What are the symptoms? Stiff neck Photophobia Ache Vomiting
Irritability Altered level of consciousness Poor feeding Rash:
purpuric and non blanching (late sign)
Slide 4
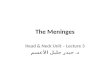
SIDE NOTE. Meningitis and subarachnoid haemorrhage can block
villi causing increased ICP Arachnoid granulations Superior
sagittal sinus Pia mater Falx cerebri CSF in subarachnoid space
One-way flow of CSF
Slide 5
What are the brain changes? Leptomeningeal enhancement (the
arachnoid and pia matter) and distension of the subarachnoid space.
What imaging is best for viewing these changes? FLAIR (Fluid
Attenuated Inversion Recovery) analysis.
Slide 6
Causative organisms? If someone is immunocompromised (e.g.
HIV), what is the likely causative pathogen? Listeria monocytogenes
Group B strep, E. coli, Listeria monocytogenes Neisseria
meningitidis Strep. pneumoniae mumps enterovirus Neisseria
meningitidis listeria monocytogenes herpes simplex Varicella
zoster
Slide 7
Differential diagnosis? Subarachnoid haemorrhage Stiff neck
Headache severe/sudden Vomiting Photophobia Blurred vision
Hypoglycaemia Altered mental state TB (esp CNS TB) History of TB
contact Resident in endemic area Signs of pulmonary disease
Encephalitis Abnormal cerebral function such as altered behaviour
Fever Brain tumour Meningitis: Fever Gradual headache
Slide 8
What signs can be elicited in someone with meningitis?
Brudzinskis sign Lift head whilst supine; Positive test if the
patient flexes knees Kernigs sign Flex hip to 90 degrees Extend
knee Positive test if the patient experiences back pain
Slide 9
What investigations should be carried out? CT When and why do
you do this before a lumbar puncture? Lumbar puncture CSF analysis
If unable to do LP do blood cultures PCR CSF or cultures for exact
cause FBC U+Es Consider CT when there is evidence of raised ICP to
prevent coning
Slide 10
Lumbar Puncture What layer does the adult spinal cord
terminate? What layer does the subarachnoid space end? What layers
does a needle move through in a LP? L1 S1-S2 1.Skin 2.Subcutaneous
fat 3.Supraspinous ligament 4.Interspinous ligament 5.Ligamentum
Flavum (Pop!) 6.Dura (Pop!)
Slide 11
What changes in the CSF in meningitis?
ConditionAppearanceCytology (mm 3) Type of CellGlucose (mmol/L)
Protein (g/L) NormalGin clear1000Mostly Neutrophils LowHigh Viral
Meningitis Clear500-1000Mostly Lymphocytes Normal
Slide 12
What is xanthochromia in the CSF? What could its presence
indicate? When RBC have been in the CSF for > 6 hours they take
on a yellowish tint. Presence may indicate a recent subarachnoid
haemorrhage.
Slide 13
What is the treatment for meningitis? Use a broad spectrum AB
until the causative agent is determined.. If immunocompromised/
pregnant/ over 55 years then also give high dose of. Ceftriaxone (a
cephlosporin) Amoxicillin IV
Slide 14
What are the complications of meningitis? Immediate
complications: septic shock, seizures Hearing loss children should
have hearing tests after meningitis Memory problems Gait problems
Kidney failure
Slide 15
What is the prevention for meningitis? Meningitis vaccine: this
vaccine prevents against meningitis caused by the A, C, X, Y and Z
variants of the Neisseria Meningitis bacterium. There is no
protection against the B strain.
Slide 16
Question time. Which of the following does not commonly cause
meningitis? Strep pneumoniae Clostridium tetani Listeria
monocytogenes Neisseria meningitidis Haem influenzae What is the
current first choice antibiotic for bacterial meningitis?
Cephalosporin Penicillin Vancomycin Erythromycin Ampicillin
Slide 17
Vaccination is recommended to prevent epidemic meningitis among
college students resulting from infection with Clostridium tetani
Haemopilus influenzae Strep pneumoniae Neisseria meningitidis
Listeria monocytogenes Diagnosis of bacterial meningitis requires a
sample of Brain Sputum CSF Urine Blood
Slide 18
How far in from the skin does a needle need to move in order to
reach the epidural space 2.5cm 4-3.5cm 4-4.5cm 4-5.5cm
4.5-5.5cm
Slide 19
Short Answers Questions Meningitis can present with symptoms of
shock. What is the definition of septic shock? Defined by sepsis,
hypotension of SBS under 90mmHg (despite fluid resus) and perfusion
abnormalities How do you diagnose systemic inflammatory response
syndrome? >1 of: Temperature less than 36 or greater than 38
Heart rate over 90/minute RR over 20/minute WWC under 4 or over
12x10 9 /dl
Slide 20
What is the treatment of severe sepsis? Give high flow 02 Give
empirical IV antibiotics Give IV fluid resusitation Take blood
cultures Take (measure) FBC and serum lactate Start to Take
accurate urine output measurments