Embed Size (px)
Citation preview

LITERATURE REVIEWJ Neurosurg 127:1361–1373, 2017
Blood-Blister aneurysms (BBAs) of the internal carotid artery (ICA) are rare vascular lesions that account for 0.3%–1.0% of all intracranial aneu-
rysms and 0.9%–6.5% of ruptured intracranial aneurysms and are associated with high morbidity and mortality.1,44 Unlike saccular aneurysms, BBAs follow a precipitous course, often enlarging and rebleeding quickly.15,35 Mor-phologically, they can appear as shallow out-pouchings of various portions of the ICA. These out-pouchings consist of fragile, thin walls with a broad communication with the parent artery and no discernable neck, making effective treatment difficult. Histologically, BBAs are character-
ized by focal vessel-wall defects, adventitial lining with-out collagen matrix, and associations with arterial dissec-tions.19,47 The pathology, location, and high probability of intra- and/or postoperative bleeding of BBAs present therapeutic challenges for physicians despite intervention-al advances.37
Surgical (clipping, wrapping, parent artery occlusion, trapping with or without bypass, and so forth), endovascu-lar (primary coil embolization, flow-diverting stents, and so forth), and combined approaches in treating BBAs have been reported in the literature; however, the complexity surrounding BBAs has led to uncertainty regarding the
ABBREVIATIONS BBA = blood-blister aneurysm; GOS = Glasgow Outcome Scale; ICA = internal carotid artery; mRS = modified Rankin Scale.SUBMITTED June 10, 2016. ACCEPTED September 27, 2016.INCLUDE WHEN CITING Published online February 17, 2017; DOI: 10.3171/2016.9.JNS161526.
Microsurgical versus endovascular interventions for blood-blister aneurysms of the internal carotid artery: systematic review of literature and meta-analysis on safety and efficacySumedh S. Shah, BS, Zachary C. Gersey, MS, Mohamed Nuh, BS, Hesham T. Ghonim, MD, Mohamed Samy Elhammady, MD, and Eric C. Peterson, MD, MS
Department of Neurological Surgery, University of Miami Miller School of Medicine, Miami, Florida
OBJECTIVE Blood-blister aneurysms (BBAs) of the internal carotid artery (ICA) have a poor natural history associated with high morbidity and mortality. Currently, both surgical and endovascular techniques are employed to treat BBAs; thus, the authors sought to perform a meta-analysis to compare the efficacy and safety of these approaches.METHODS A literature search of PubMed, MEDLINE, and Google Scholar online databases was performed to include pertinent English-language studies from 2005 to 2015 that discussed the efficacy and safety of either surgical or endo-vascular therapies to treat BBAs.RESULTS Thirty-six papers describing 256 patients with BBAs treated endovascularly (122 procedures) or surgically (139 procedures) were examined for data related to therapeutic efficacy and safety. Pooled analysis of 9 papers demon-strated immediate and late (mean 20.9 months) aneurysm occlusion rates of 88.9% (95% CI 77.6%–94.8%) and 88.4% (95% CI 76.7%–94.6%), respectively, in surgically treated patients. Pooled analysis of 12 papers revealed immediate and late aneurysm obliteration rates of 63.9% (95% CI 52.3%–74.1%) and 75.9% (95% CI 65.9%–83.7%), respectively, in endovascularly treated aneurysms. Procedure-related complications and overall poor neurological outcomes were slightly greater in the surgically treated cases than in the endovascularly treated cases (27.8% [95% CI 19.6%–37.8%] vs 26.2% [95% CI 18.4%–35.8%]), indicating that endovascular therapy may provide better outcomes.CONCLUSIONS Blood-blister aneurysms are rare, challenging lesions with a poor prognosis. Although surgical management potentially offers superior aneurysm obliteration rates immediately after treatment and at the long-term follow-up, endovascular therapy may have a better safety profile and provide better functional outcomes than surgery. A registry of patients treated for BBAs may be warranted to better document the natural course of the disease as well as treatment outcomes.https://thejns.org/doi/abs/10.3171/2016.9.JNS161526KEY WORDS aneurysm; blood-blister aneurysm; endovascular; internal carotid artery; microsurgical technique; meta-analysis; vascular disorders
©AANS, 2017 J Neurosurg Volume 127 • December 2017 1361
Unauthenticated | Downloaded 08/27/21 10:37 PM UTC

S. S. Shah et al.
J Neurosurg Volume 127 • December 20171362
optimal therapeutic modality.21,45,51 While open surgical techniques offer excellent durability, BBAs often present with thin walls that are prone to intraoperative tearing. If direct clipping cannot be achieved, then Sundt encircling clips or parent artery sacrifice may be necessary. On the other hand, in the context of a wide aneurysm neck, many BBAs cannot be endovascularly coiled without stent as-sistance.47 But during stent placement, for either assisted coiling or flow diversion, dual antiplatelet therapies are necessary, which is not ideal in cases of ruptured aneu-rysms. The uncertainty regarding the optimal therapy for patients presenting with a ruptured BBA may open dia-logue and contemplation at multidisciplinary institutions that offer both endovascular and surgical options. Both surgical and endovascular treatments come with a host of complications and concerns that must be considered be-fore administering therapy.33,36,40
Therefore, a study of the treatment options for BBA is warranted to determine the optimal course for patients re-quiring intervention. We sought to perform a systematic review of the literature and a meta-analysis to determine the efficacy and safety of microsurgical versus endovascu-lar approaches to treat BBAs of the ICA.
Methods Study Selection and Inclusion Criteria
Using the PubMed, MEDLINE, and Google Scholar systems, we performed a literature search for the years between 2005 and 2015 for all articles that included the terms “blood-blister aneurysm” and/or “blister aneurysm” located on the ICA (for example, “Blister Aneurysm”, “Blood blister aneurysm”, “blood blister-like aneurysm”, [“internal carotid artery” AND “blister aneurysm”], and so forth). Articles were limited to the English language with human subjects who had been diagnosed with an ICA BBA and who had undergone primary treatment via endo-vascular (coiling, stenting, flow-diversion) or microsurgical (clipping, wrapping, trapping with or without bypass) inter-vention. References in the obtained publications were also reviewed for additional studies. Papers with data regarding other types of aneurysms, aneurysms found at sites other than the ICA, or aneurysms whose primary treatment was neither endovascular nor surgical were excluded. Addition-ally, article types were limited to case reports, case series, retrospective studies, and clinical trials, whereas editorials, commentaries, and reviews were excluded. Duplicate pa-
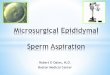
FIG. 1. Flowchart showing procedure for study exclusion and inclusion for this meta-analysis. Quantitative synthesis was per-formed in papers whose sample size was ≥ 2. Figure is available in color online only.
Unauthenticated | Downloaded 08/27/21 10:37 PM UTC

Optimal treatment for blood-blister aneurysms of the ICA
J Neurosurg Volume 127 • December 2017 1363
pers were removed, and all studies meeting the aforemen-tioned criteria underwent a full-text review.
Articles were included in this meta-analysis if we were able to extract pertinent data, such as study characteristics (first author, year study published, and design), patient de-mographics, patient clinical presentation, aneurysm data (size and location), treatment modalities used, preopera-tive hemorrhage grade, intra- and/or postoperative compli-cations, follow-up time, and outcome scores. The selection process can be viewed in Fig. 1. Our inclusion criteria did
not require a discussion of both treatment arms in studies of interest.
OutcomesThis systematic review and meta-analysis used 2 mea-
surements of outcome: treatment efficacy and safety. Ef-ficacy was determined by postoperative occlusion, con-firmed by angiography, at 2 time points: immediately and at follow-up. Occlusion was either complete or partial, and for purposes of this analysis, complete occlusion was used
TABLE 1. Literature survey of studies on BBAs of the ICA
Authors & Year
Study Type
No. of Patients
(M/F)Primary
Treatment
Required Re-Treatment
(no.)
Occlusion Data Reported Safety Data Reported
Immediate FUOutcome Score*
Intraop/Postop Complication
Ahn et al., 2008 CR 1 (0/1) Endovascular N Y Y NR YBaşkaya et al., 2008 CS 4 (3/1) Both N Y NR Y YCausin et al., 2011 CS 3 (1/2) Endovascular N Y Y Y YChalouhi et al., 2014 Retro 7 (2/5) Endovascular N Y Y Y YCho et al., 2012 CR 1 (0/1) Endovascular Y (1) Y Y NR YConsoli et al., 2012 CS 2 (1/1) Endovascular N Y Y Y YDoorenbosch et al., 2008 CR 1 (0/1) Endovascular N Y Y NR YEzaki et al., 2006 CR 1 (1/0) Endovascular N Y Y NR YFang et al., 2014 Retro 15 (2/13) Endovascular N Y Y Y YFang et al., 2013 Retro 8 (1/7) Endovascular N Y Y Y YGaughen et al., 2010 Retro 6 (1/5) Endovascular N Y Y Y YIhn et al., 2012 Retro 7 (2/5) Endovascular Y (2) Y Y Y YIshikawa et al., 2009 Retro 4 (0/4) Surgical N Y Y Y YJoo et al., 2006 CS 2 (2/0) Surgical N Y Y NR YKalani et al., 2013 Retro 17 (3/14) Surgical N Y Y Y YKamijo et al., 2010 Retro 7 (0/7) Surgical N Y Y Y YKawashima et al., 2008 CR 1 (0/1) Surgical N Y Y NR YKazumata et al., 2014 Retro 20 (5/15) Surgical N Y NR Y YKim et al., 2014 Retro 11 (3/8) Surgical N Y Y Y YKim et al., 2007 CR 1 (0/1) Endovascular N Y Y Y YKorja et al., 2008 CS 2 (1/1) Endovascular Y (1) Y Y Y YKubo et al., 2006 CS 6 (1/5) Surgical N NR Y Y YLee et al., 200930 Retro 9 (2/7) Endovascular Y (3) Y Y Y YLee et al., 200931 Retro 18 (2/16) Surgical N Y NR Y YLim et al., 2013 Retro 34 (6/28) Endovascular Y (3) Y Y Y YMcLaughlin et al., 2010 Retro 7 (3/4) Surgical N Y Y Y YMeling et al., 2008 Retro 14 (6/8) Both N NR NR Y YOtani et al., 2009 Retro 6 (1/5) Surgical N NR NR Y YPark et al., 2007 Retro 7 (1/6) Both Y (4) Y Y Y YPrinciotta et al., 2011 CR 1 (1/0) Endovascular N Y Y NR YRasskazoff et al., 2010 CR 1 (0/1) Endovascular N Y Y NR YSekula et al., 2006 CR 1 (0/1) Surgical N NR NR NR YSim et al., 2006 Retro 10 (0/10) Surgical N Y Y Y YTekkök & Bakar, 2008 CR 1 (1/0) Surgical N NR Y Y YYu-Tse et al., 2012 Retro 13 (6/7) Both Y (3) Y NR Y YÇinar et al., 2013 Retro 7 (1/6) Endovascular N NR Y Y Y
CR = case report; CS = case series; FU = follow-up; N = no; NR = not reported; retro = retrospective study; Y = yes. * Outcome scores were reported mainly using mRS or GOS, but some studies qualitatively confirmed good outcomes and were included in the statistical analysis.
Unauthenticated | Downloaded 08/27/21 10:37 PM UTC

S. S. Shah et al.
J Neurosurg Volume 127 • December 20171364
as the marker of successful treatment. Safety outcomes were qualitatively studied using reported postoperative complications and were quantified using functional scores. The 2 most common scales used to assess functional out-come are the Glasgow Outcome Scale (GOS), described by Jennett and Bond in 1975, and the modified Rankin Scale (mRS), first reported by Dr. John Rankin in 1957 but remodeled to its current form by Farrell et al. in 1991.14,20,42 Good and favorable neurological outcomes were defined as an mRS score of 0–2, which corresponds to no symp-toms, no significant disability despite symptoms, and slight disability but with the capability to look after one’s own affairs, respectively, or a GOS score of 4–5, which corresponds to moderate disability with no assistance in activities of daily living and good recovery, respectively.
We hypothesized that surgical intervention would yield higher complete occlusion rates immediately after treat-ment and at follow-up, whereas endovascular therapy would result in more favorable neurological outcomes.
Statistical AnalysisWe performed a total of 6 overall statistical analyses:
immediate endovascular occlusion, immediate surgical occlusion, endovascular occlusion at follow-up, surgical occlusion at follow-up, endovascular neurological out-comes, and surgical neurological outcomes. Meta-analysis was performed using the Comprehensive Meta-Analysis software (Biostat Inc.), and we elected to use the fixed-effects model summary effect measure as well as I2 and/or Q values with the forest plots. The random-effects model was reported when appropriate. Given the constraints in analyzing studies with a sample size of 1 patient, we did not include case reports in the quantitative analysis. Pub-lication bias was assessed using standard funnel plots as well as fixed-effects Duval and Tweedie trim and fill.10
ResultsStudy Selection
The PubMed and MEDLINE search revealed 225 pos-sible articles, while the other online database search led to an additional 130 studies. After duplicates were removed from each search and then across searches, we were left with 76 records to screen. The first selection process in-cluded a title and abstract review by 2 authors (S.S.S. and M.N.) with disagreements resolved through discussion. Thirty-seven articles were excluded given their inclusion of aneurysms other than BBAs and their analysis of BBAs located on non-ICA parent arteries, which left 39 studies for full text screening. The final phase of selection involved review by only 1 author (S.S.S.), yielding a total of 36 full-text articles to be included in this systematic review and meta-analysis (Table 1).2–9, 11–13, 15, 17,18,21–32,34,35,38,39,41,43, 46, 48, 50,51 Figure 1 displays the processes and phases of exclusion and inclusion for papers in this study.
Study Characteristics and DesignsA total of 36 papers with 256 patients undergoing 261
total treatments (either endovascular or surgical) for BBAs of the ICA were included in this review. There were 133 patients treated with stand-alone microsurgery, 119 pa-
tients treated primarily with endovascular approaches, and 4 patients who underwent combined therapy. All 36 studies were observational cohort studies evaluating en-dovascular or surgical intervention for ruptured BBAs. Twenty papers discussed retrospective studies. Eighteen studies evaluated endovascular therapy only, 14 evaluated surgery only, and 4 included both endovascular and surgi-cal interventions.3,35,39,52 For our analysis, 22 and 18 papers were examined and analyzed for endovascular and surgi-cal approaches, respectively.
Patient DemographicsA total of 256 patients were included in this meta-anal-
ysis. All papers included information regarding patient sex, and the ratio of male/female subjects was 1:3.33. Raw pooling of the extracted data revealed a mean age of 48.1 ± 11.1 years. The average aneurysm size was 3.2 ± 1.2 mm in diameter, and a majority of aneurysms were located on the supraclinoid (ophthalmic, C-6) segment of the ICA. Nu-merical data regarding treatments offered to the patients are included in Table 2. Of the 261 total treatments, 122 (46.7%) were endovascular and 139 (53.2%) were surgical. The most common endovascular procedure was coiling (71.3%), including stent-assisted coiling, and the most com-mon surgical procedure was clipping (45.3%). Finally, the average time to the most recent follow-up for all patients regardless of treatment was 20.9 months. A summary of patient demographics per endovascular and surgical treat-ment arms can be found in Tables 3 and 4, respectively.
OutcomesAmong the 36 papers, 30 had data regarding total oc-
clusion; however, 10 of them could not be statistically analyzed because of the small sample size. Among the remaining 20 papers, occlusion was assessed in 12 and 9 studies for the endovascular and surgical interventions, respectively. One study included data on both treatments and is thus included twice.3 Occlusion at follow-up was documented in 29 studies, but only 20 papers were sta-tistically evaluated for the aforementioned reason. Twelve studies reported on endovascular therapy, and 8 reported
TABLE 2. Characteristics of treatments documented in this studyEndovascular (22 papers) Surgical (18 papers)
Treatment No. Treatment No.
FD stent 12 Clip 63PED 7 Wrap 2Stent (multiple) 11 Bypass 8Coil 13 Suture 1Stent + coil 74 Clip + wrap 15Endovascular trapping 1 Clip + bypass 4Other/unspecified 4 Clip + wrap + suture 1
Surgical trapping 22Trapping + bypass 23
Total 122 139Percentage 46.7% 53.2%
FD = flow-diverting; PED = Pipeline embolization device.
Unauthenticated | Downloaded 08/27/21 10:37 PM UTC

Optimal treatment for blood-blister aneurysms of the ICA
J Neurosurg Volume 127 • December 2017 1365
TABLE 3. Summary of characteristics of patients who underwent endovascular treatment for BBA
Authors & Year
No. of Patients
Age (yrs)
Aneurysm Data Clinical Presentation
PreOp Grade
FU DataLocation on ICA Size (mm) Time Imaging Outcome Score
Ahn et al., 2008 1 64 Supraclinoid (1) NR SAH (1) NR 6 mos Angio NRBaşkaya et al.,
2008*4 40 ± 19 Supraclinoid (2),
communicating (1), ophthalmic (1)
2.6 ± 0.8 SAH (4) HH IV (4), F 3 (4)
1.75 ± 1.5 mos
Angio mRS 1 (3), 6 (1)
Causin et al., 2011
3 49 ± 7 Supraclinoid (3) 2.6 ± 0.6 SAH (3) F 3 (2), F 4 (1) 10.4 ± 4.6 mos
Angio NR†
Chalouhi et al., 2014
7 51.4 ± 11.6 Ophthalmic (1), NR (6) 2.6 ± 0.5 SAH (4), IF (2), HA (1)
NR 4 ± 1.7 mos
Angio mRS 0–2 (7)
Cho et al., 2012 1 57 Distal dorsal wall (1) 4.4 SAH (1) HH III (1), F 4 (1)
6 mos Skull radio
NR
Consoli et al., 2012
2 NR Supraclinoid 5 SAH (2) F 1 7 mos DSA NR†
Doorenbosch et al., 2008
1 44 Supraophthalmic (1) 3 SAH (1) F 2 (1) 6 wks Angio NR
Ezaki et al., 2006
1 21 Superomedial (1) NR SAH (1) HH IV (1), F 3 (1)
1 mo Angio NR
Fang et al., 2014
15 45.2 ± 10.1 Ophthalmic (8), communicating (5), C6–7 junction (2)
Max dia <10
HA (15), vom-iting (13), LOC (8)
HH I (2), II (5), III (6), IV (1), V (1)
5 days–6 mos
Angio mRS 0–1 (14), 3 (1)
Fang et al., 2013
8 45.8 ± 11.5 Communicating (3), ophthalmic (3), C6–7 junction (3)
Max dia <10
SAH (8) HH I (1), II (5), III (1), IV (1)
9.2 mos Angio mRS 0–2 (6)
Gaughen et al., 2010
6 49.7 ± 12.4 Supraclinoid (6) 2.5 ± 0.5 SAH (6) HH I (1), II (3), III (2)
6.2 ± 4.3 mos
Angio mRS 1 (5), 3 (1)
Ihn et al., 2012 7 45.6 ± 7.2 Supraclinoid (7) 3.2 ± 1.6 SAH (7) HH II (4), III (2), IV (1)
15.5 ± 5.0 mos
Angio mRS 0–1 (5), 4 (1), 6 (1)
Kim et al., 2007 1 57 Supraclinoid (1) NR SAH (1) NR 6 mos Angio GOS 5 (1)Korja et al.,
20082 51 ± 3 Supraclinoid (2) 2–3 (2) SAH (2) F 3 (2) 20 mos Angio NR†
Lee et al., 200930
9 50.3 ± 4.0 Supraclinoid (9) NR SAH (9) HH I (1), II (1), III (7)
11.1 ± 6.9 mos
Angio GOS 1 (1), 5 (8)
Lim et al., 2013 34 47.6 ± 6.7 Ant wall (31, pst wall (3)
2.7 ± 1.0 SAH (34) HH II (6), III (22), IV (5), V (1)
37 ± 18 mos
Angio mRS 0–2 (25), 3 (3), 4 (2), 6 (4)
Meling et al., 2008*
14 48.3 ± 9.3 Medial (6), lat (2), ant (1), anteromedial (5)
3.9 ± 1.3 SAH (14) F 2 (3), 3 (3), 4 (8)
NR NR GOS 1 (6), 2 (1), 3 (1), 5 (6)
Park et al., 2007*
7 35.4 ± 6.5 Dorsal surface (7) NR SAH (7) HH II (6), IV (1)
10.8 ± 2.6 mos
Angio VS (3), GR (4)
Princiotta et al., 2011
1 43 Supraclinoid (1) NR SAH (1) HH I 6 mos Angio NR
Rasskazoff et al., 2010
1 38 Lat wall (1) 2 SAH (1) F 3 6 mos Angio NR
Yu-Tse et al., 2012*
13 51.4 ± 10.7 Anteromedial wall (11), lat wall (2)
NR SAH (13) F 1 (1), 3 (8), 4 (4)
6 mos Angio mRS 0–1 (4), 3 (1), 4 (1), 5 (7)
Çinar et al., 2013
7 44.6 ± 5.9 Ant wall (4), pst wall (2), medial ICA (1)
3.86 ± 0.23 SAH (7) HH I (3), II (3), III (1)
6.4 ± 2.7 mos
Angio mRS 0–2 (5), 3 (1), 4 (1)
Angio = angiogram; ant = anterior; dia = diameter; DSA = digital subtraction angiogram; F = Fisher grade; GR = good recovery; HA = headache; HH = Hunt and Hess grade; IF = incidental finding; LOC = loss of consciousness; pst = posterior; radio = radiograph; SAH = subarachnoid hemorrhage; VS = vegetative state. Values expressed as mean ± standard deviation, unless indicated otherwise. * Studies with both endovascular and surgical data.† Outcome scores could not be extracted, but the papers qualitatively confirmed good outcomes.
Unauthenticated | Downloaded 08/27/21 10:37 PM UTC

S. S. Shah et al.
J Neurosurg Volume 127 • December 20171366
results from surgery. In all papers quantitatively exam-ined, occlusion was determined using angiography.
Cumulatively, we found 27 papers that discussed post-operative outcome, 25 from which we were able to extract the appropriate data. Fourteen papers discussed endovas-cular neurological outcomes (9 used mRS, 3 used GOS, and 2 used neither scale but provided sufficient detail to confirm favorable or unfavorable outcome). Thirteen pa-pers discussed neurological outcome postsurgery (8 used mRS, 3 used GOS, and 2 specified qualitatively or through another metric, such as the Karnofsky Performance Scale).
Two papers discussed the 2 treatment arms together and were therefore included twice.35,52
Aneurysm Occlusion After Endovascular TreatmentAnalysis of immediate aneurysm occlusion after en-
dovascular intervention revealed a rate of 63.9% (95% CI 52.3%–74.1%, p = 0.019) using the fixed-effects model and a rate of 65.6% (95% CI 47.9–79.9%, p = 0.083) with the random-effects model (104 endovascular procedures; Fig. 2A). A Q statistic of 21.83 and an I2 value of 49.61 were
TABLE 4. Summary of characteristics of patients who underwent surgical treatment for BBA
Authors & Year
No. of
PatientsAge (yrs)
Aneurysm Data Clinical Presentation
(no.)
Preop Grade (no.)
FU DataLocation on
ICA (no.)Size (mm)
Time (mos) Imaging
Outcome Score
Başkaya et al., 2008*
4 40 ± 19 Supraclinoid (2), communicating (1), ophthalmic (1)
2.6 ± 0.8 SAH (4) HH IV (4), F 3 (4)
1.75 ± 1.5 Angio mRS 1 (3), 6 (1)
Ishikawa et al., 2009
4 53.3 ± 14.6 Dorsal (4) NR SAH (4) WFNS I (2), II (2)
3 Angio mRS 0 (4)
Joo et al., 2006 2 31.5 ± 2.2 Cervical (1), petrous (1)
3 SAH (2) F 3 (1), HH III (1)
5 Angio NR
Kalani et al., 2013 17 45.2 ± 15.8 Nonbranching–un-specified (17)
2.6 ± 1.7 SAH (12), IF (5)
HH I (1), II (1), III (5), IV (5)
74.5 Angio GOS 2 (1), 3 (2), 5 (14)
Kamijo et al., 2010 7 61.0 ± 10.9 Supraclinoid (7) SAH (7) F 3 (7) 14.6 Angio GOS 5 (5) Kawashima et al.,
20081 32 Cervical (1) NR SAH (1) HH II (1) 1 Angio NR
Kazumata et al., 2014
20 51.2 ± 12.6 Anteromedial (15), other (5)
NR SAH (20) WFNS I (6), II (10), III (1), IV (3)
3 Angio mRS 0–2 (18), 4 (2)
Kim et al., 2014 11 43 ± 12 Supraclinoid ICA (11) NR SAH (11) HH II (6), III (4), IV (1)
40 ± 19 Angio mRS 0–1 (8), 4 (1), 5 (1), 6 (1)
Kubo et al., 2006 6 48.8 ± 14.8 Anteromedial (4), ant (1), anterolat (1)
1–2 SAH (6) HK II (5), III (1) 41.8 ± 20 Angio mRS 0 (6)
Lee et al., 200931 18 50.4 ± 9.0 Dorsal (6), dorsolat (1), dorsomedial (7), medial (4)
2.7 ± 0.8 SAH (18) HH II (4), III (10), IV (4)
17 (6–50) NR mRS 1–2 (14), 3 (1), 4 (1)
McLaughlin et al., 2010
7 44.7 ± 9.9 Unspecified (7) 2.9 ± 0.4 SAH (7) HH I (2), II (4), III (1)
18.1 ± 18.7 Angio mRS 0–1 (7)
Meling et al., 2008*
14 48.3 ± 9.3 Medial (6), lat (2), ant (1), anteromedial (5)
3.9 ± 1.3 SAH (14) F 2 (3), 3 (3), 4 (8)
NR NR GOS 1 (6), 2 (1), 3 (1), 5 (6)
Otani et al., 2009 6 55.2 ± 8.9 Supraclinoid (6) 2.3 ± 0.5 SAH (6) HK II (2), III (1), V (3)
NR NR NR†
Park et al., 2007* 7 35.4 ± 6.5 Dorsal surface (7) NR SAH (7) HH II (6), IV (1) 10.8 ± 2.6 Angio VS (3), GR (4)Sekula et al., 2006 1 41 Supraclinoid (1) NR SAH (1) HH 2 6 Angio NRSim et al., 2006 10 49.3 ± 9.6 Supraclinoid (10), ant
wall (7), anterolat (2), anteromedial (1)
2–8 SAH (10) NR 27.2 Angio Excellent (8), fair (1), poor (1)
Tekkök & Bakar, 2008
1 43 Supraclinoid (1) NR SAH (1) F 3 NR NR KPS 100/100
Yu-Tse et al., 2012*
13 51.4 ± 10.7 Anteromedial wall (11), lateral wall (2)
NR SAH (13) F 1 (1), 3 (8), 4 (4)
6 Angio mRS 0–1 (4), 3 (1), 4 (1), 5 (7)
HK = Hunt and Kosnik grade; KPS = Karnofsky Performance Scale; WFNS = World Federation of Neurological Societies grade. Values expressed as mean ± standard deviation, unless indicated otherwise.* Studies with both endovascular and surgical data.† Outcome scores could not be extracted, but the papers qualitatively confirmed good outcomes.
Unauthenticated | Downloaded 08/27/21 10:37 PM UTC

Optimal treatment for blood-blister aneurysms of the ICA
J Neurosurg Volume 127 • December 2017 1367
calculated, indicating moderate study heterogeneity. Our computed tau (t) value of 0.859 exposed variance within and between studies.
Aneurysm occlusion rates at the most recently reported follow-up (mean approximately 20.2 months) after endo-vascular treatment were 75.9% (95% CI 65.9%–83.7%, p < 0.0001) and 75.5% (95% CI 63.1%–84.8%, p < 0.001) using the fixed- and random-effects models, respectively (Fig. 2B). Assessed Q values (14.0) and I2 statistics (21.3) showed low heterogeneity, while our t-value of 0.469 indi-cated some variance between and within the studies.
The funnel plot looking at immediate endovascular occlusion was overall symmetric and showed no obvious signs of publication bias (Fig. 3A). Duval and Tweedie’s trim and fill revealed 1 point to the left of our calculated effect rate, and the adjusted estimate was 62.4% (95% CI 50.8%–72.7%, Q = 24.5). The funnel plot addressing pub-lication bias in occlusion rates at follow-up was faintly asymmetrical toward the right (Fig. 3B), suggesting that studies with lower occlusion rates may be missing. Duval and Tweedie’s trim and fill also revealed 1 point to the left of the effect rate, and the adjusted rate was 75.0% (95% CI 65.0%–83.0%).
Aneurysm Occlusion After Microsurgical TreatmentPooled analysis of 9 studies regarding immediate oc-
clusion after microsurgical intervention revealed occlu-sion rates of 88.9% (95% CI 77.6%–94.8%, p < 0.0001) by the fixed-effects model (70 surgical treatments; Fig. 4A). Pooling was possible due to minimal heterogeneity, as our calculated Q was 4.24 and I2 was 0. Low variance between studies and within studies was confirmed through the cal-culation of low tau values (t = 0).
Total reported occlusion rate at the most recent follow-up (mean approximately 39.1 months, 8 studies) for pa-tients in the surgical treatment arm was 88.4% (95% CI 76.7%–94.6%, p < 0.0001), which was calculated through the fixed-effects model (Fig. 4B). Tests for heterogeneity resulted in a Q of 3.87 and an I2 value of 0, which shows low heterogeneity. Tau values were again 0, which indi-cates low study variance.
Funnel plots for immediate occlusion after surgery re-vealed asymmetry toward the lower right (Fig. 5A). This finding suggests there may be some smaller studies re-porting lower total occlusion rates that are missing. Duval and Tweedie’s trim and fill exposed 4 points to the left of our effect rate, which adjusted the rate to 82.1% (95% CI 69.1%–90.4%) with a Q of 11.06. Funnel plots for occlusion at follow-up revealed a similar asymmetrical trend toward the right (Fig. 5B). Duval and Tweedie’s trim and fill ex-posed 3 points to the left of our effect rate, which adjusted the rate to 83.1% (95% CI 70.4%–91.0%) with a Q of 7.97.
FIG. 2. Immediate (A) and follow-up (B) aneurysm occlusion after an endovascular procedure.
Unauthenticated | Downloaded 08/27/21 10:37 PM UTC

S. S. Shah et al.
J Neurosurg Volume 127 • December 20171368
Neurological OutcomesThirteen studies reported outcome based on functional
scores (that is, mRS, GOS, and so forth) that we pooled for endovascular intervention. A fixed-effects model revealed unfavorable outcomes in 26.2% (95% CI 18.4%–35.8%, p < 0.0001) of patients (Fig. 6A). A Q of 8.46 and an I2 of 0 indicated low levels of study heterogeneity. The t value was 0, which implies low variance in the studies.
Thirteen papers reported neurological outcomes in pa-tients after surgical intervention. Tests of heterogeneity revealed that Q was 21.8 and I2 was 54.1, indicating mod-erate heterogeneity. A fixed-effects model and random-ef-fects model revealed unfavorable outcomes in 27.8% (95% CI 19.6%–37.8%) and 23.1% (95% CI 12.7%–38.2%) of patients, respectively (Fig. 6B).
Publication bias assessed by funnel plot in neurological outcomes of endovascular procedures showed no asym-metry (Fig. 7A). However, the funnel plot of the studies re-garding neurological outcome of surgical procedures was markedly asymmetrical toward the lower left (Fig. 7B). This suggests a publication bias toward smaller studies re-porting lower unfavorable neurological outcomes. Duval and Tweedie’s trim and fill included 4 points to the right of the observed effect rate. The adjusted estimate indicates unfavorable neurological outcomes in 34.5% of patients (95% CI 24.8%–45.7%).
ComplicationsComplications for each of the procedure arms were
pooled together as raw data from each of the included studies. The most common intraoperative complication (Fig. 8A) associated with both endovascular and surgical procedures was aneurysm rupture; however, surgical ap-proaches showed an increased incidence of rupture (28.8% vs 3.2%). The postoperative period was associated with
FIG. 3. Funnel plot with included Duval and Tweedie’s trim and fill (full black point) for immediate (A) and follow-up (B) occlusion rates after endovascular treatment.
FIG. 4. Aneurysm occlusion immediately after surgery (A) and at follow-up (B).
Unauthenticated | Downloaded 08/27/21 10:37 PM UTC

Optimal treatment for blood-blister aneurysms of the ICA
J Neurosurg Volume 127 • December 2017 1369
the most complications for either endovascular or surgi-cal aneurysm management (Fig. 8B). While vasospasm, hydrocephalus, and infarction predominated as the lead-ing observed comorbidities associated with surgical treat-ment (21.6%, 9.9%, and 6.3% respectively), endovascular management was associated with the highest reported incidence of aneurysm regrowth (8.5%), patient mortality (6.6%), and rebleeding (5.6%).
DiscussionThe incidence of BBAs represents a minute portion of
all intracranial aneurysms, yet the diagnosis and treatment of these lesions are reported to be difficult because of the peculiar zones in which they arise and their thin walls and obscure base.19,37 While advances in both endovascular and surgical approaches have led to increased procedural suc-cess and overall safety for the patient, BBAs are still un-fortunately characterized by their malignant features. The propensity for these aneurysms to rapidly expand and/or rupture makes treatment difficult, and there is controversy surrounding the optimal plan of action.1,44 The complexity and delicacy of BBAs, especially those on the ICA, present therapeutic challenges for patients. No randomized-con-trolled trial has been performed regarding endovascular versus surgical treatment of BBAs. Here, we present the most recent statistical meta-analysis on the efficacy and safety of endovascular versus surgical treatment arms to manage BBAs.
Surgery for BBAs provides higher total aneurysm occlu-sion immediately (mean 88.9%, 95% CI 77.6%–94.8%, p < 0.0001) than endovascular treatment (mean 63.9%, 95% CI 52.3%–74.1%, p = 0.019). Surgery also provides better total occlusion at the most recent patient follow-up (88.4%, 95% CI 76.7%–94.6%, p < 0.0001) than endovascular treatment (75.9%, 95% CI 65.9%–83.7%, p < 0.0001). While more efficacious in occlusion rates at both time points analyzed, surgery did not seem as safe as endovascular approaches when neurological outcome scores were compared. Nega-tive outcomes in 26.2% of patients (95% CI 18.4%–35.8%) were reported with endovascular procedures, while nega-tive outcomes in 27.8% of patients (95% CI 19.6%–37.8%) were reported with surgery. More importantly, the adjusted safety rates on negative surgical outcomes indicated that the true negative outcome rate might be closer to 35%, im-plying some inherent reporting bias and further supporting the findings that endovascular therapy may lead to better neurological outcomes than surgical intervention. Raw pooled data analysis from our paper further suggests that endovascular approaches are safer based on complications. Overall, calculated intraoperative complications for endo-vascular versus surgical approaches were 2.1% versus 14%. Postoperative complications were similar in that endovas-cular procedures resulted in some complication 29% of the time, while surgery resulted in morbidity 45% of the time.
Two recent systematic reviews published in 2014 and 2015, respectively, also assessed optimal treatment mo-dalities for BBAs of nonbranching segments of the ICA. Despite some similarities between these 2 reviews and the current study, our study is distinct and maintains novelty from the others for several reasons.16,49
Gonzalez et al. found that endovascular approaches re-sulted in less morbidity than surgical intervention, mainly clipping (3.4% vs 18%), and this claim supports our find-ings regarding the safety profile of endovascular thera-py.16 Within their methodology, Gonzalez et al. specified a search criteria cutoff of only July 1, 2013, while our search ended December 31, 2015. Our more recent cutoff revealed 5 additional papers (Chalouhi et al., 2014; Fang et al., 2014; Kalani et al., 2013; Kazumata et al., 2014; and Kim et al., 2014; 70 patients) that had not been previously analyzed. Furthermore, since the course of BBA management has evolved rapidly within the last decade, our search timeline (2005–2015) reflects what we believe to be an accurate representation of the current treatment paradigm. Addi-tionally, Gonzalez et al. solely focused on safety in terms of perioperative complication, mortality and/or morbidity, and regrowth and/or rebleeding of BBAs posttreatment without venturing to investigate which therapy (surgery vs endovascular treatment) was more efficacious. The analy-sis presented here, however, was expanded to include ef-ficacy in terms of aneurysm obliteration.
Szmuda et al. came to the ultimate conclusion that neither surgical nor endovascular therapy had an impact on clini-cal outcome, and the primary end point in their study was
FIG. 5. Funnel plots with included Duval and Tweedie’s trim and fill (full black point) for immediate (A) and follow-up (B) occlusion rates after surgical treatment.
Unauthenticated | Downloaded 08/27/21 10:37 PM UTC

S. S. Shah et al.
J Neurosurg Volume 127 • December 20171370
death.49 Their search timeframe was also shorter than the one used in our current study (2005–2015 vs 2013–2014). In addition, their paper offers no risk assessment or publi-cation bias assessment such as we have highlighted in our study. Most importantly though, our results contrast with those published by Szmuda et al. in that we suggest surgical management may have better aneurysm occlusion than endo-vascular therapy, especially immediately postprocedurally.
The strength of the evidence in our review seems to be robust. Through our assessment of publication bias by fun-nel plotting, there is some noted bias with regard to smaller articles that reported higher occlusion rates and better out-comes. However, that was to be expected, which is why we employed the Duval and Tweedie trim and fill technique to estimate the number of missing studies that might exist in our meta-analysis and the effect that these studies might have had on its results. After correcting for these missing studies, the point estimate of the overall effect size has been shown to be approximately correct, and coverage of the ef-fect size confidence intervals is substantially improved.10 With this extra technique to assess publication bias and adjust our calculated effect rates, the observed mean and the Duval and Tweedie’s adjusted mean were within only roughly 0.3%–6.8% points of each other (mean 3.5%).
The generalizability of this study is also robust. All pa-tients included in our meta-analysis had BBAs of the ICA
that were treated with commonly applied endovascular or surgical approaches. Furthermore, tests of heterogeneity revealed rather low Q and I2 values in most of the statisti-cal analyses we ran. And even in analyzing study cohorts with higher I2 values, the studies were only somewhat het-erogeneous, like with immediate aneurysm occlusion after endovascular procedures and neurological outcomes after surgery. We believe that these results can also be extrapo-lated to patients with similar thin-walled, delicate aneu-rysms. Supplementary study through clinical trial of the ef-ficacy and safety of endovascular versus surgical treatment for BBAs is definitely possible. In fact, a randomized trial in Europe, referred to as the Diversion of Flow in Intracra-nial Vertebral and Blood Blister-like Ruptured Aneurysms Trial (DIVERT), is ongoing but not recruiting patients. This trial looks to compare flow diversion to other com-monly used therapies, such as clipping, coiling, stenting, and parent artery occlusion, in patients with acute BBAs and dissecting intradural aneurysms. While the trial does not directly compare endovascular to surgical treatment, it is hoped that its results can be used to determine overall treatment efficacy and safety for patients with BBAs.
Study LimitationsThis systematic review and meta-analysis has a few
FIG. 6. Neurological outcomes in endovascularly (A) and surgically (B) treated patients.
Unauthenticated | Downloaded 08/27/21 10:37 PM UTC

Optimal treatment for blood-blister aneurysms of the ICA
J Neurosurg Volume 127 • December 2017 1371
limitations. First, none of the studies included in our anal-ysis is a randomized controlled trial. Without the benefit of randomization, there is always a possibility of selec-tion bias based on treatment. However, it is possible that some of this selection bias could have been controlled for at the treatment centers based on hypothesized clinical equipoise surrounding the treatment of BBAs. None of the studies in our analysis directly compared endovascular to surgical procedures in a case-control design either, which means that the comparison between the 2 treatment arms was based on pooled data from different studies. Second, there was marked variability in the ways that the included studies reported data, such as neurological outcome and occlusion. Some papers used the mRS to report neurologi-cal outcome while others used the GOS. Some studies did not include any information other than qualitative con-firmation of a good recovery. Even though there is some crossover between the different scales used (mRS Score 3 is approximately equal to GOS Score 4, moderate disabil-ity) and even though we believe that our proposed cutoff (mRS Score 0–2 or GOS Score 5 or qualitative equivalent) was appropriate, breaking our functional outcome scores into either a positive or a negative outcome may have led to
an incredibly generalized data point, which may not have been sensitive enough to emphasize discreet discrepancies between treatment arms. Additionally, it was difficult to discern data regarding unruptured versus ruptured BBAs in the included studies. While the natural history of rup-tured BBA is rather well documented, the natural course of unruptured BBA is still unclear. Nonetheless, we in-cluded both in our analysis and so this may represent a study limitation.
Third, some centers have different treatment inclina-tions than others. For example, some treatment centers prefer endovascular approaches to surgical approaches and save the latter as backup in case of endovascular fail-ure. Other institutions prefer a more multidisciplinary ap-proach. These predispositions can lead to selective bias toward or away from specific treatments. Furthermore, the long study period has seen a dramatic evolution in en-dovascular treatment strategies. There is a current trend toward flow diversion as the mainstay of endovascular therapy; however, the most recent literature suggests that stent-assisted coiling is the most common endovascular therapy offered to patients with BBAs, an observation
FIG. 7. Funnel plot with included Duval and Tweedie’s trim and fill (full black point) for neurological outcomes of endovascular treatment (A) and surgical treatment (B).
FIG. 8. Graphic representations of the most common complications for endovascular (blue) and surgical (red) procedures. A: Intraoperative complications. B: Postoperative complications. Tx = treatment. Figure is available in color online only.
Unauthenticated | Downloaded 08/27/21 10:37 PM UTC

S. S. Shah et al.
J Neurosurg Volume 127 • December 20171372
corroborated by multiple studies.16,49 Within the next few years, we may see a shift away from stent-assisted coiling and toward flow diversion, which would warrant further analysis and treatment considerations.
Finally, there was little uniformity in the way that the papers included in this review reported their results. We were able to extract patient demographic information and aneurysm data from only a handful of the included studies, making analysis impossible based on these vital criteria. Some papers included only information regarding aneu-rysm occlusion immediately after treatment, and others re-ported occlusion information only at follow-up. Some pa-pers did not even report occlusion information at all. Some articles did not include useable data regarding outcome scores. Thus, this observed heterogeneity in reporting data served as a main source of limitation in our study.
There were also limitations at the study level. Only 4 papers included information about both endovascular and surgical management. Ideally, all of the included papers would have contained data about both therapies. Addition-ally, some papers simply could not be statistically analyzed because of their small sample size (n = 1). Nonetheless, the plethora of case reports shows that BBAs are difficult to treat and that there is still a tremendous lack of informa-tion regarding their proper management. There may be a need to create a registry for patients treated for BBAs to further understand the differences in the natural history of ruptured versus unruptured lesions, as documentation of surgical and endovascular treatment effects.
ConclusionsBlood-blister aneurysms are a therapeutic challenge
with possibly disastrous outcomes even with state-of-the-art care. According to this systematic review and meta-analysis of BBAs of the ICA, surgical management offers superior aneurysm occlusion immediately after the pro-cedure and sustained occlusion at the follow-up. Endo-vascular procedures provide better functional outcomes than surgery but only by a moderate margin. Treatment decisions should be made only after careful consideration of the patient, the aneurysm, and the likelihood of a poor clinical outcome. A registry of patients treated for BBAs may be warranted to better document the natural course of the disease as well as treatment outcomes.
References 1. Abe M, Tabuchi K, Yokoyama H, Uchino A: Blood blister-
like aneurysms of the internal carotid artery. J Neurosurg 89:419–424, 1998
2. Ahn JY, Cho JH, Jung JY, Lee BH, Yoon PH: Blister-like aneurysms of the supraclinoid internal carotid artery: chal-lenging endovascular treatment with stent-assisted coiling. J Clin Neurosci 15:1058–1061, 2008
3. Başkaya MK, Ahmed AS, Ateş O, Niemann D: Surgical treatment of blood blister-like aneurysms of the supraclinoid internal carotid artery with extracranial-intracranial bypass and trapping. Neurosurg Focus 24(2):E13, 2008
4. Causin F, Pascarella R, Pavesi G, Marasco R, Zambon G, Battaglia R, et al: Acute endovascular treatment (< 48 hours) of uncoilable ruptured aneurysms at non-branching sites us-ing silk flow-diverting devices. Interv Neuroradiol 17:357–364, 2011
5. Chalouhi N, Zanaty M, Tjoumakaris S, Gonzalez LF, Hasan D, Kung D, et al: Treatment of blister-like aneurysms with the pipeline embolization device. Neurosurgery 74:527–532, 2014
6. Cho TG, Hwang SN, Nam TK, Park SW: Salvage surgi-cal treatment for failed endovascular procedure of a blood blister-like aneurysm. J Cerebrovasc Endovasc Neurosurg 14:99–103, 2012
7. Çinar C, Oran İ, Bozkaya H, Ozgiray E: Endovascular treat-ment of ruptured blister-like aneurysms with special refer-ence to the flow-diverting strategy. Neuroradiology 55:441–447, 2013
8. Consoli A, Nappini S, Renieri L, Limbucci N, Ricciardi F, Mangiafico S: Treatment of two blood blister-like aneurysms with flow diverter stenting. J Neurointerv Surg 4:e4, 2012
9. Doorenbosch X, Harding M: Primary treatment of a blood-blister-like aneurysm of the internal carotid artery with Guglielmi detachable coil embolisation. J Clin Neurosci 15:1276–1279, 2008
10. Duval S, Tweedie R: Trim and fill: A simple funnel-plot-based method of testing and adjusting for publication bias in meta-analysis. Biometrics 56:455–463, 2000
11. Ezaki Y, Takahata H, Kamada K, Baba S, Kaminogo M: An-eurysmal embolization of a blisterlike aneurysm of the inter-nal carotid artery: a case report and review of the literature. Surg Neurol 65:628–630, 2006
12. Fang YB, Li Q, Wu YN, Zhang Q, Yang PF, Zhao WY, et al: Overlapping stents for blood blister-like aneurysms of the in-ternal carotid artery. Clin Neurol Neurosurg 123:34–39, 2014
13. Fang YB, Li Q, Yang PF, Huang QH, Zhao WY, Xu Y, et al: Treatment of blood blister-like aneurysms of the internal ca-rotid artery with stent-assisted coil embolization. Clin Neu-rol Neurosurg 115:920–925, 2013
14. Farrell B, Godwin J, Richards S, Warlow C: The United King-dom transient ischaemic attack (UK-TIA) aspirin trial: final results. J Neurol Neurosurg Psychiatry 54:1044–1054, 1991
15. Gaughen JR Jr, Hasan D, Dumont AS, Jensen ME, McKen-zie J, Evans AJ: The efficacy of endovascular stenting in the treatment of supraclinoid internal carotid artery blister aneu-rysms using a stent-in-stent technique. AJNR Am J Neuro-radiol 31:1132–1138, 2010
16. Gonzalez AM, Narata AP, Yilmaz H, Bijlenga P, Radova-novic I, Schaller K, et al: Blood blister-like aneurysms: single center experience and systematic literature review. Eur J Radiol 83:197–205, 2014
17. Ihn YK, Kim SH, Sung JH, Kim TG: The efficacy of endo-vascular treatment of ruptured blood blister-like aneurysms using stent-assisted coil embolization. Interv Neuroradiol 18:432–441, 2012
18. Ishikawa T, Mutoh T, Nakayama N, Yasuda H, Nomura M, Kazumata K, et al: Universal external carotid artery to proxi-mal middle cerebral artery bypass with interposed radial artery graft prior to approaching ruptured blood blister-like aneurysm of the internal carotid artery. Neurol Med Chir (Tokyo) 49:553–558, 2009
19. Ishikawa T, Nakamura N, Houkin K, Nomura M: Pathologi-cal consideration of a “blister-like” aneurysm at the superior wall of the internal carotid artery: case report. Neurosur-gery 40:403–406, 1997
20. Jennett B, Bond M: Assessment of outcome after severe brain damage. Lancet 1:480–484, 1975
21. Joo SP, Kim TS, Moon KS, Kwak HJ, Lee JK, Kim JH, et al: Arterial suturing followed by clip reinforcement with circumferential wrapping for blister-like aneurysms of the internal carotid artery. Surg Neurol 66:424–429, 2006
22. Kalani MY, Zabramski JM, Kim LJ, Chowdhry SA, Mendes GA, Nakaji P, et al: Long-term follow-up of blister aneurysms of the internal carotid artery. Neurosurgery 73:1026–1033, 2013
23. Kamijo K, Matsui T: Acute extracranial-intracranial bypass
Unauthenticated | Downloaded 08/27/21 10:37 PM UTC

Optimal treatment for blood-blister aneurysms of the ICA
J Neurosurg Volume 127 • December 2017 1373
using a radial artery graft along with trapping of a ruptured blood blister–like aneurysm of the internal carotid artery. Clinical article. J Neurosurg 113:781–785, 2010
24. Kawashima A, Okada Y, Kawamata T, Onda H, Kubo O, Hori T: Successful treatment of a blood blister-like aneurysm of the internal carotid artery by trapping with a high-flow bypass. J Clin Neurosci 15:797–800, 2008
25. Kazumata K, Nakayama N, Nakamura T, Kamiyama H, Tera-saka S, Houkin K: Changing treatment strategy from clip-ping to radial artery graft bypass and parent artery sacrifice in patients with ruptured blister-like internal carotid artery aneurysms. Neurosurgery 10 (Suppl 1):66–73, 2014
26. Kim BC, Kwon OK, Oh CW, Bang JS, Hwang G, Jin SC, et al: Endovascular internal carotid artery trapping for ruptured blood blister-like aneurysms: long-term results from a single centre. Neuroradiology 56:211–217, 2014
27. Kim BM, Chung EC, Park SI, Choi CS, Won YS: Treatment of blood blister-like aneurysm of the internal carotid artery with stent-assisted coil embolization followed by stent-with-in-a-stent technique. Case report. J Neurosurg 107:1211–1213, 2007
28. Korja M, Rautio R, Valtonen S, Haapanen A: Primary treat-ment of ruptured blood blister-like aneurysms with stent-assisted coil embolization: report of two cases. Acta Radiol 49:180–183, 2008
29. Kubo Y, Ogasawara K, Tomitsuka N, Otawara Y, Watanabe M, Ogawa A: Wrap-clipping with polytetrafluoroethylene for ruptured blisterlike aneurysms of the internal carotid artery. Technical note. J Neurosurg 105:785–787, 2006
30. Lee BH, Kim BM, Park MS, Park SI, Chung EC, Suh SH, et al: Reconstructive endovascular treatment of ruptured blood blister-like aneurysms of the internal carotid artery. J Neuro-surg 110:431–436, 2009
31. Lee JW, Choi HG, Jung JY, Huh SK, Lee KC: Surgical strat-egies for ruptured blister-like aneurysms arising from the internal carotid artery: a clinical analysis of 18 consecutive patients. Acta Neurochir (Wien) 151:125–130, 2009
32. Lim YC, Kim BM, Suh SH, Jeon P, Kim SH, Ihn YK, et al: Reconstructive treatment of ruptured blood blister-like aneu-rysms with stent and coil. Neurosurgery 73:480–488, 2013
33. Mason AM, Cawley CM, Barrow DL: Surgical management of intracranial aneurysms in the endovascular era: review article. J Korean Neurosurg Soc 45:133–142, 2009
34. McLaughlin N, Laroche M, Bojanowski MW: Surgical management of blood blister-like aneurysms of the internal carotid artery. World Neurosurg 74:483–493, 2010
35. Meling TR, Sorteberg A, Bakke SJ, Slettebø H, Hernesniemi J, Sorteberg W: Blood blister-like aneurysms of the internal carotid artery trunk causing subarachnoid hemorrhage: treat-ment and outcome. J Neurosurg 108:662–671, 2008
36. Molyneux AJ, Kerr RS, Yu LM, Clarke M, Sneade M, Yar-nold JA, et al: International subarachnoid aneurysm trial (ISAT) of neurosurgical clipping versus endovascular coil-ing in 2143 patients with ruptured intracranial aneurysms: a randomised comparison of effects on survival, dependency, seizures, rebleeding, subgroups, and aneurysm occlusion. Lancet 366:809–817, 2005
37. Ogawa A, Suzuki M, Ogasawara K: Aneurysms at non-branching sites in the surpaclinoid portion of the internal carotid artery: internal carotid artery trunk aneurysms. Neu-rosurgery 47:578–586, 2000
38. Otani N, Takasato Y, Masaoka H, Hayakawa T, Yoshino Y, Yatsushige H, et al: Clinical and radiological findings and surgical management of ruptured aneurysms at the non-branching sites of the internal carotid artery. J Clin Neurosci 16:1018–1023, 2009
39. Park JH, Park IS, Han DH, Kim SH, Oh CW, Kim JE, et al: Endovascular treatment of blood blister-like aneurysms of the internal carotid artery. J Neurosurg 106:812–819, 2007
40. Plowman RS, Clarke A, Clarke M, Byrne JV: Sixteen-year single-surgeon experience with coil embolization for rup-tured intracranial aneurysms: recurrence rates and incidence of late rebleeding. Clinical article. J Neurosurg 114:863–874, 2011
41. Princiotta C, Dall’olio M, Cirillo L, Leonardi M: Staged treatment of a blood blister-like aneurysm with stent-assisted coiling followed by flow diverter in-stent insertion. A case report. Interv Neuroradiol 17:365–370, 2011
42. Rankin J: Cerebral vascular accidents in patients over the age of 60. II. Prognosis. Scott Med J 2:200–215, 1957
43. Rasskazoff S, Silvaggio J, Brouwer PA, Kaufmann A, Nis-tor A, Iancu D: Endovascular treatment of a ruptured blood blister-like aneurysm with a flow-diverting stent. Interv Neuroradiol 16:255–258, 2010
44. Satoh A, Sugiyama T, Hongo K, Kakizawa Y, Ishihara S, Matsutani M: Nationwide surveillance of IC anterior (or dor-sal) wall aneurysm: with special reference to its dissecting nature. Acta Neurochir Suppl 103:51–55, 2008
45. Segal DH, Sen C, Bederson JB, Catalano P, Sacher M, Stoll-man AL, et al: Predictive value of balloon test occlusion of the internal carotid artery. Skull Base Surg 5:97–107, 1995
46. Sekula RF Jr, Cohen DB, Quigley MR, Jannetta PJ: Primary treatment of a blister-like aneurysm with an encircling clip graft: technical case report. Neurosurgery 59 (1 Suppl 1):ONSE168, 2006
47. Silva JC, Faquini IV, Kitamura MA, Azevedo-Filho HR: Internal carotid artery blood blister-like aneurysm. Arq Neu-ropsiquiatr 66 (3A):563–565, 2008
48. Sim SY, Shin YS, Cho KG, Kim SY, Kim SH, Ahn YH, et al: Blood blister-like aneurysms at nonbranching sites of the internal carotid artery. J Neurosurg 105:400–405, 2006
49. Szmuda T, Sloniewski P, Waszak PM, Springer J, Szmuda M: Towards a new treatment paradigm for ruptured blood blister-like aneurysms of the internal carotid artery? A rapid systematic review. J Neurointerv Surg 8:488–494, 2016
50. Tekkök IH, Bakar B: Ruptured blister-like aneurysm of distal internal carotid artery: a distinct entity. Turk Neurosurg 18:439–445, 2008
51. Yanaka K, Meguro K, Nose T: Repair of a tear at the base of a blister-like aneurysm with suturing and an encircling clip: technical note. Neurosurgery 50:218–221, 2002
52. Yu-Tse L, Ho-Fai W, Cheng-Chi L, Chu-Mei K, Yi-Chou W, Tao-Chieh Y: Rupture of symptomatic blood blister-like an-eurysm of the internal carotid artery: clinical experience and management outcome. Br J Neurosurg 26:378–382, 2012
DisclosuresThe authors report no conflict of interest concerning the materi-als or methods used in this study or the findings specified in this paper.
Author ContributionsConception and design: Peterson, Shah, Gersey, Elhammady. Acquisition of data: Shah, Gersey, Nuh, Ghonim. Analysis and interpretation of data: Shah, Gersey, Nuh, Ghonim, Elhammady. Drafting the article: Shah, Gersey, Nuh, Elhammady. Critically revising the article: all authors. Reviewed submitted version of manuscript: all authors. Approved the final version of the manu-script on behalf of all authors: Peterson. Statistical analysis: Shah, Gersey. Administrative/technical/material support: Peterson, Elhammady. Study supervision: Peterson.
CorrespondenceEric C. Peterson, Lois Pope LIFE Center, 2nd Fl., 1095 NW 14th Terrace, Miami, FL 33136. email: [email protected].
Unauthenticated | Downloaded 08/27/21 10:37 PM UTC