Embed Size (px)
Citation preview
Medication Overuse Headache Medication Overuse Headache
Morris Maizels MDMorris Maizels MD
Blue Ridge Headache CenterBlue Ridge Headache Center
Asheville Asheville Hendersonville NC Hendersonville NC
Migraine RememberedMigraine Remembered
SS evere evere
UU ni- ni-
LL ateral ateral 2 of 1st 42 of 1st 4
TT hrobbing hrobbing
AA ctivity worsens ha ctivity worsens ha
NN ausea ausea
SS ensitive to light/sound ensitive to light/sound 1 of last 21 of last 2
Headache is Headache is episodicepisodic, and usually lasts 4-72 hours, and usually lasts 4-72 hours
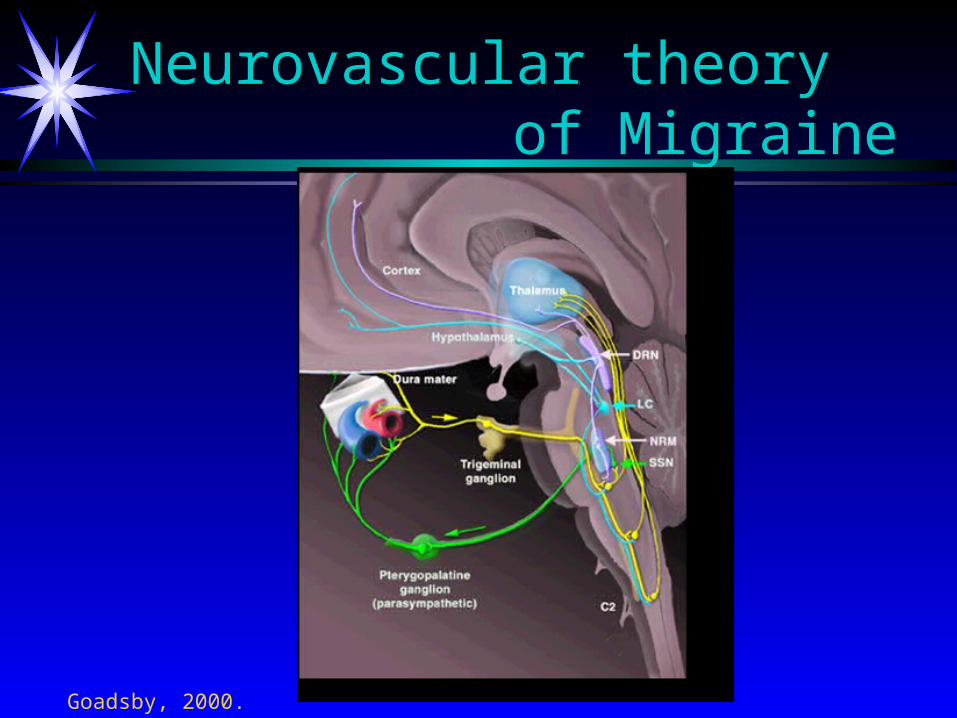
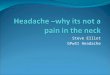
Neurovascular theory of Migraine
Neurovascular theory of Migraine
Goadsby, 2000.
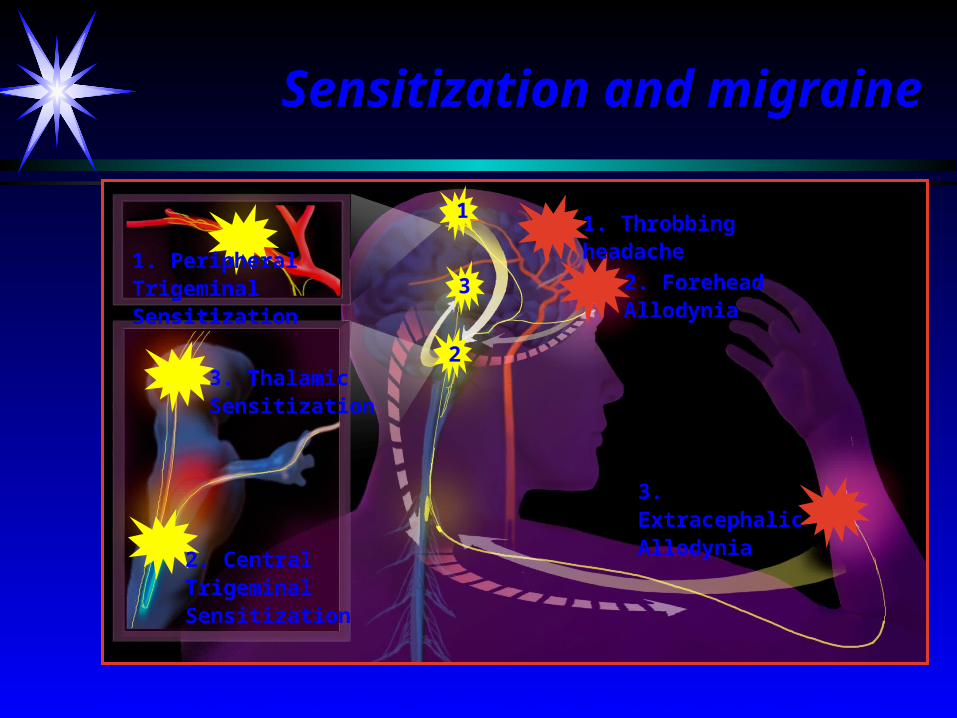
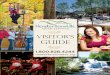
Adapted from Ambassadors program after Burstein et al., Brain 2000
1. Peripheral Trigeminal Sensitization
2. Central Trigeminal Sensitization
2. Forehead Allodynia
3. Thalamic Sensitization
3. Extracephalic Allodynia
1
3
2
Sensitization and migraineSensitization and migraine
1. Throbbing headache
Migraine TriggersMigraine Triggers
hormoneshormones emotions/stressemotions/stress disrupted sleepdisrupted sleep caffeine withdrawalcaffeine withdrawal foodsfoods changechange
THE SENSITIVE BRAINTHE SENSITIVE BRAIN
Pain control mechanisms are partiallydefective in migraine patients
Symptomatic Medication Mild to Moderate HeadachesSymptomatic Medication Mild to Moderate Headaches
NSAID’s - high dose (+/- antiemetic)NSAID’s - high dose (+/- antiemetic) ASA/acetaminophen/caffeine (Excedrin)*ASA/acetaminophen/caffeine (Excedrin)* ASA or acetaminophen/butalbital/caffeine ASA or acetaminophen/butalbital/caffeine
(Fiorinal/Fioricet)*(Fiorinal/Fioricet)* Acetaminophen/isometheptene/dichlrophenazone Acetaminophen/isometheptene/dichlrophenazone
(Midrin) - ii po at onset, then i qhr up to 5/day(Midrin) - ii po at onset, then i qhr up to 5/day Ergotamine tartrate/caffeine (Cafergot)*Ergotamine tartrate/caffeine (Cafergot)*
*** Limit use to 2 days/week ****** Limit use to 2 days/week ***
Triptans and DHETriptans and DHE
Sumatriptan (Imitrex) Sumatriptan (Imitrex) Rizatriptan (Maxalt) Rizatriptan (Maxalt) Zolmitriptan (Zomig) Zolmitriptan (Zomig) Naratriptan (Amerge) Naratriptan (Amerge) Frovatriptan (Frova)Frovatriptan (Frova) Almotriptan (Axert)Almotriptan (Axert) Eletriptan (Relpax)Eletriptan (Relpax) DHE im/sq, iv, nsDHE im/sq, iv, ns
Group byGroup by parenteralparenteral po rapid onsetpo rapid onset po slow onsetpo slow onset
rapid --> slowrapid --> slow high --> low efficacyhigh --> low efficacy high --> low relapsehigh --> low relapse more --> less se’smore --> less se’s
Triptan side effects/risksTriptan side effects/risks
Common: sedation, nausea, muscle ache, Common: sedation, nausea, muscle ache, chest tightness (2 – 5%)chest tightness (2 – 5%)
ContraindicationsContraindications
• CAD, CVA, PVDCAD, CVA, PVD
• hemiplegic/basilar migrainehemiplegic/basilar migraineRisk of serious cardiac event with triptans is Risk of serious cardiac event with triptans is
~ 1:1,000,000~ 1:1,000,000
General approach to acute RxGeneral approach to acute Rx
Who gets triptans?Who gets triptans?Which triptan?Which triptan?How to use the triptan?How to use the triptan?
Principles of acute therapyPrinciples of acute therapy
Stratified care Stratified care Early use of medication for patients with Early use of medication for patients with
episodic headacheepisodic headacheLimit use of all acute meds to 2 days/weekLimit use of all acute meds to 2 days/week
Stratified CareStratified Care
Usual level of disabilityUsual level of disabilityRapidity of onsetRapidity of onsetAssociated nausea/vomitingAssociated nausea/vomitingTendency to relapseTendency to relapseSide effect toleranceSide effect tolerance
An approach for triptan non-responders
An approach for triptan non-responders
Review diagnosisReview diagnosis
• migraine?migraine?
• daily headache (drug rebound)?daily headache (drug rebound)?Use early in attack, at sufficient doseUse early in attack, at sufficient doseTry at least 3 triptansTry at least 3 triptansPolypharmacy (NSAID/antiemetic)Polypharmacy (NSAID/antiemetic)?Mg deficiency?Mg deficiency
Alternatives for Refractory HeadachesAlternatives for Refractory Headaches
Chlorpromazine (Thorazine) 12.5 mg iv;Chlorpromazine (Thorazine) 12.5 mg iv;
mr q 20 min x 3; total 50 mgmr q 20 min x 3; total 50 mgIV Depacon 100mg/kg over 5 minIV Depacon 100mg/kg over 5 minIV DHE (q8h Raskin protocol)IV DHE (q8h Raskin protocol)IV Mg 2 gm/100 ml D5W may be added to IV Mg 2 gm/100 ml D5W may be added to
any other regimen any other regimen
Drug Rebound Headache Drug Rebound Headache
h/o episodic migraineh/o episodic migraine more frequent/dailymore frequent/daily refractory to usual Rxrefractory to usual Rx narcotics for rescuenarcotics for rescue Fiorinal - “preventive”Fiorinal - “preventive” escalating Rx useescalating Rx use trying to survivetrying to survive
““The desire to take medication is, The desire to take medication is, perhaps, the greatest feature which perhaps, the greatest feature which distinguishes man from the other distinguishes man from the other animals.”animals.”
Sir William OslerSir William Osler
What drugs cause drug rebound?What drugs cause drug rebound?
Worst offenders:Worst offenders: NarcoticsNarcotics ErgotamineErgotamine Caffeine-containing Caffeine-containing
compounds:compounds:• ExcedrinExcedrin• Fiorinal/FioricetFiorinal/Fioricet• CafergotCafergot
Lesser offenders:Lesser offenders: aspirin acetaminophen NSAID’s triptans
Innocent until proven guilty
DHE
“The Unrecognized Epidemic”“The Unrecognized Epidemic”
• 1-2% of population is affected1-2% of population is affected
• (near) daily tension-type headache, with (near) daily tension-type headache, with migrainous flaresmigrainous flares
• present upon awakeningpresent upon awakening
• refractory to other abortive or prophylactic refractory to other abortive or prophylactic measuresmeasures
• headache worsens when medication is headache worsens when medication is stoppedstopped
Treatment of Drug ReboundTreatment of Drug Rebound
Patient educationPatient education Withdraw medicationWithdraw medication Initiate prophylaxisInitiate prophylaxis Provide rescue therapyProvide rescue therapy
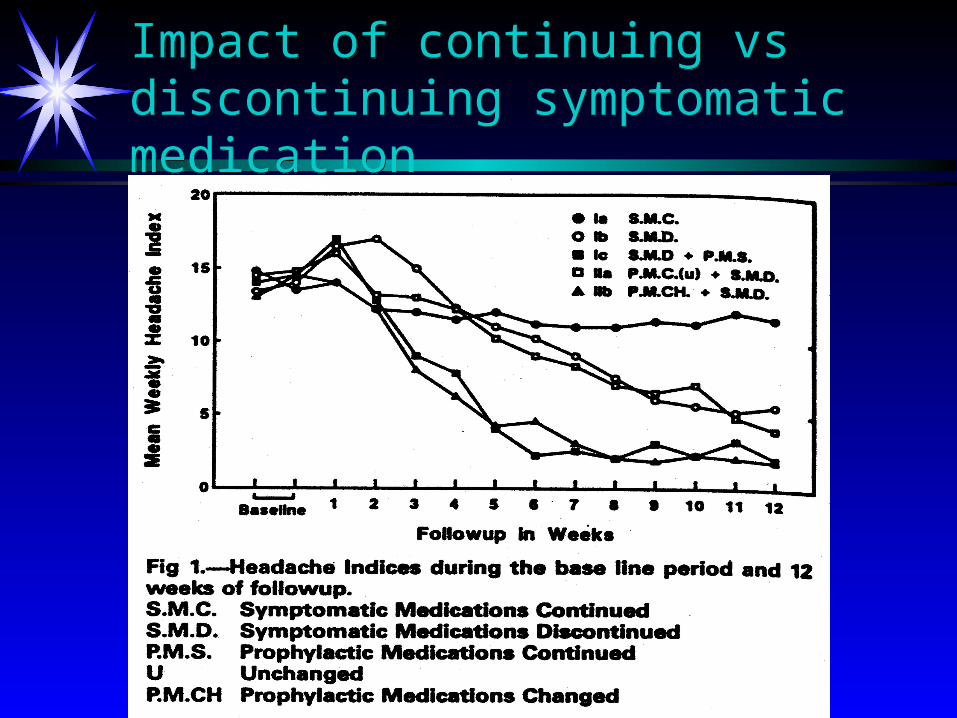
Impact of continuing vs discontinuing symptomatic medicationImpact of continuing vs discontinuing symptomatic medication
Prevention of drug reboundPrevention of drug rebound
All Rx’s state:All Rx’s state:
““Limit use to 2 days/week”Limit use to 2 days/week”
eg, Triptan A, B, or C x mg #9eg, Triptan A, B, or C x mg #9
i po at onset migraine–mr x 2 within 24 hri po at onset migraine–mr x 2 within 24 hr
Limit use to 2 days/weekLimit use to 2 days/week
All Rx’s state:All Rx’s state:
““Limit use to 2 days/week”Limit use to 2 days/week”
eg, Triptan A, B, or C x mg #9eg, Triptan A, B, or C x mg #9
i po at onset migraine–mr x 2 within 24 hri po at onset migraine–mr x 2 within 24 hr
Limit use to 2 days/weekLimit use to 2 days/week
ConclusionConclusion
Episodic disabling = migraineEpisodic disabling = migraine ““Migraine-in-a-Minute” for triageMigraine-in-a-Minute” for triage Stratify careStratify care
• treat earlytreat early• migraine-specific therapymigraine-specific therapy
Refractory headache is usually due to:Refractory headache is usually due to:• drug rebounddrug rebound• co-morbidityco-morbidity
Incorporate behavioral assessment/RxIncorporate behavioral assessment/Rx