Embed Size (px)
Citation preview

AnUpdateontheEvolvingMDHHSStrategyforCombattingtheOpioid
MortalityCrisis
MICHIGANDEPARTMENTOFHEALTH&HUMANSERVICES
P u t t i n g p e o p l e f i r s t , w i t h t h e g o a l o f h e l p i n g a l l M i c h i g a n d e r s l e a d h e a l t h i e r a n d m o r e p r o d u c t i v e l i v e s , n o m a t t e r t h e i r s t a g e i n l i f e . 1
DavidR.Neff,DOChiefMedicalDirectorOfficeofMedicalAffairs
MedicalServicesAdministrationMichiganDepartmentofHealth&HumanServices
AssistantClinicalProfessorDepartmentofFamily&CommunityMedicine
MichiganStateUniversityCollegeofOsteopathicMedicine

Objectives1. DescribethechanginglandscapeoftheOpioidMortalityCrisisin
2017
2. ProvideanOverviewoftheEvolvingMDHHSStrategytoCombattheCrisis
3. WhatYou,theProvider,CanDoToMinimizeRiskforOpioidUseDisorder,OverdoseandDeath
2

3
TheRapidlyChangingLandscapeoftheOpioidMortalityCrisisin
2017

Six Days of Drug Overdose: Cincinnati
ü In a six day period (August 19-24, 2016) Cincinnati area experienced 174 opioid overdose reactions.
ü The culprit responsible was heroin cut with a fentanyl analogue: Carfentanyl.
ü Carfentanyl is 10,000 times as potent as morphine.ü Carfentanyl is used to tranquilize elephants.
https://www.washingtonpost.com/news/morning-mix/wp/2016/08/29/this-is-unprecedented-174-heroin-overdoses-in-6-days-in-cincinnati/?utm_term=.c8e4154fc9e6

Carfentanyl Deaths in Michigan
ü September15,2016-Firstdocumentedcarfentanyloverdose seen in Kent County
ü October 6, 201619 confirmed carfentanyl overdose deaths in Wayne County since July
http://www.michigan.gov/mdhhs/0,5885,7-339--393468--,00.htmlhttp://www.michigan.gov/mdhhs/0,5885,7-339--395078--,00.html

U-47700 Death in Michigan
ü October5,2016- FirstdocumentedU47700 (aka, pink) overdose seen in White Lake, MI
ü ThethenlegaldrugwaspurchasedovertheinternetandshippedfromChina
ü ItwasdesignatedasaScheduleIrestricteddruginNovember,2016
http://www.cnn.com/2016/11/01/health/u-47700-pink-drug/index.html

Grey Death in GA, FL, OH and WV
ü May4,2017- GrayDeathisacombinationofseveralpowerfulsubstancessuchasHeroin,Fentanyl, Carfentanil andasyntheticopioidcalledU-47700
ü Thedrughastheappearanceofaconcreterock.Itischunkyandsolid,createdfromcompressedandcookedpowder
ü Atleast50peoplehavereportedlyoverdosed,somedyingaftertheirfirstdoseofthedrug
http://www.cbsnews.com/news/gray-death-opioid-dangerous-drug-combination/

https://www.nytimes.com/interactive/2017/09/02/upshot/fentanyl-drug-overdose-deaths.html?_r=0AdaptedfromCDC•NationalCenterforHealthStatistics•NationalVitalStatisticsSystemasof8/16/17
TotalUSDrugDeaths2000-2016Onaverage142peopledieeachday

DrugOverdoseDeathsintheUS2000-2016Fentanyl,FentanylAnaloguesandHeroinareOutpacingPrecipitationOpioidDeaths
https://www.nytimes.com/interactive/2017/09/02/upshot/fentanyl-drug-overdose-deaths.html?_r=0AdaptedfromCDC•NationalCenterforHealthStatistics•NationalVitalStatisticsSystemasof8/16/17

AmongOpioids,RatesofDrugOverdoseDeathsAmongAdolescentsAged15–19in2015WereHighestforHeroin
NCHSDataBrief■ No.282■ August2017

11

12

Total Drug Poisoning Deaths in MI, 1999-2016*
Source: Michigan Death Certificates, Division for Vital Records and Health Statistics/MDHHS*2016 is provisional, total is expected to change.
13

DataSummary
*Provisionaldata
*ProvisionalData
**2015Data
Indicator 2011 2016Alldrugdeaths 1,359 2,335*Allopioiddeaths 622 1,689*Opioidprescriptions 10,441,714 11,028,495Neonatal abstinencesyndrome cases
630 927**
People insubstanceusedisordertreatmentforopioidsorheroin
22,234 32,473
14

EstimatedPopulationUsingPrescriptionOpioidsinMichiganin2016
Prescriptions Medicaid(Actual)
CommercialandNo-Insurance(Estimated)
Total(Estimated)
30 Days 402,154 1,206,462 1,608,616
90Days 115,841 347,523 463,364
365Days 21,847 65,541 87,388
1/3 of the Population Has Some Form of Pain1/6 of the Population Took an Opioid

WhenthePrescriptionIstheProblem
*
*In2010,theratewas4xhigherthan1999

MMEs prescribed per capita (2015) Change in MMEs prescribed per capita (2010–2015)
ChangesinOpioidPrescribingintheMichigan,2010-15(ExcerptedFromaNationalReportfromtheCDC)

DataFromDrugUsersRespondingtotheDEANDTASurvey– 2/3ofPrescriptionOpioidsWereObtainedForFree,BoughtorStolen
2017NationalDrugThreatAssessment
• MuchofThisUseStartedforRecreationalandNotMedicinalPurposes• OncePrescribed,DistributionisLargelyOutofPrescribers’Hands

DataFromDrugUsersRespondingtotheDEANDTASurvey– 2/3ofPrescriptionOpioidsWereObtainedForFree,BoughtorStolen
2017NationalDrugThreatAssessment
• MuchofThisUseStartedforRecreationalandNotMedicinalPurposes• OncePrescribed,DistributionisLargelyOutofPrescribers’Hands

WhenHeroinistheProblemTheNationalHeroinThreatistheGreatestintheNortheastCorridorandtheMidwest

In2015-16– HeroinBecametheGreatestNationalThreatAstheControlledPrescriptionDrug(CPD)ThreatDiminished
Heroin
CPD’s

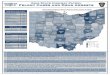
WhenFentanylAnaloguesAretheProblem— OverdoseDeathsinOhio,January–February2017
TheCauseForManyOverdoseDeathsCannotBeDeterminedWhenSyntheticOpioidsAreNotMeasured

23
AnOverviewoftheEvolvingMDHHSStrategytoCombatthe
CrisisDavidR.Neff,DO
ChiefMedicalDirectorOfficeofMedicalAffairs
MedicalServicesAdministrationMDHHS
DebraA.Pinals,M.D.ChiefPsychiatrist
MedicalDirectorof BehavioralHealthandForensicPrograms
BehavioralHealthandDevelopmentalDisabilitiesAdministration(BHDDA)
MDHHS
EdenV.Wells,MD,MPH,FACPMChiefMedicalExecutive
MichiganDepartmentofHealthandHumanServices
MedicalDirector,PopulationHealth

Reduce Supply and Demand
Early Intervention
Increase treatment services
Increase emergency services
1°
2°
3°
Prevention
Early Intervention
Treatment
Improve IT Analytics & Surveillance
Promote awareness
Identify Risk of Addiction & Overdose
Use Screening Tools (ie, SBIRT, DAST-10)
Rescue w/Naloxone
Stabilize w/MAT
Recover w/ CBT & DBT
Community ProgramsSchools
Slow Taper
Reduce Opioid Pill Counts
Informed Consent &Treatment Contracts
MAPS Narcs Care Narcs Rx MIHIN CC360
Parenting Skills
Mentoring Skills
Reduce Illicit Rx & Heroin Trafficking
Take-back Programs
Coping Skills
Identify Underlying Conditions & Comorbidities
Treat Pain w/Fewer Opioids
Multimedia Campaigns
MDHHSPublicHealthStrategicFrameworktotheOpioidCrisis

TheEvolvingStrategyisDesignedtoEmbraceAllStakeholderGroupstoHelpIndividualsandtheEntirePopulation
IndividualHealth
PopulationHealth
MDHHS LAARLARADepartment
ofEducation
PayersHealthPlans&Hospitals
LawEnforcement
&Courts
Communities(PTA’s,HeadStart,FaithBased
Programs)

APersonCenteredCommunity-basedActionPlanRequiresAllStakeholders
Payers
PersonSufferingAddiction
MDHHS

FundingSources•Medicaid
•HealthyMichigan
•SubstanceAbuseandMentalHealthServicesAdministration(SAMHSA)BlockGrant
•GeneralFund•OthergrantsoStateTargetedResponse(STR)oCentersforDiseaseControl(CDC)o1115Waiver(Pending)
27

ServicesFundedbyMedicaidServicesfundedinclude:
•MedicationAssistedTreatment
•Detoxification•OutpatientServices•CaseManagement
28

Medicaid&HealthyMichigan•Medicaidpaidover$41millioninsubstanceusedisorderservicesprovidingservicesto31,101beneficiariesinfiscalyear2016
•HealthyMichiganpaidover$53millioninsubstanceusedisorderservicesprovidingservicesto28,850beneficiariesinfiscalyear2016
29

michigan.gov/stopoverdoses
30

31
Latest Improvement Starting 11/1 - Sample Risk Score for the Electronic Health Record

PreservingandExpandingOurProviderWorkforceByCreatinga
LearningHealthSystemApproachtoImproveProviderExpertise

CreatingaLearningHealthSystemApproachtoImproveProviderExpertise
• Providersarecoretohelpingaddressthecrisis• thereisvariabilityinexpertiseandnumberswhoareableandwillingtoparticipate
• Theproviderworkforceisverywillingtoimprovepracticepatternsbasedonevidence-basedrecommendations,butneedsassistance
• Thereisahighneedtorapidlyreorientproviderstoresponsiblymanageopioids• whenandhowtostartandstopopioids• howtoidentifyriskforaddictivebehaviors• howtoidentifyriskforoverdose• howtobestassistpatientswhentheseriskbehaviorsoccur
• Thecoreprincipleistoembracea“learninghealthsystem”approachutilizingrealworlddatasourcestoapply“teachablemoments”
• ThisconceptisadaptedfromthetransformationalworkandresearchofPeterSengeandhiscolleagues.[1]
• alearningorganization facilitatestheongoinglearningofitsmembersandcontinuouslytransformsitself
[1]Senge,P.M.(1990).Theartandpracticeofthelearningorganization.Thenewparadigminbusiness:Emergingstrategiesforleadershipandorganizationalchange,126-138.

TakingaCollaborativeApproachinEmbracingALearningHealthSystem• ProfessionalSocieties
• MOA• MSMS• MISAM• MPS• MAFP• MDA• MAPA• MCNP• MHA
• Payers• MAHP• BlueCrossBlueShieldofMI• OtherCommercial
• ProfessionalDegreePrograms
• MD(Underway)• DO(Underway)• PA(Planned)• NP(Planned)• DDS(Planned)• DPM(Planned)• DVM(Planned)• PharmD(Planned)

PROVIDERCOLLABORATION- JOINT10-POINTPLANTOCOMBATTHEOPOIDMORTALITYCRISIS
1. DevelopanddisseminateaclearlydefinedandactionableoverarchingstatespecificguidelinethroughtheMichiganQualityImprovementConsortium(MQIC)thatincorporatesthe2016CDCPainGuidelines,theASAMAddictionGuidelines,otherevidencebasedbestpracticesand utilizationofkeydatasourcesthathelpdriveclinicaldecisionmakingsuchasMAPSandthesoontobereleasedNarxCare riskscoringtoolsthatcanbeembeddedintheindividualelectronicmedicalrecord.
2. DevelopandteachtoaUniformCoreEvidence-basedOpioidCurriculumthroughprofessionalschools,professionalsocieties,hospitalsandhealthplansa. Whenandhowtosparinglyinitiateopioidsincludinglimitingquantitiesforacutepainmanagementb. Whenandhowtodeterminewhetherornotanopioidshouldbecontinuedc. Whenandhowtotaperandtaperopioidsasrapidlyaspossibled. Howtomonitorforopioidtolerance,dependenceandaddictionandeithertreatorreferearlyifindicatede. Howtoappropriatelydocumentinthemedicalrecordtherationaleandtreatmentcourseofusingopioids
3. DevelopReferralCentersofExcellence&TelemedicineConsultationCallCenterstoassistprovidersmanagecomplexpainandaddictioncases
4. LeverageMAPSandNarxCare RiskIndexScorestodrivepointofcaredecisions
5. DevelopaPeerReviewProcesstoassistproviderswhoareoutliersinprescribingbehavior
6. Developopioid-relatedqualitymetricsthatrewardprovidersfordeliveringhighqualitystandardofcare
7. SupportManagedCareandPharmacySpecificProgramstocontrolhighdosesandquantitiesofprescriptionopioidsandrequirejustificationiftheyarerequireda. PharmacyPriorAuthorizationprocessb. DrugUtilizationReviewc. MedicationTherapyManagement(MTM)bypharmacistsatthePointofSale(POS)d. BeneficiaryMonitoringProgram(BMP)lock-innprograms
8. Supportcommunitybasededucationprogramstopreventinappropriatedruguseinthefirstplaceandeliminateculturalmoresthatpromoteatypicaldrugbehavior
9. Workcloselywithlawenforcementtoeliminateillicitdrugsfromourcommunities,fullynotingthatillicitlytraffickedheroin andfentanylanaloguesarenowoutpacingprescriptionopioidrelateddeathsin2015-2017
10. Supporteffortstoimprovesurveillanceanddetectionofopioidrelateddeathsincludingimprovedtoxicologyscreeningforpreviouslyundetectablefentanylanalogues

36
WhatYou,theProvider,CanDoToMinimizeRiskforOpioidUseDisorder,OverdoseandDeath

OtherNon-opioidPainManagementStrategiesIncludingCross-functionalTeamApproaches1. Osteopathicand
ChiropracticManualMedicine
2. EpiduralandFacetBlocks(forspinalpain)
3. RadiofrequencyAblation4. ComplexRegionalPain
SyndromeTechniques5. MeditationandYoga
Techniques

WhatElseCanYouDotoPreventAddiction,OverdoseandDeath– StartingOnMonday1. StayabreastwiththeconstantlyevolvingfactsthatuncovertherootcausestheOpioidEpidemic
2. RememberOpioidToleranceStartsSomewhereBetween3-7days
3. Don’tAbandonPatientswithLife-alteringPainorForcePatientsTakingLongTermOpioidstotheStreet
4. TakeaTeam-basedapproachandDon’tGoitAlone– Surgery,RehabilitationMedicince,PainManagement,AddictionManagement,BehavioralHealth
5. StartConversationsattheFirstDayofPrescribingOpioidsandContinueThemwithPatientsToDiscussThatOpioidsNeedtoBeStoppedAsSoonAsPossible
6. MonitorandScreenforTolerance,Dependence,AddictionandRiskforOverdoseandDeath
7. LearnHowtoAppropriatelyTaperExistingOpioidsandDetermineIfAnUnderlyingOpioidUseDisorder(OUD)Exists
8. UtilizePatientContractsThatIncludeMeaningfulInformedConsent
9. UseMAPSFrequentlyToDetectPatternsofMisuseorAbuseandEnsureBothCoordination&ContinuityofCarewithOtherProviders
10. UseUrineDrugScreenstoCheckforComplianceandPotentialIllicitDrugUse
11. TreatorReferEarly
12. Writefornaloxonetopatientswhoareathighriskforoverdose
13. ObtainaxDEA waivertohelpstabilizepatientswithOpioidUseDisorder(RegardlessoftheReason)
14. GetInvolvedwithYourCommunitytoStopCulturalExpectationsThatEncourageIllicitDrugUse
15. WorkThroughYourProfessionalSocietiesandPersonallyTalktoYourLegislatorsandRegulatorstoShareYourExperiencesandWhatTheyCanDotoHelpYou

Summary• Therootcausesfortheopioidepidemicarecomplexandmultifactorial
• Itisimperativetoshrinksupplyanddemandforbothprescriptionopioidsandheroin/fentanylanalogues
• Awellorganizedstate-wideplanisnecessarytoavoidabandoningpatientswith“true”painandalsonotsendpeopletothestreetforheroinandsyntheticopioids
• Focusingonlyonprescriptionopioidswithoutsimultaneouslyaddressing“heroinandfentanyltrafficking”willdramaticallyshrinkprobabilityofsuccess
• Mostofallitwill“takeavillage”– “everyvillage”hereinMichigan