Embed Size (px)
Citation preview

Methods, paradigms, and practices:
Advancing Dissemination and Implementation Science
Abby Meadema Steketee
Dissertation submitted to the faculty of the Virginia Polytechnic Institute and State
University in partial fulfillment of the requirements for the degree of
Doctor of Philosophy
In
Human Nutrition, Foods, and Exercise
Samantha M. Harden, Chair
Kevin Davy
Vivica Kraak
Charles Calderwood
December 4, 2020
Blacksburg, Virginia
Keywords: implementation, pragmatic, qualitative, RE-AIM, coaching, translational
science spectrum

Methods, paradigms, and practices: Advancing Dissemination and Implementation Science
Abby Meadema Steketee
Academic Abstract
There is a critical gap in translating scientific discoveries to public health benefit. For
example, despite a multitude of efficacious physical activity interventions, only one in four
adults in the United States meets the Physical Activity Guidelines for Americans. To bridge the
research-practice gap, Dissemination and Implementation (D&I) Science has emerged as the
study of how evidence-based interventions, programs, and policies are integrated in typical
settings. Recent research illustrates barriers to conducting D&I Science and the need for
methods that open the black box of implementation. Therefore, the overarching goal of this
dissertation was to explore novel approaches for advancing D&I Science. This exploration is
presented in three manuscripts and one report.
The first manuscript presents a pragmatic, observational study applying the RE-AIM
(Reach, Effectiveness, Adoption, Implementation, Maintenance) Framework to evaluate a
perinatal health fair. Results include that the health fair reached 42 attendees and that 23
educators and seven organizations hosted booths and educational sessions. Mom Expo required
292 implementation hours with 71% of those hours devoted to building relationships. We
generated 30 actionable strategies for implementing a health fair. The health fair developed into
a non-profit organization, and the participatory approach used can be replicated in other
communities to establish connections between local women, educators, and researchers.
The second manuscript reports a one-year autoethnography (i.e., first-person narrative) of
a perinatal health integrated research practice partnership (IRPP). Findings include three themes:
(1) permeable work boundaries, (2) blind spots toward philosophical underpinnings of
paradigms, and (3) maladaptive behaviors seemingly reinforced by the research culture. We
concluded that autoethnography is an effective novel method to leverage researcher situatedness
and capture implementation contexts, processes, and outcomes.
The third manuscript presents the longitudinal pilot test of FUEL (focus, unplug,
exercise, love), a one-on-one coaching program to promote human flourishing among D&I
researchers. Results include that the coach spent 12.96+2.82 hours per participant (N= 16)
implementing individually-tailored sessions, and that participants reported multiple, sustained
benefits related to productivity, happiness, and health. We concluded that the program is a
feasible, well-received approach with preliminary positive effects. Future work is needed to
investigate physiological or performance outcomes and, ultimately, impact on D&I.
The final report is a literature review and critical analysis of phenomenology within
behavioral and community health research. Conclusions include that (1) physical activity is
rooted in a scientific paradigm that prioritizes quantifiable mechanism over personal meaning,
and (2) phenomenology, as a complement to basic science, is a compelling method, paradigm,
and practice to improve research translation.
Based on this research, I conclude that three pathways for advancing D&I Science are
methods that capture first-person meaning, paradigms that incorporate phenomenological human
experience as an essential dimension of health research, and practices that fuel researchers’
capacity for generating transformative work. In all three pathways, the heart of elevating D&I
Science is to embrace process, person, and presence.

Methods, paradigms, and practices: Advancing Dissemination and Implementation Science
Abby Meadema Steketee
General Audience Abstract
Scientific evidence does not automatically translate to real-world behavior change. For
example, despite considerable research about the health benefits of physical activity, only one in
four American adults meets the national physical activity recommendations. To bridge the
research-practice gap, Dissemination and Implementation (D&I) Science has emerged as the
study of how scientific findings are integrated in typical settings such as schools and
communities. Recent research illustrates multiple barriers to D&I Science and a need for
methods that capture hard-to-measure, chaotic implementation processes and outcomes.
Therefore, the overarching goal of this dissertation was to explore novel approaches to D&I
Science and bridging the research-practice gap. This exploration is presented in three
manuscripts and one report.
The first manuscript describes a perinatal health fair intended to connect local parents to
community resources. The second manuscript is a 12-month autoethnography (i.e., first-person
narrative) about the culture of D&I Science, including the role, impact, and practices of
researchers themselves. The third manuscript presents the development and preliminary testing
of FUEL (focus, unplug, exercise, love), a one-on-one coaching program for D&I researchers.
The final report includes the history of randomized controlled trials as the gold standard for
physical activity research, as well as critical analysis of using phenomenology to reduce the
research-practice gap.
Findings from the first manuscript suggest that (1) authentic relationship building was the
key to launching a perinatal health fair that developed into a non-profit organization and (2) the
RE-AIM (Reach, Effectiveness, Adoption, Implementation, Maintenance) Framework is a user-
friendly D&I tool for implementing and evaluating a health fair. Findings from the second
manuscript include descriptions of (1) blind spots within the D&I Science culture, (2) potential
of autoethnography as a novel D&I method, and (3) strategies to optimize D&I researchers’
capacity to thrive amid challenges. Findings from the third manuscript suggest that the FUEL
coaching program is a promising and feasible approach to support researchers in leading “a more
productive, healthier, and happier life,” as one participant wrote. Future research on the program
is needed to evaluate causation and whether organizations would adopt it. Conclusions in the
final report include that (1) the applicability of physical activity research to daily life may be
limited by deeply held scientific ideologies and (2) phenomenology, as the study of human
meaning, may facilitate the translation of research to real-world behavior change.
Based on the research presented in this dissertation, three pathways for advancing D&I
Science are methods for how we conduct research studies, paradigms for how we collectively
approach health science, and practices for how we manage our energy and awareness. In all
three pathways, the heart of elevating D&I Science is to embrace process, person, and presence.

iv
Dedication
To Mac Hill
who, at age two,
tottered out the garage door
toward the woods with me,
flung his arms up to the sky
and proclaimed, “Trees!”
Thank
you
for
the
reminder.

v
Acknowledgements
With thanks…
To my mother, who taught me to read and write and who has fueled me through nearly four
decades.
To my dad, who blends compassion and proficiency, tenacity and laughter.1
To Pops, whose marvel and humanity I remember every day: Feet to feet!
To Ali, whose voice and letters give me courage.
To Brad, who drives me crazy and keeps me sane.
To Fletcher, who brings me squash, takes me on hikes, and saved the defense.
To Lucy, the truly “lighted one,” who keeps her priorities straight and closets disastrous.
To Lindsay, Rachel, and Chris—Morticia, hiker trash, and Luigi—whose quirks and love have
been priceless, especially these last few months.
To Dr. Samantha Harden, who gave me the opportunity to return to school and permission to
experiment with the non-experimental in the Wonderland of academia.
To Dr. Kevin Davy, who took time to talk about erging, and during the qualifying exam may
have asked me the most thought-provoking test question I’ve ever been asked.
To Dr. Vivica Kraak, whose templates and scholarly resources are almost as cool as her mask
collection.
To Dr. Charles Calderwood, who connected me with work stress literature without causing me
stress.
To the Translation Obesity Research Interdisciplinary Graduate Education Program for funding
me.
To the Margaret C. Hepler Summer Research Fellowship for supporting my summer work.
To the many community members, research participants, and Cooperative Extension agents who,
in letting me be part their lives, have deeply touched my own.
To my kindergarten teacher, Mrs. Beth Farley; middle school science teacher, Mrs. Margaret
Hardy; and high school journalism teacher, Ms. Marie Harris.
To the people who have coached me, who have coached beside me, and who have let me coach
them.
And to Steve my husband, who has done the laundry so that I can wear “our” sweatshirts. Thank
you for looking on tempests and being not shaken.
1 What does a dog receive after she finishes her PhD? A pet-degree.
vi
Attributions
Manuscript 1:
Dr. Samantha M. Harden is an associate professor in the Department of Human Nutrition, Foods,
and Exercise at Virginia Tech. She established the original research-practice partnership on
which this work was built. She also facilitated event planning, event implementation, data
analysis, and manuscript editing.
Manuscript 2
Dr. Thomas Archibald is an associate professor in the Department of Agriculture, Leadership,
and Community Education at Virginia Tech. He contributed expertise and creativity in
incorporating interdisciplinary theories and concepts, as well as interpreting results and crafting
the conclusion.
Dr. Samantha M. Harden is an associate professor in the Department of Human Nutrition, Foods,
and Exercise at Virginia Tech. She developed the initial concept for this project, was a major
contributor to the ethnographic-theoretical dialogue throughout data collection and analysis, and
provided vital feedback in the content and design of the manuscript, tables, and figures.
Manuscript 3
Susan Chen, MS, is a PhD candidate in the Department of Human Nutrition, Foods, and Exercise
at Virginia Tech. She analyzed qualitative data, generated ideas and interpretations for
discussion, and contributed to editing the manuscript.
Rachel Nelson, MS, is a PhD student in the Department of Human Nutrition, Foods, and
Exercise at Virginia Tech. She analyzed qualitative data, generated ideas and interpretations for
discussion, and contributed to editing the manuscript.
Dr. Vivica I. Kraak is an assistant professor in the Department of Human Nutrition, Foods, and
Exercise at Virginia Tech. She contributed as a third critical friend during data analysis to
resolve different interpretations of the findings, and facilitated the manuscript preparation and
editing process
Dr. Samantha M. Harden is an associate professor in the Department of Human Nutrition, Foods,
and Exercise at Virginia Tech. She facilitated designing the pilot trial, managing and analyzing
data, and editing the manuscript.
vii
Table of Contents
Academic Abstract……………………………………………………………………….….
General Abstract………………………………………………………………………….....
Dedication…………………………………………………………………………………...
Acknowledgements……………………………………………………………………….…
Attributions……………………………………………………………………………….....
Table of Contents……………………………………………………………………….…...
List of Appendices…………………………………………………………………….…….
List of Figures and Tables…………………………………………………………….…….
List of Abbreviations………………………………………………………………….…….
Introduction………………………………………………………………………………….
Manuscript 1…………………………………………………………………………………
Manuscript 2………………………………………………………………………………...
Manuscript 3…………………………………………………………………………………
Report……………………………………………………………………………………......
Conclusion…………………………………………………………………………………...
ii
iii
iv
v
vi
vii
viii
ix
x
1
16
34
78
120
164

viii
List of Appendices
Manuscript 1:
Appendix A: IRB Exemption Letter………………………………………….….………
Appendix B: Prenatal Yoga Flyer………………………………………………..………
Appendix C: Mom Expo Flyer…………………………………………………….…….
Appendix D: Mom Expo Invitation/Postcard………………………………………..…..
Appendix E: Mom Expo Poster with Schedule……………………………………….…
Appendix F: Mom Expo Educator Survey………………………………………………
Appendix G: Mom Expo Attendee Comment Card…………………………………......
Appendix H: Mom Expo Observational Log……………………………………………
Manuscript 2:
Appendix I: IRB Approval Letter……………………………………………………….
Appendix J: Standards for Reporting Qualitative Research Checklist………………….
Manuscript 3:
Appendix K: IRB Approval Letter………………………………..…………………….
Appendix L: FUEL Program Development…………………………………….……….
Appendix M: Data Collection Tools including Surveys, Scripts, and Logs…….………
Appendix N: FUEL Infographic Repository…………………………………….………
Appendix O: Detailed Reach Results…………………………………………….……..
167
168
169
170
171
172
173
174
175
176
179
180
187
205
206
ix
List of Figures and Tables
Introduction
Figure 1: Three components of the dissertation…………………………………………………….
Table 1: Overview of dissertation…………………………………………………………………..
Manuscript 1
Figure 1: Applying the RE-AIM framework to a perinatal health fair……………………….…….
Table 1: Timeline of participatory actions to plan, implement, and evaluate the event……..……..
Table 2: Seminar characteristics and attendance……………………………………………..…….
Table 3: Mom Expo effectiveness: comment card feedback from attendees………………..…….
Table 4: Problems and solutions to hosting a maternal health fair…………………………..…….
Manuscript 2
Figure 1: Autoethnography: Informing implementation processes and capturing
implementation outcomes…………………………………………………………………….……..
Figure 2: Restorying the plot and setting of the IRPP, July 2018-July 2019……………………....
Figure 3: IRPP model, member description, and process…………………………………….……
Figure 4: Themes of the researcher lived experience……………………………………………...
Figure 5: Frames of reflection within the autobiography……………………………………….….
Table 1: Results of the ethnographic-theoretical dialogue…………………………………….…...
Table 2: Reporting trustworthiness of qualitative data based on Guba and Lincoln’s criteria.……
Table 3: Potential benefits of recognizing and clarifying ontological and epistemological
paradigms……………………………………………………………………………………..……..
Manuscript 3
Figure 1: Pilot test study procedure………………………………………………………………..
Figure 2: Recruitment strategy reach to individuals who enrolled in the FUEL program or
waitlist…………………………………………………………….…………………………………
Figure 3: Implementation of the FUEL program…………………………………………………..
Figure 4: Core components of the FUEL program and how to effectively coach D&I
researchers……………………………………………………………………………….…….….....
Figure 5: Triangulating multisource data to identify promising, convergent lines of evidence
for future research on the FUEL program’s effectiveness……………………………….………....
Table 1: Strategies to fortify trustworthiness of FUEL qualitative approach and analysis.………..
Table 2: Characteristics of participants…………………………………………………….………
Table 3: Qualitative findings and codebook for participants’ open-ended responses……….……..
Table 4: Qualitative findings and codebook for proxy semi-structured interviews………….…….
Table 5: Longitudinal means and standard deviations of self-reported psychological needs,
flourishing domains, sleep quality, physical activity level, and working hours………………….…
Report
Figure 1: Timeline of historical punctuations……………………………………………………...
Figure 2: Modes of inquiry: conventional science and phenomenology………………….…….…
Figure 3: Integrating phenomenology in health research……………………………………….….
Table 1: How phenomenologists describe phenomenology…………………………………….….
Table 2: Summary of answers to Parts 1, 2, and 3 questions………………………………….…...
3
9
23
21
22
25
27
41
44
46
53
59
62
58
60
85
90
93
101
102
89
91
107
110
99
123
129
136
131
143
x
List of Abbreviations
ACSM: American College of Sports Medicine
AMA: American Medical Association
BMPN: Balanced Measure of Psychological Needs Scale
D&I: Dissemination and Implementation
EIM: Exercise is Medicine
ERM: Effort Recovery Model
FI: Flourishing Index
FUEL: Focus, Unplug, Exercise Love
GRA: Graduate Research Assistant
GWG: Gestational Weight Gain
HWC: Health and Wellness Coaching Compendium
IRPP: Integrated Research Practice Partnership
L-CAT: Stanford Leisure-Time Categorical Item
MT-DIRC: Mentoring Training for Dissemination and Implementation Research in Cancer
NCAA: National Collegiate Athletic Association
NRMN: National Research Mentoring Network
PAGA: Physical Activity Guidelines for Americans
PE: Punctuated Equilibrium
PI: Principal Investigator
RCT: Randomized Controlled Trial
RE-AIM: Reach, Effectiveness, Adoption, Implementation, Maintenance
SDT: Self Determination Theory
SRQR: Standards for Reporting Qualitative Research
SQS: Sleep Quality Scale
1
Introduction
“Once one is beyond a certain level of commitment to the sport, life begins to seem an allegory
of rowing rather than rowing an allegory of life.”
--Stephen Kiesling, member of the 1980 U.S. Olympic Rowing Team
The Shell Game: Reflections on Rowing and the Pursuit of Excellence (1)
When I lifted my hand from the oar, a chunk of skin from my palm stayed on the wood.
Hours of training on an indoor rowing machine—an “erg”—had strengthened my legs,
conditioned my heart, and given me callouses. But, as rowers say, ergs don’t float: Propelling a
boat down a river requires connecting to water with a 12-foot oar in exact time with seven other
people while balancing a narrow, 60-foot shell through river currents, wind, flocks of geese, and
whatever else the universe serves that day. Fitness developed on the erg does not automatically
translate to victories in the boat.
Likewise, scientific discoveries in laboratories and clinical trials do not automatically
translate to health benefits in communities (2,3). Applying health innovations from controlled
research environments to real-world settings is notoriously challenging (2,4,5). To address the
translational challenge, Dissemination and Implementation (D&I) Science has emerged as the
study of “how evidence-based practices, interventions, and policies are translated to and used in
real-world settings like hospitals, schools, and communities” (6). D&I studies are generally
situated in the third stage of the National Institute of Health’s translational science spectrum
(7,8), but experts have recently called for D&I principles to be integrated in all stages of research
to improve public health impact (9). Examples of D&I principles include stakeholder
engagement (10–12), adaptation to specific contexts (9,13), and balancing internal and external
validity (3,10,11).
2
In the last 20 years (14), D&I researchers have developed hundreds of implementation
strategies (15,16), models (17,18), and theories (19–21). In addition, participatory (22,23) and
pragmatic research methods (24–26) have advanced local implementation of evidence-based
practices. However, population impact of health research is still limited (27), as demonstrated by
the persistent crisis of physical inactivity (28,29). Substantial evidence links physical inactivity
to increased risk of chronic disease (30,31) and physical activity to decreased mortality risk
(32,33). In addition, meta-analyses of high quality randomized controlled trials (RCTs)
demonstrate that behavior change interventions can increase immediate and long-term physical
activity among adults (34,35). However, despite the preponderance of empirical evidence and
efficacious interventions, three out of four adults in the United States do not meet the Physical
Activity Guidelines for Americans (PAGA) (36), and 24% of adults in Virginia are physically
inactive (37). Given the persistence of this “wicked” (38,39) research-practice gap, what is
missing within D&I approaches and what can we do about it? In other words, how can we row
the health promotion boat down the community river?
To answer these questions, the initial purpose of this doctoral work was to investigate
novel D&I methods for increasing physical activity among pregnant women in community
settings. Based on my observations and experiences in the field, the work expanded to examine
scientific paradigms and daily practices of D&I researchers. In this dissertation, I present the
evolution of this work in a series of three manuscripts and one report (see Table 1 below).
3
Table 1: Overview of dissertation
Manuscript Title Publication Status
Manuscript 1 Mom Expo: Bridging the Gap Between Local
Women and Perinatal Resources
In press, The Journal of
Perinatal Education
Manuscript 2 Adjust your own oxygen mask before helping those
around you: An autoethnography of participatory
research
Published, September 2020
in Implementation Science
(40)
Manuscript 3 Fueling Dissemination and Implementation
researchers: Pilot test findings and RE-AIM
evaluation of an individualized coaching program
To be submitted,
Implementation Science
Communications
Report Phenomenology: (Re)Search for Meaning in
Behavioral and Community Health
Foundational literature
review, analysis,
recommendations, and
course syllabus
Manuscript 1: Development, implementation, and evaluation of Mom Expo
The development and evaluation of a perinatal health fair unexpectedly emerged from an
initial focus on conducting a randomized controlled trial (RCT) to inform the adaptation of a
gestational weight gain control program called HEART (Healthy Eating and Activity Readiness
for Two) (41). Six months of hospital red tape and four months of input from local women who
attended free prenatal yoga classes inspired the decision to pivot from the gestational weight gain
control program to a one-day health fair reflecting priorities articulated by expectant mothers
themselves. These priorities centered around emotional support and human connection, aligning
with research indicating the need for perinatal programs that address the non-physical demands
of pregnancy (42–44) that influence health behaviors (45), birth outcomes (46), and child
development (47,48).
To that end, the goal of the health fair was to empower, connect, and educate local
parents by connecting them to regional health care providers and holistic perinatal resources.
Pragmatic (11) measures based on the RE-AIM (reach, effectiveness, adoption, implementation,
maintenance) Framework (49,50) indicate that the health fair was a small but pivotal step in
bridging the gap between rural women and local perinatal resources. The “bridges” and social

4
infrastructure initiated through the health fair have developed into a nonprofit organization
dedicated to maternal health in Southwest Virginia.
Overall, this study is significant in four ways. First, the Mom Expo established the
foundation for sustainable perinatal support through a nonprofit organization. Second, the study
expanded the application of the RE-AIM Framework to the novel domain of health fair
evaluation. Third, the implementation process revealed actionable participatory strategies for
developing and implementing community-based health fairs. And, fourth, the study
demonstrated the power of authentic relationship building to translate science into real-world
programs.
Manuscript 2: Autoethnography of an Integrated Research Practice Partnership
As HEART evolved into the Mom Expo from July 2018 to July 2019, I conducted a 12-
month autoethnography of an integrated research practice partnership (IRPP) (22). As a novel
implementation model, the purpose of the IRPP was to connect women with the support and
resources they need during pregnancy and beyond. As a novel implementation method, the
purpose of the autoethnography was to unpack the “black box” of implementation (51),
particularly professional, practical, and personal hindrances to advancing D&I research (52,53).
An innovative component of the autoethnography was the use of restorying (54) to analyze and
report the implementation process. Restorying is an untapped method within D&I Science and
involves chronologically analyzing and presenting data through narrative with literary elements
including setting, characters, plot, conflict, theme, and resolution (54).
In conducting the autoethnography, I realized that novel implementation models and
methods are not enough to advance D&I Science: A deeper philosophical shift away from (post)
5
positivist paradigms (55–57) may be necessary. This shift centers on recognizing and leveraging
researcher situatedness (58) as an inherent and pivotal component of bridging the research-
practice gap. Strategies for leveraging this situatedness include (a) iterative critical reflection
particularly of ontological or epistemological underpinnings that constrain D&I work, (b)
evidence-based restorative practices to optimize researchers’ well-being and performance, and
(c) personal presence as a vehicle for translating science into real-world settings.
The combination of pragmatic strategies and philosophical arguments makes this study
unique. By rigorously combining third-person observation, first-person critical reflection, and
interdisciplinary theoretical dialogue (59), the autoethnographic process unveiled individual and
collective blind spots and generated strategies for addressing those blind spots. The
autoethnography offers a new perspective in embracing the “chaos” (20) and inherently
uncontrollable nature of D&I research instead of forcing it into scientific paradigms that work for
other tiers in the translational science spectrum.
Manuscript 3: Pilot study of a coaching program for D&I researchers
Building on findings from the autoethnography, I decided to develop and pilot test a
coaching program for D&I researchers. Michael Phelps has a coach. Oprah Winfrey has a
coach. Luciano Pavarotti had a coach. Why not D&I researchers? After all, in his 2013 TED
talk, Bill Gates stated, “Everyone needs a coach” (60).
Research indicates that workplace (“executive”) coaching (61) and health coaching (62)
are associated with positive outcomes related to well-being, performance, and quality of life.
However, there is a lack of detail about the design and implementation of coaching programs
(63). Moreover, there appears to be no research on coaching researchers themselves: Would

6
D&I researchers even enroll in a coaching program? Is coaching D&I researchers across the
nation feasible? What experiences and longitudinal effects are associated with the coaching
program?
To explore these questions, I applied D&I principles (10,64) to design and pilot test
FUEL (focus, unplug, exercise, love), a one-on-one, virtual coaching program for D&I
researchers. For example, program design included premortem brainstorming meetings with
stakeholders (15,65), and the RE-AIM Framework was used throughout all phases of the pilot
study to balance internal and external validity (24,49,50). For the effectiveness and maintenance
dimensions of RE-AIM, our research team emphasized longitudinal, qualitative data to capture
the full range of participants’ experiences, including ineffable, hard-to-measure dimensions often
missed in quantitative approaches (66).
This pilot study provides convergent lines of preliminary, pragmatic evidence that a one-
on-one, virtual coaching program is feasible and valuable to D&I researchers. Findings
demonstrate that the core components or active ingredients (67) of a coaching program for D&I
researchers are a transformative coach, compelling content, and individualized sessions.
Additional contributions to the field include (a) an evidence-based, dissemination-friendly
repository of infographics that other coaches or D&I researchers could use, (b) demonstration
that there is demand for coaching among researchers, including high-performing individuals, and
(c) presentation of implementation details, such as session content, that have not been reported in
previous coaching studies.

7
Report: Researching mechanism and meaning in the translational spectrum
While conducting the three previously introduced studies, I observed an inadequacy of
research approaches in capturing raw personal experiences related to behavioral and community
health. Participatory research, implementation, and coaching pivot on individual experience and
situated (58,68) meaning beyond the mechanistic outcomes and nomothetic findings favored in
conventional science (57,69–71). Conventional science, the current health research paradigm
which prioritizes research into mechanism or cause-and-effect (69), might miss or minimize the
critical dimension of meaning in real-world behaviors. To better connect science with
individuals’ daily lives we need another mode of inquiry that prioritizes the human in Human
Nutrition, Foods, and Exercise (HNFE). Phenomenology, the study of human meaning (72), is
one such mode.
Phenomenology emerged in European philosophy and literature in the 1900s (54,72,73)
and has been described as an attitude or style of thinking (74) to unearth the root of a
phenomenon beneath all assumptions—scientific or otherwise—in order to vividly describe the
concrete details of the now of a human experience (75,76). Phenomenology, like
autoethnography, is rare within implementation science (77) in which positivistic qualitative and
approaches are advocated (57,78). Phenomenological studies of chronic conditions such as
obesity appear to be increasing (79–81). However, experts question whether many of these
studies are truly phenomenological (82), and most health research focuses on the “corporeal”
body (the third-person object) instead of the “lived” body (the first-person experience)
(70,83,84).
To explore the potential of phenomenology in HNFE and the translational research
spectrum, I answer three questions in the report: Why are randomized controlled trials the gold

8
standard for physical activity research in behavioral and community health? What is
phenomenology? How can behavioral and community health researchers leverage the
transformative potential of phenomenology? The report also includes a syllabus for a graduate
course called Interdisciplinary Approaches to Health. Overall, this report is a critical piece of
this dissertation as an argument for integrating phenomenology into methods, paradigms, and
practices that drive D&I Science.
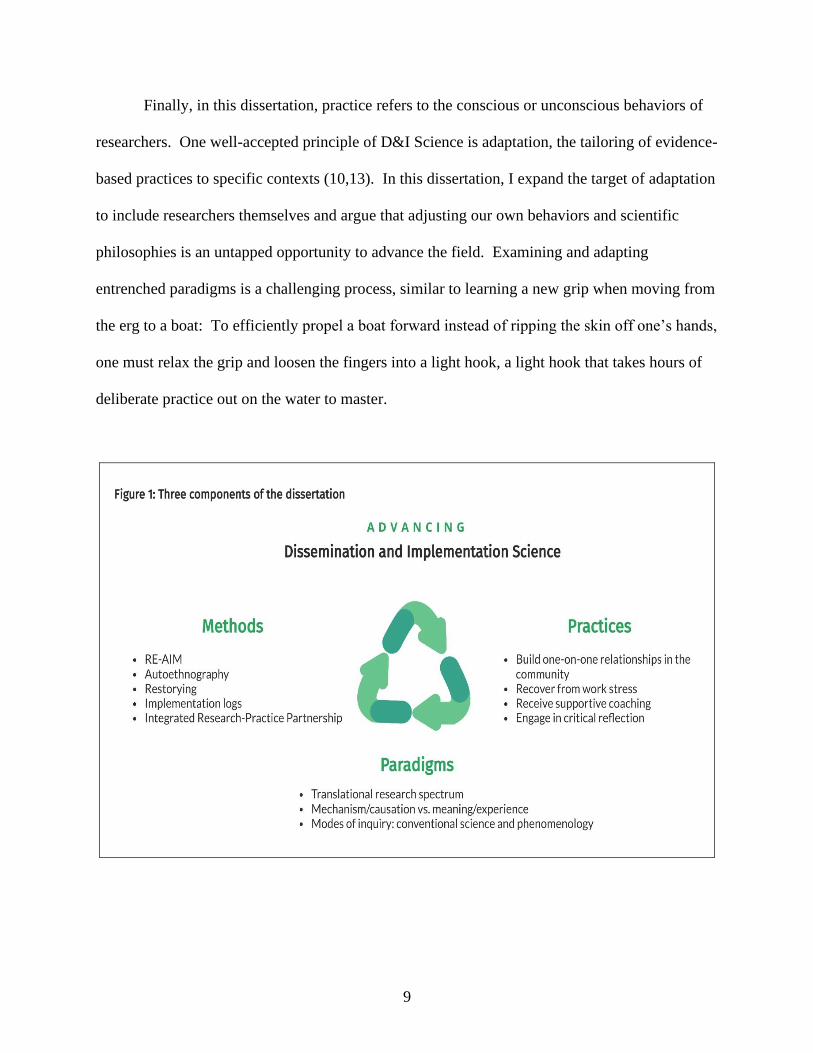
Summary
This dissertation is an examination of methods, paradigms, and practices for bridging the
research-practice gap (see Figure 1 below). The three studies presented in this dissertation share
an emphasis on pragmatic, qualitative, interdisciplinary methods. Pragmatic methods are
characterized by prioritizing the issues that matter most to stakeholders and employing measures
that are feasible and actionable in real-world settings (11,25). Qualitative methods capture
multidimensional implementation contexts, processes, and outcomes (78), as well as nuanced,
subjective experiences (54) that influence health and science translation (51,85). Finally,
interdisciplinary methods integrate constructs and approaches from various fields and are
recommended for complex problem-solving (86,87).
Compared to methods which are explicitly trained through graduate coursework,
paradigms appear unexamined. Seminal historian Thomas Kuhn defined paradigms as
“universally recognized scientific achievements that, for a time, provide model problems and
solutions for a community of practitioners”(88). For example, the paradigm of conventional or
natural science in medical research is based on the advancements of Rene Descartes, Isaac
Newton, and Auguste Comte (57,69,89).
9
Finally, in this dissertation, practice refers to the conscious or unconscious behaviors of
researchers. One well-accepted principle of D&I Science is adaptation, the tailoring of evidence-
based practices to specific contexts (10,13). In this dissertation, I expand the target of adaptation
to include researchers themselves and argue that adjusting our own behaviors and scientific
philosophies is an untapped opportunity to advance the field. Examining and adapting
entrenched paradigms is a challenging process, similar to learning a new grip when moving from
the erg to a boat: To efficiently propel a boat forward instead of ripping the skin off one’s hands,
one must relax the grip and loosen the fingers into a light hook, a light hook that takes hours of
deliberate practice out on the water to master.
10
References
1. Kiesling S. The Shell Game: Reflections on Rowing and the Pursuit of Excellence.
Ashland, OR: Nordic Knight Press; 1982.
2. Glasgow RE, Vinson C, Chambers D, Khoury MJ, Kaplan RM, Hunter C. National
institutes of health approaches to dissemination and implementation science: Current and
future directions. Am J Public Health. 2012;102(7):1274–81.
3. Bauer MS, Damschroder L, Hagedorn H, Smith J, Kilbourne AM. An introduction to
implementation science for the non-specialist. BMC Psychol. 2015;3(1):1–12.
4. Colditz GA. The Promise and Challenges of Dissemination and Implementation Research.
In: Brownson RC, Colditz GA, Proctor EK, editors. Dissemination and Implementation
Research in Health. New York, New York: Oxford University Press; 2012. p. 3–22.
5. Koorts H, Eakin E, Estabrooks P, Timperio A, Salmon J, Bauman A. Implementation and
scale up of population physical activity interventions for clinical and community settings:
the PRACTIS guide. Int J Behav Nutr Phys Act. 2018;15(51):1–11.
6. National Institutes of Health. Dissemination and Implementation (D&I) Research
[Internet]. [cited 2020 Aug 3]. Available from: https://prevention.nih.gov/research-
priorities/dissemination-implementation
7. Fort D, Herr T, Shaw P, Gutzman K, Starren J. Mapping the evolving definitions of
translational research. J Clin Transl Sci. 2017;1(01):60–6.
8. National Institutes of Health. Translational Science Spectrum [Internet]. 2020 [cited 2020
Apr 19]. Available from: https://ncats.nih.gov/translation/spectrum
9. Leppin AL, Mahoney JE, Stevens KR, Bartels SJ, Baldwin L, Dolor RJ, et al. Situating
dissemination and implementation sciences within and across the translational research
spectrum. J Clin Transl Sci. 2020;1–7.
10. Shelton RC, Lee M, Brotzman LE, Wolfenden L, Nathan N, Wainberg ML. What Is
Dissemination and Implementation Science? An Introduction and Opportunities to
Advance Behavioral Medicine and Public Health Globally. Int J Behav Med.
2020;27(1):3–20.
11. Glasgow R. What does it mean to be pragmatic? Pragmatic methods, measures, and
models to facilitate research translation. Heal Educ Behav. 2013;40(3):257–65.
12. World Health Organisation. A guide to implementation research in the prevention and
control of noncommunicable diseases [Internet]. World Health Organization. Geneva;
2016. Available from:
https://apps.who.int/iris/bitstream/handle/10665/252626/9789241511803-eng.pdf
13. Chambers D, Norton W. The Adaptome: Advancing the Science of Intervention
Adaptation. Am J Prev Med. 2016;51(4):S124–31.
14. Balas E, Boren S. Managing Clinical Knowledge for Health Care Improvement. Yearb
Med Inform [Internet]. 2000;1–6. Available from:
https://www.researchgate.net/requests/r5260046%5Cnpapers2://publication/uuid/40C2169
E-E9BA-4CF7-BCA1-341DF13AA04E
15. Powell BJ, Waltz TJ, Chinman MJ, Damschroder LJ, Smith JL, Matthieu MM, et al. A
refined compilation of implementation strategies: Results from the Expert
Recommendations for Implementing Change (ERIC) project. Implement Sci.
2015;10(1):1–14.
16. Leeman J, Birken SA, Powell BJ, Rohweder C, Shea CM. Beyond “implementation
11
strategies”: Classifying the full range of strategies used in implementation science and
practice. Implement Sci. 2017;12(1):1–9.
17. Tabak RG, Khoong EC, Chambers D, Brownson RC. Models in dissemination and
implementation research: useful tools in public health services and systems research. Am J
Prev Med. 2012;43(3):337–50.
18. ACCORDS Dissemination and Implementation Science Program, Dissemination and
Implementation Research Core D and ISC. Dissemination & Implementation Models in
Health Research & Practice [Internet]. [cited 2020 Oct 27]. Available from:
https://dissemination-implementation.org/content/diMain.aspx
19. Nilsen P. Making sense of implementation theories, models and frameworks. Implement
Sci. 2015;10(1):1–13.
20. Damschroder LJ. Clarity out of chaos: Use of theory in implementation research.
Psychiatry Res. 2019;283(June 2019).
21. Davidoff F. Understanding contexts: how explanatory theories can help. Implement Sci.
2019;14(1):1–9.
22. Estabrooks PA, Harden SM, Almeida FA, Hill JL, Johnson SB, Porter GC, et al. Using
Integrated Research-Practice Partnerships to Move Evidence-Based Principles into
Practice. Exerc Sport Sci Rev. 2019;47(3):176–87.
23. Harden SM, Johnson SB, Almeida FA, Estabrooks PA. Improving physical activity
program adoption using integrated research-practice partnerships: an effectiveness-
implementation trial. Transl Behav Med. 2017;7(1):28–38.
24. Harden SM, Smith ML, Ory MG, Smith-Ray RL, Estabrooks PA, Glasgow RE. RE-AIM
in Clinical, Community, and Corporate Settings: Perspectives, Strategies, and
Recommendations to Enhance Public Health Impact. Front Public Heal [Internet].
2018;6(March):1–10. Available from:
http://journal.frontiersin.org/article/10.3389/fpubh.2018.00071/full
25. Zuidgeest M, Goetz I, Groenwold R, Irving E, van Thiel G, Grobbe D. Series: Pragmatic
trials and real world evidence: Paper 1. Introduction. J Clin Epidemiol. 2017;88:7–13.
26. Thorpe KE, Zwarenstein M, Oxman AD, Treweek S, Furberg CD, Altman DG, et al. A
pragmatic-explanatory continuum indicator summary (PRECIS): a tool to help trial
designers. J Clin Epidemiol [Internet]. 2009;62(5):464–75. Available from:
http://dx.doi.org/10.1016/j.jclinepi.2008.12.011
27. Glasgow RE, Huebschmann AG, Brownson RC. Expanding the CONSORT Figure:
Increasing Transparency in Reporting on External Validity. Am J Prev Med [Internet].
2018;55(3):422–30. Available from: http://dx.doi.org/10.1016/j.amepre.2018.04.044
28. Kohl HW, Craig CL, Lambert EV, Inoue S, Alkandari JR, Leetongin G, et al. The
pandemic of physical inactivity: Global action for public health. Lancet.
2012;380(9838):294–305.
29. Reis RS, Salvo D, Ogilvie D, Lambert E V, Goenka S, Brownson RC. Scaling up physical
activity interventions across the globe: stepping up to larger and smarter approaches to get
people moving. Lancet [Internet]. 2016;388(10051):1337–48. Available from:
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5193005/pdf/nihms837989.pdf
30. Booth F, Roberts C, Laye M. Lack of exercise is a major cause of chronic diseases. Compr
Physiol. 2012;2(2):1143–211.
31. Lee IM, Shiroma EJ, Lobelo F, Puska P, Blair SN, Katzmarzyk PT, et al. Effect of
physical inactivity on major non-communicable diseases worldwide: An analysis of

12
burden of disease and life expectancy. Lancet. 2012;380(9838):219–29.
32. Arem H, Moore SC, Patel A, Hartge P, Berrington De Gonzalez A, Visvanathan K, et al.
Leisure time physical activity and mortality: A detailed pooled analysis of the dose-
response relationship. JAMA Intern Med. 2015;175(6):959–67.
33. Oja P, Kelly P, Pedisic Z, Titze S, Bauman A, Foster C, et al. Associations of specific
types of sports and exercise with all-cause and cardiovascular-disease mortality: a cohort
study of 80 306 British adults. Br J Sports Med. 2017;51(10):812–7.
34. Howlett N, Trivedi D, Troop NA, Chater AM. Are physical activity interventions for
healthy inactive adults effective in promoting behavior change and maintenance, and
which behavior change techniques are effective? A systematic review and meta-analysis.
Transl Behav Med. 2019;9(1):147–57.
35. Love R, Adams J, van Sluijs EMF, Foster C, Humphreys D. A cumulative meta-analysis
of the effects of individual physical activity interventions targeting healthy adults. Obes
Rev. 2018;19(8):1164–72.
36. Centers for Disease Control and Prevention. Trends in Meeting the 2008 Physical Activity
Guidelines, 2008-2018 [Internet]. Atlanta, GA; 2018. Available from:
https://www.cdc.gov/physicalactivity/downloads/trends-in-the-prevalence-of-physical-
activity-508.pdf
37. Centers for Disease Control and Prevention. Adult Physical Inactivity Prevalence Maps by
Race/Ethnicity [Internet]. Atlanta, GA; 2020 [cited 2020 Oct 27]. Available from:
https://www.cdc.gov/physicalactivity/data/inactivity-prevalence-maps/index.html
38. Rittel H, Webber M. Dilemmas in a General Theory of Planning. Policy Sci. 1973;155–
69.
39. Brown V. Tackling Wicked Problems Through the Transdisciplinary Imagination. Harris
J, Russell J, editors. London: Earthscan; 2010.
40. Steketee A, Archibald T, Harden S. Adjust your own oxygen mask before helping those
around you: An autoethnography of participatory research. Implement Sci. 2020;15(70).
41. Harden S, Beauchamp M, Pitts B, Nault E, Davy B, You W, et al. Group-based lifestyle
sessions for gestational weight gain management: a mixed method approach. Am J Health
Behav [Internet]. 2014;38(4):560–9. Available from:
http://ovidsp.ovid.com/ovidweb.cgi?T=JS&PAGE=reference&D=emed16&NEWS=N&A
N=613394541
42. Hall PJ, Foster JW, Yount KM, Jennings BM. Keeping it together and falling apart:
Women’s dynamic experience of birth. Midwifery [Internet]. 2018;58(July 2017):130–6.
Available from: https://doi.org/10.1016/j.midw.2017.12.006
43. Brady V, Lalor J. Space for human connection in antenatal education: Uncovering
women’s hopes using Participatory Action Research. Midwifery [Internet].
2017;55(January 2016):7–14. Available from:
http://dx.doi.org/10.1016/j.midw.2017.08.006
44. Racine N, Plamondon A, Hentges R, Tough S, Madigan S. Dynamic and Bidirectional
Associations Between Maternal Stress, Anxiety, and Social Support: The Critical Role of
Partner and Family Support. J Affect Disord [Internet]. 2019;252(December 2018):19–24.
Available from: https://linkinghub.elsevier.com/retrieve/pii/S0165032718332166
45. Quintanilha M, Mayan MJ, Raine KD, Bell RC. Nurturing maternal health in the midst of
difficult life circumstances: A qualitative study of women and providers connected to a
community-based perinatal program. BMC Pregnancy Childbirth. 2018;18(1):1–9.
13
46. Grigoriadis S, Graves L, Peer M, Mamisashvili L, Tomlinson G, Vigod S, et al. Maternal
Anxiety During Pregnancy and the Association with Adverse Perinatal Outcomes:
Systematic Review and Meta-Analysis. J Clin Psychiatry. 2018;79(5).
47. Gray SAO, Jones CW, Theall KP, Glackin E, Drury SS. Thinking Across Generations:
Unique Contributions of Maternal Early Life and Prenatal Stress to Infant Physiology. J
Am Acad Child Adolesc Psychol. 2018;56(11):922–9.
48. Bockting CLH, Molenaar NM, Hoogendijk WJG, El Marroun H, Hillegers MHJ, Tiemeier
H, et al. Prenatal maternal psychopathology and stress and offspring HPA axis function at
6 years. Psychoneuroendocrinology [Internet]. 2018;99(July 2018):120–7. Available from:
https://doi.org/10.1016/j.psyneuen.2018.09.003
49. Glasgow R, Vogt T, Boles S. Evaluating the Public Health Impact of Health Promotion
Interventions: The RE-AIM Framework. Am J Public Health. 1999;89(9):1322–7.
50. Glasgow RE, Harden SM, Gaglio B, Rabin B, Smith ML, Porter GC, et al. RE-AIM
Planning and Evaluation Framework: Adapting to New Science and Practice With a 20-
Year Review. Front Public Heal. 2019;7(March).
51. Green CA, Duan N, Gibbons RD, Hoagwood KE, Palinkas LA, Albert G, et al.
Approaches to Mixed Methods Dissemination and Implementation Research: Methods,
Strengths, Caveats, and Opportunities. Adm Policy Ment Heal. 2015;42(5):508–23.
52. Oliver K, Kothari A, Mays N. The dark side of coproduction: Do the costs outweigh the
benefits for health research? Heal Res Policy Syst. 2019;17(1):1–10.
53. Koorts H, Naylor PJ, Laws R, Love P, Maple JL, van Nassau F. What hinders and helps
academics to conduct Dissemination and Implementation (D&I) research in the field of
nutrition and physical activity? An international perspective. Int J Behav Nutr Phys Act.
2020;17(1):7.
54. Creswell J, Poth C. Qualitative Inquiry & Research Design. Fourth Edi. Salmon H, editor.
Thousand Oaks, CA: SAGE Publications; 2018.
55. Greenhalgh T, Raftery J, Hanney S, Glover M. Research impact: A narrative review.
BMC Med [Internet]. 2016;14(1). Available from: http://dx.doi.org/10.1186/s12916-016-
0620-8
56. Guba E, Lincoln Y. Competing Paradigms in Qualitative Research. In: Denzin NK,
Lincoln YS, editors. Handbook of Qualitative Research [Internet]. SAGE Publications,
Inc.; 1994. p. 105–17. Available from:
http://steinhardtapps.es.its.nyu.edu/create/courses/3311/reading/10-guba_lincoln_94.pdf
57. Boulton R, Sandall J, Sevdalis N. The Cultural Politics of ‘Implementation Science.’ J
Med Humanit. 2020;41(3):379–94.
58. Neumann C, Neumann I. Uses of the Self: Two Ways of Thinking about Scholarly
Situatedness and and Method. Milen J Int Stud. 2015;43(3):798–819.
59. Pink S, Morgan J. Short-term ethnography: Intense routes to knowing. Symb Interact.
2013;36(3):351–61.
60. Gates B. Teachers Need Real Feedback. In TEDTalks; 2013. Available from:
https://www.youtube.com/watch?v=81Ub0SMxZQo
61. Jones RJ, Woods SA, Guillaume YRF. The effectiveness of workplace coaching: A meta-
analysis of learning and performance outcomes from coaching. J Occup Organ Psychol.
2016;89(2):249–77.
62. Sforzo GA, Kaye MP, Todorova I, Harenberg S, Costello K, Cobus-Kuo L, et al.
Compendium of the health and wellness coaching literature. Am J Lifestyle Med.
14
2018;12(6):1–12.
63. Hill B, Richardson B, Skouteris H. Do we know how to design effective health coaching
interventions: A systematic review of the state of the literature. Am J Heal Promot.
2015;29(5):e158–68.
64. Hull L, Goulding L, Khadjesari Z, Davis R, Healey A, Bakolis I, et al. Designing high-
quality implementation research: Development, application, feasibility and preliminary
evaluation of the implementation science research development (ImpRes) tool and guide.
Implement Sci. 2019;14(1):1–20.
65. Gilmartin H, Lawrence E, Leonard C, McCreight M, Kelley L, Lippmann B, et al.
Brainwriting Premortem: A Novel Focus Group Method to Engage Stakeholders and
Identify Preimplementation Barriers. J Nurs Care Qual. 2019;34(2):94–100.
66. Tooth JA, Nielsen S, Armstrong H. Coaching effectiveness survey instruments: Taking
stock of measuring the immeasurable. Coach An Int J Theory, Res Pract. 2013;6(2):137–
51.
67. Blase K, Fixsen DL. Core intervention components: identifying and operationalizing what
makes programs work. ASPE Res Br. 2013;(February):21.
68. Vannini P. Situatedness. In: Given LM, editor. The SAGE Encyclopedia of Qualitative
Research Methods [Internet]. Thousand Oaks, CA: SAGE Publications, Inc.; 2012. p.
815–6. Available from:
https://methods.sagepub.com/base/download/ReferenceEntry/sage-encyc-qualitative-
research-methods/n424.xml
69. Harney M. Naturalizing phenomenology - A philosophical imperative. Prog Biophys Mol
Biol [Internet]. 2015;119(3):661–9. Available from:
http://dx.doi.org/10.1016/j.pbiomolbio.2015.08.005
70. Svenaeus F. A Defense of the Phenomenological Account of Health and Illness. J Med
Philos (United Kingdom). 2019;44(4):459–78.
71. Scotland J. Exploring the philosophical underpinnings of research: Relating ontology and
epistemology to the methodology and methods of the scientific, interpretive, and critical
research paradigms. English Lang Teach. 2012;5(9):9–16.
72. Van Manen M. Phenomenology of Practice. New York, New York: Routledge; 2014.
73. Starks H, Brown Trinidad S. Choose Your Method: A Comparison of Phenomenology,
Discourse Analysis, and Grounded Theory. Qual Health Res [Internet].
2007;17(10):1372–80. Available from:
https://pdfs.semanticscholar.org/a317/738b3a28d7c2c1af03fd1e22f67058342781.pdf
74. Merleau-Ponty M. Phenomenology of Perception. C. Smith,. London: Routledge and
Kegan Paul; 1962.
75. Lingis A. What Is Given in Experience: The Phenomenological Account. Qual Health
Res. 2017;27(6):805–9.
76. Van Manen M. Phenomenology in Its Original Sense. Qual Health Res. 2017;27(6):810–
25.
77. Mcwilliam CL, Kothari A, Ward-griffin C, Forbes D, Leipert B, West S, et al. Evolving
the theory and praxis of knowledge translation through social interaction: a social
phenomenological study. Implement Sci. 2009;4(26):1–14.
78. Qualitative Research in Implementation Science (QUALRIS). Qualitative Methods In
Implementation Science. 2018; Available from:
https://cancercontrol.cancer.gov/IS/docs/NCI-DCCPS-ImplementationScience-
15
WhitePaper.pdf
79. Williams O, Annandale E. Obesity, stigma and reflexive embodiment: Feeling the
‘weight’ of expectation. Health. 2018;1–21.
80. Ueland V, Furnes B, Dysvik E, Rørtveit K. Living with obesity — existential experiences.
Int J Qual Stud Health Well-being [Internet]. 2019;14(1). Available from:
https://doi.org/10.1080/17482631.2019.1651171
81. Natvik E, Råheim M, Andersen JR, Moltu C. Living a successful weight loss after severe
obesity. Int J Qual Stud Health Well-being [Internet]. 2018;13(1). Available from:
https://doi.org/10.1080/17482631.2018.1487762
82. van Manen M. But is it phenomenology? Qual Health Res. 2017;27(6):775–9.
83. Davidsen AS. Phenomenological Approaches in Psychology and Health Sciences. Qual
Res Psychol. 2013;10(3):318–39.
84. Carel H. Phenomenology and its application in medicine. Theor Med Bioeth.
2011;32(1):33–46.
85. Williams T, Hunt E, Papathomas A, Smith B. Exercise is medicine? Most of the time for
most; but not always for all. Qual Res Sport Exerc Heal. 2017;10(4):441–56.
86. Choi B, Pak A. Multidisciplinarity, interdisciplinarity, and transdisciplinarity in health
research, services, education and policy: 1. Definitions, objectives, and evidence of
effectiveness. Clin Investig Med. 2006;29(6):351–64.
87. Boon M, van Baalen S, Groeneir M. Interdisciplinary expertise in medical practice:
Challenges of using and producing knowledge in complex problem-solving. Med Teach.
2019;41(6):668–77.
88. Kuhn TS. The Structure of Scientific Revolutions. Chicago: University of Chicago Press;
1962.
89. Wilson HJ. The myth of objectivity: Is medicine moving towards a social constructivist
medical paradigm? Fam Pract. 2000;17(2):203–9.

16
Manuscript 1
Mom Expo: Bridging the Gap between Local Women and Perinatal Resources
Steketee AM, Harden, SM. Mom Expo: Bridging the Gap between Local Women and Perinatal
Resources. The Journal of Perinatal Education. In press.

17
Abstract
The purpose of this project was to describe the implementation of a perinatal health fair intended
to connect local women to holistic resources. Researchers used participatory strategies to
develop the health fair with local women and perinatal educators. Researchers evaluated the
health fair using pragmatic measures based on the RE-AIM framework. Forty-two attendees
were reached, and 23 educators hosted booths and educational sessions. Feedback indicated
strong enthusiasm for future similar events. Nearly three-quarters of the time spent
implementing the health fair was devoted to building relationships within the community.
Overall, this project provides practical and empirical information to inform the planning,
implementation, and evaluation of perinatal health fairs that establish meaningful connection
between local women, perinatal educators, and health researchers.
Keywords
Perinatal, health fair, implementation, RE-AIM
18
Introduction
Pregnancy and parenthood alter nearly every aspect of a woman’s life (1), leading to
dynamic emotional, social, and physical shifts that can be overwhelming (2). Research indicates
that over three-quarters of pregnant women experience fears related to pregnancy and childbirth
(3). In addition, women in the perinatal period struggle with daily barriers to well-being
including physical changes and complications of pregnancy, conflicts in interpersonal
relationships, and work-related challenges (4).
Supporting women through these ongoing, fluctuating challenges is crucial because
exposure to maternal psychological stress and anxiety has long-term ramifications for both the
woman and child (5,6). Social support may help prevent maternal stress (7), and many women
in the perinatal period experience an intense longing for authentic human connection (8). This
desire for human connection may explain expectant parents’ preference for face-to-face prenatal
education (9) that spans a wide-range of topics about pregnancy and parenthood (10). However,
there are significant gaps in perinatal support, as well as access to and awareness of that support
(10–12).
To address women’s social, emotional, and informational needs a holistic and
empowering approach to perinatal education is critical (1). Regional research (13–15) and direct
feedback from local perinatal care providers demonstrate the ongoing difficulty in reaching
expectant women in rural Virginia. A health fair is one untapped approach to address these
difficulties by connecting parents with a variety of perinatal educators at one time in one place.
Health fairs are “voluntary, community-based, cost-effective events” (16) that are designed to
reach underserved populations (17), such as pregnant or postpartum women. The aim of health
fairs is to increase awareness of health problems, promote healthy behaviors, and facilitate a

19
sense of connection between local individuals and healthcare providers, thereby generating
community empowerment (16,18).
Evidence-based guidelines for implementing a health fair are rare (19). There is a lack of
practical guidance for actionable strategies to establish a fair and scant literature on robust
methods for evaluating a fair (20). Therefore, researchers applied implementation science (21)
to plan and evaluate a health fair in Southwest Virginia. For planning, researchers leveraged
participatory strategies and stakeholder engagement (8,22,23) as recommended by the World
Health Organization (WHO) to improve local maternal health (24). For evaluation, researchers
employed an implementation framework called RE-AIM which was developed to translate
research into meaningful community outcomes (25,26). RE-AIM stands for reach, effectiveness,
adoption, implementation, and maintenance and has been applied to a variety of community,
clinical, and corporate settings in its 20-year history (27). It has not been applied to health fairs
and may be a pragmatic tool for optimizing the delivery and evaluation of perinatal education.
In this paper, we employ RE-AIM to describe the implementation and effectiveness of a
perinatal health fair. Findings include empirical outcomes, as well as actionable strategies that
can be adapted for health fairs in other communities. In conducting this project, researchers
strived to simultaneously serve their community and advance science.
Methods
Context and Planning
Conducted in rural, Southwest Virginia, this project emerged from an integrated research-
practice partnership (IRPP) (22) focused on local maternal well-being. Perinatal research and
projects related to the IRPP evolved over a decade (14,15) and indicated significant gaps
20
between women’s perceived perinatal needs and their access to support services related to those
needs.
To better understand local women’s perceptions, a yoga-certified graduate research
assistant (GRA) offered free prenatal yoga classes for 17 weeks (see Table 1 below). The
prenatal yoga classes were a vehicle for engaging stakeholders and giving local women a voice
in shaping the IRPP’s projects. The GRA and members of the IRPP promoted the yoga classes
through fliers and Facebook posts. The GRA taught the 75-minute yoga classes in a large,
carpeted conference room at a local medical research center. Before class, yoga participants
completed a Physical Activity Readiness Questionnaire. Yoga mats, straps, and blocks were
available for participants to use during each class.
After class, the GRA facilitated informal discussions about participants’ perinatal
experiences. Notably, the GRA’s role in the discussions was minimal with participants eagerly
sharing stories, recommendations, and hardships. Within these discussions, participants initiated
the idea of a one-day, family-friendly maternal health fair where individuals could interact with
local health care providers and perinatal educators without feeling as if they were part of a
research study.
Given this input, the GRA applied her extensive team-building experience as a collegiate
athletics coach to recruit local health care providers (“educators”) to participate in the health fair
(“mom expo”). The foundation of this recruiting was face-to-face networking and word-of-
mouth recommendations, similar to the recruitment strategies employed by athletics coaches.
Overall, the recruiting process emphasized developing interpersonal trust through conversations
at local coffee shops, walk-and-talks at local parks, and informal conversations via telephone and
text.

21
In addition to networking with individual educators, the GRA established partnerships
with a local library to co-host the event and with an existing, family-focused local organization
with 7,500 online followers. In conjunction with the local organizations, promotion for the mom
expo included online articles, emails to the organization’s followers, six television spots on local
channels, one radio interview on a local station, Facebook posts, Instagram posts, and fliers
posted at educators’ workplaces in addition to local gyms, preschools, libraries, and OB/GYN
offices.
Table 1: Timeline and hours of participatory actions to plan, implement, and evaluate the mom expo
Participatory Action (approximate hours of
GRA)
Jan. Feb. Mar. Apr. May June July Aug.
Gathering community input through prenatal yoga
classes (64). 16 16 20 12
Generating mom expo vision, intellectual/creative
tasks (37). 5 6 6 6 8 6
Recruiting educators (85). 14 18 16 13 14 10
Partnering and planning with local organizations
(60). 1 1 4 12 15 27
Promoting event through social media and local
t.v./radio (22). 2 4 4 4 8
Hosting the event including facility preparation
(16). 16
Evaluating the event (8). 8
Total time to plan, implement, and evaluate the
event (292) 292
Event Description
The mission of the mom expo was to empower, educate, and connect local women and
their partners to resources related to pregnancy, delivery, post-partum, and early parenthood.
The mom expo occurred on Saturday, July 27, 2019, at a local library from 10 am to 4 pm. The
mom expo was free to attend, but pre-registration was available through a local organization’s
website. The kick-off event from 10-10:45 am included a drum circle led by a certified music
therapist. From 11 am to 4 pm, educators and local organizations hosted information tables in
22
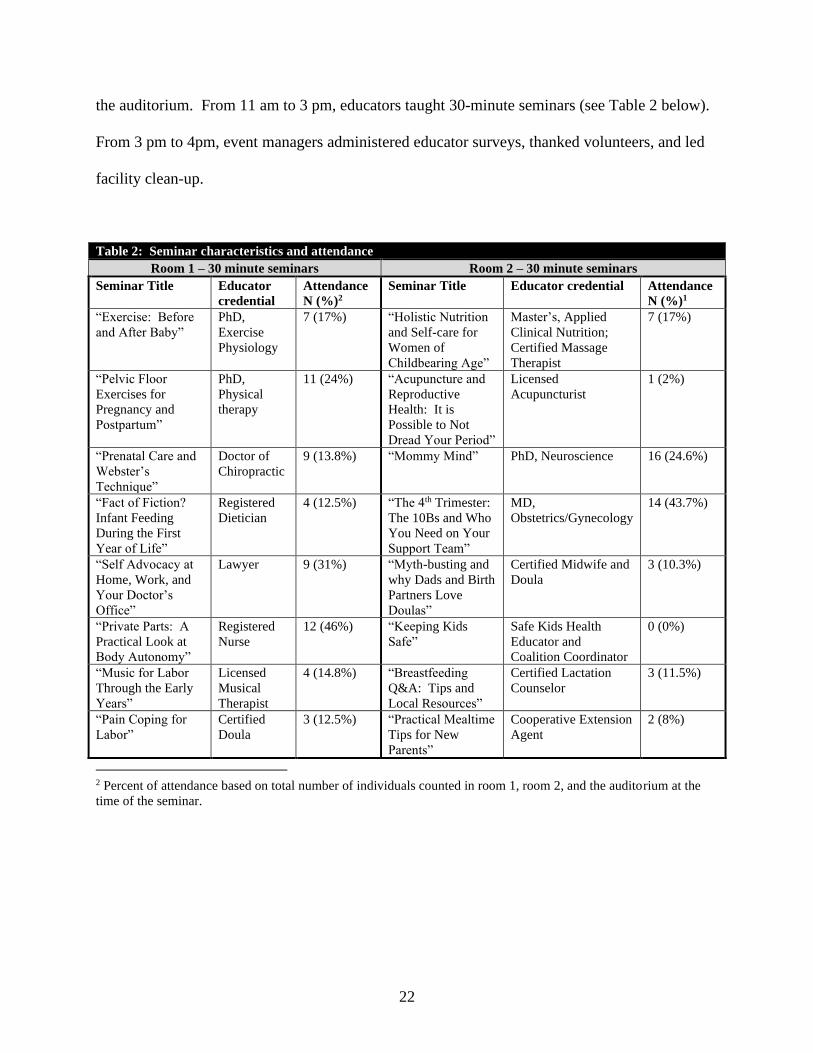
the auditorium. From 11 am to 3 pm, educators taught 30-minute seminars (see Table 2 below).
From 3 pm to 4pm, event managers administered educator surveys, thanked volunteers, and led
facility clean-up.
Table 2: Seminar characteristics and attendance
Room 1 – 30 minute seminars Room 2 – 30 minute seminars
Seminar Title Educator
credential
Attendance
N (%)2
Seminar Title Educator credential Attendance
N (%)1
“Exercise: Before
and After Baby”
PhD,
Exercise
Physiology
7 (17%) “Holistic Nutrition
and Self-care for
Women of
Childbearing Age”
Master’s, Applied
Clinical Nutrition;
Certified Massage
Therapist
7 (17%)
“Pelvic Floor
Exercises for
Pregnancy and
Postpartum”
PhD,
Physical
therapy
11 (24%) “Acupuncture and
Reproductive
Health: It is
Possible to Not
Dread Your Period”
Licensed
Acupuncturist
1 (2%)
“Prenatal Care and
Webster’s
Technique”
Doctor of
Chiropractic
9 (13.8%) “Mommy Mind” PhD, Neuroscience 16 (24.6%)
“Fact of Fiction?
Infant Feeding
During the First
Year of Life”
Registered
Dietician
4 (12.5%) “The 4th Trimester:
The 10Bs and Who
You Need on Your
Support Team”
MD,
Obstetrics/Gynecology
14 (43.7%)
“Self Advocacy at
Home, Work, and
Your Doctor’s
Office”
Lawyer 9 (31%) “Myth-busting and
why Dads and Birth
Partners Love
Doulas”
Certified Midwife and
Doula
3 (10.3%)
“Private Parts: A
Practical Look at
Body Autonomy”
Registered
Nurse
12 (46%) “Keeping Kids
Safe”
Safe Kids Health
Educator and
Coalition Coordinator
0 (0%)
“Music for Labor
Through the Early
Years”
Licensed
Musical
Therapist
4 (14.8%) “Breastfeeding
Q&A: Tips and
Local Resources”
Certified Lactation
Counselor
3 (11.5%)
“Pain Coping for
Labor”
Certified
Doula
3 (12.5%) “Practical Mealtime
Tips for New
Parents”
Cooperative Extension
Agent
2 (8%)
2 Percent of attendance based on total number of individuals counted in room 1, room 2, and the auditorium at the
time of the seminar.
23
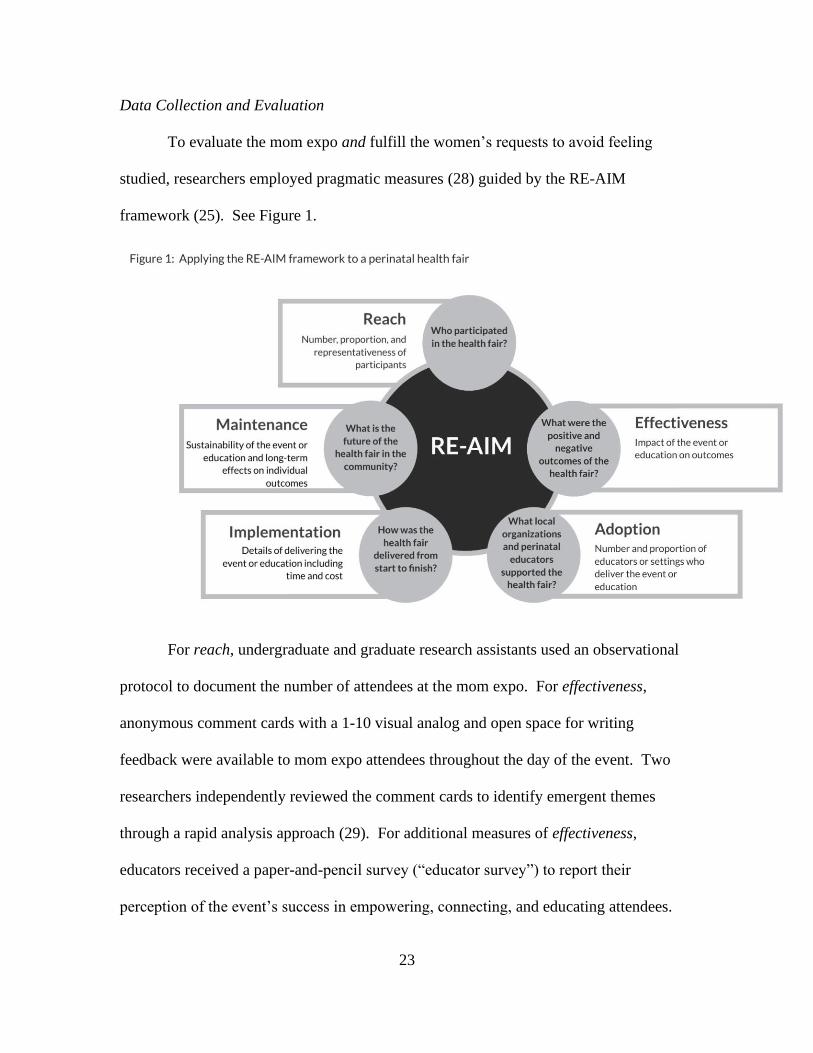
Data Collection and Evaluation
To evaluate the mom expo and fulfill the women’s requests to avoid feeling
studied, researchers employed pragmatic measures (28) guided by the RE-AIM
framework (25). See Figure 1.
For reach, undergraduate and graduate research assistants used an observational
protocol to document the number of attendees at the mom expo. For effectiveness,
anonymous comment cards with a 1-10 visual analog and open space for writing
feedback were available to mom expo attendees throughout the day of the event. Two
researchers independently reviewed the comment cards to identify emergent themes
through a rapid analysis approach (29). For additional measures of effectiveness,
educators received a paper-and-pencil survey (“educator survey”) to report their
perception of the event’s success in empowering, connecting, and educating attendees.

24
For adoption, the GRA maintained qualitative descriptions of educators and
organizations who agreed to participate. For implementation, the GRA maintained
fidelity checklists, a timeline, and expense reports. In addition, the educator survey
included measures of educators’ perceptions of the event’s implementation including
facility, location, publicity, atmosphere/energy, planning/organization leading up to the
event, management on the day of the event, overall experience, and suggestions for
improvements. For maintenance, the educator survey included one item on a 5-point
Likert scale (1= not likely, 5= very likely): “How likely are you to participate in Mom
Expo next year?”
Notably, data collection and evaluation were intended to fit seamlessly within the
mom expo to avoid disrupting attendees’ and/or educators’ experience. Likewise, data
collection did not include sensitive information. This project was Institutional Review
Board exempt.
Results
In this section, authors present results for each RE-AIM dimension. For reach,
116 community members preregistered for the mom expo, and 42 individuals attended
the event (see Table 2 above). Of those 42, 25 (59.5%) pre-registered and the remaining
17 (40.5%) were walk-ins. There are multiple appropriate denominators for determining
the proportion of the targeted population that attended. Using the approximate
membership (7,500) of the family-oriented organization who spearheaded online
promotions, the reach proportion was .0056. Using the 2018 number of live births of the
surrounding city and county (3,155), the reach proportion was .013. (30). Finally, using
the approximate number of prenatal patients (400) in local OBGYN clinics, the reach
25
proportion was .11. In terms of relative reach, the mom expo drew many more
participants than two free maternal health events hosted by other organizations in the
same summer. The other events reached 3 and 12 local women, respectively.
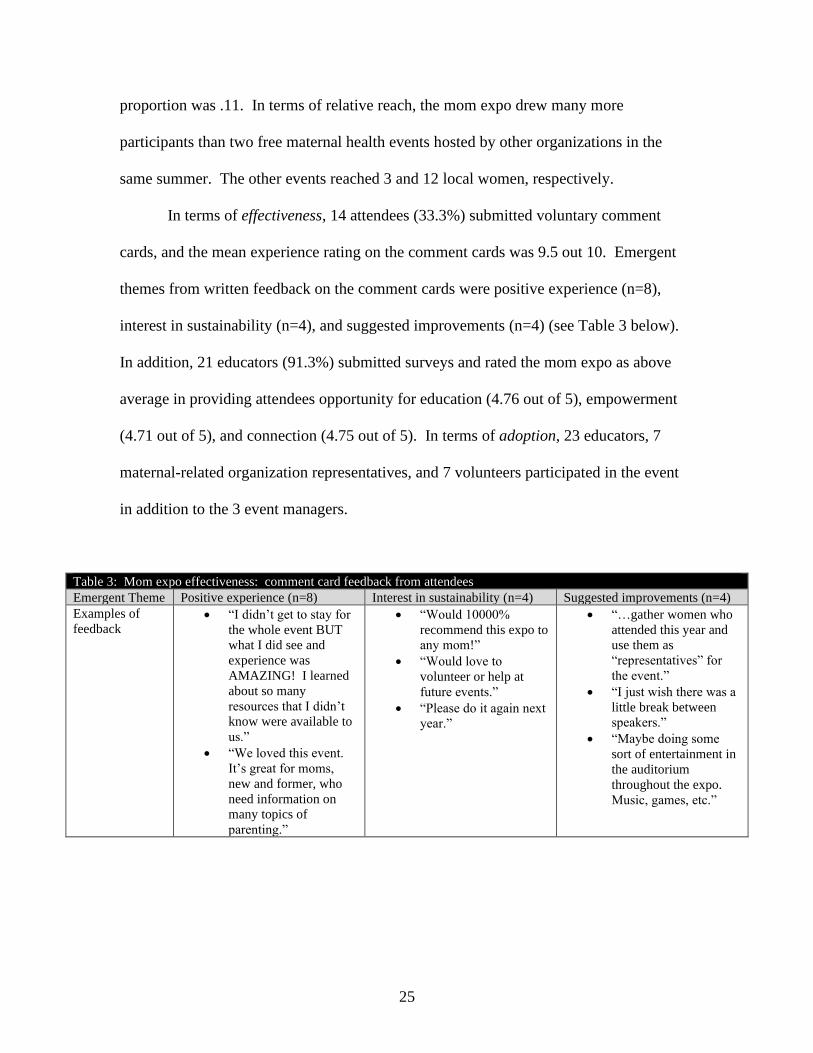
In terms of effectiveness, 14 attendees (33.3%) submitted voluntary comment
cards, and the mean experience rating on the comment cards was 9.5 out 10. Emergent
themes from written feedback on the comment cards were positive experience (n=8),
interest in sustainability (n=4), and suggested improvements (n=4) (see Table 3 below).
In addition, 21 educators (91.3%) submitted surveys and rated the mom expo as above
average in providing attendees opportunity for education (4.76 out of 5), empowerment
(4.71 out of 5), and connection (4.75 out of 5). In terms of adoption, 23 educators, 7
maternal-related organization representatives, and 7 volunteers participated in the event
in addition to the 3 event managers.
Table 3: Mom expo effectiveness: comment card feedback from attendees
Emergent Theme Positive experience (n=8) Interest in sustainability (n=4) Suggested improvements (n=4)
Examples of
feedback • “I didn’t get to stay for
the whole event BUT
what I did see and
experience was
AMAZING! I learned
about so many
resources that I didn’t
know were available to
us.”
• “We loved this event.
It’s great for moms,
new and former, who
need information on
many topics of
parenting.”
• “Would 10000%
recommend this expo to
any mom!”
• “Would love to
volunteer or help at
future events.”
• “Please do it again next
year.”
• “…gather women who
attended this year and
use them as
“representatives” for
the event.”
• “I just wish there was a
little break between
speakers.”
• “Maybe doing some
sort of entertainment in
the auditorium
throughout the expo.
Music, games, etc.”

26
For implementation, the GRA spent approximately 289 hours planning,
implementing, and evaluating the mom expo (see Table 1 above). The GRA dedicated
nearly three-quarters (72.3%) of those hours to direct interactions with community
members via face-to-face conversations and phone calls. Excluding person-hours, the
implementation cost of the mom expo was $1,003.44 including t-shirts, promotional
materials, and food on the day of the event. The library co-hosting the mom expo waived
the rental fee, and all educators and organizations volunteered their time. Educators rated
the planning/organization leading up to the event as excellent (5.0 out of 5) and the
management on the day of the event as above average (4.95 out of 5). Successful
implementation required on-going problem-solving (see Table 4 below).
In terms of maintenance, 100% of the educators who completed surveys indicated
that they are very likely (18) or likely (3) to participate in the mom expo next year. In
addition, attendees and educators who convened at the mom expo developed Huddle Up
Moms (HUM), a nonprofit organization hosting events and developing support groups.
Efforts of HUM continue to echo the mom expo mission of empowerment, education,
and connection.

27
Table 4: Problems and solutions to hosting a perinatal health fair
Potential Problem Potential Solution
Trademark of event
name. • Check the Trademark Electronic Search System on the United States Patent and
Trademark Office website.
• Leverage expertise of legal office of university or research institution.
Security at event. • Hire off-duty officer depending on number of attendees.
Facility comfort on
day of event. • Identify contact for air-conditioning/heating, restroom service, open/locked doors,
Internet access.
Breastfeeding needs. • Private space for breastfeeding, refrigeration for storing pumped breast milk.
Overwhelming
emails related to
event organization.
• Designate one person to send one group email update on a specific day each week (e.g.
every Thursday at 11 am).
• Use the same email format each week.
• Limit “to-do’s” to three action items (preferably two).
• Include a brief motivational image that reflects the mission or theme of the event; provide
contact information for individual questions or follow-up.
Nerves and confusion
among event staff. • Hold uplifting 15-minute “huddle” of all event staff on the morning of the event.
Concisely review key logistics.
• Highlight only three keys staff should remember, with one of those keys being whom
they should contact with emergencies/questions during the event.
Last minute absences
of educators. • Before the event, plan two back-up activities that can be substituted for original content.
Designate the leaders of the back-up plan.
Last minute absences
of event managers. • Share all documents (e.g. timelines, contact information, schedule) on Google Drive
among designated event managers.
Unannounced media
presence. • Before the event, determine which aspects of the event are appropriate for media and
designate two volunteers to interact with unplanned media presence.
Stroller accessibility. • Build in extra space for strollers when arranging tables and booths. Consider aisles and
free-standing chairs in auditoriums or large meeting spaces.
Issues with signs,
equipment, or
technology.
• Have registration tables and event signs at each facility entrance.
• Create toolbox of duct tape, masking tape, scotch tape, scissors, binder clips, pens,
markers, rubber bands, paper, USB port, Chlorox wipes, laptop, phone charger, camera
charger, safety pins.
• Create comfort kit of pain reliever, Tums, sanitary products, hair ties, band-aids, tissue,
etc.
Refreshments • Fuel staff by providing a meal and snacks on the day of the event.
• Personalize the meal, even in small ways such as adding individualized notes.
• Ensure that promotions accurately reflect refreshments/meals.
Commercialization
versus empowerment,
connection, and
education
• Host the event at a non-profit organization or community setting.
• Create, distribute, and review one-page event guide/expectations to the educators.
• Use the word “educator” not “vendor.”
• Select “educators” with specific expertise or service (i.e. not a product or brand).
• Require educators/staff to wear event t-shirt (i.e. not business/personal brand shirt) at the
mom expo.
• Host Meet & Greet activities for the educators to build cohesion and personal connection
with each other.
Lack of inclusivity • Use the words “parent(s)” and “partner(s).”
• On the one-page event guide and in educator/volunteer meetings, review open-
mindedness, inclusivity, and sensitivity to the many ways individuals become parents.
• Use inclusive graphics and colors on promotional materials.

28
Discussion
Based on the positive feedback from attendees and educators, the mom expo was
perceived as an effective vehicle for empowerment, education, and connection. The
mom expo reached 3 to 20 times more participants than other free perinatal health events
that summer, and the proportion of pre-registered individuals (22%) who actually
attended the mom expo aligned with other events promoted by the family-orientated
organization. However, the reach still fell below the IRPP’s aspirations. This difficulty
reaching pregnant and postpartum women reflects results of other perinatal research
conducted in this rural area (13) and may require novel approaches beyond generalities
described in current literature (16,17,19,20). For example, one attendee suggested on a
comment card that participants who attended this first mom expo could become “mom
ambassadors” in promoting the event to individuals they know. Another novel, untested
strategy for improving reach could be to generate connection between individuals who
pre-register for the event before the event. This pre-event connection could include
personalized reminders, phone calls, emails, and social media interactions, as well as
individualized invitations to participate in “ask anything” sessions with educators or even
pre-event prize drawings in which prizes are announced and drawn before the event but
must be retrieved at the event itself.
Overall, this project demonstrates the power of taking time to build meaningful
relationships between researchers and perinatal educators within the community.
Recruiting educators and building trust was time and energy intensive; however,
investing this socio-emotional energy in relationship building ended up saving money
and facilitating promotions. For example, after weeks of interactions, a library

29
administrator offered to waive the rental fee of over $800, and a prenatal yoga attendee
arranged promotional air time on a local television channel. Beyond cost savings, the
power of meaningful relationships is evident in the high adoption among educators and
volunteers. Furthermore, educators, volunteers, and women who met each other through
the mom expo are now establishing a non-profit organization as a long-term, sustainable,
local hub for holistic perinatal education, support, and connection.
Building relationships within participatory projects is an iterative, emotionally-
demanding process that belies typical empirical procedures and scientific skills (31).
Findings from this mom expo support the following actionable strategies related to
building authentic relationships and partnerships between researchers, perinatal
educators, and local women: First, members of a participatory project should carefully
choose their roles based on each member’s individual skills and capacities (32). For
example, the GRA tasked with bringing individuals together for the mom expo had 15-
years of team building experience as an athletics coach. Second, members of a
participatory project—including members who do not have networking roles—should
account for relationship building and local networking in research protocols, timelines,
discussions, etc. so that this pivotal aspect of community-based projects does not remain
invisible. Third, to manage conflicting academic and community workloads, members of
a participatory project can “batch” their responsibilities by focusing on one type of work
in a single block of time (33). For example, the GRA scheduled several email and phone
“blackout times” per week so that she could finish her academic/intellectual work without
the social “interruptions” that come with extensive relationship building. Fourth, when
actually doing the relationship building, members of a participatory project should initiate

30
contact in-person or via telephone (not email); spend more time listening than speaking;
meet in non-research settings like coffee shops or parks; match their word choice, body
language, and clothing to the meeting setting; offer appealing, free group activities—like
prenatal yoga—as natural opportunities to spend meaningful time with community
members; and intentionally shift one’s mindset from expertise and productivity to
empathy and presence.
Limitations and Future Directions
There are several limitations of this project. First, reach did not include
sociodemographic or health information, and effectiveness did not include behavioral or
physiological measures. When selecting pragmatic measures, researchers intentionally
prioritized the women’s requests to avoid feeling as if they were in a study over scientific
paradigms of more rigorous empirical methods. Second, measuring GRA hours was
complicated by overlapping tasks and the spontaneous, unpredictable nature of building
relationships within a participatory project. This type of community-driven work does
not fit neatly into traditional scientific paradigms of a priori protocols, linear processes,
and objective, measurable outcomes (31,32).
Third, one intended pragmatic measure—using LivePoll to gather demographics
and perceptions of participants at the mom expo—failed, further limiting data related to
attendee characteristics and experience. Future projects could leverage interactive
technology, such as LivePoll, to facilitate interpersonal connection and data collection at
perinatal health fairs. Future projects could also use RE-AIM in the planning stages, not
just the evaluation stages.
31
Implications for Practice
Despite these limitations, this participatory project is significant as a practically
feasible and empirically sound example of bridging the gap between rural women and
holistic perinatal support. This promising process can be replicated in other communities
in which perinatal educators and researchers establish partnerships to launch community
events planned and evaluated through the RE-AIM framework. The key to replication
will be devoting considerable time and energy to engaging stakeholders through authentic
relationship building. In this way, a perinatal health fair may be a vehicle for lasting
interpersonal connections that nurture holistic well-being and community change beyond
the research itself.
References
1. Fahey JO, Shenassa E. Understanding and meeting the needs of women in the
postpartum period: The perinatal maternal health promotion model. J Midwifery
Women’s Heal. 2013;58(6):613–21.
2. Hall PJ, Foster JW, Yount KM, Jennings BM. Keeping it together and falling
apart: Women’s dynamic experience of birth. Midwifery [Internet]. 2018;58(July
2017):130–6. Available from: https://doi.org/10.1016/j.midw.2017.12.006
3. Hanna-Leena Melender R. Experiences of Fears Associated with Pregnancy and
Childbirth: A Study of 329 Pregnant Women. Birth. 2003;29(2):101–11.
4. Quintanilha M, Mayan MJ, Raine KD, Bell RC. Nurturing maternal health in the
midst of difficult life circumstances: A qualitative study of women and providers
connected to a community-based perinatal program. BMC Pregnancy Childbirth.
2018;18(1):1–9.
5. Grigoriadis S, Graves L, Peer M, Mamisashvili L, Tomlinson G, Vigod S, et al.
Maternal Anxiety During Pregnancy and the Association with Adverse Perinatal
Outcomes: Systematic Review and Meta-Analysis. J Clin Psychiatry. 2018;79(5).
6. Madigan S, Oatley H, Racine N, Fearon P, Schumacher L, Akbari E, et al. A meta-
analysis of maternal prenatal depression and anxiety on child socioemotional
development. J Am Acad Child Adolesc Psychiatry. 2018;57(9):645–57.
7. Racine N, Plamondon A, Hentges R, Tough S, Madigan S. Dynamic and
Bidirectional Associations Between Maternal Stress, Anxiety, and Social Support:
The Critical Role of Partner and Family Support. J Affect Disord [Internet].
2019;252(December 2018):19–24. Available from:
32
https://linkinghub.elsevier.com/retrieve/pii/S0165032718332166
8. Brady V, Lalor J. Space for human connection in antenatal education: Uncovering
women’s hopes using Participatory Action Research. Midwifery [Internet].
2017;55(January 2016):7–14. Available from:
http://dx.doi.org/10.1016/j.midw.2017.08.006
9. Kovala S, Cramp AG, Xia L. Prenatal Education: Program Content and Preferred
Delivery Method From the Perspective of the Expectant Parents. J Perinat Educ.
2016;25(4):232–41.
10. Deave T, Johnson D, Ingram J. Transition to parenthood: The needs of parents in
pregnancy and early parenthood. BMC Pregnancy Childbirth. 2008;8:1–11.
11. Guerra-Reyes L, Christie VM, Prabhakar A, Siek KA. Mind the Gap: Assessing
the Disconnect Between Postpartum Health Information Desired and Health
Information Received. Women’s Heal Issues [Internet]. 2017;27(2):167–73.
Available from: http://dx.doi.org/10.1016/j.whi.2016.11.004
12. Tully KP, Stuebe AM, Verbiest SB. The fourth trimester: a critical transition
period with unmet maternal health needs. Am J Obstet Gynecol [Internet].
2017;217(1):37–41. Available from: http://dx.doi.org/10.1016/j.ajog.2017.03.032
13. deValpine MG, Jones M, Carpenter DB, Falk J. First Trimester Prenatal Care and
Local Obstetrical Delivery Options for Women in Poverty in Rural Virginia. J
Community Public Heal Nurs [Internet]. 2016;02(04):1–8. Available from:
http://www.omicsonline.org/open-access/first-trimester-prenatal-care-and-local-
obstetrical-delivery-options-for-womenin-poverty-in-rural-virginia-2471-9846-
1000137.php?aid=80513
14. Harden S, Beauchamp M, Pitts B, Nault E, Davy B, You W, et al. Group-based
lifestyle sessions for gestational weight gain management: a mixed method
approach. Am J Health Behav [Internet]. 2014;38(4):560–9. Available from:
http://ovidsp.ovid.com/ovidweb.cgi?T=JS&PAGE=reference&D=emed16&NEWS
=N&AN=613394541
15. Harden SM, Ramalingam NPS, Wilson KE, Evans-Hoeker E. Informing the
development and uptake of a weight management intervention for preconception:
A mixed-methods investigation of patient and provider perceptions. BMC Obes.
2017;4(1):1–12.
16. Dillon DL, Sternas K. Designing a successful health fair to promote individual,
family, and community health. J Community Health Nurs. 1997;14(1):1–14.
17. Murray K, Liang A, Barnack-Tavlaris J, Navarro AM. The Reach and Rationale
for Community Health Fairs. J Cancer Educ. 2014;29(1):19–24.
18. Ezeonwu M, Berkowitz B. A Collaborative Communitywide Health Fair: The
Process and Impacts on the Community. J Community Health Nurs.
2014;31(2):118–29.
19. Goldman KD, Schmalz KJ. Top Grade Health Fair: An “ A ” Fair to Remember.
Health Promot Pract. 2004;5(3):217–21.
20. Escoffery C, Liang S, Rodgers K, Haardoerfer R, Hennessy G, Gilbertson K, et al.
Process evaluation of health fairs promoting cancer screenings. BMC Cancer.
2017;17(1):1–12.
21. Bauer MS, Damschroder L, Hagedorn H, Smith J, Kilbourne AM. An introduction
to implementation science for the non-specialist. BMC Psychol. 2015;3(1):1–12.

33
22. Estabrooks PA, Harden SM, Almeida FA, Hill JL, Johnson SB, Porter GC, et al.
Using Integrated Research-Practice Partnerships to Move Evidence-Based
Principles into Practice. Exerc Sport Sci Rev. 2019;47(3):176–87.
23. Powell BJ, Waltz TJ, Chinman MJ, Damschroder LJ, Smith JL, Matthieu MM, et
al. A refined compilation of implementation strategies: Results from the Expert
Recommendations for Implementing Change (ERIC) project. Implement Sci.
2015;10(1):1–14.
24. World Health Organization. WHO Recommendations on Community Mobilization
Through Facilitated Participatory Learning and Action Cycles with Women’s
Groups For Maternal and Newborn Health [Internet]. Geneva, Switzerland; 2014.
Available from:
https://www.who.int/maternal_child_adolescent/documents/community-
mobilization-maternal-newborn/en/
25. Glasgow R, Vogt T, Boles S. Evaluating the Public Health Impact of Health
Promotion Interventions: The RE-AIM Framework. Am J Public Health.
1999;89(9):1322–7.
26. Glasgow RE, Harden SM, Gaglio B, Rabin B, Smith ML, Porter GC, et al. RE-
AIM Planning and Evaluation Framework: Adapting to New Science and Practice
With a 20-Year Review. Front Public Heal. 2019;7(March).
27. Harden SM, Smith ML, Ory MG, Smith-Ray RL, Estabrooks PA, Glasgow RE.
RE-AIM in Clinical, Community, and Corporate Settings: Perspectives, Strategies,
and Recommendations to Enhance Public Health Impact. Front Public Heal
[Internet]. 2018;6(March):1–10. Available from:
http://journal.frontiersin.org/article/10.3389/fpubh.2018.00071/full
28. Glasgow R. What does it mean to be pragmatic? Pragmatic methods, measures,
and models to facilitate research translation. Heal Educ Behav. 2013;40(3):257–
65.
29. Taylor B, Henshall C, Kenyon S, Litchfield I, Greenfield S. Can rapid approaches
to qualitative analysis deliver timely, valid findings to clinical leaders? A mixed
methods study comparing rapid and thematic analysis. BMJ Open.
2018;8(e019993):1–13.
30. Virginia Department of Health. Total live births by place of occurrence and place
of residence by race with resident live birth rates per 1,000 total projected
population by planning district and city or county [Internet]. 2018 [cited 2019 Aug
9]. Available from:
https://apps.vdh.virginia.gov/HealthStats/documents/pdf/birth_1-1_2018.pdf
31. Oliver K, Kothari A, Mays N. The dark side of coproduction: Do the costs
outweigh the benefits for health research? Heal Res Policy Syst. 2019;17(1):1–10.
32. Stoecker R. Are Academics Irrelevant? Am Behav Sci. 1999;42(5):840–54.
33. Newport C. Deep Work. New York, New York: Grand Central Publishing; 2016.

34
Manuscript 2
Adjust your own oxygen mask before helping those around you: An
autoethnography of participatory research
Steketee AM, Archibald TG, Harden, SM. Adjust your own oxygen mask before helping
those around you: An autoethnography of participatory research. Implement Sci.
2020;15(70).
© The Author(s). 2020 Open Access This article is licensed under a Creative Commons
Attribution 4.0 International License, which permits use, sharing, adaptation, distribution
and reproduction in any medium or format, as long as you give appropriate credit to the
original author(s) and the source, provide a link to the Creative Commons license, and
indicate if changes were made. The images or other third party material in this article are
included in the article's Creative Commons license, unless indicated otherwise in a credit
line to the material. If material is not included in the article's Creative Commons
license and your intended use is not permitted by statutory regulation or exceeds the
permitted use, you will need to obtain permission directly from the copyright holder. To
view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/.
The Creative Commons Public Domain Dedication waiver
http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in
this article, unless otherwise stated in a credit line to the data.
35
Abstract
Background: There is a need to unpack the empirical, practical, and personal challenges
within participatory approaches advocated to optimize implementation. The
unpredictable, chaotic nature of participatory approaches complicates application of
implementation theories, methods, and strategies which do not address researchers’
situatedness within participatory processes. Addressing one’s own situatedness through
critical reflection is important as an implementation scientist to unearth how conscious
and unconscious approaches, including ontological and epistemological underpinnings,
influence the participatory context, process, and outcomes. Therefore, the aim of this
exploratory work is to investigate the heretofore blind spot toward the lived experience of
implementation researchers within the participatory process.
Methods: We developed an integrated research-practice partnership (IRPP) to inform
the implementation of a gestational weight gain (GWG) control program. Within this
IRPP, one investigator conducted a 12-month autoethnography. Data collection and
triangulation included field notes, cultural artifacts, and systematic timeline tracking.
Data analysis included ethnographic-theoretical dialogue and restorying to synthesize key
events and epiphanies into a narrative.
Results: Analysis revealed the unpredicted evolution of the GWG program into a
maternal health fair and three themes within the researchers’ lived experience: (1)
permeable work boundaries, (2) individual and collective blind spots toward the
ontological and epistemological underpinnings of implementation paradigms, and (3)
maladaptive behaviors seemingly reinforced by the research culture. These themes
contributed to the chaos of implementation and to researchers’ experience of inadequate
recovery from cognitive, emotional, and practical demands. These themes also
36
demonstrated the importance of contextual factors, subjectivity, and value-based
judgments within implementation research.
Conclusion: Building on extant qualitative research guidelines, we suggest that
researchers anchor their approach to implementation in reflexivity, intentionally and
iteratively reflecting on their own situatedness. Through this autoethnography, we have
elucidated several strategies based on critical reflection including examining
philosophical underpinnings of research, adopting restorative practices that align with
one’s values, and embracing personal presence as a foundation of scientific productivity.
Within the predominant (post) positivism paradigms, autoethnography may be criticized
as unscientifically subjective or self-indulgent. However, this work demonstrates that
autoethnography is a vehicle for third-person observation and first-person critical
reflection that is transformative in understanding and optimizing implementation
contexts, processes, and outcomes.
Key Words: Implementation, novel methods, epistemology, knowledge translation,
context, engagement, qualitative research, anthropology
Contributions to the literature:
• This work suggests that theory-based autoethnography (i.e. personal narrative) is
a thought-provoking, action-inspiring method for capturing implementation
processes and outcomes, particularly within participatory research.
• In recognizing how their own values, beliefs, and behaviors influenced the project
at hand, researchers identified several strategies for thriving in the chaos of
implementation.

37
• These strategies emphasize reflection, well-being, and presence as tools toward
personal, professional, and scientific clarity.
Background
In translating research findings to real-world benefit, participatory research (1–4)
purportedly embodies the spirit of a quote often attributed to cultural anthropologist
Margaret Mead: “Never doubt that a small group of thoughtful, committed citizens can
change the world: indeed, it is the only thing that ever has” (5)(p.111). As a vehicle for
change, participatory research is characterized by active collaboration between
researchers and diverse stakeholders (1). This collaboration is intended to empower
stakeholders—specifically those who are underrepresented in research decision-
making—to shape all aspects of research, ultimately optimizing how a program or policy
works within stakeholders’ unique lives and communities (4,6). Overall, participatory
research holds promise as the backbone of pragmatic (7) implementation (8) to promote
feasible, user-friendly applications of research findings to the daily lives of community
members.
However, as participatory research has become more common, experts have
uncovered a “dark side” to this collaborative model with practical, personal, and
professional costs to researchers, as well as costs to stakeholders, the research itself, and
research as a profession (9). Ample evidence suggests that participatory research poses
people-oriented, emotionally-charged challenges plus complicated logistics and
scheduling barriers in constant flux (10–14). Exemplifying the emotional dimension of
these challenges, researchers in recent focus groups described pursuing Dissemination

38
and Implementation (D&I) science as “intimidating” and “career suicide”(15).
Furthermore, within participatory processes, researchers may have to navigate conflict
and tension related to organizational change and feedback loops, particularly when there
are power differentials between stakeholders (e.g. physician and patient) (10). The
unpredictable nuances of working within complex human environments can be chaotic
(10), challenging the usability of current implementation theories, methods, and strategies
(16,17) that do not specifically acknowledge researchers’ roles or intrapersonal resources
to initiate and maintain participatory processes (18).
In addition, the uncontrollable, value-laden nature of a participatory approach
(19,20) seems incommensurable (21,22) with positivist or post-positivist paradigms
reflected in mechanistic implementation advancements such as quantification of discrete
implementation activities (23) and calls for deductive qualitative research (24). In
general, (post-) positivist paradigms emphasize systematic a priori hypothesis-testing,
experimental control, elimination of bias, generalizable predictions, and research quality
determined by conventional internal and external validity aimed at explanation. In
contrast, constructivist (sometimes called interpretive) paradigms emphasize the
subjective nature of knowledge, naturalistic inquiry with participant voice, reflexivity,
iterative theorizing, and research quality determined by trustworthiness aimed at
understanding meaning (19,25,26). For additional description of scientific paradigms,
see Table 1 in Greenhalgh et al. (26) or Table 6.2 in Guba and Lincoln (19).
Indicating an opportunity to look beyond (post-) positivist paradigms, emergent
research suggests that mundane, hidden tasks fuel the implementation process (27).
However, there has been a blind spot to the effect of researchers’ “situatedness,”
39
including intrapersonal resources, values, and ideologies (28,29), within this hidden
dimension of implementation. Moreover, current literature does not include day-to-day,
concrete strategies that researchers can use to acknowledge and leverage their
situatedness and, therefore, optimally cope with professional and personal challenges
within participatory approaches (9). There is a need to critically investigate the ground-
level work within the lived experience of participatory research (11) in order to unpack
the black box of implementation (30), including how our own conscious or unconscious
situatedness as researchers influences the implementation process.
Therefore, the aim of this research was to explore and analyze what happened in
one year of a participatory research project dedicated to maternal well-being. For this
exploration, researchers employed a novel autoethnographic approach. Autoethnography
appears to be a relatively untapped methodology in implementation science (10) and
offers a fluid, qualitative approach to capturing the nuanced, inter- and intra-personal
micro-processes of how a participatory effort unfolds within an unpredictable real-world,
community context (24,25,31). We argue that autoethnography is an appropriate method
to investigate current implementation blind spots such as researchers’ situatedness. In
combining first-person and third-person perspectives, autoethnography may capture the
impact of blind spots and situatedness on all aspects of research from stakeholder
interactions to data analysis and interpretation
In exploring nuanced processes, autoethnography combines two central
components of science—observation and critical thinking (30,32). What
autoethnography lacks in conventional control and a priori systemization is made up for
by ongoing, interdisciplinary, theoretical dialogue and critical reflection. Critical
40
reflection (33–35) has not been explicitly explored as a method of implementation
inquiry above and beyond the standard integration of reflexivity within qualitative
studies. However, in fields such as education and cognitive science, critical reflection is
practiced and studied as a process “that allows us a rigorous approach to the scientific
work…because it enhances the capability of the mind to go in depth in its life” (35)(p.7).
Intentionally embracing such a subjective method within implementation science poses
various limitations, particularly within dominant (post-) positivist paradigms. Therefore,
the discussion section includes an assessment of credibility, transferability, dependability,
and confirmability as measures of trustworthiness (24,36,37).
This work is significant for three primary reasons. First, it dives beneath the
current mechanistic understanding of participatory research by attempting to capture and
narrate the complete story and lived experience of implementation, including cognitive-
social-emotional phenomena that may elude quantitative methods and current paradigms.
Second, the autoethnographic approach may be replicated in other implementation
investigations as a rigorous and meaningful method for studying contexts, processes, and
outcomes, as depicted in Figure 1 below. Third, this work informs actionable strategies
for personal stability and empirical depth within the chaos of implementation.
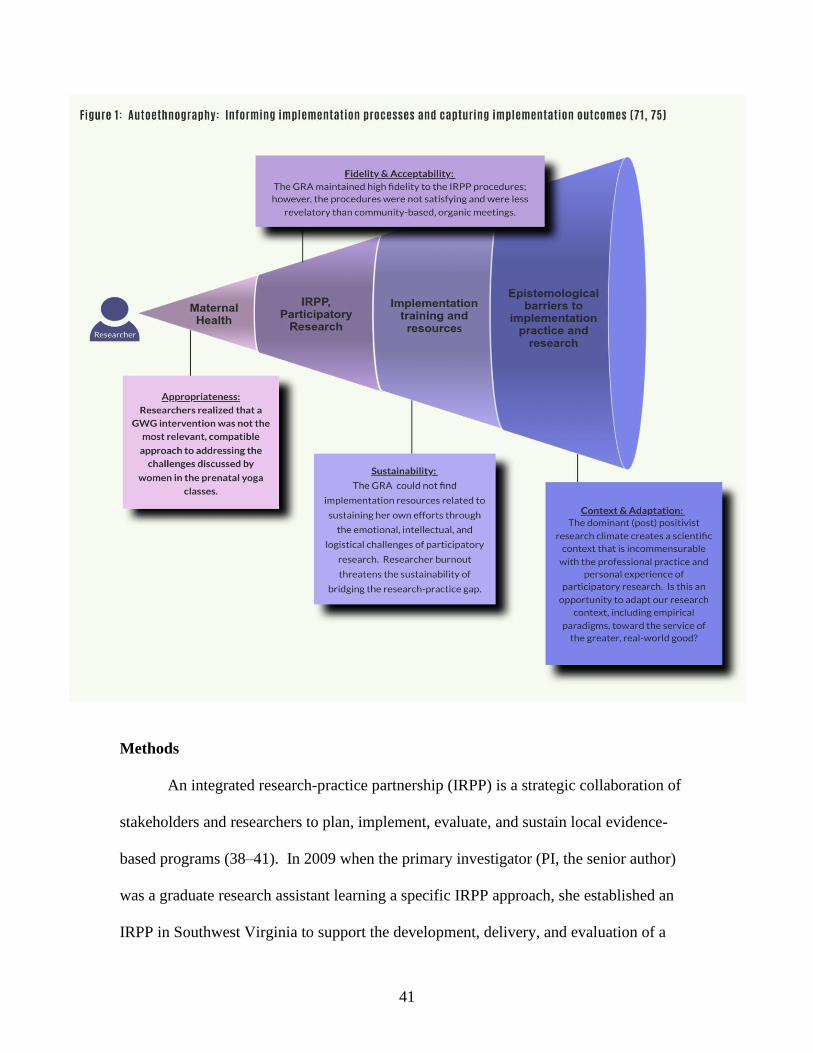
41
Methods
An integrated research-practice partnership (IRPP) is a strategic collaboration of
stakeholders and researchers to plan, implement, evaluate, and sustain local evidence-
based programs (38–41). In 2009 when the primary investigator (PI, the senior author)
was a graduate research assistant learning a specific IRPP approach, she established an
IRPP in Southwest Virginia to support the development, delivery, and evaluation of a

42
gestational weight gain (GWG) control program (42) (see Figure 2 below). However,
due to high turnover among IRPP members and the departure of the PI who accepted an
international postdoctoral position, progress on implementing the GWG control
intervention came to a halt. This reflects the common phenomenon of “parachute”
research (43,44) in which researchers disappear from a community setting when
empirical work is complete or academic demands arise.
From 2014-2018, after completing the postdoctoral fellowship, the PI re-
established her community connections and conducted foundational collaborative work
on preconception weight management. In 2018, the PI recommitted to prenatal health
interventions, pursuing her passion for disseminating evidence-based health information
and self-compassion practices to individuals within the gestational period. The graduate
research assistant (GRA) whom she hired to manage and evaluate a new IRPP is the first
author of this manuscript and conducted autoethnography of her experience
implementing the IRPP from July 2018-July 2019.
In conducting autoethnography, the GRA served as a participant observer (31,45)
simultaneously leading and studying the IRPP. The GRA recorded real-time
observations of meetings, interactions, and events as “jottings” which she subsequently
expanded into field notes (46). The GRA wrote field notes for a minimum of 10 minutes
after IRPP-related meetings and events. The GRA also collected cultural artifacts such as
meeting agenda, meeting minutes, flyers, and emails (24,30,46) and systematically
tracked attendance at meetings, start/end times of meetings, adherence to meeting agenda,
adherence to communication protocols, and a detailed timeline to measure temporality of
implementation efforts and strategies (23).
43
To capture her own cognitive-social-emotional experience within the work, the
GRA wrote general fields notes for at least one hour per week as a process of critical
reflection and self-inquiry in which she “play[ed] at the same time the role of subject who
reflects and object who is reflected” (35)(p.1). True to theoretically informed
ethnography (45), she iteratively integrated evidence-based concepts and classical
theories from other fields (47) so that the fieldnotes were simultaneously data collection
and data analysis. This ongoing interdisciplinary, (48) “ethnographic-theoretical
dialogue” (45) is rooted in qualitative research paradigms that emphasize the value-laden,
fluid nature of reality (ontology) and knowledge (epistemology) (19,20,25).
To organize and further analyze the ethnographic-theoretical dialogue,
investigators (i.e. the PI and GRA) used a chronological approach called restorying (31)
to identify epiphanies or key events within the data and synthesize them into a narrative
with the five elements of literature—characters, setting, conflict, plot/action, and
resolution. From these elements, investigators generated, interpreted, and presented
themes and practical implications of the narrative.
The investigators obtained consent from all IRPP members and protocol approval
from the university Institutional Review Board. The GRA’s approach to this work
reflects her Master’s of Public Health, academic training in journalism and human
development, 15-years of leadership experience as a collegiate swim coach, and ongoing
study of yoga. An experienced yoga teacher and practitioner, the PI’s approach to this
work incorporates her empirical and practical expertise in pragmatic methods, group
dynamics, community-based physical activity, and implementation science. Both
investigators were full, active members of the IRPP and neither investigator is a parent;
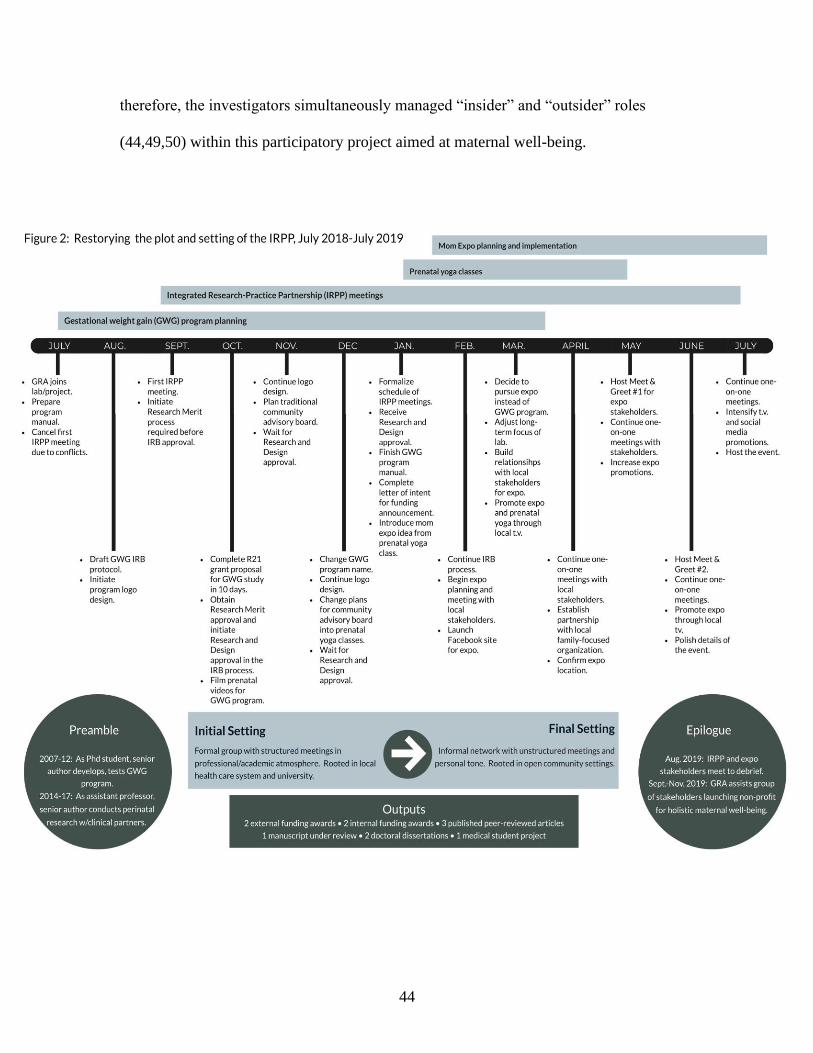
44
therefore, the investigators simultaneously managed “insider” and “outsider” roles
(44,49,50) within this participatory project aimed at maternal well-being.
45
Results
The presentation of autoethnographic results is a result in and of itself and
evidence of the difficulty operationalizing novel methods within current scientific norms
such as the common format of peer-reviewed journals. In Table 1 before the reference
list, investigators present results of the ethnographic-theoretical dialogue, and in the
subsections below, investigators report the results of restorying, including plot, setting,
characters, conflicts, themes, and resolution. In this project, separating data and
interpretation may dilute the reflective, iterative nature of ethnographic-theoretical
dialogue. Therefore, investigators suggest that readers iteratively refer to Table 1
throughout the results and discussions sections to experience the visceral-intellectual
rhythm of autoethnography and critical reflection.
Restorying: Plot and Setting
The IRPP’s narrative is set in Southwest Virginia where the connection between a
public land-grant university and local health care system developed over more than a
decade. As depicted in Figure 2, the IRPP’s “plot” within this setting dramatically
shifted from July 2018-July 2019. In July 2018, the IRPP convened to plan a randomized
controlled study (RCT) of a GWG control program. Investigators aimed for the study to
be a systematic step in “scaling out” (51) the program by delivering it through
videoconference. To adapt the program, the GRA intended to develop a community
advisory board as an additional arm of the IRPP. As the investigators worked with local
women to film prenatal physical activity videos, the plans for a community advisory
board morphed into free prenatal yoga classes. Attendees of the prenatal yoga classes
suggested the idea of a one-day, family-friendly event for local women. This idea
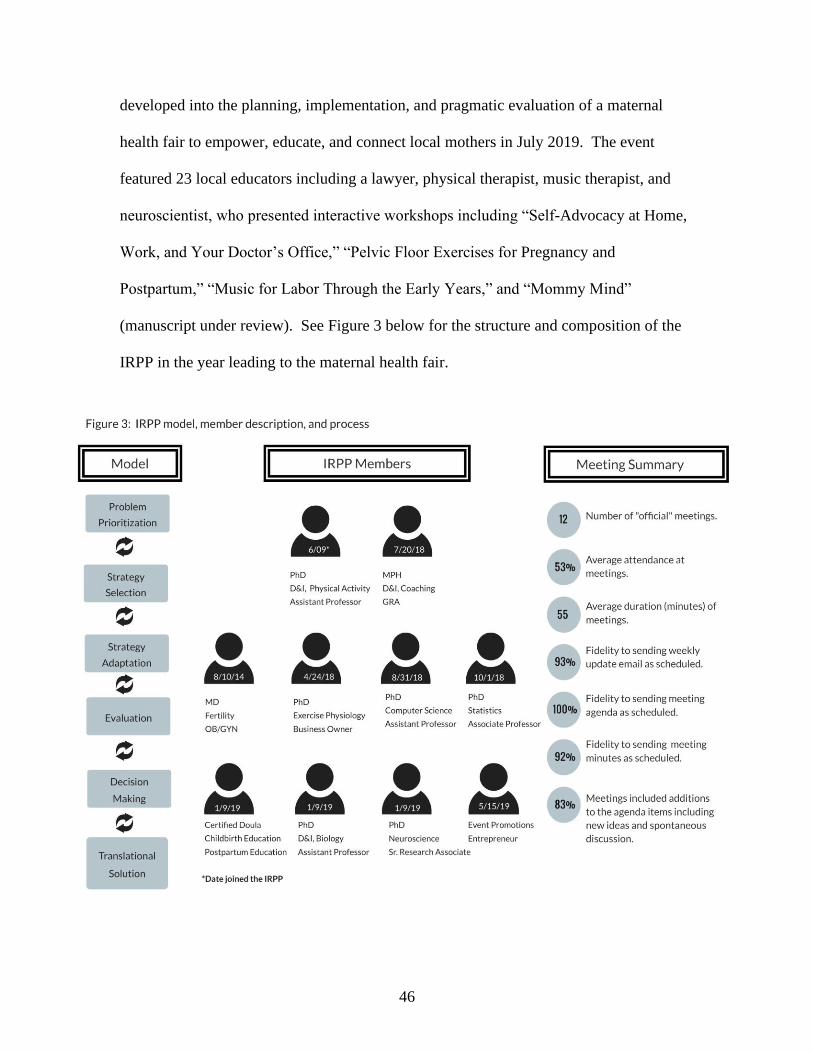
46
developed into the planning, implementation, and pragmatic evaluation of a maternal
health fair to empower, educate, and connect local mothers in July 2019. The event
featured 23 local educators including a lawyer, physical therapist, music therapist, and
neuroscientist, who presented interactive workshops including “Self-Advocacy at Home,
Work, and Your Doctor’s Office,” “Pelvic Floor Exercises for Pregnancy and
Postpartum,” “Music for Labor Through the Early Years,” and “Mommy Mind”
(manuscript under review). See Figure 3 below for the structure and composition of the
IRPP in the year leading to the maternal health fair.

47
Within data collection and analysis, it was apparent that understanding the IRPP’s
“plot” required looking beyond the 12-month autoethnography: “The IRPP isn’t in a
petri dish. [The PI] has been working on [the GWG program] since she was a graduate
student and there’s already discussion about how this is just the first Mom Expo [the
maternal health fair], just one step toward better connections for pregnant and postpartum
women. When I get caught up in the 12-month time frame of the protocol, I forget that
the IRPP actually exists on a continuum of time and life with all sorts of inputs and
outputs. It’s not like a carefully prepared sterile slide under a microscope” (field notes,
June 6, 2019). In other words, what led to this IRPP and what stems from it extends
before and after the empirical, researcher-established boundaries of a project (see
preamble and epilogue in Figure 2 above).
Within this unbounded “setting,” seemingly mundane interpersonal interactions
rippled into long-term effects. For example, the GRA established a connection with a
local community member who attended a single prenatal yoga class in March 2018. That
community member provided an introduction to a leader of an existent local non-profit
organization who agreed to host the first event of the new non-profit organization that
developed from the maternal health fair that originated in the yoga classes. In other
words, a single interpersonal relationship that developed within a prenatal yoga class that
was not part of the initial IRPP plan contributed to the significant, unpredicted long-term
community benefit of a non-profit organization for holistic maternal well-being.
Likewise, other interpersonal connections the GRA developed within the community led
to promotional spots on local television stations and reduced financial costs for hosting
the maternal health fair. “This whole thing is like the butterfly effect: I don’t know how
48
or when I meet someone will lead to something else later down the road” (field notes,
July 28, 2019). The butterfly effect, first demonstrated by Edward Lorenz in
mathematical models of weather predictions, describes how seemingly inconsequential
events eventually contribute to significant outcomes in a later state (52), as in the
flapping of a butterfly’s wings in Brazil causing a tornado in Texas (53). The butterfly
effect provides a metaphor for the dynamic, unpredicted effects of spending time with
community members within informal settings that belie conventional scientific protocol.
Based on the GRA’s initial D&I science training in a graduate course, she
expected “what happens in an IRPP” to be a slow but steady, systematic but iterative
flow. “The language about implementation frameworks, theories, and processes from
D&I class implies a slow but continuous spread: diffusion [italics included] of
innovations, 17 years to move through the traditional pipeline from basic science to
uptake in the real world, iterative and ongoing balance of fidelity and adaptation. It
sounds very Darwinian—gradual evolution, survival of the fittest. Even the language of
a diffusion ‘champion’ conjures up an image of the ‘fittest’” (field notes, December 9,
2019). However, in terms of metaphors from natural science, the full IRPP story
resembles Punctuated Equilibrium (PE) (54). PE is a model of evolution that describes
change patterns in nature as occurring through periods of relative stability suddenly
punctuated by rapid adaptation (54). Social science researchers have recently used this
evolutionary model to describe the delayed benefits of coaching when a certain event
triggers an epiphany that catalyzes an individual to suddenly enact what he or she
previously learned in coaching (55). Likewise, evaluation scientists have highlighted
“evolutionary epistemology” and posited that the natural selection of what knowledge
49
survives and spreads in the real-world is not a “foreordained” process but takes place in
“fits and starts” (56)(p.4). These fits and start are evident in the full story of the IRPP
which spans chunks of “latent” time punctuated by blocks of intense activity in 2008-
2009, 2011, 2014, and 2018-2019. Even within 2018-2019, there was a distinct shift in
pace (i.e. a punctuation) when the prenatal yoga classes catalyzed action toward the
maternal health fair. The catalysts for the action were not the mechanistic operations of
the IRPP, but the characters and conflicts within the story.
Restorying: Characters, Conflicts, and Themes
On the surface level, the PE pattern of IRPP-related work was contingent upon
investigators’ situatedness as graduate students: The highest intensity blocks occurred
during 2008-2009 when the PI initiated the GWG program and community partnerships
as a graduate student, and during 2018-2019 when the GRA managed the IRPP and
founded the health fair. Graduate education resources such as predoctoral fellowships,
protected time, and supervision from experienced advisors enabled intense empirical and
practical activity: The investigators’ “situatedness” (29) as graduate students set the
stage for generating ideas, completing time-intensive research, and establishing extensive
personal networks through a participatory approach.
Beneath the concrete academic resources, the investigators’ lived experience
demonstrated their situatedness as human beings (44) with ever-present emotions, deep
values, limited time, and finite energy making them vulnerable to strain (57) from work
demands. For example, the GRA experienced emotional exhaustion and ego depletion
(58,59) stemming from a complicated web of her own associative thinking (60),
maladaptive perfectionism (61,62), and perseverative cognition (63,64) that was
50
exacerbated by a publish or perish research culture (65,66) rooted in extrinsic motivation
(67,68) and performance achievement orientation (69): “All year I’ve felt like I’m on a
wild-goose chase or playing some Alice-in-Wonderland version of dominoes, balancing
what a dissertation committee values as science with what prenatal yoga women value as
life, all while keeping up a can-do attitude and A+ quality amidst the constant topple
of…’let’s change the name for [the GWG program]’…’actually, let’s not do the [GWG
program]’…’you have to have a research question’” (field notes, March 25, 2019). The
autoethnographic process itself helped the GRA recognize how her own cognitive
patterns contributed to her exhaustion and, subsequently, she was able to reshape
maladaptive rumination and over-analysis into insightful reflection (70,71).
Critical reflection within this research design illuminated dissonance between the
investigators’ professional, conventionally scientific roles and their person-centered
participatory roles. The difficult decision to pivot away from an RCT epitomized this
conflict: In implementing a pragmatic maternal health fair instead of an intervention
RCT, the investigators intentionally chose to prioritize participatory input over traditional
a priori empirical processes: “I can’t truly empower people in the spirit of participatory
research if the only way to achieve ‘rigor’ is to march steadily forward on a pre-fixed,
‘systematic’ path based on a priori research questions, not on the destination women
really seek” (field notes, March 13, 2019). In addition, this shift manifested
investigators’ epiphany that GWG was not local mothers’ central need: “…we get caught
up in creating band aids, not treating wounds. Bandaids are kind of like packageable,
tidy interventions for narrow health outcomes, like GWG, that are important but not the
real source of suffering, not the central thing that heals the core issue or fuels all-around
51
well-being…To achieve something sustainable that people want to maintain with fidelity,
we have to get at the underlying root issue and what really matters to people, even if it’s
hard to measure.” (field notes, February 24, 2019).
With this epiphany, the GRA’s work expanded from leading structured IRPP
meetings to spending one-on-one time with stakeholders out in the community in non-
academic, non-clinical settings such as coffee shops and libraries. From July to March,
the IRPP had inched toward launching the RCT as investigators grappled with
organizational red tape and convoluted procedures within the clinical system: “Busyness
gets in the way of business. There’s tons of horizontal movement—as in digital
horizontal movement as emailsemailsemails gobble up the day—but no vertical progress
toward the mountain peak” (field notes, October 14, 2019). In contrast, progress toward
the health fair was rapid, including partnerships with an existing family-oriented
organization and local library, as well as commitments from nearly 40 individuals to
volunteer their service, expertise, and energy at the health fair. “I get so much more input
from one-on-one get-togethers out in the community then when I run IRPP meetings with
agenda and minutes and action items. The IRPP meetings are systematic and trackable;
but for all the organization (i.e. replicable processes worth publishing in a journal), they
don’t seem nearly as authentic as the one-on-one meetings with women out in their
community…where I’m making traction, where I feel like I’m gaining insight into
community dynamics, where relationship-building doesn’t feel like a mercenary research
task” (field notes, April 12, 2019).
In living out these epiphanies and conflicts, investigators identified three themes:
(1) permeable work boundaries (72), (2) individual and collective blind spots toward the

52
ontological and epistemological underpinnings of implementation paradigms, and (3)
maladaptive behaviors seemingly reinforced by the research culture. See Figure 4 below
for a diagram of the themes and Table 1 for subthemes, ethnographic evidence,
theoretical/literature dialogue, and untapped opportunities for progress.
One lens for interpreting these intertwined themes is structuration theory (73)
which “refers to the idea that rules, policies, and structures are only made ‘valid’ when
individuals follow them and make decisions based upon them” (p. 59) (25). In other
words, the GRA’s own behaviors—her individual “micro-practices”—reinforced the
publish or perish culture and (post-) positivist paradigms that may hamper participatory
research and well-being. For example, in the first six months of the project, the GRA’s
drive for achievement reinforced her situatedness in a culture of workism (72): “I was
tossing deep thinking out the window so that I could keep driving forward as fast as
possible…my ambition to be more ‘productive’ devoured my responsibility for self-care”
(field notes, December 27, 2018). But as the IRPP work turned to relationship building
in the second six months, the GRA found some traction by distinguishing between
presence and productivity: “I cannot control all of the variables that go into scientific
productivity, but I can control where and how I choose to focus my energy…the depth
and deliberateness of my presence in each and every conversation even if I cannot control
an editor’s or committee member’s reaction to a paper I write” (field notes, March 21,
2018). This distinction did not lead to a mindful panacea of constant ease. Instead, it has
led to unease knowing that challenging the prevalent implementation structure may lead
to conflict and rejection within the field.

53

54
The field has made significant advancements in developing toolkits to clarify
empirical outcomes of implementation (74), establish skill-based mentoring (75), and
promote qualitative methods that capture nuanced micro-processes (24). Furthermore, at
the 2018 and 2019 Annual Conferences of the Science of Dissemination and
Implementation in Health, there were calls to acquire “soft” skills. However, we have yet
to appropriately operationalize these calls and advancements by determining what roles
an implementation scientist should or could realistically play within participatory
research (18) based on their unique skills, training, personality, values, and time—in
other words, based on their situatedness and finite human capacity (59). The lack of
awareness or reticence to recognize personal situatedness and limits of human capacity
(59) may be a result of traditional scientific paradigms that dominate health research:
The structure of grant writing (76), system of tenure (cultural artifact, university tenure
guidelines), emphasis on outcomes (77), and alignment with conventional benchmarks of
rigor such as objectivity and internal/external validity (7,78,79) indicate dominance of of
(post-) positivism (19,20,25).
Likewise, the general style of reporting results in peer-reviewed journals reflects a
paradigm of value-free objectivity. Researchers generally write methods sections in a
passive voice (e.g. “data was collected…”), avoid the subjective pronouns I, we, you, and
describe procedures that are measurable and replicable. Minimizing attention to the
inherent role of their own five senses and cognition, researchers often un-situate
themselves as an indication of unbiased validity and reliability. This paradigm of
projecting machine-like expertise seems incommensurable with both reflective practice
(33,34) and participatory research which hinges on researchers’ moral drive to make a

55
difference in the real-world and their ability to build trust with stakeholders (80).
Building trust is a human—not scientific—venture, and this ethnographic-theoretical
dialogue suggests that researchers’ humanness—for example, being “too tired to inspire”
(81)—is a critical component of the black box of implementation. Furthermore,
researchers’ deep philosophical views and scientific training may limit their perspective
on novel ways to open that black box. For example, authors of a recent implementation
autoethnography observed an “underlying tension between the production and use of
generalizable knowledge” caused by conflicting scientific paradigms (10)(p.6). This
paper avoids that trap by elucidating strategies to uncover paradigm conflicts that reduce
the usability of findings (see conclusion).
Fields such as education and mindfulness have embraced debates on the
ontological and epistemological foundations of research and practice (34,35,82–84), and
the emerging idea of value-based medicine (85,86) emphasizes philosophical
underpinnings and patient empowerment (20). However, implementation dialogue
focuses on the methodological level of what constitutes credible evidence, not
philosophical viewpoints of reality and knowledge (87). The lack of clarity on these
ontological and epistemological levels may contribute to the chaos (17) and lexicological
quagmire (8,47,88,89) often described within implementation science. A firm footing in
the field’s beliefs about science may provide a foundation to stabilize at least some of the
chaos: “Time and time again, I’ve seen that the swimmers who consistently win aren’t
always the ones with the most efficient stroke or highest V02 max—it’s often the ones
who had the strongest why, the clearest perspective of what a race meant, a purpose
beyond the numbers on the record board…” (field note, February 2, 2019).
56
Paradoxically, the coaches and athletes who win the most are often the ones who anchor
their focus on a purpose beyond winning, beyond tangible outcomes measured by a stop-
watch or counted in a win-loss record (90,91). In contrast, the GRA observed an
overemphasis on outcomes over process and methods over philosophy within the IRPP,
implementation literature, and academic-research environment. It was through the
process of autoethnography, that the GRA unearthed her own ontological and
epistemological assumptions; she experienced the effectiveness of reflective practice to
clarify her own philosophy as a stabilizing point within the messiness of implementation.
Restorying: Resolution
The resolution of the 12-month study indicates empirical, practical, personal, and
philosophical evolution. On the empirical level, the GWG control intervention evaluated
through RCT evolved into a health fair evaluated through the pragmatic application of the
RE-AIM framework (92) (manuscript under review). On the practical level, the GRA’s
work evolved from leading an IRPP in a systematic way to meeting community members
for coffee and “walk and talks.”
On the personal level, continuous reflection through this methodological approach
prompted the investigators to intentionally shift their behaviors and micro-practices to
optimize their own situatedness including well-being and creativity: The PI practiced
delegation and “allowed” the IRPP, health fair, and non-profit to form organically,
adjusted research focus in order to avoid emotional triggers, committed to eating lunch
before 3 pm, crafted a value-laden mission statement for the lab, and carved out time
away from email. The GRA re-vamped her morning breathing-meditation practice,
thwarted work-related rumination by listening to unrelated podcasts during her commute,
57
and stepped away from the computer to hug her husband whenever he arrived home. In
line with the Conservation of Resources theory (57,93) from industrial and organizational
psychology, these shifts helped optimize situatedness by conserving and refueling
researchers’ intrapersonal energy and interpersonal resources to meet the demands of
participatory implementation research.
Finally, at the philosophical level, the GRA evolved from focusing on novel
methodologies to grappling with deeper ontologies and epistemologies that influence or
limit implementation science and participatory research. Paradoxically, the use of a
novel methodology (i.e. autoethnography) is what revealed that novel methodologies are
not enough: There is a need to examine and align underlying ontological and
epistemological foundations of implementation science, including the roles of
subjectivity and values within participatory research. PE paleontologists Eldredge and
Gould embraced subjectivity within the scientific process when they wrote, “We do not
encounter facts as data (literally “given”) discovered objectively. All observation is
colored by theory and expectation” (54) (p.85).
With a similar nod toward embracing bias, the investigators report the
trustworthiness of this study in Table 2 below. In this paper, we have transparently
presented our own vulnerabilities and biases as examples of how researcher situatedness
may impact participatory approaches to implementation. In addition, we have leveraged
interdisciplinarity to interpret these vulnerabilities as untapped opportunities to advance
the field of implementation science.

58
Table 2: Reporting trustworthiness of qualitative data based on Guba and Lincoln’s criteria (153)
Dimension Evaluation
Dependability:
consistency and
accuracy of findings
Through iterative, ongoing immersion in peer-reviewed literature from a variety of fields, we
anchored the ethnographic observations in scientific findings. Essentially, we demonstrated
that researchers and participatory implementation processes are consistent with concepts from
the social sciences and natural sciences.
Credibility: truth of
the findings
Our reflexivity statements in the methods section and transparency with which we approached
our own struggles and situatedness indicate that the findings are true to our lived experience
within this IRPP.
Confirmability:
neutrality and
whether findings are
supported by
evidence
The findings suggest that we were not neutral and emotionless during the participatory
process; however, we transparently (and vulnerably) reported our own holistic involvement in
the process, triangulating data from cultural artifacts, the GRA field notes, collaborative
reconstruction of events, and ongoing theoretically-informed brainstorming.
Transferability:
application in other
contexts
We report our unique lived experience within a unique IRPP and do not expect our exact
thoughts, emotions, and relationships to be replicated in other contexts. However, insight to
the importance of situatedness is transferable to other researchers. Regardless of the scientific
paradigms to which we ascribe or objectivity to which we strive, other researchers can also
leverage the transformative potential of reflection to elevate personal meaning, practical
relevance, and empirical depth.
Discussion
Based on this study, we propose that implementation researcher situatedness
influences all aspects of participatory research from planning to dissemination.
Situatedness is multifaceted with personal (i.e. the researcher), interpersonal (i.e. the
researcher + IRPP), and cultural (i.e. the researcher + implementation science)
dimensions that include conscious and unconscious, adaptive and maladaptive drivers. It
stands to reason that these drivers influence many manifestations of implementation
science, not just participatory research. Therefore, the implications of this work are
applicable to all implementation scientists.
This work indicates that autoethnography is a thought-provoking, action-inspiring
method to leverage researcher situatedness through critical reflection, capturing empirical
aspects of implementation while enhancing the practice of implementation including
researchers’ own influence on the process. As shown in Figure 5 below, the reflective
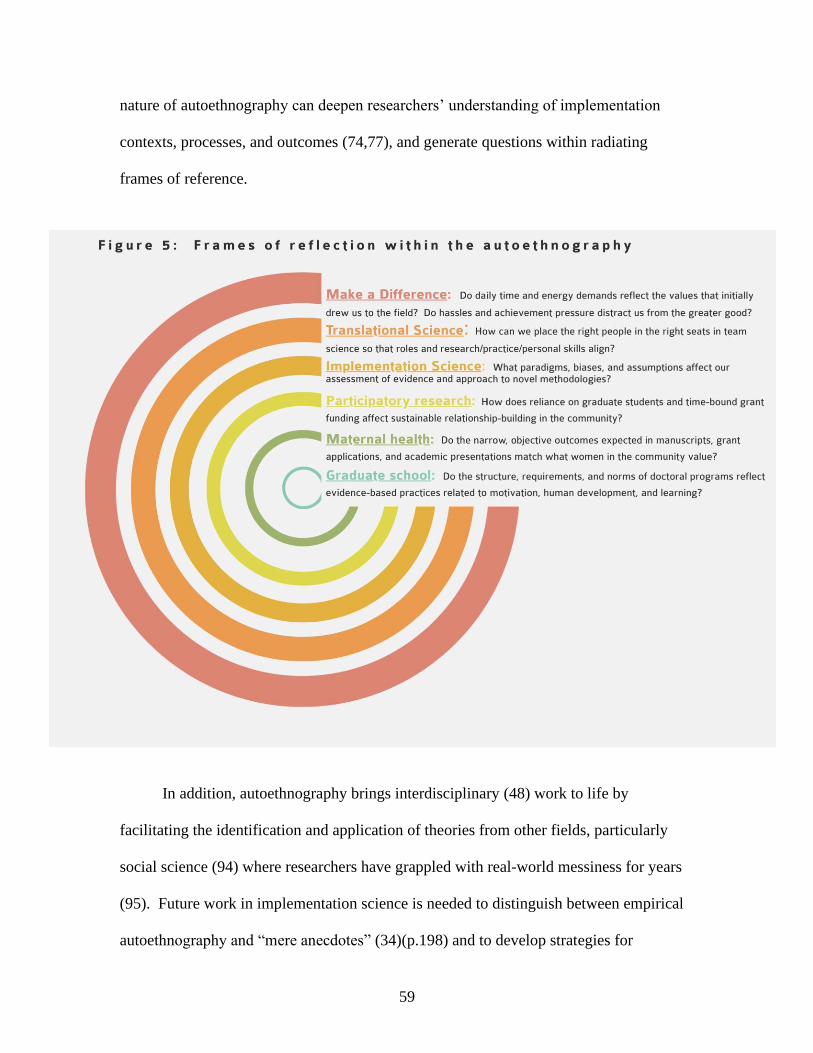
59
nature of autoethnography can deepen researchers’ understanding of implementation
contexts, processes, and outcomes (74,77), and generate questions within radiating
frames of reference.
In addition, autoethnography brings interdisciplinary (48) work to life by
facilitating the identification and application of theories from other fields, particularly
social science (94) where researchers have grappled with real-world messiness for years
(95). Future work in implementation science is needed to distinguish between empirical
autoethnography and “mere anecdotes” (34)(p.198) and to develop strategies for

60
disseminating the breadth and depth of data captured in this time- and energy-intensive
method.
Findings in this explicitly reflective work suggest that there are gaps in
acknowledging our own humanness and in investigating “invisible” drivers such as deep
ontological and epistemological foundations of implementation science. Without deeper
recognition of the ontological and epistemological components of the current
implementation paradigm, new methodologies will fall flat; we will not be able to clear
the research-realworld pipeline that we inadvertently clog through our own attachment to
traditional views of what matters and what is. Furthermore, we may exacerbate gaps and
blind spots by unintentionally behaving in maladaptive ways that reinforce the culture of
workism, demonstrable productivity, and chaos. Within this chaos, we suggest several
strategies to optimize situatedness.
First, we suggest incorporating ontological and epistemological inquiry into
academic training, team science, and efforts to advance the implementation field (see
Table 3 below). Diving beneath the current focus on matching methods to a research
question, researchers should reflect on personal philosophies that underscore or
contradict paradigms of what evidence counts (87).
Table 3: Potential benefits of recognizing and clarifying ontological and epistemological paradigms
• Improve communication across the translational spectrum from basic science to clinical science to
implementation, dissemination, and policy.
• Leverage the power of values and intrinsic motivation in fostering long-term change, as opposed to
relying only on impersonal, measurable mechanisms that do not reflect basic human psychosocial needs such
as love, connection, and autonomy (68,154).
• Engage in rich analysis of novel approaches that may otherwise be quickly rejected because of incongruence
with the analyzer or field’s deeply-held, implicit views as what counts as evidence or knowledge.
• Advance interdisciplinary and transdisciplinary approaches (48) that may be initially discarded because of
underlying, mismatched philosophical assumptions between various fields.
61
Second, we suggest that researchers adopt evidence-based restorative practices
that align with one’s own values, similar to how elite athletes prioritize recovery in their
training regimens (96,97). Potential practices include microbreaks (98,99), meaningful
off-job experiences (100), slow deep breathing (101,102), and breaks from digital
communication (103).
Third, to promote presence, we suggest that researchers focus their senses,
intellect, and emotions on the people present in a specific time and place: Acknowledge
the potential of “n-of-1” participatory research in which individual, authentic
relationships can spiral into unpredicted community benefit in a butterfly effect pattern.
Embrace personal presence as a valuable experience in and of itself in addition to being a
vehicle for relevant empirical productivity.
Conclusion
Each of these strategies incorporates reflective practice and values as stabilizing
mechanisms within the chaos of implementation: Clarity through the chaos of
implementation starts with clarity within the researcher—as a situated human being
viscerally and cerebrally experiencing life. We may not be able to control dynamic, real-
world variables and unpredictable external contexts, but we can choose to maximize our
humanness and presence. In leveraging our own situatedness through critical reflection,
we can apply implementation-related constructs to ourselves: scale inward, facilitate
one’s own capacity, protect personal sustainability, seek fidelity to values, and embrace
the present context of moment-to-moment time and space. Ultimately, through this
critical reflection, implementation scientists may epitomize what Margaret Mead meant
by thoughtful citizens changing the world.
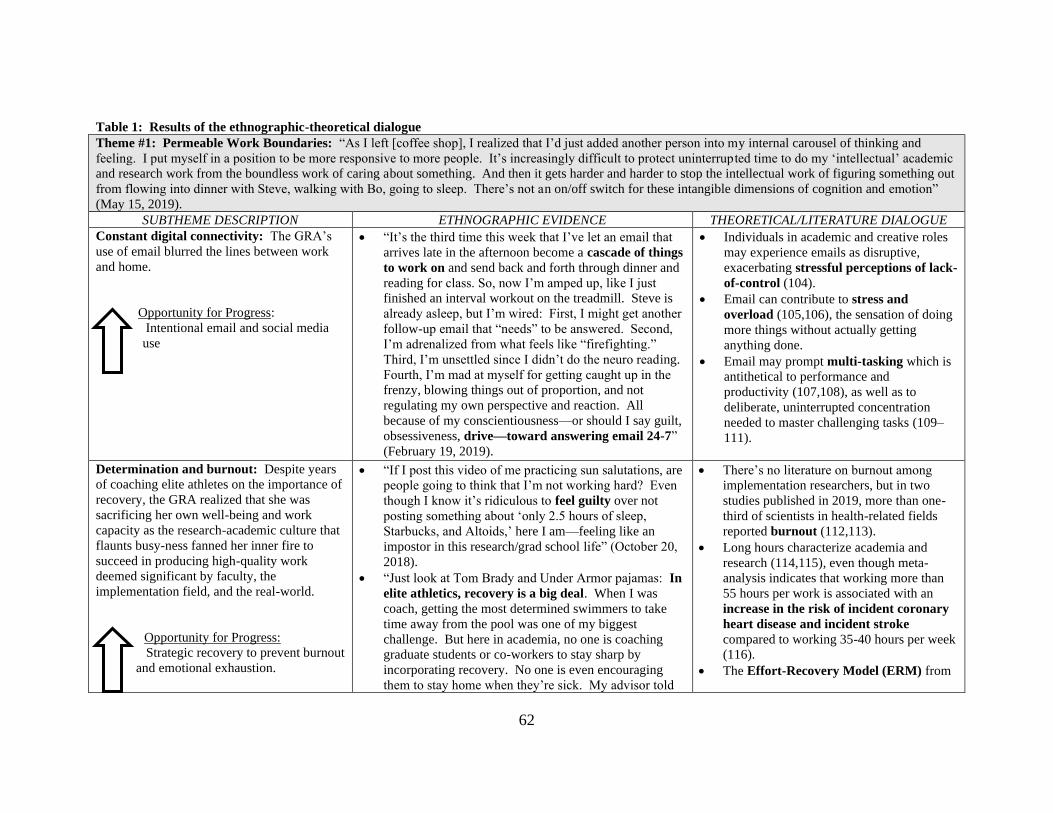
62
Table 1: Results of the ethnographic-theoretical dialogue
Theme #1: Permeable Work Boundaries: “As I left [coffee shop], I realized that I’d just added another person into my internal carousel of thinking and
feeling. I put myself in a position to be more responsive to more people. It’s increasingly difficult to protect uninterrupted time to do my ‘intellectual’ academic
and research work from the boundless work of caring about something. And then it gets harder and harder to stop the intellectual work of figuring something out
from flowing into dinner with Steve, walking with Bo, going to sleep. There’s not an on/off switch for these intangible dimensions of cognition and emotion”
(May 15, 2019).
SUBTHEME DESCRIPTION ETHNOGRAPHIC EVIDENCE THEORETICAL/LITERATURE DIALOGUE
Constant digital connectivity: The GRA’s
use of email blurred the lines between work
and home.
Opportunity for Progress:
Intentional email and social media
use
• “It’s the third time this week that I’ve let an email that
arrives late in the afternoon become a cascade of things
to work on and send back and forth through dinner and
reading for class. So, now I’m amped up, like I just
finished an interval workout on the treadmill. Steve is
already asleep, but I’m wired: First, I might get another
follow-up email that “needs” to be answered. Second,
I’m adrenalized from what feels like “firefighting.”
Third, I’m unsettled since I didn’t do the neuro reading.
Fourth, I’m mad at myself for getting caught up in the
frenzy, blowing things out of proportion, and not
regulating my own perspective and reaction. All
because of my conscientiousness—or should I say guilt,
obsessiveness, drive—toward answering email 24-7”
(February 19, 2019).
• Individuals in academic and creative roles
may experience emails as disruptive,
exacerbating stressful perceptions of lack-
of-control (104).
• Email can contribute to stress and
overload (105,106), the sensation of doing
more things without actually getting
anything done.
• Email may prompt multi-tasking which is
antithetical to performance and
productivity (107,108), as well as to
deliberate, uninterrupted concentration
needed to master challenging tasks (109–
111).
Determination and burnout: Despite years
of coaching elite athletes on the importance of
recovery, the GRA realized that she was
sacrificing her own well-being and work
capacity as the research-academic culture that
flaunts busy-ness fanned her inner fire to
succeed in producing high-quality work
deemed significant by faculty, the
implementation field, and the real-world.
Opportunity for Progress:
Strategic recovery to prevent burnout
and emotional exhaustion.
• “If I post this video of me practicing sun salutations, are
people going to think that I’m not working hard? Even
though I know it’s ridiculous to feel guilty over not
posting something about ‘only 2.5 hours of sleep,
Starbucks, and Altoids,’ here I am—feeling like an
impostor in this research/grad school life” (October 20,
2018).
• “Just look at Tom Brady and Under Armor pajamas: In
elite athletics, recovery is a big deal. When I was
coach, getting the most determined swimmers to take
time away from the pool was one of my biggest
challenge. But here in academia, no one is coaching
graduate students or co-workers to stay sharp by
incorporating recovery. No one is even encouraging
them to stay home when they’re sick. My advisor told
• There’s no literature on burnout among
implementation researchers, but in two
studies published in 2019, more than one-
third of scientists in health-related fields
reported burnout (112,113).
• Long hours characterize academia and
research (114,115), even though meta-
analysis indicates that working more than
55 hours per work is associated with an
increase in the risk of incident coronary
heart disease and incident stroke
compared to working 35-40 hours per week
(116).
• The Effort-Recovery Model (ERM) from
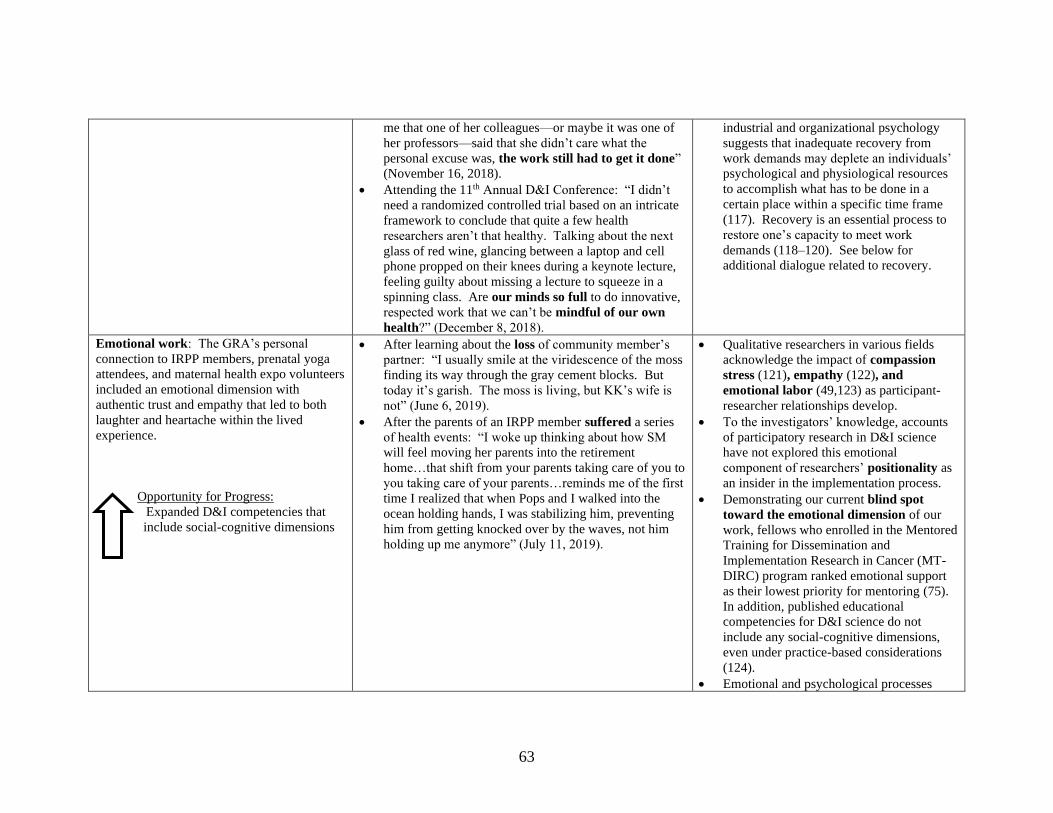
63
me that one of her colleagues—or maybe it was one of
her professors—said that she didn’t care what the
personal excuse was, the work still had to get it done”
(November 16, 2018).
• Attending the 11th Annual D&I Conference: “I didn’t
need a randomized controlled trial based on an intricate
framework to conclude that quite a few health
researchers aren’t that healthy. Talking about the next
glass of red wine, glancing between a laptop and cell
phone propped on their knees during a keynote lecture,
feeling guilty about missing a lecture to squeeze in a
spinning class. Are our minds so full to do innovative,
respected work that we can’t be mindful of our own
health?” (December 8, 2018).
industrial and organizational psychology
suggests that inadequate recovery from
work demands may deplete an individuals’
psychological and physiological resources
to accomplish what has to be done in a
certain place within a specific time frame
(117). Recovery is an essential process to
restore one’s capacity to meet work
demands (118–120). See below for
additional dialogue related to recovery.
Emotional work: The GRA’s personal
connection to IRPP members, prenatal yoga
attendees, and maternal health expo volunteers
included an emotional dimension with
authentic trust and empathy that led to both
laughter and heartache within the lived
experience.
Opportunity for Progress:
Expanded D&I competencies that
include social-cognitive dimensions
• After learning about the loss of community member’s
partner: “I usually smile at the viridescence of the moss
finding its way through the gray cement blocks. But
today it’s garish. The moss is living, but KK’s wife is
not” (June 6, 2019).
• After the parents of an IRPP member suffered a series
of health events: “I woke up thinking about how SM
will feel moving her parents into the retirement
home…that shift from your parents taking care of you to
you taking care of your parents…reminds me of the first
time I realized that when Pops and I walked into the
ocean holding hands, I was stabilizing him, preventing
him from getting knocked over by the waves, not him
holding up me anymore” (July 11, 2019).
• Qualitative researchers in various fields
acknowledge the impact of compassion
stress (121), empathy (122), and
emotional labor (49,123) as participant-
researcher relationships develop.
• To the investigators’ knowledge, accounts
of participatory research in D&I science
have not explored this emotional
component of researchers’ positionality as
an insider in the implementation process.
• Demonstrating our current blind spot
toward the emotional dimension of our
work, fellows who enrolled in the Mentored
Training for Dissemination and
Implementation Research in Cancer (MT-
DIRC) program ranked emotional support
as their lowest priority for mentoring (75).
In addition, published educational
competencies for D&I science do not
include any social-cognitive dimensions,
even under practice-based considerations
(124).
• Emotional and psychological processes

64
erode recovery. Replaying a stressful event
in one’s mind—“perseverative
cognition”—affects the cardiovascular,
immune, endocrine, and neurovisceral
systems even if a person is physically
separated from the stressor (63,64)
• For example, work-related rumination
(i.e. thinking about an element of one’s job
during off-hours) is associated with
reduced cognitive functioning (125) and co-
worker related helping behaviors (126).
Theme #2: Blind spots or conflicts within scientific paradigm: “It seems that D&I scientists can experiment with a different wavelength of thinking that
transcends the replicable methods, visible research process, and generalizable frameworks. Something deeper, something that takes courage, something like that
adage about ‘a ship is safe at shore, but that’s not what ships are built for’” (December 27, 2018).
SUBTHEME DESCRIPTION ETHNOGRAPHIC EVIDENCE THEORETICAL/LITERATURE DIALOGUE
Feasibility of pragmatic methods with
positivist/postpostivist underpinnings: The
GRA’s academic classes did not delve into
philosophical underpinnings of scientific
methods. Sensing that something was
missing, she independently read about the
ontological and epistemological foundations
of various scientific paradigms. In her
interpretation, the positivist/postpositivist
evidence preferred by the implementation
field is at odds with calls for actionable,
stakeholder-centered approaches.
Opportunity for Progress:
Reflexivity of how philosophical
underpinnings may curtail novel
approaches
• After a seminar: “Putting meta-analyses and systematic
reviews at the top of the evidence hierarchy applies to
a conventional scientific paradigm of generalizable
quantification across the translational spectrum.
Perhaps a meta-analysis is the best thing for clarifying a
cause-effect relationship between bone density and
vitamin D supplementation, something that has a literal
dose. But using meta-analysis to pinpoint the effects of
a community advisory board would be like showing
someone the electromagnetic spectrum to describe the
taste of the cold orange I ate at hour 28 of the dance
marathon” (October 13, 2018)
• Applying lessons from the D&I class to writing a
methods section for a community advisory board: “If
the main criteria for judging the significance of a
finding is its internal and external validity, then what’s
the point of community work that inspires change or
empowers people or embraces subjective experience?
The potentially expansive impact of pragmatic
community work challenges narrow definitions—or
perhaps purposes—of science” (November 14, 2018).
• Calls for pragmatic approaches entail
research methods and outcomes that
matter to stakeholders in real-world
settings (7,127). Yet, qualitative research
within implementation science is
“positivist and deductive in nature, with
their use increasingly guided by theories
and organized by one or more
implementation models or frameworks” p.
4 (24). There seems to be a tug-of-war
between finding out what stakeholders
value through genuine participatory
research versus employing a methodology
that is rapid and geared to specific issues
determined a priori.
• In other words, it seems that we are trying
to employ seemingly value-free methods
to achieve real-world value.
• Scientific paradigms are human
constructions (19,54). Paradoxically, our
deeply-held values as scientists influence

65
our drive to be objective and value-free.
• Examination of the ontological (what is
the nature of reality?) and epistemological
(what is the nature of knowledge)
foundations of the evidence that we’re
willing to accept as credible
(19,25,87,128) may facilitate our ability to
be truly pragmatic and stakeholder-
centered, acknowledging the role of values
in capturing what really matters to
stakeholders.
• Overall, it may not be feasible to
simultaneously achieve scientific rigor
characterized by systematic objectivity
and real-world relevance characterized by
practical meaning (8,129). Participatory
research that strives to accomplish both
may actually accomplish neither, having
tepid significance scientifically,
practically, and personally.
Incongruence of a prior/systematic design
within participatory process: The GRA
grappled with the need for detailed a priori
methods sections for grant applications and
dissertation proposals, even when
investigators intend the direction of the
research—including outcomes—to truly
develop from IRPP input within a
participatory approach.
Opportunity for Progress:
Funding avenues for the invisible
relational work in participatory
research
• Trying describe her method for finding community
members to teach seminars at the Mom Expo: “I’m
trying to write down how I will systematically go about
‘recruiting’ educators for the Mom Expo so that the
process could be replicated. The general action of
genuinely listening to a person in an environment in
which she is comfortable can be replicated on some
level, but there’s not an objective, systematic equation
for building true trust. Just like recruiting collegiate
swimmers, connecting with community members takes
time and emotional energy but it can’t be distilled into
something objective and traditionally ‘scientific.’ The
distilled part, the replicable part is love and
“humbition” and I don’t think that’s going to fly in the
methods section” (February 13, 2019).
• Successful D&I grant writing requires
well-reasoned clarity with pre-established
collaborators and benchmarks (76). In
addition, grant writing for the National
Institutes of Health (NIH) requires “strict
application of the scientific method to
ensure robust and unbiased experimental
design, methodology, analysis,
interpretation, and reporting” (NIH Grant
Writing handbook, page 16).
• These descriptions of what it takes to win
a grant suggest that participatory research
is not fundable—at least not participatory
research that leaves room for naturalistic
networking, authentic exploration, and
iterative enactment of what stakeholders—
66
like pregnant women—really value.
• Currently, the networking and
relationship-building inherent in
participatory research appears to be
“invisible work”—time consuming but
unrecognized (130–132)
Lack of researcher
reflexivity/situatedness/positionality: In
leading the IRPP, the GRA found that what
she had learned in various leadership trainings
was not common in implementation science.
There appeared to be no training, guidelines,
or frameworks about how to leverage her own
leadership style and personality to optimize
the participatory approach. Other
implementation researchers she met through
the year were also directly leading
participatory efforts involving stakeholders
but had received no leadership training or
instruction about the importance of
intrapersonal capacity.
Opportunity for Progress:
Leveraging researchers’ personality
strengths and honing leadership skills
• “There were mentions of soft skills at D&I [11th Annual
Conference], but the D&I competencies from the [D&I
graduate school] class syllabus don’t reflect how those
soft skills might really matter” (December 8, 2018).
• “The first thing we did in the Energizing People for
Performance Executive Education program [at
Northwestern University’s Kellogg School of Business]
was take various assessments to understand our own
behaviors, communication, and personality as a
centerpiece to effective leadership. My teams swam
much better after I realized that my intense focus was
unintentionally intimidating to my athletes and that my
analytical, perfectionistic tendencies slow down the
process of doing anything” (December 27, 2018).
• “Suddenly [in running labs, collaborating in team
science, leading meetings with stakeholders],
researchers who have grown up (in school, etc.) being
praised for accuracy, analytical skills, depth of
knowledge, and ability to navigate peer-reviewed
literature have to build spontaneity and easy-going
attitudes that work for relationship-building and
navigating real-time personal situations. It’s like when I
needed to switch from the athlete mindset of staring at
the line in the bottom the pool to the coaching mindset
of connecting with people. I didn’t have to
fundamentally change my core self, I just had to
develop awareness of my ingrained focused and
working style” (February 22, 2019).
• After listening to a podcast of Graham Duncan
describing how our greatest strengths are adjacent to
• Personality traits are related to leadership
styles (133,134) and leadership styles
influence (81) team performance including
communication and cohesion (133,135–
137).
• The influence of researchers’ leadership
styles and personalities on team science
(138) and participatory research have not
been studied, even though both
approaches are advocated. We know little
about implementation researchers’
leadership styles and personalities,
including their effects on the participatory
process.
• However, research indicates that
scientists—like all humans—have
adaptive and maladaptive personality
facets such as self-critical perfectionism
related to perseverative cognition and
inadequate recovery (61).
• On the adaptive side, researchers may also
have high levels of openness which is the
capacity for change, variety, and novelty
(139). Openness is positively associated
with creativity, number of citations, and h-
index but not number of publications (60).
(See discussion of publish or perish
below.)
• Understanding their own personalities and
strengths could help researchers prevent
67
our greatest dysfunctions: “So now I’m feeling like an
Aristotelian tragic hero: Just call me Oedipus Rex, Phd
wannabe implementation extraordinaire. The
determination that that earns me praise and the very
GRA position that I currently hold is the same
determination that causes this eye twitch from standing
in front of the computer long after I’ve lost the edge of
creativity and insight” (March 16, 2019).
fatigue and burnout by offsetting the ego
depletion that occurs when we reach the
end of our willpower (58,59). In other
words, constantly keeping natural
personality traits in check or extending
into areas that don’t suit our personal
values could deplete intrapersonal
resources related to cognitive performance
(e.g. attention) and general quality of life.
Theme #3: Research/Academia Culture: “I’m constantly reinforcing the very culture that stresses me out and slows the translational process by working
toward peer-reviewed publication. In other words, the assignments I receive and the assignments I strive to do as a D&I grad student undermine dissemination;
pouring my time into crafting information for journals and grad committees is necessary to earn my degree and paycheck, but it’s an energy suck away from
actually getting information to the public” (February 23, 2019).
SUBTHEME DESCRIPTION ETHNOGRAPHIC EVIDENCE THEORETICAL/LITERATURE DIALOGUE
Pressure to “publish or perish”: The GRA
felt torn between reinforcing the current
paradigms of productivity versus pursuing
transformational dissemination by bucking the
current focus on journals and repositories.
Opportunity for Progress:
Optimize motivation and
achievement orientation to improve
research quality and impact, instead of
overemphasizing publication quantity
• “One reason I left elite athletics was to get away from
the obsession with outcomes. But with the language
here—bean counting, line on the CV—I feel
submerged in a culture that quantifies personal worth
in productivity stats like number of publications. If I
hadn’t spent years disentangling my self-worth from
the time on a stopwatch, I would be probably be
unconsciously engrossed in this system of constantly
proving I’m enough by publishing something” (April
30, 2019).
• “It’s clear through all of the discussions at [prenatal]
yoga that women don’t want to be a research subject;
they don’t want the mom expo to feel like an
experiment. So I’ve got this choice—prioritize their
values OR prioritize peer-reviewed journal values.
They’re not mutually exclusive, but designing a study
for people who don’t want to be in a study is different
from designing a study for people who publish journals
and approve dissertations…I need to distinguish
between a service mindset and manuscript obsession”
(February 26, 2019).
• The ubiquitous pressure to publish or
perish has been called a perverse
incentive, influencing funding,
professional advancement, and even
scientific trustworthiness (65)
• On the spectrum from extrinsic to intrinsic
motivation, pressure to publish may foster
“controlled” types of motivation
associated with burnout, poorer
performance, and overall well-being
(67,68,140–142).
• Pressure to publish also reflects a
“performance” achievement orientation
that is based on proving one’s competence
in comparison to others, as opposed to a
“learning” or “mastery” achievement
orientation that is based on personal
growth regardless of comparison to others
(143–145).
68
Norms of multiple roles and
responsibilities: The GRA observed her
professors juggling teaching, research, and
service responsibilities and learned about PhD
career trajectories. She also read many online
bios of implementation researchers and
noticed the extensive email signatures. Even
though her dissertation committee encouraged
her to commit to one deep line of research
inquiry for the dissertation, she felt that
academia, implementation science, and
participatory research demand individuals to
spread themselves across multiple domains
and responsibilities.
Opportunity for Progress:
Streamline responsibilities and time
commitments to reducing competing
demands
• After reading guidelines for earning tenure: “It’s as if
tenure-track faculty are expected to be the coach, be
the swimmer, and be the referee all at one time”
(February 20, 2019).
• Reflecting on email signatures: “So. Many.
Positions. (And acronyms). It’s the opposite of
athletics. In athletics, individuals get more and more
specialized in one sport or one position in a sport as
they become more elite: They channel their energy
and invest their training time into specific sports which
is why it’s so rare to have multi-sport Olympians or
even Division I athletes. But in academia, it seems that
the road toward ‘eliteness’ requires individuals to take
on responsibilities in broader and broader realms—
to survive doing as many things as possible as opposed
to doing one or two things really, really well” (May 15,
2019).
• “It’s hard to take the reins of a new project when your
hands are already full” (scribbled in my notebook,
didn’t write the date).
• Research suggests that burnout is
associated with spending less than 20% of
one’s time on the activity that is most
meaningful to him or her (146).
• The Challenge-Hindrance Framework
from psychology posits that not all
“stress” is bad: Demanding activities that
are perceived as fulfilling (“challenges”)
are associated with beneficial outcomes
and life satisfaction while demanding
activities that are perceived as time-
consuming but meaningless
(“hindrances”) are associated with
negative outcomes and low life
satisfaction (147–150).
• “Attentional residue” between switching
focus from one job demand to another
suggests that multi-tasking may erode
work quality (108,151,152).
• In the illuminating article Are Academics
Irrelevant?, Randy Stoecker argues that
community-engaged researchers cannot
and should not expect or be expected to
have all the requisite skills to fill all of the
necessary roles, such as animator and
community organizer (18). To be relevant
and genuinely helpful to a community,
Stoecker suggests that researchers should
fill only the roles that reflect their skills.

69
References
1. Israel B, Schulz A, Parker E, Becker A. Community-based Participatory Research: Policy
Recommendations for Promoting a Partnership Approach in Health Research. Educ Heal.
2001;14(2):182–97.
2. Bodison SC, Sankaré I, Anaya H, Booker-Vaughns J, Miller A, Williams P, et al.
Engaging the Community in the Dissemination, Implementation, and Improvement of
Health-Related Research. Clin Transl Sci. 2015;8(6):814–9.
3. Livingood WC, Bilello LA, Choe U, Lukens-Bull K. Enhancing the Science of Discovery
in Public Health Systems and Services Research Through Participatory Research
Methods. Popul Health Manag. 2017;21(2):155–62.
4. Brady V, Lalor J. Space for human connection in antenatal education: Uncovering
women’s hopes using Participatory Action Research. Midwifery [Internet].
2017;55(January 2016):7–14. Available from:
http://dx.doi.org/10.1016/j.midw.2017.08.006
5. Keyes D. Earth of Omega: Passage to Planetization. First Edit. Wellesley, Massachusetts:
Brandon Publishing Co, Inc.; 1982.
6. Van Belle S, Rifkin S, Marchal B. The challenge of complexity in evaluating health
policies and programs: The case of women’s participatory groups to improve antenatal
outcomes. BMC Health Serv Res. 2017;17(1):1–6.
7. Glasgow R. What does it mean to be pragmatic? Pragmatic methods, measures, and
models to facilitate research translation. Heal Educ Behav. 2013;40(3):257–65.
8. Bauer MS, Damschroder L, Hagedorn H, Smith J, Kilbourne AM. An introduction to
implementation science for the non-specialist. BMC Psychol. 2015;3(1):1–12.
9. Oliver K, Kothari A, Mays N. The dark side of coproduction: Do the costs outweigh the
benefits for health research? Heal Res Policy Syst. 2019;17(1):1–10.
10. Reed JE, Howe C, Doyle C, Bell D. Simple rules for evidence translation in complex
systems: A qualitative study. BMC Med. 2018;16(1):1–20.
11. Howe A, Mathie E, Munday D, Cowe M, Goodman C, Keenan J, et al. Learning to work
together – lessons from a reflective analysis of a research project on public involvement.
Res Involv Engagem [Internet]. 2017;3(1):1. Available from:
http://researchinvolvement.biomedcentral.com/articles/10.1186/s40900-016-0051-x
12. Sawtell M, Sweeney L, Wiggins M, Salisbury C, Eldridge S, Greenberg L, et al.
Evaluation of community-level interventions to increase early initiation of antenatal care
in pregnancy: Protocol for the Community REACH study, a cluster randomised controlled
trial with integrated process and economic evaluations. Trials. 2018;19(1):1–13.
13. Hamilton CB, Hoens AM, Backman CL, McKinnon AM, McQuitty S, English K, et al.
An empirically based conceptual framework for fostering meaningful patient engagement
in research. Heal Expect. 2018;21(1):396–406.
14. Harvey G, McCormack B, Kitson A, Lynch E, Titchen A. Designing and implementing
two facilitation interventions within the “Facilitating Implementation of Research
Evidence (FIRE)” study: A qualitative analysis from an external facilitators’ perspective.
Implement Sci. 2018;13(1):1–14.
15. Koorts H, Naylor PJ, Laws R, Love P, Maple JL, van Nassau F. What hinders and helps
academics to conduct Dissemination and Implementation (D&I) research in the field of
nutrition and physical activity? An international perspective. Int J Behav Nutr Phys Act.

70
2020;17(1):7.
16. Davidoff F. Understanding contexts: how explanatory theories can help. Implement Sci.
2019;14(1):1–9.
17. Damschroder LJ. Clarity out of chaos: Use of theory in implementation research.
Psychiatry Res. 2019;283(June 2019).
18. Stoecker R. Are Academics Irrelevant. Am Behav Sci. 1999;42(5):840–54.
19. Guba E, Lincoln Y. Competing Paradigms in Qualitative Research. In: Denzin NK,
Lincoln YS, editors. Handbook of Qualitative Research [Internet]. SAGE Publications,
Inc.; 1994. p. 105–17. Available from:
http://steinhardtapps.es.its.nyu.edu/create/courses/3311/reading/10-guba_lincoln_94.pdf
20. Appleton J V., King L. Journeying from the philosophical contemplation of
constructivism to the methodological pragmatics of health services research. J Adv Nurs.
2002;40(6):641–8.
21. Denzin NK. Moments, mixed methods, and paradigm dialogs. Qual Inq. 2010;16(6):419–
27.
22. Syntetos A, Harwood S. Mixing methodologies and pragmatic commensurability. J Oper
Res Soc. 2011;62(4):806–9.
23. Bunger AC, Powell BJ, Robertson HA, MacDowell H, Birken SA, Shea C. Tracking
implementation strategies: A description of a practical approach and early findings. Heal
Res Policy Syst. 2017;15(1):1–12.
24. Qualitative Research in Implementation Science (QUALRIS). Qualitative Methods In
Implementation Science. 2018; Available from:
https://cancercontrol.cancer.gov/IS/docs/NCI-DCCPS-ImplementationScience-
WhitePaper.pdf
25. Tracy S. Qualitative Research Methods: Collecting Evidence, Crafting Analysis,
Communicating Impact. First. Chichester, UK: Blackwell Publishing, Ltd; 2013.
26. Greenhalgh T, Raftery J, Hanney S, Glover M. Research impact: A narrative review.
BMC Med [Internet]. 2016;14(1). Available from: http://dx.doi.org/10.1186/s12916-016-
0620-8
27. Conte KP, Shahid A, Grøn S, Loblay V, Green A, Innes-hughes C, et al. Capturing
implementation knowledge: applying focused ethnography to study how implementers
generate and manage knowledge in the scale-up of obesity prevention programs.
Implement Sci. 2019;14(91):1–14.
28. Neumann C, Neumann I. Uses of the Self: Two Ways of Thinking about Scholarly
Situatedness and and Method. Milen J Int Stud. 2015;43(3):798–819.
29. Vannini P. Situatedness. In: Given LM, editor. The SAGE Encyclopedia of Qualitative
Research Methods [Internet]. Thousand Oaks, CA: SAGE Publications, Inc.; 2012. p.
815–6. Available from:
https://methods.sagepub.com/base/download/ReferenceEntry/sage-encyc-qualitative-
research-methods/n424.xml
30. Green CA, Duan N, Gibbons RD, Hoagwood KE, Palinkas LA, Albert G, et al.
Approaches to Mixed Methods Dissemination and Implementation Research: Methods,
Strengths, Caveats, and Opportunities. 2016;42(5):508–23.
31. Creswell J, Poth C. Qualitative Inquiry & Research Design. Fourth Edi. Salmon H, editor.
Thousand Oaks, CA: SAGE Publications; 2018.
32. Rogozińska E, Marlin N, Jackson L, Rayanagoudar G, Ruifrok AE, Dodds J, et al. Effects
71
of antenatal diet and physical activity on maternal and fetal outcomes: Individual patient
data meta-analysis and health economic evaluation. Health Technol Assess (Rockv).
2017;21(41).
33. Fook J. Developing Critical Reflection As a Research Method. In: Higgs J, Titchen A,
Horsfall D, Bridges D, editors. Creative Spaces for Qualitative Researching: Living
Research. Rotterdam: Sense Publishers; 2011. p. 55–64.
34. Brookfield S. Critically Reflective Practice. J Contin Educ Health Prof. 1998;18(1st):197–
205.
35. Mortari L. Reflectivity in Research Practice. Int J Qual Methods.
2015;14(5):160940691561804.
36. Lincoln YS, Guba EG. Naturalistic Inquiry. Newbury Park, CA: SAGE Publications;
1985.
37. Van Horn L, Beto J. Research Successful Approaches in Nutrition and Dietetics. Fourth
Edi. Van Horn L, Beto J, editors. Chicago, IL: Academy of Nutrition and Dietetics; 2019.
38. Estabrooks PA, Harden SM, Almeida FA, Hill JL, Johnson SB, Porter GC, et al. Using
Integrated Research-Practice Partnerships to Move Evidence-Based Principles into
Practice. Exerc Sport Sci Rev. 2019;47(3):176–87.
39. Harden SM, Johnson SB, Almeida FA, Estabrooks PA. Improving physical activity
program adoption using integrated research-practice partnerships: an effectiveness-
implementation trial. Transl Behav Med. 2017;7(1):28–38.
40. Johnson SB, Harden SM, Estabrooks PA. Uptake of evidence-based physical activity
programs: comparing perceptions of adopters and nonadopters. Transl Behav Med
[Internet]. 2016;6(4):629–37. Available from: http://dx.doi.org/10.1007/s13142-015-0371-
7
41. Wilson ML, Strayer TE, Davis R, Harden SM. Informed Adaptations of a Strength-
Training Program through a Research–Practice Partnership. Front Public Heal [Internet].
2018;6(March):1–9. Available from:
http://journal.frontiersin.org/article/10.3389/fpubh.2018.00058/full
42. Harden S, Beauchamp M, Pitts B, Nault E, Davy B, You W, et al. Group-based lifestyle
sessions for gestational weight gain management: a mixed method approach. Am J Health
Behav [Internet]. 2014;38(4):560–9. Available from:
http://ovidsp.ovid.com/ovidweb.cgi?T=JS&PAGE=reference&D=emed16&NEWS=N&A
N=613394541
43. Gerrard N. Some painful experiences of a white feminist therapist doing research with
women of color. In: Adleman J, editor. Racism in the lives of women. Binghamton, NY:
Harrington Park Press; 1995. p. 55–64.
44. Breen LJ. The researcher ‘ in the middle ’: Negotiating the insider / outsider dichotomy.
2007;19(1):163–74.
45. Pink S, Morgan J. Short-term ethnography: Intense routes to knowing. Symb Interact.
2013;36(3):351–61.
46. Emerson MR, Fretz RI, Shaw LL. Fieldnotes in Ethnographic Research. Writ Ethnogr
Fieldnotes. 1995;1–32.
47. Nilsen P. Making sense of implementation theories, models and frameworks. Implement
Sci. 2015;10(1):1–13.
48. Choi B, Pak A. Multidisciplinarity , interdisciplinarity and transdisciplinarity in health
research , services , education and policy : 1 . Definitions , objectives , and evidence of

72
effectiveness. Clin Investig Med. 2006;29(6):351–64.
49. Ross LE. An account from the inside: Examining the emotional impact of qualitative
research through the lens of “insider” research. Qual Psychol. 2017;4(3):326–37.
50. Blythe S, Wilkes L, Jackson D, Halcomb E. The challenges of being an insider in
storytelling research. Nurse Res. 2013;21(1):8–12.
51. Aarons GA, Sklar M, Mustanski B, Benbow N, Brown CH. “Scaling-out” evidence-based
interventions to new populations or new health care delivery systems. Implement Sci.
2017;12(1):1–13.
52. Gleick J. Making a new science: Chaos. New York: Penguin Books; 1987.
53. Lorenz E. Predictability: Does the Flap of a Butterfly’s Wings in Brazil Set Off a Tornado
in Texas? [Internet]. 1972. Available from:
http://www.ias.ac.in/article/fulltext/reso/020/03/0260-02
54. Eldredge N, Gould S. Punctuated equilibria: An alternative to phyletic gradualism. In:
Schopf T, editor. Models in paleobiology. San Francisco: Freeman Cooper & Co; 1972. p.
82–115.
55. Spence GB, Stout-Rostron S, Van Reenen M, Glashoff B. Exploring the delayed effects of
leadership coaching: a pilot study. Coaching. 2019;12(2):125–46.
56. Picciotto R. Donald T . Campbell’ s Evolutionary Perspective and its Implications for
Evaluation. J Multidiscip Educ. 2019;15(33):1–15.
57. Dewe P, O’Driscoll M, Cooper C. Theories of Psychological Stress at Work. In: Gatchel
R, Schultz I, editors. Handbook of Occupational Health and Wellness. New York: Spring
Science + Business Media; 2012.
58. Baumeister R, Bratslavsky E, Muraven M, Tice D. Ego Depletion: Is the Active Self a
Limited Resource? J Pers Soc Psychol. 1998;74(5):1252–65.
59. Baumeister RF, Tice DM, Vohs KD. The Strength Model of Self-Regulation: Conclusions
From the Second Decade of Willpower Research. Perspect Psychol Sci. 2018;13(2):141–
5.
60. Grosul M, Feist GJ. The creative person in science. Psychol Aesthetics, Creat Arts.
2014;8(1):30–43.
61. Flaxman PE, Ménard J, Bond FW, Kinman G. Academics’ Experiences of a Respite From
Work: Effects of Self-Critical Perfectionism and Perseverative cognition on Postrespite
Well-Being. J Appl Psychol. 2012;97(4):854–65.
62. Flett G, Hewitt P. Perfectionism and maladjustments: An overview of theoretical,
definitional, and treatment issues. In: Flett G, Hewitt P, editors. Perfectionism: Theory,
research, and treatment. Washington, DC: American Psychological Association; 2002. p.
5–32.
63. Brosschot JF, Gerin W, Thayer JF. The perseverative cognition hypothesis: A review of
worry, prolonged stress-related physiological activation, and health. J Psychosom Res.
2006;60(2):113–24.
64. Ottaviani C, Thayer JF, Verkuil B, Lonigro A, Medea B, Couyoumdjian A, et al.
Physiological concomitants of perseverative cognition: A systematic review and meta-
analysis. Psychol Bull. 2016;142(3):231–59.
65. Grimes DR, Bauch CT, Ioannidis JPA. Modelling science trustworthiness under publish or
perish pressure. R Soc Open Sci [Internet]. 2018;5(171511):1–14. Available from:
http://dx.doi.org/10.1098/rsos.171511
66. Horne R, Petrie K, Wessley S. H-index pathology. BMJ. 2009;339:b5356:1447–8.
73
67. Marylène G, Edward LD. Self-Determination Theory and Work Motivation. J Organ
Behav [Internet]. 2005;26(4):331–62. Available from:
http://usherbrooke.summon.serialssolutions.com/link/0/eLvHCXMwTV3NCsIwDC6i4H
mgvfoCHf3feh4bgiAijs1j0y53f94f41TwFJJLAglf8h2SMLYzIAnzvDPeIVIPyCBtRC8h
WQxy_nM4jFV_dc0htH9o3hVsgfcN67v20uzF9xmASDQCaxEhEpN7H61MBhNZUFc1
0XFQMQedlHdQO5uTVtMkTcSQLMXhs6syYIBabdmSCPXE2
68. Deci E, Ryan R. Self-determination theory: A macrotheory of human motivation,
development, and health. Can Psychol. 2008;49(3):182–5.
69. Elliot AJ, McGregor HA. A 2 × 2 achievement goal framework. J Pers Soc Psychol.
2001;80(3):501–19.
70. Harrington R, Loffredo DA. Insight, rumination, and Self-Reflection as predictors of well-
being. J Psychol Interdiscip Appl. 2011;145(1):39–57.
71. Grant A, Franklin J, Langford P. The Self-Reflection and Insight Scale: A New Measure
of Private Self-Consciousness. Soc Behav Pers. 2002;30(8):821–36.
72. Thompson D. Workism is Making Americans Miserable. The Atlantic [Internet]. 2019
Feb; Available from: https://www.theatlantic.com/ideas/archive/2019/02/religion-
workism-making-americans-miserable/583441/
73. Gidden A. The constitution of society: Outline of the theory of structuration. Berkeley,
California: University of California Press; 1984.
74. Gerke D, Lewis E, Prusaczyk B, Hanley C, Baumann A, Proctor E. Implementation
Outcomes Toolkit. St. Louis, MO; 2017.
75. Padek M, Mir N, Jacob RR, Chambers DA, Dobbins M, Emmons KM, et al. Training
scholars in dissemination and implementation research for cancer prevention and control:
A mentored approach. Implement Sci. 2018;13(1):1–13.
76. Brownson RC, Colditz GA, Dobbins M, Emmons KM, Kerner JF, Padek M, et al.
Concocting that Magic Elixir: Successful Grant Application Writing in Dissemination and
Implementation Research. Clin Transl Sci. 2015;8(6):710–6.
77. Proctor E, Silmere H, Raghavan R, Hovmand P, Aarons G, Bunger A, et al. Outcomes for
implementation research: Conceptual distinctions, measurement challenges, and research
agenda. Adm Policy Ment Heal Ment Heal Serv Res. 2011;38(2):65–76.
78. Zuidgeest M, Goetz I, Groenwold R, Irving E, van Thiel G, Grobbe D. Series: Pragmatic
trials and real world evidence: Paper 1. Introduction. J Clin Epidemiol. 2017;88:7–13.
79. Thorpe KE, Zwarenstein M, Oxman AD, Treweek S, Furberg CD, Altman DG, et al. A
pragmatic-explanatory continuum indicator summary (PRECIS): a tool to help trial
designers. J Clin Epidemiol [Internet]. 2009;62(5):464–75. Available from:
http://dx.doi.org/10.1016/j.jclinepi.2008.12.011
80. Institute of Development Studies. Participatory Methods: Reflective Practice [Internet].
[cited 2020 Jan 22]. Available from: www.participatorymethods.org/methods/reflective-
practice
81. Barnes CM, Guarana CL, Kong DT. Too Tired to Inspire or Be Inspired: Sleep
Deprivation and Charismatic Leadership. J Appl Psychol. 2016;101(8):1191–9.
82. Biesta G. Why “What Works” Still Won’t Work: From Evidence-Based Education to
Value-Based Education. Stud Philos Educ. 2010;29:491–503.
83. Biesta G. On the two cultures of educational research, and how we might move ahead:
Reconsidering the ontology, axiology and praxeology of education. Eur Educ Res J.
2015;14(1):11–22.

74
84. Scotland J. Exploring the philosophical underpinnings of research: Relating ontology and
epistemology to the methodology and methods of the scientific, interpretive, and critical
research paradigms. English Lang Teach. 2012;5(9):9–16.
85. Fulford K. Values-Based Practice: A New Partner to Evidence-Based Practice and A First
for Psychiatry. Mens Sana Monogr. 2008;6(1):10–21.
86. Bae J-M. Value-based medicine: concepts and application. Epidemiol Health.
2015;37:e2015014.
87. Archibald T. Whose Extension Counts? A Plurality of Extensions and Their Implications
for Credible Evidence Debates. J Hum Sci Ext. 2019;7(2):22–35.
88. Choi B, Pak A. Multidisciplinarity, interdisciplinarity, and transdisciplinarity in health
research, services, education and policy: 1. Definitions, objectives, and evidence of
effectiveness. Clin Investig Med. 2006;29(6):351–64.
89. Tabak RG, Khoong EC, Chambers D, Brownson RC. Models in dissemination and
implementation research: useful tools in public health services and systems research. Am J
Prev Med. 2012;43(3):337–50.
90. Walton G. Beyond Winning. Champaign, IL: Leisure Press; 1992.
91. Wooden J, Jamison S. Wooden on Leadership. New York: McGraw-Hill; 2005.
92. Glasgow RE, Harden SM, Gaglio B, Rabin B, Smith ML, Porter GC, et al. RE-AIM
Planning and Evaluation Framework: Adapting to New Science and Practice With a 20-
Year Review. Front Public Heal. 2019;7(March).
93. Hobfall S. Conservation of Resources. Am Psychol. 1989;44(3):513–24.
94. Van Belle S, Van De Pas R, Marchal B. Towards an agenda for implementation science in
global health: There is nothing more practical than good (social science) theories. BMJ
Glob Heal. 2017;2(2):2016–8.
95. Law J. After Method: Mess in social science research. Abingdon, Oxon: Routledge; 2004.
96. Mujika I. Tapering and Peaking for Optimal Performance. Champaign, IL: Human
Kinetics; 2009.
97. Bales M, Swank A. ACSM’s Exercise Testing and Prescription. Bayles MP, Swank AM,
editors. Philadelphia: Wolters Kluwer; 2018.
98. Kim S, Park YA, Niu Q. Micro-break activities at work to recover from daily work
demands. J Organ Behav. 2017;38(1):28–44.
99. Lee KE, Williams KJH, Sargent LD, Williams NSG, Johnson KA. 40-second green roof
views sustain attention: The role of micro-breaks in attention restoration. J Environ
Psychol [Internet]. 2015;42:182–9. Available from:
http://dx.doi.org/10.1016/j.jenvp.2015.04.003
100. Ouyang K, Cheng BH, Lam W, Parker SK. Enjoy Your Evening, Be Proactive Tomorrow:
How Off-Job Experiences Shape Daily Proactivity. J Appl Psychol. 2019;
101. Zaccaro A, Piarulli A, Laurino M, Garbella E, Menicucci D, Neri B, et al. How Breath-
Control Can Change Your Life: A Systematic Review on Psycho-Physiological Correlates
of Slow Breathing. Front Hum Neurosci [Internet]. 2018;12(September):1–16. Available
from: https://www.frontiersin.org/article/10.3389/fnhum.2018.00353/full
102. Gerritsen RJS, Band GPH. Breath of Life: The Respiratory Vagal Stimulation Model of
Contemplative Activity. Front Hum Neurosci [Internet]. 2018;12(October):397. Available
from: https://www.frontiersin.org/article/10.3389/fnhum.2018.00397/full
103. Perlow L. Sleeping with Your Smartphone. Boston: Harvard Business Review Press;
2012.
75
104. Hair M, Renaud K V., Ramsay J. The influence of self-esteem and locus of control on
perceived email-related stress. Comput Human Behav. 2007;23(6):2791–803.
105. Kushlev K, Dunn EW. Checking email less frequently reduces stress. Comput Human
Behav [Internet]. 2015;43:220–8. Available from:
http://dx.doi.org/10.1016/j.chb.2014.11.005
106. Mano RS, Mesch GS. E-mail characteristics, work performance and distress. Comput
Human Behav [Internet]. 2010;26(1):61–9. Available from:
http://dx.doi.org/10.1016/j.chb.2009.08.005
107. Leroy S, Schmidt AM. The effect of regulatory focus on attention residue and
performance during interruptions. Organ Behav Hum Decis Process [Internet].
2016;137:218–35. Available from: http://dx.doi.org/10.1016/j.obhdp.2016.07.006
108. Leroy S. Why is it so hard to do my work ? The challenge of attention residue when
switching between work tasks. Organ Behav Hum Decis Process [Internet].
2009;109(2):168–81. Available from: http://dx.doi.org/10.1016/j.obhdp.2009.04.002
109. Csikszentmihalyi M. Flow: The psychology of optimal experience. New York, New York:
Harper Perennial; 1990.
110. Ericsson KA. Summing Up Hours of Any Type of Practice Versus Identifying Optimal
Practice Activities: Commentary on Macnamara, Moreau, & Hambrick (2016). Perspect
Psychol Sci. 2016;11(3):351–4.
111. Ericsson KA, Krampe RT, Tesch-Römer C. The role of deliberate practice in the
acquisition of expert performance. Psychol Rev. 2005;100(3):363–406.
112. Dandar V, Gribsby R, Bunton S. Burnout Among U.S. Medical School Faculty. AAMC
Anal Br. 2019;19(1).
113. Messias E, Gathright MM, Freeman ES, Flynn V, Atkinson T, Thrush CR, et al.
Differences in burnout prevalence between clinical professionals and biomedical scientists
in an academic medical centre: A cross-sectional survey. BMJ Open. 2019;9(2):1–7.
114. Holleman WL, Cofta-woerpel LM, Gritz ER. Stress and Morale of Academic Biomedical
Scientists. Acad Med. 2015;90(5):562–4.
115. Powell K. Work–life balance: Break or burn out. Nature. 2017;545(7654):375–7.
116. Kivimäki M, Jokela M, Nyberg ST, Singh-Manoux A, Fransson EI, Alfredsson L, et al.
Long working hours and risk of coronary heart disease and stroke: A systematic review
and meta-analysis of published and unpublished data for 603 838 individuals. Lancet.
2015;386(10005):1739–46.
117. Meijman TF, Mulder G. Psychological Aspects of Workload. In: Drenth PJ, Theirry H, J
de WC, editors. Work Psychology. 2nd Editio. East Sussex; 1998. p. 5–28.
118. Debus ME, Sonnentag S, Deutsch W, Nussbeck FW. Making flow happen: The effects of
being recovered on work-related flow between and within days. J Appl Psychol.
2014;99(4):713–22.
119. Binnewies C, Sonnentag S, Mojza EJ. Feeling Recovered and Thinking About the Good
Sides of One’s Work. J Occup Health Psychol. 2009;14(3):243–56.
120. Zijlstra FRH, Cropley M, Rydstedt LW. From recovery to regulation: An attempt to
reconceptualize “recovery from work.” Stress Heal. 2014;30(3):244–52.
121. Rager KB. Compassion stress and the qualitative researcher. Qual Health Res.
2005;15(3):423–30.
122. Gair S. Feeling their stories: Contemplating empathy, insider/outsider positionings, and
enriching qualitative research. Qual Health Res. 2012;22(1):134–43.
76
123. Hubbard G, Backett-milburn K. Working with emotion: issues for the researcher in
fieldwork and teamwork. Int J Soc Res Methodol. 2001;4(1):119–237.
124. Padek M, Colditz G, Dobbins M, Koscielniak N, Proctor EK, Sales AE, et al. Developing
educational competencies for dissemination and implementation research training
programs: an exploratory analysis using card sorts. Implement Sci. 2015;10(114):1–9.
125. Cropley M, Zijlstra FRH, Querstret D, Beck S. Is work-related rumination associated with
deficits in executive functioning? Front Psychol. 2016;7(SEP):1–8.
126. Calderwood C, Bennett AA, Gabriel AS, Trougakos JP, Dahling JJ. Too anxious to help?
Off-job affective rumination as a linking mechanism between work anxiety and helping. J
Occup Organ Psychol. 2018;91(3):681–7.
127. Glasgow R, Estabrooks P. Pragmatic Applications of RE-AIM for Health Care Initiatives
in Community and Clinical Settings. Prev Chronic Dis. 2018;15(E02).
128. Creswell JW. Choosing among five approaches. Qual Inq Res Des. 2012;
129. Geng EH, Peiris D, Kruk ME. Implementation science: Relevance in the real world
without sacrificing rigor. PLoS Med. 2017;14(4):1–5.
130. Star SL, Strauss A. Layers of Silence, Arenas of Voice: The Ecology of Visible and
Invisible Work. Comput Support Coop Work. 1999;8(1–2):9–30.
131. Daniels AK. Invisible Work. Soc Study Soc Probl. 1987;34(5):403–15.
132. Dhara A. Invisible work. Can Fam Physician. 2019;65(61):426–7.
133. Bono JE, Judge TA. Personality and Transformational and Transactional Leadership: A
Meta-Analysis. J Appl Psychol. 2004;89(5):901–10.
134. Hautala TM. The relationship between personality and transformational leadership. J
Manag Dev. 2006;25(8):777–94.
135. Schaubroeck J, Lam SSK, Cha SE. Embracing Transformational Leadership: Team
Values and the Impact of Leader Behavior on Team Performance. J Appl Psychol.
2007;92(4):1020–30.
136. Bass BM, Avolio BJ, Jung DI, Berson Y. Predicting unit performance by assessing
transformational and transactional leadership. J Appl Psychol. 2003;88(2):207–18.
137. Smith MJ, Arthur CA, Hardy J, Callow N, Williams D. Transformational leadership and
task cohesion in sport: The mediating role of intrateam communication. Psychol Sport
Exerc [Internet]. 2013;14(2):249–57. Available from:
http://dx.doi.org/10.1016/j.psychsport.2012.10.002
138. Syme SL. The Science of Team Science. Assessing the Value of Transdisciplinary
Research. Am J Prev Med. 2008;35(2 SUPPL.):94–5.
139. Lounsbury JW, Foster N, Patel H, Carmody P, Gibson LW, Stairs DR. An investigation of
the personality traits of scientists versus nonscientists and their relationship with career
satisfaction. R D Manag. 2012;42(1):47–59.
140. Lyness JM, Lurie SJ, Ward DS, Mooney CJ, Lambert DR. Engaging students and faculty:
Implications of self-determination theory for teachers and leaders in academic medicine.
BMC Med Educ. 2013;13(1):1.
141. Tremblay MA, Blanchard CM, Taylor S, Pelletier LG, Villeneuve M. Work Extrinsic and
Intrinsic Motivation scale: its value for organizational psychology research. Can J Behav
Sci. 2009;41(4):213–26.
142. Cerasoli CP, Nicklin JM, Ford MT. Intrinsic motivation and extrinsic incentives jointly
predict performance: A 40-year meta-analysis. Psychol Bull. 2014;140(4):980–1008.
143. Elliot AJ, Murayama K. On the Measurement of Achievement Goals: Critique,

77
Illustration, and Application. J Educ Psychol. 2008;100(3):613–28.
144. Leggett EL, Dweck CS. A Social-Cognitive Approach to Motivation and Personality.
Psychol Rev [Internet]. 1988;95(2):256–73. Available from:
http://citeseerx.ist.psu.edu/viewdoc/download?doi=10.1.1.583.9142&rep=rep1&type=pdf
145. Utman CH. Performance effects of motivational state: A meta-analysis. Personal Soc
Psychol Rev. 1997;1(2):170–82.
146. Shanafelt T, West C, Sloan J, Novotny P, Poland G, Menaker R, et al. Career fit and
burnout among academic faculty. Arch Intern Med [Internet]. 2009;169(10):990–5.
Available from:
http://www.embase.com/search/results?subaction=viewrecord&from=export&id=L35467
1349%0Ahttp://archinte.ama-
assn.org/cgi/reprint/169/10/990%0Ahttp://dx.doi.org/10.1001/archinternmed.2009.70
147. Searle B, Auton J. The Merits of Measuring Challenge and Hindrance Appraisal. Anxiety,
Stress Coping. 2015;28:121–43.
148. Boswell WR, Olson-Buchanan JB, LePine MA. Relations between stress and work
outcomes: The role of the felt challenge, job control, and psychological strain. J Vocat
Behav. 2004;64(1):165–81.
149. French KA, Allen TD, Henderson TG. Challenge and Hindrance Stressors and Metabolic
Risk Factors. 2019;24(3):307–21.
150. Cavanaugh MA, Boswell WR, Boudreau JW. “Challenge” and “Hindrance” related stress
among U.S. managers. 1998;(May 2014):27.
151. Rosen C. The Myth of Multitasking. New Atl. 2008;20(Spring):105–10.
152. González VM, Mark G. Constant, Constant, Multi-tasking Craziness”: Managing Multiple
Working Spheres. Most [Internet]. 2004;6(1):113–20. Available from:
http://portal.acm.org/citation.cfm?id=985707
153. Lincoln YS, Guba EG. Establishing Trustworthiness. Naturalistic Inquiry. Newbury Park,
CA: Sage Publications; 1985. 289–331 p.
154. Maslow A. A theory of human motivation. Psychol Rev. 1943;50:370–96.

78
Manuscript 3
Fueling Dissemination and Implementation researchers:
Pilot test and RE-AIM evaluation of an individualized coaching program

79
Abstract
Background: One-on-one coaching is a novel approach to help researchers flourish amidst the
challenges of conducting Dissemination & Implementation (D&I) Science. No coaching
programs for D&I researchers or scientists in general have been empirically evaluated.
Furthermore, coaching research is limited by conceptual and methodological issues, particularly
a lack of implementation detail. Therefore, the purpose of this exploratory work was to apply
D&I principles to the development and evaluation of a coaching program that supports D&I
researchers themselves.
Methods: Investigators operationalized the RE-AIM (Reach, Effectiveness, Adoption,
Implementation, Maintenance) Framework to pragmatically pilot test an individualized, nine
session coaching program called FUEL (Focus, Unplug, Exercise, Love) among D&I
researchers. For reach, investigators used descriptive statistics to compare recruitment strategies
and describe the study sample. Investigators also conducted rapid data analysis of baseline open-
ended questions to further describe participants. For implementation (i.e., feasibility),
investigators tracked the program through coaching and scheduling logs and also conducted
rapid qualitative data analysis of session logs. For effectiveness and maintenance, investigators
took a longitudinal qualitative approach with iterative content analysis of open-ended survey
items and proxy semi-structured interviews that they triangulated with descriptive statistics of
quantitative measures collected pre-program, post program, three month follow-up, and six
month follow-up.
Results: Reach results indicate that demand for coaching exceeded study enrollment capacity
(n=16); that listserv email was an effective recruitment strategy; and, that proxies perceived
participants as productive and successful pre-program. Implementation results include that 15
80
participants (93.75%) rescheduled at least one session; that the coach spent 12.96+2.82 hours per
participant planning and implementing sessions; and that the coach tailored session content for
each participant. Effectiveness and maintenance results indicate that participants valued the
program and experienced multiple benefits related to productivity, happiness, and health. Taken
together, RE-AIM findings demonstrate that the core components of a coaching program for
D&I researchers are (1) a transformational coach, (2) compelling content with a variety of
evidence-based tools, and (3) one-on-one flexible sessions.
Conclusion: This pilot study provides promising, convergent lines of evidence that a coaching
program is feasible and beneficial for D&I researchers. Future work is needed to investigate
adoption and understand effectiveness.
Key Words: Coaching, qualitative research, RE-AIM, flourishing, work stress, human
development
Contributions to the literature:
• This pilot study is the first empirical exploration of a coaching program for D&I
researchers.
• Unlike most coaching research among other populations, this study includes extensive
reach and implementation details that inform the delivery and core components of a
program to support the well-being and professional development of D&I researchers.
• This study contributes preliminary longitudinal evidence that a one-on-one virtual
coaching program is valued by D&I researchers as support for health, personal growth,
and professional development.
81
Introduction
Emergent research reveals multilevel barriers to conducting Dissemination and
Implementation (D&I) Science (1–3). It is not just the research-practice gap itself that is
problematic: The study of that gap is fraught with practical, empirical, and professional
challenges. These challenges include incommensurable scientific paradigms, logistical
complications, invisible work excluded from traditional benchmarks for professional
advancement, and lack of training, skills, or personal traits related to real-world implementation
(2–6). Ostensibly, strain and work stress (7) from these barriers could erode D&I researchers’
capacities to advance the field (3). One novel approach to fueling researchers’ capacities is
coaching.
Coaching involves “guiding an individual’s movement through a cycle of self-discovery
that ultimately stimulates sustained well-being and functioning” (8). Coaching is a critical
component of the deliberate practice required for expert performance in a variety of fields (9–
12). In medicine, research demonstrates that individualized coaching is a promising approach to
reduce physician burnout (13) and improve health outcomes among individuals with chronic
disease (14–16). In the workplace, meta-analyses indicate that coaching has significant positive
effects on psychosocial and performance outcomes (8,17,18). Finally, in academia, qualitative
research illustrates that coaching may cultivate transformational leadership and self-care among
college deans (19).
There appear to be no empirical investigations of coaching among D&I researchers, or
scientists in general. Within D&I Science, Mentored Training for Dissemination and
Implementation Research in Cancer (MT-DIRC) (20) and the Training Institute for
Dissemination and Implementation Research in Health (TIDIRH) (21) aim to improve early

82
career researchers’ professional competencies. However, there are no programs targeting
psychosocial capacity and personal support for D&I researchers in various career stages. This
gap reflects an academic culture of impervious workism (3,22,23) and a scientific community
that “is not very good at talking openly about personal challenges” (24).
Within this guarded scientific culture, it was not known if D&I researchers would enroll
in a coaching program and if a coaching program would be feasible among such a time-strapped
population. Furthermore, like D&I Science, coaching science is a developing field with
conceptual and methodological issues. Throughout the coaching literature, there are consistent
calls to (1) clarify theoretical bases, (2) provide program detail including development and
implementation, (3) measure longitudinal outcomes, and (4) collect multisource data beyond
self-report measures (14,16,18). There is no consensus on the best methods for measuring
coaching effectiveness or even on which outcomes to measure (17,25). Because coaching is a
highly-individualized complex phenomenon, multiple researchers recommend using qualitative
methods to capture the nuanced human experience (18,25) and elucidate the coaching process
itself (16).
Overall, it appears that D&I Science and coaching can inform each other: D&I
researchers may benefit from coaching, and coaching research may benefit from D&I principles.
Therefore, the purpose of this study was to use the RE-AIM Framework (26,27) to develop and
pilot test a coaching program to support the well-being and professional development of D&I
researchers. The first aim was to develop the coaching program through stakeholder engagement
(28) and multiple forms of empirical evidence (29,30). The second aim was to pragmatically
(31,32) explore the reach, feasibility (i.e. implementation), and longitudinal effectiveness of the
coaching program.

83
This work is significant in investigating coaching as a novel, actionable approach to fuel
researchers through the widely discussed but unaddressed challenges of conducting D&I
Science. To avoid current limitations of coaching research, we delineate implementation details
that establish a foundation for empirical replicability and practical scalability (33). In addition,
the longitudinal design emphasizing multisource, qualitative data provides insight to the highly
subjective experience of coaching. This interdisciplinary work may advance the D&I and
coaching fields while helping individual researchers thrive—not just survive—amid daily
demands.
Methods
Developing the program
Investigators developed the coaching program through stakeholder engagement (1,28),
principles of designing for dissemination (34), practice-based judgment from the principal
investigator’s (PI’s) (A.S.) previous career as a collegiate coach, and a rigorous literature view
(see Appendix L). The coaching program, FUEL, included four domains: focus (work in
efficient and meaningful ways), unplug (recover from demands), exercise (incorporate
movement and physical activity in positive ways), and love (generate goodwill to self, others,
and situations). FUEL consisted of nine one-on-one coaching sessions based on constructs from
the Self-Regulation Model of Coaching (35,36), Self-Determination Theory (37), human
flourishing (38,39), and periodization (40,41) (see Appendix L). Investigators chose to deliver
FUEL remotely based on recent evidence that distance coaching is effective in preventing
physician burnout (13) and on research suggesting that the mode of workplace coaching (e.g.,
face-to-face, blended, virtual) does not moderate performance outcomes (17,42).
84
Evaluating the program: RE-AIM
In this exploratory pilot test, investigators used a mixed-methods approach (43) with
quantitative and qualitative measures across RE-AIM dimensions: reach (number, proportion,
and representativeness of program participants), effectiveness (impact of program on outcomes);
implementation (how the program is delivered); and maintenance (how long the results last)
(26,27). See Figure 1 below. Because this is a pilot test, investigators did not measure adoption
(number or types of organizations and settings that deliver a program). The Virginia Tech
Institutional Review Board approved this study (#19-854).
Investigators aimed to recruit a purposive sample (44,45) of 16 implementation researchers
via individual email, listserv email, and word-of-mouth (see electronic recruiting flyer in
Appendix O). The sample size was a pragmatic choice hypothesized to be a feasible coaching
volume. Eligibility was limited to individuals who (1) self-identified as implementation
researchers, (2) had completed a doctoral-level degree, (3) had a full-time professional position
that included research, (4) resided in the continental United States, and (5) spoke English.
Individuals who fulfilled eligibility criteria based on a Qualtrics screening questionnaire
were emailed a link to another Qualtrics questionnaire with informed consent. Subsequently, the
PI conducted one-on-one orientation sessions via telephone. During orientation, participants
scheduled their first coaching session and chose both the delivery mode (web-conference or
telephone) and the length of their sessions (10-60 minutes). The PI, who has 15 years of
professional coaching experience, an undergraduate degree in human development, and multiple
training certifications, served as the coach and offered sessions from 6 am – 8 pm Eastern
Standard Time on all seven days of the week from December 23, 2019 – April 3, 2020.
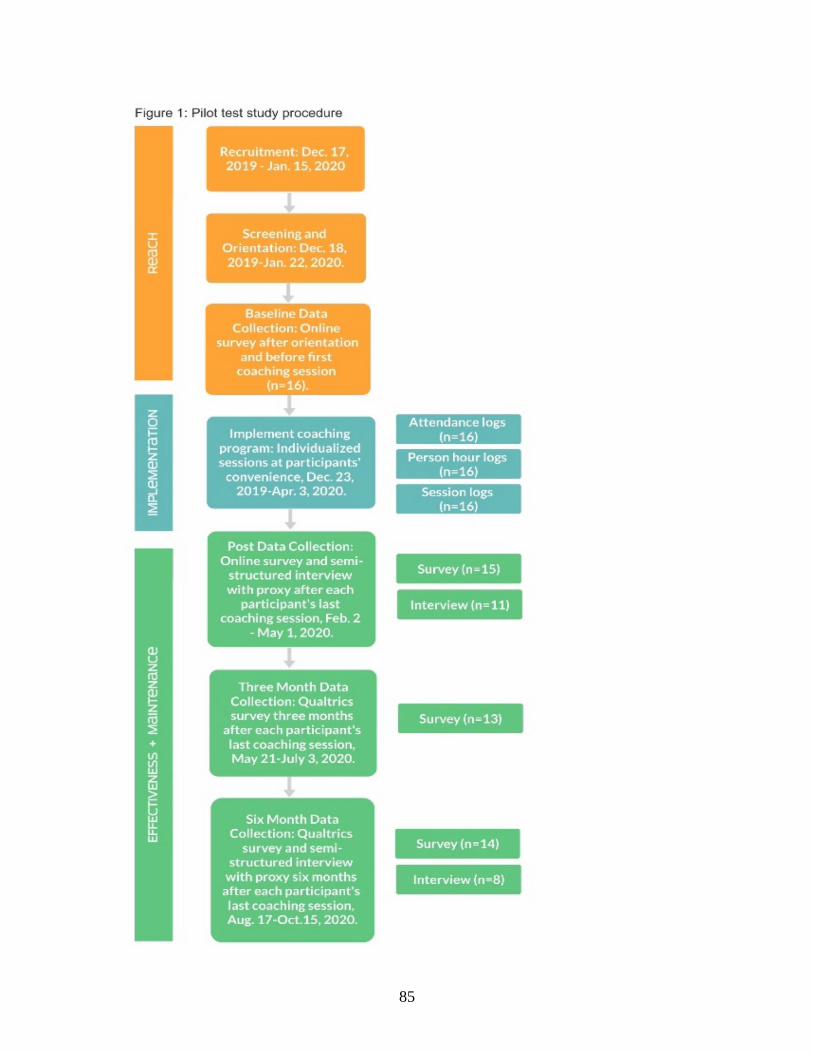
85
86
Reach
Investigators used proportions and frequencies to compare the reach of recruiting
strategies (i.e., individual email, listserv email, or word-of-mouth) and capture demographic and
professional characteristics of participants. Investigators also conducted rapid data analysis
(46,47) of baseline open-ended questions to describe participants’ work characteristics and
experiences.
Implementation
To capture implementation and assess feasibility, investigators analyzed three sets of logs
maintained by the coach through the program (see Appendix M). Attendance logs with session
start/end times, cancellations, and rescheduling were analyzed to describe fidelity to the coaching
program schedule. Person hour logs of direct participant interactions and administrative tasks
were analyzed to quantify the time investment of the coach, including overall hours, coaching
hours, and planning hours. Session logs, which the coach completed within three hours of each
session and emailed to participants for member checking (44,48), were analyzed to describe
coaching content. Originally, investigators planned to use the session logs to assess participants’
fidelity to action plans (i.e., adherence to weekly goals).
For the session logs, two investigators (A.S., S.H.) independently performed deductive
rapid data analysis (46,47) to determine whether the original components of the coaching
program were included in each session. The original components of the coaching program plus
two components that emerged early in coaching sessions were used as six pre-determined codes
(focus, unplug, exercise, love, implementation, writing). For each session log for each
participant—a total of 929 potential instances—investigators determined whether the six codes

87
appeared at least once. Inter-rater agreement was 94.00%. For the six percent discrepancies,
investigators performed consensus validation and consulted a third “critical friend” (49).
Effectiveness and maintenance: surveys and interviews
To explore effectiveness and maintenance, investigators triangulated (43,44) data from
Qualtrics surveys administered to participants with data from semi-structured interviews
conducted with a “proxy” (colleague, friend, or family member of the participant). Participants
completed Qualtrics surveys at baseline, post program, three month follow-up, and six month
follow-up. Proxies completed semi-structured interviews post program and at six month follow-
up. See Appendix M for surveys and interview guides.
Participant survey measures and analysis: Surveys included quantitative and
qualitative (open-ended) items. The open-ended items focused on participants’ experiences and
perceived effects of the coaching program. The PI and senior investigator wrote the open-ended
items based on FUEL’s theoretical underpinnings and on their professional experiences coaching
and implementing health interventions.
To analyze responses to the open-ended items, three investigators (A.S., R.N., S.C.)
conducted iterative (50) content analysis (44,51) alternating between deductive and inductive
readings of the data. For this iterative analysis, the PI developed a codebook based on the
theoretical framework of FUEL, including the Self-Regulation Model of Coaching, the Self-
Determination Theory (37), and human flourishing (38,52). Using the codebook, investigators
independently read and coded participants’ written responses. Then, in a series of meetings,
investigators revised the codebook based on their inductive readings. This inductive portion of
the process included analytic memos (44,50) to capture emergent ideas and identification of
exemplars that expressed multiple codes in one response (50).

88
Surveys also included four quantitative scales related to well-being. The Balanced
Measure of Psychological Needs (BMPN) scale (53,54) is based on the Self-Determination
Theory (37) and comprises 18 items divided into six subscales measuring autonomy
satisfaction/frustration, competence satisfaction/frustration, and relatedness
satisfaction/frustration. The Flourishing Index is a 10 item, 11 point Likert scale measuring
holistic well-being (55,56). The Single-Item Sleep Quality Scale (SQS) is a one item, 11 point
Likert scale measuring sleep quality (57). The Stanford Leisure-Time Activity Categorical Item
(L-CAT) consists of a single item with six descriptions of physical activity levels from inactive
to very active (58). In addition to these scales, surveys included two pragmatic questions to
measure work behaviors in a typical week, including number of hours worked and percentage of
time spent on the most meaningful activities compared to hassles or hindrances (59,60).
To analyze quantitative data, investigators used descriptive statistics because of the pilot
test’s exploratory nature and small sample size inappropriate for inferential statistics.
Investigators applied intent-to-treat analysis with last-value-carried-forward for missing values
(61,62).
Proxy semi-structured interviews: After the final coaching session, the PI asked each
participant for contact information of an individual (“proxy”) who could provide an external
perspective of the participant’s behavior. The PI then emailed the proxy to obtain informed
consent and schedule a semi-structured interview. Using a semi-structured interview guide, the
PI conducted two telephone interviews with each proxy. The first interview occurred
immediately post program and the second interview was at six month follow-up. Both
interviews lasted 15-20 minutes and captured proxies’ perceptions of participants’ behaviors
related to work (focus), recovery (unplug), physical activity (exercise), interpersonal interactions

89
(love), and self perceptions (love). The PI audio-recorded and transcribed the interviews
verbatim. Observers were given the option to member check (48) the interview transcript. Two
investigators (A.S., S.H.) analyzed the interview transcripts using the previously described
iterative content analysis procedure.
To maximize trustworthiness (63), investigators implemented multiple validation strategies
(43,44,50,64) throughout data analysis (see Table 1).
In addition, to reduce observer bias and expectancy effects (44,65,66), investigators took
a two-tiered approach to de-identifying data in which the PI and senior investigator maintained
separate identification codes for participants. In the first tier, the PI emailed participants a
Qualtrics link and identification code; she did not share the identification codes with the senior
investigator. In the second tier, the senior investigator managed the completed surveys,
renaming the identification codes into new codes that she did not share with the PI. Therefore,
both the PI and senior investigator were blinded during analysis of surveys. For the semi-
structured interviews, only the senior investigator was blinded. The second and third authors
were blinded throughout the entire process. See reflexivity statements preceding the reference.
Table 1: Strategies to fortify trustworthiness of FUEL qualitative approach and analysis
Validation Strategy Session logs Surveys Interviews
Triangulating qualitative and quantitative data X X
Member checking X X
Conducting negative case analysis X X
Practicing reflexivity X X X
Maintaining audit trail X X X

90
Results
Reach
Reach of recruitment strategies: Recruitment emails were sent to administrators of
implementation listservs (n = 5) and to individuals (n=73) who were either a member of an
implementation science working group or first author of a manuscript published in a premier
journal of D&I Science. Target study enrollment (n=16) was filled approximately one month
after recruitment began. Investigators established a waitlist comprised of nine individuals who
completed the screening questionnaire after study capacity had been reached. Based on study
enrollment, investigators achieved 100% of the initial reach goal (16/16). Based on the study
enrollment plus waitlist, investigators achieved 156% of the initial reach goal (25/16). The
majority of participants and waitlist enrollees learned about the study through an implementation
listserv email (see Figure 2 below). Two of the participants and waitlist enrollees knew the
PI/coach prior to recruitment. For more detailed reach results, see Appendix O.
Reach in terms of participant characteristics: See Table 2 below for
sociodemographic and professional characteristics of study participants. The majority of
participants were female (n=12, 75.00%), white (n=12, 75.00%), and over the age of 40 (n=11,
68.75%). All participants (n=16, 100.00%) reported that they conducted participatory research.

91
Half of the participants (n=8) had no previous experience working with a coach. Although all
participants identified themselves as D&I researchers, only one had a doctoral degree in
Implementation Science.
Table 2: Characteristics of participants
Characteristics N %
Gender
Female 12 75.00%
Male 4 25.00%
Race, ethnicity, origin
Asian 1 6.25%
Black or African American 2 12.50%
Middle Eastern or North African 1 6.25%
White 12 75.00%
Age
Below 30 years 1 6.25%
30 to 39 years 4 25.00%
40 to 49 years 7 43.75%
50 to 59 years 4 25.00%
Region of Residence (USA)
Midwest 2 12.50%
Northeast 4 25.00%
West 5 31.25%
South 5 31.25%
Doctoral Degree
PhD 14 87.50%
DrPH/DPhil 1 6.25%
Doctor of Health Sciences 1 6.25%
Professional Discipline
Allied Health 2 12.50%
Clinical 1 6.25%
Epidemiology 1 6.25%
Public Health 3 18.75%
Rehabilitation Research 1 6.25%
Social Science 8 50.00%
Primary Institutional Affiliation
Government agency 1 6.25%
Private academic university 2 12.50%
Public academic university 5 31.25%
Research institution 2 12.50%
University medical center 1 6.25%
University medical school 1 6.25%
Veterans Health Administration 3 18.75%
Professional Position
Assistant professor 8 50.00%
Associate professor 1 6.25%
Postdoctoral research fellows 1 6.25%
Regional research administrator 1 6.25%
Research scientist 6 37.50%
92
Rapid data analysis revealed that FUEL reached individuals with a variety of work
experiences, motivations, and reasons for joining the study. The top three reported reasons for
enrolling were (1) learn to cope with stress and prevent burnout (n=5, 31.25%), (2) find work-life
balance (n=5, 31.25%), and (3) general curiosity (n=5, 31.25%). For more baseline
characteristics, see Appendix O.
Implementation
Session Attendance: Of the 16 participants, 14 (87.50%) completed all nine FUEL
sessions. One participant completed only seven sessions within the study time horizon, and one
participant dropped out after four sessions because of an adverse health event unrelated to FUEL.
Throughout the study, 15 participants (93.75%) rescheduled at least one session. The average
number of rescheduled sessions per participant was 2.3 with a range of 1 to 6. The average
number of weeks to complete all sessions was 10 with six participants (37.50%) completing the
program in the planned eight-week time period. All participants except for one selected Zoom
videoconferencing over telephone for the sessions.
Coaching process and content: In their first sessions, all participants (n=16) expressed
the demanding nature of their workloads. Therefore, the coach eschewed formal action plans or
dogmatic self-monitoring. Instead, the coach and participants discussed potential practices to
explore in the subsequent week. This adapted approach to accountability—and abandonment of
quantifying fidelity to action plans—reflects the central purpose of FUEL to recharge, not
burden, participants. While the coach did not track fidelity to action plans, she did maintain
100% fidelity to emailing participants their session log after each session.
The coach conducted 137 sessions from December 23, 2019, to April 3, 2020. Instead of
rigidly adhering to a schedule of topics, the coach adapted the content to fit participants’ interests
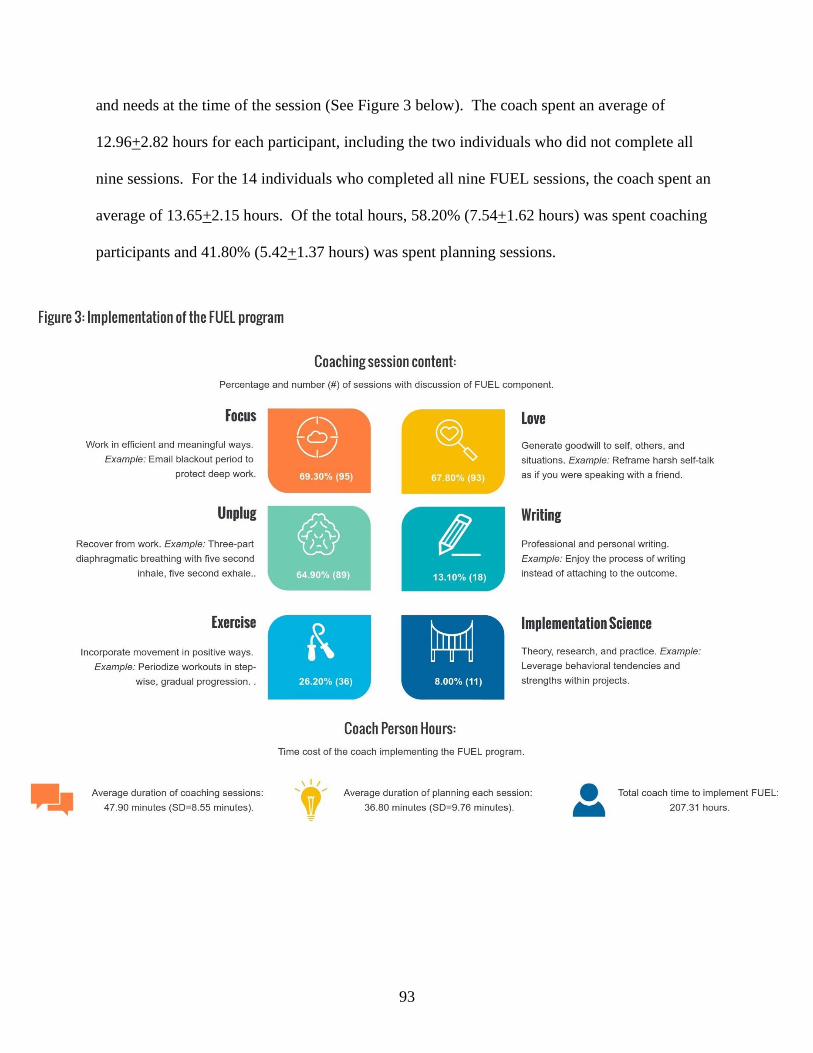
93
and needs at the time of the session (See Figure 3 below). The coach spent an average of
12.96+2.82 hours for each participant, including the two individuals who did not complete all
nine sessions. For the 14 individuals who completed all nine FUEL sessions, the coach spent an
average of 13.65+2.15 hours. Of the total hours, 58.20% (7.54+1.62 hours) was spent coaching
participants and 41.80% (5.42+1.37 hours) was spent planning sessions.
94
Effectiveness and Maintenance
Qualitative findings, open-end survey responses: Qualitative data include participants’
(P) responses to open-ended survey items at post program (n=15), three month follow-up (n=12)
and six month (n=13) follow-up. When asked at all three timepoints if they would enroll in the
FUEL program again, all participants answered affirmatively (e.g., P705, P711, P715 at six
months: “In a heartbeat”). All participants also answered affirmatively when asked in the post
survey if they would recommend FUEL coaching to other researchers (e.g., P707: “I absolutely
would! The coaching sessions have been transformative!!”) and if the coach was effective (e.g.,
P708: “YES! A million times yes”). When asked at all three timepoints if they had experienced
any negative effects of the coaching program, one participant expressed discomfort (P711:
“Showing weakness as a young academic is almost like baring your neck to an apex predator”).
The research team identified four themes, 11 subthemes, and 33 categories (see Table 3
before the references). The theme ways of being encapsulates participants’ descriptions of how
the program influenced their thoughts and behaviors (e.g., P705: “learning how to roll with the
waves and tides and tidal waves…FUEL is about being a WHOLE person”). The theme
program features comprises components of the FUEL program that participants found helpful or
effective (e.g., P709: “The face time one-on-one with a very encouraging and positive coach has
been the most helpful aspect of the program. I also really appreciated the weekly write-ups and
the tools I received from the coaching including calendar formats, fitness resources, and
infographics”). The theme perceptions of program consists of participants’ descriptions of the
value of the FUEL program (e.g., P703: “Even when I had the urge to cancel, I was always glad
I didn’t), as well as weaknesses or areas to be improved (e.g., P713: “Make it more available to
other people”).
95
Finally, the theme general experience captures participants’ descriptions of the
situational (e.g., P712: “Well, COVID-19 happened, which changed my work life quite a bit in
that I am now working 100% from home”) and temporal (e.g., P711: “I am still using strategies
from the earliest sessions at this time”) dimensions in which this longitudinal study occurred. An
exemplar summarizing these four themes comes from P715 in the three month follow-up: “This
research takes place in a space that is incredibly hard to draw connections to outcomes. Do I
think participating in FUEL made a positive difference for me? Yes. Would I do this process
again or recommend it to friends or colleagues? Yes. Were there negative outcomes that I can
identify? No. Do I still think about my exchanges with my coach during FUEL? Yes.
Weekly.” In the six month follow-up, this participant wrote, “Do I still think about my
exchanges with my coach during FUEL? Yes. Weekly.”
At all three time points, participants described benefits related to flourishing (e.g., P707:
“My life is more balanced, and I've regained some of the ‘texture’ to daily life”). They also
described benefits related to consciousness or their ability to reflect and self-regulate (e.g., P706:
“[what I have learned is] to take time to reflect and be conscious of where my attention and
energy is going and how to shift it if needed”), which they describe as enhancing their work
capacity (e.g., P705: “I manage both my work and home life so differently now than I did before
beginning FUEL, and that has allowed me to be a better researcher and take advantage of
professional opportunities I'm not sure I would have had the bandwidth to tackle before
participating in FUEL”). Likewise, at all three time points, participants listed specific strategies
or tools that they were integrating into their daily lives (e.g., P716: "body posture and sleeping
tips/time management tips"). Finally, at all three time points, participants praised the program as
a meaningful experience (e.g., P704: “I learned something valuable that helped improve my
96
approach to working each time we met”) that fills a niche (e.g., P708: “FUEL is a blending of
didactics and coaching that I've never really experienced before”).
When asked post program to identify the most helpful aspect of FUEL, 14 out of 15
participants described multiple dimensions (e.g., P704: “Weekly coaching that encouraged me
to self-reflect on how I was doing with implementing strategies we discussed the week before.
The wealth of resources provided just-in-time and specific to what I needed and would most
benefit from at that time. The coaching was personal and supportive and still nudged me to grow
when needed”). When asked at three month and six month follow-up about the first thing the
comes to mind when thinking back to FUEL, participants emphasized support from the coach
(e.g., P703: “accompaniment, understanding, non-judgment, and support”; P708: “the first thing
that comes to mind is [the coach] and her radiating positivity and the feeling of being grounded
while talking to her”). The centrality of the coach (e.g., P710: “FUEL is the face of someone
who cheers and encourages me”) presents a challenge to the program’s scalability and
sustainability (e.g., P711: "I am 100% positive that [the coach] is Fuel. The caveat to that is that
without [the coach] I truly doubt this intervention would be successful”).
At all three time points, participants described progress toward life and work goals as an
ongoing process with opportunities for growth (e.g., P713: “But FUEL helped me to realize that
at a certain point it is impossible to do it all and I need to start setting limits, that it isn't a matter
of working harder or smarter or faster, but a matter of regulating the amount of work I take on.
This was an eye-opener for me. I am still working hard on this..."). Despite ongoing growth, not
all behaviors were sustained (e.g., P706: “I know I should be making time to breathe/meditate—
but I don't follow through enough”).

97
References to the coronavirus pandemic were prevalent throughout the surveys.
Participants described uncertainty and upheaval (e.g., P714: “Things got very crazy with
COVID-19”), as well as benefits of coaching sessions (e.g., P703: “The sessions came at a time
when I had heightened anxiety due to work requirements and then later due to COVID-19. FUEL
helped me manage that anxiety”).
Qualitative findings, semi-structured interviews: Qualitative data also include semi-
structured interviews with a proxy (PR) at post program (n=11) and six month follow-up (n=8).
Investigators identified three themes, 10 subthemes, and 34 categories (see Table 4 before the
references). The theme context captures proxies’ comments about the circumstances of the
interview or the FUEL program (e.g., PR1: “we had a pretty massive tornado hit here, um, not
last night but the night before”). The theme of nature of change reflects proxies’ descriptions of
the depth, texture, or tangibility of alterations in participants’ behaviors and attitudes (e.g., PR6:
“Yeah, yeah, I think maybe it’s just me being kind of jealous of her having that [FUEL program]
experience. Cause I think it was an interesting experience for her and I think there was value in
it. So, you know, that certainly came across). Finally, the theme self-regulation: how people
are fueling themselves encompasses proxies’ observations of the way participants focus, unplug
from work, exercise, interact with others, and treat or perceive themselves (e.g., PR8: “Hmmm,
a few times definitely [there were changes] for some self care, you know, I need to go do this,
whether it be something as simple as I need to take a shower, so you’re in charge of the kids”).
As captured in the established pre program, work dynamic, and stressors categories,
proxies consistently described participants as productive, respected individuals (e.g., PR12: [the
participant] is like a breath of fresh air”) driven to help and lead others (e.g., PR6: “she wants to
solve everyone’s problems, save everyone. She’s very selfless for others and prioritizes that for
98
others”) but experiencing fatigue or doubt (e.g., PR1: “[she feels that] other researchers are apt
to see you as not as knowledgeable or expert or maybe a little bit less you know, top tier or
whatever”).
Proxies frequently expressed uncertainty or ambiguity answering questions about
observed changes in participants’ behavior because the behavior was established pre program
(e.g., PR12: “I think [his physical activity routine was] well-established before”) or because of
ambiguity related to the pandemic (e.g., PR9: “I think the problem is that life for us is different
because of the pandemic so it’s hard for me to answer these questions and separate your study
from these circumstances”).
Nevertheless, multiple proxies described participants’ ineffable shift toward a more
reflective, calm presence (e.g., PR1: “I feel like more recently he’s more aware of how he’s
feeling before it bubbles up inside”). Proxies also described a wide range of ways in which
participants appeared to be self-regulating, particularly through self-acceptance (e.g., PR9: “I
would say that she’s got a lot more self-confident”), self-permission (e.g., PR4: “she’s making
time for herself more”), and exercise (e.g., PR2: “when she was at home participating in the
study, she got the inspiration, I’ll say, to just start exercising at times when she usually wouldn’t
be exercising”).
Quantitative results: The means of self-reported variables trended in a positive
direction from baseline to six month follow-up (see Table 5 below). Because of inadvertently
omitted BMPN and FI items on the Qualtrics survey, investigators could analyze only the
autonomy, relatedness, and competence need satisfaction subscales of the BMPN (54) and the
health, purpose and meaning, character and virtue subscales of the FI (55).
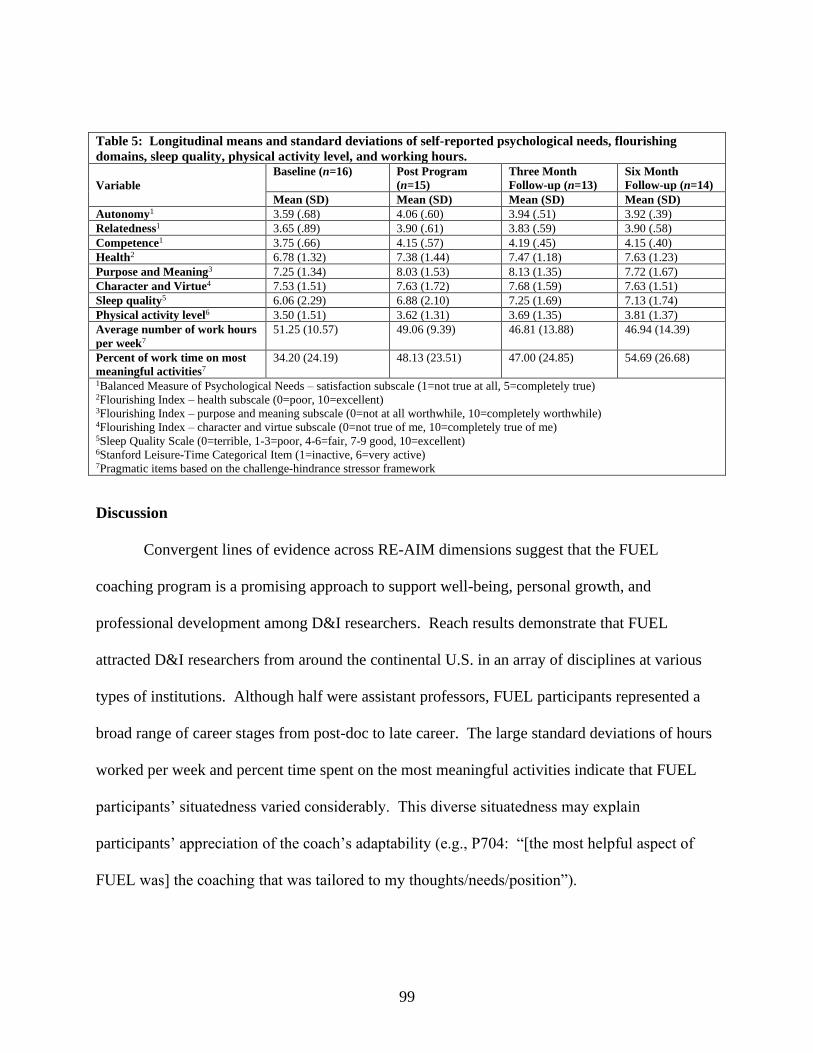
99
Table 5: Longitudinal means and standard deviations of self-reported psychological needs, flourishing
domains, sleep quality, physical activity level, and working hours.
Variable
Baseline (n=16) Post Program
(n=15)
Three Month
Follow-up (n=13)
Six Month
Follow-up (n=14)
Mean (SD) Mean (SD) Mean (SD) Mean (SD)
Autonomy1 3.59 (.68) 4.06 (.60) 3.94 (.51) 3.92 (.39)
Relatedness1 3.65 (.89) 3.90 (.61) 3.83 (.59) 3.90 (.58)
Competence1 3.75 (.66) 4.15 (.57) 4.19 (.45) 4.15 (.40)
Health2 6.78 (1.32) 7.38 (1.44) 7.47 (1.18) 7.63 (1.23)
Purpose and Meaning3 7.25 (1.34) 8.03 (1.53) 8.13 (1.35) 7.72 (1.67)
Character and Virtue4 7.53 (1.51) 7.63 (1.72) 7.68 (1.59) 7.63 (1.51)
Sleep quality5 6.06 (2.29) 6.88 (2.10) 7.25 (1.69) 7.13 (1.74)
Physical activity level6 3.50 (1.51) 3.62 (1.31) 3.69 (1.35) 3.81 (1.37)
Average number of work hours
per week7
51.25 (10.57) 49.06 (9.39) 46.81 (13.88) 46.94 (14.39)
Percent of work time on most
meaningful activities7
34.20 (24.19) 48.13 (23.51) 47.00 (24.85) 54.69 (26.68)
1Balanced Measure of Psychological Needs – satisfaction subscale (1=not true at all, 5=completely true) 2Flourishing Index – health subscale (0=poor, 10=excellent) 3Flourishing Index – purpose and meaning subscale (0=not at all worthwhile, 10=completely worthwhile) 4Flourishing Index – character and virtue subscale (0=not true of me, 10=completely true of me) 5Sleep Quality Scale (0=terrible, 1-3=poor, 4-6=fair, 7-9 good, 10=excellent) 6Stanford Leisure-Time Categorical Item (1=inactive, 6=very active) 7Pragmatic items based on the challenge-hindrance stressor framework
Discussion
Convergent lines of evidence across RE-AIM dimensions suggest that the FUEL
coaching program is a promising approach to support well-being, personal growth, and
professional development among D&I researchers. Reach results demonstrate that FUEL
attracted D&I researchers from around the continental U.S. in an array of disciplines at various
types of institutions. Although half were assistant professors, FUEL participants represented a
broad range of career stages from post-doc to late career. The large standard deviations of hours
worked per week and percent time spent on the most meaningful activities indicate that FUEL
participants’ situatedness varied considerably. This diverse situatedness may explain
participants’ appreciation of the coach’s adaptability (e.g., P704: “[the most helpful aspect of
FUEL was] the coaching that was tailored to my thoughts/needs/position”).

100
One unanticipated source for capturing participant representativeness was the semi-
structured interviews in which proxies described the many pre-program attributes and successes
of FUEL participants. The combination of these descriptions with participants’ reported reasons
for enrolling suggests that FUEL reached motivated, curious D&I researchers striving to manage
stress and prevent burnout while further elevating their work performance: There was demand
for coaching among individuals perceived as already successful. Email, particularly email via
implementation listservs, proved to be an efficient, low-cost way to reach or recruit these
individuals.
Implementation results demonstrate that it is feasible for one coach to deliver nine FUEL
sessions to approximately 16 D&I researchers via Zoom over about 15 weeks. The results
suggest that session duration should be flexible and that the program should not be limited to a
rigid eight-week timeline. FUEL implementation is streamlined compared to the two-year MT-
DIRC mentoring program which involved 15 mentors working with 15 early career fellows
approximately once per month, plus two five-day summer institutes (20).
Implementation results derived from coaching logs and the program features theme of
participants’ open-ended responses establish an evidence base for the core components or active
ingredients (67) for coaching D&I researchers (see Figure 4 below). The importance of the
coach-participant “connection” (P707, P708, P709) aligns with literature demonstrating the
central role of the working-alliance in executive coaching (68,69), athletics coaching (10,70),
and therapy (71). The FUEL coach served as a bridge connecting D&I researchers with a variety
of strategies in a “person-centered” (P711), “knowledgeable, nonpushy, empathetic way” (P203)
that left a “lasting impression” (P215) indicative of transformational leadership (72,73).

101
For example, participants’ positive perceptions of the “amazing” (P703, P712, P713)
coach reflect the transformational leadership dimension of idealized influence in which the leader
embodies admirable characteristics. The implication for implementation is that FUEL was not
just a compilation of evidence-based strategies, but a “support system” (P704) dependent on the
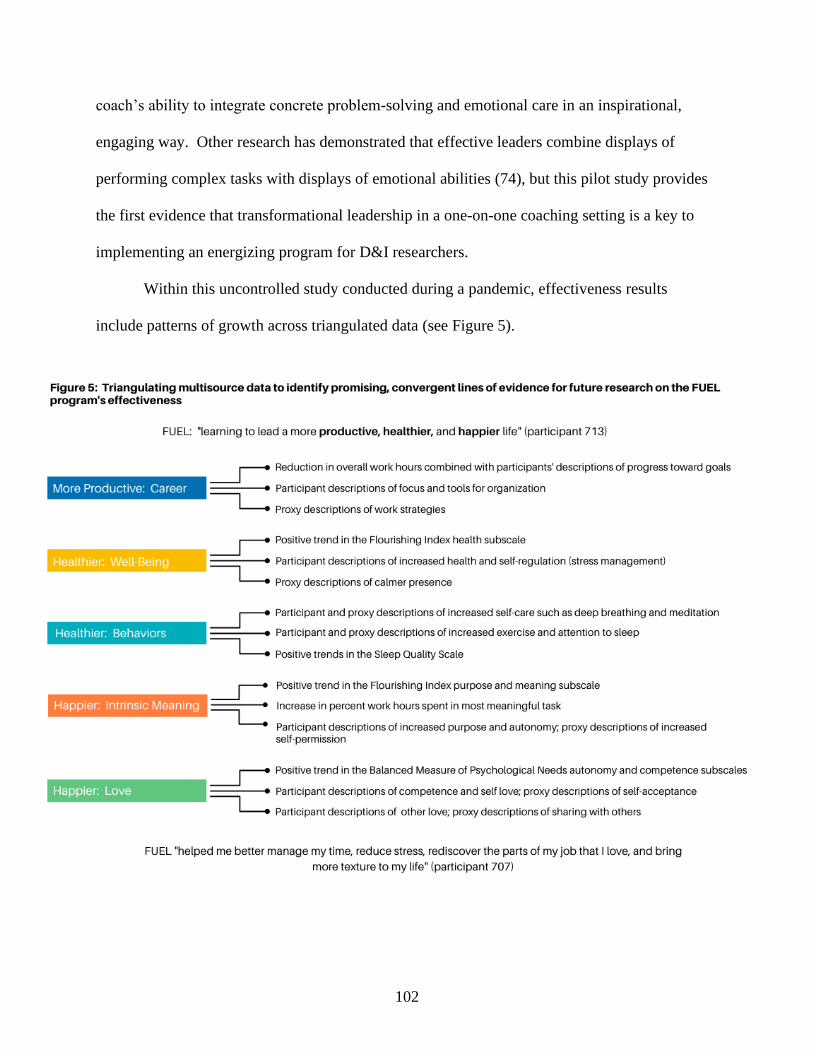
102
coach’s ability to integrate concrete problem-solving and emotional care in an inspirational,
engaging way. Other research has demonstrated that effective leaders combine displays of
performing complex tasks with displays of emotional abilities (74), but this pilot study provides
the first evidence that transformational leadership in a one-on-one coaching setting is a key to
implementing an energizing program for D&I researchers.
Within this uncontrolled study conducted during a pandemic, effectiveness results
include patterns of growth across triangulated data (see Figure 5).
103
Triangulating positive trends in quantitative data with participants’ and proxies’
consistent qualitative affirmations provides preliminary evidence that the FUEL program
supports D&I researchers’ multifaceted capacity to thrive amid demands. The program may be a
“passageway” for “resource caravans” as described in the conservation of resources (COR)
theory from organizational psychology (75,76). In alignment with COR’s principle of resource
investment, time spent in one-on-one coaching appears to be a viable strategy for D&I
researchers to fuel themselves.
Effectiveness results—particularly the increase in time spent on the most meaningful
activities—also align with the challenge stressor-hindrance stressor framework (59,60).
Actionable FUEL strategies, such as email blackout periods and “how to say no,” appear to help
researchers reroute their energy from hassles to tasks more central to productivity. This re-
routing is important because hindrance stressors are associated with detriments in motivation,
strain, and performance (60), as well as sleep quality (77). Overall, the challenge stressor-
hindrance stressor framework and COR have not been previously applied to D&I researchers and
are promising theoretical bases for coaching research (78).
Another facet of effectiveness is meaning. Retention rates and qualitative findings
demonstrate that participants valued FUEL. The program fills a niche and appears deeply
meaningful, particularly in ineffable realms rarely addressed in academia or professional
development for scientists. In terms of maintenance, the meaningful nature of participants’
experiences in FUEL appears to extend beyond the last coaching session, even through a
pandemic. At three month and six month follow-ups, participants wrote that they continue to
think about coaching conversations and engage in reflection. This sustained influence and
practice aligns with the Self-Regulation Model of Coaching in which the fundamental goal is to
104
establish skills and characteristics that catalyze and sustain long-term, self-determined growth
(35).
Within this ongoing growth, maintenance of FUEL behaviors, work strategies, and
mindsets appears dynamic with participants identifying continued challenges and areas for
improvement. Several proxies also described FUEL strategies and lessons that participants had
shared with them, indicative of a “coaching ripple effect” (79). Overall, this pilot study is not
proof that FUEL causes happiness, improves health, or enhances work performance. However,
the study does provide clear evidence that participants value the program and the support of a
coach.
This pragmatic pilot study has multiple strengths. First, investigators leveraged D&I
principles to mitigate limitations of previous coaching research that lacks implementation detail.
Second, the multisource, mixed methods findings provide a detailed portrait of FUEL and a
broad foundation for future empirical and practical work. Specifically, the emphasis on
qualitative exploration allowed investigators to highlight the intangible aspects of coaching
instead of limiting parameters of effectiveness to quantifiable measures. Furthermore,
investigators have reported at least one exemplar from each participant and each proxy (see
Tables 3 and 4). By presenting all participants’ voices in their own words, this pilot study itself
exudes the spirit of participatory research and coaching. On a more practical side, a third
strength of this pilot study is the low-cost, no-travel delivery of FUEL through videoconference
and telephone, which allowed the study to include participants across the U.S. and to continue
through a pandemic.
Despite its strengths, this pilot study has multiple limitations. First, precise denominators
and representativeness descriptions for reach were unavailable. This imprecision reflects the

105
nature of D&I Science as an emergent interdisciplinary field with an unknown number of
professionals. Second, the PI’s dual role of investigator and coach could increase bias and
observer effects despite several levels of participant identification codes to blind the PI/coach
during data analysis. Notably, participant 708 wrote, “I never felt pressured to keep going to just
make [the coach] happy/satisfied and not hurt her feelings.” A third limitation is that
investigators tracked coaching content through retrospective logs, foregoing video or audio
recording of sessions to minimize observer effects, protect privacy, and create a comfortable
environment. Fourth, the inadvertent omission of scale items and data missingness weakened the
breadth and depth of quantitative data.
Future research is needed to evaluate the adoption dimension of RE-AIM and to
investigate participant recommendations such as site visits. As an exploratory pilot test, this
study included a small sample inappropriate for inferential statistics. Future research could
include an explanatory approach and experimental design to investigate causation. This work
could include physiological health measures (e.g., blood pressure), job performance assessments
(e.g., ratings from supervisors), and cost-effectiveness. Even within an explanatory approach,
we recommend triangulating more “objective” data with qualitative findings to avoid stifling the
myriad experiences of what coaching is/means/brings about to individual participants.
Conclusion
Overall, this pilot study empirically applies D&I principles to a coaching program and
practically applies coaching processes to D&I researchers. This exploratory investigation is an
action-oriented response to the often discussed but unaddressed dilemma of thriving through the
challenges of being a D&I researcher. Building on previous work that identified D&I barriers
106
(2–4), investigators in this study developed and tested a one-on-one, person-centered coaching
program called FUEL. Convergent lines of evidence related to reach, implementation,
effectiveness, and maintenance suggest that FUEL is a promising and feasible approach to
support researchers “in learning to self-reflect and figure out ways to lead a more productive,
healthier, and happier life” (P713). While this pilot study establishes evidence for the
longitudinal value of the program, future work is needed to evaluate causation.

107
Table 3: Qualitative findings and codebook for participants’ open-ended survey responses at post (n=15), three month (n=12), and six month (n=13).
Theme/Subtheme Category Definition Exemplar: First character indicates timepoint (P=post, 3=three month,
6=six month). Second two characters indicate question number. Last
four characters indicate participant id (P705=participant 705).
TH
EM
E #
1:
Wa
ys
of
Bei
ng
Flo
uri
shin
g
HOLISTIC overall enrichment and life quality;
may be ineffable
PQ3P705: “As a result [of FUEL], I move through most days with a
sense of calm, humor, and flexibility that I was lacking when I started this
program. It is wonderful. I feel truly happy.”
HEALTH physical or mental well-being 3Q6P703: “By building-in more healthy supports (including regular
exercise and built-in breaks), the anxiety levels have dropped.”
PURPOSE intrinsic meaning, having a “why” 6Q6712: “It also helped me remember why I wanted to do this type of
work in the first place and to keep that front and center as I go about each
day.”
SD
T
COMPETENCE self-confidence or self-efficacy 3Q6P704: “Positive [outcome]: more confidence.”
AUTONOMY volition, choice, control (includes
saying “no”)
6Q1P712: "Having the ability to take control of my work life, instead of
reacting to others needs or expectations of me. "
FU
EL
Dim
ensi
on
s
FOCUS direct energy toward specific goals;
deliberate planning
6Q3P707: “Expending energy (more) wisely: I try to preserve mornings
for the things that require the most "head space" and schedule meetings in
the afternoon.”
UNPLUG recover from demands; take breaks
from work
6Q3P704: “I deleted work email from my phone completely and am no
longer stressed or distracted when I'm supposed to be 'off'. I have found
things outside of work that I can dedicate time to. I no longer work
weekends, AT ALL.”
EXERCISE movement and physical activity 6Q5P708: “I have made significant progress in my life/wellness goal in
increasing my physical activity.”
SELF LOVE self-acceptance or self-compassion PQ7P709: "[FUEL] dismantled my impostor syndrome (something I
think many many academics struggle with) more than anything else I
have done."
OTHER LOVE acceptance and compassion to others;
leadership styles
3Q2P714: "I've thought differently about the responses from my co-
workers and boss and attempted to engage in different ways with them."
Co
nsc
iou
snes
s MINDFULNESS reflection or mind-body strategies 6Q4P715: “I continue to use meditation and mindfulness exercises
encouraged by FUEL.”
SELF
REGULATION
manage stress and rumination 3Q1P705: “The FUEL program helped me learn to reframe negative
thoughts, perceptions, and interpersonal interactions in a way that helped
me remain engaged in my work at a very challenging time in my
organization.”
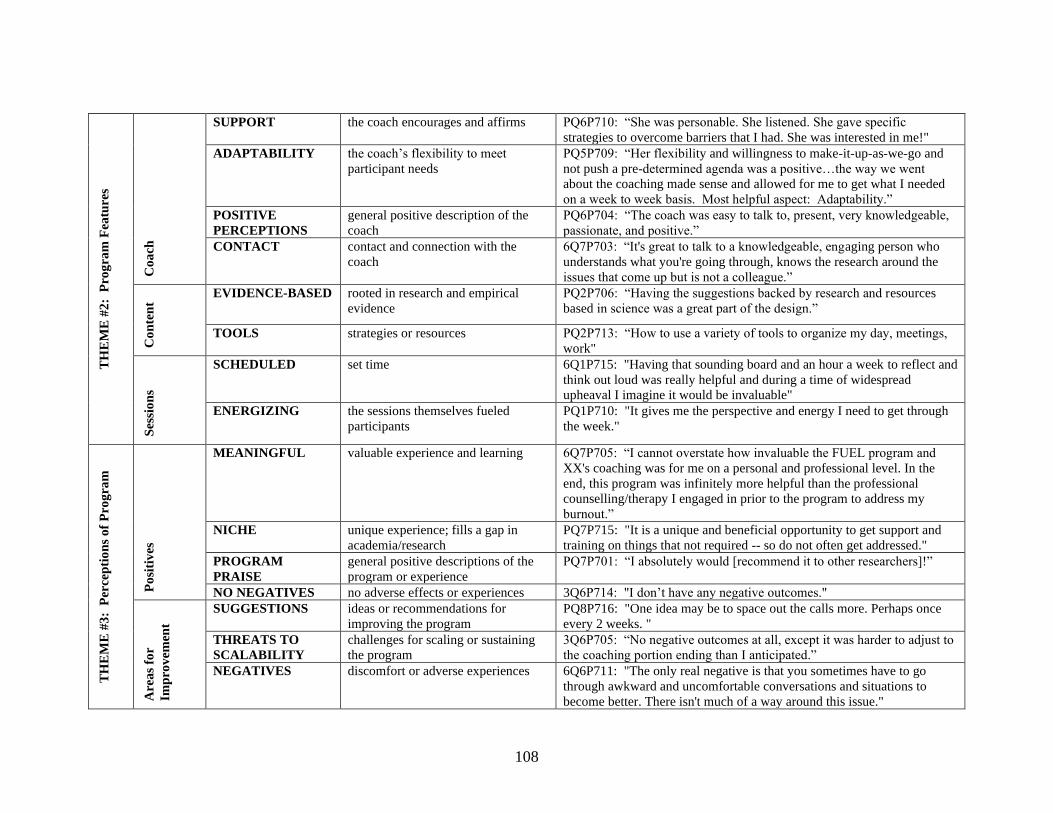
108
T
HE
ME
#2
: P
rog
ram
Fea
ture
s
Co
ach
SUPPORT the coach encourages and affirms PQ6P710: “She was personable. She listened. She gave specific
strategies to overcome barriers that I had. She was interested in me!"
ADAPTABILITY the coach’s flexibility to meet
participant needs
PQ5P709: “Her flexibility and willingness to make-it-up-as-we-go and
not push a pre-determined agenda was a positive…the way we went
about the coaching made sense and allowed for me to get what I needed
on a week to week basis. Most helpful aspect: Adaptability.”
POSITIVE
PERCEPTIONS
general positive description of the
coach
PQ6P704: “The coach was easy to talk to, present, very knowledgeable,
passionate, and positive.”
CONTACT contact and connection with the
coach
6Q7P703: “It's great to talk to a knowledgeable, engaging person who
understands what you're going through, knows the research around the
issues that come up but is not a colleague.”
Co
nte
nt
EVIDENCE-BASED rooted in research and empirical
evidence
PQ2P706: “Having the suggestions backed by research and resources
based in science was a great part of the design.”
TOOLS strategies or resources PQ2P713: “How to use a variety of tools to organize my day, meetings,
work"
Ses
sio
ns
SCHEDULED set time 6Q1P715: "Having that sounding board and an hour a week to reflect and
think out loud was really helpful and during a time of widespread
upheaval I imagine it would be invaluable"
ENERGIZING the sessions themselves fueled
participants
PQ1P710: "It gives me the perspective and energy I need to get through
the week."
TH
EM
E #
3:
Per
cep
tio
ns
of
Pro
gra
m
Po
siti
ves
MEANINGFUL valuable experience and learning 6Q7P705: “I cannot overstate how invaluable the FUEL program and
XX's coaching was for me on a personal and professional level. In the
end, this program was infinitely more helpful than the professional
counselling/therapy I engaged in prior to the program to address my
burnout.”
NICHE unique experience; fills a gap in
academia/research
PQ7P715: "It is a unique and beneficial opportunity to get support and
training on things that not required -- so do not often get addressed."
PROGRAM
PRAISE
general positive descriptions of the
program or experience
PQ7P701: “I absolutely would [recommend it to other researchers]!”
NO NEGATIVES no adverse effects or experiences 3Q6P714: "I don’t have any negative outcomes."
Are
as
for
Imp
rov
emen
t
SUGGESTIONS ideas or recommendations for
improving the program
PQ8P716: "One idea may be to space out the calls more. Perhaps once
every 2 weeks. "
THREATS TO
SCALABILITY
challenges for scaling or sustaining
the program
3Q6P705: “No negative outcomes at all, except it was harder to adjust to
the coaching portion ending than I anticipated.”
NEGATIVES discomfort or adverse experiences 6Q6P711: "The only real negative is that you sometimes have to go
through awkward and uncomfortable conversations and situations to
become better. There isn't much of a way around this issue."
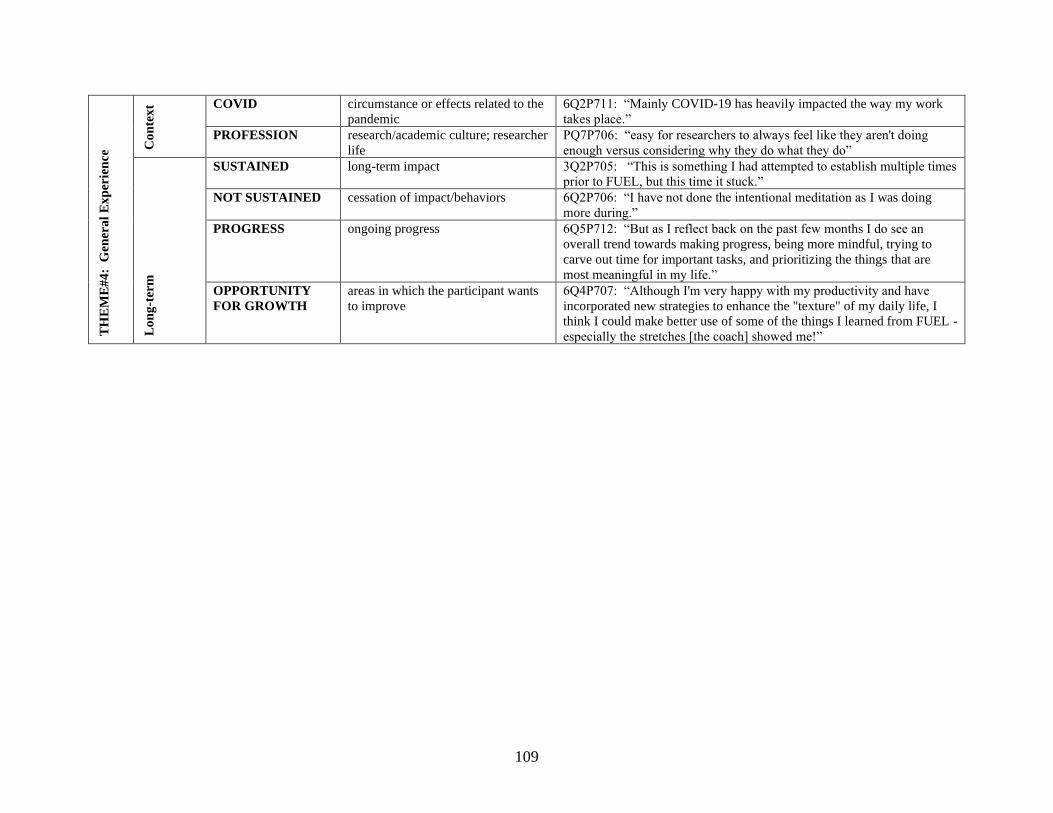
109
TH
EM
E#
4:
Gen
era
l E
xp
erie
nce
Co
nte
xt COVID circumstance or effects related to the
pandemic
6Q2P711: “Mainly COVID-19 has heavily impacted the way my work
takes place.”
PROFESSION research/academic culture; researcher
life
PQ7P706: “easy for researchers to always feel like they aren't doing
enough versus considering why they do what they do” L
on
g-t
erm
SUSTAINED long-term impact 3Q2P705: “This is something I had attempted to establish multiple times
prior to FUEL, but this time it stuck.”
NOT SUSTAINED cessation of impact/behaviors 6Q2P706: “I have not done the intentional meditation as I was doing
more during.”
PROGRESS ongoing progress 6Q5P712: “But as I reflect back on the past few months I do see an
overall trend towards making progress, being more mindful, trying to
carve out time for important tasks, and prioritizing the things that are
most meaningful in my life.”
OPPORTUNITY
FOR GROWTH
areas in which the participant wants
to improve
6Q4P707: “Although I'm very happy with my productivity and have
incorporated new strategies to enhance the "texture" of my daily life, I
think I could make better use of some of the things I learned from FUEL -
especially the stretches [the coach] showed me!”
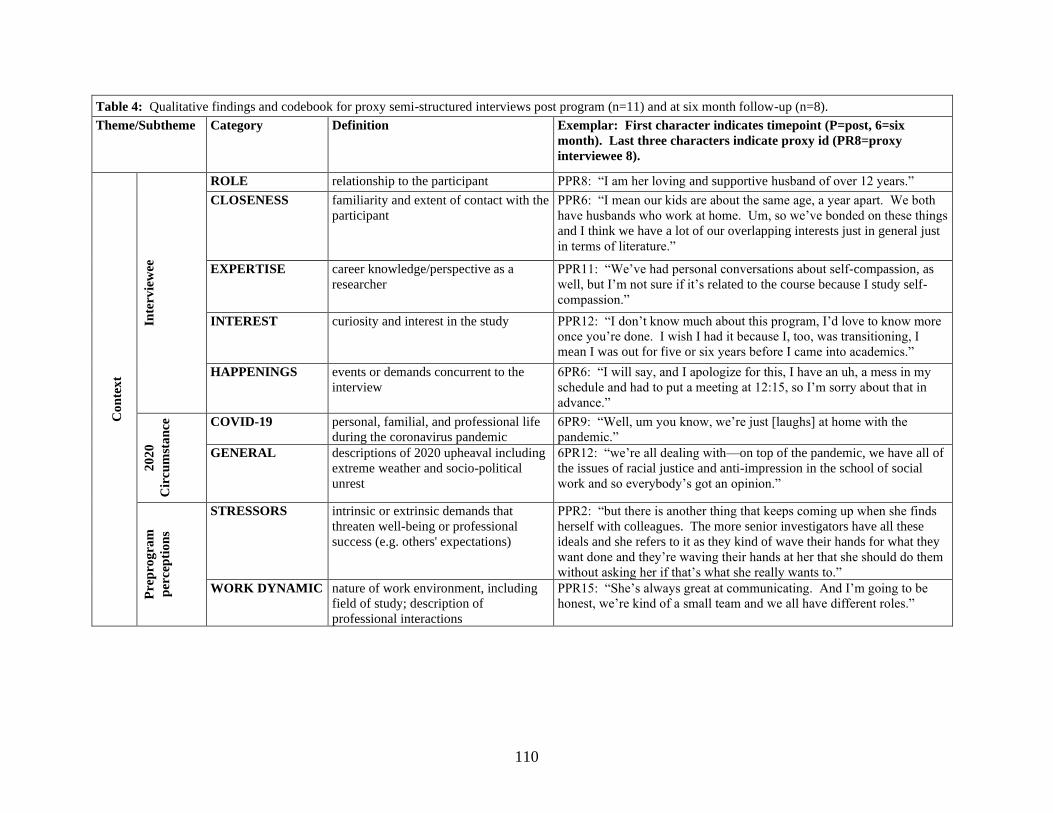
110
Table 4: Qualitative findings and codebook for proxy semi-structured interviews post program (n=11) and at six month follow-up (n=8).
Theme/Subtheme Category Definition Exemplar: First character indicates timepoint (P=post, 6=six
month). Last three characters indicate proxy id (PR8=proxy
interviewee 8).
Co
nte
xt
Inte
rvie
wee
ROLE relationship to the participant PPR8: “I am her loving and supportive husband of over 12 years.”
CLOSENESS familiarity and extent of contact with the
participant
PPR6: “I mean our kids are about the same age, a year apart. We both
have husbands who work at home. Um, so we’ve bonded on these things
and I think we have a lot of our overlapping interests just in general just
in terms of literature.”
EXPERTISE career knowledge/perspective as a
researcher
PPR11: “We’ve had personal conversations about self-compassion, as
well, but I’m not sure if it’s related to the course because I study self-
compassion.”
INTEREST curiosity and interest in the study PPR12: “I don’t know much about this program, I’d love to know more
once you’re done. I wish I had it because I, too, was transitioning, I
mean I was out for five or six years before I came into academics.”
HAPPENINGS events or demands concurrent to the
interview
6PR6: “I will say, and I apologize for this, I have an uh, a mess in my
schedule and had to put a meeting at 12:15, so I’m sorry about that in
advance.”
20
20
Cir
cu
mst
an
ce
COVID-19 personal, familial, and professional life
during the coronavirus pandemic
6PR9: “Well, um you know, we’re just [laughs] at home with the
pandemic.”
GENERAL descriptions of 2020 upheaval including
extreme weather and socio-political
unrest
6PR12: “we’re all dealing with—on top of the pandemic, we have all of
the issues of racial justice and anti-impression in the school of social
work and so everybody’s got an opinion.”
Pre
pro
gra
m
per
cep
tio
ns
STRESSORS intrinsic or extrinsic demands that
threaten well-being or professional
success (e.g. others' expectations)
PPR2: “but there is another thing that keeps coming up when she finds
herself with colleagues. The more senior investigators have all these
ideals and she refers to it as they kind of wave their hands for what they
want done and they’re waving their hands at her that she should do them
without asking her if that’s what she really wants to.”
WORK DYNAMIC nature of work environment, including
field of study; description of
professional interactions
PPR15: “She’s always great at communicating. And I’m going to be
honest, we’re kind of a small team and we all have different roles.”
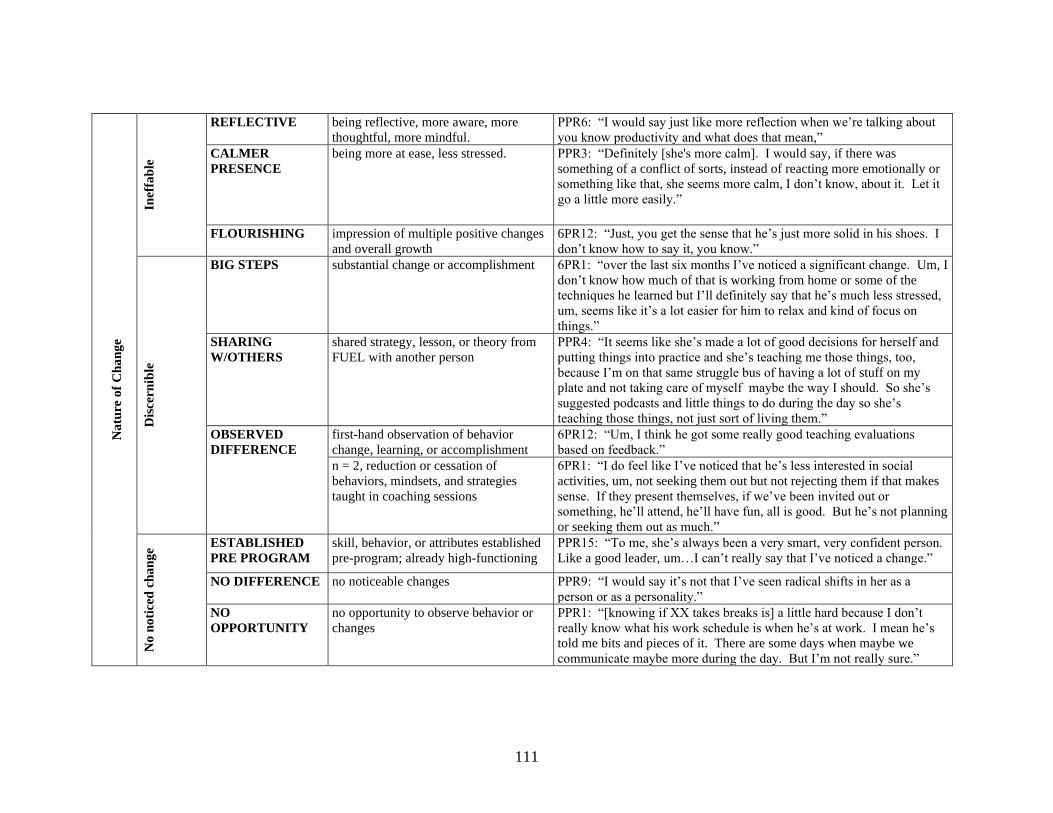
111
N
atu
re o
f C
ha
ng
e
Inef
fab
le
REFLECTIVE being reflective, more aware, more
thoughtful, more mindful.
PPR6: “I would say just like more reflection when we’re talking about
you know productivity and what does that mean,”
CALMER
PRESENCE
being more at ease, less stressed. PPR3: “Definitely [she's more calm]. I would say, if there was
something of a conflict of sorts, instead of reacting more emotionally or
something like that, she seems more calm, I don’t know, about it. Let it
go a little more easily.”
FLOURISHING impression of multiple positive changes
and overall growth
6PR12: “Just, you get the sense that he’s just more solid in his shoes. I
don’t know how to say it, you know.”
Dis
cern
ible
BIG STEPS substantial change or accomplishment 6PR1: “over the last six months I’ve noticed a significant change. Um, I
don’t know how much of that is working from home or some of the
techniques he learned but I’ll definitely say that he’s much less stressed,
um, seems like it’s a lot easier for him to relax and kind of focus on
things.”
SHARING
W/OTHERS
shared strategy, lesson, or theory from
FUEL with another person
PPR4: “It seems like she’s made a lot of good decisions for herself and
putting things into practice and she’s teaching me those things, too,
because I’m on that same struggle bus of having a lot of stuff on my
plate and not taking care of myself maybe the way I should. So she’s
suggested podcasts and little things to do during the day so she’s
teaching those things, not just sort of living them.”
OBSERVED
DIFFERENCE
first-hand observation of behavior
change, learning, or accomplishment
6PR12: “Um, I think he got some really good teaching evaluations
based on feedback.”
n = 2, reduction or cessation of
behaviors, mindsets, and strategies
taught in coaching sessions
6PR1: “I do feel like I’ve noticed that he’s less interested in social
activities, um, not seeking them out but not rejecting them if that makes
sense. If they present themselves, if we’ve been invited out or
something, he’ll attend, he’ll have fun, all is good. But he’s not planning
or seeking them out as much.”
No
no
tice
d c
ha
ng
e ESTABLISHED
PRE PROGRAM
skill, behavior, or attributes established
pre-program; already high-functioning
PPR15: “To me, she’s always been a very smart, very confident person.
Like a good leader, um…I can’t really say that I’ve noticed a change.”
NO DIFFERENCE no noticeable changes PPR9: “I would say it’s not that I’ve seen radical shifts in her as a
person or as a personality.”
NO
OPPORTUNITY
no opportunity to observe behavior or
changes
PPR1: “[knowing if XX takes breaks is] a little hard because I don’t
really know what his work schedule is when he’s at work. I mean he’s
told me bits and pieces of it. There are some days when maybe we
communicate maybe more during the day. But I’m not really sure.”

112
Pa
nd
emic
Co
nfo
un
din
g
ADAPTIVE Positive experiences or expansive
aspects of COVID-19.
6PR2: “So being able to telework, she has now incorporated more
walking breaks into her day. So she’s doing that.”
RESTRICTIVE Negative experiences or limiting aspects
of COVID-19
6PR9: “Um, we haven’t been, you know, she used to lift weights
frequently, but uh, we don’t because we have a little workout facility in
our you know shared complex in our community, but we haven’t been
doing that because of the pandemic, although it’s now open.”
AMBIGUITY Unclear, unknown, indefinite aspects of
changes related to COVID-19
PPR10: “Um [pause]. What changes have I noticed? [pause.] I mean,
it’s so hard because of COVID.”
Per
ceiv
ed S
elf-
Reg
ula
tio
n:
ho
w p
eop
le a
re
fuel
ing
th
emse
lves
FU
EL
Beh
av
iors
EXERCISE working out PPR6: “Yeah, I think, you know I’ve noticed her definitely being more
intentional to get some more exercise.”
WALK AND
TALKS
walking with at least one other person PPR11: “So, it may be that she was…that maybe we were taking a few
more walks. For breaks. We would just walk each other to go get food
or just move our bodies for 10 minutes so that we can reset and keep
writing or whatever we were doing.”
LEISURE
ACTIVITIES
engaging in self-chosen recreational
activities
PPR8: “I mean definitely the last few weeks I’ve seen XX engaging in
her own leisure activities.”
MINDFULNESS engaging in activities that cultivate
reflection, consciousness, or spirituality
PPR3: “there’s obviously always stress, so the way she’s dealing with it
a little more, more proactive about it, or almost like meditating a little bit
or listening to a lot of, uh, whatchya want to call it, meditative type
music when she’s working, things that help her calm down.
SOCIAL EVENTS engaging in social activities PPR1: “but we have tried more recently to be more socially active and
go out more and he’s been willing to do that so I would say he’s more
interested in that than, um, and he’s been more active with it. So, I
would say more participation.”
SOCIAL
SUPPORT
reaching out to other people for
emotional support and social connection
PPR11: “And, we actually, together before the coronavirus stuff, we
went to, um, a Buddhist temple together to try it out and to support each
other through this experience and we really enjoyed that time together.”
SLEEP prioritizing sleep or improving sleep
hygiene
PPR8: “Yeah, and, um, I would say that specifically that would be a
renewed focus on getting enough sleep each night, which should help her
because she’s sensitive to that and some of us are not.”
Min
dse
t SELF
PERMISSON
allowing oneself to prioritize self-care
and personal needs or goals
PPR4: “It seems like she’s making herself more of a priority then has,
uh, in the past.”
SELF
ACCEPTANCE
gentle, loving self assessment 6PR6: “Um, you know, I think that her ability to kinda stay afloat and
not have, um, and not be as self-critical during this time, um, you know
that is potentially a result of the program.”

113
Wo
rk S
tra
teg
ies
BOUNDARIES protect deep work by establishing
boundaries (email blackout, close door)
6PR2: “Um, she’s really stuck to having her email blackout times. So I
know she’s been able to be more productive in terms of getting her
manuscripts done.”
WORK SPACE set up an inspiring workspace PPR11: “Yeah, and I will say she did bring in a white board for a vision
board in our office space.”
BREAKS take breaks away from work 6PR9: “Uh, I guess I am noticing that she will take periodic timeouts
from work and reward herself by, you know, watching a YouTube video
or listening to a song or something like that. Um, and she’s been
working really, really hard.”
ORGANIZATION plan goals, work strategies, or schedule PPR10: “So, we, we usually have project agendas and he’s just paying
more attending to the agendas in advance of the meetings and then
following it more close during the meetings.”

114
Reflexivity Statements
PI: At the time of the study, AS was a PhD candidate in a community and behavioral physical
activity program. She spent 15 years as an intercollegiate swimming and diving coach in NCAA
Division I Athletics and, as a former swimmer and rower, received over two decades of
coaching. Her undergraduate degree included courses in counseling, observational methods, and
human development. The idea for the FUEL program emerged during AS’s previous
autoethnographic study of D&I culture. Throughout the FUEL program, AS applied skills from
her previous coaching career and leadership training. AS is aware of how her role as the coach,
the relationships she built with participants, and a recent project in phenomenology influenced
data analysis and writing style. Despite the consistency and intensity of participants’ words, AS
was reticent to identify transformative coaching as a core component lest this finding be
interpreted as self-promotion. Finally, throughout the study, AS grappled with how to capture
irreducibly subjective processes within conventional scientific paradigms.
Senior Author: SMH has a PhD in the behavioral physical activity promotion and postdoctoral
training in dissemination and implementation science. She transitioned from assistant to
associate professor at the midway point of this research, and was the academic advisor
overseeing the work proposed and conducted within the FUEL study. She is a co-investigator in
research projects using qualitative methodologies (n = 12) and projects applying the RE-AIM
framework (n= 18). She did not interact with nor have any known relationships with any of the
participants; she only coded deidentified data. Finally, when she met AS she was a relatively
burnt-out dissemination and implementation scientist, overseeing myriad interventions through
participatory approaches. Through their conversations, AS inspired SMH to Focus, Unplug,
Exercise, and Love and recognize one’s humanness and situatedness in all our doings. All data
was reviewed for transparency (i.e., exact word from the participants), but this lens of supporting
and believing in the tenets of FUEL must be acknowledged.
Co-Author: At the time of the study, SC was a PhD candidate in a community and behavioral
nutrition program. She is trained in both deductive and inductive qualitative research methods.
She has analyzed qualitative data for behavioral nutrition studies (n = 3). For this study, she did
not interact with research participants and only coded de-identified survey data. Through
working on this study, Susan understands the value and need of personalized coaching for
success in a research or implementation science discipline. She is now actively seeking and
practicing mindfulness techniques because she is trying to develop these habits in preparation for
her future career in academia.
Co-Author: At the time of the study, RN was PhD student in a community and behavioral
nutrition program. RN has a MS in nutrition and has worked on one other project using content
analysis. Additionally, she has utilized the RE-AIM framework to evaluate one other
intervention. While currently a student, she is familiar with the stress that a career in academia
can bring as her father was a professor. She also recognizes the impact of burnout on the other
people in the scientists’ lives. Additionally, she believes in the theoretical underpinnings of
FUEL. While acknowledging the impact of her belief in the program and lived experiences, she
strived to analyze the words of the participants as they were written. She was completely blinded
throughout the process.
115
References
1. Shelton RC, Lee M, Brotzman LE, Wolfenden L, Nathan N, Wainberg ML. What Is
Dissemination and Implementation Science? An Introduction and Opportunities to
Advance Behavioral Medicine and Public Health Globally. Int J Behav Med.
2020;27(1):3–20.
2. Koorts H, Naylor PJ, Laws R, Love P, Maple JL, van Nassau F. What hinders and helps
academics to conduct Dissemination and Implementation (D&I) research in the field of
nutrition and physical activity? An international perspective. Int J Behav Nutr Phys Act.
2020;17(1):7.
3. Steketee A, Archibald T, Harden S. Adjust your own oxygen mask before helping those
around you: An autoethnography of participatory research. Implement Sci. 2020;15(70).
4. Oliver K, Kothari A, Mays N. The dark side of coproduction: Do the costs outweigh the
benefits for health research? Heal Res Policy Syst. 2019;17(1):1–10.
5. Howe A, Mathie E, Munday D, Cowe M, Goodman C, Keenan J, et al. Learning to work
together – lessons from a reflective analysis of a research project on public involvement.
Res Involv Engagem [Internet]. 2017;3(1):1. Available from:
http://researchinvolvement.biomedcentral.com/articles/10.1186/s40900-016-0051-x
6. Reed JE, Howe C, Doyle C, Bell D. Simple rules for evidence translation in complex
systems: A qualitative study. BMC Med. 2018;16(1):1–20.
7. Dewe P, O’Driscoll M, Cooper C. Theories of Psychological Stress at Work. In: Gatchel
R, Schultz I, editors. Handbook of Occupational Health and Wellness. New York: Spring
Science + Business Media; 2012.
8. Theeboom T, Beersma B, Vianen AEM Van. Does coaching work? A meta-analysis on
the effects of coaching on individual level outcomes in an organization. J Posit Psychol
[Internet]. 2013;1–18. Available from: http://dx.doi.org/10.1080/17439760.2013.837499
9. Ericsson KA, Krampe RT, Tesch-Römer C. The role of deliberate practice in the
acquisition of expert performance. Psychol Rev. 2005;100(3):363–406.
10. Jowett S. Coaching effectiveness: the coach–athlete relationship at its heart. Curr Opin
Psychol. 2017;16:154–8.
11. Mageau GA, Vallerand RJ. The coach-athlete relationship: A motivational model. J Sports
Sci. 2003;21(11):883–904.
12. Deiorio NM, Carney PA, Kahl LE, Bonura EM, Juve AM. Coaching: A new model for
academic and career achievement. Med Educ Online. 2016;21(1).
13. Dyrbye LN, Shanafelt TD, Gill PR, Satele D V., West CP. Effect of a Professional
Coaching Intervention on the Well-being and Distress of Physicians. JAMA Intern Med.
2019;55905.
14. Hill B, Richardson B, Skouteris H. Do we know how to design effective health coaching
interventions: A systematic review of the state of the literature. Am J Heal Promot.
2015;29(5):e158–68.
15. Sforzo GA, Kaye MP, Todorova I, Harenberg S, Costello K, Cobus-Kuo L, et al.
Compendium of the health and wellness coaching literature. Am J Lifestyle Med.
2018;12(6):1–12.
16. Sforzo GA, Kaye MP, Harenberg S, Costello K, Cobus-Kuo L, Rauff E, et al.
Compendium of Health and Wellness Coaching: 2019 Addendum. Am J Lifestyle Med.

116
2020;14(2):155–68.
17. Jones RJ, Woods SA, Guillaume YRF. The effectiveness of workplace coaching: A meta-
analysis of learning and performance outcomes from coaching. J Occup Organ Psychol.
2016;89(2):249–77.
18. Grover S, Furnham A. Coaching as a developmental intervention in organisations: A
systematic review of its effectiveness and the mechanisms underlying It. PLoS One.
2016;11(7):1–41.
19. Bertrand DW. The practice of executive coaching to improve leadership capacity in
academic deans at American higher education institutions. Coach An Int J Theory, Res
Pract. 2019;12(2).
20. Padek M, Mir N, Jacob RR, Chambers DA, Dobbins M, Emmons KM, et al. Training
scholars in dissemination and implementation research for cancer prevention and control:
A mentored approach. Implement Sci. 2018;13(1):1–13.
21. National Institutes of Health. Training Institute for Dissemination and Implementation
Research in Health (TIDIRH) [Internet]. 2020 [cited 2020 Aug 19]. Available from:
https://obssr.od.nih.gov/training/training-supported-by-the-obssr/training-tidirh/
22. Powell K. Work–life balance: Break or burn out. Nature. 2017;545(7654):375–7.
23. Messias E, Gathright MM, Freeman ES, Flynn V, Atkinson T, Thrush CR, et al.
Differences in burnout prevalence between clinical professionals and biomedical scientists
in an academic medical centre: A cross-sectional survey. BMJ Open. 2019;9(2):1–7.
24. Ma WJ. The stories behind a CV. Science. 2017;357(6354):942.
25. Tooth JA, Nielsen S, Armstrong H. Coaching effectiveness survey instruments: Taking
stock of measuring the immeasurable. Coach An Int J Theory, Res Pract. 2013;6(2):137–
51.
26. Glasgow R, Vogt T, Boles S. Evaluating the Public Health Impact of Health Promotion
Interventions: The RE-AIM Framework. Am J Public Health. 1999;89(9):1322–7.
27. Glasgow RE, Harden SM, Gaglio B, Rabin B, Smith ML, Porter GC, et al. RE-AIM
Planning and Evaluation Framework: Adapting to New Science and Practice With a 20-
Year Review. Front Public Heal. 2019;7(March).
28. Powell BJ, Waltz TJ, Chinman MJ, Damschroder LJ, Smith JL, Matthieu MM, et al. A
refined compilation of implementation strategies: Results from the Expert
Recommendations for Implementing Change (ERIC) project. Implement Sci.
2015;10(1):1–14.
29. Eccles MP, Grimshaw JM, MacLennan G, Bonetti D, Glidewell L, Pitts NB, et al.
Explaining clinical behaviors using multiple theoretical models. Implement Sci.
2012;7(1):1–13.
30. Larsen KR, Michie S, Hekler EB, Gibson B, Spruijt-Metz D, Ahern D, et al. Behavior
change interventions: the potential of ontologies for advancing science and practice. J
Behav Med. 2017;40(1):6–22.
31. Glasgow R. What does it mean to be pragmatic? Pragmatic methods, measures, and
models to facilitate research translation. Heal Educ Behav. 2013;40(3):257–65.
32. Thorpe K, Zwarenstein M, Oxman A, Treweek S, Furberg C, Altman D, et al. A
pragmatic-explanatory continuum indicator summary (PRECIS): a tool to help trial
designers. J Clin Epidemiol. 2009;62:464–75.
33. Aarons GA, Sklar M, Mustanski B, Benbow N, Brown CH. “Scaling-out” evidence-based
interventions to new populations or new health care delivery systems. Implement Sci.
117
2017;12(1):1–13.
34. Brownson RC, Jacobs JA, Tabak RG, Hoehner CM, Stamatakis KA. Designing for
dissemination among public health researchers: Findings from a national survey in the
United States. Am J Public Health. 2013;103(9):1693–9.
35. Grant AM. The impact of life coaching on goal attainment, metacognition and mental
health. Soc Behav Pers. 2003;31(3):253–64.
36. Grant AM, Curtayne L, Burton G. Executive coaching enhances goal attainment,
resilience and workplace well-being: A randomised controlled study. J Posit Psychol.
2009;4(5):396–407.
37. Ryan RM, Deci EL. Self Determination Theory and the Facilitation of Intrinsic
Motivation, Social Development, and Well-Being. Am Psychol. 2000;55(1):68–78.
38. Vanderweele TJ, McNeely E, Koh HK. Reimagining Health - Flourishing. J Am Med
Assoc. 2019;02115:4–5.
39. Huta V. The Complementary Roles of Eudaimonia and Hedonia and How They Can Be
Pursued in Practice. Posit Psychol Pract Promot Hum Flourishing Work Heal Educ
Everyday Life Second Ed. 2015;(June 2015):159–82.
40. Bompa TO. Periodization. Fourth Edi. Champaign, IL: Human Kinetics; 1999.
41. Wathen D, Baechle TR, Earle RW. Periodization. In: Baechle TR, Earle RW, editors.
Essentials of Strength Training and Conditioning. Third Edit. Champaign, IL; 2008. p.
507–22.
42. Bus K, Peyer KL, Bai Y, Ellingson LD, Welk GJ. Comparison of In-Person and Online
Motivational Interviewing–Based Health Coaching. Health Promot Pract.
2018;19(4):513–21.
43. Green CA, Duan N, Gibbons RD, Hoagwood KE, Palinkas LA, Albert G, et al.
Approaches to Mixed Methods Dissemination and Implementation Research: Methods,
Strengths, Caveats, and Opportunities. Adm Policy Ment Heal. 2015;42(5):508–23.
44. Creswell J, Poth C. Qualitative Inquiry & Research Design. Fourth Edi. Salmon H, editor.
Thousand Oaks, CA: SAGE Publications; 2018.
45. Palinkas L, Horwitz S, Green C, Wisdom J, Duan N, Hoagwood K. Purposeful Sampling
for qualitative data collection and analysis in mixed method implementation research.
Adm Policy Ment Heal [Internet]. 2015;42(5):533–44. Available from:
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4012002/pdf/nihms-538401.pdf
46. Taylor B, Henshall C, Kenyon S, Litchfield I, Greenfield S. Can rapid approaches to
qualitative analysis deliver timely, valid findings to clinical leaders? A mixed methods
study comparing rapid and thematic analysis. BMJ Open. 2018;8(e019993):1–13.
47. Palinkas LA, Zatzick D. Rapid Assessment Procedure Informed Clinical Ethnography
(RAPICE) in Pragmatic Clinical Trials of Mental Health Services Implementation:
Methods and Applied Case Study. Adm Policy Ment Heal Ment Heal Serv Res [Internet].
2019;46(2):255–70. Available from: http://dx.doi.org/10.1007/s10488-018-0909-3
48. Birt L, Scott S, Cavers D, Campbell C, Walter F. Member Checking: A Tool to Enhance
Trustworthiness or Merely a Nod to Validation? Qual Health Res. 2016;26(13):1802–11.
49. Dowd A, Harden S, Estabrooks P. Adolescent Girls’ Experiences in the Go Girls! Group-
Based Lifestyle Mentoring Program. Am J Heal Behav. 2015;39(2):266–75.
50. Tracy S. Qualitative Research Methods: Collecting Evidence, Crafting Analysis,
Communicating Impact. First. Chichester, UK: Blackwell Publishing, Ltd; 2013.
51. Darnell D, Dorsey CN, Melvin A, Chi J, Lyon AR, Lewis CC. A content analysis of
118
dissemination and implementation science resource initiatives: What types of resources do
they offer to advance the field? Implement Sci. 2017;12(1):1–15.
52. Vanderweele TJ. On the promotion of human flourishing. PNAS. 2017;114(31).
53. Sheldon KM, Gunz A. Psychological needs as basic motives, not just experiential
requirements. J Pers. 2009;77(5):1467–92.
54. Sheldon KM, Hilpert JC. The balanced measure of psychological needs (BMPN) scale:
An alternative domain general measure of need satisfaction. Motiv Emot. 2012;36(4):439–
51.
55. Weziak-Bialowolska D, McNeely E, VanderWeele TJ. Flourish Index and Secure Flourish
Index–Validation in workplace settings. Cogent Psychol [Internet]. 2019;6(1). Available
from: https://doi.org/10.1080/23311908.2019.1598926
56. Wȩziak-Białowolska D, McNeely E, VanderWeele TJ. Human flourishing in cross
cultural settings. Evidence from the United States, China, Sri Lanka, Cambodia, and
Mexico. Front Psychol. 2019;10(MAY):1–13.
57. Snyder E, Cai B, DeMuro C, Morrison MF, Ball W. A new single-item sleep quality scale:
Results of psychometric evaluation in patients with chronic primary insomnia and
depression. J Clin Sleep Med. 2018;14(11):1849–57.
58. Kiernan M, Schoffman DE, Lee K, Brown SD, Fair JM, Perri MG, et al. The stanford
leisure-time activity categorical item (L-Cat): A single categorical item sensitive to
physical activity changes in overweight/obese women. Int J Obes [Internet].
2013;37(12):1597–602. Available from: http://dx.doi.org/10.1038/ijo.2013.36
59. Cavanaugh MA, Boswell WR, Roehling M V, Boudreau JW. An Empirical Examination
of Self-Reported Work Stress Among U.S. Managers. J Appl Psychol. 2000;85(1):65–74.
60. LePine J, Podsakoff N, LePine M. A meta-analytic test of the challenge stressor-hindrance
stressor framework: An explanation for inconsistent relationships among stressors and
performance. Acad Manag J. 2005;48(5):764–75.
61. Chakraborty H, Gu H. A Mixed Method Model Approach for Intent-to-Treat Analysis in
Longitudinal Clinical Trials with Missing Values [Internet]. Research Triangle Park, NC;
2009. Available from: http://www.rti.org/rtipress
62. Schwartz D, Lellouch J. Explanatory and pragmatic attitudes in therapeutical trials. J
Chronic Dis. 1967;20(8):637–48.
63. Lincoln YS, Guba EG. Naturalistic Inquiry. Newbury Park, CA: Sage Publications; 1985.
64. Qualitative Research in Implementation Science (QUALRIS). Qualitative Methods In
Implementation Science. 2018; Available from:
https://cancercontrol.cancer.gov/IS/docs/NCI-DCCPS-ImplementationScience-
WhitePaper.pdf
65. Malterud K. Qualitative research: standards, challenges, and guidelines. Lancet [Internet].
2001;358:483–8. Available from:
http://web.a.ebscohost.com.eza.udesa.edu.ar/ehost/pdfviewer/pdfviewer?vid=4&sid=418f
25c8-6388-464a-b616-d3778f3f27e3%40sessionmgr4006
66. Spano R. Observer behavior as a potential source of reactivity: Describing and quantifying
observer effects in a large-scale observational study of police. Sociol Methods Res.
2006;34(4):521–53.
67. Blase K, Fixsen DL. Core intervention components: identifying and operationalizing what
makes programs work. ASPE Res Br. 2013;(February):21.
68. de Haan E, Grant AM, Burger Y, Eriksson PO. A large-scale study of executive and
119
workplace coaching: The relative contributions of relationship, personality match, and
self-efficacy. Consult Psychol J. 2016;68(3):189–207.
69. de Haan E, Duckworth A, Birch D, Jones C. Executive coaching outcome research: The
contribution of common factors such as relationship, personality match, and self-efficacy.
Consult Psychol J. 2013;65(1):40–57.
70. Jowett S, Cockerill IM. Olympic medallists’ perspective of the athlete-coach relationship.
Psychol Sport Exerc. 2003;4(4):313–31.
71. Horvath AO, Symonds BD. Relation Between Working Alliance and Outcome in
Psychotherapy: A Meta-Analysis. J Couns Psychol. 1991;38(2):139–49.
72. Bono JE, Judge TA. Personality and Transformational and Transactional Leadership: A
Meta-Analysis. J Appl Psychol. 2004;89(5):901–10.
73. Turnnidge J, Cote J. Applying transformational leadership theory to coaching research in
youth sport: A systematic literature review. Int J Sport Exerc Psychol. 2018;16(3):327–42.
74. Kellett JB, Humphrey RH, Sleeth RG. Empathy and complex task performance: two
routes to leadership. Leadersh Q. 2002;13:523–44.
75. Hobfoll SE. Conservation of Resources: A New Attempt at Conceptualizing Stress. Am
Psychol. 1989;44(3):513–24.
76. Hobfoll S, Halbesleben J, Neveu J, Westman M. Conservation of resources in the
organizational context: The reality of resources and their consequences. Annu Rev Organ
Psychol Organ Behav. 2018;5:103–28.
77. French KA, Allen TD, Henderson TG. Challenge and hindrance stressors in relation to
sleep. Soc Sci Med [Internet]. 2019;222(January 2018):145–53. Available from:
https://doi.org/10.1016/j.socscimed.2019.01.009
78. Peláez Zuberbuhler MJ, Salanova M, Martínez IM. Coaching-Based Leadership
Intervention Program: A Controlled Trial Study. Front Psychol. 2020;10(January):1–22.
79. O’Connor S, Cavanagh M. The coaching ripple effect: The effects of developmental
coaching on wellbeing across organisational networks. Psychol Well-Being Theory, Res
Pract. 2013;3(1):2.

120
Report
Phenomenology: (Re)Search for Meaning in Behavioral and Community Health

121
Public Health Relevance Statement
Current behavioral and community health research is rooted in conventional scientific
paradigms that prioritize inquiry into objective mechanism. Deeply held ideologies drive that
paradigm and constrain the translation of science to daily life; however, phenomenology may be
a complementary mode of inquiry to investigate meaning, thereby expanding the understanding
of health and connecting research to human experience. Strategies to leverage the transformative
potential of phenomenology include novel research approaches, daily reflective practice, and
interdisciplinary courses in higher education.

122
Introduction
This is a report about uncovering ideologies that drive behavioral and community health
research. Calls for novel methods that yield scientific advancements for “wicked” (1,2) health
problems such as obesity are ubiquitous (3–5). However, philosophical assumptions within the
current scientific paradigm (6) may constrain progress. By peeling back the layers of
worldviews and historical punctuations (7,8) that shape current science, I aim to galvanize
curiosity in and reflection on modes of inquiry, such as phenomenology. This interdisciplinary,
exploratory report includes three parts with one overview figure preceding each part: In Part 1, I
track the history of randomized controlled trials (RCTs) as the gold standard for physical activity
research. In Part 2, I introduce phenomenology as a mode of inquiry that is both alternative and
complementary to conventional science. Finally, in Part 3, I propose potential ways that
behavioral and community health researchers can leverage the transformative potential of
phenomenology, the study of human meaning (9). Overall, phenomenology is a compelling,
complementary mode of inquiry that could reduce the research-practice gap and strengthen the
science-life connection.
123
124
Part 1: Why are randomized controlled trials the gold standard for physical activity
research in behavioral and community health science?
See Figure 1 for a timeline of historical punctuations
The description of randomized controlled trials (RCTs) as the “gold standard” for
medical research first appeared in The New England Journal of Medicine in 1982 (10). The
authors of this article described RCTs as “unattainable,” an elusive idea (11). The timing of
introducing “gold standard” in medical research literature was ironic because it coincided with
the United States’ abandonment of the financial gold standard (see glossary) (12), as had been
established by Isaac Newton in Britain in 1717 (10): A study design encompassing Newton’s
groundbreaking scientific reasoning began to flourish just as his international finance tool
waned.
As RCTs grew in status, there was some controversy over its representation of unitary
worldviews, dogmatism, and medical monotheism (10,13,14). RCTs reflect a worldview that
emerged in the Scientific Revolution in the 1600-1700s (10,14–17). This worldview—now
known as conventional science, natural science, or just “science”—is the dominating paradigm
for medical and biomedical research (14). Founding philosophers and scholars included Rene
Descartes, the French mathematician and philosopher who formulated mind-body dualism
(“Cartesian dualism”); Isaac Newton, the English polymath who originated four rules for
scientific reasoning; and Auguste Comte, the French philosopher who developed positivism (i.e.,
knowledge comes from verifiable, material evidence that can be empirically quantified) (14,18).
Interpretations and applications of these originary viewpoints have evolved over the last three
centuries; however, the dominant mode of inquiry in medical and health research still places

125
objectivity, realism, and mechanical causation as the foundation of how the world works
(ontology) and what counts as legitimate knowledge (epistemology) (14,19).
Because behavioral and community health research is nested in the medical domain,
RCTs have become the gold standard for studying lifestyle interventions, such as physical
activity programs. The link between physical activity and medicine has a rich history from
ancient India, Greece, and Rome (20–22) to the establishment of the American College of Sports
Medicine in 1954, to the shift from “exercise training as physical fitness” to “physical activity
health” in 1993 (23), and finally to the “Exercise is Medicine” trademark at the American
Medical Association (AMA) and ACSM joint meeting in 2007 (24).
The first RCT of a lifestyle physical activity intervention was conducted by Epstein et al.
in 1985 (25,26). In 1995, the ACSM and Centers for Disease Control and Prevention (CDC)
published the first national guidelines on Physical Activity and Public Health (27), and in 2008
the United States Department of Health and Human Services published the first Physical Activity
Guidelines for Americans (PAGA) (28). The PAGA were updated in 2018 (29). Each set of
guidelines quantifies the amount and intensity of exercise needed for health benefits among
various populations. To accomplish this quantification, the executive committees that developed
the guidelines increasingly focused on trials establishing dose-response relationships. RCTs are
a strong design for this sort of causal quantification (13,30) and their frequent citation in the
dissemination of the guidelines may have reinforced a “hierarchy of evidence” in physical
activity research. Aligned with evidence-based medicine (15,19), this hierarchy ranks meta-
analyses of RCTs and RCTs themselves as the best research designs followed by
epidemiological or observational designs and case studies (31). The hierarchy does not explicitly
include qualitative studies. The hierarchy makes sense when applied to questions of dose-
126
response or causation, but it seems myopic when applied to the entire range of research questions
or aims related to physical activity, behavioral interventions, and community health. In other
words, I contend that applying the hierarchy of evidence to multifaceted wicked problems and
the entire translational research spectrum (32) limits the breadth, depth, and applicability of
scientific inquiry to human experience.
The hierarchy of evidence with RCTs at the top has been instrumental in establishing the
efficacy of physical activity interventions (33,34). However, the fact that only 25% of
Americans meet the physical activity guidelines (35) suggests that other modes of inquiry with
different standards may be necessary to translate explanatory findings to real-world application.
Advancing behavioral and community health may require a paradigm shift, or at least an
awareness of how the current scientific paradigm may constrain research translation.
Paradigms, as defined by seminal historian Thomas Kuhn, are "universally recognized
scientific achievements that, for a time, provide model problems and solutions for a community
of practitioners” (6). In the case of medicine and health, we practice research within a natural
science paradigm as established by Descartes, Newton, etc., in the Scientific Revolution.
Methodologically, we prize a priori, controlled systematic processes that emphasize third-
person objectivity, numerical significance, causation (e.g. efficacy, effectiveness), and
nomothetic, universal findings (e.g., external validity, generalizability, transferability,
scalability). On the practical side, professional advancement, grant accrual, and academic
training reinforce the status of empirical materialism and measurable cause-and-effect as the best
indicators of scientific achievement.
Finally, the scientific community’s reliance on peer-reviewed journals perpetuates the
conventional paradigm. Paradoxically, we communicate novel findings through old
127
dissemination channels founded on objectivity. In striving to write scientifically, we strip any
indication of subjectivity from our writing: We remove researchers from the process and
minimize the situatedness of knowledge production (36) by dogmatically avoiding first-person
voice and stripping expressiveness from language. Vocative writing is labeled as colloquial or
unprofessional. Passive voice is the norm. And, as the two previous sentences demonstrate,
removing the subject from a sentence conveys a cosmic authority, as if a statement were
ordained by the universe, not crafted by a human whose physical senses and cognition enacted
(37–39) the “fact” being stated. Overall, there appears to be a subjectivity taboo that negates the
role of human consciousness in doing science (40).
I believe that this negation of subjectivity is one reason the research-practice gap persists.
The cause-and-effect science of engaging in 150 minutes of moderate physical activity each
week (29) is not the same as the meaning-laden life practice of finding the time, place, and
motivation to exercise from childhood to old age. As neurosurgeon and neuroscientist Paul
Kalanithi wrote:
We build scientific theories to organize and manipulate the world, to reduce
phenomena into manageable units. Science is based on reproducibility and
manufactured objectivity. As strong as that makes its ability to generate claims
about matter and energy, it also makes scientific knowledge inapplicable to the
existential, visceral nature of human life, which is unique and subjective and
unpredictable. Science may provide the most useful way to organize empirical,
reproducible data, but its power to do so is predicated on its inability to grasp the
most central aspects of human life: hope, fear, love, beauty, envy, honor,
weakness, striving, suffering, virtue (41).
In this quote, Kalanithi couches his critique of science in the conventional, natural paradigm.
And the limited ontology within that paradigm creates a science-life schism. The
methodological and practical manifestations of that paradigm are easily visible, but the
underlying philosophical assumptions are not so easily grasped. Examining ontological (what is
128
being?) and epistemological (what is knowledge?) assumptions is intellectually challenging and
emotionally charged. But looking deeply at what is beneath the statistics and qualitative coding
of “science” could open modes of inquiry (see Figure 2) that connect the mechanism of physical
activity with the meaning of daily life.

129
130
Part 2: What is phenomenology?
See Figure 2 for a comparison of conventional science and phenomenology
American psychologist and philosopher William James posited that there are two forms
of research questions: questions of mechanism and questions of meaning (42). Questions of
meaning encapsulate values, subjectivity, and consciousness that reflect a world of fluctuating
reality as experienced through individual perception. In this worldview of multiple ontologies,
first person accounts and idiographic experiences are a legitimate, necessary aspect of research
(43). However, modes of inquiry that address research questions related to meaning do not fit
the current scientific paradigm of objectivity and nomothetic answers. We need to identify and
practice a mode of inquiry that could complement the current paradigm to more fully address
human health by rigorously investigating questions of meaning. Phenomenology may be one
such complement (18,44,45).
Phenomenology is the study of meaning and emerged in European philosophy and
literature in the 1900s (9,46,47). German philosopher and mathematician Edmund Husserl is
considered the founder of phenomenology, specifically transcendental or descriptive
phenomenology which rejects positivism in favor of an epistemology based on immediate, inner
experiential evidence (9,48,49). Another German philosopher-mathematician crucial to
phenomenology is Martin Heidegger. Heidegger focused on ontology and founded hermeneutic
or interpretive phenomenology. He introduced the existential turn and insisted upon grappling
with the inceptual challenge of meaning, including the ontological implications of technology
and language (9,44,48,50). Language, particularly writing as a mode of inquiry and the
imperialistic nature of naming things, plays a central role in phenomenology. The centrality of
writing is unsurprising since phenomenology is associated with existential literature (9) and the
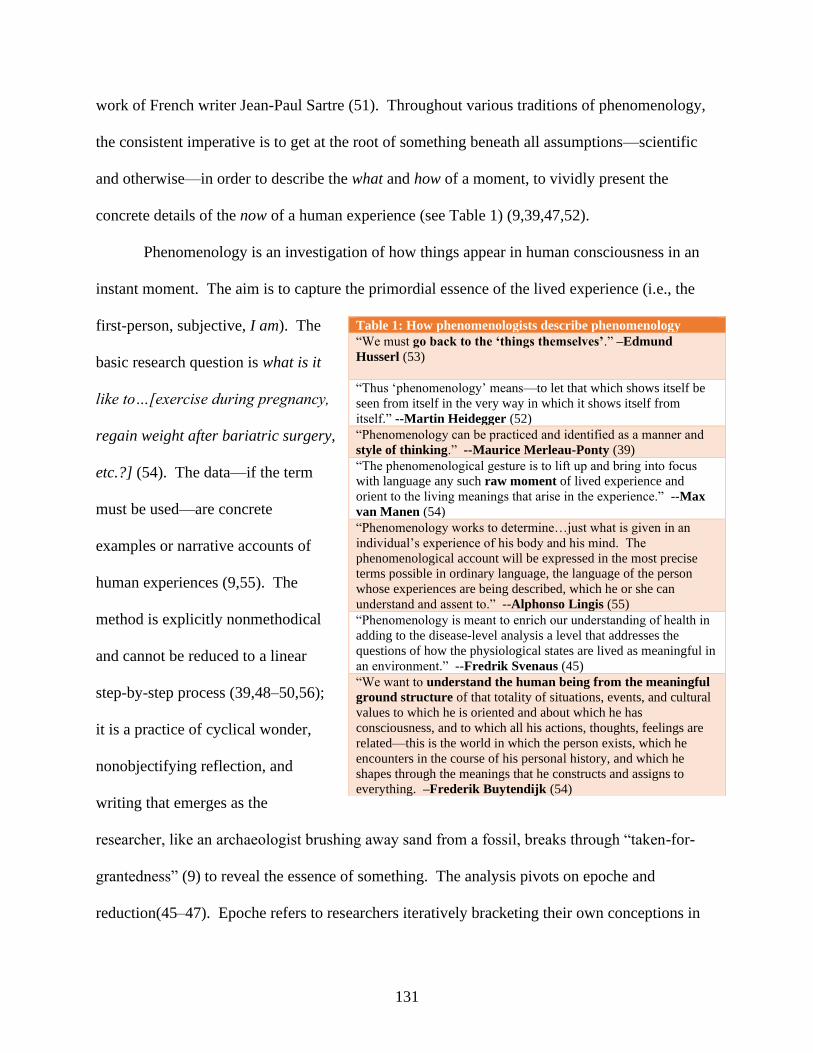
131
work of French writer Jean-Paul Sartre (51). Throughout various traditions of phenomenology,
the consistent imperative is to get at the root of something beneath all assumptions—scientific
and otherwise—in order to describe the what and how of a moment, to vividly present the
concrete details of the now of a human experience (see Table 1) (9,39,47,52).
Phenomenology is an investigation of how things appear in human consciousness in an
instant moment. The aim is to capture the primordial essence of the lived experience (i.e., the
first-person, subjective, I am). The
basic research question is what is it
like to…[exercise during pregnancy,
regain weight after bariatric surgery,
etc.?] (54). The data—if the term
must be used—are concrete
examples or narrative accounts of
human experiences (9,55). The
method is explicitly nonmethodical
and cannot be reduced to a linear
step-by-step process (39,48–50,56);
it is a practice of cyclical wonder,
nonobjectifying reflection, and
writing that emerges as the
researcher, like an archaeologist brushing away sand from a fossil, breaks through “taken-for-
grantedness” (9) to reveal the essence of something. The analysis pivots on epoche and
reduction(45–47). Epoche refers to researchers iteratively bracketing their own conceptions in
Table 1: How phenomenologists describe phenomenology
“We must go back to the ‘things themselves’.” –Edmund
Husserl (53)
“Thus ‘phenomenology’ means—to let that which shows itself be
seen from itself in the very way in which it shows itself from
itself.” --Martin Heidegger (52)
“Phenomenology can be practiced and identified as a manner and
style of thinking.” --Maurice Merleau-Ponty (39)
“The phenomenological gesture is to lift up and bring into focus
with language any such raw moment of lived experience and
orient to the living meanings that arise in the experience.” --Max
van Manen (54)
“Phenomenology works to determine…just what is given in an
individual’s experience of his body and his mind. The
phenomenological account will be expressed in the most precise
terms possible in ordinary language, the language of the person
whose experiences are being described, which he or she can
understand and assent to.” --Alphonso Lingis (55)
“Phenomenology is meant to enrich our understanding of health in
adding to the disease-level analysis a level that addresses the
questions of how the physiological states are lived as meaningful in
an environment.” --Fredrik Svenaus (45)
“We want to understand the human being from the meaningful
ground structure of that totality of situations, events, and cultural
values to which he is oriented and about which he has
consciousness, and to which all his actions, thoughts, feelings are
related—this is the world in which the person exists, which he
encounters in the course of his personal history, and which he
shapes through the meanings that he constructs and assigns to
everything. –Frederik Buytendijk (54)
132
order to open themselves to phenomena as free—or as free as possible—from presuppositions.
Reduction refers to stripping away “taken-for-grantedness in order to make contact with the
prereflective world” (9).
Although many forms of qualitative inquiry embrace subjectivity (57–59), not all
qualitative research is phenomenology (47,60). In health research (61), the predominant
qualitative methods that include checklists of rigor and trustworthiness (62,63), coding
procedures (47), and an emphasis on theory (47,61,64), reflect conventional notions of science,
or at least are crafted to fit within “scientific” structures such as peer-reviewed journals. In
addition, the typical subjectivity in qualitative research consists of reflective opinions. In
contrast, phenomenology aims for a concrete description or detailed narrative of a momentary
experience as it happened. Phenomenology is unique among qualitative approaches in its focus
on prereflective, unmediated experience (39,54)—not on current feelings of a past experience,
but an account of what happened back in the original moment. For example, in evaluating a
coaching intervention, our research team included a typical qualitative item: Was the coach
effective? Why or why not? A more phenomenological question would have taken the
participant back to a specific moment, perhaps of initially meeting the coach: Think back to your
first coaching session, specifically the beginning of the first session. Describe the first moment
of meeting the coach.
In phenomenology, the authority of the research comes from the concrete details of a
raw moment itself, whereas many other forms of qualitative inquiry, such as ethnography (see
Additional Material A), derive authority from integrating theories, models, and frameworks
throughout the research process (47,57,65). Phenomenology’s rejection of confining human
experience to theories, models, and frameworks reflects a primary distinction from conventional

133
inquiry, including inquiry in behavioral (66,67) and implementation science (61,68): Instead of
seeking control or order, phenomenology thrives on tension, paradox, unpredictability, and
noncognitive sensibilities (9).
This focus on ontological paradox and circularity may be criticized as inefficient or
impractical (37), particularly in addressing pressing corporeal needs (e.g., does irisin, a hormone
secreted from muscles in response to exercise, have a therapeutic effect on COVID-19 patients
(69)?). In addition, the phenomenological emphasis on language and philosophy may be
esoteric, pretentious, and “fragile” (9,70). Phenomenological writing itself is vivid and poetic,
embedded with meaning that is not easily paraphrased or condensed for traditional peer-reviewed
publications. This fragility and depth is in contrast to the “robust” and operative nature of
information-based, conventional scientific writing (9). A final criticism of the nonmethod
method of phenomenology is the difficulty appraising research that denies universal validation
criteria.
Many of these criticisms reflect phenomenology’s ontological differences from the
current paradigm of medical and health research which focuses on the corporeal body—the third-
person, the object, the body they have. Phenomenology acknowledges the lived body—the first-
person, the agent, the body I am (48,50,56). One way to understand these two perspectives of
the same body is to consider disease as studied, diagnosed, and treated compared to dis-ease as
what the patient experiences (44). This second perspective of the body—the lived body—
reflects Maurice Merleau-Ponty’s expression of embodied phenomenology in which the coupling
of body objectivity and subjectivity forms—enacts—the existential situation (i.e., the raw
moment experienced by a human), just as two palms pressed together are both the subject/object
creating the experience of simultaneously touching and being touched (39). Merleau-Ponty’s

134
description of attunement, or bodily orientation, relates to the important dimension of meaning in
behavior. With attunement, behavior is not mere stimulus-response, and perception is not just
disembodied consciousness or mental representations. Instead, behavior and human actions are
afforded by the world enacted through embodied perception and cognition (18,37,39,50). This
brain-teasing description boils down to the basic phenomenological worldview of experientially-
derived relational (not dualistic) ontology. This worldview “consists in commitments to a reality
that includes possibility, meaning, temporality, and final causation—that is, an ontology which is
far more inclusive than that of conventional positivistic science” (18).
The inclusiveness of the phenomenological ontology could provide a broad foundation
for behavioral and community health research. The phenomenological worldview may translate
more readily to real-world health behaviors and practices than the depersonalized, disembodied
worldview of conventional science. The current pandemic is a powerful example of the
difficulty connecting science to real-world health behaviors (71,72), such as social distancing
which does not fit well into mathematical models of intention-behavior relationships (73). Only
32% of adults say that medical research scientists provide fair or accurate information most of
the time (74). Public doubt in science during the pandemic appears to reflect a web of religious
and political beliefs (75), as well as concerns over loss of personal/human control (76). Herein
lies the importance of rigorously considering multiple ontologies in the conduct and
dissemination of health science: Humans need to see themselves in the research.
Overall, phenomenology is not a rejection of science, but a recognition of the ontological
and epistemological limitations and assumptions within conventional science (18,44).
Conventional science, epitomized by the gold standard of RCTs, suspends ontological
complexities and depersonalizes phenomena to accomplish practical research tasks and
135
investigate mechanism (40). In contrast, phenomenology foregrounds (38) philosophical
considerations and personal experience to gain insight into life as we live it (9) and investigate
meaning. It is the differences between conventional science and phenomenology that makes
them complementary in cultivating a health research landscape that equally includes mechanism
and meaning. Continuing the current hegemony of mechanism over meaning may perpetuate the
research-practice, science-life gap.
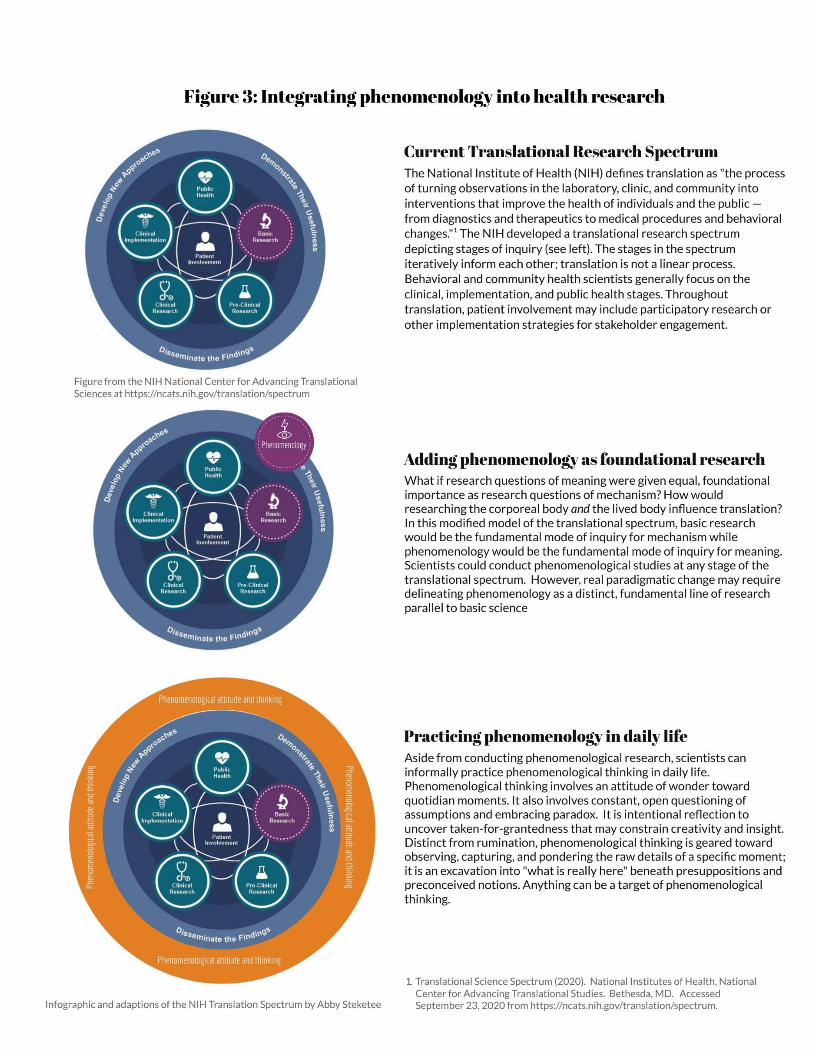
136
137
Part 3: How can behavioral and community health scientists leverage the
transformative potential of phenomenology?
See Figure 3 for integrating phenomenology in health research
A central argument in this report is that phenomenology has potential as a
complement, not replacement, for conventional natural science in health research and
practice (18,44). The complementary use of phenomenology and conventional science
would expand the scope—and, therefore, translational foundation—of health research to
understand both mechanism (the corporeal body) and meaning (the lived body). What
follows is a description of radical to moderate actions3 for integrating phenomenology in
health research and practice. In research, applications include an additional domain on
the translational research spectrum; a novel perspective of mixed-methods research; and
phenomenological investigation of emergent topics such as coaching and yoga. In
practice, phenomenology may be a vehicle for intellectual conditioning and cognitive
calibration that facilitate inclusive, transparent research.
Research
Explicitly adding phenomenology to the National Institute of Health’s (NIH)
translational science spectrum (32) may be radical and unlikely, but would support a
paradigm shift granting equal importance to mechanism and meaning, instead of the
current hegemony of mechanism as the preeminent research target. In this radical shift,
phenomenology and basic science would play parallel roles of informing and being
informed by research at all stages of the translational spectrum. Phenomenology would
reveal fundamental meaning(s) of disease and behavior, while basic science would reveal
3 In this paper, I use the word radical to refer to phenomenological applications that I perceive as more
revolutionary or revisionistic, such as updating the NIH’s Translational Research Spectrum. I use the word
moderate for phenomenological applications that are less sweeping or extreme, such as conducting a single
phenomenological study.
138
fundamental mechanism(s). For example, in understanding the combination of obesity
and osteoporosis, basic science investigation may focus on genes that influence both bone
turnover and obesity, while phenomenological investigation may uncover what it is like
for an older adult in Appalachia to live with obesity and osteoporosis.
The importance of including phenomenology—or at least rigorous investigation
of meaning—in the translational spectrum was illustrated in my experience attempting to
implement a gestational weight gain control intervention in rural Southwest Virginia (77).
Extensive research demonstrating the deleterious effects of excessive gestational weight
gain was readily available (78–80). However, when our research team directly interacted
with pregnant women in the community, we realized that the scientific prerogative to
control gestational weight gain did not match the women’s daily priorities and needs:
The basic objective science of the corporeal body did not capture the basic human
experience of the lived body. Empirical evidence was not the same as phenomenological
listening. There was a science-life gap that formative phenomenological research may
have prevented (see Additional Material A).
A less radical option for integrating phenomenology is to rethink mixed method
approaches. Mixed method approaches, as advocated in behavioral and implementation
science, combine quantitative and qualitative measures and analysis (30,81–83).
Rethinking this approach involves shifting from the methodological level (e.g.,
performing quantitative and qualitative procedures) to an axiological level (e.g., valuing
research questions of mechanism and of meaning). The shift amounts to
reconceptualizing “mixed methods” as “dual purpose” with two research questions. For
example, consider an investigation with the long-term goal of establishing community-
139
based programs for individuals with obesity and osteoporosis. Toward that goal, the aim
of one study may be to pilot test a yoga coaching program in rural Southwest Virginia.
The dual research questions could be (1) what is it like for individuals with obesity and
osteoporosis to participate in a 12-week yoga program? and (2) what is the effect of the
12-week yoga program on bone biomarkers and grip strength? Researchers would
investigate the first research question of meaning through phenomenological interviews
(9,84) and investigate the second question of mechanism through bone turnover markers
(e.g., serum N-terminal propeptide of type I procollagen (P1NP) and serum C-terminal
telopeptide of type I collagen (85)) and hand-held dynameters (86).
The key in this example is not the combination of qualitative and quantitative
methods, but equal, deliberate worth to first-person, idiographic experience and third-
person, physiological indicators. It’s not only about the doing of the methods; it’s about
the value or ranking of the methods—the way qualitative research is a side kick but
rarely the full protagonist. This distinction between mixed method and dual purpose may
seem subtle but is indicative of underlying values and assumptions of what matters in
science versus what matters in an individual’s daily life.
The value gap may perpetuate the difficulty of translating science to public
policy. Foregrounding values within research establishes a foundation for balancing
objectivity and advocacy (87) as is necessary for developing health policy. By
operationalizing Simon Chapman’s advice that “values are everything,” (88)
phenomenology may bridge the “parallel universes” (87) of researchers and policymakers
when applied in its original sense (70). The idiographic nature of phenomenology may
initially seem antithetical to nomothetic public health and policy. However, the vividness
140
and situatedness of phenomenological accounts may be emotionally- and regionally-
salient to policy makers motivated to enhance the daily lives of their constituents. In
other words, phenomenological content and writing may connect science to policy
makers, thereby enhancing research translation.
Even less radical than reconceptualizing mixed methods approaches is conducting
individual phenomenological studies within behavioral and community health. Two
potential research topics are coaching and yoga. Coaching, which is quickly rising as a
person-centered approach to health (89–92), involves cultivating connections between
empirically-based evidence and experientially-based life. In constantly uncovering inner
meaning, coaching is inherently phenomenological. But phenomenological approaches
have not been applied in coaching research. Phenomenological research on yoga is also
rare (93,94), despite consistent calls for first-person investigation into contemplative (i.e.,
mindfulness) practices such as yoga and meditation (95–97). Answering these calls for
phenomenological research will require scientists to reflect on their own assumptions of
what counts as legitimate evidence and to partner with phenomenologists or spend
considerable time delving into worldviews that differ from their implicit or explicit
scientific training. The pay-off of this deep work will be more inclusive, person-centered
translational research that encompasses diverse human experience.
Practice
Researchers can also leverage phenomenology as a daily practice and mode of
thinking. As philosopher Max Van Manen wrote, phenomenology “nurtures a measure of
thoughtfulness and tact in the practice of our professions and everyday life” (9). I
envision phenomenological thinking as intellectual conditioning, similar to cross-training
141
in elite swimming. Even though swimmers compete in the water, they do extensive
exercises on land (e.g., “strength and conditioning”) to prevent injuries and build
foundational athletic capacities. Pull-ups are not an Olympic swimming event; however,
most swimmers deliberately train them to build strength toward a faster 100 meter time.
Likewise, health researchers may not conduct or publish phenomenology, but examining
philosophical assumptions underlying their methods will help them be better
“competitors” and “teammates” by cultivating foundational intellectual capacities such as
critical thinking, wonder, open observation, and clear writing.
Another metaphor for phenomenology is cognitive calibration. We calibrate
microscopes: Why not calibrate our own thinking as a fundamental instrument of inquiry
in science? The way we use our five senses—and possibly sixth sense of consciousness
(40)—“enacts” science (37,38). Research is an “embodied” (39) action with perception
as the foundation on which all other research tools depend. Practicing phenomenological
awareness by iteratively questioning and peeling away assumptions may fine-tune or
broaden our perception and cognition. This calibration may foster ongoing personal
development and insight unconstrained by paradigmatic ideology and expectations.
Furthermore, cognitive calibration and intellectual conditioning may fuel more
inclusive research—research that acknowledges the animistic traditions of many
indigenous populations or Eastern nondualist beliefs; research that delves into health-
related dimensions of Black Lives Matter; research that checks itself for both scientism
and solipsism. A practical phenomenological attitude involves intentional examination of
worldviews so that the only marker of science is not how true is it? as measured by
quantifiable, statistical, or generalizable significance, but also for
142
whom/what/when/where/why might it be good? in terms of subjective meaning and
“goodness(es)” (38) across diverse individuals. Current pushes for realist (98–100) or
pragmatic (101,102) research seem to reflect this idea of multiple goodness(es) and
variable experience. However, they do not go far enough to liberate exploration of
meaning from conventional scientific assumptions of truth, such as the need to base
research in theory and use reproducible, systematic methods. The pressure to be
scientific or exude objectivity is one reason the practice of a phenomenological attitude is
important: It gives us a vehicle for examining the unspoken expectation to uphold a
certain paradigm. It reminds us to consider the roots of our reactions to content in grant
applications, research protocols, and manuscripts—do we reject something because it
does not fit within our constructed definition of science or do are we reject it because of
unethical, sloppy, or shallow aspects? Along the way, do we remember that research,
whether answering questions of mechanism or meaning, is a human process?
A daily phenomenological attitude toward this human process may foster
intentionality—not dogma—as a catalyst for transparency and openness. Transparency
and openness may improve interdisciplinary, or even transdisciplinary, approaches to
wicked health problems (2). Interdisciplinary thinking (see Additional Material C) is one
way to describe what I have repeatedly advocated in this report: the complementary use
of modes of inquiry from different paradigms that can balance the other’s strengths and
weaknesses, blind spots, and insights.

143
Conclusion
See Table 2 for summary of Parts 1, 2, and 3
Table 2: Summary of answers to Parts 1, 2, and 3 questions
Part 1: Why are randomized controlled trials
the gold standard for physical activity research
in behavioral and community health science?
…because research into physical activity lifestyle
interventions is part of the historical Exercise is
Medicine movement, and the Exercise is Medicine
movement emerged from medical research in which
the conventional science paradigm dominates.
Part 2: What is phenomenology? …the study of meaning and how things appear in
human consciousness in an instant moment; the
search for the root of a phenomenon beneath all
assumptions—scientific and otherwise—in order to
describe the what and how of a moment, to vividly
present the concrete details of the now of a human
experience.
Part 3: How can behavioral and community
health researchers leverage the transformative
potential of phenomenology?
…radically add phenomenology to the NIH’s
translational research spectrum; shift from mixed-
methods to dual-purpose approaches; conduct
individual phenomenological studies of coaching
and contemplative practices; practice
phenomenological attitude and thinking in daily life.
Philosophy for scientists?
This report is not an attack on conventional or basic science, but a call to examine
the philosophies on which any science is constructed. For health researchers, what is the
use of studying the history and philosophy of science, of considering ontology and
epistemology? Should we not spend all of our time on content-specific study or research
methodology? Albert Einstein answered this question in a letter to a young physicist on
December 7, 1944:
I fully agree with you about the significance and educational value of
methodology as well as history and philosophy of science. So many people
today—and even professional scientists—seem to me like somebody who has
seen thousands of trees but has never seen a forest. A knowledge of the
historic and philosophical background gives that kind of independence from
prejudices of his generation from which most scientists are suffering. This
independence created by philosophical insight is—in my opinion—the mark
of distinction between a mere artisan or specialist and a real seeker after truth
(103).

144
Later, in a memorial address for physicist Ernst Mach, Einstein again championed
vigorous investigation of epistemology:
Concepts that have proven useful in ordering things easily achieve such an
authority over us that we forget their earthly origins and accept them as
unalterable givens. Thus they come to be stamped as “necessities of thought,”
“a priori givens,” etc. The path of scientific advance is often made
impassable for a long time through such errors. For that reason, it is by no
means an idle game if we become practiced in analyzing the long
commonplace concepts and exhibiting those circumstances upon which their
justification and usefulness depend, how they have grown up, individually,
out of the givens of experience (104).
In other words, science and knowledge production is a human process, and we, as
humans, have permission to participate. But, if we participate, there is an
intellectual—possibly even moral—imperative to examine the deep assumptions
within our work. Phenomenology is one mode of inquiry for that examination.
Limitations and future directions
This report is not an exhaustive history, systematic review, or philosophical
treatise. Limitations include the general use of terms such as health, perception,
assumption, fact, and evidence which vary in definition and connotation from field to
field. Other limitations include the tacit inclusion of post-positivism within positivism
and impression that conventional science and phenomenology are the only or best modes
of inquiry for all health research.
In this report, I have depicted questions of mechanism and meaning as separate.
This simplistic depiction has been a rhetorical convenience, just as the separation of
objectivity and subjectivity may be a methodological convenience in conducting hard
science. Questions of mechanism and meaning are not mutually exclusive. However, the
tension between them has implications in all stages of research. What is important is

145
recognizing the tension and making research decisions—rhetorical, methodological, or
otherwise—deliberately.
A final limitation is that I have not formally conducted phenomenological
research myself. My style of thinking, writing, coaching, and being is inherently
phenomenological, but I did not recognize it as such until I read the original works of
phenomenologists. Before an independent study in the fall of 2020, my exposure to
phenomenology had been only the few pages in qualitative textbooks. My awareness of
and training in worldviews was similarly limited. The statistics and research methods
classes I completed at two different universities had only passing mention (a short
introductory reading and no class discussion or assignments) of scientific worldviews,
and neither of my graduate degrees have required coursework in worldviews or
philosophy. This gap in education is evidence of the assumed or unexamined nature of
the philosophies that undergird translational research and dominate behavioral and
community health science.
To foreground these philosophies, I have designed a graduate level courses for
interdisciplinary approaches to health research (see Additional Material C). Students in
the course will engage with challenging, interdisciplinary texts as they examine
paradigms; explore definitions of science, research, and health; cultivate their own
ontological and epistemological ideologies; and generate novel approaches and
perspectives to wicked problems. As a whole, the course builds a foundation for long-
term critical thinking and deep work.
Final note

146
In this report, I have attributed positivism to Auguste Comte. Comte certainly
coined the term, but the modern connotation of positivism as cold and mechanical
obfuscates the complexities of his dynamic work in which he integrated science and
politics, including the motto “Love as principle, order as basis, progress as end” (105).
The complexities within Comte’s original positivism illustrate the inseparability of love
and science, value and fact, mechanism and meaning. It is this intertwined complexity
that establishes the possibility of conventional science and phenomenology as
complementary modes of inquiry for health research.

147
Glossary
Axiology: philosophical assumption about the role of values (47)
Epistemology: philosophical assumption about what counts as knowledge and the relationship between
the knower and the known (47)
Gold standard (financial): defining national monetary units in quantities of gold so that exchange rates
between countries who adopt the gold standard are fixed; dates back to 1717 when Isaac Newton, as Master
of the Mint, made a historic mistake in calculating that one gold guinea equaled 21 shillings—or one gold
coin equaled 21 silver coins (12)
Implementation: integrating evidence-based interventions, practices, or policies in usual settings (106);
applying research findings to real-world settings
Idiographic: concerned with the individual and uniqueness (107)
Interdisciplinary: thinking, research, or collaboration that “analyzes, synthesizes, and harmonizes links
between disciplines into a coordinated and coherent whole” (108)
Mixed method research: studies that integrate quantitative and qualitative approaches (81)
Nomothetic: concerned with general laws that apply to all people (107)
Ontology: philosophical assumption about the nature of reality or “being” (47)
Paradigm: “universally recognized scientific achievements that, for a time, provide model problems and
solutions for a community of practitioners” (6); pervasive worldview within a culture or group of people
Philosophy: from the Latin philosophia (“love of wisdom”); the discipline of analyzing the grounds of
fundamental beliefs; a system of ideologies, concepts, or attitudes (109)
Pragmatic health research: investigate whether a program works under “usual, real-world” conditions
rather than under ideal, controlled conditions (101)
Randomized controlled trial (RCT): research design that involves assigning participants by chance to an
experimental group that receives an intervention or to a control group that does not receive the intervention;
generally considered the best design to investigate efficacy and effectiveness (30)
Realist health research: testing context-mechanism-outcome configurations; investigating “what is it
about this intervention or program that works for whom?” (99)
Situatedness: “involvement within a context” (110); how an entity (such as a researcher or research) is
“shaped by linguistic, biographical, historical, political, economic, cultural, ideological, material, and
spatial dimensions” (110); dynamic and shifting ways of being depending on positionality and context
Translation: “the process of turning observations in the laboratory, clinic, and community into
interventions that improve the health of individuals and the public” (32)
Translational science: “the field of investigation focused on understanding the scientific and operational
principles underlying each step of the translational process” (32)
Wicked problem: issues that are embedded in society and have many causes and multiple interests (2)
Worldview: “intertwined, interrelated, interconnected system of beliefs” (111)
148
References
1. Rittel H, Webber M. Dilemmas in a General Theory of Planning. Policy Sci.
1973;155–69.
2. Brown V. Tackling Wicked Problems Through the Transdisciplinary Imagination.
Harris J, Russell J, editors. London: Earthscan; 2010.
3. Mcpherson AC, Ball GDC, Swift JA, Cairney J, Knibbe TJ, Krog K. A Call to
Action: Setting the Research Agenda for Addressing Obesity and Weight-Related
Topics in Children with Physical Disabilities. 2016;12(1):59–69.
4. Kaiser KA, Neumeier WH, Carson TL, Dhurandhar EJ, Cardel MI. Biobehavioural
approaches to prevention and treatment : A call for implementation science in
obesity research. 2020;(June 2019):3–9.
5. Duke University. IGNITE Childhood Obesity Research -- Internal Call for
Interdisciplinary Grants for Novel and Innovative Teams to Engage in Childhood
Obesity Research [Internet]. 2019 [cited 2020 Oct 5]. Available from:
https://researchfunding.duke.edu/ignite-childhood-obesity-research-internal-call-
interdisciplinary-grants-novel-and-innovative-teams
6. Kuhn TS. The Structure of Scientific Revolutions. Chicago: University of Chicago
Press; 1962.
7. Eldredge N, Gould S. Punctuated equilibria: An alternative to phyletic gradualism.
In: Schopf T, editor. Models in paleobiology. San Francisco: Freeman Cooper &
Co; 1972. p. 82–115.
8. Picciotto R. Donald T. Campbell’s Evolutionary Perspective and its Implications
for Evaluation. J Multidiscip Educ. 2019;15(33):1–15.
9. Van Manen M. Phenomenology of Practice. New York, New York: Routledge;
2014.
10. Jones DS, Podolsky SH. The history and fate of the gold standard. Lancet
[Internet]. 2015;385(9977):1502–3. Available from:
http://dx.doi.org/10.1016/S0140-6736(15)60742-5
11. Feinstein A, Horwitz R. Double standards, scientific methods, and epidemiologic
research. New Engl J Med. 1982;307:1611–7.
12. Cooper RN. The Facts Gold and Standard: Future Historical Prospects [Internet].
1982. Available from: https://www.brookings.edu/wp-
content/uploads/1982/01/1982a_bpea_cooper_dornbusch_hall.pdf
13. McCambridge J, Kypri K, Elbourne D. In randomization we trust? There are
overlooked problems in experimenting with people in behavioral intervention
trials. J Clin Epidemiol [Internet]. 2014;67(3):247–53. Available from:
http://dx.doi.org/10.1016/j.jclinepi.2013.09.004
14. Wilson HJ. The myth of objectivity: Is medicine moving towards a social
constructivist medical paradigm? Fam Pract. 2000;17(2):203–9.
15. Meldrum M. A Brief History of the Randomized Controlled Trial. Hematol Clin
North Am. 2000;14(4):745–60.
16. Alderson P. Theories in health care and research: The importance of theories in
health care. BMJ. 1998;317:1007–10.
17. Kent J. The Impact of the Scientific Revolution: A Brief History of the
Experimental Method in the 17th Century [Internet]. OpenStax CNX; 2006.
149
Available from: http://cnx.org/contents/39ba7a28-338d-4995-b2e5-
45562bf46024@1
18. Harney M. Naturalizing phenomenology - A philosophical imperative. Prog
Biophys Mol Biol [Internet]. 2015;119(3):661–9. Available from:
http://dx.doi.org/10.1016/j.pbiomolbio.2015.08.005
19. Rosenberg W, Donald A. Evidence based medicine: an approach to clinical
problem-solving. BMJ. 1995;310:1122–6.
20. Berryman JW. Exercise is medicine: A historical perspective. Curr Sports Med
Rep. 2010;9(4):195–201.
21. Berryman JW. The Tradition of the “Six Things Non-Natural”: Exercise and
Medicine from Hippocrates through Ante-Bellum America. Exerc Sport Sci Rev
[Internet]. 1989;17(1). Available from: https://journals.lww.com/acsm-
essr/Fulltext/1989/00170/The_Tradition_of_the__Six_Things_Non_Natural__.17.
aspx
22. Tipton C. The history of “Exercise is Medicine” in ancient civilizations. Adv
Physiol Educ. 2014;38(2):109–17.
23. Haskell W. Health consequences of physical activity: understanding and
challenges regarding dose-response. In: JB Wolffe Memorial Lecture, American
College of Sports Medicine. 1993. p. 649–58.
24. American College of Sports Medicine. EIM in Action [Internet]. 2020. [cited 2020
Sep 9]. Available from:
https://www.exerciseismedicine.org/support_page.php/eim-in-action/
25. Dunn AL. Effectiveness of Lifestyle Physical Activity Interventions to Reduce
Cardiovascular Disease. Am J Lifestyle Med. 2009;3(1_suppl):11S-18S.
26. Epstein LH, Wing RR, Koeske R, Valoski A. A comparison of lifestyle exercise,
aerobic exercise, and calisthenics on weight loss in obese children. Behav Ther.
1985;16(4):345–56.
27. Haskell WL, Lee IM, Pate RR, Powell KE, Blair SN, Franklin BA, et al. Physical
activity and public health: Updated recommendation for adults from the American
College of Sports Medicine and the American Heart Association. Circulation.
2007;116(9):1081–93.
28. Early W, Obesity C, Initiative P, Start H, Taken S, Activity P, et al. Physical
Activity Guidelines for Americans. 2013;(202).
29. US Department of Health and Human Services. 2018 Physical Activity Guidelines
Advisory Committee Scientific Report. To the Secretary of Health and Human
Service [Internet]. 2018. Available from: https://health.gov/paguidelines/second-
edition/report/pdf/PAG_Advisory_Committee_Report.pdf
30. Van Horn L, Beto J. Research Successful Approaches in Nutrition and Dietetics.
Fourth Edi. Van Horn L, Beto J, editors. Chicago, IL: Academy of Nutrition and
Dietetics; 2019.
31. Murad MH, Asi N, Alsawas M, Alahdab F. New evidence pyramid.
2016;21(4):125–7.
32. National Institutes of Health. Translational Science Spectrum [Internet]. 2020
[cited 2020 Apr 19]. Available from: https://ncats.nih.gov/translation/spectrum
33. Love R, Adams J, van Sluijs EMF, Foster C, Humphreys D. A cumulative meta-
analysis of the effects of individual physical activity interventions targeting

150
healthy adults. Obes Rev. 2018;19(8):1164–72.
34. Howlett N, Trivedi D, Troop NA, Chater AM. Are physical activity interventions
for healthy inactive adults effective in promoting behavior change and
maintenance, and which behavior change techniques are effective? A systematic
review and meta-analysis. Transl Behav Med. 2019;9(1):147–57.
35. Centers for Disease Control and Prevention. Trends in Meeting the 2008 Physical
Activity Guidelines, 2008-2018 [Internet]. Atlanta, GA; 2018. Available from:
https://www.cdc.gov/physicalactivity/downloads/trends-in-the-prevalence-of-
physical-activity-508.pdf
36. Latour B, Woolgar S. Laboratory Life: The Construction of Scientific Facts.
Princeton, New Jersey: Princeton University Press; 1979.
37. Varela F, Thompson E, Rosch E. The Embodied Mind: Cognitive Science and
Human Experience. Cambridge, Mass: MIT Press; 1993.
38. Mol A. The Body Multiple: Ontology in Medical Practice. Durham, NC: Duke
University Press; 2002.
39. Merleau-Ponty M. Phenomenology of Perception. C. Smith,. London: Routledge
and Kegan Paul; 1962.
40. Wallace BA. The Taboo of Subjectivity: Toward a New Science of Consciousness.
New York, New York: Oxford University Press; 2000.
41. Kalanithi P. When Breath Becomes Air. New York, New York: Random House;
2016.
42. James W. The Varieties of Religious Experience: A Study in Human Nature
[Internet]. Project Gu. New York: Project Gutenberg; 2014. Available from:
http://www.gutenberg.org/license
43. James W. Does “Consciousness” Exist". J Philos Psychol Sci Methods [Internet].
1904;1:477–91. Available from:
https://psychclassics.yorku.ca/James/consciousness.htm
44. Svenaeus F. A Defense of the Phenomenological Account of Health and Illness. J
Med Philos (United Kingdom). 2019;44(4):459–78.
45. Svenaeus F. The Phenomenology of Health and Illness. In: Kay S, Toombs,
Dordrecht, editors. Handbook of Phenomenology and Medicine. Kluwer; 2001. p.
87–108.
46. Starks H, Brown Trinidad S. Choose Your Method: A Comparison of
Phenomenology, Discourse Analysis, and Grounded Theory. Qual Health Res
[Internet]. 2007;17(10):1372–80. Available from:
https://pdfs.semanticscholar.org/a317/738b3a28d7c2c1af03fd1e22f67058342781.p
df
47. Creswell J, Poth C. Qualitative Inquiry & Research Design. Fourth Edi. Salmon H,
editor. Thousand Oaks, CA: SAGE Publications; 2018.
48. Davidsen AS. Phenomenological Approaches in Psychology and Health Sciences.
Qual Res Psychol. 2013;10(3):318–39.
49. Neubauer BE, Witkop CT, Varpio L. How phenomenology can help us learn from
the experiences of others. Perspect Med Educ. 2019;8(2):90–7.
50. Carel H. Phenomenology and its application in medicine. Theor Med Bioeth.
2011;32(1):33–46.
51. Sartre JP. Being and Nothingness. Barnes H, editor. New York, New York:
151
Washington Square Press; 1956.
52. Heidegger M. Being and Time. J. MacQuar. New York, New York: Harper and
Row; 1962.
53. Husserl E. The Criseis of the European Sciences and Transcendental
Phenomenology. D. Carr T, editor. Evanston, IL: Northwestern University Press;
1970.
54. Van Manen M. Phenomenology in Its Original Sense. Qual Health Res.
2017;27(6):810–25.
55. Lingis A. What Is Given in Experience: The Phenomenological Account. Qual
Health Res. 2017;27(6):805–9.
56. Fernandez AV. Embodiment and Objectification in Illness and Health Care:
Taking Phenomenology from Theory to Practice. J Clin Nurs. 2020;(May):1–10.
57. Tracy S. Qualitative Research Methods: Collecting Evidence, Crafting Analysis,
Communicating Impact. First. Chichester, UK: Blackwell Publishing, Ltd; 2013.
58. Guba E, Lincoln Y. Competing Paradigms in Qualitative Research. In: Denzin
NK, Lincoln YS, editors. Handbook of Qualitative Research [Internet]. SAGE
Publications, Inc.; 1994. p. 105–17. Available from:
http://steinhardtapps.es.its.nyu.edu/create/courses/3311/reading/10-
guba_lincoln_94.pdf
59. Scotland J. Exploring the philosophical underpinnings of research: Relating
ontology and epistemology to the methodology and methods of the scientific,
interpretive, and critical research paradigms. English Lang Teach. 2012;5(9):9–16.
60. Hall PJ, Foster JW, Yount KM, Jennings BM. Keeping it together and falling
apart: Women’s dynamic experience of birth. Midwifery [Internet]. 2018;58(July
2017):130–6. Available from: https://doi.org/10.1016/j.midw.2017.12.006
61. Qualitative Research in Implementation Science (QUALRIS). Qualitative Methods
In Implementation Science. 2018; Available from:
https://cancercontrol.cancer.gov/IS/docs/NCI-DCCPS-ImplementationScience-
WhitePaper.pdf
62. Lincoln YS, Guba EG. Establishing Trustworthiness. Naturalistic Inquiry.
Newbury Park, CA: Sage Publications; 1985. 289–331 p.
63. O’Brien B, Harris I, Beckman T, Reed D, Cook D. Standards for reporting
qualitative research: a synthesis of recommendations. Acad Med.
2014;89(9):1245–51.
64. Pink S, Morgan J. Short-term ethnography: Intense routes to knowing. Symb
Interact. 2013;36(3):351–61.
65. Palinkas LA, Zatzick D. Rapid Assessment Procedure Informed Clinical
Ethnography (RAPICE) in Pragmatic Clinical Trials of Mental Health Services
Implementation: Methods and Applied Case Study. Adm Policy Ment Heal Ment
Heal Serv Res [Internet]. 2019;46(2):255–70. Available from:
http://dx.doi.org/10.1007/s10488-018-0909-3
66. Blase K, Fixsen DL. Core intervention components: identifying and
operationalizing. ASPE Res Br. 2013;(February):21.
67. Michie S, West R, Sheals K, Godinho CA. Evaluating the effectiveness of
behavior change techniques in health-related behavior: A scoping review of
methods used. Transl Behav Med. 2018;8(2):212–24.
152
68. Damschroder LJ. Clarity out of chaos: Use of theory in implementation research.
Psychiatry Res. 2019;283(June 2019).
69. Oliveira M De, Teresa M, Sibio D, Solla L, Moretto B, Eliana M, et al. Molecular
and Cellular Endocrinology Irisin modulates genes associated with severe
coronavirus disease (COVID- 19) outcome in human subcutaneous adipocytes cell
culture. Mol Cell Endocrinol [Internet]. 2020;515(June):110917. Available from:
https://doi.org/10.1016/j.mce.2020.110917
70. van Manen M. But is it phenomenology? Qual Health Res. 2017;27(6):775–9.
71. Barry C, Han H, McGinty B. Trust in Science and COVID-19 [Internet].
Baltimore, MD; 2020. Available from: https://www.jhsph.edu/covid-
19/articles/trust-in-science-and-covid-19.html
72. Kofman A. Bruno Latour, the Post-Truth Philosopher, Mounts a Defense of
Science. The New York Times Magazine [Internet]. 2018 Oct; Available from:
https://www.nytimes.com/2018/10/25/magazine/bruno-latour-post-truth-
philosopher-science.html
73. Hagger MS, Smith SR, Keech JJ, Moyers SA, Hamilton K. Predicting Social
Distancing Intention and Behavior During the COVID-19 Pandemic: An
Integrated Social Cognition Model. Ann Behav Med. 2020;713–27.
74. Funk C, Hefferon M, Kennedy B, Johnson C. Trust and Mistrust in Americans’
Views of Scientific Experts [Internet]. Washington, DC; 2019. Available from:
https://www.pewresearch.org/science/2019/08/02/trust-and-mistrust-in-americans-
views-of-scientific-experts/
75. Agley J. Assessing changes in US public trust in science amid the COVID-19
pandemic. Public Health [Internet]. 2020;183:122–5. Available from:
https://doi.org/10.1016/j.puhe.2020.05.004
76. Funk C. Key findings about Americans’ confidence in science and their views on
scientists’ role in society [Internet]. Washington, DC; 2020. Available from:
https://www.pewresearch.org/fact-tank/2020/02/12/key-findings-about-americans-
confidence-in-science-and-their-views-on-scientists-role-in-society/
77. Steketee A, Archibald T, Harden S. Adjust your own oxygen mask before helping
those around you: An autoethnography of participatory research. Implement Sci.
2020;15(70).
78. Siega-Riz AM, Viswanathan M, Moos MK, Deierlein A, Mumford S, Knaack J, et
al. A systematic review of outcomes of maternal weight gain according to the
Institute of Medicine recommendations: birthweight, fetal growth, and postpartum
weight retention. Am J Obstet Gynecol [Internet]. 2009;201(4):339.e1-339.e14.
Available from: http://dx.doi.org/10.1016/j.ajog.2009.07.002
79. Starling AP, Brinton JT, Glueck DH, Shapiro AL, Harrod CS, Lynch AM, et al.
Associations of maternal BMI and gestational weight gain with neonatal adiposity
in the Healthy Start study. Am J Clin Nutr. 2015;101(2):302–9.
80. Walsh JM, McGowan CA, Mahony RM, Foley ME, McAuliffe FM. Obstetric and
metabolic implications of excessive gestational weight gain in pregnancy. Obesity.
2014;22(7):1594–600.
81. Green CA, Duan N, Gibbons RD, Hoagwood KE, Palinkas LA, Albert G, et al.
Approaches to Mixed Methods Dissemination and Implementation Research:
Methods, Strengths, Caveats, and Opportunities. Adm Policy Ment Heal.
153
2015;42(5):508–23.
82. Palinkas L, Aarons G, Horwitz S, Chamberlain P, Hurlburt M, Landsverk J. Mixed
Method Designs in Implementation Research. Adm Policy Ment Heal Ment Heal
Serv Res. 2011;38:44–53.
83. Denzin NK. Moments, mixed methods, and paradigm dialogs. Qual Inq.
2010;16(6):419–27.
84. Przyrembel M, Singer T. Experiencing meditation – Evidence for di ff erential e ff
ects of three contemplative mental practices in micro-phenomenological
interviews. Conscious Cogn [Internet]. 62:82–101. Available from:
https://doi.org/10.1016/j.concog.2018.04.004
85. Bauer D, Krege J, Lane N, Leary E, Libanati C, Miller P, et al. National Bone
Health Alliance Bone Turnover Marker Project: Current practices and the need for
US harmonization, standardization, and common reference ranges. Osteoporos Int.
2012;23(10):2425–33.
86. Bohannon RW. Grip strength: An indispensable biomarker for older adults. Clin
Interv Aging. 2019;14:1681–91.
87. Brownson RC, Royer C, Ewing R, McBride TD. Researchers and policymakers:
Travelers in parallel universes. Am J Prev Med. 2006;30(2):164–72.
88. Chapman S. Reflections on a 38-year career in public health advocacy: 10 pieces
of advice to early career researchers and advocates. Public Heal Res Pract.
2015;25(2):1–5.
89. Sforzo GA, Kaye MP, Todorova I, Harenberg S, Costello K, Cobus-Kuo L, et al.
Compendium of the health and wellness coaching literature. Am J Lifestyle Med.
2018;12(6):1–12.
90. Sforzo GA, Kaye MP, Harenberg S, Costello K, Cobus-Kuo L, Rauff E, et al.
Compendium of Health and Wellness Coaching: 2019 Addendum. Am J Lifestyle
Med. 2020;14(2):155–68.
91. Roche N, Bourbeau J. Health coaching: Another component of personalized
medicine for patients with chronic obstructive pulmonary disease. Am J Respir
Crit Care Med. 2016;194(6):647–9.
92. van Rinsum C, Gerards S, Rutten G, Philippens N, Janssen E, Winkens B, et al.
The coaching on lifestyle (CooL) intervention for overweight and obesity: A
longitudinal study into participants’ lifestyle changes. Int J Environ Res Public
Health. 2018;15(4).
93. Aderze ́N-Carlsson A, Lundholm U, Kohn M, Westerdahl E. Medical yoga:
Another way of being in the world--A phenomenologicalstudy from the
perspective of persons suffering from stress-related symptoms. Int J Qual Stud
Health Well-being. 2014;1:1–10.
94. Rhodes AM. Claiming peaceful embodiment through yoga in the aftermath of
trauma. Complement Ther Clin Pract [Internet]. 2015;21(4):247–56. Available
from: http://dx.doi.org/10.1016/j.ctcp.2015.09.004
95. Sullivan MB, Erb M, Schmalzl L, Moonaz S, Taylor JN, Porges SW, et al. Yoga
Therapy and Polyvagal Theory: The Convergence of Traditional Wisdom and
Contemporary Neuroscience for Self-Regulation and Resilience. Hypothesis and
Theory. 2018;12(February):1–15.
96. Davidson RJ, Dahl CJ. Outstanding Challenges in Scientific Research on

154
Mindfulness and Meditation. Perspect Psychol Sci. 2018;13(1):62–5.
97. Kabat-Zinn J. Mindfulness-Based Interventions in Contex: Past, Present, and
Future. Am Psychol Asssociation. 2003;10(2):144–56.
98. Lacouture A, Breton E, Guichard A, Ridde V. The concept of mechanism from a
realist approach: A scoping review to facilitate its operationalization in public
health program evaluation. Implement Sci. 2015;10(1):1–10.
99. Pawson R, Greenhalgh T, Harvey G, Walshe K. Realist review - A new method of
systematic review designed for complex policy interventions. J Heal Serv Res
Policy. 2005;10(SUPPL. 1):21–34.
100. MacDonald M, Pauly B, Wong G, Schick-Makaroff K, van Roode T, Strosher
HW, et al. Supporting successful implementation of public health interventions:
Protocol for a realist synthesis. Syst Rev [Internet]. 2016;5(1):1–11. Available
from: http://dx.doi.org/10.1186/s13643-016-0229-1
101. Glasgow R. What does it mean to be pragmatic? Pragmatic methods, measures,
and models to facilitate research translation. Heal Educ Behav. 2013;40(3):257–
65.
102. Thorpe KE, Zwarenstein M, Oxman AD, Treweek S, Furberg CD, Altman DG, et
al. A pragmatic-explanatory continuum indicator summary (PRECIS): a tool to
help trial designers. J Clin Epidemiol [Internet]. 2009;62(5):464–75. Available
from: http://dx.doi.org/10.1016/j.jclinepi.2008.12.011
103. Howard D, Giovanelli M. Einstein’s Philosophy of Science [Internet]. Fall 2019.
Zalta EN, editor. Stanford Encyclopedia of Philosophy. 2019. Available from:
https://plato.stanford.edu/entries/einstein-philscience/
104. Einstein A. Ernst Mach. In: Stachel J, editor. The Collected Papers of Albert
Einstein. Princeton, University: Princeton University Press;
105. Bourdeau M. Auguste Comte. Stanford Encycl Philos [Internet]. 2020;Winter 202.
Available from: https://plato.stanford.edu/archives/win2020/entries/comte/
106. Rabin BA, Brownson RS. Developing the Terminology for Dissemination and
Implementation Research. In: Brownson RC, Colditz GA, Proctor EK, editors.
Dissemination and Implementation Research in Health. New York, New York:
Oxford University Press; 2012. p. 23–51.
107. Beltz AM, Wright AGC, Sprague BN, Molenaar PCM. Bridging the Nomothetic
and Idiographic Approaches to the Analysis of Clinical Data. Assessment.
2016;23(4):447–58.
108. Choi B, Pak A. Multidisciplinarity, interdisciplinarity, and transdisciplinarity in
health research, services, education and policy: 1. Definitions, objectives, and
evidence of effectiveness. Clin Investig Med. 2006;29(6):351–64.
109. Philosophy [Internet]. Merriam-Webster. 2020 [cited 2020 Sep 29]. Available
from: https://www.merriam-webster.com/dictionary/philosophy
110. Vannini P. Situatedness. In: Given LM, editor. The SAGE Encyclopedia of
Qualitative Research Methods [Internet]. Thousand Oaks, CA: SAGE
Publications, Inc.; 2012. p. 815–6. Available from:
https://methods.sagepub.com/base/download/ReferenceEntry/sage-encyc-
qualitative-research-methods/n424.xml
111. DeWitt R. Worldviews: An Introduction to the History and Philosophy of Science.
Third. Hoboken, New Jersey: Wiley; 2018.
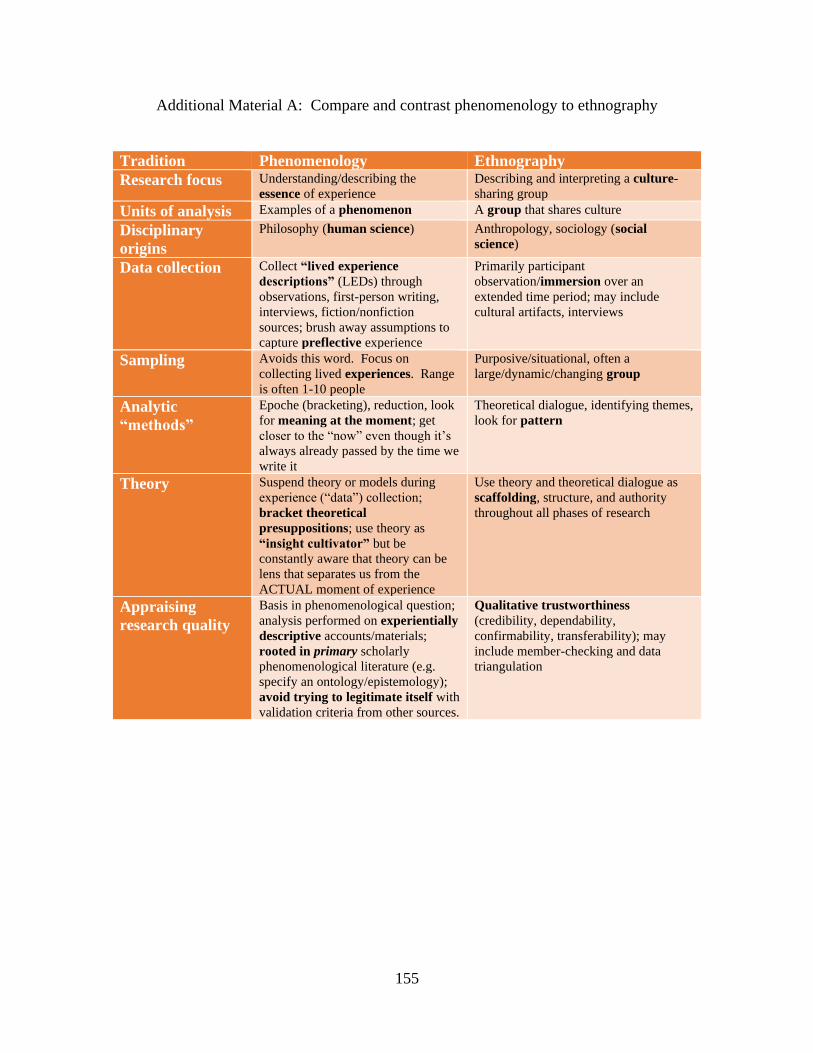
155
Additional Material A: Compare and contrast phenomenology to ethnography
Tradition Phenomenology Ethnography
Research focus Understanding/describing the
essence of experience
Describing and interpreting a culture-
sharing group
Units of analysis Examples of a phenomenon A group that shares culture
Disciplinary
origins
Philosophy (human science) Anthropology, sociology (social
science)
Data collection Collect “lived experience
descriptions” (LEDs) through
observations, first-person writing,
interviews, fiction/nonfiction
sources; brush away assumptions to
capture preflective experience
Primarily participant
observation/immersion over an
extended time period; may include
cultural artifacts, interviews
Sampling Avoids this word. Focus on
collecting lived experiences. Range
is often 1-10 people
Purposive/situational, often a
large/dynamic/changing group
Analytic
“methods”
Epoche (bracketing), reduction, look
for meaning at the moment; get
closer to the “now” even though it’s
always already passed by the time we
write it
Theoretical dialogue, identifying themes,
look for pattern
Theory Suspend theory or models during
experience (“data”) collection;
bracket theoretical
presuppositions; use theory as
“insight cultivator” but be
constantly aware that theory can be
lens that separates us from the
ACTUAL moment of experience
Use theory and theoretical dialogue as
scaffolding, structure, and authority
throughout all phases of research
Appraising
research quality
Basis in phenomenological question;
analysis performed on experientially
descriptive accounts/materials;
rooted in primary scholarly
phenomenological literature (e.g.
specify an ontology/epistemology);
avoid trying to legitimate itself with
validation criteria from other sources.
Qualitative trustworthiness
(credibility, dependability,
confirmability, transferability); may
include member-checking and data
triangulation
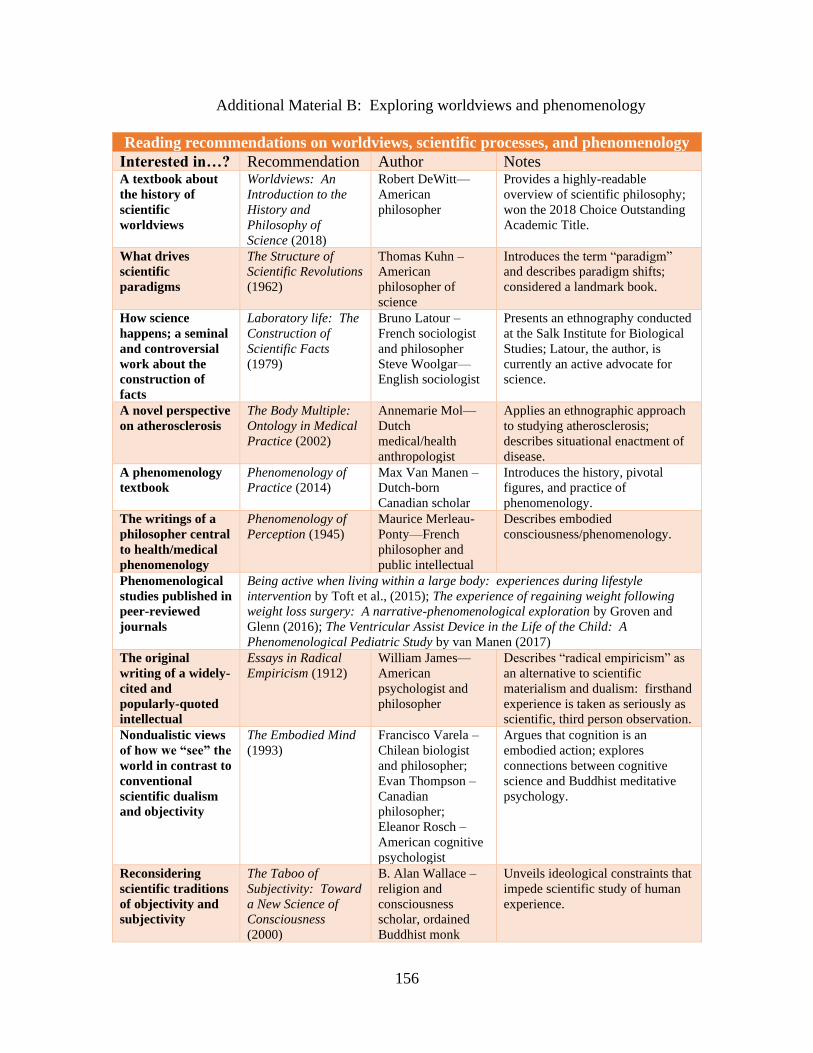
156
Additional Material B: Exploring worldviews and phenomenology
Reading recommendations on worldviews, scientific processes, and phenomenology
Interested in…? Recommendation Author Notes A textbook about
the history of
scientific
worldviews
Worldviews: An
Introduction to the
History and
Philosophy of
Science (2018)
Robert DeWitt—
American
philosopher
Provides a highly-readable
overview of scientific philosophy;
won the 2018 Choice Outstanding
Academic Title.
What drives
scientific
paradigms
The Structure of
Scientific Revolutions
(1962)
Thomas Kuhn –
American
philosopher of
science
Introduces the term “paradigm”
and describes paradigm shifts;
considered a landmark book.
How science
happens; a seminal
and controversial
work about the
construction of
facts
Laboratory life: The
Construction of
Scientific Facts
(1979)
Bruno Latour –
French sociologist
and philosopher
Steve Woolgar—
English sociologist
Presents an ethnography conducted
at the Salk Institute for Biological
Studies; Latour, the author, is
currently an active advocate for
science.
A novel perspective
on atherosclerosis
The Body Multiple:
Ontology in Medical
Practice (2002)
Annemarie Mol—
Dutch
medical/health
anthropologist
Applies an ethnographic approach
to studying atherosclerosis;
describes situational enactment of
disease.
A phenomenology
textbook
Phenomenology of
Practice (2014)
Max Van Manen –
Dutch-born
Canadian scholar
Introduces the history, pivotal
figures, and practice of
phenomenology.
The writings of a
philosopher central
to health/medical
phenomenology
Phenomenology of
Perception (1945)
Maurice Merleau-
Ponty—French
philosopher and
public intellectual
Describes embodied
consciousness/phenomenology.
Phenomenological
studies published in
peer-reviewed
journals
Being active when living within a large body: experiences during lifestyle
intervention by Toft et al., (2015); The experience of regaining weight following
weight loss surgery: A narrative-phenomenological exploration by Groven and
Glenn (2016); The Ventricular Assist Device in the Life of the Child: A
Phenomenological Pediatric Study by van Manen (2017)
The original
writing of a widely-
cited and
popularly-quoted
intellectual
Essays in Radical
Empiricism (1912)
William James—
American
psychologist and
philosopher
Describes “radical empiricism” as
an alternative to scientific
materialism and dualism: firsthand
experience is taken as seriously as
scientific, third person observation.
Nondualistic views
of how we “see” the
world in contrast to
conventional
scientific dualism
and objectivity
The Embodied Mind
(1993)
Francisco Varela –
Chilean biologist
and philosopher;
Evan Thompson –
Canadian
philosopher;
Eleanor Rosch –
American cognitive
psychologist
Argues that cognition is an
embodied action; explores
connections between cognitive
science and Buddhist meditative
psychology.
Reconsidering
scientific traditions
of objectivity and
subjectivity
The Taboo of
Subjectivity: Toward
a New Science of
Consciousness
(2000)
B. Alan Wallace –
religion and
consciousness
scholar, ordained
Buddhist monk
Unveils ideological constraints that
impede scientific study of human
experience.

157
Additional Material C: Syllabus for Graduate Course
Course Title: Interdisciplinary Approaches to Health
3C, 3H
2 days per week/90 minute class
Instruction Type: Lecture
Catalogue Description
Integration of methods and evidence from different fields. Examination of blind spots
within worldviews and paradigms that drive health research. Generation of
interdisciplinary approaches to wicked problems, inclusivity and diversity, and
communicating science. Emphasis on translating critical analysis and originary thinking
to actionable strategies. Intensive practice of oral, written, and graphic communication
skills.
Learning Objectives
After this course, students will be able to:
1. Analyze scientific paradigms and foundational worldviews to uncover blind spots in
research, design, conduct, and translation.
2. Integrate multiple modes of inquiry for studying wicked problems along the
translational research spectrum.
3. Develop actionable, novel strategies for addressing systemic issues such as inclusive
research, public trust of science, and the peer-reviewed publication process.
4. Design and tailor dissemination of interdisciplinary evidence, arguments, or research
to target audiences through specific channels.
Justification
This course provides an arena for generating rigorous, novel, and ethical interdisciplinary
health research. To meet the demand for health research that translates to real-world
benefit, students need training that cultivates critical reflection and incisive
communication. This course integrates content-driven didactic lectures with practical
exercises that cultivate oral, written, and graphic communication skills. The purpose is to
connect originary thinking with actionable strategies for health research, practice, and/or
policy. This course challenges students to explore beneath the surface of topics and
methodologies in human nutrition, foods, and exercise.
This course is appropriate for graduate students in any HNFE track or working along any
aspect of the translational science spectrum. This course will support students interested
in addressing wicked problems and systemic issues such as diversity and inclusion,
public trust of science, and the peer-reviewed publication process. Overall, this course
cultivates deep, ethical thinking for long-term personal development, team science, and
real-world impact.
This course is taught at the graduate level because students need a foundation of HNFE
content on which to apply interdisciplinary approaches. Without a firm grasp of HNFE

158
methodologies, students will not be able to explore beneath the surface of current
paradigms. This course will help graduate students leverage their field-specific expertise
and experiences into critical reflection and sophisticated communication.
Overall, this course challenges students to slow down, look again, and generate
awareness of how health research is conducted, disseminated, and translated. In our
digital world with multifaceted global challenges, it has never been more important to
nurture intentionality among our future health scientists and leaders.
Topics Syllabus
Course Outline
Week Topic Day 1 Day 2
1 A. Introduction
B. Philosophical framework – what is
ontology, epistemology, axiology,
methodology, praxis?
C. What is science? When did it start?
D. What is evidence? What is knowledge?
A. Introduction
B. Science jukebox
C. Syllabus review
D. Lecture:
Philosophical
framework
HW due: Nothing
A. Lecture: Science,
evidence, knowledge
B. Writing practice #1
HW due: Quote
w/proper citation for
research anthology
2 A. What is interdisciplinary?
B. Who “made up” disciplines?
C. What disciplines relate to human
nutrition, foods, and exercise?
A. Reading quiz #1
B. Lecture: History of
disciplines
HW due:
Interdisciplinary
readings for quiz
A. Writing practice #1
continued: courage to
receive feedback;
specificity and
sensitivity in giving
feedback
B. Scavenger hunt –
interdisciplinary
approaches related to
nutrition, foods, and
exercise
HW due:
Editing/reworking last
week’s writing practice
3 A. What is a worldview?
B. What is a paradigm?
C. Does philosophy matter in HNFE and
A. Reading quiz #2
B. Lecture:
Worldviews and
A. Speaking practice
#1: Fillers
B. Forum #1: Does
Topic Percent of Course
Topic 1: Interdisciplinarity 20%
Topic 2: Translational science 20%
Subtopic 1: Wicked problems (10%)
Subtopic 2: Systemic challenges (10%)
Topic 3: Philosophy, worldviews, paradigm 20%
Topic 5: History of Exercise is Medicine 10%
Topic 6: Being and Doing in Science 30%
Subtopic 1: Communication skills (15%)
Subtopic 2: Reflection (7.5%)
Subtopic 3: Thriving strategies (7.5%)
Total 100%

159
translational science?
paradigms
C. Forum explanation
HW due: Worldview
and paradigm readings
for quiz
philosophy matter in
HNFE and translation
science? Based on your
answer, what should we
do?
HW due: Prepare for
forum #2
4 A. What is a wicked problem?
B. What is the connection between wicked
problems and the translational science
spectrum?
A. Reading quiz #3:
flipped quiz
B. Lecture: Wicked
problems and
translational research
HW due: Wicked
problems and
translational science
readings for quiz
A. Speaking practice
#2: Incisive questions,
active listening.
B. Forum #2: How
does current scientific or
translational paradigm
affect our approach to
wicked problems? Do
any of your individual
worldviews differ from
prevalent paradigm?
Based on your answer,
what should you do?
HW due: Prepare for
Forum #2
5 A. Part 1 - How do scholars or researchers
in various disciplines approach a specific
topic in HNFE?
B. Part 1 – How does interdisciplinary
research look in practice?
[For Part 2 in Week 11, another panel will
come to class.]
A. Interdisciplinary
Panel (guest speakers)
HW due: Reading(s)
assigned from each
speaker. Submit two
questions for each
speaker.
A. Writing practice #3:
When less is more.
B. Graphic practice #1:
Mapping
interdisciplinary
approaches to a wicked
problem [including
concept mapping,
tracking sources]
HW due: Written
response to panel
discussion.
6 A. Skills intensive week: Graphics and
abstracts
B. Review: Philosophy, worldview,
paradigm, wicked problem, translational
science, interdisciplinary
A. Lecture: Review +
history of “human
subjects research”
HW due: Draft of
interdisciplinary map
(instructor will provide
feedback)
A. Writing practice #4:
Creative warm-ups +
abstract writing
B. Graphic practice #1
(continued): Edit
interdisciplinary map
HW due: Draft of paper
about interdisciplinary
map (instructor will
provide feedback)
7 How can scientists thrive amidst the
demands of research, particularly
interdisciplinary research?
A. Lecture: Evidence-
based and evidence-
informed strategies for
A. Forum #3:
Presenting
interdisciplinary map: 4
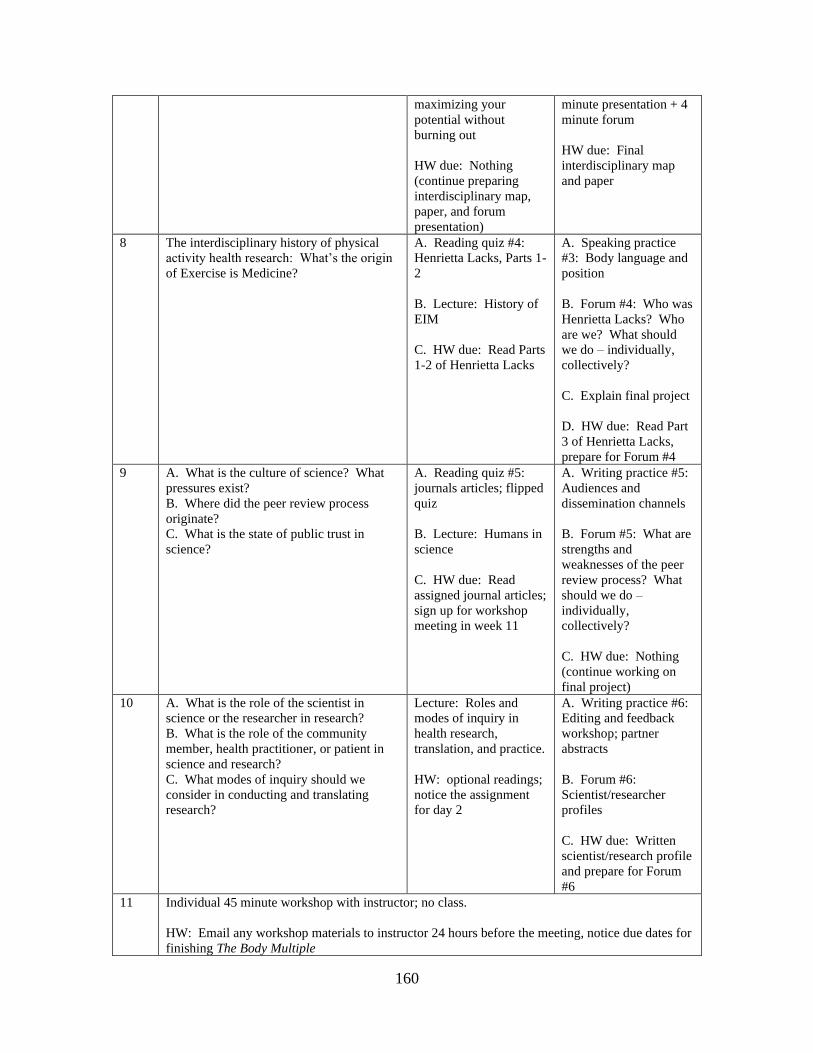
160
maximizing your
potential without
burning out
HW due: Nothing
(continue preparing
interdisciplinary map,
paper, and forum
presentation)
minute presentation + 4
minute forum
HW due: Final
interdisciplinary map
and paper
8 The interdisciplinary history of physical
activity health research: What’s the origin
of Exercise is Medicine?
A. Reading quiz #4:
Henrietta Lacks, Parts 1-
2
B. Lecture: History of
EIM
C. HW due: Read Parts
1-2 of Henrietta Lacks
A. Speaking practice
#3: Body language and
position
B. Forum #4: Who was
Henrietta Lacks? Who
are we? What should
we do – individually,
collectively?
C. Explain final project
D. HW due: Read Part
3 of Henrietta Lacks,
prepare for Forum #4
9 A. What is the culture of science? What
pressures exist?
B. Where did the peer review process
originate?
C. What is the state of public trust in
science?
A. Reading quiz #5:
journals articles; flipped
quiz
B. Lecture: Humans in
science
C. HW due: Read
assigned journal articles;
sign up for workshop
meeting in week 11
A. Writing practice #5:
Audiences and
dissemination channels
B. Forum #5: What are
strengths and
weaknesses of the peer
review process? What
should we do –
individually,
collectively?
C. HW due: Nothing
(continue working on
final project)
10 A. What is the role of the scientist in
science or the researcher in research?
B. What is the role of the community
member, health practitioner, or patient in
science and research?
C. What modes of inquiry should we
consider in conducting and translating
research?
Lecture: Roles and
modes of inquiry in
health research,
translation, and practice.
HW: optional readings;
notice the assignment
for day 2
A. Writing practice #6:
Editing and feedback
workshop; partner
abstracts
B. Forum #6:
Scientist/researcher
profiles
C. HW due: Written
scientist/research profile
and prepare for Forum
#6
11 Individual 45 minute workshop with instructor; no class.
HW: Email any workshop materials to instructor 24 hours before the meeting, notice due dates for
finishing The Body Multiple
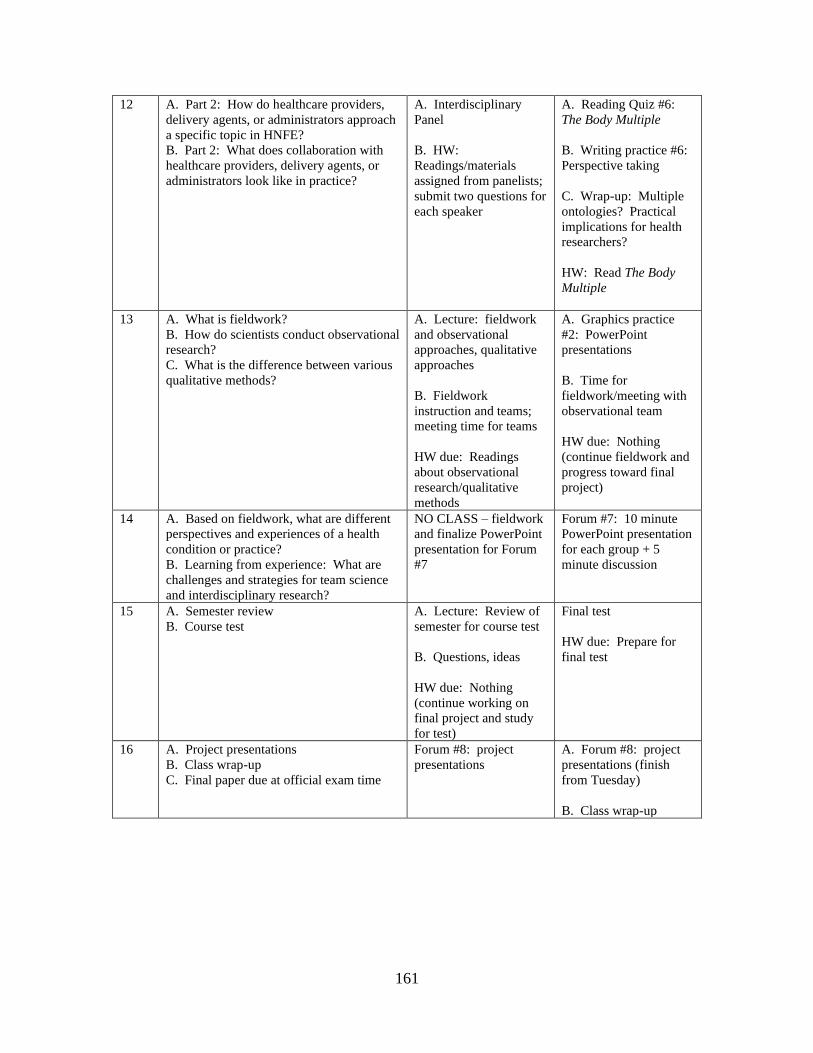
161
12 A. Part 2: How do healthcare providers,
delivery agents, or administrators approach
a specific topic in HNFE?
B. Part 2: What does collaboration with
healthcare providers, delivery agents, or
administrators look like in practice?
A. Interdisciplinary
Panel
B. HW:
Readings/materials
assigned from panelists;
submit two questions for
each speaker
A. Reading Quiz #6:
The Body Multiple
B. Writing practice #6:
Perspective taking
C. Wrap-up: Multiple
ontologies? Practical
implications for health
researchers?
HW: Read The Body
Multiple
13 A. What is fieldwork?
B. How do scientists conduct observational
research?
C. What is the difference between various
qualitative methods?
A. Lecture: fieldwork
and observational
approaches, qualitative
approaches
B. Fieldwork
instruction and teams;
meeting time for teams
HW due: Readings
about observational
research/qualitative
methods
A. Graphics practice
#2: PowerPoint
presentations
B. Time for
fieldwork/meeting with
observational team
HW due: Nothing
(continue fieldwork and
progress toward final
project)
14 A. Based on fieldwork, what are different
perspectives and experiences of a health
condition or practice?
B. Learning from experience: What are
challenges and strategies for team science
and interdisciplinary research?
NO CLASS – fieldwork
and finalize PowerPoint
presentation for Forum
#7
Forum #7: 10 minute
PowerPoint presentation
for each group + 5
minute discussion
15 A. Semester review
B. Course test
A. Lecture: Review of
semester for course test
B. Questions, ideas
HW due: Nothing
(continue working on
final project and study
for test)
Final test
HW due: Prepare for
final test
16 A. Project presentations
B. Class wrap-up
C. Final paper due at official exam time
Forum #8: project
presentations
A. Forum #8: project
presentations (finish
from Tuesday)
B. Class wrap-up

162
Assignments and Grades
Assignment Details
Reading quizzes (6 total): These in-class, closed-book quizzes provide feedback on
students’ comprehension of the assigned reading. The quizzes include a variety of
question formats including multiple choice, fill-in-the-blank, and short answer.
Forum (8 total): Forum refers to in-class discussions to exchange and generate ideas
about critical topics. Students will practice skills from the previous class communication
exercises as they connect philosophical ideas with practical strategies. Students are
expected to connect their arguments with readings and class materials. The forum is an
opportunity for creativity and incisiveness; it is not intended for diatribe. The instructor
will provide a rubric before each forum. The eight forum presentations are as follows:
(1) discussion of philosophy’s relevance to health researchers, (2) discussion of
paradigm/worldview effects on research translation and wicked problems, (3) four minute
individual presentation of interdisciplinary map graphic, (4) discussion of Henrietta
Lacks, (5) debate about peer-reviewed publications, (6) four minute individual
presentation of scientist profile, (7) ten minute PowerPoint group presentation of
fieldwork, (8) ten minute individual presentation of final paper.
Interdisciplinary map and paper: Students will explore interdisciplinary approaches
and research on a health-related topic of their choice. The paper must include at least
three disciplines, including a specific area or track of science within HNFE. The paper
must include a graphic depicting the interdisciplinary model (“map”) they create. The
instructor will provide the rubric before the assignment. In addition, the instructor will
provide feedback on the draft of the paper in the week before the final paper is due.
Final paper: The final paper is an opportunity for students to think deeply about a topic
that matters to them. The paper is also a chance to explore disciplines, paradigms, and
worldviews outside of HNFE. Students are expected to apply an interdisciplinary lens to
their topic and demonstrate the written and graphic communication skills practiced in
class. Students may choose one of the following formats:
(1) Manuscript following the author guidelines for Perspectives submitted to
Science, Analytic Essays submitted to the American Journal of Public Health, or another
manuscript for a specific peer reviewed publication as agreed upon by the student and
instructor.
Assigning Points ~Percentage
Reading quizzes (6 quizzes*10 pts each) 60 16.67%
Forum (8 presentations*20 pts each) 160 44.44%
Interdisciplinary map and paper 20 5.56%
Final test 60 16.67&
Final project paper 60 16.67%
Extra credit (4 options*10 pts each) [40] [11.11%]
Total 360 100%
163
(2) Grant application (i.e., aims, approach) following the guidelines in a specific
Request for Application (RFA) as agreed upon by the student and instructor.
The final grade will reflect rigor of critical analysis and/or creativity; appropriate and
justifiable integration of interdisciplinary approaches; demonstration of communication
skills practiced throughout the course; and adherence to proper citation and referencing.
Final test: The final test will be on the last day of class. Like the reading quizzes, the
final test will include a variety of question formats. The test covers lectures and readings
from the entire semester. Students will have 90 minutes to complete the test.
Extra credit: Students have the option to submit four extra credit assignments as
described in class. They can submit the assignments at any point until the due date of the
final paper. Each submitted extra credit activity is worth up to 10 points.
Individual workshop: This non-graded coaching-style meeting is intended to support
students within the class and beyond. The meeting provides a one-on-one opportunity to
discuss the final paper, as well as other ideas and topics related to the class.
Required Texts
DeWitt, R. (2018). Worldviews: An Introduction to the History and Philosophy of
Science. Third Edition. Wiley: Hoboken, NJ.
Mol, A. (2002). The Body Multiple: Ontology in Medical Practice. Duke University
Press: Durham, NC.
Skloot, R. (2010). The Immortal Life of Henrietta Lacks. Random House, Inc.: New
York, NY.
164
Conclusion
This dissertation reveals three interconnected pathways of methods, paradigms,
and practices for addressing the overarching questions of what is missing within D&I
approaches and what can we do about it? Currently missing are methods that capture
emergent, cascading implementation processes including researchers’ situatedness within
those processes; paradigms that leverage subjectivity in uncontrolled settings to
investigate personal experience and meaning; and practices that optimize researchers’
capacities for productivity. Based on research presented in this dissertation, what we can
do about these missing elements is embrace process, person, and presence in all three
pathways:
Methods
• Disseminate the RE-AIM Framework to health educators by publishing research
findings in journals of professional organizations (e.g., Lamaze International’s
Journal of Perinatal Education).
• Conduct autoethnography analyzed through restorying as an interdisciplinary
approach to assess implementation contexts, processes, and outcomes.
• Maintain user-friendly logs, such as the FUEL session logs, which can be used as
components of behavioral interventions and pragmatic data collection tools for
capturing implementation.
• Report at least one quotation (e.g., the raw words) from as many participants as
feasible to leverage the potential of qualitative methods for (a) improving
inclusivity, (b) humanizing findings, and (c) staying as close as possible to the
first-person, lived experience of individuals.
Paradigms
• Challenge beliefs about what constitutes evidence for core components of
interventions.
• Conduct pragmatic pilot studies of behavioral interventions as an efficient and
stakeholder-salient alternative to the traditional efficacy-effectiveness pipeline.
• Generate flexible participatory research protocols that accommodate stakeholders’
emergent ideas and needs.
• Balance the hegemony of mechanism over meaning in the translational science
spectrum by developing an “evidence map” for research questions of meaning as
a complement to the existing “evidence hierarchy” for research questions of
mechanism.
165
Practices
• Establish authentic and consistent presence in the community through informal
walk-and-talks or coffee meetings that engage stakeholders beyond formal
partnerships or models.
• Engage in one-on-one coaching that cultivates a “caravan of resources” to thrive
within the chaos of D&I Science and daily life.
• Explore micro-practices, such as email blackout periods and 5-4-3-2-1 sensory
breaks, to decrease hindrance stressors, enhance recovery, and nurture a sense of
purpose.
Embracing the personal aspect of these pathways could have policy implications. For
example, redesigning the NIH’s translational spectrum to include phenomenology (see
Figure 3 on page 136) could affect funding opportunities and training initiatives. In
terms of funding, the Patient Centered Outcome Research Institute (PCORI) (1) includes
importance of research results, patient-centeredness, and stakeholder engagement as three
of its six merit review criteria. These criteria are a promising indication of prioritizing
what matters most to people in real-world settings. However, PCORI’s review criterium
of technical merit includes designs consistent with principles and findings from
implementation science. This criterium limits the possibilities of innovation by
restricting “novelty” to methods that fit current paradigm. Therefore, I propose that
PCORI add language in the technical merit criterium, such as designs consistent with
principles and findings from implementation science or well-justified, innovative designs
that advance methodological approaches to patient-centered research. Overall, the
PCORI technical merit criterium demonstrates how funding policies embody the
“scientific paradigms with blind spots and conflicts” theme from the autoethnography.
The autoethnography also demonstrated the importance of philosophical
underpinnings. This importance could influence undergraduate or graduate degree
requirements. As part of training in research methods, graduate departments could adopt
166
a policy that requires doctoral students to complete at least one course in philosophy.
After all, PhD stands for doctor of philosophy. In addition, training for D&I
competencies and capacities could be expanded to include leadership, soft skills, and self-
care as illuminated in the Mom Expo implementation results, ethnographic-theoretical
dialogue about work stress, and FUEL effectiveness results.
Overall, policy can be a result and driver of methods, paradigms, and practices that
improve research translation.
Final Note
At the intersection of these pathways is phenomenology, the study of human
meaning. Phenomenology functions as a method, paradigm, and practice that is
particularly relevant to D&I Science because, as this dissertation demonstrates, people
are the research-practice bridge. However, in the pressure to demonstrate scientific
objectivity, human presence is often diminished. We forget that it takes rowers to move
the boat. In rowing, every finish line is a starting point, a place from which to see further
down the river. May the end of this dissertation be that sort of place.
Reference
1. Patient-Centered Outcomes Research Institute. Merit Review Criteria for
Implementation PFA [Internet]. 2020. [cited 2020 Dec 5]. Available from:
https://www.pcori.org/funding-opportunities/merit-review/merit-review-criteria/merit-
review-criteria-implementation-pfa

167
Appendix A: IRB Exemption Letter

168
Appendix B: Prenatal Yoga Flyer
169
Appendix C: Mom Expo Flyer

170
Appendix D: Mom Expo Invitation/Postcard
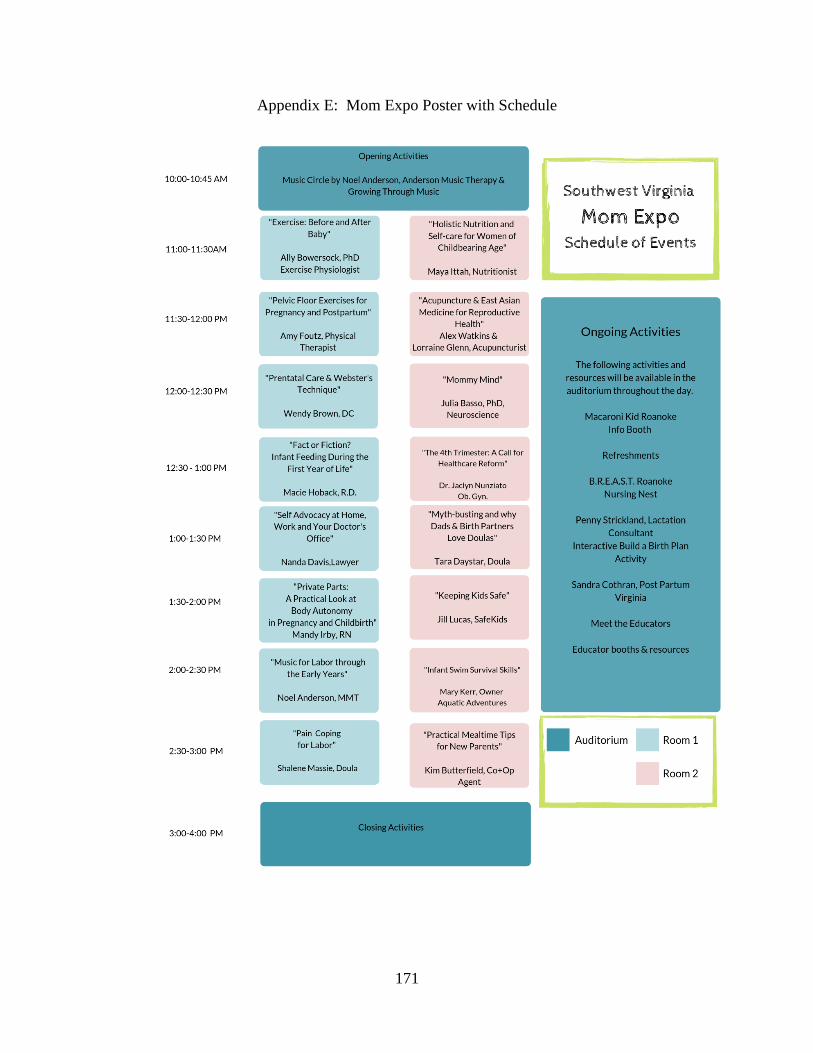
171
Appendix E: Mom Expo Poster with Schedule
172
Appendix F: Mom Expo Educator Survey
Name (optional): ___________________________________________________________
Please rate the following aspects of the Mom Expo by placing a check in the appropriate box.
Excellent Above Average Average Below Average Poor
Attendance
Opportunity for
education
Opportunity for
empowerment
Opportunity for
connection
Planning/organization
leading up to the event
Management on the
day of the event
Facility
Location
Publicity
Atmosphere/energy
Overall experience
In your opinion, how successful was Mom Expo at connecting women to resources/support they
need? Circle one:
Very Successful Successful Fairly Successful A Little Successful Not At All Successful
How likely are you to participate in Mom Expo next year? Circle one:
Very Likely Likely Moderate Unlikely Definitely not
In your opinion, what was the best part of Mom Expo (i.e. the strengths)?
In your opinion, what needs improvement (i.e. the weaknesses)?
Any other comments, suggestions, or ideas? Feel free to use the back of this sheet.

173
Appendix G: Mom Expo Attendee Comment Card
Thank you for attending the Mom Expo! This event was brought to you by the Virginia Tech Physical Activity Research and Community Implementation Lab, Macaroni Kid Roanoke, and the South County Library. We would love your feedback on whether Mom Expo connected you to helpful resources, information, and support. From 1 (horrible) to 10 (fantastic), how was your experience today? Please circle one:
1 2 3 4 5 6 7 8 9 10
Please use the back of this card to provide comments about your
experience. We welcome your feedback!
174
Appendix H: Mom Expo Observational Log
175
Appendix I: IRB Approval Letter
176
Appendix J: Standards for Reporting Qualitative Research
Submitted with the autoethnography manuscript* to Implementation Science
*page/line numbers refer to the accepted manuscript Title and abstract Page/line no(s).
Title - Concise description of the nature and topic of the study Identifying the study as
qualitative or indicating the approach (e.g., ethnography, grounded theory) or data collection
methods (e.g., interview, focus group) is recommended Pg 1/Line 8
Abstract - Summary of key elements of the study using the abstract format of the intended
publication; typically includes background, purpose, methods, results, and conclusions Pg 2/Line 21
Introduction
Problem formulation - Description and significance of the problem/phenomenon studied;
review of relevant theory and empirical work; problem statement Pg 5/Line 96
Purpose or research question - Purpose of the study and specific objectives or questions Pg 5/Line 100
Methods
Qualitative approach and research paradigm - Qualitative approach (e.g., ethnography,
grounded theory, case study, phenomenology, narrative research) and guiding theory if
appropriate; identifying the research paradigm (e.g., postpositivist, constructivist/
interpretivist) is also recommended; rationale** Pg 5/Line 102
Researcher characteristics and reflexivity - Researchers’ characteristics that may
influence the research, including personal attributes, qualifications/experience, relationship
with participants, assumptions, and/or presuppositions; potential or actual interaction
between researchers’ characteristics and the research questions, approach, methods, results,
and/or transferability
Pg 6/Line 129, Pg
8/Line 169
Context - Setting/site and salient contextual factors; rationale**
Pg 6/Line 130,
Figures 2-3
Sampling strategy - How and why research participants, documents, or events were
selected; criteria for deciding when no further sampling was necessary (e.g., sampling
saturation); rationale**
Pg 7/Line 144
(hiring the GRA to
conduct
autoethnography)
Ethical issues pertaining to human subjects - Documentation of approval by an
appropriate ethics review board and participant consent, or explanation for lack thereof;
other confidentiality and data security issues Pg 8/Line 168
177
Data collection methods - Types of data collected; details of data collection procedures
including (as appropriate) start and stop dates of data collection and analysis, iterative
process, triangulation of sources/methods, and modification of procedures in response to
evolving study findings; rationale** Pg 7/Line 147
Data collection instruments and technologies - Description of instruments (e.g., interview
guides, questionnaires) and devices (e.g., audio recorders) used for data collection; if/how
the instrument(s) changed over the course of the study Pg 7/Line 147
Units of study - Number and relevant characteristics of participants, documents, or events
included in the study; level of participation (could be reported in results) Figures 2 and 3
Data processing - Methods for processing data prior to and during analysis, including
transcription, data entry, data management and security, verification of data integrity, data
coding, and anonymization/de-identification of excerpts
Pg 7/ Line 155, Pg
8/Line 189
Data analysis - Process by which inferences, themes, etc., were identified and developed,
including the researchers involved in data analysis; usually references a specific paradigm or
approach; rationale**
Pg 7/Line 157, Pg
8/Line 163
Techniques to enhance trustworthiness - Techniques to enhance trustworthiness and
credibility of data analysis (e.g., member checking, audit trail, triangulation); rationale** Table 2
Results/findings
Synthesis and interpretation - Main findings (e.g., interpretations, inferences, and
themes); might include development of a theory or model, or integration with prior research
or theory Figures 1, 2, 4
Links to empirical data - Evidence (e.g., quotes, field notes, text excerpts, photographs) to
substantiate analytic findings
Table 1,
Throughout
results/discussion
starting at Pg
9/Line 199
Discussion
Integration with prior work, implications, transferability, and contribution(s) to the
field - Short summary of main findings; explanation of how findings and conclusions
connect to, support, elaborate on, or challenge conclusions of earlier scholarship; discussion
of scope of application/generalizability; identification of unique contribution(s) to
scholarship in a discipline or field
Figure 1, Figure 2,
Table 2, Table 3;
implications start at
Pg 18/Line 394
Limitations - Trustworthiness and limitations of findings
Table 2; Pg 5/Line
115, Pg 15/Line
342
178
Other
Conflicts of interest - Potential sources of influence or perceived influence on study
conduct and conclusions; how these were managed Table 2
Funding - Sources of funding and other support; role of funders in data collection,
interpretation, and reporting Pg 42/Line 484
Reference:
O'Brien BC, Harris IB, Beckman TJ, Reed DA, Cook DA. Standards for reporting qualitative research: a
synthesis of recommendations. Academic Medicine, Vol. 89, No. 9 / Sept 2014
DOI: 10.1097/ACM.0000000000000388

179
Appendix K: IRB Approval Letter
180
Appendix L: FUEL Program Development
Method: Designing the coaching program
The first aim of this pilot study was to design a coaching program for
Dissemination and Implementation (D&I) researchers. Based on recent
recommendations for developing complex behavioral interventions (1), investigators
designed the coaching program by integrating evidence from a variety of sources. These
sources included meta-analyses, randomized controlled trials, observational studies, and
interdisciplinary theories as outlined and cited in Table 1 below. In addition, sources for
developing the coaching program included stakeholder engagement (2) and practice-
based human judgment based on the principal investigator’s (PI)(A.S.) previous career as
an NCAA Division I head swimming and diving coach. Investigators decided to call the
program FUEL based on four dimensions of focus, unplug, exercise, and love. The name
FUEL also represents the intent that coaching sessions themselves would energize
participants, restoring their capacity for productivity.
After determining the name, investigators engaged stakeholders through
pragmatic “premortem” brainstorming meetings (3,4) to identify potential invention
weaknesses and implementation barriers. The PI conducted the meetings through in-
person conversations, Zoom videoconferencing, and telephone during the fall of 2019.
The meetings consisted of a convenience sample of stakeholders (n=7) who worked in
multiple domains (e.g., research and community), considered themselves D&I
researchers, or had academic and practical coaching expertise. Brainstorming meetings
were informal and flexible to facilitate natural discussion. The PI summarized the
181
meetings in written notes. Investigators A.S. and S.H. independently reviewed the
meeting summaries and applied insights to refine the FUEL program.
Periodization
One unique aspect of the program is periodization. Periodization is a sport
science concept that refers to structuring training into specific phases with varying
training dosages and goals (5). By intentionally progressing the dosage and skill,
periodization optimizes long-term growth (6,7). Within this approach to sports training,
the coach integrates observation, tacit knowledge (8), and each participant’s feedback to
customize and adapt workloads. Recovery from work bouts is a crucial component of
periodization (5–7). Periodization aligns with D&I principles of pragmatic processes (9)
such as adaptation, context, feasibility, and outcomes that are relevant to stakeholders.
However, as far as investigators know, periodization has not been applied to designing or
implementing behavioral interventions.
Self-Regulation Model of Coaching
In addition to periodization, the FUEL program is based on the Self-Regulation
through Coaching Model (10,11). This model includes (a) setting a goal, (b) developing
an action plan, (c) working through a cycle of action, (d) monitoring through self-
reflection, (e) evaluating through insight, and (f) changing what is not working well or
doing more of what works. In this model, the role of the coach is to facilitate solution-
focused self-reflection and insight within an action-oriented process intended to build a
foundation for long-term growth beyond the coaching sessions (10,11).

182
Table 1: Empirical and practical foundations of FUEL
F = Focus U = Unplug E = Exercise L = Love
Dimension Description
Focus: Work in
efficient and meaningful
ways.
Unplug: Recover from
work; take a break from
job-related tasks and
thoughts.
Exercise: Incorporate
movement in positive
ways.
Love: Generate
goodwill to self, others,
and situations
Broad Theoretical and Empirical Bases
Deliberate practice
(uninterrupted,
intentional, sustained
effort) to maximize
growth and performance
(12,13); flow or optimal
psychological
experience (14)
Burnout (15,16),
allostastis, chronic
stress, and theories of
work-related stress
(17–20); ego depletion
(21,22); Effort
Recovery Model and
recovery (23,24); work-
related rumination and
perseverative cognition
(25,26)
Physical activity is
associated with
reduced risk of
mortality and chronic
disease (27,28);
exercise-induced
cognitive benefits (29–
31); Physical Activty
Guidelines for
Americans (32);
upward spiral theory
of lifestyle change (33)
Belongingness as
human need (34);
relatedness as basic
psychological need in
the Self Determination
Theory (35)
Examples: Evidence-based strategies
Intentional email use
(36), periodized work
cycles with alternating
blocks of intense effort
and recovery (5,6); goal
setting and
achievement
orientation that
emphasizes growth and
process instead of
outcomes and
interpersonal
comparisons (37–39)
Sleep (40–42); slow
diaphragmatic
breathing (43–46);
nature micro-breaks
(47); meditation and
mindfulness practices
(48–51)
High-intensity
incidental physical
activity (52); variety of
physical activity (53);
using individually-
selected music during
physical activity (54)
Metta (lovingkindness)
meditation (55); acts of
kindness (56,57);
journaling (58);
counting blessings (59);
writing letters of
gratitude (60)
Examples: Practice-based strategies
Protecting deep work
(61); Richard Feynman
saying “no” (62)
Albert Einstein’s violin
(“combinatory play”)
(63); Bill Gates’
meditation (64).
St. Louis Stanley Cup
and “Gloria” (65);
belief effect (66)
Ariana Huffington’s
three things and Oprah
Winfrey’s electronic
gratitude journal (67)
References
1. Larsen KR, Michie S, Hekler EB, Gibson B, Spruijt-Metz D, Ahern D, et al.
Behavior change interventions: the potential of ontologies for advancing science
and practice. J Behav Med. 2017;40(1):6–22.
2. Powell BJ, Waltz TJ, Chinman MJ, Damschroder LJ, Smith JL, Matthieu MM, et
al. A refined compilation of implementation strategies: Results from the Expert
Recommendations for Implementing Change (ERIC) project. Implement Sci.
2015;10(1):1–14.
3. Gilmartin H, Lawrence E, Leonard C, McCreight M, Kelley L, Lippmann B, et al.
Brainwriting Premortem: A Novel Focus Group Method to Engage Stakeholders
and Identify Preimplementation Barriers. J Nurs Care Qual. 2019;34(2):94–100.
183
4. O’Haire C, McPheeters M, Nakamoto E, LaBrant L, Most C, Lee K, et al.
Engaging Stakeholders To Identify and Prioritize Future Research Needs. Methods
Futur Res Needs Rep No 4 [Internet]. 2011;(11-EHC044-EF). Available from:
www.effectivehealthcare.ahrq.gov/reports/final.cfm
5. Bompa TO. Periodization. Fourth Edi. Champaign, IL: Human Kinetics; 1999.
6. Wathen D, Baechle TR, Earle RW. Periodization. In: Baechle TR, Earle RW,
editors. Essentials of Strength Training and Conditioning. Third Edit. Champaign,
IL; 2008. p. 507–22.
7. Mujika I. Tapering and Peaking for Optimal Performance. Champaign, IL: Human
Kinetics; 2009.
8. Nash C, Collins D. Tacit knowledge in expert coaching: Science or art? Quest.
2006;58(4):465–77.
9. Glasgow R. What does it mean to be pragmatic? Pragmatic methods, measures,
and models to facilitate research translation. Heal Educ Behav. 2013;40(3):257–
65.
10. Grant AM. The impact of life coaching on goal attainment, metacognition and
mental health. Soc Behav Pers. 2003;31(3):253–64.
11. Grant AM, Curtayne L, Burton G. Executive coaching enhances goal attainment,
resilience and workplace well-being: A randomised controlled study. J Posit
Psychol. 2009;4(5):396–407.
12. Ericsson KA, Krampe RT, Tesch-Römer C. The role of deliberate practice in the
acquisition of expert performance. Psychol Rev. 2005;100(3):363–406.
13. Ericsson KA. Summing Up Hours of Any Type of Practice Versus Identifying
Optimal Practice Activities: Commentary on Macnamara, Moreau, & Hambrick
(2016). Perspect Psychol Sci. 2016;11(3):351–4.
14. Csikszentmihalyi M. Flow: The psychology of optimal experience. New York,
New York: Harper Perennial; 1990.
15. Maslach C, Jackson S, Leiter M. Maslach Burnout Inventory Model. 3rd editio.
Palo Alto, CA: Consulting Psychologists Press; 1996.
16. Kristensen TS, Borritz M, Villadsen E, Christensen KB. The Copenhagen Burnout
Inventory: A new tool for the assessment of burnout. Work Stress.
2005;19(3):192–207.
17. McEwen B, Stellar E. Stress and the Individual: Mechanisms Leading to Disease.
JAMA Intern Med. 1993;153(18):2085–92.
18. McEwen BS. Allostasis and the epigenetics of brain and body health over the life
course: The brain on stress. JAMA Psychiatry. 2017;74(6):551–2.
19. Bartlett L, Martin A, Neil AL, Memish K, Otahal P, Kilpatrick M, et al.
Supplemental Material for A Systematic Review and Meta-Analysis of Workplace
Mindfulness Training Randomized Controlled Trials. J Occup Health Psychol.
2019;24(1):108–26.
20. Dewe P, O’Driscoll M, Cooper C. Theories of Psychological Stress at Work. In:
Gatchel R, Schultz I, editors. Handbook of Occupational Health and Wellness.
New York: Spring Science + Business Media; 2012.
21. Baumeister RF, Tice DM, Vohs KD. The Strength Model of Self-Regulation:
Conclusions From the Second Decade of Willpower Research. Perspect Psychol
Sci. 2018;13(2):141–5.
184
22. Baumeister R, Bratslavsky E, Muraven M, Tice D. Ego Depletion: Is the Active
Self a Limited Resource? J Pers Soc Psychol. 1998;74(5):1252–65.
23. Zijlstra FRH, Cropley M, Rydstedt LW. From recovery to regulation: An attempt
to reconceptualize “recovery from work.” Stress Heal. 2014;30(3):244–52.
24. Meijman TF, Mulder G. Psychological Aspects of Workload. In: Drenth PJ,
Theirry H, J de WC, editors. Work Psychology. 2nd Editio. East Sussex; 1998. p.
5–28.
25. Cropley M, Zijlstra FRH, Querstret D, Beck S. Is work-related rumination
associated with deficits in executive functioning? Front Psychol. 2016;7(SEP):1–8.
26. Ottaviani C, Thayer JF, Verkuil B, Lonigro A, Medea B, Couyoumdjian A, et al.
Physiological concomitants of perseverative cognition: A systematic review and
meta-analysis. Psychol Bull. 2016;142(3):231–59.
27. Oja P, Kelly P, Pedisic Z, Titze S, Bauman A, Foster C, et al. Associations of
specific types of sports and exercise with all-cause and cardiovascular-disease
mortality: a cohort study of 80 306 British adults. Br J Sports Med.
2017;51(10):812–7.
28. Arem H, Moore SC, Patel A, Hartge P, Berrington De Gonzalez A, Visvanathan
K, et al. Leisure time physical activity and mortality: A detailed pooled analysis of
the dose-response relationship. JAMA Intern Med. 2015;175(6):959–67.
29. Erickson J, Leckie Ri, Weinstein A. Physical activity, fitness, and gray matter
volume. Neurobiol Aging. 2014;35(20–28):1720–7.
30. Raji CA, Merrill DA, Eyre H, Mallam S, Torosyan N, Erickson KI, et al.
Longitudinal Relationships between Caloric Expenditure and Gray Matter in the
Cardiovascular Health Study. J Alzheimer’s Dis. 2016;52(2):719–29.
31. Stimpson NJ, Davison G, Javadi AH. Joggin’ the Noggin: Towards a Physiological
Understanding of Exercise-Induced Cognitive Benefits. Neurosci Biobehav Rev.
2018;88(January):177–86.
32. US Department of Health and Human Services. 2018 Physical Activity Guidelines
Advisory Committee Scientific Report. To the Secretary of Health and Human
Service [Internet]. 2018. Available from: https://health.gov/paguidelines/second-
edition/report/pdf/PAG_Advisory_Committee_Report.pdf
33. Cappellen P, Rice E, Catalino L, Fredrickson B. Positive Affect Processes
Underlie Postive Health Behavior Change. 2019;33(1):77–97.
34. Maslow A. A theory of human motivation. Psychol Rev. 1943;50:370–96.
35. Ryan RM, Deci EL. Self Determination Theory and the Facilitation of Intrinsic
Motivation, Social Development, and Well-Being. Am Psychol. 2000;55(1):68–78.
36. Kushlev K, Dunn EW. Checking email less frequently reduces stress. Comput
Human Behav [Internet]. 2015;43:220–8. Available from:
http://dx.doi.org/10.1016/j.chb.2014.11.005
37. Cellar DF, Stuhlmacher AF, Young SK, Fisher DM, Adair CK, Haynes S, et al.
Trait Goal Orientation, Self-Regulation, and Performance: A Meta-Analysis. J Bus
Psychol. 2011;26(4):467–83.
38. Payne SC, Youngcourt SS, Beaubien JM. A meta-analytic examination of the goal
orientation nomological net. J Appl Psychol. 2007;92(1):128–50.
39. Utman CH. Performance effects of motivational state: A meta-analysis. Personal
Soc Psychol Rev. 1997;1(2):170–82.
185
40. Simon E Ben, Oren N, Sharon H, Kirschner A, Goldway N, Okon-Singer H, et al.
Losing neutrality: The neural basis of impaired emotional control without sleep. J
Neurosci. 2015;35(38):13194–205.
41. Barnes CM, Guarana CL, Kong DT. Too Tired to Inspire or Be Inspired: Sleep
Deprivation and Charismatic Leadership. J Appl Psychol. 2016;101(8):1191–9.
42. Ma N, Dinges DF, Basner M, Rao H. How Acute Total Sleep Loss Affects the
Attending Brain: A Meta-Analysis of Neuroimaging Studies. Sleep.
2015;38(2):233–40.
43. Gerritsen RJS, Band GPH. Breath of Life: The Respiratory Vagal Stimulation
Model of Contemplative Activity. Front Hum Neurosci [Internet].
2018;12(October):397. Available from:
https://www.frontiersin.org/article/10.3389/fnhum.2018.00397/full
44. Doll A, Hölzel BK, Mulej Bratec S, Boucard CC, Xie X, Wohlschläger AM, et al.
Mindful attention to breath regulates emotions via increased amygdala-prefrontal
cortex connectivity. Neuroimage [Internet]. 2016;134:305–13. Available from:
http://dx.doi.org/10.1016/j.neuroimage.2016.03.041
45. Zaccaro A, Piarulli A, Laurino M, Garbella E, Menicucci D, Neri B, et al. How
Breath-Control Can Change Your Life: A Systematic Review on Psycho-
Physiological Correlates of Slow Breathing. Front Hum Neurosci [Internet].
2018;12(September):1–16. Available from:
https://www.frontiersin.org/article/10.3389/fnhum.2018.00353/full
46. Ma X, Yue ZQ, Gong ZQ, Zhang H, Duan NY, Shi YT, et al. The effect of
diaphragmatic breathing on attention, negative affect and stress in healthy adults.
Front Psychol. 2017;8(JUN):1–12.
47. Korpela K, De Bloom J, Sianoja M, Pasanen T, Kinnunen U. Nature at home and
at work: Naturally good? Links between window views, indoor plants, outdoor
activities and employee well-being over one year. Landsc Urban Plan [Internet].
2017;160:38–47. Available from:
http://dx.doi.org/10.1016/j.landurbplan.2016.12.005
48. Boccia M, Piccardi L, Guariglia P. The Meditative Mind: A Comprehensive Meta-
Analysis of MRI Studies. Biomed Res Int. 2015;2015:1–11.
49. Davidson RJ, Dahl CJ. Outstanding Challenges in Scientific Research on
Mindfulness and Meditation. Perspect Psychol Sci. 2018;13(1):62–5.
50. Fox KCR, Nijeboer S, Dixon ML, Floman JL, Ellamil M, Rumak SP, et al. Is
meditation associated with altered brain structure? A systematic review and meta-
analysis of morphometric neuroimaging in meditation practitioners. Neurosci
Biobehav Rev [Internet]. 2014;43:48–73. Available from:
http://dx.doi.org/10.1016/j.neubiorev.2014.03.016
51. Berkovich-ohana A, Wilf M, Kahana R, Arieli A, Malach R. Repetitive speech
elicits widespread deactivation in the human cortex : the “ Mantra ” effect ?
2015;346:1–13.
52. Stamatakis E, Johnson NA, Powell L, Hamer M, Rangul V, Holtermann A. Short
and sporadic bouts in the 2018 US physical activity guidelines: Is high-intensity
incidental physical activity the new HIIT? Br J Sports Med. 2019;2018–20.
53. Sylvester BD, Standage M, McEwan D, Wolf SA, Lubans DR, Eather N, et al.
Variety support and exercise adherence behavior: experimental and mediating

186
effects. J Behav Med. 2016;39(2):214–24.
54. Ballmann CG, Maynard DJ, Lafoon ZN, Marshall MR, Williams TD, Rogers RR.
Effects of Listening to Preferred versus Non-Preferred Music on Repeated
Wingate Anaerobic Test Performance. Sports. 2019;7(8):185.
55. Kok BE, Coffey KA, Cohn MA, Catalino LI, Vacharkulksemsuk T, Algoe SB, et
al. How Positive Emotions Build Physical Health: Perceived Positive Social
Connections Account for the Upward Spiral Between Positive Emotions and Vagal
Tone. Psychol Sci. 2013;24(7):1123–32.
56. Rowland L, Curry O. A Range of Kindness Activities Boost Happiness. J Soc
Psychol. 2019;159(340–343).
57. Curry OS, Rowland LA, Van Lissa CJ, Zlotowitz S, McAlaney J, Whitehouse H.
Happy to help? A systematic review and meta-analysis of the effects of performing
acts of kindness on the well-being of the actor. J Exp Soc Psychol [Internet].
2018;76(March):320–9. Available from: https://doi.org/10.1016/j.jesp.2018.02.014
58. Beck AR, Verticchio H. Effectiveness of a method for teaching self-compassion to
communication sciences and disorders graduate students. Am J Speech-Language
Pathol. 2018;27(1):192–206.
59. Emmons RA, McCullough ME. Counting Blessings Versus Burdens: An
Experimental Investigation of Gratitude and Subjective Well-Being in Daily Life.
J Pers Soc Psychol. 2003;84(2):377–89.
60. Toepfer SM, Cichy K, Peters P. Letters of Gratitude: Further Evidence for Author
Benefits. J Happiness Stud. 2012;13(1):187–201.
61. Newport C. Deep Work. New York, New York: Grand Central Publishing; 2016.
62. Feynman RP. The Pleasure of Finding Things Out: The Best Short Works.
Robbins J, editor. Helix Books; 1999. 288 p.
63. Isaacson W. Benjamin Franklin: An American Life. New York, New York: Simon
& Schuster; 2017.
64. Gates B. Why I’m into meditation [Internet]. gatesnotes. 2018. Available from:
https://www.gatesnotes.com/Books/The-Headspace-Guide-to-Meditation-and-
Mindfulness
65. Pinkert C. Gloria! The story behind the Blues new (old) postgame victory song.
NHL News [Internet]. 2019; Available from:
https://www.nhl.com/blues/news/gloria-the-story-behind-the-blues-new-old-
postgame-victory-song/c-304750776
66. Hutchinson A. Endure. New York, New York: Harper Collins; 2018.
67. Mejia Z. How Arianna Huffington, Tony Robbins and Oprah Winfrey use
gratitude as a strategy for success. CNBC [Internet]. 2018; Available from:
https://www.cnbc.com/2018/02/16/how-arianna-huffington-tony-robbins-and-
oprah-use-gratitude-to-succeed.html
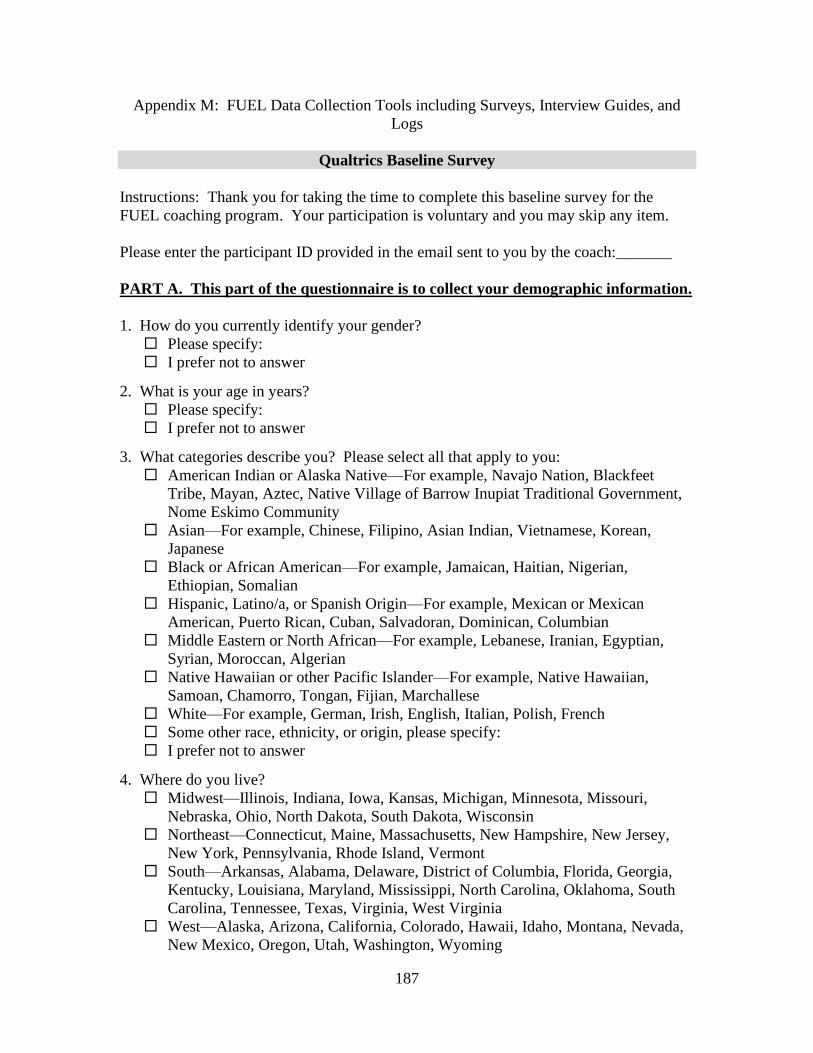
187
Appendix M: FUEL Data Collection Tools including Surveys, Interview Guides, and
Logs
Qualtrics Baseline Survey
Instructions: Thank you for taking the time to complete this baseline survey for the
FUEL coaching program. Your participation is voluntary and you may skip any item.
Please enter the participant ID provided in the email sent to you by the coach:_______
PART A. This part of the questionnaire is to collect your demographic information.
1. How do you currently identify your gender?
Please specify:
I prefer not to answer
2. What is your age in years?
Please specify:
I prefer not to answer
3. What categories describe you? Please select all that apply to you:
American Indian or Alaska Native—For example, Navajo Nation, Blackfeet
Tribe, Mayan, Aztec, Native Village of Barrow Inupiat Traditional Government,
Nome Eskimo Community
Asian—For example, Chinese, Filipino, Asian Indian, Vietnamese, Korean,
Japanese
Black or African American—For example, Jamaican, Haitian, Nigerian,
Ethiopian, Somalian
Hispanic, Latino/a, or Spanish Origin—For example, Mexican or Mexican
American, Puerto Rican, Cuban, Salvadoran, Dominican, Columbian
Middle Eastern or North African—For example, Lebanese, Iranian, Egyptian,
Syrian, Moroccan, Algerian
Native Hawaiian or other Pacific Islander—For example, Native Hawaiian,
Samoan, Chamorro, Tongan, Fijian, Marchallese
White—For example, German, Irish, English, Italian, Polish, French
Some other race, ethnicity, or origin, please specify:
I prefer not to answer
4. Where do you live?
Midwest—Illinois, Indiana, Iowa, Kansas, Michigan, Minnesota, Missouri,
Nebraska, Ohio, North Dakota, South Dakota, Wisconsin
Northeast—Connecticut, Maine, Massachusetts, New Hampshire, New Jersey,
New York, Pennsylvania, Rhode Island, Vermont
South—Arkansas, Alabama, Delaware, District of Columbia, Florida, Georgia,
Kentucky, Louisiana, Maryland, Mississippi, North Carolina, Oklahoma, South
Carolina, Tennessee, Texas, Virginia, West Virginia
West—Alaska, Arizona, California, Colorado, Hawaii, Idaho, Montana, Nevada,
New Mexico, Oregon, Utah, Washington, Wyoming
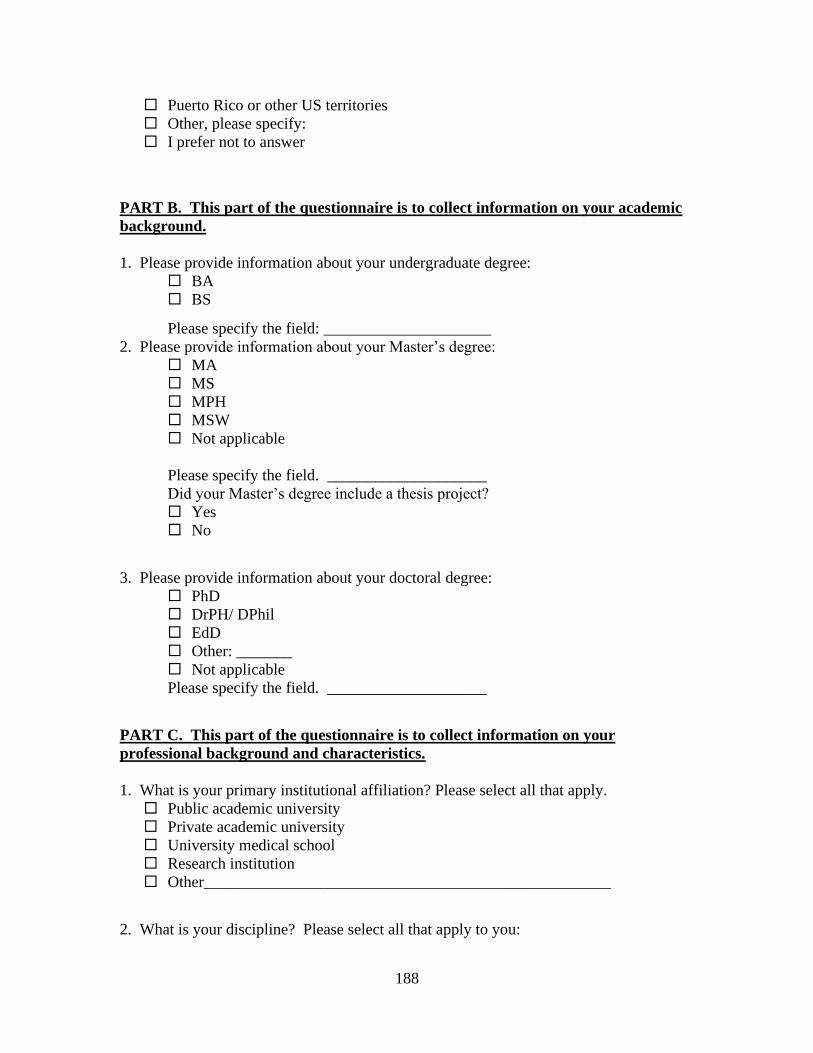
188
Puerto Rico or other US territories
Other, please specify:
I prefer not to answer
PART B. This part of the questionnaire is to collect information on your academic
background.
1. Please provide information about your undergraduate degree:
BA
BS
Please specify the field: _____________________
2. Please provide information about your Master’s degree:
MA
MS
MPH
MSW
Not applicable
Please specify the field. ____________________
Did your Master’s degree include a thesis project?
Yes
No
3. Please provide information about your doctoral degree:
PhD
DrPH/ DPhil
EdD
Other: _______
Not applicable
Please specify the field. ____________________
PART C. This part of the questionnaire is to collect information on your
professional background and characteristics.
1. What is your primary institutional affiliation? Please select all that apply.
Public academic university
Private academic university
University medical school
Research institution
Other___________________________________________________
2. What is your discipline? Please select all that apply to you:

189
Allied health (i.e. non-nurse, non-physician health care providers). For
example—physical therapists, dieticians, health care administrators.
Public health
Social science
Basic science
Clinical
Other, please specify:
I prefer not to answer
3. What is your position? Please select all that apply to you:
Research scientist
Assistant professor
Associate professor
Professor
Other, please specify:
I prefer not to answer
4. If applicable, what is your full-time appointment? Please select all that apply to you:
Not applicable, please skip to the next question.
Research, please indicate percentage of full-time appointment:
Teaching, please indicate percentage of full-time appointment:
Service, please indicate percentage of full-time appointment:
Administration, please indicate percentage of full-time appointment:
Other, please indicate percentage of full-time appointment:
5. Do you conduct participatory research (i.e. collaborate with community members,
clinicians, policy makers, and/or stakeholders who are not researchers)?
Yes
No
I don’t know
I prefer not to answer
6. On average, how many hours do you work in a typical week, including time at an
office, in the field, or working at home?
Please specify a total number of hours for the week:
I prefer not to answer
7. On average, what percentage of your work time in a typical week is spent on the
activities that mean the most to you compared to time spent on “hassles” or less-
meaningful responsibilities?
Please specify a percentage for the week:
I prefer not to answer
8. What is your current h-index?
Please specify: ____
I don’t know
I prefer not to answer
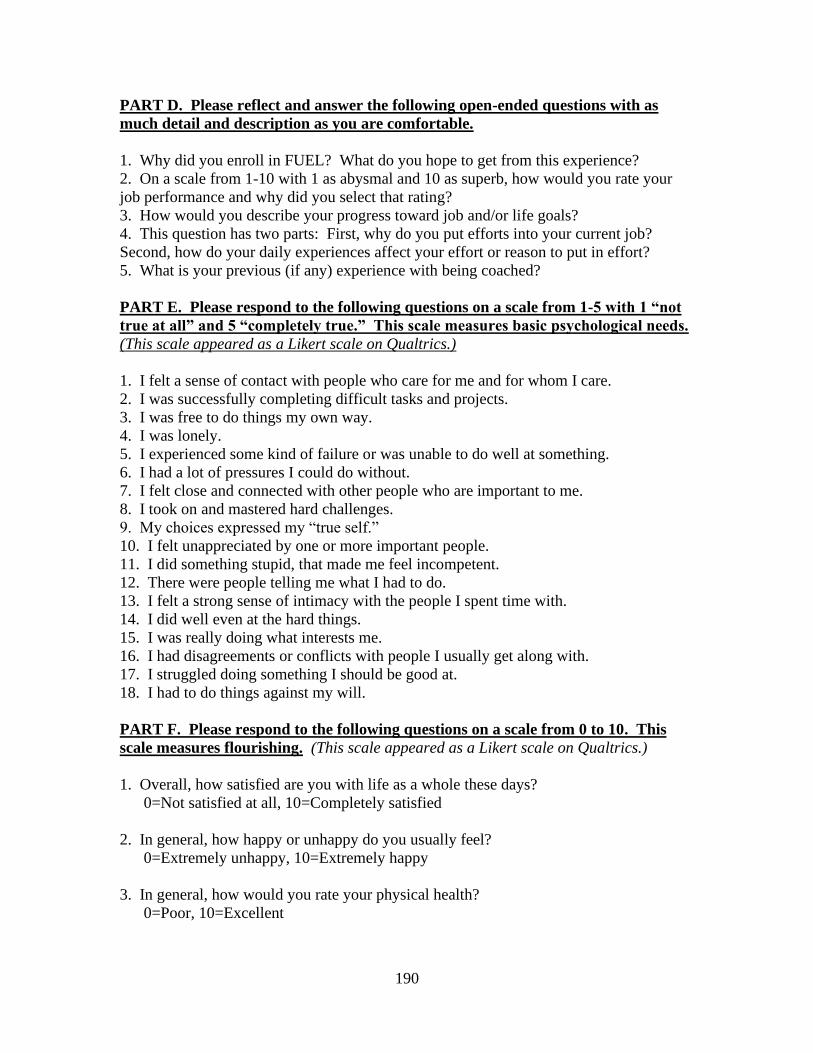
190
PART D. Please reflect and answer the following open-ended questions with as
much detail and description as you are comfortable.
1. Why did you enroll in FUEL? What do you hope to get from this experience?
2. On a scale from 1-10 with 1 as abysmal and 10 as superb, how would you rate your
job performance and why did you select that rating?
3. How would you describe your progress toward job and/or life goals?
4. This question has two parts: First, why do you put efforts into your current job?
Second, how do your daily experiences affect your effort or reason to put in effort?
5. What is your previous (if any) experience with being coached?
PART E. Please respond to the following questions on a scale from 1-5 with 1 “not
true at all” and 5 “completely true.” This scale measures basic psychological needs.
(This scale appeared as a Likert scale on Qualtrics.)
1. I felt a sense of contact with people who care for me and for whom I care.
2. I was successfully completing difficult tasks and projects.
3. I was free to do things my own way.
4. I was lonely.
5. I experienced some kind of failure or was unable to do well at something.
6. I had a lot of pressures I could do without.
7. I felt close and connected with other people who are important to me.
8. I took on and mastered hard challenges.
9. My choices expressed my “true self.”
10. I felt unappreciated by one or more important people.
11. I did something stupid, that made me feel incompetent.
12. There were people telling me what I had to do.
13. I felt a strong sense of intimacy with the people I spent time with.
14. I did well even at the hard things.
15. I was really doing what interests me.
16. I had disagreements or conflicts with people I usually get along with.
17. I struggled doing something I should be good at.
18. I had to do things against my will.
PART F. Please respond to the following questions on a scale from 0 to 10. This
scale measures flourishing. (This scale appeared as a Likert scale on Qualtrics.)
1. Overall, how satisfied are you with life as a whole these days?
0=Not satisfied at all, 10=Completely satisfied
2. In general, how happy or unhappy do you usually feel?
0=Extremely unhappy, 10=Extremely happy
3. In general, how would you rate your physical health?
0=Poor, 10=Excellent

191
4. How would you rate your overall mental health?
0=Poor, 10=Excellent
5. Overall, to what extent do you feel the things in your life are worthwhile?
0=Not at all worthwhile, 10=Completely worthwhile
6. I understand my purpose in life.
0=Strongly Disagree, 10=Strongly agree
7. I always act to promote good in all circumstances, even in difficult or challenging
situations.
0=Not true of me, 10=Completely true of me
8. I am always able to give up some happiness now for greater happiness later.
0=Not true of me, 10=Completely true of me
9. I am content with my friendships and relationships.
0=Strongly Disagree, 10=Strongly Agree
10. My relationships are as satisfying as I would want them to be.
0=Strongly Disagree, 10=Strongly Agree
PART G. The following question refers to your overall sleep quality for the
majority of the nights in the past 7 days only. Please think about the quality of your
sleep overall, such as how many hours of sleep you got, how easily you fell asleep,
how often you woke up during the night (except to go to the bathroom), how often
you woke up earlier than you had to in the morning, and how refreshing your sleep
was.
During the past 7 days, how would you rate your sleep quality overall?
PART H. During the past month, which statement best describes the kinds of
physical activity you usually did? Do not include the time you spent working at a
job. Please read all six statements before SELECTING ONE.
I did not do much physical activity. I mostly did things like watching television,
reading, playing cards, or playing computer games. Only occasionally, no more than
once or twice a month, did I do anything more active such as going for a walk or
playing tennis.

192
Once or twice a week, I did light activities such as going outdoors on the weekends
for an easy walk or maybe once or twice a week, I did chores around the house such
as sweeping floors or vacuuming.
About three times a week, I did moderate activities such as brisk walking, swimming,
or riding a bike for about 15–20 minutes each time. Or about once a week, I did
moderately difficult chores such as raking or mowing the lawn for about 45–60
minutes. Or about once a week, I played sports such as softball, basketball, or soccer
for about 45–60 minutes.
Almost daily, that is five or more times a week, I did moderate activities such as brisk
walking, swimming, or riding a bike for 30 minutes or more each time. Or about once
a week, I did moderately difficult chores or played sports for 2 hours or more.
About three times a week, I did vigorous activities such as running or riding hard on a
bike for 30 minutes or more each time.
Almost daily, that is five or more times a week, I did vigorous activities such as
running or riding hard on a bike for 30 minutes or more each time.
Qualtrics Post Program Survey
Instructions: Thank you for taking the time to complete this questionnaire for the FUEL
coaching program. Your participation is voluntary and you may skip any item.
Please enter the participant ID provided in the email sent to you by the coach:_______
PART A. This part of the questionnaire is to collect information on ways your
professional situation or characteristics may have changed over the FUEL program.
1. Has your job changed in the last month? For example, do you have a new position or
responsibilities?
Yes, please explain:
No.
2. On average, how many hours do you work in a typical week, including time at an
office, in the field, or working at home?
Please specify a total number of hours for the week:
I prefer not to answer
3. On average, what percentage of your work time in a typical week is spent on the
activities that mean the most to you compared to time spent on “hassles” or less-
meaningful responsibilities?
Please specify a percentage for the week:
I prefer not to answer

193
PART B. Please reflect and answer the following open-ended questions with as
much detail and description as you are comfortable.
1. What does FUEL mean to you?
2. What have you learned about yourself, life, or work in the last eight weeks during
FUEL?
3. What FUEL strategies or behaviors do you intend to use now that coaching has
ended?
4. On a scale from 1-10 with 1 as abysmal and 10 as superb, how would you rate your
job performance and why did you select that rating?
5. How would you describe your progress toward job-related and or life goals?
6. What specific benefits (if any) have you experienced during FUEL coaching?
7. What specific negative effects or outcomes (if any) have you experienced during
FUEL coaching?
8. What have been the most helpful aspects of FUEL?
9. Whas the coach effective? Why or why not?
10. Would you recommend FUEL coaching to other researchers? Why or why not?
11. How can we improve FUEL for other potential participants?
PART C. Please respond to the following questions on a scale from 1-5 with 1 “not
true at all” and 5 “completely true.” This scale measures basic psychological needs.
(This scale appeared as a Likert scale on Qualtrics.)
1. I felt a sense of contact with people who care for me and for whom I care.
2. I was successfully completing difficult tasks and projects.
3. I was free to do things my own way.
4. I was lonely.
5. I experienced some kind of failure or was unable to do well at something.
6. I had a lot of pressures I could do without.
7. I felt close and connected with other people who are important to me.
8. I took on and mastered hard challenges.
9. My choices expressed my “true self.”
10. I felt unappreciated by one or more important people.
11. I did something stupid, that made me feel incompetent.
12. There were people telling me what I had to do.
13. I felt a strong sense of intimacy with the people I spent time with.
14. I did well even at the hard things.
15. I was really doing what interests me.
16. I had disagreements or conflicts with people I usually get along with.
17. I struggled doing something I should be good at.
18. I had to do things against my will.
194
PART D. Please respond to the following questions on a scale from 0 to 10. This
scale measures flourishing. (This scale appeared as a Likert scale on Qualtrics.)
1. Overall, how satisfied are you with life as a whole these days?
0=Not satisfied at all, 10=Completely satisfied
2. In general, how happy or unhappy do you usually feel?
0=Extremely unhappy, 10=Extremely happy
3. In general, how would you rate your physical health?
0=Poor, 10=Excellent
4. How would you rate your overall mental health?
0=Poor, 10=Excellent
5. Overall, to what extent do you feel the things in your life are worthwhile?
0=Not at all worthwhile, 10=Completely worthwhile
6. I understand my purpose in life.
0=Strongly Disagree, 10=Strongly agree
7. I always act to promote good in all circumstances, even in difficult or challenging
situations.
0=Not true of me, 10=Completely true of me
8. I am always able to give up some happiness now for greater happiness later.
0=Not true of me, 10=Completely true of me
9. I am content with my friendships and relationships.
0=Strongly Disagree, 10=Strongly Agree
10. My relationships are as satisfying as I would want them to be.
0=Strongly Disagree, 10=Strongly Agree
PART E. The following question refers to your overall sleep quality for the
majority of the nights in the past 7 days only. Please think about the quality of your
sleep overall, such as how many hours of sleep you got, how easily you fell asleep,
how often you woke up during the night (except to go to the bathroom), how often
you woke up earlier than you had to in the morning, and how refreshing your sleep
was.
During the past 7 days, how would you rate your sleep quality overall?
195
PART F. During the past month, which statement best describes the kinds of
physical activity you usually did? Do not include the time you spent working at a
job. Please read all six statements before SELECTING ONE.
I did not do much physical activity. I mostly did things like watching television,
reading, playing cards, or playing computer games. Only occasionally, no more than
once or twice a month, did I do anything more active such as going for a walk or
playing tennis.
Once or twice a week, I did light activities such as going outdoors on the weekends
for an easy walk or maybe once or twice a week, I did chores around the house such
as sweeping floors or vacuuming.
About three times a week, I did moderate activities such as brisk walking, swimming,
or riding a bike for about 15–20 minutes each time. Or about once a week, I did
moderately difficult chores such as raking or mowing the lawn for about 45–60
minutes. Or about once a week, I played sports such as softball, basketball, or soccer
for about 45–60 minutes.
Almost daily, that is five or more times a week, I did moderate activities such as brisk
walking, swimming, or riding a bike for 30 minutes or more each time. Or about once
a week, I did moderately difficult chores or played sports for 2 hours or more.
About three times a week, I did vigorous activities such as running or riding hard on a
bike for 30 minutes or more each time.
Almost daily, that is five or more times a week, I did vigorous activities such as
running or riding hard on a bike for 30 minutes or more each time.
Qualtrics Three Month Post Program Survey
Instructions: Thank you for taking the time to complete this questionnaire for the FUEL
coaching program. Your participation is voluntary and you may skip any item.
Please enter the participant ID provided in the email sent to you by the coach:_______
PART A. This part of the questionnaire is to collect information on ways your
professional situation or characteristics may have changed over the FUEL program.
1. Has your job changed in the last month? For example, do you have a new position or
responsibilities?
Yes, please explain:
No.

196
2. On average, how many hours do you work in a typical week, including time at an
office, in the field, or working at home?
Please specify a total number of hours for the week:
I prefer not to answer
3. On average, what percentage of your work time in a typical week is spent on the
activities that mean the most to you compared to time spent on “hassles” or less-
meaningful responsibilities?
Please specify a percentage for the week:
I prefer not to answer
PART B. Please reflect and answer the following open-ended questions with as
much detail and description as you are comfortable.
1. What’s the first thing that comes to mind when you think back to the FUEL program?
2. Reflect on your feelings, thoughts, and behaviors since FUEL coaching ended. What
(if anything) has changed or emerged in the way you feel, think, or act in the last three
months?
3. What (if any) FUEL strategies, lessons, and/or behaviors do you use in your daily life?
How do you use them?
4. On a scale from 1-10 with 1 as abysmal and 10 as superb, how would you rate your
job performance and why did you select that rating?
5. How would you describe your progress toward job and/or life goals?
6. What specific positive and negative outcomes have you experienced from FUEL
coaching?
7. Would you enroll in FUEL again—why or why not?
PART C. Please respond to the following questions on a scale from 1-5 with 1 “not
true at all” and 5 “completely true.” This scale measures basic psychological needs.
(This scale appeared as a Likert scale on Qualtrics.)
1. I felt a sense of contact with people who care for me and for whom I care.
2. I was successfully completing difficult tasks and projects.
3. I was free to do things my own way.
4. I was lonely.
5. I experienced some kind of failure or was unable to do well at something.
6. I had a lot of pressures I could do without.
7. I felt close and connected with other people who are important to me.
8. I took on and mastered hard challenges.
9. My choices expressed my “true self.”
10. I felt unappreciated by one or more important people.
11. I did something stupid, that made me feel incompetent.
12. There were people telling me what I had to do.
13. I felt a strong sense of intimacy with the people I spent time with.
14. I did well even at the hard things.
15. I was really doing what interests me.

197
16. I had disagreements or conflicts with people I usually get along with.
17. I struggled doing something I should be good at.
18. I had to do things against my will.
PART D. Please respond to the following questions on a scale from 0 to 10. This
scale measures flourishing. (This scale appeared as a Likert scale on Qualtrics.)
1. Overall, how satisfied are you with life as a whole these days?
0=Not satisfied at all, 10=Completely satisfied
2. In general, how happy or unhappy do you usually feel?
0=Extremely unhappy, 10=Extremely happy
3. In general, how would you rate your physical health?
0=Poor, 10=Excellent
4. How would you rate your overall mental health?
0=Poor, 10=Excellent
5. Overall, to what extent do you feel the things in your life are worthwhile?
0=Not at all worthwhile, 10=Completely worthwhile
6. I understand my purpose in life.
0=Strongly Disagree, 10=Strongly agree
7. I always act to promote good in all circumstances, even in difficult or challenging
situations.
0=Not true of me, 10=Completely true of me
8. I am always able to give up some happiness now for greater happiness later.
0=Not true of me, 10=Completely true of me
9. I am content with my friendships and relationships.
0=Strongly Disagree, 10=Strongly Agree
10. My relationships are as satisfying as I would want them to be.
0=Strongly Disagree, 10=Strongly Agree
PART E. The following question refers to your overall sleep quality for the
majority of the nights in the past 7 days only. Please think about the quality of your
sleep overall, such as how many hours of sleep you got, how easily you fell asleep,
how often you woke up during the night (except to go to the bathroom), how often
you woke up earlier than you had to in the morning, and how refreshing your sleep
was.

198
During the past 7 days, how would you rate your sleep quality overall?
PART F. During the past month, which statement best describes the kinds of
physical activity you usually did? Do not include the time you spent working at a
job. Please read all six statements before SELECTING ONE.
I did not do much physical activity. I mostly did things like watching television,
reading, playing cards, or playing computer games. Only occasionally, no more than
once or twice a month, did I do anything more active such as going for a walk or
playing tennis.
Once or twice a week, I did light activities such as going outdoors on the weekends
for an easy walk or maybe once or twice a week, I did chores around the house such
as sweeping floors or vacuuming.
About three times a week, I did moderate activities such as brisk walking, swimming,
or riding a bike for about 15–20 minutes each time. Or about once a week, I did
moderately difficult chores such as raking or mowing the lawn for about 45–60
minutes. Or about once a week, I played sports such as softball, basketball, or soccer
for about 45–60 minutes.
Almost daily, that is five or more times a week, I did moderate activities such as brisk
walking, swimming, or riding a bike for 30 minutes or more each time. Or about once
a week, I did moderately difficult chores or played sports for 2 hours or more.
About three times a week, I did vigorous activities such as running or riding hard on a
bike for 30 minutes or more each time.
Almost daily, that is five or more times a week, I did vigorous activities such as
running or riding hard on a bike for 30 minutes or more each time.
Qualtrics Six Month Survey
Instructions: Thank you for taking the time to complete this questionnaire for the FUEL
coaching program. Your participation is voluntary and you may skip any item.
Please enter the participant ID provided in the email sent to you by the coach:_______

199
PART A. This part of the questionnaire is to collect information on ways your
professional situation or characteristics may have changed over the FUEL program.
1. Has your job changed in the last month? For example, do you have a new position or
responsibilities?
Yes, please explain:
No.
2. On average, how many hours do you work in a typical week, including time at an
office, in the field, or working at home?
Please specify a total number of hours for the week:
I prefer not to answer
3. On average, what percentage of your work time in a typical week is spent on the
activities that mean the most to you compared to time spent on “hassles” or less-
meaningful responsibilities?
Please specify a percentage for the week:
I prefer not to answer
PART B. Please reflect and answer the following open-ended questions with as
much detail and description as you are comfortable.
1. What’s the first thing that comes to mind when you think back to the FUEL program?
2. Reflect on your feelings, thoughts, and behaviors since FUEL ended? What (if
anything) has changed or emerged in the way you feel, think, or act in the last six
months?
3. What (if any) FUEL strategies, lessons, or behaviors do you use in your daily life?
How do you use them?
4. On a scale from 1-10 with 1 as abysmal and 10 as superb, how would you rate your
job performance and why did you select that rating?
5. How would you describe your progress toward job and/or life goals?
6. What specific positive and negative outcomes have you experienced from coaching?
7. Would you enroll in FUEL again—why or why not?
8. This question has two parts: First, why do you put efforts into your current job?
Second, how do your daily experiences affect your effort or reason to put in effort?
PART C. Please respond to the following questions on a scale from 1-5 with 1 “not
true at all” and 5 “completely true.” This scale measures basic psychological needs.
(This scale appeared as a Likert scale on Qualtrics.)
1. I felt a sense of contact with people who care for me and for whom I care.
2. I was successfully completing difficult tasks and projects.
3. I was free to do things my own way.
4. I was lonely.
5. I experienced some kind of failure or was unable to do well at something.
6. I had a lot of pressures I could do without.
200
7. I felt close and connected with other people who are important to me.
8. I took on and mastered hard challenges.
9. My choices expressed my “true self.”
10. I felt unappreciated by one or more important people.
11. I did something stupid, that made me feel incompetent.
12. There were people telling me what I had to do.
13. I felt a strong sense of intimacy with the people I spent time with.
14. I did well even at the hard things.
15. I was really doing what interests me.
16. I had disagreements or conflicts with people I usually get along with.
17. I struggled doing something I should be good at.
18. I had to do things against my will.
PART D. Please respond to the following questions on a scale from 0 to 10. This
scale measures flourishing. (This scale appeared as a Likert scale on Qualtrics.)
1. Overall, how satisfied are you with life as a whole these days?
0=Not satisfied at all, 10=Completely satisfied
2. In general, how happy or unhappy do you usually feel?
0=Extremely unhappy, 10=Extremely happy
3. In general, how would you rate your physical health?
0=Poor, 10=Excellent
4. How would you rate your overall mental health?
0=Poor, 10=Excellent
5. Overall, to what extent do you feel the things in your life are worthwhile?
0=Not at all worthwhile, 10=Completely worthwhile
6. I understand my purpose in life.
0=Strongly Disagree, 10=Strongly agree
7. I always act to promote good in all circumstances, even in difficult or challenging
situations.
0=Not true of me, 10=Completely true of me
8. I am always able to give up some happiness now for greater happiness later.
0=Not true of me, 10=Completely true of me
9. I am content with my friendships and relationships.
0=Strongly Disagree, 10=Strongly Agree
10. My relationships are as satisfying as I would want them to be.
0=Strongly Disagree, 10=Strongly Agree
201
PART E. The following question refers to your overall sleep quality for the
majority of the nights in the past 7 days only. Please think about the quality of your
sleep overall, such as how many hours of sleep you got, how easily you fell asleep,
how often you woke up during the night (except to go to the bathroom), how often
you woke up earlier than you had to in the morning, and how refreshing your sleep
was.
During the past 7 days, how would you rate your sleep quality overall?
PART F. During the past month, which statement best describes the kinds of
physical activity you usually did? Do not include the time you spent working at a
job. Please read all six statements before SELECTING ONE.
I did not do much physical activity. I mostly did things like watching television,
reading, playing cards, or playing computer games. Only occasionally, no more than
once or twice a month, did I do anything more active such as going for a walk or
playing tennis.
Once or twice a week, I did light activities such as going outdoors on the weekends
for an easy walk or maybe once or twice a week, I did chores around the house such
as sweeping floors or vacuuming.
About three times a week, I did moderate activities such as brisk walking, swimming,
or riding a bike for about 15–20 minutes each time. Or about once a week, I did
moderately difficult chores such as raking or mowing the lawn for about 45–60
minutes. Or about once a week, I played sports such as softball, basketball, or soccer
for about 45–60 minutes.
Almost daily, that is five or more times a week, I did moderate activities such as brisk
walking, swimming, or riding a bike for 30 minutes or more each time. Or about once
a week, I did moderately difficult chores or played sports for 2 hours or more.
About three times a week, I did vigorous activities such as running or riding hard on a
bike for 30 minutes or more each time.
Almost daily, that is five or more times a week, I did vigorous activities such as
running or riding hard on a bike for 30 minutes or more each time.
202
Semi-Structured Interview Guide #1
Greeting and Introduction
Hello, my name is Abby Steketee, and I am a graduate student at Virginia Tech
conducting research about well-being. Thank you for replying to the email and sending
me your consent to participate in this interview.
Do you have questions about the study?
Do you have questions about the consent process?
Is this still a convenient time for the 15-20 minute interview?
If yes, continue below.
If no, but the interviewee is interested in participating, determine a better time to
call back.
If no, thank you for your time.
Interview Guide
1. What is your relationship with insert participant name?
2. How long have you known insert participant name?
3. How often do you interact with or see insert participant name?
4. What, if any, changes have you noticed in insert participant name in the last nine
weeks [six months for interview #2]?
5. If not described in #4: What, if any, changes have you noticed in how insert
participant name gets her work done?
6. If not described in #4: What, if any, changes have you noticed in how insert
participant name takes breaks from work?
7. If not described in #4: What, if any, changes have you noticed related to insert
participant name’s physical activity level, exercise, or working out?
8. If not described in #4: What, if any, changes have you noticed in how insert
participant’s name interacts with other people?
9. If not described in #4: What about how insert participant name treats or talks about
himself or herself?
10. Depending on responses to 5-8: Are there any other behaviors/attitudes/things he or
she says that seem new or different?
Closing
Thank you for your time and engagement today. Would you like to receive a transcript
of this interview? If so, is (insert email address) the best email address to use?
Thank you again.
Semi-Structured Interview Guide #2
Greeting and Introduction
Hello, my name is Abby Steketee, and I am a graduate student at Virginia Tech
conducting research about well-being. Thank you for scheduling this call. We spoke six
months ago during the first semi-structured interview. This is the second and last semi-
structured interview.
203
Do you have questions about the study?
Is this still a convenient time for the 15-20 minute interview?
If yes, continue below.
If no, but the interviewee is interested in participating, determine a better time to
call back.
If no, thank you for your time.
Interview Guide
1. What is your relationship with insert participant name?
2. How long have you known insert participant name?
3. How often do you interact with or see insert participant name?
4. What, if any, changes have you noticed in insert participant name in the last six
months (since we last spoke)?
5. If not described in #4: What, if any, changes have you noticed in how insert
participant name gets her work done?
6. If not described in #4: What, if any, changes have you noticed in how insert
participant name takes breaks from work?
7. If not described in #4: What, if any, changes have you noticed related to insert
participant name’s physical activity level, exercise, or working out?
8. If not described in #4: What, if any, changes have you noticed in how insert
participant’s name interacts with other people?
9. If not described in #4: What about how insert participant name treats or talks about
himself or herself?
10. Depending on responses to 5-8: Are there any other behaviors/attitudes/things he or
she says that seem new or different?
Closing
Thank you for your time and engagement today. Would you like to receive a transcript
of this interview? If so, is (insert email address) the best email address to use?
Thank you again.
Implementation Logs
Table 1: Attendance Log Template
Coachee:______________________________
Date of Enrollment:______________________
Date of
scheduling
meeting
Scheduled
meeting
Date of re-
scheduling
meeting
Re-
scheduled
meeting
Start
Time
End
Time Notes
Session 1
Session 2
Session 3
204
Session 4
Session 5
Session 6
Session 7
Session 8
Session 9
Table 2: Coach Person-Hour Log Template
Coachee:
Date Category* Total time (minutes) Notes
*Categories: Coaching (i.e., directly interacting with participants) or Administrative (i.e., planning,
tracking, etc.)
Table 3: Session log template
Coachee:
Session Number: Date Major Discussion Points Practices for the week
Session 1:
Session 2:
Session 3:
Session 4:
Session 5:
Session 6:
Session 7:
Session 8:
Session 9/closure:
205
Appendix N: Example Infographics from FUEL Repository
FUEL Concepts and Tools: Infographics* about evidence-based practices. *Accessible via hyperlink.
Building Habits
Combinatory Play
Deliberate Practice
Goal Setting
Insight vs Rumination
Metta Meditation
Micro-breaks
Mind Body Strategies
Kindness
Sleep
Three Part Breath
Three Flavors of Happiness
Transformational Leadership
Workout Boosts
Work Recovery
Created by Abby Steketee, MPH for FUEL.
206
Appendix O: Detailed Reach Results
Overview
This appendix provides additional details on the reach dimension of the RE-AIM
Framework. By reporting the “how” and “whom” of recruitment and reach, investigators
aim to facilitate empirical replication and practical scalability of the FUEL program.
Figure 1: Recruitment flyer emailed to listserv administrators and researchers
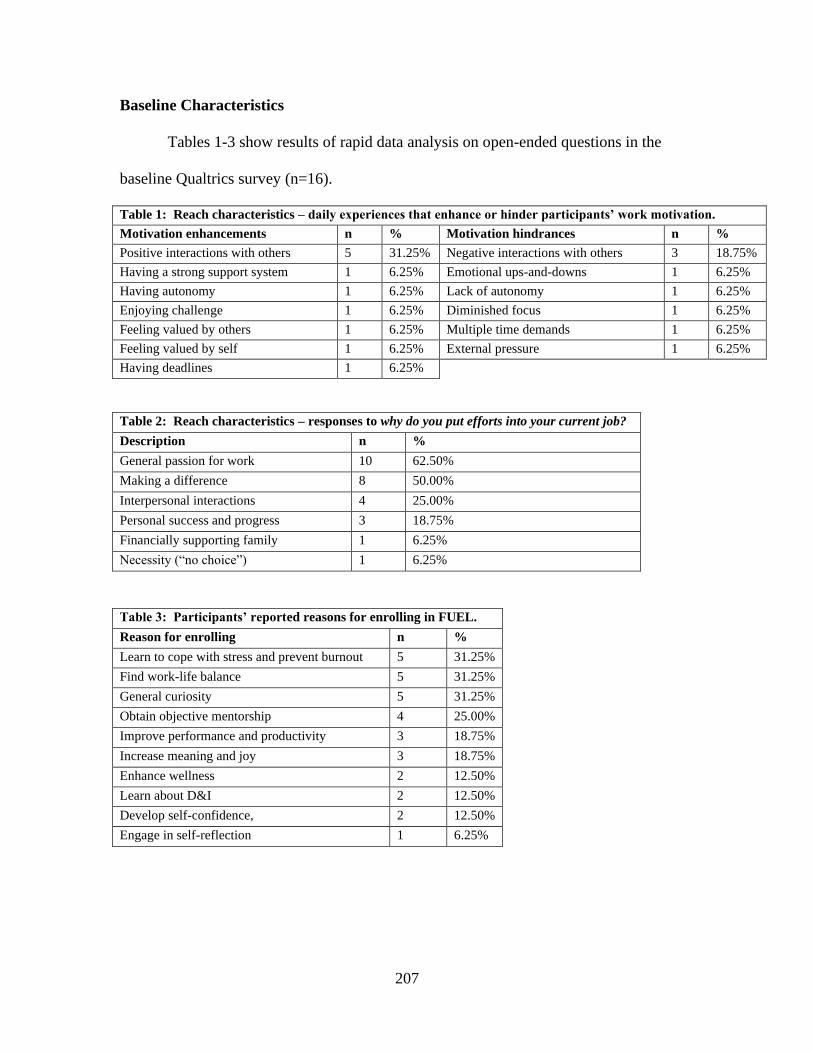
207
Baseline Characteristics
Tables 1-3 show results of rapid data analysis on open-ended questions in the
baseline Qualtrics survey (n=16).
Table 1: Reach characteristics – daily experiences that enhance or hinder participants’ work motivation.
Motivation enhancements n % Motivation hindrances n %
Positive interactions with others 5 31.25% Negative interactions with others 3 18.75%
Having a strong support system 1 6.25% Emotional ups-and-downs 1 6.25%
Having autonomy 1 6.25% Lack of autonomy 1 6.25%
Enjoying challenge 1 6.25% Diminished focus 1 6.25%
Feeling valued by others 1 6.25% Multiple time demands 1 6.25%
Feeling valued by self 1 6.25% External pressure 1 6.25%
Having deadlines 1 6.25%
Table 2: Reach characteristics – responses to why do you put efforts into your current job?
Description n %
General passion for work 10 62.50%
Making a difference 8 50.00%
Interpersonal interactions 4 25.00%
Personal success and progress 3 18.75%
Financially supporting family 1 6.25%
Necessity (“no choice”) 1 6.25%
Table 3: Participants’ reported reasons for enrolling in FUEL.
Reason for enrolling n %
Learn to cope with stress and prevent burnout 5 31.25%
Find work-life balance 5 31.25%
General curiosity 5 31.25%
Obtain objective mentorship 4 25.00%
Improve performance and productivity 3 18.75%
Increase meaning and joy 3 18.75%
Enhance wellness 2 12.50%
Learn about D&I 2 12.50%
Develop self-confidence, 2 12.50%
Engage in self-reflection 1 6.25%
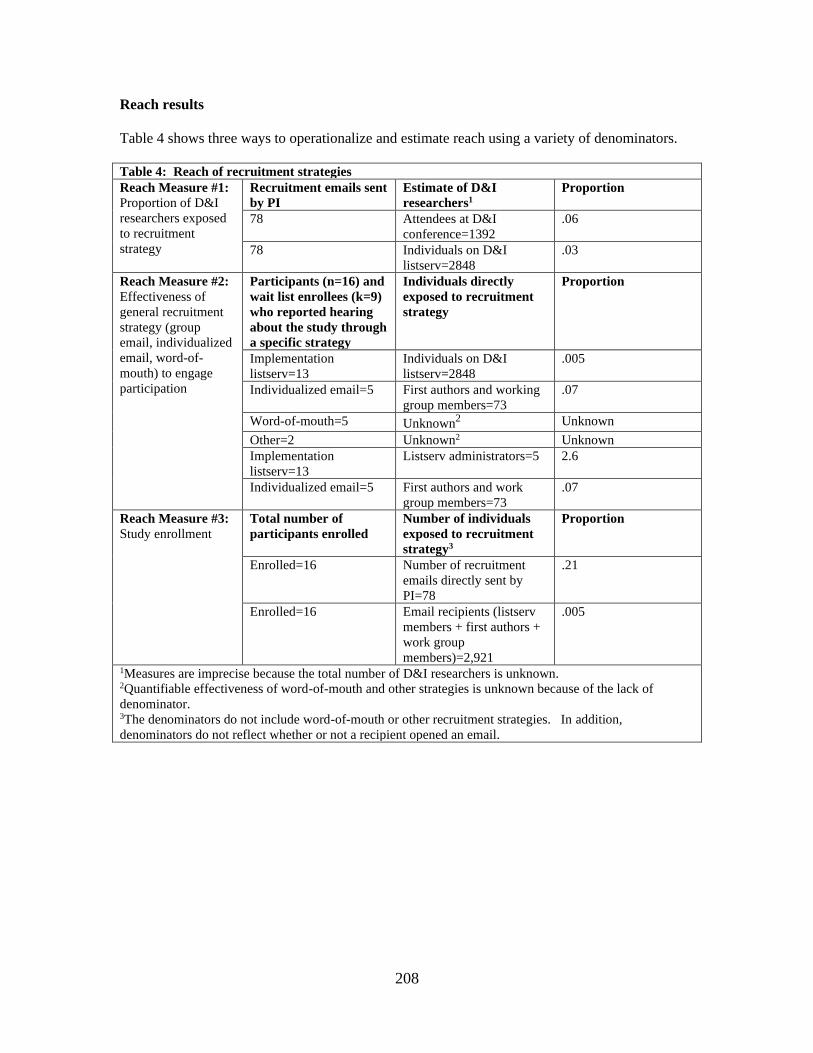
208
Reach results
Table 4 shows three ways to operationalize and estimate reach using a variety of denominators.
Table 4: Reach of recruitment strategies
Reach Measure #1:
Proportion of D&I
researchers exposed
to recruitment
strategy
Recruitment emails sent
by PI
Estimate of D&I
researchers1
Proportion
78 Attendees at D&I
conference=1392
.06
78 Individuals on D&I
listserv=2848
.03
Reach Measure #2:
Effectiveness of
general recruitment
strategy (group
email, individualized
email, word-of-
mouth) to engage
participation
Participants (n=16) and
wait list enrollees (k=9)
who reported hearing
about the study through
a specific strategy
Individuals directly
exposed to recruitment
strategy
Proportion
Implementation
listserv=13
Individuals on D&I
listserv=2848
.005
Individualized email=5 First authors and working
group members=73
.07
Word-of-mouth=5 Unknown2 Unknown
Other=2 Unknown2 Unknown
Implementation
listserv=13
Listserv administrators=5 2.6
Individualized email=5 First authors and work
group members=73
.07
Reach Measure #3:
Study enrollment
Total number of
participants enrolled
Number of individuals
exposed to recruitment
strategy3
Proportion
Enrolled=16 Number of recruitment
emails directly sent by
PI=78
.21
Enrolled=16 Email recipients (listserv
members + first authors +
work group
members)=2,921
.005
1Measures are imprecise because the total number of D&I researchers is unknown. 2Quantifiable effectiveness of word-of-mouth and other strategies is unknown because of the lack of
denominator. 3The denominators do not include word-of-mouth or other recruitment strategies. In addition,
denominators do not reflect whether or not a recipient opened an email.