Embed Size (px)
Citation preview

MHEDIC Structure and AccomplishmentsNaorah Lockhart, Liz Mellin, Paul Flaspohler, & Seth Bernstein

SOCIAL NETWORK ANALYSIS OF MHEDIC

INTRODUCTION AND BACKGROUND
Interdisciplinary collaborative groups increasing in both research and practice
Often use network language (members/actors and relational ties) to describe these collaborations
Social network analysis (SNA) – measures interdependent relationships among group members – important for understanding the structure and accomplishments of social networks like MHEDIC

CURRENT STUDY Document the structure of MHEDIC and knowledge
transfer across traditional disciplinary/professional boundaries.
Examination of the way in which members are tied with other members from their home discipline/profession and members from other disciplines or professions.
Future analyses will also examine ties among members across different status positions (e.g., faculty members and graduate students, male and female, level of position) and how collaboration varies across these positions.

METHODS Sociometric (complete) network design Eligible if attended at least 2 MHEDIC meetings
between Fall 2010 and Fall 2013 (36 members eligible)
Developed survey based on Haines et al., (2011) that asked each member about his/her connections to other members within 6 different types of relationships (cite, co-author, grants, met professionally, mentoring, co-present)
UCINET 6.0 to analyze networks Open-ended questions or additional context

SOCIAL NETWORK ANALYSIS TERMS
Network: The elements of a collaboration linked by relationships between actors that forms a structure.
Actors: members of MHEDIC Relationships: ways actors affiliate within the
network• cited, co-authored, co-presented, submitted a grant
with, mentored, met with professionally• Isolates: actors with no ties within the relationship
Terms and key structural concepts are adapted from Haines, Godley & Hawe, 2010.

KEY STRUCTURAL CONCEPTS Density (expressed as a percentage): the number of ties between
network members out of all possible ties. Higher density indicates more interaction.
Degree centralization: the extent that the relationship is clustered around influential network members
Reciprocity (expressed as a percentage): the ratio of the number of pairs with a reciprocated tie relative to the number of pairs with any tie
Betweenness centrality: the degree to which certain members are more central than others to the network. This should decline as the network matures and influence distributes across the network.
Subgroup: strongly interrelated groups within the network where all the members of the group are directly connected to one another (and in which no additional person in the network is connected to all the members). Subgroups help drive collaboration.

NETWORK DENSITY &DEGREE CENTRALIZATIONRelationship Density No. of
tiesDegreeCentralization
Cited 25% 311 50%
Co-authored 11% 139 31%
Grants 4% 52 33%
Met withprofessionally
20% 247 60%
Mentoring 20% 248 57%
Co-presented 17% 215 38%
Network density: the ratio of actual ties compared to possible ties within a relationship
Degree centralization: the extent the relationship is clustered around influential network members
Over time, density percentages should increase and degree centralization should decrease resulting in a more cohesive network
We are citing 25% of MHEDIC members, but of those citations, 50% are clustered around just few key members of the group.

ISOLATES
Relationship Isolates
Cited 1
Co-authored 6
Grants 14
Met withprofessionally
0
Mentoring 0
Co-presented 0
• Network members who are not tied to a relationship
• Should decrease as the network matures
• Reducing isolates indicates increased interaction between members and more knowledge sharing
Overall, MHEDIC is inclusive. MHEDIC members are included in the network in multiple ways. When people are not included, it may make sense based on their professional role (i.e., practitioner, policymaker). Grants is an area to consider for improvement.

RECIPROCITY
Relationship Reciprocity
Cited 45%
Met withprofessionally
51%
The extent to which ties are returned between actors within a relationship (in this case, relationships that are not inherently reciprocal).
Percentages should increase over time Important for interdisciplinary
collaboration to diversify knowledge exchange

BETWEENNESS CENTRALITY
Relationship BetweennessCentrality
Cited 19%
Co-authored 15%
Grants 12%
Met withprofessionally
33%
Mentoring 21%
Co-presented 18%
Extent to which certain members are more central than others in the network.
The higher the percentage, the more distributed the relationship is across members of MHEDIC.
As the network matures, these percentages should increase, demonstrating an increase in ties directly between two actors rather than through highly centralized (or influential) actors.Grants are clustered across a narrow group of whereas mentoring relationships are more widely distributed.

NUMBER OF SUBGROUPS(3 people or more)
Relationship Subgroups
Cited 66
Co-authored 19
Grants 7
Met withprofessionally
68
Mentoring 47
Co-presented 46
• An indication of network cohesiveness• Opportunities for shared perspectives• Mini “think tanks” within the network• Over time, both the amount of
subgroups for each relationship and individual membership to subgroups should increase

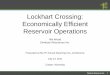
CITED
Larger nodes signify more influential members.
Same network, just different view sorted by discipline
M01 = Liz M10 = MarkM15 = AnnaM29 = DawnM37 = AidynPink = CounselingOrange = EducationBlue = PsychologyGreen = Social Work

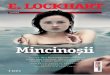
CO-AUTHORED
MHEDIC members not included in this relational network
M01 = Liz M10 = MarkM15 = AnnaM29 = DawnM37 = AidynPink = CounselingOrange = EducationBlue = PsychologyGreen = Social Work

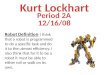
GRANTS
M01 = Liz M10 = MarkM15 = AnnaM29 = DawnM37 = AidynPink = CounselingOrange = EducationBlue = PsychologyGreen = Social Work

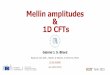
MET WITHPROFESSIONALLY
M01 = Liz M10 = MarkM15 = AnnaM29 = DawnM37 = AidynPink = CounselingOrange = EducationBlue = PsychologyGreen = Social Work

MENTORING
M01 = Liz M10 = MarkM15 = AnnaM29 = DawnM37 = AidynPink = CounselingOrange = EducationBlue = PsychologyGreen = Social Work

CO-PRESENTED
M01 = Liz M10 = MarkM15 = AnnaM29 = DawnM37 = AidynPink = CounselingOrange = EducationBlue = PsychologyGreen = Social Work

PROFESSIONAL/INSTITUTIONAL CONSTRAINTS TO MHEDIC INVOLVEMENT Limited travel funding and/or funding for
travel that prioritizes traditional conference presentations
Critical climates both within and outside of MHEDIC (related to status position in MHEDIC or value of interdisciplinary work by home profession/institution)
Tenure and review criteria that prioritize contributions to home profession/discipline

VALUE OF INTERDISCIPLINARITY IN MHEDIC
COLLABORATIVE SUCCESSES– Expanding network – Professional
advancement– New ways of thinking,
new knowledge– Diversifying ideas in
home profession/discipline
MISSED OPPORTUNITIES– Lack of representation
from education in membership
– Funded research – Disciplinary/profession
centrism within the group

REFLECTIONS AND DISCUSSION
What stood out to you as you looked at the maps and understood the data?
What relationships were not measured that you think would be useful to consider in the future?
How is this helpful to ongoing MHEDIC development?
Pros/cons/comments to repeating this every X years?