Embed Size (px)
Citation preview

Mild Traumatic Brain Injury in Military Veterans: Clinical Implications for Assessment &
Treatment
Karen Gallagher, Ph.D., CCC-SLP

High Cognitive Demands of CollegeToday’s discussion will largely focus on this growing group of military veterans
2.6 million deployed to Iraq and Afghanistan over the past 17+ years 1
1.7 million have left military service and another quarter of a million more per year will do so over the next few years 1
The majority enter college after separation from service 2
1. Chairman’s Office on Reintegration Report, 2014; 2. Steele, J.L., Salcedo, N., & Coley, J. (November, 2010)

The number of military affiliated students at ASU are rising
Number of student veterans has increased drastically on a national level
In 2009 there were approximately 500,000 and in 2013 there were over 1 million
National Center for Education Statistics, 2016

Who are Student Veterans?
• Mostly male• Females are over represented• Older• Almost half have children• Almost half are married• Over 60% are first in their families to go to college
There are unique challenges in this population
ASU State Press, 2015

There is disagreement about academic success in military veteran college students
Student Veterans of America: 72% academic success among veterans (2017)
Only 51% of veterans graduate vs. 59% of non-veterans (National Center for Education Statistics, 2013)
There is an 88% attenuation rate (Briggs, 2012)

6
1) Defense and Brain Injury Center, 2015; 2) U.S. Department of Veterans Affairs; Dolan et al., 2012; 3) National Alliance on Mental Illness; 4) Lew et al., 2010; 5) CDC; 6) U.S. Department of Veterans Affairs; 7) Anxiety and Depression Association of America; 8) Lew et al., 2010
Civilians~8% (adult) 5
6.8% 6
6.7% 7
18% yearly 7
Veterans20 - 33% 1
14 - 44% 2
14% 3
??
TBI (mTBI)PTSDepressionAnxiety Disorders
PTS within mTBI ??33 – 39%8
Service-Related Conditions

Results from Azuma & Gallagher presented at ICCDC, 2017
Condition Veterans (N=138)
Civilians (N=213)
Group Differences
Depression 24.3% 15.0% χ2=4.38, p=.036*PTSD 11.6% 1.4% χ2=17.00,
p<.001**mTBI (Diagnosed or Suspected)
25.4% 24.9% χ2<1
mTBI Group Only N=35 N=53mTBI + Depression 31.4% 9.4% χ2=6.86, p=.009**mTBI + PTSD 28.6% 0.0% χ2=17.08,
p<.001**
Table 1. Self-Reported Rates of Depression, PTSD, and mTBI in the Veteran and Civilian Groups

Challenges in Assessment and Treatment of Cognitive Symptoms Related to mTBI in Military Veterans
Military Culture
Injury Environment
TransitionOther
Conditions

What is Military Culture?
Military Culture

Defined by a unique vocabulary, rules, and belief systems (Reger et al., 2007)
Attitude that seeking healthcare services is an indication of weakness
Barrier to care
Military Culture

Injury Environment

Combat
Training
• Loss of life and limb• Delay the mission• Delay discharge/return home
• “Recycled”• Failure
Injury Environment
Barrier to care

Transition

Transition
Military-to-Civilian Transition can create stress and anxiety
Mobbs, M.C., Bonanno, G.A., (2018). Behond war and PTSD: The crucial role of transition stress in the lives of military veterans. Clinical Psychology Review, 59, 137-144.
Identity
Moral Injury
Civilian-military divide
Stereotypes
Barrier to care

Other Conditions
Commonly Reported Overlapping Symptoms
mTBI
PTS
Depression
Anxiety Disorders
Memory
Attention
Sleep
Anxiety

Overlapping symptoms of depression, anxiety and PTS and the frequent concomitance with mTBI, provides one of the largest hurdles in assessment of unremitting mTBI symptoms (Karr et al., 2014; Lange et al., 2012)
Other Conditions
Barrier to care

Military Culture
Injury Environment
TransitionOther
Conditions
Delay in Reporting
Absence of Reporting
Misdiagnosis

Questions&
Discussion
Military Culture
Injury Environment
TransitionOther
Conditions

Long-term Cognitive Symptoms related to mTBI in Military Veterans
• Memory• Attention• Executive Function• Speed of Processing
Symptoms present more than a year after injury

“…in contrast to the prevailing view that most symptoms of concussion are resolved within 3 months post injury, approximately half of individuals with a single mTBI demonstrate long-term cognitive impairment.”
Mcinnes, K., Friesen, C.L., MacKenzie, D.E., Westwood, D.A., and Boe, S.G. (2017). Mild Traumatic Brain Injury (mTBI) and chronic cognitive impairment: A scoping review. PLoS OnE 12(4).

Assessment of Unremitting mTBI Symptoms
Concomitant PTSD or Depression account for the deficits (Lang et al., 2012; Seal, 2016; Verfaellie et al., 2014)
No long-term neuropsychological deficits associated with mTBI (Storzbach et al., 2015)
Based on commonly used clinical neuropsychological assessments
Symptom report related to mTBI is often dismissed due to lack of neuropsychological test evidence (Spencer et al., 2010; Verfaellie et al., 2014)
Despite subjective reports of long-term symptoms related to mTBI in military veterans… (Hartikainen et al., 2010; Schneiderman et al., 2008)

Why don’t standardized assessments consistently capture subtle deficits related to chronic mTBI?
• Tests were not designed to measure chronic cognitive deficits related to mTBI
• Standardized to elicit the best possible performance
• Do not reflect real-world demands that may exacerbate “subtle” deficits
• Performance may only be affected when the task is challenging and placing more demands on the cognitive system (Cicerone, 2009)

Measuring MemoryDigit Span
• Forward• Backward
Word Lists• AVLT• Paired Associates
For the most part, these are decontextualized rote memory tasks that don’t reflect real-world demands

Our studies have included traditional clinical tasks, experimental tasks and self-report of symptoms
• Rote memory• Episodic memory tasks• Working memory• Executive function• Decision making• Attention

• Completed at home• 107 questions• Demographic information• Military, Medical, and Educational Background
25
Online Questionnaire

VETERANS WITH mTBI: Utilizing Self-Report Information
Krug & Turkstra (2015)

Comprehensive survey as part of the assessment
Circumstances
Situational Checklist
Self-assessment and ratingMemoryAttentionAnxiety
VETERANS WITH mTBI: Asking the Right Questions
Military Service

• Beck Depression Inventory• Beck Anxiety Inventory • Informal Memory and Attention Ratings
28
Self-Assessment and Rating
“Compared to other people my age, my OVERALL memory is:5 = much better4 = slightly better3 = the same2 = slightly worse1 = far worse”

History of Military Service
• Enlistment length
• Military Occupation
• Deployment
This information can lead to more specific questions and can direct your assessment and referral decisions

Diagnosed and Suspected Head InjuriesDescription of Circumstances
Who diagnosed the injury?
What caused the injury?
Where did the injury happen?
Suspected TBI?Symptoms
Immediately experienced
Still experiencing Mayo Classification System for Traumatic Brain Injury Severity (Malec et al., 2008)

In-Person Testing
At ASU
• Approximately 2 to 2 ½ hours
• Mostly computerized tasks

Commonly Used Neuropsychological Tasks
• Digit Span• Trail Making
Performance on these tasks were not related to mTBI or PTSD
Did provide evidence of effort

Reliable Digit Span Score (RDS): combining the highest span set where both trials were accurately recalled in both the forward and backward condition1
1) Heinely et al., 2005; Loring, Goldstein, Chen, Drane, Lah, Zhao, & Larrabee, 20162) Schroeder, Twumasi-Ankrah, Baade, & Marshall, 2012
Digit Span as a Measure of Effort
An RDS of <7 is considered evidence of lack of effort2
In my study no participant earned an RDS below 10
33

Documenting Reported Deficits
We need ecologically valid, complex tasks that:
• Shift from simple memory tasks• Tasks should mirror real-world demands• Tasks should tap higher-order cognitive processes

Memory in Real Life
• Stories • Lectures• Conversations• Events
This type of memory is complex, requiring sequencing and recall of semantic information

Narrative Recall Tasks
Logical Memory I (Immediate)Participants were told two stories.After each story, the participant was asked to retell the story “in as much detail and using as many of the same words as possible.”
Logical Memory II (Delayed) After a 20-30 minute delay, the participant was asked to retell each story.
WMS-IV (Wechsler, 2009)
Gallagher, K., & Azuma, T. (2018). Analysis of story recall in military veterans with and without mild traumatic brain injury: Preliminary results. American Journal of Speech-Language Pathology, 27(1S), 485-494.

Control Group(N=42)
mTBI Group(N=22)
Females 13 (31%) 2 (9%)
Mean Age (yrs) 31.7 (6.5) 32.9 (7.3)
PTSD 5 (12%) 9 (41%)
Depression 11 (26%) 7 (32%)
Anxiety 24 (57%) 16 (73%)
Study Participants

Results
A Mixed-factor Analysis of Covariance (ANCOVA) was conducted on the data.
Delay (Immediate vs. Delayed): Within-subjects variable
Group (mTBI vs. Control): Between-subjects variablePTS, Depression: Covariates

This interaction was significant even when PTS and Depression were included as covariates.
PTS: F (1, 60) = 2.57, p = .114Depression: F (1, 60) = 2.70, p = .106
Significant main effect of Delay (F(1,60) = 44.49, p < .001, ηp
2 = .43) Significant Delay X Group interaction
(F(1,60) = 5.8, p = .019, ηp2 =.088)
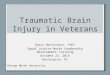
Significant Findings

LM 1: Immediate Condition
Mea
n Sc
ores
No group difference
(t<1)
10
15
20
25
30
35
Control mTBI

t (62) = 1.97, p =.043
Mea
n Sc
ores
LM 2: Delayed Condition
10
15
20
25
30
35
Control mTBI

42
• Widely used in both clinical and healthy populations (Lezak et al., 2012)
• Measure higher-order cognitive skills (Bagneux et al., 2013; Cui et al., 2015)
• Shown to be sensitive to deficits associated TBI (Bechara, 2007)
including risk-taking
Computerized using PEBL version 0.14 (Meuller & Piper, 2014)
Decision Making: The Iowa Gambling Task Bechara et al., 1994

43

44
Significant: mTBIβ = -.264, t = -2.05, p = .045
The regression model was significant (F (1,56) = 4.50, p = .045)
Multiple Regression AnalysisDependent Variable: Advantageous Deck Score (Low Risk decks) – (High Risk decks)Predictor Variable: mTBI

45
Trials were divided into blocks of 201
1. Based on conventional scoring methods for the IGT, (Bechara, 2007; Bagneux et al., 2013; Cotrena et al., 2014; Brenner et al., 2015)
2 (Group: Control vs. mTBI) X 4 (Block Advantageous Deck Selection Score for Blocks 2, 3, 4, 5) mixed-factor Analysis of Variance (ANOVA)

46
-1
0
1
2
3
4
5
6
7
8
9
10
11
Block 2 Block 3 Block 4 Block 5
ControlmTBI
Mea
n Ad
vant
ageo
us D
eck
Scor
e
* Denotes significantly different from Block 2 (p<.008)
There was a significant main effect of Block (F(3, 165)=7.34 p<.001, partial ɳ2=.118)
No significant effect of Group (F(1,55)=2.29, p=.136, partial ɳ2=.04)
Marginally significant Block X Group interaction (F(3,165)=3.91, p=.053 partial ɳ2=.066)
Healthy control group, there was a significant effect of Block (F(3,105)=12.33, p<.001)mTBI group no effect of Block (F<1)
*
**

050403070908WRONG!
Visual Serial Addition

Longer task
Stress inducing
Time pressure (4 seconds)
Aversive feedbackWRONG!TOO SLOW!
Requires Updating and Inhibition (Executive Function Skills)

Results
Group (Control vs. mTBI): Between-subjects variable
Quartile (1, 2, 3, 4): Within-subjects variable
PTS: Covariate
A Mixed-factor Analysis of Covariance (ANCOVA)
The trials were divided into quartiles (25 trials per quartile).
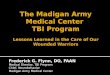
Accuracy
Significant effect of Quartile (F(3, 150)=4.86, p=.003, ɳp2=.089)
No significant effect of Group (F(1,50)=1.68, p=.201, ɳp2 =.033)
Significant Quartile X Group interaction (F(3,150)=3.08, p=.029, ɳp2 =.058)

0.6
0.65
0.7
0.75
0.8
0.85
0.9
1st Quartile 2nd Quartile 3rd Quartile 4th Quartile
Mea
n Ac
cura
cy
ControlmTBI
**
Control : No effect of Quartile (F<1)mTBI: Significant effect of Quartile (F(3,54)=5.18, p=.003, ɳ2
p =.224)
* Compared to 2nd quartile, p<.008

51
Valid and reliable working memory measures (Unsworth et al., 2005; Conway et al., 2005)
Measure higher-level skills (Unsworth & Engle, 2007)
Operation Span Task (Turner & Engle, 1989)
Experimental Measure of Complex Verbal Memory Span

( 3 * 4) – 4 = ?
Set sizes 4-6Possible Score range = 0-30Total Score = Total Correct
Computerized using E-Prime 2.0 software (Psychology Software Tools, Pittsburgh, PA)52
FK6
True False
Recall the letters in the order you saw them
Operation Span Task, Turner & Engle, 1989
Computerized Operation Span Task

Data presented by Gallagher, Azuma, Bacon, and Ingram at INS Conference 2019, New York City

Correlational analyses were used to examine the relationship between commonly reported service-related conditions/self-ratings (mTBI, PTS, Memory Rating, BDI) and Operation Span Score


When evaluating cognitive skills in military veterans with mTBI it is important to:
Consider the unique nature of military cultureHow it impacts report of injury
Consider the environmentHow it may delay diagnosisWhy the mTBI may be more traumatic
Consider possible service-related concomitant disorders Overlapping symptoms complicate assessmentReferrals may be needed
Overview
Consider the impact of transition Which support systems can be activated

There is emerging research that provides support for the validity of veterans’ self-assessments (Krug & Turkstra, 2015)
We can’t dismiss their symptom reports based on simple memory tests.
Researchers and clinicians are responsible for finding the right tests.
If we fail to document existing memory impairments, veterans don’t get needed services

Treatment & Treatment Resources
mTBI
PTS
Depression
Anxiety Disorders
Memory
Attention
Sleep
Anxiety
Transdisciplinary care is necessary

At ASU:
Grant-funded Veteran Specialty Clinic in the Speech and Hearing Clinic
Collaboration with the Pat Tillman Veteran Center
Specialized training given to the Disability Resource Center
Collaboration with the Counseling Center

Teammates vs. Expert-Patient Relationship
• Cognitive Coaching• Motivational Interviewing• Respects military values • Considers the transition experience• Vocationally/Academically relevant
Kennedy, M.R.T. (2017). Coaching College Students with Executive Function Problems. New York, NY: Guilford Press.

Veteran Specialty Clinic
Veterans self-select for intervention regardless of diagnosis
They complete 7-10 one-hour sessions with a graduate clinician supervised by me

During the initial session Veterans: Identified executive skills strengths and
weaknesses using the adult version of the Executive Skills Checklist1
Provided course information, work schedules, samples of notes, and descriptions of organization and studying strategies
Dawson, Peg, & Guare, Richard. (2012). Coaching Students with Executive Skills Deficits. Practical Intervention in the Schools Series (Vol. 20). Guilford Press. 72 Spring Street, New York, NY 10012.

During weekly sessions Veterans: Identified goals related to academic success, steps
to achieving goals, and barriers to achieving goals Identified memory, attention, and organization
strategies to be used during the week and defined the academic areas where those strategies would be applied
Reviewed strategy use and effectiveness and identified reasons for success or lack of success
Revised strategy use

During weekly sessions, Clinicians: Established a teammate rapport (vs. expert –
patient) Offered evidence-based organization, memory,
attention, and active studying strategy options for application on existing courses
Used motivational interviewing techniques to facilitate participant exploration and self-discovery of barrier behaviors and attitudes

Working Group to Develop a Clinician’s Guide to Cognitive Rehabilitation in mTBI: Application for Military Service Members and Veterans. (2016). Clinician’s guide to cognitive rehabilitation in mild traumatic brain injury: Application for military service members and veterans. Rockville, MD: American Speech-Language-Hearing Association. Available from http://www.asha.org/uploadedFiles/ASHA/Practice_Portal/Clinical_Topics/Traumatic_Brain_Injury_in_Adults /Clinicians-Guide-to-Cognitive-Rehabilitation-in-Mild-Traumatic-Brain-Injury.pdf
Clinician’s Guide to Cognitive Rehabilitation in Mild Traumatic Brain Injury: Application for Military Service Members and Veterans

Questions&
Discussion

67
ReferencesBagneux V, Thomassin N, Gonthier C, Roulin J-L (2013) Working Memory in the Processing of the Iowa Gambling Task: An Individual Differences
Approach. PLoS ONE 8(11): e81498.
Bechara A, Damasio AR, Damasio H, Anderson SW (1994) Insensitivity to future consequences following damage to human prefrontal cortex. Cognition 50: 7-15. doi:10.1016/0010-0277(94)90018-3. PubMed:8039375.
Beck AT, Epstein N, Brown G, . (1988) An inventory for measuring clinical anxiety: Psychometric properties. Journal of Consulting and Clinical Psychology 56(6): 893.
Beck AT, Ward CH, Mendelson M, Mock JE, Erbaugh JK. An inventory for measuring depression. Arch Gen Psychiatry. 1961;4:561-71.
Cohen, S., and Williamson, G. (1988). “Perceived stress in a probability sample of the United States,” in The Social Psychology of Health: Claremont Symposium on Applied Social Psychology, eds S. Spacapan and S. Oskamp (Newbury Park, CA: Sage Publications, Inc.) 31–67.
Conway, A. R. A., Kane, M. J., Bunting, M. F., Hambrick, D. Z., Wilhelm, O., & Engle, R. W. (2005). Working memory span tasks: A methodological review and user's guide. Psychonomic Bulletin & Review: A Journal of the Psychonomic Society, Inc, 12(5), 769.
Cooper, D. B., Bunner, A. E., Kennedy, J. E., Balldin, V., Tate, D. F., Eapen, B. C., & Jaramillo, C. A. (2015). Treatment of persistent post-concussive symptoms after mild traumatic brain injury: A systematic review of cognitive rehabilitation and behavioral health interventions in military service members and veterans. Brain Imaging and Behavior, 9(3), 403-420.
Dawson, Peg, & Guare, Richard. (2012). Coaching Students with Executive Skills Deficits. Practical Intervention in the Schools Series (Vol. 20). Guilford Press. 72 Spring Street, New York, NY 10012.
Department of Defense (2016) Defense and Veterans Brain Injury Center. Retrieved from http://dvbic.dcoe.mil/
Department of Veterans Affairs (2014) Education Program Beneficiaries. Retrieved from https://www.va.gov/vetdata/docs/quickfacts/Education_Beneficiaries.pdf
Dolan, S., Martindale, S., Robinson, J., Kimbrel, N.A., Meyer, E.C., Kruse, M.I., Morissette, S.B., Young, K.A., Gulliver, S.B. (2012). Neuropsychological sequelae of PTSD and TBI following war deployment among OEF/OIF veterans. Neuropsychology Review, 22 (1), 21-34.
Gallagher, K., & Azuma, T. (2018). Analysis of Story Recall in Military Veterans With and Without Mild Traumatic Brain Injury: Preliminary Results. American Journal of Speech-language Pathology, 27(1S), 485-494.
Gallagher, K.L., Azuma, T. The Effect of Anxiety and Working Memory on Decision-Making Patterns in Young Military Veterans. Oral Presentation, American Speech-Language Hearing Association Convention, Los Angeles, 2017.

68
Gallagher, K.L., Azuma, T. Self-report of Cognitive and Anxiety Symptoms in Military Veteran and Non-veteran College Students with Mild Traumatic Brain Injury. Poster, Defense Centers of Excellence for Psychological Health and Traumatic Brain Injury Summit: Advances in the State of the Science and Best Practices, 2017.
Gallagher, K.L., Azuma, T. Memory and mTBI: Narrative Recall in Veterans with Mild Traumatic Brain Injury. Oral Presentation, American Speech-Language Hearing Association Convention, Philadelphia, 2016.
Gallagher, K.L., Azuma, T. Analysis of Story Recall in Military Veterans with and without mTBI: Preliminary Results. Poster, Clinical Aphasiology Conference, Virginia, 2016.
Hoge, C. W., Castro, C. A., Messer, S. C., McGurk, D., Cotting, D. I., & Koffman, R. L. (2004). Combat duty in Iraq and Afghanistan, mental health problems, and barriers to care. The New England Journal of Medicine, 351(1), 13-22.
Hyatt, K., Davis, L. L., & Barroso, J. (2014). Chasing the care: Soldiers experience following combat-related mild traumatic brain injury. Military Medicine, 179(8), 849-855.
Kennedy, M.R.T. (2017). Coaching College Students with Executive Function Problems. New York, NY: Guilford Press.
Kane, M. J., Hambrick, D. Z., Tuholski, S. W., Wilhelm, O., Payne, T. W., & Engle, R. W. (2004). The generality of working memory capacity: A latent-variable approach to verbal and visuospatial memory span and reasoning. Journal of Experimental Psychology: General, 133(2), 189–217.
Krug, H., Turkstra, L.S. (2015). Assessment of Cognitive-Communication Disorders in Adults with Mild Traumatic Brain Injury. Perspectives on Neurophysiology and Neurogenic Speech and Language Disorders, 25, 17-35.
Karr, J. E., Areshenkoff, C. N., Duggan, E. C., & Garcia-Barrera, M. A. (2014). Blast-related mild traumatic brain injury: A bayesian random-effects meta-analysis on the cognitive outcomes of concussion among military personnel. Neuropsychology Review, 24(4), 428-444.
Lange, R. T., Brickell, T. A., French, L. M., Merritt, V. C., Bhagwat, A., Pancholi, S., & Iverson, G. L. (2012). Neuropsychological outcome from uncomplicated mild, complicated mild, and moderate traumatic brain injury in US military personnel. Archives of Clinical Neuropsychology: The Official Journal of the National Academy of Neuropsychologists, 27(5), 480.
Lew, H. L., Vanderploeg, R. D., Moore, D. F., Schwab, K., Friedman, L., Yesavage, J.. Sigford, B. J. (2008). Overlap of mild TBI and mental health conditions in returning OIF/OEF service members and veterans. Journal of Rehabilitation Research and Development, 45(3), xi.
Lezak, M. D., Howieson, D.B., Bigler, E.D., Tranel, D. (2012). Neuropsychological assessment (5th ed.). Oxford; New York; Oxford University Press.

69
Malec, J.F., Brown, A.W., Leibson, C.L., Flaada, J.T., Mandrekar, J.N., Diehl, N.N., and Perkins, P.K. (2007). The Mayo Classification System for Traumatic Brain Injury Severity. Journal of Neurotrauma, 24(9): 1417-1424.
Mcinnes, K., Friesen, C.L., MacKenzie, D.E., Westwood, D.A., and Boe, S.G. (2017). Mild Traumatic Brain Injury (mTBI) and chronic cognitive impairment: A scoping review. PLoS OnE 12(4).
Meuller, S.T. & Piper, B.J. (2014). The psychology experiment building language (PEBL) and PEBL test battery. Journal of Neuroscience Methods, 222, 250-259.
National Center for Education Statistics. (2016). After the post-9/11 GI bill: A profile of military service members and veterans enrolled in undergraduate and graduate education: Statistics in brief;2016 ASI 4826-10.118;NCES 2016-435.
Rigg, J. L., & Mooney, S. R. (2011). Concussions and the military: Issues specific to service members. PM & R: The Journal of Injury, Function, and Rehabilitation, 3(10 Suppl 2), S380.
Spencer, R., Drag, L., Walker, S., & Bieliauskas, L. (2010). Self-reported cognitive symptoms following mild traumatic brain injury are poorly associated with neuropsychological performance in OIF/OEF veterans. Journal of Rehabilitation Research and Development, 47(6), 521-30.
Storzbach, D., O'Neil, M. E., Roost, S., Kowalski, H., Iverson, G. L., Binder, L. M.. . Huckans, M. (2015). Comparing the neuropsychological test performance of operation enduring Freedom/Operation iraqi freedom (OEF/OIF) veterans with and without blast exposure, mild traumatic brain injury, and posttraumatic stress symptoms. Journal of the International Neuropsychological Society: JINS, 21(5), 353-363.
Unsworth, N., & Engle R.W. (2007) On the division of short-term and working memory: an examination of simple and complex spans and their relation to higher order abilities. Psychological Bulletin, 133, 1038-1066.
Unsworth, N., Heitz, R. P., Schrock, J. C., & Engle, R. W. (2005). An automated version of the operation span task.Behavior Research Methods, 37(3), 498-505.
Vanderploeg, R., Curtiss, G., & Belanger, H. (2005). Long-term neuropsychological outcomes following mild traumatic brain injury. Journal Of The International Neuropsychological Society, 11(3), 228-236.
Verfaellie, M., Lafleche, G., Spiro, A., & Bousquet, K. (2014). Neuropsychological outcomes in OEF/OIF veterans with self-report of blast exposure: Associations with mental health, but not MTBI. Neuropsychology, 28(3), 337-346.
Wechsler, D. (2009). Wechsler Memory Scales – Fourth Edition. San Antonio, TX: Pearson.