Embed Size (px)
Citation preview

BLOOD VOL 80, NO 9
The Journal of The American Socieg of Hemutology
NOVEMBER 1, 1992 ~
REVIEW ARTICLE
Molecular Basis of Inherited Human Antithrombin Deficiency
By Morris A. Blajchman, Richard C. Austin, FranGoise Fernandez-Rachubinski, and William P. Sheffield
NTITHROMBIN (AT) deficiency is a heterogeneous A group of disorders that is inherited in an autosomal- dominant fashion. Were it not for the presence of inhibitors of coagulation, like AT, the unopposed presence of acti- vated clotting factors in the circulation would result in thrombus formation within intact blood vessels, often with life-threatening consequences. The most abundant of these inhibitors is a plasma glycoprotein generally known as AT III.1*2 The existence of such an anticoagulant was described initially in 1905 by M~rawi t z ,~ who introduced the term progressive antithrombin activity to describe the ability of human plasma to neutralize thrombin slowly. With the discovery of heparin, and its subsequent clinical use as an anticoagulant, it was soon realized that heparin was effec- tive only in the presence of a plasma component. This activity was referred to as heparin cofactor ac t i~ i ty .~ ,~ A number of other AT activities were described subsequently. In 1954, Seegars et aI6 proposed a numerical classification to bring some order to the description of the various AT activities. AT I represented the ability of a fibrin clot to absorb thrombin and thus to neutralize its activity.6 AT I1 represented the previously described heparin cofactor activ- it^.^,^ AT I11 became the term used to describe the progres- sive antithrombin activity initially described by Morawitz?f6 AT IV represented the thrombin inhibitory activity seen in association with prothrombin activation.6 AT V was desig- nated the AT activity found in the plasma of a patient with hypergammaglobulinemia in which the pathologic globulin inhibited thrombh6s7 AT VI represented the inhibition of thrombin produced by fibrin split products.6,8
With the isolation of the plasma protein that was associ- ated with progressive AT activity, it was realized that this protein (AT 111) was the major plasma anticoagulant and that it also had heparin cofactor activity (AT II).* The availability of large quantities of this protein subsequently provided convincing evidence that the plasma component involved in progressive AT activity and that producing heparin cofactor activity were one and the same.1J A confusion point in the nomenclature was the fact that AT I11 also has been shown to inhibit other activated serine proteases, including factor Xa. Nonetheless, for mainly historical reasons, the term AT I11 continues to be used. Attempts to change the name have been partially success- ful, and in recent years the term antithrombin has come to be used interchangeably with AT IIL9Jo To further confuse
the issue, another protein with both progressive AT and heparin cofactor activities has been described.11J2 This latter moiety has been called heparin cofactor 11, a term used by Tollefsen et all2 to differentiate it from heparin cofactor I (ie, AT 111). In this report, rather than perpetu- ate the continued use of the atavistic term AT 111, we have chosen to use the simpler term antithrombin to describe this plasma glycoprotein exhibiting both progressive AT and heparin cofactor activities.
The existence of a deficiency state involving AT was recognized first by Egebergl3 who described a family, some of whose members suffered from episodes of recurrent venous thromboembolism. The plasma of affected members of this kindred was characterized by the reduction in both progressive AT activity and heparin cofactor activity.13 In fact, this kindred represents the first description ever of an inherited prothrombotic state! Subsequent to this first description of AT deficiency, many other kindreds with classical AT deficiency have been described from diverse geographic locations worldwide, with a reported prevalence of 1:2,000 to 1:5,000.'0J4-16
A decade after the initial description of classical AT deficiency, Sas et all7 described what was believed to be the first report of a kindred with a qualitative AT deficiency caused by the presence in the circulation of a mutant AT protein; AT Budapest. Another decade passed before the specific molecular pathology of an individual with an AT deficiency state was elucidated.18 This was the description of AT-Toyama, by Koide et al,18 who reported the substitu- tion of Arg47 by Cys in this AT molecule. Since this first
From the Canadian Red Cross Society Blood Transfusion Service and the Departments of Pathology and Medicine, McMaster Univer- sity, Hamilton, Ontario, Canada.
Submitted February 12, 1992; accepted June 26,1992. Supported by a Canadian Red Cross Society (CRCS) Blood Services
R&D Fund Grant No. HA-01-92, RC.A. was a recipient of a research fellowship award from the Heart and Stroke Foundation of Canada; F.F.-R. is a recipient of a postdoctoral fellowship from the Medical Research Council (MRC) of Canada; and W.P.S. is a recipient of a scholar award from the CRCSIMileslMRC Scholar Program.
Address reprint requests to M.A. Blajchman, MD, FRCP(C), Room 2N31, McMaster University Health Sciences Centre, 1200 Main St Hamilton, Ontario LSN 325 Canada.
0 1992 by The American Society of Hematology. 0006-4971 /92/80O9-0010$3.00/0
Blood, Vol80, No 9 (November 1). 1992: pp 2159-2171 2159
For personal use only.on April 4, 2019. by guest www.bloodjournal.orgFrom

2160 BLAJCHMAN ET AL
elucidation of a mutant AT molecule, the identification of the molecular defects of many kindreds with AT deficiency has proceeded very rapidly.19-z2 As of March 1992, the specific characterization of AT mutations has been re- ported for more than 100 kindreds. Because some muta- tions have been reported more than once, approximately 40 different specific mutations, resulting in an absent or a pathologic AT gene product, causing clinical AT deficiency, have been reported.
THE SERINE PROTEASE INHIBITOR SUPERFAMILY: THE SERPINS
AT shares structural and functional homology with other members of a superfamily of proteins known as the serine protease inhibitors or s e r p i n ~ . ~ ~ - ~ ~ The degree of homology amongst the serpins suggests that they evolved from a common ancestral molecule about 300 to 600 million years ago.23 The serpins consist of single-chain glycoprotein molecules, of approximately 400 amino acids in length. More than 40 members of the serpin family have been identified in viruses, plants, and in higher animals, with approximately 30% homology at the amino acid level, with each other.10,26 Although most serpins function as inhibitors of serine proteases, not all have retained such function. Some have evolved other roles, such as carriers of lipophilic molecules (thyroxin- and cortisol-binding globulins), or as peptide hormone precursors (angiotensinogen), or have no recognizable function ( o v a l b ~ m i n ) . ~ ~ ~ ~ ~ The noninhibitory serpins are included in the serpin superfamily on the basis of amino acid homology with the inhibitory serpins.
Amino acid sequence alignment, based on the crystal structure of the cleaved form of the archetypal serpin a-1-antitrypsin, indicates that the serpins share a common, highly ordered structure.27 Each of the inhibitory serpins has a similar reactive center (designated Pl-Pl’), which is believed to act as a pseudosubstrate for the target protease. Protease inactivation by inhibitory serpins is by the forma- tion of a 1:l stoichiometric covalent complex between the active site of the serine protease and the reactive center of the serpin. This inactivation process involves at least two separate but interrelated events-hydrolysis of the serpin’s reactive center by its cognate protease followed by covalent complex f o r m a t i ~ n . ~ ~ - ~ ~
The reactive center’s P1 residue, situated toward the amino terminal of the molecule, has been shown to partially confer inhibitor specificity for the inhibitory serpins. For example, AT, which inhibits proteases that cleave next to an arginyl residue, has an arginine at position P1, while a-1-antitrypsin, the primary inhibitor of elastase, has a methionine at this position. The mutant a-l-antitrypsin- Pittsburgh molecule, in which there is a single Met358Arg substitution at the P1 site, converts the usual elastase specificity of a-1-antitrypsin from elastase to that of throm- bin. Thus, a-1-antitrypsin-Pittsburgh was converted from an inhibitor of elastase into a potent inhibitor of thrombin. This mutation manifested clinically as a lethal bleeding d i ~ o r d e r . ~ ~ , ~ ~
Crystallographic studies of serpin structure indicate that the inhibitory serpins exist in a conformation that facilitates
attack by their cognate serine proteases, and that the transition from an intact to a cleaved form is a thermodynam- ically favored event.lO~~~ Recent analysis of the crystal structure of the noninhibitory serpin, ovalbumin, showed that it has a peptide loop analogous to that of the reactive center of the inhibitory serpins. This takes the form of a protruding a-helix, consisting of the reactive center and 10 to 15 amino acid residues amino-terminal to the flanking sequence.34
While the presence of this mobile, exposed reactive loop appears to be common to all members of the serpin family, there is considerable structural diversity elsewhere in the molecule. This diversity likely reflects the various physio- logic roles that these molecules assume, either as an allosteric binding site for heparin in AT or heparin cofactor- 11, or as a peptide donor in angiotensinogen.
PRIMARY PROTEIN AND GENE STRUCTURE OF HUMAN ANTITHROMBIN
Plasma-derived human AT consists of a single-chain glycoprotein of molecular mass of approximately 60 Kd, comprising 432 amino acid r e s i d ~ e s . ~ ~ - ~ ~ There are three disulphide bonds linking cysteine residues 8 and 128,21 and 95, and 247 and 430.35,39 The molecule also contains four oligosaccharide side chains, which comprise approximately 15% of the molecular ~ n a s s . ~ , ~ ~ These are coupled to Asn residues 96, 135, 155, and 192, r e ~ p e c t i v e l y . ~ ~ , ~ ~ ~ ~ ~ An underglycosylated form of plasma-derived AT, which repre- sents approximately 10% of the total plasma concentration of AT, is glycosylated at only three of the four Asn residues, not including Asn 135.44,45
Molecular cloning has allowed the determination of the complete nucleotide sequence of human AT cDNA. Al- most simultaneously, three independent research groups reported the isolation of the cDNA of human AT and the identification of the gene.36-38 The work of these three groups of investigators showed that the mRNA contains an open reading frame of 1,392 nucleotides, of which 96 nucleotides encode the 32-amino acid signal peptide, and 1,296 nucleotides the 432-amino acid form of circulating plasma AT. Subsequent analysis showed that the transcrip- tional start site lies 70 nucleotides upstream from the initiator m e t h i ~ n i n e . ~ ~ , ~ ~ At the 3’ end of the gene, the termination codon and the polyA tail are separated by 87 nucleotides containing a typical polyadenylation signal 54 nucleotides downstream from the termination ~ o d o n . ~ ~ - ~ ~
The human gene consists of seven exons and six interven- ing sequences distributed over approximately 19 kb of the long arm of chromosome 1 (Fig 1).37,48,49 The margins of each of the seven exons comprising the human AT gene are shown in Table 1. In this report, we have chosen to designate exons 3a and 3b as exons 3 and 4, respectively. We believe that numbering the exons 1 to 7 more accurately reflects the structure of this gene than does the nomencla- ture of Bock et al.49
Several restriction fragment length polymorphisms (RFLP) have been described within the human AT gene as follows: in the 5’ untranslated region; in exon 2, the signal peptide; in exon 4, codon 305; in exon 4, codon 395; in
For personal use only.on April 4, 2019. by guest www.bloodjournal.orgFrom

INHERITED ANTITHROMBIN DEFICIENCY 2161
H I k b
V n n i i f i r 1 1
+I : I .I I : I+ exon 1 2 3 4 5 6 7
W (38) (4) (5) 0
e- l frameshift mutation P single base substiion resulting in a stop codon
portion of the gene deleted
Fig 1. Schematic diagram indicating the site of reported AT gene mutations associated with type 1 AT deficiency. The numbers in parentheses refer to the exon numbers used by Bock et aLQ
intervening sequence 5, position 160; and in exon 6, codon 359.22,373-52 Recently, we identified two previously unre- ported repeat sequences in intervening sequence 5 of the gene. These repeat sequences are likely to be similar to the previously described variable number tandem repeat (VNTR) sequences that have been discovered in the human g e n ~ m e . ~ ~ ” ~ Using the polymerase chain reaction (PCR) method, we hope to detect various length polymor- phisms related to these VNTRs to perform linkage analyses in the various kindreds that have been reported to have identical mutations. Such data will likely provide important information about whether the so-called hot spots noted in the human AT gene are real or related to a founder effect.56
The 5’ upstream region of the human AT gene is relatively unexplored. To date, only two studies have addressed the question of genetic control of AT gene expression. The upstream region of the AT gene lacks a discernible TATA However, it has been reported to contain an enhancer region, identified on the basis of homology to the Jk-Ck enhancer of the Ig K chain gene.47 These studies indicate that this putative enhancer region is sensitive to liver-specific cellular elements in regulating AT gene expre~s ion .~~ This putative enhancer region lies be- tween nucleotides -173 and -129 relative to the start codon. The second reported study examined the binding of nuclear proteins to upstream DNA sequences.57 Such investigations provided evidence that an as-yet-unidentified
Table 1. Margins of the Seven Exons Comprising the Human AT Gene
No. of Amino Exon 5’-Margin 3‘-Margin Acid Residues
1
2 codon -18 3 (3A)* codon 105 4 (38) codon 177 5 (4) codon 223 6 (5) codon 354 7 (6) codon 375
70 bp 5’ to the start codon
codon -19 14
codon 104 122 codon 176 72 codon 222 46 codon 353 131 codon 374 21 84 bp 3’ to the 58
stop codon ~ ~~
*The numbers in parentheses refer to the exon numbers used by Bock et al.49
protein binds to a region between nucleotides -89 and -68.57 If this region of the AT gene were indeed critical to the control of human AT gene expression, then its deletion from reporter constructs should decrease or abolish pro- moter activity. However, such experiments have yet to be reported.
A number of independent studies have shown that the human AT gene is localized to the long arm of chromosome 1.58-61 Linkage analysis had previously shown that the human AT gene was linked to the red blood cell D u Q gene.58 More recent studies have clearly established the localization of the human AT gene to chromosome 1. This was accomplished both by observing AT deficiency in individuals in a kindred with a finite chromosomal deletion in the regions lq22 to lq25, and by precise mapping of partial AT cDNA clones to the region lq23 to 1q25.58-61
MECHANISM OF ACTION OF ANTITHROMBIN
AT has been shown to be the primary inhibitor of the various activated serine protease clotting factors, including thrombin, IXa, Xa, XIa, XIIa, kallekrein, plasmin, uroki- nase, and t ryp~in .1 ,2 ,~~-~~ It is likely that the most important of these physiologically is the inhibition of thrombin, which is relatively slow under physiologic conditions, but greatly accelerated in the presence of h e ~ a r i n . ~ ~ - ~ ~ As indicated above, protease inactivation by AT involves
the formation of a 1:l molar complex between the active site serine of the protease and the reactive center of AT. The reactive center Arg393-Ser394 of AT is situated toward the carboxy-terminal domain of the molecule.10.30,76.77 When thrombin interacts with AT, the two molecules form a covalent, stable, stoichiometric complex that is rapidly removed from the c i r c ~ l a t i o n . ~ ~ , ~ ~ The formation of this stable covalent complex initially involves the cleavage of the Arg393-Ser394 peptide bond by the serine active site of thrombin and then the association between the serine at the active site of thrombin and the arginine (Pl) of the cleaved AT by the formation of a covalent ester linkage.30~78.80,81 The margins of the thrombin-interactive domain of AT have yet to be defined precisely. However, some naturally occurring AT mutants that show impaired inhibitory activity have mutations adjacent to the reactive center. These natural mutations suggest that the margins of the reactive center of the human AT molecule spans, at least, from residues 382
The inhibition of thrombin, as well as other serine proteases of the coagulation pathway, by AT is relatively slow in the absence of heparin but can be enhanced more than a thousandfold in its p r e ~ e n c e . ~ ~ , ~ ~ This enhancement is mediated by the binding of heparin to AT, resulting in a conformational change in the inhibitor, thought to promote attack by the protease.83 Thus, heparin binding to AT has been shown to activate Lys 236 such that it enhances its ability to undergo chemical modification. Heparin binding has also been shown to alter the overall fluorescence spectrum of AT, suggesting a conformational change as the result of such i n t e r a ~ t i o n . ~ ~
The heparin-binding domain of AT appears to consist of two regions, encompassing amino acids 41 to 49 and 107 to
to 407.19,49,82
For personal use only.on April 4, 2019. by guest www.bloodjournal.orgFrom

2162 BLAJCHMAN ET AL
156, respe~tively. '~.~ Both regions consist of clusters of basic amino acids localized toward the amino-terminus of the molecule. Two lines of evidence indicate that the region encompassing amino acid residues 41 to 49 is involved in heparin binding. Biochemical experiments have shown that the chemical modification of Trp49 results in impaired heparin binding to AT.85 This modification also abolishes the heparin-catalyzed inhibition of thrombin by modified AT.85 The second line of evidence implicating the 41-49 region involves experiments of nature. The study of affected individuals has shown that mutations at Pro41 and Arg47 interfere directly or indirectly with heparin binding to AT.1s,86-97 The second heparin-binding region has been proposed to consist of the positively charged amino acid residues Lys 107, Lys 114, Lys 125, Arg129, Arg 132, and Lys 133 at the surface of the AT m o l e ~ u l e . ~ ~ ~ ~ ~ Evidence in support of this hypothesis was provided when the chemical modification of the Lys and Arg residues encompassing amino acids 107 to 156 resulted in an AT moiety with impaired heparin cofactor a ~ t i v i t y . ~ ~ , ~ ~ Additional evidence that this region might be important for heparin binding consists of data that indicate that heparin binds to a peptide comprising amino acid residues 114 to 156.98 Moreover, polyclonal antibodies with specificity toward the synthetic peptide comprising residues 124 to 145 block the binding of heparin to AT.99 Another piece of evidence implicating this region, as involved in heparin binding, is the recent report of a naturally occurring mutation located within this second heparin-binding region, at Arg 129. In AT-Geneva, there is an Argl29Gln substitution.lOOJO1
Interestingly, the analysis of a three-dimensional struc- ture model of AT (based on the crystal structure of a-1 antitrypsin) puts the two heparin-binding regions adjacent to each 0 t h e r . 2 ~ J ~ ~ Thus, these two putative heparin- binding regions are adjacent to each other when the molecule assumes its three-dimensional format. Moreover, together these two regions provide a clearly defined posi- tively charged domain suitable for heparin binding to AT. However, the relative contribution of each of these two heparin-binding regions to the presumed heparin-binding domain of the intact molecule has not been established. In this context, it has been shown recently that the disulphide bond between Cys8 and Cys128 (located within the second heparin-binding domain) is required for the integrity of heparin binding to intact AT.'" It has been proposed that the integrity of this disulphide linkage is required for Arg47 to be in a position to facilitate favorable cooperativity for heparin binding with Arg129.1°1 Thus, it is likely that the two heparin-binding regions 41-49 and 107-156 together cooperatively constitute one heparin-binding domain when plasma AT assumes its tertiary structure.
CLASSIFICATION OF ANTITHROMBIN DEFICIENCY
In attempting a classification of AT deficiency, a number of difficulties arise. Some of these are listed in Table 2. First is the absence of a decision by an appropriate international committee concerning the name of the thrombin inhibitor under discussion. Various opinions range from antithrom- bin, antithrombin 111, heparin cofactor I, serpin I, etc. As
Table 2. Problems With the Classification of AT Deficiency
1. The name of the progressive thrombin inhibitor (AT 111 v AT). 2. Multiple classification schemes. 3. Nomenclature to describe specific defects(top0nyms v mo-
4. Homozygosity v heterozygosity. 5. Repeat reporting of the same molecular defect. 6. Numbering of the exons of the human AT gene.
lecular defect).
indicated earlier, we would recommend the term antithrom- bin.
A second difficulty occurs because different classification schemes have been proposed to describe the various types of AT deficiency state. Some investigators prefer to classify AT deficiency into only two types,21,22 whereas others have classified AT deficiency into up to five different types.2O In this review, we propose a classification based on the known, or presumed, site of the molecular pathology of the AT gene and its resultant effect on the circulating AT molecule. In our proposed classification, AT deficiency is divided into four types, based on the site of the mutation (see Table 3).
Another problem with the classification of AT deficiency is the nomenclature used for the past 2 decades to describe the various types of AT deficiency. In general, the various investigators have used the name of the city where the propositus resided (ie, a toponym). The use of toponyms may have been necessary before the capability of elucidat- ing the specific molecular pathology existed. Presently, it is relatively easy to characterize a specific mutation. There- fore, the use of toponyms should be discouraged. We would suggest that all newly characterized mutations be desig- nated by the specific mutation. For example, AT-Toyama, with a substitution of the Arg47 residue by Cys, should be referred to as AT-Arg47Cy~.'~ Thus, the repetitive report- ing of the same molecular defect might be discouraged. In this regard, the AT-Toyama defect, first described in 1984, has been reported nine different times from different geographic locations. Thus, the Arg47Cys mutation has been reported as AT-Toyama, -Tours, -Alger, -Amiens, -Barcelona-2, -Paris-1, -Paris-2, -Padua-2, and -Kumamo- to.18,s6-92 While it is of considerable interest that the same mutation occurs in different parts of the world, suggesting a mutational hot it is possible that many of these kindreds, particularly the European ones, derive from the same founder.
Another problem with present classifications is that there is no indication of the zygosity of the mutation in a given kindred. For example, the clinical or phenotypic expression of a particular defect is, in part, dependent on the zygosity; ie, whether the individual is homozygous or heterozygous for the disorder. While most individuals with AT deficiency
Table 3. Proposed Classification of Inherited AT Deficiency
Type 1 : AT gene product absent from the plasma. Type 2: AT gene defect affecting the thrombin-binding domain of the
Type 3: AT gene defect affecting the heparin-binding domain of the
Type 4: None of the above (miscellaneous group).
molecule.
molecule.
For personal use only.on April 4, 2019. by guest www.bloodjournal.orgFrom

INHERITED ANTITHROMBIN DEFICIENCY 2163
have been reported to have a heterozygous defect, there have been reports of homozygous individuals and even some with doubly heterozygous defects.ts~s7J04~to5 Reports of AT deficiency should have the zygosity clearly indicated as this has relevance to the clinical management (see below).
INHERITED ANTITHROMBIN DEFICIENCY
The prevalence of AT deficiency in individuals with symptomatic thrombotic disease is approximately 5%.'06 In the normal population, AT deficiency has been estimated to affect from 1 to 2,000 to 1 to 5,000 individual^.'^-'^ However, it has been reported recently that the incidence of AT deficiency may be higher than previously estimated.'" The prevalence of AT deficiency in normal individuals has been estimated, in a Scottish study, to be 0.4% or 1 in 25O.lo7 Sixteen of over 4,000 blood donors, ages 18 to 65 (2,611 male and 1,578 female), had persistent AT deficiency.Io7 One had type 1 deficiency, 2 had type 2 deficiency, and 13 had a type 3 deficiency (as defined in Table 3). These findings suggest a prevalence of 1 in 4,200 for type 1 AT deficiency; a 1 in 2,100 prevalence for a type 2 deficiency; and a prevalence of 1 in 350 for type 3 deficiency. Further studies are required to define more precisely the prevalence of AT deficiency, which may vary from one population to another.
Type 1 AT deficiency is character- ized by a decrease of both antigenic and functional levels to approximately 50% of those observed in normal individu- als. For the purposes of this review, we define type 1 AT deficiency as being a quantitative defect only. We specify that no gene product of the affected AT allele should be detectable in the plasma of an affected type 1 individual. Table 4 lists some of the possible causes of a type 1 AT deficiency. Table 5 summarizes the elucidated mutations that have been associated with type 1 AT deficiency. There have been two reports where a complete AT gene deletion was associated with type 1 AT deficiency.60J08 In one of these kindreds, the AT deficiency was associated with a visible deletion of a portion of the long arm of chromosome 1.60 In our laboratory, we have recently characterized a kindred with a partial, but extensive, gene deletion of one AT allele.84 All genetic information upstream of a point between exons 2 and 3 is deleted. We have recently established the exact location of the breakpoint to be 480 nucleotides upstream to the 5' boundary of exon 3.1a9 There have been reports of 11 frameshift mutations associated with type 1 AT deficiency, resulting from either an insertion of one nucleotide or a deletion of one to four nucleo-
Type 1 ATdeficiency.
Table 4. Putative Causes for Inherited Type 1 AT Deficiency, Defined as a Quantitative Deficiency Without Evidence in the Plasma of a
Gene Product From the Affected Allele
1. A complete gene deletion. 2. A partial gene deletion. 3. A mutation causing a transcription defect. 4. A mutation causing a translation defect. 5. A mutation causing a protein secretion defect. 6. Combinations of the above.
t i d e ~ . ~ l ~ - ' l ~ In addition, there have been several reports of kindreds with a type 1 deficiency resulting from a single C to T substitution in the first base of codon 129, mutating an Arg (CGA) codon to a stop (TGA) ~ o d o n . " ~ , ~ ~ ~ The details of these mutations are summarized in Fig 1.
The molecular pathology of most kindreds with type 1 AT deficiency has not yet been elucidated. Of 16 kindreds examined by Bock and Pro~hownik,"~ only one was re- ported to be completely lacking in one AT allele. All others had RFLP patterns indistinguishable from normal individu- als. Such analyses suggests that the molecular defects in most kindreds with AT deficiency are caused by point mutations at key positions within the AT gene. The poten- tial causes of such mutations are listed in Table 4. The advent of direct sequencing of PCR-amplified portions of genomic DNA from affected individuals should make it possible to characterize various other mutations leading to type 1 AT deficiency.
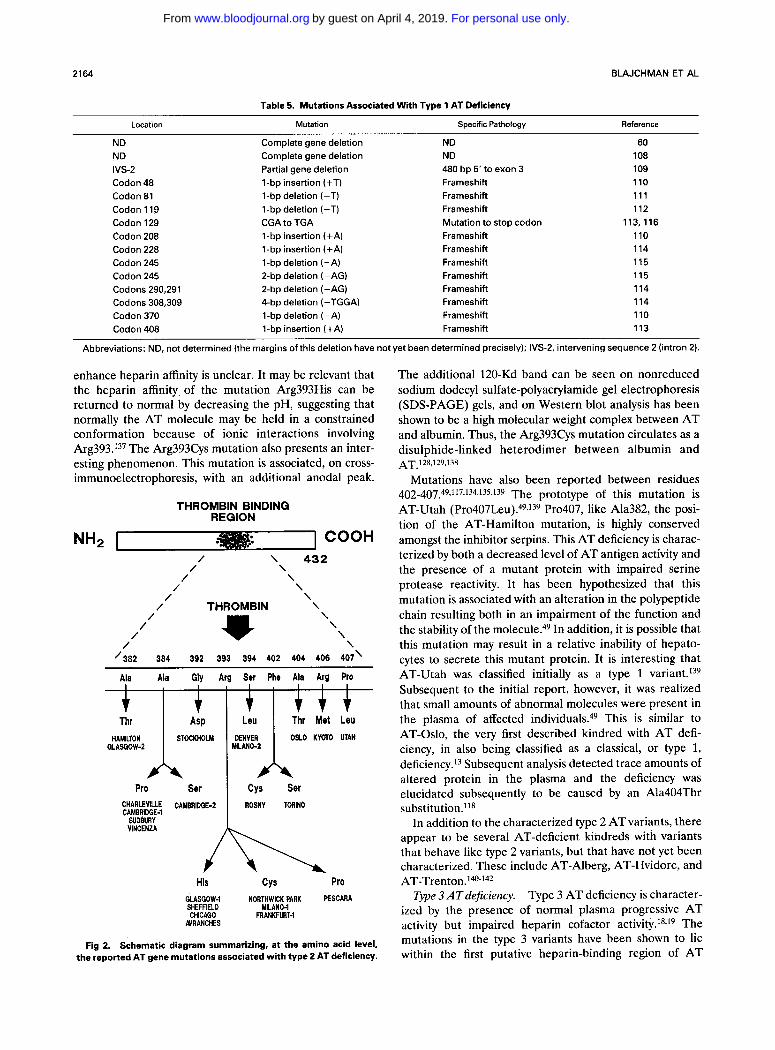
Type 2 AT deficiency is character- ized by a mutation within the AT gene resulting in a circulating protein with impaired serine protease inhibitory activity. All type 2 mutations characterized to date have been single nucleotide substitutions altering codons be- tween amino acid residues 382 and 407, the region adjacent to the AT reactive center Arg393-Ser394. The reported type 2 AT variants are summarized in Fig 2. While there have been reports of at least 24 kindreds from diverse geographic locations having type 2 AT deficiency, there have been only 14 specific mutations identified.49is2,90~"8-'35 Patients with type 2 AT deficiency have normal plasma AT antigen 1e~els. l~ However, they have impaired serine pro- tease inhibitory activity both in the presence and absence of heparin. The first reported elucidation of a type 2 deficiency was that of A T - D e n ~ e r . ~ ~ ~ . ' ~ ~ This mutation was shown to be a Ser394Leu substitution, which rendered the AT molecule incapable of complexing with its cognate pro- tease, t h r ~ m b i n . ~ ~ ~ J ~ ~
The region amino-terminal to the reactive center has been characterized by a number of mutations. The first of these reported was AT-Hamilton, consisting of an Ala382Thr substitution.82 Unlike AT-Denver, the AT- Hamilton molecule is capable of being a substrate for thrombin and factor Xa, but is incapable of inhibiting either protease.28 Two molecular defects at position 384 have been described; Ala 384 Pro and Ala 384 Ser.90J20-123 Both of these mutant ATs behave similarly to AT-Hamilton in that they can be substrates for their cognate proteases, but do not form inhibitory complexes with them.z2J22J36
Recently, we described an interesting P2 mutation. A Gly392Asp substitution was found to render the mutant protein, termed AT-Stockholm, devoid of thrombin- inhibiting activity. Evidence provided by this mutation suggests that the P2 residue may importantly influence the reactive center of AT.124
Three AT mutants with substitutions at Arg393 have been described. These include Arg393His, Arg393Cys, and A r g 3 9 3 P r 0 . ' ~ ~ - ~ ~ ~ These mutant proteins are of considerable interest because they are associated with increased heparin affinity.'" The mechanism whereby these substitutions
Type 2ATdeficiency.
For personal use only.on April 4, 2019. by guest www.bloodjournal.orgFrom
2164 BLAJCHMAN ET AL
t
Table 5. Mutations Associated With Type 1 AT Deficiency
t l t l t t t
Location Mutation Specific Pathology Reference
G;g;!2k2LM Pro Ser
ND ND IVS-2 Codon 48 Codon 81 Codon 119 Codon 129 Codon 208 Codon 228 Codon 245 Codon 245 Codons 290,291 Codons 308,309 Codon 370 Codon 408
Thr Met Leu MI LA NO-2 D:;:A OSLO KYOTO UTAH
Cys Ser
Complete gene deletion Complete gene deletion Partial gene deletion 1-bp insertion (+T) 1-bp deletion (-T) 1-bp deletion (-T) CGA to TGA 1-bp insertion (+A) 1-bp insertion (+A) 1-bp deletion (-A) 2-bp deletion (FAG) 2-bp deletion (-AG) 4-bp deletion (-TGGA) 1-bp deletion (-A) 1-bp insertion (+A)
ND ND 480 bp 5' to exon 3 Frameshift Frameshift Frameshift Mutation to stop codon Frameshift Frameshift Frameshift Frameshift Frameshift Frameshift Frameshift Frameshift
60 108 109 110 111 112
113,116 110 114 115 115 114 114 110 113
~~ ~
Abbreviations: ND, not determined (the margins of this deletion have not yet been determined precisely); IVS-2, intervening sequence 2 (intron 2).
enhance heparin affinity is unclear. It may be relevant that the heparin affinity of the mutation Arg393His can be returned to normal by decreasing the pH, suggesting that normally the AT molecule may be held in a constrained conformation because of ionic interactions involving Arg393.137 The Arg393Cys mutation also presents an inter- esting phenomenon. This mutation is associated, on cross- immunoelectrophoresis, with an additional anodal peak.
THROMBIN BINDING REGION
] COOH NH2 I / \ 432
/ \ / \
/ \ /- \
/ THROMBIN \ \ \ \ * \
/ /
/ /
'302 304 392 393 394 402 404 406 401'
Ala Ala Gly Arg Ser Phe Ala Arg Pro
CAMERIDGE-1 SUDBURY VUJCENZA
His CYS Pro GLASGOW-1 NORTHWICK PARK PESCARA SHE F F I E L D
NRANCHES
MILAN04 CHICAGO FRANKFURT-1
Fig 2. Schematic diagram summarizing, at the amino acid level, the reported AT gene mutations associated with type 2 AT deficiency.
The additional 120-Kd band can be seen on nonreduced sodium dodecyl sulfate-polyacrylamide gel electrophoresis (SDS-PAGE) gels, and on Western blot analysis has been shown to be a high molecular weight complex between AT and albumin. Thus, the Arg393Cys mutation circulates as a disulphide-linked heterodimer between albumin and
Mutations have also been reported between residues 402-407.49J17J34J35J39 The prototype of this mutation is AT-Utah (Pr0407Leu).~~>l~~ Pro407, like Ala382, the posi- tion of the AT-Hamilton mutation, is highly conserved amongst the inhibitor serpins. This AT deficiency is charac- terized by both a decreased level of AT antigen activity and the presence of a mutant protein with impaired serine protease reactivity. It has been hypothesized that this mutation is associated with an alteration in the polypeptide chain resulting both in an impairment of the function and the stability of the m0lecule.4~ In addition, it is possible that this mutation may result in a relative inability of hepato- cytes to secrete this mutant protein. It is interesting that AT-Utah was classified initially as a type 1 variant.139 Subsequent to the initial report, however, it was realized that small amounts of abnormal molecules were present in the plasma of affected individual^.^^ This is similar to AT-Oslo, the very first described kindred with AT defi- ciency, in also being classified as a classical, or type 1, deficiency.l3 Subsequent analysis detected trace amounts of altered protein in the plasma and the deficiency was elucidated subsequently to be caused by an Ala404Thr substitution.118
In addition to the characterized type 2 AT variants, there appear to be several AT-deficient kindreds with variants that behave like type 2 variants, but that have not yet been characterized. These include AT-Alberg, AT-Hvidore, and AT-Trent~n ." '@~~~
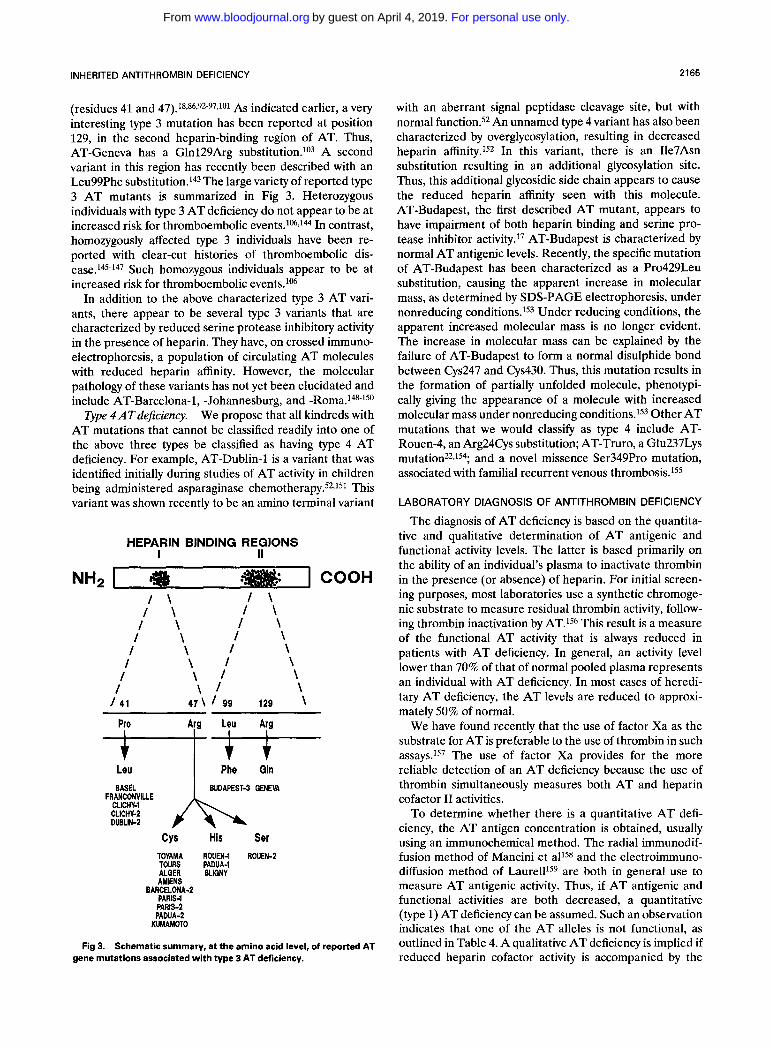
Type 3 AT deficiency is character- ized by the presence of normal plasma progressive AT activity but impaired heparin cofactor a~tivity. '~. '~ The mutations in the type 3 variants have been shown to lie within the first putative heparin-binding region of AT
AT.128,129,138
Type 3 ATdeficiency.
For personal use only.on April 4, 2019. by guest www.bloodjournal.orgFrom
INHERITED ANTITHROMBIN DEFICIENCY 2165
(residues 41 and 47).18,86392-97,101 As indicated earlier, a very interesting type 3 mutation has been reported at position 129, in the second heparin-binding region of AT. Thus, AT-Geneva has a Glnl29Arg substitution.lo3 A second variant in this region has recently been described with an Leu99Phe substitution.143 The large variety of reported type 3 AT mutants is summarized in Fig 3. Heterozygous individuals with type 3 AT deficiency do not appear to be at increased risk for thromboembolic events.lM,14 In contrast, homozygously affected type 3 individuals have been re- ported with clear-cut histories of thromboembolic dis- ease.145-147 Such homozygous individuals appear to be at increased risk for thromboembolic events.lo6
In addition to the above characterized type 3 AT vari- ants, there appear to be several type 3 variants that are characterized by reduced serine protease inhibitory activity in the presence of heparin. They have, on crossed immuno- electrophoresis, a population of circulating AT molecules with reduced heparin affinity. However, the molecular pathology of these variants has not yet been elucidated and include AT-Barcelona-1, -Johannesburg, and -Roma.148-150
We propose that all kindreds with AT mutations that cannot be classified readily into one of the above three types be classified as having type 4 AT deficiency. For example, AT-Dublin-1 is a variant that was identified initially during studies of AT activity in children being administered asparaginase c h e m ~ t h e r a p y . ~ ~ , ~ ~ ~ This variant was shown recently to be an amino terminal variant
Type 4ATdeJiciency.
HEPARIN BINDING REGIONS I II
\ I \ \ I \ \ I \ \ I \ \ I \
\ \
\ f
\ \ f \ f
4 7 \ f 99 129 \ Pro Arg Leu Arg I ! -
I V V
FR ANCONVILLE CLICHW CLICHlc2 DUBLK?
Cys His Ser TOYAMA ROUEN-1 ROUEN-2 TOURS PADUA-1 ALGER BLIGNY AMIENS
BARCELONA-? PARIS-1 PARIS-2 PADUA-2
KUMAMOTO
Fig 3. Schematic summary, at the amino acid level, of reported AT gene mutations associated with type 3 AT deficiency.
with an aberrant signal peptidase cleavage site, but with normal function.52 An unnamed type 4 variant has also been characterized by overglycosylation, resulting in decreased heparin affinity.152 In this variant, there is an Ile7Asn substitution resulting in an additional glycosylation site. Thus, this additional glycosidic side chain appears to cause the reduced heparin affinity seen with this molecule. AT-Budapest, the first described AT mutant, appears to have impairment of both heparin binding and serine pro- tease inhibitor activity.17 AT-Budapest is characterized by normal AT antigenic levels. Recently, the specific mutation of AT-Budapest has been characterized as a Pro429Leu substitution, causing the apparent increase in molecular mass, as determined by SDS-PAGE electrophoresis, under nonreducing ~0nd i t ions . l~~ Under reducing conditions, the apparent increased molecular mass is no longer evident. The increase in molecular mass can be explained by the failure of AT-Budapest to form a normal disulphide bond between Cys247 and Cys430. Thus, this mutation results in the formation of partially unfolded molecule, phenotypi- cally giving the appearance of a molecule with increased molecular mass under nonreducing conditions.153 Other AT mutations that we would classify as type 4 include AT- Rouen-4, an Arg24Cys substitution; AT-Truro, a Glu237Lys m u t a t i ~ n ~ ~ , ~ ~ ~ ; and a novel missence Ser349Pro mutation, associated with familial recurrent venous thrombosis.lS5
LABORATORY DIAGNOSIS OF ANTITHROMBIN DEFICIENCY
The diagnosis of AT deficiency is based on the quantita- tive and qualitative determination of AT antigenic and functional activity levels. The latter is based primarily on the ability of an individual's plasma to inactivate thrombin in the presence (or absence) of heparin. For initial screen- ing purposes, most laboratories use a synthetic chromoge- nic substrate to measure residual thrombin activity, follow- ing thrombin inactivation by AT.lS6 This result is a measure of the functional AT activity that is always reduced in patients with AT deficiency. In general, an activity level lower than 70% of that of normal pooled plasma represents an individual with AT deficiency. In most cases of heredi- tary AT deficiency, the AT levels are reduced to approxi- mately 50% of normal.
We have found recently that the use of factor Xa as the substrate for AT is preferable to the use of thrombin in such assays.lS7 The use of factor Xa provides for the more reliable detection of an AT deficiency because the use of thrombin simultaneously measures both AT and heparin cofactor I1 activities.
To determine whether there is a quantitative AT defi- ciency, the AT antigen concentration is obtained, usually using an immunochemical method. The radial immunodif- fusion method of Mancini et alls8 and the electroimmuno- diffusion method of L a ~ r e l l ' ~ ~ are both in general use to measure AT antigenic activity. Thus, if AT antigenic and functional activities are both decreased, a quantitative (type 1) AT deficiency can be assumed. Such an observation indicates that one of the AT alleles is not functional, as outlined in Table 4. A qualitative AT deficiency is implied if reduced heparin cofactor activity is accompanied by the
For personal use only.on April 4, 2019. by guest www.bloodjournal.orgFrom
2166 BLAJCHMAN ET AL
presence of normal antigenic activity. Determination of progressive thrombin and/or factor Xa inactivation, as well as the performance of crossed immunoelectrophoresis with or without heparin, are required to identify the functional domain of the impaired AT molecule.160 For example, a sample with decreased progressive thrombin and/or factor Xa inactivation together with a normal crossed immunoelec- trophoresis pattern, both in the presence or absence of heparin, suggests an abnormality at or near the reactive center of the molecule. However, a sample with normal progressive inactivation of thrombin and/or factor Xa but with an abnormal crossed immunoelectrophoresis pattern, in the presence of heparin, is presumed to have an abnormal heparin-binding region.
To further characterize AT variants at the molecular level, the determination of the amino acid sequence and/or the DNA sequence is desirable. Development of molecular techniques such as PCR have enabled the rapid elucidation of the molecular defects involved in patients with AT deficiency.l6l
reported in such studies, is overestimated. This is because the clinical diagnosis of venous thromboembolism is usually not confirmed with objective testing. Thus, many subjects with clinically suspected deep venous thrombosis do not actually have deep venous thrombosis.162 Furthermore, in most of the reports of thromboembolism, in AT-deficient individuals, it is not clear whether the diagnosis of venous thrombosis was made without knowledge of the AT status of the study subjects. Such knowledge has the potential to cause diagnostic suspicion bias, which could result in the overestimation of the prevalence of venous thrombosis in such a population.
We have recently performed a cross-sectional study to estimate the prevalence of objectively proven thrombotic events in patients with AT deficiency.163 The large kindred chosen had a type 2 AT deficiency (AT-Hamilton).8Z Sixty-seven subjects, constituting the majority (83%) of the available family members, were evaluated. Six of 31 (19.4%) AT-deficient subjects had evidence of one or more throm- botic events. None of the 36 nondeficient subjects had evidence of a thrombotic event. The initial thrombotic episode, in five of the six subjects who had such an episode, had occurred in association with predisposing f a ~ t 0 r s . l ~ ~ On
TREATMENT OF PATIENTS WITH ANTITHROMBIN DEFICIENCY
Hereditary AT deficiency is a well-recognized cause of thrombophilia,16J06 and individuals with this disorder are at increased risk to develop venous thrombosis and are often treated with anticoagulants indefinitely. Therefore, the management of asymptomatic AT-deficient individuals is problematic, because data concerning the relative risks and benefits of lifelong anticoagulant, or replacement therapy, are lacking. This is largely because reliable estimates of the prevalence of venous thrombosis in AT-deficient individu- als are not yet available. Based on the available literature, the reported prevalence of venous thrombosis in AT deficiency subjects is approximately 50%.'06 In our opinion, it is likely that the true prevalence of venous thrombosis,
the basis of this study, we have postulated that the inci- dence of thrombotic events in people with AT deficiency may be significantly lower than heretofore estimated and that they occur predominantly in association with predispos- ing factors. Thus, we believe that lifelong prophylaxis with anticoagulants, or replacement, is probably not warranted in asymptomatic AT-deficient individuals, and that use of prophylaxis in such individuals be limited to high-risk p e r i o d ~ . ~ ~ ~ J ~ In contrast, patients with established deep venous thrombosis should be treated with heparin and oral anticoagulants, with the length of treatment dependent on the clinical setting. In some situations, AT replacement is probably indicated; however, at this time there are insuffi-
HEPARIN BINDING REGIONS I II
THROMBIN BINDING REGION
e I COOH NH2 I I \ I \ / 432
I \ I \ I \ I \ / \
/ / \
I \ / \ / THROMBIN \
/ \
/ \
I \ \ \
I \ I
\ I \ I
\ / I \ I
I \ I \
\ /
4I\ I 99 129 237 349 '382 301 392 393 394 402 404 400 407' 429
Atg 1;
A I 9 AI S; P[ i 9 ; ; 9 7 7 9 A m Cys Phr Gln Lyr Pro Thr Asp Leu Thr Met Leu Leu
-- - I 24 1 4 t --
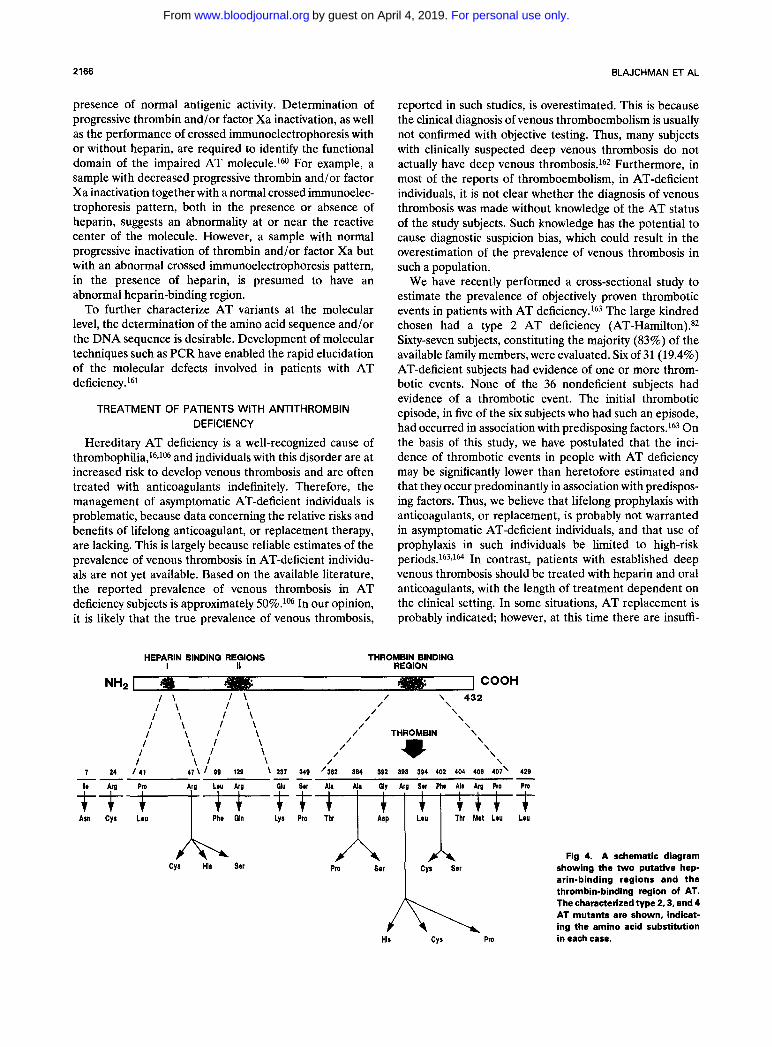
Fig 4. A schematic diagram showing the two putative hep- arin-binding regions and the thrombin-binding region of AT. The characterized type 2,3, and 4 AT mutants are shown, indicat- ing the amino acid substitution in each case.
For personal use only.on April 4, 2019. by guest www.bloodjournal.orgFrom

INHERITED ANTITHROMBIN DEFICIENCY 2167
cient data available to evaluate the value of AT replace- ment. Recommendations for the treatment of AT defi- ciency have recently been published and should be consulted for further details.164
Patients with type 3 AT deficiency are considered not to be at risk for thromboembolic events, except if they are homozygous or double heterozygotes.lwJo6J4 Recently Vidaud et allw reported a kindred with double heterozy- gous AT deficiency in two brothers. In one allele the mutation appeared to be a type 3 deficiency, while in the other there was a type 1 deficiency. Both brothers had evidence of recurrent thromboembolism. The mother of the two affected brothers had a typical type 3 AT deficiency phenotype and was asymptomatic; the father, who mani- fested several thromboembolic episodes, appeared to have a type 1 AT deficiency.lo4
There has been only a single report of a kindred with homozygous type 1 AT deficiency.Io5 In this kindred, two homozygously affected offspring died within the first 3
REFER 1. Abilgaard U: Purification of two progressive antithrombins of
human plasma. Scand J Clin Lab Invest 19190,1967 2. Rosenberg RD, Damus PS: The purification and mechanism
of action of human antithrombin-heparin cofactor. J Biol Chem 248:6490,1973
3. Morawitz P: Die Chemie der Blutgerinnung. Ergeb Physiol 4307,1905
4. Brinkhous KM, Smith HP, Warner ED, Seegers WH: The inhibition of blood clotting: An unidentified substance which acts in conjunction with heparin to prevent the conversion of prothrom- bin into thrombin. Am J Physiol 125:683, 1939
5. Howell WH, Holt E: Two new factors in blood coagulation: Heparin and oro-antithrombin. Am J Physiol47:328,1918
6. Seegers WH, Johnson JF, Fall C An antithrombin reaction related to prothrombin activation. Am J Physiol 176:97,1954
7. Loeliger A, Hers JFP: Chronic antithrombinaemia (antithrom- bin V) with haemorrhagic diathesis in a case of rheumatoid arthritis with hypergammaglobulinemia. Thromb Diath Haemorrh 1:499,1957
8. Niewiarowski S, Kowalski E: Un nouvel anticoagulant derivC du fibrinogkne. Rev HCmatol13:320,1958
9. Rosenberg RD: Biochemistry of heparin antithrombin inter- actions, and the physiologic role of this natural anticoagulant mechanism. Am J Med 87:28,1989 (suppl3B)
10. Carrell RW, Christey PB, Boswell DR: Serpins: Antithrom- bin and other inhibitors of coagulation and fibrinolysis. Evidence from amino acid sequences, in Vertsraete M, Vermylen J, Lijnen R, Arnout J (eds): Thrombosis and Haemostasis. Leuven, Belgium, Leuven University, 1987, p 1
11. Briginshaw GF, Shanberge JN: Identification of two distinct heparin cofactors in human plasma: 1. Separation and partial purification. Arch Biochem Biophys 161:683,1974
12. Tollefsen DM, Majerus DW, Blank M K Heparin cofactor 11. Purification and properties of a heparin-dependent inhibition of thrombin in human plasma. J Biol Chem 257:2162,1982
13. Egeberg 0: Inherited antithrombin deficiency causing throm- bophilia. Thromb Diath Haemorrh 13316,1965
14. Winter JH, Fenech A, Ridley W, Bennett B, Cumming AM, Mackie M, Douglas AS: Familial antithrombin Ill deficiency. Quart J Med 51:373,1982
weeks of life. The data from this consanguineous family indicate that homozygous type 1 and probably type 2 AT deficiency is incompatible with long life, except if lifelong replacement therapy were to be administered, as has been reported with homozygous protein C deficiency.165
SUMMARY
Figures 1 and 4 summarize the various AT mutations that have been described. The molecular elucidation, over the past decade, of the various AT deficiency types has pro- vided important new insights into functional-structural relationships of AT. This knowledge, together with data provided by monoclonal antibodies and x-ray crystallo- graphic studies of related molecules, has provided impor- tant new insights as to how the AT molecule functions in vivo. Finally, such knowledge might, in the foreseeable future, lead to the production of AT molecules that are specifically genetically engineered to be of use in a variety of clinical situations.
IENCES
15. Abilgaard U: Antithrombin and related inhibitors of coagu- lation, in Poller L (ed): Recent Advances in Blood Coagulation. Edinburgh, Scotland, Churchill Livingstone, 1981, p 151
16. Thaler E, Lechner K Antithrombin 111 deficiency and thromboembolism. Clin Haematol10:369,1981
17. Sas G, Blasko G, Banhegyi D, Jako J, Palos L A Abnormal antithrombin 111 (antithrombin 111 “Budapest”) as a cause of familial thrombophilia. Thromb Diath Haemorrh 32105,1974
18. Koide T, Odani S, Takahashi K, Ono T, Sakuragama N Antithrombin-I11 Toyama: Replacement of arginine-47 by cysteine in hereditary abnormal antithrombin that lacks heparin-binding ability. Proc Natl Acad Sci USA 81:289,1984
19. Manson HE, Austin RC, Fernandez-Rachubiski F, Rachu- binski RA, Blajchman MA: The molecular pathology of inherited human antithrombin I11 deficiency. Transfusion Med Rev 3:264, 1989
20. Prochownik E V Molecular genetics of inherited antithrom- bin 111 deficiencies. Am J Med 87:15S, 1989 (suppl3B)
21. Sas G: Classification of antithrombin 111 deficiencies. Thromb Haemost 60530,1989
22. Lane DA, Ireland H, Olds RJ, Thein SL, Perry DJ, Aiach M: Antithrombin 111: A database of mutations. Thromb Haemost 66:657, 1991
23. Hunt LT, Dayoff MO: A surprising new protein super-family containing ovalbumin, antithrombin 111, and alpha 1-proteinase inhibitor. Biochem Biophys Res Commun 95:864,1980
24. Carrell RW, Boswell RD, Brennan SO, Owen MC: Active site of al-antitrypsin: Homologous site in antithrombin 111. Bio- chem Biophys Res Commun 93:399,1980
25. Chandra T, Stackhouse R, Kidd VJ, Robson KJH, Woo SLC Sequence homology between human al-antichymotrypsin, al-antitrypsin, and antithrombin 111. Biochemistry 22:5055,1983
26. Carrell RW, Aulak KS, Owen MC: The molecular pathology of the serpins. Mol Biol Med 6:35, 1989
27. Huber R, Carrell RW: Implications of the three-dimen- sional structure of al-antitrypsin for the structure and function of serpins. Biochemistry 28:8951,1989
28. Austin RC, Rachubinski RA, Ofosu FA, Blajchman MA: Antithrombin-111-Hamilton, Ala382 to Thr: An antithrombin 111
For personal use only.on April 4, 2019. by guest www.bloodjournal.orgFrom
2168 BLAJCHMAN ET AL
variant which acts as a substrate but not an inhibitor of thrombin and factor Xa. Blood 772185,1991
29. Bjork I, Danielsson A, Fenton JW, Jornvall H: The site in human antithrombin for functional proteolytic cleavage by throm- bin. FEBS Lett 126:257,1981
30. Bjork I, Jackson CM, Jornvall H, Lavine KK, Nordling K, Salsgiver WJ: The active site of antithrombin. Release of the same proteolytically cleaved form of the inhibitor from complexes with factor IXa, factor Xa and thrombin. J Biol Chem 2572406,1982
31. Lewis JH, Iammarino RM, Spero JA, Hasiba U: Antithrom- bin Pittsburgh: An alpha 1-antitrypsin variant causing hemorrhagic disease. Blood 51:129,1978
32. Owen MC, Brennan SO, Lewis JH, Carrell RW: Mutation of antitrypsin to antithrombin alpha 1-antitrypsin Pittsburgh (358 Met-Arg), a fatal bleeding disorder. N Engl J Med 309:694,1983
33. Carrell RW, Owen MC: Plakalbumin, alpha-1 antitrypsin, antithrombin and the mechanism of inflammatory disease. Nature 317:730,1985
34. Stein PE, Leslie AGW, Finch JT, Turnell WG, McLaughlin PJ, Carrell RW: Crystal structure of ovalbumin as a model for the reactive centre of serpins. Nature 347:99,1990
35. Peterson TE, Dudek-Wojciechowska G, Sottrup-Jensen L, Magnusson S: Primary structure of antithrombin 111 heparin cofactor. Partial homology between al-antitrypsin and antithrom- bin 111, in Collen D, Wiman B, Verstraete M (eds): The Physiolog- ical Inhibitors of Coagulation and Fibrinolysis. Amsterdam, The Netherlands, Elsevier, North-Holland Biomedical, 1979, p 43
36. Bock SC, Wion KL, Vehar GA, Lawn RM: Cloning and expression of the cDNA for human antithrombin 111. Nucleic Acids Res 10:8113,1982
37. Prochownik EV, Markham AF, Orkin S H Isolation of a cDNA clone for human antithrombin 111. J Biol Chem 258:8389, 1983
38. Stackhouse R, Chandra T, Robson KJH, Woo SLC: Purifica- tion of antithrombin 111 mRNA and cloning of its cDNA. J Biol Chem 258:703,1983
39. Sun X-J, Chang J-Y: Heparin binding domain of human antithrombin 111 inferred from the sequential reduction of its three disulfide linkages. J Biol Chem 264:11288,1989
40. Miller-Anderson J, Borg H, Anderson LO: Purification of antithrombin 111 by affinity chromatography. Thromb Res 5:439, 1974
41. Kurachi K, Schmer G, Hermodson MA, Teller DC, Davie EW: Characterization of human, bovine and horse antithrombin 111. Biochemistry 15:368, 1976
42. Franzen L-E, Svensson S, Larm 0: Structural studies on the carbohydrate portion of human antithrombin 111. J Biol Chem 255:5090,1980
43. Mizuochi T, Fuji J, Kurachi K, Kobata A Structural studies of the carbohydrate moiety of human antithrombin 111. Arch Biochem Biophys 203:458,1980
44. Peterson CB, Blackburn MN: Isolation and characterization of a antithrombin-I11 variant with reduced carbohydrate content and enhanced heparin binding. J Biol Chem 2601723,1985
45. Brennan SO, George PM, Jordan RE: Physiological variant of antithrombin 111 lacks carbohydrate side chain at Asn135. FEBS Lett 219:431,1987
46. Prochownik EV, Orkin SH: In vivo transcription of a human antithrombin 111 “minigene.” J Biol Chem 259:15386, 1984
47. Prochownik EV: Relationship between an enhancer element in the human antithrombin 111 gene and an immunoglobulin light-chain gene enhancer. Nature 316:845,1985
48. Jagd S, Vibe-Pedersen K, Magnusson S: Location of two of the introns in the antithrombin-I11 gene. FEBS Lett 293:213, 1985
49. Bock SC, Marrinan JA, Radziejewska E: Antithrombin I11 Utah: Proline-407 to leucine mutation in a highly conserved region near the inhibitor reactive site. Biochemistry 27:6171,1988
50. Bock SC, Levitan DJ: Characterization of an unusual length polymorphism 5’ to the human antithrombin 111 gene. Nucleic Acids Res 11:8569,1983
51. Daly ME, Perry DJ: Dde 1 polymorphism in intron 5 in the antithrombin 111 gene. Nucleic Acids Res 18:5583,1990
52. Daly M, Bruce D, Perry DJ, Price J, Harper PL, O’Meara A, Carrell R W Antithrombin Dublin-3 Val + Glu: An N-terminal variant which has an aberrant signal peptidase cleavage site. FEBS Lett 273:87, 1990
53. Jeffries AJ: Highly variable minisatellites and DNA finger- prints. Biochem SOC Trans 15:309,1987
54. Jeffries AJ, Neumann R, Wilson V: Repeat unit sequence variation in minisatellites: A novel source of DNA polymorphisms for studying variation and mutation by single molecule analysis. Cell 60473,1990
55. Decorte R, Cuppens H, Malynen P, Cassiman JJ: Rapid detection of hypervariable regions by the polymerase chain reac- tion technique. DNA Cell Biol9:461,1991
56. Perry DJ, Carrell RW: CpG dinucleotides are “hotspots” for mutation in the antithrombin 111 gene: Twelve variants identified using the polymerase chain reaction. Mol Biol Med 6:239,1989
57. Ochoa A, Brunel F, Mendelzon D, &hen GN, Zakin MM: Different liver nuclear proteins bind to similar DNA sequences in the 5’-flanking regions of three hepatic genes. Nucleic Acids Res 17:119, 1989
58. Lovrien EW, Magenis RE, Rivas ML, Goodnight S, More- land R, Rowe s: Linkage study of antithrombin 111. Cytogenet Cell Genet 22319,1978
59. Kao FT, Morse HG, Law ML, Lidsky A, Chandra T, Woo SLC: Genetic mapping of the structural gene for antithrombin 111 to human chromosome 1. Hum Genet 67:34,1984
60. Winter JH, Bennett B, Watt JL, Brown T, San Roman C, Schinzel A, King J, Cook PJL Confirmation of linkage between antithrombin 111 and DulTy blood group and assignment of AT3 to lq22 + q25. Ann Hum Genet 46:29,1982
61. Bock SC, Harris JF, Schwartz CE, Ward JH, Hershgold El, Skolnik MH: Hereditaxy thrombosis in a Utah kindred is caused by dysfunctional antithrombin 111 gene. Am J Hum Genet 3732, 1985
62. Rosenberg JS, McKenna PW, Rosenberg RD: Inhibition of human factor IXa by human antithrombin. J Biol Chem 250:8883, 1975
63. Kurachi K, Schmer G, Hermodson MA, Teller DC, Davie E W Inhibition of bovine factor IXa and Xa by antithrombin 111. Biochemistry 15:373,1976
64. B igs R, Denson KWE, Akman N, Borrett R, Hadden M: Antithrombin 111, antifactor Xa and heparin. Br J Haematol 19:283,1970
65. Damus PS, Hicks M, Rosenberg RD: Anticoagulant action of heparin. Nature 246:355,1973
66. Scott CF, Colman RW: Factors influencing the acceleration of human factor Xa inactivation by antithrombin 111. Blood 73:1873,1989
67. Stead N, Kaplan AP, Rosenberg RD: Inhibition of activated factor XI1 by antithrombin-heparin cofactor. J Biol Chem 251: 6481,1976
68. Pixley RA, Schapira M, Colman R W Effect of heparin on the inactivation rate of human activated Factor XI1 by antithrom- bin 111. Blood 66:198,1985
69. Lahiri B, Rosenberg R, Talamo RC, Mitchell B, Bagdasar- ian A, Colman RW: Antithrombin 111: An inhibitor of human plasma kallikrein. Fed Proc 33:642,1974 (abstr)
For personal use only.on April 4, 2019. by guest www.bloodjournal.orgFrom
INHERITED ANTITHROMBIN DEFICIENCY 2169
70. Highsmith RF, Rosenberg RD: The inhibition of human antithrombin 111 in the absence and presence of heparin. Thromb Haemost 39:616,1974
71. Clemmensen I: Inhibition of urokinase by complex forma- tion with human antithrombin in the absence and presence of heparin. Thromb Haemost 39:616,1978
72. Danielsson A, Bjork I: Mechanism of inactivation of trypsin by antithrombin 111. Biochem J 207:21,1982
73. Jordan RE, Oosta GM, Gardner WT, Rosenberg RD: The kinetics of hemostatic enzyme-antithrombin interactions in the presence of low molecular weight heparin. J Biol Chem 255:10081, 1976
74. Olson ST, Shore JD: Binding of high affinity heparin to antithrombin 111. Characterization of the protein fluorescence enhancement. J Biol Chem 256:11065,1981
75. Ofosu FA, Modi GJ, Smith LM, Cerskus AL, Hirsh J, Blajchman M A Heparan sulfate and dermatan sulfate inhibit the generation of thrombin activity in plasma by complementary pathways. Blood 54:727,1984
76. Jornvall H, Fish WW, Bjork I: The thrombin cleavage site in bovine antithrombin. FEBS Lett 106:358, 1979
77. Carrell RW, Pemberton PA, Boswell DR: The serpins: Evolution and adaptation in a family of protease inhibitors. Cold Spring Harb Symp Quant Biol52527,1987
78. Longas MO, Finlay TH: The covalent nature of the human antithrombin 111-thrombin bond. Biochem J 189:481, 1980
79. Shifman MA, Pizzo SV: The in vivo metabolism of antithrom- bin 111 and antithrombin 111 complexes. J Biol Chem 257:3243, 1982
80. Fish WW, Orre K, Bjork I: Routes of thrombin action in the production of proteolytically modified, secondary forms of anti- thrombin-thrombin complex. Eur J Biochem 101:39,1979
81. Owen MC: Evidence for the formation of an ester between thrombin and heparin cofactor. Biophys Biochim Acta 405:380, 1975
82. Devraj-Kizuk R, Chui DHK, Prochownik EV, Carter CJ, Ofosu FA, Blajchman M A Antithrombin-111-Hamilton: A gene with a point mutation (guanine to adenine) in codon 382 causing impaired serine protease reactivity. Blood 72:1518,1988
83. Chang J - Y Binding of heparin to human antithrombin I11 activates selective chemical modification at Lys 236. J Biol Chem 264:3111,1989
84. Sheffield WP, Fernandez-Rachubinski F, Austin RC, Blajch- man M A Molecular defects in antithrombin 111 deficiency, in Hoyer LW, Drohan WN (eds): Recombinant Technology in Hemostasis and Thrombosis. New York, NY, Plenum, 1991, p 133
85. Blackburn MN, Smith RL, Carson J, Sibley C C The heparin binding site of antithrombin 111. J Biol Chem 259:939,1984
86. Duchange N, Chasse J-F, Cohen GN, Zakin MM: Molecular characterization of the antithrombin 111 Tours deficiency. Thromb Res 45:115,1987
87. Brunel F, Duchange N, Fischer AM, Cohen GN, Zakin MM: Antithrombin I11 Alger: A new case of Arg 47 Cys mutation. Am J Hematol25:223, 1987
88. Roussel B, Dieval J, Delobel J, Fernandez-Rachubinski F, Eng B, Rachubinski RA, Blajchman M A Antithrombin-III- Amiens:A new family with an Arg47 -j Cys inherited variant of antithrombin I11 with impaired heparin cofactor activity. Am J Hematol3625, 1991
89. Owen MC, Shaw GJ, Grau E, Fontcuberta J, Carrell RW, Boswell DR: Molecular characterization of antithrombin Barce- lona 2: 47 arginine to cysteine. Thromb Res 55:451,1989
90. Mohlo-Sabatier P, Aiach M, Gaillard I, Fressinger J-N, Fischer A-M, Chadeuf G, Clauser E: Molecular characterization of antithrombin 111 (ATIII) variants using polymerase chain reaction.
Identification of the ATIII Charleville as an ala 384 pro mutation. J Clin Invest 84:1236,1989
91. Olds RJ, Lane DA, Cas0 R, Girolani A, Thein S L Anti- thrombin I11 Padua 11: A single base substitution in exon 2 detected using PCR and direct genomic sequencing. Nucleic Acids Res 18:1926,1990
92. Ueyama H, Murakami T, Nishiguchi S, Maeda S, Hashimoto Y, Okajima K, Shimada K, Araki S: Antithrombin I11 Kumamoto: Identification of a point mutation and genotype analysis of the family. Thromb Haemost 63:231,1990
93. Chang J-Y, Tran TH: Antithrombin-I11 Basel. Identification of a Pro to Leu substitution in a hereditary abnormal antithrombin with impaired heparin cofactor activity. J Biol Chem 261:1174, 1986
94. deRoux N, Chadeuf G, Mohlo-Sabatier P, Plouin P-F, Aiach M: Clinical and biochemical characterization of antithrombin I11 Franconville, a variant with Pro 41 Leu mutation. Br J Haematol 75:222, 1990
95. Borg J-Y, Owen MC, Soria C, Soria J, Caen J, Carrell R W Proposed heparin binding site in antithrombin based on arginine 47. A new variant Rouen-11, 47 Arg to Ser. J Clin Invest 81:1292, 1988
96. Wolf M, Boyer-Neumann C, Molho-Sabatier P, Neumann C, Meyer D, Larrieu MJ: Familial variant of antithrombin 111 (AT 111 Bligny, 47arg to his) associated with protein C deficiency. Thromb Haemost 63:215,1990
97. Caso R, Lane DA, Thompson E, Zangouras D, Panico M, Morris H, Olds RJ, Thein SL, Girolami A Antithrombin Padua 1: Impaired heparin binding caused by an Arg47 to His (CGT to CAT) substitution. Thromb Res 58:185,1990
98. Smith JW, Knauer DJ: A heparin binding site in antithrom- bin 111. J Biol Chem 262:11964,1987
99. Smith JW, Dey N, Knauer DJ: Heparin binding domain of antithrombin 111: Characterization using a synthetic peptide di- rected polyclonal antibody. Biochemistry 29:8950,1990
100. deMoerloose PA, Reber G, Vernet P, Minazio P, Bouvier C A Antithrombin 111 Geneva: A hereditary abnormal AT I11 with defective heparin cofactor activity. Thromb Haemost 57:154, 1987
101. Gandrille S, Aiach M, Lane DA, Vidaud D, Molho- Sabatier P, Cas0 R, deMoerloose P, Fiessinger J-N, Clauser E: Important role of arginine 129 in heparin-binding of antithrombin 111. J Biol Chem 265:18997,1990
102. Beresford CH, Owen MC: Antithrombin 111. Int J Biochem 22:121, 1990
103. Sun X-J, Chang J-Y: Re-formation of disulphide bonds in reduced antithrombin 111. Biochem J 269665,1990
104. Vidaud D, Sirieix ME, Alhere-Gelas M, Cladeuf G, Aillaud MF, Juhan-Vague I, Aiach M: A double heterozygosity in 2 brothers with antithrombin (ATIII) deficiency due to the associa- tion of an Arg 47 to His mutation with a 9 base pair (bp) deletion in exon VI. Thromb Haemost 65:838,1991 (abstr)
105. Hakten M, Deniz U, Ozbay G, Ulutin ON: Two cases of homozygous antithrombin 111 deficiency in a family with congenital deficiency of AT-111, in Senzinger H, Vinazzer H (eds): Thrombo- sis and Haemorrhagic Disorders. Proc. of the 6th International Meeting of the Danubian League Against Thrombosis and Haem- morrhagic Disorders. Wurzburg, Germany, Schmitt and Meyer GmbH, 1989, p 177
106. Hirsh J, Piovella F, Pini M: Congenital antithrombin 111 deficiency. Am J Med 87:34S, 1989 (suppl3B)
107. Tait RC, Walker ID, Perry DJ, Carrell RW, Islam SIA, McCall F, Mitchell R: Prevalence of antithrombin I11 deficiency subtypes in 4000 healthy blood donors. Thromb Haemost 65:839, 1991 (abstr)
For personal use only.on April 4, 2019. by guest www.bloodjournal.orgFrom
2170 BLAJCHMAN ET AL
108. Prochownik EV, Antonarakis S, Bauer KA, Rosenberg RD, Fearon ER, Orkin SH: Molecular heterogeneity of inherited antithrombin 111 deficiency. N Engl J Med 308:1549,1983
109. Fernandez-Rachubinski F, Rachubinski RA, Blajchman M A Partial deletion of an antithrombin 111 allele in a kindred with a type 1 deficiency. Blood 80:1476,1992
110. Daly M, Perry DJ, Harper PL, Daly HM, Rogues AWW, Carrell RW: Insertions/deletions in the antithrombin gene: 3 Mutations associated with non-expression. Thromb Haemost 6 7 521,1992
111. Olds RJ, Lane DA, Ireland H, Leone G, DeStefano V, Cazenave JP, Wiesel ML, Thien S L Novel point mutations leading to type l a antithrombin deficiency and thrombosis. Br J Haematol 78:408,1991
112. Olds RJ, Lane DA, Finazzi G, Barbui T, Thein S-L A frameshift mutation leading to type 1 antithrombin deficiency and thrombosis. Blood 762182,1990
113. Gandrille S, Vidaud D, Emmerich J, Clauser E, Sie P, Fiessinger JN, Alhenc-Gelas M, Priollet P, Aiach M: Molecular basis for hereditary antithrombin 111 quantitative deficiencies: A stop codon in exon IIIa and a frameshift in exon VI. Br J Haematol 78:414, 1991
114. Vidaud D, Emmerich J, Sirieix ME, Sie P, Alhenc-Gelas M, Aiach M: Molecular basis for antithrombin 111 type 1 deficiency: Three novel mutations located in exon IV. Blood 78:2305,1991
115. Grundy CB, Thomas F, Millar DS, Krawczak M, Melissari E, Lindo V, Moffat E, Kakkar W, Cooper DN: Recurrent deletion in the human antithrombin 111 gene. Blood 78:1027,1991
116. Olds RJ, Lane DA, Ireland A, Finazzi G, Barbui T, Abilgaard U, Girolami A, Thein S-L A common point mutation producing type 1A antithrombin 111 deficiency: AT129 CGA to TGA (Arg to stop). Thromb Res 64:621, 1991
117. Bock SC, Prochownik EV: Molecular genetic survey of sixteen kindreds with hereditary antithrombin 111 deficiency. Blood 70:1273,1987
118. Hultin MB, McKay J, Abilgaard U: Antithrombin Oslo: Type l b classification of the first report antithrombin-deficient family, with a review of hereditary antithrombin variants. Thromb Haemost 59:468,1988
119. Ireland H, Lane DA, Thompson E, Walker ID, Blench I, Morris H, Freyssinet JM, Grunebaum L, Olds R, Thein SL: Antithrombin Glasgow 11: Alanine 382 to threonine mutation in the serpin P12 position, resulting in a substrate reaction with thrombin. Br J Haematol79:70,1991
120. Perry DJ, Harper PL, Fairham S, Daly M, Carrell RW: Antithrombin Cambridge, 384 ala to pro: A new variant identified using the polymerase chain reaction. FEBS Lett 254:174,1989
121. Pewarchuk WJ, Fernandez-Rachubinski F, Rachubinski RA, Blajchman M A Antithrombin 111 Sudbury: An Ala384 + Pro mutation with abnormal thrombin-binding activity and thrombotic diathesis. Thromb Res 59:793,1990
122. Cas0 R, Lane DA, Thompson EA, Olds RJ, Thein SL, Panico M, Morris HR, Freyssinet JM, Aiach M, Rodeghiero F, Finazzi G: Antithrombin Vincenza, Ala 384 to Pro (GCA to CCA) mutation, transforming the inhibitor into a substrate. Br J Haema- to1 77:87, 1990
123. Harper PL, Luddington RJ, Daly M, Bruce D, Williamson D, Edgar PF, Perry DJ, Carrell RW: The incidence of dysfunc- tional antithrombin variants: Four cases in 210 patients with thromboembolic disease. Br J Haematol77:360,1991
124. Blajchman MA, Fernandez-Rachubinski F, Sheffield W, Austin RC, Schulman S: Antithrombin-111-Stockholm: A codon 392 (Gly+ Asp) mutation with normal heparin binding and impaired serine protease reactivity. Blood 79:1428,1992
125. Erdjument H, Lane DA, Panico M, DiMarzo V, Morris HR: Single amino acid substitutions in the reactive site of antithrom- bin leading to thrombosis. Congenital substitution of arginine 393 to cysteine in antithrombin Northwick Park and to histidine in antithrombin Glasgow. J Biol Chem 2635589,1988
126. Lane DA, Erdjument A, Glynn V, DiMarzo H, Panico M, Morris HR, Greaves M, Dolan G, Preston FE: Antithrombin Sheffield: Amino acid substitution at the reactive site (Arg393 to His) causing thrombosis. Br J Haematol71:91,1989
127. Erdjument H, Lane DA, Panico M, DiMarzo V, Morris HR, Bauer K, Rosenberg RD: Antithrombin Chicago, amino acid substitution of arginine 393 to histidine. Thromb Res 54:613, 1989
128. Erdjument H, Lane DA, Ireland H, DiMarzo V, Panico M, Morris HR, Tripodi A, Mannucci PM: Antithrombin 111 Milano. Single amino acid substitution at the reactive site, Arg393 to Cys. Thromb Haemost 60471,1988
129. Ireland H, Lane DA, Thompson E, Olds R, Thein SL, Hach-Wunderle V, Scharrer I: Antithrombin Frankfurt I: Arginine to cysteine substitution at the reactive site and formation of a variant antithrombin-albumin covalent complex. Thromb Haemost 65:913,1991
130. Lane DA, Erdjument H, Thompson E, Panico M, DiMarzo V, Morris HR, Leone G, DeStefano V, Thein S L A novel amino acid substitution in a congenital variant antithrombin: Antithrom- bin Pescara, Arg393 to Pro, caused by a CGT to CCT mutation. J Biol Chem 264:10200,1989
131. Stephens AW, Thalley BS, Hirs C H W Antithrombin-III- Denver, a Ser to Leu 394 variant without protease inhibitory activity. Thromb Haemost 5449, 1985 (abstr)
132. Stephens AW, Thalley BS, Hirs CHW: Antithrombin-I11 Denver, a reactive site variant. J Biol Chem 262:1044,1987
133. Olds RJ, Lane DA, Cas0 R, Tripodi A, Mannucci PM, Thein S L Antithrombin 111 Milano 2: A single base substitution in the thrombin binding domain detected with PCR and direct genomic sequencing. Nucleic Acids Res 1710511,1989
134. Olds RJ, Thein SL, Ireland H, Lane DA, Boisclair M, Conard J, Horellou MH: Identification of 402 phenylalanine as a functionally important residue in antithrombin. Thromb Haemost 65:670, 1990 (abstr)
135. Nakagawa M, Tanaka H, Tsuji H, Takada 0, Uno M, Hashimoto-Gotoh T, Wagatsuma M: Congenital antithrombin 111 deficiency (AT-I11 Kyoto): Identification of a point mutation altering arginine-406 to methionine behind the reactive site. Thromb Res 64:101,1991
136. Austin RC, Rachubinski RA, Blajchman MA: Site-directed mutagenesis of alanine 382 of human antithrombin 111. FEBS Lett 280:254,1991
137. Owen MC, Beresford CH, Carrell RW: Antithrombin Glasgow, 393 Arg to His, a PI reactive site variant with increased heparin affinity but no thrombin inhibitory activity. FEBS Lett 231:317,1988
138. Lane DA, Flynn A, Ireland H, Erdjument H, Samson D, Howarth D, Thompson E: Antithrombin 111 Northwick Park Demonstration of an inactive high MW complex with increased affinity for heparin. Br J Haematol65:451,1987
139. Bock SC, Harris JF, Schwartz CE, Ward JH, Hershgold EJ, Skolnik MH: Hereditary thrombosis in a Utah kindred is caused by dysfunctional antithrombin 111 gene. Am J Hum Genet 37:32,1985
140. Sorensen PJ, Sas G, Pet0 I, Blasko G, Kremmer T, Samu A. Distinction of two pathologic antithrombin 111 molecules: Anti- thrombin 111 “Aalborg” and antithrombin 111 “Budapest.” Thromb Res 26211,1982
141. Jorgensen M, Peterson LC, Thorsen S: Purification and characterization of hereditary abnormal antithrombin 111 with impaired thrombin binding. J Lab Clin Med 104:242,1984
For personal use only.on April 4, 2019. by guest www.bloodjournal.orgFrom
INHERITED ANTITHROMBIN DEFICIENCY 2171
142. Girolami A, Marafioti F, Rubertelli M, Vicariato MA, Cappellato G, Mazzuccato M: Antithrombin I11 Trento: A “new” congenital AT-I11 abnormality with a peculiar crossed immunoelec- trophoresis pattern in the absence of heparin. Acta Haematol 72:73,1984
143. Olds RJ, Lane DA, Boisclair M, Sas G, Bock SC, Thein S-L Antithrombin Budapest 3: Antithrombin variant with reduced heparin affinity resulting from the substitution L99F. FEBS Lett 300:241,1992
144. Finazzi G, Caccia R, Barbui T: Different prevalence of thromboembolism in the subtypes of congenital antithrombin I11 deficiency: Review of 404 cases. Thromb Haemost 58:1094, 1987 (letter)
145. Fischer AM, Cornu P, Sternberg C, Meriane F, Dautzen- berg MD, Chafa 0, Beguin S, Desnos M: Antithrombin 111 Alger: A new homozygous AT-I11 variant. Thromb Haemost 55:218,1986
146. Boyer C, Wolf M, Vedrinni J, Meyer D, Larrieu MJ: Homozygous variant of antithrombin 111: AT-I11 Fontainebleau. Thromb Haemost 56:18,1986
147. Sakuragawa N, Takahashi K, Kondo S, Koide T Antithrom- bin 111 Toyama: A hereditary abnormal antithrombin 111 of a patient with recurrent thrombophlebitis. Thromb Res 31:305,1983
148. Grau E, Fontcuberta J, FClez J, deDiego I, Soto R, Rutllant M L ATIII Barcelona: A familial quantitative-qualitative ATIII deficiency. Thromb Haemost 59:13,1988
149. Gomperts ED, Feesey M, Vander Walt TD: Two dimen- sional immunoelectrophoretic studies in antithrombin I11 defi- ciency. Thromb Res 8:713,1976
150. DeStefano V, Leone G, Ferrelli R, DiDonfrancesco A, DeMartini D, Bizzi B: Further characterization of a pathological isoantithrombin with no affinity to heparin. Thromb Res 48:23, 1987
151. Daly M, O’Meara A, Hallinan FM: Identification and characterization of a new antithrombin familial variant (AT Dublin) with possible increased frequency in children with cancer. Br J Haematol65:457,1987
152. Brennan SO, Borg J-Y, George PM, Soria C, Soria J, Caen J, Carrell RW: New carbohydrate site in mutant antithrombin (7Ile -+ Asn) with decreased heparin affinity. FEBS Lett 237118, 1988
153. Olds RJ, Lane DA, Cas0 R, Panico M, Morris HR, Sas G, Dawes J, Thein S-L Antithrombin 111 Budapest: A single amino
acid substitution (429 Pro to Leu) in a region highly conserved in the serpin family. Blood 79:1206, 1992
154. Borg J-Y, Brennan SO, Carrell RW, George P, Perry DJ, Shaw J: Antithrombin Rouen IV 24 Arg to Cys: The amino terminal contribution to heparin binding. FEBS Lett 266:163,1990
155. Grundy CB, Holding S, Millar DS, Kakkar W, Cooper D N A novel missence mutation in the antithrombin 111 gene (Ser 349 - Pro) causing recurrent venous thrombosis. Hum Genet 88:707,1992
156. Abilgaard U, Lie M, Odegard O R Antithrombin (heparin cofactor) assay with ‘new’ chromogenic substrates (S-2238 and Chromozym TH). Thromb Res 11:549,1977
157. Demers C, Ginsberg JS, Mitchell L, Henderson P, Johnson M, Ofosu FA, Fernandez-Rachubinski F, Andrew M, Blajchman M A Comparison of three antithrombin 111 (AT-111) assays in AT-111 deficient individuals. Blood 78:212a, 1991 (abstr, suppl 1)
158. Mancini G, Carbonara AO, Heremans J F Immunochemi- cal quantitation of antigens by simple radial immunodiffusion. Int J Immunochem 2:235,1965
159. Laurel1 CB: Quantitative estimation of proteins by electro- phoresis in agarose gel containing antibodies. Ann Biochem 15:45, 1966
160. Sas G, Pepper DS, Cash JD: Plasma and serum antithrom- bin 111: Differentiation by crossed immunoelectrophoresis. Thromb Res 6:87,1975
161. Saiki RJ, Scarf S, Faloma F, Mullis KB, Horn GT, Erhich HA, Arnheim N: Enzymatic amplification of P-globin genomic sequences and restriction site analysis for detection of sickle cell anemia. Science 230:1350, 1985
162. Hull RD, Raskob GE, Leclerc JR, Jay RM, Hirsh J: The diagnosis of clinically suspected venous thrombosis. Clin Chest Med 5:439,1984
163. Demers C, Ginsberg JS, Hirsh J, Henderson P, Blajchman M A Thrombosis in antithrombin I l l deficient individuals: Report of a large kindred and literature review. Ann Int Med 116:754,1992
164. Blajchman MA, Wells P: Antithrombin 111, Protein C and Protein S deficiency, in Brain MC, Carbone PP (eds): Current Therapy in Hematology-Oncology-4. Philadelphia, PA, Decker, 1991, p 123
165. Dreyfus M, Magny JF, Bridey F, Schwarz HP, PlanchC C, Dehan M, Tchernia G: Treatment of homozygous protein C deficiency and neonatal purpura fulminans with a purified protein C concentrate. N Engl J Med 325:1565,1991
For personal use only.on April 4, 2019. by guest www.bloodjournal.orgFrom
1992 80: 2159-2171
MA Blajchman, RC Austin, F Fernandez-Rachubinski and WP Sheffield Molecular basis of inherited human antithrombin deficiency
http://www.bloodjournal.org/content/80/9/2159.full.htmlUpdated information and services can be found at:
Articles on similar topics can be found in the following Blood collections
http://www.bloodjournal.org/site/misc/rights.xhtml#repub_requestsInformation about reproducing this article in parts or in its entirety may be found online at:
http://www.bloodjournal.org/site/misc/rights.xhtml#reprintsInformation about ordering reprints may be found online at:
http://www.bloodjournal.org/site/subscriptions/index.xhtmlInformation about subscriptions and ASH membership may be found online at:
Copyright 2011 by The American Society of Hematology; all rights reserved.Society of Hematology, 2021 L St, NW, Suite 900, Washington DC 20036.Blood (print ISSN 0006-4971, online ISSN 1528-0020), is published weekly by the American
For personal use only.on April 4, 2019. by guest www.bloodjournal.orgFrom





























