Embed Size (px)
Citation preview

ARTICLE IN PRESS
0021-9290/$ - se
doi:10.1016/j.jb
�CorrespondE-mail addr
Journal of Biomechanics 40 (2007) 1794–1805
www.elsevier.com/locate/jbiomech
www.JBiomech.com
Modelling the circle of Willis to assess the effects of anatomicalvariations and occlusions on cerebral flows
J. Alastrueya,b, K.H. Parkerb, J. Peiroa, S.M. Byrdc, S.J. Sherwina,�
aDepartment of Aeronautics, South Kensington Campus, Imperial College London, SW7 2AZ, UKbDepartment of Bioengineering, South Kensington Campus, Imperial College London, SW7 2AZ, UK
cNHLI, International Centre for Circulatory Health, Imperial College London, W2 1LA, UK
Accepted 28 July 2006
Abstract
Blood flow in the circle of Willis (CoW) is modelled using the 1-D equations of pressure and flow wave propagation in compliant
vessels. The model starts at the left ventricle and includes the largest arteries that supply the CoW. Based on published physiological data,
it is able to capture the main features of pulse wave propagation along the aorta, at the brachiocephalic bifurcation and throughout the
cerebral arteries. The collateral ability of the complete CoW and its most frequent anatomical variations is studied in normal conditions
and after occlusion of a carotid or vertebral artery (VA). Our results suggest that the system does not require collateral pathways through
the communicating arteries to adequately perfuse the brain of normal subjects. The communicating arteries become important in cases of
missing or occluded vessels, the anterior communicating artery (ACoA) being a more critical collateral pathway than the posterior
communicating arteries (PCoAs) if an internal carotid artery (ICA) is occluded. Occlusions of the VAs proved to be far less critical than
occlusions of the ICAs. The worst scenario in terms of reduction in the mean cerebral outflows is a CoW without the first segment of an
anterior cerebral artery combined with an occlusion of the contralateral ICA. Furthermore, in patients without any severe occlusion of a
carotid or VA, the direction of flow measured at the communicating arteries corresponds to the side of the CoW with an absent or
occluded artery. Finally, we study the effect of partial occlusions of the communicating arteries on the cerebral flows, which again
confirms that the ACoA is a more important collateral pathway than the PCoAs if an ICA is occluded.
r 2006 Elsevier Ltd. All rights reserved.
Keywords: Circle of Willis; Anatomical variations; Collateral flow; One-dimensional modelling; Pulse wave propagation
1. Introduction
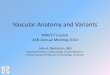
The brain critically depends on the cerebral circulationsince it has a high metabolic rate and is very sensitive toischemia (insufficient blood supply). Sufficient bloodsupply to the brain is maintained by a network of collateralvessels and a precise system of autoregulation by vasodi-latation and vasoconstriction. Blood is delivered to thebrain through the two internal carotid arteries (ICAs) andthe two vertebral arteries (VAs) (see Fig. 1, left). Each ICAbifurcates to form a middle cerebral artery (MCA) and ananterior cerebral artery (ACA) to perfuse the temporal,parietal and frontal regions of the brain (anterior circula-
e front matter r 2006 Elsevier Ltd. All rights reserved.
iomech.2006.07.008
ing author. Tel.: +44 20 7594 5052; fax: +44 20 7584 8120.
ess: [email protected] (S.J. Sherwin).
tion). The two VAs anastomose into the basilar artery,which divides into the right and left posterior cerebralarteries (PCAs) to deliver blood to the regions of the brainstem (posterior circulation). The anterior and the posteriorcirculations are interconnected by the anterior and poster-ior communicating arteries (ACoA and PCoAs). Theresulting ring-like arterial structure, called the circle ofWillis (CoW), is the main collateral pathway in the cerebralcirculation. It provides collateral blood supply to theefferent (outflow) arteries in case of missing or occludedvessels.Unfortunately, many anatomical variations of the
haemodynamically complete and well-balanced CoWshown in Fig. 1 (left) are commonly observed. Based onmore than 50 radiological and anatomical studies, Lippertand Pabst (1985) found that about 50% of the population

ARTICLE IN PRESS
Fig. 1. Schematic representation of the circle of Willis (left) and of the arterial network simulated (right), which includes the aorta, brachial, carotid,
vertebral and the main cerebral arteries. Numbers refer to names in Table 1 and arrows in the communicating arteries indicate the positive flow directions.
J. Alastruey et al. / Journal of Biomechanics 40 (2007) 1794–1805 1795
has a CoW with at least one artery absent or hypoplastic(very small or incompletely developed). These anatomicalvariations reduce the collateral availability and increase therisk of stroke and transient ischemic attack (TIA) inpatients with severe stenosis in an ICA (Henderson et al.,2000). Knowledge of the compensatory capacity of theCoW is important for neurosurgeons, vascular surgeonsand interventional radiologists when a procedure in theintracranial or extracranial cerebral arteries is to beattempted (Hoksbergen et al., 2003). Such proceduresinclude carotid endarterectomy (surgical incision in thecarotid artery to remove plaque in patients with a severecarotid stenosis), angioplasty (balloon expansion of anartery) and stenting (introduction of a mesh to keep thelumen open after angioplasty) (Henderson et al., 2000;Cebral et al., 2003).
Several mathematical studies have been carried out toinvestigate the capability of the CoW to reduce the effectsof haemodynamic pathological alterations. According toHillen et al. (1986) and based on a non-linear, 1-D modelof a complete and well-balanced CoW, blood flows in theafferent (inflow) vessels and in the segments of the CoW ofhealthy subjects are strongly influenced by their ownresistances, whereas flow in the efferent vessels is domi-nated by the peripheral resistances. With a similar model ofthe CoW, Cassot et al. (1995) claimed that small changes inthe diameter of the ACoA (within the range of 0.4–1.6mm)
have a strong influence on regulating cerebral haemody-namics in case of ICA stenosis. Viedma et al. (1997)investigated different combinations of the diameters of thecommunicating arteries that can lead to insufficientcerebral perfusion in case of an occlusion of an ICA.Moorhead et al. (2004) used a linear, 1-D model with time-varying resistances in the efferent vessels to account forvasodilatation and vasoconstriction. They showed that theomission of a single circulus vessel can be compensated forby the CoW and autoregulation to maintain the requiredefferent flow rates in case of an occlusion of an ICA.Although their model neglects flow pulsatility, it offers thepossibility of analytical solutions (Hillen et al., 1988;Cassot et al., 2000). The problem has also been approachedwith a non-linear, 2-D model with time-varying resistances,but with rigid arterial walls (Ferrandez et al., 2002; Davidet al., 2003). Ferrandez et al. (2002) found that the worstconfiguration of the CoW when an ICA is partiallyoccluded is that of a missing ipsalateral A1 segment ofthe ACA. David et al. (2003) suggested that the PCoA andother small arteries of the CoW, which are often non-visible by non-invasive magnetic-resonance (MR) techni-ques, can be better visualised by performing the scan at thespecific point in time when the flux is maximum accordingto the simulation. They also pointed out that anysimulation will be improved if it can take into accountthe correct time delay between the inlet flow waves at the

ARTICLE IN PRESSJ. Alastruey et al. / Journal of Biomechanics 40 (2007) 1794–18051796
ICAs and VAs. Several 3-D models have been used tosimulate the injection of a contrast agent and to study wall-shear stress distributions (Cebral et al., 2003), to investigatethe role played by haemodynamics in the formation,development and rupture of cerebral aneurysms (Oshima,2004), and to study autoregulation (Moore et al.2005,2006).
In this study, we apply a previously published non-linear, 1-D algorithm (Sherwin et al., 2003b) to simulateblood flow wave propagation in an elastic model of thecerebral arteries that includes the aorta, the subclavianarteries (SCAs), the brachial arteries, the common carotidarteries (CCAs), the external carotid arteries (ECAs) andthe VAs (Fig. 1, right). In this model, the time delaybetween the inflow waves at the ICAs and VAs is implicitlydetermined by the pulse wave speeds of the vesselssupplying them from the ascending aorta. Only an inflowboundary condition at the ascending aorta is required.Although 3-D models consider a better definition of thegeometry and they might account for the deformation ofthe arterial wall, they are computationally too expensive tosimulate pulse wave propagation in our model of the CoW.Because of the large wavelength of the arterial pulsecompared to the arterial diameters, 1-D modelling permitsan efficient and fast simulation of pulse wave propagation.The accuracy of our 1-D model has been successfullyvalidated in Alastruey (2006) against a well-definedhydrodynamic 1:1 replica of the left ventricle and the 55largest human conduit arteries made by Segers et al. (1998).A successful validation of our code against anothernumerical method has also been published (Sherwin etal., 2003a), along with an application to the study ofmonochorionic placentas (Franke et al., 2003).
Our objective is to investigate the effects of the mostfrequent anatomical variations and diameters of the CoWon cerebral outflows and pulse wave propagation, in
PCA, P1(9%)
ACA, A1(6%)
PCoA & contralateralPCA, P1 (9%)
Complete CoW ACoA PCoA PCoAs(49%) (1%) (9%) (9%)
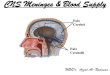
Fig. 2. Anatomical variations of the CoW studied. In each case, we
indicate the artery absent (depicted only on one side, but it can also be
absent on the other side) and its frequency, according to Lippert and Pabst
(1985). We do not consider variations involving vessels outside the CoW.
healthy conditions and after a complete occlusion of anICA or a VA. This study is limited to the most frequentanatomical variations reported in Lippert and Pabst (1985)with one or two circulus arteries absent or hypoplastic(simulated as absent). Fig. 2 shows the cases studied andtheir estimated frequency. Although the ACoA is missingin less than 1% of the cases, we include this anatomicalvariation because the ACoA is commonly recognised as thefunctionally most important collateral route in case ofsevere occlusion of an ICA (Cassot et al., 1995; Hillen etal., 1988; Hoksbergen et al., 2000b).
2. Methodology
2.1. Mathematical model
2.1.1. Governing equations
The mathematical model is based on the non-linear, 1-Dequations of pressure and flow wave propagation incompliant vessels. The governing system of equationsresults from conservation of mass and momentum appliedto a 1-D impermeable and deformable tubular controlvolume of incompressible and Newtonian fluid. They takethe form (Sherwin et al., 2003b; Alastruey, 2006)
qA
qtþ
qðAUÞ
qx¼ 0, (1)
qU
qtþU
qU
qx¼ �
1
rqp
qxþ
f
rA, (2)
where x is the axial coordinate along the vessel, t is thetime, Aðx; tÞ is the cross-sectional area of the vessel, Uðx; tÞis the average axial velocity, pðx; tÞ is the average internalpressure over the cross-section, r is the density of the bloodtaken here to be 1050Kgm�3 and f ðx; tÞ is the friction forceper unit length, which is modelled as f ¼ �22pmU
according to Smith et al. (2001), with m the viscosity ofthe blood taken here to be 4.5mPa s.The system of equations is completed with a pressur-
e–area relation previously used in Olufsen (1999), Sherwinet al. (2003b), Alastruey (2006). It assumes a thin,homogeneous and elastic arterial wall and it takes the form
p ¼ p0 þb
A0ðffiffiffiffiAp�
ffiffiffiffiffiffiA0
pÞ; b ¼
ffiffiffipp
hE
ð1� s2Þ, (3)
where A0 and h are the sectional area and wall thickness atthe reference state ðp0;U0Þ, with p0 and U0 assumed to bezero, E is the Young’s modulus and s is the Poisson’s ratio,typically taken to be s ¼ 1
2since biological tissue is
practically incompressible. The parameter b is related tothe speed of pulse wave propagation, c, through (Sherwinet al., 2003b; Alastruey, 2006)
c2 ¼b
2rA0A1=2. (4)

ARTICLE IN PRESSJ. Alastruey et al. / Journal of Biomechanics 40 (2007) 1794–1805 1797
2.1.2. Treatment of boundary conditions and bifurcations
The hyperbolic system of partial differential equations(1)–(3) is solved in each arterial segment of Fig. 1 (right)with the following boundary conditions. At the proximalend of the ascending aorta we enforce a periodical inflowrate QðtÞ with a period of 1 s. Each period consists of a half-sinusoidal flow rate wave with a peak value Q of 485ml s�1
(adjusted to produce a physiological cardiac output andaortic mean pressure with the peripheral resistances shownin Table 1) and a duration t ¼ 0:3 s (systole). Flow rate iszero in the rest of the period (diastole),
QðtÞ ¼Q sin pt
t
� �if tot;
0 otherwise:
((5)
This boundary condition acts as a total reflector when flowrate is zero, simulating the closure of the aortic valveduring diastole.
Boundary conditions of the arterial segments joining atjunctions are prescribed by enforcing conservation of mass
Table 1
Physiological data used in the model shown in Fig. 1 (right) based upon the da
al. (2006)
Arterial segment Length Initial Thickne
(cm) radius (cm)
(cm)
1. Ascending aorta 4.0 1.200 0.163
2. Aortic arch I 2.0 1.120 0.126
3. Brachiocephalic 3.4 0.620 0.080
4. Aortic arch II 3.9 1.070 0.115
5. L. common carotid 20.8 0.250 0.063
6. R. common carotid 17.7 0.250 0.063
7. R. subclavian 3.4 0.423 0.067
8. Thoracic aorta 15.6 0.999 0.110
9. L. subclavian 3.4 0.423 0.067
10. L. ext. carotid 17.7 0.150 0.038
11. L. int. carotid I 17.7 0.200 0.050
12. R. int. carotid I 17.7 0.200 0.050
13. R. ext. carotid 17.7 0.150 0.038
14. R. vertebral 14.8 0.136 0.034
15. R. brachial 42.2 0.403 0.067
16. L. brachial 42.2 0.403 0.067
17. L. vertebral 14.8 0.136 0.034
18. L. int. carotid II 0.5 0.200 0.050
19. L. PCoA 1.5 0.073 0.018
20. R. PCoA 1.5 0.073 0.018
21. R. int. carotid II 0.5 0.200 0.050
22. Basilar 2.9 0.162 0.040
23. L. MCA 11.9 0.143 0.036
24. R. MCA 11.9 0.143 0.036
25. L. ACA, A1 1.2 0.117 0.029
26. R. ACA, A1 1.2 0.117 0.029
27. L. PCA, P1 0.5 0.107 0.027
28. R. PCA, P1 0.5 0.107 0.027
29. L. ACA, A2 10.3 0.120 0.030
30. R. ACA, A2 10.3 0.120 0.030
31. ACoA 0.3 0.074 0.019
32. L. PCA, P2 8.6 0.105 0.026
33. R. PCA, P2 8.6 0.105 0.026
and continuity of the total pressure pþ 12rU2. The distal
end of each terminal branch is coupled to a three-elementlumped parameter model, consisting of two resistances, R1
and R2, and a compliance, C, to account for both theresistive and the compliant effects of the vessels supplied bythe terminal arteries. This terminal model produces morephysiological pulse waves than a purely reflective model, asused in Sherwin et al. (2003b); Wang and Parker (2004),because it partially reflects and smoothes any incomingwave, causing a phase delay between pressure and flow. Itis governed by the differential equation
p1D þ R2Cdp1D
dt¼ pv þ ðR1 þ R2ÞQ1D þ R1R2C
dQ1D
dt,
(6)
where p1D and Q1D are the pressure and volume flow rate atthe distal end of the 1-D terminal artery, and pv representsthe pressure at the entrance of the venous system, taken tobe 5mmHg.
ta collected by Stergiopulos et al. (1992), Fahrig et al. (1999) and Moore et
ss Elastic Peripheral Peripheral
modulus resistance compliance
ð106 PaÞ ð109 Pa sm�3Þ ð10�10 m3 Pa�1Þ
0.4 — —
0.4 — —
0.4 — —
0.4 — —
0.4 — —
0.4 — —
0.4 — —
0.4 0.18 38.70
0.4 — —
0.8 5.43 1.27
0.8 — —
0.8 — —
0.8 5.43 1.27
0.8 — —
0.4 2.68 2.58
0.4 2.68 2.58
0.8 — —
1.6 — —
1.6 — —
1.6 — —
1.6 — —
1.6 — —
1.6 5.97 1.16
1.6 5.97 1.16
1.6 — —
1.6 — —
1.6 — —
1.6 — —
1.6 8.48 0.82
1.6 8.48 0.82
1.6 — —
1.6 11.08 0.62
1.6 11.08 0.62

ARTICLE IN PRESSJ. Alastruey et al. / Journal of Biomechanics 40 (2007) 1794–18051798
At any point in the network we can simulate a totalocclusion by enforcing the condition U ¼ 0 at the desiredpoint, or a partial occlusion by decreasing locally thecalibre of the artery.
2.1.3. Numerical scheme
Eqs. (1)–(3) are solved using a discontinuous Galerkinscheme with a spectral/hp spatial discretisation and asecond-order Adams–Bashforth time-integration scheme.This scheme is suitable for the 1-D formulation because itcan propagate waves of different frequencies withoutsuffering from excessive dispersion and diffusion errors.Details on this algorithm can be found in (Karniadakis andSherwin, 2003; Sherwin et al., 2003b).
2.2. Physiological data
The physiological parameters used in each arterialsegment are given in Table 1. Our model aims atrepresenting the arterial geometry and elasticity of ahealthy young adult. In the absence of detailed knowledgeof these properties, the geometry and wall elasticity of thearteries up to the carotids and vertebrals are based on datapublished in Stergiopulos et al. (1992). In the cerebralarteries, we consider the lengths published in Fahrig et al.(1999), obtained from average values from several pub-lished sources. The radii at the reference state ðp0;U0Þ
correspond to an average of 13 magnetic-resonanceangiographies (MRAs) of complete CoWs (Moore et al.,2006). In all the cerebral vessels, we assume h to be 25% ofthe radius at reference conditions. In the carotids and VAswe consider E ¼ 8� 105 Pa, and in the remaining vesselsE ¼ 16� 105 Pa, since they are stiffer than extracranialarteries with similar calibres (Hayashi et al., 1980).
At the distal end of each terminal branch, we assume R1
to be equal to the characteristic impedance of the terminalbranch, Z0 ¼ rc0=A0 with c0 ¼ cðA0Þ (4), since it is thevalue that minimises the total impedance of the three-element lumped parameter model (Rainest et al., 1974).The total resistance of the arterial system in normalconditions is considered to be RT ¼ 1:34� 108 Pa s m�3,according to Stergiopulos et al. (1992). The value of eachperipheral resistance Rp ¼ R1 þ R2 is determined byassuming the following flow distribution in normalconditions: 15% of the cardiac output perfuses the head(Burton, 1965), 5% supplies each arm and 75% flows to therest of the body through the thoracic aorta. In the terminalvessels of the head, outflows are assumed to be propor-tional to the initial cross-sectional areas of the perfusingterminal arteries.
The total volume compliance of the arterial system innormal conditions is taken to be 9:45� 10�9 m3 Pa�1
(Simon et al., 1979). This value corresponds to thecompliance of each arterial segment, calculated throughA0l=rc20 (l is the length of the segment) (Milisic andQuarteroni, 2004), plus the total peripheral compliance. Inthe absence of any data, we distribute the total peripheral
compliance among the terminal branches in the sameproportion as the flow distribution determined by theperipheral resistances.
3. Results and discussion
Our algorithm allows us to easily modify the geometryand connectivity of each arterial segment, to partially ortotally occlude arteries, and to calculate pressure and flowtime histories at any point in the system. We initiallyassume Aðx; 0Þ ¼ A0 and Uðx; 0Þ ¼ 0 in all the arteries, andwe run each simulation for sufficient cardiac cycles untilthe waveforms become periodic. This typically takesaround 10 cycles.In Section 3.1, we analyse pressure and flow wave
propagation along the aorta, the brachiocephalic bifurca-tion and the rest of vessels supplying the CoW. In Section3.2, we investigate how cerebral flows are affected byanatomical variations (Section 3.2.1), by the total occlusionof an ICA or a VA (Section 3.2.2) and by several degrees ofpartial occlusions of the communicating arteries (Section3.2.3). This study focuses on flow rates, because they areclinically important in brain perfusion and they can bemeasured non-invasively with phase-contrast MR (PC-MR) (Cebral et al., 2003), and on flow velocity patterns,which can be measured non-invasively with transcranialcolour-coded duplex ultrasonography (TCCD) (Hoksber-gen et al., 2003) and PC-MR (Cebral et al., 2003).
3.1. Wave propagation along the aorta and in the arteries
supplying the CoW
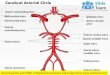
Our model is able to capture the main wave propagationfeatures observed in in vivo measurements along the aorta(McDonald, 1960; O’Rourke, 1967), such as the increase inpulse pressure as we move away from the heart, the dicroticnotch at the end of systole and the diastolic decay due tothe windkessel effect (Fig. 3, left). Moreover, the peak flowdecreases as we move down the aorta, though thecharacteristic backward flow after the closure of the aorticvalve is almost absent (Fig. 3, right), because of theapproximated inflow rate (5) at the inlet of the ascendingaorta without any reversal flow. At the inlet of theascending aorta, the systolic pressure is 17.3 kPa(130mmHg) and the diastolic pressure is 10.1 kPa(76mmHg). The cardiac output is 5:7 lmin�1.Our model is also able to predict the in vivo observed
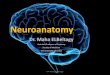
pressure and flow patterns at the brachiocephalic bifurca-tion. In vivo Doppler measurements of velocity in thebrachiocephalic artery (BrA) (parent) and the right SCAand CCA (daughters) of a healthy young adult (all takenapproximately 1 cm from the bifurcation) show a signifi-cant difference between velocity waveforms (Fig. 4, top).Flow is always directed towards the head (antegrade) in theCCA, ensuring cerebral blood supply at any instant duringthe cardiac cycle, whereas in the BrA and right SCA flow isbiphasic, with a period of backward flow at the end of

ARTICLE IN PRESS
Fig. 3. Pressure (left) and flow volume rate (right) over one cardiac cycle along the aorta. The legend indicates the distance of the measurement from the
left ventricle.
Fig. 4. Flow velocity at the brachiocephalic (BrA), right subclavian (SCA) and right common carotid (CCA) arteries measured in vivo with Doppler
ultrasound in a healthy young adult (top) and predicted by our model 1 cm proximal to the bifurcating point (bottom left). We also show the predicted
pressures (bottom right).
J. Alastruey et al. / Journal of Biomechanics 40 (2007) 1794–1805 1799

ARTICLE IN PRESSJ. Alastruey et al. / Journal of Biomechanics 40 (2007) 1794–18051800
systole. These measurements are in agreement with thevelocity waveforms from a young normal subject publishedby Oates (2001). The results predicted by our simulation inthe BrA and the right SCA and CCA are in goodqualitative agreement with the in vivo measurements(Fig. 4, bottom left). We notice that a quantitativecomparison cannot be achieved because we lack informa-tion about the inflow at the ascending aorta, the arterialgeometry and elasticity and the terminal impedances of oursubject. The simulated flow patterns where the left CCAbranches off the aortic arch and the two VAs branch offthe corresponding SCA present the same pattern as in thebrachiocephalic bifurcation, so that flow is always ante-grade during the cardiac cycle in the four arteries perfusingthe head. These results are also in agreement with theDoppler measurements published by Oates (2001).
According to our model, flow is antegrade in the CCAsand the VAs of all the anatomical variations depicted inFig. 2, even though the predicted pressure waveforms inthese vessels are very similar to the corresponding pressuresin their adjacent arteries (Fig. 4, bottom right). Therefore,antegrade flow is a consequence of the length, diameter,elasticity and mean flow (determined by the terminalresistances) of the CCAs, VAs and their adjacent arteries.
3.2. Flow in the cerebral arteries
3.2.1. Normal conditions
Our model predicts very similar flow patterns in all theefferent arteries of the complete CoW (Fig. 5, left), withflows always directed towards the brain. Differencesbetween the same efferent artery at both sides of theCoW cannot be appreciated in the scale of the figure, whichindicates that flows in the cerebral arteries are not affectedby the asymmetry introduced by the BrA. Table 2 (firststudy case) shows the mean volume outflows in the cerebral
Fig. 5. Flow velocity over one cardiac cycle in the middle point of the efferen
(left) and after occlusion of the right ICA (right). In normal conditions, the
distinguished in the scale of the figure. With the occlusion, only the results on t
with slightly higher values. Positive values in the communicating arteries follo
arteries. We observe that the MCAs receive the highestblood supply, followed by the ACAs. The values anddistribution of these outflows are within acceptablephysiological ranges compared to average in vivo measure-ments calculated in Fahrig et al. (1999) based on severalpublished sources (last row of Table 2).Fig. 5 (left) shows that flows in the communicating
arteries are small but sufficiently significant to maintainthese vessels active. They arise from pressure phase delaysbetween both sides of the CoW, as a consequence of theasymmetry introduced by the BrA. Table 2 shows that thevolume flow rates along these arteries are about two ordersof magnitude smaller than the volume outflow rates in theefferent arteries, which suggests that the system does notrequire the collateral flow pathways through the commu-nicating arteries to adequately perfuse the brain of healthysubjects with a complete CoW. Their MCAs and ACAs aresupplied with flow coming mainly from the ipsalateral ICAand their PCAs with flow through the basilar artery.Anatomical variations with missing communicating
arteries present mean volume outflow rates in the efferentarteries and the remaining communicating arteries thatdiffer in less than 1% the results obtained for the completeCoW (Table 2). The flow patterns in their efferent arteriesalso differ in less than 1% the results shown in Fig. 5 (left)for the complete CoW.When one of the ACAs (A1) or PCAs (P1) is absent or
hypoplastic, our model predicts high collateral volume flowrates through the communicating arteries, since they arethe only possible pathway to an efferent vessel (Table 2).Flows in the efferent arteries present the same patterns asshown in Fig. 5 (left) for the complete CoW, though withdifferences of less than 15% in the value of flow velocities.In terms of mean volume outflows, the differences betweenthese anatomies and a complete CoW are also less than15% (Table 2), which suggests that collateral flows through
t and communicating arteries of the complete CoW, in normal conditions
results in the same cerebral vessel at both sides of the CoW cannot be
he right side are shown. On the left side, they present a similar pattern but
w the direction of the arrows in Fig. 1 (right).

ARTICLE IN PRESS
Table 2
Mean volume flow rates (in ml=s) at the outlet of the efferent arteries and in the middle of the communicating arteries for different study cases
Study case RACA LACA RMCA LMCA RPCA LPCA RPCoA LPCoA ACoA
Complete circle 1.16 1.16 1.73 1.72 0.90 0.89 �0.01 0.01 �0.05
ACoA absent 1.16 1.16 1.73 1.72 0.90 0.89 �0.01 0.02 —
RPCoA absent 1.16 1.16 1.73 1.72 0.89 0.89 — 0.01 �0.05
LPCoA absent 1.16 1.16 1.73 1.72 0.90 0.90 0.00 — �0.05
PCoAs absent 1.16 1.16 1.73 1.72 0.90 0.90 — — �0.05
RACA (A1) absent 1.07 1.11 1.78 1.68 0.90 0.90 �0.22 0.22 1.07
LACA (A1) absent 1.12 1.08 1.69 1.78 0.90 0.90 0.18 �0.19 �1.08
RPCA (P1) absent 1.15 1.16 1.70 1.72 0.79 0.93 �0.79 0.27 0.21
LPCA (P1) absent 1.16 1.15 1.73 1.70 0.93 0.79 0.25 �0.79 �0.32
RPCA (P1) and LPCoA absent 1.15 1.15 1.70 1.71 0.79 0.94 �0.79 — 0.14
LPCA (P1) and RPCoA absent 1.15 1.14 1.72 1.69 0.94 0.79 — �0.79 �0.25
Fahrig et al. (1999) 1.1 1.1 2.0 2.0 0.8 0.8 — — —
The last row shows an average of published in vivo measurements at the efferent arteries calculated by Fahrig et al. (1999). Positive values of flow in the
communicating arteries follow the direction of the arrows in Fig. 1 (right). R stands for right and L for left.
Fig. 6. Flow velocity over one cardiac cycle in the middle point of the ACoA (left) and the left PCoA (right) (similar results are obtained in the right
PCoA) of the complete CoW (thick solid lines) and the anatomical variations with missing vessels as indicated in the figures. Positive values follow the
direction of the arrows in Fig. 1 (right). We notice that the direction of flow in the ACoA and the PCoAs depends upon the side of the CoW where there is
the hypoplastic ACA (A1) or PCA (P1).
J. Alastruey et al. / Journal of Biomechanics 40 (2007) 1794–1805 1801
the communicating arteries are sufficient to perfuse all theareas of the brain in subjects with a hypoplastic ACA (A1)or PCA (P1). Although fluxes are reduced in some efferentvessels, the vasoconstriction and vasodilatation of thecerebral vessels and the wall remodelling in the activecollateral vessels to increase the calibre of their lumen arelikely to compensate for any reduction in blood flows.However, these autoregulation mechanisms have not beenconsidered in our simulations.
Therefore, when flow or volume flow rate in anycommunicating artery is high enough to be measured in apatient without a significant stenosis in any afferent artery,at least one of the ACAs (A1) or PCAs (P1) is hypoplastic.Fig. 6 (left) shows that the direction of flow in the ACoAindicates the side of the CoW where there is a hypoplasticACA (A1) or PCA (P1). Furthermore, flow waveforms inthe ACoA are similar to flow waveforms in the ACAs (A2)in anatomies with a hypoplastic ACA (A1), which suggeststhat TCCD measurements in the ACoA should allow us to
detect the presence of a disfunctional ACA (A1). Thedirection of flow in the PCoAs also indicates the side wherethere is a disfunctional ACA (A1) or PCA (P1) (Fig. 6,right). In this case, flow waveforms in a PCoA are similarto flow waveforms in the ipsalateral PCA (P2) if theipsalateral PCA (P1) is hypoplastic.The mean flow rates given in Table 2 depend on the
input flow rate enforced at the ascending aorta and theperipheral resistances. For the cases with an absent ACA(A1) or PCA (P1) they also depend on the resistance of thecommunicating arteries. Consequently, cerebral mean flowrates are very sensitive to changes in the geometry andelasticity of the communicating arteries when an ACA (A1)or PCA (P1) is absent. Changes in the rest of the arteriessimulated (within physiological ranges) affect pulse wave-forms but not mean flows.Finally, we notice that MRA techniques may not be able
to detect the presence of the communicating arteries insubjects with a complete CoW or with anatomical

ARTICLE IN PRESSJ. Alastruey et al. / Journal of Biomechanics 40 (2007) 1794–18051802
variations involving these arteries, since flow velocities inthe communicating arteries of these anatomies are abouttwo orders of magnitude smaller than in the rest of thecerebral vessels, according to our model.
3.2.2. The effects of occlusions of the afferent arteries
The occlusion of an ICA considerably increases flow inthe communicating arteries of the complete CoW (Fig. 5,right) and all the anatomical variations studied.
Fig. 7 shows the ability of each anatomical variation in Fig.2 to maintain sufficient efferent outflow rates after anocclusion of either the right ICA (dark numbers) or the rightVA (light numbers). The number at the outlet of each efferentartery indicates the percentage of reduction in mean outflowrate calculated as ðQNC �QOCÞ=QNC � 100, where QNC isthe mean outflow rate in normal conditions (shown inTable 2) and QOC is the mean outflow rate with the occlusion.
Fig. 7. Reduction in mean outflow rate at the outlet of the efferent arteries of
bottom of each case), when the right ICA (black numbers) or the right VA (lig
mean outflow rate with the occlusion, as explained in the text. Numbers with
We notice that in all the cases studied the occlusion ofthe VA has relative little effect compared to the occlusionof the ICA. If the right ICA is occluded, the right MCA isthe efferent artery with the highest reduction in outflowrate in all the anatomies, followed by the right ACA (A2).In anatomical variations involving the communicatingarteries, the absence of the ACoA is the case with thehighest decrease in efferent mean outflows, becausecollateral flow from the left ICA to the right ACA (A2)and MCA has less viscous dissipation through the ACoAthan through the PCoAs, since the former route is shorter.Hence, the ACoA is a more critical collateral pathway thanboth PCoAs if an ICA is occluded. This is in agreementwith the results obtained in Cassot et al. (1995), Hillen et al.(1988), Hoksbergen et al. (2000b). If the right VA isoccluded, the PCAs (P2) are the efferent arteries with thehighest reduction in flow rates and the PCoAs become the
each anatomical variation studied (the arteries absent are indicated at the
ht numbers) are occluded. Numbers express the percentage of reduction in
‘‘+’’ indicate an increase in mean outflow rates.

ARTICLE IN PRESS
Fig. 8. Mean outflows in the right efferent arteries and in the ACoA and right PCoA of the complete CoW as a function of the diameter of the ACoA (left)
and the right PCoA (right). The right ICA is completely occluded in its middle point.
J. Alastruey et al. / Journal of Biomechanics 40 (2007) 1794–1805 1803
collateral routes that play a more important role in thecompensatory mechanism of the CoW.
Among all the cases studied, the anatomical variationwithout an ACA (A1) and with a complete occlusion of thecontralateral ICA presents the highest reduction in meanoutflow rates in three efferent arteries. Therefore, weconclude that this is the anatomy at the highest risk of TIAand cerebral stroke.
3.2.3. Partial occlusions of the communicating arteries
In this section we study the effect on cerebral flows ofpartial occlusions of the communicating arteries of thecomplete CoW combined with the occlusion of the rightICA. Fig. 8 shows the effect of the calibre of the ACoA(left) and the right PCoA (right) on the mean outflow ratesin the three right efferent arteries, when the right ICA iscompletely occluded in its middle point. We observe thatthe outflows of the ACA (A2) and the MCA dependstrongly on the calibre of the ACoA in the range of calibresfrom 0.4 to 1.6mm, approximately, whereas the outflow atthe PCA (P2) remains almost constant in all the range ofcalibres studied. On the other hand, the calibre of the rightPCoA affects the outflows at the three efferent arteries,specially in the range of calibres from 0.8 to 2.2mm. For agiven calibre, collateral flow through the ACoA is higherthan through the right PCoA. Furthermore, a reduction inthe calibre of the ACoA produces a higher reduction in themean flow rates of the ACA (A2) and MCA than areduction in the calibre of the right PCoA. Theseobservations confirm the previous results showing thatthe ACoA is a more important collateral pathway than thePCoAs if an ICA is occluded.
We also observe that the mean flow rate of the right PCA(P2) decreases with increasing calibre of the right PCoA,since more blood from the posterior circulation istransported to the anterior circulation through the PCoA.
Using TCCD measurements and postmortem anatomy,Hoksbergen et al. (2000a) determined that the thresholddiameter allowing for collateral flow through the commu-nicating arteries is between 0.4 and 0.6mm. Cassot et al.(1995) and Dickey et al. (1996) computationally obtained athreshold calibre of 0.4mm for the ACoA. Moreover,Dickey et al. found that the threshold diameter for thePCoA in patients with a well-functioning ACoA and withan occlusion of an ICA is between 0.5 and 0.6mm.According to our model, collateral flow in the ACoA startsfor smaller calibres than in the PCoA (0.2 versus 0.4mm).The efferent outflows significantly change for calibreshigher than 0.4mm in the ACoA and 0.8 in the PCoA,approximately (Fig. 8). We believe that the minimumdiameter allowing for collateral flow through the PCoA islarger than through the ACoA because the longer length ofthe PCoAs compared to the length of the ACoA producesa higher resistance to flow.
4. Conclusions
We have presented a 1-D model of pulse wavepropagation that is able to capture the main wavepropagation features observed in vivo in the aorta, thecerebral arteries and the arteries supplying them from theaorta. From the origin of the carotid and VAs and up tothe efferent vessels of the CoW, our model predicts acontinuous blood flow towards the brain during all thecardiac cycles, which is in agreement with in vivomeasurements (Fig. 4 and Oates, 2001).We have used this model to study the effects of the most
frequent anatomical variations of the CoW on flow ratesand pulse waveforms in the communicating and efferentarteries. According to our results, the system does notrequire collateral pathways through the communicatingarteries to adequately perfuse the brain of healthy subjects.The communicating arteries become important to maintain

ARTICLE IN PRESSJ. Alastruey et al. / Journal of Biomechanics 40 (2007) 1794–18051804
sufficient brain perfusion in anatomical variations with amissing ACA (A1) or PCA (P1), or when an ICA or a VAis occluded. Moreover, the ACoA is a more criticalcollateral pathway than the PCoAs if an ICA is occluded,which is in agreement with other clinical and numericalstudies (Cassot et al., 1995; Hillen et al., 1988; Hoksbergenet al., 2000b). If a VA is occluded, the reductions in meanefferent flow rates are significantly smaller than if an ICA isoccluded, and the PCoAs are the collateral routes that playa more important role in the compensatory mechanism ofthe CoW. The worst scenario among all the anatomiesstudied in terms of reduction in the mean cerebral outflowsis a CoW without an ACA (A1) and with a completeocclusion of the contralateral ICA.
Our model also predicts that in subjects without asignificant stenosis in any afferent artery a hypoplasticACA (A1) can be detected with flow measurements at theACoA and a hypoplastic PCA (P1) with flow measure-ments at the PCoAs. Moreover, the direction of flow in thecommunicating arteries indicates the side of the CoW withsuch a hypoplastic artery. It is also important to notice thatin subjects with a complete CoW or with anatomicalvariations involving the communicating arteries, flowvelocities within these arteries may be too small forMRA techniques to detect their presence.
An obvious drawback of this study is the lack ofexperimental confirmation, because of the lack of detailedinformation on the geometry and elasticity of the arterialnetwork and on the boundary conditions. The resultspresented depend on the physiological data used, which isbased on published measurements in healthy young adults.
All the simulations have always been carried out with thesame peripheral impedances and, hence, this work hasanalysed the compensatory ability of the CoW itself to reducethe effects of pathological alterations. This is the firstmechanism of autoregulation that takes place. Othermechanisms such as vasodilatation, vasoconstriction and wallremodelling have been ignored. As mentioned previously,autoregulation by vasodilatation and vasoconstriction can besimulated with time-varying resistances (Ferrandez et al.,2002; David et al., 2003; Moorhead et al., 2004).
Our 1-D model is a fast and powerful research tool toenhance the understanding of blood flow patterns anddistributions throughout the brain within a prescribedgeometry. If used in conjunction with patient-specificgeometry, it can predict the haemodynamic effect ofclinical interventions such as carotid endarterectomy,angioplasty and stenting. It can be also applied to studythe effect on cerebral outflows of time-dependent changeswithin the cardiac output, since it allows for a non-periodicinflow boundary condition at the ascending aorta.Furthermore, it has the potential to simulate local flowsin detail if coupled to a 3-D simulation of a local area ofthe cerebral circulation, which, in turn, can be used toinvestigate, for instance, the flow patterns that lead toincreased probability of formation of atherosclerosis orintracranial aneurysms.
Acknowledgements
The authors would like to acknowledge Jazmın Aguadofor her contributions. This work was partially supported bythe EU RTN Haemodel Project (contract number HPRN-CT-2002-00270). The last author would also like toacknowledge partial support under an EPSRC AdvancedResearch Fellowship.
References
Alastruey, J., 2006. Numerical modelling of pulse wave propagation in the
cardiovascular system: development, validation and clinical applica-
tions. Ph.D. Thesis, Departments of Bioengineering and Aeronautics,
Imperial College London.
Burton, A.C., 1965. Physiology and Biophysics of the Circulation. Year
Book Medical Publishers.
Cassot, F., Vergeur, V., Bossuet, P., Hillen, B., Zagzoule, M., Marc-
Vergnes, J.P., 1995. Effects of anterior communicating artery diameter
on cerebral hemodynamics in internal carotid artery disease. Circula-
tion 92, 3122–3131.
Cassot, F., Zagzoule, M., Marc-Vergnes, J.P., 2000. Hemodynamic role of
the circle of Willis in stenoses of internal carotid arteries. An analytical
solution of a linear model. Journal of Biomechanics 33, 395–405.
Cebral, J.R., Castro, M.A., Soto, O., Lohner, R., Alperin, N., 2003.
Blood-flow models of the circle of Willis from magnetic resonance
data. Journal of Engineering Mathematics 47, 369–386.
David, T., Brown, M., Ferrandez, A., 2003. Auto-regulation and blood
flow in the cerebral circulation. International Journal for Numerical
Methods in Fluids 43, 701–713.
Dickey, P.S., Kailasnath, P., Bloomgarden, G., Goodrich, I., Chaloupa,
J., 1996. Computer modeling of cerebral blood flow following internal
carotid occlusion. Neurological Research 18, 259–266.
Fahrig, R., Nikolov, H., Fox, A.J., Holdsworth, D.W., 1999. A three-
dimensional cerebrovascular flow phantom. Medical Physics 26,
1589–1599.
Ferrandez, A., David, T., Brown, M., 2002. Numerical models of auto-
regulation and blood flow in the cerebral circulation. Computer
Methods in Biomechanics and Biomedical Engineering 5, 7–20.
Franke, V.E., Parker, K.H., Wee, L.Y., Fisk, N.M., Sherwin, S.J., 2003.
Time domain computational modelling of 1D arterial networks in
monochorionic placentas. Mathematical Modelling and Numerical
Analysis 37, 557–580.
Hayashi, K., Handa, H., Nagasawa, S., Okumura, A., Moritake, K., 1980.
Stiffness and elastic behavior of human intracranial and extracranial
arteries. Journal of Biomechanics 13, 175–184.
Henderson, R.D., Eliasziw, M., Fox, A.J., Rothwell, P.M., Barnett,
H.J.M., 2000. Angiographycally defined collateral circulation and risk
of stroke in patients with severe carotid artery stenosis. Stroke 31,
128–132.
Hillen, B., Hoogstraten, H., Post, L., 1986. A mathematical model of the
flow in the circle of Willis. Journal of Biomechanics 19, 187–194.
Hillen, B., Drinkenburg, A.H., Hoogstraten, H.W., Post, L., 1988.
Analysis of flow and vascular resistance in a model of the circle of
Willis. Journal of Biomechanics 21, 807–814.
Hoksbergen, A.W.J., Fulesdi, B., Legemate, D.A., Csiba, L., 2000a.
Collateral configuration of the circle of Willis. Transcranial color-
coded duplex ultrasonography and comparison with postmortem
anatomy. Stroke 31, 1346–1351.
Hoksbergen, A.W.J., Legemate, D.A., Ubbink, D.T., Jacobs, M.J.H.M.,
2000b. Collateral variations in circle of Willis in atherosclerotic
population assessed by means of transcranial color-coded duplex
ultrasonography. Stroke 31, 1656–1660.
Hoksbergen, A.W.J., Majoie, C.B.L., Hulsmans, F.J.H., Legemate, D.A.,
2003. Assessment of the collateral function of the circle of Willis:
three-dimensional time-of-flight MR angiography compared with

ARTICLE IN PRESSJ. Alastruey et al. / Journal of Biomechanics 40 (2007) 1794–1805 1805
transcranial color-coded duplex sonography. American Journal of
Neuroradiology 24, 456–462.
Karniadakis, G.E., Sherwin, S.J., 2003. Spectral/hp Element Methods for
CFD. Oxford University Press, Oxford.
Lippert, H., Pabst, R., 1985. Arterial Variations in Man: Classification
and Frequency. J.F. Bergmann, Munich.
McDonald, D.A., 1960. Blood Flow in Arteries. Williams and Wilkins,
Baltimore.
Milisic, V., Quarteroni, A., 2004. Analysis of lumped parameter
models for blood flow simulations and their relation with 1D
models. Mathematical Modelling and Numerical Analysis 38,
613–632.
Moore, S.M., Moorhead, K.T., Chase, J.G., David, T., Fink, J., 2005.
One-dimensional and three-dimensional models of cerebrovascular
flow. Journal of Biomechanical Engineering 127, 440–449.
Moore, S.M., David, T., Chase, J.G., Arnold, J., Fink, J., 2006. 3D
models of blood flow in the cerebral vasculature. Journal of
Biomechanics 39, 1454–1463.
Moorhead, K.T., Doran, C.V., Chase, J.G., David, T., 2004. Lumped
parameter and feedback control models of the auto-regulatory
response in the circle of Willis. Computer Methods in Biomechanics
and Biomedical Engineering 7, 121–130.
Oates, C., 2001. Cardiovascular Haemodynamics and Doppler Wave-
forms Explained. Greenwich Medical Media LTD.
Olufsen, M.S., 1999. Structured tree outflow condition for blood flow in
larger systemic arteries. American Journal of Physiology 276,
H257–H268.
O’Rourke, M.F., 1967. Pressure and flow waves in systemic arteries and
the anatomical design of the arterial system. Journal of Applied
Physiology 23, 139–149.
Oshima, M., 2004. A new approach to cerebral hemodynamics. Patient-
specific modelling and numerical simulation of blood and arterial wall
interaction. IACM Expressions 16, 4–9.
Rainest, J.K., Jaffrin, M.Y., Shapiro, A.H., 1974. A computer simulation of
arterial dynamics in the human leg. Journal of Biomechanics 7, 77–91.
Segers, P., Dubois, F., DeWachter, D., Verdonck, P., 1998. Role and
relevancy of a cardiovascular simulator. Cardiovascular Engineering 3,
48–56.
Sherwin, S.J., Formaggia, L., Peiro, J., Franke, V., 2003a. Computational
modelling of 1D blood flow with variable mechanical properties and its
application to the simulation of wave propagation in the human
arterial system. International Journal for Numerical Methods in Fluids
43, 673–700.
Sherwin, S.J., Franke, V., Peiro, J., Parker, K.H., 2003b. One-dimensional
modelling of a vascular network in space–time variables. Journal of
Engineering Mathematics 47, 217–250.
Simon, A.C., Safar, M.E., Levenson, J.A., London, G.M., Levy, B.I.,
Chau, N.P., 1979. An evaluation of large arteries compliance in man.
American Journal of Physiology 237, H550–H554.
Smith, N.P., Pullan, A.J., Hunter, P.J., 2001. An anatomically based
model of transient coronary blood flow in the heart. SIAM Journal on
Applied Mathematics 62, 990–1018.
Stergiopulos, N., Young, D.F., Rogge, T.R., 1992. Computer simulation
of arterial flow with applications to arterial and aortic stenoses.
Journal of Biomechanics 25, 1477–1488.
Viedma, A., Jimenez, C., Marco, V., 1997. Extended Willis circle model to
explain clinical observations in periorbital arterial flow. Journal of
Biomechanics 30, 265–272.
Wang, J.J., Parker, K.H., 2004. Wave propagation in a model of the
arterial circulation. Journal of Biomechanics 37, 457–470.