Embed Size (px)
Citation preview

Metastatic Carcinoma of the Colon Similar
to Crohn’s Disease:A Case Report
Kohji Tanakaya , Hitoshi Takeuchi , Yoshimasa Yasui , Akira Takeda ,
Yuzo Umeda , and Ichiro Murakami
Department of Surgery and Department of Pathology, Iwakuni National Hospital, Iwakuni 740-8510, Japan
A 68-year-old Japanese man with a history of linitis plastica carcinoma of the stomach and
subsequent gastrectomy 8 years previously presented with lower abdominal pain. Radiological and
endoscopic examinations showed multiple submucosal nodular lesions similar to Crohn’s disease in the
ileocecal area. A firm diagnosis could not be made after initial multiple biopsies. Finally, a
submucosal biopsy revealed adenocarcinoma. The ileocecal lesion was diagnosed as a recurrence
because of the histological findings, which included mucosal preservation, a similarity with the
histologic type of stomach carcinoma, and atypical immunoreactivity for primary colon carcinoma;the lesion was negative for both cytokeratin 7 and cytokeratin 20. In cases where metastatic
carcinoma of the colon is suspected, we recommend early consideration of a submucosal biopsy.
Key words:metastatic carcinoma, colon, Crohn’s disease
M etastatic carcinoma of the colon is rare. It has
been reported to occur in 0.1-1 of colon
malignancies[1]. The diagnosis is defined by clinical and
histologic findings, and is often difficult to make because
the metastatic lesion usually spreads into the submucosal
space preserved with normal mucosa.We report here a case of metastatic ileocecal car-
cinoma. Considering the clinical course and histologic
examination, this case was quite difficult to diagnose.
Case Report
A 68-year-old Japanese man presented with lower
abdominal pain in January 1995.The patient had undergone a total gastrectomy for
linitis plastica carcinoma of the stomach 8 years previous-
ly. Histological evaluations of the gastric carcinoma had
revealed signet ring cell carcinoma with areas of poorly
differentiated adenocarcinoma, and the depth of invasion
was subserosa. The case was classified as a pT2, pN2,sH0, sP0, sM0, f Stage IIIA gastric carcinoma, accord-ing to the Japanese Classification of Gastric Carcinoma[2]. Two of 5 harvested lymph nodes (LN)along the
lesser curvature(LN No. 3)and 1 of 6 LN along the left
gastric artery(LN No. 7)were positive for metastasis.Immunohistochemical examination of the gastric tumor
revealed partially positive staining for cytokeratin 7(DAKO, Denmark)but not for cytokeratin 20(DAKO).The carcinoembryonic antigen(CEA)was elevated to
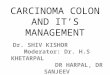
9.1 ng/ml. A barium enema showed a serrated contour
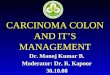
and stricture of the ileocecal region(Fig. 1). A colono-scopy showed multiple submucosal nodular lesions of the
cecum(Fig. 2). The lesions were similar in appearance to
the cobblestone appearance of Crohn’s disease but without
ulceration. We weren’t able to obtain a firm diagnosis by
routine multiple biopsies. Finally, 50 days after admis-
Received August 4,2003;accepted February 26,2004.Corresponding author.Phone:+81-827-31-7121;Fax:+81-827-31-7059
E-mail:tanakaya@iwakuni-nh.go.jp(K.Tanakaya)
http://www.lib.okayama-u.ac.jp/www/acta/
Acta Med. Okayama, 2004
Vol. 58, No. 4, pp. 217-220
Case Report
Copyrightc2004 by Okayama University Medical School.

sion, a diagnosis of adenocarcinoma was made by a
submucosal biopsy using a strip biopsy technique[3].The patient underwent an ileocecal resection.Gross exploration of the abdomen showed that the
recurrence had occurred solely in the ileocecal area.Gross findings of the resected specimen demonstrated
intestinal wall thickening and multiple submucosal nodular
lesions covered with normal mucosa(Fig. 3).Histological examination of the resected specimen
revealed signet ring cell carcinoma with areas of poorly
differentiated adenocarcinoma expanding from the sub-mucosa to the subserosa. Mucosal preservation was
clearly demonstrated by positive staining for CAM5.2(DAKO)(Fig. 4). Two of 11 harvested lymph nodes(LN)along the paracolic vessels were positive for metas-tasis. Neither cytokeratin 7 nor cytokeratin 20 revealed
immunoreactivity in the ileocecal lesion.Although 8 years had passed since the gastrectomy,
the ileocecal lesion was diagnosed as a metastasis from
gastric carcinoma because of histologic findings such as
mucosal preservation and a similarity to stomach car-cinoma. The patient died from peritoneal dissemination of
the carcinoma 16 months after the second surgery.
Discussion
Metastatic carcinoma of the colon usually originates
from carcinoma of the stomach, breast, skin, kidney,prostate, or ovary[4, 5].Findings of the history-taking and examination are
very important for making a diagnosis of metastatic
carcinoma. A recurrence of stomach carcinoma usually
occurs within 5 years of surgery, often in multiple organs.In the present case, the recurrence occurred after a long
interval from the initial stomach carcinoma, and the
ileocecal area was the only lesion in which recurrence was
Tanakaya et al. Acta Med. Okayama Vol. 58, No. 4 218
Fig.1 A barium enema showed a serrated contour and stricture of
the ileocecal region(arrow heads).
Fig. 3 Gross findings of the resected specimen demonstrated
intestinal wall thickening and multiple submucosal nodular lesions
covered with normal mucosa(arrow heads).
Fig.2 A colonoscopy showed multiple submucosal nodular lesions
of the cecum.

suspected. Recurrence was suspected because of the
CEA elevation, but the CEA is often elevated by other
mechanisms.In cases with metastatic carcinoma of the colon, a
barium enema usually reveals segmental colonic strictures.Endoscopic examination normally shows granular and
friable lesions with a loss of the normal vascular pattern,occasionally with submucosal nodularity or superficial
erosions[6], and rarely polyposis[4].Metastatic carcinoma of the colon can be misdiagnosed
as primary linitis plastica carcinoma, Crohn’s disease,ischemic colitis, tuberculosis, or diverticulitis[6].Several authors have reported cases with metastatic
carcinoma of the colon similar to Crohn’s disease[6-9].In cases with Crohn’s disease, there is often colonic
involvement. A barium enema reveals a stenotic bowel
segment and nodular irregularity, the so-called “string
sign”and“cobblestone appearance,”respectively.In cases showing linitis plastica carcinoma or signet
ring cell carcinoma of the colon, the differentiation
between primary and metastatic carcinoma is often made
by the exclusion of other malignancies. Primary signet
ring cell carcinoma is a rare form of colorectal malignancy
usually affecting young patients, and the differentiation is
not always clear at microscopy. Primary carcinoma
infiltrates from the mucosa to the serosa, with metastatic
lesions beginning as submucosal or serosal implants.Recently, immunohistochemical examination for cytoker-atin 7 and cytokeratin 20 has been reported to be useful
for differentiation between signet ring cell carcinoma of the
Metastatic Carcinoma of the Colon August 2004
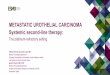
Fig.4 Histological examination of the stomach and ileocecal lesion. A, The stomach lesion showed signet ring cell carcinoma. HE stain,high power field. Bar indicates 20μm. B, The ileocecal lesion showed mucosal preservation, as clearly demonstrated by positive staining
for CAM5.2. ABC method, low power field. Bar indicates 500μm. C, The ileocecal lesion showed the signet ring cell carcinoma with areas
of poorly differentiated adenocarcinoma expanding from the submucosa to the subserosa. HE stain, middle power field. Bar indicates 50μm.D, The ileocecal lesion showed signet ring cell carcinoma. HE stain, high power field. Bar indicates 20μm.
219

stomach and colon[10]. A colon primary is supported if
the neoplastic cells have a cytokeratin 7(-)/cytokeratin
20(+)staining pattern, and a gastric primary is support-ed if the cells have a cytokeratin 7(+)/cytokeratin 20(-)staining pattern.In the present case, the gastric lesion revealed a
partially positive staining pattern for cytokeratin 7 and a
negative staining pattern for cytokeratin 20, while the
ileocecal lesion revealed negative patterns for both cyto-keratin 7 and cytokeratin 20. Although metastatic lesions
sometimes reveal histologic features different from those
of the primary lesion, the ileocecal lesion did not show a
typical staining pattern for colon signet ring cell car-cinoma. In the present case, the ileocecal lesion was
diagnosed as a recurrence because of the histologic
findings, which included mucosal preservation, a similar-ity to the histologic type of stomach carcinoma, and
atypical cytokeratin 7 and cytokeratin 20 staining patterns
for primary colon carcinoma.The usual endoscopic biopsy often fails to define the
diagnosis. In the present case, we initially suspected
Crohn’s disease or malignant lymphoma, and we required
50 days to make a correct diagnosis using a strip biopsy
resection technique[3]. The biopsy specimen obtained
by this technique includes both submucosal and mucosal
tissues. Therefore, when metastatic carcinoma of the
colon is suspected, we recommend early consideration of
a submucosal biopsy.
References
1. Balthazar EJ, Rosenberg HD and Davidian MM:Primary and metas-tatic scirrhous carcinoma of the rectum. Am J Roentgenol(1979)132:711-715.
2. Japanese Gastric Cancer Association:Japanese Classification of
Gastric Carcinoma-2nd English Edition-. Gastric Cancer (1998)1:10-24.
3. Karita M, Tada M, Okita K and Kodama T:Endoscopic therapy for
early colon cancer:The strip biopsy resection technique. Gastrointest
Endosc(1991)37:128-132.4. Ogiwara H, Konno H, Kitayama Y, Kino I and Baba S:Metastasis
from gastric adenocarcinoma presenting as multiple colonic polyps:Report of a case. Surgery Today(1994)24:473-475.
5. Fayemi AO, Ali M and Braun EV:Metastatic carcinoma simulating
linitis plastica of the colon. A case report. Am J Gastroenterology(1979)71:311-314.
6. Kanter MA, Isaacson NH, Knoll SM and Nochomovitz LE:The diag-nostic challenge of metastatic linitis plastica. Two cases and a
consideration of the problem. Am Surg (1986)52:510-513.
7. Lammer J, Dirschmid K and Hugel H:Carcinomatous metastases to
the colon simulating Crohn’s disease. Gastrointest Radiol (1981)6:89-91.
8. Katon RM, Brendler SJ and Ireland K:Gastric linitis plastica with
metastases to the colon:A mimic of Crohn’s disease. J Clin Gas-troenterol(1989)11:555-560.
9. Cox MR, Heinz AW, Fisher AL and Smart P:Linitis plastica carcinoma
of the colon mimicking Crohn’s colitis. Aust N Z J Surg (1992)62:654-657.
10. Goldstein NS, Long A, Kuan SF and Hart J:Colon signet ring cell
adenocarcinoma:Immunohistochemical characterization and compari-son with gastric and typical colon adenocarcinomas. Appl Immunohis-tochem Mol Morphol(2000)8:183-188.
Tanakaya et al. Acta Med. Okayama Vol. 58, No. 4 220