Embed Size (px)
Citation preview
Model Strategies: Strategic Communications and Systematic
Messaging
David Schonfeld, MD, Facilitator Joseph Bocchini, MD, Presenter
Bill Cosgrove, MD, Presenter, Utah Susan Penfield, MD, Presenter, Texas
Robert Schechter, MD, Presenter, California
-1-
LWW/JPHMP PHH200233 November 18, 2010 22:10 Char Count= 0
Public Health Communication with FrontlineClinicians During the First Wave of the 2009Influenza Pandemic
Catherine J. Staes, BSN, MPH, PhD; Amyanne Wuthrich, MS; Per Gesteland, MD, MS;
Mandy A. Allison, MD, MSPH; Molly Leecaster, PhD; Julie H. Shakib, DO, MPH; Marjorie E. Carter, MSPH;
Brittany M. Mallin, MA, MPH; Susan Mottice, PhD; Robert Rolfs, MD, MPH; Andrew T. Pavia, MD;
Brent Wallace, MD; Adi V. Gundlapalli, MD, PhD, MS; Matthew Samore, MD; Carrie L. Byington, MD
� � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � �
Context: During public health emergencies, office-based
frontline clinicians are critical partners in the detection,
treatment, and control of disease. Communication between
public health authorities and frontline clinicians is critical, yet
public health agencies, medical societies, and healthcare
delivery organizations have all called for improvements.
Objectives: Describe communication processes between public
health and frontline clinicians during the first wave of the 2009
novel influenza A (H1N1) pandemic; assess clinicians’ use of and
knowledge about public health guidance; and assess clinicians’
perceptions and preferences about communication during a
public health emergency. Design and Methods: During the first
wave of the pandemic, we performed a process analysis and
surveyed 509 office-based primary care providers in Utah.
Setting and Participants: Public health and healthcare leaders
from major agencies involved in emergency response in Utah
and office-based primary care providers located throughout
Utah. Main Outcome Measure(s): Communication process and
information flow, distribution of e-mails, proportion of clinicians
who accessed key Web sites at least weekly, clinicians’
knowledge about recent guidance and perception about e-mail
load, primary information sources, and qualitative findings from
clinician feedback. Results: The process analysis revealed
redundant activities and messaging. The 141 survey respondents
(28%) received information from a variety of sources: 68%
received information from state public health; almost 100%
received information from health care organizations. Only
one-third visited a state public health or institutional Web site
J Public Health Management Practice, 2011, 17(1), 36–44
Copyright C© 2011 Wolters Kluwer Health | Lippincott Williams & Wilkins
frequently enough (at least weekly) to obtain updated guidance.
Clinicians were knowledgeable about guidance that did not
change during the first wave; however, correct knowledge was
lower after guidance changed. Clinicians felt overwhelmed by
e-mail volume, preferred a single institutional e-mail for clinical
guidance, and suggested that new information be concise and
clearly identified. Conclusion: Communication between public
health, health care organizations and clinicians was redundant
and overwhelming and can be enhanced considering clinician
preferences and institutional communication channels.
KEY WORDS: disease outbreaks, influenza, interdisciplinarycommunication, public health practice
During public health emergencies, frontline clini-cians are critical partners in the detection, treatment,and control of disease.1-7 Public health authorities rely
Author Affiliations: Department of Biomedical Informatics (Dr Staes), Division
of Epidemiology (Mss Wuthrich, Carter, and Mallin and Drs Leecaster,
Gundlapalli, and Samore), Department of Pediatrics (Drs Gesteland, Allison,
Shakib, Pavia, and Byington), University of Utah School of Medicine, Salt Lake
City, Utah Department of Health, University of Utah (Drs Mottice and Rolfs),
Intermountain Healthcare (Drs Gesteland and Wallace), VA Medical Center
(Drs Leecaster and Samore), Salt Lake City, Utah.
We thank our collaborators with the Utah Health Research Network, Intermoun-
tain Healthcare, University Healthcare, and HealthInsight for their assistance with
the survey. This work was partially supported by the CDC Center of Excellence
in Public Health Informatics grant #8P01HK000030 (CS, AW, PG, MA, ML, JS,
MC, BM, SM, RR, MS, CB), NIH/Eunice Kennedy Shriver NICHD K24-HD047249
(CLB), PHS National Center for Research Resources (grant UL1-RR025764) (PG),
Agency for Healthcare Research and Quality grant K08 HS018538-01 (PG) and
NIH/NIAID Rocky Mountain Regional Center of Excellence for Biodefense and
Emerging Infectious Diseases Research grant U 54 AI-065357 (AVG).
Correspondence: Catherine J. Staes, BSN, MPH, PhD, Department of Biomed-
ical Informatics, University of Utah, 26 South 2000 East (HSEB 5700), Salt Lake
City, UT 84112 ([email protected]).
Copyright © 2011 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
36
-2-

LWW/JPHMP PHH200233 November 18, 2010 22:10 Char Count= 0
Communication With Frontline Clinicians During the 2009 Influenza Pandemic ❘ 37
on clinicians to make appropriate decisions aboutwhom to test, how to collect specimens, what treat-ments to use, and to implement or support public healthreporting when it is required by the state law for diseasesurveillance. Similarly, clinicians refer to public healthfor guidance to control the spread of the disease andthe latest intelligence concerning the pathogen. Com-munication between public health authorities and clin-icians is particularly critical when the pathogen has thepotential for rapid spread, there is widespread pub-lic concern, and the epidemiology and optimal man-agement are unclear, particularly concerning those atrisk for severe disease. These factors were present inApril, May, and June 2009 during the first wave of the2009 novel influenza A (H1N1) pandemic in the UnitedStates.6,8,9
● Background
Communication between public health authorities andfrontline clinicians is a critical component of anypublic health emergency response plan. For the past10 years, public health agencies, medical societies, andhealth care delivery organizations have all called forimprovements.1-5,10,11 Even so, we found only 3 limitedevaluations of communication during the recent pan-demic in the medical literature5,12,13 and no literaturethat objectively assessed communication between pub-lic health authorities and frontline clinicians during apublic health emergency.
Communication between public health authoritiesand clinicians is complex. Multiple barriers must beovercome to support an appropriate emergency publichealth response. In particular, clinicians must be ableto identify the authoritative and appropriate sourcefor clinical guidance among the variety of messagesavailable from federal, state, and local public healthauthorities, professional organizations, and their owninstitutions.7,14-17 The variety of messages may lead tomixed messages and overload; moreover, their impactis unknown.
In April and May 2009, as H1N1 outbreak be-gan in the United States, challenges with producingand delivering guidance became evident in Utah andelsewhere.5,18-20 There was a rapid increase in newinformation targeting clinicians, particularly concern-ing personal protective equipment, high-risk patientgroups, diagnostic testing, antiviral therapies, and im-munization. We hypothesized that clinicians wouldface challenges in keeping up with evolving and tai-lored messages from multiple organizations at a timewhen clinic volumes, patient concerns, and media ex-posure were increasing. We targeted our investigationtoward office-based primary care providers for 2 major
reasons: first, information flow may differ in the hospi-tal setting; and second, office-based care is the most fre-quent usual source of care for individuals in the UnitedStates.21 In fact, according to the 2008 Utah HealthcareAccess Survey, of 88.33% of Utahns who report that theyhave a usual place that they go when they are sick orneed advice about their health, 79.5% report that theygo to a private clinic or doctor’s office.22
The objectives of our investigation were to (1) de-scribe the communication processes between the CDC,state/local public health agencies, health care organi-zations and institutions, and office-based primary careclinicians during the first wave of the H1N1 pandemic;(2) assess clinicians’ knowledge about public healthguidance concerning the detection, treatment, preven-tion, and control of H1N1 virus; and (3) determine clin-ician preferences and perceptions about communica-tion during a public health emergency to improve theprocess.
● Methods
Process analysis
To describe the process for communicating guidance tofrontline clinicians in Utah, we interviewed key infor-mants and diagrammed process and information flowby using business process modeling techniques.23 Thekey informants represent clinical and epidemiologicleaders from the state and largest county health depart-ments and the 2 major health care organizations in Utahwith a combined majority of the market share in thestate. Between May and July 2009, we gathered infor-mation from the most senior epidemiologist at the UtahDepartment of Health (UDOH) and the Salt Lake ValleyHealth Department, and from clinicians and adminis-trators at the 2 major health care organizations in Utah:Intermountain Healthcare (Intermountain) and Univer-sity of Utah Healthcare (University). Several study au-thors (P.G., S.M., R.R., A.T.P., B.W., I.R., A.V.G., andC.L.B) were key participants in surveillance and guid-ance development activities. Findings were validatedby the above key participants and senior leadership atIntermountain and University. We reviewed the guid-ance e-mailed from Intermountain to clinicians and in-formation posted on the CDC, UDOH, and Salt LakeValley Health Department Web sites between May 1and May 11.
Survey
Study population
The study population included office-based primarycare clinicians located in urban and rural communi-ties throughout Utah. We used 3 major Utah-based
Copyright © 2011 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
-3-

LWW/JPHMP PHH200233 November 18, 2010 22:10 Char Count= 0
38 ❘ Journal of Public Health Management and Practice
organizations to reach the study population. We sur-veyed clinicians affiliated with University, including98 clinicians with the community clinics and 17 pe-diatricians affiliated with the Department of GeneralPediatrics. We surveyed 315 primary care cliniciansemployed by or affiliated with Intermountain, an inte-grated health care system that operates more than 100ambulatory care clinics throughout Utah. These clini-cians were identified by the Intermountain HealthcareOffice of Physician Relations. Finally, we surveyed 79office-based primary care clinicians from small grouppractices in rural Utah not affiliated with Intermoun-tain or University. These clinicians were identifiedby HealthInsight,24 a not-for-profit community-basedorganization that routinely works with independentoffice-based primary care providers throughout Utah.HealthInsight is the Agency for Healthcare Researchand Quality–designated Chartered Value Exchange,the Health Information Technology Regional ExtensionCenter, and the Medicare Quality Improvement Orga-nization in Nevada and Utah.
Survey design and procedure
We performed a descriptive, cross-sectional survey thatincluded questions to assess clinicians’ use of and ac-cess to public health guidance concerning the detec-tion, treatment, prevention, and control of H1N1 virus;knowledge about public health reporting and guide-lines; and preferences and perceptions about differentsources of information. An e-mail with a link to ananonymous Web-based survey was sent to study partic-ipants. Two (Intermountain) or 3 (all others) sequentiale-mails were sent at least 1 week apart. Individual clin-icians could respond to the survey only once. Surveyswere completed between May 26 and June 30, 2009,during the first wave in Utah (Figure 1).25 Institutional
FIGURE 1 ● Daily Counts of Positive Tests for Influenza A,Intermountain Healthcare, Utah, 2009� � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � �
review board approval was obtained from Intermoun-tain and the University of Utah.
Survey data analysis
We used descriptive statistics to describe the frequencyand sources of information pushed to the clinicians inUtah, the frequency and sources of Web-based infor-mation they accessed, and clinician knowledge aboutpublic health guidance that would affect a clinician’sclinical decision making. We specifically queried about4 potential e-mail sources from the CDC, UDOH, In-termountain, and University. We used the Fisher exacttest to compare responses between clinicians employedby Intermountain, University, or neither organization(other).
To assess clinician preferences and perceptions aboutcommunication, we used 3 strategies. We queriedabout their primary source of information for clinicaldecision-making and classified sources as institutional,local/state public health, national, or other. We assessedthe relationship between the number of e-mail sourcesand the clinician’s perception about the amount of e-mail received. We used the Fisher exact test to com-pare the observed and expected percentages, assumingthat perceptions of e-mail amount were independent ofthe numbers of e-mail sources. Finally, we performed aqualitative analysis of the responses to an open-endedquestion. The free text comments were coded using anadaptation to the Grounded Theory Approach18 andthen grouped into themes.
● Results
Analysis of communication processes as thepandemic unfolded
On April 24, 2009 (Figure 1), the CDC reported thatan H1N1 virus was responsible for a large outbreak ofrespiratory illness in Mexico and was associated withwidespread human-to-human transmission. The keyinformant interviews, process analysis, and commu-nication artifacts (Web sites, e-mails, and alerts) illus-trated the activated public health response to the threatof pandemic influenza. During the ensuing weeks, com-munication efforts increased both nationally and locallyto serve the information needs of clinicians and to en-hance the compilation of surveillance data.
On the national level, the CDC used several estab-lished communication systems to target clinicians, in-cluding Clinician Outreach and Communication Activ-ity (COCA) e-mails, Health Advisory Network alerts,and Morbidity and Mortality Weekly Report (MMWR) dis-patches and publications (Figure 2).7,14-17 The COCAalerts target clinicians. Health Advisory Network alerts
Copyright © 2011 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
-4-
LWW/JPHMP PHH200233 November 18, 2010 22:10 Char Count= 0
Communication With Frontline Clinicians During the 2009 Influenza Pandemic ❘ 39
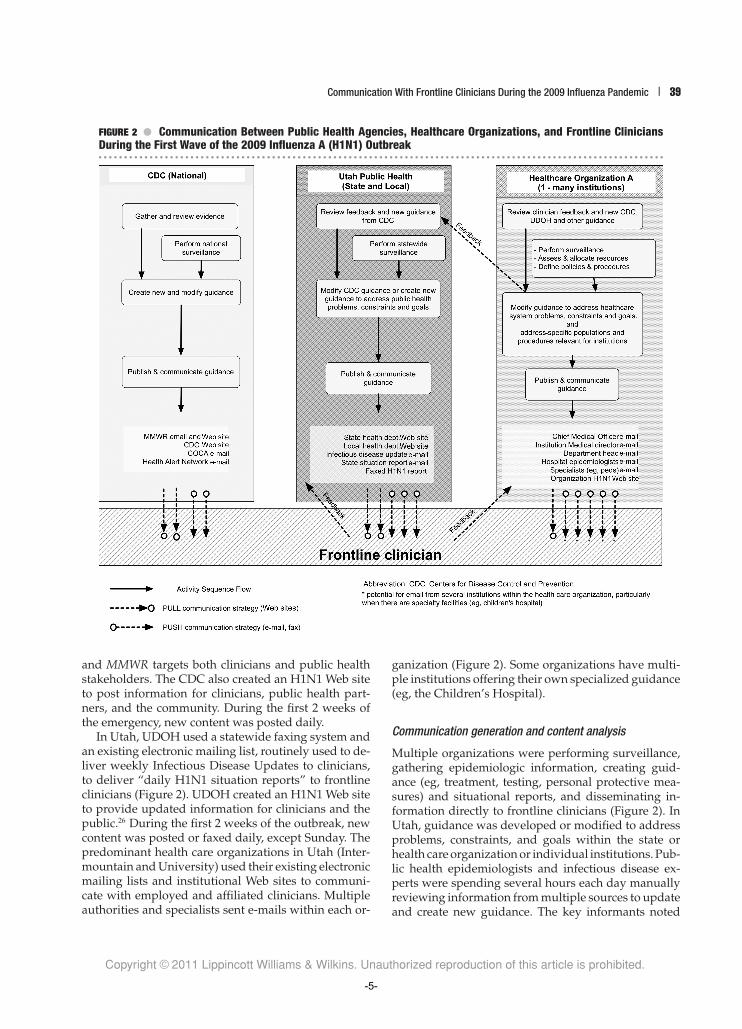
FIGURE 2 ● Communication Between Public Health Agencies, Healthcare Organizations, and Frontline CliniciansDuring the First Wave of the 2009 Influenza A (H1N1) Outbreak� � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � �
and MMWR targets both clinicians and public healthstakeholders. The CDC also created an H1N1 Web siteto post information for clinicians, public health part-ners, and the community. During the first 2 weeks ofthe emergency, new content was posted daily.
In Utah, UDOH used a statewide faxing system andan existing electronic mailing list, routinely used to de-liver weekly Infectious Disease Updates to clinicians,to deliver “daily H1N1 situation reports” to frontlineclinicians (Figure 2). UDOH created an H1N1 Web siteto provide updated information for clinicians and thepublic.26 During the first 2 weeks of the outbreak, newcontent was posted or faxed daily, except Sunday. Thepredominant health care organizations in Utah (Inter-mountain and University) used their existing electronicmailing lists and institutional Web sites to communi-cate with employed and affiliated clinicians. Multipleauthorities and specialists sent e-mails within each or-
ganization (Figure 2). Some organizations have multi-ple institutions offering their own specialized guidance(eg, the Children’s Hospital).
Communication generation and content analysis
Multiple organizations were performing surveillance,gathering epidemiologic information, creating guid-ance (eg, treatment, testing, personal protective mea-sures) and situational reports, and disseminating in-formation directly to frontline clinicians (Figure 2). InUtah, guidance was developed or modified to addressproblems, constraints, and goals within the state orhealth care organization or individual institutions. Pub-lic health epidemiologists and infectious disease ex-perts were spending several hours each day manuallyreviewing information from multiple sources to updateand create new guidance. The key informants noted
Copyright © 2011 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
-5-

LWW/JPHMP PHH200233 November 18, 2010 22:10 Char Count= 0
40 ❘ Journal of Public Health Management and Practice
that information in guidance documents was usuallydesigned to meet institutional needs and resourcesrather than to provide a comprehensive set of all the in-formation required by frontline clinicians. For example,early CDC guidance described which patients shouldbe tested and then included the caveat that “Clini-cians should be aware of local guidance on testing.”27
Simultaneously, health care institutions tailored mes-sages based on the availability of their resources (eg,personal protective equipment, antiviral medications,vaccine) and included links to public health Web sitesbut did not explicitly describe differences.
At 2 weeks into the outbreak, the CDC and UDOHstarted specifying the “date of last update” for con-tent linked to their Web sites, but they did not iden-tify the updated content within the multipage docu-ments. Therefore, the reader would have had to readthe entire document and determine new content on hisor her own. In addition, we identified inconsistencies:one guidance document posted 2 weeks into the emer-gency included 4 different names for the virus: “novelInfluenza A H1N1,” “2009 H1N1 Influenza A,” “S-OIVinfection,” and “novel H1N1 flu (swine flu).”28 This re-flected the national and international confusion regard-ing the nomenclature for this virus.
Description of survey respondents
Of the 509 clinicians surveyed, 141 (28%) respondedand were included in this analysis; 7 were excluded be-cause they did not practice office-based primary care,and 368 did not complete the survey. The respondentswere experienced clinicians, mostly physicians (95%),with a median of 15 years of professional experience.Half (46%) of the respondents reported that at least one-fourth of their patients were younger than 18 years. Therespondents worked in outpatient primary care settingslocated in 7 of the 8 multicounty Utah health districts,comprising rural and urban communities throughoutUtah. The clinicians were employed by Intermountain(n = 53), University (n = 32), both Intermountain andUniversity (n = 1), and neither of these organizations(other) (n = 55). The 3 groups of clinicians had simi-lar years of experience and pediatric practice, althoughUniversity clinicians were less likely to work full-timeseeing patients (P < .01).
Description of communication receivedand sought by clinicians
During the first month of the outbreak (Figure 1), amajority (68%) of frontline clinicians received informa-tion pushed from UDOH, by either fax (38%) or e-mail(56%); 21% received the information e-mailed by theCDC COCA system. Receipt of e-mail messages from
UDOH or CDC was not related to a clinician’s em-ployer. In contrast, UDOH faxes were less likely to bereceived by Intermountain (34%) or University (12%)clinicians than other (58%) clinicians (P < .0001). Nearly100% of the respondents employed by Intermountain orUniversity received the e-mails from their chief medi-cal officer. The e-mails from Intermountain also reached68% of the clinicians in small-group, rural practicesunaffiliated with Intermountain, although they mighthave admitting privileges at Intermountain facilities.
Respondents’ use of Web sites during the first monthof the outbreak varied. Approximately half (53%) re-ported visiting the CDC H1N1 flu Web site at leastonce each week. In contrast, only one-third visitedthe UDOH (35%) or their institutional (38%) Web siteat least once each week. Half the respondents neversought information from the UDOH Web site (50%) ortheir own institution Web site (46%); 17% never visitedthe CDC Web site. Two-thirds (67%) of the clinicians didnot read MMWR during the first month. The use of Websites did not significantly differ by clinician affiliation(P > .09).
Clinician knowledge about public health guidance
The respondents had a high level of correct knowl-edge for questions about high-risk groups, testing,and treatment (Table 1). These guidelines remainedfairly constant during the 1-month survey period. How-ever, when guidance changed during the survey pe-riod (eg, reporting requirements), the subsequent sur-vey respondents had lower levels of correct knowledge(Table 1). There was no significant difference by clini-cian affiliation (P > .05).
Clinician preferences and perceptions aboutcommunication
Primary sources of information for clinical decision making
Concerning who and how to test for the emerginginfluenza virus, most (73%) Intermountain and Uni-versity clinicians used their own institution as theirprimary source of information; in contrast, the otherclinicians used institutional (38%), state (33%), and na-tional (24%) sources as their primary source (P = 0.001).Table 2 demonstrates primary sources of informationfor all respondents. Concerning treatment guidance, in-stitutional sources were the preferred source (55%), re-gardless of employer; CDC (28%) and local/state pub-lic health (13%) sources were less frequently preferred.For patient educational materials, the CDC Web site(40%) and institutional sources (32%) were the pre-ferred sources, regardless of employer. For population-based data about the epidemiology of influenza, the
Copyright © 2011 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
-6-
LWW/JPHMP PHH200233 November 18, 2010 22:10 Char Count= 0
Communication With Frontline Clinicians During the 2009 Influenza Pandemic ❘ 41
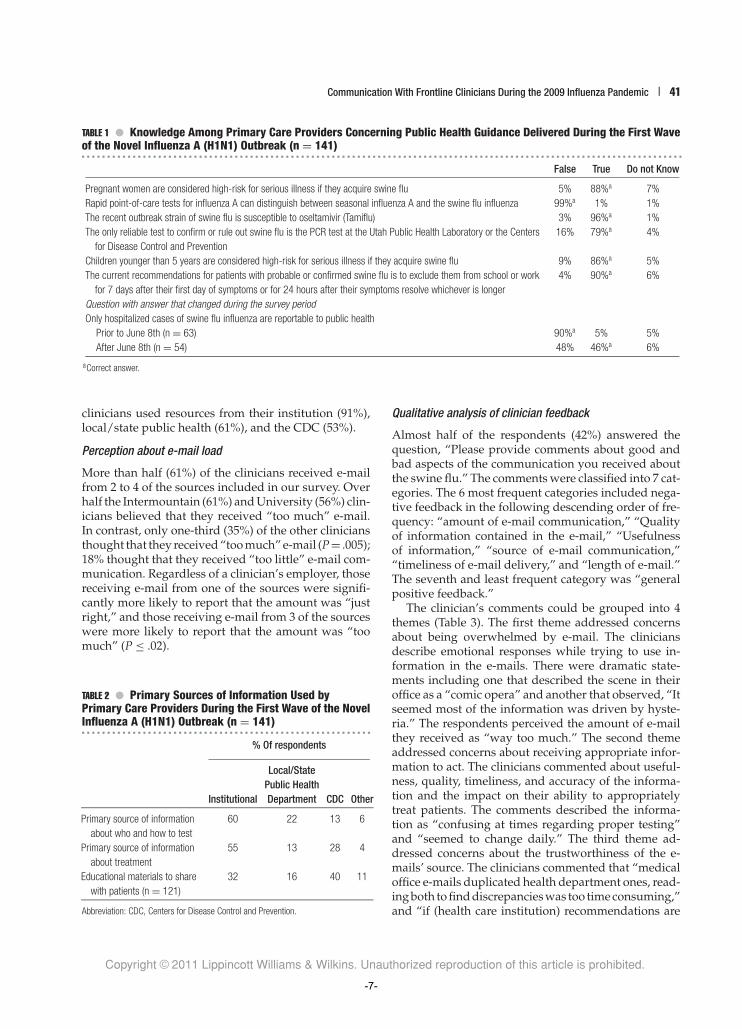
TABLE 1 ● Knowledge Among Primary Care Providers Concerning Public Health Guidance Delivered During the First Waveof the Novel Influenza A (H1N1) Outbreak (n = 141)� � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � �
False True Do not Know
Pregnant women are considered high-risk for serious illness if they acquire swine flu 5% 88%a 7%
Rapid point-of-care tests for influenza A can distinguish between seasonal influenza A and the swine flu influenza 99%a 1% 1%
The recent outbreak strain of swine flu is susceptible to oseltamivir (Tamiflu) 3% 96%a 1%
The only reliable test to confirm or rule out swine flu is the PCR test at the Utah Public Health Laboratory or the Centers
for Disease Control and Prevention
16% 79%a 4%
Children younger than 5 years are considered high-risk for serious illness if they acquire swine flu 9% 86%a 5%
The current recommendations for patients with probable or confirmed swine flu is to exclude them from school or work
for 7 days after their first day of symptoms or for 24 hours after their symptoms resolve whichever is longer
4% 90%a 6%
Question with answer that changed during the survey period
Only hospitalized cases of swine flu influenza are reportable to public health
Prior to June 8th (n = 63) 90%a 5% 5%
After June 8th (n = 54) 48% 46%a 6%
aCorrect answer.
clinicians used resources from their institution (91%),local/state public health (61%), and the CDC (53%).
Perception about e-mail load
More than half (61%) of the clinicians received e-mailfrom 2 to 4 of the sources included in our survey. Overhalf the Intermountain (61%) and University (56%) clin-icians believed that they received “too much” e-mail.In contrast, only one-third (35%) of the other cliniciansthought that they received “too much” e-mail (P= .005);18% thought that they received “too little” e-mail com-munication. Regardless of a clinician’s employer, thosereceiving e-mail from one of the sources were signifi-cantly more likely to report that the amount was “justright,” and those receiving e-mail from 3 of the sourceswere more likely to report that the amount was “toomuch” (P ≤ .02).
TABLE 2 ● Primary Sources of Information Used byPrimary Care Providers During the First Wave of the NovelInfluenza A (H1N1) Outbreak (n = 141)� � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � �
% Of respondents
Local/StatePublic Health
Institutional Department CDC Other
Primary source of information
about who and how to test
60 22 13 6
Primary source of information
about treatment
55 13 28 4
Educational materials to share
with patients (n = 121)
32 16 40 11
Abbreviation: CDC, Centers for Disease Control and Prevention.
Qualitative analysis of clinician feedback
Almost half of the respondents (42%) answered thequestion, “Please provide comments about good andbad aspects of the communication you received aboutthe swine flu.” The comments were classified into 7 cat-egories. The 6 most frequent categories included nega-tive feedback in the following descending order of fre-quency: “amount of e-mail communication,” “Qualityof information contained in the e-mail,” “Usefulnessof information,” “source of e-mail communication,”“timeliness of e-mail delivery,” and “length of e-mail.”The seventh and least frequent category was “generalpositive feedback.”
The clinician’s comments could be grouped into 4themes (Table 3). The first theme addressed concernsabout being overwhelmed by e-mail. The cliniciansdescribe emotional responses while trying to use in-formation in the e-mails. There were dramatic state-ments including one that described the scene in theiroffice as a “comic opera” and another that observed, “Itseemed most of the information was driven by hyste-ria.” The respondents perceived the amount of e-mailthey received as “way too much.” The second themeaddressed concerns about receiving appropriate infor-mation to act. The clinicians commented about useful-ness, quality, timeliness, and accuracy of the informa-tion and the impact on their ability to appropriatelytreat patients. The comments described the informa-tion as “confusing at times regarding proper testing”and “seemed to change daily.” The third theme ad-dressed concerns about the trustworthiness of the e-mails’ source. The clinicians commented that “medicaloffice e-mails duplicated health department ones, read-ing both to find discrepancies was too time consuming,”and “if (health care institution) recommendations are
Copyright © 2011 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
-7-

LWW/JPHMP PHH200233 November 18, 2010 22:10 Char Count= 0
42 ❘ Journal of Public Health Management and Practice
TABLE 3 ● Themes That Emerged in Comments From Clinicians in Response to an Open-Ended QuestionRequesting Feedback� � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � �
Theme 1 Overwhelmed by e-mail communicationDescription: Describes the emotional response to the communication
Sample feedback “The communication was too confusing and voluminous to be helpful.”
“Daily memos are information overload. Eventually I stopped reading them.”
“I received 10–20 e-mails/day, all with virtually identical info; the problem was, I didn’t’ know which ones were new/different.”
Theme 2 Appropriate information to actDescription Describes the difficulties of using the information relayed through e-mails to determine how to best treat patients.
Sample feedback “Recommendations on contact and respiratory isolation/protection procedures were not particularly helpful.”
“Extremely confusing.”
Theme 3 Trusting the sourceDescription Describes the difficulties of sifting through information from several different agencies
Sample feedback “One source would be best.”
“There were inconsistencies between what the CDC, State of Utah and our healthcare system were advocating in terms of testing and
treatment—mainly due to differences in available resources and lack of coordination locally.”
Theme 4 Improve communicationDescription Describes suggestions to improve e-mail and other communication strategies
Sample feedback: “. . .if you need to update please highlight changes so we know what we really need to read of new version.”
“A single web site with consistent and updated info would work better.”
“It would have been very useful to have email with a bulleted list of changes and [a] summary of [the] current state of the
epidemic/treatment/testing. . ..”
different than the CDC’s, then this difference shouldbe explicitly noted and explained.” The fourth and fi-nal theme concerned clinicians’ suggestions to improvecommunication during future public health emergen-cies. They suggested that communication be more con-cise and clearly highlight information tailored to thelocal environment that is new or different from publichealth recommendations.
Communication process after survey
During the summer of 2009, in preparation for wave 2,a new organizational strategy for communication wasestablished in Utah. Leaders from UDOH, Intermoun-tain, University, and other smaller health care organiza-tions operating in Utah created a taskforce to coordinatepublic health messaging and create unified messages.Chief medical officers were assigned the responsibilityfor distributing a unified message within their organi-zation. In addition, UDOH changed the e-mail messageformat to prominently display new and updated infor-mation using bullets at the top of each e-mail.
● Discussion
To the best of our knowledge, this study is the firstto present an objective analysis of communication be-tween public health agencies, health care organizations,and frontline clinicians during a public health emer-
gency. Frontline clinicians were receiving and seekingclinical guidance from multiple sources. The creationand distribution of content from national and localsources was often redundant. The volume of e-mailrelated to H1N1 was too great for most clinicians toprocess efficiently. Health care organizations and insti-tutions played a key role in distributing public healthguidance to clinicians and were the preferred sourcefor treatment and testing guidance for clinicians em-ployed by a health care system. Clinicians identifiedWeb sites as an important source of information, yetonly one-third visited Web sites frequently enough toaccess up-to-date information tailored for Utah clini-cians. Respondents had a high level of knowledge aboutthe testing and treatment of H1N1 when guidance wasstable; however, correct knowledge was lower afterguidance changed, as in the case of reporting require-ments. Frontline clinicians offered important practicalsuggestions for improving communication.
The process analysis validated our hypothesis thatthe current communication process is multidirectionaland redundant, relies on daily action, and requires ef-fort to be expended by personnel at many organiza-tions to achieve the same task. Within Utah, epidemiol-ogists and physicians at health departments and healthcare institutions were reviewing the situation and newguidance daily to identify changes, determine a re-sponse, and craft messages. Each source would thenattempt to communicate directly with clinicians, re-sulting in communication overload. An organizational
Copyright © 2011 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
-8-

LWW/JPHMP PHH200233 November 18, 2010 22:10 Char Count= 0
Communication With Frontline Clinicians During the 2009 Influenza Pandemic ❘ 43
communication model described by Te’eni et al mayexplain communication problems we observed.29 Theypropose that action-oriented messages intending to im-prove clinical decision-making29 should contextualizethe information and use short, structured messages.These principles may improve the design of e-mails andWeb sites and allow the clinician to quickly identify newinformation.
The survey provided unique information about com-munication during a public health emergency. Clini-cians reported using public health Web sites, but notfrequently enough to keep up with frequent changes.While most clinicians reported receiving e-mail frommultiple sources, most clinicians affiliated with an in-stitution preferred their institutional source for guid-ance about testing and treatment. Given the poten-tial for communication overload and preference forinstitutional sources, public health emergency com-munication plans should bring together public healthagencies as sources of accurate information with exist-ing institutional communication channels to distributeguidance to their affiliated clinicians. This could maxi-mize the benefits of consistent and authoritative techni-cal recommendations developed by national and statesubject-matter experts and the trusted and convenientaspects of institutional resources. In the future, the in-creasing use of electronic health records may enable thedistribution of public health alerts directly within theclinician workflow.30
The qualitative analysis of comments from the front-line clinicians provided a synthesis of communicationproblems and suggestions for improvement. The mostimportant suggestions included the following: (1) limite-mail to a single credible source, such as the chief medi-cal officer from the local health care institution, (2) iden-tify new information so clinicians do not have to searchfor it, and (3) note when local recommendations differfrom CDC recommendations and explain why differ-ences exist. These findings support previous empiricrecommendations to identify a local credible, authori-tative communication leader and deliver one straight-forward message using a clear communication path-way that is developed in consultation with health careproviders.4,5,10
Our study results informed the communication planin Utah for the second wave of the outbreak (Figure 1).During the second wave, the incidence of disease wors-ened; however, based on the author’s experience (P.G.,M.A., J.S., S.M., R.R., A.T.P., B.W., I.R., A.V.G., andC.L.B.), changes in communication reduced the numberof e-mail sources, improved synchronization and clar-ity of messages, and appeared to better support clini-cians. Several factors may have contributed to improve-ment. First, using data from this study and resourcesfrom the CDC-funded Center of Excellence in Public
Health Informatics (grant 8P01HK000030), we rapidlydeveloped the new organizational strategy for com-munication. The taskforce established by leaders fromUDOH and the major health care organizations dur-ing the summer of 2009 resulted in coordinated publichealth messaging. We believe that the enhanced com-munication allowed the state to respond effectively tothe second wave of the pandemic and for clinicians andhospitals to provide care for patients with H1N1 infec-tion while maintaining normal operating procedures.
Our study has several limitations. First, the surveyresponse rate was low. Physician surveys often havelow response rates31 and this survey was undertakenduring a public health emergency. Nevertheless, objec-tive and qualitative information was provided by 141experienced clinicians throughout Utah. In addition,the low response rate may have introduced bias that un-derestimates communication problems. The clinicianswho responded to our e-mail may have been more tech-nologically competent and less overwhelmed with e-mail than clinicians who did not respond. It is alsopossible, though, clinicians with a higher level of frus-tration were more motivated to complete the survey.Despite these limitations, the qualitative findings sup-port the process analysis and survey results and pro-vide rich details about the frontline clinician’s experi-ence with communication during the midst of a publichealth emergency. Our findings provide more compre-hensive and objective information about communica-tion with frontline clinicians during the pandemic thandescribed in recent publications.5,12,13
● Conclusion
During a public health emergency, frontline clinicianswould prefer a single source of authoritative informa-tion and the ability to easily recognize new informa-tion or information specific to their location or practicethat differs from national sources. Clinicians often pre-fer to receive information from their health care insti-tution. Therefore, when developing strategies to com-municate during public health emergencies, plannersshould consider distribution networks within healthcare organizations and institutions in their jurisdiction.Public health authorities can collaborate with these in-stitutions to distribute public health messages to affili-ated clinicians. We recommend a single e-mail from aninstitution with any differences from national or stateguidance explicitly explained.
REFERENCES
1. Sundwall DN, Rolfs RT. Utah Pandemic Influenza ResponsePlan. Salt Lake City: Utah Department of Health; 2007.
Copyright © 2011 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
-9-
LWW/JPHMP PHH200233 November 18, 2010 22:10 Char Count= 0
44 ❘ Journal of Public Health Management and Practice
2. American College of Physicians. The health care responseto pandemic influenza. Ann Intern Med. 2006;145(2):135-137.
3. Campos-Outcalt D. You, your public health departmentand the next flu pandemic. Fam Pract Manag. 2007;14(3):11-12.
4. Whitley RJ, Bartlett J, Hayden FG, Pavia AT, Tapper M, MontoAS. Seasonal and pandemic influenza: recommendations forpreparedness in the United States. J Infect Dis. 2006194(Suppl2):S155-S161.
5. Eizenberg P. The general practice experience of the swineflu epidemic in Victoria—lessons from the front line. Med JAustral. 2009;191(3):151-153.
6. Centers for Disease Control and Prevention. Swine influenzaA (H1N1) infection in two children—Southern California,March–April 2009. Morb Mortal Wkly Rep. 2009;58(15):400-402.
7. Centers for Disease Control and Prevention. Oseltamivir-resistant novel influenza A (H1N1) virus infection in two im-munosuppressed patients—Seattle, Washington, 2009. MorbMortal Wkly Rep. 2009;58(Dispatch):1-4.
8. Centers for Disease Control and Prevention. Update: novelinfluenza A (H1N1) virus infections —Worldwide, May 6,2009. Morb Mortal Wkly Rep. 2009;58(17):453-458.
9. Centers for Disease Control and Prevention. Update: in-fluenza activity—United States, April-August 2009. MorbMort Wkly Rep. 2009;58(36):1009-1012.
10. Gensheimer KF, Meltzer MI, Postema AS, Strikas RA.Influenza pandemic preparedness. Emerg Infect Dis.2003;9(12):1645-1648.
11. Khan AS, Ashford DA. Ready or not—preparedness forbioterrorism. N Engl J Med. 2001;345(4):287-289.
12. Ringel JS, Trentacost E, Lurie N. How well did healthdepartments communicate about risk at the start of theswine flu epidemic in 2009? Health Aff. 2009;28(4):w743-w50.
13. Kotsimbos T, Waterer G, Jenkins C, et al. InfluenzaA/H1N1 09: Australia and New Zealand’s winter of discon-tent. Am J Respir Crit Care Med. 2010;181(4):300-306.
14. Centers for Disease Control and Prevention. Epi-X: The Epi-demic Information Exchange. Atlanta, GA: Centers for Dis-ease Control and Prevention; 2009. http://www.cdc.gov/mmwr/epix/epix.html. Accessed August 15, 2009.
15. Centers for Disease Control and Prevention. Clinician Out-reach and Communication Activity (COCA). Atlanta, GA: Cen-ters for Disease Control and Prevention; 2009 http://www.bt.cdc.gov/coca/. Accessed August 15, 2009.
16. Centers for Disease Control and Prevention. Health alertnetwork—HAN message archive. 2009 http://www2a.cdc.gov/HAN/ArchiveSys/. Accessed August 11, 2009.
17. Centers for Disease Control and Prevention. Morbidityand Mortality Weekly Report. Atlanta: Centers for Dis-ease Control and Prevention; 2009. http://www.cdc.gov/mmwr/about.html. Accessed August 15, 2009.
18. Lurie N. H1N1 influenza, public health preparedness, andhealth care reform. N Engl J Med. 2009;9(361):843-845.
19. Nicoll A, Ammon A, Amato A, et al. Experience and lessonsfrom surveillance and studies of the 2009 pandemic in Eu-rope. Public Health. 2010;1(124):14-23.
20. Schwarzinger M, Flicoteaux R, Cortarenoda S, Obadia Y,Moatti JP. Low acceptability of A/H1N1 pandemic vaccina-tion in French adult population: did public health policy fuelpublic dissonance? PLoS One. 2010;4(5):e10199.
21. Agency for Healthcare Research and Quality. Table 1:usual source of health care and selected population char-acteristics, United States, 2007. Medical Expenditure PanelSurvey Component Data. Generated interactively. http://www.meps.ahrq.gov/mepsweb. Accessed June 19, 2010.
22. 2008 Utah Healthcare Access Survey, Office of Public HealthAssessment, Utah Department of Health. Special data re-quest, June 22, 2010. For more information, please contactKimberly Partain McNamara ([email protected]) or Jen-nifer Wrathall ([email protected]).
23. White S. Introduction to business process modeling notation(BPMN). 2004. Object Management Group/Business ProcessManagement initiative. http://www.bpmn.org/. AccessedJune 21, 2010.
24. HealthInsight. 2009. http://www.healthinsight.org/. Ac-cessed June 19, 2010.
25. Intermountain Healthcare. Germ Watch: Respiratory VirusSurveillance. Salt Lake City: Intermountain Healthcare; 2009.https://intermountain.net/portal/site/mdvsi/menuitem.1c5f03515dc95dd9c897511005744df9/. Accessed February 9,2010.
26. Utah Department of Health. Pandemic A (H1N1) 2009(swine flu) Information & resource Page. 2009. http://health.utah.gov/epi/h1n1flu/index.html. Accessed August11, 2009.
27. Centers for Disease Control and Prevention. Interim Guidancefor Clinicians on Identifying and Caring for Patients with Swine-Origin Influenza A (H1N1) Virus Infection. Atlanta, GA: Cen-ters for Disease Control; 2009. (No longer available, but orig-inally from http://cdc.gov/h1n1flu/identifyingpatients.htm). Updated May 4, 2009. Accessed May 5, 2009.
28. Utah Department of Health. Novel H1N1 Flu (Swine Flu)Utah Public Health Notification for Clinicians (5/6/2009). SaltLake City: Utah Department of Health; 2009. http://health.utah.gov/epi/h1n1flu/. Accessed May 7, 2009.
29. Te’eni D, Sagie A, Schwartz D, Zaidman N, YA-H. The processof organizational communication: a model and field study.IEEE Trans Prof Comunication. 2001;44(1):6-20.
30. Garrett NMN, Nichols B, Staes CJ, Akin A, Safran C. Char-acterization of public health alerts and their suitability foralerting in electronic health record systems. J Public HealthManag Pract. 2010(in press).
31. Asch DA, Jedrziewski MK, Christakis NA. Response rates tomail surveys published in medical journals. J Clin Epidemiol.1997;50(10):1129-1136.
Copyright © 2011 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
-10-
Public Health Communication with Utah Clinicians During the 2009
PandemicCarrie L. Byington, MD, FAAP
HA and Edna Benning Presidential Professor of Pediatrics
University of UtahVice Chair‐AAP COID
Goal for Communication
Clinicians must be able to identify the authoritative and appropriate source for clinical guidance among the variety of messages available from federal, state, and local public health authorities, professional organizations, and their own institutions
Wave 1 Communication Process Analysis Survey
• Primary Care Physicians– University of Utah– Intermountain Healthcare– Unaffiliated Rural
• 509 surveyed with 141 responding (28%)– ~ Half reported at least 25% of patients < 18 years
Dr Bocchini's Presentation
-11-
Primary Sources of Information
Institutional Local/State Health Dept
CDC Other
Who and How to Test
60% 22% 13% 6%
Treatment 55% 13% 28% 4%
Patient Education Materials
32% 16% 40% 11%
Problems Identified
• Multiple sources of information• Conflicting messages• Frequent changes• “Feeling over‐whelmed by information”• Want information from a single trusted source
– Prefer their home institution
TimeLine Solutions
• Task Force– Meets daily and crafts single message– New items are bulleted– If advice is different from past or from national sources, reason is explained
• Single message each day (week) from Chief Medical Officer
• Pediatric Hospital coordinated with task force and AAP to deliver accurate messaging for children
Dr Bocchini's Presentation
-12-
Pediatric Partnerships to Promote Pandemic Preparedness
• Utah• 1/3 of population is under 18• Important Players:• Utah Department of Health, VFC Program, Utah Statewide Immunization Information
System• 12 Autonomous Health Districts• 2 Large integrated health systems: University of Utah Health System, Intermountain• 1 Children’s Hospital: Primary Children’s Medical Center• Utah Chapter AAP• Utah Chapter AAFP• State Emergency Operations Center
Communication Efforts During the 2009 H1N1 Pandemic:
E-mail listserves from:CDCUtah Department of HealthChief Medical Officers of the Health Systems
Web Sites:CDCUtah Department of HealthGermwatch
USIIS was used for quick assessments of vaccine inventories
What Worked?
Survey of Utah Clinicians During the Pandemic
• “Public Health Communication with Frontline Clinicians During the First Wave of the 2009 Influenza Pandemic” Staes, C.J. et al
• J Public Health Management Practice, 2011, 17(1), 36-44• 141 Respondants of 509 surveyed• Results:
– 68% received e-mail/fax from UDOH– 21% received e-mail from CDC– 100% of clinicians employed by the University System or Intermountain received
e-mail from their Chief Medical Officer– 68% of non-affiliated, small, or rural practices also received the e-mails from
Intermountain
Survey of Utah Clinicians During the Pandemic
• Web Sites:– 53% visited CDC web site– 35% visited UDOH web site– 38% visited their institutional web site
– 1/3 read MMWR
Dr Cosgrove's Presentation
-13-

Communication: What did not work well?
Information Overload:in the survey, 61% received e-mail from 2 to 4 sources
“those receiving e-mail from one of the sources were significantly more likely to report the amount was “just right”.”
those receiving e-mail from 3 of the sources were more likely to report that the amount was “too much”
Suggestions:
• First, a metaphor change. Communication is not a “pipeline” pouring out information, (and certainly not three pipelines pouring out three slightly different versions of that information), but an exchange. Like the hand-off of a baton in a relay, the passing of information critically depends on the readiness and trust-level of the receiver. No matter how accurate the information, if the recipient doesn’t fully trust its validity, or its source, or can’t easily wade through the complexity of the information to confirm its validity himself, then the message is lost. The baton is dropped. Consistently having the information delivered by a known and trusted spokesman, or having the information vetted through trusted local medical organizations, ensures better pass-through of the information.
Action Steps:• Emergency Operations Center
– Staffed by already trusted spokepersons/experts.– The spokespersons should represent the local organizations (AAP, AAFP,
Hospital Systems, etc) who as a committee will vet the information, and give a local stamp of approval.
– Two-way communication back to this committee. Improves trust.– All messages should be time-stamped, include the logo of the vetting
organizations, and clearly identify any new changes.– All interactions with local media should be referred to the committee.
Dr Cosgrove's Presentation
-14-
Strategic Communications and Systematic Messaging
Susan Penfield, MDApril 27, 2011
Key Challenges
Everything is bigger…Size of state complicates disaster response254 counties
Regional variabilityDemographicSocioeconomicEnvironmentalPublic health infrastructure
Action Steps
Develop regional sentinel networkQuantify current demand for pediatric servicesQuantify current remaining capacityReport on status of critical supplies and limited resourcesReport on efficacy of public health efforts at the points of careNetwork could post on AAP Chapter website or Facebook page
Action Steps
Develop regional communication directorsCoordinate with the Department of State Health Services (DSHS) to create systematic messaging relevant to the pediatric population
Coordinate with local PH
Message for clinician vs. general public
Provide immediate pediatric consultation to PH
Dr Penfield's Presentation
-15-
Action Steps
Develop regional communication directorsMatch resources with message content
Plan for various responses to message
Manage expectations
Minimize variability of message
“Trusted Leader”
Action Steps
Schedule episodic topic-specific meetingsConference calls vs. webinarsDisease/disaster burden; testing; treatmentSurge burden and capacity data by regionPrimary and secondary preventionCreate archive for offline reviewEnsures right topical message gets to right people
Action Steps
Pre-disaster planning and preparednessEstablish partnerships
“Normal” communication with partners
Enhanced communication and coordination during a disaster
Dr Penfield's Presentation
-16-
Pandemic PreparednessStrategic Communications & Systematic Messaging
California District 9 (AAP-CA)American Academy of Pediatrics
April 2011
NameCalifornia Department of Public HealthImmunization BranchSectionDate
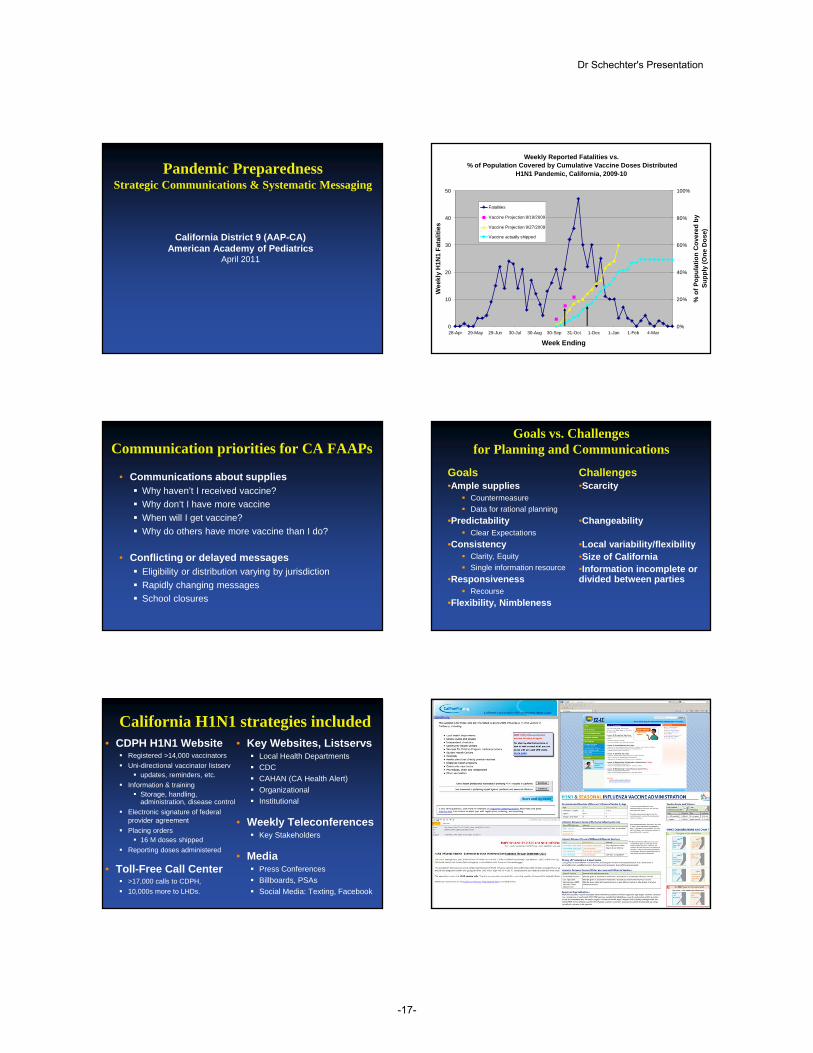
Weekly Reported Fatalities vs.% of Population Covered by Cumulative Vaccine Doses Distributed
H1N1 Pandemic, California, 2009-10
0
10
20
30
40
50
28-Apr 29-May 29-Jun 30-Jul 30-Aug 30-Sep 31-Oct 1-Dec 1-Jan 1-Feb 4-Mar
Week Ending
Wee
kly
H1N
1 Fa
talit
ies
0%
20%
40%
60%
80%
100%
% o
f Pop
ulat
ion
Cov
ered
by
Supp
ly (O
ne D
ose)
Fatalities
Vaccine Projection 8/19/2009
Vaccine Projection 9/27/2009
Vaccine actually shipped
Communication priorities for CA FAAPs
• Communications about suppliesWhy haven’t I received vaccine?Why don’t I have more vaccineWhen will I get vaccine?Why do others have more vaccine than I do?
• Conflicting or delayed messagesEligibility or distribution varying by jurisdictionRapidly changing messagesSchool closures
Goals vs. Challengesfor Planning and Communications
Goals•Ample supplies
CountermeasureData for rational planning
•PredictabilityClear Expectations
•ConsistencyClarity, EquitySingle information resource
•ResponsivenessRecourse
•Flexibility, Nimbleness
Challenges•Scarcity
•Changeability
•Local variability/flexibility•Size of California•Information incomplete or divided between parties
California H1N1 strategies included• CDPH H1N1 Website
Registered >14,000 vaccinators Uni-directional vaccinator listserv
updates, reminders, etc.Information & training
Storage, handling, administration, disease control
Electronic signature of federal provider agreementPlacing orders
16 M doses shippedReporting doses administered
• Toll-Free Call Center>17,000 calls to CDPH, 10,000s more to LHDs.
• Key Websites, ListservsLocal Health DepartmentsCDCCAHAN (CA Health Alert)OrganizationalInstitutional
• Weekly TeleconferencesKey Stakeholders
• Media Press ConferencesBillboards, PSAsSocial Media: Texting, Facebook
Dr Schechter's Presentation
-17-
Multiple resources AAP-CA Workplan Includes
Creating or Enhancing Statewide…
• Communication to minimize inconsistency of messages
• Bi-directional listserv
• Data: Practice database to facilitate appropriate prioritization of scarce resources
Could also enhance communications
Thank you for your efforts in pandemic preparedness!
Dr Schechter's Presentation
-18-












![Oracle Communications Messaging Server Installation and ... · 1[]Oracle® Communications Messaging Server Installation and Configuration Guide for Cassandra Message Store Release](https://img.pdfslide.net/doc/110x75/5e7374e0941139347653a89d/oracle-communications-messaging-server-installation-and-1oracle-communications.jpg)
















