Embed Size (px)
Citation preview

Netherlands Journal of Critical Care
NETH J CRIT CARE - VOLUME 14 - NO 1 - FEBRUARY 201036
Introduction
Persistent hypotension is a common problem in intensive care unit
(ICU) treatment. Hypotension is caused either by a low systemic
vascular resistance (sepsis, spinal shock, vasodilatory medica-
tion), low stroke volume (hypovolaemia, adrenal insufficiency,
tachyarrhythmia, tamponade, high PEEP, pulmonary embolism,
right and left sided heart failure, valvular dysfunction) or low heart
rate. Chronic hypotension and inotropic dependency is less com-
mon. Treatment can be challenging when blood pressure remains
low due to continuous or intermittent haemodialysis.
This report covers two hypotensive patients who are both suf-
fering from renal insufficiency with concurrent heart disease. In
addition, the introduction of midodrine therapy is discussed.
Case A
A 60-year-old man was referred to the department of internal
medicine because of a six-month history of fatigue and recurrent
infections. His medical history was positive for chronic obstruc-
tive pulmonary disease and he was not taking any medication.
After bone marrow examination, the diagnosis of multiple my-
eloma, stage Ia according to the Durie-Salmon staging system,
was made. During induction chemotherapy and autologous stem
cell transplantation the patient gained weight and developed
shortness of breath. Transthoracic echocardiography (E/A < 1;
Deceleration time > 220 msec; E’ 6.4 cm/sec; E/E’ 13.8) and
cardiac MRI (Figure 1 and http://www.nvic.nl/njcc.php) demon-
strated severe hypertrophy of the left and right ventricles as well
as a hypertrophic interatrial septum, causing diastolic dysfunc-
tion with delayed relaxation. The late enhancement pattern was
highly suggestive of cardiac amyloidosis. Furthermore, the pa-
tient developed severe renal insufficiency that required the start
of intermittent haemodialysis which was complicated by severe
hypotension. The patient was transferred to the ICU and treat-
ment with norepinephrine and continuous venovenous haemo-
filtration (CVVH) was started. After 3 weeks a peritoneal dialysis
(PD) catheter was implanted and PD was started. Despite the
discontinuation of CVVH the patient remained dependent on in-
travenous vasopressor therapy. Oral ibopamine was added to
the medication but the patient developed ventricular tachycardia
within 24 hours. Following this the patient was started on oral
caffeine, which was soon discontinued due to side effects. Fi-
nally, we decided to introduce oral midodrine which was started
at a low dose of 2.5 mg three times daily (tid). After more than 60
days, the patient was weaned off norepinephrine and discharged
from the ICU using midodrine 10 mg tid.
Case B
A 76-year-old man was admitted to the ICU following aortic valve
replacement. He had a medical history of coronary surgery (1978),
redo-coronary surgery (1991), severe aortic valve calcification
and stenosis, reduced left ventricular function, and renal failure
due to familial polycystic kidney disease. Intermittent haemodi-
alysis was started in May 2008. One day post-surgery CVVH was
initiated. However, profound hypotension associated with CVVH
therapy forced us to start intravenous norepinephrine which was
later replaced by dopamine as the patient experienced severe
peripheral vasoconstriction. After 2 weeks the dopamine treat-
ment was tapered. However, the patient’s systolic blood pres-
sure dropped below 55-60 mm Hg. Intravenous inotropic treat-
ment was reintroduced. Three days later, midodrine 2.5 mg tid
was initiated and the patient was weaned from inotropic support.
CVVH therapy was terminated and after 33 days in the ICU the
patient was discharged. The final invasive blood pressure before
discharge was 124/69 mm Hg.
RMA van de wal1, MJ Swaans1, VH Deneer2, H Biemond-Moeniralam3,4, AJ Meinders3,4
1 Department of Cardiology, St. Antonius Hospital, Nieuwegein, The Netherlands
2 Department of Clinical Pharmacy, St. Antonius Hospital, Nieuwegein, The Netherlands
3 Department of Anaesthesiology, Intensive Care and Pain Management, St. Antonius Hospital, Nieuwegein, The Netherlands
4 Department of Internal Medicine, St. Antonius Hospital, Nieuwegein, The Netherlands
Abstract - Hypotension is a common clinical problem in the intensive care unit, and intravenous inotropic or vasopressor therapy is
often necessary. In dialysis-dependent patients the process of tapering the dose of intravenous inotropics can be complicated by refrac-
tory hypotension. The two cases described in this report outline the successful introduction of midodrine, an oral α1-receptor agonist,
in two patients suffering from refractory hypotension.
Keywords - midodrine, hypotension, intensive care, inotropic therapy
Copyright © 2010, Nederlandse Vereniging voor Intensive Care. All Rights Reserved. Received July 2009; accepted November 2009
Midodrine for ICU patients suffering from refractory hypotension
CASE REPORT
RMA van de Wal
E-mail: [email protected]
Correspondence
2010 NVIC_NJCC 01 v1.indd 36 27-01-2010 12:01:16

NETH J CRIT CARE - VOLUME 14 - NO 1 - FEBRUARY 2010 37
Netherlands Journal of Critical Care
Midodrine for ICU patients suffering from refractory hypotension
Discussion
Common causes of hypotension in patients in the ICU are sep-
sis, the use of vasodilatory medication, and adrenal insufficiency.
Both patients in this report did not use antihypertensive or va-
sodilatory medication. Furthermore, infection was ruled out as a
possible cause of hypotension and the blood pressure of both
patients did not react to treatment with hydrocortisone.
Cardiac involvement is frequent in systemic amyloidosis, of-
ten leading to diastolic dysfunction and restrictive cardiomyopa-
thy [1]. In addition, amyloidosis may induce dysfunction of the
autonomic nervous system. In case report A, we present a patient
suspected of cardiac amyloidosis who simultaneously suffered
from end stage renal failure, initially leading to CVVH and later
to PD. Both amyloidosis and haemodialysis have been associ-
ated with hypotension. In this particular case, ultrafiltration in-
duced plasma depletion, probably causing inadequate filling of
a hypertrophic heart muscle, which when combined with an im-
paired compensatory increase in sympathetic tone led to severe
hypotension [2]. In order to induce appropriate vasoconstriction
norepinephrine was started. After unsuccessful oral treatment
with the dopamine agonist ibopamine and the adenosine recep-
tor antagonist caffeine, this patient (A) was treated with mido-
drine. Norephinephrine was successfully discontinued. In case B,
the pathophysiological mechanism underlying the patient’s low
blood pressure also involved diastolic dysfunction. However, in
this patient hypertrophy and impaired relaxation of the left ven-
tricle were caused by severe aortic stenosis. Furthermore, his left
ventricular systolic function was impaired.
Instead of using sympathicomimetic amines in the initial
stage of stabilization, treatment with the phosphodiesterase III
inhibitor enoximone could have been effective for this patient.
Given the underlying pathophysiological considerations, the
α-sympathicomimetic properties of norepinephrine were pre-
ferred over the vasodilatory effects of enoximone in patient A [3].
Theoretically, the calcium sensitizer levosimendan could become
an alternative therapy for similar patients in the future. It appears
to be more beneficial and it has also proved to be energetically
less disadvantageous for the myocardium than existing inotropic
agents [4]. Both enoximone and levosimendan could potentially
have been effective in the stabilization of patient B as his left
ventricular function was impaired. After stabilization, patient B
was treated with low-dose midodrine and he was able to resume
intermittent dialysis after a post-operative interval of CVVH.
Midodrine is a selective α1-receptor agonist and is a prod-
rug of 1-(2´5´-dimethoxyphenyl)-2-aminoethanol (DMAE) that
combines glycine by a peptide bond. After oral administration,
the bioavailability of midodrine is reported to be approximately
100%, whereas that of DMAE is approximately 50%. The me-
tabolite increases peripheral resistance by inducing constriction
of both arterial and venous capacitance vessels and it prevents
venous pooling of the blood thus increasing blood pressure. Its
action is identical to that of other α1-adrenoceptor stimulants,
such as phenylephrine. Peak levels of the active metabolite in
serum are achieved in 1 hour and its half-life is approximately 3
hours. In patients with end stage renal disease, the half-life will
be prolonged three times. Importantly, haemodialysis effectively
removes both the prodrug and active metabolite [5]. In patients
with a normal renal function the usual starting dose is 2.5 mg tid.
The dose can be gradually increased up to 10 mg tid. In a previ-
ous report, the pharmacokinetic characteristics of the prodrug
and its active metabolite in a dialysis patient approximated those
reported for patients with normal renal function [6]. This seems to
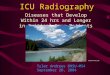
Figure 1. Steady-state free precession (SSFP) image during a)
diastole and b) systole showing severe thickened left ventricular
walls with preserved systolic function (kissing walls in systole).
There is also hypertrophy of the right ventricle and interatrial
septum and pleural effusion.
A
B
2010 NVIC_NJCC 01 v1.indd 37 27-01-2010 12:01:17

Netherlands Journal of Critical Care
NETH J CRIT CARE - VOLUME 14 - NO 1 - FEBRUARY 201038
RMA van de Wal, MJ Swaans, VH Deneer, H Biemond-Moeniralam, AJ Meinders
1 Falk, RH. Diagnosis and management of the cardiac amyloidoses. Circulation
2005;112:2047-2060.
2 Daugirdas, JT. Pathophysiology of dialysis hypotension: an update. Am. J. Kidney
Dis. 2001;38:S11-S17.
3 Lehtonen LA, Antila S, Pentikainen PJ. Pharmacokinetics and pharmacodynamics of
intravenous inotropic agents. Clin. Pharmacokinet. 2004;43: 187-203.
4 Fuhrmann JT, Schmeisser A, Schulze MR, Wunderlich C, Schoen SP, Rauwolf T,
Weinbrenner C, Strasser RH. Levosimendan is superior to enoximone in refractory car-
diogenic shock complicating acute myocardial infarction. Crit Care Med. 2008;36: 2257-
2266.
5 Blowey DL, Balfe JW, Gupta I, Gajaria MM, Koren G. Midodrine efficacy and phar-
macokinetics in a patient with recurrent intradialytic hypotension. Am. J. Kidney Dis.
1996;28: 132-136.
6 Blowey DL, Balfe JW, Gupta I, Gajaria MM, Koren G. Midodrine efficacy and phar-
macokinetics in a patient with recurrent intradialytic hypotension. Am. J. Kidney Dis.
1996;28: 132-136.
7 Angeli P, Volpin R, Gerunda G, Craighero R, Roner P, Merenda R, Amodio P, Sticca
A, Caregaro L, Maffei-Faccioli A, Gatta A. Reversal of type 1 hepatorenal syndrome with
the administration of midodrine and octreotide. Hepatology 1999;29: 1690-1697.
8 H.Lahrmann, P.Cortelli, M.Hilz, C.J.Mathias, W.Struhal, M.Tassinari. 2006. EFNS
guidelines on the diagnosis and management of orthostatic hypotension. Eur. J. Neurol.
13: 930-936.
9 Cruz DN, Mahnensmith RL, Brickel HM, Perazella MA. Midodrine is effective and safe
therapy for intradialytic hypotension over 8 months of follow-up. Clin. Nephrol. 1998; 50:
101-107.
10 Fang JT, Huang CC. Midodrine hydrochloride in patients on hemodialysis with
chronic hypotension. Ren Fail. 1996;18: 253-260.
11 Prakash S, Garg AX, Heidenheim AP, House AA. Midodrine appears to be safe and
effective for dialysis-induced hypotension: a systematic review. Nephrol. Dial. Transplant.
2004;19: 2553-2558.
References
suggest that similar dosing schedules could be used for patients
on dialysis. In patients with end stage renal disease who are not
on dialysis, the dose is not yet clear and great care should be
taken when midodrine is administered in these patients. Several
side effects have been reported, such as scalp paraesthesias,
heartburn, flushing, headache, urinary retention, supine hyper-
tension, neck soreness and weakness. However, please note that
none of our patients experienced any of these side effects.
Midodrine is known to increase glomerular pressure and has
been used therapeutically to reverse endogenous vasodilators
that result in low glomerular pressure in hepatorenal syndrome
[7]. Furthermore, midodrine has been prescribed for the treat-
ment of neurogenic orthostatic hypotension in patients with
spinal cord injury, for patients with neurocardiogenic syncope,
for the treatment of hypotension associated with carotid artery
stenting, and for several other indications [8]. Although still under
investigation, midodrine has also been studied in the treatment
of dialysis induced hypotension [9,10]. Unfortunately, these stud-
ies were small and not always randomized. While there are no
known studies in patients on peritoneal dialysis, trials in patients
on haemodialysis have shown that midodrine is safe and can be
useful in the treatment of symptomatic dialysis-related hypoten-
sion [11]. To our knowledge no studies have been published that
describe the use of midodrine as a replacement therapy for intra-
venous inotropic or vasopressive agents.
Conclusion
In these case reports, we have described the successful intro-
duction of midodrine as an oral alternative for low-dose intrave-
nous inotropic or vasopressive therapy in patients in the intensive
care unit.
2010 NVIC_NJCC 01 v1.indd 38 27-01-2010 12:01:17