Embed Size (px)
Citation preview
1112017
1
Michigan Association of Osteopathic Family Physicians
(MAOFP)
January 19 2017
bull American Academy of Sleep Medicine guidelines for treatment of OSA include oral appliances for mild or moderate OSA to be provided by a dentist who is well versed in sleep and Temporomandibular Disorders I only treat these two diagnoses and
have been certified as Diplomat in Sleep from the American Sleep and Breathing Academy the American Academy of Craniofacial Pain and Sleep and in TMD from the American Academy of Craniofacial Pain the American Academy of Pain Management and Mastership in the International College of Craniomandibular Orthopaedics
bull I will concentrate on the AASM statement during the next 50 minutes as well as a perfunctory synopsis of OSA ramifications and treatments
Dr Richard Klein
A very brief overview of TMD and OA with contraindications for OSA
bullTMJ Internal DerangementsbullSigns and symptoms of TMDbullLack of Dental Support
1112017
2
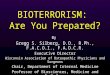
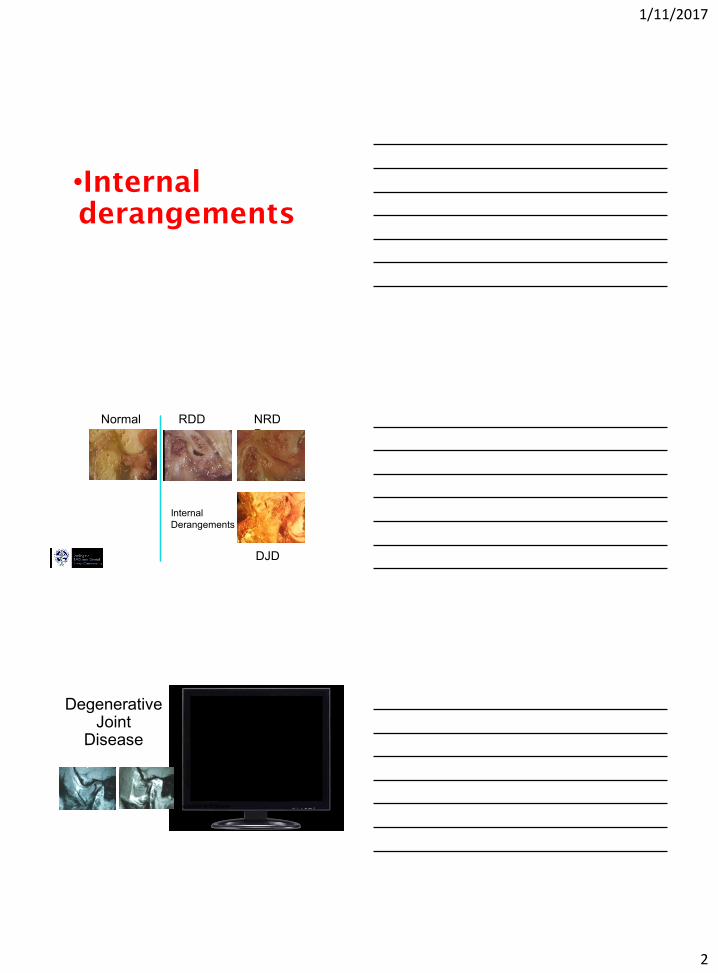
bullInternal
derangements
Normal RDD NRD
D
DJD
Internal
Derangements
Dr Per-Lennart Westesson and Dr Lars Eriksson
Degenerative Joint
Disease
Westesson amp Eriksson
1112017
3
Symptoms of TMD TMD is not a disorder that only affects the jaws The muscles which
posture the correct occlusion are found in the face the head the neck and the upper back
When any of these muscles are in spasm a domino effect on adjacent areas initiates symptoms that are not often thought of in the context of TMD but which definitely may be causally related by it
Dr Janet Travell knew this when she was President Kennedys personal physician and was unfortunately denigrated by the medical community as spouting heresy
Common Ear symptoms of TMD
bull Otalgia
bull Ear congestion
bull Tinnitus which can be extremely ldquoear-attating
bull Buzzing of the ear
bull lightheadedness dizziness loss of balance
bull Hyperacusis
bull Subjective loss of hearing
bull Itchy ear
1112017
4
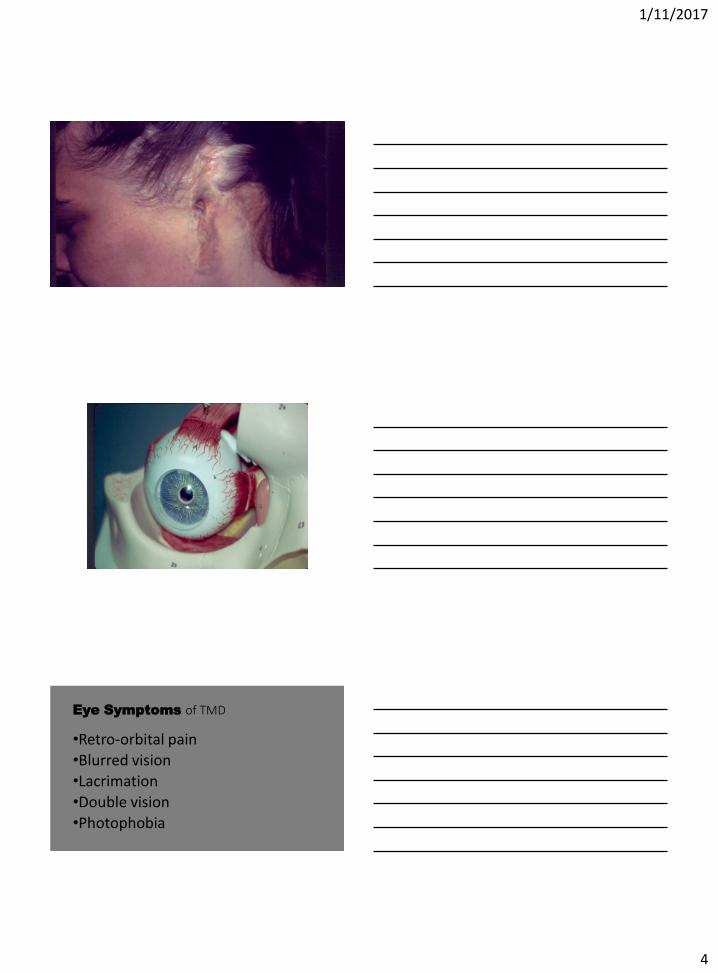
Eye Symptoms of TMD
bullRetro-orbital pain
bullBlurred vision
bullLacrimation
bullDouble vision
bullPhotophobia
1112017
5
RETRO-ORBITAL PAIN
bull Gary Hack etal at the University of Maryland observed a new muscle which they named the SPHENOMANDIBULARIS The muscle was consistently observed as originating from the maxillary surface of the sphenoid bone and inserting on the temporal crest (internal oblique line) of the mandible Controversy exists as to it actually being a new and separate muscle However when tense it will pull on the sphenoid bone which is painful
TBI
I am not ashamed to
admit that the first
time I heard TBI in
our clinical rounds
I thought the speech
pathologist was
referring to tooth brush instructions
1112017
6
Conversely she was
confused when I
spoke of a jaw registration as
articulation
TBI and OSA
Approximately 17 million people sustain a traumatic brain injury (TBI) every year in the United States with 14 million seeking treatment 250000 hospitalizations and 50000 deaths are documented
bull Why are these studies important
bull They are pertinent because they show a direct link between traumatic brain injury and obstructive sleep apnea
bull Not diagnosing obstructive sleep apnea in someone who has sustained a brain injury could impede recovery and rehabilitation
bull As more and more soldiers are coming back from a war that has turned young men and women into mere glimpses of their former selves ndash and as more and more professional athletes especially football players are suffering from the lingering effects of the sport this link is becoming increasingly more important
1112017
7
Prevalence and Consequences of Sleep Disorders in Traumatic Brain Injury
bullThe authors reviewed evidence that cognitive dysfunction is a well known problem after TBI and is a major factor preventing return to independent living social readaptation and vocational pursuits Richard J Castriotta MD12 Mark C Wilde PsyD12 Jenny M Lai MD12 Strahil
Atanasov MD3 Brent E Masel MD4 and Samuel T Kuna MD56
Findings
bull 54 of that population had a normal polysomnography 46 had a sleep disorder (other studies have documented up to 23 had a SBD)
bull This is significantly higher that that of the general population
bull 23 had obstructive sleep apnea Again this finding is much higher than that of those who did or did not vote for our last President
ConclusionbullThe authors concluded that there was a high prevalence of sleep-disorders and excessive daytime sleepiness in individuals who had TBI and that consideration should be given to having all TBI patients evaluated for sleep disorders
1112017
8
Wersquoll discuss this later as it refers to pain
bullBut 1st letrsquos consider OSA since it is highly prevalent in your TBI patients
Sleep Apnea May Hasten Memory Loss and Alzheimers
bullPublished in the journal Neurology the study2 found that patients with sleep apnea andor snoring were diagnosed with mild cognitive impairment more than a decade earlier than those without sleep apnea
bull 2 Neurology April 15 2015
bullOn average those with untreated obstructed sleep apnea started experiencing cognitive impairment at the age of 77 compared to 90 among those without breathing problems
bullThose who used a CPAP machine to address their sleep apnea started declining mentally at the same age as those who did not have sleep apnea
1112017
9
Scary video by WatchPAT
Obstructive SleepApnea
Definition of Sleep apnea
bullSleep Apnea occurs when the soft tissue in your mouth (the tongue tonsils pharynx uvula etc) relax too much and collapse at the back of your throat and cut off the airway making it difficult or impossible to breath
AHI Three levels of severity
Mild 5 to 15 times per hour
Moderate 15 to 30 times per hour
Severe gt30 times per hour
Copyright 2011 Braebon
1112017
10
SLEEP APNEA SYMPTOMS
bull Short term memory problems
bull Weight gain
bull Tiredness
bull Dry mouth
bull Sore throat
bull Slow metabolism
bull Bed partner frustration
bull AND A PLETHORA OF SERIOUS MEDICAL DISEASES DISORDERS AND MALADIES
High blood pressure
Heart failure
Heart rhythm disturbances
Atherosclerotic heart disease
Pulmonary hypertension
Insulin resistance
Sudden death
Erectile dysfunction
Memory problems
Depression
Anxiety
Gastroesophageal reflux
Sleep Apnea Increases Risk of
bull It has been estimated that 80 of depressed patients complain of disturbed sleep and sleeplessness is a risk factor for impaired mood
bull helliphelliphelliphelliphelliphelliphelliphellip The most common complaint of helliphelliphelliphelliphelliphelliphelliphellip PTSD is sleeplessness and 50 -helliphelliphelliphelliphelliphelliphelliphellip 70 of chronic pain patients helliphelliphelliphelliphelliphelliphelliphelliphellip report disturbed sleep
Consequences
1112017
11
Headachesbull Headaches are the most commonly reported pain complaint in the
population (textbook of pain)
bull Sleep disorders such as sleep apnea are found among headache patients at rates greater than what is found in the general population TX of sleep disorders decreases headache complaints Cephalgia is the most common complaint of TMD
bull (Archives of Internal Medicine)
Risk Factors
ObesityLarge neckSnoringNon-restorative sleepDaytime sleepinessfatigueHigh arched palateRetrognathiaCrowded airwaySmokingdrinking
(and remember sleep apnea occurs in women children and skinny guys toohellipthese are just risk factors)
Life Cycle of a LEAF
1112017
12
The cells in our body deteriorate as we age but they do so much quicker without oxygen
The Beatles were only partially correct when they sang
ldquoAll you need is loverdquo
The Hollies had a better understanding of life when they sangrdquo
ldquoAll I need is the air that I breath and to love yourdquo
1112017
13
NORMAL SLEEP
bull CHARACTERIZED BY A DECREASE IN
bull BODY TEMPERATURE
bull BLOOD PRESSURE
bull BREATHING RATE
bull MOST OTHER BODY FUNCTIONS
bull INCREASED NASAL RESISTANCE
bull CHARACTERIZED BY AN bull ACTIVE BRAIN
1112017
14
Copyright 2011 BRAEBON
Normal healthy breathing during sleep
Wake-up-gasping-choking-and-die-in-your-sleep-diseaserdquo ndash No sound during event
Who gets sent for a sleep study
1112017
15
Who usually doesnrsquot
Sleep apnoea is a common occurrence in femalesKarl A Franklin et al European Respiratory Journal August 2012
bull We investigated 400 females from a population-based random sample of 10000 females aged 20ndash70 years with a questionnaire and anovernight polysomnography
bull Obstructive sleep apnoea was found in 50 of females aged 20ndash70 years
bull Sleep apnoea was related to age obesity and hypertension but not to daytime sleepiness
bull Severe sleep apnoea was scored in 14 of females aged 55ndash70 years and in 31 of obese females with a body-mass index of gt30 kgmiddotmminus2 aged 50ndash70 years
1112017
16
EPWORTH SLEEPINESS SCALEINTERPRETATIONbull 0-7 IT IS UNLIKELY THAT YOU ARE ABNORMALLY SLEEPY
bull 8-9 YOU HAVE AN AVERAGE AMOUNT OF DAYTIME SLEEPINESS
bull 10-15 YOU MAY BE EXCESSIVELY SLEEPY DEPENDING ON THE SITUATION YOU MAY WANT TO CONSIDER SEEKING MEDICAL ATTENTION
bull 16-24 YOU ARE EXCESSIVELY SLEEPY AND SHOULD CONSIDER SEEKING MEDICAL ATTENTION
This person most likely is simply tired or had a bad nightrsquos sleep OSA is not
indicated
I referred this patient to a sleep physician
1112017
17
MALLAMPATI
1112017
18
Lavigne GJ Kato T Kolta A Sessle BJ Neurobiological mechanisms involved in sleep bruxism Crit Rev Oral Biol Med 20031430-46
bullSleep-related bruxism (SB) is characterized by the grinding or clenching of the teeth during sleep usually associated with sleep arousals although the incidence of sleep arousals in SB subjects is within the normal range (up to 14 arousalshour of sleep is considered normal)
IT HAS BEEN SHOWN THAT CPAP ELIMINATION OF OSA alsoELIMINATES SNORING
IT HAS NOT BEEN DEMONSTRATED THAT CPAP TREATMENT OF OSA
ELIMINATES OR REDUCES S-B
Neurobiological mechanisms involved in sleep bruxismLavigne GJ1 Kato T Kolta A Sessle BJ
bull Sleep bruxism (SB) is mainly associated with rhythmic masticatory muscle activity (RMMA) characterized by repetitive jaw muscle contractions (3 bursts or more at a frequency of 1 Hz)
bull The consequences of SB may include tooth destruction jaw pain headaches or the limitation of mandibular movement as well as tooth-grinding sounds that disrupt the sleep of bed partners RMMA is observed in 60 of normal sleepers
1112017
19
bull The pathophysiology of SB is becoming clearer
bull There is an abundance of evidence outlining the neurophysiology and neurochemistry of rhythmic jaw movements (RJM) in relation to chewing swallowing and breathing Several brainstem structures (eg reticular pontis oralis pontis caudalis) and neurochemicals (eg serotonin dopamine gamma aminobutyric acid [GABA] noradrenaline) are involved in both the genesis of RJM and the modulation of muscle tone during sleep
bull It creates a co-activation of both jaw-opening and jaw-closing muscles instead of the alternating jaw-opening and jaw-closing muscle activity pattern typical of chewing
Journal of Pain amp Symptom Management
bullPain duration and intensitywere correlated with decreased sleep impaired sleep quality and delayed sleep onset
Multiple Medical Studies
bullHave published that the majority (59 67 74) of OSA patients will not appropriately wear the CPAP
1112017
20
bull IN 1995 Johnny Cochran said ldquoIf the glove doesnrsquot fithellipyou must acquitrdquo As DR Dement intimated in the 1970s ldquoWe didnt know what to measurehellipso we measured everything we could think ofhellip and it stuckrdquo
bull Almost forty years later some of what ldquostuckrdquo is being revised reinterpreted and common sense is beginning to prevail Seven to eight hours of sleep per night is recommended
The Other 72 of Sleep
bull Sticking with the antiquated definition of a ldquocompliant userrdquo of a
CPAP (4 hrsnight and 5 nightsweek) one must use it roughly 28 of the time
bull WHAT ABOUT THE OTHER 72 OF SLEEP
bull Is it acceptable to not get the O2 we need simply because an antiquated standard ldquostuckrdquo
bull In 1995 CPAP became the gold standard Now in the 21st century I
say ldquoif the mask doesnrsquot fit hellipdonrsquot quitrdquo because an oral appliance may save your health and your life
Treatment of Sleep Apnea
Tracheotomy Oral
Surgery CPAPBiPAP
OA
Behavioral Modification
1112017
21
Orofacial Findings
bullThe most common orofacial characteristics include a retrognathic mandible narrow palate large neck circumference long soft palate tonsillar hypertrophy nasal septal deviation and relative macroglossia
Oral Appliances for Sleep Apnea amp Snoring
Tongue Retaining Devices Mandibular Repositioning Appliances
Oral Appliances (OA)
bull Properly fabricated an oral appliance will protrude the tongue and reposition the mandible anteriorly and inferiorly to the most beneficial neuromuscular position to prevent posterior airway collapse
bull This position is titratable and individualized to exact patient requirements and may need periodic adjustments just as does CPAP
1112017
22
BEFORE
APPLIANCE
7c
WITH
APPLIANCE
9 cc
1112017
23
Copyright 2011 BRAEBON
More Directly Related to hellipDental Sleep Medicine
bull EACH PATIENT IS AN INDIVIDUAL AND JUST AS CPAP PRESSURE IS INDIVIDUALLY TITRATEDhellipSO TOO ARE ORAL APPLIANCES
bull IF I DELIVER AN OA TO A PATIENT WHO WILL NOT UTILIZE THE CPAPhellipI WILL PROVIDE ONE OR SEVERAL HOME SLEEP STUDIES TO ASCERTAIN THE EFFICACY OF THE OAhellip AND THEN I REQUIRE THAT THEY RETURN TO THEIR SLEEP
bull DOCTOR FOR A SUBSEQUENT STUDY WHILE helliphelliphelliphelliphelliphelliphellipUTILIZINGTHE OA
Positional Apnea in a 73-Year Old Male with Atrial Fibrillation
bull This case study illustrates the cost-effective approach to successful outcomes associated with positional therapy that are not surprising and are consistent with a recent study which concluded ldquopositional therapy is equivalent to CPAP at normalizing the AHI in patients with positional OSA with similar effects on sleep quality and nocturnal oxygenationrdquo
bull Journal Sleep Diagnosis and Therapy
1112017
24
HOW THE ORAL APPLIANCE TREATS OSA
bull Prevent collapse of airwaybull Forward advancement of jawbull Support forward tongue positionbull Change shape of pharyngeal airwaybull Increase vertical dimension of occlusionbull Correct dysphagia bull Increase volume of space for tonguebull Trains protrusive tongue reflexesbull Alter position of hyoid bone relative to
mandible
THE VARYING ROLES OF THE NOSE AND MOUTH IN BREATHING
1112017
25
THE NOSE
bull A recent pediatric study reveals why addressing the tongue is so important for resolving sleep apnea As explained in this study having an abnormally short lingual frenulum can result in impaired orofacial growth in early childhood reducing the width of the upper airway
bull The upper airway is very pliable so this increases the risk of it collapsing during sleep They found that children with an untreated short frenulum developed abnormal tongue function early in life which also impacted their orofacial growth and led to disordered breathing during sleep
WHAT IS THE ROLE OF THE NOSE
ITS FUNCTIONS ARE VITAL
bull WARMING
bull HUMIDIFICATION
bull FILTERING
bull CLEANING
OF AMBIENT AIR INHALED INTO THE LUNGS
INFUSION OF NITRIC OXIDE
1112017
26
Humidification and
Dehumidification
bull During intake air is humidified to increase lung oxygen facilitation
bull Upon exhalation air is dehumidified to keep water in our cells
bull If this were not the case we would dehydrate unless we continually drank water
NARES
CONSTRICT
NARES FLARE
SNIFF TEST
1112017
27
Cosmetic Surgery
bullHe couldnrsquot breath through his small nose became hypercapnic and helliphelliphellipdied
Effect of treating severe nasal obstruction on the severity of obstructive sleep apnoea
bull HA McLean AM Urton HS Driver AKW Tan AG Day+ PW Munt and MF Fitzpatrick
bullThis study demonstrates that relief of severe nasal obstruction in patients with a normal retroglossal airway is associated with a significant reduction in mouth breathing during sleep improved sleep architecture and a modest improvement in OSA severity
1112017
28
bullThere are several novel aspects to these findings First the study documents a clearly increased upper airway resistance in association with oral breathing during stable sleep as compared with nasal breathing irrespective of central or OSA
bullSecondly this methodology included simultaneous documentation of oral and nasal ventilation during sleep to confirm the absence of any nasal airflow in the oral breathing condition and vice versa
1112017
29
bullThe substantially higher resistive load posed by the oral breathing route provides a plausible explanation for the observation that inhaled ventilation occurs almost exclusively via the nasal route during sleep in subjects with normal nasal resistance
bull Many studies have shown that nasal obstruction can induce or increase apnea frequency in OSA patients When nasal resistance is high a greater pressure drop is required to achieve the same flow and hence collapse of the pharynx is facilitated and this could mitigate the effect of mandibular advancement
bull Moreover high nasal resistance is associated with mouth breathing which could potentially limit the beneficial effect of mandibular advancement
bull Dental Appliance Treatment for Obstructive
bull Andrew S L Chan Richard W W Lee and Peter A Cistulli
bull httpchestjournalchestpubsorgcontent1322693fullhtml
1112017
30
bullCurrent evidence suggests that despite the superior efficacy of CPAP both treatments produce similar subjective and objective health benefits
bullThe superior self-reported tolerance and compliance associated with MAD treatment is a likely explanation
bullThe practice parameters of the AASM recommend the use of oral appliances for mild-to-moderate OSA or for patients with severe OSA who are unable to tolerate CPAP or refuse treatment with CPAP with a required written prescription by a sleep physician
The following are Medicare rules
1) A diagnosis of OSA is not within the dental scope of practice A dentist providing an OA
must do so under the and with the team effort of a licensed Physician with a written
prescription
2) A physician is not skilled in the intricacies of fabricating fitting monitoring adjusting
and choosing an appropriate Oral Appliance individualized per patient
3) A dentist may not provide an oral appliance if the patient has an active
Temporomandibular Disorder
4) The OA must be fabricated within 90 days of the patientrsquos appointment with the sleep
physician
Since the rules are clear and they involve both of our professions it would behoove
both DOMD and DDS to communicate for the benefit of OSA patients
1112017
31
Subsequent to my 3 hour 2013 Meeting with the US Department of Transportation regarding Truckers
bull During the State Board of Dental Examiners meeting Board members put sleep Dentistry in squarely back into the spotlight The Board has addressed sleep Dentistry issues in a public hearing and all four Board meetings in 2013
bull There was discussion that there can be a shared relationship between the Dental and medical scopes of practice
bull Under the proposed rule a Dentist may treat benign snoring with an oral appliance after referral to a licensed physician where appropriate within the standard of care By contrast a Dentist may not diagnose treat or monitor OSA without collaboration with a licensed physician Additionally an oral appliance shall only be fabricated by a licensed Dentist or by a Dental lab under a prescription or work order prepared by a Dentist
American Dental Association
bull Treatment using an oral appliance designed specifically to treat OSA should be fabricated by a dentist familiar with device design maintenance and therapeutic efficacy and who has an association with and a referral from a sleep team
bull JADA Vol 136 p 1123
Donrsquot be afraid of OSA Get a grip on the facts and save patientrsquos lives
1112017
32
bullA SYMBIOTIC RELATION BETWEEN PHYSICIANS SLEEP PROFESSIONALS AND DENTISTS CAN SIGNIFICANTLY IMPROVE THE SLEEP HEALTH OF MILLIONS OF PEOPLE EACH AND EVERY YEAR
bull THAT RELATIONSHIP IS NOT A ONE WAY STREET AND THE
American Sleep amp Breathing Academy of over 8000 members UNDERSTANDS THAThellip JUST LOOK AT THE MULTITUDE OF SLEEP PROFESSIONAL CATAGORIES ON THEIR BOARD OF DIRECTORS
THE END
Thank you for your interest I hope this presentation was helpful
Dr Richard Klein
1112017
2
bullInternal
derangements
Normal RDD NRD
D
DJD
Internal
Derangements
Dr Per-Lennart Westesson and Dr Lars Eriksson
Degenerative Joint
Disease
Westesson amp Eriksson
1112017
3
Symptoms of TMD TMD is not a disorder that only affects the jaws The muscles which
posture the correct occlusion are found in the face the head the neck and the upper back
When any of these muscles are in spasm a domino effect on adjacent areas initiates symptoms that are not often thought of in the context of TMD but which definitely may be causally related by it
Dr Janet Travell knew this when she was President Kennedys personal physician and was unfortunately denigrated by the medical community as spouting heresy
Common Ear symptoms of TMD
bull Otalgia
bull Ear congestion
bull Tinnitus which can be extremely ldquoear-attating
bull Buzzing of the ear
bull lightheadedness dizziness loss of balance
bull Hyperacusis
bull Subjective loss of hearing
bull Itchy ear
1112017
4
Eye Symptoms of TMD
bullRetro-orbital pain
bullBlurred vision
bullLacrimation
bullDouble vision
bullPhotophobia
1112017
5
RETRO-ORBITAL PAIN
bull Gary Hack etal at the University of Maryland observed a new muscle which they named the SPHENOMANDIBULARIS The muscle was consistently observed as originating from the maxillary surface of the sphenoid bone and inserting on the temporal crest (internal oblique line) of the mandible Controversy exists as to it actually being a new and separate muscle However when tense it will pull on the sphenoid bone which is painful
TBI
I am not ashamed to
admit that the first
time I heard TBI in
our clinical rounds
I thought the speech
pathologist was
referring to tooth brush instructions
1112017
6
Conversely she was
confused when I
spoke of a jaw registration as
articulation
TBI and OSA
Approximately 17 million people sustain a traumatic brain injury (TBI) every year in the United States with 14 million seeking treatment 250000 hospitalizations and 50000 deaths are documented
bull Why are these studies important
bull They are pertinent because they show a direct link between traumatic brain injury and obstructive sleep apnea
bull Not diagnosing obstructive sleep apnea in someone who has sustained a brain injury could impede recovery and rehabilitation
bull As more and more soldiers are coming back from a war that has turned young men and women into mere glimpses of their former selves ndash and as more and more professional athletes especially football players are suffering from the lingering effects of the sport this link is becoming increasingly more important
1112017
7
Prevalence and Consequences of Sleep Disorders in Traumatic Brain Injury
bullThe authors reviewed evidence that cognitive dysfunction is a well known problem after TBI and is a major factor preventing return to independent living social readaptation and vocational pursuits Richard J Castriotta MD12 Mark C Wilde PsyD12 Jenny M Lai MD12 Strahil
Atanasov MD3 Brent E Masel MD4 and Samuel T Kuna MD56
Findings
bull 54 of that population had a normal polysomnography 46 had a sleep disorder (other studies have documented up to 23 had a SBD)
bull This is significantly higher that that of the general population
bull 23 had obstructive sleep apnea Again this finding is much higher than that of those who did or did not vote for our last President
ConclusionbullThe authors concluded that there was a high prevalence of sleep-disorders and excessive daytime sleepiness in individuals who had TBI and that consideration should be given to having all TBI patients evaluated for sleep disorders
1112017
8
Wersquoll discuss this later as it refers to pain
bullBut 1st letrsquos consider OSA since it is highly prevalent in your TBI patients
Sleep Apnea May Hasten Memory Loss and Alzheimers
bullPublished in the journal Neurology the study2 found that patients with sleep apnea andor snoring were diagnosed with mild cognitive impairment more than a decade earlier than those without sleep apnea
bull 2 Neurology April 15 2015
bullOn average those with untreated obstructed sleep apnea started experiencing cognitive impairment at the age of 77 compared to 90 among those without breathing problems
bullThose who used a CPAP machine to address their sleep apnea started declining mentally at the same age as those who did not have sleep apnea
1112017
9
Scary video by WatchPAT
Obstructive SleepApnea
Definition of Sleep apnea
bullSleep Apnea occurs when the soft tissue in your mouth (the tongue tonsils pharynx uvula etc) relax too much and collapse at the back of your throat and cut off the airway making it difficult or impossible to breath
AHI Three levels of severity
Mild 5 to 15 times per hour
Moderate 15 to 30 times per hour
Severe gt30 times per hour
Copyright 2011 Braebon
1112017
10
SLEEP APNEA SYMPTOMS
bull Short term memory problems
bull Weight gain
bull Tiredness
bull Dry mouth
bull Sore throat
bull Slow metabolism
bull Bed partner frustration
bull AND A PLETHORA OF SERIOUS MEDICAL DISEASES DISORDERS AND MALADIES
High blood pressure
Heart failure
Heart rhythm disturbances
Atherosclerotic heart disease
Pulmonary hypertension
Insulin resistance
Sudden death
Erectile dysfunction
Memory problems
Depression
Anxiety
Gastroesophageal reflux
Sleep Apnea Increases Risk of
bull It has been estimated that 80 of depressed patients complain of disturbed sleep and sleeplessness is a risk factor for impaired mood
bull helliphelliphelliphelliphelliphelliphelliphellip The most common complaint of helliphelliphelliphelliphelliphelliphelliphellip PTSD is sleeplessness and 50 -helliphelliphelliphelliphelliphelliphelliphellip 70 of chronic pain patients helliphelliphelliphelliphelliphelliphelliphelliphellip report disturbed sleep
Consequences
1112017
11
Headachesbull Headaches are the most commonly reported pain complaint in the
population (textbook of pain)
bull Sleep disorders such as sleep apnea are found among headache patients at rates greater than what is found in the general population TX of sleep disorders decreases headache complaints Cephalgia is the most common complaint of TMD
bull (Archives of Internal Medicine)
Risk Factors
ObesityLarge neckSnoringNon-restorative sleepDaytime sleepinessfatigueHigh arched palateRetrognathiaCrowded airwaySmokingdrinking
(and remember sleep apnea occurs in women children and skinny guys toohellipthese are just risk factors)
Life Cycle of a LEAF
1112017
12
The cells in our body deteriorate as we age but they do so much quicker without oxygen
The Beatles were only partially correct when they sang
ldquoAll you need is loverdquo
The Hollies had a better understanding of life when they sangrdquo
ldquoAll I need is the air that I breath and to love yourdquo
1112017
13
NORMAL SLEEP
bull CHARACTERIZED BY A DECREASE IN
bull BODY TEMPERATURE
bull BLOOD PRESSURE
bull BREATHING RATE
bull MOST OTHER BODY FUNCTIONS
bull INCREASED NASAL RESISTANCE
bull CHARACTERIZED BY AN bull ACTIVE BRAIN
1112017
14
Copyright 2011 BRAEBON
Normal healthy breathing during sleep
Wake-up-gasping-choking-and-die-in-your-sleep-diseaserdquo ndash No sound during event
Who gets sent for a sleep study
1112017
15
Who usually doesnrsquot
Sleep apnoea is a common occurrence in femalesKarl A Franklin et al European Respiratory Journal August 2012
bull We investigated 400 females from a population-based random sample of 10000 females aged 20ndash70 years with a questionnaire and anovernight polysomnography
bull Obstructive sleep apnoea was found in 50 of females aged 20ndash70 years
bull Sleep apnoea was related to age obesity and hypertension but not to daytime sleepiness
bull Severe sleep apnoea was scored in 14 of females aged 55ndash70 years and in 31 of obese females with a body-mass index of gt30 kgmiddotmminus2 aged 50ndash70 years
1112017
16
EPWORTH SLEEPINESS SCALEINTERPRETATIONbull 0-7 IT IS UNLIKELY THAT YOU ARE ABNORMALLY SLEEPY
bull 8-9 YOU HAVE AN AVERAGE AMOUNT OF DAYTIME SLEEPINESS
bull 10-15 YOU MAY BE EXCESSIVELY SLEEPY DEPENDING ON THE SITUATION YOU MAY WANT TO CONSIDER SEEKING MEDICAL ATTENTION
bull 16-24 YOU ARE EXCESSIVELY SLEEPY AND SHOULD CONSIDER SEEKING MEDICAL ATTENTION
This person most likely is simply tired or had a bad nightrsquos sleep OSA is not
indicated
I referred this patient to a sleep physician
1112017
17
MALLAMPATI
1112017
18
Lavigne GJ Kato T Kolta A Sessle BJ Neurobiological mechanisms involved in sleep bruxism Crit Rev Oral Biol Med 20031430-46
bullSleep-related bruxism (SB) is characterized by the grinding or clenching of the teeth during sleep usually associated with sleep arousals although the incidence of sleep arousals in SB subjects is within the normal range (up to 14 arousalshour of sleep is considered normal)
IT HAS BEEN SHOWN THAT CPAP ELIMINATION OF OSA alsoELIMINATES SNORING
IT HAS NOT BEEN DEMONSTRATED THAT CPAP TREATMENT OF OSA
ELIMINATES OR REDUCES S-B
Neurobiological mechanisms involved in sleep bruxismLavigne GJ1 Kato T Kolta A Sessle BJ
bull Sleep bruxism (SB) is mainly associated with rhythmic masticatory muscle activity (RMMA) characterized by repetitive jaw muscle contractions (3 bursts or more at a frequency of 1 Hz)
bull The consequences of SB may include tooth destruction jaw pain headaches or the limitation of mandibular movement as well as tooth-grinding sounds that disrupt the sleep of bed partners RMMA is observed in 60 of normal sleepers
1112017
19
bull The pathophysiology of SB is becoming clearer
bull There is an abundance of evidence outlining the neurophysiology and neurochemistry of rhythmic jaw movements (RJM) in relation to chewing swallowing and breathing Several brainstem structures (eg reticular pontis oralis pontis caudalis) and neurochemicals (eg serotonin dopamine gamma aminobutyric acid [GABA] noradrenaline) are involved in both the genesis of RJM and the modulation of muscle tone during sleep
bull It creates a co-activation of both jaw-opening and jaw-closing muscles instead of the alternating jaw-opening and jaw-closing muscle activity pattern typical of chewing
Journal of Pain amp Symptom Management
bullPain duration and intensitywere correlated with decreased sleep impaired sleep quality and delayed sleep onset
Multiple Medical Studies
bullHave published that the majority (59 67 74) of OSA patients will not appropriately wear the CPAP
1112017
20
bull IN 1995 Johnny Cochran said ldquoIf the glove doesnrsquot fithellipyou must acquitrdquo As DR Dement intimated in the 1970s ldquoWe didnt know what to measurehellipso we measured everything we could think ofhellip and it stuckrdquo
bull Almost forty years later some of what ldquostuckrdquo is being revised reinterpreted and common sense is beginning to prevail Seven to eight hours of sleep per night is recommended
The Other 72 of Sleep
bull Sticking with the antiquated definition of a ldquocompliant userrdquo of a
CPAP (4 hrsnight and 5 nightsweek) one must use it roughly 28 of the time
bull WHAT ABOUT THE OTHER 72 OF SLEEP
bull Is it acceptable to not get the O2 we need simply because an antiquated standard ldquostuckrdquo
bull In 1995 CPAP became the gold standard Now in the 21st century I
say ldquoif the mask doesnrsquot fit hellipdonrsquot quitrdquo because an oral appliance may save your health and your life
Treatment of Sleep Apnea
Tracheotomy Oral
Surgery CPAPBiPAP
OA
Behavioral Modification
1112017
21
Orofacial Findings
bullThe most common orofacial characteristics include a retrognathic mandible narrow palate large neck circumference long soft palate tonsillar hypertrophy nasal septal deviation and relative macroglossia
Oral Appliances for Sleep Apnea amp Snoring
Tongue Retaining Devices Mandibular Repositioning Appliances
Oral Appliances (OA)
bull Properly fabricated an oral appliance will protrude the tongue and reposition the mandible anteriorly and inferiorly to the most beneficial neuromuscular position to prevent posterior airway collapse
bull This position is titratable and individualized to exact patient requirements and may need periodic adjustments just as does CPAP
1112017
22
BEFORE
APPLIANCE
7c
WITH
APPLIANCE
9 cc
1112017
23
Copyright 2011 BRAEBON
More Directly Related to hellipDental Sleep Medicine
bull EACH PATIENT IS AN INDIVIDUAL AND JUST AS CPAP PRESSURE IS INDIVIDUALLY TITRATEDhellipSO TOO ARE ORAL APPLIANCES
bull IF I DELIVER AN OA TO A PATIENT WHO WILL NOT UTILIZE THE CPAPhellipI WILL PROVIDE ONE OR SEVERAL HOME SLEEP STUDIES TO ASCERTAIN THE EFFICACY OF THE OAhellip AND THEN I REQUIRE THAT THEY RETURN TO THEIR SLEEP
bull DOCTOR FOR A SUBSEQUENT STUDY WHILE helliphelliphelliphelliphelliphelliphellipUTILIZINGTHE OA
Positional Apnea in a 73-Year Old Male with Atrial Fibrillation
bull This case study illustrates the cost-effective approach to successful outcomes associated with positional therapy that are not surprising and are consistent with a recent study which concluded ldquopositional therapy is equivalent to CPAP at normalizing the AHI in patients with positional OSA with similar effects on sleep quality and nocturnal oxygenationrdquo
bull Journal Sleep Diagnosis and Therapy
1112017
24
HOW THE ORAL APPLIANCE TREATS OSA
bull Prevent collapse of airwaybull Forward advancement of jawbull Support forward tongue positionbull Change shape of pharyngeal airwaybull Increase vertical dimension of occlusionbull Correct dysphagia bull Increase volume of space for tonguebull Trains protrusive tongue reflexesbull Alter position of hyoid bone relative to
mandible
THE VARYING ROLES OF THE NOSE AND MOUTH IN BREATHING
1112017
25
THE NOSE
bull A recent pediatric study reveals why addressing the tongue is so important for resolving sleep apnea As explained in this study having an abnormally short lingual frenulum can result in impaired orofacial growth in early childhood reducing the width of the upper airway
bull The upper airway is very pliable so this increases the risk of it collapsing during sleep They found that children with an untreated short frenulum developed abnormal tongue function early in life which also impacted their orofacial growth and led to disordered breathing during sleep
WHAT IS THE ROLE OF THE NOSE
ITS FUNCTIONS ARE VITAL
bull WARMING
bull HUMIDIFICATION
bull FILTERING
bull CLEANING
OF AMBIENT AIR INHALED INTO THE LUNGS
INFUSION OF NITRIC OXIDE
1112017
26
Humidification and
Dehumidification
bull During intake air is humidified to increase lung oxygen facilitation
bull Upon exhalation air is dehumidified to keep water in our cells
bull If this were not the case we would dehydrate unless we continually drank water
NARES
CONSTRICT
NARES FLARE
SNIFF TEST
1112017
27
Cosmetic Surgery
bullHe couldnrsquot breath through his small nose became hypercapnic and helliphelliphellipdied
Effect of treating severe nasal obstruction on the severity of obstructive sleep apnoea
bull HA McLean AM Urton HS Driver AKW Tan AG Day+ PW Munt and MF Fitzpatrick
bullThis study demonstrates that relief of severe nasal obstruction in patients with a normal retroglossal airway is associated with a significant reduction in mouth breathing during sleep improved sleep architecture and a modest improvement in OSA severity
1112017
28
bullThere are several novel aspects to these findings First the study documents a clearly increased upper airway resistance in association with oral breathing during stable sleep as compared with nasal breathing irrespective of central or OSA
bullSecondly this methodology included simultaneous documentation of oral and nasal ventilation during sleep to confirm the absence of any nasal airflow in the oral breathing condition and vice versa
1112017
29
bullThe substantially higher resistive load posed by the oral breathing route provides a plausible explanation for the observation that inhaled ventilation occurs almost exclusively via the nasal route during sleep in subjects with normal nasal resistance
bull Many studies have shown that nasal obstruction can induce or increase apnea frequency in OSA patients When nasal resistance is high a greater pressure drop is required to achieve the same flow and hence collapse of the pharynx is facilitated and this could mitigate the effect of mandibular advancement
bull Moreover high nasal resistance is associated with mouth breathing which could potentially limit the beneficial effect of mandibular advancement
bull Dental Appliance Treatment for Obstructive
bull Andrew S L Chan Richard W W Lee and Peter A Cistulli
bull httpchestjournalchestpubsorgcontent1322693fullhtml
1112017
30
bullCurrent evidence suggests that despite the superior efficacy of CPAP both treatments produce similar subjective and objective health benefits
bullThe superior self-reported tolerance and compliance associated with MAD treatment is a likely explanation
bullThe practice parameters of the AASM recommend the use of oral appliances for mild-to-moderate OSA or for patients with severe OSA who are unable to tolerate CPAP or refuse treatment with CPAP with a required written prescription by a sleep physician
The following are Medicare rules
1) A diagnosis of OSA is not within the dental scope of practice A dentist providing an OA
must do so under the and with the team effort of a licensed Physician with a written
prescription
2) A physician is not skilled in the intricacies of fabricating fitting monitoring adjusting
and choosing an appropriate Oral Appliance individualized per patient
3) A dentist may not provide an oral appliance if the patient has an active
Temporomandibular Disorder
4) The OA must be fabricated within 90 days of the patientrsquos appointment with the sleep
physician
Since the rules are clear and they involve both of our professions it would behoove
both DOMD and DDS to communicate for the benefit of OSA patients
1112017
31
Subsequent to my 3 hour 2013 Meeting with the US Department of Transportation regarding Truckers
bull During the State Board of Dental Examiners meeting Board members put sleep Dentistry in squarely back into the spotlight The Board has addressed sleep Dentistry issues in a public hearing and all four Board meetings in 2013
bull There was discussion that there can be a shared relationship between the Dental and medical scopes of practice
bull Under the proposed rule a Dentist may treat benign snoring with an oral appliance after referral to a licensed physician where appropriate within the standard of care By contrast a Dentist may not diagnose treat or monitor OSA without collaboration with a licensed physician Additionally an oral appliance shall only be fabricated by a licensed Dentist or by a Dental lab under a prescription or work order prepared by a Dentist
American Dental Association
bull Treatment using an oral appliance designed specifically to treat OSA should be fabricated by a dentist familiar with device design maintenance and therapeutic efficacy and who has an association with and a referral from a sleep team
bull JADA Vol 136 p 1123
Donrsquot be afraid of OSA Get a grip on the facts and save patientrsquos lives
1112017
32
bullA SYMBIOTIC RELATION BETWEEN PHYSICIANS SLEEP PROFESSIONALS AND DENTISTS CAN SIGNIFICANTLY IMPROVE THE SLEEP HEALTH OF MILLIONS OF PEOPLE EACH AND EVERY YEAR
bull THAT RELATIONSHIP IS NOT A ONE WAY STREET AND THE
American Sleep amp Breathing Academy of over 8000 members UNDERSTANDS THAThellip JUST LOOK AT THE MULTITUDE OF SLEEP PROFESSIONAL CATAGORIES ON THEIR BOARD OF DIRECTORS
THE END
Thank you for your interest I hope this presentation was helpful
Dr Richard Klein
1112017
3
Symptoms of TMD TMD is not a disorder that only affects the jaws The muscles which
posture the correct occlusion are found in the face the head the neck and the upper back
When any of these muscles are in spasm a domino effect on adjacent areas initiates symptoms that are not often thought of in the context of TMD but which definitely may be causally related by it
Dr Janet Travell knew this when she was President Kennedys personal physician and was unfortunately denigrated by the medical community as spouting heresy
Common Ear symptoms of TMD
bull Otalgia
bull Ear congestion
bull Tinnitus which can be extremely ldquoear-attating
bull Buzzing of the ear
bull lightheadedness dizziness loss of balance
bull Hyperacusis
bull Subjective loss of hearing
bull Itchy ear
1112017
4
Eye Symptoms of TMD
bullRetro-orbital pain
bullBlurred vision
bullLacrimation
bullDouble vision
bullPhotophobia
1112017
5
RETRO-ORBITAL PAIN
bull Gary Hack etal at the University of Maryland observed a new muscle which they named the SPHENOMANDIBULARIS The muscle was consistently observed as originating from the maxillary surface of the sphenoid bone and inserting on the temporal crest (internal oblique line) of the mandible Controversy exists as to it actually being a new and separate muscle However when tense it will pull on the sphenoid bone which is painful
TBI
I am not ashamed to
admit that the first
time I heard TBI in
our clinical rounds
I thought the speech
pathologist was
referring to tooth brush instructions
1112017
6
Conversely she was
confused when I
spoke of a jaw registration as
articulation
TBI and OSA
Approximately 17 million people sustain a traumatic brain injury (TBI) every year in the United States with 14 million seeking treatment 250000 hospitalizations and 50000 deaths are documented
bull Why are these studies important
bull They are pertinent because they show a direct link between traumatic brain injury and obstructive sleep apnea
bull Not diagnosing obstructive sleep apnea in someone who has sustained a brain injury could impede recovery and rehabilitation
bull As more and more soldiers are coming back from a war that has turned young men and women into mere glimpses of their former selves ndash and as more and more professional athletes especially football players are suffering from the lingering effects of the sport this link is becoming increasingly more important
1112017
7
Prevalence and Consequences of Sleep Disorders in Traumatic Brain Injury
bullThe authors reviewed evidence that cognitive dysfunction is a well known problem after TBI and is a major factor preventing return to independent living social readaptation and vocational pursuits Richard J Castriotta MD12 Mark C Wilde PsyD12 Jenny M Lai MD12 Strahil
Atanasov MD3 Brent E Masel MD4 and Samuel T Kuna MD56
Findings
bull 54 of that population had a normal polysomnography 46 had a sleep disorder (other studies have documented up to 23 had a SBD)
bull This is significantly higher that that of the general population
bull 23 had obstructive sleep apnea Again this finding is much higher than that of those who did or did not vote for our last President
ConclusionbullThe authors concluded that there was a high prevalence of sleep-disorders and excessive daytime sleepiness in individuals who had TBI and that consideration should be given to having all TBI patients evaluated for sleep disorders
1112017
8
Wersquoll discuss this later as it refers to pain
bullBut 1st letrsquos consider OSA since it is highly prevalent in your TBI patients
Sleep Apnea May Hasten Memory Loss and Alzheimers
bullPublished in the journal Neurology the study2 found that patients with sleep apnea andor snoring were diagnosed with mild cognitive impairment more than a decade earlier than those without sleep apnea
bull 2 Neurology April 15 2015
bullOn average those with untreated obstructed sleep apnea started experiencing cognitive impairment at the age of 77 compared to 90 among those without breathing problems
bullThose who used a CPAP machine to address their sleep apnea started declining mentally at the same age as those who did not have sleep apnea
1112017
9
Scary video by WatchPAT
Obstructive SleepApnea
Definition of Sleep apnea
bullSleep Apnea occurs when the soft tissue in your mouth (the tongue tonsils pharynx uvula etc) relax too much and collapse at the back of your throat and cut off the airway making it difficult or impossible to breath
AHI Three levels of severity
Mild 5 to 15 times per hour
Moderate 15 to 30 times per hour
Severe gt30 times per hour
Copyright 2011 Braebon
1112017
10
SLEEP APNEA SYMPTOMS
bull Short term memory problems
bull Weight gain
bull Tiredness
bull Dry mouth
bull Sore throat
bull Slow metabolism
bull Bed partner frustration
bull AND A PLETHORA OF SERIOUS MEDICAL DISEASES DISORDERS AND MALADIES
High blood pressure
Heart failure
Heart rhythm disturbances
Atherosclerotic heart disease
Pulmonary hypertension
Insulin resistance
Sudden death
Erectile dysfunction
Memory problems
Depression
Anxiety
Gastroesophageal reflux
Sleep Apnea Increases Risk of
bull It has been estimated that 80 of depressed patients complain of disturbed sleep and sleeplessness is a risk factor for impaired mood
bull helliphelliphelliphelliphelliphelliphelliphellip The most common complaint of helliphelliphelliphelliphelliphelliphelliphellip PTSD is sleeplessness and 50 -helliphelliphelliphelliphelliphelliphelliphellip 70 of chronic pain patients helliphelliphelliphelliphelliphelliphelliphelliphellip report disturbed sleep
Consequences
1112017
11
Headachesbull Headaches are the most commonly reported pain complaint in the
population (textbook of pain)
bull Sleep disorders such as sleep apnea are found among headache patients at rates greater than what is found in the general population TX of sleep disorders decreases headache complaints Cephalgia is the most common complaint of TMD
bull (Archives of Internal Medicine)
Risk Factors
ObesityLarge neckSnoringNon-restorative sleepDaytime sleepinessfatigueHigh arched palateRetrognathiaCrowded airwaySmokingdrinking
(and remember sleep apnea occurs in women children and skinny guys toohellipthese are just risk factors)
Life Cycle of a LEAF
1112017
12
The cells in our body deteriorate as we age but they do so much quicker without oxygen
The Beatles were only partially correct when they sang
ldquoAll you need is loverdquo
The Hollies had a better understanding of life when they sangrdquo
ldquoAll I need is the air that I breath and to love yourdquo
1112017
13
NORMAL SLEEP
bull CHARACTERIZED BY A DECREASE IN
bull BODY TEMPERATURE
bull BLOOD PRESSURE
bull BREATHING RATE
bull MOST OTHER BODY FUNCTIONS
bull INCREASED NASAL RESISTANCE
bull CHARACTERIZED BY AN bull ACTIVE BRAIN
1112017
14
Copyright 2011 BRAEBON
Normal healthy breathing during sleep
Wake-up-gasping-choking-and-die-in-your-sleep-diseaserdquo ndash No sound during event
Who gets sent for a sleep study
1112017
15
Who usually doesnrsquot
Sleep apnoea is a common occurrence in femalesKarl A Franklin et al European Respiratory Journal August 2012
bull We investigated 400 females from a population-based random sample of 10000 females aged 20ndash70 years with a questionnaire and anovernight polysomnography
bull Obstructive sleep apnoea was found in 50 of females aged 20ndash70 years
bull Sleep apnoea was related to age obesity and hypertension but not to daytime sleepiness
bull Severe sleep apnoea was scored in 14 of females aged 55ndash70 years and in 31 of obese females with a body-mass index of gt30 kgmiddotmminus2 aged 50ndash70 years
1112017
16
EPWORTH SLEEPINESS SCALEINTERPRETATIONbull 0-7 IT IS UNLIKELY THAT YOU ARE ABNORMALLY SLEEPY
bull 8-9 YOU HAVE AN AVERAGE AMOUNT OF DAYTIME SLEEPINESS
bull 10-15 YOU MAY BE EXCESSIVELY SLEEPY DEPENDING ON THE SITUATION YOU MAY WANT TO CONSIDER SEEKING MEDICAL ATTENTION
bull 16-24 YOU ARE EXCESSIVELY SLEEPY AND SHOULD CONSIDER SEEKING MEDICAL ATTENTION
This person most likely is simply tired or had a bad nightrsquos sleep OSA is not
indicated
I referred this patient to a sleep physician
1112017
17
MALLAMPATI
1112017
18
Lavigne GJ Kato T Kolta A Sessle BJ Neurobiological mechanisms involved in sleep bruxism Crit Rev Oral Biol Med 20031430-46
bullSleep-related bruxism (SB) is characterized by the grinding or clenching of the teeth during sleep usually associated with sleep arousals although the incidence of sleep arousals in SB subjects is within the normal range (up to 14 arousalshour of sleep is considered normal)
IT HAS BEEN SHOWN THAT CPAP ELIMINATION OF OSA alsoELIMINATES SNORING
IT HAS NOT BEEN DEMONSTRATED THAT CPAP TREATMENT OF OSA
ELIMINATES OR REDUCES S-B
Neurobiological mechanisms involved in sleep bruxismLavigne GJ1 Kato T Kolta A Sessle BJ
bull Sleep bruxism (SB) is mainly associated with rhythmic masticatory muscle activity (RMMA) characterized by repetitive jaw muscle contractions (3 bursts or more at a frequency of 1 Hz)
bull The consequences of SB may include tooth destruction jaw pain headaches or the limitation of mandibular movement as well as tooth-grinding sounds that disrupt the sleep of bed partners RMMA is observed in 60 of normal sleepers
1112017
19
bull The pathophysiology of SB is becoming clearer
bull There is an abundance of evidence outlining the neurophysiology and neurochemistry of rhythmic jaw movements (RJM) in relation to chewing swallowing and breathing Several brainstem structures (eg reticular pontis oralis pontis caudalis) and neurochemicals (eg serotonin dopamine gamma aminobutyric acid [GABA] noradrenaline) are involved in both the genesis of RJM and the modulation of muscle tone during sleep
bull It creates a co-activation of both jaw-opening and jaw-closing muscles instead of the alternating jaw-opening and jaw-closing muscle activity pattern typical of chewing
Journal of Pain amp Symptom Management
bullPain duration and intensitywere correlated with decreased sleep impaired sleep quality and delayed sleep onset
Multiple Medical Studies
bullHave published that the majority (59 67 74) of OSA patients will not appropriately wear the CPAP
1112017
20
bull IN 1995 Johnny Cochran said ldquoIf the glove doesnrsquot fithellipyou must acquitrdquo As DR Dement intimated in the 1970s ldquoWe didnt know what to measurehellipso we measured everything we could think ofhellip and it stuckrdquo
bull Almost forty years later some of what ldquostuckrdquo is being revised reinterpreted and common sense is beginning to prevail Seven to eight hours of sleep per night is recommended
The Other 72 of Sleep
bull Sticking with the antiquated definition of a ldquocompliant userrdquo of a
CPAP (4 hrsnight and 5 nightsweek) one must use it roughly 28 of the time
bull WHAT ABOUT THE OTHER 72 OF SLEEP
bull Is it acceptable to not get the O2 we need simply because an antiquated standard ldquostuckrdquo
bull In 1995 CPAP became the gold standard Now in the 21st century I
say ldquoif the mask doesnrsquot fit hellipdonrsquot quitrdquo because an oral appliance may save your health and your life
Treatment of Sleep Apnea
Tracheotomy Oral
Surgery CPAPBiPAP
OA
Behavioral Modification
1112017
21
Orofacial Findings
bullThe most common orofacial characteristics include a retrognathic mandible narrow palate large neck circumference long soft palate tonsillar hypertrophy nasal septal deviation and relative macroglossia
Oral Appliances for Sleep Apnea amp Snoring
Tongue Retaining Devices Mandibular Repositioning Appliances
Oral Appliances (OA)
bull Properly fabricated an oral appliance will protrude the tongue and reposition the mandible anteriorly and inferiorly to the most beneficial neuromuscular position to prevent posterior airway collapse
bull This position is titratable and individualized to exact patient requirements and may need periodic adjustments just as does CPAP
1112017
22
BEFORE
APPLIANCE
7c
WITH
APPLIANCE
9 cc
1112017
23
Copyright 2011 BRAEBON
More Directly Related to hellipDental Sleep Medicine
bull EACH PATIENT IS AN INDIVIDUAL AND JUST AS CPAP PRESSURE IS INDIVIDUALLY TITRATEDhellipSO TOO ARE ORAL APPLIANCES
bull IF I DELIVER AN OA TO A PATIENT WHO WILL NOT UTILIZE THE CPAPhellipI WILL PROVIDE ONE OR SEVERAL HOME SLEEP STUDIES TO ASCERTAIN THE EFFICACY OF THE OAhellip AND THEN I REQUIRE THAT THEY RETURN TO THEIR SLEEP
bull DOCTOR FOR A SUBSEQUENT STUDY WHILE helliphelliphelliphelliphelliphelliphellipUTILIZINGTHE OA
Positional Apnea in a 73-Year Old Male with Atrial Fibrillation
bull This case study illustrates the cost-effective approach to successful outcomes associated with positional therapy that are not surprising and are consistent with a recent study which concluded ldquopositional therapy is equivalent to CPAP at normalizing the AHI in patients with positional OSA with similar effects on sleep quality and nocturnal oxygenationrdquo
bull Journal Sleep Diagnosis and Therapy
1112017
24
HOW THE ORAL APPLIANCE TREATS OSA
bull Prevent collapse of airwaybull Forward advancement of jawbull Support forward tongue positionbull Change shape of pharyngeal airwaybull Increase vertical dimension of occlusionbull Correct dysphagia bull Increase volume of space for tonguebull Trains protrusive tongue reflexesbull Alter position of hyoid bone relative to
mandible
THE VARYING ROLES OF THE NOSE AND MOUTH IN BREATHING
1112017
25
THE NOSE
bull A recent pediatric study reveals why addressing the tongue is so important for resolving sleep apnea As explained in this study having an abnormally short lingual frenulum can result in impaired orofacial growth in early childhood reducing the width of the upper airway
bull The upper airway is very pliable so this increases the risk of it collapsing during sleep They found that children with an untreated short frenulum developed abnormal tongue function early in life which also impacted their orofacial growth and led to disordered breathing during sleep
WHAT IS THE ROLE OF THE NOSE
ITS FUNCTIONS ARE VITAL
bull WARMING
bull HUMIDIFICATION
bull FILTERING
bull CLEANING
OF AMBIENT AIR INHALED INTO THE LUNGS
INFUSION OF NITRIC OXIDE
1112017
26
Humidification and
Dehumidification
bull During intake air is humidified to increase lung oxygen facilitation
bull Upon exhalation air is dehumidified to keep water in our cells
bull If this were not the case we would dehydrate unless we continually drank water
NARES
CONSTRICT
NARES FLARE
SNIFF TEST
1112017
27
Cosmetic Surgery
bullHe couldnrsquot breath through his small nose became hypercapnic and helliphelliphellipdied
Effect of treating severe nasal obstruction on the severity of obstructive sleep apnoea
bull HA McLean AM Urton HS Driver AKW Tan AG Day+ PW Munt and MF Fitzpatrick
bullThis study demonstrates that relief of severe nasal obstruction in patients with a normal retroglossal airway is associated with a significant reduction in mouth breathing during sleep improved sleep architecture and a modest improvement in OSA severity
1112017
28
bullThere are several novel aspects to these findings First the study documents a clearly increased upper airway resistance in association with oral breathing during stable sleep as compared with nasal breathing irrespective of central or OSA
bullSecondly this methodology included simultaneous documentation of oral and nasal ventilation during sleep to confirm the absence of any nasal airflow in the oral breathing condition and vice versa
1112017
29
bullThe substantially higher resistive load posed by the oral breathing route provides a plausible explanation for the observation that inhaled ventilation occurs almost exclusively via the nasal route during sleep in subjects with normal nasal resistance
bull Many studies have shown that nasal obstruction can induce or increase apnea frequency in OSA patients When nasal resistance is high a greater pressure drop is required to achieve the same flow and hence collapse of the pharynx is facilitated and this could mitigate the effect of mandibular advancement
bull Moreover high nasal resistance is associated with mouth breathing which could potentially limit the beneficial effect of mandibular advancement
bull Dental Appliance Treatment for Obstructive
bull Andrew S L Chan Richard W W Lee and Peter A Cistulli
bull httpchestjournalchestpubsorgcontent1322693fullhtml
1112017
30
bullCurrent evidence suggests that despite the superior efficacy of CPAP both treatments produce similar subjective and objective health benefits
bullThe superior self-reported tolerance and compliance associated with MAD treatment is a likely explanation
bullThe practice parameters of the AASM recommend the use of oral appliances for mild-to-moderate OSA or for patients with severe OSA who are unable to tolerate CPAP or refuse treatment with CPAP with a required written prescription by a sleep physician
The following are Medicare rules
1) A diagnosis of OSA is not within the dental scope of practice A dentist providing an OA
must do so under the and with the team effort of a licensed Physician with a written
prescription
2) A physician is not skilled in the intricacies of fabricating fitting monitoring adjusting
and choosing an appropriate Oral Appliance individualized per patient
3) A dentist may not provide an oral appliance if the patient has an active
Temporomandibular Disorder
4) The OA must be fabricated within 90 days of the patientrsquos appointment with the sleep
physician
Since the rules are clear and they involve both of our professions it would behoove
both DOMD and DDS to communicate for the benefit of OSA patients
1112017
31
Subsequent to my 3 hour 2013 Meeting with the US Department of Transportation regarding Truckers
bull During the State Board of Dental Examiners meeting Board members put sleep Dentistry in squarely back into the spotlight The Board has addressed sleep Dentistry issues in a public hearing and all four Board meetings in 2013
bull There was discussion that there can be a shared relationship between the Dental and medical scopes of practice
bull Under the proposed rule a Dentist may treat benign snoring with an oral appliance after referral to a licensed physician where appropriate within the standard of care By contrast a Dentist may not diagnose treat or monitor OSA without collaboration with a licensed physician Additionally an oral appliance shall only be fabricated by a licensed Dentist or by a Dental lab under a prescription or work order prepared by a Dentist
American Dental Association
bull Treatment using an oral appliance designed specifically to treat OSA should be fabricated by a dentist familiar with device design maintenance and therapeutic efficacy and who has an association with and a referral from a sleep team
bull JADA Vol 136 p 1123
Donrsquot be afraid of OSA Get a grip on the facts and save patientrsquos lives
1112017
32
bullA SYMBIOTIC RELATION BETWEEN PHYSICIANS SLEEP PROFESSIONALS AND DENTISTS CAN SIGNIFICANTLY IMPROVE THE SLEEP HEALTH OF MILLIONS OF PEOPLE EACH AND EVERY YEAR
bull THAT RELATIONSHIP IS NOT A ONE WAY STREET AND THE
American Sleep amp Breathing Academy of over 8000 members UNDERSTANDS THAThellip JUST LOOK AT THE MULTITUDE OF SLEEP PROFESSIONAL CATAGORIES ON THEIR BOARD OF DIRECTORS
THE END
Thank you for your interest I hope this presentation was helpful
Dr Richard Klein
1112017
4
Eye Symptoms of TMD
bullRetro-orbital pain
bullBlurred vision
bullLacrimation
bullDouble vision
bullPhotophobia
1112017
5
RETRO-ORBITAL PAIN
bull Gary Hack etal at the University of Maryland observed a new muscle which they named the SPHENOMANDIBULARIS The muscle was consistently observed as originating from the maxillary surface of the sphenoid bone and inserting on the temporal crest (internal oblique line) of the mandible Controversy exists as to it actually being a new and separate muscle However when tense it will pull on the sphenoid bone which is painful
TBI
I am not ashamed to
admit that the first
time I heard TBI in
our clinical rounds
I thought the speech
pathologist was
referring to tooth brush instructions
1112017
6
Conversely she was
confused when I
spoke of a jaw registration as
articulation
TBI and OSA
Approximately 17 million people sustain a traumatic brain injury (TBI) every year in the United States with 14 million seeking treatment 250000 hospitalizations and 50000 deaths are documented
bull Why are these studies important
bull They are pertinent because they show a direct link between traumatic brain injury and obstructive sleep apnea
bull Not diagnosing obstructive sleep apnea in someone who has sustained a brain injury could impede recovery and rehabilitation
bull As more and more soldiers are coming back from a war that has turned young men and women into mere glimpses of their former selves ndash and as more and more professional athletes especially football players are suffering from the lingering effects of the sport this link is becoming increasingly more important
1112017
7
Prevalence and Consequences of Sleep Disorders in Traumatic Brain Injury
bullThe authors reviewed evidence that cognitive dysfunction is a well known problem after TBI and is a major factor preventing return to independent living social readaptation and vocational pursuits Richard J Castriotta MD12 Mark C Wilde PsyD12 Jenny M Lai MD12 Strahil
Atanasov MD3 Brent E Masel MD4 and Samuel T Kuna MD56
Findings
bull 54 of that population had a normal polysomnography 46 had a sleep disorder (other studies have documented up to 23 had a SBD)
bull This is significantly higher that that of the general population
bull 23 had obstructive sleep apnea Again this finding is much higher than that of those who did or did not vote for our last President
ConclusionbullThe authors concluded that there was a high prevalence of sleep-disorders and excessive daytime sleepiness in individuals who had TBI and that consideration should be given to having all TBI patients evaluated for sleep disorders
1112017
8
Wersquoll discuss this later as it refers to pain
bullBut 1st letrsquos consider OSA since it is highly prevalent in your TBI patients
Sleep Apnea May Hasten Memory Loss and Alzheimers
bullPublished in the journal Neurology the study2 found that patients with sleep apnea andor snoring were diagnosed with mild cognitive impairment more than a decade earlier than those without sleep apnea
bull 2 Neurology April 15 2015
bullOn average those with untreated obstructed sleep apnea started experiencing cognitive impairment at the age of 77 compared to 90 among those without breathing problems
bullThose who used a CPAP machine to address their sleep apnea started declining mentally at the same age as those who did not have sleep apnea
1112017
9
Scary video by WatchPAT
Obstructive SleepApnea
Definition of Sleep apnea
bullSleep Apnea occurs when the soft tissue in your mouth (the tongue tonsils pharynx uvula etc) relax too much and collapse at the back of your throat and cut off the airway making it difficult or impossible to breath
AHI Three levels of severity
Mild 5 to 15 times per hour
Moderate 15 to 30 times per hour
Severe gt30 times per hour
Copyright 2011 Braebon
1112017
10
SLEEP APNEA SYMPTOMS
bull Short term memory problems
bull Weight gain
bull Tiredness
bull Dry mouth
bull Sore throat
bull Slow metabolism
bull Bed partner frustration
bull AND A PLETHORA OF SERIOUS MEDICAL DISEASES DISORDERS AND MALADIES
High blood pressure
Heart failure
Heart rhythm disturbances
Atherosclerotic heart disease
Pulmonary hypertension
Insulin resistance
Sudden death
Erectile dysfunction
Memory problems
Depression
Anxiety
Gastroesophageal reflux
Sleep Apnea Increases Risk of
bull It has been estimated that 80 of depressed patients complain of disturbed sleep and sleeplessness is a risk factor for impaired mood
bull helliphelliphelliphelliphelliphelliphelliphellip The most common complaint of helliphelliphelliphelliphelliphelliphelliphellip PTSD is sleeplessness and 50 -helliphelliphelliphelliphelliphelliphelliphellip 70 of chronic pain patients helliphelliphelliphelliphelliphelliphelliphelliphellip report disturbed sleep
Consequences
1112017
11
Headachesbull Headaches are the most commonly reported pain complaint in the
population (textbook of pain)
bull Sleep disorders such as sleep apnea are found among headache patients at rates greater than what is found in the general population TX of sleep disorders decreases headache complaints Cephalgia is the most common complaint of TMD
bull (Archives of Internal Medicine)
Risk Factors
ObesityLarge neckSnoringNon-restorative sleepDaytime sleepinessfatigueHigh arched palateRetrognathiaCrowded airwaySmokingdrinking
(and remember sleep apnea occurs in women children and skinny guys toohellipthese are just risk factors)
Life Cycle of a LEAF
1112017
12
The cells in our body deteriorate as we age but they do so much quicker without oxygen
The Beatles were only partially correct when they sang
ldquoAll you need is loverdquo
The Hollies had a better understanding of life when they sangrdquo
ldquoAll I need is the air that I breath and to love yourdquo
1112017
13
NORMAL SLEEP
bull CHARACTERIZED BY A DECREASE IN
bull BODY TEMPERATURE
bull BLOOD PRESSURE
bull BREATHING RATE
bull MOST OTHER BODY FUNCTIONS
bull INCREASED NASAL RESISTANCE
bull CHARACTERIZED BY AN bull ACTIVE BRAIN
1112017
14
Copyright 2011 BRAEBON
Normal healthy breathing during sleep
Wake-up-gasping-choking-and-die-in-your-sleep-diseaserdquo ndash No sound during event
Who gets sent for a sleep study
1112017
15
Who usually doesnrsquot
Sleep apnoea is a common occurrence in femalesKarl A Franklin et al European Respiratory Journal August 2012
bull We investigated 400 females from a population-based random sample of 10000 females aged 20ndash70 years with a questionnaire and anovernight polysomnography
bull Obstructive sleep apnoea was found in 50 of females aged 20ndash70 years
bull Sleep apnoea was related to age obesity and hypertension but not to daytime sleepiness
bull Severe sleep apnoea was scored in 14 of females aged 55ndash70 years and in 31 of obese females with a body-mass index of gt30 kgmiddotmminus2 aged 50ndash70 years
1112017
16
EPWORTH SLEEPINESS SCALEINTERPRETATIONbull 0-7 IT IS UNLIKELY THAT YOU ARE ABNORMALLY SLEEPY
bull 8-9 YOU HAVE AN AVERAGE AMOUNT OF DAYTIME SLEEPINESS
bull 10-15 YOU MAY BE EXCESSIVELY SLEEPY DEPENDING ON THE SITUATION YOU MAY WANT TO CONSIDER SEEKING MEDICAL ATTENTION
bull 16-24 YOU ARE EXCESSIVELY SLEEPY AND SHOULD CONSIDER SEEKING MEDICAL ATTENTION
This person most likely is simply tired or had a bad nightrsquos sleep OSA is not
indicated
I referred this patient to a sleep physician
1112017
17
MALLAMPATI
1112017
18
Lavigne GJ Kato T Kolta A Sessle BJ Neurobiological mechanisms involved in sleep bruxism Crit Rev Oral Biol Med 20031430-46
bullSleep-related bruxism (SB) is characterized by the grinding or clenching of the teeth during sleep usually associated with sleep arousals although the incidence of sleep arousals in SB subjects is within the normal range (up to 14 arousalshour of sleep is considered normal)
IT HAS BEEN SHOWN THAT CPAP ELIMINATION OF OSA alsoELIMINATES SNORING
IT HAS NOT BEEN DEMONSTRATED THAT CPAP TREATMENT OF OSA
ELIMINATES OR REDUCES S-B
Neurobiological mechanisms involved in sleep bruxismLavigne GJ1 Kato T Kolta A Sessle BJ
bull Sleep bruxism (SB) is mainly associated with rhythmic masticatory muscle activity (RMMA) characterized by repetitive jaw muscle contractions (3 bursts or more at a frequency of 1 Hz)
bull The consequences of SB may include tooth destruction jaw pain headaches or the limitation of mandibular movement as well as tooth-grinding sounds that disrupt the sleep of bed partners RMMA is observed in 60 of normal sleepers
1112017
19
bull The pathophysiology of SB is becoming clearer
bull There is an abundance of evidence outlining the neurophysiology and neurochemistry of rhythmic jaw movements (RJM) in relation to chewing swallowing and breathing Several brainstem structures (eg reticular pontis oralis pontis caudalis) and neurochemicals (eg serotonin dopamine gamma aminobutyric acid [GABA] noradrenaline) are involved in both the genesis of RJM and the modulation of muscle tone during sleep
bull It creates a co-activation of both jaw-opening and jaw-closing muscles instead of the alternating jaw-opening and jaw-closing muscle activity pattern typical of chewing
Journal of Pain amp Symptom Management
bullPain duration and intensitywere correlated with decreased sleep impaired sleep quality and delayed sleep onset
Multiple Medical Studies
bullHave published that the majority (59 67 74) of OSA patients will not appropriately wear the CPAP
1112017
20
bull IN 1995 Johnny Cochran said ldquoIf the glove doesnrsquot fithellipyou must acquitrdquo As DR Dement intimated in the 1970s ldquoWe didnt know what to measurehellipso we measured everything we could think ofhellip and it stuckrdquo
bull Almost forty years later some of what ldquostuckrdquo is being revised reinterpreted and common sense is beginning to prevail Seven to eight hours of sleep per night is recommended
The Other 72 of Sleep
bull Sticking with the antiquated definition of a ldquocompliant userrdquo of a
CPAP (4 hrsnight and 5 nightsweek) one must use it roughly 28 of the time
bull WHAT ABOUT THE OTHER 72 OF SLEEP
bull Is it acceptable to not get the O2 we need simply because an antiquated standard ldquostuckrdquo
bull In 1995 CPAP became the gold standard Now in the 21st century I
say ldquoif the mask doesnrsquot fit hellipdonrsquot quitrdquo because an oral appliance may save your health and your life
Treatment of Sleep Apnea
Tracheotomy Oral
Surgery CPAPBiPAP
OA
Behavioral Modification
1112017
21
Orofacial Findings
bullThe most common orofacial characteristics include a retrognathic mandible narrow palate large neck circumference long soft palate tonsillar hypertrophy nasal septal deviation and relative macroglossia
Oral Appliances for Sleep Apnea amp Snoring
Tongue Retaining Devices Mandibular Repositioning Appliances
Oral Appliances (OA)
bull Properly fabricated an oral appliance will protrude the tongue and reposition the mandible anteriorly and inferiorly to the most beneficial neuromuscular position to prevent posterior airway collapse
bull This position is titratable and individualized to exact patient requirements and may need periodic adjustments just as does CPAP
1112017
22
BEFORE
APPLIANCE
7c
WITH
APPLIANCE
9 cc
1112017
23
Copyright 2011 BRAEBON
More Directly Related to hellipDental Sleep Medicine
bull EACH PATIENT IS AN INDIVIDUAL AND JUST AS CPAP PRESSURE IS INDIVIDUALLY TITRATEDhellipSO TOO ARE ORAL APPLIANCES
bull IF I DELIVER AN OA TO A PATIENT WHO WILL NOT UTILIZE THE CPAPhellipI WILL PROVIDE ONE OR SEVERAL HOME SLEEP STUDIES TO ASCERTAIN THE EFFICACY OF THE OAhellip AND THEN I REQUIRE THAT THEY RETURN TO THEIR SLEEP
bull DOCTOR FOR A SUBSEQUENT STUDY WHILE helliphelliphelliphelliphelliphelliphellipUTILIZINGTHE OA
Positional Apnea in a 73-Year Old Male with Atrial Fibrillation
bull This case study illustrates the cost-effective approach to successful outcomes associated with positional therapy that are not surprising and are consistent with a recent study which concluded ldquopositional therapy is equivalent to CPAP at normalizing the AHI in patients with positional OSA with similar effects on sleep quality and nocturnal oxygenationrdquo
bull Journal Sleep Diagnosis and Therapy
1112017
24
HOW THE ORAL APPLIANCE TREATS OSA
bull Prevent collapse of airwaybull Forward advancement of jawbull Support forward tongue positionbull Change shape of pharyngeal airwaybull Increase vertical dimension of occlusionbull Correct dysphagia bull Increase volume of space for tonguebull Trains protrusive tongue reflexesbull Alter position of hyoid bone relative to
mandible
THE VARYING ROLES OF THE NOSE AND MOUTH IN BREATHING
1112017
25
THE NOSE
bull A recent pediatric study reveals why addressing the tongue is so important for resolving sleep apnea As explained in this study having an abnormally short lingual frenulum can result in impaired orofacial growth in early childhood reducing the width of the upper airway
bull The upper airway is very pliable so this increases the risk of it collapsing during sleep They found that children with an untreated short frenulum developed abnormal tongue function early in life which also impacted their orofacial growth and led to disordered breathing during sleep
WHAT IS THE ROLE OF THE NOSE
ITS FUNCTIONS ARE VITAL
bull WARMING
bull HUMIDIFICATION
bull FILTERING
bull CLEANING
OF AMBIENT AIR INHALED INTO THE LUNGS
INFUSION OF NITRIC OXIDE
1112017
26
Humidification and
Dehumidification
bull During intake air is humidified to increase lung oxygen facilitation
bull Upon exhalation air is dehumidified to keep water in our cells
bull If this were not the case we would dehydrate unless we continually drank water
NARES
CONSTRICT
NARES FLARE
SNIFF TEST
1112017
27
Cosmetic Surgery
bullHe couldnrsquot breath through his small nose became hypercapnic and helliphelliphellipdied
Effect of treating severe nasal obstruction on the severity of obstructive sleep apnoea
bull HA McLean AM Urton HS Driver AKW Tan AG Day+ PW Munt and MF Fitzpatrick
bullThis study demonstrates that relief of severe nasal obstruction in patients with a normal retroglossal airway is associated with a significant reduction in mouth breathing during sleep improved sleep architecture and a modest improvement in OSA severity
1112017
28
bullThere are several novel aspects to these findings First the study documents a clearly increased upper airway resistance in association with oral breathing during stable sleep as compared with nasal breathing irrespective of central or OSA
bullSecondly this methodology included simultaneous documentation of oral and nasal ventilation during sleep to confirm the absence of any nasal airflow in the oral breathing condition and vice versa
1112017
29
bullThe substantially higher resistive load posed by the oral breathing route provides a plausible explanation for the observation that inhaled ventilation occurs almost exclusively via the nasal route during sleep in subjects with normal nasal resistance
bull Many studies have shown that nasal obstruction can induce or increase apnea frequency in OSA patients When nasal resistance is high a greater pressure drop is required to achieve the same flow and hence collapse of the pharynx is facilitated and this could mitigate the effect of mandibular advancement
bull Moreover high nasal resistance is associated with mouth breathing which could potentially limit the beneficial effect of mandibular advancement
bull Dental Appliance Treatment for Obstructive
bull Andrew S L Chan Richard W W Lee and Peter A Cistulli
bull httpchestjournalchestpubsorgcontent1322693fullhtml
1112017
30
bullCurrent evidence suggests that despite the superior efficacy of CPAP both treatments produce similar subjective and objective health benefits
bullThe superior self-reported tolerance and compliance associated with MAD treatment is a likely explanation
bullThe practice parameters of the AASM recommend the use of oral appliances for mild-to-moderate OSA or for patients with severe OSA who are unable to tolerate CPAP or refuse treatment with CPAP with a required written prescription by a sleep physician
The following are Medicare rules
1) A diagnosis of OSA is not within the dental scope of practice A dentist providing an OA
must do so under the and with the team effort of a licensed Physician with a written
prescription
2) A physician is not skilled in the intricacies of fabricating fitting monitoring adjusting
and choosing an appropriate Oral Appliance individualized per patient
3) A dentist may not provide an oral appliance if the patient has an active
Temporomandibular Disorder
4) The OA must be fabricated within 90 days of the patientrsquos appointment with the sleep
physician
Since the rules are clear and they involve both of our professions it would behoove
both DOMD and DDS to communicate for the benefit of OSA patients
1112017
31
Subsequent to my 3 hour 2013 Meeting with the US Department of Transportation regarding Truckers
bull During the State Board of Dental Examiners meeting Board members put sleep Dentistry in squarely back into the spotlight The Board has addressed sleep Dentistry issues in a public hearing and all four Board meetings in 2013
bull There was discussion that there can be a shared relationship between the Dental and medical scopes of practice
bull Under the proposed rule a Dentist may treat benign snoring with an oral appliance after referral to a licensed physician where appropriate within the standard of care By contrast a Dentist may not diagnose treat or monitor OSA without collaboration with a licensed physician Additionally an oral appliance shall only be fabricated by a licensed Dentist or by a Dental lab under a prescription or work order prepared by a Dentist
American Dental Association
bull Treatment using an oral appliance designed specifically to treat OSA should be fabricated by a dentist familiar with device design maintenance and therapeutic efficacy and who has an association with and a referral from a sleep team
bull JADA Vol 136 p 1123
Donrsquot be afraid of OSA Get a grip on the facts and save patientrsquos lives
1112017
32
bullA SYMBIOTIC RELATION BETWEEN PHYSICIANS SLEEP PROFESSIONALS AND DENTISTS CAN SIGNIFICANTLY IMPROVE THE SLEEP HEALTH OF MILLIONS OF PEOPLE EACH AND EVERY YEAR
bull THAT RELATIONSHIP IS NOT A ONE WAY STREET AND THE
American Sleep amp Breathing Academy of over 8000 members UNDERSTANDS THAThellip JUST LOOK AT THE MULTITUDE OF SLEEP PROFESSIONAL CATAGORIES ON THEIR BOARD OF DIRECTORS
THE END
Thank you for your interest I hope this presentation was helpful
Dr Richard Klein
1112017
5
RETRO-ORBITAL PAIN
bull Gary Hack etal at the University of Maryland observed a new muscle which they named the SPHENOMANDIBULARIS The muscle was consistently observed as originating from the maxillary surface of the sphenoid bone and inserting on the temporal crest (internal oblique line) of the mandible Controversy exists as to it actually being a new and separate muscle However when tense it will pull on the sphenoid bone which is painful
TBI
I am not ashamed to
admit that the first
time I heard TBI in
our clinical rounds
I thought the speech
pathologist was
referring to tooth brush instructions
1112017
6
Conversely she was
confused when I
spoke of a jaw registration as
articulation
TBI and OSA
Approximately 17 million people sustain a traumatic brain injury (TBI) every year in the United States with 14 million seeking treatment 250000 hospitalizations and 50000 deaths are documented
bull Why are these studies important
bull They are pertinent because they show a direct link between traumatic brain injury and obstructive sleep apnea
bull Not diagnosing obstructive sleep apnea in someone who has sustained a brain injury could impede recovery and rehabilitation
bull As more and more soldiers are coming back from a war that has turned young men and women into mere glimpses of their former selves ndash and as more and more professional athletes especially football players are suffering from the lingering effects of the sport this link is becoming increasingly more important
1112017
7
Prevalence and Consequences of Sleep Disorders in Traumatic Brain Injury
bullThe authors reviewed evidence that cognitive dysfunction is a well known problem after TBI and is a major factor preventing return to independent living social readaptation and vocational pursuits Richard J Castriotta MD12 Mark C Wilde PsyD12 Jenny M Lai MD12 Strahil
Atanasov MD3 Brent E Masel MD4 and Samuel T Kuna MD56
Findings
bull 54 of that population had a normal polysomnography 46 had a sleep disorder (other studies have documented up to 23 had a SBD)
bull This is significantly higher that that of the general population
bull 23 had obstructive sleep apnea Again this finding is much higher than that of those who did or did not vote for our last President
ConclusionbullThe authors concluded that there was a high prevalence of sleep-disorders and excessive daytime sleepiness in individuals who had TBI and that consideration should be given to having all TBI patients evaluated for sleep disorders
1112017
8
Wersquoll discuss this later as it refers to pain
bullBut 1st letrsquos consider OSA since it is highly prevalent in your TBI patients
Sleep Apnea May Hasten Memory Loss and Alzheimers
bullPublished in the journal Neurology the study2 found that patients with sleep apnea andor snoring were diagnosed with mild cognitive impairment more than a decade earlier than those without sleep apnea
bull 2 Neurology April 15 2015
bullOn average those with untreated obstructed sleep apnea started experiencing cognitive impairment at the age of 77 compared to 90 among those without breathing problems
bullThose who used a CPAP machine to address their sleep apnea started declining mentally at the same age as those who did not have sleep apnea
1112017
9
Scary video by WatchPAT
Obstructive SleepApnea
Definition of Sleep apnea
bullSleep Apnea occurs when the soft tissue in your mouth (the tongue tonsils pharynx uvula etc) relax too much and collapse at the back of your throat and cut off the airway making it difficult or impossible to breath
AHI Three levels of severity
Mild 5 to 15 times per hour
Moderate 15 to 30 times per hour
Severe gt30 times per hour
Copyright 2011 Braebon
1112017
10
SLEEP APNEA SYMPTOMS
bull Short term memory problems
bull Weight gain
bull Tiredness
bull Dry mouth
bull Sore throat
bull Slow metabolism
bull Bed partner frustration
bull AND A PLETHORA OF SERIOUS MEDICAL DISEASES DISORDERS AND MALADIES
High blood pressure
Heart failure
Heart rhythm disturbances
Atherosclerotic heart disease
Pulmonary hypertension
Insulin resistance
Sudden death
Erectile dysfunction
Memory problems
Depression
Anxiety
Gastroesophageal reflux
Sleep Apnea Increases Risk of
bull It has been estimated that 80 of depressed patients complain of disturbed sleep and sleeplessness is a risk factor for impaired mood
bull helliphelliphelliphelliphelliphelliphelliphellip The most common complaint of helliphelliphelliphelliphelliphelliphelliphellip PTSD is sleeplessness and 50 -helliphelliphelliphelliphelliphelliphelliphellip 70 of chronic pain patients helliphelliphelliphelliphelliphelliphelliphelliphellip report disturbed sleep
Consequences
1112017
11
Headachesbull Headaches are the most commonly reported pain complaint in the
population (textbook of pain)
bull Sleep disorders such as sleep apnea are found among headache patients at rates greater than what is found in the general population TX of sleep disorders decreases headache complaints Cephalgia is the most common complaint of TMD
bull (Archives of Internal Medicine)
Risk Factors
ObesityLarge neckSnoringNon-restorative sleepDaytime sleepinessfatigueHigh arched palateRetrognathiaCrowded airwaySmokingdrinking
(and remember sleep apnea occurs in women children and skinny guys toohellipthese are just risk factors)
Life Cycle of a LEAF
1112017
12
The cells in our body deteriorate as we age but they do so much quicker without oxygen
The Beatles were only partially correct when they sang
ldquoAll you need is loverdquo
The Hollies had a better understanding of life when they sangrdquo
ldquoAll I need is the air that I breath and to love yourdquo
1112017
13
NORMAL SLEEP
bull CHARACTERIZED BY A DECREASE IN
bull BODY TEMPERATURE
bull BLOOD PRESSURE
bull BREATHING RATE
bull MOST OTHER BODY FUNCTIONS
bull INCREASED NASAL RESISTANCE
bull CHARACTERIZED BY AN bull ACTIVE BRAIN
1112017
14
Copyright 2011 BRAEBON
Normal healthy breathing during sleep
Wake-up-gasping-choking-and-die-in-your-sleep-diseaserdquo ndash No sound during event
Who gets sent for a sleep study
1112017
15
Who usually doesnrsquot
Sleep apnoea is a common occurrence in femalesKarl A Franklin et al European Respiratory Journal August 2012
bull We investigated 400 females from a population-based random sample of 10000 females aged 20ndash70 years with a questionnaire and anovernight polysomnography
bull Obstructive sleep apnoea was found in 50 of females aged 20ndash70 years
bull Sleep apnoea was related to age obesity and hypertension but not to daytime sleepiness
bull Severe sleep apnoea was scored in 14 of females aged 55ndash70 years and in 31 of obese females with a body-mass index of gt30 kgmiddotmminus2 aged 50ndash70 years
1112017
16
EPWORTH SLEEPINESS SCALEINTERPRETATIONbull 0-7 IT IS UNLIKELY THAT YOU ARE ABNORMALLY SLEEPY
bull 8-9 YOU HAVE AN AVERAGE AMOUNT OF DAYTIME SLEEPINESS
bull 10-15 YOU MAY BE EXCESSIVELY SLEEPY DEPENDING ON THE SITUATION YOU MAY WANT TO CONSIDER SEEKING MEDICAL ATTENTION
bull 16-24 YOU ARE EXCESSIVELY SLEEPY AND SHOULD CONSIDER SEEKING MEDICAL ATTENTION
This person most likely is simply tired or had a bad nightrsquos sleep OSA is not
indicated
I referred this patient to a sleep physician
1112017
17
MALLAMPATI
1112017
18
Lavigne GJ Kato T Kolta A Sessle BJ Neurobiological mechanisms involved in sleep bruxism Crit Rev Oral Biol Med 20031430-46
bullSleep-related bruxism (SB) is characterized by the grinding or clenching of the teeth during sleep usually associated with sleep arousals although the incidence of sleep arousals in SB subjects is within the normal range (up to 14 arousalshour of sleep is considered normal)
IT HAS BEEN SHOWN THAT CPAP ELIMINATION OF OSA alsoELIMINATES SNORING
IT HAS NOT BEEN DEMONSTRATED THAT CPAP TREATMENT OF OSA
ELIMINATES OR REDUCES S-B
Neurobiological mechanisms involved in sleep bruxismLavigne GJ1 Kato T Kolta A Sessle BJ
bull Sleep bruxism (SB) is mainly associated with rhythmic masticatory muscle activity (RMMA) characterized by repetitive jaw muscle contractions (3 bursts or more at a frequency of 1 Hz)
bull The consequences of SB may include tooth destruction jaw pain headaches or the limitation of mandibular movement as well as tooth-grinding sounds that disrupt the sleep of bed partners RMMA is observed in 60 of normal sleepers
1112017
19
bull The pathophysiology of SB is becoming clearer
bull There is an abundance of evidence outlining the neurophysiology and neurochemistry of rhythmic jaw movements (RJM) in relation to chewing swallowing and breathing Several brainstem structures (eg reticular pontis oralis pontis caudalis) and neurochemicals (eg serotonin dopamine gamma aminobutyric acid [GABA] noradrenaline) are involved in both the genesis of RJM and the modulation of muscle tone during sleep
bull It creates a co-activation of both jaw-opening and jaw-closing muscles instead of the alternating jaw-opening and jaw-closing muscle activity pattern typical of chewing
Journal of Pain amp Symptom Management
bullPain duration and intensitywere correlated with decreased sleep impaired sleep quality and delayed sleep onset
Multiple Medical Studies
bullHave published that the majority (59 67 74) of OSA patients will not appropriately wear the CPAP
1112017
20
bull IN 1995 Johnny Cochran said ldquoIf the glove doesnrsquot fithellipyou must acquitrdquo As DR Dement intimated in the 1970s ldquoWe didnt know what to measurehellipso we measured everything we could think ofhellip and it stuckrdquo
bull Almost forty years later some of what ldquostuckrdquo is being revised reinterpreted and common sense is beginning to prevail Seven to eight hours of sleep per night is recommended
The Other 72 of Sleep
bull Sticking with the antiquated definition of a ldquocompliant userrdquo of a
CPAP (4 hrsnight and 5 nightsweek) one must use it roughly 28 of the time
bull WHAT ABOUT THE OTHER 72 OF SLEEP
bull Is it acceptable to not get the O2 we need simply because an antiquated standard ldquostuckrdquo
bull In 1995 CPAP became the gold standard Now in the 21st century I
say ldquoif the mask doesnrsquot fit hellipdonrsquot quitrdquo because an oral appliance may save your health and your life
Treatment of Sleep Apnea
Tracheotomy Oral
Surgery CPAPBiPAP
OA
Behavioral Modification
1112017
21
Orofacial Findings
bullThe most common orofacial characteristics include a retrognathic mandible narrow palate large neck circumference long soft palate tonsillar hypertrophy nasal septal deviation and relative macroglossia
Oral Appliances for Sleep Apnea amp Snoring
Tongue Retaining Devices Mandibular Repositioning Appliances
Oral Appliances (OA)
bull Properly fabricated an oral appliance will protrude the tongue and reposition the mandible anteriorly and inferiorly to the most beneficial neuromuscular position to prevent posterior airway collapse
bull This position is titratable and individualized to exact patient requirements and may need periodic adjustments just as does CPAP
1112017
22
BEFORE
APPLIANCE
7c
WITH
APPLIANCE
9 cc
1112017
23
Copyright 2011 BRAEBON
More Directly Related to hellipDental Sleep Medicine
bull EACH PATIENT IS AN INDIVIDUAL AND JUST AS CPAP PRESSURE IS INDIVIDUALLY TITRATEDhellipSO TOO ARE ORAL APPLIANCES
bull IF I DELIVER AN OA TO A PATIENT WHO WILL NOT UTILIZE THE CPAPhellipI WILL PROVIDE ONE OR SEVERAL HOME SLEEP STUDIES TO ASCERTAIN THE EFFICACY OF THE OAhellip AND THEN I REQUIRE THAT THEY RETURN TO THEIR SLEEP
bull DOCTOR FOR A SUBSEQUENT STUDY WHILE helliphelliphelliphelliphelliphelliphellipUTILIZINGTHE OA
Positional Apnea in a 73-Year Old Male with Atrial Fibrillation
bull This case study illustrates the cost-effective approach to successful outcomes associated with positional therapy that are not surprising and are consistent with a recent study which concluded ldquopositional therapy is equivalent to CPAP at normalizing the AHI in patients with positional OSA with similar effects on sleep quality and nocturnal oxygenationrdquo
bull Journal Sleep Diagnosis and Therapy
1112017
24
HOW THE ORAL APPLIANCE TREATS OSA
bull Prevent collapse of airwaybull Forward advancement of jawbull Support forward tongue positionbull Change shape of pharyngeal airwaybull Increase vertical dimension of occlusionbull Correct dysphagia bull Increase volume of space for tonguebull Trains protrusive tongue reflexesbull Alter position of hyoid bone relative to
mandible
THE VARYING ROLES OF THE NOSE AND MOUTH IN BREATHING
1112017
25
THE NOSE
bull A recent pediatric study reveals why addressing the tongue is so important for resolving sleep apnea As explained in this study having an abnormally short lingual frenulum can result in impaired orofacial growth in early childhood reducing the width of the upper airway
bull The upper airway is very pliable so this increases the risk of it collapsing during sleep They found that children with an untreated short frenulum developed abnormal tongue function early in life which also impacted their orofacial growth and led to disordered breathing during sleep
WHAT IS THE ROLE OF THE NOSE
ITS FUNCTIONS ARE VITAL
bull WARMING
bull HUMIDIFICATION
bull FILTERING
bull CLEANING
OF AMBIENT AIR INHALED INTO THE LUNGS
INFUSION OF NITRIC OXIDE
1112017
26
Humidification and
Dehumidification
bull During intake air is humidified to increase lung oxygen facilitation
bull Upon exhalation air is dehumidified to keep water in our cells
bull If this were not the case we would dehydrate unless we continually drank water
NARES
CONSTRICT
NARES FLARE
SNIFF TEST
1112017
27
Cosmetic Surgery
bullHe couldnrsquot breath through his small nose became hypercapnic and helliphelliphellipdied
Effect of treating severe nasal obstruction on the severity of obstructive sleep apnoea
bull HA McLean AM Urton HS Driver AKW Tan AG Day+ PW Munt and MF Fitzpatrick
bullThis study demonstrates that relief of severe nasal obstruction in patients with a normal retroglossal airway is associated with a significant reduction in mouth breathing during sleep improved sleep architecture and a modest improvement in OSA severity
1112017
28
bullThere are several novel aspects to these findings First the study documents a clearly increased upper airway resistance in association with oral breathing during stable sleep as compared with nasal breathing irrespective of central or OSA
bullSecondly this methodology included simultaneous documentation of oral and nasal ventilation during sleep to confirm the absence of any nasal airflow in the oral breathing condition and vice versa
1112017
29
bullThe substantially higher resistive load posed by the oral breathing route provides a plausible explanation for the observation that inhaled ventilation occurs almost exclusively via the nasal route during sleep in subjects with normal nasal resistance
bull Many studies have shown that nasal obstruction can induce or increase apnea frequency in OSA patients When nasal resistance is high a greater pressure drop is required to achieve the same flow and hence collapse of the pharynx is facilitated and this could mitigate the effect of mandibular advancement
bull Moreover high nasal resistance is associated with mouth breathing which could potentially limit the beneficial effect of mandibular advancement
bull Dental Appliance Treatment for Obstructive
bull Andrew S L Chan Richard W W Lee and Peter A Cistulli
bull httpchestjournalchestpubsorgcontent1322693fullhtml
1112017
30
bullCurrent evidence suggests that despite the superior efficacy of CPAP both treatments produce similar subjective and objective health benefits
bullThe superior self-reported tolerance and compliance associated with MAD treatment is a likely explanation
bullThe practice parameters of the AASM recommend the use of oral appliances for mild-to-moderate OSA or for patients with severe OSA who are unable to tolerate CPAP or refuse treatment with CPAP with a required written prescription by a sleep physician
The following are Medicare rules
1) A diagnosis of OSA is not within the dental scope of practice A dentist providing an OA
must do so under the and with the team effort of a licensed Physician with a written
prescription
2) A physician is not skilled in the intricacies of fabricating fitting monitoring adjusting
and choosing an appropriate Oral Appliance individualized per patient
3) A dentist may not provide an oral appliance if the patient has an active
Temporomandibular Disorder
4) The OA must be fabricated within 90 days of the patientrsquos appointment with the sleep
physician
Since the rules are clear and they involve both of our professions it would behoove
both DOMD and DDS to communicate for the benefit of OSA patients
1112017
31
Subsequent to my 3 hour 2013 Meeting with the US Department of Transportation regarding Truckers
bull During the State Board of Dental Examiners meeting Board members put sleep Dentistry in squarely back into the spotlight The Board has addressed sleep Dentistry issues in a public hearing and all four Board meetings in 2013
bull There was discussion that there can be a shared relationship between the Dental and medical scopes of practice
bull Under the proposed rule a Dentist may treat benign snoring with an oral appliance after referral to a licensed physician where appropriate within the standard of care By contrast a Dentist may not diagnose treat or monitor OSA without collaboration with a licensed physician Additionally an oral appliance shall only be fabricated by a licensed Dentist or by a Dental lab under a prescription or work order prepared by a Dentist
American Dental Association
bull Treatment using an oral appliance designed specifically to treat OSA should be fabricated by a dentist familiar with device design maintenance and therapeutic efficacy and who has an association with and a referral from a sleep team
bull JADA Vol 136 p 1123
Donrsquot be afraid of OSA Get a grip on the facts and save patientrsquos lives
1112017
32
bullA SYMBIOTIC RELATION BETWEEN PHYSICIANS SLEEP PROFESSIONALS AND DENTISTS CAN SIGNIFICANTLY IMPROVE THE SLEEP HEALTH OF MILLIONS OF PEOPLE EACH AND EVERY YEAR
bull THAT RELATIONSHIP IS NOT A ONE WAY STREET AND THE
American Sleep amp Breathing Academy of over 8000 members UNDERSTANDS THAThellip JUST LOOK AT THE MULTITUDE OF SLEEP PROFESSIONAL CATAGORIES ON THEIR BOARD OF DIRECTORS
THE END
Thank you for your interest I hope this presentation was helpful
Dr Richard Klein
1112017
6
Conversely she was
confused when I
spoke of a jaw registration as
articulation
TBI and OSA
Approximately 17 million people sustain a traumatic brain injury (TBI) every year in the United States with 14 million seeking treatment 250000 hospitalizations and 50000 deaths are documented
bull Why are these studies important
bull They are pertinent because they show a direct link between traumatic brain injury and obstructive sleep apnea
bull Not diagnosing obstructive sleep apnea in someone who has sustained a brain injury could impede recovery and rehabilitation
bull As more and more soldiers are coming back from a war that has turned young men and women into mere glimpses of their former selves ndash and as more and more professional athletes especially football players are suffering from the lingering effects of the sport this link is becoming increasingly more important
1112017
7
Prevalence and Consequences of Sleep Disorders in Traumatic Brain Injury
bullThe authors reviewed evidence that cognitive dysfunction is a well known problem after TBI and is a major factor preventing return to independent living social readaptation and vocational pursuits Richard J Castriotta MD12 Mark C Wilde PsyD12 Jenny M Lai MD12 Strahil
Atanasov MD3 Brent E Masel MD4 and Samuel T Kuna MD56
Findings
bull 54 of that population had a normal polysomnography 46 had a sleep disorder (other studies have documented up to 23 had a SBD)
bull This is significantly higher that that of the general population
bull 23 had obstructive sleep apnea Again this finding is much higher than that of those who did or did not vote for our last President
ConclusionbullThe authors concluded that there was a high prevalence of sleep-disorders and excessive daytime sleepiness in individuals who had TBI and that consideration should be given to having all TBI patients evaluated for sleep disorders
1112017
8
Wersquoll discuss this later as it refers to pain
bullBut 1st letrsquos consider OSA since it is highly prevalent in your TBI patients
Sleep Apnea May Hasten Memory Loss and Alzheimers
bullPublished in the journal Neurology the study2 found that patients with sleep apnea andor snoring were diagnosed with mild cognitive impairment more than a decade earlier than those without sleep apnea
bull 2 Neurology April 15 2015
bullOn average those with untreated obstructed sleep apnea started experiencing cognitive impairment at the age of 77 compared to 90 among those without breathing problems
bullThose who used a CPAP machine to address their sleep apnea started declining mentally at the same age as those who did not have sleep apnea
1112017
9
Scary video by WatchPAT
Obstructive SleepApnea
Definition of Sleep apnea
bullSleep Apnea occurs when the soft tissue in your mouth (the tongue tonsils pharynx uvula etc) relax too much and collapse at the back of your throat and cut off the airway making it difficult or impossible to breath
AHI Three levels of severity
Mild 5 to 15 times per hour
Moderate 15 to 30 times per hour
Severe gt30 times per hour
Copyright 2011 Braebon
1112017
10
SLEEP APNEA SYMPTOMS
bull Short term memory problems
bull Weight gain
bull Tiredness
bull Dry mouth
bull Sore throat
bull Slow metabolism
bull Bed partner frustration
bull AND A PLETHORA OF SERIOUS MEDICAL DISEASES DISORDERS AND MALADIES
High blood pressure
Heart failure
Heart rhythm disturbances
Atherosclerotic heart disease
Pulmonary hypertension
Insulin resistance
Sudden death
Erectile dysfunction
Memory problems
Depression
Anxiety
Gastroesophageal reflux
Sleep Apnea Increases Risk of
bull It has been estimated that 80 of depressed patients complain of disturbed sleep and sleeplessness is a risk factor for impaired mood
bull helliphelliphelliphelliphelliphelliphelliphellip The most common complaint of helliphelliphelliphelliphelliphelliphelliphellip PTSD is sleeplessness and 50 -helliphelliphelliphelliphelliphelliphelliphellip 70 of chronic pain patients helliphelliphelliphelliphelliphelliphelliphelliphellip report disturbed sleep
Consequences
1112017
11
Headachesbull Headaches are the most commonly reported pain complaint in the
population (textbook of pain)
bull Sleep disorders such as sleep apnea are found among headache patients at rates greater than what is found in the general population TX of sleep disorders decreases headache complaints Cephalgia is the most common complaint of TMD
bull (Archives of Internal Medicine)
Risk Factors
ObesityLarge neckSnoringNon-restorative sleepDaytime sleepinessfatigueHigh arched palateRetrognathiaCrowded airwaySmokingdrinking
(and remember sleep apnea occurs in women children and skinny guys toohellipthese are just risk factors)
Life Cycle of a LEAF
1112017
12
The cells in our body deteriorate as we age but they do so much quicker without oxygen
The Beatles were only partially correct when they sang
ldquoAll you need is loverdquo
The Hollies had a better understanding of life when they sangrdquo
ldquoAll I need is the air that I breath and to love yourdquo
1112017
13
NORMAL SLEEP
bull CHARACTERIZED BY A DECREASE IN
bull BODY TEMPERATURE
bull BLOOD PRESSURE
bull BREATHING RATE
bull MOST OTHER BODY FUNCTIONS
bull INCREASED NASAL RESISTANCE
bull CHARACTERIZED BY AN bull ACTIVE BRAIN
1112017
14
Copyright 2011 BRAEBON
Normal healthy breathing during sleep
Wake-up-gasping-choking-and-die-in-your-sleep-diseaserdquo ndash No sound during event
Who gets sent for a sleep study
1112017
15
Who usually doesnrsquot
Sleep apnoea is a common occurrence in femalesKarl A Franklin et al European Respiratory Journal August 2012
bull We investigated 400 females from a population-based random sample of 10000 females aged 20ndash70 years with a questionnaire and anovernight polysomnography
bull Obstructive sleep apnoea was found in 50 of females aged 20ndash70 years
bull Sleep apnoea was related to age obesity and hypertension but not to daytime sleepiness
bull Severe sleep apnoea was scored in 14 of females aged 55ndash70 years and in 31 of obese females with a body-mass index of gt30 kgmiddotmminus2 aged 50ndash70 years
1112017
16
EPWORTH SLEEPINESS SCALEINTERPRETATIONbull 0-7 IT IS UNLIKELY THAT YOU ARE ABNORMALLY SLEEPY
bull 8-9 YOU HAVE AN AVERAGE AMOUNT OF DAYTIME SLEEPINESS
bull 10-15 YOU MAY BE EXCESSIVELY SLEEPY DEPENDING ON THE SITUATION YOU MAY WANT TO CONSIDER SEEKING MEDICAL ATTENTION
bull 16-24 YOU ARE EXCESSIVELY SLEEPY AND SHOULD CONSIDER SEEKING MEDICAL ATTENTION
This person most likely is simply tired or had a bad nightrsquos sleep OSA is not
indicated
I referred this patient to a sleep physician
1112017
17
MALLAMPATI
1112017
18
Lavigne GJ Kato T Kolta A Sessle BJ Neurobiological mechanisms involved in sleep bruxism Crit Rev Oral Biol Med 20031430-46
bullSleep-related bruxism (SB) is characterized by the grinding or clenching of the teeth during sleep usually associated with sleep arousals although the incidence of sleep arousals in SB subjects is within the normal range (up to 14 arousalshour of sleep is considered normal)
IT HAS BEEN SHOWN THAT CPAP ELIMINATION OF OSA alsoELIMINATES SNORING
IT HAS NOT BEEN DEMONSTRATED THAT CPAP TREATMENT OF OSA
ELIMINATES OR REDUCES S-B
Neurobiological mechanisms involved in sleep bruxismLavigne GJ1 Kato T Kolta A Sessle BJ
bull Sleep bruxism (SB) is mainly associated with rhythmic masticatory muscle activity (RMMA) characterized by repetitive jaw muscle contractions (3 bursts or more at a frequency of 1 Hz)
bull The consequences of SB may include tooth destruction jaw pain headaches or the limitation of mandibular movement as well as tooth-grinding sounds that disrupt the sleep of bed partners RMMA is observed in 60 of normal sleepers
1112017
19
bull The pathophysiology of SB is becoming clearer
bull There is an abundance of evidence outlining the neurophysiology and neurochemistry of rhythmic jaw movements (RJM) in relation to chewing swallowing and breathing Several brainstem structures (eg reticular pontis oralis pontis caudalis) and neurochemicals (eg serotonin dopamine gamma aminobutyric acid [GABA] noradrenaline) are involved in both the genesis of RJM and the modulation of muscle tone during sleep
bull It creates a co-activation of both jaw-opening and jaw-closing muscles instead of the alternating jaw-opening and jaw-closing muscle activity pattern typical of chewing
Journal of Pain amp Symptom Management
bullPain duration and intensitywere correlated with decreased sleep impaired sleep quality and delayed sleep onset
Multiple Medical Studies
bullHave published that the majority (59 67 74) of OSA patients will not appropriately wear the CPAP
1112017
20
bull IN 1995 Johnny Cochran said ldquoIf the glove doesnrsquot fithellipyou must acquitrdquo As DR Dement intimated in the 1970s ldquoWe didnt know what to measurehellipso we measured everything we could think ofhellip and it stuckrdquo
bull Almost forty years later some of what ldquostuckrdquo is being revised reinterpreted and common sense is beginning to prevail Seven to eight hours of sleep per night is recommended
The Other 72 of Sleep
bull Sticking with the antiquated definition of a ldquocompliant userrdquo of a
CPAP (4 hrsnight and 5 nightsweek) one must use it roughly 28 of the time
bull WHAT ABOUT THE OTHER 72 OF SLEEP
bull Is it acceptable to not get the O2 we need simply because an antiquated standard ldquostuckrdquo
bull In 1995 CPAP became the gold standard Now in the 21st century I
say ldquoif the mask doesnrsquot fit hellipdonrsquot quitrdquo because an oral appliance may save your health and your life
Treatment of Sleep Apnea
Tracheotomy Oral
Surgery CPAPBiPAP
OA
Behavioral Modification
1112017
21
Orofacial Findings
bullThe most common orofacial characteristics include a retrognathic mandible narrow palate large neck circumference long soft palate tonsillar hypertrophy nasal septal deviation and relative macroglossia
Oral Appliances for Sleep Apnea amp Snoring
Tongue Retaining Devices Mandibular Repositioning Appliances
Oral Appliances (OA)
bull Properly fabricated an oral appliance will protrude the tongue and reposition the mandible anteriorly and inferiorly to the most beneficial neuromuscular position to prevent posterior airway collapse
bull This position is titratable and individualized to exact patient requirements and may need periodic adjustments just as does CPAP
1112017
22
BEFORE
APPLIANCE
7c
WITH
APPLIANCE
9 cc
1112017
23
Copyright 2011 BRAEBON
More Directly Related to hellipDental Sleep Medicine
bull EACH PATIENT IS AN INDIVIDUAL AND JUST AS CPAP PRESSURE IS INDIVIDUALLY TITRATEDhellipSO TOO ARE ORAL APPLIANCES
bull IF I DELIVER AN OA TO A PATIENT WHO WILL NOT UTILIZE THE CPAPhellipI WILL PROVIDE ONE OR SEVERAL HOME SLEEP STUDIES TO ASCERTAIN THE EFFICACY OF THE OAhellip AND THEN I REQUIRE THAT THEY RETURN TO THEIR SLEEP
bull DOCTOR FOR A SUBSEQUENT STUDY WHILE helliphelliphelliphelliphelliphelliphellipUTILIZINGTHE OA
Positional Apnea in a 73-Year Old Male with Atrial Fibrillation
bull This case study illustrates the cost-effective approach to successful outcomes associated with positional therapy that are not surprising and are consistent with a recent study which concluded ldquopositional therapy is equivalent to CPAP at normalizing the AHI in patients with positional OSA with similar effects on sleep quality and nocturnal oxygenationrdquo
bull Journal Sleep Diagnosis and Therapy
1112017
24
HOW THE ORAL APPLIANCE TREATS OSA
bull Prevent collapse of airwaybull Forward advancement of jawbull Support forward tongue positionbull Change shape of pharyngeal airwaybull Increase vertical dimension of occlusionbull Correct dysphagia bull Increase volume of space for tonguebull Trains protrusive tongue reflexesbull Alter position of hyoid bone relative to
mandible
THE VARYING ROLES OF THE NOSE AND MOUTH IN BREATHING
1112017
25
THE NOSE
bull A recent pediatric study reveals why addressing the tongue is so important for resolving sleep apnea As explained in this study having an abnormally short lingual frenulum can result in impaired orofacial growth in early childhood reducing the width of the upper airway
bull The upper airway is very pliable so this increases the risk of it collapsing during sleep They found that children with an untreated short frenulum developed abnormal tongue function early in life which also impacted their orofacial growth and led to disordered breathing during sleep
WHAT IS THE ROLE OF THE NOSE
ITS FUNCTIONS ARE VITAL
bull WARMING
bull HUMIDIFICATION
bull FILTERING
bull CLEANING
OF AMBIENT AIR INHALED INTO THE LUNGS
INFUSION OF NITRIC OXIDE
1112017
26
Humidification and
Dehumidification
bull During intake air is humidified to increase lung oxygen facilitation
bull Upon exhalation air is dehumidified to keep water in our cells
bull If this were not the case we would dehydrate unless we continually drank water
NARES
CONSTRICT
NARES FLARE
SNIFF TEST
1112017
27
Cosmetic Surgery
bullHe couldnrsquot breath through his small nose became hypercapnic and helliphelliphellipdied
Effect of treating severe nasal obstruction on the severity of obstructive sleep apnoea
bull HA McLean AM Urton HS Driver AKW Tan AG Day+ PW Munt and MF Fitzpatrick
bullThis study demonstrates that relief of severe nasal obstruction in patients with a normal retroglossal airway is associated with a significant reduction in mouth breathing during sleep improved sleep architecture and a modest improvement in OSA severity
1112017
28
bullThere are several novel aspects to these findings First the study documents a clearly increased upper airway resistance in association with oral breathing during stable sleep as compared with nasal breathing irrespective of central or OSA
bullSecondly this methodology included simultaneous documentation of oral and nasal ventilation during sleep to confirm the absence of any nasal airflow in the oral breathing condition and vice versa
1112017
29
bullThe substantially higher resistive load posed by the oral breathing route provides a plausible explanation for the observation that inhaled ventilation occurs almost exclusively via the nasal route during sleep in subjects with normal nasal resistance
bull Many studies have shown that nasal obstruction can induce or increase apnea frequency in OSA patients When nasal resistance is high a greater pressure drop is required to achieve the same flow and hence collapse of the pharynx is facilitated and this could mitigate the effect of mandibular advancement
bull Moreover high nasal resistance is associated with mouth breathing which could potentially limit the beneficial effect of mandibular advancement
bull Dental Appliance Treatment for Obstructive
bull Andrew S L Chan Richard W W Lee and Peter A Cistulli
bull httpchestjournalchestpubsorgcontent1322693fullhtml
1112017
30
bullCurrent evidence suggests that despite the superior efficacy of CPAP both treatments produce similar subjective and objective health benefits
bullThe superior self-reported tolerance and compliance associated with MAD treatment is a likely explanation
bullThe practice parameters of the AASM recommend the use of oral appliances for mild-to-moderate OSA or for patients with severe OSA who are unable to tolerate CPAP or refuse treatment with CPAP with a required written prescription by a sleep physician
The following are Medicare rules
1) A diagnosis of OSA is not within the dental scope of practice A dentist providing an OA
must do so under the and with the team effort of a licensed Physician with a written
prescription
2) A physician is not skilled in the intricacies of fabricating fitting monitoring adjusting
and choosing an appropriate Oral Appliance individualized per patient
3) A dentist may not provide an oral appliance if the patient has an active
Temporomandibular Disorder
4) The OA must be fabricated within 90 days of the patientrsquos appointment with the sleep
physician
Since the rules are clear and they involve both of our professions it would behoove
both DOMD and DDS to communicate for the benefit of OSA patients
1112017
31
Subsequent to my 3 hour 2013 Meeting with the US Department of Transportation regarding Truckers
bull During the State Board of Dental Examiners meeting Board members put sleep Dentistry in squarely back into the spotlight The Board has addressed sleep Dentistry issues in a public hearing and all four Board meetings in 2013
bull There was discussion that there can be a shared relationship between the Dental and medical scopes of practice
bull Under the proposed rule a Dentist may treat benign snoring with an oral appliance after referral to a licensed physician where appropriate within the standard of care By contrast a Dentist may not diagnose treat or monitor OSA without collaboration with a licensed physician Additionally an oral appliance shall only be fabricated by a licensed Dentist or by a Dental lab under a prescription or work order prepared by a Dentist
American Dental Association
bull Treatment using an oral appliance designed specifically to treat OSA should be fabricated by a dentist familiar with device design maintenance and therapeutic efficacy and who has an association with and a referral from a sleep team
bull JADA Vol 136 p 1123
Donrsquot be afraid of OSA Get a grip on the facts and save patientrsquos lives
1112017
32
bullA SYMBIOTIC RELATION BETWEEN PHYSICIANS SLEEP PROFESSIONALS AND DENTISTS CAN SIGNIFICANTLY IMPROVE THE SLEEP HEALTH OF MILLIONS OF PEOPLE EACH AND EVERY YEAR
bull THAT RELATIONSHIP IS NOT A ONE WAY STREET AND THE
American Sleep amp Breathing Academy of over 8000 members UNDERSTANDS THAThellip JUST LOOK AT THE MULTITUDE OF SLEEP PROFESSIONAL CATAGORIES ON THEIR BOARD OF DIRECTORS
THE END
Thank you for your interest I hope this presentation was helpful
Dr Richard Klein
1112017
7
Prevalence and Consequences of Sleep Disorders in Traumatic Brain Injury
bullThe authors reviewed evidence that cognitive dysfunction is a well known problem after TBI and is a major factor preventing return to independent living social readaptation and vocational pursuits Richard J Castriotta MD12 Mark C Wilde PsyD12 Jenny M Lai MD12 Strahil
Atanasov MD3 Brent E Masel MD4 and Samuel T Kuna MD56
Findings
bull 54 of that population had a normal polysomnography 46 had a sleep disorder (other studies have documented up to 23 had a SBD)
bull This is significantly higher that that of the general population
bull 23 had obstructive sleep apnea Again this finding is much higher than that of those who did or did not vote for our last President
ConclusionbullThe authors concluded that there was a high prevalence of sleep-disorders and excessive daytime sleepiness in individuals who had TBI and that consideration should be given to having all TBI patients evaluated for sleep disorders
1112017
8
Wersquoll discuss this later as it refers to pain
bullBut 1st letrsquos consider OSA since it is highly prevalent in your TBI patients
Sleep Apnea May Hasten Memory Loss and Alzheimers
bullPublished in the journal Neurology the study2 found that patients with sleep apnea andor snoring were diagnosed with mild cognitive impairment more than a decade earlier than those without sleep apnea
bull 2 Neurology April 15 2015
bullOn average those with untreated obstructed sleep apnea started experiencing cognitive impairment at the age of 77 compared to 90 among those without breathing problems
bullThose who used a CPAP machine to address their sleep apnea started declining mentally at the same age as those who did not have sleep apnea
1112017
9
Scary video by WatchPAT
Obstructive SleepApnea
Definition of Sleep apnea
bullSleep Apnea occurs when the soft tissue in your mouth (the tongue tonsils pharynx uvula etc) relax too much and collapse at the back of your throat and cut off the airway making it difficult or impossible to breath
AHI Three levels of severity
Mild 5 to 15 times per hour
Moderate 15 to 30 times per hour
Severe gt30 times per hour
Copyright 2011 Braebon
1112017
10
SLEEP APNEA SYMPTOMS
bull Short term memory problems
bull Weight gain
bull Tiredness
bull Dry mouth
bull Sore throat
bull Slow metabolism
bull Bed partner frustration
bull AND A PLETHORA OF SERIOUS MEDICAL DISEASES DISORDERS AND MALADIES
High blood pressure
Heart failure
Heart rhythm disturbances
Atherosclerotic heart disease
Pulmonary hypertension
Insulin resistance
Sudden death
Erectile dysfunction
Memory problems
Depression
Anxiety
Gastroesophageal reflux
Sleep Apnea Increases Risk of
bull It has been estimated that 80 of depressed patients complain of disturbed sleep and sleeplessness is a risk factor for impaired mood
bull helliphelliphelliphelliphelliphelliphelliphellip The most common complaint of helliphelliphelliphelliphelliphelliphelliphellip PTSD is sleeplessness and 50 -helliphelliphelliphelliphelliphelliphelliphellip 70 of chronic pain patients helliphelliphelliphelliphelliphelliphelliphelliphellip report disturbed sleep
Consequences
1112017
11
Headachesbull Headaches are the most commonly reported pain complaint in the
population (textbook of pain)
bull Sleep disorders such as sleep apnea are found among headache patients at rates greater than what is found in the general population TX of sleep disorders decreases headache complaints Cephalgia is the most common complaint of TMD
bull (Archives of Internal Medicine)
Risk Factors
ObesityLarge neckSnoringNon-restorative sleepDaytime sleepinessfatigueHigh arched palateRetrognathiaCrowded airwaySmokingdrinking
(and remember sleep apnea occurs in women children and skinny guys toohellipthese are just risk factors)
Life Cycle of a LEAF
1112017
12
The cells in our body deteriorate as we age but they do so much quicker without oxygen
The Beatles were only partially correct when they sang
ldquoAll you need is loverdquo
The Hollies had a better understanding of life when they sangrdquo
ldquoAll I need is the air that I breath and to love yourdquo
1112017
13
NORMAL SLEEP
bull CHARACTERIZED BY A DECREASE IN
bull BODY TEMPERATURE
bull BLOOD PRESSURE
bull BREATHING RATE
bull MOST OTHER BODY FUNCTIONS
bull INCREASED NASAL RESISTANCE
bull CHARACTERIZED BY AN bull ACTIVE BRAIN
1112017
14
Copyright 2011 BRAEBON
Normal healthy breathing during sleep
Wake-up-gasping-choking-and-die-in-your-sleep-diseaserdquo ndash No sound during event
Who gets sent for a sleep study
1112017
15
Who usually doesnrsquot
Sleep apnoea is a common occurrence in femalesKarl A Franklin et al European Respiratory Journal August 2012
bull We investigated 400 females from a population-based random sample of 10000 females aged 20ndash70 years with a questionnaire and anovernight polysomnography
bull Obstructive sleep apnoea was found in 50 of females aged 20ndash70 years
bull Sleep apnoea was related to age obesity and hypertension but not to daytime sleepiness
bull Severe sleep apnoea was scored in 14 of females aged 55ndash70 years and in 31 of obese females with a body-mass index of gt30 kgmiddotmminus2 aged 50ndash70 years
1112017
16
EPWORTH SLEEPINESS SCALEINTERPRETATIONbull 0-7 IT IS UNLIKELY THAT YOU ARE ABNORMALLY SLEEPY
bull 8-9 YOU HAVE AN AVERAGE AMOUNT OF DAYTIME SLEEPINESS
bull 10-15 YOU MAY BE EXCESSIVELY SLEEPY DEPENDING ON THE SITUATION YOU MAY WANT TO CONSIDER SEEKING MEDICAL ATTENTION
bull 16-24 YOU ARE EXCESSIVELY SLEEPY AND SHOULD CONSIDER SEEKING MEDICAL ATTENTION
This person most likely is simply tired or had a bad nightrsquos sleep OSA is not
indicated
I referred this patient to a sleep physician
1112017
17
MALLAMPATI
1112017
18
Lavigne GJ Kato T Kolta A Sessle BJ Neurobiological mechanisms involved in sleep bruxism Crit Rev Oral Biol Med 20031430-46
bullSleep-related bruxism (SB) is characterized by the grinding or clenching of the teeth during sleep usually associated with sleep arousals although the incidence of sleep arousals in SB subjects is within the normal range (up to 14 arousalshour of sleep is considered normal)
IT HAS BEEN SHOWN THAT CPAP ELIMINATION OF OSA alsoELIMINATES SNORING
IT HAS NOT BEEN DEMONSTRATED THAT CPAP TREATMENT OF OSA
ELIMINATES OR REDUCES S-B
Neurobiological mechanisms involved in sleep bruxismLavigne GJ1 Kato T Kolta A Sessle BJ
bull Sleep bruxism (SB) is mainly associated with rhythmic masticatory muscle activity (RMMA) characterized by repetitive jaw muscle contractions (3 bursts or more at a frequency of 1 Hz)
bull The consequences of SB may include tooth destruction jaw pain headaches or the limitation of mandibular movement as well as tooth-grinding sounds that disrupt the sleep of bed partners RMMA is observed in 60 of normal sleepers
1112017
19
bull The pathophysiology of SB is becoming clearer
bull There is an abundance of evidence outlining the neurophysiology and neurochemistry of rhythmic jaw movements (RJM) in relation to chewing swallowing and breathing Several brainstem structures (eg reticular pontis oralis pontis caudalis) and neurochemicals (eg serotonin dopamine gamma aminobutyric acid [GABA] noradrenaline) are involved in both the genesis of RJM and the modulation of muscle tone during sleep
bull It creates a co-activation of both jaw-opening and jaw-closing muscles instead of the alternating jaw-opening and jaw-closing muscle activity pattern typical of chewing
Journal of Pain amp Symptom Management
bullPain duration and intensitywere correlated with decreased sleep impaired sleep quality and delayed sleep onset
Multiple Medical Studies
bullHave published that the majority (59 67 74) of OSA patients will not appropriately wear the CPAP
1112017
20
bull IN 1995 Johnny Cochran said ldquoIf the glove doesnrsquot fithellipyou must acquitrdquo As DR Dement intimated in the 1970s ldquoWe didnt know what to measurehellipso we measured everything we could think ofhellip and it stuckrdquo
bull Almost forty years later some of what ldquostuckrdquo is being revised reinterpreted and common sense is beginning to prevail Seven to eight hours of sleep per night is recommended
The Other 72 of Sleep
bull Sticking with the antiquated definition of a ldquocompliant userrdquo of a
CPAP (4 hrsnight and 5 nightsweek) one must use it roughly 28 of the time
bull WHAT ABOUT THE OTHER 72 OF SLEEP
bull Is it acceptable to not get the O2 we need simply because an antiquated standard ldquostuckrdquo
bull In 1995 CPAP became the gold standard Now in the 21st century I
say ldquoif the mask doesnrsquot fit hellipdonrsquot quitrdquo because an oral appliance may save your health and your life
Treatment of Sleep Apnea
Tracheotomy Oral
Surgery CPAPBiPAP
OA
Behavioral Modification
1112017
21
Orofacial Findings
bullThe most common orofacial characteristics include a retrognathic mandible narrow palate large neck circumference long soft palate tonsillar hypertrophy nasal septal deviation and relative macroglossia
Oral Appliances for Sleep Apnea amp Snoring
Tongue Retaining Devices Mandibular Repositioning Appliances
Oral Appliances (OA)
bull Properly fabricated an oral appliance will protrude the tongue and reposition the mandible anteriorly and inferiorly to the most beneficial neuromuscular position to prevent posterior airway collapse
bull This position is titratable and individualized to exact patient requirements and may need periodic adjustments just as does CPAP
1112017
22
BEFORE
APPLIANCE
7c
WITH
APPLIANCE
9 cc
1112017
23
Copyright 2011 BRAEBON
More Directly Related to hellipDental Sleep Medicine
bull EACH PATIENT IS AN INDIVIDUAL AND JUST AS CPAP PRESSURE IS INDIVIDUALLY TITRATEDhellipSO TOO ARE ORAL APPLIANCES
bull IF I DELIVER AN OA TO A PATIENT WHO WILL NOT UTILIZE THE CPAPhellipI WILL PROVIDE ONE OR SEVERAL HOME SLEEP STUDIES TO ASCERTAIN THE EFFICACY OF THE OAhellip AND THEN I REQUIRE THAT THEY RETURN TO THEIR SLEEP
bull DOCTOR FOR A SUBSEQUENT STUDY WHILE helliphelliphelliphelliphelliphelliphellipUTILIZINGTHE OA
Positional Apnea in a 73-Year Old Male with Atrial Fibrillation
bull This case study illustrates the cost-effective approach to successful outcomes associated with positional therapy that are not surprising and are consistent with a recent study which concluded ldquopositional therapy is equivalent to CPAP at normalizing the AHI in patients with positional OSA with similar effects on sleep quality and nocturnal oxygenationrdquo
bull Journal Sleep Diagnosis and Therapy
1112017
24
HOW THE ORAL APPLIANCE TREATS OSA
bull Prevent collapse of airwaybull Forward advancement of jawbull Support forward tongue positionbull Change shape of pharyngeal airwaybull Increase vertical dimension of occlusionbull Correct dysphagia bull Increase volume of space for tonguebull Trains protrusive tongue reflexesbull Alter position of hyoid bone relative to
mandible
THE VARYING ROLES OF THE NOSE AND MOUTH IN BREATHING
1112017
25
THE NOSE
bull A recent pediatric study reveals why addressing the tongue is so important for resolving sleep apnea As explained in this study having an abnormally short lingual frenulum can result in impaired orofacial growth in early childhood reducing the width of the upper airway
bull The upper airway is very pliable so this increases the risk of it collapsing during sleep They found that children with an untreated short frenulum developed abnormal tongue function early in life which also impacted their orofacial growth and led to disordered breathing during sleep
WHAT IS THE ROLE OF THE NOSE
ITS FUNCTIONS ARE VITAL
bull WARMING
bull HUMIDIFICATION
bull FILTERING
bull CLEANING
OF AMBIENT AIR INHALED INTO THE LUNGS
INFUSION OF NITRIC OXIDE
1112017
26
Humidification and
Dehumidification
bull During intake air is humidified to increase lung oxygen facilitation
bull Upon exhalation air is dehumidified to keep water in our cells
bull If this were not the case we would dehydrate unless we continually drank water
NARES
CONSTRICT
NARES FLARE
SNIFF TEST
1112017
27
Cosmetic Surgery
bullHe couldnrsquot breath through his small nose became hypercapnic and helliphelliphellipdied
Effect of treating severe nasal obstruction on the severity of obstructive sleep apnoea
bull HA McLean AM Urton HS Driver AKW Tan AG Day+ PW Munt and MF Fitzpatrick
bullThis study demonstrates that relief of severe nasal obstruction in patients with a normal retroglossal airway is associated with a significant reduction in mouth breathing during sleep improved sleep architecture and a modest improvement in OSA severity
1112017
28
bullThere are several novel aspects to these findings First the study documents a clearly increased upper airway resistance in association with oral breathing during stable sleep as compared with nasal breathing irrespective of central or OSA
bullSecondly this methodology included simultaneous documentation of oral and nasal ventilation during sleep to confirm the absence of any nasal airflow in the oral breathing condition and vice versa
1112017
29
bullThe substantially higher resistive load posed by the oral breathing route provides a plausible explanation for the observation that inhaled ventilation occurs almost exclusively via the nasal route during sleep in subjects with normal nasal resistance
bull Many studies have shown that nasal obstruction can induce or increase apnea frequency in OSA patients When nasal resistance is high a greater pressure drop is required to achieve the same flow and hence collapse of the pharynx is facilitated and this could mitigate the effect of mandibular advancement
bull Moreover high nasal resistance is associated with mouth breathing which could potentially limit the beneficial effect of mandibular advancement
bull Dental Appliance Treatment for Obstructive
bull Andrew S L Chan Richard W W Lee and Peter A Cistulli
bull httpchestjournalchestpubsorgcontent1322693fullhtml
1112017
30
bullCurrent evidence suggests that despite the superior efficacy of CPAP both treatments produce similar subjective and objective health benefits
bullThe superior self-reported tolerance and compliance associated with MAD treatment is a likely explanation
bullThe practice parameters of the AASM recommend the use of oral appliances for mild-to-moderate OSA or for patients with severe OSA who are unable to tolerate CPAP or refuse treatment with CPAP with a required written prescription by a sleep physician
The following are Medicare rules
1) A diagnosis of OSA is not within the dental scope of practice A dentist providing an OA
must do so under the and with the team effort of a licensed Physician with a written
prescription
2) A physician is not skilled in the intricacies of fabricating fitting monitoring adjusting
and choosing an appropriate Oral Appliance individualized per patient
3) A dentist may not provide an oral appliance if the patient has an active
Temporomandibular Disorder
4) The OA must be fabricated within 90 days of the patientrsquos appointment with the sleep
physician
Since the rules are clear and they involve both of our professions it would behoove
both DOMD and DDS to communicate for the benefit of OSA patients
1112017
31
Subsequent to my 3 hour 2013 Meeting with the US Department of Transportation regarding Truckers
bull During the State Board of Dental Examiners meeting Board members put sleep Dentistry in squarely back into the spotlight The Board has addressed sleep Dentistry issues in a public hearing and all four Board meetings in 2013
bull There was discussion that there can be a shared relationship between the Dental and medical scopes of practice
bull Under the proposed rule a Dentist may treat benign snoring with an oral appliance after referral to a licensed physician where appropriate within the standard of care By contrast a Dentist may not diagnose treat or monitor OSA without collaboration with a licensed physician Additionally an oral appliance shall only be fabricated by a licensed Dentist or by a Dental lab under a prescription or work order prepared by a Dentist
American Dental Association
bull Treatment using an oral appliance designed specifically to treat OSA should be fabricated by a dentist familiar with device design maintenance and therapeutic efficacy and who has an association with and a referral from a sleep team
bull JADA Vol 136 p 1123
Donrsquot be afraid of OSA Get a grip on the facts and save patientrsquos lives
1112017
32
bullA SYMBIOTIC RELATION BETWEEN PHYSICIANS SLEEP PROFESSIONALS AND DENTISTS CAN SIGNIFICANTLY IMPROVE THE SLEEP HEALTH OF MILLIONS OF PEOPLE EACH AND EVERY YEAR
bull THAT RELATIONSHIP IS NOT A ONE WAY STREET AND THE
American Sleep amp Breathing Academy of over 8000 members UNDERSTANDS THAThellip JUST LOOK AT THE MULTITUDE OF SLEEP PROFESSIONAL CATAGORIES ON THEIR BOARD OF DIRECTORS
THE END
Thank you for your interest I hope this presentation was helpful
Dr Richard Klein
1112017
8
Wersquoll discuss this later as it refers to pain
bullBut 1st letrsquos consider OSA since it is highly prevalent in your TBI patients
Sleep Apnea May Hasten Memory Loss and Alzheimers
bullPublished in the journal Neurology the study2 found that patients with sleep apnea andor snoring were diagnosed with mild cognitive impairment more than a decade earlier than those without sleep apnea
bull 2 Neurology April 15 2015
bullOn average those with untreated obstructed sleep apnea started experiencing cognitive impairment at the age of 77 compared to 90 among those without breathing problems
bullThose who used a CPAP machine to address their sleep apnea started declining mentally at the same age as those who did not have sleep apnea
1112017
9
Scary video by WatchPAT
Obstructive SleepApnea
Definition of Sleep apnea
bullSleep Apnea occurs when the soft tissue in your mouth (the tongue tonsils pharynx uvula etc) relax too much and collapse at the back of your throat and cut off the airway making it difficult or impossible to breath
AHI Three levels of severity
Mild 5 to 15 times per hour
Moderate 15 to 30 times per hour
Severe gt30 times per hour
Copyright 2011 Braebon
1112017
10
SLEEP APNEA SYMPTOMS
bull Short term memory problems
bull Weight gain
bull Tiredness
bull Dry mouth
bull Sore throat
bull Slow metabolism
bull Bed partner frustration
bull AND A PLETHORA OF SERIOUS MEDICAL DISEASES DISORDERS AND MALADIES
High blood pressure
Heart failure
Heart rhythm disturbances
Atherosclerotic heart disease
Pulmonary hypertension
Insulin resistance
Sudden death
Erectile dysfunction
Memory problems
Depression
Anxiety
Gastroesophageal reflux
Sleep Apnea Increases Risk of
bull It has been estimated that 80 of depressed patients complain of disturbed sleep and sleeplessness is a risk factor for impaired mood
bull helliphelliphelliphelliphelliphelliphelliphellip The most common complaint of helliphelliphelliphelliphelliphelliphelliphellip PTSD is sleeplessness and 50 -helliphelliphelliphelliphelliphelliphelliphellip 70 of chronic pain patients helliphelliphelliphelliphelliphelliphelliphelliphellip report disturbed sleep
Consequences
1112017
11
Headachesbull Headaches are the most commonly reported pain complaint in the
population (textbook of pain)
bull Sleep disorders such as sleep apnea are found among headache patients at rates greater than what is found in the general population TX of sleep disorders decreases headache complaints Cephalgia is the most common complaint of TMD
bull (Archives of Internal Medicine)
Risk Factors
ObesityLarge neckSnoringNon-restorative sleepDaytime sleepinessfatigueHigh arched palateRetrognathiaCrowded airwaySmokingdrinking
(and remember sleep apnea occurs in women children and skinny guys toohellipthese are just risk factors)
Life Cycle of a LEAF
1112017
12
The cells in our body deteriorate as we age but they do so much quicker without oxygen
The Beatles were only partially correct when they sang
ldquoAll you need is loverdquo
The Hollies had a better understanding of life when they sangrdquo
ldquoAll I need is the air that I breath and to love yourdquo
1112017
13
NORMAL SLEEP
bull CHARACTERIZED BY A DECREASE IN
bull BODY TEMPERATURE
bull BLOOD PRESSURE
bull BREATHING RATE
bull MOST OTHER BODY FUNCTIONS
bull INCREASED NASAL RESISTANCE
bull CHARACTERIZED BY AN bull ACTIVE BRAIN
1112017
14
Copyright 2011 BRAEBON
Normal healthy breathing during sleep
Wake-up-gasping-choking-and-die-in-your-sleep-diseaserdquo ndash No sound during event
Who gets sent for a sleep study
1112017
15
Who usually doesnrsquot
Sleep apnoea is a common occurrence in femalesKarl A Franklin et al European Respiratory Journal August 2012
bull We investigated 400 females from a population-based random sample of 10000 females aged 20ndash70 years with a questionnaire and anovernight polysomnography
bull Obstructive sleep apnoea was found in 50 of females aged 20ndash70 years
bull Sleep apnoea was related to age obesity and hypertension but not to daytime sleepiness
bull Severe sleep apnoea was scored in 14 of females aged 55ndash70 years and in 31 of obese females with a body-mass index of gt30 kgmiddotmminus2 aged 50ndash70 years
1112017
16
EPWORTH SLEEPINESS SCALEINTERPRETATIONbull 0-7 IT IS UNLIKELY THAT YOU ARE ABNORMALLY SLEEPY
bull 8-9 YOU HAVE AN AVERAGE AMOUNT OF DAYTIME SLEEPINESS
bull 10-15 YOU MAY BE EXCESSIVELY SLEEPY DEPENDING ON THE SITUATION YOU MAY WANT TO CONSIDER SEEKING MEDICAL ATTENTION
bull 16-24 YOU ARE EXCESSIVELY SLEEPY AND SHOULD CONSIDER SEEKING MEDICAL ATTENTION
This person most likely is simply tired or had a bad nightrsquos sleep OSA is not
indicated
I referred this patient to a sleep physician
1112017
17
MALLAMPATI
1112017
18
Lavigne GJ Kato T Kolta A Sessle BJ Neurobiological mechanisms involved in sleep bruxism Crit Rev Oral Biol Med 20031430-46
bullSleep-related bruxism (SB) is characterized by the grinding or clenching of the teeth during sleep usually associated with sleep arousals although the incidence of sleep arousals in SB subjects is within the normal range (up to 14 arousalshour of sleep is considered normal)
IT HAS BEEN SHOWN THAT CPAP ELIMINATION OF OSA alsoELIMINATES SNORING
IT HAS NOT BEEN DEMONSTRATED THAT CPAP TREATMENT OF OSA
ELIMINATES OR REDUCES S-B
Neurobiological mechanisms involved in sleep bruxismLavigne GJ1 Kato T Kolta A Sessle BJ
bull Sleep bruxism (SB) is mainly associated with rhythmic masticatory muscle activity (RMMA) characterized by repetitive jaw muscle contractions (3 bursts or more at a frequency of 1 Hz)
bull The consequences of SB may include tooth destruction jaw pain headaches or the limitation of mandibular movement as well as tooth-grinding sounds that disrupt the sleep of bed partners RMMA is observed in 60 of normal sleepers
1112017
19
bull The pathophysiology of SB is becoming clearer
bull There is an abundance of evidence outlining the neurophysiology and neurochemistry of rhythmic jaw movements (RJM) in relation to chewing swallowing and breathing Several brainstem structures (eg reticular pontis oralis pontis caudalis) and neurochemicals (eg serotonin dopamine gamma aminobutyric acid [GABA] noradrenaline) are involved in both the genesis of RJM and the modulation of muscle tone during sleep
bull It creates a co-activation of both jaw-opening and jaw-closing muscles instead of the alternating jaw-opening and jaw-closing muscle activity pattern typical of chewing
Journal of Pain amp Symptom Management
bullPain duration and intensitywere correlated with decreased sleep impaired sleep quality and delayed sleep onset
Multiple Medical Studies
bullHave published that the majority (59 67 74) of OSA patients will not appropriately wear the CPAP
1112017
20
bull IN 1995 Johnny Cochran said ldquoIf the glove doesnrsquot fithellipyou must acquitrdquo As DR Dement intimated in the 1970s ldquoWe didnt know what to measurehellipso we measured everything we could think ofhellip and it stuckrdquo
bull Almost forty years later some of what ldquostuckrdquo is being revised reinterpreted and common sense is beginning to prevail Seven to eight hours of sleep per night is recommended
The Other 72 of Sleep
bull Sticking with the antiquated definition of a ldquocompliant userrdquo of a
CPAP (4 hrsnight and 5 nightsweek) one must use it roughly 28 of the time
bull WHAT ABOUT THE OTHER 72 OF SLEEP
bull Is it acceptable to not get the O2 we need simply because an antiquated standard ldquostuckrdquo
bull In 1995 CPAP became the gold standard Now in the 21st century I
say ldquoif the mask doesnrsquot fit hellipdonrsquot quitrdquo because an oral appliance may save your health and your life
Treatment of Sleep Apnea
Tracheotomy Oral
Surgery CPAPBiPAP
OA
Behavioral Modification
1112017
21
Orofacial Findings
bullThe most common orofacial characteristics include a retrognathic mandible narrow palate large neck circumference long soft palate tonsillar hypertrophy nasal septal deviation and relative macroglossia
Oral Appliances for Sleep Apnea amp Snoring
Tongue Retaining Devices Mandibular Repositioning Appliances
Oral Appliances (OA)
bull Properly fabricated an oral appliance will protrude the tongue and reposition the mandible anteriorly and inferiorly to the most beneficial neuromuscular position to prevent posterior airway collapse
bull This position is titratable and individualized to exact patient requirements and may need periodic adjustments just as does CPAP
1112017
22
BEFORE
APPLIANCE
7c
WITH
APPLIANCE
9 cc
1112017
23
Copyright 2011 BRAEBON
More Directly Related to hellipDental Sleep Medicine
bull EACH PATIENT IS AN INDIVIDUAL AND JUST AS CPAP PRESSURE IS INDIVIDUALLY TITRATEDhellipSO TOO ARE ORAL APPLIANCES
bull IF I DELIVER AN OA TO A PATIENT WHO WILL NOT UTILIZE THE CPAPhellipI WILL PROVIDE ONE OR SEVERAL HOME SLEEP STUDIES TO ASCERTAIN THE EFFICACY OF THE OAhellip AND THEN I REQUIRE THAT THEY RETURN TO THEIR SLEEP
bull DOCTOR FOR A SUBSEQUENT STUDY WHILE helliphelliphelliphelliphelliphelliphellipUTILIZINGTHE OA
Positional Apnea in a 73-Year Old Male with Atrial Fibrillation
bull This case study illustrates the cost-effective approach to successful outcomes associated with positional therapy that are not surprising and are consistent with a recent study which concluded ldquopositional therapy is equivalent to CPAP at normalizing the AHI in patients with positional OSA with similar effects on sleep quality and nocturnal oxygenationrdquo
bull Journal Sleep Diagnosis and Therapy
1112017
24
HOW THE ORAL APPLIANCE TREATS OSA
bull Prevent collapse of airwaybull Forward advancement of jawbull Support forward tongue positionbull Change shape of pharyngeal airwaybull Increase vertical dimension of occlusionbull Correct dysphagia bull Increase volume of space for tonguebull Trains protrusive tongue reflexesbull Alter position of hyoid bone relative to
mandible
THE VARYING ROLES OF THE NOSE AND MOUTH IN BREATHING
1112017
25
THE NOSE
bull A recent pediatric study reveals why addressing the tongue is so important for resolving sleep apnea As explained in this study having an abnormally short lingual frenulum can result in impaired orofacial growth in early childhood reducing the width of the upper airway
bull The upper airway is very pliable so this increases the risk of it collapsing during sleep They found that children with an untreated short frenulum developed abnormal tongue function early in life which also impacted their orofacial growth and led to disordered breathing during sleep
WHAT IS THE ROLE OF THE NOSE
ITS FUNCTIONS ARE VITAL
bull WARMING
bull HUMIDIFICATION
bull FILTERING
bull CLEANING
OF AMBIENT AIR INHALED INTO THE LUNGS
INFUSION OF NITRIC OXIDE
1112017
26
Humidification and
Dehumidification
bull During intake air is humidified to increase lung oxygen facilitation
bull Upon exhalation air is dehumidified to keep water in our cells
bull If this were not the case we would dehydrate unless we continually drank water
NARES
CONSTRICT
NARES FLARE
SNIFF TEST
1112017
27
Cosmetic Surgery
bullHe couldnrsquot breath through his small nose became hypercapnic and helliphelliphellipdied
Effect of treating severe nasal obstruction on the severity of obstructive sleep apnoea
bull HA McLean AM Urton HS Driver AKW Tan AG Day+ PW Munt and MF Fitzpatrick
bullThis study demonstrates that relief of severe nasal obstruction in patients with a normal retroglossal airway is associated with a significant reduction in mouth breathing during sleep improved sleep architecture and a modest improvement in OSA severity
1112017
28
bullThere are several novel aspects to these findings First the study documents a clearly increased upper airway resistance in association with oral breathing during stable sleep as compared with nasal breathing irrespective of central or OSA
bullSecondly this methodology included simultaneous documentation of oral and nasal ventilation during sleep to confirm the absence of any nasal airflow in the oral breathing condition and vice versa
1112017
29
bullThe substantially higher resistive load posed by the oral breathing route provides a plausible explanation for the observation that inhaled ventilation occurs almost exclusively via the nasal route during sleep in subjects with normal nasal resistance
bull Many studies have shown that nasal obstruction can induce or increase apnea frequency in OSA patients When nasal resistance is high a greater pressure drop is required to achieve the same flow and hence collapse of the pharynx is facilitated and this could mitigate the effect of mandibular advancement
bull Moreover high nasal resistance is associated with mouth breathing which could potentially limit the beneficial effect of mandibular advancement
bull Dental Appliance Treatment for Obstructive
bull Andrew S L Chan Richard W W Lee and Peter A Cistulli
bull httpchestjournalchestpubsorgcontent1322693fullhtml
1112017
30
bullCurrent evidence suggests that despite the superior efficacy of CPAP both treatments produce similar subjective and objective health benefits
bullThe superior self-reported tolerance and compliance associated with MAD treatment is a likely explanation
bullThe practice parameters of the AASM recommend the use of oral appliances for mild-to-moderate OSA or for patients with severe OSA who are unable to tolerate CPAP or refuse treatment with CPAP with a required written prescription by a sleep physician
The following are Medicare rules
1) A diagnosis of OSA is not within the dental scope of practice A dentist providing an OA
must do so under the and with the team effort of a licensed Physician with a written
prescription
2) A physician is not skilled in the intricacies of fabricating fitting monitoring adjusting
and choosing an appropriate Oral Appliance individualized per patient
3) A dentist may not provide an oral appliance if the patient has an active
Temporomandibular Disorder
4) The OA must be fabricated within 90 days of the patientrsquos appointment with the sleep
physician
Since the rules are clear and they involve both of our professions it would behoove
both DOMD and DDS to communicate for the benefit of OSA patients
1112017
31
Subsequent to my 3 hour 2013 Meeting with the US Department of Transportation regarding Truckers
bull During the State Board of Dental Examiners meeting Board members put sleep Dentistry in squarely back into the spotlight The Board has addressed sleep Dentistry issues in a public hearing and all four Board meetings in 2013
bull There was discussion that there can be a shared relationship between the Dental and medical scopes of practice
bull Under the proposed rule a Dentist may treat benign snoring with an oral appliance after referral to a licensed physician where appropriate within the standard of care By contrast a Dentist may not diagnose treat or monitor OSA without collaboration with a licensed physician Additionally an oral appliance shall only be fabricated by a licensed Dentist or by a Dental lab under a prescription or work order prepared by a Dentist
American Dental Association
bull Treatment using an oral appliance designed specifically to treat OSA should be fabricated by a dentist familiar with device design maintenance and therapeutic efficacy and who has an association with and a referral from a sleep team
bull JADA Vol 136 p 1123
Donrsquot be afraid of OSA Get a grip on the facts and save patientrsquos lives
1112017
32
bullA SYMBIOTIC RELATION BETWEEN PHYSICIANS SLEEP PROFESSIONALS AND DENTISTS CAN SIGNIFICANTLY IMPROVE THE SLEEP HEALTH OF MILLIONS OF PEOPLE EACH AND EVERY YEAR
bull THAT RELATIONSHIP IS NOT A ONE WAY STREET AND THE
American Sleep amp Breathing Academy of over 8000 members UNDERSTANDS THAThellip JUST LOOK AT THE MULTITUDE OF SLEEP PROFESSIONAL CATAGORIES ON THEIR BOARD OF DIRECTORS
THE END
Thank you for your interest I hope this presentation was helpful
Dr Richard Klein
1112017
9
Scary video by WatchPAT
Obstructive SleepApnea
Definition of Sleep apnea
bullSleep Apnea occurs when the soft tissue in your mouth (the tongue tonsils pharynx uvula etc) relax too much and collapse at the back of your throat and cut off the airway making it difficult or impossible to breath
AHI Three levels of severity
Mild 5 to 15 times per hour
Moderate 15 to 30 times per hour
Severe gt30 times per hour
Copyright 2011 Braebon
1112017
10
SLEEP APNEA SYMPTOMS
bull Short term memory problems
bull Weight gain
bull Tiredness
bull Dry mouth
bull Sore throat
bull Slow metabolism
bull Bed partner frustration
bull AND A PLETHORA OF SERIOUS MEDICAL DISEASES DISORDERS AND MALADIES
High blood pressure
Heart failure
Heart rhythm disturbances
Atherosclerotic heart disease
Pulmonary hypertension
Insulin resistance
Sudden death
Erectile dysfunction
Memory problems
Depression
Anxiety
Gastroesophageal reflux
Sleep Apnea Increases Risk of
bull It has been estimated that 80 of depressed patients complain of disturbed sleep and sleeplessness is a risk factor for impaired mood
bull helliphelliphelliphelliphelliphelliphelliphellip The most common complaint of helliphelliphelliphelliphelliphelliphelliphellip PTSD is sleeplessness and 50 -helliphelliphelliphelliphelliphelliphelliphellip 70 of chronic pain patients helliphelliphelliphelliphelliphelliphelliphelliphellip report disturbed sleep
Consequences
1112017
11
Headachesbull Headaches are the most commonly reported pain complaint in the
population (textbook of pain)
bull Sleep disorders such as sleep apnea are found among headache patients at rates greater than what is found in the general population TX of sleep disorders decreases headache complaints Cephalgia is the most common complaint of TMD
bull (Archives of Internal Medicine)
Risk Factors
ObesityLarge neckSnoringNon-restorative sleepDaytime sleepinessfatigueHigh arched palateRetrognathiaCrowded airwaySmokingdrinking
(and remember sleep apnea occurs in women children and skinny guys toohellipthese are just risk factors)
Life Cycle of a LEAF
1112017
12
The cells in our body deteriorate as we age but they do so much quicker without oxygen
The Beatles were only partially correct when they sang
ldquoAll you need is loverdquo
The Hollies had a better understanding of life when they sangrdquo
ldquoAll I need is the air that I breath and to love yourdquo
1112017
13
NORMAL SLEEP
bull CHARACTERIZED BY A DECREASE IN
bull BODY TEMPERATURE
bull BLOOD PRESSURE
bull BREATHING RATE
bull MOST OTHER BODY FUNCTIONS
bull INCREASED NASAL RESISTANCE
bull CHARACTERIZED BY AN bull ACTIVE BRAIN
1112017
14
Copyright 2011 BRAEBON
Normal healthy breathing during sleep
Wake-up-gasping-choking-and-die-in-your-sleep-diseaserdquo ndash No sound during event
Who gets sent for a sleep study
1112017
15
Who usually doesnrsquot
Sleep apnoea is a common occurrence in femalesKarl A Franklin et al European Respiratory Journal August 2012
bull We investigated 400 females from a population-based random sample of 10000 females aged 20ndash70 years with a questionnaire and anovernight polysomnography
bull Obstructive sleep apnoea was found in 50 of females aged 20ndash70 years
bull Sleep apnoea was related to age obesity and hypertension but not to daytime sleepiness
bull Severe sleep apnoea was scored in 14 of females aged 55ndash70 years and in 31 of obese females with a body-mass index of gt30 kgmiddotmminus2 aged 50ndash70 years
1112017
16
EPWORTH SLEEPINESS SCALEINTERPRETATIONbull 0-7 IT IS UNLIKELY THAT YOU ARE ABNORMALLY SLEEPY
bull 8-9 YOU HAVE AN AVERAGE AMOUNT OF DAYTIME SLEEPINESS
bull 10-15 YOU MAY BE EXCESSIVELY SLEEPY DEPENDING ON THE SITUATION YOU MAY WANT TO CONSIDER SEEKING MEDICAL ATTENTION
bull 16-24 YOU ARE EXCESSIVELY SLEEPY AND SHOULD CONSIDER SEEKING MEDICAL ATTENTION
This person most likely is simply tired or had a bad nightrsquos sleep OSA is not
indicated
I referred this patient to a sleep physician
1112017
17
MALLAMPATI
1112017
18
Lavigne GJ Kato T Kolta A Sessle BJ Neurobiological mechanisms involved in sleep bruxism Crit Rev Oral Biol Med 20031430-46
bullSleep-related bruxism (SB) is characterized by the grinding or clenching of the teeth during sleep usually associated with sleep arousals although the incidence of sleep arousals in SB subjects is within the normal range (up to 14 arousalshour of sleep is considered normal)
IT HAS BEEN SHOWN THAT CPAP ELIMINATION OF OSA alsoELIMINATES SNORING
IT HAS NOT BEEN DEMONSTRATED THAT CPAP TREATMENT OF OSA
ELIMINATES OR REDUCES S-B
Neurobiological mechanisms involved in sleep bruxismLavigne GJ1 Kato T Kolta A Sessle BJ
bull Sleep bruxism (SB) is mainly associated with rhythmic masticatory muscle activity (RMMA) characterized by repetitive jaw muscle contractions (3 bursts or more at a frequency of 1 Hz)
bull The consequences of SB may include tooth destruction jaw pain headaches or the limitation of mandibular movement as well as tooth-grinding sounds that disrupt the sleep of bed partners RMMA is observed in 60 of normal sleepers
1112017
19
bull The pathophysiology of SB is becoming clearer
bull There is an abundance of evidence outlining the neurophysiology and neurochemistry of rhythmic jaw movements (RJM) in relation to chewing swallowing and breathing Several brainstem structures (eg reticular pontis oralis pontis caudalis) and neurochemicals (eg serotonin dopamine gamma aminobutyric acid [GABA] noradrenaline) are involved in both the genesis of RJM and the modulation of muscle tone during sleep
bull It creates a co-activation of both jaw-opening and jaw-closing muscles instead of the alternating jaw-opening and jaw-closing muscle activity pattern typical of chewing
Journal of Pain amp Symptom Management
bullPain duration and intensitywere correlated with decreased sleep impaired sleep quality and delayed sleep onset
Multiple Medical Studies
bullHave published that the majority (59 67 74) of OSA patients will not appropriately wear the CPAP
1112017
20
bull IN 1995 Johnny Cochran said ldquoIf the glove doesnrsquot fithellipyou must acquitrdquo As DR Dement intimated in the 1970s ldquoWe didnt know what to measurehellipso we measured everything we could think ofhellip and it stuckrdquo
bull Almost forty years later some of what ldquostuckrdquo is being revised reinterpreted and common sense is beginning to prevail Seven to eight hours of sleep per night is recommended
The Other 72 of Sleep
bull Sticking with the antiquated definition of a ldquocompliant userrdquo of a
CPAP (4 hrsnight and 5 nightsweek) one must use it roughly 28 of the time
bull WHAT ABOUT THE OTHER 72 OF SLEEP
bull Is it acceptable to not get the O2 we need simply because an antiquated standard ldquostuckrdquo
bull In 1995 CPAP became the gold standard Now in the 21st century I
say ldquoif the mask doesnrsquot fit hellipdonrsquot quitrdquo because an oral appliance may save your health and your life
Treatment of Sleep Apnea
Tracheotomy Oral
Surgery CPAPBiPAP
OA
Behavioral Modification
1112017
21
Orofacial Findings
bullThe most common orofacial characteristics include a retrognathic mandible narrow palate large neck circumference long soft palate tonsillar hypertrophy nasal septal deviation and relative macroglossia
Oral Appliances for Sleep Apnea amp Snoring
Tongue Retaining Devices Mandibular Repositioning Appliances
Oral Appliances (OA)
bull Properly fabricated an oral appliance will protrude the tongue and reposition the mandible anteriorly and inferiorly to the most beneficial neuromuscular position to prevent posterior airway collapse
bull This position is titratable and individualized to exact patient requirements and may need periodic adjustments just as does CPAP
1112017
22
BEFORE
APPLIANCE
7c
WITH
APPLIANCE
9 cc
1112017
23
Copyright 2011 BRAEBON
More Directly Related to hellipDental Sleep Medicine
bull EACH PATIENT IS AN INDIVIDUAL AND JUST AS CPAP PRESSURE IS INDIVIDUALLY TITRATEDhellipSO TOO ARE ORAL APPLIANCES
bull IF I DELIVER AN OA TO A PATIENT WHO WILL NOT UTILIZE THE CPAPhellipI WILL PROVIDE ONE OR SEVERAL HOME SLEEP STUDIES TO ASCERTAIN THE EFFICACY OF THE OAhellip AND THEN I REQUIRE THAT THEY RETURN TO THEIR SLEEP
bull DOCTOR FOR A SUBSEQUENT STUDY WHILE helliphelliphelliphelliphelliphelliphellipUTILIZINGTHE OA
Positional Apnea in a 73-Year Old Male with Atrial Fibrillation
bull This case study illustrates the cost-effective approach to successful outcomes associated with positional therapy that are not surprising and are consistent with a recent study which concluded ldquopositional therapy is equivalent to CPAP at normalizing the AHI in patients with positional OSA with similar effects on sleep quality and nocturnal oxygenationrdquo
bull Journal Sleep Diagnosis and Therapy
1112017
24
HOW THE ORAL APPLIANCE TREATS OSA
bull Prevent collapse of airwaybull Forward advancement of jawbull Support forward tongue positionbull Change shape of pharyngeal airwaybull Increase vertical dimension of occlusionbull Correct dysphagia bull Increase volume of space for tonguebull Trains protrusive tongue reflexesbull Alter position of hyoid bone relative to
mandible
THE VARYING ROLES OF THE NOSE AND MOUTH IN BREATHING
1112017
25
THE NOSE
bull A recent pediatric study reveals why addressing the tongue is so important for resolving sleep apnea As explained in this study having an abnormally short lingual frenulum can result in impaired orofacial growth in early childhood reducing the width of the upper airway
bull The upper airway is very pliable so this increases the risk of it collapsing during sleep They found that children with an untreated short frenulum developed abnormal tongue function early in life which also impacted their orofacial growth and led to disordered breathing during sleep
WHAT IS THE ROLE OF THE NOSE
ITS FUNCTIONS ARE VITAL
bull WARMING
bull HUMIDIFICATION
bull FILTERING
bull CLEANING
OF AMBIENT AIR INHALED INTO THE LUNGS
INFUSION OF NITRIC OXIDE
1112017
26
Humidification and
Dehumidification
bull During intake air is humidified to increase lung oxygen facilitation
bull Upon exhalation air is dehumidified to keep water in our cells
bull If this were not the case we would dehydrate unless we continually drank water
NARES
CONSTRICT
NARES FLARE
SNIFF TEST
1112017
27
Cosmetic Surgery
bullHe couldnrsquot breath through his small nose became hypercapnic and helliphelliphellipdied
Effect of treating severe nasal obstruction on the severity of obstructive sleep apnoea
bull HA McLean AM Urton HS Driver AKW Tan AG Day+ PW Munt and MF Fitzpatrick
bullThis study demonstrates that relief of severe nasal obstruction in patients with a normal retroglossal airway is associated with a significant reduction in mouth breathing during sleep improved sleep architecture and a modest improvement in OSA severity
1112017
28
bullThere are several novel aspects to these findings First the study documents a clearly increased upper airway resistance in association with oral breathing during stable sleep as compared with nasal breathing irrespective of central or OSA
bullSecondly this methodology included simultaneous documentation of oral and nasal ventilation during sleep to confirm the absence of any nasal airflow in the oral breathing condition and vice versa
1112017
29
bullThe substantially higher resistive load posed by the oral breathing route provides a plausible explanation for the observation that inhaled ventilation occurs almost exclusively via the nasal route during sleep in subjects with normal nasal resistance
bull Many studies have shown that nasal obstruction can induce or increase apnea frequency in OSA patients When nasal resistance is high a greater pressure drop is required to achieve the same flow and hence collapse of the pharynx is facilitated and this could mitigate the effect of mandibular advancement
bull Moreover high nasal resistance is associated with mouth breathing which could potentially limit the beneficial effect of mandibular advancement
bull Dental Appliance Treatment for Obstructive
bull Andrew S L Chan Richard W W Lee and Peter A Cistulli
bull httpchestjournalchestpubsorgcontent1322693fullhtml
1112017
30
bullCurrent evidence suggests that despite the superior efficacy of CPAP both treatments produce similar subjective and objective health benefits
bullThe superior self-reported tolerance and compliance associated with MAD treatment is a likely explanation
bullThe practice parameters of the AASM recommend the use of oral appliances for mild-to-moderate OSA or for patients with severe OSA who are unable to tolerate CPAP or refuse treatment with CPAP with a required written prescription by a sleep physician
The following are Medicare rules
1) A diagnosis of OSA is not within the dental scope of practice A dentist providing an OA
must do so under the and with the team effort of a licensed Physician with a written
prescription
2) A physician is not skilled in the intricacies of fabricating fitting monitoring adjusting
and choosing an appropriate Oral Appliance individualized per patient
3) A dentist may not provide an oral appliance if the patient has an active
Temporomandibular Disorder
4) The OA must be fabricated within 90 days of the patientrsquos appointment with the sleep
physician
Since the rules are clear and they involve both of our professions it would behoove
both DOMD and DDS to communicate for the benefit of OSA patients
1112017
31
Subsequent to my 3 hour 2013 Meeting with the US Department of Transportation regarding Truckers
bull During the State Board of Dental Examiners meeting Board members put sleep Dentistry in squarely back into the spotlight The Board has addressed sleep Dentistry issues in a public hearing and all four Board meetings in 2013
bull There was discussion that there can be a shared relationship between the Dental and medical scopes of practice
bull Under the proposed rule a Dentist may treat benign snoring with an oral appliance after referral to a licensed physician where appropriate within the standard of care By contrast a Dentist may not diagnose treat or monitor OSA without collaboration with a licensed physician Additionally an oral appliance shall only be fabricated by a licensed Dentist or by a Dental lab under a prescription or work order prepared by a Dentist
American Dental Association
bull Treatment using an oral appliance designed specifically to treat OSA should be fabricated by a dentist familiar with device design maintenance and therapeutic efficacy and who has an association with and a referral from a sleep team
bull JADA Vol 136 p 1123
Donrsquot be afraid of OSA Get a grip on the facts and save patientrsquos lives
1112017
32
bullA SYMBIOTIC RELATION BETWEEN PHYSICIANS SLEEP PROFESSIONALS AND DENTISTS CAN SIGNIFICANTLY IMPROVE THE SLEEP HEALTH OF MILLIONS OF PEOPLE EACH AND EVERY YEAR
bull THAT RELATIONSHIP IS NOT A ONE WAY STREET AND THE
American Sleep amp Breathing Academy of over 8000 members UNDERSTANDS THAThellip JUST LOOK AT THE MULTITUDE OF SLEEP PROFESSIONAL CATAGORIES ON THEIR BOARD OF DIRECTORS
THE END
Thank you for your interest I hope this presentation was helpful
Dr Richard Klein
1112017
10
SLEEP APNEA SYMPTOMS
bull Short term memory problems
bull Weight gain
bull Tiredness
bull Dry mouth
bull Sore throat
bull Slow metabolism
bull Bed partner frustration
bull AND A PLETHORA OF SERIOUS MEDICAL DISEASES DISORDERS AND MALADIES
High blood pressure
Heart failure
Heart rhythm disturbances
Atherosclerotic heart disease
Pulmonary hypertension
Insulin resistance
Sudden death
Erectile dysfunction
Memory problems
Depression
Anxiety
Gastroesophageal reflux
Sleep Apnea Increases Risk of
bull It has been estimated that 80 of depressed patients complain of disturbed sleep and sleeplessness is a risk factor for impaired mood
bull helliphelliphelliphelliphelliphelliphelliphellip The most common complaint of helliphelliphelliphelliphelliphelliphelliphellip PTSD is sleeplessness and 50 -helliphelliphelliphelliphelliphelliphelliphellip 70 of chronic pain patients helliphelliphelliphelliphelliphelliphelliphelliphellip report disturbed sleep
Consequences
1112017
11
Headachesbull Headaches are the most commonly reported pain complaint in the
population (textbook of pain)
bull Sleep disorders such as sleep apnea are found among headache patients at rates greater than what is found in the general population TX of sleep disorders decreases headache complaints Cephalgia is the most common complaint of TMD
bull (Archives of Internal Medicine)
Risk Factors
ObesityLarge neckSnoringNon-restorative sleepDaytime sleepinessfatigueHigh arched palateRetrognathiaCrowded airwaySmokingdrinking
(and remember sleep apnea occurs in women children and skinny guys toohellipthese are just risk factors)
Life Cycle of a LEAF
1112017
12
The cells in our body deteriorate as we age but they do so much quicker without oxygen
The Beatles were only partially correct when they sang
ldquoAll you need is loverdquo
The Hollies had a better understanding of life when they sangrdquo
ldquoAll I need is the air that I breath and to love yourdquo
1112017
13
NORMAL SLEEP
bull CHARACTERIZED BY A DECREASE IN
bull BODY TEMPERATURE
bull BLOOD PRESSURE
bull BREATHING RATE
bull MOST OTHER BODY FUNCTIONS
bull INCREASED NASAL RESISTANCE
bull CHARACTERIZED BY AN bull ACTIVE BRAIN
1112017
14
Copyright 2011 BRAEBON
Normal healthy breathing during sleep
Wake-up-gasping-choking-and-die-in-your-sleep-diseaserdquo ndash No sound during event
Who gets sent for a sleep study
1112017
15
Who usually doesnrsquot
Sleep apnoea is a common occurrence in femalesKarl A Franklin et al European Respiratory Journal August 2012
bull We investigated 400 females from a population-based random sample of 10000 females aged 20ndash70 years with a questionnaire and anovernight polysomnography
bull Obstructive sleep apnoea was found in 50 of females aged 20ndash70 years
bull Sleep apnoea was related to age obesity and hypertension but not to daytime sleepiness
bull Severe sleep apnoea was scored in 14 of females aged 55ndash70 years and in 31 of obese females with a body-mass index of gt30 kgmiddotmminus2 aged 50ndash70 years
1112017
16
EPWORTH SLEEPINESS SCALEINTERPRETATIONbull 0-7 IT IS UNLIKELY THAT YOU ARE ABNORMALLY SLEEPY
bull 8-9 YOU HAVE AN AVERAGE AMOUNT OF DAYTIME SLEEPINESS
bull 10-15 YOU MAY BE EXCESSIVELY SLEEPY DEPENDING ON THE SITUATION YOU MAY WANT TO CONSIDER SEEKING MEDICAL ATTENTION
bull 16-24 YOU ARE EXCESSIVELY SLEEPY AND SHOULD CONSIDER SEEKING MEDICAL ATTENTION
This person most likely is simply tired or had a bad nightrsquos sleep OSA is not
indicated
I referred this patient to a sleep physician
1112017
17
MALLAMPATI
1112017
18
Lavigne GJ Kato T Kolta A Sessle BJ Neurobiological mechanisms involved in sleep bruxism Crit Rev Oral Biol Med 20031430-46
bullSleep-related bruxism (SB) is characterized by the grinding or clenching of the teeth during sleep usually associated with sleep arousals although the incidence of sleep arousals in SB subjects is within the normal range (up to 14 arousalshour of sleep is considered normal)
IT HAS BEEN SHOWN THAT CPAP ELIMINATION OF OSA alsoELIMINATES SNORING
IT HAS NOT BEEN DEMONSTRATED THAT CPAP TREATMENT OF OSA
ELIMINATES OR REDUCES S-B
Neurobiological mechanisms involved in sleep bruxismLavigne GJ1 Kato T Kolta A Sessle BJ
bull Sleep bruxism (SB) is mainly associated with rhythmic masticatory muscle activity (RMMA) characterized by repetitive jaw muscle contractions (3 bursts or more at a frequency of 1 Hz)
bull The consequences of SB may include tooth destruction jaw pain headaches or the limitation of mandibular movement as well as tooth-grinding sounds that disrupt the sleep of bed partners RMMA is observed in 60 of normal sleepers
1112017
19
bull The pathophysiology of SB is becoming clearer
bull There is an abundance of evidence outlining the neurophysiology and neurochemistry of rhythmic jaw movements (RJM) in relation to chewing swallowing and breathing Several brainstem structures (eg reticular pontis oralis pontis caudalis) and neurochemicals (eg serotonin dopamine gamma aminobutyric acid [GABA] noradrenaline) are involved in both the genesis of RJM and the modulation of muscle tone during sleep
bull It creates a co-activation of both jaw-opening and jaw-closing muscles instead of the alternating jaw-opening and jaw-closing muscle activity pattern typical of chewing
Journal of Pain amp Symptom Management
bullPain duration and intensitywere correlated with decreased sleep impaired sleep quality and delayed sleep onset
Multiple Medical Studies
bullHave published that the majority (59 67 74) of OSA patients will not appropriately wear the CPAP
1112017
20
bull IN 1995 Johnny Cochran said ldquoIf the glove doesnrsquot fithellipyou must acquitrdquo As DR Dement intimated in the 1970s ldquoWe didnt know what to measurehellipso we measured everything we could think ofhellip and it stuckrdquo
bull Almost forty years later some of what ldquostuckrdquo is being revised reinterpreted and common sense is beginning to prevail Seven to eight hours of sleep per night is recommended
The Other 72 of Sleep
bull Sticking with the antiquated definition of a ldquocompliant userrdquo of a
CPAP (4 hrsnight and 5 nightsweek) one must use it roughly 28 of the time
bull WHAT ABOUT THE OTHER 72 OF SLEEP
bull Is it acceptable to not get the O2 we need simply because an antiquated standard ldquostuckrdquo
bull In 1995 CPAP became the gold standard Now in the 21st century I
say ldquoif the mask doesnrsquot fit hellipdonrsquot quitrdquo because an oral appliance may save your health and your life
Treatment of Sleep Apnea
Tracheotomy Oral
Surgery CPAPBiPAP
OA
Behavioral Modification
1112017
21
Orofacial Findings
bullThe most common orofacial characteristics include a retrognathic mandible narrow palate large neck circumference long soft palate tonsillar hypertrophy nasal septal deviation and relative macroglossia
Oral Appliances for Sleep Apnea amp Snoring
Tongue Retaining Devices Mandibular Repositioning Appliances
Oral Appliances (OA)
bull Properly fabricated an oral appliance will protrude the tongue and reposition the mandible anteriorly and inferiorly to the most beneficial neuromuscular position to prevent posterior airway collapse
bull This position is titratable and individualized to exact patient requirements and may need periodic adjustments just as does CPAP
1112017
22
BEFORE
APPLIANCE
7c
WITH
APPLIANCE
9 cc
1112017
23
Copyright 2011 BRAEBON
More Directly Related to hellipDental Sleep Medicine
bull EACH PATIENT IS AN INDIVIDUAL AND JUST AS CPAP PRESSURE IS INDIVIDUALLY TITRATEDhellipSO TOO ARE ORAL APPLIANCES
bull IF I DELIVER AN OA TO A PATIENT WHO WILL NOT UTILIZE THE CPAPhellipI WILL PROVIDE ONE OR SEVERAL HOME SLEEP STUDIES TO ASCERTAIN THE EFFICACY OF THE OAhellip AND THEN I REQUIRE THAT THEY RETURN TO THEIR SLEEP
bull DOCTOR FOR A SUBSEQUENT STUDY WHILE helliphelliphelliphelliphelliphelliphellipUTILIZINGTHE OA
Positional Apnea in a 73-Year Old Male with Atrial Fibrillation
bull This case study illustrates the cost-effective approach to successful outcomes associated with positional therapy that are not surprising and are consistent with a recent study which concluded ldquopositional therapy is equivalent to CPAP at normalizing the AHI in patients with positional OSA with similar effects on sleep quality and nocturnal oxygenationrdquo
bull Journal Sleep Diagnosis and Therapy
1112017
24
HOW THE ORAL APPLIANCE TREATS OSA
bull Prevent collapse of airwaybull Forward advancement of jawbull Support forward tongue positionbull Change shape of pharyngeal airwaybull Increase vertical dimension of occlusionbull Correct dysphagia bull Increase volume of space for tonguebull Trains protrusive tongue reflexesbull Alter position of hyoid bone relative to
mandible
THE VARYING ROLES OF THE NOSE AND MOUTH IN BREATHING
1112017
25
THE NOSE
bull A recent pediatric study reveals why addressing the tongue is so important for resolving sleep apnea As explained in this study having an abnormally short lingual frenulum can result in impaired orofacial growth in early childhood reducing the width of the upper airway
bull The upper airway is very pliable so this increases the risk of it collapsing during sleep They found that children with an untreated short frenulum developed abnormal tongue function early in life which also impacted their orofacial growth and led to disordered breathing during sleep
WHAT IS THE ROLE OF THE NOSE
ITS FUNCTIONS ARE VITAL
bull WARMING
bull HUMIDIFICATION
bull FILTERING
bull CLEANING
OF AMBIENT AIR INHALED INTO THE LUNGS
INFUSION OF NITRIC OXIDE
1112017
26
Humidification and
Dehumidification
bull During intake air is humidified to increase lung oxygen facilitation
bull Upon exhalation air is dehumidified to keep water in our cells
bull If this were not the case we would dehydrate unless we continually drank water
NARES
CONSTRICT
NARES FLARE
SNIFF TEST
1112017
27
Cosmetic Surgery
bullHe couldnrsquot breath through his small nose became hypercapnic and helliphelliphellipdied
Effect of treating severe nasal obstruction on the severity of obstructive sleep apnoea
bull HA McLean AM Urton HS Driver AKW Tan AG Day+ PW Munt and MF Fitzpatrick
bullThis study demonstrates that relief of severe nasal obstruction in patients with a normal retroglossal airway is associated with a significant reduction in mouth breathing during sleep improved sleep architecture and a modest improvement in OSA severity
1112017
28
bullThere are several novel aspects to these findings First the study documents a clearly increased upper airway resistance in association with oral breathing during stable sleep as compared with nasal breathing irrespective of central or OSA
bullSecondly this methodology included simultaneous documentation of oral and nasal ventilation during sleep to confirm the absence of any nasal airflow in the oral breathing condition and vice versa
1112017
29
bullThe substantially higher resistive load posed by the oral breathing route provides a plausible explanation for the observation that inhaled ventilation occurs almost exclusively via the nasal route during sleep in subjects with normal nasal resistance
bull Many studies have shown that nasal obstruction can induce or increase apnea frequency in OSA patients When nasal resistance is high a greater pressure drop is required to achieve the same flow and hence collapse of the pharynx is facilitated and this could mitigate the effect of mandibular advancement
bull Moreover high nasal resistance is associated with mouth breathing which could potentially limit the beneficial effect of mandibular advancement
bull Dental Appliance Treatment for Obstructive
bull Andrew S L Chan Richard W W Lee and Peter A Cistulli
bull httpchestjournalchestpubsorgcontent1322693fullhtml
1112017
30
bullCurrent evidence suggests that despite the superior efficacy of CPAP both treatments produce similar subjective and objective health benefits
bullThe superior self-reported tolerance and compliance associated with MAD treatment is a likely explanation
bullThe practice parameters of the AASM recommend the use of oral appliances for mild-to-moderate OSA or for patients with severe OSA who are unable to tolerate CPAP or refuse treatment with CPAP with a required written prescription by a sleep physician
The following are Medicare rules
1) A diagnosis of OSA is not within the dental scope of practice A dentist providing an OA
must do so under the and with the team effort of a licensed Physician with a written
prescription
2) A physician is not skilled in the intricacies of fabricating fitting monitoring adjusting
and choosing an appropriate Oral Appliance individualized per patient
3) A dentist may not provide an oral appliance if the patient has an active
Temporomandibular Disorder
4) The OA must be fabricated within 90 days of the patientrsquos appointment with the sleep
physician
Since the rules are clear and they involve both of our professions it would behoove
both DOMD and DDS to communicate for the benefit of OSA patients
1112017
31
Subsequent to my 3 hour 2013 Meeting with the US Department of Transportation regarding Truckers
bull During the State Board of Dental Examiners meeting Board members put sleep Dentistry in squarely back into the spotlight The Board has addressed sleep Dentistry issues in a public hearing and all four Board meetings in 2013
bull There was discussion that there can be a shared relationship between the Dental and medical scopes of practice
bull Under the proposed rule a Dentist may treat benign snoring with an oral appliance after referral to a licensed physician where appropriate within the standard of care By contrast a Dentist may not diagnose treat or monitor OSA without collaboration with a licensed physician Additionally an oral appliance shall only be fabricated by a licensed Dentist or by a Dental lab under a prescription or work order prepared by a Dentist
American Dental Association
bull Treatment using an oral appliance designed specifically to treat OSA should be fabricated by a dentist familiar with device design maintenance and therapeutic efficacy and who has an association with and a referral from a sleep team
bull JADA Vol 136 p 1123
Donrsquot be afraid of OSA Get a grip on the facts and save patientrsquos lives
1112017
32
bullA SYMBIOTIC RELATION BETWEEN PHYSICIANS SLEEP PROFESSIONALS AND DENTISTS CAN SIGNIFICANTLY IMPROVE THE SLEEP HEALTH OF MILLIONS OF PEOPLE EACH AND EVERY YEAR
bull THAT RELATIONSHIP IS NOT A ONE WAY STREET AND THE
American Sleep amp Breathing Academy of over 8000 members UNDERSTANDS THAThellip JUST LOOK AT THE MULTITUDE OF SLEEP PROFESSIONAL CATAGORIES ON THEIR BOARD OF DIRECTORS
THE END
Thank you for your interest I hope this presentation was helpful
Dr Richard Klein
1112017
11
Headachesbull Headaches are the most commonly reported pain complaint in the
population (textbook of pain)
bull Sleep disorders such as sleep apnea are found among headache patients at rates greater than what is found in the general population TX of sleep disorders decreases headache complaints Cephalgia is the most common complaint of TMD
bull (Archives of Internal Medicine)
Risk Factors
ObesityLarge neckSnoringNon-restorative sleepDaytime sleepinessfatigueHigh arched palateRetrognathiaCrowded airwaySmokingdrinking
(and remember sleep apnea occurs in women children and skinny guys toohellipthese are just risk factors)
Life Cycle of a LEAF
1112017
12
The cells in our body deteriorate as we age but they do so much quicker without oxygen
The Beatles were only partially correct when they sang
ldquoAll you need is loverdquo
The Hollies had a better understanding of life when they sangrdquo
ldquoAll I need is the air that I breath and to love yourdquo
1112017
13
NORMAL SLEEP
bull CHARACTERIZED BY A DECREASE IN
bull BODY TEMPERATURE
bull BLOOD PRESSURE
bull BREATHING RATE
bull MOST OTHER BODY FUNCTIONS
bull INCREASED NASAL RESISTANCE
bull CHARACTERIZED BY AN bull ACTIVE BRAIN
1112017
14
Copyright 2011 BRAEBON
Normal healthy breathing during sleep
Wake-up-gasping-choking-and-die-in-your-sleep-diseaserdquo ndash No sound during event
Who gets sent for a sleep study
1112017
15
Who usually doesnrsquot
Sleep apnoea is a common occurrence in femalesKarl A Franklin et al European Respiratory Journal August 2012
bull We investigated 400 females from a population-based random sample of 10000 females aged 20ndash70 years with a questionnaire and anovernight polysomnography
bull Obstructive sleep apnoea was found in 50 of females aged 20ndash70 years
bull Sleep apnoea was related to age obesity and hypertension but not to daytime sleepiness
bull Severe sleep apnoea was scored in 14 of females aged 55ndash70 years and in 31 of obese females with a body-mass index of gt30 kgmiddotmminus2 aged 50ndash70 years
1112017
16
EPWORTH SLEEPINESS SCALEINTERPRETATIONbull 0-7 IT IS UNLIKELY THAT YOU ARE ABNORMALLY SLEEPY
bull 8-9 YOU HAVE AN AVERAGE AMOUNT OF DAYTIME SLEEPINESS
bull 10-15 YOU MAY BE EXCESSIVELY SLEEPY DEPENDING ON THE SITUATION YOU MAY WANT TO CONSIDER SEEKING MEDICAL ATTENTION
bull 16-24 YOU ARE EXCESSIVELY SLEEPY AND SHOULD CONSIDER SEEKING MEDICAL ATTENTION
This person most likely is simply tired or had a bad nightrsquos sleep OSA is not
indicated
I referred this patient to a sleep physician
1112017
17
MALLAMPATI
1112017
18
Lavigne GJ Kato T Kolta A Sessle BJ Neurobiological mechanisms involved in sleep bruxism Crit Rev Oral Biol Med 20031430-46
bullSleep-related bruxism (SB) is characterized by the grinding or clenching of the teeth during sleep usually associated with sleep arousals although the incidence of sleep arousals in SB subjects is within the normal range (up to 14 arousalshour of sleep is considered normal)
IT HAS BEEN SHOWN THAT CPAP ELIMINATION OF OSA alsoELIMINATES SNORING
IT HAS NOT BEEN DEMONSTRATED THAT CPAP TREATMENT OF OSA
ELIMINATES OR REDUCES S-B
Neurobiological mechanisms involved in sleep bruxismLavigne GJ1 Kato T Kolta A Sessle BJ
bull Sleep bruxism (SB) is mainly associated with rhythmic masticatory muscle activity (RMMA) characterized by repetitive jaw muscle contractions (3 bursts or more at a frequency of 1 Hz)
bull The consequences of SB may include tooth destruction jaw pain headaches or the limitation of mandibular movement as well as tooth-grinding sounds that disrupt the sleep of bed partners RMMA is observed in 60 of normal sleepers
1112017
19
bull The pathophysiology of SB is becoming clearer
bull There is an abundance of evidence outlining the neurophysiology and neurochemistry of rhythmic jaw movements (RJM) in relation to chewing swallowing and breathing Several brainstem structures (eg reticular pontis oralis pontis caudalis) and neurochemicals (eg serotonin dopamine gamma aminobutyric acid [GABA] noradrenaline) are involved in both the genesis of RJM and the modulation of muscle tone during sleep
bull It creates a co-activation of both jaw-opening and jaw-closing muscles instead of the alternating jaw-opening and jaw-closing muscle activity pattern typical of chewing
Journal of Pain amp Symptom Management
bullPain duration and intensitywere correlated with decreased sleep impaired sleep quality and delayed sleep onset
Multiple Medical Studies
bullHave published that the majority (59 67 74) of OSA patients will not appropriately wear the CPAP
1112017
20
bull IN 1995 Johnny Cochran said ldquoIf the glove doesnrsquot fithellipyou must acquitrdquo As DR Dement intimated in the 1970s ldquoWe didnt know what to measurehellipso we measured everything we could think ofhellip and it stuckrdquo
bull Almost forty years later some of what ldquostuckrdquo is being revised reinterpreted and common sense is beginning to prevail Seven to eight hours of sleep per night is recommended
The Other 72 of Sleep
bull Sticking with the antiquated definition of a ldquocompliant userrdquo of a
CPAP (4 hrsnight and 5 nightsweek) one must use it roughly 28 of the time
bull WHAT ABOUT THE OTHER 72 OF SLEEP
bull Is it acceptable to not get the O2 we need simply because an antiquated standard ldquostuckrdquo
bull In 1995 CPAP became the gold standard Now in the 21st century I
say ldquoif the mask doesnrsquot fit hellipdonrsquot quitrdquo because an oral appliance may save your health and your life
Treatment of Sleep Apnea
Tracheotomy Oral
Surgery CPAPBiPAP
OA
Behavioral Modification
1112017
21
Orofacial Findings
bullThe most common orofacial characteristics include a retrognathic mandible narrow palate large neck circumference long soft palate tonsillar hypertrophy nasal septal deviation and relative macroglossia
Oral Appliances for Sleep Apnea amp Snoring
Tongue Retaining Devices Mandibular Repositioning Appliances
Oral Appliances (OA)
bull Properly fabricated an oral appliance will protrude the tongue and reposition the mandible anteriorly and inferiorly to the most beneficial neuromuscular position to prevent posterior airway collapse
bull This position is titratable and individualized to exact patient requirements and may need periodic adjustments just as does CPAP
1112017
22
BEFORE
APPLIANCE
7c
WITH
APPLIANCE
9 cc
1112017
23
Copyright 2011 BRAEBON
More Directly Related to hellipDental Sleep Medicine
bull EACH PATIENT IS AN INDIVIDUAL AND JUST AS CPAP PRESSURE IS INDIVIDUALLY TITRATEDhellipSO TOO ARE ORAL APPLIANCES
bull IF I DELIVER AN OA TO A PATIENT WHO WILL NOT UTILIZE THE CPAPhellipI WILL PROVIDE ONE OR SEVERAL HOME SLEEP STUDIES TO ASCERTAIN THE EFFICACY OF THE OAhellip AND THEN I REQUIRE THAT THEY RETURN TO THEIR SLEEP
bull DOCTOR FOR A SUBSEQUENT STUDY WHILE helliphelliphelliphelliphelliphelliphellipUTILIZINGTHE OA
Positional Apnea in a 73-Year Old Male with Atrial Fibrillation
bull This case study illustrates the cost-effective approach to successful outcomes associated with positional therapy that are not surprising and are consistent with a recent study which concluded ldquopositional therapy is equivalent to CPAP at normalizing the AHI in patients with positional OSA with similar effects on sleep quality and nocturnal oxygenationrdquo
bull Journal Sleep Diagnosis and Therapy
1112017
24
HOW THE ORAL APPLIANCE TREATS OSA
bull Prevent collapse of airwaybull Forward advancement of jawbull Support forward tongue positionbull Change shape of pharyngeal airwaybull Increase vertical dimension of occlusionbull Correct dysphagia bull Increase volume of space for tonguebull Trains protrusive tongue reflexesbull Alter position of hyoid bone relative to
mandible
THE VARYING ROLES OF THE NOSE AND MOUTH IN BREATHING
1112017
25
THE NOSE
bull A recent pediatric study reveals why addressing the tongue is so important for resolving sleep apnea As explained in this study having an abnormally short lingual frenulum can result in impaired orofacial growth in early childhood reducing the width of the upper airway
bull The upper airway is very pliable so this increases the risk of it collapsing during sleep They found that children with an untreated short frenulum developed abnormal tongue function early in life which also impacted their orofacial growth and led to disordered breathing during sleep
WHAT IS THE ROLE OF THE NOSE
ITS FUNCTIONS ARE VITAL
bull WARMING
bull HUMIDIFICATION
bull FILTERING
bull CLEANING
OF AMBIENT AIR INHALED INTO THE LUNGS
INFUSION OF NITRIC OXIDE
1112017
26
Humidification and
Dehumidification
bull During intake air is humidified to increase lung oxygen facilitation
bull Upon exhalation air is dehumidified to keep water in our cells
bull If this were not the case we would dehydrate unless we continually drank water
NARES
CONSTRICT
NARES FLARE
SNIFF TEST
1112017
27
Cosmetic Surgery
bullHe couldnrsquot breath through his small nose became hypercapnic and helliphelliphellipdied
Effect of treating severe nasal obstruction on the severity of obstructive sleep apnoea
bull HA McLean AM Urton HS Driver AKW Tan AG Day+ PW Munt and MF Fitzpatrick
bullThis study demonstrates that relief of severe nasal obstruction in patients with a normal retroglossal airway is associated with a significant reduction in mouth breathing during sleep improved sleep architecture and a modest improvement in OSA severity
1112017
28
bullThere are several novel aspects to these findings First the study documents a clearly increased upper airway resistance in association with oral breathing during stable sleep as compared with nasal breathing irrespective of central or OSA
bullSecondly this methodology included simultaneous documentation of oral and nasal ventilation during sleep to confirm the absence of any nasal airflow in the oral breathing condition and vice versa
1112017
29
bullThe substantially higher resistive load posed by the oral breathing route provides a plausible explanation for the observation that inhaled ventilation occurs almost exclusively via the nasal route during sleep in subjects with normal nasal resistance
bull Many studies have shown that nasal obstruction can induce or increase apnea frequency in OSA patients When nasal resistance is high a greater pressure drop is required to achieve the same flow and hence collapse of the pharynx is facilitated and this could mitigate the effect of mandibular advancement
bull Moreover high nasal resistance is associated with mouth breathing which could potentially limit the beneficial effect of mandibular advancement
bull Dental Appliance Treatment for Obstructive
bull Andrew S L Chan Richard W W Lee and Peter A Cistulli
bull httpchestjournalchestpubsorgcontent1322693fullhtml
1112017
30
bullCurrent evidence suggests that despite the superior efficacy of CPAP both treatments produce similar subjective and objective health benefits
bullThe superior self-reported tolerance and compliance associated with MAD treatment is a likely explanation
bullThe practice parameters of the AASM recommend the use of oral appliances for mild-to-moderate OSA or for patients with severe OSA who are unable to tolerate CPAP or refuse treatment with CPAP with a required written prescription by a sleep physician
The following are Medicare rules
1) A diagnosis of OSA is not within the dental scope of practice A dentist providing an OA
must do so under the and with the team effort of a licensed Physician with a written
prescription
2) A physician is not skilled in the intricacies of fabricating fitting monitoring adjusting
and choosing an appropriate Oral Appliance individualized per patient
3) A dentist may not provide an oral appliance if the patient has an active
Temporomandibular Disorder
4) The OA must be fabricated within 90 days of the patientrsquos appointment with the sleep
physician
Since the rules are clear and they involve both of our professions it would behoove
both DOMD and DDS to communicate for the benefit of OSA patients
1112017
31
Subsequent to my 3 hour 2013 Meeting with the US Department of Transportation regarding Truckers
bull During the State Board of Dental Examiners meeting Board members put sleep Dentistry in squarely back into the spotlight The Board has addressed sleep Dentistry issues in a public hearing and all four Board meetings in 2013
bull There was discussion that there can be a shared relationship between the Dental and medical scopes of practice
bull Under the proposed rule a Dentist may treat benign snoring with an oral appliance after referral to a licensed physician where appropriate within the standard of care By contrast a Dentist may not diagnose treat or monitor OSA without collaboration with a licensed physician Additionally an oral appliance shall only be fabricated by a licensed Dentist or by a Dental lab under a prescription or work order prepared by a Dentist
American Dental Association
bull Treatment using an oral appliance designed specifically to treat OSA should be fabricated by a dentist familiar with device design maintenance and therapeutic efficacy and who has an association with and a referral from a sleep team
bull JADA Vol 136 p 1123
Donrsquot be afraid of OSA Get a grip on the facts and save patientrsquos lives
1112017
32
bullA SYMBIOTIC RELATION BETWEEN PHYSICIANS SLEEP PROFESSIONALS AND DENTISTS CAN SIGNIFICANTLY IMPROVE THE SLEEP HEALTH OF MILLIONS OF PEOPLE EACH AND EVERY YEAR
bull THAT RELATIONSHIP IS NOT A ONE WAY STREET AND THE
American Sleep amp Breathing Academy of over 8000 members UNDERSTANDS THAThellip JUST LOOK AT THE MULTITUDE OF SLEEP PROFESSIONAL CATAGORIES ON THEIR BOARD OF DIRECTORS
THE END
Thank you for your interest I hope this presentation was helpful
Dr Richard Klein
1112017
12
The cells in our body deteriorate as we age but they do so much quicker without oxygen
The Beatles were only partially correct when they sang
ldquoAll you need is loverdquo
The Hollies had a better understanding of life when they sangrdquo
ldquoAll I need is the air that I breath and to love yourdquo
1112017
13
NORMAL SLEEP
bull CHARACTERIZED BY A DECREASE IN
bull BODY TEMPERATURE
bull BLOOD PRESSURE
bull BREATHING RATE
bull MOST OTHER BODY FUNCTIONS
bull INCREASED NASAL RESISTANCE
bull CHARACTERIZED BY AN bull ACTIVE BRAIN
1112017
14
Copyright 2011 BRAEBON
Normal healthy breathing during sleep
Wake-up-gasping-choking-and-die-in-your-sleep-diseaserdquo ndash No sound during event
Who gets sent for a sleep study
1112017
15
Who usually doesnrsquot
Sleep apnoea is a common occurrence in femalesKarl A Franklin et al European Respiratory Journal August 2012
bull We investigated 400 females from a population-based random sample of 10000 females aged 20ndash70 years with a questionnaire and anovernight polysomnography
bull Obstructive sleep apnoea was found in 50 of females aged 20ndash70 years
bull Sleep apnoea was related to age obesity and hypertension but not to daytime sleepiness
bull Severe sleep apnoea was scored in 14 of females aged 55ndash70 years and in 31 of obese females with a body-mass index of gt30 kgmiddotmminus2 aged 50ndash70 years
1112017
16
EPWORTH SLEEPINESS SCALEINTERPRETATIONbull 0-7 IT IS UNLIKELY THAT YOU ARE ABNORMALLY SLEEPY
bull 8-9 YOU HAVE AN AVERAGE AMOUNT OF DAYTIME SLEEPINESS
bull 10-15 YOU MAY BE EXCESSIVELY SLEEPY DEPENDING ON THE SITUATION YOU MAY WANT TO CONSIDER SEEKING MEDICAL ATTENTION
bull 16-24 YOU ARE EXCESSIVELY SLEEPY AND SHOULD CONSIDER SEEKING MEDICAL ATTENTION
This person most likely is simply tired or had a bad nightrsquos sleep OSA is not
indicated
I referred this patient to a sleep physician
1112017
17
MALLAMPATI
1112017
18
Lavigne GJ Kato T Kolta A Sessle BJ Neurobiological mechanisms involved in sleep bruxism Crit Rev Oral Biol Med 20031430-46
bullSleep-related bruxism (SB) is characterized by the grinding or clenching of the teeth during sleep usually associated with sleep arousals although the incidence of sleep arousals in SB subjects is within the normal range (up to 14 arousalshour of sleep is considered normal)
IT HAS BEEN SHOWN THAT CPAP ELIMINATION OF OSA alsoELIMINATES SNORING
IT HAS NOT BEEN DEMONSTRATED THAT CPAP TREATMENT OF OSA
ELIMINATES OR REDUCES S-B
Neurobiological mechanisms involved in sleep bruxismLavigne GJ1 Kato T Kolta A Sessle BJ
bull Sleep bruxism (SB) is mainly associated with rhythmic masticatory muscle activity (RMMA) characterized by repetitive jaw muscle contractions (3 bursts or more at a frequency of 1 Hz)
bull The consequences of SB may include tooth destruction jaw pain headaches or the limitation of mandibular movement as well as tooth-grinding sounds that disrupt the sleep of bed partners RMMA is observed in 60 of normal sleepers
1112017
19
bull The pathophysiology of SB is becoming clearer
bull There is an abundance of evidence outlining the neurophysiology and neurochemistry of rhythmic jaw movements (RJM) in relation to chewing swallowing and breathing Several brainstem structures (eg reticular pontis oralis pontis caudalis) and neurochemicals (eg serotonin dopamine gamma aminobutyric acid [GABA] noradrenaline) are involved in both the genesis of RJM and the modulation of muscle tone during sleep
bull It creates a co-activation of both jaw-opening and jaw-closing muscles instead of the alternating jaw-opening and jaw-closing muscle activity pattern typical of chewing
Journal of Pain amp Symptom Management
bullPain duration and intensitywere correlated with decreased sleep impaired sleep quality and delayed sleep onset
Multiple Medical Studies
bullHave published that the majority (59 67 74) of OSA patients will not appropriately wear the CPAP
1112017
20
bull IN 1995 Johnny Cochran said ldquoIf the glove doesnrsquot fithellipyou must acquitrdquo As DR Dement intimated in the 1970s ldquoWe didnt know what to measurehellipso we measured everything we could think ofhellip and it stuckrdquo
bull Almost forty years later some of what ldquostuckrdquo is being revised reinterpreted and common sense is beginning to prevail Seven to eight hours of sleep per night is recommended
The Other 72 of Sleep
bull Sticking with the antiquated definition of a ldquocompliant userrdquo of a
CPAP (4 hrsnight and 5 nightsweek) one must use it roughly 28 of the time
bull WHAT ABOUT THE OTHER 72 OF SLEEP
bull Is it acceptable to not get the O2 we need simply because an antiquated standard ldquostuckrdquo
bull In 1995 CPAP became the gold standard Now in the 21st century I
say ldquoif the mask doesnrsquot fit hellipdonrsquot quitrdquo because an oral appliance may save your health and your life
Treatment of Sleep Apnea
Tracheotomy Oral
Surgery CPAPBiPAP
OA
Behavioral Modification
1112017
21
Orofacial Findings
bullThe most common orofacial characteristics include a retrognathic mandible narrow palate large neck circumference long soft palate tonsillar hypertrophy nasal septal deviation and relative macroglossia
Oral Appliances for Sleep Apnea amp Snoring
Tongue Retaining Devices Mandibular Repositioning Appliances
Oral Appliances (OA)
bull Properly fabricated an oral appliance will protrude the tongue and reposition the mandible anteriorly and inferiorly to the most beneficial neuromuscular position to prevent posterior airway collapse
bull This position is titratable and individualized to exact patient requirements and may need periodic adjustments just as does CPAP
1112017
22
BEFORE
APPLIANCE
7c
WITH
APPLIANCE
9 cc
1112017
23
Copyright 2011 BRAEBON
More Directly Related to hellipDental Sleep Medicine
bull EACH PATIENT IS AN INDIVIDUAL AND JUST AS CPAP PRESSURE IS INDIVIDUALLY TITRATEDhellipSO TOO ARE ORAL APPLIANCES
bull IF I DELIVER AN OA TO A PATIENT WHO WILL NOT UTILIZE THE CPAPhellipI WILL PROVIDE ONE OR SEVERAL HOME SLEEP STUDIES TO ASCERTAIN THE EFFICACY OF THE OAhellip AND THEN I REQUIRE THAT THEY RETURN TO THEIR SLEEP
bull DOCTOR FOR A SUBSEQUENT STUDY WHILE helliphelliphelliphelliphelliphelliphellipUTILIZINGTHE OA
Positional Apnea in a 73-Year Old Male with Atrial Fibrillation
bull This case study illustrates the cost-effective approach to successful outcomes associated with positional therapy that are not surprising and are consistent with a recent study which concluded ldquopositional therapy is equivalent to CPAP at normalizing the AHI in patients with positional OSA with similar effects on sleep quality and nocturnal oxygenationrdquo
bull Journal Sleep Diagnosis and Therapy
1112017
24
HOW THE ORAL APPLIANCE TREATS OSA
bull Prevent collapse of airwaybull Forward advancement of jawbull Support forward tongue positionbull Change shape of pharyngeal airwaybull Increase vertical dimension of occlusionbull Correct dysphagia bull Increase volume of space for tonguebull Trains protrusive tongue reflexesbull Alter position of hyoid bone relative to
mandible
THE VARYING ROLES OF THE NOSE AND MOUTH IN BREATHING
1112017
25
THE NOSE
bull A recent pediatric study reveals why addressing the tongue is so important for resolving sleep apnea As explained in this study having an abnormally short lingual frenulum can result in impaired orofacial growth in early childhood reducing the width of the upper airway
bull The upper airway is very pliable so this increases the risk of it collapsing during sleep They found that children with an untreated short frenulum developed abnormal tongue function early in life which also impacted their orofacial growth and led to disordered breathing during sleep
WHAT IS THE ROLE OF THE NOSE
ITS FUNCTIONS ARE VITAL
bull WARMING
bull HUMIDIFICATION
bull FILTERING
bull CLEANING
OF AMBIENT AIR INHALED INTO THE LUNGS
INFUSION OF NITRIC OXIDE
1112017
26
Humidification and
Dehumidification
bull During intake air is humidified to increase lung oxygen facilitation
bull Upon exhalation air is dehumidified to keep water in our cells
bull If this were not the case we would dehydrate unless we continually drank water
NARES
CONSTRICT
NARES FLARE
SNIFF TEST
1112017
27
Cosmetic Surgery
bullHe couldnrsquot breath through his small nose became hypercapnic and helliphelliphellipdied
Effect of treating severe nasal obstruction on the severity of obstructive sleep apnoea
bull HA McLean AM Urton HS Driver AKW Tan AG Day+ PW Munt and MF Fitzpatrick
bullThis study demonstrates that relief of severe nasal obstruction in patients with a normal retroglossal airway is associated with a significant reduction in mouth breathing during sleep improved sleep architecture and a modest improvement in OSA severity
1112017
28
bullThere are several novel aspects to these findings First the study documents a clearly increased upper airway resistance in association with oral breathing during stable sleep as compared with nasal breathing irrespective of central or OSA
bullSecondly this methodology included simultaneous documentation of oral and nasal ventilation during sleep to confirm the absence of any nasal airflow in the oral breathing condition and vice versa
1112017
29
bullThe substantially higher resistive load posed by the oral breathing route provides a plausible explanation for the observation that inhaled ventilation occurs almost exclusively via the nasal route during sleep in subjects with normal nasal resistance
bull Many studies have shown that nasal obstruction can induce or increase apnea frequency in OSA patients When nasal resistance is high a greater pressure drop is required to achieve the same flow and hence collapse of the pharynx is facilitated and this could mitigate the effect of mandibular advancement
bull Moreover high nasal resistance is associated with mouth breathing which could potentially limit the beneficial effect of mandibular advancement
bull Dental Appliance Treatment for Obstructive
bull Andrew S L Chan Richard W W Lee and Peter A Cistulli
bull httpchestjournalchestpubsorgcontent1322693fullhtml
1112017
30
bullCurrent evidence suggests that despite the superior efficacy of CPAP both treatments produce similar subjective and objective health benefits
bullThe superior self-reported tolerance and compliance associated with MAD treatment is a likely explanation
bullThe practice parameters of the AASM recommend the use of oral appliances for mild-to-moderate OSA or for patients with severe OSA who are unable to tolerate CPAP or refuse treatment with CPAP with a required written prescription by a sleep physician
The following are Medicare rules
1) A diagnosis of OSA is not within the dental scope of practice A dentist providing an OA
must do so under the and with the team effort of a licensed Physician with a written
prescription
2) A physician is not skilled in the intricacies of fabricating fitting monitoring adjusting
and choosing an appropriate Oral Appliance individualized per patient
3) A dentist may not provide an oral appliance if the patient has an active
Temporomandibular Disorder
4) The OA must be fabricated within 90 days of the patientrsquos appointment with the sleep
physician
Since the rules are clear and they involve both of our professions it would behoove
both DOMD and DDS to communicate for the benefit of OSA patients
1112017
31
Subsequent to my 3 hour 2013 Meeting with the US Department of Transportation regarding Truckers
bull During the State Board of Dental Examiners meeting Board members put sleep Dentistry in squarely back into the spotlight The Board has addressed sleep Dentistry issues in a public hearing and all four Board meetings in 2013
bull There was discussion that there can be a shared relationship between the Dental and medical scopes of practice
bull Under the proposed rule a Dentist may treat benign snoring with an oral appliance after referral to a licensed physician where appropriate within the standard of care By contrast a Dentist may not diagnose treat or monitor OSA without collaboration with a licensed physician Additionally an oral appliance shall only be fabricated by a licensed Dentist or by a Dental lab under a prescription or work order prepared by a Dentist
American Dental Association
bull Treatment using an oral appliance designed specifically to treat OSA should be fabricated by a dentist familiar with device design maintenance and therapeutic efficacy and who has an association with and a referral from a sleep team
bull JADA Vol 136 p 1123
Donrsquot be afraid of OSA Get a grip on the facts and save patientrsquos lives
1112017
32
bullA SYMBIOTIC RELATION BETWEEN PHYSICIANS SLEEP PROFESSIONALS AND DENTISTS CAN SIGNIFICANTLY IMPROVE THE SLEEP HEALTH OF MILLIONS OF PEOPLE EACH AND EVERY YEAR
bull THAT RELATIONSHIP IS NOT A ONE WAY STREET AND THE
American Sleep amp Breathing Academy of over 8000 members UNDERSTANDS THAThellip JUST LOOK AT THE MULTITUDE OF SLEEP PROFESSIONAL CATAGORIES ON THEIR BOARD OF DIRECTORS
THE END
Thank you for your interest I hope this presentation was helpful
Dr Richard Klein
1112017
13
NORMAL SLEEP
bull CHARACTERIZED BY A DECREASE IN
bull BODY TEMPERATURE
bull BLOOD PRESSURE
bull BREATHING RATE
bull MOST OTHER BODY FUNCTIONS
bull INCREASED NASAL RESISTANCE
bull CHARACTERIZED BY AN bull ACTIVE BRAIN
1112017
14
Copyright 2011 BRAEBON
Normal healthy breathing during sleep
Wake-up-gasping-choking-and-die-in-your-sleep-diseaserdquo ndash No sound during event
Who gets sent for a sleep study
1112017
15
Who usually doesnrsquot
Sleep apnoea is a common occurrence in femalesKarl A Franklin et al European Respiratory Journal August 2012
bull We investigated 400 females from a population-based random sample of 10000 females aged 20ndash70 years with a questionnaire and anovernight polysomnography
bull Obstructive sleep apnoea was found in 50 of females aged 20ndash70 years
bull Sleep apnoea was related to age obesity and hypertension but not to daytime sleepiness
bull Severe sleep apnoea was scored in 14 of females aged 55ndash70 years and in 31 of obese females with a body-mass index of gt30 kgmiddotmminus2 aged 50ndash70 years
1112017
16
EPWORTH SLEEPINESS SCALEINTERPRETATIONbull 0-7 IT IS UNLIKELY THAT YOU ARE ABNORMALLY SLEEPY
bull 8-9 YOU HAVE AN AVERAGE AMOUNT OF DAYTIME SLEEPINESS
bull 10-15 YOU MAY BE EXCESSIVELY SLEEPY DEPENDING ON THE SITUATION YOU MAY WANT TO CONSIDER SEEKING MEDICAL ATTENTION
bull 16-24 YOU ARE EXCESSIVELY SLEEPY AND SHOULD CONSIDER SEEKING MEDICAL ATTENTION
This person most likely is simply tired or had a bad nightrsquos sleep OSA is not
indicated
I referred this patient to a sleep physician
1112017
17
MALLAMPATI
1112017
18
Lavigne GJ Kato T Kolta A Sessle BJ Neurobiological mechanisms involved in sleep bruxism Crit Rev Oral Biol Med 20031430-46
bullSleep-related bruxism (SB) is characterized by the grinding or clenching of the teeth during sleep usually associated with sleep arousals although the incidence of sleep arousals in SB subjects is within the normal range (up to 14 arousalshour of sleep is considered normal)
IT HAS BEEN SHOWN THAT CPAP ELIMINATION OF OSA alsoELIMINATES SNORING
IT HAS NOT BEEN DEMONSTRATED THAT CPAP TREATMENT OF OSA
ELIMINATES OR REDUCES S-B
Neurobiological mechanisms involved in sleep bruxismLavigne GJ1 Kato T Kolta A Sessle BJ
bull Sleep bruxism (SB) is mainly associated with rhythmic masticatory muscle activity (RMMA) characterized by repetitive jaw muscle contractions (3 bursts or more at a frequency of 1 Hz)
bull The consequences of SB may include tooth destruction jaw pain headaches or the limitation of mandibular movement as well as tooth-grinding sounds that disrupt the sleep of bed partners RMMA is observed in 60 of normal sleepers
1112017
19
bull The pathophysiology of SB is becoming clearer
bull There is an abundance of evidence outlining the neurophysiology and neurochemistry of rhythmic jaw movements (RJM) in relation to chewing swallowing and breathing Several brainstem structures (eg reticular pontis oralis pontis caudalis) and neurochemicals (eg serotonin dopamine gamma aminobutyric acid [GABA] noradrenaline) are involved in both the genesis of RJM and the modulation of muscle tone during sleep
bull It creates a co-activation of both jaw-opening and jaw-closing muscles instead of the alternating jaw-opening and jaw-closing muscle activity pattern typical of chewing
Journal of Pain amp Symptom Management
bullPain duration and intensitywere correlated with decreased sleep impaired sleep quality and delayed sleep onset
Multiple Medical Studies
bullHave published that the majority (59 67 74) of OSA patients will not appropriately wear the CPAP
1112017
20
bull IN 1995 Johnny Cochran said ldquoIf the glove doesnrsquot fithellipyou must acquitrdquo As DR Dement intimated in the 1970s ldquoWe didnt know what to measurehellipso we measured everything we could think ofhellip and it stuckrdquo
bull Almost forty years later some of what ldquostuckrdquo is being revised reinterpreted and common sense is beginning to prevail Seven to eight hours of sleep per night is recommended
The Other 72 of Sleep
bull Sticking with the antiquated definition of a ldquocompliant userrdquo of a
CPAP (4 hrsnight and 5 nightsweek) one must use it roughly 28 of the time
bull WHAT ABOUT THE OTHER 72 OF SLEEP
bull Is it acceptable to not get the O2 we need simply because an antiquated standard ldquostuckrdquo
bull In 1995 CPAP became the gold standard Now in the 21st century I
say ldquoif the mask doesnrsquot fit hellipdonrsquot quitrdquo because an oral appliance may save your health and your life
Treatment of Sleep Apnea
Tracheotomy Oral
Surgery CPAPBiPAP
OA
Behavioral Modification
1112017
21
Orofacial Findings
bullThe most common orofacial characteristics include a retrognathic mandible narrow palate large neck circumference long soft palate tonsillar hypertrophy nasal septal deviation and relative macroglossia
Oral Appliances for Sleep Apnea amp Snoring
Tongue Retaining Devices Mandibular Repositioning Appliances
Oral Appliances (OA)
bull Properly fabricated an oral appliance will protrude the tongue and reposition the mandible anteriorly and inferiorly to the most beneficial neuromuscular position to prevent posterior airway collapse
bull This position is titratable and individualized to exact patient requirements and may need periodic adjustments just as does CPAP
1112017
22
BEFORE
APPLIANCE
7c
WITH
APPLIANCE
9 cc
1112017
23
Copyright 2011 BRAEBON
More Directly Related to hellipDental Sleep Medicine
bull EACH PATIENT IS AN INDIVIDUAL AND JUST AS CPAP PRESSURE IS INDIVIDUALLY TITRATEDhellipSO TOO ARE ORAL APPLIANCES
bull IF I DELIVER AN OA TO A PATIENT WHO WILL NOT UTILIZE THE CPAPhellipI WILL PROVIDE ONE OR SEVERAL HOME SLEEP STUDIES TO ASCERTAIN THE EFFICACY OF THE OAhellip AND THEN I REQUIRE THAT THEY RETURN TO THEIR SLEEP
bull DOCTOR FOR A SUBSEQUENT STUDY WHILE helliphelliphelliphelliphelliphelliphellipUTILIZINGTHE OA
Positional Apnea in a 73-Year Old Male with Atrial Fibrillation
bull This case study illustrates the cost-effective approach to successful outcomes associated with positional therapy that are not surprising and are consistent with a recent study which concluded ldquopositional therapy is equivalent to CPAP at normalizing the AHI in patients with positional OSA with similar effects on sleep quality and nocturnal oxygenationrdquo
bull Journal Sleep Diagnosis and Therapy
1112017
24
HOW THE ORAL APPLIANCE TREATS OSA
bull Prevent collapse of airwaybull Forward advancement of jawbull Support forward tongue positionbull Change shape of pharyngeal airwaybull Increase vertical dimension of occlusionbull Correct dysphagia bull Increase volume of space for tonguebull Trains protrusive tongue reflexesbull Alter position of hyoid bone relative to
mandible
THE VARYING ROLES OF THE NOSE AND MOUTH IN BREATHING
1112017
25
THE NOSE
bull A recent pediatric study reveals why addressing the tongue is so important for resolving sleep apnea As explained in this study having an abnormally short lingual frenulum can result in impaired orofacial growth in early childhood reducing the width of the upper airway
bull The upper airway is very pliable so this increases the risk of it collapsing during sleep They found that children with an untreated short frenulum developed abnormal tongue function early in life which also impacted their orofacial growth and led to disordered breathing during sleep
WHAT IS THE ROLE OF THE NOSE
ITS FUNCTIONS ARE VITAL
bull WARMING
bull HUMIDIFICATION
bull FILTERING
bull CLEANING
OF AMBIENT AIR INHALED INTO THE LUNGS
INFUSION OF NITRIC OXIDE
1112017
26
Humidification and
Dehumidification
bull During intake air is humidified to increase lung oxygen facilitation
bull Upon exhalation air is dehumidified to keep water in our cells
bull If this were not the case we would dehydrate unless we continually drank water
NARES
CONSTRICT
NARES FLARE
SNIFF TEST
1112017
27
Cosmetic Surgery
bullHe couldnrsquot breath through his small nose became hypercapnic and helliphelliphellipdied
Effect of treating severe nasal obstruction on the severity of obstructive sleep apnoea
bull HA McLean AM Urton HS Driver AKW Tan AG Day+ PW Munt and MF Fitzpatrick
bullThis study demonstrates that relief of severe nasal obstruction in patients with a normal retroglossal airway is associated with a significant reduction in mouth breathing during sleep improved sleep architecture and a modest improvement in OSA severity
1112017
28
bullThere are several novel aspects to these findings First the study documents a clearly increased upper airway resistance in association with oral breathing during stable sleep as compared with nasal breathing irrespective of central or OSA
bullSecondly this methodology included simultaneous documentation of oral and nasal ventilation during sleep to confirm the absence of any nasal airflow in the oral breathing condition and vice versa
1112017
29
bullThe substantially higher resistive load posed by the oral breathing route provides a plausible explanation for the observation that inhaled ventilation occurs almost exclusively via the nasal route during sleep in subjects with normal nasal resistance
bull Many studies have shown that nasal obstruction can induce or increase apnea frequency in OSA patients When nasal resistance is high a greater pressure drop is required to achieve the same flow and hence collapse of the pharynx is facilitated and this could mitigate the effect of mandibular advancement
bull Moreover high nasal resistance is associated with mouth breathing which could potentially limit the beneficial effect of mandibular advancement
bull Dental Appliance Treatment for Obstructive
bull Andrew S L Chan Richard W W Lee and Peter A Cistulli
bull httpchestjournalchestpubsorgcontent1322693fullhtml
1112017
30
bullCurrent evidence suggests that despite the superior efficacy of CPAP both treatments produce similar subjective and objective health benefits
bullThe superior self-reported tolerance and compliance associated with MAD treatment is a likely explanation
bullThe practice parameters of the AASM recommend the use of oral appliances for mild-to-moderate OSA or for patients with severe OSA who are unable to tolerate CPAP or refuse treatment with CPAP with a required written prescription by a sleep physician
The following are Medicare rules
1) A diagnosis of OSA is not within the dental scope of practice A dentist providing an OA
must do so under the and with the team effort of a licensed Physician with a written
prescription
2) A physician is not skilled in the intricacies of fabricating fitting monitoring adjusting
and choosing an appropriate Oral Appliance individualized per patient
3) A dentist may not provide an oral appliance if the patient has an active
Temporomandibular Disorder
4) The OA must be fabricated within 90 days of the patientrsquos appointment with the sleep
physician
Since the rules are clear and they involve both of our professions it would behoove
both DOMD and DDS to communicate for the benefit of OSA patients
1112017
31
Subsequent to my 3 hour 2013 Meeting with the US Department of Transportation regarding Truckers
bull During the State Board of Dental Examiners meeting Board members put sleep Dentistry in squarely back into the spotlight The Board has addressed sleep Dentistry issues in a public hearing and all four Board meetings in 2013
bull There was discussion that there can be a shared relationship between the Dental and medical scopes of practice
bull Under the proposed rule a Dentist may treat benign snoring with an oral appliance after referral to a licensed physician where appropriate within the standard of care By contrast a Dentist may not diagnose treat or monitor OSA without collaboration with a licensed physician Additionally an oral appliance shall only be fabricated by a licensed Dentist or by a Dental lab under a prescription or work order prepared by a Dentist
American Dental Association
bull Treatment using an oral appliance designed specifically to treat OSA should be fabricated by a dentist familiar with device design maintenance and therapeutic efficacy and who has an association with and a referral from a sleep team
bull JADA Vol 136 p 1123
Donrsquot be afraid of OSA Get a grip on the facts and save patientrsquos lives
1112017
32
bullA SYMBIOTIC RELATION BETWEEN PHYSICIANS SLEEP PROFESSIONALS AND DENTISTS CAN SIGNIFICANTLY IMPROVE THE SLEEP HEALTH OF MILLIONS OF PEOPLE EACH AND EVERY YEAR
bull THAT RELATIONSHIP IS NOT A ONE WAY STREET AND THE
American Sleep amp Breathing Academy of over 8000 members UNDERSTANDS THAThellip JUST LOOK AT THE MULTITUDE OF SLEEP PROFESSIONAL CATAGORIES ON THEIR BOARD OF DIRECTORS
THE END
Thank you for your interest I hope this presentation was helpful
Dr Richard Klein
1112017
14
Copyright 2011 BRAEBON
Normal healthy breathing during sleep
Wake-up-gasping-choking-and-die-in-your-sleep-diseaserdquo ndash No sound during event
Who gets sent for a sleep study
1112017
15
Who usually doesnrsquot
Sleep apnoea is a common occurrence in femalesKarl A Franklin et al European Respiratory Journal August 2012
bull We investigated 400 females from a population-based random sample of 10000 females aged 20ndash70 years with a questionnaire and anovernight polysomnography
bull Obstructive sleep apnoea was found in 50 of females aged 20ndash70 years
bull Sleep apnoea was related to age obesity and hypertension but not to daytime sleepiness
bull Severe sleep apnoea was scored in 14 of females aged 55ndash70 years and in 31 of obese females with a body-mass index of gt30 kgmiddotmminus2 aged 50ndash70 years
1112017
16
EPWORTH SLEEPINESS SCALEINTERPRETATIONbull 0-7 IT IS UNLIKELY THAT YOU ARE ABNORMALLY SLEEPY
bull 8-9 YOU HAVE AN AVERAGE AMOUNT OF DAYTIME SLEEPINESS
bull 10-15 YOU MAY BE EXCESSIVELY SLEEPY DEPENDING ON THE SITUATION YOU MAY WANT TO CONSIDER SEEKING MEDICAL ATTENTION
bull 16-24 YOU ARE EXCESSIVELY SLEEPY AND SHOULD CONSIDER SEEKING MEDICAL ATTENTION
This person most likely is simply tired or had a bad nightrsquos sleep OSA is not
indicated
I referred this patient to a sleep physician
1112017
17
MALLAMPATI
1112017
18
Lavigne GJ Kato T Kolta A Sessle BJ Neurobiological mechanisms involved in sleep bruxism Crit Rev Oral Biol Med 20031430-46
bullSleep-related bruxism (SB) is characterized by the grinding or clenching of the teeth during sleep usually associated with sleep arousals although the incidence of sleep arousals in SB subjects is within the normal range (up to 14 arousalshour of sleep is considered normal)
IT HAS BEEN SHOWN THAT CPAP ELIMINATION OF OSA alsoELIMINATES SNORING
IT HAS NOT BEEN DEMONSTRATED THAT CPAP TREATMENT OF OSA
ELIMINATES OR REDUCES S-B
Neurobiological mechanisms involved in sleep bruxismLavigne GJ1 Kato T Kolta A Sessle BJ
bull Sleep bruxism (SB) is mainly associated with rhythmic masticatory muscle activity (RMMA) characterized by repetitive jaw muscle contractions (3 bursts or more at a frequency of 1 Hz)
bull The consequences of SB may include tooth destruction jaw pain headaches or the limitation of mandibular movement as well as tooth-grinding sounds that disrupt the sleep of bed partners RMMA is observed in 60 of normal sleepers
1112017
19
bull The pathophysiology of SB is becoming clearer
bull There is an abundance of evidence outlining the neurophysiology and neurochemistry of rhythmic jaw movements (RJM) in relation to chewing swallowing and breathing Several brainstem structures (eg reticular pontis oralis pontis caudalis) and neurochemicals (eg serotonin dopamine gamma aminobutyric acid [GABA] noradrenaline) are involved in both the genesis of RJM and the modulation of muscle tone during sleep
bull It creates a co-activation of both jaw-opening and jaw-closing muscles instead of the alternating jaw-opening and jaw-closing muscle activity pattern typical of chewing
Journal of Pain amp Symptom Management
bullPain duration and intensitywere correlated with decreased sleep impaired sleep quality and delayed sleep onset
Multiple Medical Studies
bullHave published that the majority (59 67 74) of OSA patients will not appropriately wear the CPAP
1112017
20
bull IN 1995 Johnny Cochran said ldquoIf the glove doesnrsquot fithellipyou must acquitrdquo As DR Dement intimated in the 1970s ldquoWe didnt know what to measurehellipso we measured everything we could think ofhellip and it stuckrdquo
bull Almost forty years later some of what ldquostuckrdquo is being revised reinterpreted and common sense is beginning to prevail Seven to eight hours of sleep per night is recommended
The Other 72 of Sleep
bull Sticking with the antiquated definition of a ldquocompliant userrdquo of a
CPAP (4 hrsnight and 5 nightsweek) one must use it roughly 28 of the time
bull WHAT ABOUT THE OTHER 72 OF SLEEP
bull Is it acceptable to not get the O2 we need simply because an antiquated standard ldquostuckrdquo
bull In 1995 CPAP became the gold standard Now in the 21st century I
say ldquoif the mask doesnrsquot fit hellipdonrsquot quitrdquo because an oral appliance may save your health and your life
Treatment of Sleep Apnea
Tracheotomy Oral
Surgery CPAPBiPAP
OA
Behavioral Modification
1112017
21
Orofacial Findings
bullThe most common orofacial characteristics include a retrognathic mandible narrow palate large neck circumference long soft palate tonsillar hypertrophy nasal septal deviation and relative macroglossia
Oral Appliances for Sleep Apnea amp Snoring
Tongue Retaining Devices Mandibular Repositioning Appliances
Oral Appliances (OA)
bull Properly fabricated an oral appliance will protrude the tongue and reposition the mandible anteriorly and inferiorly to the most beneficial neuromuscular position to prevent posterior airway collapse
bull This position is titratable and individualized to exact patient requirements and may need periodic adjustments just as does CPAP
1112017
22
BEFORE
APPLIANCE
7c
WITH
APPLIANCE
9 cc
1112017
23
Copyright 2011 BRAEBON
More Directly Related to hellipDental Sleep Medicine
bull EACH PATIENT IS AN INDIVIDUAL AND JUST AS CPAP PRESSURE IS INDIVIDUALLY TITRATEDhellipSO TOO ARE ORAL APPLIANCES
bull IF I DELIVER AN OA TO A PATIENT WHO WILL NOT UTILIZE THE CPAPhellipI WILL PROVIDE ONE OR SEVERAL HOME SLEEP STUDIES TO ASCERTAIN THE EFFICACY OF THE OAhellip AND THEN I REQUIRE THAT THEY RETURN TO THEIR SLEEP
bull DOCTOR FOR A SUBSEQUENT STUDY WHILE helliphelliphelliphelliphelliphelliphellipUTILIZINGTHE OA
Positional Apnea in a 73-Year Old Male with Atrial Fibrillation
bull This case study illustrates the cost-effective approach to successful outcomes associated with positional therapy that are not surprising and are consistent with a recent study which concluded ldquopositional therapy is equivalent to CPAP at normalizing the AHI in patients with positional OSA with similar effects on sleep quality and nocturnal oxygenationrdquo
bull Journal Sleep Diagnosis and Therapy
1112017
24
HOW THE ORAL APPLIANCE TREATS OSA
bull Prevent collapse of airwaybull Forward advancement of jawbull Support forward tongue positionbull Change shape of pharyngeal airwaybull Increase vertical dimension of occlusionbull Correct dysphagia bull Increase volume of space for tonguebull Trains protrusive tongue reflexesbull Alter position of hyoid bone relative to
mandible
THE VARYING ROLES OF THE NOSE AND MOUTH IN BREATHING
1112017
25
THE NOSE
bull A recent pediatric study reveals why addressing the tongue is so important for resolving sleep apnea As explained in this study having an abnormally short lingual frenulum can result in impaired orofacial growth in early childhood reducing the width of the upper airway
bull The upper airway is very pliable so this increases the risk of it collapsing during sleep They found that children with an untreated short frenulum developed abnormal tongue function early in life which also impacted their orofacial growth and led to disordered breathing during sleep
WHAT IS THE ROLE OF THE NOSE
ITS FUNCTIONS ARE VITAL
bull WARMING
bull HUMIDIFICATION
bull FILTERING
bull CLEANING
OF AMBIENT AIR INHALED INTO THE LUNGS
INFUSION OF NITRIC OXIDE
1112017
26
Humidification and
Dehumidification
bull During intake air is humidified to increase lung oxygen facilitation
bull Upon exhalation air is dehumidified to keep water in our cells
bull If this were not the case we would dehydrate unless we continually drank water
NARES
CONSTRICT
NARES FLARE
SNIFF TEST
1112017
27
Cosmetic Surgery
bullHe couldnrsquot breath through his small nose became hypercapnic and helliphelliphellipdied
Effect of treating severe nasal obstruction on the severity of obstructive sleep apnoea
bull HA McLean AM Urton HS Driver AKW Tan AG Day+ PW Munt and MF Fitzpatrick
bullThis study demonstrates that relief of severe nasal obstruction in patients with a normal retroglossal airway is associated with a significant reduction in mouth breathing during sleep improved sleep architecture and a modest improvement in OSA severity
1112017
28
bullThere are several novel aspects to these findings First the study documents a clearly increased upper airway resistance in association with oral breathing during stable sleep as compared with nasal breathing irrespective of central or OSA
bullSecondly this methodology included simultaneous documentation of oral and nasal ventilation during sleep to confirm the absence of any nasal airflow in the oral breathing condition and vice versa
1112017
29
bullThe substantially higher resistive load posed by the oral breathing route provides a plausible explanation for the observation that inhaled ventilation occurs almost exclusively via the nasal route during sleep in subjects with normal nasal resistance
bull Many studies have shown that nasal obstruction can induce or increase apnea frequency in OSA patients When nasal resistance is high a greater pressure drop is required to achieve the same flow and hence collapse of the pharynx is facilitated and this could mitigate the effect of mandibular advancement
bull Moreover high nasal resistance is associated with mouth breathing which could potentially limit the beneficial effect of mandibular advancement
bull Dental Appliance Treatment for Obstructive
bull Andrew S L Chan Richard W W Lee and Peter A Cistulli
bull httpchestjournalchestpubsorgcontent1322693fullhtml
1112017
30
bullCurrent evidence suggests that despite the superior efficacy of CPAP both treatments produce similar subjective and objective health benefits
bullThe superior self-reported tolerance and compliance associated with MAD treatment is a likely explanation
bullThe practice parameters of the AASM recommend the use of oral appliances for mild-to-moderate OSA or for patients with severe OSA who are unable to tolerate CPAP or refuse treatment with CPAP with a required written prescription by a sleep physician
The following are Medicare rules
1) A diagnosis of OSA is not within the dental scope of practice A dentist providing an OA
must do so under the and with the team effort of a licensed Physician with a written
prescription
2) A physician is not skilled in the intricacies of fabricating fitting monitoring adjusting
and choosing an appropriate Oral Appliance individualized per patient
3) A dentist may not provide an oral appliance if the patient has an active
Temporomandibular Disorder
4) The OA must be fabricated within 90 days of the patientrsquos appointment with the sleep
physician
Since the rules are clear and they involve both of our professions it would behoove
both DOMD and DDS to communicate for the benefit of OSA patients
1112017
31
Subsequent to my 3 hour 2013 Meeting with the US Department of Transportation regarding Truckers
bull During the State Board of Dental Examiners meeting Board members put sleep Dentistry in squarely back into the spotlight The Board has addressed sleep Dentistry issues in a public hearing and all four Board meetings in 2013
bull There was discussion that there can be a shared relationship between the Dental and medical scopes of practice
bull Under the proposed rule a Dentist may treat benign snoring with an oral appliance after referral to a licensed physician where appropriate within the standard of care By contrast a Dentist may not diagnose treat or monitor OSA without collaboration with a licensed physician Additionally an oral appliance shall only be fabricated by a licensed Dentist or by a Dental lab under a prescription or work order prepared by a Dentist
American Dental Association
bull Treatment using an oral appliance designed specifically to treat OSA should be fabricated by a dentist familiar with device design maintenance and therapeutic efficacy and who has an association with and a referral from a sleep team
bull JADA Vol 136 p 1123
Donrsquot be afraid of OSA Get a grip on the facts and save patientrsquos lives
1112017
32
bullA SYMBIOTIC RELATION BETWEEN PHYSICIANS SLEEP PROFESSIONALS AND DENTISTS CAN SIGNIFICANTLY IMPROVE THE SLEEP HEALTH OF MILLIONS OF PEOPLE EACH AND EVERY YEAR
bull THAT RELATIONSHIP IS NOT A ONE WAY STREET AND THE
American Sleep amp Breathing Academy of over 8000 members UNDERSTANDS THAThellip JUST LOOK AT THE MULTITUDE OF SLEEP PROFESSIONAL CATAGORIES ON THEIR BOARD OF DIRECTORS
THE END
Thank you for your interest I hope this presentation was helpful
Dr Richard Klein
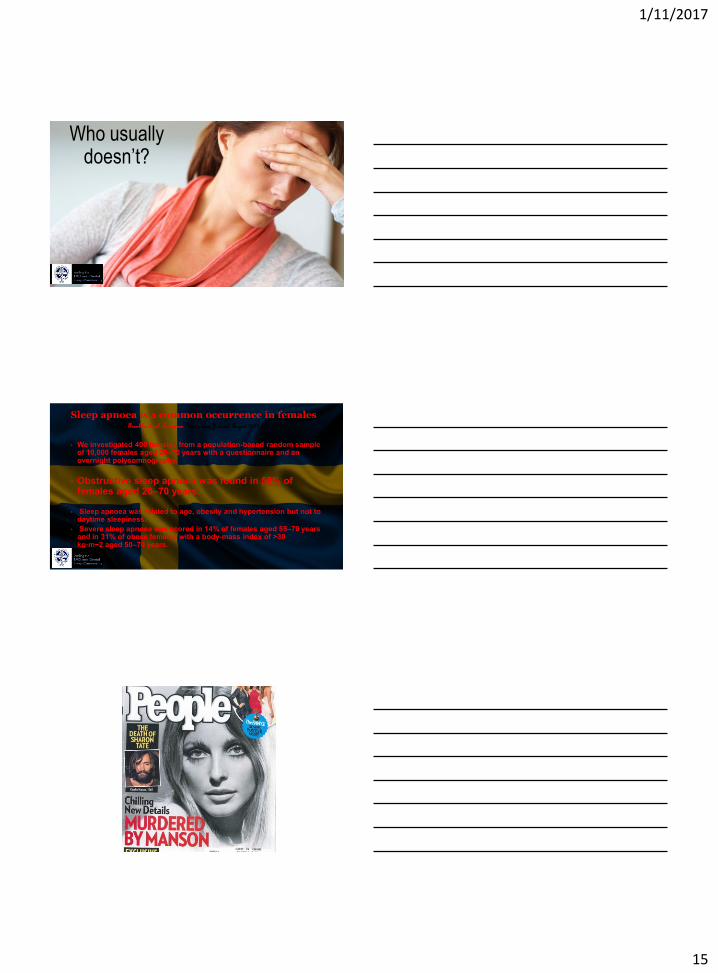
1112017
15
Who usually doesnrsquot
Sleep apnoea is a common occurrence in femalesKarl A Franklin et al European Respiratory Journal August 2012
bull We investigated 400 females from a population-based random sample of 10000 females aged 20ndash70 years with a questionnaire and anovernight polysomnography
bull Obstructive sleep apnoea was found in 50 of females aged 20ndash70 years
bull Sleep apnoea was related to age obesity and hypertension but not to daytime sleepiness
bull Severe sleep apnoea was scored in 14 of females aged 55ndash70 years and in 31 of obese females with a body-mass index of gt30 kgmiddotmminus2 aged 50ndash70 years
1112017
16
EPWORTH SLEEPINESS SCALEINTERPRETATIONbull 0-7 IT IS UNLIKELY THAT YOU ARE ABNORMALLY SLEEPY
bull 8-9 YOU HAVE AN AVERAGE AMOUNT OF DAYTIME SLEEPINESS
bull 10-15 YOU MAY BE EXCESSIVELY SLEEPY DEPENDING ON THE SITUATION YOU MAY WANT TO CONSIDER SEEKING MEDICAL ATTENTION
bull 16-24 YOU ARE EXCESSIVELY SLEEPY AND SHOULD CONSIDER SEEKING MEDICAL ATTENTION
This person most likely is simply tired or had a bad nightrsquos sleep OSA is not
indicated
I referred this patient to a sleep physician
1112017
17
MALLAMPATI
1112017
18
Lavigne GJ Kato T Kolta A Sessle BJ Neurobiological mechanisms involved in sleep bruxism Crit Rev Oral Biol Med 20031430-46
bullSleep-related bruxism (SB) is characterized by the grinding or clenching of the teeth during sleep usually associated with sleep arousals although the incidence of sleep arousals in SB subjects is within the normal range (up to 14 arousalshour of sleep is considered normal)
IT HAS BEEN SHOWN THAT CPAP ELIMINATION OF OSA alsoELIMINATES SNORING
IT HAS NOT BEEN DEMONSTRATED THAT CPAP TREATMENT OF OSA
ELIMINATES OR REDUCES S-B
Neurobiological mechanisms involved in sleep bruxismLavigne GJ1 Kato T Kolta A Sessle BJ
bull Sleep bruxism (SB) is mainly associated with rhythmic masticatory muscle activity (RMMA) characterized by repetitive jaw muscle contractions (3 bursts or more at a frequency of 1 Hz)
bull The consequences of SB may include tooth destruction jaw pain headaches or the limitation of mandibular movement as well as tooth-grinding sounds that disrupt the sleep of bed partners RMMA is observed in 60 of normal sleepers
1112017
19
bull The pathophysiology of SB is becoming clearer
bull There is an abundance of evidence outlining the neurophysiology and neurochemistry of rhythmic jaw movements (RJM) in relation to chewing swallowing and breathing Several brainstem structures (eg reticular pontis oralis pontis caudalis) and neurochemicals (eg serotonin dopamine gamma aminobutyric acid [GABA] noradrenaline) are involved in both the genesis of RJM and the modulation of muscle tone during sleep
bull It creates a co-activation of both jaw-opening and jaw-closing muscles instead of the alternating jaw-opening and jaw-closing muscle activity pattern typical of chewing
Journal of Pain amp Symptom Management
bullPain duration and intensitywere correlated with decreased sleep impaired sleep quality and delayed sleep onset
Multiple Medical Studies
bullHave published that the majority (59 67 74) of OSA patients will not appropriately wear the CPAP
1112017
20
bull IN 1995 Johnny Cochran said ldquoIf the glove doesnrsquot fithellipyou must acquitrdquo As DR Dement intimated in the 1970s ldquoWe didnt know what to measurehellipso we measured everything we could think ofhellip and it stuckrdquo
bull Almost forty years later some of what ldquostuckrdquo is being revised reinterpreted and common sense is beginning to prevail Seven to eight hours of sleep per night is recommended
The Other 72 of Sleep
bull Sticking with the antiquated definition of a ldquocompliant userrdquo of a
CPAP (4 hrsnight and 5 nightsweek) one must use it roughly 28 of the time
bull WHAT ABOUT THE OTHER 72 OF SLEEP
bull Is it acceptable to not get the O2 we need simply because an antiquated standard ldquostuckrdquo
bull In 1995 CPAP became the gold standard Now in the 21st century I
say ldquoif the mask doesnrsquot fit hellipdonrsquot quitrdquo because an oral appliance may save your health and your life
Treatment of Sleep Apnea
Tracheotomy Oral
Surgery CPAPBiPAP
OA
Behavioral Modification
1112017
21
Orofacial Findings
bullThe most common orofacial characteristics include a retrognathic mandible narrow palate large neck circumference long soft palate tonsillar hypertrophy nasal septal deviation and relative macroglossia
Oral Appliances for Sleep Apnea amp Snoring
Tongue Retaining Devices Mandibular Repositioning Appliances
Oral Appliances (OA)
bull Properly fabricated an oral appliance will protrude the tongue and reposition the mandible anteriorly and inferiorly to the most beneficial neuromuscular position to prevent posterior airway collapse
bull This position is titratable and individualized to exact patient requirements and may need periodic adjustments just as does CPAP
1112017
22
BEFORE
APPLIANCE
7c
WITH
APPLIANCE
9 cc
1112017
23
Copyright 2011 BRAEBON
More Directly Related to hellipDental Sleep Medicine
bull EACH PATIENT IS AN INDIVIDUAL AND JUST AS CPAP PRESSURE IS INDIVIDUALLY TITRATEDhellipSO TOO ARE ORAL APPLIANCES
bull IF I DELIVER AN OA TO A PATIENT WHO WILL NOT UTILIZE THE CPAPhellipI WILL PROVIDE ONE OR SEVERAL HOME SLEEP STUDIES TO ASCERTAIN THE EFFICACY OF THE OAhellip AND THEN I REQUIRE THAT THEY RETURN TO THEIR SLEEP
bull DOCTOR FOR A SUBSEQUENT STUDY WHILE helliphelliphelliphelliphelliphelliphellipUTILIZINGTHE OA
Positional Apnea in a 73-Year Old Male with Atrial Fibrillation
bull This case study illustrates the cost-effective approach to successful outcomes associated with positional therapy that are not surprising and are consistent with a recent study which concluded ldquopositional therapy is equivalent to CPAP at normalizing the AHI in patients with positional OSA with similar effects on sleep quality and nocturnal oxygenationrdquo
bull Journal Sleep Diagnosis and Therapy
1112017
24
HOW THE ORAL APPLIANCE TREATS OSA
bull Prevent collapse of airwaybull Forward advancement of jawbull Support forward tongue positionbull Change shape of pharyngeal airwaybull Increase vertical dimension of occlusionbull Correct dysphagia bull Increase volume of space for tonguebull Trains protrusive tongue reflexesbull Alter position of hyoid bone relative to
mandible
THE VARYING ROLES OF THE NOSE AND MOUTH IN BREATHING
1112017
25
THE NOSE
bull A recent pediatric study reveals why addressing the tongue is so important for resolving sleep apnea As explained in this study having an abnormally short lingual frenulum can result in impaired orofacial growth in early childhood reducing the width of the upper airway
bull The upper airway is very pliable so this increases the risk of it collapsing during sleep They found that children with an untreated short frenulum developed abnormal tongue function early in life which also impacted their orofacial growth and led to disordered breathing during sleep
WHAT IS THE ROLE OF THE NOSE
ITS FUNCTIONS ARE VITAL
bull WARMING
bull HUMIDIFICATION
bull FILTERING
bull CLEANING
OF AMBIENT AIR INHALED INTO THE LUNGS
INFUSION OF NITRIC OXIDE
1112017
26
Humidification and
Dehumidification
bull During intake air is humidified to increase lung oxygen facilitation
bull Upon exhalation air is dehumidified to keep water in our cells
bull If this were not the case we would dehydrate unless we continually drank water
NARES
CONSTRICT
NARES FLARE
SNIFF TEST
1112017
27
Cosmetic Surgery
bullHe couldnrsquot breath through his small nose became hypercapnic and helliphelliphellipdied
Effect of treating severe nasal obstruction on the severity of obstructive sleep apnoea
bull HA McLean AM Urton HS Driver AKW Tan AG Day+ PW Munt and MF Fitzpatrick
bullThis study demonstrates that relief of severe nasal obstruction in patients with a normal retroglossal airway is associated with a significant reduction in mouth breathing during sleep improved sleep architecture and a modest improvement in OSA severity
1112017
28
bullThere are several novel aspects to these findings First the study documents a clearly increased upper airway resistance in association with oral breathing during stable sleep as compared with nasal breathing irrespective of central or OSA
bullSecondly this methodology included simultaneous documentation of oral and nasal ventilation during sleep to confirm the absence of any nasal airflow in the oral breathing condition and vice versa
1112017
29
bullThe substantially higher resistive load posed by the oral breathing route provides a plausible explanation for the observation that inhaled ventilation occurs almost exclusively via the nasal route during sleep in subjects with normal nasal resistance
bull Many studies have shown that nasal obstruction can induce or increase apnea frequency in OSA patients When nasal resistance is high a greater pressure drop is required to achieve the same flow and hence collapse of the pharynx is facilitated and this could mitigate the effect of mandibular advancement
bull Moreover high nasal resistance is associated with mouth breathing which could potentially limit the beneficial effect of mandibular advancement
bull Dental Appliance Treatment for Obstructive
bull Andrew S L Chan Richard W W Lee and Peter A Cistulli
bull httpchestjournalchestpubsorgcontent1322693fullhtml
1112017
30
bullCurrent evidence suggests that despite the superior efficacy of CPAP both treatments produce similar subjective and objective health benefits
bullThe superior self-reported tolerance and compliance associated with MAD treatment is a likely explanation
bullThe practice parameters of the AASM recommend the use of oral appliances for mild-to-moderate OSA or for patients with severe OSA who are unable to tolerate CPAP or refuse treatment with CPAP with a required written prescription by a sleep physician
The following are Medicare rules
1) A diagnosis of OSA is not within the dental scope of practice A dentist providing an OA
must do so under the and with the team effort of a licensed Physician with a written
prescription
2) A physician is not skilled in the intricacies of fabricating fitting monitoring adjusting
and choosing an appropriate Oral Appliance individualized per patient
3) A dentist may not provide an oral appliance if the patient has an active
Temporomandibular Disorder
4) The OA must be fabricated within 90 days of the patientrsquos appointment with the sleep
physician
Since the rules are clear and they involve both of our professions it would behoove
both DOMD and DDS to communicate for the benefit of OSA patients
1112017
31
Subsequent to my 3 hour 2013 Meeting with the US Department of Transportation regarding Truckers
bull During the State Board of Dental Examiners meeting Board members put sleep Dentistry in squarely back into the spotlight The Board has addressed sleep Dentistry issues in a public hearing and all four Board meetings in 2013
bull There was discussion that there can be a shared relationship between the Dental and medical scopes of practice
bull Under the proposed rule a Dentist may treat benign snoring with an oral appliance after referral to a licensed physician where appropriate within the standard of care By contrast a Dentist may not diagnose treat or monitor OSA without collaboration with a licensed physician Additionally an oral appliance shall only be fabricated by a licensed Dentist or by a Dental lab under a prescription or work order prepared by a Dentist
American Dental Association
bull Treatment using an oral appliance designed specifically to treat OSA should be fabricated by a dentist familiar with device design maintenance and therapeutic efficacy and who has an association with and a referral from a sleep team
bull JADA Vol 136 p 1123
Donrsquot be afraid of OSA Get a grip on the facts and save patientrsquos lives
1112017
32
bullA SYMBIOTIC RELATION BETWEEN PHYSICIANS SLEEP PROFESSIONALS AND DENTISTS CAN SIGNIFICANTLY IMPROVE THE SLEEP HEALTH OF MILLIONS OF PEOPLE EACH AND EVERY YEAR
bull THAT RELATIONSHIP IS NOT A ONE WAY STREET AND THE
American Sleep amp Breathing Academy of over 8000 members UNDERSTANDS THAThellip JUST LOOK AT THE MULTITUDE OF SLEEP PROFESSIONAL CATAGORIES ON THEIR BOARD OF DIRECTORS
THE END
Thank you for your interest I hope this presentation was helpful
Dr Richard Klein
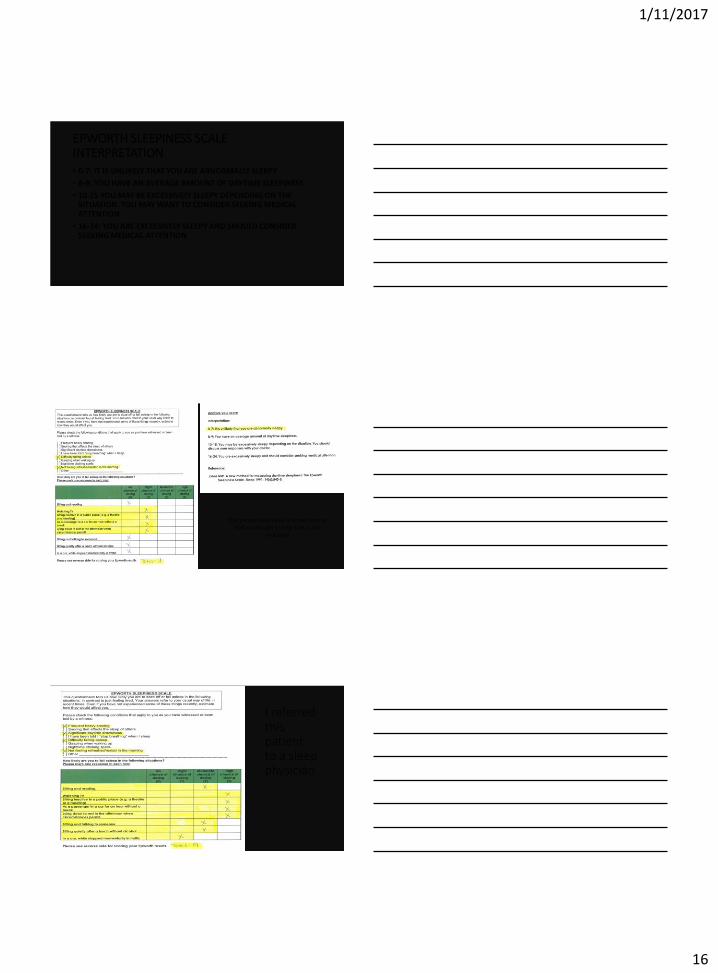
1112017
16
EPWORTH SLEEPINESS SCALEINTERPRETATIONbull 0-7 IT IS UNLIKELY THAT YOU ARE ABNORMALLY SLEEPY
bull 8-9 YOU HAVE AN AVERAGE AMOUNT OF DAYTIME SLEEPINESS
bull 10-15 YOU MAY BE EXCESSIVELY SLEEPY DEPENDING ON THE SITUATION YOU MAY WANT TO CONSIDER SEEKING MEDICAL ATTENTION
bull 16-24 YOU ARE EXCESSIVELY SLEEPY AND SHOULD CONSIDER SEEKING MEDICAL ATTENTION
This person most likely is simply tired or had a bad nightrsquos sleep OSA is not
indicated
I referred this patient to a sleep physician
1112017
17
MALLAMPATI
1112017
18
Lavigne GJ Kato T Kolta A Sessle BJ Neurobiological mechanisms involved in sleep bruxism Crit Rev Oral Biol Med 20031430-46
bullSleep-related bruxism (SB) is characterized by the grinding or clenching of the teeth during sleep usually associated with sleep arousals although the incidence of sleep arousals in SB subjects is within the normal range (up to 14 arousalshour of sleep is considered normal)
IT HAS BEEN SHOWN THAT CPAP ELIMINATION OF OSA alsoELIMINATES SNORING
IT HAS NOT BEEN DEMONSTRATED THAT CPAP TREATMENT OF OSA
ELIMINATES OR REDUCES S-B
Neurobiological mechanisms involved in sleep bruxismLavigne GJ1 Kato T Kolta A Sessle BJ
bull Sleep bruxism (SB) is mainly associated with rhythmic masticatory muscle activity (RMMA) characterized by repetitive jaw muscle contractions (3 bursts or more at a frequency of 1 Hz)
bull The consequences of SB may include tooth destruction jaw pain headaches or the limitation of mandibular movement as well as tooth-grinding sounds that disrupt the sleep of bed partners RMMA is observed in 60 of normal sleepers
1112017
19
bull The pathophysiology of SB is becoming clearer
bull There is an abundance of evidence outlining the neurophysiology and neurochemistry of rhythmic jaw movements (RJM) in relation to chewing swallowing and breathing Several brainstem structures (eg reticular pontis oralis pontis caudalis) and neurochemicals (eg serotonin dopamine gamma aminobutyric acid [GABA] noradrenaline) are involved in both the genesis of RJM and the modulation of muscle tone during sleep
bull It creates a co-activation of both jaw-opening and jaw-closing muscles instead of the alternating jaw-opening and jaw-closing muscle activity pattern typical of chewing
Journal of Pain amp Symptom Management
bullPain duration and intensitywere correlated with decreased sleep impaired sleep quality and delayed sleep onset
Multiple Medical Studies
bullHave published that the majority (59 67 74) of OSA patients will not appropriately wear the CPAP
1112017
20
bull IN 1995 Johnny Cochran said ldquoIf the glove doesnrsquot fithellipyou must acquitrdquo As DR Dement intimated in the 1970s ldquoWe didnt know what to measurehellipso we measured everything we could think ofhellip and it stuckrdquo
bull Almost forty years later some of what ldquostuckrdquo is being revised reinterpreted and common sense is beginning to prevail Seven to eight hours of sleep per night is recommended
The Other 72 of Sleep
bull Sticking with the antiquated definition of a ldquocompliant userrdquo of a
CPAP (4 hrsnight and 5 nightsweek) one must use it roughly 28 of the time
bull WHAT ABOUT THE OTHER 72 OF SLEEP
bull Is it acceptable to not get the O2 we need simply because an antiquated standard ldquostuckrdquo
bull In 1995 CPAP became the gold standard Now in the 21st century I
say ldquoif the mask doesnrsquot fit hellipdonrsquot quitrdquo because an oral appliance may save your health and your life
Treatment of Sleep Apnea
Tracheotomy Oral
Surgery CPAPBiPAP
OA
Behavioral Modification
1112017
21
Orofacial Findings
bullThe most common orofacial characteristics include a retrognathic mandible narrow palate large neck circumference long soft palate tonsillar hypertrophy nasal septal deviation and relative macroglossia
Oral Appliances for Sleep Apnea amp Snoring
Tongue Retaining Devices Mandibular Repositioning Appliances
Oral Appliances (OA)
bull Properly fabricated an oral appliance will protrude the tongue and reposition the mandible anteriorly and inferiorly to the most beneficial neuromuscular position to prevent posterior airway collapse
bull This position is titratable and individualized to exact patient requirements and may need periodic adjustments just as does CPAP
1112017
22
BEFORE
APPLIANCE
7c
WITH
APPLIANCE
9 cc
1112017
23
Copyright 2011 BRAEBON
More Directly Related to hellipDental Sleep Medicine
bull EACH PATIENT IS AN INDIVIDUAL AND JUST AS CPAP PRESSURE IS INDIVIDUALLY TITRATEDhellipSO TOO ARE ORAL APPLIANCES
bull IF I DELIVER AN OA TO A PATIENT WHO WILL NOT UTILIZE THE CPAPhellipI WILL PROVIDE ONE OR SEVERAL HOME SLEEP STUDIES TO ASCERTAIN THE EFFICACY OF THE OAhellip AND THEN I REQUIRE THAT THEY RETURN TO THEIR SLEEP
bull DOCTOR FOR A SUBSEQUENT STUDY WHILE helliphelliphelliphelliphelliphelliphellipUTILIZINGTHE OA
Positional Apnea in a 73-Year Old Male with Atrial Fibrillation
bull This case study illustrates the cost-effective approach to successful outcomes associated with positional therapy that are not surprising and are consistent with a recent study which concluded ldquopositional therapy is equivalent to CPAP at normalizing the AHI in patients with positional OSA with similar effects on sleep quality and nocturnal oxygenationrdquo
bull Journal Sleep Diagnosis and Therapy
1112017
24
HOW THE ORAL APPLIANCE TREATS OSA
bull Prevent collapse of airwaybull Forward advancement of jawbull Support forward tongue positionbull Change shape of pharyngeal airwaybull Increase vertical dimension of occlusionbull Correct dysphagia bull Increase volume of space for tonguebull Trains protrusive tongue reflexesbull Alter position of hyoid bone relative to
mandible
THE VARYING ROLES OF THE NOSE AND MOUTH IN BREATHING
1112017
25
THE NOSE
bull A recent pediatric study reveals why addressing the tongue is so important for resolving sleep apnea As explained in this study having an abnormally short lingual frenulum can result in impaired orofacial growth in early childhood reducing the width of the upper airway
bull The upper airway is very pliable so this increases the risk of it collapsing during sleep They found that children with an untreated short frenulum developed abnormal tongue function early in life which also impacted their orofacial growth and led to disordered breathing during sleep
WHAT IS THE ROLE OF THE NOSE
ITS FUNCTIONS ARE VITAL
bull WARMING
bull HUMIDIFICATION
bull FILTERING
bull CLEANING
OF AMBIENT AIR INHALED INTO THE LUNGS
INFUSION OF NITRIC OXIDE
1112017
26
Humidification and
Dehumidification
bull During intake air is humidified to increase lung oxygen facilitation
bull Upon exhalation air is dehumidified to keep water in our cells
bull If this were not the case we would dehydrate unless we continually drank water
NARES
CONSTRICT
NARES FLARE
SNIFF TEST
1112017
27
Cosmetic Surgery
bullHe couldnrsquot breath through his small nose became hypercapnic and helliphelliphellipdied
Effect of treating severe nasal obstruction on the severity of obstructive sleep apnoea
bull HA McLean AM Urton HS Driver AKW Tan AG Day+ PW Munt and MF Fitzpatrick
bullThis study demonstrates that relief of severe nasal obstruction in patients with a normal retroglossal airway is associated with a significant reduction in mouth breathing during sleep improved sleep architecture and a modest improvement in OSA severity
1112017
28
bullThere are several novel aspects to these findings First the study documents a clearly increased upper airway resistance in association with oral breathing during stable sleep as compared with nasal breathing irrespective of central or OSA
bullSecondly this methodology included simultaneous documentation of oral and nasal ventilation during sleep to confirm the absence of any nasal airflow in the oral breathing condition and vice versa
1112017
29
bullThe substantially higher resistive load posed by the oral breathing route provides a plausible explanation for the observation that inhaled ventilation occurs almost exclusively via the nasal route during sleep in subjects with normal nasal resistance
bull Many studies have shown that nasal obstruction can induce or increase apnea frequency in OSA patients When nasal resistance is high a greater pressure drop is required to achieve the same flow and hence collapse of the pharynx is facilitated and this could mitigate the effect of mandibular advancement
bull Moreover high nasal resistance is associated with mouth breathing which could potentially limit the beneficial effect of mandibular advancement
bull Dental Appliance Treatment for Obstructive
bull Andrew S L Chan Richard W W Lee and Peter A Cistulli
bull httpchestjournalchestpubsorgcontent1322693fullhtml
1112017
30
bullCurrent evidence suggests that despite the superior efficacy of CPAP both treatments produce similar subjective and objective health benefits
bullThe superior self-reported tolerance and compliance associated with MAD treatment is a likely explanation
bullThe practice parameters of the AASM recommend the use of oral appliances for mild-to-moderate OSA or for patients with severe OSA who are unable to tolerate CPAP or refuse treatment with CPAP with a required written prescription by a sleep physician
The following are Medicare rules
1) A diagnosis of OSA is not within the dental scope of practice A dentist providing an OA
must do so under the and with the team effort of a licensed Physician with a written
prescription
2) A physician is not skilled in the intricacies of fabricating fitting monitoring adjusting
and choosing an appropriate Oral Appliance individualized per patient
3) A dentist may not provide an oral appliance if the patient has an active
Temporomandibular Disorder
4) The OA must be fabricated within 90 days of the patientrsquos appointment with the sleep
physician
Since the rules are clear and they involve both of our professions it would behoove
both DOMD and DDS to communicate for the benefit of OSA patients
1112017
31
Subsequent to my 3 hour 2013 Meeting with the US Department of Transportation regarding Truckers
bull During the State Board of Dental Examiners meeting Board members put sleep Dentistry in squarely back into the spotlight The Board has addressed sleep Dentistry issues in a public hearing and all four Board meetings in 2013
bull There was discussion that there can be a shared relationship between the Dental and medical scopes of practice
bull Under the proposed rule a Dentist may treat benign snoring with an oral appliance after referral to a licensed physician where appropriate within the standard of care By contrast a Dentist may not diagnose treat or monitor OSA without collaboration with a licensed physician Additionally an oral appliance shall only be fabricated by a licensed Dentist or by a Dental lab under a prescription or work order prepared by a Dentist
American Dental Association
bull Treatment using an oral appliance designed specifically to treat OSA should be fabricated by a dentist familiar with device design maintenance and therapeutic efficacy and who has an association with and a referral from a sleep team
bull JADA Vol 136 p 1123
Donrsquot be afraid of OSA Get a grip on the facts and save patientrsquos lives
1112017
32
bullA SYMBIOTIC RELATION BETWEEN PHYSICIANS SLEEP PROFESSIONALS AND DENTISTS CAN SIGNIFICANTLY IMPROVE THE SLEEP HEALTH OF MILLIONS OF PEOPLE EACH AND EVERY YEAR
bull THAT RELATIONSHIP IS NOT A ONE WAY STREET AND THE
American Sleep amp Breathing Academy of over 8000 members UNDERSTANDS THAThellip JUST LOOK AT THE MULTITUDE OF SLEEP PROFESSIONAL CATAGORIES ON THEIR BOARD OF DIRECTORS
THE END
Thank you for your interest I hope this presentation was helpful
Dr Richard Klein
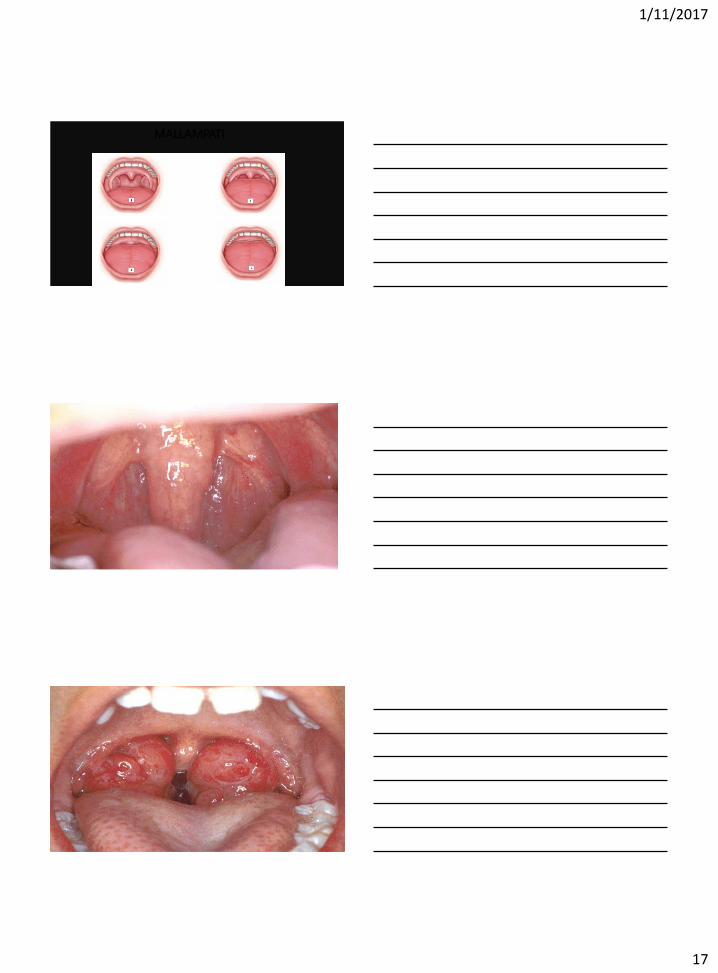
1112017
17
MALLAMPATI
1112017
18
Lavigne GJ Kato T Kolta A Sessle BJ Neurobiological mechanisms involved in sleep bruxism Crit Rev Oral Biol Med 20031430-46
bullSleep-related bruxism (SB) is characterized by the grinding or clenching of the teeth during sleep usually associated with sleep arousals although the incidence of sleep arousals in SB subjects is within the normal range (up to 14 arousalshour of sleep is considered normal)
IT HAS BEEN SHOWN THAT CPAP ELIMINATION OF OSA alsoELIMINATES SNORING
IT HAS NOT BEEN DEMONSTRATED THAT CPAP TREATMENT OF OSA
ELIMINATES OR REDUCES S-B
Neurobiological mechanisms involved in sleep bruxismLavigne GJ1 Kato T Kolta A Sessle BJ
bull Sleep bruxism (SB) is mainly associated with rhythmic masticatory muscle activity (RMMA) characterized by repetitive jaw muscle contractions (3 bursts or more at a frequency of 1 Hz)
bull The consequences of SB may include tooth destruction jaw pain headaches or the limitation of mandibular movement as well as tooth-grinding sounds that disrupt the sleep of bed partners RMMA is observed in 60 of normal sleepers
1112017
19
bull The pathophysiology of SB is becoming clearer
bull There is an abundance of evidence outlining the neurophysiology and neurochemistry of rhythmic jaw movements (RJM) in relation to chewing swallowing and breathing Several brainstem structures (eg reticular pontis oralis pontis caudalis) and neurochemicals (eg serotonin dopamine gamma aminobutyric acid [GABA] noradrenaline) are involved in both the genesis of RJM and the modulation of muscle tone during sleep
bull It creates a co-activation of both jaw-opening and jaw-closing muscles instead of the alternating jaw-opening and jaw-closing muscle activity pattern typical of chewing
Journal of Pain amp Symptom Management
bullPain duration and intensitywere correlated with decreased sleep impaired sleep quality and delayed sleep onset
Multiple Medical Studies
bullHave published that the majority (59 67 74) of OSA patients will not appropriately wear the CPAP
1112017
20
bull IN 1995 Johnny Cochran said ldquoIf the glove doesnrsquot fithellipyou must acquitrdquo As DR Dement intimated in the 1970s ldquoWe didnt know what to measurehellipso we measured everything we could think ofhellip and it stuckrdquo
bull Almost forty years later some of what ldquostuckrdquo is being revised reinterpreted and common sense is beginning to prevail Seven to eight hours of sleep per night is recommended
The Other 72 of Sleep
bull Sticking with the antiquated definition of a ldquocompliant userrdquo of a
CPAP (4 hrsnight and 5 nightsweek) one must use it roughly 28 of the time
bull WHAT ABOUT THE OTHER 72 OF SLEEP
bull Is it acceptable to not get the O2 we need simply because an antiquated standard ldquostuckrdquo
bull In 1995 CPAP became the gold standard Now in the 21st century I
say ldquoif the mask doesnrsquot fit hellipdonrsquot quitrdquo because an oral appliance may save your health and your life
Treatment of Sleep Apnea
Tracheotomy Oral
Surgery CPAPBiPAP
OA
Behavioral Modification
1112017
21
Orofacial Findings
bullThe most common orofacial characteristics include a retrognathic mandible narrow palate large neck circumference long soft palate tonsillar hypertrophy nasal septal deviation and relative macroglossia
Oral Appliances for Sleep Apnea amp Snoring
Tongue Retaining Devices Mandibular Repositioning Appliances
Oral Appliances (OA)
bull Properly fabricated an oral appliance will protrude the tongue and reposition the mandible anteriorly and inferiorly to the most beneficial neuromuscular position to prevent posterior airway collapse
bull This position is titratable and individualized to exact patient requirements and may need periodic adjustments just as does CPAP
1112017
22
BEFORE
APPLIANCE
7c
WITH
APPLIANCE
9 cc
1112017
23
Copyright 2011 BRAEBON
More Directly Related to hellipDental Sleep Medicine
bull EACH PATIENT IS AN INDIVIDUAL AND JUST AS CPAP PRESSURE IS INDIVIDUALLY TITRATEDhellipSO TOO ARE ORAL APPLIANCES
bull IF I DELIVER AN OA TO A PATIENT WHO WILL NOT UTILIZE THE CPAPhellipI WILL PROVIDE ONE OR SEVERAL HOME SLEEP STUDIES TO ASCERTAIN THE EFFICACY OF THE OAhellip AND THEN I REQUIRE THAT THEY RETURN TO THEIR SLEEP
bull DOCTOR FOR A SUBSEQUENT STUDY WHILE helliphelliphelliphelliphelliphelliphellipUTILIZINGTHE OA
Positional Apnea in a 73-Year Old Male with Atrial Fibrillation
bull This case study illustrates the cost-effective approach to successful outcomes associated with positional therapy that are not surprising and are consistent with a recent study which concluded ldquopositional therapy is equivalent to CPAP at normalizing the AHI in patients with positional OSA with similar effects on sleep quality and nocturnal oxygenationrdquo
bull Journal Sleep Diagnosis and Therapy
1112017
24
HOW THE ORAL APPLIANCE TREATS OSA
bull Prevent collapse of airwaybull Forward advancement of jawbull Support forward tongue positionbull Change shape of pharyngeal airwaybull Increase vertical dimension of occlusionbull Correct dysphagia bull Increase volume of space for tonguebull Trains protrusive tongue reflexesbull Alter position of hyoid bone relative to
mandible
THE VARYING ROLES OF THE NOSE AND MOUTH IN BREATHING
1112017
25
THE NOSE
bull A recent pediatric study reveals why addressing the tongue is so important for resolving sleep apnea As explained in this study having an abnormally short lingual frenulum can result in impaired orofacial growth in early childhood reducing the width of the upper airway
bull The upper airway is very pliable so this increases the risk of it collapsing during sleep They found that children with an untreated short frenulum developed abnormal tongue function early in life which also impacted their orofacial growth and led to disordered breathing during sleep
WHAT IS THE ROLE OF THE NOSE
ITS FUNCTIONS ARE VITAL
bull WARMING
bull HUMIDIFICATION
bull FILTERING
bull CLEANING
OF AMBIENT AIR INHALED INTO THE LUNGS
INFUSION OF NITRIC OXIDE
1112017
26
Humidification and
Dehumidification
bull During intake air is humidified to increase lung oxygen facilitation
bull Upon exhalation air is dehumidified to keep water in our cells
bull If this were not the case we would dehydrate unless we continually drank water
NARES
CONSTRICT
NARES FLARE
SNIFF TEST
1112017
27
Cosmetic Surgery
bullHe couldnrsquot breath through his small nose became hypercapnic and helliphelliphellipdied
Effect of treating severe nasal obstruction on the severity of obstructive sleep apnoea
bull HA McLean AM Urton HS Driver AKW Tan AG Day+ PW Munt and MF Fitzpatrick
bullThis study demonstrates that relief of severe nasal obstruction in patients with a normal retroglossal airway is associated with a significant reduction in mouth breathing during sleep improved sleep architecture and a modest improvement in OSA severity
1112017
28
bullThere are several novel aspects to these findings First the study documents a clearly increased upper airway resistance in association with oral breathing during stable sleep as compared with nasal breathing irrespective of central or OSA
bullSecondly this methodology included simultaneous documentation of oral and nasal ventilation during sleep to confirm the absence of any nasal airflow in the oral breathing condition and vice versa
1112017
29
bullThe substantially higher resistive load posed by the oral breathing route provides a plausible explanation for the observation that inhaled ventilation occurs almost exclusively via the nasal route during sleep in subjects with normal nasal resistance
bull Many studies have shown that nasal obstruction can induce or increase apnea frequency in OSA patients When nasal resistance is high a greater pressure drop is required to achieve the same flow and hence collapse of the pharynx is facilitated and this could mitigate the effect of mandibular advancement
bull Moreover high nasal resistance is associated with mouth breathing which could potentially limit the beneficial effect of mandibular advancement
bull Dental Appliance Treatment for Obstructive
bull Andrew S L Chan Richard W W Lee and Peter A Cistulli
bull httpchestjournalchestpubsorgcontent1322693fullhtml
1112017
30
bullCurrent evidence suggests that despite the superior efficacy of CPAP both treatments produce similar subjective and objective health benefits
bullThe superior self-reported tolerance and compliance associated with MAD treatment is a likely explanation
bullThe practice parameters of the AASM recommend the use of oral appliances for mild-to-moderate OSA or for patients with severe OSA who are unable to tolerate CPAP or refuse treatment with CPAP with a required written prescription by a sleep physician
The following are Medicare rules
1) A diagnosis of OSA is not within the dental scope of practice A dentist providing an OA
must do so under the and with the team effort of a licensed Physician with a written
prescription
2) A physician is not skilled in the intricacies of fabricating fitting monitoring adjusting
and choosing an appropriate Oral Appliance individualized per patient
3) A dentist may not provide an oral appliance if the patient has an active
Temporomandibular Disorder
4) The OA must be fabricated within 90 days of the patientrsquos appointment with the sleep
physician
Since the rules are clear and they involve both of our professions it would behoove
both DOMD and DDS to communicate for the benefit of OSA patients
1112017
31
Subsequent to my 3 hour 2013 Meeting with the US Department of Transportation regarding Truckers
bull During the State Board of Dental Examiners meeting Board members put sleep Dentistry in squarely back into the spotlight The Board has addressed sleep Dentistry issues in a public hearing and all four Board meetings in 2013
bull There was discussion that there can be a shared relationship between the Dental and medical scopes of practice
bull Under the proposed rule a Dentist may treat benign snoring with an oral appliance after referral to a licensed physician where appropriate within the standard of care By contrast a Dentist may not diagnose treat or monitor OSA without collaboration with a licensed physician Additionally an oral appliance shall only be fabricated by a licensed Dentist or by a Dental lab under a prescription or work order prepared by a Dentist
American Dental Association
bull Treatment using an oral appliance designed specifically to treat OSA should be fabricated by a dentist familiar with device design maintenance and therapeutic efficacy and who has an association with and a referral from a sleep team
bull JADA Vol 136 p 1123
Donrsquot be afraid of OSA Get a grip on the facts and save patientrsquos lives
1112017
32
bullA SYMBIOTIC RELATION BETWEEN PHYSICIANS SLEEP PROFESSIONALS AND DENTISTS CAN SIGNIFICANTLY IMPROVE THE SLEEP HEALTH OF MILLIONS OF PEOPLE EACH AND EVERY YEAR
bull THAT RELATIONSHIP IS NOT A ONE WAY STREET AND THE
American Sleep amp Breathing Academy of over 8000 members UNDERSTANDS THAThellip JUST LOOK AT THE MULTITUDE OF SLEEP PROFESSIONAL CATAGORIES ON THEIR BOARD OF DIRECTORS
THE END
Thank you for your interest I hope this presentation was helpful
Dr Richard Klein
1112017
18
Lavigne GJ Kato T Kolta A Sessle BJ Neurobiological mechanisms involved in sleep bruxism Crit Rev Oral Biol Med 20031430-46
bullSleep-related bruxism (SB) is characterized by the grinding or clenching of the teeth during sleep usually associated with sleep arousals although the incidence of sleep arousals in SB subjects is within the normal range (up to 14 arousalshour of sleep is considered normal)
IT HAS BEEN SHOWN THAT CPAP ELIMINATION OF OSA alsoELIMINATES SNORING
IT HAS NOT BEEN DEMONSTRATED THAT CPAP TREATMENT OF OSA
ELIMINATES OR REDUCES S-B
Neurobiological mechanisms involved in sleep bruxismLavigne GJ1 Kato T Kolta A Sessle BJ
bull Sleep bruxism (SB) is mainly associated with rhythmic masticatory muscle activity (RMMA) characterized by repetitive jaw muscle contractions (3 bursts or more at a frequency of 1 Hz)
bull The consequences of SB may include tooth destruction jaw pain headaches or the limitation of mandibular movement as well as tooth-grinding sounds that disrupt the sleep of bed partners RMMA is observed in 60 of normal sleepers
1112017
19
bull The pathophysiology of SB is becoming clearer
bull There is an abundance of evidence outlining the neurophysiology and neurochemistry of rhythmic jaw movements (RJM) in relation to chewing swallowing and breathing Several brainstem structures (eg reticular pontis oralis pontis caudalis) and neurochemicals (eg serotonin dopamine gamma aminobutyric acid [GABA] noradrenaline) are involved in both the genesis of RJM and the modulation of muscle tone during sleep
bull It creates a co-activation of both jaw-opening and jaw-closing muscles instead of the alternating jaw-opening and jaw-closing muscle activity pattern typical of chewing
Journal of Pain amp Symptom Management
bullPain duration and intensitywere correlated with decreased sleep impaired sleep quality and delayed sleep onset
Multiple Medical Studies
bullHave published that the majority (59 67 74) of OSA patients will not appropriately wear the CPAP
1112017
20
bull IN 1995 Johnny Cochran said ldquoIf the glove doesnrsquot fithellipyou must acquitrdquo As DR Dement intimated in the 1970s ldquoWe didnt know what to measurehellipso we measured everything we could think ofhellip and it stuckrdquo
bull Almost forty years later some of what ldquostuckrdquo is being revised reinterpreted and common sense is beginning to prevail Seven to eight hours of sleep per night is recommended
The Other 72 of Sleep
bull Sticking with the antiquated definition of a ldquocompliant userrdquo of a
CPAP (4 hrsnight and 5 nightsweek) one must use it roughly 28 of the time
bull WHAT ABOUT THE OTHER 72 OF SLEEP
bull Is it acceptable to not get the O2 we need simply because an antiquated standard ldquostuckrdquo
bull In 1995 CPAP became the gold standard Now in the 21st century I
say ldquoif the mask doesnrsquot fit hellipdonrsquot quitrdquo because an oral appliance may save your health and your life
Treatment of Sleep Apnea
Tracheotomy Oral
Surgery CPAPBiPAP
OA
Behavioral Modification
1112017
21
Orofacial Findings
bullThe most common orofacial characteristics include a retrognathic mandible narrow palate large neck circumference long soft palate tonsillar hypertrophy nasal septal deviation and relative macroglossia
Oral Appliances for Sleep Apnea amp Snoring
Tongue Retaining Devices Mandibular Repositioning Appliances
Oral Appliances (OA)
bull Properly fabricated an oral appliance will protrude the tongue and reposition the mandible anteriorly and inferiorly to the most beneficial neuromuscular position to prevent posterior airway collapse
bull This position is titratable and individualized to exact patient requirements and may need periodic adjustments just as does CPAP
1112017
22
BEFORE
APPLIANCE
7c
WITH
APPLIANCE
9 cc
1112017
23
Copyright 2011 BRAEBON
More Directly Related to hellipDental Sleep Medicine
bull EACH PATIENT IS AN INDIVIDUAL AND JUST AS CPAP PRESSURE IS INDIVIDUALLY TITRATEDhellipSO TOO ARE ORAL APPLIANCES
bull IF I DELIVER AN OA TO A PATIENT WHO WILL NOT UTILIZE THE CPAPhellipI WILL PROVIDE ONE OR SEVERAL HOME SLEEP STUDIES TO ASCERTAIN THE EFFICACY OF THE OAhellip AND THEN I REQUIRE THAT THEY RETURN TO THEIR SLEEP
bull DOCTOR FOR A SUBSEQUENT STUDY WHILE helliphelliphelliphelliphelliphelliphellipUTILIZINGTHE OA
Positional Apnea in a 73-Year Old Male with Atrial Fibrillation
bull This case study illustrates the cost-effective approach to successful outcomes associated with positional therapy that are not surprising and are consistent with a recent study which concluded ldquopositional therapy is equivalent to CPAP at normalizing the AHI in patients with positional OSA with similar effects on sleep quality and nocturnal oxygenationrdquo
bull Journal Sleep Diagnosis and Therapy
1112017
24
HOW THE ORAL APPLIANCE TREATS OSA
bull Prevent collapse of airwaybull Forward advancement of jawbull Support forward tongue positionbull Change shape of pharyngeal airwaybull Increase vertical dimension of occlusionbull Correct dysphagia bull Increase volume of space for tonguebull Trains protrusive tongue reflexesbull Alter position of hyoid bone relative to
mandible
THE VARYING ROLES OF THE NOSE AND MOUTH IN BREATHING
1112017
25
THE NOSE
bull A recent pediatric study reveals why addressing the tongue is so important for resolving sleep apnea As explained in this study having an abnormally short lingual frenulum can result in impaired orofacial growth in early childhood reducing the width of the upper airway
bull The upper airway is very pliable so this increases the risk of it collapsing during sleep They found that children with an untreated short frenulum developed abnormal tongue function early in life which also impacted their orofacial growth and led to disordered breathing during sleep
WHAT IS THE ROLE OF THE NOSE
ITS FUNCTIONS ARE VITAL
bull WARMING
bull HUMIDIFICATION
bull FILTERING
bull CLEANING
OF AMBIENT AIR INHALED INTO THE LUNGS
INFUSION OF NITRIC OXIDE
1112017
26
Humidification and
Dehumidification
bull During intake air is humidified to increase lung oxygen facilitation
bull Upon exhalation air is dehumidified to keep water in our cells
bull If this were not the case we would dehydrate unless we continually drank water
NARES
CONSTRICT
NARES FLARE
SNIFF TEST
1112017
27
Cosmetic Surgery
bullHe couldnrsquot breath through his small nose became hypercapnic and helliphelliphellipdied
Effect of treating severe nasal obstruction on the severity of obstructive sleep apnoea
bull HA McLean AM Urton HS Driver AKW Tan AG Day+ PW Munt and MF Fitzpatrick
bullThis study demonstrates that relief of severe nasal obstruction in patients with a normal retroglossal airway is associated with a significant reduction in mouth breathing during sleep improved sleep architecture and a modest improvement in OSA severity
1112017
28
bullThere are several novel aspects to these findings First the study documents a clearly increased upper airway resistance in association with oral breathing during stable sleep as compared with nasal breathing irrespective of central or OSA
bullSecondly this methodology included simultaneous documentation of oral and nasal ventilation during sleep to confirm the absence of any nasal airflow in the oral breathing condition and vice versa
1112017
29
bullThe substantially higher resistive load posed by the oral breathing route provides a plausible explanation for the observation that inhaled ventilation occurs almost exclusively via the nasal route during sleep in subjects with normal nasal resistance
bull Many studies have shown that nasal obstruction can induce or increase apnea frequency in OSA patients When nasal resistance is high a greater pressure drop is required to achieve the same flow and hence collapse of the pharynx is facilitated and this could mitigate the effect of mandibular advancement
bull Moreover high nasal resistance is associated with mouth breathing which could potentially limit the beneficial effect of mandibular advancement
bull Dental Appliance Treatment for Obstructive
bull Andrew S L Chan Richard W W Lee and Peter A Cistulli
bull httpchestjournalchestpubsorgcontent1322693fullhtml
1112017
30
bullCurrent evidence suggests that despite the superior efficacy of CPAP both treatments produce similar subjective and objective health benefits
bullThe superior self-reported tolerance and compliance associated with MAD treatment is a likely explanation
bullThe practice parameters of the AASM recommend the use of oral appliances for mild-to-moderate OSA or for patients with severe OSA who are unable to tolerate CPAP or refuse treatment with CPAP with a required written prescription by a sleep physician
The following are Medicare rules
1) A diagnosis of OSA is not within the dental scope of practice A dentist providing an OA
must do so under the and with the team effort of a licensed Physician with a written
prescription
2) A physician is not skilled in the intricacies of fabricating fitting monitoring adjusting
and choosing an appropriate Oral Appliance individualized per patient
3) A dentist may not provide an oral appliance if the patient has an active
Temporomandibular Disorder
4) The OA must be fabricated within 90 days of the patientrsquos appointment with the sleep
physician
Since the rules are clear and they involve both of our professions it would behoove
both DOMD and DDS to communicate for the benefit of OSA patients
1112017
31
Subsequent to my 3 hour 2013 Meeting with the US Department of Transportation regarding Truckers
bull During the State Board of Dental Examiners meeting Board members put sleep Dentistry in squarely back into the spotlight The Board has addressed sleep Dentistry issues in a public hearing and all four Board meetings in 2013
bull There was discussion that there can be a shared relationship between the Dental and medical scopes of practice
bull Under the proposed rule a Dentist may treat benign snoring with an oral appliance after referral to a licensed physician where appropriate within the standard of care By contrast a Dentist may not diagnose treat or monitor OSA without collaboration with a licensed physician Additionally an oral appliance shall only be fabricated by a licensed Dentist or by a Dental lab under a prescription or work order prepared by a Dentist
American Dental Association
bull Treatment using an oral appliance designed specifically to treat OSA should be fabricated by a dentist familiar with device design maintenance and therapeutic efficacy and who has an association with and a referral from a sleep team
bull JADA Vol 136 p 1123
Donrsquot be afraid of OSA Get a grip on the facts and save patientrsquos lives
1112017
32
bullA SYMBIOTIC RELATION BETWEEN PHYSICIANS SLEEP PROFESSIONALS AND DENTISTS CAN SIGNIFICANTLY IMPROVE THE SLEEP HEALTH OF MILLIONS OF PEOPLE EACH AND EVERY YEAR
bull THAT RELATIONSHIP IS NOT A ONE WAY STREET AND THE
American Sleep amp Breathing Academy of over 8000 members UNDERSTANDS THAThellip JUST LOOK AT THE MULTITUDE OF SLEEP PROFESSIONAL CATAGORIES ON THEIR BOARD OF DIRECTORS
THE END
Thank you for your interest I hope this presentation was helpful
Dr Richard Klein
1112017
19
bull The pathophysiology of SB is becoming clearer
bull There is an abundance of evidence outlining the neurophysiology and neurochemistry of rhythmic jaw movements (RJM) in relation to chewing swallowing and breathing Several brainstem structures (eg reticular pontis oralis pontis caudalis) and neurochemicals (eg serotonin dopamine gamma aminobutyric acid [GABA] noradrenaline) are involved in both the genesis of RJM and the modulation of muscle tone during sleep
bull It creates a co-activation of both jaw-opening and jaw-closing muscles instead of the alternating jaw-opening and jaw-closing muscle activity pattern typical of chewing
Journal of Pain amp Symptom Management
bullPain duration and intensitywere correlated with decreased sleep impaired sleep quality and delayed sleep onset
Multiple Medical Studies
bullHave published that the majority (59 67 74) of OSA patients will not appropriately wear the CPAP
1112017
20
bull IN 1995 Johnny Cochran said ldquoIf the glove doesnrsquot fithellipyou must acquitrdquo As DR Dement intimated in the 1970s ldquoWe didnt know what to measurehellipso we measured everything we could think ofhellip and it stuckrdquo
bull Almost forty years later some of what ldquostuckrdquo is being revised reinterpreted and common sense is beginning to prevail Seven to eight hours of sleep per night is recommended
The Other 72 of Sleep
bull Sticking with the antiquated definition of a ldquocompliant userrdquo of a
CPAP (4 hrsnight and 5 nightsweek) one must use it roughly 28 of the time
bull WHAT ABOUT THE OTHER 72 OF SLEEP
bull Is it acceptable to not get the O2 we need simply because an antiquated standard ldquostuckrdquo
bull In 1995 CPAP became the gold standard Now in the 21st century I
say ldquoif the mask doesnrsquot fit hellipdonrsquot quitrdquo because an oral appliance may save your health and your life
Treatment of Sleep Apnea
Tracheotomy Oral
Surgery CPAPBiPAP
OA
Behavioral Modification
1112017
21
Orofacial Findings
bullThe most common orofacial characteristics include a retrognathic mandible narrow palate large neck circumference long soft palate tonsillar hypertrophy nasal septal deviation and relative macroglossia
Oral Appliances for Sleep Apnea amp Snoring
Tongue Retaining Devices Mandibular Repositioning Appliances
Oral Appliances (OA)
bull Properly fabricated an oral appliance will protrude the tongue and reposition the mandible anteriorly and inferiorly to the most beneficial neuromuscular position to prevent posterior airway collapse
bull This position is titratable and individualized to exact patient requirements and may need periodic adjustments just as does CPAP
1112017
22
BEFORE
APPLIANCE
7c
WITH
APPLIANCE
9 cc
1112017
23
Copyright 2011 BRAEBON
More Directly Related to hellipDental Sleep Medicine
bull EACH PATIENT IS AN INDIVIDUAL AND JUST AS CPAP PRESSURE IS INDIVIDUALLY TITRATEDhellipSO TOO ARE ORAL APPLIANCES
bull IF I DELIVER AN OA TO A PATIENT WHO WILL NOT UTILIZE THE CPAPhellipI WILL PROVIDE ONE OR SEVERAL HOME SLEEP STUDIES TO ASCERTAIN THE EFFICACY OF THE OAhellip AND THEN I REQUIRE THAT THEY RETURN TO THEIR SLEEP
bull DOCTOR FOR A SUBSEQUENT STUDY WHILE helliphelliphelliphelliphelliphelliphellipUTILIZINGTHE OA
Positional Apnea in a 73-Year Old Male with Atrial Fibrillation
bull This case study illustrates the cost-effective approach to successful outcomes associated with positional therapy that are not surprising and are consistent with a recent study which concluded ldquopositional therapy is equivalent to CPAP at normalizing the AHI in patients with positional OSA with similar effects on sleep quality and nocturnal oxygenationrdquo
bull Journal Sleep Diagnosis and Therapy
1112017
24
HOW THE ORAL APPLIANCE TREATS OSA
bull Prevent collapse of airwaybull Forward advancement of jawbull Support forward tongue positionbull Change shape of pharyngeal airwaybull Increase vertical dimension of occlusionbull Correct dysphagia bull Increase volume of space for tonguebull Trains protrusive tongue reflexesbull Alter position of hyoid bone relative to
mandible
THE VARYING ROLES OF THE NOSE AND MOUTH IN BREATHING
1112017
25
THE NOSE
bull A recent pediatric study reveals why addressing the tongue is so important for resolving sleep apnea As explained in this study having an abnormally short lingual frenulum can result in impaired orofacial growth in early childhood reducing the width of the upper airway
bull The upper airway is very pliable so this increases the risk of it collapsing during sleep They found that children with an untreated short frenulum developed abnormal tongue function early in life which also impacted their orofacial growth and led to disordered breathing during sleep
WHAT IS THE ROLE OF THE NOSE
ITS FUNCTIONS ARE VITAL
bull WARMING
bull HUMIDIFICATION
bull FILTERING
bull CLEANING
OF AMBIENT AIR INHALED INTO THE LUNGS
INFUSION OF NITRIC OXIDE
1112017
26
Humidification and
Dehumidification
bull During intake air is humidified to increase lung oxygen facilitation
bull Upon exhalation air is dehumidified to keep water in our cells
bull If this were not the case we would dehydrate unless we continually drank water
NARES
CONSTRICT
NARES FLARE
SNIFF TEST
1112017
27
Cosmetic Surgery
bullHe couldnrsquot breath through his small nose became hypercapnic and helliphelliphellipdied
Effect of treating severe nasal obstruction on the severity of obstructive sleep apnoea
bull HA McLean AM Urton HS Driver AKW Tan AG Day+ PW Munt and MF Fitzpatrick
bullThis study demonstrates that relief of severe nasal obstruction in patients with a normal retroglossal airway is associated with a significant reduction in mouth breathing during sleep improved sleep architecture and a modest improvement in OSA severity
1112017
28
bullThere are several novel aspects to these findings First the study documents a clearly increased upper airway resistance in association with oral breathing during stable sleep as compared with nasal breathing irrespective of central or OSA
bullSecondly this methodology included simultaneous documentation of oral and nasal ventilation during sleep to confirm the absence of any nasal airflow in the oral breathing condition and vice versa
1112017
29
bullThe substantially higher resistive load posed by the oral breathing route provides a plausible explanation for the observation that inhaled ventilation occurs almost exclusively via the nasal route during sleep in subjects with normal nasal resistance
bull Many studies have shown that nasal obstruction can induce or increase apnea frequency in OSA patients When nasal resistance is high a greater pressure drop is required to achieve the same flow and hence collapse of the pharynx is facilitated and this could mitigate the effect of mandibular advancement
bull Moreover high nasal resistance is associated with mouth breathing which could potentially limit the beneficial effect of mandibular advancement
bull Dental Appliance Treatment for Obstructive
bull Andrew S L Chan Richard W W Lee and Peter A Cistulli
bull httpchestjournalchestpubsorgcontent1322693fullhtml
1112017
30
bullCurrent evidence suggests that despite the superior efficacy of CPAP both treatments produce similar subjective and objective health benefits
bullThe superior self-reported tolerance and compliance associated with MAD treatment is a likely explanation
bullThe practice parameters of the AASM recommend the use of oral appliances for mild-to-moderate OSA or for patients with severe OSA who are unable to tolerate CPAP or refuse treatment with CPAP with a required written prescription by a sleep physician
The following are Medicare rules
1) A diagnosis of OSA is not within the dental scope of practice A dentist providing an OA
must do so under the and with the team effort of a licensed Physician with a written
prescription
2) A physician is not skilled in the intricacies of fabricating fitting monitoring adjusting
and choosing an appropriate Oral Appliance individualized per patient
3) A dentist may not provide an oral appliance if the patient has an active
Temporomandibular Disorder
4) The OA must be fabricated within 90 days of the patientrsquos appointment with the sleep
physician
Since the rules are clear and they involve both of our professions it would behoove
both DOMD and DDS to communicate for the benefit of OSA patients
1112017
31
Subsequent to my 3 hour 2013 Meeting with the US Department of Transportation regarding Truckers
bull During the State Board of Dental Examiners meeting Board members put sleep Dentistry in squarely back into the spotlight The Board has addressed sleep Dentistry issues in a public hearing and all four Board meetings in 2013
bull There was discussion that there can be a shared relationship between the Dental and medical scopes of practice
bull Under the proposed rule a Dentist may treat benign snoring with an oral appliance after referral to a licensed physician where appropriate within the standard of care By contrast a Dentist may not diagnose treat or monitor OSA without collaboration with a licensed physician Additionally an oral appliance shall only be fabricated by a licensed Dentist or by a Dental lab under a prescription or work order prepared by a Dentist
American Dental Association
bull Treatment using an oral appliance designed specifically to treat OSA should be fabricated by a dentist familiar with device design maintenance and therapeutic efficacy and who has an association with and a referral from a sleep team
bull JADA Vol 136 p 1123
Donrsquot be afraid of OSA Get a grip on the facts and save patientrsquos lives
1112017
32
bullA SYMBIOTIC RELATION BETWEEN PHYSICIANS SLEEP PROFESSIONALS AND DENTISTS CAN SIGNIFICANTLY IMPROVE THE SLEEP HEALTH OF MILLIONS OF PEOPLE EACH AND EVERY YEAR
bull THAT RELATIONSHIP IS NOT A ONE WAY STREET AND THE
American Sleep amp Breathing Academy of over 8000 members UNDERSTANDS THAThellip JUST LOOK AT THE MULTITUDE OF SLEEP PROFESSIONAL CATAGORIES ON THEIR BOARD OF DIRECTORS
THE END
Thank you for your interest I hope this presentation was helpful
Dr Richard Klein
1112017
20
bull IN 1995 Johnny Cochran said ldquoIf the glove doesnrsquot fithellipyou must acquitrdquo As DR Dement intimated in the 1970s ldquoWe didnt know what to measurehellipso we measured everything we could think ofhellip and it stuckrdquo
bull Almost forty years later some of what ldquostuckrdquo is being revised reinterpreted and common sense is beginning to prevail Seven to eight hours of sleep per night is recommended
The Other 72 of Sleep
bull Sticking with the antiquated definition of a ldquocompliant userrdquo of a
CPAP (4 hrsnight and 5 nightsweek) one must use it roughly 28 of the time
bull WHAT ABOUT THE OTHER 72 OF SLEEP
bull Is it acceptable to not get the O2 we need simply because an antiquated standard ldquostuckrdquo
bull In 1995 CPAP became the gold standard Now in the 21st century I
say ldquoif the mask doesnrsquot fit hellipdonrsquot quitrdquo because an oral appliance may save your health and your life
Treatment of Sleep Apnea
Tracheotomy Oral
Surgery CPAPBiPAP
OA
Behavioral Modification
1112017
21
Orofacial Findings
bullThe most common orofacial characteristics include a retrognathic mandible narrow palate large neck circumference long soft palate tonsillar hypertrophy nasal septal deviation and relative macroglossia
Oral Appliances for Sleep Apnea amp Snoring
Tongue Retaining Devices Mandibular Repositioning Appliances
Oral Appliances (OA)
bull Properly fabricated an oral appliance will protrude the tongue and reposition the mandible anteriorly and inferiorly to the most beneficial neuromuscular position to prevent posterior airway collapse
bull This position is titratable and individualized to exact patient requirements and may need periodic adjustments just as does CPAP
1112017
22
BEFORE
APPLIANCE
7c
WITH
APPLIANCE
9 cc
1112017
23
Copyright 2011 BRAEBON
More Directly Related to hellipDental Sleep Medicine
bull EACH PATIENT IS AN INDIVIDUAL AND JUST AS CPAP PRESSURE IS INDIVIDUALLY TITRATEDhellipSO TOO ARE ORAL APPLIANCES
bull IF I DELIVER AN OA TO A PATIENT WHO WILL NOT UTILIZE THE CPAPhellipI WILL PROVIDE ONE OR SEVERAL HOME SLEEP STUDIES TO ASCERTAIN THE EFFICACY OF THE OAhellip AND THEN I REQUIRE THAT THEY RETURN TO THEIR SLEEP
bull DOCTOR FOR A SUBSEQUENT STUDY WHILE helliphelliphelliphelliphelliphelliphellipUTILIZINGTHE OA
Positional Apnea in a 73-Year Old Male with Atrial Fibrillation
bull This case study illustrates the cost-effective approach to successful outcomes associated with positional therapy that are not surprising and are consistent with a recent study which concluded ldquopositional therapy is equivalent to CPAP at normalizing the AHI in patients with positional OSA with similar effects on sleep quality and nocturnal oxygenationrdquo
bull Journal Sleep Diagnosis and Therapy
1112017
24
HOW THE ORAL APPLIANCE TREATS OSA
bull Prevent collapse of airwaybull Forward advancement of jawbull Support forward tongue positionbull Change shape of pharyngeal airwaybull Increase vertical dimension of occlusionbull Correct dysphagia bull Increase volume of space for tonguebull Trains protrusive tongue reflexesbull Alter position of hyoid bone relative to
mandible
THE VARYING ROLES OF THE NOSE AND MOUTH IN BREATHING
1112017
25
THE NOSE
bull A recent pediatric study reveals why addressing the tongue is so important for resolving sleep apnea As explained in this study having an abnormally short lingual frenulum can result in impaired orofacial growth in early childhood reducing the width of the upper airway
bull The upper airway is very pliable so this increases the risk of it collapsing during sleep They found that children with an untreated short frenulum developed abnormal tongue function early in life which also impacted their orofacial growth and led to disordered breathing during sleep
WHAT IS THE ROLE OF THE NOSE
ITS FUNCTIONS ARE VITAL
bull WARMING
bull HUMIDIFICATION
bull FILTERING
bull CLEANING
OF AMBIENT AIR INHALED INTO THE LUNGS
INFUSION OF NITRIC OXIDE
1112017
26
Humidification and
Dehumidification
bull During intake air is humidified to increase lung oxygen facilitation
bull Upon exhalation air is dehumidified to keep water in our cells
bull If this were not the case we would dehydrate unless we continually drank water
NARES
CONSTRICT
NARES FLARE
SNIFF TEST
1112017
27
Cosmetic Surgery
bullHe couldnrsquot breath through his small nose became hypercapnic and helliphelliphellipdied
Effect of treating severe nasal obstruction on the severity of obstructive sleep apnoea
bull HA McLean AM Urton HS Driver AKW Tan AG Day+ PW Munt and MF Fitzpatrick
bullThis study demonstrates that relief of severe nasal obstruction in patients with a normal retroglossal airway is associated with a significant reduction in mouth breathing during sleep improved sleep architecture and a modest improvement in OSA severity
1112017
28
bullThere are several novel aspects to these findings First the study documents a clearly increased upper airway resistance in association with oral breathing during stable sleep as compared with nasal breathing irrespective of central or OSA
bullSecondly this methodology included simultaneous documentation of oral and nasal ventilation during sleep to confirm the absence of any nasal airflow in the oral breathing condition and vice versa
1112017
29
bullThe substantially higher resistive load posed by the oral breathing route provides a plausible explanation for the observation that inhaled ventilation occurs almost exclusively via the nasal route during sleep in subjects with normal nasal resistance
bull Many studies have shown that nasal obstruction can induce or increase apnea frequency in OSA patients When nasal resistance is high a greater pressure drop is required to achieve the same flow and hence collapse of the pharynx is facilitated and this could mitigate the effect of mandibular advancement
bull Moreover high nasal resistance is associated with mouth breathing which could potentially limit the beneficial effect of mandibular advancement
bull Dental Appliance Treatment for Obstructive
bull Andrew S L Chan Richard W W Lee and Peter A Cistulli
bull httpchestjournalchestpubsorgcontent1322693fullhtml
1112017
30
bullCurrent evidence suggests that despite the superior efficacy of CPAP both treatments produce similar subjective and objective health benefits
bullThe superior self-reported tolerance and compliance associated with MAD treatment is a likely explanation
bullThe practice parameters of the AASM recommend the use of oral appliances for mild-to-moderate OSA or for patients with severe OSA who are unable to tolerate CPAP or refuse treatment with CPAP with a required written prescription by a sleep physician
The following are Medicare rules
1) A diagnosis of OSA is not within the dental scope of practice A dentist providing an OA
must do so under the and with the team effort of a licensed Physician with a written
prescription
2) A physician is not skilled in the intricacies of fabricating fitting monitoring adjusting
and choosing an appropriate Oral Appliance individualized per patient
3) A dentist may not provide an oral appliance if the patient has an active
Temporomandibular Disorder
4) The OA must be fabricated within 90 days of the patientrsquos appointment with the sleep
physician
Since the rules are clear and they involve both of our professions it would behoove
both DOMD and DDS to communicate for the benefit of OSA patients
1112017
31
Subsequent to my 3 hour 2013 Meeting with the US Department of Transportation regarding Truckers
bull During the State Board of Dental Examiners meeting Board members put sleep Dentistry in squarely back into the spotlight The Board has addressed sleep Dentistry issues in a public hearing and all four Board meetings in 2013
bull There was discussion that there can be a shared relationship between the Dental and medical scopes of practice
bull Under the proposed rule a Dentist may treat benign snoring with an oral appliance after referral to a licensed physician where appropriate within the standard of care By contrast a Dentist may not diagnose treat or monitor OSA without collaboration with a licensed physician Additionally an oral appliance shall only be fabricated by a licensed Dentist or by a Dental lab under a prescription or work order prepared by a Dentist
American Dental Association
bull Treatment using an oral appliance designed specifically to treat OSA should be fabricated by a dentist familiar with device design maintenance and therapeutic efficacy and who has an association with and a referral from a sleep team
bull JADA Vol 136 p 1123
Donrsquot be afraid of OSA Get a grip on the facts and save patientrsquos lives
1112017
32
bullA SYMBIOTIC RELATION BETWEEN PHYSICIANS SLEEP PROFESSIONALS AND DENTISTS CAN SIGNIFICANTLY IMPROVE THE SLEEP HEALTH OF MILLIONS OF PEOPLE EACH AND EVERY YEAR
bull THAT RELATIONSHIP IS NOT A ONE WAY STREET AND THE
American Sleep amp Breathing Academy of over 8000 members UNDERSTANDS THAThellip JUST LOOK AT THE MULTITUDE OF SLEEP PROFESSIONAL CATAGORIES ON THEIR BOARD OF DIRECTORS
THE END
Thank you for your interest I hope this presentation was helpful
Dr Richard Klein
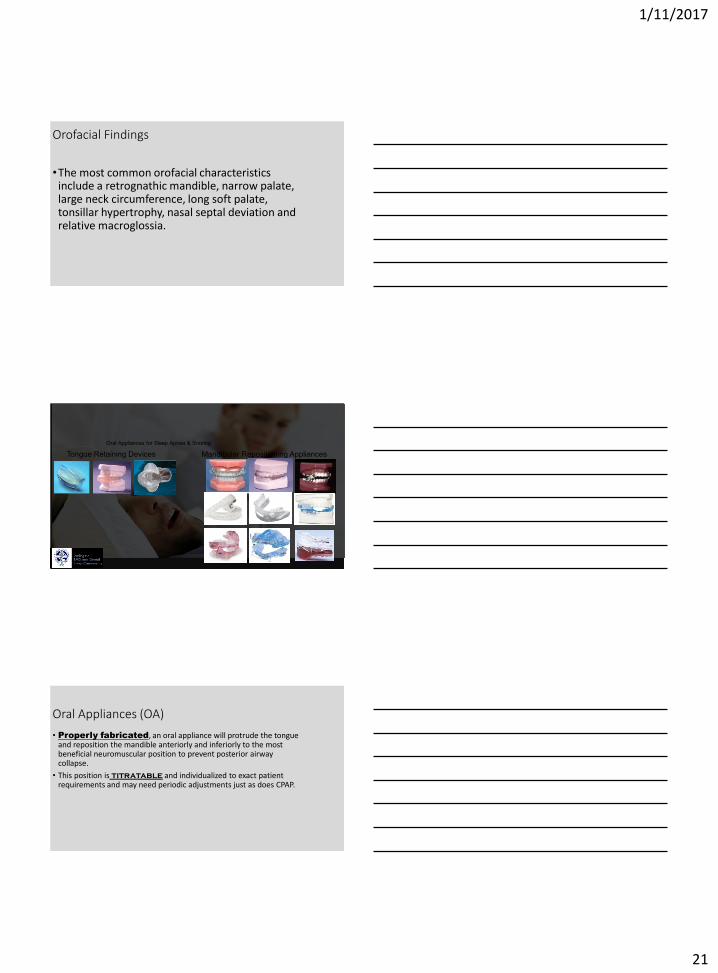
1112017
21
Orofacial Findings
bullThe most common orofacial characteristics include a retrognathic mandible narrow palate large neck circumference long soft palate tonsillar hypertrophy nasal septal deviation and relative macroglossia
Oral Appliances for Sleep Apnea amp Snoring
Tongue Retaining Devices Mandibular Repositioning Appliances
Oral Appliances (OA)
bull Properly fabricated an oral appliance will protrude the tongue and reposition the mandible anteriorly and inferiorly to the most beneficial neuromuscular position to prevent posterior airway collapse
bull This position is titratable and individualized to exact patient requirements and may need periodic adjustments just as does CPAP
1112017
22
BEFORE
APPLIANCE
7c
WITH
APPLIANCE
9 cc
1112017
23
Copyright 2011 BRAEBON
More Directly Related to hellipDental Sleep Medicine
bull EACH PATIENT IS AN INDIVIDUAL AND JUST AS CPAP PRESSURE IS INDIVIDUALLY TITRATEDhellipSO TOO ARE ORAL APPLIANCES
bull IF I DELIVER AN OA TO A PATIENT WHO WILL NOT UTILIZE THE CPAPhellipI WILL PROVIDE ONE OR SEVERAL HOME SLEEP STUDIES TO ASCERTAIN THE EFFICACY OF THE OAhellip AND THEN I REQUIRE THAT THEY RETURN TO THEIR SLEEP
bull DOCTOR FOR A SUBSEQUENT STUDY WHILE helliphelliphelliphelliphelliphelliphellipUTILIZINGTHE OA
Positional Apnea in a 73-Year Old Male with Atrial Fibrillation
bull This case study illustrates the cost-effective approach to successful outcomes associated with positional therapy that are not surprising and are consistent with a recent study which concluded ldquopositional therapy is equivalent to CPAP at normalizing the AHI in patients with positional OSA with similar effects on sleep quality and nocturnal oxygenationrdquo
bull Journal Sleep Diagnosis and Therapy
1112017
24
HOW THE ORAL APPLIANCE TREATS OSA
bull Prevent collapse of airwaybull Forward advancement of jawbull Support forward tongue positionbull Change shape of pharyngeal airwaybull Increase vertical dimension of occlusionbull Correct dysphagia bull Increase volume of space for tonguebull Trains protrusive tongue reflexesbull Alter position of hyoid bone relative to
mandible
THE VARYING ROLES OF THE NOSE AND MOUTH IN BREATHING
1112017
25
THE NOSE
bull A recent pediatric study reveals why addressing the tongue is so important for resolving sleep apnea As explained in this study having an abnormally short lingual frenulum can result in impaired orofacial growth in early childhood reducing the width of the upper airway
bull The upper airway is very pliable so this increases the risk of it collapsing during sleep They found that children with an untreated short frenulum developed abnormal tongue function early in life which also impacted their orofacial growth and led to disordered breathing during sleep
WHAT IS THE ROLE OF THE NOSE
ITS FUNCTIONS ARE VITAL
bull WARMING
bull HUMIDIFICATION
bull FILTERING
bull CLEANING
OF AMBIENT AIR INHALED INTO THE LUNGS
INFUSION OF NITRIC OXIDE
1112017
26
Humidification and
Dehumidification
bull During intake air is humidified to increase lung oxygen facilitation
bull Upon exhalation air is dehumidified to keep water in our cells
bull If this were not the case we would dehydrate unless we continually drank water
NARES
CONSTRICT
NARES FLARE
SNIFF TEST
1112017
27
Cosmetic Surgery
bullHe couldnrsquot breath through his small nose became hypercapnic and helliphelliphellipdied
Effect of treating severe nasal obstruction on the severity of obstructive sleep apnoea
bull HA McLean AM Urton HS Driver AKW Tan AG Day+ PW Munt and MF Fitzpatrick
bullThis study demonstrates that relief of severe nasal obstruction in patients with a normal retroglossal airway is associated with a significant reduction in mouth breathing during sleep improved sleep architecture and a modest improvement in OSA severity
1112017
28
bullThere are several novel aspects to these findings First the study documents a clearly increased upper airway resistance in association with oral breathing during stable sleep as compared with nasal breathing irrespective of central or OSA
bullSecondly this methodology included simultaneous documentation of oral and nasal ventilation during sleep to confirm the absence of any nasal airflow in the oral breathing condition and vice versa
1112017
29
bullThe substantially higher resistive load posed by the oral breathing route provides a plausible explanation for the observation that inhaled ventilation occurs almost exclusively via the nasal route during sleep in subjects with normal nasal resistance
bull Many studies have shown that nasal obstruction can induce or increase apnea frequency in OSA patients When nasal resistance is high a greater pressure drop is required to achieve the same flow and hence collapse of the pharynx is facilitated and this could mitigate the effect of mandibular advancement
bull Moreover high nasal resistance is associated with mouth breathing which could potentially limit the beneficial effect of mandibular advancement
bull Dental Appliance Treatment for Obstructive
bull Andrew S L Chan Richard W W Lee and Peter A Cistulli
bull httpchestjournalchestpubsorgcontent1322693fullhtml
1112017
30
bullCurrent evidence suggests that despite the superior efficacy of CPAP both treatments produce similar subjective and objective health benefits
bullThe superior self-reported tolerance and compliance associated with MAD treatment is a likely explanation
bullThe practice parameters of the AASM recommend the use of oral appliances for mild-to-moderate OSA or for patients with severe OSA who are unable to tolerate CPAP or refuse treatment with CPAP with a required written prescription by a sleep physician
The following are Medicare rules
1) A diagnosis of OSA is not within the dental scope of practice A dentist providing an OA
must do so under the and with the team effort of a licensed Physician with a written
prescription
2) A physician is not skilled in the intricacies of fabricating fitting monitoring adjusting
and choosing an appropriate Oral Appliance individualized per patient
3) A dentist may not provide an oral appliance if the patient has an active
Temporomandibular Disorder
4) The OA must be fabricated within 90 days of the patientrsquos appointment with the sleep
physician
Since the rules are clear and they involve both of our professions it would behoove
both DOMD and DDS to communicate for the benefit of OSA patients
1112017
31
Subsequent to my 3 hour 2013 Meeting with the US Department of Transportation regarding Truckers
bull During the State Board of Dental Examiners meeting Board members put sleep Dentistry in squarely back into the spotlight The Board has addressed sleep Dentistry issues in a public hearing and all four Board meetings in 2013
bull There was discussion that there can be a shared relationship between the Dental and medical scopes of practice
bull Under the proposed rule a Dentist may treat benign snoring with an oral appliance after referral to a licensed physician where appropriate within the standard of care By contrast a Dentist may not diagnose treat or monitor OSA without collaboration with a licensed physician Additionally an oral appliance shall only be fabricated by a licensed Dentist or by a Dental lab under a prescription or work order prepared by a Dentist
American Dental Association
bull Treatment using an oral appliance designed specifically to treat OSA should be fabricated by a dentist familiar with device design maintenance and therapeutic efficacy and who has an association with and a referral from a sleep team
bull JADA Vol 136 p 1123
Donrsquot be afraid of OSA Get a grip on the facts and save patientrsquos lives
1112017
32
bullA SYMBIOTIC RELATION BETWEEN PHYSICIANS SLEEP PROFESSIONALS AND DENTISTS CAN SIGNIFICANTLY IMPROVE THE SLEEP HEALTH OF MILLIONS OF PEOPLE EACH AND EVERY YEAR
bull THAT RELATIONSHIP IS NOT A ONE WAY STREET AND THE
American Sleep amp Breathing Academy of over 8000 members UNDERSTANDS THAThellip JUST LOOK AT THE MULTITUDE OF SLEEP PROFESSIONAL CATAGORIES ON THEIR BOARD OF DIRECTORS
THE END
Thank you for your interest I hope this presentation was helpful
Dr Richard Klein
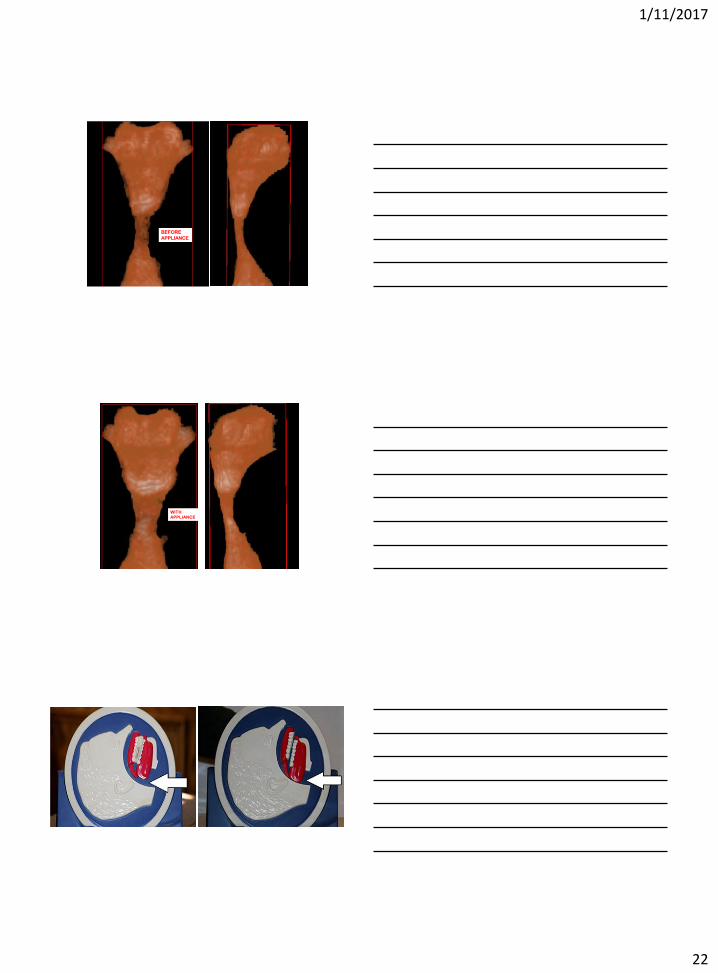
1112017
22
BEFORE
APPLIANCE
7c
WITH
APPLIANCE
9 cc
1112017
23
Copyright 2011 BRAEBON
More Directly Related to hellipDental Sleep Medicine
bull EACH PATIENT IS AN INDIVIDUAL AND JUST AS CPAP PRESSURE IS INDIVIDUALLY TITRATEDhellipSO TOO ARE ORAL APPLIANCES
bull IF I DELIVER AN OA TO A PATIENT WHO WILL NOT UTILIZE THE CPAPhellipI WILL PROVIDE ONE OR SEVERAL HOME SLEEP STUDIES TO ASCERTAIN THE EFFICACY OF THE OAhellip AND THEN I REQUIRE THAT THEY RETURN TO THEIR SLEEP
bull DOCTOR FOR A SUBSEQUENT STUDY WHILE helliphelliphelliphelliphelliphelliphellipUTILIZINGTHE OA
Positional Apnea in a 73-Year Old Male with Atrial Fibrillation
bull This case study illustrates the cost-effective approach to successful outcomes associated with positional therapy that are not surprising and are consistent with a recent study which concluded ldquopositional therapy is equivalent to CPAP at normalizing the AHI in patients with positional OSA with similar effects on sleep quality and nocturnal oxygenationrdquo
bull Journal Sleep Diagnosis and Therapy
1112017
24
HOW THE ORAL APPLIANCE TREATS OSA
bull Prevent collapse of airwaybull Forward advancement of jawbull Support forward tongue positionbull Change shape of pharyngeal airwaybull Increase vertical dimension of occlusionbull Correct dysphagia bull Increase volume of space for tonguebull Trains protrusive tongue reflexesbull Alter position of hyoid bone relative to
mandible
THE VARYING ROLES OF THE NOSE AND MOUTH IN BREATHING
1112017
25
THE NOSE
bull A recent pediatric study reveals why addressing the tongue is so important for resolving sleep apnea As explained in this study having an abnormally short lingual frenulum can result in impaired orofacial growth in early childhood reducing the width of the upper airway
bull The upper airway is very pliable so this increases the risk of it collapsing during sleep They found that children with an untreated short frenulum developed abnormal tongue function early in life which also impacted their orofacial growth and led to disordered breathing during sleep
WHAT IS THE ROLE OF THE NOSE
ITS FUNCTIONS ARE VITAL
bull WARMING
bull HUMIDIFICATION
bull FILTERING
bull CLEANING
OF AMBIENT AIR INHALED INTO THE LUNGS
INFUSION OF NITRIC OXIDE
1112017
26
Humidification and
Dehumidification
bull During intake air is humidified to increase lung oxygen facilitation
bull Upon exhalation air is dehumidified to keep water in our cells
bull If this were not the case we would dehydrate unless we continually drank water
NARES
CONSTRICT
NARES FLARE
SNIFF TEST
1112017
27
Cosmetic Surgery
bullHe couldnrsquot breath through his small nose became hypercapnic and helliphelliphellipdied
Effect of treating severe nasal obstruction on the severity of obstructive sleep apnoea
bull HA McLean AM Urton HS Driver AKW Tan AG Day+ PW Munt and MF Fitzpatrick
bullThis study demonstrates that relief of severe nasal obstruction in patients with a normal retroglossal airway is associated with a significant reduction in mouth breathing during sleep improved sleep architecture and a modest improvement in OSA severity
1112017
28
bullThere are several novel aspects to these findings First the study documents a clearly increased upper airway resistance in association with oral breathing during stable sleep as compared with nasal breathing irrespective of central or OSA
bullSecondly this methodology included simultaneous documentation of oral and nasal ventilation during sleep to confirm the absence of any nasal airflow in the oral breathing condition and vice versa
1112017
29
bullThe substantially higher resistive load posed by the oral breathing route provides a plausible explanation for the observation that inhaled ventilation occurs almost exclusively via the nasal route during sleep in subjects with normal nasal resistance
bull Many studies have shown that nasal obstruction can induce or increase apnea frequency in OSA patients When nasal resistance is high a greater pressure drop is required to achieve the same flow and hence collapse of the pharynx is facilitated and this could mitigate the effect of mandibular advancement
bull Moreover high nasal resistance is associated with mouth breathing which could potentially limit the beneficial effect of mandibular advancement
bull Dental Appliance Treatment for Obstructive
bull Andrew S L Chan Richard W W Lee and Peter A Cistulli
bull httpchestjournalchestpubsorgcontent1322693fullhtml
1112017
30
bullCurrent evidence suggests that despite the superior efficacy of CPAP both treatments produce similar subjective and objective health benefits
bullThe superior self-reported tolerance and compliance associated with MAD treatment is a likely explanation
bullThe practice parameters of the AASM recommend the use of oral appliances for mild-to-moderate OSA or for patients with severe OSA who are unable to tolerate CPAP or refuse treatment with CPAP with a required written prescription by a sleep physician
The following are Medicare rules
1) A diagnosis of OSA is not within the dental scope of practice A dentist providing an OA
must do so under the and with the team effort of a licensed Physician with a written
prescription
2) A physician is not skilled in the intricacies of fabricating fitting monitoring adjusting
and choosing an appropriate Oral Appliance individualized per patient
3) A dentist may not provide an oral appliance if the patient has an active
Temporomandibular Disorder
4) The OA must be fabricated within 90 days of the patientrsquos appointment with the sleep
physician
Since the rules are clear and they involve both of our professions it would behoove
both DOMD and DDS to communicate for the benefit of OSA patients
1112017
31
Subsequent to my 3 hour 2013 Meeting with the US Department of Transportation regarding Truckers
bull During the State Board of Dental Examiners meeting Board members put sleep Dentistry in squarely back into the spotlight The Board has addressed sleep Dentistry issues in a public hearing and all four Board meetings in 2013
bull There was discussion that there can be a shared relationship between the Dental and medical scopes of practice
bull Under the proposed rule a Dentist may treat benign snoring with an oral appliance after referral to a licensed physician where appropriate within the standard of care By contrast a Dentist may not diagnose treat or monitor OSA without collaboration with a licensed physician Additionally an oral appliance shall only be fabricated by a licensed Dentist or by a Dental lab under a prescription or work order prepared by a Dentist
American Dental Association
bull Treatment using an oral appliance designed specifically to treat OSA should be fabricated by a dentist familiar with device design maintenance and therapeutic efficacy and who has an association with and a referral from a sleep team
bull JADA Vol 136 p 1123
Donrsquot be afraid of OSA Get a grip on the facts and save patientrsquos lives
1112017
32
bullA SYMBIOTIC RELATION BETWEEN PHYSICIANS SLEEP PROFESSIONALS AND DENTISTS CAN SIGNIFICANTLY IMPROVE THE SLEEP HEALTH OF MILLIONS OF PEOPLE EACH AND EVERY YEAR
bull THAT RELATIONSHIP IS NOT A ONE WAY STREET AND THE
American Sleep amp Breathing Academy of over 8000 members UNDERSTANDS THAThellip JUST LOOK AT THE MULTITUDE OF SLEEP PROFESSIONAL CATAGORIES ON THEIR BOARD OF DIRECTORS
THE END
Thank you for your interest I hope this presentation was helpful
Dr Richard Klein
1112017
23
Copyright 2011 BRAEBON
More Directly Related to hellipDental Sleep Medicine
bull EACH PATIENT IS AN INDIVIDUAL AND JUST AS CPAP PRESSURE IS INDIVIDUALLY TITRATEDhellipSO TOO ARE ORAL APPLIANCES
bull IF I DELIVER AN OA TO A PATIENT WHO WILL NOT UTILIZE THE CPAPhellipI WILL PROVIDE ONE OR SEVERAL HOME SLEEP STUDIES TO ASCERTAIN THE EFFICACY OF THE OAhellip AND THEN I REQUIRE THAT THEY RETURN TO THEIR SLEEP
bull DOCTOR FOR A SUBSEQUENT STUDY WHILE helliphelliphelliphelliphelliphelliphellipUTILIZINGTHE OA
Positional Apnea in a 73-Year Old Male with Atrial Fibrillation
bull This case study illustrates the cost-effective approach to successful outcomes associated with positional therapy that are not surprising and are consistent with a recent study which concluded ldquopositional therapy is equivalent to CPAP at normalizing the AHI in patients with positional OSA with similar effects on sleep quality and nocturnal oxygenationrdquo
bull Journal Sleep Diagnosis and Therapy
1112017
24
HOW THE ORAL APPLIANCE TREATS OSA
bull Prevent collapse of airwaybull Forward advancement of jawbull Support forward tongue positionbull Change shape of pharyngeal airwaybull Increase vertical dimension of occlusionbull Correct dysphagia bull Increase volume of space for tonguebull Trains protrusive tongue reflexesbull Alter position of hyoid bone relative to
mandible
THE VARYING ROLES OF THE NOSE AND MOUTH IN BREATHING
1112017
25
THE NOSE
bull A recent pediatric study reveals why addressing the tongue is so important for resolving sleep apnea As explained in this study having an abnormally short lingual frenulum can result in impaired orofacial growth in early childhood reducing the width of the upper airway
bull The upper airway is very pliable so this increases the risk of it collapsing during sleep They found that children with an untreated short frenulum developed abnormal tongue function early in life which also impacted their orofacial growth and led to disordered breathing during sleep
WHAT IS THE ROLE OF THE NOSE
ITS FUNCTIONS ARE VITAL
bull WARMING
bull HUMIDIFICATION
bull FILTERING
bull CLEANING
OF AMBIENT AIR INHALED INTO THE LUNGS
INFUSION OF NITRIC OXIDE
1112017
26
Humidification and
Dehumidification
bull During intake air is humidified to increase lung oxygen facilitation
bull Upon exhalation air is dehumidified to keep water in our cells
bull If this were not the case we would dehydrate unless we continually drank water
NARES
CONSTRICT
NARES FLARE
SNIFF TEST
1112017
27
Cosmetic Surgery
bullHe couldnrsquot breath through his small nose became hypercapnic and helliphelliphellipdied
Effect of treating severe nasal obstruction on the severity of obstructive sleep apnoea
bull HA McLean AM Urton HS Driver AKW Tan AG Day+ PW Munt and MF Fitzpatrick
bullThis study demonstrates that relief of severe nasal obstruction in patients with a normal retroglossal airway is associated with a significant reduction in mouth breathing during sleep improved sleep architecture and a modest improvement in OSA severity
1112017
28
bullThere are several novel aspects to these findings First the study documents a clearly increased upper airway resistance in association with oral breathing during stable sleep as compared with nasal breathing irrespective of central or OSA
bullSecondly this methodology included simultaneous documentation of oral and nasal ventilation during sleep to confirm the absence of any nasal airflow in the oral breathing condition and vice versa
1112017
29
bullThe substantially higher resistive load posed by the oral breathing route provides a plausible explanation for the observation that inhaled ventilation occurs almost exclusively via the nasal route during sleep in subjects with normal nasal resistance
bull Many studies have shown that nasal obstruction can induce or increase apnea frequency in OSA patients When nasal resistance is high a greater pressure drop is required to achieve the same flow and hence collapse of the pharynx is facilitated and this could mitigate the effect of mandibular advancement
bull Moreover high nasal resistance is associated with mouth breathing which could potentially limit the beneficial effect of mandibular advancement
bull Dental Appliance Treatment for Obstructive
bull Andrew S L Chan Richard W W Lee and Peter A Cistulli
bull httpchestjournalchestpubsorgcontent1322693fullhtml
1112017
30
bullCurrent evidence suggests that despite the superior efficacy of CPAP both treatments produce similar subjective and objective health benefits
bullThe superior self-reported tolerance and compliance associated with MAD treatment is a likely explanation
bullThe practice parameters of the AASM recommend the use of oral appliances for mild-to-moderate OSA or for patients with severe OSA who are unable to tolerate CPAP or refuse treatment with CPAP with a required written prescription by a sleep physician
The following are Medicare rules
1) A diagnosis of OSA is not within the dental scope of practice A dentist providing an OA
must do so under the and with the team effort of a licensed Physician with a written
prescription
2) A physician is not skilled in the intricacies of fabricating fitting monitoring adjusting
and choosing an appropriate Oral Appliance individualized per patient
3) A dentist may not provide an oral appliance if the patient has an active
Temporomandibular Disorder
4) The OA must be fabricated within 90 days of the patientrsquos appointment with the sleep
physician
Since the rules are clear and they involve both of our professions it would behoove
both DOMD and DDS to communicate for the benefit of OSA patients
1112017
31
Subsequent to my 3 hour 2013 Meeting with the US Department of Transportation regarding Truckers
bull During the State Board of Dental Examiners meeting Board members put sleep Dentistry in squarely back into the spotlight The Board has addressed sleep Dentistry issues in a public hearing and all four Board meetings in 2013
bull There was discussion that there can be a shared relationship between the Dental and medical scopes of practice
bull Under the proposed rule a Dentist may treat benign snoring with an oral appliance after referral to a licensed physician where appropriate within the standard of care By contrast a Dentist may not diagnose treat or monitor OSA without collaboration with a licensed physician Additionally an oral appliance shall only be fabricated by a licensed Dentist or by a Dental lab under a prescription or work order prepared by a Dentist
American Dental Association
bull Treatment using an oral appliance designed specifically to treat OSA should be fabricated by a dentist familiar with device design maintenance and therapeutic efficacy and who has an association with and a referral from a sleep team
bull JADA Vol 136 p 1123
Donrsquot be afraid of OSA Get a grip on the facts and save patientrsquos lives
1112017
32
bullA SYMBIOTIC RELATION BETWEEN PHYSICIANS SLEEP PROFESSIONALS AND DENTISTS CAN SIGNIFICANTLY IMPROVE THE SLEEP HEALTH OF MILLIONS OF PEOPLE EACH AND EVERY YEAR
bull THAT RELATIONSHIP IS NOT A ONE WAY STREET AND THE
American Sleep amp Breathing Academy of over 8000 members UNDERSTANDS THAThellip JUST LOOK AT THE MULTITUDE OF SLEEP PROFESSIONAL CATAGORIES ON THEIR BOARD OF DIRECTORS
THE END
Thank you for your interest I hope this presentation was helpful
Dr Richard Klein
1112017
24
HOW THE ORAL APPLIANCE TREATS OSA
bull Prevent collapse of airwaybull Forward advancement of jawbull Support forward tongue positionbull Change shape of pharyngeal airwaybull Increase vertical dimension of occlusionbull Correct dysphagia bull Increase volume of space for tonguebull Trains protrusive tongue reflexesbull Alter position of hyoid bone relative to
mandible
THE VARYING ROLES OF THE NOSE AND MOUTH IN BREATHING
1112017
25
THE NOSE
bull A recent pediatric study reveals why addressing the tongue is so important for resolving sleep apnea As explained in this study having an abnormally short lingual frenulum can result in impaired orofacial growth in early childhood reducing the width of the upper airway
bull The upper airway is very pliable so this increases the risk of it collapsing during sleep They found that children with an untreated short frenulum developed abnormal tongue function early in life which also impacted their orofacial growth and led to disordered breathing during sleep
WHAT IS THE ROLE OF THE NOSE
ITS FUNCTIONS ARE VITAL
bull WARMING
bull HUMIDIFICATION
bull FILTERING
bull CLEANING
OF AMBIENT AIR INHALED INTO THE LUNGS
INFUSION OF NITRIC OXIDE
1112017
26
Humidification and
Dehumidification
bull During intake air is humidified to increase lung oxygen facilitation
bull Upon exhalation air is dehumidified to keep water in our cells
bull If this were not the case we would dehydrate unless we continually drank water
NARES
CONSTRICT
NARES FLARE
SNIFF TEST
1112017
27
Cosmetic Surgery
bullHe couldnrsquot breath through his small nose became hypercapnic and helliphelliphellipdied
Effect of treating severe nasal obstruction on the severity of obstructive sleep apnoea
bull HA McLean AM Urton HS Driver AKW Tan AG Day+ PW Munt and MF Fitzpatrick
bullThis study demonstrates that relief of severe nasal obstruction in patients with a normal retroglossal airway is associated with a significant reduction in mouth breathing during sleep improved sleep architecture and a modest improvement in OSA severity
1112017
28
bullThere are several novel aspects to these findings First the study documents a clearly increased upper airway resistance in association with oral breathing during stable sleep as compared with nasal breathing irrespective of central or OSA
bullSecondly this methodology included simultaneous documentation of oral and nasal ventilation during sleep to confirm the absence of any nasal airflow in the oral breathing condition and vice versa
1112017
29
bullThe substantially higher resistive load posed by the oral breathing route provides a plausible explanation for the observation that inhaled ventilation occurs almost exclusively via the nasal route during sleep in subjects with normal nasal resistance
bull Many studies have shown that nasal obstruction can induce or increase apnea frequency in OSA patients When nasal resistance is high a greater pressure drop is required to achieve the same flow and hence collapse of the pharynx is facilitated and this could mitigate the effect of mandibular advancement
bull Moreover high nasal resistance is associated with mouth breathing which could potentially limit the beneficial effect of mandibular advancement
bull Dental Appliance Treatment for Obstructive
bull Andrew S L Chan Richard W W Lee and Peter A Cistulli
bull httpchestjournalchestpubsorgcontent1322693fullhtml
1112017
30
bullCurrent evidence suggests that despite the superior efficacy of CPAP both treatments produce similar subjective and objective health benefits
bullThe superior self-reported tolerance and compliance associated with MAD treatment is a likely explanation
bullThe practice parameters of the AASM recommend the use of oral appliances for mild-to-moderate OSA or for patients with severe OSA who are unable to tolerate CPAP or refuse treatment with CPAP with a required written prescription by a sleep physician
The following are Medicare rules
1) A diagnosis of OSA is not within the dental scope of practice A dentist providing an OA
must do so under the and with the team effort of a licensed Physician with a written
prescription
2) A physician is not skilled in the intricacies of fabricating fitting monitoring adjusting
and choosing an appropriate Oral Appliance individualized per patient
3) A dentist may not provide an oral appliance if the patient has an active
Temporomandibular Disorder
4) The OA must be fabricated within 90 days of the patientrsquos appointment with the sleep
physician
Since the rules are clear and they involve both of our professions it would behoove
both DOMD and DDS to communicate for the benefit of OSA patients
1112017
31
Subsequent to my 3 hour 2013 Meeting with the US Department of Transportation regarding Truckers
bull During the State Board of Dental Examiners meeting Board members put sleep Dentistry in squarely back into the spotlight The Board has addressed sleep Dentistry issues in a public hearing and all four Board meetings in 2013
bull There was discussion that there can be a shared relationship between the Dental and medical scopes of practice
bull Under the proposed rule a Dentist may treat benign snoring with an oral appliance after referral to a licensed physician where appropriate within the standard of care By contrast a Dentist may not diagnose treat or monitor OSA without collaboration with a licensed physician Additionally an oral appliance shall only be fabricated by a licensed Dentist or by a Dental lab under a prescription or work order prepared by a Dentist
American Dental Association
bull Treatment using an oral appliance designed specifically to treat OSA should be fabricated by a dentist familiar with device design maintenance and therapeutic efficacy and who has an association with and a referral from a sleep team
bull JADA Vol 136 p 1123
Donrsquot be afraid of OSA Get a grip on the facts and save patientrsquos lives
1112017
32
bullA SYMBIOTIC RELATION BETWEEN PHYSICIANS SLEEP PROFESSIONALS AND DENTISTS CAN SIGNIFICANTLY IMPROVE THE SLEEP HEALTH OF MILLIONS OF PEOPLE EACH AND EVERY YEAR
bull THAT RELATIONSHIP IS NOT A ONE WAY STREET AND THE
American Sleep amp Breathing Academy of over 8000 members UNDERSTANDS THAThellip JUST LOOK AT THE MULTITUDE OF SLEEP PROFESSIONAL CATAGORIES ON THEIR BOARD OF DIRECTORS
THE END
Thank you for your interest I hope this presentation was helpful
Dr Richard Klein
1112017
25
THE NOSE
bull A recent pediatric study reveals why addressing the tongue is so important for resolving sleep apnea As explained in this study having an abnormally short lingual frenulum can result in impaired orofacial growth in early childhood reducing the width of the upper airway
bull The upper airway is very pliable so this increases the risk of it collapsing during sleep They found that children with an untreated short frenulum developed abnormal tongue function early in life which also impacted their orofacial growth and led to disordered breathing during sleep
WHAT IS THE ROLE OF THE NOSE
ITS FUNCTIONS ARE VITAL
bull WARMING
bull HUMIDIFICATION
bull FILTERING
bull CLEANING
OF AMBIENT AIR INHALED INTO THE LUNGS
INFUSION OF NITRIC OXIDE
1112017
26
Humidification and
Dehumidification
bull During intake air is humidified to increase lung oxygen facilitation
bull Upon exhalation air is dehumidified to keep water in our cells
bull If this were not the case we would dehydrate unless we continually drank water
NARES
CONSTRICT
NARES FLARE
SNIFF TEST
1112017
27
Cosmetic Surgery
bullHe couldnrsquot breath through his small nose became hypercapnic and helliphelliphellipdied
Effect of treating severe nasal obstruction on the severity of obstructive sleep apnoea
bull HA McLean AM Urton HS Driver AKW Tan AG Day+ PW Munt and MF Fitzpatrick
bullThis study demonstrates that relief of severe nasal obstruction in patients with a normal retroglossal airway is associated with a significant reduction in mouth breathing during sleep improved sleep architecture and a modest improvement in OSA severity
1112017
28
bullThere are several novel aspects to these findings First the study documents a clearly increased upper airway resistance in association with oral breathing during stable sleep as compared with nasal breathing irrespective of central or OSA
bullSecondly this methodology included simultaneous documentation of oral and nasal ventilation during sleep to confirm the absence of any nasal airflow in the oral breathing condition and vice versa
1112017
29
bullThe substantially higher resistive load posed by the oral breathing route provides a plausible explanation for the observation that inhaled ventilation occurs almost exclusively via the nasal route during sleep in subjects with normal nasal resistance
bull Many studies have shown that nasal obstruction can induce or increase apnea frequency in OSA patients When nasal resistance is high a greater pressure drop is required to achieve the same flow and hence collapse of the pharynx is facilitated and this could mitigate the effect of mandibular advancement
bull Moreover high nasal resistance is associated with mouth breathing which could potentially limit the beneficial effect of mandibular advancement
bull Dental Appliance Treatment for Obstructive
bull Andrew S L Chan Richard W W Lee and Peter A Cistulli
bull httpchestjournalchestpubsorgcontent1322693fullhtml
1112017
30
bullCurrent evidence suggests that despite the superior efficacy of CPAP both treatments produce similar subjective and objective health benefits
bullThe superior self-reported tolerance and compliance associated with MAD treatment is a likely explanation
bullThe practice parameters of the AASM recommend the use of oral appliances for mild-to-moderate OSA or for patients with severe OSA who are unable to tolerate CPAP or refuse treatment with CPAP with a required written prescription by a sleep physician
The following are Medicare rules
1) A diagnosis of OSA is not within the dental scope of practice A dentist providing an OA
must do so under the and with the team effort of a licensed Physician with a written
prescription
2) A physician is not skilled in the intricacies of fabricating fitting monitoring adjusting
and choosing an appropriate Oral Appliance individualized per patient
3) A dentist may not provide an oral appliance if the patient has an active
Temporomandibular Disorder
4) The OA must be fabricated within 90 days of the patientrsquos appointment with the sleep
physician
Since the rules are clear and they involve both of our professions it would behoove
both DOMD and DDS to communicate for the benefit of OSA patients
1112017
31
Subsequent to my 3 hour 2013 Meeting with the US Department of Transportation regarding Truckers
bull During the State Board of Dental Examiners meeting Board members put sleep Dentistry in squarely back into the spotlight The Board has addressed sleep Dentistry issues in a public hearing and all four Board meetings in 2013
bull There was discussion that there can be a shared relationship between the Dental and medical scopes of practice
bull Under the proposed rule a Dentist may treat benign snoring with an oral appliance after referral to a licensed physician where appropriate within the standard of care By contrast a Dentist may not diagnose treat or monitor OSA without collaboration with a licensed physician Additionally an oral appliance shall only be fabricated by a licensed Dentist or by a Dental lab under a prescription or work order prepared by a Dentist
American Dental Association
bull Treatment using an oral appliance designed specifically to treat OSA should be fabricated by a dentist familiar with device design maintenance and therapeutic efficacy and who has an association with and a referral from a sleep team
bull JADA Vol 136 p 1123
Donrsquot be afraid of OSA Get a grip on the facts and save patientrsquos lives
1112017
32
bullA SYMBIOTIC RELATION BETWEEN PHYSICIANS SLEEP PROFESSIONALS AND DENTISTS CAN SIGNIFICANTLY IMPROVE THE SLEEP HEALTH OF MILLIONS OF PEOPLE EACH AND EVERY YEAR
bull THAT RELATIONSHIP IS NOT A ONE WAY STREET AND THE
American Sleep amp Breathing Academy of over 8000 members UNDERSTANDS THAThellip JUST LOOK AT THE MULTITUDE OF SLEEP PROFESSIONAL CATAGORIES ON THEIR BOARD OF DIRECTORS
THE END
Thank you for your interest I hope this presentation was helpful
Dr Richard Klein
1112017
26
Humidification and
Dehumidification
bull During intake air is humidified to increase lung oxygen facilitation
bull Upon exhalation air is dehumidified to keep water in our cells
bull If this were not the case we would dehydrate unless we continually drank water
NARES
CONSTRICT
NARES FLARE
SNIFF TEST
1112017
27
Cosmetic Surgery
bullHe couldnrsquot breath through his small nose became hypercapnic and helliphelliphellipdied
Effect of treating severe nasal obstruction on the severity of obstructive sleep apnoea
bull HA McLean AM Urton HS Driver AKW Tan AG Day+ PW Munt and MF Fitzpatrick
bullThis study demonstrates that relief of severe nasal obstruction in patients with a normal retroglossal airway is associated with a significant reduction in mouth breathing during sleep improved sleep architecture and a modest improvement in OSA severity
1112017
28
bullThere are several novel aspects to these findings First the study documents a clearly increased upper airway resistance in association with oral breathing during stable sleep as compared with nasal breathing irrespective of central or OSA
bullSecondly this methodology included simultaneous documentation of oral and nasal ventilation during sleep to confirm the absence of any nasal airflow in the oral breathing condition and vice versa
1112017
29
bullThe substantially higher resistive load posed by the oral breathing route provides a plausible explanation for the observation that inhaled ventilation occurs almost exclusively via the nasal route during sleep in subjects with normal nasal resistance
bull Many studies have shown that nasal obstruction can induce or increase apnea frequency in OSA patients When nasal resistance is high a greater pressure drop is required to achieve the same flow and hence collapse of the pharynx is facilitated and this could mitigate the effect of mandibular advancement
bull Moreover high nasal resistance is associated with mouth breathing which could potentially limit the beneficial effect of mandibular advancement
bull Dental Appliance Treatment for Obstructive
bull Andrew S L Chan Richard W W Lee and Peter A Cistulli
bull httpchestjournalchestpubsorgcontent1322693fullhtml
1112017
30
bullCurrent evidence suggests that despite the superior efficacy of CPAP both treatments produce similar subjective and objective health benefits
bullThe superior self-reported tolerance and compliance associated with MAD treatment is a likely explanation
bullThe practice parameters of the AASM recommend the use of oral appliances for mild-to-moderate OSA or for patients with severe OSA who are unable to tolerate CPAP or refuse treatment with CPAP with a required written prescription by a sleep physician
The following are Medicare rules
1) A diagnosis of OSA is not within the dental scope of practice A dentist providing an OA
must do so under the and with the team effort of a licensed Physician with a written
prescription
2) A physician is not skilled in the intricacies of fabricating fitting monitoring adjusting
and choosing an appropriate Oral Appliance individualized per patient
3) A dentist may not provide an oral appliance if the patient has an active
Temporomandibular Disorder
4) The OA must be fabricated within 90 days of the patientrsquos appointment with the sleep
physician
Since the rules are clear and they involve both of our professions it would behoove
both DOMD and DDS to communicate for the benefit of OSA patients
1112017
31
Subsequent to my 3 hour 2013 Meeting with the US Department of Transportation regarding Truckers
bull During the State Board of Dental Examiners meeting Board members put sleep Dentistry in squarely back into the spotlight The Board has addressed sleep Dentistry issues in a public hearing and all four Board meetings in 2013
bull There was discussion that there can be a shared relationship between the Dental and medical scopes of practice
bull Under the proposed rule a Dentist may treat benign snoring with an oral appliance after referral to a licensed physician where appropriate within the standard of care By contrast a Dentist may not diagnose treat or monitor OSA without collaboration with a licensed physician Additionally an oral appliance shall only be fabricated by a licensed Dentist or by a Dental lab under a prescription or work order prepared by a Dentist
American Dental Association
bull Treatment using an oral appliance designed specifically to treat OSA should be fabricated by a dentist familiar with device design maintenance and therapeutic efficacy and who has an association with and a referral from a sleep team
bull JADA Vol 136 p 1123
Donrsquot be afraid of OSA Get a grip on the facts and save patientrsquos lives
1112017
32
bullA SYMBIOTIC RELATION BETWEEN PHYSICIANS SLEEP PROFESSIONALS AND DENTISTS CAN SIGNIFICANTLY IMPROVE THE SLEEP HEALTH OF MILLIONS OF PEOPLE EACH AND EVERY YEAR
bull THAT RELATIONSHIP IS NOT A ONE WAY STREET AND THE
American Sleep amp Breathing Academy of over 8000 members UNDERSTANDS THAThellip JUST LOOK AT THE MULTITUDE OF SLEEP PROFESSIONAL CATAGORIES ON THEIR BOARD OF DIRECTORS
THE END
Thank you for your interest I hope this presentation was helpful
Dr Richard Klein
1112017
27
Cosmetic Surgery
bullHe couldnrsquot breath through his small nose became hypercapnic and helliphelliphellipdied
Effect of treating severe nasal obstruction on the severity of obstructive sleep apnoea
bull HA McLean AM Urton HS Driver AKW Tan AG Day+ PW Munt and MF Fitzpatrick
bullThis study demonstrates that relief of severe nasal obstruction in patients with a normal retroglossal airway is associated with a significant reduction in mouth breathing during sleep improved sleep architecture and a modest improvement in OSA severity
1112017
28
bullThere are several novel aspects to these findings First the study documents a clearly increased upper airway resistance in association with oral breathing during stable sleep as compared with nasal breathing irrespective of central or OSA
bullSecondly this methodology included simultaneous documentation of oral and nasal ventilation during sleep to confirm the absence of any nasal airflow in the oral breathing condition and vice versa
1112017
29
bullThe substantially higher resistive load posed by the oral breathing route provides a plausible explanation for the observation that inhaled ventilation occurs almost exclusively via the nasal route during sleep in subjects with normal nasal resistance
bull Many studies have shown that nasal obstruction can induce or increase apnea frequency in OSA patients When nasal resistance is high a greater pressure drop is required to achieve the same flow and hence collapse of the pharynx is facilitated and this could mitigate the effect of mandibular advancement
bull Moreover high nasal resistance is associated with mouth breathing which could potentially limit the beneficial effect of mandibular advancement
bull Dental Appliance Treatment for Obstructive
bull Andrew S L Chan Richard W W Lee and Peter A Cistulli
bull httpchestjournalchestpubsorgcontent1322693fullhtml
1112017
30
bullCurrent evidence suggests that despite the superior efficacy of CPAP both treatments produce similar subjective and objective health benefits
bullThe superior self-reported tolerance and compliance associated with MAD treatment is a likely explanation
bullThe practice parameters of the AASM recommend the use of oral appliances for mild-to-moderate OSA or for patients with severe OSA who are unable to tolerate CPAP or refuse treatment with CPAP with a required written prescription by a sleep physician
The following are Medicare rules
1) A diagnosis of OSA is not within the dental scope of practice A dentist providing an OA
must do so under the and with the team effort of a licensed Physician with a written
prescription
2) A physician is not skilled in the intricacies of fabricating fitting monitoring adjusting
and choosing an appropriate Oral Appliance individualized per patient
3) A dentist may not provide an oral appliance if the patient has an active
Temporomandibular Disorder
4) The OA must be fabricated within 90 days of the patientrsquos appointment with the sleep
physician
Since the rules are clear and they involve both of our professions it would behoove
both DOMD and DDS to communicate for the benefit of OSA patients
1112017
31
Subsequent to my 3 hour 2013 Meeting with the US Department of Transportation regarding Truckers
bull During the State Board of Dental Examiners meeting Board members put sleep Dentistry in squarely back into the spotlight The Board has addressed sleep Dentistry issues in a public hearing and all four Board meetings in 2013
bull There was discussion that there can be a shared relationship between the Dental and medical scopes of practice
bull Under the proposed rule a Dentist may treat benign snoring with an oral appliance after referral to a licensed physician where appropriate within the standard of care By contrast a Dentist may not diagnose treat or monitor OSA without collaboration with a licensed physician Additionally an oral appliance shall only be fabricated by a licensed Dentist or by a Dental lab under a prescription or work order prepared by a Dentist
American Dental Association
bull Treatment using an oral appliance designed specifically to treat OSA should be fabricated by a dentist familiar with device design maintenance and therapeutic efficacy and who has an association with and a referral from a sleep team
bull JADA Vol 136 p 1123
Donrsquot be afraid of OSA Get a grip on the facts and save patientrsquos lives
1112017
32
bullA SYMBIOTIC RELATION BETWEEN PHYSICIANS SLEEP PROFESSIONALS AND DENTISTS CAN SIGNIFICANTLY IMPROVE THE SLEEP HEALTH OF MILLIONS OF PEOPLE EACH AND EVERY YEAR
bull THAT RELATIONSHIP IS NOT A ONE WAY STREET AND THE
American Sleep amp Breathing Academy of over 8000 members UNDERSTANDS THAThellip JUST LOOK AT THE MULTITUDE OF SLEEP PROFESSIONAL CATAGORIES ON THEIR BOARD OF DIRECTORS
THE END
Thank you for your interest I hope this presentation was helpful
Dr Richard Klein
1112017
28
bullThere are several novel aspects to these findings First the study documents a clearly increased upper airway resistance in association with oral breathing during stable sleep as compared with nasal breathing irrespective of central or OSA
bullSecondly this methodology included simultaneous documentation of oral and nasal ventilation during sleep to confirm the absence of any nasal airflow in the oral breathing condition and vice versa
1112017
29
bullThe substantially higher resistive load posed by the oral breathing route provides a plausible explanation for the observation that inhaled ventilation occurs almost exclusively via the nasal route during sleep in subjects with normal nasal resistance
bull Many studies have shown that nasal obstruction can induce or increase apnea frequency in OSA patients When nasal resistance is high a greater pressure drop is required to achieve the same flow and hence collapse of the pharynx is facilitated and this could mitigate the effect of mandibular advancement
bull Moreover high nasal resistance is associated with mouth breathing which could potentially limit the beneficial effect of mandibular advancement
bull Dental Appliance Treatment for Obstructive
bull Andrew S L Chan Richard W W Lee and Peter A Cistulli
bull httpchestjournalchestpubsorgcontent1322693fullhtml
1112017
30
bullCurrent evidence suggests that despite the superior efficacy of CPAP both treatments produce similar subjective and objective health benefits
bullThe superior self-reported tolerance and compliance associated with MAD treatment is a likely explanation
bullThe practice parameters of the AASM recommend the use of oral appliances for mild-to-moderate OSA or for patients with severe OSA who are unable to tolerate CPAP or refuse treatment with CPAP with a required written prescription by a sleep physician
The following are Medicare rules
1) A diagnosis of OSA is not within the dental scope of practice A dentist providing an OA
must do so under the and with the team effort of a licensed Physician with a written
prescription
2) A physician is not skilled in the intricacies of fabricating fitting monitoring adjusting
and choosing an appropriate Oral Appliance individualized per patient
3) A dentist may not provide an oral appliance if the patient has an active
Temporomandibular Disorder
4) The OA must be fabricated within 90 days of the patientrsquos appointment with the sleep
physician
Since the rules are clear and they involve both of our professions it would behoove
both DOMD and DDS to communicate for the benefit of OSA patients
1112017
31
Subsequent to my 3 hour 2013 Meeting with the US Department of Transportation regarding Truckers
bull During the State Board of Dental Examiners meeting Board members put sleep Dentistry in squarely back into the spotlight The Board has addressed sleep Dentistry issues in a public hearing and all four Board meetings in 2013
bull There was discussion that there can be a shared relationship between the Dental and medical scopes of practice
bull Under the proposed rule a Dentist may treat benign snoring with an oral appliance after referral to a licensed physician where appropriate within the standard of care By contrast a Dentist may not diagnose treat or monitor OSA without collaboration with a licensed physician Additionally an oral appliance shall only be fabricated by a licensed Dentist or by a Dental lab under a prescription or work order prepared by a Dentist
American Dental Association
bull Treatment using an oral appliance designed specifically to treat OSA should be fabricated by a dentist familiar with device design maintenance and therapeutic efficacy and who has an association with and a referral from a sleep team
bull JADA Vol 136 p 1123
Donrsquot be afraid of OSA Get a grip on the facts and save patientrsquos lives
1112017
32
bullA SYMBIOTIC RELATION BETWEEN PHYSICIANS SLEEP PROFESSIONALS AND DENTISTS CAN SIGNIFICANTLY IMPROVE THE SLEEP HEALTH OF MILLIONS OF PEOPLE EACH AND EVERY YEAR
bull THAT RELATIONSHIP IS NOT A ONE WAY STREET AND THE
American Sleep amp Breathing Academy of over 8000 members UNDERSTANDS THAThellip JUST LOOK AT THE MULTITUDE OF SLEEP PROFESSIONAL CATAGORIES ON THEIR BOARD OF DIRECTORS
THE END
Thank you for your interest I hope this presentation was helpful
Dr Richard Klein
1112017
29
bullThe substantially higher resistive load posed by the oral breathing route provides a plausible explanation for the observation that inhaled ventilation occurs almost exclusively via the nasal route during sleep in subjects with normal nasal resistance
bull Many studies have shown that nasal obstruction can induce or increase apnea frequency in OSA patients When nasal resistance is high a greater pressure drop is required to achieve the same flow and hence collapse of the pharynx is facilitated and this could mitigate the effect of mandibular advancement
bull Moreover high nasal resistance is associated with mouth breathing which could potentially limit the beneficial effect of mandibular advancement
bull Dental Appliance Treatment for Obstructive
bull Andrew S L Chan Richard W W Lee and Peter A Cistulli
bull httpchestjournalchestpubsorgcontent1322693fullhtml
1112017
30
bullCurrent evidence suggests that despite the superior efficacy of CPAP both treatments produce similar subjective and objective health benefits
bullThe superior self-reported tolerance and compliance associated with MAD treatment is a likely explanation
bullThe practice parameters of the AASM recommend the use of oral appliances for mild-to-moderate OSA or for patients with severe OSA who are unable to tolerate CPAP or refuse treatment with CPAP with a required written prescription by a sleep physician
The following are Medicare rules
1) A diagnosis of OSA is not within the dental scope of practice A dentist providing an OA
must do so under the and with the team effort of a licensed Physician with a written
prescription
2) A physician is not skilled in the intricacies of fabricating fitting monitoring adjusting
and choosing an appropriate Oral Appliance individualized per patient
3) A dentist may not provide an oral appliance if the patient has an active
Temporomandibular Disorder
4) The OA must be fabricated within 90 days of the patientrsquos appointment with the sleep
physician
Since the rules are clear and they involve both of our professions it would behoove
both DOMD and DDS to communicate for the benefit of OSA patients
1112017
31
Subsequent to my 3 hour 2013 Meeting with the US Department of Transportation regarding Truckers
bull During the State Board of Dental Examiners meeting Board members put sleep Dentistry in squarely back into the spotlight The Board has addressed sleep Dentistry issues in a public hearing and all four Board meetings in 2013
bull There was discussion that there can be a shared relationship between the Dental and medical scopes of practice
bull Under the proposed rule a Dentist may treat benign snoring with an oral appliance after referral to a licensed physician where appropriate within the standard of care By contrast a Dentist may not diagnose treat or monitor OSA without collaboration with a licensed physician Additionally an oral appliance shall only be fabricated by a licensed Dentist or by a Dental lab under a prescription or work order prepared by a Dentist
American Dental Association
bull Treatment using an oral appliance designed specifically to treat OSA should be fabricated by a dentist familiar with device design maintenance and therapeutic efficacy and who has an association with and a referral from a sleep team
bull JADA Vol 136 p 1123
Donrsquot be afraid of OSA Get a grip on the facts and save patientrsquos lives
1112017
32
bullA SYMBIOTIC RELATION BETWEEN PHYSICIANS SLEEP PROFESSIONALS AND DENTISTS CAN SIGNIFICANTLY IMPROVE THE SLEEP HEALTH OF MILLIONS OF PEOPLE EACH AND EVERY YEAR
bull THAT RELATIONSHIP IS NOT A ONE WAY STREET AND THE
American Sleep amp Breathing Academy of over 8000 members UNDERSTANDS THAThellip JUST LOOK AT THE MULTITUDE OF SLEEP PROFESSIONAL CATAGORIES ON THEIR BOARD OF DIRECTORS
THE END
Thank you for your interest I hope this presentation was helpful
Dr Richard Klein
1112017
30
bullCurrent evidence suggests that despite the superior efficacy of CPAP both treatments produce similar subjective and objective health benefits
bullThe superior self-reported tolerance and compliance associated with MAD treatment is a likely explanation
bullThe practice parameters of the AASM recommend the use of oral appliances for mild-to-moderate OSA or for patients with severe OSA who are unable to tolerate CPAP or refuse treatment with CPAP with a required written prescription by a sleep physician
The following are Medicare rules
1) A diagnosis of OSA is not within the dental scope of practice A dentist providing an OA
must do so under the and with the team effort of a licensed Physician with a written
prescription
2) A physician is not skilled in the intricacies of fabricating fitting monitoring adjusting
and choosing an appropriate Oral Appliance individualized per patient
3) A dentist may not provide an oral appliance if the patient has an active
Temporomandibular Disorder
4) The OA must be fabricated within 90 days of the patientrsquos appointment with the sleep
physician
Since the rules are clear and they involve both of our professions it would behoove
both DOMD and DDS to communicate for the benefit of OSA patients
1112017
31
Subsequent to my 3 hour 2013 Meeting with the US Department of Transportation regarding Truckers
bull During the State Board of Dental Examiners meeting Board members put sleep Dentistry in squarely back into the spotlight The Board has addressed sleep Dentistry issues in a public hearing and all four Board meetings in 2013
bull There was discussion that there can be a shared relationship between the Dental and medical scopes of practice
bull Under the proposed rule a Dentist may treat benign snoring with an oral appliance after referral to a licensed physician where appropriate within the standard of care By contrast a Dentist may not diagnose treat or monitor OSA without collaboration with a licensed physician Additionally an oral appliance shall only be fabricated by a licensed Dentist or by a Dental lab under a prescription or work order prepared by a Dentist
American Dental Association
bull Treatment using an oral appliance designed specifically to treat OSA should be fabricated by a dentist familiar with device design maintenance and therapeutic efficacy and who has an association with and a referral from a sleep team
bull JADA Vol 136 p 1123
Donrsquot be afraid of OSA Get a grip on the facts and save patientrsquos lives
1112017
32
bullA SYMBIOTIC RELATION BETWEEN PHYSICIANS SLEEP PROFESSIONALS AND DENTISTS CAN SIGNIFICANTLY IMPROVE THE SLEEP HEALTH OF MILLIONS OF PEOPLE EACH AND EVERY YEAR
bull THAT RELATIONSHIP IS NOT A ONE WAY STREET AND THE
American Sleep amp Breathing Academy of over 8000 members UNDERSTANDS THAThellip JUST LOOK AT THE MULTITUDE OF SLEEP PROFESSIONAL CATAGORIES ON THEIR BOARD OF DIRECTORS
THE END
Thank you for your interest I hope this presentation was helpful
Dr Richard Klein
1112017
31
Subsequent to my 3 hour 2013 Meeting with the US Department of Transportation regarding Truckers
bull During the State Board of Dental Examiners meeting Board members put sleep Dentistry in squarely back into the spotlight The Board has addressed sleep Dentistry issues in a public hearing and all four Board meetings in 2013
bull There was discussion that there can be a shared relationship between the Dental and medical scopes of practice
bull Under the proposed rule a Dentist may treat benign snoring with an oral appliance after referral to a licensed physician where appropriate within the standard of care By contrast a Dentist may not diagnose treat or monitor OSA without collaboration with a licensed physician Additionally an oral appliance shall only be fabricated by a licensed Dentist or by a Dental lab under a prescription or work order prepared by a Dentist
American Dental Association
bull Treatment using an oral appliance designed specifically to treat OSA should be fabricated by a dentist familiar with device design maintenance and therapeutic efficacy and who has an association with and a referral from a sleep team
bull JADA Vol 136 p 1123
Donrsquot be afraid of OSA Get a grip on the facts and save patientrsquos lives
1112017
32
bullA SYMBIOTIC RELATION BETWEEN PHYSICIANS SLEEP PROFESSIONALS AND DENTISTS CAN SIGNIFICANTLY IMPROVE THE SLEEP HEALTH OF MILLIONS OF PEOPLE EACH AND EVERY YEAR
bull THAT RELATIONSHIP IS NOT A ONE WAY STREET AND THE
American Sleep amp Breathing Academy of over 8000 members UNDERSTANDS THAThellip JUST LOOK AT THE MULTITUDE OF SLEEP PROFESSIONAL CATAGORIES ON THEIR BOARD OF DIRECTORS
THE END
Thank you for your interest I hope this presentation was helpful
Dr Richard Klein
1112017
32
bullA SYMBIOTIC RELATION BETWEEN PHYSICIANS SLEEP PROFESSIONALS AND DENTISTS CAN SIGNIFICANTLY IMPROVE THE SLEEP HEALTH OF MILLIONS OF PEOPLE EACH AND EVERY YEAR
bull THAT RELATIONSHIP IS NOT A ONE WAY STREET AND THE
American Sleep amp Breathing Academy of over 8000 members UNDERSTANDS THAThellip JUST LOOK AT THE MULTITUDE OF SLEEP PROFESSIONAL CATAGORIES ON THEIR BOARD OF DIRECTORS
THE END
Thank you for your interest I hope this presentation was helpful
Dr Richard Klein