Embed Size (px)
Citation preview
310medicofriendcircle bulletin
April - May 2005
CHW: Survivals and Revivals-Shyam Ashtekar1
CHW Debacle in India
The CHW scheme, an important 1978 option forreaching primary care/first contact care to villages ofIndia was a dying scheme by mid-eighties; and now itis no more in 2002. The vacuum has been filled partiallyby somewhat similar variants from governments, butin the main by private doctors of various kinds indifferent states of India. As the already belated optionof CHW failed to answer an important social need,markets have provided some options; for which theState and its policy makers and bureaucrats have toshare the blame. Recent evidence suggests that thereis very little that is learnt from this nationwide failure.
To set the record straight, Government must publishthe formal post-mortem report of the CHW scheme,and if anything what was done to salvage the schemethrough two decades. It concerned five lakh CHWsand their villages. In absence of such an officialstatement on the issue, I am sharing my thoughts andconcerns.
First of all, the Indian health system planned underthe Bhore Committee Report had little to offer on villagelevel services, based as it was on a doctor-hospitalcentric state model of health care. The CHW appendixdid not stick to the system. In contrast China’s effortwas much better, but our policy community is unwillingto admit this fact. It is noteworthy that Mahatma
1Email: < [email protected]> Contact: Dr ShyamAshtekar, Bharat Vaidyaka Sanstha, Contact: Sriramwadi, MGRoad, Nasik, 422 001, Telefax 0253-580147
Gandhi had started preparations forvillage level healers (see Home and Village Doctor byDr. Dasgupta) but the initiative was lost in oblivionafter Independence.
Even though it was a belated effort to make amends,especially after the Alma Ata mandate, the schemelacked steam in several departments: conceptualization,technical design, content, training, politicalmanagement, finance, monitoring, linkages, etc.Subsequent handing over to Family WelfareDepartment put the last nail on the coffin. The Janataregime lasted only 30 months and the later CongressGovernment was not impressed with the scheme.Medicines were withdrawn in eighties and then peopleforgot the CHW. Honoraria continued as litigationsdragged and finally that too stopped.
There was not much light at the other end of thetunnel either—the global experience of CHWs. A 1992WHO review (TRS 780) was seized of this and so wereother experts (Frankel, 1992). In a personal conversationin 2000, David Werner, author of the famous WhereThere is No Doctor, also could not find any large-scalecountry CHW programme worth mentioning. China wasa solid exception and others countries who had the Abbreviations: CHW : (Community Health Workers), COPC:Community Oriented Primary Care, JSR: (Jana SwasthyaRakshak-the new CHW programme in Madhya Pradesh) FCC:(First Contact Care), FRU (First referral Unit- the rural 30-100 bedded hospital), PHC: Primary Health Care, PMP: PrivateMedical Practitioner (“Quacks”), PRMP: Private RMP, NHP:National Health Programme.

2 mfc bulletin/April-May 2005CHW scheme offered attenuated versions (Philippinesfor instance). Brazil had introduced a CHW programmeas late as in 1995. Was there then something geneticallywrong with the CHW programme? Was it unfit for anynational system and only good for NGO islands?
A hard look at various states in India shows thatvillage-doctors that nobody made or dreamt of inNirman Bhavan or Lodhi Road have been spreading inevery state of India—east and west, south and north.Although some states like MP and Chattisgarh aretrying CHW variants in the states, at least the MP JSRscheme is headed the same way as the old CHWscheme (our own unpublished study, 2001). This makesit imperative that we take a closer look at the issuesand problems.
Understanding the Jigsaw Puzzle
The social engineering of CHW scheme is a complexmatter and we see very different models in variouscountries and NGO areas. To make the issue moreexplicit, all the three words in the classicalnomenclature ‘Community Health Worker’ are rathervague concepts, especially in practice. Our questionsare summarized in the table below.
2 This is an impression from Janani, an organizationworking in Bihar and adjoining states. Their understanding isthat each village has more than one private medicalpractitioner.
Are CHWs Necessary for Primary Care in India?
In the new century, primary care is surely still necessaryand valid; but is a CHW necessary for primary care?
CHWs (or some of its variant) are surely necessary for
Community? Health? Worker?
Village? ‘Development’? Liberator, change agent?
Panchayat? Health-especially primary health care/prevention? Worker (lackey)?
Government health dept? National health programmes? Guide (only IEC?)?
NGO? Narrow or vertical programmes? Volunteer (little or no pay)?
SHG? Primary medicare? ‘A doctor’ where there is nodoctor?
Only left to individual ? Little of each above?
primary care in villages (also parts of urban areas) inmany states, if not all. However situation varies, as itmay not be necessary like, say in Kerala. Conversely,in Bihar it may be frustrating to reintroduce the CHWas most villages have a home grown local medicalpractitioner.2 Come to states like Maharashtra andMadhya Pradesh, there are large number of privatemedical practitioners in rural areas, but they are clusteredin some rural centers. In one study in Maharashtra(Ashtekar and Mankad, 2001), we found that in 737villages there were 555 doctors of all types, but theywere all practicing in just 16% of the villages. On aroadside village in MP, we found over 30 clinics ofdoctors (in addition to the mini-PHC) and obviouslythey depended upon surrounding villages for theirclientele. In such situations, it is still possible tointroduce CHWs in peripheral villages but they willhave to prove themselves against the ‘doctors’. I amaware that many experts may not like this connectionbut the reality is that even good CHWs find they loseout when an injection-doctor even starts visiting theirvillage. First goes the curative and later go other healthcomponents. In short, a CHW may be theoreticallynecessary in all villages, but in the vicinity of ‘doctors’,the CHW option melts away. This is difficult tounderstand from a planner’s and activist’s end but veryeasy to grasp from the community’s perspective. Thisleaves us with two tasks, an easy one and a difficultone: of choosing villages for CHW programmes and ofimproving the content of the programmes in severalways.
There are some fresh initiatives on CHWs in somestates: MP, Chattisgarh, AP and in Maharashtra. TheNational Health Policy also makes some not very
mfc bulletin/April-May 2005 3
Expanding the Search for Primary Care ‘Model’
Since the main objective is and must be primary careand CHW only a means to it, I have included villagedoctors as a pragmatic and existing option, and I amnot alone on this since there are experts like Jon Rohdewho wrote a book on rural doctors (Rohde andViswanathan, 1995). On this wider canvass of primarycare by CHW schemes, NGO experiments and privatevillage doctors, the complexities deepen. Theapproaches, inputs, processes, and outputs changeaccording to the vehicle of primary care. My argumentis that even if a classical State CHW model is not feasiblein some states/districts, it is still feasible to make use
3I had a brief interview with Dr Gerald Bloom, anexpert of the Bristol University, who has an intimateunderstanding of the China health scenario. As I was describingthe ubiquitous PMP-quacks in India, he shrugged and saidthat it sounds much like China’s rural doctors in the villagehealth stations, many of whom have little training and arerarely monitored. I was taken aback by the comparison, canproducts of two entirely different systems be alike?
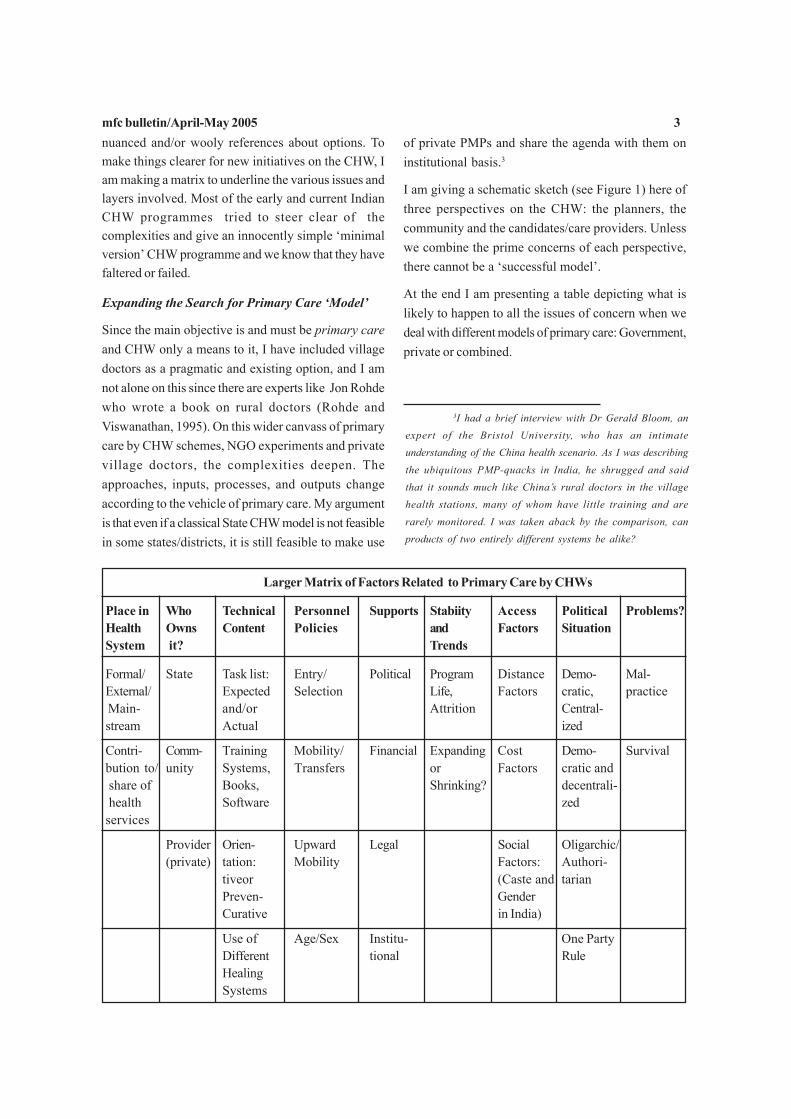
nuanced and/or wooly references about options. Tomake things clearer for new initiatives on the CHW, Iam making a matrix to underline the various issues andlayers involved. Most of the early and current IndianCHW programmes tried to steer clear of thecomplexities and give an innocently simple ‘minimalversion’ CHW programme and we know that they havefaltered or failed.
Larger Matrix of Factors Related to Primary Care by CHWs
Place in Who Technical Personnel Supports Stabiity Access Political Problems?Health Owns Content Policies and Factors SituationSystem it? Trends
Formal/ State Task list: Entry/ Political Program Distance Demo- Mal-External/ Expected Selection Life, Factors cratic, practice Main- and/or Attrition Central-stream Actual ized
Contri- Comm- Training Mobility/ Financial Expanding Cost Demo- Survivalbution to/ unity Systems, Transfers or Factors cratic and share of Books, Shrinking? decentrali- health Software zedservices
Provider Orien- Upward Legal Social Oligarchic/(private) tation: Mobility Factors: Authori-
tiveor (Caste and tarianPreven- GenderCurative in India)
Use of Age/Sex Institu- One PartyDifferent tional RuleHealingSystems
of private PMPs and share the agenda with them oninstitutional basis.3
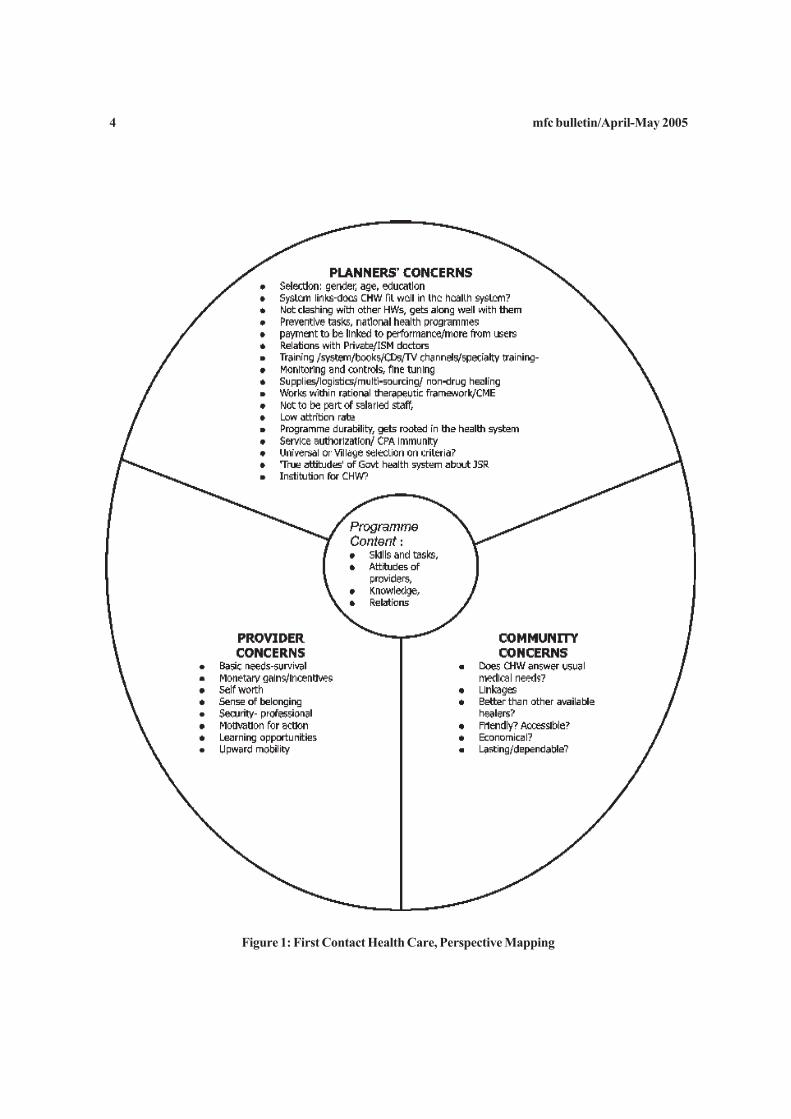
I am giving a schematic sketch (see Figure 1) here ofthree perspectives on the CHW: the planners, thecommunity and the candidates/care providers. Unlesswe combine the prime concerns of each perspective,there cannot be a ‘successful model’.
At the end I am presenting a table depicting what islikely to happen to all the issues of concern when wedeal with different models of primary care: Government,private or combined.
4 mfc bulletin/April-May 2005
Figure 1: First Contact Health Care, Perspective Mapping
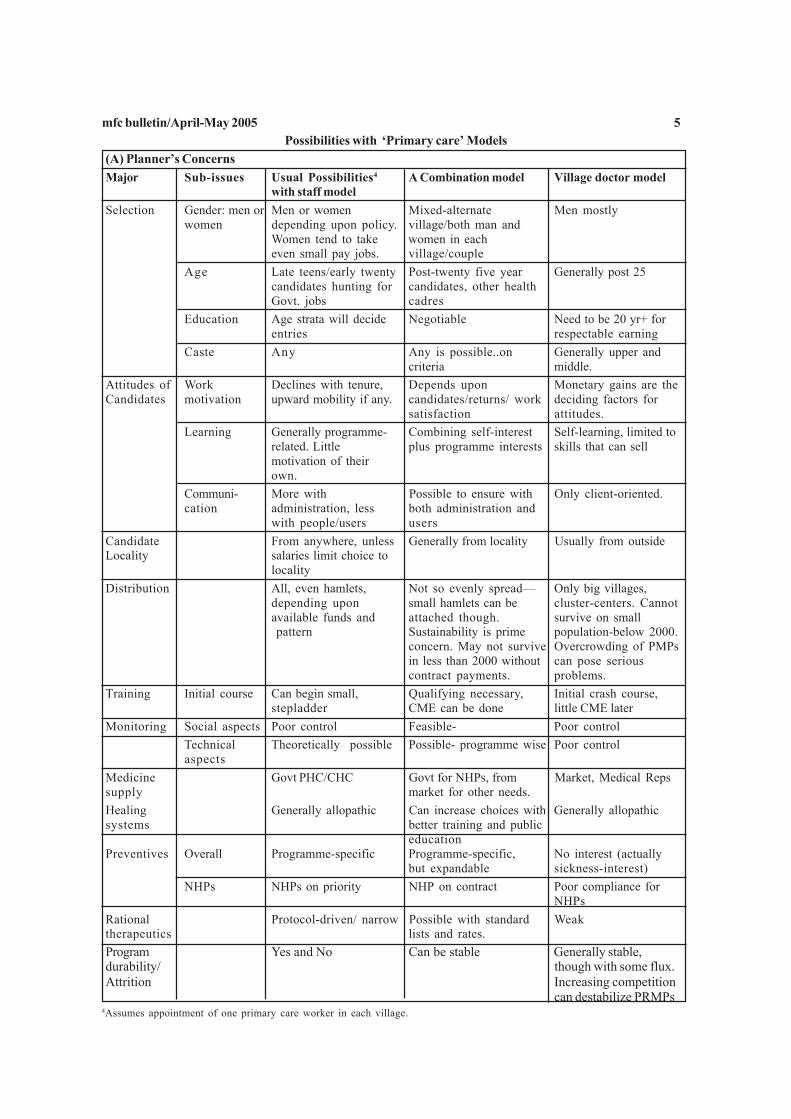
mfc bulletin/April-May 2005 5Possibilities with ‘Primary care’ Models
(A) Planner’s ConcernsMajor Sub-issues Usual Possibilities4 A Combination model Village doctor model
with staff modelSelection Gender: men or Men or women Mixed-alternate Men mostly
women depending upon policy. village/both man andWomen tend to take women in eacheven small pay jobs. village/couple
Age Late teens/early twenty Post-twenty five year Generally post 25candidates hunting for candidates, other healthGovt. jobs cadres
Education Age strata will decide Negotiable Need to be 20 yr+ forentries respectable earning
Caste Any Any is possible..on Generally upper andcriteria middle.
Attitudes of Work Declines with tenure, Depends upon Monetary gains are theCandidates motivation upward mobility if any. candidates/returns/ work deciding factors for
satisfaction attitudes.Learning Generally programme- Combining self-interest Self-learning, limited to
related. Little plus programme interests skills that can sellmotivation of theirown.
Communi- More with Possible to ensure with Only client-oriented.cation administration, less both administration and
with people/users usersCandidate From anywhere, unless Generally from locality Usually from outsideLocality salaries limit choice to
localityDistribution All, even hamlets, Not so evenly spread— Only big villages,
depending upon small hamlets can be cluster-centers. Cannotavailable funds and attached though. survive on small pattern Sustainability is prime population-below 2000.
concern. May not survive Overcrowding of PMPsin less than 2000 without can pose seriouscontract payments. problems.
Training Initial course Can begin small, Qualifying necessary, Initial crash course,stepladder CME can be done little CME later
Monitoring Social aspects Poor control Feasible- Poor controlTechnical Theoretically possible Possible- programme wise Poor controlaspects
Medicine Govt PHC/CHC Govt for NHPs, from Market, Medical Repssupply market for other needs.Healing Generally allopathic Can increase choices with Generally allopathicsystems better training and public
educationPreventives Overall Programme-specific Programme-specific, No interest (actually
but expandable sickness-interest)NHPs NHPs on priority NHP on contract Poor compliance for
NHPsRational Protocol-driven/ narrow Possible with standard Weaktherapeutics lists and rates.Program Yes and No Can be stable Generally stable,durability/ though with some flux.Attrition Increasing competition
can destabilize PRMPs4Assumes appointment of one primary care worker in each village.
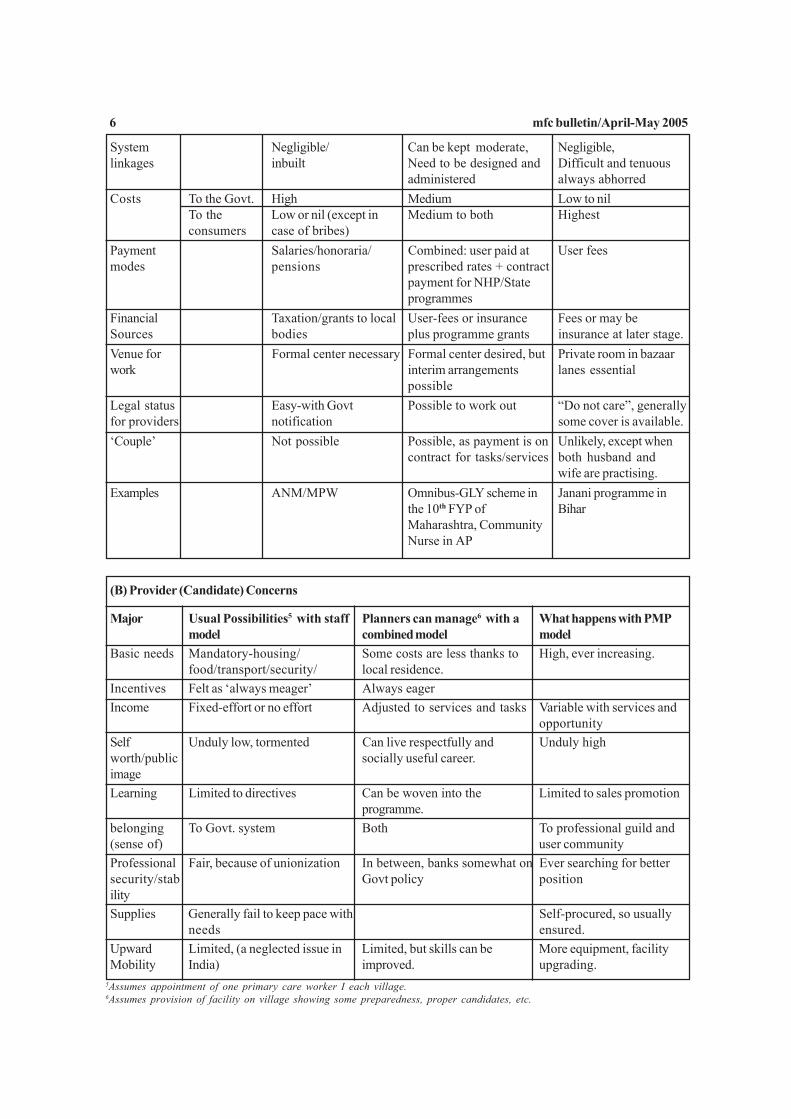
6 mfc bulletin/April-May 2005
System Negligible/ Can be kept moderate, Negligible,linkages inbuilt Need to be designed and Difficult and tenuous
administered always abhorredCosts To the Govt. High Medium Low to nil
To the Low or nil (except in Medium to both Highestconsumers case of bribes)
Payment Salaries/honoraria/ Combined: user paid at User feesmodes pensions prescribed rates + contract
payment for NHP/Stateprogrammes
Financial Taxation/grants to local User-fees or insurance Fees or may beSources bodies plus programme grants insurance at later stage.Venue for Formal center necessary Formal center desired, but Private room in bazaarwork interim arrangements lanes essential
possibleLegal status Easy-with Govt Possible to work out “Do not care”, generallyfor providers notification some cover is available.‘Couple’ Not possible Possible, as payment is on Unlikely, except when
contract for tasks/services both husband andwife are practising.
Examples ANM/MPW Omnibus-GLY scheme in Janani programme inthe 10th FYP of BiharMaharashtra, CommunityNurse in AP
(B) Provider (Candidate) Concerns
Major Usual Possibilities5 with staff Planners can manage6 with a What happens with PMPmodel combined model model
Basic needs Mandatory-housing/ Some costs are less thanks to High, ever increasing.food/transport/security/ local residence.
Incentives Felt as ‘always meager’ Always eagerIncome Fixed-effort or no effort Adjusted to services and tasks Variable with services and
opportunitySelf Unduly low, tormented Can live respectfully and Unduly highworth/public socially useful career.imageLearning Limited to directives Can be woven into the Limited to sales promotion
programme.belonging To Govt. system Both To professional guild and(sense of) user communityProfessional Fair, because of unionization In between, banks somewhat on Ever searching for bettersecurity/stab Govt policy positionilitySupplies Generally fail to keep pace with Self-procured, so usually
needs ensured.Upward Limited, (a neglected issue in Limited, but skills can be More equipment, facilityMobility India) improved. upgrading.
5Assumes appointment of one primary care worker I each village.6Assumes provision of facility on village showing some preparedness, proper candidates, etc.

mfc bulletin/April-May 2005 7
Omnibus S cheme on Gramin Lokswasthya Yojna(GLY) in 10th FYP in MaharashtraEven as the CHW scheme vanishes in thin air and padahealth workers scheme is equally evanescent, theprimary care group of Maharashtra was arguing for acomprehensive and realistic alternative scheme forneedy villages. Thanks to various circumstances andforces, five years of efforts resulted in inclusion ofGLY in the 10th FYP of Maharashtra. I call it ‘omnibus’for various strategic and conceptual reasons. Thescheme will be tried on a pilot basis in 1000 villagesfirst, with help of NGOs to start with. Later it will beexpanded. We are trying to mainstream it with help ofthe Open University, legal status under MMC,panchayats & SHGs.
7Assumes appointment of one primary care worker in eachvillage.8Assumes provision of facility on village showing some pre-paredness, proper candidates, etc.
References
1. Dasgupta. Home Village Doctor. Khadi Pratisthan,Calcutta, 1942.
2. WHO: Strengthening the Performance ofCommunity Health Workers in Primary HealthCare. TRS 780, Geneva, 1989.
3. Frankel, Stephen. Overview, The CommunityHealth Worker. OUP, 1992, pp 1- 62.
4. PHA Calcutta. “Document Resolutions”, p3. PHASecretariat, Bangalore, Dec 2000.
5. Ashtekar, Shyam and Dhruv Mankad. “WhoCares? Rural Health Practitioners in India”.Economic and Political Weekly, Feb 3-9, 2001.
6. Rohde, Jon and Hema Viswanathan. The RuralPrivate Practitioner. OUP, Delhi 1995, pp 37-57.
(C) Community Concerns
Major Usual Possibilities7 with staff Planners can manage8 with a What happens with PMPmodel combined model model
Healing: Only limited, may not satisfy, Good healing + satisfaction Satisfying it must be (but(Medical may or may not heal. mandatory for survival may or may not heal)needs)Access Time bound, programme- Ensuring good access is Time: elastic, but often
linked, not dependable precondition distant. So access is limitedEconomical? May be free, if not doing Can save access costs and High costs, and also hidden
private practice needless medication costsFriendly? Depends upon the person Professional requirement. Professional requirement.Lasting? transfers, and visiting nature Can be Generally
makes it look less like lastingdependable Not really-because of various Generally dependable and
factors accountableUser control Poor, works through long Can be fairly controlled. Poor control on quality of
politico-administrative links. care
Available Revised Edition
Impoverishing the Poor:Pharmaceuticals and Drug Pricing in India
Publishers: LOCOST, Vadodara and JSS Bilaspur, Dec 2004Pages 180, Price Rs 100/-
For copies, write to <[email protected]> or <[email protected]>

8 mfc bulletin/April-May 2005
National Rural Health Mission1 :
1. The Common Minimum Programme adopted by the UPAgovernment was a conscious effort to respond to the mandategiven by the electorate in the recent elections that broughtthe UPA to power. The National (Rural) Health Mission, asa response to this mandate is welcomed by the Jan SwasthyaAbhiyan.2. There was an initial apprehension that the National HealthMission would be reduced to a targeted contraceptiveprogramme that is neither desirable nor effective. Recentassurances that this would not be so were accepted by thenational health action networks and this has led to our engagingin this process of responding to the Health Mission agenda.3. On the 18th of December 2004, the National CoordinationCommittee of the Jan Swasthya Abhiyan met and formulatedits response to the proposed Mission agenda and actionplan. Dr Antia who had been following up the developmentswith the Prime Minister’s office, with the Health Ministryand the Planning Commission, briefed the members ofcoordination committee on the developments in the formationof the mission and the initiatives he had taken to shape theagenda of the Mission.4. After discussions the National Coordination Committeeof Jan Swasthya Abhiyan decided to put forth a broadconsensus on basic concerns regarding the Mission and itssuggestions for strengthening the Mission for strengtheningprimary health care.5. The broad consensus that has emerged is articulatedbelow as five guiding principles that are essential to implementthe mandate of the Common Minimum Programme:5.1 The Mission should be based on a sustained increasedbudgetary allocation to health care and not be based on donorfunds or ad hoc reallocation of funds from the very limitedexisting scanty resources available in the health sector. Theneed for an immediate and substantially increased budgetaryallocation to health, at least doubling of this by the year2009, has a very broad based consensus and is one of thecornerstones of the CMP section on health; the Missionshould be seen to be responding to this consensus.5.2 The Mission should call for and coordinate with increasedinvestments and better design and implementation in a numberof sectors related to health – especially food security, waterand sanitation, elementary education, shelter, urbandevelopment, environmental safety, poverty alleviationprogrammes and livelihood issues. The universalisation ofthe ICDS programme must be part of the same mission ormust proceed in parallel and close synergy with this effort.5.3 The Mission should ensure that investments in healthnot only increase universal access but also address issues ofgender and socio-economic inequities in health status andhealth care services. Health and access to quality health care
Comments by the National Coordination Committee of Jan Swasthya Abhiyanservices are basic inalienable human rights and should not bedependent on the ability of the citizen to pay for health care.For example, basing the proposed Community Health Workerprogramme on the charging of user fees would run completelycounter to this perspective.5.4 The Mission should be a programme to strengthencomprehensive Primary Health Care within which RCH mustbe positioned as one of the components. The rural healthcare mission should not become yet another vertical“fragmented” program. While recognising the need torationalise the use of resources, improve access and qualityof services in the public health system, the Mission needs toensure that the planned interventions strengthen public healthsystems and build upon the basic framework of the facilitiesbuilt up over the decades.5.5 The Mission would have to have strong links with thePanchayati Raj System and move towards devolution ofgreater funds and responsibilities in health care to thePanchayati raj system.
In terms of strengthening public health systems the Missionhas proposals in four areas to which we submit the followingresponse:a. Community Health Worker Programmeb. The Subcenter and the ANMc. The Primary Health Center and Community Health
Centerd. Role of the Private Sector
a) Community Health Worker ProgrammeThe move for a nationwide community health workerprogramme is a most welcome development. We refer here tothe proposed ASHA, which we refer to by the generic termcommunity health worker (CHW). However the lessons ofthe past programmes, the evidence from detailed evaluationreports and our shared theoretical understandings of thepotentialities of the community heath worker programmelead us to draw your attention to some major concerns andsuggestions:
1. Not a substitute but a supplement to ANM: The CHW ispart of an approach to strengthening the public health system:The CHW should not be seen as a substitute to the ANMand the subcenter, but as a supplement to these. These twodifferent functionaries are both needed and have distinctfunctions. The introduction of the CHW must therefore beaccompanied by parallel measures to strengthen the sub-center. Any move to replace an adequately paid,systematically trained and supported cadre by a much lesspaid and less trained and supported CHW would be a bigstep backward and would rightly be seen as using the CHWas an excuse to dismantle the health system. The CHW/ASHA programme must become an idiom of strengtheningpublic health systems – not an element of weakening it.
2. CHW’s important role in securing – health services as
1The official power point presentation on the Rural HealthMission is available at < http://mohfw.nic.in/nrhm.html>.

mfc bulletin/April-May 2005 9basic rights: One essential corrective is to strongly introduceaccountability of the health system and securing of healthrights of the people into the work definition of the CHW.This requires strong community support and mobilisation.It also requires that though the CHW works with the ANMand anganwadi-worker – she does not work under them.
3. No to user fees for prescriptions and services – rejectionof the RMP model: The CHW’s remuneration should NOTbe based on her charging fees for prescription as a privatepractitioner prescribing drugs in the open market- similar towhat was attempted under the Jan Swasthya Rakshakprogramme. Glorifying this as a social entrepreneur shouldnot blind us to the evidence accumulating that in programmeslike the earlier Jan Swasthya Rakshak programme, the rise ofsuch a cadre of ill qualified private practitioners raises thecost of medical care to the poor without any correspondingincrease in health benefits.
The evaluation report of the JSR scheme in Madhya Pradeshpoints out that 90% of the JSRs had dropped out within ayear of being trained! Most of those who were functionalwere not practicing rational medical care and were indulgingin irrational, exploitative “injection practice”. The criticismwe raise of not accrediting or building a health care systemaround the illegal and unqualified rural practitioners is basedon an objective recognition of what such care means in medicaland social terms. Studies that have commented positively ontheir service have typically failed to include the rationalityof care within their scope of the study. Hence they havefailed to recognise that most care given by the RMP andsimilar informal practitioners of modern medicine is wastefuland redundant care for trivial self-limiting illness, orinappropriate and often hazardous care for serious illness.The vulnerability of Jan Swasthya Rakshaks and similar healthcare providers to unethical influence from pharmaceuticalcompanies is also underestimated. We strongly feel that ifthe Rural Health Mission leads to addition of lakhs of illtrained RMPs to the existing menace of RMPs, the wholepurpose of ensuring Primary Health Care to the rural poorwould be lost. We note that with the spread of such “RMPs”health care expenditure has now emerged as an importantcontributor to rural indebtedness. Most of such expenditureis totally unnecessary and senseless, this wastage should becondemned rather than encouraged. Irrationally practicingRMPs are an index of the failure of the system, a part of theproblem and not a part of its solution. Introduction of anRMP-like CHW scheme is our single greatest area ofdisagreement with the Mission draft as it is currentlyarticulated.4. Selection of women candidates by the community andwhat it implies – To enhance the process of empowermentof women, this skilled work should be entrusted only towomen. The process of CHW selection should be carried outby the community, through a process that ensures that thischoice is made after the community has been well informedof the programme and after due care is taken that the voicesof weaker sections have been facilitated and have been givenspace during the selection process. This requires that thedecision is always made in the general body of the habitation,
but is also facilitated by trained, sensitised facilitators througha monitored process and that the elected panchayat formallyratifies the selection.5. Hamlet as unit or village as the unit? There is a strong casefor insisting that the habitation and not the hamlet should bethe unit of selection. The one per 1000 population wouldmean that the main hamlet – largely of upper caste would getadequately covered and the smaller outlying hamlets usuallywhere the needs are greater and the population moremarginalised would again get left out. This has been theexperience of the entire anganwadi programme and even ofearlier CHW programmes. Geographical distances makevillage as the unit untenable in places like Chhattisgarh,Jharkhand and Rajasthan while caste tension make it nonfunctional in places like Bihar and Uttar Pradesh. Situatingthe CHW in each habitation instead of each village cuts acrossthese problems. This of course increases the number of CHWsproposed substantially, and it increases costs proportionately– but it would dramatically increase outreach and diffusionof messages and services.6. Qualifications and certification: How essential/feasible arethey? Educational qualifications should be a desirablequalification and not a mandatory rule. Otherwise the pooresthabitations will find no suitable candidate or would have toagree to candidates from a different socio-economic class.Similarly certifying them all through one syllabus fixedcentrally is neither feasible nor desirable. Local processesshould be built around a core syllabus, both in terms ofcontent and method of training. Assessment should be madeat the local levels (with the block as the unit) to ascertainwhether they have reached the desired knowledge and skilllevels, based on a standardized regional curriculum.Certification would be for functioning as CHW in theirhabitation and within the programme guidelines only.7. Build on – do not replace – existing CHW programmes:Existing CHW programmes run by NGOs or run by stategovernments would continue- with necessary strengthening– rather than be replaced by the Mission initiated CHWprogramme.8. Training and support should be a continuous effort andnot one time – the programme should therefore be built andbudgeted to continue for at least a five year period. Thetraining programme should be in short spurts of three to fivedays at a time once in two to three months till the necessarycompetence is built up. This may take as long as 18 monthsto build up. Following the foundation training, continuinginputs such as follow up training, skill upgradation, revisionclasses and annual assessment should continue for a periodof at least five years from the initiation of the programme.9. Curative Care is essential though not central. Curativecare would be an essential part of the training programmeand CHW function- but it would be supplementary and notcentral to the definition of the CHW and her functioning.10.Financial Compensation to the CHW: The compensationfor the services carried out by the community health workermay take the form of enhanced incentives paid for loss oflivelihood on the days of training (about Rs 100 per day of

10 mfc bulletin/April-May 2005training). With 30 days of training in the first year, 15 daysof meetings and training in subsequent years, the trainingcompensation would amount to Rs 3000 in the first year andRs 1500 per year in subsequent four years. To this may beadded from the second year onwards a performance-linkedhonorarium / incentive, which should be commensurate withthe average number of hours spent by the CHW per day invarious types of health related work, and may be calculatedat least at the level of the rate of minimum wages for skilledwork. This performance-linked honorarium would be paidby the Gram Panchayat, based on an annual grant receivedby it from the Government. Payment of this performancelinked honorarium could be based on two types of annualassessment:
a) The general body of the habitation (equivalent to GramSabha), assisted by the hamlet health committee, wouldannually assess the social performance of the CHW on thebasis of certain specific parameters (actions taken by CHWto help the community to assert their health rights; monitoringof village level health services expected to be delivered byANM / MPW; whether nutritional advice is given to mothers;monitoring and support to the Anganwadi by CHW on behalfof the community; assistance given by the CHW to patientsby enabling them to obtain care at the PHC, etc.)b) The ANM / MPW, assisted by Hamlet health committee,would annually assess the technical performance of the CHWin terms of knowledge of a sample group of mothers aboutbasic nutritional practices; number of patients who havereceived appropriate First Contact Care; attendance of eligiblechildren/pregnant women during village immunisationsessions; attendance by pregnant women during villageantenatal checkup sessions; number of suspected seriouscases referred to the PHC by the CHW etc.11. Process sensitive selection of programme leadership:There is a need for full time staff recruited from motivatedNGOs, for monitoring and training support at the level of acluster of villages, at the block , district and state level. Insome of these levels, in some of the districts we would findNGOs to whom this role can be contracted out. In manydistricts and blocks these full time programme leaders wouldhave to emerge from a process of social mobilisation thatprecedes and continues through the programme. We notethat very often the issue is raised that “we cannot get anArole or an Antia at each block to provide the sort of motivatedleadership Jamkhed had”. Unfortunately such an assertionbecomes grounds for therefore dumping all the basic processelements of the CHW programme in favour of some welltested and failed short cut approaches like the user fee. Thetrue answer to this assertion is a question “ yes – there is anArole or an Antia in every district, indeed there are many-but what processes should we follow so that they wouldemerge?” We reply to this question saying that there aremany possible answers in each district. But to find them oneneeds to ensure that in project implementation there is a civilsociety partnership provided at the state and national level,which can physically visit the various districts and catalysethe emergence of project teams in a flexible and principledmanner. This is one of the key lessons of the Mitanin
programme that are worth emulating.12. We note that Mitanin programme has been oneprogramme that has scaled up CHW interventions to thestate level and the problems and design changes that scalingup create should be studied here and used for designing thenational programme.13. State specific names for CHWs: Finally, though we arenot making an issue of it, we suggest that instead of ASHAwe allow each state to choose its own name- like Mitanin,Sakhi, Swasthya Karmi etc., and in official papers use CHWor CHV as the generic name. This is not only on theoreticalgrounds (should she be accredited, what does social healthmean and should we not use activist if in practice she is goingto focus on ) but also keeping in mind what would be attractivein the popular idiom and what term would create betterownership amongst the states.
b) Strengthening of the Subcenter
1. Jan Swasthya Abhiyan notes that one of the mosteffective components of the existing public health system isthe subcenter and within this the Multipurpose Worker –Female, otherwise referred to as the ANM. We also note thateven this component needs far more investment and designimprovements to reach minimum desired levels ofeffectiveness.2. The single most important suggestion we put forth is tohave two ANMs per subcenter. The budgetary burden ofthis would work out to a sum of Rs 80 crores per year, whichis extremely affordable (note, for purposes of comparison,that the Govt. was committed to raising 1800 crores for sixAIIMS). A second ANM is every subcenter halves the workburden of the ANM- and would be a welcome step. In tribalareas it would become one per 1500 population or even less-almost the norms proposed for the CHW. The capacity togenerate so many ANMs is relatively easier to build up.Also by halving her work burden one finds the space tomake her work more comprehensive and therefore moreresponsive to the community’s felt needs. Further if thereare two ANMs per subcenter the subcenter can be keptopen during all days allowing it to undertake functions likeinstitutional delivery.3. The location of subcenter buildings may be rationalisedso that optimum coverage is attained. Since most buildingsare not built it is an opportunity for the Mission to completethe gap in this infrastructure through a one time all out effortand simultaneously improve the efficiency of these servicesby better location. The estimated budgetary support forinfrastructure gaps at the subcenter level is in the range of Rs5000 crores. Spread out over five years at Rs1000 crores peryear this goal of an adequate subcenter as per norms alongwith accommodation for the ANM can be attained.4. Expanding the ANM drug kit to 25 drugs and a betterlevel of training on curative skills and home and herbalremedies based on standard treatment guidelines evolved forparamedicals would also enable the ANM to respond muchbetter to felt health care needs and therefore give her muchmore credibility and respect in the local community. We notethat it is incongruous to express so much interest in training

mfc bulletin/April-May 2005 11RMPs and a new cadre of CHWs without ensuring that thecurrent functionary most available in the periphery is notyet trained on such curative care. Nor is this perceived asincreased work burden. Indeed there is a request from ANMsto receive such training as it gains her better local acceptance.(At 10 patients per day per subcentre, 250 patients per month,Rs. 5/- average drug cost per patient, the medicine cost worksout to about Rs. 15,000 per year per subcenter.)5. The male worker may continued as a state governmentfunded cadre but retrained to provide all the support servicesneeded as a paramedical- the functions of dresser,compounder, basic laboratory technician, communicabledisease control interventions with the community as well asto provide support to the ANMs.6. The subcenter needs to be strengthened withcommunication facilities, road access and transport accessso that it can be a site from which referral transport can becalled for and referral to higher levels undertaken where needed.7. The subcenter and the ANMs need the CHW programmefor effectively reaching the core health system goals. One isnot a replacement of the other. The CHW as a semi-honoraryworker should not be burdened with routine service deliverytasks of the ANM, and it may be kept in mind that she does nothave infrastructure and much equipment with her. Her roleis more in increasing awareness, mobilisation andorganisation of women and the community for health, andfacilitating village level service delivery including provisionof First Contact Care. The subcenter is on the other handaims to provide all the services that paramedicals can betrained to provide. And therefore its functionaries are thereforegiven a full day’s wage. (We note that the Ministry’spresentation on the inadequacy of the subcenter had locatedthe problem exclusively at its being made to follow apopulation norm instead of a village or geographical norm.This is at best a very simplistic reduction and whimsicalunderstanding of the subcenter’s limitations and perhapsaccounts for the lack of sufficient discussion of the means ofimproving subcenters.)8. Problems of accountability and decentralisation are bestmet by making the ANMs and MPWs a block level cadrerecruited and paid by the block and village panchayats towhom the entire funds of the subcenters are devolved.(Existing ANMs are deputed to the block level cadre.)
c) Primary Health Center and Community Health Center1) There has been a mistaken trend to recommend doingaway with or diluting the Primary Health Center. This is notexplicit but the situational analysis is indicative. Moreworrying there seems to be a large informal consensus buildingup against this facility amongst some “experts” which sinceit is not placed before formal public scrutiny is not beingrefuted. Even if these suggestions are well meaning – they arenevertheless seriously mistaken.2) The case for the primary health center rests on two criteria– one epidemiological and one social. The epidemiologicalstatement is that the burden of diseases in a population of30,000 is such that it requires medical attention and cannotbe managed by the CHW or subcenter alone. This may
include short periods of inpatient care, e.g., care in cases ofdiarrhea with dehydration, institutional delivery, epilepticattack, first aid/first contact curative care prior to transfer,for example in snake bite or poisoning. However inpatientcare is peripheral to its function. The sociologicalconsideration is that there is a general correlation betweenthe distance people travel to seek treatment and the nature ofillness that they have. Patients could not bear the expenseand time loss of seeking health care at too much distance inmost circumstances –unless there is a serious prolonged illnesswhich gives them enough time and compulsion to raise thefunds and make the journey. Nearer the facility, the earlierthe patient would seek care and therefore the greater thereduction in mortality and long-term sequelae.3) The very poor utilisation and therefore cost-effectivenessof the PHC at present is mainly due to its very poorfunctionality. At such poor levels of utilisation of all threefacilities, only a subcenter and a CHC approach may appearto suffice - but that is conceding to very poor levels of careprovision which would be sub-critical for major reductionsin mortality and morbidity. The poor functionality of thePHC owes to three design weaknesses of the PHC:a. A very selective package of care provided by the PHCwhich is completely mismatched with people’s felt and urgenthealth care needs- thereby destroying the credibility of thePHC as a health services provider and also seriouslyunderutlising the doctor and support staff.b. Building up all care around the presence of a doctor – allthe other six to eight staff seen as adjuvant to the doctor.This in a context where the medical doctor is often notavailable at any time of the day and almost universally notavailable on a 24-hour basis. Thus on one hand we almostinvariably have number of underutilized staff available inparallel with vacant staff positions—and all of them renderedwasted when the doctor is absent.c. A failure to differentiate the nature of in-patient careprovided in the PHC, from that at the secondary care level(leading to the curious statement in the Mission introductionthat the problem with the PHC is the failure to differentiateoutpatient work from in-patient work.4) To strengthen the PHC, there are five key suggestions:
a. Firstly to ensure that all sectors (a health administrativearea corresponding to a PHC) have a PHC. Currently aboutone third of sectors in the weaker states do not have one.b. Secondly to close various infrastructure gaps in the PHC.c. Thirdly to build the services on a 24 hour basis aroundtrained multiskilled paramedicals operating in shifts providingpreventive, promotive services plus a wide variety of basiccurative services built around a paramedical’s standardtreatment guidelines. (This includes basic curative work,institutional delivery, first aid for injuries, immediatetreatment before referral for more serious illness, managementof diarrhoeal epidemics, etc.d. Fourthly, especially in difficult and medically underservedareas, it has been seen that non-availability of the doctorreduces the functionality of the PHC, which may be the only

12 mfc bulletin/April-May 2005facility capable of giving the services of a qualified doctorand short indoor care in the remote locality. Keeping this inmind, assurance of proper living and transport facilities,backup electricity arrangements, a possible schooling / familyallowance (to support the schooling of children in a nearbytown) and time-bound short postings (ceiling of two years)for doctors working in remote, ‘difficult’ PHCs may beconsidered, as measures to help ensure the attendance ofdoctors.e. Placing the sector PHCs, including all the paramedicalstaff under the district and block panchayats as a districtcadre with recruitment and services linked to the districtsituations, may be considered. The funds for this may begiven to the district panchayats and block panchayats. Wherethe area is medically underserved the panchayats can besomewhat flexible with pay packets and perks as well aswith other options, while observing certain basic norms.5) The role of the CHC has been recognised in all theMission’s background documents. The objective of reachingabout 7000 well-equipped secondary care centers-approximately at one per 100,000 population, is excellent.But the situational analysis does not seem to recognise allthe reasons why this has not happened so far- despite thisneed being well recognised over the last thirty years at least.Other than the well-recognised constraints of funds andequipment the other major constraints relate to governanceissues linked to workforce management policies as well asthe approach to getting the necessary specialist skills in place.These latter constraints are not impossible to overcome, butthey require both political will and astute administrativeaction.6) The danger lies in the readiness to accept the accreditingof private sector as the main -even sometimes as onlyalternative- to break the deadlock in the creation of secondarycare centers in the public health system. The Jan SwasthyaAbhiyan cautions that given the problems of governanceand the completely unregulated environment in which thecommercial private sector works, the hasty switch to public-private partnerships as the main means of closing this gapin secondary centers is bound to be disastrous. Not only willthe private sector fail to fill this gap. In the process thethrust to build up the secondary centers network in the publichealth system linked to the primary care network would beseriously undermined. For considerations of costeffectiveness, governance issues and of feasibility of providingan adequate dispersal of these centers, the bulk of secondarycare provision would have to remain as public provided andpublic funded facilities.7) The Mission’s suggestions for strengthening urban healthcare, referral transport services etc are all welcome. Wehowever need to make the same cautions that we made forprivate provisioning of secondary health care regarding tooreadily accept the weaknesses of the public sector asinevitable given the nature of governance available today andjumping into untested notions of public private partnershipwhich would suffer even more from these same problems ofgovernance.8) The National Human Rights Commission has adopted a
set of recommendations for moving towards the attainmentof health as a basic human right. These recommendationslook also at policy frameworks that are needed and monitoringand regulatory mechanisms that are needed to make the healthsystem function better. These also need to be incorporatedinto the Mission objectives
d) Role of the Private Sector
1. The need to involve the private sector in the provision ofthe affordable services for the poor and to contribute tonational health goals is appreciated. But there are someimportant concerns to be addressed before this becomespolicy.2. The flourishing unregulated and illegal sector (often calledthe informal sector or RMPs), is symptomatic of the breakdown of the health care system and this must not be projectedas the solution to rural health problems- much less equatedwith the private sector in health and as a structure that needsonly training and accrediting for integrating into the healthsystem. Recognising that this informal sector exists becausepeople have no where else to go and also noting that it reducessharply in extent once qualified service of even moderatequality becomes available, there is no need to activelyproscribe and punish the informal practitioner (as demandedby the IMA). However, we note that their continuationdepends so closely on the mystified doctor-disease-drugperception of health care that they have become one of themain means of propagation of a wrong perception of healthin the public and actively contribute to poverty by a wastefulconsumption of unnecessary health goods. In the context ofa large CHW programme, a strengthened subcenter and aPHC and CHC structure made functional, there would be noneed to invest in this informal structure, which by its verynature would be impossible to regulate and is now a pivot ofall wasteful and wrong notions of health care.3. The formal “qualified” private sector is also almostcompletely unregulated - in pricing of services, in quality ofservices and in ethics. A regulatory mechanism in place wouldbe mandatory before public private partnerships can beforged. We note that the National Human Rights Commissionhas also called for such regulatory mechanisms to come intoforce.4. The experience of private provisioning and public fundingof services is limited and problematic. Most of the dealshave had poor transparency and no public scrutiny. Theyhave required considerable public investments in privatehands with poor access to the poor in return. The cost benefitsand cost effectiveness of such options have not been workedout. There are no social insurance programmes reaching outto the poor to which private provisioning and public fundingof the programme may be linked and in its absencereimbursement alone would prove too costly. A national policyframework for engaging the private sector, incorporatingregulation of the private health sector, and with safeguardsagainst such initiatives becoming avenues for expandingmisgovernance, must be drawn up and scrutinised bythorough public debate before it is finalised.

mfc bulletin/April-May 2005 13
Public Hearings for the Right to Health:An Analysis of Different Approaches
-Abhijit Das1
Public hearings have emerged as an importantmechanism for sharing violations of economic, socialand cultural rights in India. The campaign on the Rightto Information has pioneered the use of public hearingsand now it is being increasingly applied to health relatedrights.A series of regional public hearings organised by theNational Human Rights Commission and the JanSwasthya Abhiyan concluded with the National PublicHearing on the Right to Health Care on December 16-17, 2004. One of the successes of this process was theadoption of a National Action Plan by the NHRC thatsuggests further actions for realising the right to healthcare. The success of this series of public hearings,coming as it does on the heels of the earlier successesof the Right to Information campaign, highlight theimportance of this mechanism in asserting and claimingsocial, economic and cultural rights which areotherwise non-justiciable.
Health in the Context of Human Rights
Though many human rights experts claim that thedivision of human rights into civil-political on one sideand social-economic-cultural on the other is an artificialone, the acknowledgement of this division is of greatimportance where the lives of the poor and marginalisedgroups are concerned. Civil and political rights are thosehuman rights which not only enjoy legal protection,but also much greater recognition and visibility.Arbitrary detention, torture and extra-judicialexecutions are some instances where individual civiland political rights are applicable. Social, economic andcultural rights, on the other hand, do not enjoy specificlegal protection. This is unfortunate, because most ofthe human rights, which are necessary for the dignifiedsurvival of marginalised communities, fall into thisdomain, including, among others, the right to health(Article 12 of the ICESCR). The right to health is alsorecognised and reinforced by sections in the CEDAW(Convention on the Elimination of All forms ofDiscrimination Against Women), CRC (Convention onthe Rights of the Child), and ICERD (International
Convention on the Elimination of All forms of RacialDiscrimination), as well as regional human rightstreaties. Despite much official recognition, these rightsare not protected by law, and the internationalconsensus is that the principle of progressiverealisation should apply. In the case of India, theConstitution takes note of these rights in Part IV, or theDirective Principles of State Policy.Although these rights are supposed to be fundamentalin the governance of the country, and although it isthe duty of the state to apply them while making law,they cannot be enforced in a court. Progressiverealisation has proceeded at a very slow pace (if at all)and the Indian state often fails in its duties as describedin the constitution. Thus the distinction between civiland political rights and economic, social and culturalrights is important because it reminds us of areas wherecommitments have been made but justice mechanismsare lacking, and that we still have a long way to go tobefore we can ensure a dignified life to all citizens ofthe country.Neo-liberal globalisation is a well-known threat to thelives of the economically vulnerable and often leadsthem to further destitution. Neo-liberal globalisationalso champions the rights of individuals (and eventhat of corporate entities) to trade without anyrestrictions based upon the protection of states fortheir right to do so. However, neo-liberal economicreforms pay little or no heed to economic, social andcultural rights, including the right to health care. In therealm of public health, neo-liberal reforms aremanifested in increased privatisation and fee-for-service policies which make it even more difficult forthe poor to access health care services. While theNational Action Plan adopted by the NHRC (after thePublic Hearing on the Right to Healthcare) has manyprovisions and activities for realising the right to healthcare, given the realities of our country, this processwill continue to remain an uphill task. The poor andmarginalised will need to continually assert and demandthat their rights and entitlements be respected, protectedand fulfilled. If public hearings are emerging as one ofthe mechanisms through which this assertion may bemade, it is necessary to examine the strengths and1Email:<[email protected]>

14 mfc bulletin/April-May 2005limitations of this process as well.
As Mechanism for Asserting and Claiming HumanRights
The articulation of a human right is several steps awayfrom either protecting or claiming a human right. TheUnited Nations Conventions and Committees engagein a process of clarification and interpretation bypreparing General Comments and GeneralRecommendations. In the case of the right to health, orspecifically “The right of everyone to the enjoymentof the highest attainable standard of physical and mentalhealth”, this has been through the General Comment14 of the ICESCR. While international health expertsnote that the right to health does receive legalprotection through some regional human rightsmechanisms, and that domestic mechanisms exist insome countries (Report of the Special Rapporteur onRight to Health 2003 E/CN.4/2003/58), specificinternational mechanisms to ensure and protect thisright have not been developed. In the absence of suchmechanisms there is a need to develop alternativemethods for claiming and protecting this right, andpublic hearings can be seen as one such method.State action for ensuring and protecting human rightsincludes the process of framing specific laws,developing monitoring mechanisms and ensuringjustice. While this is often adequate for civil and politicalrights, for economic social and cultural rightsgovernments need to institute special programmes forproviding services – as in the case of health oreducation. In India, there are few constitutionalprotections for the right to health. Aside frominterpretations of the right to life, there are some laws,which relate to health, such as the National MaternalBenefit Act, Child Marriage Restraint Act, ESI Act,MTP Act, Consumer Protection Act, and others. Somesections of the Indian Penal Code, notably thoserelating to consent, homicide, negligence and hurt canbe applied to the realm of irresponsible serviceprovision. However, these mechanisms are grosslyinadequate to protect the right to life of over one andquarter lakh women who die during pregnancy andchildbirth, even though mother and child health havebeen areas of special attention for health programs sinceindependence. Tuberculosis continues to affect overtwo million new people every year and kill approximately500,000, even though it has been part of a separate
national thrust for over 30 years. Many governmenthospitals and health centres remain unoperational,without doctors or drugs, and the equipment andsupplies lie rusting or rotting while the poor are forcedto take recourse to potentially dangerous, unqualifiedpractitioners. Tens of millions remain without safedrinking water and sanitation is a distant reality for anequal number of people. It is clear that the right tohealth has tremendous implications for the life anddignity of a large proportion of the citizens of India,even though it enjoys little protection.
Public Hearings and Truth and ReconciliationNon-state and international interventions forprotecting human rights include identification of rightsviolations, fact-finding of such cases, institutingmonitoring mechanisms, the preparation of reports, insome cases setting up tribunals, as well as lobbyingand advocacy to ensure redress and compensationsto victims and punishment to perpetrators. Truth andreconciliation commissions have also emerged asmechanisms for addressing large-scale human rightsviolations which take place in repressive politicalregimes. These are usually instituted after a new regimehas come to power and are meant to bring some form ofclosure to the humiliation faced by the repressedgroups. In India, public interest litigation has emergedas a legal mechanism to expand the interpretation ofexisting law for the protection of human rights, wherespecific provisions do not exist. It is necessary to finda place for public hearings within this broad set ofmechanisms.
Among the interventions mentioned, above publichearings can perhaps be compared to truth andreconciliation commissions, however there are somedifferences as well. Truth and reconciliationcommissions (TRCs) have been constituted in anumber of countries, though the one in South Africa isthe most renowned. These are extra-judicialcommissions where survivors and perpetrators of anacknowledged event in which human rights violationstook place are expected to provide testimonies. For thesurvivors it is a public acknowledgement of theirexperiences, and for the perpetrators it is anacknowledgement of their role in the violation of rights.It is expected to bring closure to the suffering and senseof violation of the survivors and simultaneously makethe perpetrators publicly acknowledge their culpability.

mfc bulletin/April-May 2005 15
1 Information on the Right to Information campaign wasobtained from <www.freedominfo.org> and<www.transparency.org>
TRCs do not typically include punishment, but thepublic acknowledgement of the suffering of survivorshelps those groups come to terms with their past andface their future with a new sense of purpose.There are a number of differences between publichearings in the current Indian context and a TRC. First,the public hearings that are under consideration takeplace in more or less the same political andadministrative setting that in which the human rightsviolation took place. Second, the perpetrators (whoare administrative and governance systems) are alsoreluctant either to recognise their violations or assumeculpability. Third, TRCs have usually been organisedto address gross civil and political rights violationsand not address social issues like livelihood, food,women’s rights or health.
Issues and Challenges
In India, as has already been mentioned, publichearings became popular mechanisms for communitiesto express their dissatisfaction and expose humanrights violations as part of the Right to Informationcampaign. Public hearings were organised to exposethe huge corruption that had taken place in spendingdevelopment funds in Rajasthan and elsewhere.Subsequently the National Women’s Commission anddifferent state commission’s have started usinghearings to address women’s issues. There is onesignificant difference between these hearings,organised by statutory commissions and the onesorganised by civil society campaigns. The women’scommissions are para-judicial bodies of the state andare empowered to take action and give instruction todifferent agencies of the state. The hearings organisedby the women’s commissions include representativesof different government departments and instant justiceis delivered by instructing these officials to redressthe grievances of individual claims and complaints. Inthis regard these hearings do not represent thecollective expression of a single claim, but are acollection of individual claims, most of which are of asimilar nature. Public hearings organised by the Rightto Information campaign, on the other hand, representthe collective expression of a single claim or violation.This distinction is important to understand in order to
examine the use of public hearings in cases of the rightto health.
As mentioned at the outset the notion of a jan sunwai,or public hearing, has been used by the Right toInformation campaign as a mechanism of non-violentprotest. However, it goes beyond mere protest byadding evidence and documentation to substantiatethe common violations faced by the poor in a communityand by arguing that development-related corruptionand deprivation are in fact violations of the right to life.Apart from being a practical weapon for exposingcorruption, these hearings also provide an opportunityfor deprived communities to assert their citizenshiprights in a democracy.1
The violation of the right to health care affects amarginalised community uniformly inasmuch as thewhole community is either deprived of health careservices or has inefficient, callous and corrupt services.However, this lack of services has a much greater impacton those with a perceived health problem than onthose without. In this regard, a public hearing can appearto be a set of grievances of individuals rather than anentire community’s claim for health. This difference hasa significant impact on how the claim is perceived andexpressed. If the public hearing emerges as a platformto voice individual complaints, then the purpose ofestablishing a common community claim may be diluted.
Individual Grievances or Collective Claim?
The distinction between a “collection of individualgrievances” and a “single collective claim” can beunderstood by considering public health in the contextof a human-rights framework. Classically, human rightswere applied only in the context of an individual’s rightto remain free and autonomous and to receive thesupport of the state in order to do so. It has even beenargued that the concept of individual rights is applicableto the developed world of America and Western Europebut conflicts with the sense of traditional communityidentity that is prevalent in much of the developingworld. Over the years, however, human rights scholarsand practitioners have applied an individual rightsconcept to make claims for the rights of marginalisedgroups. Since most traditional communities are deeplyhierarchical, they allege that the human rights of amarginalised group are made up of the individual and

16 mfc bulletin/April-May 2005common claims of each member of the marginalisedgroup, and in this way, the group can be seen as acollection of individuals. The right to health care canbe understood within this framework. Thus publichearings on the right to health ought to addressindividual violations but at the same time weave theseindividual testimonies into a more complete and unifiedexpression of a community claim. The sense of unifiedcommunity assertiveness is essential for the struggleto claim the right to make demands beyond the life ofthe public hearing. Quick fulfillment of individual claimsmay be detrimental to this process. Addressingindividual ‘cases’ may also deflect attention from thesystemic failures and inadequacies that lead toviolations of rights in the first place.
Another issue that needs careful consideration duringthe public hearing is the role and presence of theperpetrator group (health service providers andmanagers). In the case of a TRC, the perpetratorsobviously do not enjoy the same privileges that theydid earlier and so are forced to come face-to-face withtheir abusive acts. But in public hearings, especiallythose organised by civil society movements, it can bedifficult to ensure the presence of government parties,and even more difficult to make them accept culpability,even when they are present. In para-judicial publichearings (those organised by legally constitutedcommissions) where the presence of governmentagencies can be ensured, case by case orders forgrievance redressal can be detrimental to the overallpurpose of establishing a common community rightsviolation, for the reasons described above. Thegovernment parties can also challenge individualtestimonies, seriously undermining the fragile self-esteem of vulnerable groups. And finally, individualswho share their testimonies may later be victimised bythe agencies that are indicted. This can reduce thesense of assertion, which had enabled the marginalisedgroups to come forward with their claim or violation inthe first place.
All of this is not to argue that the redressal of individualrights violations or claims for compensation shouldnot be expressed through public hearings. Whatperhaps needs to be addressed is how this demand ismade and followed-up. This leads to the question ofwho takes the initiative for organising public hearings
and what should be the essential follow-up after it hasbeen organised. Public hearings are and should be seenas essentially political events of assertion of a claimand expression of a violation. They are significantlydifferent from a public consultation or dialogue whereindividual’s testimonies are presented so that commonelements can be derived from the various stories andthen the powers-that-be can decide on their course ofaction. The greater the distance between the communitywhose rights have been violated and the location ofthe hearing, the greater the chances that the publichearing will become an academic exercise rather than apolitical one, because distance determines whoorganises the event.The ownership of the public hearing should ideally bewith the community who is expressing its claim/violation. It should be a process initiated and controlledby the community. This precludes individual grievanceredressal taking precedence over the expression of acollective claim. Even the individual claims for redressaland compensation can then be followed up through acollective process. When claims are settled, the victorywould not simply belong to one individual but ratherto the whole community. Similarly, as an assertion ofits collective strength, the community can engage inother interventions such as filing cases in criminal orconsumer courts, raising public interest litigation, orother forms of collective action. The role of anintermediary organisation has to be seen in this contextand should not supercede that of the community.
Conclusion
The imperatives of economic reforms often leadgovernments to abandon basic social sector reform. Inthis age of neo-liberal reforms, the Indian health sectorseems to be condemned to die a natural, slow death.However, this is against the core interests of hundredsof millions of citizens in our country. It not only leadsto poorer health outcomes at the individual level, italso stands against the fundamental tenets of theconstitution. In such a situation, public hearings canbecome both a powerful mechanism for communitiesto demand health related rights and also a political toolto strengthen the process of participatory democracy.But they must be designed, carried out and followedup in such a way that it assists individual redressaland strengthen community processes at the same time.

mfc bulletin/April-May 2005 17
1Email: <[email protected]>
Dear readers, this is a series of narratives of womenwho have been living in far flung villages in Kashmirnot known to many people outside the state. Thevillages are remote and underdeveloped with minimalcontact with people outside the boundaries of theirvillages. These villages as is the story of most villagesin Kashmir have in the last sixteen to seventeen yearsof conflict survived almost without a trained or aqualified doctor. This series has been written to bringforth the women who are living in these villages silentlybearing the brunt of a war that they never understoodor wanted. I confess that in terms of the state of medicalcondition this series has nothing new to put forth. Butthere is just one difference; and that is the rangingconflict in the state for the last sixteen years. The stateof Kashmir has a medical infrastructure that is as defunctas the medical system in any part of India plus it has aranging battle to negotiate. It is this conflict that makeslife as been termed by the research participants“unbearable”.The second reason that has bothered me enough toput this series together is the fact that prominentscholars wanting to know why the right of reproductivehealth is such a big concern during the years of conflictwhen there are other major issues to be looked into?The only thing that I want to say is that women likeother people in conflict have rights and when thereproductive rights of the rest of the population arenot taken away then why are women denied this right.
Badila
Badila is a forty-year-old woman mother of two livingin a small village. She is supporting her family singlehanded, as her husband due to his leg disability is notable to work for a living. Badila considers it her luckthat in days when women’s education was not heardof, her parents educated her till the tenth grade. Evennow she is one of the few women in her village who iseducated and the only one who is working.She describes the various bans imposed on women asa way of subjugating them. She is a devoted followerof her faith yet does not understand the bans that wereimposed on people in general and women in particular.She describes them as a method to exercise controlespecially on the women of the valley. She says thateven if some of the bans were justified by the holybook (Koran), yet one has to see them in the light ofthe period in which they are being imposed. Citing herown family as an example she explains why the ban onmovement of women was irrational. She says that Koranhad divided work for men and women by which men
Women’s Narratives from Kashmir-1-Zamrooda Khandey1
were to go outside the house in search of work whilewomen were to look after the house. This system workedvery well in those days. But today, in her own house ifshe was not to go outside and work who would feedher family. “We would all die of starvation. They wantedto spread their terror all around that is all…Today whenI look at it I think they really wanted to send us womenback to dark ages.”Women and especially women’s health was the mostaffected by the militancy in the state. She says thathospitals were allowed to function because themilitants needed them for their own treatment as well.Yet the circumstances made the hospitalsdysfunctional. Destruction of infrastructure, lack ofstaff and supplies, unavailability of safe transport forstaff to be able to report on duty or for that matter forthe patients to be able to reach the hospitals renderedthe available services ineffective. People in the villageswere left with no choices but to rely on untrained medicalpractitioners posing to be doctors. Badila is very openabout saying that these un-trained doctors were thelifelines of the villages. If it were not for them manypeople would have died without any medication. Sheis honest in saying that though she is aware that thesedoctors can harm a patient yet in times of need shewould definitely consult them.Talking of bans, Badila says that she could rationaliseall bans but can never understand or justify the ban onfamily planning methods imposed by the militants. Thiswas a ban that bought in hardships like women hadnever seen earlier. “Hardships that really affected thehealth of the women, it became almost impossible forwomen to get any kind of safe treatment in thehospitals.”When asked what she meant by safe treatment shesaid that, “the hospitals were watched, so women couldnot avail the facilities offered by them. Even if a womanwould gather enough courage to go to a hospital thedoctors would refuse her. Everyone was scared.”Narrating her own experience in organising a “safe”ligation operation for herself this is what she had tosay:(She smiles): “Yes, I did, but only I know what I wentthrough for that operation. No hospital, no doctor waswilling and I was sure that I did not want it done by alocal doctor. There was this one doctor from our village,who was very good. He was in the hospital in Srinagar.I knew his family very well. Finally I requested him todo something for me. At first even he was not ready. Iliterally had to fall on his feet to make him agree. If ithad not been for him I don’t think I would have evermanaged the operation. He took pity on my state in life

18 mfc bulletin/April-May 2005and arranged for the operation. He arranged for anambulance to come and collect me in the middle of thenight. I was taken to some place I did not know. I wasoperated upon and before morning I was back home.No one knew of it except for my husband and the doctor.For a very long time I did not tell my in-laws. Theywould have been very upset, and they were when theygot to know about it, (smiles) but by then it was toolate for them to do anything. I was not the only womanwho must have hidden it like this. We had no choice.The militants would have gunned us down if they hadcome to know about it. Now when things are better wehave started talking about it. But even now one is carefulabout whom one talks to.”She goes on to say that there were times when evenparents or husbands were not informed.According to Badila, what made things worse was thefact that the ban was not followed in totality. She saysthat people always found ways to get around them. “Itis similar to my case. No doctor was willing to operateyet I got my operation done, similarly if one knew theright people one could get an abortion done as well.But yes it was not easy. Hearing me talk about it youmay feel that it was all very easy but believe me it wasnot. We had to face a lot of problems and theseoperations were done in conditions, which were notsafe for even an animal. Actually women were treatedlike animals in those days. Why else will otherwise allthese restrictions be placed only on us? There wasnever any ban on the men. They were free to dowhatever they wanted to.“Treatments were carried on in utmost secrecy andwould not be done unless the “doctor” knew youpersonally or you were well referred. It was not easy togain access to these doctors. The conditions underwhich the treatments were carried out were so bad. Ionce accompanied a relative of mine. When I saw theroom in which it was done I thanked my God that I didnot have to go through what I was a witness to. It wasa small shanty room in back lane of a poorneighbourhood of the city. There was just the doctorand me. All through the operation I kept wonderingwhat if something goes wrong what will happen to her.The closest hospital was about 4 kilometres away. Morethan anything else the fear that someone may come inwas traumatising not only for the patient, but for thedoctor as well as me who was accompanying the patient.We all knew that if some one came to know we wouldbe killed within a second. I am still amazed that thedoctor actually managed to do the operationsuccessfully. To be honest if I was in his position Iwould never have had the heart to go through so muchpressure and tension. That was the only time I agreedto accompany a person for an operation. After thatone experience I simply refused I did not have thecourage to go through it again.” (To be contd.)
The adivasi belt of Panchmahaals and Dahod has oftenbeen referred to as a drought-prone or flood-hit region.Scratch the surface a bit harder and the stark reality ofthe issues of food insecurity stare at the peopledwelling in this region unblinkingly.As part of the Anna Suraksha Adhikar Abhiyan,Gujarat, ANANDI (Area Networking and DevelopmentInitiatives) along with Devgadh Mahila Sangathan andPanam Mahila Sangathan organized a two-dayconvention on Dec 6-7, 2004 to create awareness andexpose the irregularities that exist in the system.The public distribution system (PDS) lies in shamblesas “unfair shops” are running without a bother. Themanner in which APL (Above Poverty Line) and (BelowPoverty Line) cards are distributed raises doubts.Widows, jobless adivasis, old and impoverished oneshave been “awarded” with APL cards, therebydepriving them of basic rights to food security.Issues pertaining to lack of proper implementation invarious government schemes were discussed on Dec 6in group meetings to create awareness among the womenwho gathered in droves at Sagar Mahal in DevgadhBaria. Nutritional food insecurity could be one of thecontributing factors for high prevalence of anemiaand chronic energy deficiency among the womenparticipants.On the second day, a play by the tribal artists on issuesof food insecurity created room for Jan Sunwai. Over afifteen hundred affected people from Panchmahaals,Dahod, Sabarkanta, Bharuch, Surat, Narmata, Valsadand Baroda district besides people from Saurashtra andCentral Gujarat and Chhattisgarh shared theirgrievances at the Jan Sunwai.Bajiben Rathwa of Diviya said no road ever reachedtheir village, which lies in the midst of forest,inaccessible to the outside world, as there were notransport facilities. There is no fair price shop (FPS) inDiviya. Their condition worsened during flood andthere was a case of death in the area where in the victimBodiben starved to death, as she had no money to buyfrom regular shops. In Gajapara 49 cardholders (BPL)have been given only 5 kg wheat 2 kgs of rice while theentries are made for 9 kg and 3 and half kgs.As per a recent Government of Gujarat GR, per cardallocation of food grain has been increased from 12and half to 25 kgs only as against Supreme Courtorder of 35kg. However, the additional food grain isavailable at higher rates thereby violating SC orders.Five women in Ankli were not given edible oil in themonth of September, but the entries for the same weremade in their ration cards.According to Budhabhai Titiyabhai of Lavaria(Devgadh Baria taluka), “I get only 5 kgs of wheat and3 kgs of rice every month in the Antyodaya Yojana.”
ReportAdivasis Speak out for
Implementation of Supreme CourtOrders

mfc bulletin/April-May 2005 19As per the Yojana he is entitled to 35 kg of grains.Gangaben Baria, a widow from Ranjitnagar (Ghoghambataluka) has no ration card. Her son is disabled and hasno other source of income and is deprived ofgovernment schemes.When the panelists asked how many people there arefacing similar problems, barring a few, all hands wentup.Sayeedaben from Boru (Kalol) spoke on behalf of other176 Muslim families of her village. Their ration cardsand other important documents were reduced to ashesduring the riots of 2002. “The Sarpanch of the villagealso fled and we are left in the middle of nowhere,” shesaid.Navliben Mura of Gajapara (Ghoghamba taluka) holdsa BPL card, which was later, stamped as APL. Similarly,several others like Mangiben Ratan of village Bor(Ghoghamba) and Dayliben Shankar Gajapara(Ghoghamba taluka) faced the same problem. Duringthe discussion it was found that most of the peoplepresent there had the same confusion whether theywere APL or BPL. All panelists agreed that there is nomarked difference in determining “how poor is a poorperson” and is based on individual perception. ShriPrashant Joshi, DSO (Panchmahaals), responded bymaintaining that as their department lacked manpower,the task of preparing the cards was given to a “privatecompany” which led to the confusion. He has, however,committed to taking a look at these cards and revisingthem if necessary.The panel was chaired by noted journalist and activistShri Indukumar Jani and included senior officials,activists and researchers.Kailashben Baria from Ruparel village (Ghoghamba)and Veenaben Parmar of Chandranagar (Ghoghamba)complained about irregularities in mid-day meals. Thestock also finds a way to the co-cordinator’s house.Santokben Baria of Bara (Baria), a cook in a primaryschool for mid-day meal scheme said, there was nokitchen shed, which is a necessity as per the SC order.Dinesh Baria from Baria falia in Panchmahaals districtcontributed his land for building a school. When heapplied for the post of co-ordinator (mid-day meal) hisapplications was rejected under the pretext that he wasnot “old enough” and rudely asked to get out of theoffice.Kokilaben from Ruparel said there was nosupplementary nutrition (mamara) for the past sixmonths. For three months the helper fed from her ownincome. In response to this Mr.Lalubhai Desai said “Ispoke to the person who runs this factory in Mehsana.He told me that the state of Gujarat has not paid him forsix months due to which he had stopped the supply.But rot runs even deeper. Mr.Amitabh Mukhopadhyaymade a startling revelation that no audit report hasbeen tabled for discussion in the Vidhan Sabha inGujarat from the past ten years.The Collector, Mr. Solanki, assured that action wouldbe taken to ensure food security in the region. He urged
the tribal people to come forward and submit theirgrievances along with proof following which theshutters of unfair shops will be pulled down.The DSO (Panchmahals) stated that they will follow upthe cases and respond to them in writing as soon aspossible. Mr.Samir Garg shared his experiences of Right to FoodCampaign in Chattisgarh where in strong grassro9otsmovement along with state level advocacy led tocancellation of 4,000 licensees of Fair Price Shopsacross six tribal districts.
Other HighlightsØ Panchmahaals and Dahod districts (combined)have been identified as one of the 100 most impover-ished districts of India by the government.Ø Despite the fact that Gujarat counts as one of themost prosperous states in the country today, 20.4%population gets less than the required 1890 calorieswhich is higher than the entire nation’s 13.4% as per aresearch carried out by the M.S. Swaminathan ResearchFoundation (Chennai).Ø The Supreme Court has passed 11 interim orderspertaining to enhancement and strengthening of theprovisions and monitoring mechanisms for variousgovernment schemes affecting to food securityparticularly the marginalized groups. This is in light ofthe PIL for Right to Food, filed by PUCL (People’s Unionfor Civil Liberties), Rajasthan.Ø For more details refer to<www.righttofoodindia.org>Ø As per a recent survey in 1,435 families inPanchmahaals and Dahod, 80% families face foodinsecurity for over six months. Only 10% families haveproper meals throughout the year for all members.Panchmahaals (undivided) is the most food insecuredistrict in Gujarat.Some other events during this two-day convention:Ø An audio cassette release of “Andhare Atwaiye”(Caught in darkness) was held on Monday. The 11 folksongs in the cassette have been written and sung bythe tribal artists of Devgadh Mahila Sangathan. Thesongs mainly deal with issues related to food insecuritylike irregularities in mid-day meal scheme. AntoyodayYojana, Annapurna Yojana and Targeted PublicDistribution Scheme.Ø A mashaal rally wherein over 600 adivasi womenand men participated was carried out in Devgadh Bariatown in the evening.As part of Anna Suraksha Adhikar Abhiyanconventions would be held in Rajkot, Jamnagar andBhavnagar in the next three months.-ANANDI (Area Networking and Development Initiatives)For more details please contact Neeta Hardikar – (02678)220226, 221097,email: <[email protected]>
20 mfc bulletin/April-May 2005
ContentsCHW: Survivals and Revivals -Shyam Ashtekar 1National Rural Health Mission: Comments - JSA NCC 8Public Hearings for the Right to Health:An Analysis of Different Approaches -Abhijit Das 13Women’s Narratives from Kashmir-1 -Zamrooda Khandey 17Adivasis Speak out for Implementation of Supreme Court Orders -ANANDI 18
Editorial Committee: Anant Bhan, Neha Madhiwalla, Dhruv Mankad, Amita Pitre, C. Sathyamala, Veena Shatrugna,Chinu Srinivasan. Editorial Office: c/o, LOCOST, 1st Floor, Premananda Sahitya Bhavan, Dandia Bazar, Vadodara 390 001email: [email protected]. Ph: 0265 234 0223/233 3438. Edited & Published by: S.Srinivasan for Medico Friend Circle,11 Archana Apartments, 163 Solapur Road, Hadapsar, Pune 411 028.
Views and opinions expressed in the bulletin are those of the authors and not necessarily of the MFC. Manuscripts may besent by email or by post to the Editor at the Editorial Office address.
MEDICO FRIEND CIRCLE BULLETINPRINTED MATTER - PERIODICAL
Registration Number:If Undelivered, Return to Editor, c/o, LOCOST,1st Floor, Premananda Sahitya BhavanDandia Bazar, Vadodara 390 001
Economical Tools Available for HealthWork
For the village health workersThermometersTeaching stethoscopesBreath counterPictorial formularyGrowth monitoring booklets
For communitiesA paper strip test for detecting contaminateddrinking water and disinfection systemMosquito repellent oilSafe delivery kitAmylase rich flourORS packets
For rural laboratories and mobile clinicsAnemia detection kitsElectrophoresis kit for sickle cell anemiaTests for urinary tract infectionConcentration test for detection of TB bacteriaLow cost carbon dioxide incubator for cultivationof TB bacteriaCleaning system for glasswareVaginal infection diagnostic kit
For the clinic and pharmacyPortable StadiometerTablet breaking deviceParacetamol in gel form
Come and learn more about these tools and kits at
a workshop, on March 25-26, 2005 at JeevanDarshan, Fatehgunj, Baroda. For details contact:Jan Swasthya Sahyog,, I-4, Parijat Colony, NehruNagar, Bilaspur- 495 001, Chhattisgarh.Email:<[email protected]>Phone andfax: 07752-270 966. or LOCOST at 0265-283009,email: <[email protected]>
Subscription Rates
Rs. U.S$ Rest ofIndv. Inst. Asia world
Annual 100 200 10 15Life 1000 2000 100 200The Medico Friend Circle bulletin is the officialpublication of the MFC. Both the organisation andthe Bulletin are funded solely through membership/subscription fees and individual donations.Cheques/money orders/DDs payable at Pune, tobe sent in favour of Medico Friend Circle, addressedto Manisha Gupte, 11 Archana Apartments, 163Solapur Road, Hadapsar, Pune - 411028. (Pleaseadd Rs. 15/- for outstation cheques). email:<[email protected]>
MFC ConvenerRitu Priya, 1312, Poorvanchal, JNU Campus,New Delhi -110 067. Email: <[email protected]>MFC website:<http://www.mfcindia.org>





























