Embed Size (px)
DESCRIPTION
Presented at the Philippine General Hospital 1st Intravenous Therapy Nursing Update 2011
Citation preview

IV Insulin Therapy:
The Yale Insulin Infusion Protocol
Iris Thiele Isip Tan MD, FPCP, FPSEMClinical Associate Professor, UP College of MedicineSection of Endocrinology, Diabetes & MetabolismDepartment of Medicine, Philippine General Hospital
http://www.flickr.com/photos/jill_a_brown/2628388839/

Outline
•AACE/ADA Consensus on Inpatient Glycemic Control
•Characteristics of an ideal insulin infusion protocol
•PGH-Modified Yale Insulin Infusion Protocol

Critically ill
140-180 mg/dL(7.8-10 mmol/L)
2009 AACE/ADA Consensus Statement
Moghissi E et al. Endocrine Practice 2009;15(4):1-17
http://www.sxc.hu/photo/1176209

Moghissi E et al. Endocrine Practice 2009;15(4):1-17
IV insulin infusion preferred
Validated insulin infusion protocol: effective with low rates of hypoglycemia
http://www.sxc.hu/photo/253396

IV insulin infusion protocol
More consistent glucose control
Reduction in trial & error patterns
Maintain blood glucose within desired range
Earlier treatment of hypoglycemic events
Anger et al Pharmacotherapy 2006;26(2)214-28
http
://w
ww
.sxc
.hu/
phot
o/11
3144
6

An ideal insulin infusion protocol ...
... adapts to individual patient responses to insulin
Anger et al Pharmacotherapy 2006;26(2)214-28
http://www.sxc.hu/photo/1142176

An ideal insulin infusion protocol ...
... balances stability and responsiveness
to maintain target blood glucose
Anger et al Pharmacotherapy 2006;26(2)214-28
http://www.sxc.hu/photo/1142177

An ideal insulin infusion protocol ...
... varies the frequency of glucose monitoring
based on trends
Anger et al Pharmacotherapy 2006;26(2)214-28
http://www.sxc.hu/photo/1142175

An ideal insulin infusion protocol ...
... addresses potassium supplementation
Anger et al Pharmacotherapy 2006;26(2)214-28
http://www.sxc.hu/photo/805380

An ideal insulin infusion protocol ...
... clearly communicates instructions to the nurses responsible for titrating infusion
Anger et al Pharmacotherapy 2006;26(2)214-28
http://www.sxc.hu/photo/1148437

A ideal insulin infusion protocol ...
... streamlines decision making& eliminates need for complex calculations
Anger et al Pharmacotherapy 2006;26(2)214-28
http://www.sxc.hu/photo/1148436

modified
Yale protocol

Goldberg PA et al (2004). Implementation of a Safe and Effective Insulin Infusion Protocol in a Medical Intensive Care Unit. Diabetes Care 27(2):461-7.
Target blood glucose 90-119 mg/dL
Yale Protocol
“Modified” 100-139 mg/dL
PGH-modified Yale 140-180 mg/dL

Not to be used for DKA or HHS!
Call MD if BG >500 mg/dL
Yale Protocol
http://www.sxc.hu/photo/1156296

Yale Protocol
Initiating the Insulin Infusion
Insulin infusion: 1 u human regular insulin per 1 cc 0.9% NaCl per infusion pump (increments of 1 u/h)
Priming: Flush 50 cc through all IV tubing before infusion begins
Threshold: Start IV insulin if BG >180 mg/dL

Yale Protocol
Initiating the Insulin Infusion
Target blood glucose: 140-180 mg/dL
Bolus & initial insulin infusion rate:
Initial BG 181-299: divide by 100, round to nearest 1 unit for initial drip rate (NO bolus)
Initial BG >300: divide by 100, round to nearest 1 unit for initial drip rate AND bolus to be given
http://www.sxc.hu/photo/689723

http://www.sxc.hu/photo/485480Blood glucose monitoring
Check BG hourly until stable (3 consecutive values within target range)
Use blood from indwelling catheter for hypotensive patients

http://www.sxc.hu/photo/1215187
Once stable for 12-24 h, check BG q 2 h
May check BG q 4 h IF: no significant change in clinical condition AND no significant change in nutritional intake
Blood glucose monitoring

http://www.sxc.hu/photo/1215187
Consider hourly BG monitoring again (until stable) IF:
any change in insulin infusion rate (i.e. BG out of target range)
significant changes in clinical condition
initiation/cessation of pressor/steroid, renal replacement therapy, nutritional support (TPN, PPN, tube feedings, etc.)
Blood glucose monitoring

Blood glucose <50 mg/dL 50-69 mg/dL 70-99 mg/dL
Insulin infusion
D/C D/CD/C
for 30 min
D50 IV 1 amp
1 amp if symptomatic;
1/2 amp if asymptomatic
None
Recheck BG
q 15 min
q 15 min if symptomatic;
q 30 min if asymptomatic
q 30 min
If BG >100 mg/dL, wait 1 h. If repeat BG still >100 mg/dL, resume insulin drip at
If BG >100 mg/dL, resume
insulin drip at 75% of previous
Insulin drip rate
50% of previous 75% of previous

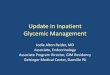
Determine the current BG level
BG 100-130 mg/dL
BG 140-179 mg/dL
BG 180-249 mg/dL
BG >250 mg/dL
identifies a COLUMN in the table

BG 100-130 BG 140-179 BG 180-249 BG >250 InstructionsBG ↑ by >40 mg/
dL/hBG ↑ ↑ DRIP by “2Δ”
BG ↑ by >20 mg/dL/h
BG ↑ by 1-40 mg/dL/h OR
BG UNCHANGED
BG UNCHANGED
OR BG ↓ by 1-40
mg/dL/h
↑ DRIP by “Δ”
BG ↑
BG ↑ by >20 mg/dL/h, BG
UNCHANGED, OR BG ↓ by 1-20 mg/
dL/h
BG ↓ by 1-40 mg/dL/h
BG ↓ by 41-80 mg/dL/h
NO DRIP CHANGE
BG unchanged OR BG ↓ by
1-20 mg/dL/h
BG ↓ by 21-40 mg/dL/h
BG ↓ by 41-80 mg/dL/h
BG ↓ by 81-120 mg/dL/h
↓ DRIP by “Δ”
BG ↓ by>20 mg/dL/h*
BG ↓ by >40 mg/dL/h
BG ↓ by >80 mg/dL/h
BG ↓ by >120 mg/dL/h
HOLD DRIP x 30 min then ↓ DRIP
by “2Δ”
Determine the rate of change from prior BG
* D/C insulin drip, check CBG q 30 min, when BG >100 mg/dL, resume drip at 75% of previous rate.

Changes in infusion rate (“Δ”) determined by current rate
Current Rate(units/hr)
Δ = rate change
(units/hr)
2Δ= 2x rate change
(units/hr)
<3 0.5 13-6 1 2
6.5 – 9.5 1.5 310-14.5 2 415-19.5 3 620-24.5 4 8≥25 ≥5 10 (consult MD)

Let’s practice ...

Let’s practice ...
•64/F admitted for pneumonia; not a known diabetic

Let’s practice ...
•64/F admitted for pneumonia; not a known diabetic
•Initial CBG 321 mg/dL

Let’s practice ...
•64/F admitted for pneumonia; not a known diabetic
•Initial CBG 321 mg/dL
•321/100 = 3.21 so give HR 3 units bolus and start insulin drip at 3 units/h

Let’s practice ...
•64/F admitted for pneumonia; not a known diabetic
•Initial CBG 321 mg/dL
•321/100 = 3.21 so give HR 3 units bolus and start insulin drip at 3 units/h
•CBG after 1 h is 285 mg/dL

Let’s practice ...
•64/F admitted for pneumonia; not a known diabetic
•Initial CBG 321 mg/dL
•321/100 = 3.21 so give HR 3 units bolus and start insulin drip at 3 units/h
•CBG after 1 h is 285 mg/dL
•321-285 = 36 mg/dL

BG 100-130 BG 140-179 BG 180-249 BG >250 InstructionsBG ↑ by >40 mg/
dL/hBG ↑ ↑ DRIP by “2Δ”
BG ↑ by >20 mg/dL/h
BG ↑ by 1-40 mg/dL/h OR
BG UNCHANGED
BG UNCHANGED
OR BG ↓ by 1-40
mg/dL/h
↑ DRIP by “Δ”
BG ↑
BG ↑ by >20 mg/dL/h, BG
UNCHANGED, OR BG ↓ by 1-20 mg/
dL/h
BG ↓ by 1-40 mg/dL/h
BG ↓ by 41-80 mg/dL/h
NO DRIP CHANGE
BG unchanged OR BG ↓ by
1-20 mg/dL/h
BG ↓ by 21-40 mg/dL/h
BG ↓ by 41-80 mg/dL/h
BG ↓ by 81-120 mg/dL/h
↓ DRIP by “Δ”
BG ↓ by>20 mg/dL/h*
BG ↓ by >40 mg/dL/h
BG ↓ by >80 mg/dL/h
BG ↓ by >120 mg/dL/h
HOLD DRIP x 30 min then ↓ DRIP
by “2Δ”
Determine the rate of change from prior BG
* D/C insulin drip, check CBG q 30 min, when BG >100 mg/dL, resume drip at 75% of previous rate.

Changes in infusion rate (“Δ”) determined by current rate
Current Rate(units/hr)
Δ = rate change
(units/hr)
2Δ= 2x rate change
(units/hr)
<3 0.5 13-6 1 2
6.5 – 9.5 1.5 310-14.5 2 415-19.5 3 620-24.5 4 8≥25 ≥5 10 (consult MD)

One more time ...

One more time ...
•54/M type 2 diabetic with pancreatitis; on NPO

One more time ...
•54/M type 2 diabetic with pancreatitis; on NPO
•Initial CBG 240 mg/dL

One more time ...
•54/M type 2 diabetic with pancreatitis; on NPO
•Initial CBG 240 mg/dL
•240/100 = 2.4 so start insulin drip at 2 units/h

One more time ...
•54/M type 2 diabetic with pancreatitis; on NPO
•Initial CBG 240 mg/dL
•240/100 = 2.4 so start insulin drip at 2 units/h
•CBG after 1 h is 170 mg/dL

One more time ...
•54/M type 2 diabetic with pancreatitis; on NPO
•Initial CBG 240 mg/dL
•240/100 = 2.4 so start insulin drip at 2 units/h
•CBG after 1 h is 170 mg/dL
•240-170 = 70 mg/dL

BG 100-130 BG 140-179 BG 180-249 BG >250 InstructionsBG ↑ by >40 mg/
dL/hBG ↑ ↑ DRIP by “2Δ”
BG ↑ by >20 mg/dL/h
BG ↑ by 1-40 mg/dL/h OR
BG UNCHANGED
BG UNCHANGED
OR BG ↓ by 1-40
mg/dL/h
↑ DRIP by “Δ”
BG ↑
BG ↑ by >20 mg/dL/h, BG
UNCHANGED, OR BG ↓ by 1-20 mg/
dL/h
BG ↓ by 1-40 mg/dL/h
BG ↓ by 41-80 mg/dL/h
NO DRIP CHANGE
BG unchanged OR BG ↓ by
1-20 mg/dL/h
BG ↓ by 21-40 mg/dL/h
BG ↓ by 41-80 mg/dL/h
BG ↓ by 81-120 mg/dL/h
↓ DRIP by “Δ”
BG ↓ by>20 mg/dL/h*
BG ↓ by >40 mg/dL/h
BG ↓ by >80 mg/dL/h
BG ↓ by >120 mg/dL/h
HOLD DRIP x 30 min then ↓ DRIP
by “2Δ”
Determine the rate of change from prior BG
* D/C insulin drip, check CBG q 30 min, when BG >100 mg/dL, resume drip at 75% of previous rate.

Changes in infusion rate (“Δ”) determined by current rate
Current Rate(units/hr)
Δ = rate change
(units/hr)
2Δ= 2x rate change
(units/hr)
<3 0.5 13-6 1 2
6.5 – 9.5 1.5 310-14.5 2 415-19.5 3 620-24.5 4 8≥25 ≥5 10 (consult MD)

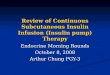
Goldberg PA et al (2004). Implementation of a Safe and Effective Insulin Infusion Protocol in a Medical Intensive Care Unit. Diabetes Care 27(2):461-7.
Histogram of 2242 hourly BG recordings after achievement of target BG levels

Goldberg PA et al (2004). Implementation of a Safe and Effective Insulin Infusion Protocol in a Medical Intensive Care Unit. Diabetes Care 27(2):461-7.
Yale IIP patients vs historical controls