Embed Size (px)
Citation preview

Michael Solle MD in collaboration with Thomas Bouldin MDNeuroradiology and Neuropathology, UNC-CH

Case # 1 History:
25 yo female with PMH of TTP (Dx 4-2008) transferred with 2 days of bloody emesis and diarrhea. She had thrombocytopenia, microangiopathic hemolytic anemia, and renal failure. Treated with plasma exchange & steroids.
1 week later:○ After single treatment with rituxan as part of NIH trial,
BP was elevated with systolic >200's, and patient had headache, then a seizure, and bilateral blindness.
Head CT & Brain MRI obtained.


Additional History:Patient’s vision improved after aggressive blood
pressure control measures were taken.TTP failed to respond to IV steroids and PLEX,
and vincristine chemotherapy to prevent further hemolysis was initiated. Renal function continued to improve, but she had worsening abdominal pain in the afternoon after chemotherapy; ultrasound showed an inflamed pancreas but no signs of gallstones.
She had increasing somnolence and tachypnea overnight.
Apnea and arrest.Autopsy performed.

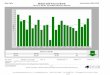
Postmortem brain. Left panel: low power view shows small hemorrhage (arrow) in cerebral cortex. Right panel: high power view shows thrombus (arrow) within a small cortical vessel. Perivascular ischemic necrosis of cortex and hemorrhage are associated with the thrombosed vessel.

• Classically presents with the five findings of microangiopathic hemolytic anemia, thrombocytopenia, renal abnormalities, neurologic manifestations, and fever.
• Neurologic manifestations include headache, confusion, stupor, focal neurologic signs, seizures, and coma.
• Peak incidence is middle-aged adults, with a female predominance.
• With improved recognition of TTP and better therapies, mortality rate has dropped from 90% to 20%.
• Pathogenesis of idiopathic TTP involves autoantibodies to ADAMTS13, a metalloprotease that normally cleaves the large multimers of von Willebrand factor (vWF) produced by the vascular endothelial cells. Persistence of these large vWF multimers leads to the formation of platelet-rich thrombi in small vessels.
• TTP may be associated with HIV infection, pregnancy, or drug therapy.
• MRI may show a posterior reversible leukoencephalopathy syndrome (PRES) and/or edema of basal ganglia.
• Plasma exchange (PLEX) is the current treatment of choice for TTP.
Idiopathic thrombotic thrombocytopenic purpura (TTP)
Rowland, Lewis P.; Pedley, Timothy A, eds. Merritt’s Neurology, 12 th ed., 2009, p. 1000.

Case # 2 History:
9 mo female previously healthy, 3-day history of not being able to sit up, and has "not been acting herself" over the last week. Mother noted that child becomes wobbly and falls to the right upon sitting up. Further history: approximately 5-10 staring spells/day that last 2-3 min each. During these episodes child does not respond to movement in front of her eyes. She had 1 episode of emesis this AM when awakening.
MRI obtained.Neurosurgical procedure and biopsy performed.


Biopsy. Left panel: high power view shows densely cellular small blue cell tumor. Right panel: low power view shows the pale-staining nodules (arrow) that characterize the desmoplastic/nodular variant of medulloblastoma.

Follow up study shows development of diffuse
leptomeningeal metastases.

Medulloblastoma
Mostly solid & show enhancement Often dense on CT Can have restricted diffusion
○ Most do not have cysts or calcium
Hydrocephalus at presentation Arise from roof of fourth ventricle CSF spread at diagnosis is assumed

Case # 3 History:
13 yo female referred for a posterior fossa mass. She had persistent and worsening headaches which were accompanied by fatigue, double vision, and nausea. Headaches were initially attributed to menstrual migraines and became continuous for past week. Headaches described as throbbing and pressure over occiput, worsened by touching chin to chest and improved by sitting up.
CT and brain and spine MRI were done.


Biopsy. Left panel shows astrocytic proliferation with moderate cellularity, mild atypia, and no mitotic figures. Center panel shows numerous brightly eosinophilic Rosenthal fibers (arrow) in an H&E-stained section. Right panel shows eosinophilic granular bodies (arrow) in a PAS-stained section.

Pilocytic astrocytoma Low T1 and high T2 cystic mass Homogeneous enhancement of a mural
nodule
Together with medulloblastoma, most common infratentorial neoplasms in pediatric age group
DDX: Child: medulloblastoma, ependymoma Adult: hemangioblastoma (flow voids due to
hypervascularity) and metastasesSyrinx resolved after resection of mass.

Case # 4
History:40 yo male with sensory symptoms and
weakness in hands starting 4-5 years ago. Symptoms spread to toes, left then right. Feels unsteady when walking and thinks symptoms are steadily progressing, especially during the last year. He cannot run anymore.
MRI of spine was done.Neurosurgical procedure and biopsy performed.


Biopsy. Left panel: low power view shows glial proliferation with pseudorosette formation around blood vessels (arrow).Right panel: high power view shows true ependymal rosette.

Spinal cord ependymoma
Most common spinal cord tumor of adults Most common in patients with NF-2 Rarely high grade (anaplastic) ependymoma

Case # 5
History:53 yo male transferred with dystonic
movements of left arm and leg concerning for partial seizures.
CT and brain MRI were done.Neurosurgical procedure and biopsy
performed.


Biopsy. Left panel: low power view shows brain with multiple areas of inflammation (encephalitis).Right panel: high power view shows fungal hyphae (arrow), neutrophils, and multinucleated giant cells.

Fungal encephalitis Cultures grew Scedosporium apiospermum.
S. apiospermum is the asexual form of Pseudallescheria boydii and is a ubiquitous environmental mold. Infection is typically described in immunocompromised hosts, but localized infections are also well described in immunocompetent individuals.

Case # 6 History:
74 yo female with a history of hypertension and colon cancer with possible metastases to the lung. She presents with a 1-week history of difficulty with gait, dizziness, and nausea.
Head CT and brain MRI were done.A neurosurgical procedure and biopsy were
performed.


Biopsy. Low power view shows a circumscribed adenocarcinoma within the cerebellum. The immunohistochemical profile of this metastatic adenocarcinoma was consistent with a colonic primary.







![INDEX [tngenweb.org] · 2020. 1. 12. · VOLUMEXXII WCGABULLETIN FALL&WINTER2013 INDEX 16thTennessee Bates, Barbara, 41, Bouldin, Christine BRYSON,43 Infantry, 6, …](https://img.pdfslide.net/doc/110x75/60bdeed92f5d0555db4afcf5/index-2020-1-12-volumexxii-wcgabulletin-fallwinter2013-index-16thtennessee.jpg)