Embed Size (px)
Citation preview
Michigan Purchasers Health Alliance September 20,2007
Readiness to Change Survey:Employers’ readiness to adopt value-based benefit strategies
Larry S. BoressPresident & CEO
Midwest Business Group on Health
Copyright MBGH 20072
Midwest Business Group on Health
MBGH is a Chicago-based, non-profit coalition of Midwest employers working together to improve the quality and cost-effectiveness of health care for purchasers and the health status of their constituents.
Founded in 1980, membership includes over 80 large, self-funded, public and private employers such as Abbott Laboratories, Boeing, City of Chicago, Kraft, Target, State of Illinois and University of Chicago. Member organizations cover over 2 million lives and spend over $2.5 billion on health care.
Employers are represented by those responsible for designing and managing health benefits: VP of HR, Director/Manager of Benefits, Medical Director, Wellness Coordinator
MBGH is one of over 60 coalitions in U.S. A member of the National Business Coalition on Health
Copyright MBGH 20073
MBGH Activities Buying Groups for Audits, Chicago HMOs, Disease Management, Incentive
Programs; Worksite & Health Management Programs, and Pharmacy Benefits Health Benefit Strategy Pilots & Quality Initiatives
“HPQ-Select” – Employer tool to identify how employees’ health impacts their productivity
“Taking Control of Your Health” – an “Asheville Model” Diabetes Ten City Challenge pilot to determine if waived drug co-pays linked to pharmacist diabetic counselors increases diabetic patient compliance with treatments
“Readiness to Change “ survey to determine employers readiness to adopt value-based benefit strategies
Learning Network Programs on health benefit management, strategies and trends Networking & benchmarking health benefit roundtables Roundtables on pharmacy management, union benefits, wellness programs
and CDHPs Medicare Employer Forum calls Health Plan & Health System User Groups
The Deterioration of the House of Benefits

Copyright MBGH 20075
Employers believe it’s time for an extreme makeover to their House of Benefits
Copyright MBGH 20076
Our house and neighborhood have been deteriorating
• Care processes are fragmented and confusing to patients;• Access to care difficult for many; • More are concerned about losing their health insurance than
losing jobs or terrorist attacks;• Uncertain value of new drugs and technologies; • Low morale within provider community; • Employees don’t recognize the real cost of health services;• Few patients take responsibility for own health;• Increasing talk of single payer system; and• Serious and systemic quality problems exist
Copyright MBGH 20077
What happened?
“The HMO – managed care strategy worked as long as new structures and incentives were at play. They were not sustained for the most part due to employers and government failing to compel HMOs to be accountable for their impact on patients’ health outcomes.
There was a lack of a public oversight mechanism for the health system’s performance. Another factor was the inclusion of non-coordinated IPAs and discount-only PPO networks that weren’t designed or committed to manage care, only to manage cost.”
- Paul Ellwood
“As major purchasers of health care services, employers have the clout to insist on change. Unfortunately, they have also been part of the problem. In buying health care services, companies have forgotten some basiclessons about how competition works and how to buy intelligently.”
- Michael E. Porter
Copyright MBGH 20078
How purchasers contributed to the problems
Strategy missteps We were reluctant to direct employees to better performing plans, giving
them the same contributions for any plan they selected We created an attitude of entitlement, rather than engagement We carved out services to obtain customized programs, better information
and services, resulting in greater fragmentation and confusion in the health system, the loss of integrated data and poor coordination of vendor services
We treated wellness as a fringe benefit, not an integral part of human capital management
We expected employees would broadly participate in health promotion and disease management programs just because we offered them
We treated health benefits as an expense, not an investment
Copyright MBGH 20079
We need an extreme makeover of our House of Benefits
The new foundation is built on integration of data and maintenance of health
The support beams: Engagement and incentives Self-management of health and chronic conditions Health management and wellness Health and quality information Transparency of physician, hospital, drug and procedure
effectiveness and cost Consumerism
Copyright MBGH 200710
A renovated House of Benefits must address a business problem
The business problem: Human capital costs Direct health costs = 1/3 of total costs Indirect costs = 2/3 of total costs
Productivity Absenteeism Presenteeism
Safety Critical incidences Poor decision-making

TechnologyWork PracticesManagement Practices - Quality Improvement - Training
Health Status
The Ceiling of Opportunity (Human Factors)
The Ceiling of Opportunity (Human Factors)
Health Status
Copyright MBGH 200712
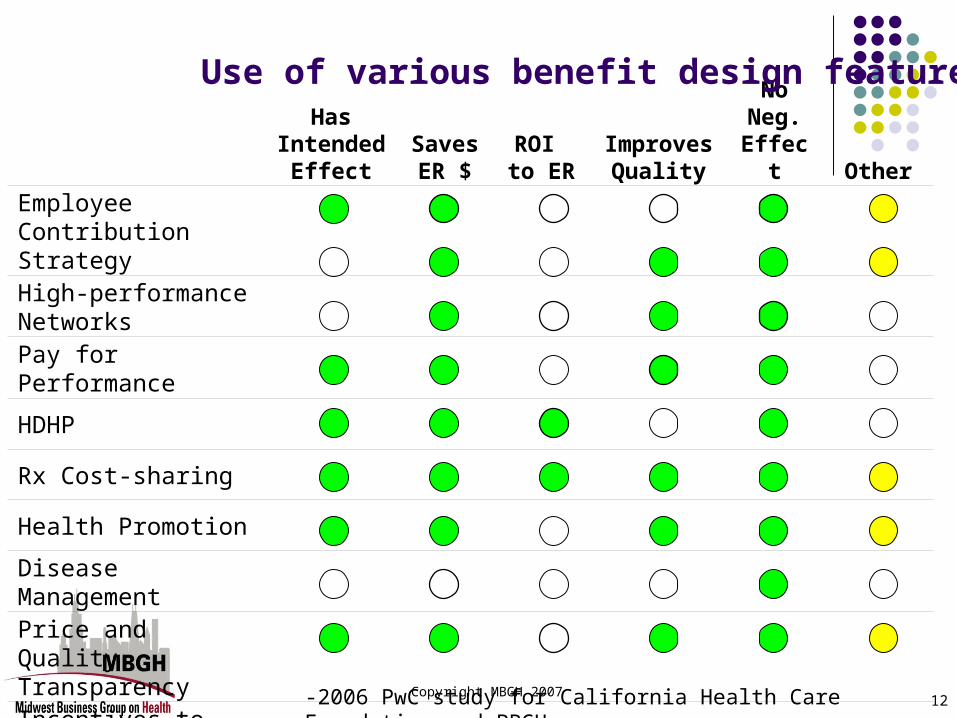
Has Intended
EffectSaves ER $
ROI to ER
Improves Quality
No Neg.
Effect Other
Employee Contribution StrategyHigh-performance Networks
Pay for Performance
HDHP
Rx Cost-sharing
Health Promotion
Disease Management
Price and Quality TransparencyIncentives to Activate Consumers
Use of various benefit design features
-2006 PwC study for California Health Care Foundation and PBGH
MBGH Readiness to Change Survey
Copyright MBGH 200714
Objectives of Survey Determine employer familiarity, understanding, use of and
readiness to adopt various “value-based benefit design” (VBBD) strategies: Incentives for employees Pay-for-Performance programs Consumer engagement strategies Removing barriers to improve compliance with treatment
Determine employers use and understanding of: The data required to see the total costs of health Health’s impact on productivity Adherence, compliance, quality and wellness programs
Determine the key elements required for organizations to adopt new benefit strategies
Identify what strategies or elements contribute to lower cost trends
Copyright MBGH 200715
Methodology
Review of previous surveys and literature on VBBD to determine what strategies and experiences currently are being promoted or utilized
Survey questions reviewed by Project Advisory Council composed of leading employers, coalitions, researchers, health plans and consultants
Survey and reminder disseminated via email by fourteen business coalitions to over 400 employers in various parts of country
Results received from 163 employers Analysis conducted by MBGH staff Funding and research support provided by GlaxoSmithKline
Copyright MBGH 200716
Components of Survey
Demographics of employer Cost trends from 2003-2005 Positions on various benefit philosophies Data activities Perspectives and experience with value-based
benefit strategies Perspectives on availability of quality information Sources and influencers of benefit strategy
information
Demographics of Respondents
Copyright MBGH 200718
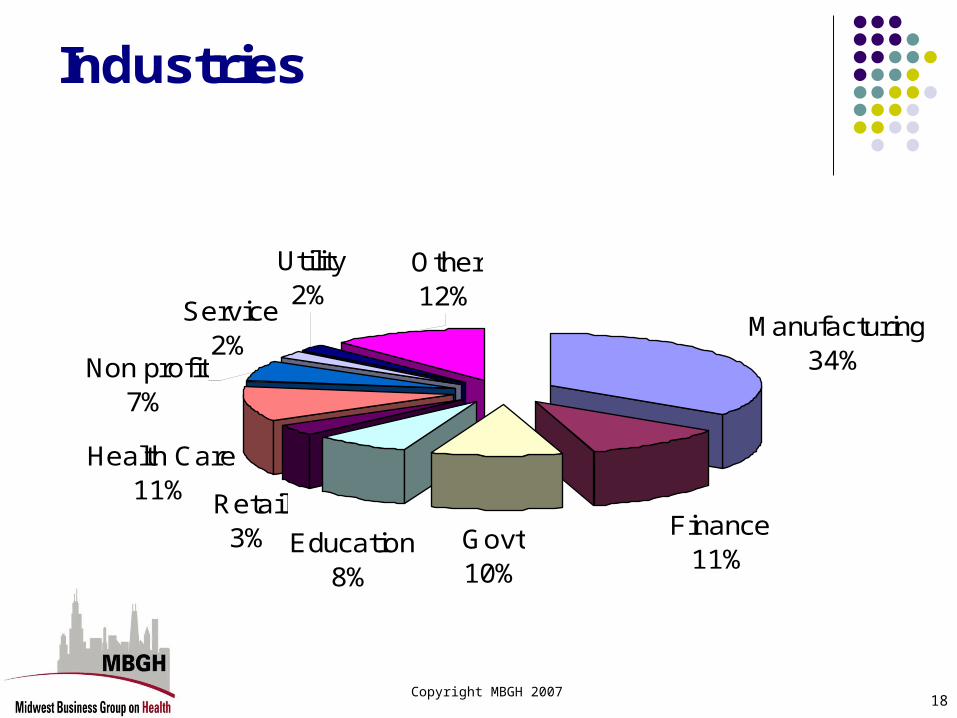
Industries
Manufacturing34%
Finance11%
Govt10%
Retail3%
Health Care11%
Service2%
Non profit7%
Education8%
Utility2%
Other12%
Copyright MBGH 200719
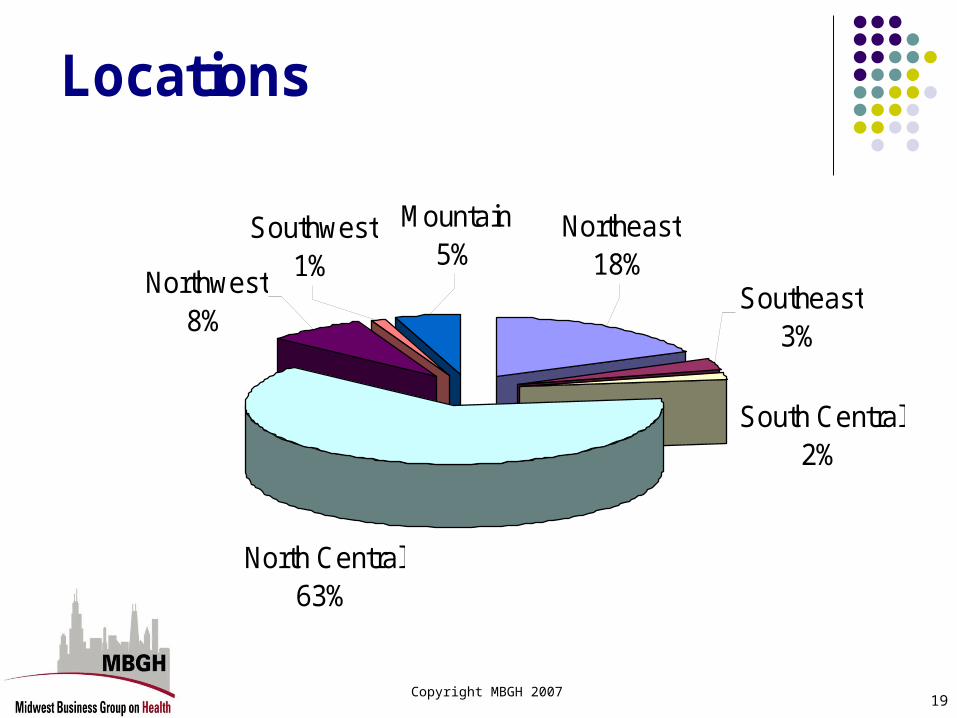
Locations
North Central63%
Northwest8%
Southwest1%
Southeast3%
Northeast18%
Mountain5%
South Central2%

Copyright MBGH 200720
Size of Employer
<50032%
501-10009%1001-5000
21%
>10,00017%
5001 - 10,00021%
Copyright MBGH 200721
If you’ve seen one employer…
“Leading Edge” – 21% of respondents Employers willing to try new benefit strategies based on
their perceived, yet untested, value
“Careful Watchers” – 54% of respondents Employers willing to try a new benefit strategy once
competitors adopt it or preliminary evidence of ROI exists
“Conservative” – 25% of respondents Employers willing to try a new benefit strategy once it is
viewed as an industry standard benefit design.
Copyright MBGH 200722
Characteristics of self-identified “Leading Edge” firms
The organization is highly supportive of improving employee health Senior leadership is highly influential in designing health benefits They see a link between an employee's health and his/her
productivity In addition to company data, they look to experiences of other
“leading edge” firms and academic research to determine their benefit directions
Health benefits are seen a necessary cost of doing business and an investment in human capital, with a measurable outcome
Copyright MBGH 200723
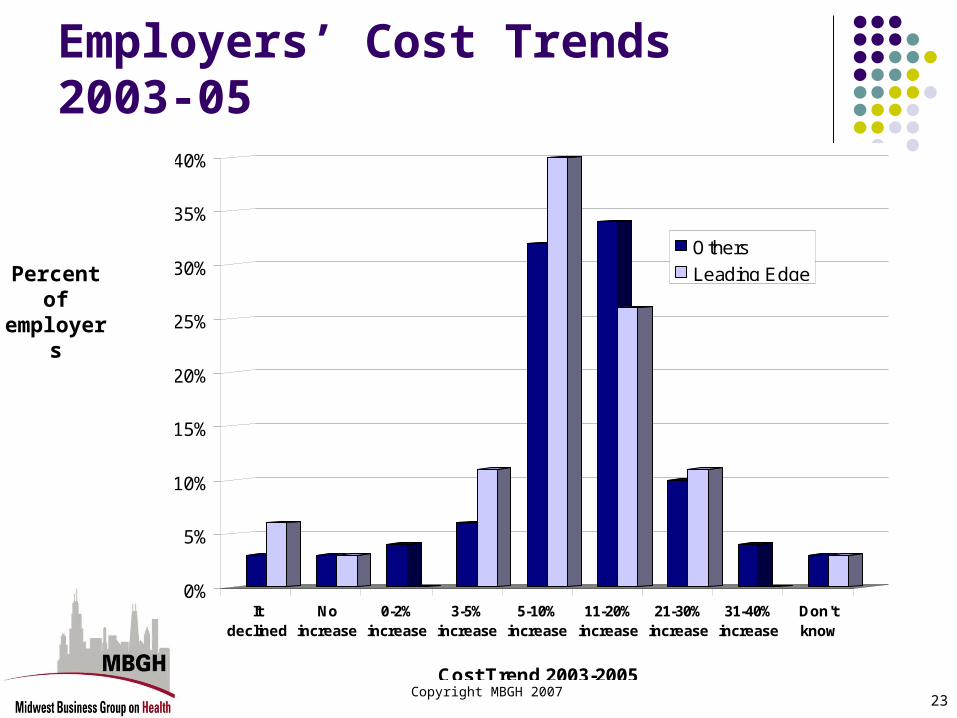
Percent of employers
Employers’ Cost Trends 2003-05
0%
5%
10%
15%
20%
25%
30%
35%
40%
Itdeclined
Noincrease
0-2%increase
3-5%increase
5-10%increase
11-20%increase
21-30%increase
31-40%increase
Don'tknow
Cost Trend 2003-2005
Others
Leading Edge
Use of Data
Copyright MBGH 200725
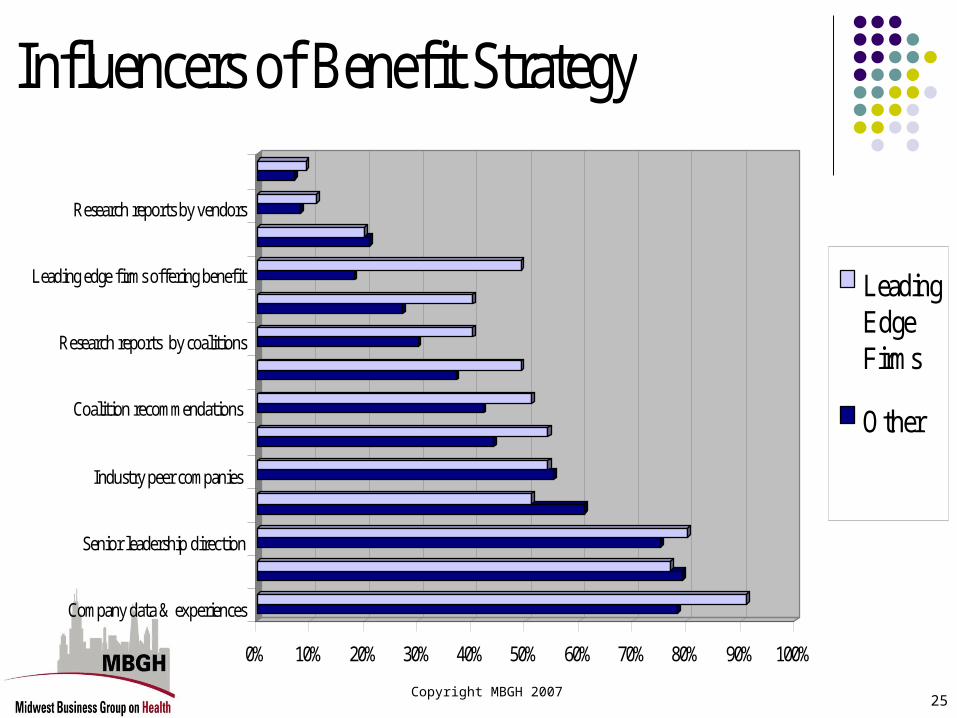
0% 10% 20% 30% 40% 50% 60% 70% 80% 90% 100%
Company data & experiences
Senior leadership direction
Industry peer companies
Coalition recommendations
Research reports by coalitions
Leading edge firms offering benefit
Research reports by vendors
Influencers of Benefit Strategy
LeadingEdgeFirms
Other
Copyright MBGH 200726
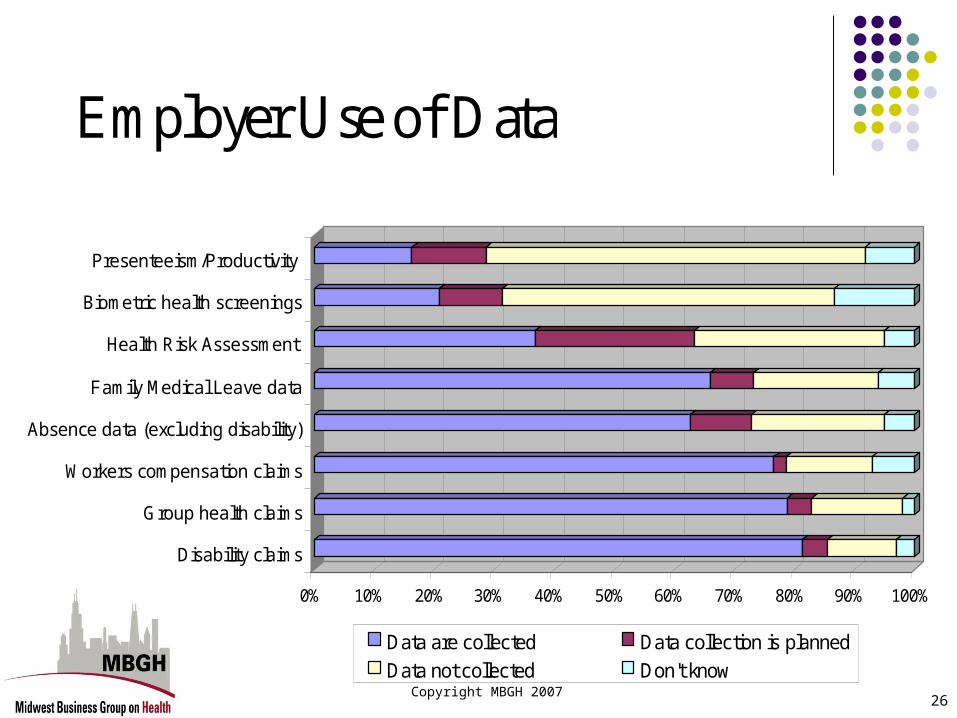
0% 10% 20% 30% 40% 50% 60% 70% 80% 90% 100%
Disability claims
Group health claims
Workers compensation claims
Absence data (excluding disability)
Family Medical Leave data
Health Risk Assessment
Biometric health screenings
Presenteeism/Productivity
Employer Use of Data
Data are collected Data collection is planned
Data not collected Don't know
Copyright MBGH 200727
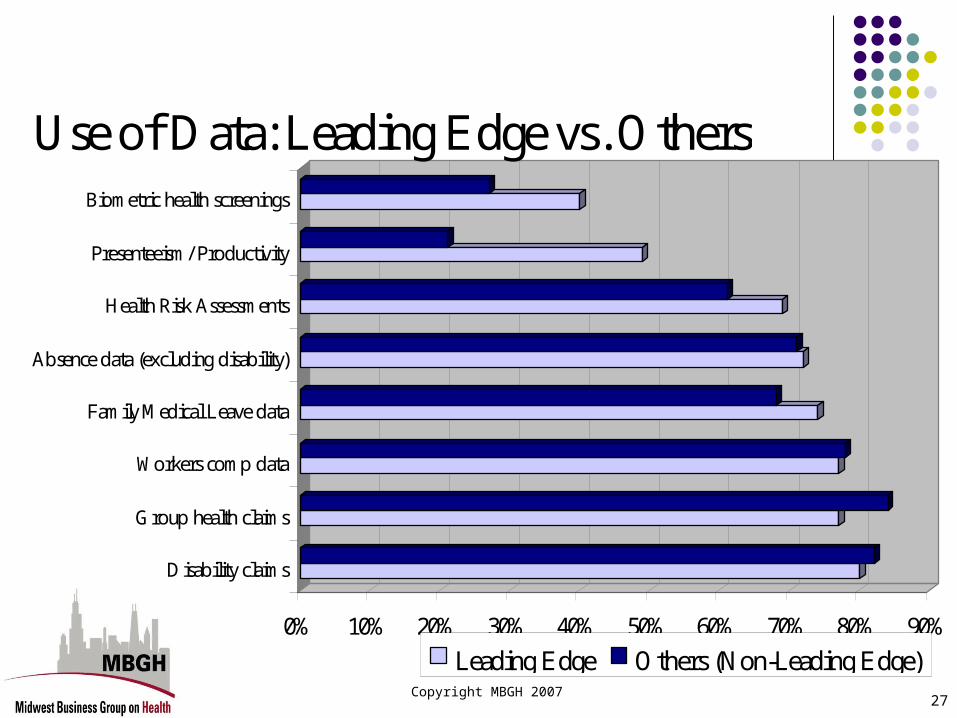
0% 10% 20% 30% 40% 50% 60% 70% 80% 90%
Disability claims
Group health claims
Workers comp data
Family Medical Leave data
Absence data (excluding disability)
Health Risk Assessments
Presenteeism/ Productivity
Biometric health screenings
Use of Data: Leading Edge vs. Others
Leading Edge Others (Non-Leading Edge)
Copyright MBGH 200728
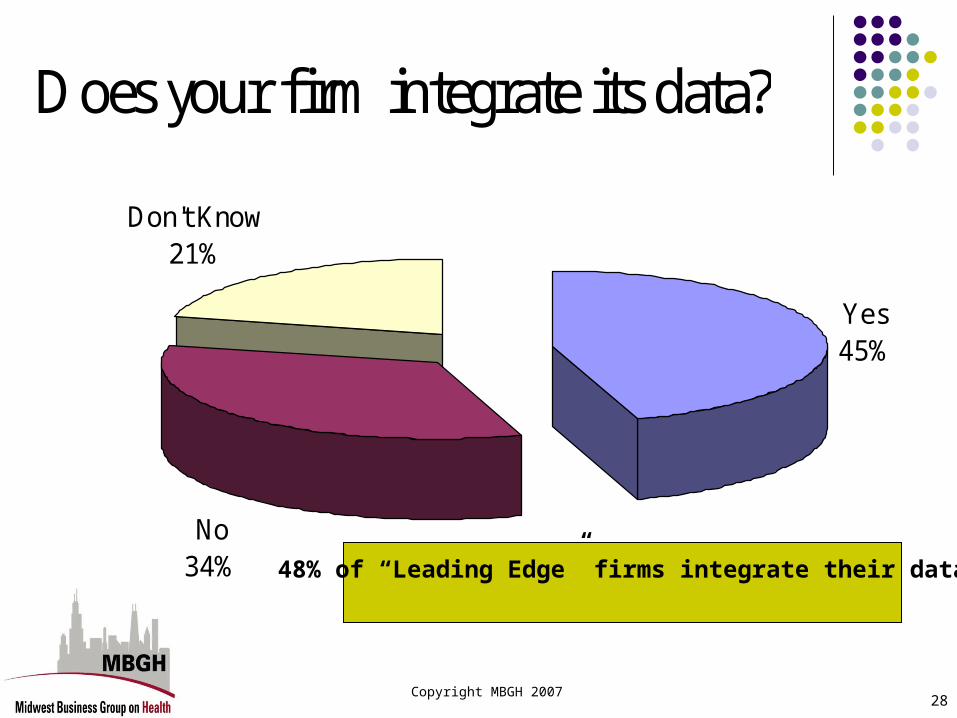
Does your firm integrate its data?
Yes45%
No 34%
Don't Know21%
48% of “Leading Edge” firms integrate their data

The Value of Healthand Related Benefit
Strategies

Copyright MBGH 200730
Employer views on the value of health
95% of employers agree that there is a link between an employee’s health and their productivity
84% of employers believe that health benefits are a necessary cost of doing business
85% of employers view health benefits as an investment in human capital with a measurable outcome
75% of employers are highly supportive of improving employee health
62% of employers who view themselves as “Leading Edge” will provide cash or other incentives to motivate use of preventive services, compared to 40% of other employers
Copyright MBGH 200731
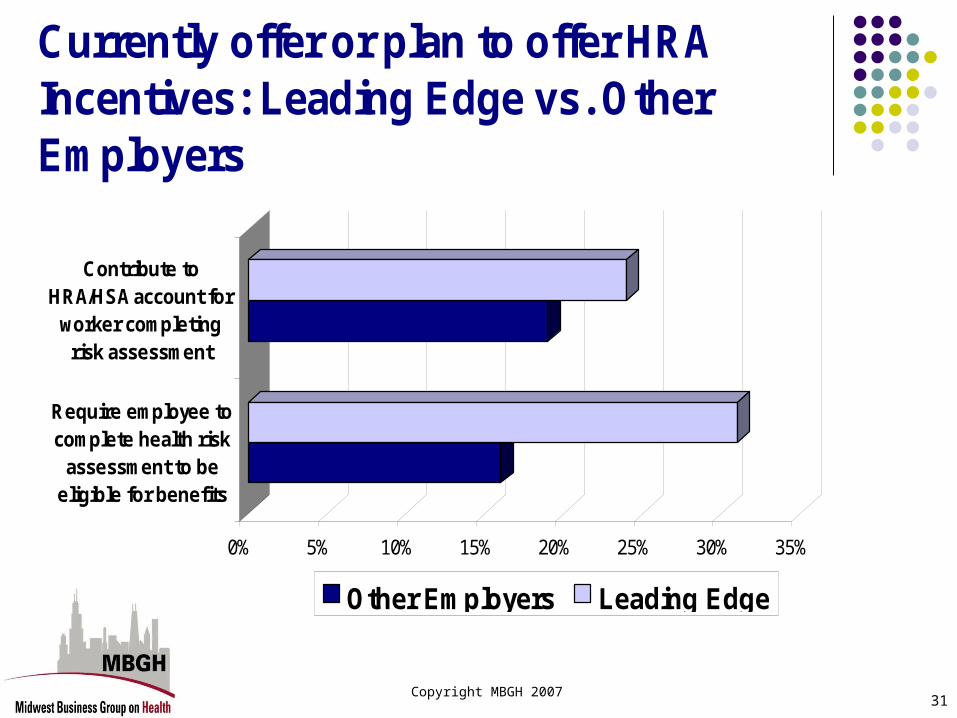
0% 5% 10% 15% 20% 25% 30% 35%
Require employee tocomplete health risk
assessment to beeligible for benefits
Contribute toHRA/HSA account for
worker completingrisk assessment
Currently offer or plan to offer HRA Incentives: Leading Edge vs. Other Employers
Other Employers Leading Edge

Copyright MBGH 200732
0% 5% 10% 15% 20% 25% 30% 35% 40% 45%
Employer contribution set to lowest cost benefitoption
Employee health premiums set by salary tiers
Higher employer contributions to HRA/HSAaccounts for those with chronic conditions
Employer contributions to an HSA/HRA accountbased on salary level of worker
Contribution Strategies: Leading Edge vs. Other Employers
Other Employers Leading Edge
Views and Strategies Around Cost-Sharing, Performance
Information and Quality

Copyright MBGH 200734
Employer views on cost-sharing
53% of employers agree that increased cost-sharing reduces physician visits
75% of employers believe an employee’s health impacts their sensitivity to cost-sharing
94% of employers agree that employees need to know their out-of-pocket costs to make informed decisions to obtain health services
Copyright MBGH 200735
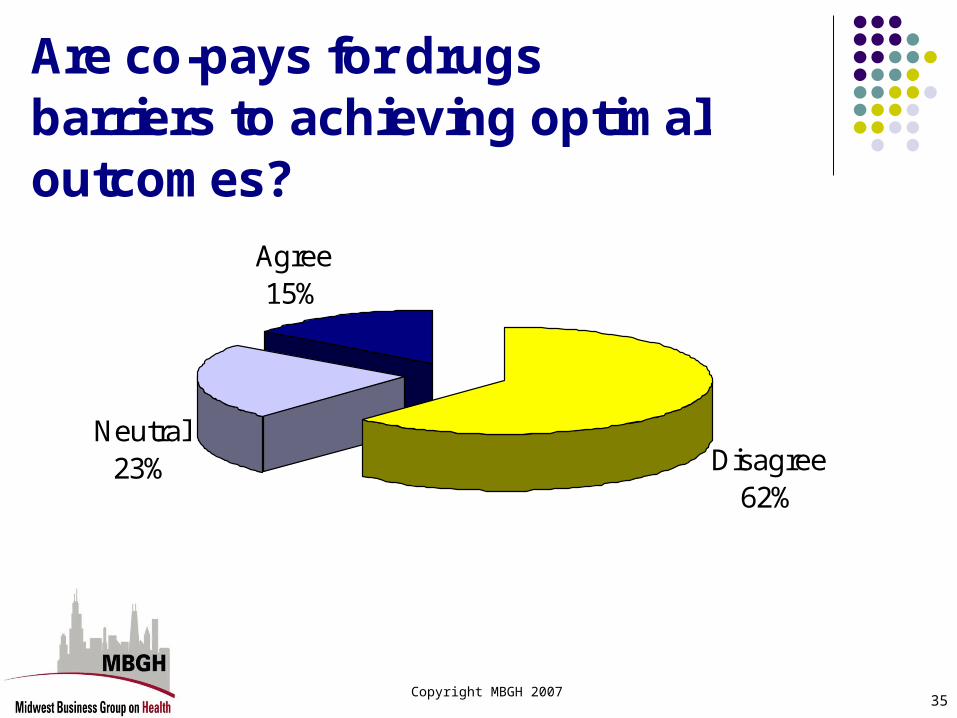
Are co-pays for drugs barriers to achieving optimal outcomes?
Disagree62%
Neutral23%
Agree15%
Copyright MBGH 200736
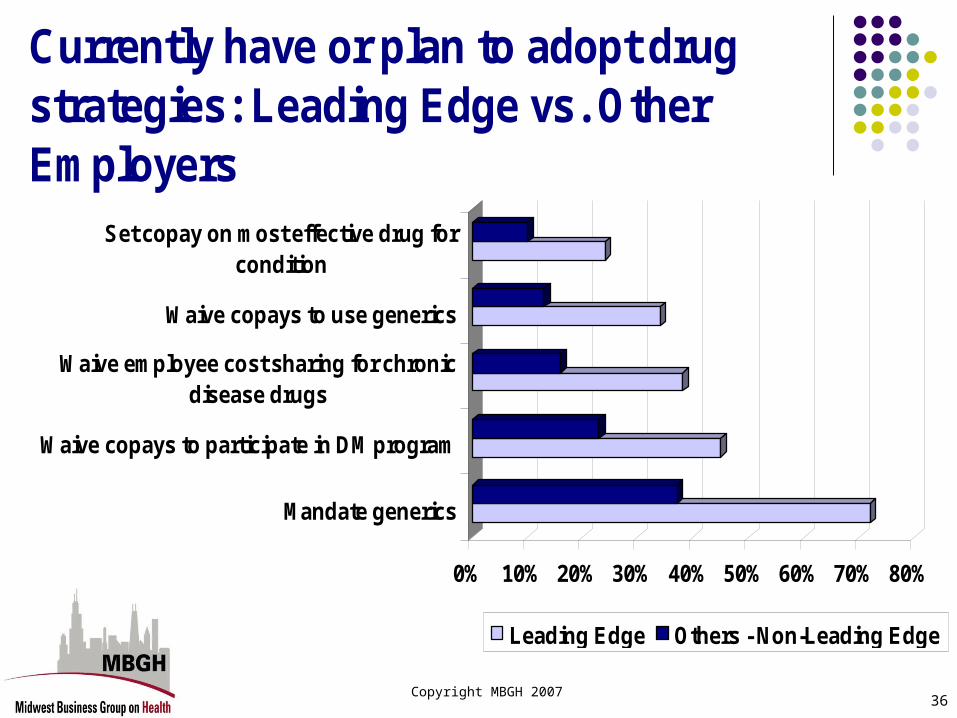
0% 10% 20% 30% 40% 50% 60% 70% 80%
Mandate generics
Waive copays to participate in DM program
Waive employee cost sharing for chronicdisease drugs
Waive copays to use generics
Set copay on most effective drug forcondition
Currently have or plan to adopt drug strategies: Leading Edge vs. Other Employers
Leading Edge Others - Non-Leading Edge

Copyright MBGH 200737
0%
10%
20%
30%
40%
50%
60%
70%
Selecting ageneric drug when
it is an option
Selecting a higherquality hospital
Changing to ahigher quality
doctor
Going to a Centerof Excellencefacility for aprocedure
Participating in adisease
managementprogram
Participating in apreventivescreening
Completing ahealth risk
assessment
< $25
$25 - $50
$51 - $100
$101 - $300
$301 - $500
>$500
Don't know
Employers views on level of dollar incentives to change behavior

Copyright MBGH 200738
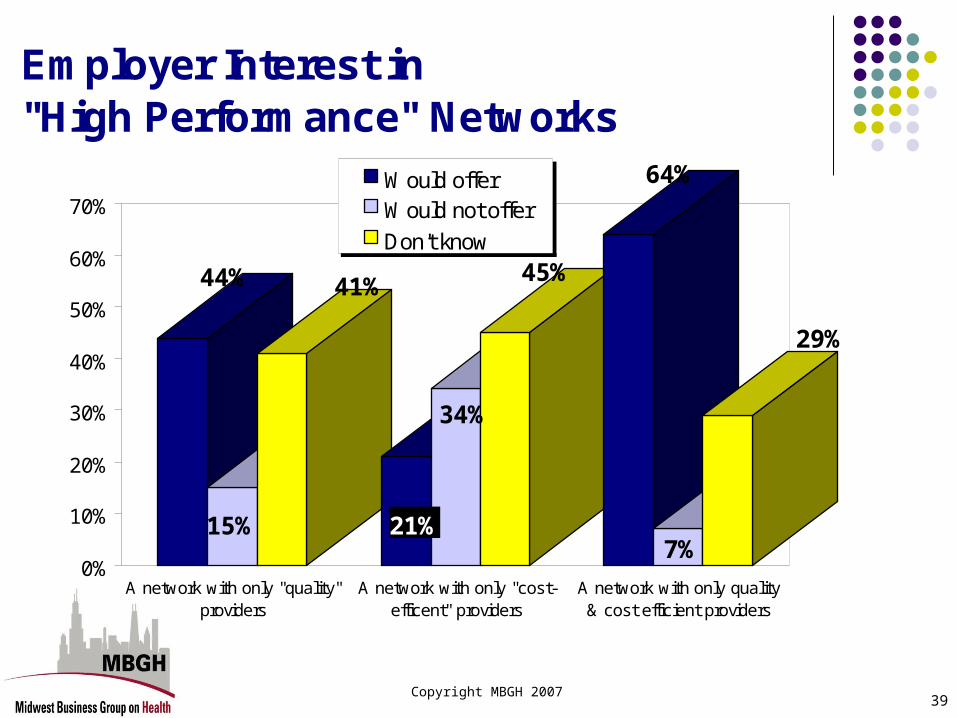
Copyright MBGH 200739
44%
15%
41%
21%
34%
45%
64%
7%
29%
0%
10%
20%
30%
40%
50%
60%
70%
A network with only "quality"providers
A network with only "cost-efficent" providers
A network with only quality& cost efficient providers
Employer Interest in "High Performance" Networks
Would offerWould not offer
Don't know

Copyright MBGH 200740
66%
15%
20%
59%
18%
23%
54%
19%
27%
0%
10%
20%
30%
40%
50%
60%
70%
Quality ofphysicians
Quality of drugs Quality and safetyof hospitals
Is information for employees available for informed choices?
Disagree Neutral Agree
Copyright MBGH 200741
Employer views on quality and cost
48% of employers believe employees have sufficient price information on prescription drugs to enable them to make informed choices
77% of employers agree that using drugs proven effective for a condition will reduce other services for that condition
60% of employers believe employees would change to better performing providers if they understood how quality varies and affects outcomes
70% of employers believe they should not pay hospitals or be billed for services provided due to preventable medical errors or infections, not related to the admission of a patient
Views on Incentives & Pay for Performance
Copyright MBGH 200743
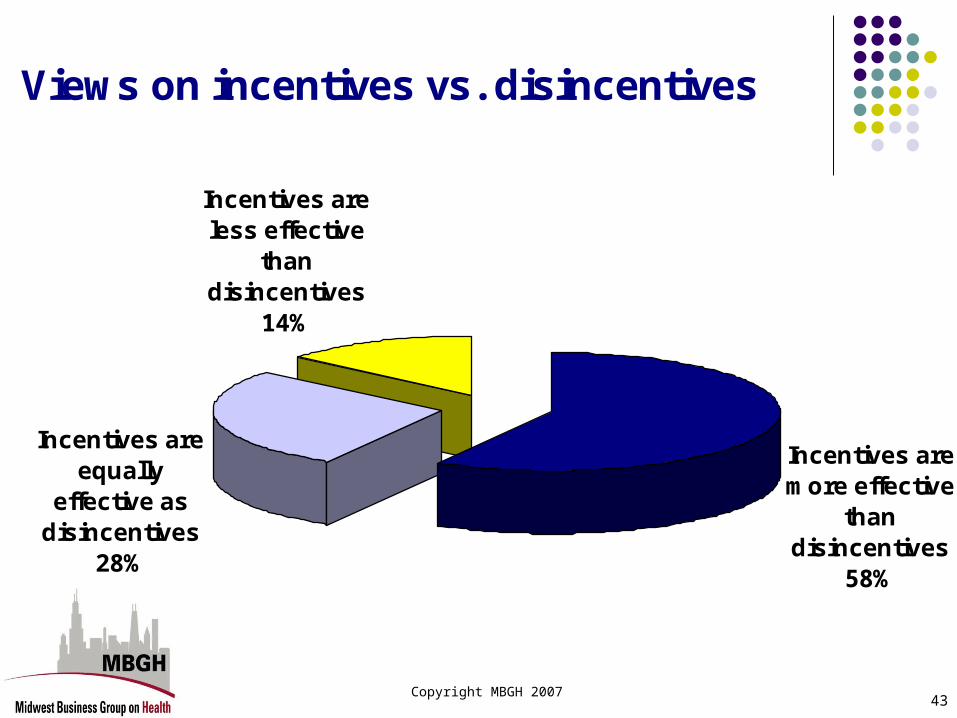
Views on incentives vs. disincentives
Incentives are more effective
than disincentives
58%
Incentives are equally
effective as disincentives
28%
Incentives are less effective
than disincentives
14%
Copyright MBGH 200744
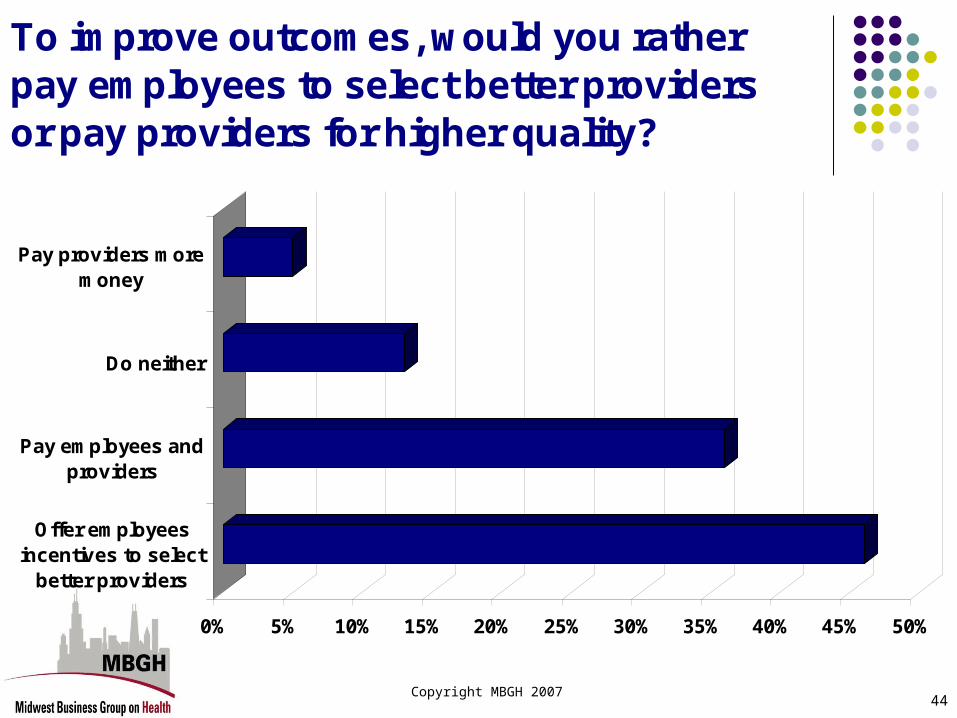
0% 5% 10% 15% 20% 25% 30% 35% 40% 45% 50%
Offer employeesincentives to select
better providers
Pay employees andproviders
Do neither
Pay providers moremoney
To improve outcomes, would you rather pay employees to select better providers or pay providers for higher quality?

Copyright MBGH 200745
0% 10% 20% 30% 40% 50% 60% 70%
Incentive to use Center of Excellence
Incentive to use higher quality hospitals
Incentive to use higher quality doctors
Incentive to complete health risk assessment
Incentive to obtain preventive services
Currently use or plan to use incentive strategies: Leading Edge vs. Other Employers
Leading Edge Other Employers
Copyright MBGH 200746
Summary Value-based benefit designs are being utilized by only a small percent
of employers, primarily leading edge organizations Key leading edge approaches:
Incentives for participation in wellness, DM and adherence programs Integration of cost and productivity data Enhancing the health of employees
Major employer concern: Lack of quality and cost data on providers Adopting “leading –edge” strategies can be most effective in reducing
cost trend and improving health of workforce Over two-thirds of employers do not collect or utilize
productivity/presenteeism data Less than half of employers are integrating their data to determine the
total impact of health on their populations Two-thirds of employers have not considered or are unwilling to use
incentives tied to premiums to reduce smoking
Copyright MBGH 200747
Next Steps
Follow-up survey to see if more employers are willing to adopt VBBD
Drill down on some areas Expand number of employer respondents Develop programs to help “activate” employees and address health
literacy barriers.
For further information…
Larry [email protected]
312-372-9090 x1
Jessica [email protected]
312-372-9090 x2





























