Embed Size (px)
DESCRIPTION
meningitis
Citation preview

MENINGITISMENINGITIS
Dr. Takdir Setiawan Sp.SDr. Takdir Setiawan Sp.S

Meningitis
• Definition– Bacterial meningitis is an inflammatory response to
bacterial infection of the pia-arachnoid and CSF of the subarachnoid space
• Epidemiology– Incidence is between 3-5 per 100,000– More than 2,000 deaths annually in the U.S.– Relative frequency of bacterial species varies with
age.

• Bacterial• Viral ( aseptic)• TB• Fungal • Chemical• Parasitic• ? Carcinomatous

Meningitis
• Epidemiology– Neonates (< 1 Month)
• Gm (-) bacilli 50-60%• Grp B Strep 20-40%• Listeria sp. 2-10%• H. influenza 0-3%• S. pneumo 0-5%

Meningitis
• Epidemiology– Children (1 month to 15 years)
• H. influenzae 40-60%– Declining dramatically in many geographic
regions• N. meningitidis 25-40%• S. pneumo 10-20%

Meningitis
• Epidemiology– Adults (> 15 years)
• S. pneumo 30-50%• N. Meningitidis 10-35%
– Major cause in epidemics
• Gm (-) Bacilli 1-10%– Elderly
• S. aureus 5-15%• H. influenzae 1-3%
– >60 include Listeria, E. coli, Pseudomonas

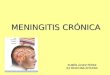
Bakteri Pada Meningitis BayiBakteri Pada Meningitis Bayi
Streptococcus agalactiae E. coli Staphylococcus Sp.
Listeria monocytogenes Pseudomonas aeruginosa Citrobacter

Bakteri pada meningitis dewasaBakteri pada meningitis dewasa
Streptococcus Pneumonia
Neisseria meningitides
Haemophilus influenzae

Meningitis
• Pathogenesis– Majority of cases are hematogenous in
origin– Organisms have virulence factors that
allow bypassing of normal defenses• Proteases• Polysaccharidases

Meningitis
• Pathology and Pathogenesis– Sequential steps allow the pathogen into the CSF
• Nasopharyngeal colonization• Nasopharyngeal epithelial cell invasion• Bloodstream invasion• Bacteremia with intravascular survival• Crossing of the BBB and entry into the CSF• Survival and replication in the subarachnoid space



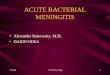
The The wall of the venulewall of the venule
L - lumen, E - endothelium, M - smooth muscle cell, C - collagen fibres in the perivascular space of Virchow-Robin.

Meningitis
• Pathology– Hallmark
• Exudate in the subarachnoid space• Accumulation of exudate in the dependent areas of the
brain• Large numbers of PMN’s • Within 2-3 days inflammation in the walls of the small
and medium-sized blood vessels• Blockage of normal CSF pathways and blockage of the
normal absorption may lead to obstructive hydrocephalus

Meningitis
• Clinical Manifestations– Headache– Fever– Meningismus– Cerebral dysfunction
• Confusion, delirium, decreased level of consciousness
– N/V– Photophobia

Meningitis• Clinical Manifestations – Nuchal rigidity
– Kernig’s• Pt supine with flexed knee has increased pain with passive
extension of the same leg– Brudzinski’s
• Supine pt with neck flexed will raise knees to take pressure off of the meninges
• Present in 50% of acute bacterial meningitis cases– Cranial Nerve Palsies
• IV, VI, VII– Seizures




KELUMPUHAN SARAF OTAK PADA MENINGITIS


LumbalLumbalPungsiPungsi


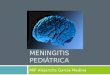
Tuberculosis of the brain with cerebritis and tuberculoma formation. MRI scans of a patient are shown including post-contrast T1WI (A) and T2WI (B)

Empiric Therapy of CNS Infections

Acute Bacterial Meningitis (ABM) (cont’d)

Pengobatan TBC pada orang dewasaPengobatan TBC pada orang dewasa
Kategori 1 : 2HRZE/4H3R3Selama 2 bulan minum obat INH, rifampisin, pirazinamid, dan etambutol setiap hari (tahap intensif), dan 4 bulan selanjutnya minum obat INH dan rifampisin tiga kali dalam seminggu (tahap lanjutan).Diberikan kepada:
Penderita baru TBC paru BTA positif.Penderita TBC ekstra paru (TBC di luar paru-paru) berat.
Kategori 2 : HRZE/5H3R3E3Diberikan kepada:
Penderita kambuh.Penderita gagal terapi.Penderita dengan pengobatan setelah lalai minum obat.
Kategori 3 : 2HRZ/4H3R3Diberikan kepada:
Penderita BTA (+) dan rontgen paru mendukung aktif.