Embed Size (px)
Citation preview

Mind the Gap: AF and the Evolving
Strategies in Anticoagulation
In Cooperation with

Faculty DisclosuresFred M. Kusomoto, MD, FACCMayo ClinicConsulting Fees/Honoraria: Medtronic
Ralph J. Verdino, MD, FACCUniversity of PennsylvaniaConsulting Fees/Honoraria: Biosense Webster; Biotronic, Inc.; Boston Scientific; Medtronic; St. Jude Medical; ZollOfficer, Director, Trustee or Other Fiduciary Role: LifeWatch, Inc.

Acknowledgement
Boehringer Ingelheim Pharmaceuticals, Inc. is a Founding Sponsor for the Mind the
Gap Forums.

“Atrial Fibrillation is the Low Back Pain of Cardiology.”
Mike Crawford

Program Objectives
Upon completion of this session, attendees should be able to —
•Implement evidence-based anticoagulation regimens for atrial fibrillation patients based on individual risks and patients’ preferences•Recognize common barriers associated with managing chronic anticoagulation in atrial fibrillation patients

2.2 million people have AF–3.3 million in 2020; 5.6 million by
2050–Above age 70: 10% incidence–Lifetime risk: 25%–Risk increases with increasing age
Atrial Fibrillation (AF) in the U.S

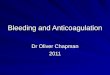
Future of Atrial FibrillationATRIA Study
Go et al. Go et al. JAMAJAMA. 2001;285;2370-2375.. 2001;285;2370-2375.
Projected Number of Adults With AF in the US 1995 to 2050Projected Number of Adults With AF in the US 1995 to 2050A
dul
ts W
ith
AF
(m
illi
ons)
Ad
ults
Wit
h A
F (
mil
lion
s)
7.07.0
2.082.08
5.615.615.425.425.165.16
4.784.784.344.34
3.803.80
3.333.332.942.94
2.662.662.442.442.262.26
6.06.0
5.05.0
4.04.0
3.03.0
4.04.0
2.02.0
1.01.0
0019901990 19951995 20002000 20052005 20102010 20152015 20202020 20252025 20302030 20352035 20402040 20452045 20502050
YearYear

Ann Int Med 1995
Prevalence
Biennial rate/1000 person exams
Age
Incidence
Benjamin EJ JAMA 1994; Framingham Heart Study

Risks/causative factors:– HTN, DM, CHF, age, valvular heart
disease, MI, pulmonary embolus, cardiomyopathy, pulmonary disease, hyperthyroidism
– Genetics: Most common in “Lone AF”•Connexin-40•Potassium channels: KCNQ1, KCNE2, KCNJ2, KCNH2
•ANF peptide frame shift mutation
Atrial Fibrillation in the U.S. (Cont.)


• Stroke is the most common and devastating complication of AF1,2
• Incidence of all-cause stroke in patients with AF is 5%1
• AF is an independent risk factor for stroke2
• Approximately 15% of all strokes in the US are caused by AF3
Atrial Fibrillation (AF) and Stroke
1. Fuster V, et al. Circulation. 2006;114:e257-354. 2. Benjamin EJ, et al. Circulation. 1998;98:946-52.
3. Lloyd-Jones D, et al. Circulation. 2009;119:e21-181.

Stroke Rates in Placebo-Treated Patients With AF*
*This represents patients who are not anticoagulated; *This represents patients who are not anticoagulated; ††Secondary prevention.Secondary prevention.Hart et al.Hart et al. Ann Intern Med. Ann Intern Med. 1999;131:492-501. 1999;131:492-501.
Str
oke
(%)
AFASAKAFASAK SPAFSPAF BAATAFBAATAF CAFACAFA SPINAFSPINAF EAFTEAFT††

• Risk of stroke increases with age1
• Ischemic stroke associated with AF is often more severe than stroke of other etiologies4
• Stroke risk persists even in asymptomatic AF5
• Asymptomatic AF implicated as a cause of cryptogenic stroke6
Atrial Fibrillation and Stroke (Cont.)
4. Dulli DA, et al. Neuroepidemiology. 2003;22:118-23. 5. Page RL, et al. Circulation. 2003;107:1141-56. Bhatt A, et al. Stroke Res Treat. 2011; 2011: 1-5

CHADS2
Congestive heart failureHypertensionAge >75 yearsDiabetes mellitusPrior Stroke or TIA (*2 points)
Gage, BF, et al. JAMA. 2001;285:2864-70

Stroke Risk in AFACP/AAFP Guidelines
Snow V, et al. Ann Intern Med. 2003;139:1009-17
CHADS2
ScoreAdjusted Stroke Rate*
(95% CI)CHADS2
Risk Level
0 1.9 (1.2-3.0) Low
1 2.8 (2.0-3.8) Low
2 4.0 (3.1-5.1) Moderate
3 5.9 (4.6-7.3) Moderate
4 8.5 (6.3-11.1) High
5 12.5 (8.2-17.5) High
6 18.2 (10.5-27.4) High
Warfarin
*Expected rate of stroke per 100 patient-years
Aspirin
Aspirin/Warfarin

CHADS2
Congestive heart failureHypertensionAge >75 yearsDiabetes mellitusPrior Stroke or TIA (*2 points)
Gage, BF, et al. JAMA. 2001;285:2864-70

CHADS2
Congestive heart failureHypertensionAge >75 yearsDiabetes mellitusPrior Stroke or TIA (*2 points)CHADS2 did not consider other important
risk factors:– Female gender (not confirmed in all studies)– Thyrotoxicosis– LA size– HOCM– Valvular heart disease
Gage, BF, et al. JAMA. 2001;285:2864-70

CHADS2
Lip et al Chest 2010

CHA2DS2-VASc
Clinical Feature Points
CHF 1
HTN 1
Age ≥ 75 2
Diabetes mellitus 1
Stroke, TIA, or embolism 2
Female gender 1
Age 65 - 74 1
Vascular disease (prior MI, PVD, aortic plaque 1

CHADS2 vs. CHA2DS2-VASc
Lip et al Chest 2010

ESC Guidelines for Antithrombotic
Therapy
CHA2DS2VASc score Adjusted stroke rate (%/year)
Recommended antithrombotic therapy
0 0 ASA 75-325mg or no therapy. No therapy
preferred
1 1.3 Either oral anticoagulation or ASA 75-325mg daily,
anticoagulation preferred
2 2.2 Oral anticoagulation
3 3.2 Oral anticoagulation
4 4.0 Oral anticoagulation
5 6.7 Oral anticoagulation
6 9.8 Oral anticoagulation
7 9.6 Oral anticoagulation
8 6.7 Oral anticoagulation
9 15.2 Oral anticoagulation
Europace 2010; 12: 1360-1420

Stroke Prevention: Coumadin
Warfarin
AFASAK
BAATAF
SPAF
CAFA
SPINAF
Warfarin/ASA
EAFT
SPAF II
AFASAK



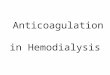
Warfarin: Risk-Benefit Profile
Fuster V, et al. Circulation. 2006;114:e257-354.
Ischemic Stroke
Intracranial Bleeding
20
15
10
5
1
1.0 2.0 3.0 4.0 5.0 6.0 7.0 8.0
Odd
s R
atio
INR

Warfarin and Drug Interactions
Warfarin is metabolized by the hepatic P450 enzyme CYP2C9
Warfarin concentration (and therefore INR) is increased by drugs that inhibit CYP2C9. INR must be closely followed and warfarin dosage decreased
CYP2C9 inhibitors include:• Amiodarone • Statins simvastatin and rosuvastatin (not atorvastatin,
pravastatin)• Fibrates (fenofibrate, gemfibrozil)• Antibiotics (sulfamethoxazole/trimethoprim, metronidazole)• Azole antifungals (fluconazole, miconazole, voriconazole)

Warfarin and Drug Interactions (Cont.)
Drugs that induce CYP2C9: warfarin’s effectiveness is decreased, reducing INR - Rifampin
• Other drugs interactions not via CYP2C metabolism - Thyroid hormone
For more information visit www.qtdrugs.org (Arizona CERT) or http://medicine.iupui.edu/clinpharm/ddis/table.asp (Indiana University, Prof D.A. Flockhart)

Quality of Warfarin Control in AF Patients on Chronic
Anticoagulation
Tim
e S
pen
t in
T
hera
peu
tic
INR
R
an
ge (
%)
55% 63%51%
Baker WL, et al. J Manag Care Pharm. 2009;15:244-52.
Only 48% of eligible patients in this analysis received warfarin

Time Spent in Therapeutic INR Range and Clinical
Outcomes
Morgan CL, et al. Thromb Res. 2009;124:37-41.
• Groups stratified by time spent in therapeutic INR range (2.0-3.0)
• All patients had a CHADS2 score ≥ 2

Warfarin in Eligible PatientsATRIA Study
Age (years)Age (years)Go et al. Go et al. Ann Intern MedAnn Intern Med. . 1999;131:927-934.1999;131:927-934.
<55<55 55-6455-64 65-7465-74 75-8475-84 8585 OverallOverall
% U
se in
Eli
gib
le P
atie
nts
% U
se in
Eli
gib
le P
atie
nts

Warfarin in Eligible PatientsATRIA Study
Age (years)Age (years)Go et al. Go et al. Ann Intern MedAnn Intern Med. . 1999;131:927-934.1999;131:927-934.
<55<55 55-6455-64 65-7465-74 75-8475-84 8585 OverallOverall
% U
se in
Eli
gib
le P
atie
nts
% U
se in
Eli
gib
le P
atie
nts

ACTIVE Investigators. Lancet. 2006;367:1903-12.
ACTIVE-W: Warfarin vs. Dual Antiplatelet Therapy for Prevention
of Cardiovascular EventsCumulative risk of primary composite endpointa
aStroke, MI, non-CNS systemic embolism, or vascular death.
Cu
mu
lati
ve H
azar
d R
ates
Cu
mu
lati
ve H
azar
d R
ates
RR = 1.44 (1.18-1.76), P = 0.0003RR = 1.44 (1.18-1.76), P = 0.0003
Time (years)Time (years)

ACTIVE-A: Dual Antiplatelet Therapy Reduces the Incidence of Vascular
Events in AF When Warfarin Therapy Is “Unsuitable”
Cu
mu
lati
ve I
nci
den
ce
Time (years) Time (years)
Primary Composite Endpointa
aStroke, MI, non-CNS systemic embolism, or vascular death.
Stroke
ACTIVE Investigators. N Engl J Med. 2009;360:2066-78.
P = 0.01P = 0.01 P < 0.001P < 0.001

ACTIVE-A: Dual Antiplatelet Therapy Increases the Risk of
Bleeding
0
2
4
6
8
10
12
Major Bleeding Minor Bleeding Any Bleeding
Perc
ent/
year
Bleeding Events
ASA ASA+clopidogrel
P<0.001
P<0.001
P<0.001

•Class IIb (New Recommendation)
•The addition of clopidogrel to aspirin (ASA) to reduce the risk of major vascular events, including stroke, might be considered in patients with AF in whom oral anticoagulation with warfarin is considered unsuitable due to patient preference or the physician’s assessment of the patient’s ability to safely sustain anticoagulation. (Level of Evidence: B)
•Single reference: ACTIVE A2011 ACCF/AHA/HRS Focused Update on the Management of Patients with Atrial Fibrillation (Updating the 2006 Guideline). Circulation 2011;123:104-123.
2011 Focused Update Recommendation


New Pharmacologic Approaches for Stroke
Reduction in AFOral direct thrombin inhibitors
– Fixed-dose, no monitoring•Dabigatran
Oral factor Xa inhibitors– Fixed-dose, no monitoring
•Apixaban•Edoxaban•Rivaroxaban

Antithrombotic Therapy in Atrial Fibrillation. Circulation 2011;75:1539-1547.

Direct Thrombin Inhibitors
Ximelagatran– Tested in Stroke Prevention Using
an Oral Thrombin Inhibitor in Atrial Fibrillation (SPORTIF) III (open label) and V (double blind)
– Ximelagatran as effective as warfarin with lower risk of bleeding
– Did not make it to market due to liver toxicity

RE-LY: Randomized Evaluation of Long-term Anticoagulation Therapy• 18,113 patients with atrial fibrillation
randomized to dabigatran (110 mg or 150 mg twice daily) versus warfarin (INR target 2.0-3.0)
• Mean CHADS2 score = 2.1
• By intention-to-treat analysis dabigatran 110 mg was non-inferior (p < 0.001) while dabigatran 150 mg was superior( p<0.001) to warfarin
• INR was in the therapeutic range 64% of the time
NEJM 10.1056

RE-LY“High risk” AF patients:
– At least one of:• Prior CVA or TIA• LVEF < 40%;• NYHA Class I or greater CHF• Age >75 yrs• Age 65-74 and on of:
– DM– HTN– CAD
Exclusions: “severe valve disease;” CVA <14 days or “severe CVA” <6 months; increased bleeding risk; active liver disease; CrCl <30; pregnancy

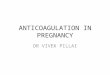
RE-LY: Dabigatran Reduces the Risk of Stroke in AF
Patients
Connolly SJ, et al. N Engl J Med. 2009;361:1139-51.
Cu
mu
lati
ve H
azar
d R
ate
Time (months)

RE-LY: Safety Outcomes with Dabigatran
Dabigatran 110 mg
vs. Warfarin
Dabigatran 150 mg
vs. Warfarin
Event RR (95% CI) P value RR (95% CI) P value
Major bleeding 0.80 (0.69-0.93) 0.003 0.93 (0.81-1.07) 0.31
Life threatening 0.68 (0.55-0.83) < 0.001 0.81 (0.66-0.99) 0.04
Gastrointestinal bleeding
1.10 (0.86-1.41) 0.43 1.50 (1.19-1.89) < 0.001
Major or minor bleeding
0.78 (0.74-0.83) < 0.001 0.91 (0.86-0.97) 0.002
Intracranial bleeding 0.31 (0.20-0.47) < 0.001 0.40 (0.27-0.60) < 0.001
Modified from Connolly SJ, et al. N Engl J Med. 2009;361:1139-51.

FDA Approval for Dabigatran:
Beasley BN, Unger EF, Temple R. Anticoagulant Options – Why the FDA Approved a Higher but Not a Lower Dose of Dabigatran. NEJM 2011 (online first).
• Dabigatran 150 was superior to warfarin and dabigatran 110 mg for stroke prevention;
• Dabigatran 150 mg was similar to warfarin for bleeding risk but inferior to dabigatran 110 mg.
• Among the elderly (40% of Re-Ly patients over age 75), thromboembolism risk was lower with dabi-150 than with dabi-110, but bleeding risk was higher. Because bleeding is “less undesirable” than stroke, dabi-110 not felt to be advantageous.

FDA Approval for Dabigatran:
75 mg q12h
Beasley BN, Unger EF, Temple R. Anticoagulant Options – Why the FDA Approved a Higher but Not a Lower Dose of Dabigatran. NEJM 2011 (online first).
• Among pts with impaired renal function (CrCl 30-50), stroke risk for dabi-150 was 1/2 that of dabi-110 but bleeding risk was not higher.
==> dabi-110 was not felt to offer any advantage, and it was felt that most patients should receive the higher dosage.
• The decision to approve the 75 mg q12h dose was based on pharmacokinetic and pharmacodynamic modeling; there is no safety or efficacy data.

Antithrombotic Therapy in Atrial Fibrillation. Circulation 2011;75:1539-1547.

Antithrombotic Therapy in Atrial Fibrillation. Circulation 2011;75:1539-1547.

Apixaban: AVERROES Trial5599 patients with AF deemed “unsuitable” for
warfarin randomized to apixaban (5mg twice daily) or aspirin (81-324mg daily)
Primary endpoint: stroke or systemic embolismTrial terminated early due to superiority of apixaban
1.6 3.5 1.4
12.6
3.7 4.4 1.2
15.9
stroke/embolism Death major bleeding CV hospitalization
Per
cen
t/ye
ar
Apixaban Aspirin
P<0.001P=0.57
P=0.07
P<0.001
Connolly et al. NEJM 2011 364: 806-17

ROCKET-AF: Rivaroxaban for the Prevention of Stroke and Non-CNS
Embolism• 14,264 patients with atrial fibrillation
randomized to rivaroxaban (20mg once daily) versus warfarin (INR target 2.5)
• Mean CHADS2 score = 3.5
• By intention-to-treat analysis rivaroxaban was non-inferior (p < 0.0001) but not superior ( p =0.12) to warfarin
• INR was in the therapeutic range only 55 percent of the time
• Currently before the FDA for AF indication• Safety: overall similar bleeding rates with less
life-threatening (fatal or intracranial) hemorrhage
NEJM 10.1056

2011 ACCF/AHA/HRS Focused Update on the Management of Patients with Atrial Fibrillation
(Update on Dabigatran)



Case 1 – 76-year-old Female with Dyspnea

• HPI– Shortness of breath and DOE for
several months– Denies palpitations, chest pain, or
dizziness
• PMH– Obesity, diabetes, HTN, chronic
kidney disease, hyperlipidemia, DJD– Does not smoke or drink– Meds: diltiazem, celecoxib,
metformin, pravastatin

• PE– VS: BP 164/92, HR 94 – CV: irregularly irregular, no murmurs
• Data– ECG: atrial fibrillation with controlled VR,
LVH by voltage– BUN/Cr: 36/2.1, other labs incl LFTs nl– CXR: mild cardiomegaly, o/w normal– Stress echo: nl LV function, mild LVH, no
sig valve dz, no ischemia

a)High (~8-18%)b)Medium (~4-6%)c) Low (~2-3%)
Question
What is her risk of stroke?

Stroke Risk in AFACP/AAFP Guidelines
Snow V, et al. Ann Intern Med. 2003;139:1009-17
CHADS2
ScoreAdjusted Stroke Rate*
(95% CI)CHADS2
Risk Level
0 1.9 (1.2-3.0) Low
1 2.8 (2.0-3.8) Low
2 4.0 (3.1-5.1) Moderate
3 5.9 (4.6-7.3) Moderate
4 8.5 (6.3-11.1) High
5 12.5 (8.2-17.5) High
6 18.2 (10.5-27.4) High
Warfarin
*Expected rate of stroke per 100 patient-years
Aspirin
Aspirin/Warfarin

CHA2DS2-VASc
Clinical Feature Points
CHF 1
HTN 1
Age ≥ 75 2
Diabetes mellitus 1
Stroke, TIA, or embolism 2
Female gender 1
Age 65 - 74 1
Vascular disease (prior MI, PVD, aortic plaque)
1

ESC Guidelines for Antithrombotic Therapy
CHA2DS2VASc score Adjusted stroke rate (%/year)
Recommended antithrombotic therapy
0 0 ASA 75-325mg or no therapy. No therapy
preferred
1 1.3 Either oral anticoagulation or ASA 75-325mg daily,
anticoagulation preferred
2 2.2 Oral anticoagulation
3 3.2 Oral anticoagulation
4 4.0 Oral anticoagulation
5 6.7 Oral anticoagulation
6 9.8 Oral anticoagulation
7 9.6 Oral anticoagulation
8 6.7 Oral anticoagulation
9 15.2 Oral anticoagulation
Europace 2010; 12: 1360-1420
ESC Guidelines for Antithrombotic Therapy

a)Highb)Mediumc) Low
Question
What is her risk of bleeding with anticoagulation?

HAS-BLED Score
Clinical Feature Points
SBP ≥ 160 mmHg 1
Abnormal renal function 1
Abnormal liver function 1
Prior CVA 1
Bleeding 1
Labile INRs 1
Age > 65 1
Taking antiplatelets/NSAIDs 1
Alcohol intake 1
HAS-BLED score ≥3 indicates increased one year risk of intracranial bleed, bleed requiring hospitalization, or drop in hemoglobin ≥2gm/L or requiring transfusion.

HAS-BLED score in the SPORTIF
cohort
Lip et al JACC 2011
%
Score

What is her risk of stroke/bleeding?
a)CHADS2 score=3 (annual stroke risk=5.9%)
b)CHADS2VASc=5 (annual stroke risk=6.7%)
c) 3. HASBLED score=4 (annual bleeding risk=5.6%)
Question

Which anticoagulation regimen is most appropriate for her?a)Aspirinb)Warfarinc) Dabigatran 75mg twice dailyd)Dabigatran 150 mg twice dailye)Aspirin/clopidogrel
Question

AF and Strokes
• 15% of ischemic strokes are due to cardioemboli => 75,000 events/year
• 45% of cardioemboli are due to atrial fibrillation
• Risk of stroke 5-7x increased in patients with atrial fibrillation

Which Anticoagulation Regimen is Most Appropriate for Her?
http://www.vhpharmsci.com/sparc/

Which Anticoagulation Regimen to Use?
http://www.vhpharmsci.com/sparc/

Which Anticoagulation Regimen to Use?
http://www.vhpharmsci.com/sparc/

Case 1 Teaching Points• When using oral anticoagulants,
balancing the risks of bleeding vs the risks of stroke can be difficult.
• Scoring systems that predict risk (CHADS2, CHA2DS2Vasc, HASBLED) can help with decision making.

Questions and Answers

Case 2 – 59-year-old Man Presents with Acute Chest
Pain

- 10 years ago first diagnosed with hypertension
- 5 years ago acute inferior MI Cath showed - 95% RCA 70% LAD 90% OM1
Underwent CABG x3
- 6 month f/u - EF 40% by echo with inferior and posterior severe hypokinesia
Past History

- 4 years ago nuclear stress showed EF 35-40%, inferior and posterior scar without ischemia diminished functional status- 6 months ago maintained on Lisinopril 40 mgqd, Carvedilol 20 q12h, Aspirin 81mgqd, Simvastatin 40 mgqd, NYHA Class III CHF symptoms- 3 months ago presented on OV with atrial fibrillation with controlled rate; warfarin begun
Past History (Cont.)

Native coronaries 100% RCA 95% prox LAD 100% OM1 95% proximal LCx stenosis
- Patent LIMA and LAD, graft to PDA - Occluded graft to OM1 - Placed on clopidogrel full dose aspirin and underwent PCI of LCx with bare metal stent
Present Coronary Anatomy

a) Continue warfarin indefinitely with aspirin, clopidogrel for one yearb) Substitute dabigatran with aspirin, clopidogrel for one yearc) Stop warfarin, aspirin and clopidogrel for one month and resume warfarind) Stop warfarin, aspirin and clopidogrel for one month then add dabigatran
What would you do next?
Question

Triple Rx: Bleeding and Mortality in a Danish
Registry after MI
Sorensen et al Lancet 2009

a) Continue warfarin indefinitely with aspirin, clopidogrel for one yearb) Substitute dabigatran with aspirin, clopidogrel for one yearc) Stop warfarin, aspirin and clopidogrel for one month and resume warfarind) Stop warfarin, aspirin and clopidogrel for one month then add dabigatran
What would you do next?
Question

Guidelines for the Management of Atrial Fibrillation. European Heart Journal 2010; 31: 2369 - 2429.

Guidelines for the Management of Atrial Fibrillation. European Heart Journal 2010; 31: 2369 - 2429.

Faxon et al Hemostasis and Thrombosis 2011.
Risk Management:Stent Thrombosis vs. Bleeding vs. Stroke
Risk Management:Stent Thrombosis vs. Bleeding vs. Stroke

Managing Risk• Stent Thrombosis
• Discontinuing DAPT• Procedural: TIMI < 3,
Discontinuing DAPT, residual dissection, bifurcations stents, incomplete stent apposition, stent length, proximal dz
• Patient: Malignancy, diabetes, renal failure
• Bleeding• HAS-BLED
• Stroke• CHADS2 or CHA2DS2-VASc

Faxon et al Hemostasis and Thrombosis 2011.
Risk Management:Stent Thrombosis vs. Bleeding vs. Stroke
Risk Management:Stent Thrombosis vs. Bleeding vs. Stroke

Randomized Trials on Triple Therapy• ISAR-TRIPLE:
600 patients after DES will be randomized to either a short course (6 weeks) or long course (6 months), followed by aspirin and warfarin. 1°: Composite of death, MI, definite stent thrombosis, or major bleeding at 9 months
• WOEST: 496 patients randomized oral anticoagulation and clopidogrel or triple therapy. 1°: Bleeding at 1 year
• MUSICA-2: 304 patients (CHADS≤ 2) randomized to DAPT or triple Rx

Case 2 Teaching Points• Choose BMS if patient will require anti-thrombotic therapy long
term• Presentation with ACS implies that patient should ideally be
treated with dual anti-platelet therapy for 1 year but needs to be judged relative to bleeding risk
• Data on triple therapy is limited• No data on dabigitran in this setting and nothing in guidelines

Questions and Answers

Mind the Gap: Summary• Atrial fibrillation is going to become more
common
• Stroke is the most devastating complication of atrial fibrillation
• Old and new options
• Managing patients in “real life” is difficult


Case 3 – 80-year-old Male with Renal Cell Cancer

HPIRenal cell cancer recently diagnosedNephrectomy is plannedUrologic surgeon requests peri-op cardiac management
PMHPermanent atrial fibrillation for > 5 years, managed with metoprolol and warfarinMeds: metoprolol, warfarin, lisinopril, pravastatin, aspirin

VS: BP 134/68, HR 78 irreg irreg
CV: irregularly irregular, no murmursData
ECG: atrial fibrillation with controlled VR
INR 2.3
Physical Exam

In preparation for surgery, you should:a)Admit the patient to the hospital, stop warfarin and administer IV heparin until the morning of surgeryb)Stop warfarin 5 days prior to surgery and initiate LMWH until the morning of surgeryc)Stop warfarin 5 days prior to surgery without bridging anticoagulation
Question

Risks Associated with Temporary Discontinuation
of Warfarin• After warfarin is stopped, it takes about 4 days
for the INR to reach 1.5.
• Once the INR is 1.5 surgery can be safely performed.
• Therefore, if warfarin is held 4 days before surgery and treatment is started as soon as possible after surgery, patients can be expected to have a subtherapeautic INR for two days before and two days after surgery.

ACC/AHA/ESC 2006 Guidelines for Perioperative
Management of Atrial Fibrillation
• Anticoagulation may be interrupted for a period of up to one week for surgery.
• In high risk patients (prior stroke, TIA, or systemic embolism) unfractionated or low-molecular-weight heparin may be used.

ACCP 8th Edition Evidence-Based Clinical Practice Guidelines: Managing
Non-therapeutic INRsFor patients with INRs of ≥ 5.0 but < 9.0 and no significant bleeding:
–Omit the next one or two doses of warfarin–Monitor more frequently–Resume therapy at an appropriately adjusted dose when the INR is at a therapeutic level (Grade 1C)–Alternatively, omit a dose and administer 1 to 2.5 mg oral vitamin K, particularly if the patient is at increased risk of bleeding (Grade 2A)
Ansell J, et al. Chest. 2008;133:160S-98S.

Peri-operative Management of Dabigatran
• With normal kidney function, miss two doses of dabigatran before surgery.
• With impaired kidney function, miss 3-4 doses of dabigatran before surgery.
• If surgery carries a high risk of bleeding, consider stopping dabigatran 2 days before surgery with normal renal function and 3-5 days with impaired renal function.

a) Initiate a rhythm control drug
b) Discharge on beta-blocker alone
What would you do?
Question

Case 3 Teaching Points• Most patients, unless they have had
prior stroke, TIA, or systemic embolism do not require bridging of anticoagulation.
• Warfarin can be stopped for 5 days prior to surgery while dabigatran can be stopped just 1-2 days prior to surgery.