Embed Size (px)
Citation preview

Featured Article
Meningiomas May Be a Component Tumor of Multiple EndocrineNeoplasia Type 1
Behnam Asgharian,1 Yuan-Jia Chen,1
Nicholas J. Patronas,2 Paolo L. Peghini,1
James C. Reynolds,3 Alexander Vortmeyer,4
Zhengping Zhuang,4 David J. Venzon,5
Fathia Gibril,1 and Robert T. Jensen1
1Digestive Diseases Branch, National Institute of Diabetes andDigestive and Kidney Diseases, NIH; 2Diagnostic RadiologyDepartment, Warren Grant Magnuson Clinical Center, NIH; 3NuclearMedicine Department, Warren Grant Magnuson Clinical Center, NIH;4Molecular Pathogenesis Unit, Surgical Neurology Branch, NationalInstitute of Neurological Disorders and Stroke, NIH; and5Biostatistics and Data Management Section, National CancerInstitute, NIH, Bethesda, Maryland
AbstractPurpose: Recently, an increased incidence of some non-
endocrine tumors are reported in patients with multipleendocrine neoplasia type 1 (MEN 1). There are rare reportsof meningiomas and other central nervous system tumors inthese patients, but it is unknown if they are more frequent orif allelic loss of the MEN1 gene is important in their patho-genesis. The aim of this study was to address these two latterquestions.
Experimental Design: Results from a prospective studyof 74 MEN 1 patients with suspected/proven pancreaticendocrine tumors (PETs) were analyzed, as well as molecu-lar studies performed on a resected meningioma. All pa-tients had serial brain imaging studies (computed tomogra-phy, magnetic resonance imaging, and octreoscanning since1994) and yearly studies evaluating MEN 1 involvementwith a mean follow-up of 7.2 years. Results were comparedwith 185 patients with sporadic Zollinger-Ellison syndrome.
Results: Six patients (8%) had meningiomas. Meningi-omas were single and found late in the MEN 1 course (meanage � 51 years). Magnetic resonance imaging/computedtomography were more sensitive than octreoscanning. Theirdiagnosis averaged 18 years after the onset of hyperpara-thyroidism, 10–15 years after pituitary disease or PETs.Meningiomas were 11 times more frequent in patients withPETs with MEN 1 than without MEN 1 (P � 0.017). Noclinical, laboratory, or MEN 1 feature distinguished patients
with meningiomas. Meningiomas were asymptomatic and60% showed no growth. A resected meningioma showed lossof heterozygosity at 11q13 and 1p, including at p73 andARHI/NOEY2 locus, but not at the neurofibromatosis 2gene locus.
Conclusions: These results show meningiomas are notan infrequent occurrence in MEN 1, and loss of the functionof the MEN1 gene product plays a role in their pathogenesisin these patients.
IntroductionMultiple endocrine neoplasia type 1 (MEN 1) is an auto-
somal dominant disorder caused by mutations in the MEN1 geneon chromosome 11q13 (1, 2). Patients characteristically developtumors of the parathyroid, enteropancreatic tissue, and anteriorpituitary (1–4). More recently, an increased occurrence of otherendocrine tumors as well as nonendocrine tumors are reported inpatients with MEN 1, including skin tumors (melanomas, col-lagenomas, and angiofibromas), carcinoids (thymus, lung, andgastric), lipomas, as well as tumors of the adrenal and smoothmuscle (1, 2, 5–15). Some of these tumors [parathyroid, pitui-tary, pancreatic endocrine tumors (PETs), carcinoids, smoothmuscle, and skin tumors] have allelic losses at the MEN1 locuson 11q13; therefore, alterations in the MEN1 gene play a keyrole in their pathogenesis, whereas with others (thymic carci-noids, and adrenal), this is not the case (1, 2, 5–15) and theirpathogenesis remains unclear.
Central nervous system (CNS) tumors, including ependy-momas (16, 17), schwannomas (9, 18, 19), and meningiomas(20, 21), have rarely been reported in patients with MEN 1 orMEN 1-variant syndromes. However, some of the tumors suchas meningiomas are common CNS tumors in the general pop-ulation with an annual rate of 7.8/100,000, comprising 20% ofall CNS tumors (22) and have rarely been reported in MEN 1(20, 21). Therefore, whether meningiomas or any of these CNStumors occur with increased frequency in patients with MEN 1is unknown. It is also unknown if they do occur whether alleliclosses in the MEN1 gene are found in these tumors, and there-fore, alterations in this gene plays a central role in their patho-genesis in MEN 1 patients.
In our ongoing prospective study of patients with possiblePETs with MEN 1, in addition to serial evaluations of MEN 1involvement, CNS assessments using brain magnetic resonanceimaging (MRI) and computed tomography (CT) are performedinitially and at yearly evaluations. This study reports the anal-ysis of this prospective study and reveals that 8% of the 74patients with MEN 1 followed up to 19 years developed men-ingiomas. A comparison with similar patients without MEN 1with PETs showed this was a highly significant increase andmolecular studies of a meningioma from a MEN 1 patientrevealed allelic loss at 11q13 at the MEN1 locus as well as atchromosome 1p but not at the neurofibromatosis 2 (NF2) locus.
Received 6/17/03; revised 10/8/03; accepted 10/22/03.The costs of publication of this article were defrayed in part by thepayment of page charges. This article must therefore be hereby markedadvertisement in accordance with 18 U.S.C. Section 1734 solely toindicate this fact.Note: B. A. and Y-J. C. contributed equally to this work.Requests for reprints: Robert T. Jensen, NIH/NIDDK/DDB, Building10, Room 9C-103, 10 Center Drive MSC 1804, Bethesda, MD 20892-1804. Phone: (301) 496-4201; Fax: (301) 402-0600; E-mail: [email protected].
869Vol. 10, 869–880, February 1, 2004 Clinical Cancer Research
Research. on August 5, 2021. © 2004 American Association for Cancerclincancerres.aacrjournals.org Downloaded from

Materials and MethodsOne hundred twenty-eight consecutive patients with MEN
1 with or without Zollinger-Ellison syndrome (ZES) evaluatedbetween July 1975 and August 2002 at NIH were considered forthis study. Patients were eligible for the study if they had regularpituitary and whole brain imaging with CT scanning or MRI.
This study is part of an ongoing prospective study ofpatients with ZES with or without MEN 1 since 1975 and isapproved by the Clinical Research Committee of the NationalInstitute of Diabetes, Digestive, and Kidney Diseases.
Diagnostic criteria for MEN 1, as previously described (23,24), included presence of a combination of PET, pituitary dis-ease, hyperparathyroidism, positive genetic test for MEN 1, orthe presence of any of the above with a known family history ofMEN 1. Of the 74 patients with MEN1, we have completedsequencing of the MEN1 gene in 62 patients, of which, 90% hada germ-line mutation. We have not sequenced all of the patientswith sporadic ZES; however, we have sequenced 35 consecutivecases of sporadic ZES, including 1 patient with sporadic ZESwith a meningioma and none had MEN1 gene mutations. Thepresence or absence of a PET was determined by surgicalexploration or by imaging alone. The diagnosis of ZES wasmade biochemically as described previously (25). Serum gastrinconcentrations were measured by Bioscience Laboratories (NewYork, NY) and by Mayo Clinic Laboratories (Rochester, MN).
Study Protocol. During the initial evaluation at the NIH,all patients underwent studies to determine the extent of in-volvement of MEN 1 as described previously (23, 24). Theseincluded a detailed review of symptoms compatible with gastricacid hypersecretion, a personal or family history of MEN 1-related symptoms, and laboratory studies to assess for presenceof hormonal activity (parathyroid, pituitary, adrenal, and pan-creas). Laboratory studies included measurement of serum par-athyroid hormone (intact and mid-molecule), prolactin, fastingserum gastrin, calcium (ionized and total), proinsulin, insulinand simultaneous glucose, growth hormone, glucagon, adreno-corticorticotropic hormone, thyrotropin, chromogranin A, pan-creatic polypeptide, albumin, and urinary cortisol. For the diag-nosis of ZES, the patients had assessment of gastric acidsecretory rate, measurement of fasting serum gastrin concentra-tion on 3 separate days (25), and secretin provocative testing(when secretin was available) with a bolus injection of 2 clinicalunits of secretin/kg body weight (25, 26). To define the extentand location of PETs, all patients underwent abdominal imagingas previously described (27, 28) with ultrasound, CT scanningwith i.v. contrast, MRI, and selective abdominal angiography ifthe results were unclear. Somatostatin receptor scintigraphy(SRS) was performed routinely since 1994 by injection of(111In-DTPA-D-Phe1) octreotide followed by whole body aswell as single-photon emission computed tomography images asdescribed previously (27, 28). The onset of a PET was deter-mined either as the time of onset of symptoms in the patientswith functional PETs or as the time of the first imaging diag-nosis with a nonfunctional PET. The duration of the PET wasdetermined as the time of onset of the PET until their lastfollow-up or death.
The onset of MEN 1 was determined as the time of onsetof symptoms compatible with MEN 1, including nephrolithiasis,
pituitary disease, symptomatic PET, detection of a PET, or thetime of first detection of an abnormal laboratory value compat-ible with MEN 1 hormonal overactivity in an asymptomaticpatient with known family history of MEN 1. The time ofdiagnosis of MEN 1 was the time of confirmation of MEN 1 atthe initial visit or the time of first diagnosis before NIH pres-entation at an outside institution. In patients with multiple par-athyroidectomies, the initial parathyroid surgery was taken formeasurement of years from parathyroidectomy.
All patients had brain imaging with a CT scan or MRI aswell as imaging of the pituitary fossa initially and during eachsubsequent evaluation. MRI was generally used with CT scan-ning performed in patients with a contraindication to MRI. Inpatients with any abnormality, both studies were done. MRIscans were performed using a 1.5-T magnet (General Electric,Milwaukee, WI). T1-weighted (repetition time in ms/echo timein ms, 415-550/11-16) and T2-weighted (2500-4384/90-110)spin-echo images were obtained, with a 5-mm section of thick-ness. The T1-weighted scans were repeated after the adminis-tration of 0.1 mmol of gadopentetate dimeglumine/kg bodyweight (Magnevist; Berlex Laboratories, Wayne, NJ). CT scanswere performed using Isovue (Bracco Diagnostic, Inc., Prince-ton, NJ). The time of diagnosis of a meningioma was deter-mined as the first time it was identified on imaging. An expe-rienced neuroradiologist (N. P.) diagnosed all meningiomas.The radiological diagnosis of meningioma was made by thepresence of an extra axial dural-based mass that was uniformlyand markedly enhanced with contrast materials (22, 29, 30).Possible symptoms of the meningioma were evaluated by adetailed review of likely CNS symptoms. The largest diameterof each meningioma was determined initially and comparedwith the diameter in the last study to assess change in size of themeningioma.
All patients had serial studies with all but 1 patient in thepresent study having serial follow-up evaluations at least yearly.During the follow-up visits, in addition to brain and pituitaryimaging, abdomen imaging, as well as the plasma hormoneassays listed above that were performed on the initial study,were all repeated. Patients with metastatic disease had follow-upvisits every 3–6 months to assess changes in extent of themetastases as described previously (31, 32).
The frequency of meningiomas in the 65 patients withMEN 1 with ZES was compared with that of 185 patients withZES without MEN 1 (i.e., sporadic ZES) who had undergonesimilar brain imaging studies.
Statistics. Continuous variables were compared usingthe Mann-Whitney U test and discontinuous variables usingFisher’s exact test or �2 test. P � 0.05 was considered signifi-cant. Results are reported as mean � SE.
DNA Samples. Tumor tissue from the meningioma of 1of the patients with MEN 1 was obtained by microdissectionfrom the formalin-fixed, paraffin-embedded sample. Tumor tis-sue was microdissected from four different areas on one slideand was digested in four tubes to release tumor genomic DNAby a 3-day incubation in 30 �l of TE solution [10 mM Tris (pH8.0)-1 mM EDTA, 0.5 mg/ml proteinase K, 0.5% Tween 20] at37°C. Normal genomic DNA from the patient as well as fromher mother was isolated from peripheral blood leukocytes using
870 Meningiomas in MEN 1
Research. on August 5, 2021. © 2004 American Association for Cancerclincancerres.aacrjournals.org Downloaded from

the Puregene DNA isolation kit (Gentra System, Minneapolis,MN). DNA was stored at 4°C until PCR amplification.
Microsatellite DNA Markers. Six polymorphic markers(D11S480, D1S1883, PYGM, D11S4946, D11S449, and
INT-2) spanning the MEN1 locus (33, 34) and 5 markers span-ning the NF2 suppressor gene (D22S268, D22S1163, D22S929,D22S280, and D22S282; Ref. 35) as well as 12 markers span-ning chromosome 1p were ordered from Invitrogen, ResGen
Table 1 Comparison of clinical and laboratory characteristics of patients with multiple endocrine neoplasia type 1 (MEN 1) with andwithout meningiomas
Number (percentage)a
Meningioma present Meningioma absent Total
Patient number 6 68 74Age at onset of MEN 1 (yrs)b 33.2 � 5.9 29.8 � 1.2 30.1 � 1.2Age at diagnosis of MEN 1 (yrs) 41.8 � 9.2 36.0 � 1.4 36.5 � 1.5Age at diagnosis of hyperparathyroidism (yrs) 40.0 � 9.9 35.4 � 1.3 35.7 � 1.3Male gender 2 (33%) 32 (47%) 34 (46%)Follow-up duration at NIH (yrs)c 7.6 � 4.2 7.2 � 0.8 7.2 � 0.8MEN 1 duration (yrs)d 20.5 � 6.2 18.4 � 1.4 18.6 � 1.4MEN 1-related death during follow-up 0 (0%) 2 (3%) 2 (3%)Family history of MEN 1 5 (83%) 50 (73%) 55 (74%)Fasting serum gastrin (pg/ml)e
Mean � SE 425 � 297f 23,500 � 14,000 21,675 � 12,800Median 165 735 577(Range) (28–1,900) (24–930,000) (24–930,000)
Serum chromogranin A (ng/ml)e
Mean � SE 227 � 110 470 � 149 448 � 136(Range) (12–582) (4.3–6,639) (4.3–6,639)
Serum prolactin (�g/liter)e
Mean � SE 27.5 � 8.4 26.9 � 5.9 26.9 � 5.5(Range) (11–68) (2–377) (2–377)
a Percentage of MEN 1 patients with the characteristic in the indicated meningioma category.b Age at first MEN 1 symptom or discovery of abnormal laboratory value.c Time from first NIH evaluation to present.d Time from MEN 1 onset to present.e Normal reference values: fasting serum gastrin (�200 pg/ml), chromogranin A (�5.6 ng/ml), and prolactin (�11 �g/liter).f P � 0.02 compared with patients without meningiomas.
Table 2 Comparison of MEN 1 features in patients with or without meningioma
Number (percentage)a
Meningioma present (n � 6) Meningioma absent (n � 68) Total
Hyperparathyroidism present 5 (83%) 68 (100%) 73 (98%)Parathyroidectomy 4 (67%) 58 (85%) 62 (84%)Years from parathyroidectomyb 15.8 � 7.0 12.5 � 1.4 12.7 � 1.3
Pancreatic endocrine tumor (PET) present 4 (67%) 61 (90%) 65 (96%)Zollinger-Ellison syndrome 4 (67%) 61 (90%) 65 (96%)Duration of PETc 11.2 � 5.8 11.0 � 1.0 11.0 � 1.0
PET extentd
Localized 4 (67%) 47 (69%) 51 (69%)Liver metastasis 0 (0%) 14 (20%) 14 (19%)
PET Resection 3 (50%) 39 (57%) 42 (57%)Years from PET resectionb 5.6 � 3.9 7.4 � 1.0 7.3 � 0.9
Pituitary adenoma present 3 (50%) 27 (40%) 30 (40%)Pituitary adenoma resection 1 (17%) 9 (13%) 10 (14%)Years from adenoma resectionb 37.8 10.3 � 2.6 13.0 � 3.6
Other tumorse 1 (17%) 16 (24%) 17 (23%)a Percentage in each meningioma category.b Years from surgery to present.c Years from diagnosis of PET to present.d Extent determined by surgical pathology (n � 42) or radiological imaging (n � 32). ‘Localized’ refers to presence of a PET without distant
metastasis (i.e., bone, liver).e Other tumors include: papillary thyroid cancer (n � 1); prostate cancer (n � 1); renal cell papillary cancer (n � 1); basal cell cancer (n � 2);
uterine fibroid (n � 1); renal cystadenoma (n � 1); renal angiolipoma (n � 1); esophageal leiomyoma (n � 2); esophageal cancer (n � 1); melanoma(n � 3); uterine leiomyosarcoma (n � 1); bladder cancer (n � 1); uterine adenocarcinoma (n � 1); rhabdomyosarcoma sarcoma (n � 1); and coloncancer (n � 1).
871Clinical Cancer Research
Research. on August 5, 2021. © 2004 American Association for Cancerclincancerres.aacrjournals.org Downloaded from

(Carlsbad, CA) based on the published papers (36) and onlinedata.6
PCR. The tumor DNA and leukocyte DNA of the pa-tient, as well as the leukocyte DNA of her mother, were ampli-fied by PCR using a GeneAmp PCR system 9700 Thermo-cycler (PE Applied Biosystems, Foster City, CA) with thefollowing conditions: 94°C for 5 min; 94°C for 45 s; annealingat 59°C for 45 s; and extension at 72°C for 45 s for total 35cycles. Each reaction contained 1.5 �l of 10� PCR buffer, 1.5�l of tumor DNA or normal control DNA (�10–20 ng), 10pmol of each primer, 2.5 units of Gold Taq polymerase (PEApplied Biosystems), and 130 �M each of deoxynucleosidetriphosphate. The final concentration of Mg2� was 1.5 mM, and-P32-dCTP (0.1 �l/reaction; 3000 Ci/mmol) was included ineach PCR reaction.
Analysis of Allele Loss. After PCR, products weremixed with loading dye (v/v � 1/1), denatured at 95°C for 10min, then chilled immediately at 4°C. Four �l of products wereanalyzed by electrophoresis through a 6 or 8% denaturing poly-acrylamide gel in 1� Tris-borate EDTA buffer. The gels werethen dried and exposed to X-ray films (Kodak X-Omat AR;Eastman Kodak Company, Rochester, NY) with or without anintensive screen for 8 h to 3 days. The intensity of signals in thefilms was analyzed and quantified by using Kodak Image station440 system (Eastman Kodak Company). Loss of heterozygosity
(LOH) was defined as a reduction of at least 50% observed inthe allelic ratio between the tumor and normal DNA (37, 38).
ResultsSeventy-four patients met the study criteria in that they all
had brain and pituitary imaging on admission and subsequentfollow-ups. In these 74 patients, 92% had an initial MRI, and theremainder had an initial CT either because MRI was not avail-able at the time or was contraindicated. The 74 patients had amean age of onset and diagnosis of MEN 1 in the fourth decade,and mean duration of total follow-up from MEN 1 onset was 19years with 7.2 years occurring at NIH (Table 1).
A meningioma was identified in 6 of the 74 patients byimaging (Table 1). In the 6 patients with meningiomas, 5 of 6(83%) had hyperparathyroidism, 4 of 6 (67%) had a PET withZES, and 3 of 6 (50%) had a pituitary adenoma (Table 2).Meningioma was found late in the course of the MEN 1 with amean time of 17.6 years after the onset of the MEN 1 (Table 3)at a mean age of 51 years. However, there was a wide range inage at diagnosis of the meningioma, varying from 29 to 76 years(Table 3). The meningioma was diagnosed on the average 18years after the onset of hyperparathyroidism and 14 years afterthe onset of ZES and pituitary disease (Table 3). Meningiomaswere also diagnosed after patients had been treated for the morecommon manifestations of MEN 1 with parathyroidectomies,pituitary surgery, or resection of a PET (Table 3). In no case wasthe meningioma diagnosed caused by symptoms, instead in all 6cases, it was found on routine imaging studies (Table 4).
MEN 1 patients with or without meningiomas did not differin their age at onset or at diagnosis of MEN 1, age at diagnosisof hyperparathyroidism, percentage with male gender, durationof follow-up for MEN 1-related disorders, percentage with afamily history of MEN 1, the mean serum prolactin, or the meanchromogranin A levels (Table 1). The mean serum gastrin level
6 Internet address: http://www.gdb.org.
Table 3 Characteristics of multiple endocrine neoplasia type 1(MEN 1) patients with meningiomas
Number (%)
Age (yrs) at diagnosis of meningiomaMean � SE 50.8 � 7.6(Range) (29–76)
Onset of MEN 1 to meningiomaMean � SE 17.6 � 6.1(Range) (2–37.8)
Onset of hyperparathyroidism to meningiomaMean � SE 18.2 � 5.8(Range) (2–30.9)
Onset of ZES to meningiomaMean � SE 13.9 � 6.0(Range) (1.5–25.7)
Onset of pituitary disease to meningiomaa
Mean � SE 14.1 � 11.4(Range) (0.5–37)
Years from pancreatic endocrine tumorresection to meningiomab
Mean � SE 4.0 � 4.1(Range) (0.4–12)
Pituitary resection 1 (17%)Years from pituitary resection to meningioma 36.7Parathyroidectomyc 4 (66%)Years from parathyroidectomy to meningioma
Mean � SE 11.5 � 6.6(Range) (2.6–27.7)
a Three of the 6 patients with meningiomas had pituitary disease.b Four of the 6 patients had a pancreatic endocrine tumor.c Five of the 6 patients had hyperparathyroidism.
Table 4 Characteristics of meningiomas in the six MEN 1 patients
Number (%)
Symptoms related to meningioma 0Location
Frontal lobe 2 (33%)Planum sphenoidale 3 (50%)
Intraosseous 1 (17%)Posterior fossa 1 (17%)
Octreotide scan positivea 3 (60%)Follow-up of meningioma (yrs) 3.6 � 1.8Initial size (mm)b
Mean � SE 16.0 � 3.2(Range) (8–30)
Increase in size during follow-upc,d 2 (40%)Extent increase in size (mm) 1.4 � 1.2% increase in size (mm) 16.7 � 14.7% increase in size/year 17.3 � 13.7
a Five of 6 patients had octreotide scan.b Size was determined as the largest diameter with computed to-
mography scan or magnetic resonance imaging at initial discovery.c Change in size was determined from serial computed tomography
scan and magnetic resonance imaging and is expressed as mm change indiameter over the follow-up period.
d Five of 6 patients had follow-up imaging. One patient had me-ningioma recently discovered.
872 Meningiomas in MEN 1
Research. on August 5, 2021. © 2004 American Association for Cancerclincancerres.aacrjournals.org Downloaded from

was significantly higher in patients without meningiomas (P �0.02 without correction for multiple, highly correlated compar-isons; Table 1).
The manifestations of MEN 1 in patients with or without ameningioma are compared in Table 2. Almost all patients in thenonmeningioma (83%) and meningioma (100%) groups hadhyperparathyroidism, and the percentage having a previous par-athyroidectomy at the time the meningioma was diagnosed wasnot significantly different (85 versus 67%, P � 0.24) nor wasthe duration from the parathyroidectomy (Table 2). The majorityof the patients in the meningioma group (67%) had a PET withZES, as did the patients in the nonmeningioma group (90%),and the duration of the PET was not significantly different in thetwo groups (i.e., 11.2 and 11.0 years; Table 2). The extent of thePET was similar in both groups with each having two-thirds ofthe patients with localized disease (Table 2). Although there wasa trend for patients without a meningioma to have more aggres-sive PETs with liver metastases (20 versus 0%), this differencedid not reach significance. Patients with or without meningiomadid not differ in the percentage who had previous PET resec-tions (�50%) or the time from these resections (Table 2).Pituitary adenomas occurred in 40% of all of the patients andneither their frequency, percentage of the patients requiringpituitary surgery, nor the duration of time from that surgerydiffered between the two groups (Table 2). Other non-MEN1-related cancers (prostate, renal, uterine, esophageal, bladder,
and colon) and less common MEN 1-related tumors (thyroidcancer, angiolipoma, leiomyomata, melanoma, leiomyosarco-ma; Refs. 4–7) occurred in 23% of the patients, and theirfrequency did not differ in patients with or without meningio-mas (Table 2).
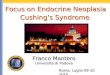
Two of the 6 meningiomas were in the frontal lobe, 3 in theplanum sphenoidale, and 1 in the posterior fossa (Table 4). Fiveof the 6 patients had an octreotide scan performed that includedwhole body images, and in 3 patients, there was uptake in thebrain area corresponding to the site of meningioma on the MRI.Examples of the somatostatin receptor scintigraphy and MRIresults in 2 patients are shown in Figs. 1 and 2. In the patientshown in Fig. 1, the meningioma in the dura of the planumsphenoidole was seen on both the MRI and somatostatin recep-tor scintigraphy studies, whereas in the patient in Fig. 2, themeningioma seen in the left frontal lobe with the MRI was notseen on the somatostatin receptor scintigraphy study. The meaninitial size of the meningiomas was 16 mm with a range of 8–30mm (Table 4). The average follow-up duration of the meningi-oma was 3.6 years with a range of 0.5–11 years. One patientwith a 30-mm meningioma underwent resection. Two of the 5meningiomas evaluated for changes in size over time showed anincrease in size with an average increase of 1.4 mm or 16.7% oftheir original length, which represented a 17.3% increase in theiroriginal length/year of follow-up (Table 4). The patient with thegreater increase in size of the meningioma was a patient with
Fig. 1 Magnetic resonance imaging (MRI)and somatostatin receptor scintigraphy (SRS)showing location of the meningioma in apatient (no. 5) with multiple endocrine neo-plasia type 1. Left panel, coronal (top) andsagittal (bottom) after contrast views of theT1-weighted MRI images. An extracerebralmass is identified originating form the duraof the planum sphenoidale. The mass com-presses the inferior aspect of the left frontallobe and projects into the interhemisphericfissure. There is homogeneous enhancementpresent. These findings are typical for menin-gioma. Right panel, coronal (top) and trans-verse (bottom) views on SRS showing en-hanced uptake of radionucleotide in themeningioma.
873Clinical Cancer Research
Research. on August 5, 2021. © 2004 American Association for Cancerclincancerres.aacrjournals.org Downloaded from

two prior pituitary surgeries and postoperative radiation. He hasalso had other MEN 1-related conditions, including hyperpara-thyroidism, ZES, and had an early age of presentation of theMEN 1. None of the other patients with meningiomas hadreceived radiation.
To compare the frequency of meningioma in patients withZES with or without MEN 1, the rate of occurrence of menin-giomas of 4 cases in 65 patients with ZES and MEN 1 wascompared with that in 185 patients with ZES without MEN 1who also had repeated brain imaging. Each of the 185 patientswith sporadic ZES (i.e., without MEN 1) were involved in aprospective protocol with yearly evaluations with biochemicaland imaging studies similar to that outlined for the MEN 1patients in “Materials and Methods.”
Meningiomas were significantly (P � 0.017) more fre-quent in the patients with ZES and MEN 1 [6.2% (4 of 65)versus 0.5% (1 of 185), respectively]. This difference occurredalthough the 185 patients without MEN 1 were older (49.8 �0.8 versus 47.7 � 1.8 years, P � 0.058) and had a longerfollow-up at the NIH (10.3 � 0.4 versus 8.0 � 0.9 years, P �0.0011). Furthermore, this difference in frequency was not dueto the difference in duration of the ZES (17.7 � 0.6 versus17.1 � 1.2 years, P � 0.49), male gender (46 versus 57%, P �0.09), or the severity of the ZES because fasting gastrin levels(median, 610 versus 1000 pg/ml, P � 0.10) were not signifi-cantly different, and in fact, the basal acid output was higher inthe sporadic cases (44.9 versus 41.6 mEq/h, P � 0.044).
Previous studies have shown a high frequency of LOH onchromosome 1p LOH (28–57%) and at 22q12 (44–100%) at the
NF2 tumor suppressor gene locus (28, 35, 39–48) in sporadicmeningiomas and in NF2-associated meningiomas (49), andtheir presence correlates with an aggressive growth pattern,tumor site, high histological grade, and decreased recurrence-free survival (40, 41, 44–46). To assess these genetic alterations(NF2 and 1p) as well as possible LOH at the MEN1 locus onchromosome 11q13 in this MEN 1-associated meningioma, eachof these regions was examined with polymorphic microsatellitemarkers (Figs. 3–5). On chromosome 11q13, LOH was identi-fied by all six polymorphic markers over the MEN1 locus (Figs.3 and 5). No LOH was found on chromosome 22q in the regionof the NF2 gene (Figs. 3 and 5). LOH was identified in six lociof 1p (Figs. 4 and 5). LOH in chromosome 1p at the D1S468locus indicated loss of p73 gene (50), the homologue of p53 (51,52). Loss of another novel putative tumor suppressor gene,ARHI/NOEY2, on 1p31 (53), was identified with three markersflanking the gene (D1S2638, D1S1665, and D1S500) and oneintragenic marker (D1S2829; Ref. 36; Figs. 4 and 5). ARHI/NOEY2 is a maternal imprinted gene (53), whereas p73 may bea paternal imprinted gene (51). By comparing the allelotypingdata of the patient’s normal DNA with her mother’s normalDNA amplified by PCR using marker D1S468, it was demon-strated that the paternal allele of p73 is lost in the tumor (i.e., theupper band disappeared in the tumor; Fig. 4). Similarly, loss ofthe paternal allele (functional allele) of ARHI/NOEY2 in thismeningioma (T1) was shown with markers D1S2638 (data notshown) and D1S1665 that flank ARHI/NOEY2 gene (Ref. 36;Fig. 4). These data demonstrated that ARHI/NOEY2 gene wascompletely inactivated in the meningioma by loss of its func-
Fig. 2 Magnetic resonance imaging (MRI) butnot somatostatin receptor scintigraphy (SRS) lo-calization of the meningioma in a patient (no. 4)with MEN 1. Left panel, axial (top) and coronal(bottom) after contrast T1-weighted MRI images.An extracerebral mass (arrow) is identified in theleft frontal region. The mass has a flat surface ofattachment to the dura and compresses the adja-cent brain parenchyma. There is homogenous en-hancement present. Right panel, transverse (top)and coronal (bottom) images on SRS showing nouptake in the region corresponding to the MRIfinding.
874 Meningiomas in MEN 1
Research. on August 5, 2021. © 2004 American Association for Cancerclincancerres.aacrjournals.org Downloaded from

tional allele, i.e., paternal allele, whereas p73 might not becompletely inactivated because it lost the imprinted paternalallele. LOH of NF2 gene, which was shown to be frequentlypresent in sporadic meningiomas (35, 39–41), was not shown inthis MEN 1-related meningioma (Figs. 3 and 5).
DiscussionLOH at the MEN1 locus on chromosome 11q13 has been
identified in many of the endocrine tumors that occur in patientswith MEN 1, including PETs, parathyroid tumors, pituitarytumors, cutaneous angiofibromas, smooth muscle leiomyomas,lipomas, and carcinoids of the lung and stomach (2, 3, 5, 7–10,
54). Also, the phenotype of MEN 1 knockout mice is similar tothe features of the human MEN 1 disorder (55), suggesting thatloss of this tumor suppressor gene plays a critical role in thepathogenesis of this disorder. However, in a subset of the tumorsmentioned above, MEN1 LOH was not identified (5, 7–10, 54).Moreover, in some tumors that occur in MEN 1 patients such asmost adrenocortical tumors, thyroid tumors, and all thymiccarcinoids, no LOH of the MEN1 gene is identified (2, 5, 11,14). These findings suggested that the molecular pathogenesis ofthese various tumors differ. In the present study, we demon-strated for the first time that a MEN 1-related meningioma hadLOH at all six loci examined on the MEN1 gene. This resultdemonstrates that the meningioma occurring in this patient is anMEN 1 tumor and that alterations in the MEN1 gene play a rolein its pathogenesis.
Although this study is the first to establish the occurrenceof meningioma as a specific MEN 1 tumor, two previous studies(20, 21) report a meningioma in a patient with MEN 1. AlthoughMEN 1 was not proven, meningiomas have been reported inpatients with hyperparathyroidism (56–59) and in patients withpituitary adenomas (57, 60–63). The association of meningio-mas with pituitary adenomas is complicated by the recognitionthat intracranial irradiation for pituitary disease or other causesis associated with occurrence of meningiomas (60, 62, 64, 65).Patients with pituitary adenomas and meningiomas without pre-vious radiation are described previously (60, 61, 63); however,in no case was the presence of MEN 1 investigated. Only 1 ofour patients with MEN 1 had previous pituitary radiation, so thissuggests pituitary irradiation is not necessary for the develop-ment of meningiomas in MEN 1 patients. However, these resultsdo not exclude the possibility that meningiomas could be morefrequent in MEN 1 patients receiving pituitary radiation. Inaddition to the above associations, a patient with a meningioma,gastric myofibroma, thyroid disease, and an ileal carcinoidtumor has been previously reported (66), as well as a patientwith multiple lipomas, thyroid disease, prolactin-secreting pitu-itary adenoma, and meningioma (63).
Other CNS tumors, including spinal ependymomas (16, 17)and schwannomas (19, 20), are occasionally reported in patientswith MEN 1 (16, 67) or MEN 1-variant syndromes (19). How-ever, in none of these tumors have studies established that theydemonstrate LOH at the MEN1 locus as was shown in thepresent study for meningiomas in MEN 1 patients. Although theexact factors are unknown that contribute to the development ofmeningiomas in MEN 1 patients and perhaps these other CNStumors, a possible contributing factor in some patients could beelevated plasma levels of either gastrin or other gastrointestinalhormones that are frequently secreted by gastrinomas and otherPETs these patients commonly develop (25, 68, 69). Gastrin hasbeen shown to cause the proliferation of meningiomas as well asother CNS tumors (70) and meningiomas and other CNS tumorsshown to possess CCK/gastrin receptors (71, 72) as well asneurotensin receptors (73), a hormone frequently released bygastrinomas as well as other PETs (68, 74). The present studyprovides some insights into this possibility. Meningiomas were11 times more frequent in patients with ZES and MEN 1 thanwith ZES alone. This difference was not because of the MEN 1patients being older, having higher serum gastrin levels, moresevere ZES, or longer follow-up. These results suggest that the
Fig. 3 Assessment of chromosome 11q13 (left panel) and 22q (rightpanel) loss of heterozygosity (LOH) in a meningioma from a patientwith multiple endocrine neoplasia type 1 (MEN 1). Shown are resultsfrom normal tissue (N; i.e., leukocytes) and from tumor (T1). The thinarrows show the retained allele, and bold arrows show LOH. In the leftpanel are shown results of assessment for 11q13 LOH (MEN1 locus)using marker D11S480, D11S1883, PYGM, and D11S449. MEN 1LOH in the meningioma is seen with all four markers. In the right panelare shown results of assessment for LOH in 22q at the neurofibromatosis2 (NF2) loci with marker D22S280 and D22S929 (intragenetic marker).No NF2 LOH is seen.
875Clinical Cancer Research
Research. on August 5, 2021. © 2004 American Association for Cancerclincancerres.aacrjournals.org Downloaded from

presence of the MEN 1 is the important contributing factor tothe increased frequency of meningiomas in MEN 1 patients.Secondly, there was no correlation in our study with the pres-ence or absence of a meningioma and the magnitude of hyper-gastrinemia. Thirdly, 2 of the 6 patients with MEN 1 withmeningiomas in the present study did not have hypergastrinemiaor any PET imaged, demonstrating meningioma can occur with-out associated ZES or another PET.
The meningiomas in patients with MEN 1 have similaritiesand differences from those reported in patients without MEN 1.They resemble sporadic meningiomas with a female predomi-nance of 2:1 in MEN 1 patients similar to the 2:1 or 3:2 ratioreported in sporadic meningiomas (22). In all patients with
MEN 1, the meningiomas were asymptomatic and detected byimaging studies, whereas 40–80% are symptomatic in patientswith sporadic meningiomas in different series (22, 75–77). Incomparison to patients with asymptomatic sporadic meningio-mas, the mean age of our patients with MEN 1 at the time ofdiagnosis of the meningioma was lower [51 versus 57–67 year(six studies; Refs. 29, 75, 77–80)]. However, the mean age inour patients at diagnosis of the meningioma was not as low asthe third or fourth decade usually seen in patients with NF2 (81).The mean size of the meningioma in our patients at initialdetection was smaller than those with asymptomatic sporadicmeningiomas [i.e., 1.6 versus 2.2 cm (29), 2.9 cm (75), 2.1 cm(78), or 2.6 cm (82)]. Although the numbers of meningiomas in
Fig. 4 Results of assessmentfor loss of heterozygosity (LOH)at 1p in a meningioma from apatient with multiple endocrineneoplasia type 1. In the left panelis shown the chromosome loca-tion of the loci identified by thedifferent markers. In the middlepanel are shown results fromnormal tissue (N; i.e., leuko-cytes) and from two different ar-eas of the meningioma (T1 andT2). The thin arrows show theretained allele, and bold arrowsshow LOH. In the right panel areshown results from the leukocyteDNA of the patient with the me-ningioma (D) and from hermother (M). The arrows in theright panel show the paternal al-lele and maternal allele in the pa-tient’s normal tissue. The middlepanel shows that the top allele islost in the meningioma at locusD1S468. Comparison with theD1S468 data in the right upperpanel from the patient’s normaltissue (D) and her mother’s nor-mal tissue (M) indicates thatthere is loss of the paternal alleleat D1S468 (i.e., p73) in the me-ningioma. In the middle panelat locus D1S2638, D1S2829(intragenetic marker), andD1S1665, the meningioma hadLOH of the ARHI/NOEY2 gene.In the T18 meningioma, the topallele and bottom allele are lost atD1S2638 and D1S1665, respec-tively. Comparison with the dataof D1S1665 from the patient andher mother’s normal tissue in theright panel indicates that there isloss of the paternal allele (func-tional allele) of ARHI/NOEY2gene in the meningioma (T18).Also the lower allele is lost in theT20 meningioma, which indi-cates loss of the maternal allele(imprinted allele) of ARHI/NOEY2 gene at this site in themeningioma (T20).
876 Meningiomas in MEN 1
Research. on August 5, 2021. © 2004 American Association for Cancerclincancerres.aacrjournals.org Downloaded from

different locations in our study were low, the 50% distributionin the sphenoid area in our study suggests a possible differentdistribution from patients with asymptomatic sporadic menin-giomas in which 10–12% are found in the sphenoidal area (29,75, 78), with 54–66% instead found in the convexity and/or falxarea (29, 75, 78). During follow-up over a mean of 3.6 years, in60% of the patients with MEN 1, the meningiomas demon-strated no growth. This compares to a similar percentage growthrate of 11–35% in six studies of patients with sporadic menin-giomas accidentally discovered followed over a mean 2.7–5years (29, 76, 76, 78, 80, 82). Similarly, the annual mean growthrate of the meningiomas in our patients was similar to thatreported in patients with sporadic meningiomas [i.e., 0.17 versus0.24–0.31 cm/year (29, 78)]. Of interest was the fact that the 1patient receiving previous pituitary radiation had the highestgrowth rate (i.e., 71% change in diameter/year). This result isconsistent with previous reports that meningiomas arise in thiscontext may be more aggressive than sporadic tumors (64, 65).None of our patients developed symptoms from the meningiomaduring follow-up, which is similar to the low rate (i.e., 0.5–3%)reported in patients with accidentally discovered sporadic men-ingiomas in four studies (29, 78–80) but different from anotherstudy where 12% became symptomatic (82). Lastly, recentstudies demonstrate 100% of sporadic meningiomas have highdensities of somatostatin receptors which bind octreotide withhigh affinity (i.e., sst2,3,5) and that radiolabeled octreotide can beused to image these tumors (83–87). Our data show that men-
ingiomas in patients with MEN 1 also frequently possess highdensities of these receptors, with 60% (3 of 5) of patients withmeningiomas who underwent somatostatin receptor scintigra-phy having a positive scan. This percentage may be lower thanthe 98–100% reported in studies of sporadic meningiomas (83–87), possibly because of the smaller size of the meningiomas inour patients. Recently, studies imaging PETs with somatostatinreceptor scintigraphy demonstrate the detection rate is propor-tional to tumor size and a similar relationship may exist formeningiomas (88). These results demonstrate that it is notsufficient to rely on somatostatin receptor scintigraphy to detectall patients with MEN 1 with meningiomas but instead an MRIof the brain should be performed at the time of evaluation forpossible pituitary adenoma.
A number of different endocrine (parathyroid, pituitary,PETs, and adrenal) and nonendocrine (cutaneous angiofibro-mas, smooth muscle leiomyomas, thymic and gastric carcinoids,and lipomas) tumors (4, 5, 7, 8, 54) can develop in patients withMEN 1, and the current study provides some insights into thefrequency and temporal relationship between some of thesetumors and meningiomas in these patients. Meningiomas werefound in 8% of the MEN 1 patients studied, which was signif-icantly less frequent than the frequency in the same patients ofparathyroid hyperplasia (98%), PETs (96%), or pituitary adeno-mas (40%). This frequency, however, was similar to that forsmooth muscle tumors (4%) in these patients and is approxi-mately equal to that reported for bronchial or thymic carcinoids(0–8%) in MEN 1 patients (2, 14, 15), less frequent than gastriccarcinoids (15–35%; Ref. 15), adrenocortical tumors (16–40%;Refs. 2, 12), lipomas (20–34%; Refs. 2, 3), or cutaneous angio-fibromas (88%; Ref. 2). The higher frequency of occurrence ofmeningiomas in females with MEN 1 (2:1) is similar to pituitaryadenomas and bronchial carcinoids in MEN 1 patients, whichare also more frequent in females (3) but differs from thymiccarcinoids that occur almost exclusively in men (14), and hy-perparathyroidism or PETs, which occur with equal frequencyin MEN 1 patients of both sexes (3). In general, the developmentof a meningioma was a late feature of MEN 1, occurring 10–15years later than the development of hyperparathyroidism, PETs,or pituitary disease. Its peak time of diagnosis at age 50 years issimilar to the late time course for the development of gastriccarcinoids and thymic carcinoid tumors in MEN 1 patients (14,89). Similar to that recently reported with the development ofthymic carcinoids (14), no clinical parameter, laboratory value,or other MEN 1 feature distinguished patients who did or did notdevelop a meningioma. Therefore, because it cannot be pre-dicted which patient with MEN 1 will develop a meningioma, itwill be necessary to perform routine brain MRIs to detect them.Because the youngest age any patient was first diagnosed witha meningioma in our study was 29 years old, we would recom-mend an initial brain MRI be performed by age 25 years. Atpresent, we have insufficient data to propose when brain MRIsshould be repeated if initially negative.
Previous studies in sporadic meningiomas show a highfrequency (44–100%) of LOH on chromosome 22q12 at NF2gene locus (35, 39–44), and patients with NF2 develop meni-giomas that have a high frequency of NF2 gene LOH (49). Ourresults from allelotyping of 22q12 in the MEN 1-associatedmeningioma show that there is no LOH on chromosome 22q12
Fig. 5 Summary of loss of heterozygosity (LOH) assessment in chro-mosome 1p, 11q13, and 22q in a meningioma from a patient with MEN1. Shown are the microsatellite markers as well as their chromosomelocation and their distance in centimorgans (cM). The results for thetumor with each marker are shown. Results at each locus assessed areexpressed as LOH and retention of heterozygosity (R), determined asdescribed in “Materials and Methods.” cM data are from Marshfieldchromosome sex-average linkage map.6
877Clinical Cancer Research
Research. on August 5, 2021. © 2004 American Association for Cancerclincancerres.aacrjournals.org Downloaded from

in the region of the NF2 gene. This data suggested that LOH ofNF2 gene may not be involved in the tumorigenesis of MEN1-associated meningioma.
Chromosome 1p LOH is the second most common chro-mosomal abnormality (28–57%) reported in sporadic meningi-omas (39, 44–46, 46–48). The present study demonstrated that1p LOH occurred at 6 of 12 loci on chromosome 1p examinedin the MEN 1-related meningioma. Two tumor suppressor genes(p73 and ARHI/NOEY2) have been localized on 1p36 and 1p31,respectively (50, 53), and in our study, at each locus in the MEN1-associated meningioma, LOH was found. ARHI/NOEY2 is amaternal imprinted tumor suppressor gene (53), and our datademonstrates that the paternal (functional) allele of ARHI/NOEY2 gene was lost in the MEN 1-associated meningioma.This means that ARHI/NOEY2 gene is completely inactivatedin this meningioma, suggesting that loss of this tumor suppres-sor gene could be contributing to the tumorigenesis of themeningioma in MEN 1 patients. However, with the paternalimprinted gene p73 (51, 90), which is a homologue of p53 (51,52, 91), loss of the paternal allele was found, indicating that thep73 gene might not be involved in the pathogenesis of menin-gioma in MEN 1 patients.
AcknowledgmentsWe thank Dr. Stephen J. Marx, Metabolic Diseases Branch, Na-
tional Institutes of Diabetes, Digestive and Kidney Diseases, NIH, forhelping to provide tissues from one patient who underwent surgicalresection of the meningioma and normal DNA from leukocytes from thepatient’s mother.
References1. Thakker, R. V. Multiple endocrine neoplasia type 1. Endocrinol.Metab. Clin. N. Am., 29: 541–567, 2000.2. Marx, S., Spiegel, A. M., Skarulis, M. C., Doppman, J. L., Collins,F. S., and Liotta, L. A. Multiple endocrine neoplasia type 1: clinical andgenetic topics. Ann. Intern. Med., 129: 484–494, 1998.3. Metz, D. C., Jensen, R. T., Bale, A. E., Skarulis, M. C., Eastman,R. C., Nieman, L., Norton, J. A., Friedman, E., Larrson, C., Amorosi,A., Brandi, M. L., and Marx, S. J. Multiple endocrine neoplasia type 1:clinical features and management. In: J. P. Bilezekian, M. A. Levine,and R. Marcus (eds.), The Parathyroids, pp. 591–646. New York: RavenPress Publishing Co., 1994.4. Eberle, F., and Grun, R. Multiple endocrine neoplasia, type I (MENI). Ergeb. Inn. Med. Kinderheilkd, 46: 76–149, 1981.5. Vortmeyer, A. O., Lubensky, I. A., Skarulis, M., Li, G., Moon,Y. W., Park, W. S., Weil, R., Barlow, C., Spiegel, A. M., Marx, S. J.,and Zhuang, Z. Multiple endocrine neoplasia type 1: atypical presenta-tion, clinical course, and genetic analysis of multiple tumors. Mod.Pathol., 12: 919–924, 1999.6. Nord, B., Platz, A., Smoczynski, K., Kytola, S., Robertson, G.,Calender, A., Murat, A., Weintraub, D., Burgess, J., Edwards, M.,Skogseid, B., Owen, D., Lassam, N., Hogg, D., Larsson, C., and Teh,B. T. Malignant melanoma in patients with multiple endocrine neoplasiatype 1 and involvement of the MEN1 gene in sporadic melanoma. Int. J.Cancer, 87: 463–467, 2000.7. Dong, Q., Debelenko, L. V., Chandrasekharappa, S., Lotterman, C.,Skarulis, M., Emmert-Buck, M. R., Zhuang, Z., Guru, S. C., Manickam,P., Lubensky, I. A., Liotta, L. A., Collins, F. S., Marx, S. J., and Spiegel,A. M. Loss of heterozygosity at 11q13: analysis of pituitary tumors,lung carcinoids, lipomas, and other uncommon tumors in subjects withfamilial multiple endocrine neoplasia type 1. J. Clin. Endocrinol.Metab., 82: 1416–1420, 1997.
8. Debelenko, L. V., Zhuang, Z. P., Emmert-Buck, M. R., Chan-drasekharappa, S., Manickam, P., Guru, S. C., Marx, S. J., Skarulis, M.,Spiegel, A. M., Collins, F. S., Jensen, R. T., Liotta, L. A., and Lubensky,I. A. Allelic deletions on chromosome 11q13 in multiple endocrineneoplasia type-I-associated sporadic gastrinomas and pancreatic endo-crine tumors. Cancer Res., 57: 2238–2243, 1997.
9. Pack, S., Turner, M. L., Zhuang, Z., Vortmeyer, A. O., Boni, R.,Skarulis, M., Marx, S. J., and Darling, T. N. Cutaneous tumors inpatients with multiple endocrine neoplasia type 1 show allelic deletionof the MEN1 gene. J. Investig. Dermatol., 110: 438–440, 1998.
10. Debelenko, L. V., Emmert-Buck, M. R., Zhuang, Z., Epshteyn, E.,Moskaluk, C. A., Jensen, R. T., Liotta, L. A., and Lubensky, I. A. Themultiple endocrine neoplasia type 1 gene locus is involved in thepathogenesis of type II gastric carcinoids. Gastroenterology, 113: 773–782, 1997.
11. Skogseid, B., Larsson, C., Lindgren, P. G., Kvanta, E., Rastad, J.,Theodorsson, E., Wide, L., Wilander, E., and Oberg, K. Clinical andgenetic features of adrenocortical lesions in multiple endocrine neopla-sia type 1. J Clin. Endocrinol. Metab., 75: 76–81, 1992.
12. Komminoth, P., Heitz, P. U., and Kloppel, G. Pathology of MEN-1:morphology, clinicopathologic correlations, and tumour development.J. Intern. Med., 243: 455–464, 1998.
13. Solcia, E., Capella, C., Fiocca, R., Rindi, G., and Rosai, J. Gastricargyrophil carcinoidosis in patients with Zollinger-Ellison syndromedue to type 1 multiple endocrine neoplasia. A newly recognized asso-ciation. Am. J. Surg. Pathol., 14: 503–513, 1990.
14. Gibril, F., Chen, Y-J., Schrump, D. S., Vortmeyer, A., Zhuang,Z. P., Lubensky, I. A., Reynolds, J. G., Louie, J. V., Entsuah, L., Huang,K., Asgharian, B., and Jensen, R. T. Prospective study of thymiccarcinoids in patients with multiple endocrine neoplasia type 1. J. Clin.Endocrinol. Metab., 88: 1066–1081, 2003.
15. Jensen, R. T. MEN-1 carcinoids: diagnosis and therapy. In: SeventhInternational Workshop on Multiple Neoplasia, pp. 67–72. Gubbio,Italy: 1999.
16. Kato, H., Uchimura, I., Morohoshi, M., Fujisawa, K., Kobayashi,Y., Numano, F., Goseki, N., Endo, M., Tamura, A., and Nagashima, C.Multiple endocrine neoplasia type 1 associated with spinal ependy-moma. Intern. Med., 35: 285–289, 1996.
17. Giraud, S., Choplin, H., Teh, B. T., Lespinasse, J., Jouvet, A.,Labat-Moleur, F., Lenoir, G., Hamon, B., Hamon, P., and Calender, A.A large multiple endocrine neoplasia type 1 family with clinical expres-sion suggestive of anticipation. J. Clin. Endocrinol. Metab., 82: 3487–3492, 1997.
18. Croisier, J. C., Azerad, E., and Lubetzki, J. Polyendocrine adeno-matosis (Wermer’s syndrome) apropos of a personal case. Review of theliterature (in French). Sem. Hop., 47: 494–525, 1971.
19. Doumith, R., de Gennes, J. L., Cabane, J. P., and Zygelman, N.Pituitary prolactinoma, adrenal aldosterone-producing adenomas, gas-tric schwannoma and colonic polyadenomas: a possible variant of mul-tiple endocrine neoplasia (MEN) type I. Acta Endocrinol., 100: 189–195, 1982.20. Chigot, J. P., Bendib, S., Turpin, G., and Benlian, P. Characteristicpathological associations in multiple endocrine neoplasia type 1 (inFrench). Presse. Med., 25: 1229–1233, 1996.21. Banik, S., Hasleton, P. S., and Lyon, R. L. An unusual variant ofmultiple endocrine neoplasia syndrome: a case report. Histopathology,8: 135–144, 1984.22. DeAngelis, L. M. Brain tumors. N. Engl. J. Med., 344: 114–123,2001.23. Benya, R. V., Metz, D. C., Venzon, D. J., Fishbeyn, V. A., Strader,D. B., Orbuch, M., and Jensen, R. T. Zollinger-Ellison syndrome can bethe initial endocrine manifestation in patients with multiple endocrineneoplasia-type 1. Am. J. Med., 97: 436–444, 1994.24. Gibril, F., Venzon, D. J., Ojeaburu, J. V., Bashir, S., and Jensen,R. T. Prospective study of the natural history of gastrinoma in patientswith MEN1: definition of an aggressive and a nonaggressive form.J. Clin. Endocrinol. Metab., 86: 5282–5293, 2001.
878 Meningiomas in MEN 1
Research. on August 5, 2021. © 2004 American Association for Cancerclincancerres.aacrjournals.org Downloaded from

25. Roy, P., Venzon, D. J., Shojamanesh, H., Abou-Saif, A., Peghini,P., Doppman, J. L., Gibril, F., and Jensen, R. T. Zollinger-Ellisonsyndrome: clinical presentation in 261 patients. Medicine (Baltim.), 79:379–411, 2000.
26. Fishbeyn, V. A., Norton, J. A., Benya, R. V., Pisegna, J. R.,Venzon, D. J., Metz, D. C., and Jensen, R. T. Assessment and predictionof long-term cure in patients with Zollinger-Ellison syndrome: the bestapproach. Ann. Intern. Med., 119: 199–206, 1993.
27. Gibril, F., Reynolds, J. C., Doppman, J. L., Chen, C. C., Venzon,D. J., Termanini, B., Weber, H. C., Stewart, C. A., and Jensen, R. T.Somatostatin receptor scintigraphy: its sensitivity compared with that ofother imaging methods in detecting primary and metastatic gastrinomas:a prospective study. Ann. Intern. Med., 125: 26–34, 1996.28. Norton, J. A., Alexander, H. R., Fraker, D. L., Venzon, D. J., Gibril,F., and Jensen, R. T. Comparison of surgical results in patients withadvanced and limited disease with multiple endocrine neoplasia type 1and Zollinger-Ellison syndrome. Ann. Surg., 234: 495–506, 2001.29. Olivero, W. C., Lister, J. R., and Elwood, P. W. The natural historyand growth rate of asymptomatic meningiomas: a review of 60 patients.J. Neurosurg., 83: 222–224, 1995.30. Ginsberg, L. E. Radiology of meningiomas. J. Neurooncol., 29:229–238, 1996.31. Sutliff, V. E., Doppman, J. L., Gibril, F., Yu, F., Serrano, J.,Venzon, D. J., and Jensen, R. T. Growth of newly diagnosed, untreatedmetastatic gastrinomas and predictors of growth patterns. J. Clin. On-col., 15: 2420–2431, 1997.32. Yu, F., Venzon, D. J., Serrano, J., Goebel, S. U., Doppman, J. L.,Gibril, F., and Jensen, R. T. Prospective study of the clinical course,prognostic factors and survival in patients with longstanding Zollinger-Ellison syndrome. J. Clin. Oncol., 17: 615–630, 1999.33. Gadelha, M. R., Une, K. N., Rohde, K., Vaisman, M., Kineman,R. D., and Frohman, L. A. Isolated familial somatotropinomas: estab-lishment of linkage to chromosome 11q13.1-11q13.3 and evidence for apotential second locus at chromosome 2p16-12. J. Clin. Endocrinol.Metab., 85: 707–714, 2000.34. Heppner, C., Kester, M. B., Agarwal, S. K., Debelenko, L. V.,Emmert-Buck, M. R., Guru, S. C., Manickam, P., Olufemi, S. E.,Skarulis, M. C., Doppman, J. L., Alexander, R. H., Kim, Y. S., Saggar,S. K., Lubensky, I. A., Zhuang, Z., Liotta, L. A., Chandrasekharappa,S. C., Collins, F. S., Spiegel, A. M., Burns, A. L., and Marx, S. J.Somatic mutation of the MEN1 gene in parathyroid tumours. Nat.Genet., 16: 375–378, 1997.35. Ueki, K., Wen-Bin, C., Narita, Y., Asai, A., and Kirino, T. Tightassociation of loss of merlin expression with loss of heterozygosity atchromosome 22q in sporadic meningiomas. Cancer Res., 59: 5995–5998, 1999.36. Peng, H., Xu, F., Pershad, R., Hunt, K. K., Frazier, M. L., Berchuck,A., Hogg, D., Bast, R. C., Jr., Gray, J. W., and Yu, Y. ARHI is the centerof allelic deletion on chromosome 1p31 in ovarian and breast cancers.Int. J. Cancer, 86: 690–694, 2000.37. Kitamura, Y., Shimizu, K., Tanaka, S., Ito, K., and Emi, M. Asso-ciation of allelic loss on 1q, 4p, 7q, 9p, 9q, and 16q with postoperativedeath in papillary thyroid carcinoma. Clin. Cancer Res., 6: 1819–1825,2000.38. Kitamura, Y., Shimizu, K., Tanaka, S., Ito, K., and Emi, M. Al-lelotyping of anaplastic thyroid carcinoma: frequent allelic losses on 1q,9p, 11, 17, 19p, and 22q. Genes Chromosomes Cancer, 27: 244–251,2000.39. Leone, P. E., Bello, M. J., deCampos, J. M., Vaquero, J., Sarasa,J. L., Pestana, A., and Rey, J. A. NF2 gene mutations and allelic statusof 1p, 14q and 22q in sporadic meningiomas. Oncogene, 18: 2231–2239, 1999.40. Leuraud, P., Marie, Y., Robin, E., Huguet, S., He, J., Mokhtari, K.,Cornu, P., Hoang-Xuan, K., and Sanson, M. Frequent loss of 1p32region but no mutation of the p18 tumor suppressor gene in meningio-mas. J. Neuro-Oncol., 50: 207–213, 2000.41. Kros, J., deGreve, K., van Tilborg, A., Hop, W., Pieterman, H.,Avezaat, C., ditDeprez, R. L., and Zwarthoff, E. NF2 status of menin-
giomas is associated with tumour localization and histology. J. Pathol.,194: 367–372, 2001.
42. Ruttledge, M. H., Sarrazin, J., Rangaratnam, S., Phelan, C. M.,Twist, E., Merel, P., Delattre, O., Thomas, G., Nordenskjold, M., andCollins, V. P. Evidence for the complete inactivation of the NF2 gene inthe majority of sporadic meningiomas. Nat. Genet., 6: 180–184, 1994.43. Papi, L., DeVitis, L. R., Vitelli, F., Ammannati, F., Mennonna, P.,Montali, E., and Bigozzi, U. Somatic mutations in the neurofibromatosistype 2 gene in sporadic meningiomas. Hum. Genet., 95: 347–351, 1995.44. Lamszus, K., Kluwe, L., Matschke, J., Meissner, H., Laas, R., andWestphal, M. Allelic losses at 1p, 9q, 10q, 14q, and 22q in the progres-sion of aggressive meningiomas and undifferentiated meningeal sarco-mas. Cancer Genet. Cytogenet., 110: 103–110, 1999.45. Muller, P., Henn, W., Niedermayer, I., Ketter, R., Feiden, W.,Steudel, W. I., Zang, K. D., and Steilen-Gimbel, H. Deletion of chro-mosome 1p and loss of expression of alkaline phosphatase indicateprogression of meningiomas. Clin. Cancer Res., 5: 3569–3577, 1999.46. Sulman, E. P., Dumanski, J. P., White, P. S., Zhao, H., Maris, J. M.,Mathiesen, T., Bruder, C., Cnaan, A., and Brodeur, G. M. Identificationof a consistent region of allelic loss of 1p32 in meningiomas: correlationwith increased morbidity. Cancer Res., 58: 3226–3230, 1998.47. Alonso, M. E., Bello, M. J., Gonzalez-Gomez, P., Lomas, J., Ar-jona, D., deCampos, J. M., Kusak, M. E., Sarasa, J. L., Isla, A., and Rey,J. A. Mutation analysis of the p73 gene in nonastrocytic brain tumours.Br. J. Cancer, 85: 204–208, 2001.48. Bello, M. J., deCampos, J. M., Vaquero, J., Kusak, M. E., Sarasa,J. L., and Rey, J. A. High-resolution analysis of chromosome arm 1palterations in meningioma. Cancer Genet. Cytogenet., 120: 30–36,2000.49. Lamszus, K., Vahldiek, F., Mautner, V. F., Schichor, C., Tonn, J.,Stavrou, D., Fillbrandt, R., Westphal, M., and Kluwe, L. Allelic lossesin neurofibromatosis 2-associated meningiomas. J. Neuropathol. Exp.Neurol., 59: 504–512, 2000.50. Perri, P., Praml, C., Savelyeva, L., Pillmann, A., and Schwab, M.Fine mapping of distal 1p loci reveals TP73 at D1S468. Cytogenet. CellGenet., 84: 111–114, 1999.51. Kaghad, M., Bonnet, H., Yang, A., Creancier, L., Biscan, J. C.,Valent, A., Minty, A., Chalon, P., Lelias, J. M., Dumont, X., Ferrara, P.,McKeon, F., and Caput, D. Monoallelically expressed gene related top53 at 1p36, a region frequently deleted in neuroblastoma and otherhuman cancers. Cell, 90: 809–819, 1997.52. Jost, C. A., Marin, M. C., and Kaelin, W. G., Jr. p73 is a humanp53-related protein that can induce apoptosis. Nature (Lond.), 389:191–194, 1997.53. Yu, Y., Xu, F., Peng, H., Fang, X., Zhao, S., Li, Y., Cuevas, B.,Kuo, W. L., Gray, J. W., Siciliano, M., Mills, G. B., and Bast, R. C., Jr.NOEY2 (ARHI), an imprinted putative tumor suppressor gene in ovar-ian and breast carcinomas. Proc. Natl. Acad. Sci. USA, 96: 214–219,1999.54. Hessman, O., Skogseid, B., Westin, G., and Akerstrom, G. Multipleallelic deletions and intratumoral genetic heterogeneity in MEN1 pan-creatic tumors. J. Clin. Endocrinol. Metab., 86: 1355–1361, 2001.55. Crabtree, J. S., Scacheri, P. C., Ward, J. M., Garrett-Beal, L.,Emmert-Buck, M. R., Edgemon, K. A., Lorang, D., Libutti, S. K.,Chandrasekharappa, S. C., Marx, S. J., Spiegel, A. M., and Collins, F. S.A mouse model of multiple endocrine neoplasia, type 1, developsmultiple endocrine tumors. Proc. Natl. Acad. Sci. USA, 98: 1118–1123,2001.56. Grinblat, J., Seidenstein, B., Lerman, P., and Lewitus, Z. Meningi-oma associated with parathyroid adenoma. Am. J. Med. Sci., 272:327–330, 1976.57. Hemminki, K., and Jiang, Y. Second primary neoplasms after19281 endocrine gland tumours: aetiological links? Eur. J. Cancer, 37:1886–1894, 2001.58. Yamakita, N., Ikeda, T., Shimizu, Y., Hirata, T., Kawamura, S.,Komaki, T., and Kitada, M. Undefined complications of parathyroidadenoma, parathyroid hyperplasia (primary hyperparathyroidism), thy-roid follicular adenoma, thyroid papillary carcinoma, temporal astrocy-
879Clinical Cancer Research
Research. on August 5, 2021. © 2004 American Association for Cancerclincancerres.aacrjournals.org Downloaded from

toma, cerebellar meningioma, and hemangioma of external auditorymeatus and oral papilloma. Intern. Med., 39: 814–819, 2000.59. Bingham, W. F. Meningioma and primary hyperparathyroidism.Conn. Med., 47: 321–323, 1983.60. Honegger, J., Buchfelder, M., Schrell, U., Adams, E. F., and Fahl-busch, R. The coexistence of pituitary adenomas and meningiomas:three case reports and a review of the literature. Br. J. Neurosurg., 3:59–69, 1989.61. Zentner, J., and Gilsbach, J. Pituitary adenoma and meningioma inthe same patient. Eur. Arch. Psychiatr. Neurol. Sci., 238: 144–148,1989.62. Cannavo, S., Curto, L., Fazio, R., Paterniti, S., Blandino, A., Ma-rafioti, T., and Trimarchi, F. Coexistence of growth hormone-secretingpituitary adenoma and intracranial meningioma: a case report and re-view of the literature. J. Endocrinol. Investig., 16: 703–708, 1993.63. Abs, R., Parizel, P. M., Willems, P. J., Van DeKelft, E., Verlooy, J.,Mahler, C., Verhelst, J., VanMarck, E., and Martin, J. J. The associationof meningioma and pituitary adenoma: report of seven cases and reviewof the literature. Eur. Neurol., 33: 416–422, 1993.64. Waga, S., and Handa, H. Radiation-induced meningioma: withreview of literature. Surg. Neurol., 5: 215–219, 1976.65. Rubinstein, A. B., Shalit, M. N., Cohen, M. L., Zandbank, U., andReichenthal, E. Radiation-induced cerebral meningioma: a recognizableentity. J. Neurosurg., 61: 966–971, 1984.66. Bankl, H., Grunert, V., and Sunder-Plassmann, M. Endokrinepolyadenomatose kombiniert mit einem tentoriummeningiom. Wein.Klin. Wochenschr., 82: 257–259, 1970.67. Aach, R., and Kissane, J. E. Multiple endocrine adenomatosis(Clinicopathologic Conference). Am. J. Med., 47: 608–618, 1969.68. Chiang, H. C., O’Dorisio, T. M., Huang, S. C., Maton, P. N.,Gardner, J. D., and Jensen, R. T. Multiple hormone elevations inpatients with Zollinger-Ellison syndrome: prospective study of clinicalsignificance and of the development of a second symptomatic pancreaticendocrine tumor syndrome. Gastroenterology, 99: 1565–1575, 1990.69. Jensen, R. T., and Gardner, J. D. Gastrinoma. In: V. L. W. Go, E. P.DiMagno, J. D. Gardner, E. Lebenthal, H. A. Reber, and G. A. Scheele(eds.), The Pancreas: Biology, Pathobiology, and Disease, pp. 931–978.New York: Raven Press Publishing Co., 1993.70. Camby, I., Nagy, N., Rombaut, K., Gras, T., Duponchelle, C.,Pasteels, J. L., Brotchi, J., Kiss, R., and Salmon, I. Influence of epider-mal growth factor and gastrin on the cell proliferation of human men-ingiomas versus astrocytic tumors maintained as ex vivo tissue cultures.Neuropeptides, 31: 217–225, 1997.71. Reubi, J. C., Schaer, J. C., and Waser, B. Cholecystokinin (CCK)-Aand CCK-B/gastrin receptors in human tumors. Cancer Res., 57: 1377–1386, 1997.72. Mailleux, P., and Vanderhaeghen, J. J. Cholecystokinin receptors ofA type in the human dorsal medulla oblongata and meningiomas, and ofB type in small cell lung carcinomas. Neurosci. Lett., 117: 243–247,1990.73. Przedborski, S., Levivier, M., and Cadet, J. L. Neurotensin recep-tors in human meningiomas. Ann. Neurol., 30: 650–654, 1991.74. Blackburn, A. M., Bryant, M. G., Adrian, T. E., and Bloom, S. R.Pancreatic tumours produce neurotensin. J. Clin. Endocrinol. Metab.,52: 820–822, 1981.75. Kamiguchi, H., Shiobara, R., and Toya, S. Accidentally detectedbrain tumors: clinical analysis of a series of 110 patients. Clin. Neurol.Neurosurg., 98: 171–175, 1996.76. Kuratsu, J., Kochi, M., and Ushio, Y. Incidence and clinical featuresof asymptomatic meningiomas. J. Neurosurg., 92: 766–770, 2000.
77. Nishizaki, T., Ozaki, S., Kwak, T., and Ito, H. Clinical features andsurgical outcome in patients with asymptomatic meningiomas. Br. J.Neurosurg., 13: 52–55, 1999.
78. Go, R. S., Taylor, B. V., and Kimmel, D. W. The natural history ofasymptomatic meningiomas in Olmsted County, Minnesota. Neurology,51: 1718–1720, 1998.
79. Firsching, R. P., Fischer, A., Peters, R., Thun, F., and Klug, N.Growth rate of incidental meningiomas. J. Neurosurg., 73: 545–547,1990.
80. Yoneoka, Y., Fujii, Y., and Tanaka, R. Growth of incidental men-ingiomas. Acta Neurochir. (Wien), 142: 507–511, 2000.
81. Antinheimo, J., Haapasalo, H., Haltia, M., Tatagiba, M., Thomas,S., Brandis, A., Sainio, M., Carpen, O., Samii, M., and Jaaskelainen, J.Proliferation potential and histological features in neurofibromatosis2-associated and sporadic meningiomas. J. Neurosurg., 87: 610–614,1997.
82. Niiro, M., Yatsushiro, K., Nakamura, K., Kawahara, Y., and Ku-ratsu, J. Natural history of elderly patients with asymptomatic menin-giomas. J. Neurol. Neurosurg. Psychiatry, 68: 25–28, 2000.
83. Jensen, R. T. Peptide therapy. Recent advances in the use ofsomatostatin and other peptide receptor agonists and antagonists. In:J. H. Lewis and A. Dubois (eds.), Current Clinical Topics in Gastroin-testinal Pharmacology, pp. 144–223. Malden, MA: Blackwell Science,Inc., 1997.
84. Krenning, E. P., Kwekkeboom, D. J., Bakker, W. H., Breeman,W. A. P., Kooij, P. P. M., Oei, H. Y., van Hagen, M., Postema, P. T. E.,de Jong, M., Reubi, J. C., Visser, T. J., Reijs, A. E. M., Hofland, L. J.,Koper, J. W., and Lamberts, S. W. J. Somatostatin receptor scintigraphywith [111In-DTPA-D-Phe1]- and [123I-Tyr3]-octreotide: the Rotterdamexperience with more than 1000 patients. Eur. J. Nucl. Med., 20:716–731, 1993.
85. Maini, C. L., Sciuto, R., Tofani, A., Ferraironi, A., Carapella, C. M.,Occhipinti, E., Mottolese, M., and Crecco, M. Somatostatin receptorimaging in CNS tumours using 111In-octreotide. Nucl. Med. Commun.,16: 756–766, 1995.86. Hildebrandt, G., Scheidhauer, K., Luyken, C., Schicha, H., Klug,N., Dahms, P., and Frisch, B. High sensitivity of the in vivo detection ofsomatostatin receptors by 111indium (DTPA-ocretotide)-scintigraphy inmeningioma patients. Acta Neurochir. (Wien), 126: 63–71, 1994.87. Haldemann, A. R., Rosler, H., Barth, A., Waser, B., Geiger, L.,Godoy, N., Markwalder, R. V., Seiler, R. W., Sulzer, M., and Reubi,J. C. Somatostatin receptor scintigraphy in central nervous systemtumors: role of blood-brain barrier permeability. J. Nucl. Med., 36:40–410, 1995.88. Alexander, H. R., Fraker, D. L., Norton, J. A., Barlett, D. L., Tio, L.,Benjamin, S. B., Doppman, J. L., Goebel, S. U., Serrano, J., Gibril, F.,and Jensen, R. T. Prospective study of somatostatin receptor scintigra-phy and its effect on operative outcome in patients with Zollinger-Ellison syndrome. Ann. Surg., 228: 228–238, 1998.89. Rindi, G., Bordi, C., Rappel, S., La Rosa, S., Stolte, M., and Solcia,E. Gastric carcinoids and neuroendocrine carcinomas: pathogenesis,pathology, and behavior. World J. Surg., 20: 168–172, 1996.90. Mai, M., Qian, C., Yokomizo, A., Tindall, D. J., Bostwick, D.,Polychronakos, C., Smith, D. I., and Liu, W. Loss of imprinting andallele switching of p73 in renal cell carcinoma. Oncogene, 17: 1739–1741, 1998.91. Irwin, M., Marin, M. C., Phillips, A. C., Seelan, R. S., Smith, D. I.,Liu, W., Flores, E. R., Tsai, K. Y., Jacks, T., Vousden, K. H., andKaelin, W. G., Jr. Role for the p53 homologue p73 in E2F-1-inducedapoptosis. Nature (Lond.), 407: 645–648, 2000.
880 Meningiomas in MEN 1
Research. on August 5, 2021. © 2004 American Association for Cancerclincancerres.aacrjournals.org Downloaded from

2004;10:869-880. Clin Cancer Res Behnam Asgharian, Yuan-Jia Chen, Nicholas J. Patronas, et al. Endocrine Neoplasia Type 1Meningiomas May Be a Component Tumor of Multiple
Updated version
http://clincancerres.aacrjournals.org/content/10/3/869
Access the most recent version of this article at:
Cited articles
http://clincancerres.aacrjournals.org/content/10/3/869.full#ref-list-1
This article cites 84 articles, 12 of which you can access for free at:
Citing articles
http://clincancerres.aacrjournals.org/content/10/3/869.full#related-urls
This article has been cited by 3 HighWire-hosted articles. Access the articles at:
E-mail alerts related to this article or journal.Sign up to receive free email-alerts
SubscriptionsReprints and
To order reprints of this article or to subscribe to the journal, contact the AACR Publications
Permissions
Rightslink site. (CCC)Click on "Request Permissions" which will take you to the Copyright Clearance Center's
.http://clincancerres.aacrjournals.org/content/10/3/869To request permission to re-use all or part of this article, use this link
Research. on August 5, 2021. © 2004 American Association for Cancerclincancerres.aacrjournals.org Downloaded from




![Neoplasie Endocrine Multiple: Linee Guida - Aimen · Introduzione In generale si definisce Neoplasia Endocrina Multipla [Multiple Endocrine Neoplasia (MEN)], una sindrome tumorale](https://img.pdfslide.net/doc/110x75/5ac1f4477f8b9aca388daa37/neoplasie-endocrine-multiple-linee-guida-aimen-in-generale-si-definisce-neoplasia.jpg)























