Embed Size (px)
DESCRIPTION
Sepsis, Severe Sepsis & Septic Shock. Meral SÖNMEZOĞLU, Assoc Prof Yeditepe University Hospital Infectious Diseases Department. Overview. Differentiation between Septic Shock in relation to other conditions in current code, Sepsis, and Severe Sepsis - PowerPoint PPT Presentation
Citation preview

1
Meral SÖNMEZOĞLU, Assoc ProfYeditepe University Hospital
Infectious Diseases Department
Sepsis, Severe Sepsis & Septic Shock

2
Overview
• Differentiation between Septic Shock in relation to other conditions in current code, Sepsis, and Severe Sepsis
• Disease Epidemiology, Incidence and Mortality• Inadequacy of Current Diagnostic Codes• Proposed Modifications and Clarification• Discussion

Systemic Inflammatory Response
• At least 2 of 4 ( abnormal temp or leukocytes count is a must)
—Core temp >38.5 or <36
—Tachycardia: HR >2 sd above Normal for age or bradycardia <10% for age
—Tachypnea: RR >2 sd for age or mechanical ventilation for acute process
—Leukocyte elevated or depressed for age or >10% immature neutrophils
3

Definitions
• Infection: Suspected or proven caused by any pathogen Or clinical syndrome associated with high probability of infection
• Sepsis: SIRS in the presence of or as a result of suspected of proven infection
4

Definitions
• Severe Sepsis: sepsis + one—Cardiovascular dysfunction
—ARDS
—OR 2 or more other organ dysfunctions
• Septic shock—Sepsis and cardiovascular organ dysfunction
5

6
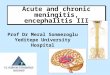
Sepsis: Defining a Disease Continuum
A clinical response arising from a nonspecific insult, including 2 of the following:
• Temperature 38oC or 36oC• HR 90 beats/min• Respirations 20/min• WBC count 12,000/mm3 or
4,000/mm3 or >10% immature neutrophils
SIRS = Systemic Inflammatory Response Syndrome
SIRS with a presumed or confirmed infectious process
SepsisSepsisSIRSSIRSInfection/Infection/TraumaTrauma Severe SepsisSevere Sepsis
Adapted from: Bone RC, et al. Chest 1992;101:1644Opal SM, et al. Crit Care Med 2000;28:S81

7
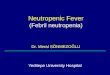
Sepsis: Defining a Disease Continuum
Bone et al. Chest 1992;101:1644; Wheeler and Bernard. N Engl J Med 1999;340:207
SepsisSepsisSIRSSIRSInfection/Infection/TraumaTrauma Severe SepsisSevere Sepsis
Sepsis with 1 sign of organ failure
Cardiovascular (refractory hypotension)
RenalRespiratoryHepaticHematologicCNSMetabolic acidosis
ShockShock

8Bone et al. Bone et al. ChestChest 1992;101:1644 1992;101:1644
Relationship Of Infection, SIRS, Sepsis Severe Sepsis and Septic Shock
SIRSINFECTION
PANCREATITIS
BURNS
TRAUMA
OTHER
SEPSIS
SEVERESEPSIS
SEPTICSHOCK

9
Inflamatory Cascade
Lipid Mediators
Clotting Abnormalities
Vasodilation
Capillary Leak
FeverMetabolic ChangesHormonal Changes*
Adhesion Molecules
Superoxide RadicalsLysosomal Enzymes
NeutrophilAccumulation
Tissue Factor
Coagulation System
Nitric Oxide
Chemotaxis
CytokinesTNF-, IL-1, IL-6, IL-8, etc.
ComplementSystem
EndothelialCells
Neutrophils
MonocyticCells
Bradykinin
= inhibited by rBPI in vivo or in vitro
= not investigated*
Gram-negative Bacteria/
Endotoxin
Hypotension, ARDS, DIC,
Multiple Organ Failure, Death

10Russell J. N Engl J Med 2006;355:1699-1713
SEPSIS MEDIATORS

11
Mortality
Septic Shock
53-63%
20-53%Severe Sepsis300,000
7-17%Sepsis
400,000
Incidence
Balk, R.A. Crit Care Clin 2000;337:52
Mortality Increases in Septic Shock Patients
Approximately 200,000 patients including 70,000 Medicare patients have septic shock annually

12
ICD-9-CM code 785.5X Population
785.59 Details
88,600
10,100
45,200
Septic Shock is Unique within 785.59
Septic Shock patients have a longer length of stay and a higher cost than other patients within 785.59
* Represents Septic Shock Patients
Population Mortality Length
Of Stay
Cost
With infection *
70,900 51% 17.1 $30,300
Without infection
17,700 52% 8.9 $17,400
785.5UnspecifiedShock7%
785.51Cardiogenic Shock 31%
785.59 Other Shock62%

www.themegallery.com
Severe Sepsis: A Significant Healthcare Challenge
11Major cause of morbidity and mortality worldwide
Leading cause of death in noncoronary ICU (US)* 11th leading cause of death overall (US) †§
22About 1,000,000 cases of severe sepsis in US annually‡
33In the US, about 600-1000 patients die of severe sepsis daily
*Sands KE et al. *Sands KE et al. JAMAJAMA. 1997;278:234-40; . 1997;278:234-40; †Based on data for septicemia. Based on data for septicemia. §Murphy SL. National Vital Statistics Reports. ‡Angus DC et al. ‡Angus DC et al. Crit Care MedCrit Care Med. 2001 (In Press); reflects hospital-wide cases of severe sepsis as defined by . 2001 (In Press); reflects hospital-wide cases of severe sepsis as defined by infection ininfection in the presence of organ failure. the presence of organ failure.

www.themegallery.com
Sepsis Epidemiology: Effect of the Aging Population
0
5
10
15
20
25
30
35
40
45
0 1 5 10 15 20 25 30 35 40 45 50 55 60 65 70 75 80 85
Without Comorbidity
With Comorbidity
Overal

www.themegallery.com
Severe Sepsis: Comparison With Other Major Diseases
0
50
100
150
200
250
300
AIDS* Colon Breast
Cancer§
CHF† Severe Sepsis‡
Cas
es/1
00,0
00
Incidence of Severe Sepsis Mortality of Severe Sepsis
AIDS* SevereSepsis‡
AMI†Breast Cancer§
Dea
ths/
Yea
r
†National Center for Health Statistics, 2001. §American Cancer Society, 2001. *American Heart Association. 2000.
‡Angus DC et al. Crit Care Med. 2001

www.themegallery.com
Mortality of Sepsis over TimeP
rop
ort
ion
of
Pa
tien
ts w
ith
Se
ps
is W
ho
Die
d
1979 1981 1983 1985 1987 1989 1991 1993 1995 1997 1999 2001

www.themegallery.com
Economics of Sepsis
• Severe SepsisSevere Sepsis $22,000 per case$22,000 per case US annual cost US annual cost $16.7$16.7 BillionBillion
• Nosocomial SepsisNosocomial Sepsis increased LOS - ICU 8 days, Hosp 24 days$40,890 per case
Angus CCM, 2001Pittet JAMA, 1994

www.themegallery.com
Time Sensitive Interventions
AMI
Stroke“Time is Brain” The sooner that treatment begins, the better are one’s chances of survival without disability.
Trauma“The Golden Hour” Requires immediate response and medical care “on the scene.” Patients typically transferred to a qualified trauma center for care.
“Door to PCI” Focus on the timely return of blood flow to the affected areas of the heart. (percutanous coronary intervention)

www.themegallery.com
Trauma vs. Sepsis Patient CareWhere we spend our efforts

www.themegallery.com
Severe Sepsis vs. Current Care Priorities
Care PrioritiesU.S.
Incidence# of Deaths Mortality Rate
AMI (1) 900,000 225,000 25%
Stroke (2) 700,000 163,500 23%
Trauma (3)
(Motor Vehicle)
2.9 million (injuries)
42,643 1.5%
Severe Sepsis (4) 751,000 215,000 29%
Source: (1) Ryan TJ, et al. ACC/AHA Guidelines for management of patients with AMI. JACC. 1996; 28: 1328-1428. (2) American Heart Association. Heart Disease and Stroke Statistics – 2005 Update. Available at: www.americanheart.org. (3) National Highway Traffic Safety Administration. Traffic Safety Facts 2003: A Compilation of Motor Vehicle Crash Data from the Fatality Analysis Reporting System and the General Estimates System. Available at http://www.nhtsa.dot.gov/. (4) Angus DC et al. Crit Care Med 2001;29(7): 1303-1310.

www.themegallery.com
The Surviving Sepsis Campaign
25% Reduction In Sepsis Mortality within next 5 yrs = ~ 50,000 people in the United States each year.
= ~ 1,100,000 individuals worldwide each year.
Angus DC, et al. Epidemiology of severe sepsis in the United States: Analysis of incidence, outcome, and associated costs of care. Critical Care Medicine. Jul 2001;29(7):1303-1310.

Cardiovascular Dysfunction
• Despite administration of isotonic intravenous fluid• bolus ≥40 mL/kg in 1 hr
—Hypotension: BP <5th % or <2 sd OR—Need for vasoactive drug to maintain BP (dopamine >5
mcg/kg/min or dob, epi, or norepi at any dose) OR—Two of the following
Unexplained metabolic acidosis: Base deficit >5.0 mEq/L Arterial lactate: >2 times upper limit of normal Oliguria: Urine output <0.5 mL/kg/hr Capillary refill: >5 secs Core to peripheral temperature gap >3°C
22

Respiratory Dysfunction
• PaO2 /Fio2 <300 in absence of cyanotic heart• disease or preexisting lung disease OR• PaCo2 >65 or 20 mm Hg over baseline Paco2 OR• Need or >50% Fio2 to maintain saturation ≥92%
OR• Need for non-elective invasive or non-invasive• mechanical ventilation
23

Neurologic Dysfunction
• Glasgow Coma Score ≤11 OR
• Acute change in mental status with a decrease in Glasgow Coma Score ≥3 points from abnormal baseline
24

Hematologic Dysfunction
• Platelet count <80,000/mm or a decline of 50% in platelet count from highest value recorded over the past 3 days
• INR >2
25

Renal Dysfunction
• Serum creatinine ≥2 times upper limit of• normal for age or
• 2-fold increase in baseline creatinine
26

Hepatic Dysfunction
• Total bilirubin ≥4 mg/dL (not applicable for• newborn) OR
• ALT 2 times upper limit of normal for age
27

Mortality and SIRS
28

Mortality

Mortality

31
Conclusion
• Septic shock has distinct characteristics that support the creation of a unique code (785.52)• Septic shock should be linked to severe sepsis• Modification of current SIRS coding will better
represent the clinical presentation of the sepsis syndrome
— 995.51, sepsis
— Modification to “code also” list in 995.92

Deficiencies of 1991 Consensus Conference
• Limitations inherent in these definitions:—Incomplete agreement as to what defines
“Systemic Response" Inflammation only?
—Organ/System failures not defined Except hypotension (SBP <90 mmHg or >40 mmHg
decline from baseline; need for vasopressor support)
"Dear SIRS, I do not like you"
Jean Louis Vincent

33
2001 Sepsis Definitions Conference• Current definitions will remain unchanged• However, will accept the uncertainty of definitions• SIRS expanded to signs and symptoms
—Chills—Alteration in temperature—Tachypnea—Change in mental status—Tachycardia—Altered WBC, Bandemia—Thrombocytopenia—Decreased perfusion: mottling, poor capillary refill— Increased blood sugar—Petichiae/Purpura

34
2001 Sepsis Definitions Conference
• PIRO staging system proposed—Predisposition: Genetics, Chronic illness
—Insult: Infection, Injury, Ischemia
—Response: Physiologic, Mediators, Markers
—Organ Dysfunction: Outcome, Organ dysfunction
To be published 2002 (Verbal communication Mitchell Levy, SCCM 2002)

35
Russell J. N Engl J Med 2006;355:1699-1713
Inflammatory Responses to Sepsis

36
Russell J. N Engl J Med 2006;355:1699-1713
Procoagulant Response in Sepsis

37

38

39

Treatment

Severe Sepsis/Septic Shock Goals
CVP 8 – 12 mmHg
MAP 65 mmHg
SBP > 90 mmHg
SaO2 93%
ScVO2 > 70%

Sepsis Resuscitation
Emergency Department
and
Intensive Care Unit

Sepsis Resuscitation Bundle
• Serum lactate measured
• Blood cultures obtained prior to antibiotic administration
• From the time of presentation, broad-spectrum antibiotics administered:— within 3 hours for ED admissions — within 1 hour for non-ED ICU admissions
• In the event of hypotension and/or lactate > 4 mmol/L (36 mg/dl): — Deliver an initial minimum of 20-30 ml/kg of crystalloid (or colloid
equivalent) — Apply vasopressors for hypotension not responding to initial fluid
resuscitation to maintain MAP > 65 mmHg
• In the event of persistent hypotension despite fluid resuscitation (septic shock) and/or lactate > 4 mmol/L (36 mg/dl):
— Achieve central venous pressure (CVP) of > 8 mmHg — Achieve central venous oxygen saturation (ScvO2) of > 70%
Information taken from Institute for Healthcare Improvement, Sepsis Module: http://www.ihi.org/IHI/Topics/CriticalCare/Sepsis/

SOP

www.themegallery.com
Bundle Completion and OutcomeA 2-year Implementation Experience
40%
21%
Bundle NotCompleted
BundleCompleted
Mortality (p=0.003) Hospital LOS (p=0.22)
12.9
10.9
Bundle NotCompleted
BundleCompleted
Nguyen, Ann Emerg Med, 2005 - ACEP Annual Meeting; and Crit Care Med, 2005 - Critical Care Congress
Total Patients = 330 patients from Oct 2003 – Sept 2005Bundle Not Completed = 253; Bundle Completed = 77

Serum Lactate
• Hyperlactatemia is typically present in patients with severe sepsis or septic shock and may be secondary to anaerobic metabolism due to hypoperfusion.
• The prognostic value of raised blood lactate levels has been well established in septic shock patients, particularly if the high levels persist (that’s why we trend them).
• Obtaining serum lactate is essential to identifying tissue hypoperfusion in patients who are not yet hypotensive but who are at risk for septic shock.
Information taken from Institute for Healthcare Improvement, Sepsis Module: http://www.ihi.org/IHI/Topics/CriticalCare/Sepsis/

Blood cultures
• The incidence of sepsis and bacteremia in critically ill patients has been increasing in the past two decades.
— 30 - 50% of patients presenting with a clinical syndrome of severe sepsis or shock have positive blood cultures.
— Therefore, blood should be obtained for culture in any critically ill septic patient.
• Collecting blood cultures prior to antibiotic administration offers the best hope of identifying the organism that caused severe sepsis in an individual patient.
— Failure to check blood cultures prior to antibiotic infusion will perhaps affect the growth of any blood borne bacteria and prevent a culture from becoming positive later.
Information taken from Institute for Healthcare Improvement, Sepsis Module: http://www.ihi.org/IHI/Topics/CriticalCare/Sepsis/

Broad Spectrum Antibiotics
• The balance of evidence unwaveringly suggests that early administration of appropriate antibiotics reduces mortality in patients with Gram-positive and Gram-negative bacteremias.
— Some of the evidence supporting early administration is based upon the assumption that patients who fail to receive appropriate antibiotics essentially represent a set of patients for whom delay has occurred in antibiotic delivery.
— Several studies have confirmed the mortality benefit associated with appropriate antimicrobials in patients with severe infections due to Gram-negative and Gram-positive bacteria.
— All patients should receive a full loading dose of each antimicrobial. However, patients with sepsis or septic shock often have abnormal renal
or hepatic function and may have abnormal volumes of distribution due to aggressive fluid resuscitation. The ICU pharmacist should be consulted to ensure that serum concentrations are attained that maximize efficacy and minimize toxicity
Information taken from Institute for Healthcare Improvement, Sepsis Module: http://www.ihi.org/IHI/Topics/CriticalCare/Sepsis/

Antibiotics and Mortality
• In addition, the major sources of infection in severe sepsis or shock are pneumonia and intra-abdominal infections and other sources generally account for < 5 percent of cases.
— The prevalence of pneumonia as a cause of sepsis lends support to the case for treating severe sepsis with early antibiotic administration.
— In a recent study of ventilator acquired pneumonia, patients with significant organ dysfunction who received antibiotics later had far greater ICU mortality: 37 percent vs. 7 percent, P=0.006; hospital mortality: 44 percent vs. 15 percent, P=0.01.
Information taken from Institute for Healthcare Improvement, Sepsis Module: http://www.ihi.org/IHI/Topics/CriticalCare/Sepsis/
0%
10%
20%
30%
40%
50%
ICU Hospital
Mortality
Late Antibiotics Early Antibiotics
p = 0.006p = 0.01

Fluid Resuscitation• The Severe Sepsis Resuscitation Bundle calls for an initial
administration of 20 – 30 ml/kg of crystalloid as a fluid challenge in cases of suspected hypovolemia or actual cases of serum lactate greater than 4 mmol/L (36 g/dl).
— A colloid equivalent is an acceptable alternative to crystalloid, and an equivalent dose generally ranges from 0.2 g/kg to 0.3 g/kg depending upon the colloid.
• Fluid resuscitation should be commenced as early as possible in the course of septic shock (even before intensive care unit admission). Requirements for fluid infusion are not easily determined so that repeated fluid challenges should be performed.
• The bundle does not restrict the amount and extent of an initial fluid challenge, but rather defines a minimum challenge. Subsequent actions in the bundle are undertaken only for hypotension not responding to fluid challenge or for an elevated lactate level as above.
Information taken from Institute for Healthcare Improvement, Sepsis Module: http://www.ihi.org/IHI/Topics/CriticalCare/Sepsis/

Vasopressor Support
• Adequate fluid resuscitation is a prerequisite for the successful and appropriate use of vasopressors in patients with septic shock.
— In general, the end points of fluid resuscitation are the same as those for the use of pharmacologic hemodynamic support, i.e. MAP > 65 mmHg. Sometimes, fluid resuscitation alone may suffice.
— When an appropriate fluid challenge fails to restore an adequate arterial pressure and organ perfusion, therapy with vasopressor agents should be started. Vasopressor therapy may also be required transiently to sustain life and maintain perfusion in the face of life-threatening hypotension, even when hypovolemia has not been resolved or when a fluid challenge is in progress
• Either norepinephrine or dopamine (through a central catheter as soon as placement is possible) is the first-choice vasopressor agent to correct hypotension in septic shock.
Information taken from Institute for Healthcare Improvement, Sepsis Module: http://www.ihi.org/IHI/Topics/CriticalCare/Sepsis/

Maintaining Hemodynamics
• Goal-directed therapy represents an attempt to predefine resuscitation end-points to help clinicians at the bedside to resuscitate patients in septic shock.
— The end-points used vary according to the clinical study but attempt to adjust cardiac preload, contractility, and afterload to balance systemic oxygen delivery with demand.
• Two essential features of early goal directed therapy include: — maintaining an adequate central venous pressure (CVP) to carryout other
hemodynamic adjustments— maximizing mixed or central venous oxygen saturation (ScVO2)
• Special patients:— In mechanically ventilated patients, a higher target central venous pressure of
12–15 mmHg is recommended to account for the presence of positive end expiratory pressure and increases in intrathoracic pressure.
— Similar consideration to the above may be warranted in circumstances of increased abdominal pressure.
Information taken from Institute for Healthcare Improvement, Sepsis Module: http://www.ihi.org/IHI/Topics/CriticalCare/Sepsis/

Sepsis Management
Intensive Care Unit

Early Goal-directed therapy in the treatment of severe sepsis and septic shock
Rivers et al; NEJM 2001;345:1368

www.themegallery.com
Early Recognition of Adult Patients with Severe Sepsis/Septic Shock
NO
NO YES NO
YES
NO NO
YESYES
SuspectedInfection
SepsisSepsisSBP < 90
after Bolus
SepticShock
SepticShock
Lactate > 4 mmol/L or Multi-Organ Dysfunction
Severe Sepsis High Risk
Severe Sepsis High Risk
Early Intervention to Resolve Organ Hypoperfusion Early Intervention to Resolve Organ Hypoperfusion
Two or more of the following:
1) Temp >38.3C(100.9F) or <36.0C(96.8F)2) Heart Rate >903) Resp Rate >20 or PaCO2 <32 mmHg4) WBC >12K, <4K or >10% Bands
Two or more of the following:
1) Temp >38.3C(100.9F) or <36.0C(96.8F)2) Heart Rate >903) Resp Rate >20 or PaCO2 <32 mmHg4) WBC >12K, <4K or >10% Bands
Re-Assess
Re-Assess
Antibiotics & IVF
Re-Assess
Obtain Appropriate
Cultures
Check Lactate
Lactate > 2 mmol/L or Organ
Dysfunction
YES
Severe Sepsis Low Risk
Severe Sepsis Low Risk
Antibiotics & IVFRe-check Lactate

Sepsis Management Bundle
• Low-dose steroids administered for septic shock
• Glucose control maintained: 80 - 150 mg/dl
• Inspiratory plateau pressures maintained < 30 cm H2O for mechanically ventilated patients
• Drotrecogin alfa (Xigris) administered in accordance with a standardized ICU policy
Information taken from Institute for Healthcare Improvement, Sepsis Module: http://www.ihi.org/IHI/Topics/CriticalCare/Sepsis/

Corticosteroid use
• Intravenous corticosteroids are recommended in patients with septic shock who despite adequate fluid replacement require vasopressor therapy to maintain adequate blood pressure.
—Hydrocortisone 200–300 mg/day in three or four divided doses for 7 days Hydrocortisone 50 mg IV q6h Hydrocortisone 100 mg IV q8h Doses > 300 mg per day are associated with
increased mortality
Information taken from Institute for Healthcare Improvement, Sepsis Module: http://www.ihi.org/IHI/Topics/CriticalCare/Sepsis/

Glucose control
• Following initial stabilization of patients with severe sepsis, blood glucose should be maintained 80 – 150 mg/dL.
— Studies supporting the role of glycemic control have used continuous infusion of insulin and glucose.
— With this protocol, glucose should be monitored frequently after initiation of the protocol (every 60 minutes) and on a regular basis (every 4 hours) once the blood glucose concentration has stabilized.
• Hyperglycemia, caused by insulin resistance in the liver and muscle, is a common finding in intensive care unit (ICU) patients.
— It can be considered an adaptive response, providing glucose for the brain, red cells, and wound healing, and is generally only treated when blood glucose increases to > 215 mg/dL (>12 mmol/L).
— Conventional wisdom in the ICU has been that hyperglycemia is beneficial and that hypoglycemia is dangerous and should be avoided. This concept has been challenged recently, and controlling blood glucose levels by intensive insulin therapy decreased mortality and morbidity in surgical critically ill patients.
Information taken from Institute for Healthcare Improvement, Sepsis Module: http://www.ihi.org/IHI/Topics/CriticalCare/Sepsis/

Plateau Pressures
• Patients with sepsis are at increased risk for developing acute respiratory failure, and most patients with severe sepsis and septic shock will require endotracheal intubation and mechanical ventilation.
— Nearly 50% of patients with severe sepsis will develop acute lung injury (ALI)/acute respiratory distress syndrome (ARDS).
• High tidal volumes that are coupled with high plateau pressures should be avoided in ALI/ARDS.
— Clinicians should use as a starting point a reduction in tidal volumes over 1 to 2 hours to a “low” tidal volume (6 mL/kg lean body weight) as a goal in conjunction with the goal of maintaining end-inspiratory plateau pressures of < 30 cm H2O.
Information taken from Institute for Healthcare Improvement, Sepsis Module: http://www.ihi.org/IHI/Topics/CriticalCare/Sepsis/

Drotrecogin alfa
• Drotrecogin Alfa (Activated), a.k.a. recombinant activated protein C (rhAPC), is recommended in patients at high risk of death (APACHE II of > 25, sepsis-induced multiple organ failure, septic shock, or sepsis-induced acute respiratory distress syndrome) and no absolute contraindication related to bleeding risk or relative contraindication that outweighs the potential benefit of rhAPC.
• The inflammatory response in severe sepsis is integrally linked to pro-coagulant
activity and endothelial activation. The inflammatory response in sepsis is pro-coagulant in the early stages. In a large, multicenter, randomized, controlled trial, the PROWESS trial (Recombinant Human Activated Protein C Worldwide Evaluation in Severe Sepsis) rhAPC, an endogenous anticoagulant with anti-inflammatory properties, has been shown to improve survival in patients with sepsis-induced organ dysfunction.
• At present, risk assessment is best determined by bedside clinical evaluation and judgment. The use of a standardized policy in intensive care units for the administration of rhAPC is essential to avoid capricious and unscientific decision-making about applying rhAPC.
Information taken from Institute for Healthcare Improvement, Sepsis Module: http://www.ihi.org/IHI/Topics/CriticalCare/Sepsis/

Therapies

Vasopressors
• Norepinephrine and Dopamine—First line therapy—Central line preferred
• Vasopressin—Give at doses of 0.04 units/minute in addition to
norepinephrine or dopamine—Not titrated
• Phenylephrine/Epinephrine—Not used as first line due to risk of ischemia—In septic patients, it is added in shock refractory to
norepinephrine or dopamine

Dobutamine
• When it’s used: after fluid resuscitation, it is considered (in conjunction with hematocrit evaluation) to increase ScVO2 > 70%.
• How it works: Dobutamine directly stimulates ß1 receptors of the heart to increase myocardial contractility and stroke volume, resulting in increased cardiac output.
• Dosing: — Increase by 2 mcg/kg/minute with each ScVO2 reading that is <
70%
• Monitoring:— Monitor for hypotension, arrhythmia

Blood products
• When it’s used: if the ScVO2 remains < 70% despite adequate fluid resuscitation, consider transfusion to a hematocrit of 30%.
• How it works: Increases blood carrying capacity to the tissues.
• Dosing: — Patient specific (however, 1 unit of PRBCs should increase the
hematocrit by ~3%)
• Monitoring:— Per routine

Fluids• Crystalloids:
—Another name for IV fluids—Isotonic crystalloid solutions should
be used for resuscitation NSS or LR
Use caution with LR in patients with renal disease or electrolyte abnormalities (contains Na, K, Ca, Cl, and lactate)
Lactate content has not been shown to affect serum lacate levels NOT: D5W, D5W/½NSS, ½NSS, etc.
• Colloids:—Solutions like albumin and blood
Also, hespan/hextend

Initial Resussitation
• Begin as soon as the sepsis syndrome is recognized
66

Initial Fluid Resuscitation
• Central venous pressure: 8–12 mm Hg• Mean arterial pressure ≥65 mm Hg (adult)• Urine output ≥0.5 mL·kg−1 ·hr−1• Central venous (superior vena cava) or mixed
venous oxygen saturation ≥70%
Grade B
67

Initial Fluid Resuscitation
• sVO2 >70% is not achieved with CVP 8–12 mm Hg, then transfuse PRBC to achieve a hematocrit of 30% and/or
• Dobutamine infusion (up to a maximum of 20 mcg/kg/min)
Grade B
68

Diagnosis
• Appropriate cultures should always be obtained before antimicrobial therapy is initiated • at least 2 B/C should be obtained at least one
drawn percutaneously and one drawn through each vascular access device.• Cultures of other sites such as urine, CSF,
wounds, respiratory secretions, or other body fluids should be obtained before antibiotic therapy
69

Antibiotic Therapy
• Started within the first hour of recognition of severe sepsis after cultures (Grade E)• One or more drugs with activity against the likely pathogens• Penetrate into the presumed source of sepsis • Guided by the susceptibility patterns of mo.s in the
community and in the hospital (Grade D)• Reassess after 48–72 hrs, aim for narrow spectrum
antibiotic• Duration 7–10 days and guided by clinical response.(Grade
E)
70

71
Novel Therapies
• Steroids JAMA. 2002 Aug 21;288(7):862-71
Many (>50%) septic patients have relative adrenocortical insufficiency.
Physiological hydrocortisone improves mortality in this group (63% → 53%, p=0.02 in this study, n=229)
Antiinflammatory

72
Novel Therapies
• Activated Protein C (Drotrecogin α) N Engl J Med. 2001 Mar 8;344(10):699-709
Antithrombotic, antiinflammatory, profibrinolytic 1690 patients, Mortality 30.8% →24.7% p<0.01 Increased bleeding 2% →3.5% p=0.06
Caution in meningococcal sepsis / trauma / ICH / pregnant! $17181 / patient Consensus in NZ is restricted last resort use in selected ICU patients

73
Novel Therapies
• Tight glucose control with insulin
N Engl J Med. 2001 Nov 8;345(19):1359-67.
Mortality reduction 8→4.6% (p<0.04) all icu patients
Biggest reductions in severe sepsis / long stayers
Also reduced bacteraemic episodes / icu neuropathy
Aim 4.4-6.1mmol/L

74
Novel Therapies
• rBacteriocidal/Permeability-increasing protein
— In neutrophil granules
— Binds to and inactivates endotoxin Lancet. 2000 Sep 16;356(9234):961-7. 393 Children with clinical meningococcaemia Mortality 9.9% → 7.4% p=0.48 Amputations 7.4% → 3.6%, p=0.067 Better functional outcome 66.3% → 77.3% p=0.019

75
Novel Therapies
• NAC Crit. Care. Med. 2003 31 (11) 2574-78
—Nuclear factor-κB controls expression inflammatory mediators
—NAC inhibits NFKB in vitro
—Pilot trial 20 patients, randomised 72 hrs NAC or placebo IL-8 suppressed (may be implicated in lung injury) Recommend larger human trials

76
Summary
• Sepsis may be obvious or subtle early• There is a high mortality and morbidity• Have a high index of suspicion• Know local organisms / susceptibilities• Take appropriate cultures• Treat early and aggressively• Investigate early and aggressively• Refer early and aggressively• Be aware of new developments

TUS 2012
77

TUS 2012
78

TUS 2012
79

TUS 2012
80

TUS 2012
81

TUS 2012
• Tanısı radyolojik olarak da doğrulanmış bir nekrotizan pankreatit olgusunda vücut sıcaklığı 39°C, kalp atım hızı: 104/dak ve beyaz küre sayısı: 5000/mm3 bulunuyor. Peripankreatik sıvıdan alınan örnekte iltihap olduğu ve oligüri geliştiği görülüyor.• Arteryal kan basıncı sıvı resusitasyonuna cevap veren bu
hastada en olası tanı aşağıdakilerden hangisidir?• A) Sistemik inflamatuvar yanıt sendromu• B) Bakteriyemi• C) Sepsis• D) Ciddi sepsis• E) Septik şok
82

TUS 2012
• Tanısı radyolojik olarak da doğrulanmış bir nekrotizan pankreatit olgusunda vücut sıcaklığı 39°C, kalp atım hızı: 104/dak ve beyaz küre sayısı: 5000/mm3 bulunuyor. Peripankreatik sıvıdan alınan örnekte iltihap olduğu ve oligüri geliştiği görülüyor.• Arteryal kan basıncı sıvı resusitasyonuna cevap veren bu
hastada en olası tanı aşağıdakilerden hangisidir?• A) Sistemik inflamatuvar yanıt sendromu• B) Bakteriyemi• C) Sepsis• D) Ciddi sepsis• E) Septik şok
83