Embed Size (px)
Citation preview

Journal of Neuro-Oncology 6:227-230 (1988) © Kluwer Academic Publishers - Printed in the Netherlands 227
Misonidazole neuropathy A prospective study
B. Melgaard 1, O. Kohler 1, H. Sand Hansen 2, J. Overgaard 3, J. Munck-Hansen 2 and O. B. Paulson 1,4 1Neurology Service, Finseninstituttet, Copenhagen; 2The Department of Head- and Neck Oncology, Finseninstituttet, Copenhagen; 3Danish Cancer Society, Department of Experimental Clinical Oncology, NOrrebrogade 44, Aarhus C; and 4The Department of Neurology, Rigshospitalet, Copenhagen, Denmark
Key words: cancer, polyneuropathy, misonidazole
Abstract
The frequency with which polyneuropathy developed Was investigated in patients with cancer of the larynx and pharynx who participated in a double-blind trial of the radiosensitizing drug misonidazole. Fourteen of 36 patients receiving misonidazole (total dose of about 11 g/m 2) developed neuropathy, while this occurred in only 2 of 34 patients in the placebo group.
Vibration perception threshold increased in all patients who developed neuropathy, but also in 12 (5 misonidazole and 7 placebo treated) without other symptoms or signs of neuropathy.
Pharmacokinetic studies of misonidazole revealed a correlation between development of neuropathy and a high 'peak plasma concentration/g misonidazole in each fraction' and especially a high 'area under plasma concentration curve/g misonidazole in each fraction'.
The first clinical pilot studies of the hypoxic radio- sensitizing drug misonidazole in the treatment of solid tumours resulted in the development of a peripheral neuropathy in 3 0 - 5 0 % of the patients [1- 7]. Symptoms are dominated by severe pain, and detailed investigations have shown an axonal de- generation in peripheral nerves [8].
As a consequence of the initial experiences the maximum dose of misonidazole given in the Danish Head and Neck Cancer Trial was reduced from 12 to 11 g/m 2 given over 4 weeks [7]. The aim of the present prospective study was to evaluate the fre- quency of peripheral neuropathy in a group of pa- tients receiving placebo or misonidazole in a total dose of 11 g /m 2 as part of the treatment in the Dan- ish Head and Neck Cancer Trial [7].
Materials and methods
Seventy-nine patients referred to the Finsen Institute
for radiotherapy of cancer of the pharynx or larynx were examined. All patients were treated according to the Danish Head and Neck Cancer study protocol [2, 7], a randomized double-blind trial analyzing the potential effect of the hypoxic radiosensitizer mis- onidazole as an adjuvant to radiotherapy. Nine pa- tients were excluded either because they showed signs of peripheral neuropathy prior to treatment, or because they did not complete the treatment sched- ule for other reasons than symptoms of peripheral neuropathy. The remaining 70 patients consisted of 52 males and 18 females with a median age of 61 and 60 years, respectively. Placebo or misonidazole were given orally during the first four-week period of treatment. The total dose of misonidazole was ap- proximately 11 g /m 2 administrated in 8 or 20 frac- tion schedules [7].
All patients were examined before start of treat- ment, and three weeks and eight weeks later. Vibra- tion perception thresholds (VPT) were measured on

228
the pulps of the big toes using a 'Biothesiometer' (Chagrin Falls, Ohio, Mass.) which delivers harmon- ic mechanical oscillations of I00 Hz and a variable amplitude. VPT was recorded as the average of three consecutive measurements at each toe.
Plasma pharmacokinetic parameters of misoni- dazole were estimated on the basis of analysis of heparinized blood-samples taken 4, 8 and 24 hours after the first dose of misonidazole. Plasma concen- trations were determined by reverse-phase high-pres- sure liquid chromatography as previously described [9, 10]. The plasma pharmacokinetic parameters are described on the assumption of first order absorp- tion and elimination kinetics. The peak plasma concentration is represented by the 4-hour concen- tration level. The elimination constant k e is deter- mined by the least square regression calculation of the slope of the log-linear plot of plasma concentra- tion versus time. The elimination half life is then given by ln2/k e. The area under the curve (AUC) which gives an expression of the concentration × time exposure to the drug was obtained by the for- mula AUC = Co/k e - Co/k a, where Co is the dose at time 0 obtained by extrapolation of the log-linear elimination curve, and k a the absorption rate [10].
Results
Fourteen patients out of 36 receiving misonidazole (38%) developed neuropathy while this occurred in only two patients in the placebo group of 34 patients (X2=10.8; P<0.005). Symptoms and signs ap- peared during or, in most cases, shortly after termi- nation of treatment. Symptoms consisted of painful paraesthesia in the feet and sometimes in the hands accompanied in some patients by loss of sensation in the feet resulting in difficulties. Signs ranged from loss of touch-and-pain sense in the toes to severe im- pairment of all sensory modalities in the feet and lower legs. Achilles tendon reflexes were preserved in all patients.
In 10 of the 54 patients without symptoms or signs of neuropathy the levels of VPT increased more than 50% from the first to the second or third exami- nation. In 2 patients increases between 20 and 50°7o were found, while in the remaining the levels re-
mained unchanged. Seven patients with VPT in- creases had received placebo while 5 had received misonidazole.
In the misonidazole-group no differences were found between those who developed peripheral neu- ropathy and those who did not with regard to age, average daily alcohol intake, fractioning of mis- onidazole or VPT levels preceding therapy. However, females had a significantly higher risk of developing neuropathy than males (Table 1), but this corre- sponded to a higher AUC in females.
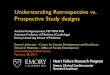
Plasma pharmacokinetic parameters were ob- tained in 31 patients receiving misonidazole. The relationship between the pharmacokinetics of mis- onidazole and peripheral neuropathy is shown in Ta- ble 1. Since both the peak plasma concentration and the AUC have a linear relationship with a given dose the 8 and 20 fraction schedules may be compared by estimating these parameters per g misonidazole in each fraction. In patients developing neuropathy, the mean peak plasma concentration was signifi- cantly increased as compared to patients without symptoms. A similar although not statistically sig- nificant trend was found for the elimination half life. Consequently, the AUC was also significantly higher in the neuropathy group both when calculated as AUC/g and as total AUC. In fact, the AUC was found to be a highly significant prognostic parame- ter for the development of neuropathy. Thus in pa- tients with an AUC/g ~ 400, the incidence of neu- ropathy was 71% compared with only 12% in the patients with values below 400 #g ml -~ g-1 (Fig. 1, Table 1).
Discussion
The occurrence of peripheral neuropathy in this double-blind study was as frequent as previously reported [1-6] although a smaller total dose of mis- onidazole was employed. There was, however, a ten- dency towards milder and in some cases transient symptoms. This neuropathy is a striking clinical en- tity completely dominated by sensory symptoms which are often very painful and with preserved Achilles tendon reflexes consistently found at clinical examination [8]. We found that neither initial VPT

229
Table 1. Pharmacokinetics of misonidazole and patient characteristics in relation to peripheral neuropathy (Mean _+ SD)
No neuropathy Neuropathy
Number of patients in whom pharmacokinetics was performed 17 (55%)
Median age (range) 58 ( 3 9 - 7 9 )
Female 3 (27%) Total dose (g) 19.9_+ 2.8 Dose (g m -z) 10.9_+ 0.3
8 vs. 20 fractions (%:%) 21 : 79 Peak plasma conc/g (~g/m1-1 g- l)§ 19.2_+ 3.8
Plasma half-life (h) 10.3 _+ 2.9
A U C / g (#g m1-1 g - I h)§ 335 _+ 66 Total A U C (/zg m1-1 h)§§ 6669 _+ 1501 A U X / g >__ 400/zg m l - 1 g - 1 12o/0
14 (45 °7o)
68 (53 - 83)
p<0 .05* 8 (73%) N.S.** 18.9_+ 2.0
N.S.** 11.0+ 0.3
N.S.* 41 : 59
p<0 .05** 22.0+ 3.8
N,S.** 11.2_+ 2.4
p<0.001** 446 _+ 98 p<0 .01** 8421 +2067
p<0 .001* 71°/o
* X 2 t e s t .
** Student's t-test. § Peak plasma conc, respective AUC pr. g misonidazole in each fraction (total dose/number of fractions).
§§ Total A U C = A U C x number of fractions.
S
t~
;4
l
X
O m <
700
500
400
300
• MALE
o FEMALE
|
• o
8
Q
2OO NO NEUROPATHY NEUROPATHY
Fig. 1. Values of Area Under the Curve (AUC)/gram misonida- zole in each fraction in patients who developed neuropathy and in patients who did not develop neuropathy following misonida- zole treatment.
levels nor reported alcohol intake could predict the development of peripheral neuropathy.
Subclinical evaluation of the development of pe- ripheral neuropathy by means of VPT measurement proved non-useful as those patients without neuro- pathy in whom an increase was found was evenly divided between the placebo and misonidazole groups. In contrast, VPT has previously been report- ed to be a reliable method for the detection of de- velopment of peripheral neuropathy in chronic renal failure [11].
Studies indicate that treatment with steroids or phenytoin [12, 13], may prevent the development of misonidazole neuropathy. The effect of phenytoin is mediated through a shortening of plasma half-life of misonidazole whereas steroids are thought to restore and stabilize cell surface properties.
The increased incidence of neuropathy in females was not a function of sex per se, but simply due to the fact that patients with a small surface area ( < 1.7 m 2) [14] have a higher plasma concentration per given dose than larger patients. Thus, the AUC values in females were generally higher than in males (Fig. 1).
Although only a single plasma profile was ob- tained in each patient an initial unpublished pilot study revealed that the day-to-day variation in AUC was without any significant influence on the results.

230
However, in order to avoid drug accumula t ion in the
dai ly f rac t iona t ion schedule the p lasma samples
were no rma l ly ob ta ined dur ing the first t rea tment
day.
The signif icantly increased A U C values in pa-
tients developing neuropa thy indicate that a phar-
macok ine t i c screening may be a valuable tool to re-
duce the incidence o f the t roub lesome neuropathy.
Therefore, we are current ly reducing the dose in pa-
tients with high A U C values, and this has marked ly
reduced the incidence o f neuropathy.
Acknowledgements
Suppor ted by the Danish Cancer Society (grants
5 /80 and 24/79) and 'Grosserer Sigurd A b r a h a m s o n
og hustru Addle A b r a h a m s o n s minde lega t ' .
References
1. Dische S: The neurotoxicity of misonidazole: Pooling of data from five centres. Br J Radiol 51:1023-1024, 1978
2. Adams GE: MRC randomized studies of misonidazole in combination with radiotherapy. Br J Radiol 55:464-465, 1982
3. Kogelnik HD: Clinical experience with misonidazole. High dose fractions versus daily low doses. Cancer Clin Trials 3:179-186, 1980
4. Saunders MI, Dische S, Anderson P, Flockhart IR: The neu- rotoxicity of misonidazole and its relationship to dose, half- life and concentration in the serum. Br J Cancer 37, Suppl 1II:268-270, 1978
5. Urtasun RC, Chapman JD, Feldstein ML, Band RP, Rabin HR, Wilson AF, Marynowski B, Starreveld E, Shnitka T: Peripheral neuropathy related to misonidazole: Br J Cancer 37, Suppl 111:271-275, 1978
6. Wasserman TH, Stetz J, Phillips TL: Radiation therapy oncology group clinical trials with misonidazole. Cancer 47:2382-2390, 1981
7. Overgaard J, Andersen AP, Jensen RH, Hjelm-Hansen M,
Jorgensen K, Petersen M, Sandberg E, Sand Hansen H: Mis- onidazole combined with splitcourse radiotherapy in the treatment of invasive carcinoma of the larynx and the phar- ynx. A preliminary report of the Danish Head and Neck Cancer Study (DAHANCA) protocol 2. Acta Otolaryngol, Suppl 386:215-220, 1982
8. Melgaard B, Sand Hansen H, Kamieniecka Z, Paulson OB, Gersel Pedersen A, Tang X, Trojaborg W: Misonidazole neu- ropathy: Ann Neurol 12:10-17, 1982
9. Overgaard J, Overgaard M, Nielsen OS, Kirstein Pedersen Thimoty AR: A comparative investigation of nimorazole and misonidazole as hypoxic radiosensitizers in a C3H mammary carcinoma in vivo. Br J Cancer 46:904-911, 1982
10. Overgaard J, Overgaard M, Timoty AR: Studies of the pharmacokinetic properties of nimorazole. Br J Cancer 48:27-34, 1983
11. Nielsen VK: The peripheral nerve function in chronic renal failure. Acta Med Scan 191:287-296, 1972
12. Urtasun RL, Tanasichuk H, Fulton D, Agboola O, Turner AR, Koziol D, Raleigh J: High-dose misonidazole dexa- methasone rescue: A possible approach to circumvent neuro- toxicity. Int J Radiation Oncology Biol Phys 8:365-368, 1982
13. Moore JL, Paterson ICM, Dawes PJDK, Henk JM: Mis- onidazole in patients receiving radical radiotherapy: Phar- macokinetic effects of phenytoin, tumour response and neu- rotoxicity. Int J Radiation Oncology Biol Phys 8:361-364, 1983
14. Overgaard J, Sand Hansen H, Andersen AP, Hjelm-Hansen M, Jorgensen K, Sandberg E, RygArd J, Jensen RH, Pedersen M: Misonidazole as an adjuvant to radiotherapy in the treat- ment of invasive carcinoma of the larynx and the pharynx. 2nd Interim analysis of the Danish Head and Neck Cancer study (DAHANCA) - protocol 2. In: K/ircher KH et al. (eds): Progress in Radio-Oncology III, ICRO, Vienna, pp 137-147, 1987
Address for offprints: O. B. Paulson, Department of Neurology, Righshopitalet 9, Blegdamsvej, DK-2100 Copenhagen, Denmark