Embed Size (px)
Citation preview

Accession information: (02)00445-3a.pdf (short code: txt001ksb); 11 April 2002ISSN 1462-3994 ©2002 Cambridge University Press
http://www-ermm.cbcu.cam.ac.uk
1
expert reviewsin molecular medicine
Mit
och
on
dri
a as
tar
get
s fo
r d
etec
tio
n a
nd
tre
atm
ent
of
can
cer
Mitochondria as targets for detection
and treatment of cancer
Josephine S. Modica-Napolitano and Keshav K. Singh
Mitochondria are dynamic intracellular organelles that play a central role inoxidative metabolism and apoptosis. The recent resurgence of interest in thestudy of mitochondria has been fuelled in large part by the recognition thatgenetic and/or metabolic alterations in this organelle are causative orcontributing factors in a variety of human diseases including cancer. Severaldistinct differences between the mitochondria of normal cells and cancer cellshave already been observed at the genetic, molecular and biochemical levels.As reviewed in this article, certain of these alterations in mitochondrial structureand function might prove clinically useful either as markers for the earlydetection of cancer or as unique molecular sites against which novel andselective chemotherapeutic agents might be targeted.
Josephine S. Modica-NapolitanoAssociate Professor, Department of Biology, Merrimack College, North Andover, MA 01845, USA.Tel: +1 978 837 5000 x4459; Fax: +1 978 837 5029; E-mail: [email protected]
Keshav Singh (corresponding author)Assistant Professor, Johns Hopkins Oncology Center, Bunting-Blaustein Cancer Research Building,1650 Orleans St, Baltimore, MD 21231, USA. Tel: +1 410 614 5128; Fax: +1 410 502 7234/7244; E-mail:[email protected]
Early studies of differences between themitochondria of normal cells and those ofcancer cells focused on the respiratorydeficiencies common to rapidly growing cancercells. This led Otto Warburg to propose in 1930that respiratory deficiency might result in de-differentiation of cells and hence neoplastictransformation (Refs 1, 2). Other early studiessuggested that transformation was the result ofsubmolecular micro-electronic changes involvingerrant dismantling and rebuilding of the electrontransport chain during cell division (Ref. 3), andthat mutations in mitochondria might causecancers (Ref. 4). More recently, a great deal ofresearch has been conducted that substantiates,extends and provides new insight into the role
of mitochondria in cancer (Refs 5, 6, 7, 8). Thisreview summarises the important aspects ofmitochondrial structure and function, highlightsthe observed differences in mitochondria betweennormal and cancer cells, and discusses how thesedifferences might be exploited in the detection andtreatment of cancer.
Mitochondria structure,function and genome
Historical perspectiveEarly cytological studies (reviewed in Ref. 9)indicated the presence of subcellular granulessimilar in size and shape to bacteria in a varietyof different cell types. In 1890, Altman postulatedthat these granules, which he termed ‘bioblasts’,

Accession information: (02)00445-3a.pdf (short code: txt001ksb); 11 April 2002ISSN 1462-3994 ©2002 Cambridge University Press
http://www-ermm.cbcu.cam.ac.uk
2
expert reviewsin molecular medicine
Mit
och
on
dri
a as
tar
get
s fo
r d
etec
tio
n a
nd
tre
atm
ent
of
can
cer
were the basic units of cellular activity.Interestingly, Altman further speculated thatbioblasts were capable of an independentexistence, yet formed a colonial association withthe cytoplasm of a host cell, and that it wasthrough this association that the host cell acquiredthe properties of life. The term ‘mitochondrion’,meaning thread-like granule, was first applied tothese subcellular structures by Benda in 1898 .
During the period 1900–1930, most cytologistsrecognised the mitochondrion as a well-definedand ubiquitous organelle, although at that timethere was no agreement about its function. Theidentification of mitochondria as centres of energymetabolism came at the heels of refinements incell fractionation techniques during the late 1940s,which allowed the successful separation ofrelatively pure, functionally intact mitochondriafrom other cellular components in liver cellhomogenates (Refs 10, 11). By 1949, thesemitochondrial fractions were shown to containsuccinate oxidase and cytochrome oxidaseactivities, as well as the enzyme systems requiredfor fatty acid oxidation and the citric acid cycle(Refs 12, 13; reviewed in Ref. 9). Today, it is knownthat mitochondria produce up to 80% of theenergy needs of a cell and perform a host ofadditional cellular functions.
Mitochondrial structureThe mitochondria of different tissues are similarin their gross morphology (reviewed in Ref. 9). Inelectron micrographs of fixed tissue specimens,mitochondria are most commonly observed asoval particles, 1–2 µm in length and 0.5–1 µm inwidth. These dimensions approximate to those ofthe bacterium Escherichia coli. The organelle isbounded by two membranes. The peripheral, orouter, membrane encloses the entire contents ofthe mitochondrion. The inner membrane has amuch greater surface area and forms a series offolds or invaginations, called cristae, which projectinward towards the interior space of the organelle.The total surface area of the inner membranevaries considerably depending upon the tissueand type of cell. Since the enzymes involved inoxidative phosphorylation are located on theinner mitochondrial membrane, its surface areaand number of cristae are generally correlatedwith the degree of metabolic activity exhibited bya cell. The spatial arrangement of the outer andinner membranes creates two distinct internalcompartments: the intermembrane space is
located between the outer and inner membranes;and the matrix is the space enclosed by the innermitochondrial membrane.
By contrast to the static, ‘cigar-shaped’organelles commonly observed in electronmicrographs, living cells stained with thelipophilic cation rhodamine 123 (Rh123) andobserved by fluorescence microscopy revealmitochondria as a dynamic network of longfilamentous structures, capable of profoundchanges in size, form and location (Ref. 14). Thesemitochondria can be seen extending, contracting,fragmenting and even fusing with one another asthey move in three dimensions throughout thecytoplasm. Interestingly, the treatment of cellswith microtubule-depolymerising agents has beenshown to result in an altered distribution ofmitochondria (Refs 15, 16). This suggests thatmitochondria are associated with and travel alonga molecular ‘highway’ composed of a cytoplasmicmicrotubule network.
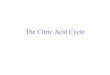
Mitochondrial functionMitochondria play a central role in oxidativemetabolism in eukaryotes (reviewed in Ref. 9).In the catabolism of carbohydrates (Fig. 1a), thisbegins with the transport of pyruvate fromthe cytosol into the mitochondrion, and itssubsequent oxidative decarboxylation to acetylCoA by a soluble, multi-enzyme pyruvatedehydrogenase complex, which is located in themitochondrial matrix. The oxidation of acetylCoA is achieved by a cyclic process involvingeight catalytic steps. This process is known aseither the citric acid or the tricarboxylic acid(TCA) cycle. All but one of the TCA cycleenzymes are soluble proteins found in the innermitochondrial matrix compartment. The singleinsoluble enzyme, succinate dehydrogenase, istightly bound to the matrix side of the innermitochondrial membrane. Each round of theTCA cycle results in the production of twomolecules of CO2, three molecules of reducednicotinamide adenine dinucleotide (NADH), onemolecule of reduced flavin adenine dinucleotide(FADH2), and one molecule of GTP (the energeticequivalent of ATP).
The next stage of aerobic metabolism isoxidative phosphorylation, an energy-generatingprocess that couples the oxidation of respiratorysubstrates (such as the NADH and FADH2generated through the TCA cycle) to the synthesisof ATP. Substrate oxidation involves a series of

Accession information: (02)00445-3a.pdf (short code: txt001ksb); 11 April 2002ISSN 1462-3994 ©2002 Cambridge University Press
http://www-ermm.cbcu.cam.ac.uk
3
expert reviewsin molecular medicine
Mit
och
on
dri
a as
tar
get
s fo
r d
etec
tio
n a
nd
tre
atm
ent
of
can
cer
Figure 1. Schematic of key mitochondrial metabolic pathways. (a) Carbohydrate metabolism. Pyruvateproduced from glycolysis undergoes oxidative decarboxylation to acetyl CoA, which is then oxidised in aneight-step process known as the tricarboxylic acid (TCA) cycle. The respiratory substrates NADH and FADH2
generated through the TCA cycle are next oxidised in a process coupled to ATP synthesis. Electrons aretransferred from NADH and FADH2 to oxygen via enzyme complexes located on the inner mitochondrialmembrane. Three of the electron carriers (complexes I, III and IV) are proton pumps, and couple the energyreleased by electron transfer to the translocation of protons from the matrix side to the external side of the innermitochondrial membrane. Energy stored in the resulting proton gradient (i.e. the proton-motive force) is usedto drive the synthesis of ATP via the mitochondrial enzyme ATP synthetase (complex V). (b) Fatty acid oxidation.Fatty acids undergo oxidative decarboxylation in the mitochondrial matrix to give acetyl CoA, which is fed intothe TCA cycle, and new acyl CoA molecules that are successively shortened with each round of the cycle.Under certain conditions (e.g. fasting), acetyl CoA molecules are converted into ketones for use as an alternativeenergy source. (c) Urea cycle. Amino acid degradation resulting in excretion of nitrogen as urea occurs partlyin the mitochondrion. The mitochondrion is also essential for several other processes (not shown), includinggluconeogenesis, regulation of cytosolic NAD+, intracellular homeostasis of inorganic ions, and apoptosis(fig001ksb).
Fatty acid oxidationCarbohydrate metabolism
Ornithine
Citrulline
(Sometimes)e.g. fastingor disease
Ketones
(Mostly)
ATP
NADHFADH2
GTPCO2
Acetyl CoA Acetyl CoA
Pyruvate Fatty acidsUrea
Ureacycle
Urea cycle
Cytosol
Matrix ofmito-chondrion
Membrane
a b c
Schematic of key mitochondrial metabolic pathwaysExpert Reviews in Molecular Medicine C 2002 Cambridge University Press
Oxidativedecarbox-ylase
Oxidativedecarbox-ylase
Oxidation TCAcycle V
V
Fattyacidcycle
V
V
Oxidativephosphorylation
Succinatedehydrogenase(inner membrane)
+
+
+
+
+
Respiratory enzymecomplexes I-V(inner membrane)
Energy use: in cytosol(and by mitochondrion)
Energy source: brainheart, etc.
Adenine nucleotidetranslocase
Solubleenzymesin matrix
Matrixenzymes
β-oxidation

Accession information: (02)00445-3a.pdf (short code: txt001ksb); 11 April 2002ISSN 1462-3994 ©2002 Cambridge University Press
http://www-ermm.cbcu.cam.ac.uk
4
expert reviewsin molecular medicine
Mit
och
on
dri
a as
tar
get
s fo
r d
etec
tio
n a
nd
tre
atm
ent
of
can
cer
respiratory enzyme complexes that are located onthe inner mitochondrial membrane and arecapable of accepting and donating electrons ina specific sequence based on their relativeoxidation–reduction potentials and substratespecificity. Complex I (NADH-ubiquinonereductase) transfers electrons from NADH tothe mobile electron carrier ubiquinone, orcoenzyme Q. It is the largest and most labileof all the respiratory enzyme complexes. Inbovine heart, for example, complex I comprisesat least 41 different protein subunits. ComplexII (succinate-ubiquinone reductase) transfersreducing equivalents from succinate toubiquinone. It comprises four protein subunits,one of which is the FADH2-linked TCA cycleenzyme succinate dehydrogenase. Complex III(ubiquinone-cytochrome c reductase) is an 11-subunit respiratory enzyme complex involved inthe transfer of electrons from membrane-boundubiquinone to oxidised cytochrome c, anothermobile electron carrier located on the outer surfaceof the inner mitochondrial membrane. ComplexIV, or cytochrome c oxidase (COX), is the terminalelectron acceptor. It comprises 13 different proteinsubunits and functions in the transfer of electronsfrom reduced cytochrome c to molecular oxygen,to form H2O.
The energy released by the exergonic transferof electrons from respiratory substrate tooxygen is coupled to the translocation ofprotons from the matrix side to the external sideof the inner mitochondrial membrane at threesites: respiratory enzyme complexes I, III and IV.In intact, well-coupled mitochondria, the innermembrane is relatively impermeable to theback flow of these protons. According to theChemiosmotic Hypothesis, which was firstproposed by Peter Mitchell in 1961 (and for whichhe received the Nobel Prize in Chemistry in 1978),the energy stored in the resulting proton gradient(i.e. the proton-motive force) is used to drive thesynthesis of ATP via complex V, the mitochondrialenzyme ATP synthetase (Ref. 17).
The ATP that is produced by aerobicmetabolism and not used by the mitochondrionis transported across the inner mitochondrialmembrane in exchange for cytosolic ADP by theenzyme adenine nucleotide translocase (ANT).This exchange ensures not only the availabilty ofmitochondrial ADP, which is the principalcontrol molecule for the rate of oxidativephosphorylation, but also the availability of
cytosolic ATP. Oxidative phosphorylation thussupplies a majority of the cellular energyproduced under aerobic conditions and requiredto sustain cell viability and normal cell functions.
Fatty acid oxidation is another importantmetabolic activity located in the mitochondria(Fig. 1b). The beta-oxidation pathway involvesfour separate enzymes that are soluble in themitochondrial matrix and that function in arepetitive cycle. With each round of the cycle, afatty acid undergoes oxidative decarboxylation toproduce one molecule of acetyl CoA and onemolecule of a new acyl CoA that is two carbonsshorter than the starting fatty acid. The processcontinues until the original fatty acid molecule iscompletely degraded to acetyl CoA (for example,the 16-carbon palmitoyl CoA would undergoseven rounds of beta-oxidation to yield eightmolecules of acetyl CoA). The acetyl CoAmolecules thus generated normally enter into theTCA cycle where they undergo oxidation to CO2.However, during conditions of prolonged fastingand starvation, or in certain metabolic diseases(e.g. diabetes mellitus), the acetyl CoA moleculesgenerated by fatty acid oxidation are convertedinto ketones (e.g. β-hydroxybutyrate, acetoacetateand acetone) by enzymes also located in themitochondrial matrix. These molecules are thentransported through the blood to other tissues,such as brain and heart, where they are used asan alternative energy source to glucose.
In addition to its central role in oxidativemetabolism, the mitochondrion is involved in avariety of other important cellular functions. Forexample, certain enzymes of the urea cycle (Fig.1c) and gluconeogenesis are located in themitochondrial matrix. Mitochondria are involvedin the regeneration of cytosolic NAD+ (requiredfor the substrate-level phosphorylation step inglycolysis) and in the intracellular homeostasis ofinorganic ions such as calcium and phosphate. Awealth of recent studies show that mitochondriaalso play an integral role in the cascade ofintracellular events that lead to apoptosis, orprogrammed cell death (Refs 18, 19).
Mitochondrial genomeMammalian cells typically contain 103–104 copiesof mitochondrial DNA (mtDNA). The genome isa 16.5 kb closed-circular, double-helical moleculethat encodes two rRNAs, 22 tRNAs and 13polypeptides (reviewed in Ref. 5). Each of thesepolypeptides is a highly hydrophobic subunit of

Accession information: (02)00445-3a.pdf (short code: txt001ksb); 11 April 2002ISSN 1462-3994 ©2002 Cambridge University Press
http://www-ermm.cbcu.cam.ac.uk
5
expert reviewsin molecular medicine
Mit
och
on
dri
a as
tar
get
s fo
r d
etec
tio
n a
nd
tre
atm
ent
of
can
cer
one of four respiratory enzyme complexeslocalised to the inner mitochondrial membrane.They include seven subunits of respiratoryenzyme complex I, one subunit of complex III,three subunits of complex IV, and two subunitsof complex V. All other mitochondrial proteins,including those involved in the replication,transcription and translation of mtDNA, areencoded by nuclear genes and are targeted tothe mitochondrion by a specific transportsystem (Ref. 20). In humans and other mammals,mitochondrial genes display a maternalinheritance (i.e. are inherited from the femaleparent). This is probably because the number ofmtDNA copies in the egg is typically 103-foldgreater than that in the sperm (Ref. 21).Alternatively, paternal genomes and organellesmight be preferentially degraded in the zygote(Refs 22, 23).
Although the mitochondrial and nucleargenomes are physically distinct, the high degreeof functional interdependence between them issuggestive of a host–parasite relationship. The‘endosymbiont’ theory proposes that early inthe evolution of the eukaryote, a primitive proto-eukaryote cell that was incapable of aerobicrespiration served as host to a eubacteriumwith the unique capacity for oxidativemetabolism (Ref. 24). During the early stages ofthis endosymbiotic association, the eubacteriumretained its genetic autonomy. In time, however,most of its genetic material was transferred to thenuclear genome of the host. The resultingmitochondrion retained only those few (i.e. 13)genes encoding polypeptides that are essential toaerobic ATP production yet have a hydrophobicitythat precludes nuclear synthesis and cytoplasmictransport to mitochondria. It is of interest torecall Altman’s perceptive characterisation ofmitochondrial function, and his suggestion of acolonial association between the newly discovered‘bioblasts’ and the host cell within which theyreside.
Mitochondria and diseaseThe first mitochondrial disease was describedby Rolf Luft in 1962 (Ref. 25), a year prior tothe discovery of mtDNA (Ref. 26). At thegenetic level, mitochondrial disease was notdefinitively described until 1988 with theidentification of mtDNA mutations in patientswith mitochondrial myopathies, as well as themolecular genetic characterisation of patients
with Leber’s hereditary optic neuropathy andfamilial mitochondrial encephalomyopathy(Refs 27, 28, 29). Since then, there has been asteady growth in the list of diseases associatedwith mitochondrial dysfunction arising frommtDNA mutations (Table 1).
Although mtDNA represents less than 1% oftotal cellular DNA, its gene products are essentialfor normal cell function. Unlike nuclear DNA,mammalian mtDNA contains no introns, has noprotective histones and is exposed to deleterious
Table 1. Mitochondrial diseasesa
(tab001ksb)
Tissue/organaffected Clinical condition
Blood Pearson’s syndrome
Brain SeizuresMyoclonusAtaxiaStrokeDemetiaMigraine
Colon Pseudo-obstruction
Eye Optic neuropathyOphthalmoplegiaRetinopathy
Heart Conduction disorderWolff–Parkinson–White
syndromeCardiomyopathy
Inner ear Sensorineural hearing loss
Kidney Fanconi’s syndromeGlomerulopathy
Liver Hepatopathy
Skeletal muscle MyopathyNeuropathy
a Data in the table are derived from Ref. 38.Mitochondrial diseases can arise from mutations innuclear DNA or in mitochondrial DNA. Deficits inATP production might result from altered functionsof proteins involved directly in oxidativephosphorylation or involved in communicationbetween the nucleus and mitochondria, and mighthave deleterious effects on several organ systems.Many mitochondrial diseases are so new that theyhave not yet been mentioned in the medicaltextbooks or in the medical literature.

Accession information: (02)00445-3a.pdf (short code: txt001ksb); 11 April 2002ISSN 1462-3994 ©2002 Cambridge University Press
http://www-ermm.cbcu.cam.ac.uk
6
expert reviewsin molecular medicine
Mit
och
on
dri
a as
tar
get
s fo
r d
etec
tio
n a
nd
tre
atm
ent
of
can
cer
reactive oxygen species generated by oxidativephosphorylation. In addition, replication ofmtDNA might be error prone (Refs 8, 30, 31, 32,33, 34). The accumulation of mutations in mtDNAis approximately tenfold greater than that innuclear DNA (Refs 35, 36).
Inherited disorders of mitochondria producechildhood and adult diseases with a variety ofclinical symptoms (Ref. 37). Mitochondrialdysfunction has been found frequently as thebasis of developmental defects. It is estimated thatof the 4 million children born each year in theUSA, up to 4000 develop diseases related tomitochondrial dysfunction (Refs 5, 30). Congenitalmitochondrial diseases such as Kearns–Sayre/chronic progressive external opthalmoplegia andLeber’s hereditary optic neuropathy are eithermaternally inherited or are derived from afounder mutation early in embryogenesis. Sincemitochondria perform a variety of differentfunctions in different tissues, since the proportionof normal to mutated mtDNA can vary, and sincetissues have different aerobic dependencies, eachmtDNA mutation can produce a wide spectrumof phenotypes that have proven to be extremelyperplexing to scientists and physicians.
Mitochondrial dysfunction is also increasinglyrecognised as an important cause of adult humanpathology (reviewed in Ref. 5). Dysfunctionalmitochondria are found in diverse adult-onsetdiseases, including diabetes, cardiomyopathy,infertility, migraine, blindness, deafness, kidneyand liver diseases, and stroke. The accumulationof somatic mutations in mtDNA has beensuggested to play a causative or contributingrole in aging, in age-related neurodegenerativedisorders such as Parkinson’s, Alzheimer’s andHuntington’s disease, and in cancer (seebelow). Other adult-onset pathologies mightresult from the biochemical toxicity or mtDNAdamage caused by various drugs, including thoseused against human immunodeficiency virus(HIV) (Ref. 38), or by other endogenous orenvironmental agents (Refs 30, 39). Althoughhuman mitochondrial diseases are often multi-system disorders, constitutively highly oxidativetissues such as myocardium, brain and kidney,as well as episodically oxidative tissues suchas skeletal muscle, are especially vulnerable tomtDNA damage (Refs 35, 36). To date, over100 point mutations and 200 deletions andrearrangements have been shown to be associatedwith mitochondrial disease and new mutations
are being described every year (Ref. 37). Thus,mitochondria play a central role in many diseasesthat can affect any organ, at any age.
Mitochondria and cancerPhenotypic differences in tumourmitochondriaCancer cells have an altered metabolism thatincludes: a higher rate of glycolysis (Ref. 39), anincreased rate of glucose transport (Ref. 40),increased gluconeogenesis (Ref. 41), reducedpyruvate oxidation and increased lactic acidproduction (Ref. 42), increased glutaminolyticactivity (Ref. 43), reduced fatty acid oxidation (Ref.44), increased glycerol and fatty acid turnover(Ref. 45), modified amino acid metabolism (Ref.46), and increased pentose phosphate pathwayactivity (Ref. 47).
Mitochondria are involved either directly orindirectly in many aspects of altered metabolismin cancer cells (Ref. 48) and several notabledifferences between the mitochondria of normalversus transformed cells have been discovered(reviewed in Refs 49, 50 and 51). For example,various tumour cell lines exhibit differences inthe number, size and shape of their mitochondriarelative to normal controls. The mitochondria ofrapidly growing tumours tend to be fewer innumber, smaller and have fewer cristae thanmitochondria from slowly growing tumours;the latter are larger and have characteristicsmore closely resembling those of normal cells.Interestingly, the usually benign oncocytoma ofthyroid, salivary gland, kidney, parathyroidand breast is characterised by the presence ofcells containing abnormally large numbers ofmitochondria, and high levels of oxidativeenzymes (Ref. 52). The ultrastructural featuresof mitochondria in these cells show similaritieswith mitochondrial encephalomyopathies, wheremitochondria are found as large aggregates anddisplay a variety of morphological alterations.MtDNA mutations are also commonly found inoncocytic tumours (Ref. 52).
Alterations in the molecular composition of theinner membranes of tumour mitochondria havealso been noted (Refs 53, 54, 55, 56, 57, 58).Polypeptide profiles of normal liver versushepatoma mitochondria demonstrate differencesin the appearance and/or relative abundance ofseveral protein subunits. One major band that isdeficient or absent in several tumours studied hasa mobility near or equal to the B subunit of the F1-

Accession information: (02)00445-3a.pdf (short code: txt001ksb); 11 April 2002ISSN 1462-3994 ©2002 Cambridge University Press
http://www-ermm.cbcu.cam.ac.uk
7
expert reviewsin molecular medicine
Mit
och
on
dri
a as
tar
get
s fo
r d
etec
tio
n a
nd
tre
atm
ent
of
can
cer
ATPase (approximately 57 kDa). Other bands thatare present in tumour mitochondria appear to bedeficient or absent in control mitochondria. Inaddition, analysis of the inner membrane lipidcomposition of various tumour mitochondria hasindicated elevated levels of cholesterol, varyingtotal phospholipid content, and/or changes in theamount of individual phospholipids relative tonormal controls.
Many differences in the mitochondria ofnormal versus transformed cells have also beennoted with regard to: (1) the preference forsubstrates oxidised; (2) the magnitude of theacceptor control ratio; (3) the rates of electron andanion transport; (4) the capacity to accumulate andretain calcium; (5) the amounts and forms of DNA;and (6) the rates of protein synthesis and organelleturnover. However, there is apparently nouniversal metabolic alteration that is commonto all tumours. For example, although thepathogenesis of prostate cancer involves themitochondrial metabolic transformation of citrate-producing cells to citrate-oxidising cells, thismetabolic abnormality is not reported in othercancers (Ref. 59). Additionally, it is important tonote that the altered metabolism in cancer cells isprobably not the cause of malignancy but, rather,a secondary, albeit essential, adaptation to supportmalignant activities (Ref. 59).
Rh123 uptakeIn the early 1980s, Chen and colleagues discoveredan interesting phenotype that was found to becommon to nearly all types of carcinoma tested(Refs 14, 60, 61). It was observed that the lipophiliccation Rh123 could serve as a highly specificvital stain for mitochondria, providing low-background, high-resolution fluorescent imagesof the organelle in a variety of cell types (Fig. 2).It was further observed that relative to themitochondria of normal epithelial cells, themitochondria of carcinoma cells displayed anincreased uptake and prolonged retention ofRh123, and that this phenomenon correlated witha selective cytotoxicity for carcinoma cells in vitroand in vivo (Refs 62, 63, 64). For example, whereasRh123 was shown to have a minimal effect on theclonal growth of those cell types that display littleuptake and short retention of the dye (e.g. primarycultures of normal mouse bladder epithelial cells;and CCL-34 and BSC-1, the non-tumourigenicdog and monkey kidney epithelial cell lines,respectively), it markedly inhibited the clonal
growth of those cultured carcinomas cell lines thatdisplay high uptake and prolonged retention ofRh123 (e.g. MB49, the transformed mouseepithelial cell line; and MCF-7 and HUT, thehuman breast and lung carcinoma cell lines,respectively). In addition, at a constant exposureof 10 µg/ml Rh123, greater than 50% cell deathoccurred within seven days in 9/9 of thecarcinoma cell types tested, whereas 6/6 controlepithelial cell types remained unaffected.Standard chemotherapeutic agents such asarabinosyl cytosine (Ara-c) and methotrexateexhibit no such selectivity for carcinoma cells. Invivo, Rh123 was shown to prolong the survivalof mice implanted with Ehrlich ascites tumouror MB49 mouse bladder carcinoma cells asmuch as 260%, although the extent of survivalprolongation was highly dependent on the doseand schedule of administration of the dye. Asexpected, Rh123 did not significantly prolong thesurvival rate of mice implanted with tumoursof cell types shown to be short retainers of thedye (e.g. L1210 and P388 leukaemias, and B6melanoma).
Figure 2. Mitochondria of neuron revealed bystaining with a rhodamine 123 derivative. Neuronswere stained with tetramethylrhodamine, ethylester, perchlorate (TMRE). TMRE accumulates inmitochondria and emits high fluorescence. The cellimages were recorded with a digital camera andprocessed to generate high-resolution images. Theimage is courtesy of Dr Gary E. Gibson, Weill MedicalCollege of Cornell University, Burke MedicalResearch Institute, White Plains, NY 10605, USA.Magnification, ~X760 (fig002ksb).
Mitochondria of neuron revealed by staining with a rhodamine 123 derivativeExpert Reviews in Molecular Medicine C 2002 Cambridge University Press

Accession information: (02)00445-3a.pdf (short code: txt001ksb); 11 April 2002ISSN 1462-3994 ©2002 Cambridge University Press
http://www-ermm.cbcu.cam.ac.uk
8
expert reviewsin molecular medicine
Mit
och
on
dri
a as
tar
get
s fo
r d
etec
tio
n a
nd
tre
atm
ent
of
can
cer
Increased membrane potential incarcinoma cellsIt became apparent from early studies that twochemical properties of Rh123 were important inpromoting its uptake into mitochondria. The firstis the lipophilicity of Rh123, which allows thecompound to penetrate the hydrophobic barriersof the plasma and mitochondrial membranes; andthe second is its electrical charge – rhodaminesthat are positively charged at physiological pHstain mitochondria specifically, whereas theneutral rhodamines do not (Ref. 14). Initially, therewas much indirect evidence to suggest that Rh123uptake occurs as a function of the magnitude ofthe mitochondrial membrane potential. Forexample, the addition of ionophores that dissipatethe mitochondrial electrical gradient (such asvalinomycin or dinitrophenol), or respiratoryinhibitors that prevent the establishment of theelectrical gradient (such as cyanide, antimycin orrotenone), were demonstrated to diminishmitochondrial-specific fluorescence in cells pre-stained with the dye (Ref. 61). Later, experimentalmanipulation of the membrane potential inisolated mitochondria and concurrentmeasurement of the amount of Rh123 associatedwith the organelle definitively established thatRh123 is concentrated by cells and intomitochondria in response to negative-insidetransmembrane potentials (Ref. 65). Furthermore,it was determined that the mitochondrialmembrane potential of carcinoma cells isapproximately 60 mV higher than that of controlepithelial cells (Ref. 65). Since Rh123 distributesacross the inner mitochondrial membrane inaccordance with the Nernst equation (Ref. 66), thisdifference alone is sufficient to account for atenfold greater accumulation of the compound incarcinoma versus control epithelial mitochondria.In whole cells, however, the plasma membranepotential pre-concentrates Rh123 relative to theexternal medium, thus affecting the cytoplasmicconcentration of Rh123 and the amount of dyeavailable for mitochondrial uptake. The higherplasma membrane potential observed in somecarcinoma cells versus control epithelial cell typestherefore further contributes to increased Rh123accumulation in carcinoma mitochondria (Ref.67). Finally, Rh123 was found to exhibit aconcentration-dependent toxicity in mitochondriaby inhibition of ATP synthetase (Refs 68, 69). Sincemitochondria are the primary sites of ATPsynthesis in cells undergoing aerobic metabolism,
selective mitochondrial toxicity in carcinoma cellsresulting from enhanced uptake and retention ofRh123 provided the basis for the selective anti-carcinoma activity displayed by this compound.
Delocalised lipophilic cationsRh123 provided a prototype for a new class ofanti-cancer agents that exploit the difference inmitochondrial membrane potential betweennormal epithelial and carcinoma cells to achievea selective mitochondrial toxicity and consequentselective cytotoxicity for carcinoma cells. In thepast few years, several members of this class ofcompounds, known collectively as delocalisedlipophilic cations (DLCs), have exhibited at leastsome degree of efficacy in carcinoma cell killingin vitro and/or in vivo (Refs 70, 71, 72, 73, 74, 75).For example, dequalinium chloride (DECA) hasdemonstrated 100-fold greater inhibition of theclonal growth of carcinoma versus controlepithelial cells in culture, anti-carcinoma activityin human colon adenocarcinoma cells injectedsubcutaneously in nude mice, and significantregression of tumours in rats carrying in situmammary adenocarcinomas induced bydimethyl-bezanthracene (Refs 71, 72). Thethiopyrylium AA-1 was shown to prolong thesurvival of mice implanted with either mousebladder carcinoma, human melanoma, andhuman ovarian carcinoma cell lines, achievingtreated:control ratios as high as 450% (Ref. 74).The rhodacyanine MKT-077 also appearsparticularly promising (Refs 73, 76, 77). In recentstudies, MKT-077 demonstrated significantgrowth-inhibitory activity against a variety ofkeratin-positive human cancer cell lines, asmeasured by clonogenic assays and growthinhibition of cultured cells. In vivo, MKT-077demonstrated significant anti-tumour activity innude mice implanted with either the humanmelanoma LOX, the human renal carcinoma A498,or the human prostate carcinoma DU145, all ofwhich are highly refractory to a variety oftraditional therapies. As the first DLC with afavourable pharmacological and toxicologicalprofile in preclinical studies, MKT-077 hasundergone Phase I clinical trials, approved by theUS Food and Drug Administration, for thetreatment of carcinoma.
Mechanism of action of DLCsIt is of interest to note that, although all DLCs aretaken up into mitochondria by a common

Accession information: (02)00445-3a.pdf (short code: txt001ksb); 11 April 2002ISSN 1462-3994 ©2002 Cambridge University Press
http://www-ermm.cbcu.cam.ac.uk
9
expert reviewsin molecular medicine
Mit
och
on
dri
a as
tar
get
s fo
r d
etec
tio
n a
nd
tre
atm
ent
of
can
cer
mechanism (i.e. in response to negative-insidetransmembrane potentials), the mechanism ofmitochondrial toxicity exhibited by thesecompounds is quite varied. For example, amongthe DLCs that display a concentration-dependenttoxicity to mitochondria, Rh123 and AA-1 inhibitmitochondrial ATP synthesis at the level of F0F1-ATPase activity (Refs 68, 74), whereas DECA andcertain DLC thiacarbocyanines interfere withNADH-ubiquinone reductase activity (Refs 70,72). In addition, the selective cytotoxicity tocarcinoma cells exhibited by MKT-077 in vitroand in vivo has been attributed to a selectiveinhibition of mitochondrial respiration in cancercells, most probably as a result of a generalperturbation of mitochondrial membranes andconsequent inhibition of the activity ofmembrane-bound enzymes (Ref. 76). The selectivecytotoxicity might also be a consequence of a mildto moderate degradative effect on mtDNA, butnot nuclear DNA, of various carcinoma cell types(Ref. 76).
It is of further interest to note that, althoughincreased membrane potential is necessary toachieve selective cytotoxicity by DLCs, it alone isnot sufficient. If this were the case then cardiacmuscle cells, which have also been shown toexhibit a high mitochondrial membrane potential(Ref. 78), would be susceptible to the cytotoxiceffects of these compounds. Yet significant cardiactoxicity has not been observed following in vivoadministration of either MKT-077 or DECA. Thissuggests the sensitivity of any particular celltype to the effects of DLCs might depend ondifferent cytoplasmic characteristics, such as thoseinvolving the kinetics of uptake and retention ofthe compound, or on properties inherent to themitochondria, such as differential sensitivity ofthe target molecule against which the DLC exertsits cytotoxic effect.
DLCs and photochemotherapySome research groups have explored the use ofcertain DLCs in photochemotherapy (PCT), aninvestigational cancer treatment involvinglight activation of a photoreactive drug, orphotosensitiser, that is selectively taken up orretained by malignant cells (Refs 79, 80, 81, 82).There has been considerable interest recently inPCT as a form of treatment for neoplasms of theskin, lung, breast, bladder, brain or any othertissue accessible to light transmitted eitherthrough the body surface or internally via fibre
optic endoscopes. Cationic photosensitisers areparticularly promising as potential PCT agents.Like other DLCs, these compounds areconcentrated by cells into mitochondria inresponse to negative-inside transmembranepotentials, and are thus selectively accumulatedin the mitochondria of carcinoma cells. In responseto localised photoirradiation, the photosensitisercan be converted to a more reactive and highlytoxic species, thus enhancing the selective toxicityto carcinoma cells and providing a means ofhighly specific tumour cell killing without injuryto normal cells.
Several cationic photosensitisers have shownpromise for use in PCT. For example, selectivephototoxicity of carcinomas in vitro and in vivohas been observed for a series of triarylmethanederivatives (Ref. 83), and for 2-ethyl-1,3-dioxylenekryptocyanine (EDKC) (Ref. 77). Both Rh123 andthe chalcogenapyrylium dye 8b have beenevaluated as photosensitisers for thephotochemotherapy of malignant gliomas (Refs84, 85, 86). As is the case for the non-photosensitising DLCs, the mitochondrion hasbeen implicated as an important, perhaps primary,subcellular site of damage by these and severalother cationic photosensitisers (Refs 79, 87, 88, 89,90, 91). Again, the mechanisms of mitochondrialtoxicity exhibited by these compounds have beenshown to vary from an inhibition of NADH-ubiquinone reductase (e.g. in the case of EDKC,and the triarylmethane derivative VB-BO) to anon-specific perturbation of mitochondrialfunction most probably resulting from membranedamage induced by singlet oxygen (e.g. in the caseof certain chalcogenapyrylium dyes). Morerecently, photoactivation has been shown toenhance the mitochondrial toxicity of MKT-077,with evidence for the involvement of lipidperoxidation in this process. These results havepositive implications for the use of MKT-077 inPCT.
Future directions for researchinvolving DLCsAlthough the use of DLCs as anti-cancer agentshas shown promise, as yet there is no realunderstanding of the biochemical basis for theincreased mitochondrial membrane potential incarcinoma cells. Consequently, the choice for thedesign or selection of potentially therapeuticlipophilic cations has been based almost solelyon physical properties (i.e. lipid solubilty,

Accession information: (02)00445-3a.pdf (short code: txt001ksb); 11 April 2002ISSN 1462-3994 ©2002 Cambridge University Press
http://www-ermm.cbcu.cam.ac.uk
10
expert reviewsin molecular medicine
Mit
och
on
dri
a as
tar
get
s fo
r d
etec
tio
n a
nd
tre
atm
ent
of
can
cer
delocalisation of positive charge, etc.), andpreliminary screening for the selective cytotoxicityof these compounds has been empirical. Althoughthere is sufficient evidence to support the idea thata therapeutic mechanism based on differencesin mitochondrial membrane potential mightbe exploited for the treatment of cancers, aknowledge of the specific biochemical alterationsthat account for increased mitochondrialmembrane potential in these cells wouldundoubtedly lead to a more rational approach tothe choice of highly selective DLCs for clinical use.To this end, a comprehensive, comparativebiochemical analysis of mitochondria isolatedfrom several control and carcinoma cell lines thatdisplay differences in mitochondrial membranepotential is currently under way (J.S. Modica-Napolitano, unpublished). This type of studywill contribute to an understanding of thephenomenon of increased uptake of DLCs bycarcinoma mitochondria and might also revealmolecular differences between the mitochondriaof normal epithelial and carcinoma cells againstwhich novel, selective and site-specific DLCscould be targeted. The information obtained willbe used in the rational design of a more efficaciousform of DLC that exhibits a dual selectivity forcarcinoma cells based on both differentialaccumulation and selective action against aunique molecular target.
Molecular basis for increased membranepotential in carcinoma cellsIt is logical to assume that the observed differencesin the magnitude of the mitochondrial membranepotential between normal epithelial andcarcinoma cells might arise from differences inthe structure and function of one or more ofthose organelle components that serve to createand/or maintain the electrical gradient.Possibilities include differences in mitochondrialrespiratory enzyme complexes, electron carriers,ATP synthetase, ANT and membrane lipidstructure. Differences that affect electron transferactivity, or proton translocation, utilisation orconductance, are also candidates for the molecularbasis for increased mitochondrial membranepotential in carcinoma cells.
Interestingly, some differences of these typesare already known to exist between themitochondria of normal and malignant cells.For example, under certain assay conditions,mitochondria isolated from hepatomas of varying
growth rates and degrees of differentiationdisplay a decreased capacity for uncoupler-stimulated ATP hydrolysis relative to thatfound in normal liver (Ref. 92). In addition,mitochondria isolated from biopsies of humanhepatocellular carcinoma have decreased ratesof respiration-linked ATP synthesis and areduced phosphorylative capacity compared withnormal human liver (Refs 93, 94). Furthermore,the measured maximal velocity for ATPaseactivity in submitochondrial particles isolatedfrom hepatocellular carcinoma is considerablylower than that in normal liver. It has beensuggested that these alterations in enzymefunction might be associated with a decreasein immunodetectable levels of the B subunitof the F1 component of mitochondrial ATPaseand/or with overexpression of the ATPaseinhibitor protein (IF1) in tumour mitochondria(Refs 93, 94, 95).
COX activityA comparison of COX activities in culturedcarcinoma versus normal epithelial cells suggestsa possible correlation between membranepotential and the activity of this enzyme.Measurements of COX activity in samples fromthe total cellular homogenate and themitochondrial subfraction from the culturedhuman carcinoma cell lines MCF-7 (breast), T47D(breast) and DU-145 (prostate) demonstratesignificantly lower specific activities of theenzyme compared with that measured in thenormal monkey kidney epithelial cell line CV-1(Ref. 96). Similar decreases in COX activity werefound when comparing the specific activity ofthe enzyme in biopsies of human colonicadenocarcinoma versus normal colon mucosa(Ref. 97), and in cultured rat HC252 hepatomacells versus non-neoplastic liver (Ref. 98).
It is not clear whether the decrease in specificactivity of COX in cancer cells can be explainedby alterations in the level of gene expression.For example, in one study involving humancolonic biopsies, the mean level of expression ofmitochondrially encoded COX subunit III wasfound to be lower in carcinoma versus normalmucosa samples (Ref. 99). Cultured HT29 coloncarcinoma cells also exhibited low levels of theCOX III transcript; however, expression of COXIII returned to higher (normal) levels when thecells were induced to differentiate by exposureto sodium butyrate. By contrast, increased

Accession information: (02)00445-3a.pdf (short code: txt001ksb); 11 April 2002ISSN 1462-3994 ©2002 Cambridge University Press
http://www-ermm.cbcu.cam.ac.uk
11
expert reviewsin molecular medicine
Mit
och
on
dri
a as
tar
get
s fo
r d
etec
tio
n a
nd
tre
atm
ent
of
can
cer
levels of RNA transcripts of the nuclear-encodedsubunit COX IV and mitochondrially encodedCOX subunits I and II have been observed inZajdela hepatoma as compared with normal liver(Ref. 100).
Alternatively, and perhaps more interestingly,the decreased specific activity of COX in tumourmitochondria might reflect a kinetic differencecaused by genetic mutations that alter thestructure and function of the enzyme. These samestructural changes might be hypothesised to affectthe proton-pumping capacity of the enzyme,and thus the magnitude of the mitochondrialmembrane potential.
Mitochondrial permeability transitionpore activityThe magnitude of the mitochondrial membranepotential might also be dependent uponmembrane permeability as regulated generallyby the membrane lipid–protein structure, or morespecifically by the mitochondrial permeabilitytransition pore (MPTP). This is a multi-proteinstructure formed at contact sites between the innerand outer mitochondrial membranes. It is avoltage-dependent, cyclosporin-A-sensitive,high-conductance inner membrane channel, theopening of which transiently depolarises themitochondrial membrane potential. Althoughthe complete physiological role of the MPTP isunknown at this time, it is probably involvedin the early apoptotic changes that affectmitochondrial membrane permeability. Severaldifferences have been found when comparing theMPTP in normal versus malignant cells.
One of the key structural components of theMPTP complex is ANT. The primary role of ANTis to facilitate the one-for-one exchange of ATP(out) for ADP (in) across the inner mitochondrialmembrane. More recently, it has been suggestedthat ANT also acts as a non-specific pore thatrenders the mitochondrial inner membranepermeable to solutes less than 1.5 kDa in size (Ref.101). Interestingly, the adenine nucleotideexchange function of ANT is known to bedecreased in certain hepatoma versus normal livermitochondria (Refs 102, 103, 104). In addition, thesensitivity of this enzyme to bongkrekic acid, aninhibitor of both adenine nucleotide exchange andformation of the MPTP is also decreased inhepatoma versus normal liver (Refs 104, 105, 106).Furthermore, high transcript levels for ANT2, thegene encoding one of three isoforms of the
translocase, have been observed in several de-differentiated, proliferating, renal tumour celltypes, whereas expression of ANT2 is usuallyrepressed in quiescent cells (Refs 107, 108).
Additional known or putative MPTPcomponents also exhibit alterations in geneexpression between normal and cancer cells.Among those genes overexpressed in cancer cellsare the anti-apoptotic oncogenes encoding Bcl-2and Bcl-XL, which have a direct inhibitory effecton pore opening, and genes encoding theperipheral benzodiazepin receptor (PBR), thePBR-associated protein Prax-1, and mitochondrialcreatine kinase (Refs 109, 110, 111, 112, 113, 114,115, 116). Conversely, the expression of BAX, a pro-apoptotic, inner mitochondrial membrane proteinthat facilitates pore opening, has been shown tobe reduced in some cancer cell lines (Refs 117, 118).However, whether these changes in geneexpression contribute to steady-state differencesin membrane permeability between normalepithelial and carcinoma cells has yet to bedetermined.
Mitochondrial DNA mutations incarcinoma cellsMitochondrial dysfunction is one of the mostprofound features of cancer cells. Consistently,mutations in mtDNA have been reported in avariety of cancers. These include ovarian, thyroid,salivary, kidney, liver, lung, colon, gastric, brain,bladder, head and neck, and breast cancers, andleukaemia (see Table 2 for references). The typesof mutations observed in mtDNA range frompoint mutations, to deletions and duplications.Most tumours contain homoplasmic (100% pure)mutant mtDNA because of the clonal nature ofcancers (Refs 5, 6, 119).
The abundance and homoplasmic nature ofmitochondria make mtDNA an attractivemolecular marker of cancer. Indeed, mutantmtDNA in tumour cells is reported to be 220 timesas abundant as a mutated nuclear marker (Ref.119). Furthermore, a recent study of mtDNA frompatients with bladder, head and neck, and lungcancers reported that mutated mtDNA is readilydetectable in urine, blood and saliva samplesfrom these patients (Ref. 119). Thus, mtDNAmutation might prove to be an extremely usefulbiomarker for the detection of many cancers.Ongoing research on DNA repair genes involvedin maintaining the genetic integrity of themitochondrial genome combined with further

Accession information: (02)00445-3a.pdf (short code: txt001ksb); 11 April 2002ISSN 1462-3994 ©2002 Cambridge University Press
http://www-ermm.cbcu.cam.ac.uk
12
expert reviewsin molecular medicine
Mit
och
on
dri
a as
tar
get
s fo
r d
etec
tio
n a
nd
tre
atm
ent
of
can
cer
analysis of the nature of mtDNA mutations willgreatly aid progress in this area.
Mitochondrial dysfunction also has importantimplications in cancer therapy. This has beendemonstrated by measuring the cell survivalof a cervical tumour cell line (with parentalmitochondrial function, i.e. Rho+) and itsderivative isogenic cell line that completely lackedmtDNA (with dysfunctional mitochondria, i.e.Rho0) after exposure to a variety of anti-canceragents (Ref. 119). It was found that mitochondrialdysfunction leads to increased cell survivalafter exposure to cancer therapeutic agentssuch as adriamycin and porphyrin-catalysedphototoxicity. By contrast, no measurabledifference was found in the cell survival of theRho+ and Rho0 cells to high doses of ionisingradiation. These results underscore theimportance of the mitochondrial genome indevelopment of cancer therapeutic drugs.
Concluding remarksand clinical implications
The many distinct differences in mitochondrialstructure and function between normal cells andcancer cells offer a unique potential for the clinicaluse of mitochondria as markers for the earlydetection of cancer. Additionally, these differencesoffer the possibility for the design and synthesisof effective anti-cancer agents that deliver potentmitochondrial inhibitors to selectively kill tumourcells (reviewed in Ref. 120). As summarisedpreviously, one current chemotherapeutic strategy
utilises lipophilic cations that accumulateselectively in carcinoma cells in response toincreased mitochondrial membrane potential.An alternative strategy employs mitochondrialprotein-import machinery to delivermacromolecules to mitochondria. For example, amitochondrial signal sequence has been used todirect green fluorescent protein to mitochondria,which allows the visualisation of mitochondriawithin living cells (Ref. 121). Interestingly, certainshort peptides readily penetrate the mitochondrialmembrane and become toxic when internalisedinto the targeted cells by disruption ofmitochondrial membranes (Ref. 122). Anotherchemotherapeutic strategy employs specificinteraction of drugs with certain mitochondrialproteins (Ref. 101).
Traditional chemotherapies, aimed at DNAreplication in actively dividing cells, haveachieved only limited success in the treatment ofcancer largely because of their lack of specificityfor cells of tumourigenic origin. It is important,therefore, to search for novel cellular targetsthat are sufficiently different between normal cellsand cancer cells so as to provide a basis forselective cytotoxicity. As this review suggests, themitochondrion is one such target.
Acknowledgements and fundingWe thank the members of our laboratories for theircontributions to this article. Our research has beensupported by grants from the National Institutesof Health (RO1-097714, P50 CA88843, P20CA86346), an American Heart AssociationScientist Development Award (9939223N) toK.K.S., and a National Institutes of Health grant(R15 Ca78323-01S1) to J.S.M-N. We also thank DrJune R. Aprille, Tufts University, Medford, MA,USA and Lene J. Rasmussen, Roskilde University,Roskilde, Denmark for their helpful critique of thisarticle.
References1 Warburg, O. (1930) Metabolism of Tumors,
Arnold Constable, London, UK2 Warburg, O. (1956) On the origin of cancer cells.
Science 123, 309-3143 Szent-Gyorgyi, A. (1977) Electronic biology and
cancer. In Search and Discovery: A Tribute toAlbert Szent-Gyorgyi (Kaminer, B., ed.,), pp. 329-335, Academic Press, New York, USA
4 Woods, M.W. and DuBuy, H.G. (1945)Cytoplasmic diseases and cancer. Science 102,
Table 2. Mitochondrial DNA mutation incancersa (tab002ksb)
Cancer Refs
Leukaemia 123, 124, 125, 126, 127Ovary 128Thyroid 129, 130Salivary 131, 132Kidney 133, 134, 135Liver 136, 137Lung 138Colon 6, 139Gastric 140Brain 141Goiter 52Breast 142
a Point mutations, deletions or duplications ofmitochondrial DNA mutations are found in a widerange of cancers.

Accession information: (02)00445-3a.pdf (short code: txt001ksb); 11 April 2002ISSN 1462-3994 ©2002 Cambridge University Press
http://www-ermm.cbcu.cam.ac.uk
13
expert reviewsin molecular medicine
Mit
och
on
dri
a as
tar
get
s fo
r d
etec
tio
n a
nd
tre
atm
ent
of
can
cer
591-5935 Singh, K.K. (1998) Mitochondrial DNA
Mutations in Aging, Disease, and Cancer,Springer, New York, USA
6 Polyak, K. et al. (1998) Somatic mutations of themitochondrial genome in human colorectaltumours. Nat Genet 20, 291-293, PubMed ID:99021388
7 Kroemer, G. and Reed, J.C. (2000) Mitochondrialcontrol of cell death. Nat Med 6, 513-519,PubMed ID: 20264559
8 Singh, K.K. (2000) Mitochondrion me and themitochondrial journal. Mitochondrion 1, 1-2
9 Tzagoloff, A. (1982) Mitochondria, Plenum Press,New York, NY, USA
10 Claude, A. (1946) Fractionation of mammalianliver cells by differential centrifugation: II.Experimental procedures and results. J. Exp.Med. 84, 61
11 Hogeboom, G.H., Schneider, W.C. and Palade,G.E. (1948) Cytochemical studies of mammaliantissue. I. Isolation of intact mitochondria from ratliver; some biochemical properties ofmitochondria and submiscroscopic particulatematerial. J. Biol. Chem. 172, 619-635
12 Green, D.E., Loomis, W.F. and Auerbach, V.H.(1948) Studies on the cyclophorase system. I. Thecomplete oxidation of pyruvic acid to carbondioxide and water. J. Biol. Chem. 172, 389-403
13 Kennedy, E.P. and Lehninger, A.L. (1949)Oxidation of fatty acids and tricarboxylic acidcycle intermediates by isolated livermitochondria. J. Biol. Chem. 179, 957-972
14 Johnson, L.V., Walsh, M.L. and Chen, L.B. (1980)Localization of mitochondria in living cells withrhodamine 123. Proc Natl Acad Sci U S A 77, 990-994, PubMed ID: 80145797
15 Aufderheide, K.J. (1980) Mitochondrialassociations with specific microtubularcomponents of the cortex of Tetrahymenathermophila. II. Response of the mitochondrialpattern to changes in the microtubule pattern. JCell Sci 42, 247-260, PubMed ID: 80249708
16 Summerhayes, I.C., Wong, D. and Chen, L.B.(1983) Effect of microtubules and intermediatefilaments on mitochondrial distribution. J CellSci 61, 87-105, PubMed ID: 83291373
17 Mitchell, P. (1961) Coupling of phosphorylationto electron and hydorgen transfer by achemiosmotic type of mechanism. Nature 191,144-148
18 Petit, P.X. and Kroemer, G. (1998) Mitochondrialregulation of apoptosis. In Mitochondial DNA
Mutations in Aging, Disease and Cancer (Singh,K.K., ed.), pp. 147-165, Springer-Verlag, Berlin,Germany
19 Zamzami, N. et al. (1996) Mitochondrial controlof nuclear apoptosis. J Exp Med 183, 1533-1544,PubMed ID: 96261655
20 Schatz, G. (1996) The protein import system ofmitochondria. J Biol Chem 271, 31763-31766,PubMed ID: 97112957
21 Birky, C.W.J. (1994) Relaxed and stringentgenomes: why cytoplasmic genes don’t obeyMendel’s laws. J Hered 85, 355-36624
22 Hiraoka, J. and Hirao, Y. (1988) Fate of sperm tailcomponents after incorporation into the hamsteregg. Gamete Res 19, 369-380, PubMed ID:89065541
23 Kaneda, H. et al. (1995) Elimination of paternalmitochondrial DNA in intraspecific crossesduring early mouse embryogenesis. Proc NatlAcad Sci U S A 92, 4542-4546, PubMed ID:95273399
24 Gray, M.W. (1992) The endosymbiont hypothesisrevisited. Int Rev Cytol 141, 233-357, PubMed ID:93084476
25 Luft, R. et al. (1962) A case of severehypermetabolism of nonthyroid origin with adefect in the maintenance of mitochondrialrespiratory control: a correlated clinical,biochemical and morphological study. J ClinInvest 41, 1776-1804
26 Nass, S. and Nass, M.M.K. (1963)Intramitochondrial fibers with DNAcharacteristics. J Cell Biol 19, 613-629
27 Wallace, D.C. et al. (1988) Mitochondrial DNAmutation associated with Leber’s hereditaryoptic neuropathy. Science 242, 1427-1430,PubMed ID: 89072713
28 Holt, I.J., Harding, A.E. and Morgan-Hughes,J.A. (1988) Deletions of muscle mitochondrialDNA in patients with mitochondrial myopathies.Nature 331, 717-719, PubMed ID: 88143157
29 Zeviani, M. et al. (1988) Deletions ofmitochondrial DNA in Kearns-Sayre syndrome.Neurology 38, 1339-1346, PubMed ID: 88319290
30 Singh, K.K. et al. (2001) Inactivation ofSaccharomyces cerevisiae OGG1 DNA repairgene leads to an increased frequency ofmitochondrial mutants. Nucleic Acids Res 29,1381-1388, PubMed ID: 21138442
31 Kunkel, T.A. and Loeb, L.A. (1981) Fidelity ofmammalian DNA polymerases. Science 213, 765-767, PubMed ID: 81249139
32 Matsukage, A., Bohn, E.W. and Wilson, S.H.

Accession information: (02)00445-3a.pdf (short code: txt001ksb); 11 April 2002ISSN 1462-3994 ©2002 Cambridge University Press
http://www-ermm.cbcu.cam.ac.uk
14
expert reviewsin molecular medicine
Mit
och
on
dri
a as
tar
get
s fo
r d
etec
tio
n a
nd
tre
atm
ent
of
can
cer
(1975) On the DNA polymerase III of mousemyeloma: partial purification andcharacterization. Biochemistry 14, 1006-1020,PubMed ID: 75146411
33 Shay, J.W. and Werbin, H. (1987) Aremitochondrial DNA mutations involved in thecarcinogenic process? Mutat Res 186, 149-160,PubMed ID: 87315142
34 Torri, A.F., Kunkel, T.A. and Englund, P.T. (1994)A beta-like DNA polymerase from themitochondrion of the trypanosomatid Crithidiafasciculata. J Biol Chem 269, 8165-8171, PubMedID: 94179191
35 Grossman, L.I. and Shoubridge, E.A. (1996)Mitochondrial genetics and human disease.Bioessays 18, 983-991, PubMed ID: 97130392
36 Johns, D.R. (1995) Seminars in medicine of theBeth Israel Hospital, Boston. Mitochondrial DNAand disease. N Engl J Med 333, 638-644, PubMedID: 95364863
37 Naviaux, R.K. (2000) Mitochondrial DNAdisorders. Eur J Pediatr 159 Suppl 3, S219-226,PubMed ID: 21084744
38 White, A.J. (2001) Mitochondrial toxicity andHIV therapy. Sex Transm Infect 77, 158-173,PubMed ID: 21295616
39 Pedersen, P.S. et al. (1999) Ion transport inepithelial spheroids derived from human airwaycells. Am J Physiol 276, L75-80, PubMed ID:99103968
40 Dang, C.V. et al. (1997) Oncogenes in tumormetabolism, tumorigenesis, and apoptosis. JBioenerg Biomembr 29, 345-354, PubMed ID:98048336
41 Lundholm, K. et al. (1982) Glucose turnover,gluconeogenesis from glycerol, and estimation ofnet glucose cycling in cancer patients. Cancer 50,1142-1150, PubMed ID: 82258815
42 Mazurek, S., Boschek, C.B. and Eigenbrodt, E.(1997) The role of phosphometabolites in cellproliferation, energy metabolism, and tumortherapy. J Bioenerg Biomembr 29, 315-330,PubMed ID: 98048333
43 Fischer, C.P., Bode, B.P. and Souba, W.W. (1998)Adaptive alterations in cellular metabolism withmalignant transformation. Ann Surg 227, 627-634; discussion 634-626, PubMed ID: 98266691
44 Ockner, R.K., Kaikaus, R.M. and Bass, N.M.(1993) Fatty-acid metabolism and thepathogenesis of hepatocellular carcinoma: reviewand hypothesis. Hepatology 18, 669-676, PubMedID: 93366320
45 Shaw, J.H. and Wolfe, R.R. (1987) Fatty acid and
glycerol kinetics in septic patients and in patientswith gastrointestinal cancer. The response toglucose infusion and parenteral feeding. AnnSurg 205, 368-376, PubMed ID: 87183717
46 Souba, W.W. (1993) Glutamine and cancer. AnnSurg 218, 715-728, PubMed ID: 94079452
47 Boros, L.G. et al. (1998) Inhibition of theoxidative and nonoxidative pentose phosphatepathways by somatostatin: a possible mechanismof antitumor action. Med Hypotheses 50, 501-506, PubMed ID: 98374098
48 Peluso, G. et al. (2000) Cancer and anticancertherapy-induced modifications on metabolismmediated by carnitine system. J Cell Physiol 182,339-350, PubMed ID: 20119343
49 Pedersen, P.L. (1978) Tumor mitochondria andthe bioenergetics of cancer cells. Prog Exp TumorRes 22, 190-274, PubMed ID: 78227271
50 Weinhouse, S. (1955) Oxidative metabolism ofneoplastic tissues. Adv. Cancer Res. 3, 269-325
51 Carafoli, E. (1980) Mitochondria and disease.Mol. Aspects Med. 3, 295-429
52 Maximo, V. and Sobrinho-Simoes, M. (2000)Hurthle cell tumours of the thyroid. A reviewwith emphasis on mitochondrial abnormalitieswith clinical relevance. Virchows Arch 437, 107-115, PubMed ID: 20445365
53 Chang, L.O., Schnaitman, C.A. and Morris, H.P.(1971) Comparison of the mitochondrialmembrane proteins in rat liver and hepatomas.Cancer Res 31, 108-113, PubMed ID: 71125206
54 Irwin, C.C. and Malkin, L.I. (1976) Differences intotal mitochondrial proteins andmitochondrially-synthesized proteins from ratliver and Morris hepatomas. Fed. Proc. Am. Soc.Exp. Biol. 35, 1583
55 Catterall, W.A. and Pedersen, P.L. (1971)Adenosine triphosphatase from rat livermitochondria. I. Purification, homogeneity, andphysical properties. J Biol Chem 246, 4987-4994,PubMed ID: 71288578
56 Catterall, W.A., Coty, W.A. and Pedersen, P.L.(1973) Adenosine triphosphatase from rat livermitochondria. 3. Subunit composition. J BiolChem 248, 7427-7431, PubMed ID: 74012057
57 Feo, F. et al. (1975) Effect of cholesterol contenton some physical and functional properties ofmitochondria isolated from adult rat liver, fetalliver, cholesterol-enriched liver and hepatomasAH-130, 3924A and 5123. Biochim Biophys Acta413, 116-134, PubMed ID: 76062570
58 Parlo, R.A. and Coleman, P.S. (1984) Enhancedrate of citrate export from cholesterol-rich

Accession information: (02)00445-3a.pdf (short code: txt001ksb); 11 April 2002ISSN 1462-3994 ©2002 Cambridge University Press
http://www-ermm.cbcu.cam.ac.uk
15
expert reviewsin molecular medicine
Mit
och
on
dri
a as
tar
get
s fo
r d
etec
tio
n a
nd
tre
atm
ent
of
can
cer
hepatoma mitochondria. The truncated Krebscycle and other metabolic ramifications ofmitochondrial membrane cholesterol. J BiolChem 259, 9997-10003, PubMed ID: 84289473
59 Costello, L.C. and Franklin, R.B. (2000) Theintermediary metabolism of the prostate: a key tounderstanding the pathogenesis and progressionof prostate malignancy. Oncology 59, 269-282,PubMed ID: 20549295
60 Summerhayes, I.C. et al. (1982) Unusual retentionof rhodamine 123 by mitochondria in muscle andcarcinoma cells. Proc Natl Acad Sci U S A 79,5292-5296, PubMed ID: 83039355
61 Johnson, L.V. et al. (1981) Monitoring of relativemitochondrial membrane potential in living cellsby fluorescence microscopy. J Cell Biol 88, 526-535, PubMed ID: 81168401
62 Bernal, S.D. et al. (1982) Rhodamine-123selectively reduces clonal growth of carcinomacells in vitro. Science 218, 1117-1119, PubMed ID:83067410
63 Lampidis, T.J. et al. (1983) Selective toxicity ofrhodamine 123 in carcinoma cells in vitro. CancerRes 43, 716-720, PubMed ID: 83076897
64 Bernal, S.D. et al. (1983) Anticarcinoma activity invivo of rhodamine 123, a mitochondrial- specificdye. Science 222, 169-172, PubMed ID: 84017536
65 Modica-Napolitano, J.S. and Aprille, J.R. (1987)Basis for the selective cytotoxicity of rhodamine123. Cancer Res 47, 4361-4365, PubMed ID:87273236
66 Nicholls, D.G. (1981) Bioenergetics: anIntroduction to the Chemiosmotic Theory,Academic Press, New York, USA
67 Davis, S. et al. (1985) Mitochondrial and plasmamembrane potentials cause unusualaccumulation and retention of rhodamine 123 byhuman breast adenocarcinoma-derived MCF-7cells. J Biol Chem 260, 13844-13850, PubMed ID:86033856
68 Modica-Napolitano, J.S. et al. (1984) Rhodamine123 inhibits bioenergetic function in isolated ratliver mitochondria. Biochem Biophys ResCommun 118, 717-723, PubMed ID: 84153846
69 Emaus, R.K., Grunwald, R. and Lemasters, J.J.(1986) Rhodamine 123 as a probe oftransmembrane potential in isolated rat- livermitochondria: spectral and metabolic properties.Biochim Biophys Acta 850, 436-448, PubMed ID:86269938
70 Anderson, W.M. et al. (1993) Cytotoxic effect ofthiacarbocyanine dyes on human coloncarcinoma cells and inhibition of bovine heart
mitochondrial NADH-ubiquinone reductaseactivity via a rotenone-type mechanism by twoof the dyes. Biochem Pharmacol 45, 691-696,PubMed ID: 93183171
71 Bleday, R. et al. (1986) Inhibition of rat colontumor isograft growth with dequaliniumchloride. Arch Surg 121, 1272-1275, PubMed ID:87048126
72 Weiss, M.J. et al. (1987) Dequalinium, a topicalantimicrobial agent, displays anticarcinomaactivity based on selective mitochondrialaccumulation. Proc Natl Acad Sci U S A 84, 5444-5448, PubMed ID: 87261002
73 Koya, K. et al. (1996) MKT-077, a novelrhodacyanine dye in clinical trials, exhibitsanticarcinoma activity in preclinical studiesbased on selective mitochondrial accumulation.Cancer Res 56, 538-543, PubMed ID: 96147266
74 Sun, X. et al. (1994) AA1, a newly synthesizedmonovalent lipophilic cation, expresses potent invivo antitumor activity. Cancer Res 54, 1465-1471,PubMed ID: 94184962
75 Rideout, D., Bustamante, A. and Patel, J. (1994)Mechanism of inhibition of FaDuhypopharyngeal carcinoma cell growth bytetraphenylphosphonium chloride. Int J Cancer57, 247-253, PubMed ID: 94208957
76 Modica-Napolitano, J.S. et al. (1996) Selectivedamage to carcinoma mitochondria by therhodacyanine MKT-077. Cancer Res 56, 544-550,PubMed ID: 96147267
77 Weisberg, E.L. et al. (1996) In vivo administrationof MKT-077 causes partial yet reversibleimpairment of mitochondrial function. CancerRes 56, 551-555, PubMed ID: 96147268
78 Lampidis, T.J. et al. (1984) Effects of themitochondrial probe rhodamine 123 and relatedanalogs on the function and viability of pulsatingmyocardial cells in culture. Agents Actions 14,751-757, PubMed ID: 84303640
79 Modica-Napolitano, J.S. et al. (1990)Mitochondrial toxicity of cationicphotosensitizers for photochemotherapy. CancerRes 50, 7876-7881, PubMed ID: 91070553
80 Dougherty, T.J., Weishaupt, K.R. and Boyle, D.G.(1985) Photodynamic Sensitizers, J.B. LipincottCo., Philadelphia, PA, USA
81 Wilson, B.C. and Jeeves, W.P. (1987)Photodynamic therapy of cancer. InPhotomedicine (Vol. 2) (Ben-Hur, E. andRosenthal, I., eds), pp. 127-177, CRC Press, BocaRaton, FL, USA
82 Powers, S.K. (1988) Photochemotherapy. In

Accession information: (02)00445-3a.pdf (short code: txt001ksb); 11 April 2002ISSN 1462-3994 ©2002 Cambridge University Press
http://www-ermm.cbcu.cam.ac.uk
16
expert reviewsin molecular medicine
Mit
och
on
dri
a as
tar
get
s fo
r d
etec
tio
n a
nd
tre
atm
ent
of
can
cer
Application of Lasers in Neurosurgery (Cerullo,L.J., ed.), pp. 137-155, Year Book MedicalPublishers, Inc., Chicago, IL, USA
83 Kowaltowski, A.J. et al. (1999) Mitochondrialeffects of triarylmethane dyes. J BioenergBiomembr 31, 581-590, PubMed ID: 20145121
84 Oseroff, A.R. et al. (1987) Strategies for selectivecancer photochemotherapy: antibody-targetedand selective carcinoma cell photolysis.Photochem Photobiol 46, 83-96, PubMed ID:87290165
85 Powers, S.K. et al. (1986) Laserphotochemotherapy of rhodamine-123 sensitizedhuman glioma cells in vitro. J Neurosurg 64, 918-923, PubMed ID: 86198943
86 Beckman, W.C., Jr. et al. (1987) Differentialretention of rhodamine 123 by avian sarcomavirus-induced glioma and normal brain tissue ofthe rat in vivo. Cancer 59, 266-270, PubMed ID:87102460
87 Powers, S.K. et al. (1989) Photosensitization ofhuman glioma cells by chalcogenapyryliumdyes. J Neurooncol 7, 179-188, PubMed ID:89381799
88 Oseroff, A.R. et al. (1986) Intramitochondrialdyes allow selective in vitro photolysis ofcarcinoma cells. Proc Natl Acad Sci U S A 83,9729-9733, PubMed ID: 87092321
89 Ara, G. et al. (1987) Mechanisms ofmitochondrial photosensitization by the cationicdye, N,N- bis(2-ethyl-1,3-dioxylene)kryptocyanine (EDKC): preferentialinactivation of complex I in the electron transportchain. Cancer Res 47, 6580-6585, PubMed ID:88052644
90 Walstad, D.L., Brown, J.T. and Powers, S.K.(1989) The effect of a chalcogenapyrylium dyewith and without photolysis on mitochondrialfunction in normal and tumor cells. PhotochemPhotobiol 49, 285-291, PubMed ID: 89283000
91 Modica-Napolitano, J.S. et al. (1998)Photoactivation enhances the mitochondrialtoxicity of the cationic rhodacyanine MKT-077.Cancer Res 58, 71-75, PubMed ID: 98086029
92 Pedersen, P.L. and Morris, H.P. (1974) Uncoupler-stimulated adenosine triphosphatase activity.Deficiency in intact mitochondria from Morrishepatomas and ascites tumor cells. J Biol Chem249, 3327-3334, PubMed ID: 74172590
93 Capuano, F., Guerrieri, F. and Papa, S. (1997)Oxidative phosphorylation enzymes in normaland neoplastic cell growth. J Bioenerg Biomembr29, 379-384, PubMed ID: 98048339
94 Capuano, F. et al. (1996) Oxidativephosphorylation and F(O)F(1) ATP synthaseactivity of human hepatocellular carcinoma.Biochem Mol Biol Int 38, 1013-1022, PubMed ID:97013420
95 Cuezva, J.M. et al. (1997) Mitochondrialbiogenesis in the liver during development andoncogenesis. J Bioenerg Biomembr 29, 365-377,PubMed ID: 98048338
96 Modica-Napolitano, J.S. and Touma, S.E. (2000)Functional differences in mitochondrial enzymesfrom normal epithelial and carcinoma cells. InMitochondrial Dysfunction in Pathogenesis, AKeystone Symposium (15–20 January, Santa Fe,USA), p. 64, Keystone Symposia, Silverthorne,CO 80498, USA
97 Sun, A.S., Sepkowitz, K. and Geller, S.A. (1981) Astudy of some mitochondrial and peroxisomalenzymes in human colonic adenocarcinoma. LabInvest 44, 13-17, PubMed ID: 81097387
98 Sun, A.S. and Cederbaum, A.I. (1980)Oxidoreductase activities in normal rat liver,tumor-bearing rat liver, and hepatoma HC-252. Cancer Res 40, 4677-4681, PubMed ID:81064485
99 Heerdt, B.G. et al. (1990) Expression ofmitochondrial cytochrome c oxidase in humancolonic cell differentiation, transformation, andrisk for colonic cancer. Cancer Res 50, 1596-1600,PubMed ID: 90150125
100 Luciakova, K. and Kuzela, S. (1992) Increasedsteady-state levels of several mitochondrial andnuclear gene transcripts in rat hepatoma with alow content of mitochondria. Eur J Biochem 205,1187-1193, PubMed ID: 92249325
101 Costantini, P. et al. (2000) Mitochondrion as anovel target of anticancer chemotherapy. J NatlCancer Inst 92, 1042-1053, PubMed ID: 20341836
102 Chan, S.H. and Barbour, R.L. (1983) Adeninenucleotide transport in hepatoma mitochondria.Characterization of factors influencing thekinetics of ADP and ATP uptake. BiochimBiophys Acta 723, 104-113, PubMed ID: 83153600
103 Sul, H.S. et al. (1979) Comparison of the adeninenucleotide translocase in hepatomas and rat livermitochondria. Biochim Biophys Acta 551, 148-155, PubMed ID: 79145476
104 Woldegiorgis, G. and Shrago, E. (1985) Adeninenucleotide translocase activity and sensitivity toinhibitors in hepatomas. Comparison of theADP/ATP carrier in mitochondria and in apurified reconstituted liposome system. J BiolChem 260, 7585-7590, PubMed ID: 85207805

Accession information: (02)00445-3a.pdf (short code: txt001ksb); 11 April 2002ISSN 1462-3994 ©2002 Cambridge University Press
http://www-ermm.cbcu.cam.ac.uk
17
expert reviewsin molecular medicine
Mit
och
on
dri
a as
tar
get
s fo
r d
etec
tio
n a
nd
tre
atm
ent
of
can
cer
105 Halestrap, A.P. and Davidson, A.M. (1990)Inhibition of Ca2(+)-induced large-amplitudeswelling of liver and heart mitochondria bycyclosporin is probably caused by the inhibitorbinding to mitochondrial-matrix peptidyl-prolylcis-trans isomerase and preventing it interactingwith the adenine nucleotide translocase. BiochemJ 268, 153-160, PubMed ID: 90262539
106 Bernardi, P. et al. (1998) The mitochondrialpermeability transition. Biofactors 8, 273-281,PubMed ID: 99113258
107 Faure Vigny, H. et al. (1996) Expression ofoxidative phosphorylation genes in renal tumorsand tumoral cell lines. Mol Carcinog 16, 165-172,PubMed ID: 96313221
108 Giraud, S. et al. (1998) Expression of humanANT2 gene in highly proliferative cells: GRBOX,a new transcriptional element, is involved in theregulation of glycolytic ATP import intomitochondria. J Mol Biol 281, 409-418, PubMedID: 98365507
109 Reed, J.C. (1994) Bcl-2 and the regulation ofprogrammed cell death. J Cell Biol 124, 1-6,PubMed ID: 94124601
110 Kroemer, G. (1997) The proto-oncogene Bcl-2 andits role in regulating apoptosis. Nat Med 3, 614-620, PubMed ID: 97319583
111 Reed, J.C. (1997) Double identity for proteins ofthe Bcl-2 family. Nature 387, 773-776, PubMedID: 97337864
112 Venturini, I. et al. (1998) Up-regulation ofperipheral benzodiazepine receptor system inhepatocellular carcinoma. Life Sci 63, 1269-1280,PubMed ID: 98442858
113 Galiegue, S. et al. (1999) Cloning andcharacterization of PRAX-1. A new protein thatspecifically interacts with the peripheralbenzodiazepine receptor. J Biol Chem 274, 2938-2952, PubMed ID: 99115641
114 O’Gorman, E. et al. (1997) The role of creatinekinase in inhibition of mitochondrialpermeability transition. FEBS Lett 414, 253-257,PubMed ID: 97459736
115 Schiemann, S. et al. (1998) Molecular analysis oftwo mammary carcinoma cell lines at thetranscriptional level as a model system forprogression of breast cancer. Clin Exp Metastasis16, 129-139, PubMed ID: 98173027
116 Beurdeley-Thomas, A. et al. (2000) Theperipheral benzodiazepine receptors: a review. JNeurooncol 46, 45-56, PubMed ID: 20353100
117 Rampino, N. et al. (1997) Somatic frameshiftmutations in the BAX gene in colon cancers of
the microsatellite mutator phenotype. Science275, 967-969, PubMed ID: 97172557
118 Brimmell, M. et al. (1998) BAX frameshiftmutations in cell lines derived from humanhaemopoietic malignancies are associated withresistance to apoptosis and microsatelliteinstability. Oncogene 16, 1803-1812, PubMed ID:98243036
119 Singh, K.K. et al. (1999) Mitochondrial DNAdetermines the cellular response to cancertherapeutic agents. Oncogene 18, 6641-6646,PubMed ID: 20065137
120 Weissig, V. and Torchilin, V.P., eds (2001) Drugand DNA delivery to mitochondria. Adv DrugDeliv Rev 49, 1-2, PubMed ID: 21271658
121 Rizzuto, R. et al. (1992) Rapid changes ofmitochondrial Ca2+ revealed by specificallytargeted recombinant aequorin. Nature 358, 325-327, PubMed ID: 92350252
122 Ellerby, H.M. et al. (1999) Anti-cancer activity oftargeted pro-apoptotic peptides. Nat Med 5,1032-1038, PubMed ID: 99401083
123 Clayton, D.A. and Vinograd, J. (1967) Circulardimer and catenate forms of mitochondrial DNAin human leukaemic leucocytes. J Pers 35, 652-657, PubMed ID: 68135375
124 Clayton, D.A. and Vinograd, J. (1969) Complexmitochondrial DNA in leukemic and normalhuman myeloid cells. Proc Natl Acad Sci U S A62, 1077-1084, PubMed ID: 69244656
125 Gamen, S. et al. (1995) mtDNA-depleted U937cells are sensitive to TNF and Fas-mediatedcytotoxicity. FEBS Lett 376, 15-18, PubMed ID:96096778
126 Boultwood, J. et al. (1996) Amplification ofmitochondrial DNA in acute myeloid leukaemia.Br J Haematol 95, 426-431, PubMed ID: 97060858
127 Ivanova, R. et al. (1998) Mitochondrial DNAsequence variation in human leukemic cells. Int JCancer 76, 495-498, PubMed ID: 98250006
128 Hudson, B. and Vinograd, J. (1967) Catenatedcircular DNA molecules in HeLa cellmitochondria. Nature 216, 647-652, PubMed ID:68135373
129 Welter, C. et al. (1989) Alteration ofmitochondrial DNA in human oncocytomas.Genes Chromosomes Cancer 1, 79-82, PubMedID: 91120367
130 Tallini, G. (1998) Oncocytic tumours. VirchowsArch 433, 5-12, PubMed ID: 98355568
131 Tallini, G. et al. (1994) Analysis of nuclear andmitochondrial DNA alterations in thyroid andrenal oncocytic tumors. Cytogenet Cell Genet 66,

Accession information: (02)00445-3a.pdf (short code: txt001ksb); 11 April 2002ISSN 1462-3994 ©2002 Cambridge University Press
http://www-ermm.cbcu.cam.ac.uk
18
expert reviewsin molecular medicine
Mit
och
on
dri
a as
tar
get
s fo
r d
etec
tio
n a
nd
tre
atm
ent
of
can
cer
253-259, PubMed ID: 94215316132 Heddi, A. et al. (1996) Coordinate expression of
nuclear and mitochondrial genes involved inenergy production in carcinoma andoncocytoma. Biochim Biophys Acta 1316, 203-209, PubMed ID: 96375169
133 Kovacs, A. et al. (1992) Mitochondrial andchromosomal DNA alterations in humanchromophobe renal cell carcinomas. J Pathol 167,273-277, PubMed ID: 92389115
134 Horton, T.M. et al. (1996) Novel mitochondrialDNA deletion found in a renal cell carcinoma.Genes Chromosomes Cancer 15, 95-101, PubMedID: 96431090
135 Selvanayagam, P. and Rajaraman, S. (1996)Detection of mitochondrial genome depletion bya novel cDNA in renal cell carcinoma. Lab Invest74, 592-599, PubMed ID: 96175616
136 Yamamoto, H. et al. (1992) Significant existenceof deleted mitochondrial DNA in cirrhotic liversurrounding hepatic tumor. Biochem BiophysRes Commun 182, 913-920, PubMed ID: 92134320
137 Fukushima, S. et al. (1995) The frequency of 4977base pair deletion of mitochondrial DNA in
various types of liver disease and in normal liver.Hepatology 21, 1547-1551, PubMed ID: 95286138
138 El Meziane, A. et al. (1998) MitochondrialtRNALeu isoforms in lung carcinoma cybridcells containing the np 3243 mtDNA mutation.Hum Mol Genet 7, 2141-2147, PubMed ID:99036686
139 Savre-Train, I, Piatyszek, M.A. and Shay, J.W.(1992) Transcription of deleted mitochondrialDNA in human colon adenocarcinoma cells.Hum Mol Genet 1, 203-204, PubMed ID:93265014
140 Burgart, L.J. et al. (1995) Somatic mitochondrialmutation in gastric cancer. Am J Pathol 147, 1105-1111, PubMed ID: 96010274
141 Liang, B.C. (1996) Evidence for association ofmitochondrial DNA sequence amplification andnuclear localization in human low-gradegliomas. Mutat Res 354, 27-33, PubMed ID:96305473
142 Richard, S.M. et al. (2000) Nuclear andmitochondrial genome instability in humanbreast cancer. Cancer Res 60, 4231-4237, PubMedID: 20399732

Accession information: (02)00445-3a.pdf (short code: txt001ksb); 11 April 2002ISSN 1462-3994 ©2002 Cambridge University Press
http://www-ermm.cbcu.cam.ac.uk
19
expert reviewsin molecular medicine
Mit
och
on
dri
a as
tar
get
s fo
r d
etec
tio
n a
nd
tre
atm
ent
of
can
cer
Citation details for this article
Josephine S. Modica-Napolitano and Keshav K. Singh (2002) Mitochondria as targets for detection andtreatment of cancer. Exp. Rev. Mol. Med. 11 April, http://www-ermm.cbcu.cam.ac.uk/02004453h.htm
Features associated with this article
FiguresFigure 1. Schematic of key mitochondrial metabolic pathways (fig001ksb).Figure 2. Mitochondria of neuron revealed by staining with a rhodamine 123 derivative (fig002ksb).
TablesTable 1. Mitochondrial diseases (tab001ksb).Table 2. Mitochondrial DNA mutation in cancers (tab002ksb).
Further reading, resources and contacts
Wallace, D.C. (1997) Mitochondrial DNA in aging and disease. Sci Am 277, 40-47, PubMed ID: 97388606
Singh, K.K. (1998) Mitochondrial DNA Mutation in Aging, Disease and Cancer, Springer, New York
Scheffler, I.E. (1999) Mitochondria, Wiley-Liss, New York
Naviaux, R.K. (1997) Spectrum of Mitochondrial Diseases, Exceptional Parent, http://biochemgen.ucsd.edu/mmdc/ep-toc.htm
The Mitochondria Research Society website provides basic information and useful links on mitochonrialdisease for scientists, clinicians and patients.
http://www.mitoresearch.org
Website providing introduction to mitochondrial DNA for students (‘The fire within: the unfolding story ofhuman mtDNA’):
http://biocrs.biomed.brown.edu/books/essays/mitochondrialDNA.html
The Mitomap database lists polymorphisms and mutations of human mitochondrial DNA.
http://www.gen.emory.edu/mitomap.html
Keshav K. Singh home page:
http://www.jhmi.edu/~kksingh