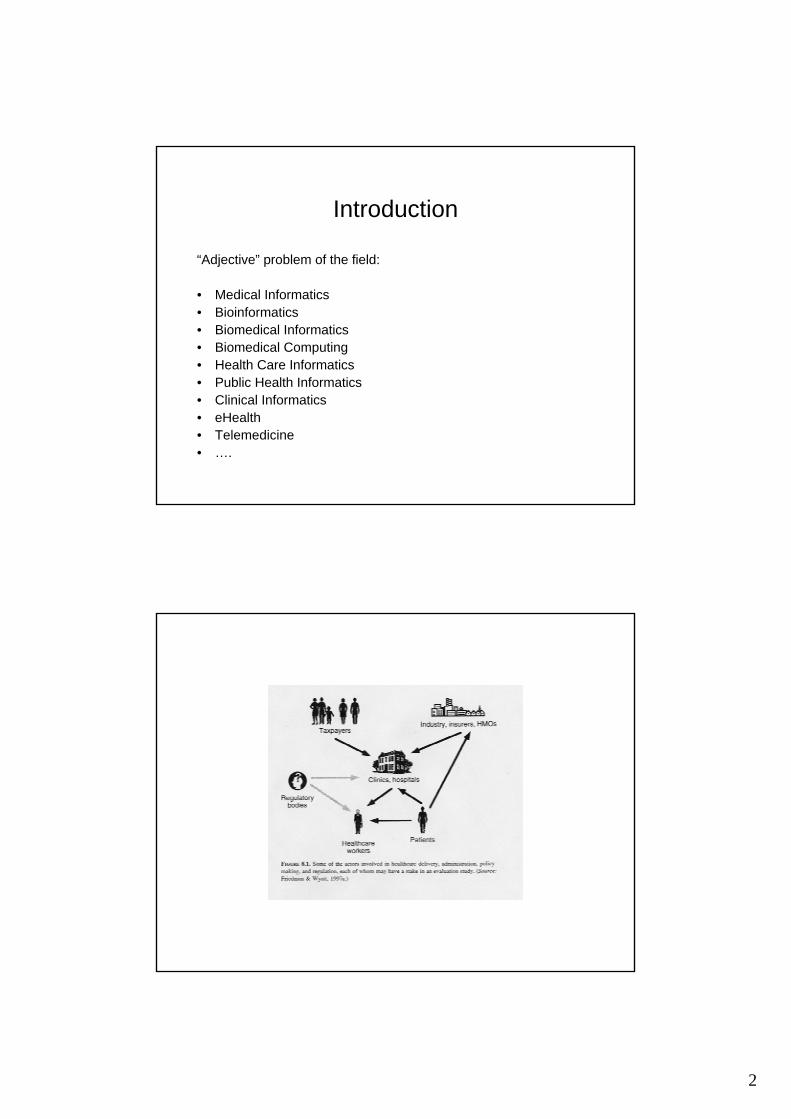
Introduction

4

5
Functions of computers in medicine
• Data acquisition and presentation• Record keeping and access• Communication and integration of information• Surveillance• Information storage and retrieval• Data analysis• Decision support• Education

6
Types of doctors
• Primary care provider– Internist, family practitioner, pediatrician
• Specialist– Medical– Surgical
• Hospital based provider– Anesthesiologist– Pathologist– Radiologist
Types of health interaction
• Healthy visit• Chronic visit• Diagnostic visit• Acute care

7
Locations of health care and documentation
• Office• Hospital• Home• Chronic care• Other hospitals• Abroad• Etc.
Types of information
• Textual• Trend• Lab data• 2/3D images• Administrative• Billing

8

9

10

11
• 2 and 3-d data sets– Echocardiography

12
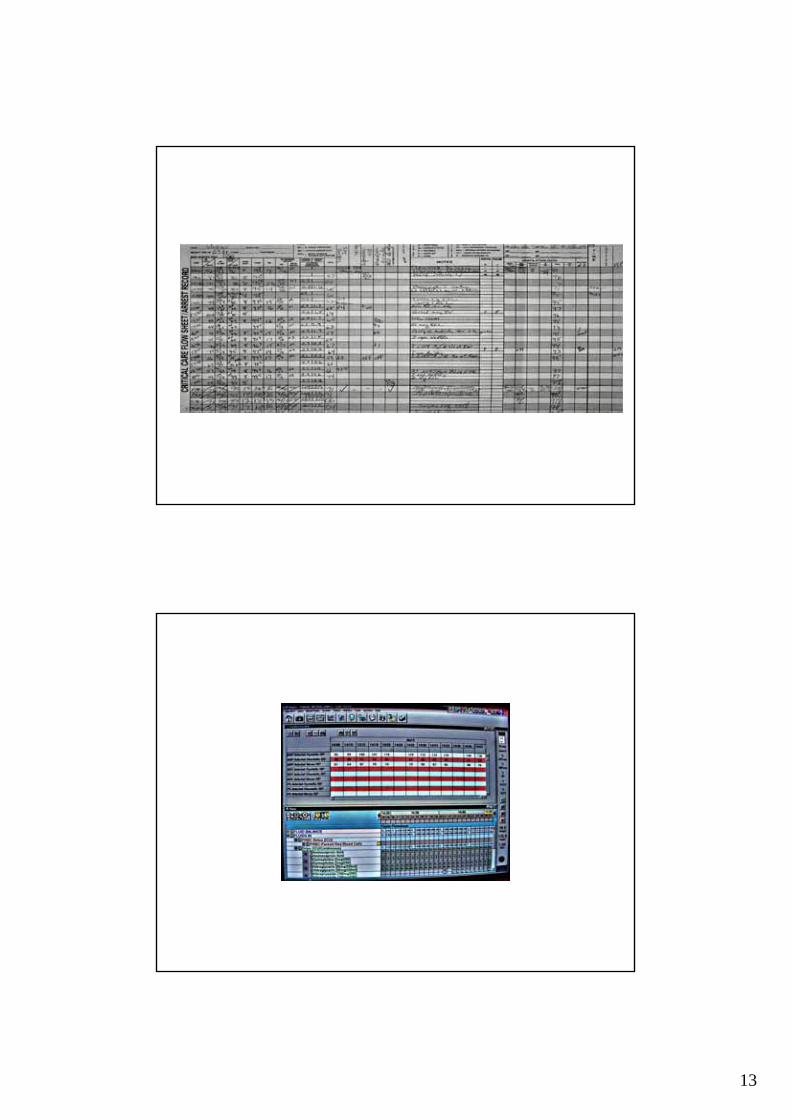
Data storage
• Current approaches• Computerized approaches• Visualization of data
13

14

15
History• John Snow (1813-1858)
a legendary figure in the history of public health, epidemiologyand anesthesiology.
http://www.ph.ucla.edu/epi/snow.html
The year was 1854; the scene was the Soho District of west London. During the stifling beat of August, there had been a handful of deaths from the dreaded disease cholera. Not unusual, in itself. But on August 31, the situation exploded: In a single evening, within a radius of only blocks, doctors reported 56 new cholera cases. By the next evening there were 143, and the death toll had reached 70 and was climbing. Residents started fleeing the district in panic. Medical authorities debated around the clock but couldn't settle on a plan of action.

16
17
Issues• Nature of medical information• Technical challenges• Uses of medical information
– medicine– research
• Status of development in field• Ethical concerns• (Professional Career Trajectories)
Uses of Medical Records
• Medical decision making-individual cases• Contractual (insurance…)
– Legal• Process improvement
– Clinical trials, evaluation of therapy• Basic human research

18
Information Types
• Textual– chief complaint, symptoms, history of present
illness, history, family history, physical exam, insurance information…
• Graphical– ECG, ultrasound, X-ray, hand-drawn figures…– longitudinal data (blood pressure graph)
• Digital/Image(X-rays, …)
Text Information• Structured Data Entry (forms)• Natural Language
– Processing essential for interpretation• “parsing” algorithms• Thesauri
– thrombophlebitis=phlebothrombosis, DVT, blood clot in the leg, milk leg, phlegmasia caeruleadolens, dropsy…
– generalized idiopathic lymphandenopathy (1980) => AIDS!!!
» “Change over time”
19
Text Standards
• Ideal Terminology– Complete, Formal, Universal, Translatable
• Candidate languages– SNOMED, UMLS, ICD, Read Codes, DSM
• Digital– Entry, storage, retrieval, usage?
Graphs/Images
• Archivable• Sharable• Searchable• Transmittable• Multiple input/output formats
– X-rays, ultrasounds, cameras…

20
Problems in Patient Records
• Errors, omissions, uncertainties
• Variability– Patient (day to day)– Physician
Current Provider Interface…48 yo wm ≠ 7d h/o N/V/Abdpain ≠ bilious emesis 3xQd –D –melena/BRBPR/mucous + f/c(t→102) ↓uop –UTI Sx + postprandial pain + EtOH(1case Qd)…
Pancreatitis/obstruction

21
Provider Input Interface
• Direct computer entry• Pen input/Speech recognition• Customizable, adaptable interface
Provider Display Interface
• Terminal– Patient Records– Supplementary info
• Drug characteristics• Medline records…
• Palmtop/PocketPC• Pocket reference

22
Patient Interface?
• WWW?• Physician• Physician extender
• Synchronous• Asynchronous• Reliable?
Impediments to Electronic Records
• Terminology/data types• Data entry methods• Diverse information needs
– ear infection vs bone-marrow transplant• Impact on physician-patient• Impact on physician-patient-society
– confidentiality, responsibility

23
Experience with Electronic Records
• Reliability problems– Why not as good as electronic banking!
• Free-text fields (clinical notes)– Nomenclature
• Interfacing with other systems• Enormous cost of switchover
– who pays that cost, especially in era of direct accountability in patient care?
Medical Uses of Enhanced Records
• Enhance clinical decision making• UKHMO: what are your current meds?• Rapid, rational query of records• Potential for increased use of knowledge systems (eg.
Drug interactions)– ACE inhibitor sensitivity, ER doc
• Enhanced delivery of care• Monitoring clinical success
– all patient records become clinical trials

24
Medical Delivery Issues
• Periodic health screening– enhanced reminders
• Physician variability– managed care can reduce variability
• Data quality, type varies from physician to physician
Research Uses
• Epidemiology– Infectious disease– Life history, risk factor...
• Medical Genetics– Basic disease work
• Pharmacogenomics
• Tissue Banks• Pedigrees/Populations• DATAMINING
25
Research Uses
• Cancer Immunology• Cancer Diagnostics
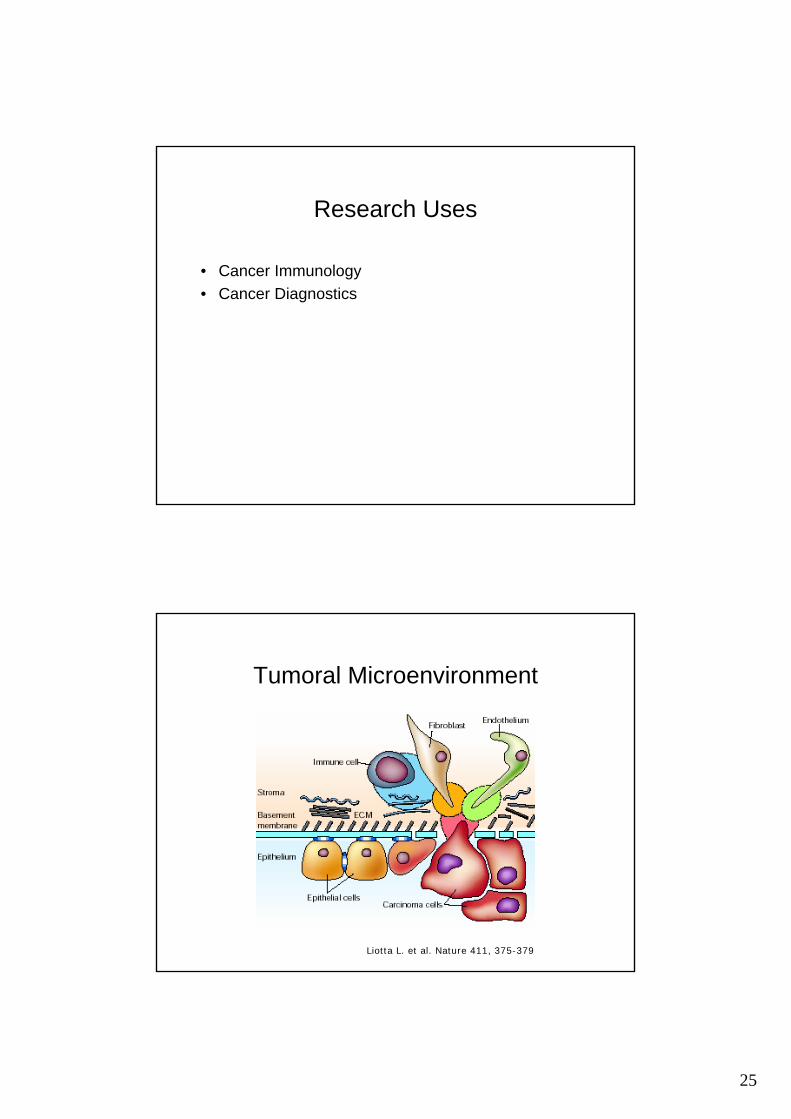
Tumoral Microenvironment
Liotta L. et al. Nature 411, 375-379

26
Tumoral Microenvironment
• How to analyze?– Fluorescence Activated Cell Sorter (FACS)
(different molecules on single cells)• Phenotypic studies• Proliferation studies
– cDNA Microarrays (average transcript levels across cell populations)
– Tissue Microarrays• Prerequisites
– Information• on patient or donor• on experimental conditions
FACS
• Important tool to answer immunological questions (since 1970)– How many cells express a target antigen?
• Distinguish between several cell types
– The size of cells– Distribution of cells according to antigen density
• Same cell types may express different levels of antigen depending upon development and physiological state
– Proliferation analysis

27
FACS
• Phenotype Analysis– Phenotype is a physical manifestation of internally
coded, inheritable information of a genotype, which encodes and maintains the cells entire behaviour and structure.
– to distinguish different cell populations within a multicomponent mixture
• Proliferation Analysis– to examine the cells‘s behaviour of cell division
under certain conditions
FACS – Phenotype Analysis(2 parameters, 8 gates, 50 antigens)
X
- % of cell population
CD3- MFI of cell population
MFI
%

28
CFSE
IL-15
0
CD3
CD3
FSC
SSC
SSC
MFI proliferating T cells % proliferating T cells
Number of cell cycles
% T cells
% Non-proliferatingT cells (and MFI)
1 cell cycle% Cells alive% dead andapoptotic cells
% proliferating cells
increase / decrease
FACS – Proliferation Analysis(10 parameters, 4 activations, 11 stimulations)





























