Embed Size (px)
Citation preview

Multi-Analyte Testing of
Respiratory Viruses
Molecular Pathology : Principles in
Clinical Practice
AACC / AMP
May 8, 2012
Karen M. Frank, M.D., Ph.D.
REVISED

Speaker Disclosure Information
Grant / Research Support: bioMerieux
Learning Objectives
1. Describe different technologies used in molecular
diagnostic assays of respiratory viruses.
2. List critical factors when choosing a testing
platform for a specific institution, and compare
available commercial instruments.
3. Discuss issues that a clinician must consider
when interpreting the results of the respiratory
virus testing as a treatment plan is created.
After this presentation, you should be able to:

Outline (1) Epidemiology
(2) Molecular Testing Methodologies
(3) Controversial Issues: When to Test?
(4) Rapid Antigen Assays
(5) Example Patients and Treatment Options
(6) Infection Control
(7) Co-infection
(8) Future Issues

Epidemiology of Respiratory Syncytial Virus
• Most common cause of bronchiolitis and pneumonia in
children < 1 year of age worldwide.
• 60 million episodes & 3-4 million hospitalizations
• 66,000 – 600,000 deaths per year, 90% in developing areas.
• U.S. Data: 75,000 – 125,000 infant hospitalizations each yr.
• 400 Deaths in Infants
Villarruel et al. (2010) MMWR 59:230-233.
Nair et al. (2010) Lancet 375:1545-1555.
WHO (2009) Acute Resp. Inf. Update.
Krilov LR (2011) Expert Rev.
Infect Ther.9:27-32.
Mahony, JB (2010) Expert Rev.
Anti Infect Ther. 8:1273-1292.

Epidemiology of Influenza Virus
• In United States, 62,000 hospitalizations in 2010-
11 season.
•Range of deaths over 31 years is 3,000 to 49,000
annually.
Centers for Disease Control and Prevention
http://www.cdc.gov

• Mahony table of prevalence – make histogram with error bars
Popow and Aberle (2011) Open Micro Jnl. 5: (S2-M2) 128-134.
Regamy et al. (2008) Ped. Inf. Dis. J. 27:100-105.
Atmar et al. (2012) J. Clin. Microbiol. 50:506-508.
Mahony (2010) Expert Rev. Anti. Infect. Ther. 8:1273-1292.
Gaunt et al. (2011) J. Clin. Virol. 52:215-221.
Martin et al. (2012) Infl. Other Resp. Viruses 6:71-77.
Pavia (2011) Clin. Inf. Dis. 52(S4):S284-289.
Prevalence of Respiratory Viruses Detected during Illness

?

Disease Burden Due to Specific Viruses Varies by Age
Disease Burden Histogram Does Not Correlate with Viral Prevalence
Gaunt, E.R. et al. (2011) J. Clin. Virol. 52:215-221.

Molecular Testing Offers Significantly
Higher Assay Sensitivity
Method Sensitivity (%)
Specificity (%)
DFA or Culture
50 - >80 98 - 100
Ginocchio, G, et al. (2009) J. Clin. Virol. 45:191-195.
Leland, D. and Ginocchio, C.C. (2007) Clin. Microbiol. Rev. 20:49-78.
Liao, R. S. et al. (2009) J. Clin. Microbiol. 47:527-532.

Multiple Newly Developed Technologies
are Utilized for Multi-Analyte Testing
Caliendo, A. (2011) Clin. Inf. Dis. 52(S4):S326-S330.
Mahony, J.B. (2011) Crit. Rev. Clin. Lab. Sci. 48:217-249.
Olofsson S. et al. (2011) Expert Rev. Anti Infect. Ther. 9:615-626.
Ginocchio, C. (2011) Clin. Inf. Dis. 52(S4):S312-S325.
Endimiani, A. et al. (2011) Clin. Inf. Dis. 52(S4):S373-S383.
Gharabaghi, F. et al. (2011) Clin. Microbiol. Inf. 17:1900-1906.
Zhang, S. et al. (2011) Curr. Infect. Dis. Rep. 13:149-158.

Multiple Newly Developed Technologies are
Utilized for Multi-Analyte Testing

Multiple Newly Developed Technologies are
Utilized for Multi-Analyte Testing

http://www.luminexcorp.com
Luminex xTAG RVP

Luminex
Ginocchio, C. (2011) Clin. Inf.
Dis. 52(S4):S312-S325.
Exo=Exonuclease I
SAP=Shrimp Alkaline
Phosphatase
B=Biotin-dCTP
PE=Phycoerythrin

http://www.cepheid.com
Cepheid GenExpert
1. Integrated
Extraction
2. Real-time
Reverse Transcription
PCR.

Gen-Probe Pro-Flu + (Previously Prodesse)
http://www.cepheid.com
http://www.gen-probe.com
http://www.biomerieux-usa.com
Cepheid Smart Cycler
bioMerieux NucliSens EasyMag
1. Separate
Extraction
2. Real-time
Reverse Transcription
PCR.
Separate Assays:
ProFlu+
ProFAST
Pro hMPV+
ProAdeno+
ProParaflu+

Nanosphere Verigene RV+
http://www.nanosphere.us
1. Extraction
2. Reverse
Transcription PCR,
when needed.
3. Complementary
Oligo on Solid Array
Support.
4. Mediator Oligo on
Gold Nanoparticle.
5. Silver Amplification
of Signal.

Autogenomics Infinity RVP+
http://www.autogenomics.com
1. Integrated Extraction and Subsequent Reactions.
2. Multiplex PCR.
3. BioFilmChip Solid Microarray
Other assays:
Factor II
Factor V Leiden
Warfarin
CYP2C19

http://www.ibisbiosciences.com
Abbott PLEX-ID
1. Extraction
2. Multiplex PCR
in 96 well
plate.
3. Electrospray
Ionization
Mass
Spectrometry.
4. Multi-locus
base
composition
analysis. Multiple classes of microorganisms can be identified.

http://www.idahotech.com
Idaho Technology FilmArray
(1) Extraction of nucleic acids from sample.
(2) Nested multiplex PCR.
(3) Singleplex second-stage PCR
(4) Endpoint melting curve data.

Iquum Liat Analyzer
http://www.iquum.com
Turn-around-time of 20 minutes.

Different Sets of
Viruses are
Included in
Different
Multi-Analyte
Assays
1. Luminex xTAG RVP
2. Luminex xTAG RVP FAST
3. Gen-probe ProFlu+ (Prodesse)
4. Idaho Technologies FilmArray
5. Abbott PLEX-ID
6. Nanosphere Verigene
7. IQuum Liat Analyzer
8. Qiagen ResPlex II
9. Focus Diagnostics Simplexa
10. Autogenomics INFINITI RVP Plus
11. Seegene SeePlex
12. EraGen MultiCode PLx (Luminex)
13. PathoFinder RespiFinder

Different Sets of
Viruses are Included
in Different
Multi-Analyte Assays

Sensitivity and Specificity of Molecular Assays
is Quite High
Mahony, J.B. (2011) Crit. Rev. Clin. Lab. Sci. 48:217-249.
Gharabaghi, F. et al. (2011) Clin. Microbiol. Inf. 17:1900-1906.
Krunic, N. et al. (2011) Ann. N.Y. Acad. Sci. 1222:6-13.
Rand, K. H. et al. (2011) J. Clin. Microbiol. 49:2449-2453.
Pierce, V. M. et al. (2012) J. Clin. Microbiol. 50:364-371.
Loeffelholz, M.J. et al. (2011) J. Clin. Microbiol. 49:4083-4088.
Poritz, M. A. et al. (2011) PLoS ONE 6:e26047.
Pabbaraju, K. et al. (2011) J. Clin. Microbiol. 49:1738-1744.
Raymaekers, M. et al. (2011) J. Clin. Virol. 52:314-316.
Jannetto, R. J. et al. (2010) J. Clin. Microbiol. 48:3997-4002.
Pabbaraju, K. et al. (2008) J. Clin. Microbiol. 46:3056-3062.
Gadsby, N. J. et al. (2010) J. Clin. Microbiol. 48:2213-2216.
Arens, M. Q. et al. (2010) J. Clin. Microbiol. 48:2387-2395.
Miller, S. et al. (2010) J. Clin. Microbiol. 48:4684-4685.
Selvaraju, S. B. and Selvarangan, R. (2012) Diag. Microbiol. Inf. Dis. 72:278-281.
Balada-Llasat, J.-M. et al. (2011) J. Clin. Virol. 50:42-45.
Chen, K.-F. et al. (2011) J. Virol. Methods 173:60-66.
Hayden, R. T. et al. (2012) J. Clin. Virol. doi.10.1016/j.jcv.2011.12.020.
Caution Needed to Interpret Data Due of Reference Standard
& Number of EACH SPECIFIC VIRUS Tested

Specificity of Molecular Assays is Very High

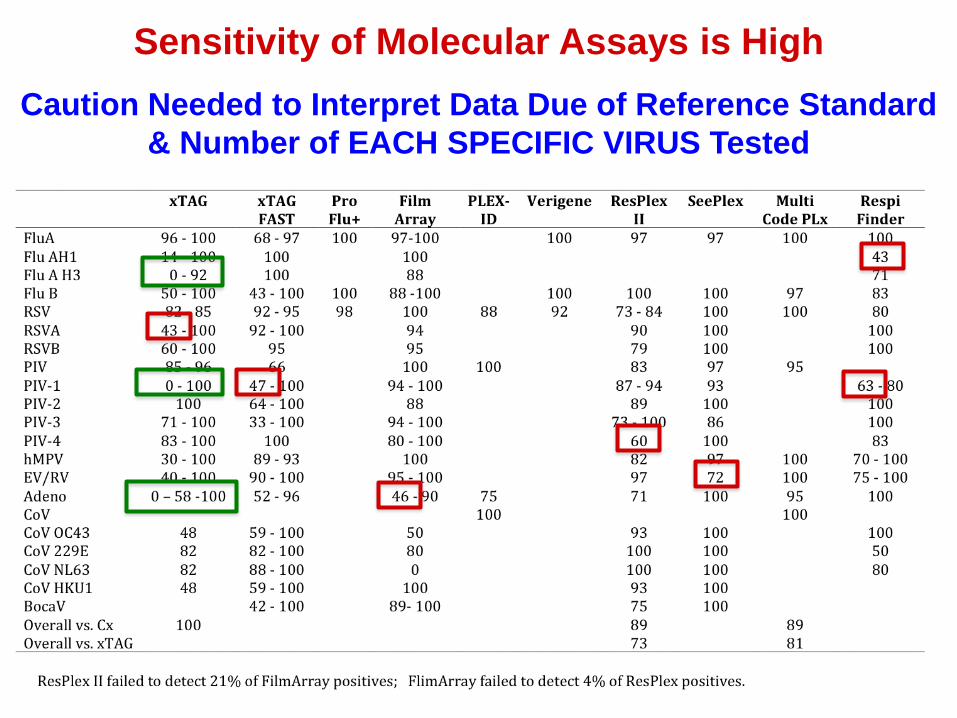
Sensitivity of Molecular Assays is High
Caution Needed to Interpret Data Due of Reference Standard
& Number of EACH SPECIFIC VIRUS Tested
Sensitivity of Molecular Assays is High
Caution Needed to Interpret Data Due of Reference Standard
& Number of EACH SPECIFIC VIRUS Tested

How do I pick a method for MY LAB?!
1. Determine of viruses you want to detect.
2. Consider if instrument is approved.
3. Determine that matches your budget.
4. Decide level of you have.
5. Determine required.
6. EVALUATE performance: literature & colleagues.
7. Consider needs and combining assays.

Do we really need
respiratory virus
molecular testing
anyway?

Be
ds
Number of Hospital Beds Range 250 -5000
0
200
400
600
800
1000
1200
1400
1600
1800
2000
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29
Series1
5000
Survey of Microbiology Laboratories
through Contacts on ClinMicroNet
Current Practice for Respiratory Virus Testing

Labs Offer Multiple Methods for Single Target
0
2
4
6
8
10
1 2 3 4 5
Series1
Influenza
0 1 2 3 4
0
5
10
15
1 2 3 4 5
Series1
Parainfluenza
0 1 2 3 4 0
2
4
6
8
10
12
14
1 2 3 4 5
Series1
Adenovirus
0 1 2 3 4 0
2
4
6
8
10
12
14
1 2 3 4 5
Series1
Rhinovirus/Enterovirus
0 1 2 3 4
0
2
4
6
8
10
1 2 3 4 5
Series1
RSV
0 1 2 3 4
hMPV
0
2
4
6
8
10
12
14
1 2 3 4 5
Series1
0 1 2 3 4
Number of Tests

Methods Currently in Use for Influenza Testing
0
1
2
3
4
5
6
7
8
9
10
11
12
13
1 2 3 4 5 6 7 8 9 10
Series1
Nu
mb
er
of
Lab
s
#2 Survey

CAP Proficiency Survey Shows High Use of Rapid Antigen Assays
Survey Method Virus 2009 2010 2011
VR1 Culture Influenza A Influenza B
RSV Parainfluenza
350 330 320
VR2 Direct Fluorescent
Antibody
Influenza A Influenza B
RSV Parainfluenza
290-320 240-290 240-280
VR2 Direct Fluorescent
Antibody
Metapneumo-virus
84 94
VR4 Rapid Antigen Assay
Influenza A Influenza B
RSV
1800-2800 1900-2300 1900-2300
VR4 Rapid Antigen Assay
Adenovirus 50 50-60

Survey
Method Organism 2009 2010 2011
ID2 Molecular Influenza 104 200 260
ID2 Molecular RSV 79 155 193
ID2 Molecular Parainfluenza 51 100 132
ID2 Molecular Adenovirus 70 105 133
ID2 Molecular Metapneumo-virus
53 103
ID2 Molecular Coronavirus 17 28
D Bacterial Culture E. coli/Staphyloco
ccus
2300-2800
F Mycology Culture Candida 1000
E Mycobacterial Culture
Mycobacteria 420
CAP Proficiency Survey Shows Increasing Use of Molecular Assays

Comment from Survey Participant
“Here is a Reality Check for you Karen!
Resources are limited. We function without
molecular tests.”
“I haven’t ordered a respiratory virus test in
the past 3 years.”
UCMC Primary Care Physician

Method Relative Cost To Lab
Relative Charge
to Patient
Labor Time
Labor Expertise
Rapid Antigen 1 1 Low Low
Culture 3 3 Days Medium
Direct Fluorescent
Ab
3 1.5 Hours Medium Expertise
Prodesse 7
(3 virus panel)
3 Hours High
Luminex 9
(12 virus panel)
11 Whole Shift
High
Comparison of Molecular versus Traditional Methods
Centers for Disease Control and Prevention
http://www.cdc.gov
Rapid antigen assays for Influenza generally have
sensitivities of 40-70% (range reported is 10-80%).
“Results from these rapid tests are not accurate.”
Rapid Antigen Assays
#7 Rapid Ag Test

16 year old student with respiratory symptoms
No admission, symptoms mild
Influenza Rapid Antigen Assay
True Positive
Influenza
correctly
detected
True Negative
No influenza
Other virus likely.
False Positive
Incorrectly
diagnose
Influenza.
Likely other virus,
but not realized.
False Negative
Influenza
Not detected.
Falsely think it is
other virus.
Otherwise Healthy Person with Mild Disease
Send home
Educate on good respiratory hygiene.
Return to class based on clinical symptoms

True Positive
RSV correctly
identified.
Treat with
ribavirin.
Cohort correctly.
True Negative
Organism not
identified.
No ribavirin.
How cohort for
other viruses?
.
False Positive
Organism not
identified.
Give ribavirin.
Limit work-up.
Expose child to
RSV.
False Negative.
RSV
not detected.
Do not give
ribavirin.
Work-up ordered.
Exposing RSV-
children.
Isolation and Cohorting
2 year old child admitted
with significant with respiratory symptoms
RSV Rapid Antigen Assay

www.cdc.gov
Percent of Influenza Positive Tests is Most Often Below 40%

Prevalence Matters!!
RAPID Ag

Prevalence Matters!!
Molecular

Prevalence Matters!!
Off
Season

Oncologist Finds Testing Helpful
• Testing is indicated due to immune compromise from
chemotherapy, even as an outpatient, even with mild
symptoms, even outside of regular flu season.
• Therapy is affected by result
- Duration of therapy with Tamiflu
- Decision to start Ribavirin or Liposomal cidofavir
- Empiric therapy started for flu, but not for other viruses.
- In come cases, reduce or stop empiric bacterial coverage,
but often still worried about superinfection with bacteria.

Example #1 Molecular Test Useful: HIV
• 45 y/o male in respiratory distress with history of
asthma/COPD, HIV/AIDS, substance abuse, non-
adherence to his HAART therapy
• Differential DX: COPD/asthma exacerbation
Community-acquired pneumonia
Pneumocystis.
• Positive for RSV
• 31 y/o with AML-M2, status post matched-related
stem cell transplant 2 months ago, with mild graft
versus host disease and diabetes mellitus presents
with fever and cough.
• Respiratory testing positive for adenovirus
Example #2 Molecular Test Useful: Stem Cell Transplant Patient

Stem Cell Transplant Patient (cont.)
• Adenovirus PCR from the blood > 2 million copies
• Liver biopsy 5 days later: Adenovirus hepatitis with
marked hemosiderosis
• No fibrosis, Clusters of hepatocytes with some
nuclear inclusions
• Immunostain confirmed Adenovirus

• 84-year-old man with history of coronary artery disease, congestive heart failure, complete heart block, status post pacemaker placement, atrial fibrillation, numerous orthopedic issues presents with cough and fatigue.
• Positive for Influenza A
Heart condition vs infection?
Example #3 Molecular Test Useful: Heart Disease

Actions that can be taken based on test results:
(1)Stop Influenza antiviral.
(2)Start other antiviral agents.
(3)Stop some antibiotics.
(4)Cancel further diagnostic tests.
(5)Change type of isolation precautions.
Influenza Therapy Does Not Require Testing
• M2 channel inhibitors: amantidine and rimantidine
(only effective for FluA)
• Neuraminidase inhibitors – oseltamivir and zanamavir
• Should be given within first 48 h following infection
• Treatment should NOT wait for laboratory confirmation.
• Treat for 5 days, longer in some patients.
Centers for Disease Control and Prevention, http://www.cdc.gov
• Due to high levels of resistance, adamantanes not
recommended in 2010-2011 season
• Adamantane-resistant H3N2 FluA circulating since 2003
• Oseltamivir-resistant seasonal H1N1 since 2007
• Adamantane-resistent 2009 H1N1 since 2009
• Since 9/2009, 99% of flu in US is susceptible to
neuraminidase inhibitor
Influenza Treatment Depends on Resistance Patterns
When should you subtype?
MMWR (2011) 60:1
Hayden, F.G. and deJong, M.D. (2011) J. Inf. Dis. 203:6.
MMWR (2010) 59:1651
MMWR (2010) 59:901

• Low rate of resistance to oseltamivir for pandemic H1N1
• H274Y mutation in N causes resistance to oseltamivir
• S247N mutation in N causes some resistance to oseltamivir
and zanamivir.
• Dual mutation S247N/H275Y had 7000 increase in IC50 to
oseltamivir and 5 fold increase in IC50 to zanamivir.
• Other mutations: I223R in N
http://www.ecdc.europa.edu
http://www.who.int
MMWR (2009) 58:1236.
Mai, L.Q. et al. (2010) N. Engl. J. Med. 362:86-87.
Nguyen, H.T. et al. (2010) Clin. Inf. Dis. 51:983.
Flu Mutations Causing Anti-Viral Resistance
Mutations may also affect detection

RSV Treatment
Krilov, L.R. (2011) Expert Rev. Infect Ther. 9:27-32
• Ribavirin – guanosine analog
• Administered by prolonged aerosol via a small-
particle generator.
• High cost
• Cumbersome method of delivery
• Concerns about secondary exposure to caretakers
• So use is limited.

• N=603
• Children with proven RSV had 1 day shorter
hospitalization than children without a pathogen
identified.
• Fewer antibiotics 54% vs 69%
• Shorter duration of antibiotics 6.2 vs 9.3 days.
Study Demonstrating Benefit of RSV
Identification in Children
Ginocchio and colleagues: Manji, R. et al. (2009) J. Clin. Pathol. 62:998-1002.

Shadman and Wald (2011) Expert Opin Biol. Ther. 11:1455-1467.
RSV Prophylaxis Decreases Disease Burden
• Palivizumab is a humanized, murine, monoclonal antibody
that binds to RSV F protein.
• 45- 55% reduction in hospitalizations
• The 2009 Recommendations regarding Palivizumab from
the American Academy of Pediatrics attempt to balance
the cost with clinical benefit, compared to previous
recommendations.

Shadman, K.A. and Wald, E.R. (2011) Expert. Opin. Biol. Ther. 11:1455-1467.
Cox Dunn, M.C. et al. (2011) Antiviral Therapy 16:309-317.
• Leflunomide examined as a possible treatment of RSV
using rat model.
Emerging Vaccines and Drugs for RSV Treatment

Wendt, CH (1992) N. Engl. J. Med. 326:921
Nichols, W.G. (2001) Blood 98:573.
Elizaga (2001) J. Clin. Infect. Dis. 32:413
Chakrabarti, S. (2000) Clin. Infect. Dis. 31:1516.
Cobian, L. (1995) Clin. Infect. Dis. 21:1040.
Wright, J.J. (2005) J. Heart Lung Transplant 24:343.
Ison, M.G. Antivir. The.r (2007) 12:627
Alymova, I.V. (2005) Antimicrob Agents Chemother 49:398.
Alymova, I.V. (2004) Antimicrob Agents Chemother 48:1495.
Hermos, C.R. et al. (2010) Clin. Lab. Med. 30:131-148.
Wilkesmann, A. et al. (2006) Eur. J. Pediatr. 165:467-475.
Hamelin, M. et al. (2004) Clin. Inf. Dis. 38:983-990.
Wolf, D.G. et al. (2006) Pediatr. Inf. Dis. J. 25:320-324.
Beneri, C. et al. (2009) Inf. Contr. Hosp. Epidemiol. 30:1240-1241. Neofytos, D. (2007) Biol Blood Marrow Transplant 13:74.
Legrand, F. (2001) Bone Marrow Transplant 27:621
Ljungman, P. et al. (2003) Bone Marrow Transplant 31:481.
Doan, M.L. et al. (2007) J. Heart Lung Transplant 26:883.
Myers, G.D. et al. (2007) Bone Marrow Transplant 39:677.
http://clinicaltrials.gov
Limited Treatment for Respiratory Viruses

Limited Treatment for Respiratory Viruses
• Parainfluenza – Variable reports for ribavirin
• hMPV – Trial examining ribavirin
• Adenovirus – Cidofovir, Liposomal Cidofovir,
Intravenous Immune Globulin
• Oseltamivir – 600 patients
• Palivizumab – 130 patients
• Ribavirin – 50 patients
Limited Use of Antivirals at University of Chicago 2010-2011
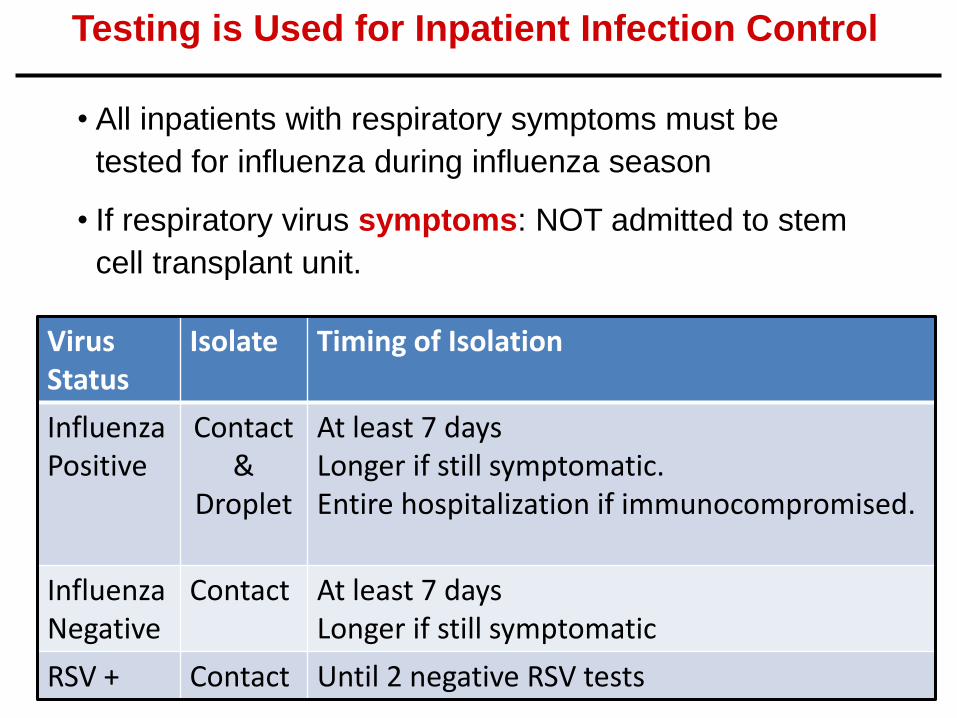
Testing is Used for Inpatient Infection Control
Virus Status
Isolate Timing of Isolation
Influenza Positive
Contact &
Droplet
At least 7 days Longer if still symptomatic. Entire hospitalization if immunocompromised.
Influenza Negative
Contact At least 7 days Longer if still symptomatic
RSV + Contact Until 2 negative RSV tests
• All inpatients with respiratory symptoms must be
tested for influenza during influenza season
• If respiratory virus symptoms: NOT admitted to stem
cell transplant unit.

Patient/Symptoms
Admit?
Testing ?
Treat ?
Infection Control
Mild, no comorbidtiy
No No No
Mild + comorbidity
No Yes, as needed
Yes, as needed
Severe Yes Yes Yes Contact + Droplet
University Student
No No No Return after afebrile 24h off anti-pyretic
Clinical Student
No No No Afebrile 24h off anti-pyretic. Wear mask if symptoms.
Not permitted on immunosuppressived
patient units or NICU for 7 days from symptom onset
UCMC Testing Guidelines When we DON’T test.

Coinfection /Codetection
• Coinfection with influenza reported as high as 20%.
• Co-infection more frequent than would happen randomly due
to co-circulating viruses.
• Rhinovirus and Coronaviruses = most common coinfections
• 30-40% incidence of bacterial coinfection in children/infants
ventilated for RSV infection
Esper, FP et al., J. Infection (2011) doi:10.1016/j.jinf.2011.04.004
Leven, D. et al. (2010) Pediatr. Crit. Care Med. 11:390-395.
Thorburn, K. (2011) Pediatri. Crit. Care Med. 12:119
Alberle, J.H. et al. (2005) Pediatr. Inf. Dis. J. 24:605-610.
Subbarao, E.K. et al. (1989) Diagn Microbiol. Infect. Dis. 12:327-332.
Drews, A.L. et al. (1997) Clin. Infect. Dis. 25:1421-1429.
Brunstein, J.D. et al. (2008) J. Clin. Microbiol. 46:97-102.

Clinical Significance of Co-infections Not Yet Clear
• Study #1 with N=229: Patients co-infected with rhinovirus
had less severe disease than those with non-rhinovirus
coinfections, without changes in influenza viral titer.
• Study #2 with N=566: Detection of multiple viruses
correlated with less severe disease.
• Study #3 with N=645: Did not confirm a significant
association between co-infection and ICU mortality.
Esper, FP et al., J. Infection (2011) doi:10.1016/j.jinf.2011.04.004
Martin, E.T. et al. (2011) Influ. & Other Resp. Viruses
DOI:10.1111/j.1750-2659.2011.00265.x.
Martin-Loechis, I. et al. (2011) Chest 139:555-562

Further Studies are Needed to Understand Co-infection
• Some reports suggest increased morbidity with co-infection,
while other studies report no increase in morbidity.
• Not all studies group by specific viral combinations in co-
infection. This may be partially responsible for difference in
results.
• Animal models: depending on specific combination, results
showed increased severity or viral interference
Esper, FP et al., J. Infection (2011) doi:10.1016/j.jinf.2011.04.004

How Many Viruses Should We Include?
Influenza A H1N1
Influenza A 2009 H1N1
Influenza A H3N2
Influenza B
RSV A
RSV B
Parainfluenza 1
Parainfluenza 2
Parainfluenza 3
Parainfluenza 4
Adenovirus
Metapneumovirus
Rhinovirus
Rhinovirus
Enterovirus
Coronavirus HKU1
Coronavirus NL63
Coronavirus 229E
Coronavirus OC43
Polyomavirus WU/K1
Parvovirus 4/5
Influenza C
Bocavirus
SARS Coronavirus
Influenza H5N1
CMV
HSV 27

Organisms Resistance Genes
Streptococcus pneumoniae mecA
Haemophilus influenzae blaTEM
Mycobacterium tuberculosois blaKPC
Moraxella catarrhalis blaVIM
Staphylococcus aureus blaIMP
Bordetella pertussis blaOXA
Mycoplasma pneumoniae
Chlamydophila pneumoniae
Chlamydophila psittaci
Legionella pneumophila
Pseudomonas aeruginosa
Enterobacteriaceae
Stenotrphomonas maltophilia
Acinetobacter spp.
Bacterial and Resistance Targets
to be Considered for Respiratory Disease Diagnosis
Adaped from: Tenover, F. (2011)
Clin. Inf. Dis. 52:S338-S345.

• Some studies support a correlation of more severe disease
with higher viral load, but other studies do not see a
correlation.
• Answer may be virus specific.
• Role of quantification is not yet clearly defined, particularly
for organisms that frequently colonize airways.
El Saleeby et al. (2011) J. Inf. Dis. 204:996-1002.
Utokaparch et al. (2011) Pediatr. Infect. Dis. 30:e18-e23.
Tregoning, J. S. et al. (2010) Clin. Micro. Rev. 23:74-98.
Fodha, I. et al. (2007) J. Med. Virol. 79:1951-1958.
Van Leeuwen, J.C. et al. (2012) Pediatr. Inf. Dis. J. 31:1-2.
Discrepant Result from Studies of Quantification

• Serum procalcitonin is increased with bacterial
infection and sepsis.
• Studies have identified gene expression profile
from peripheral blood to distinguish bacterial
from viral infection.
Gilbert, D.N. (2011) Clin. Inf. Dis. S346.
Amanatidou, V. et al. (2011) Crit. Rev. Immunol. 31:341-356.
Zaas et al. (2009) Cell Host Microbe 6:207-217.
Huang et al. (2011) PLoS Genet. 7:e1002234.
Biomarkers May Play a Role in Future
Diagnosis of Respiratory Infections

Severe Acute Respiratory Syndrome
•8096 cases reported
•774 deaths
•Case-fatality rate of 9.6%
Centers for Disease Control and Prevention
Molecular Testing Capabilities in More Labs
Provides Versatility
H5N1
•502 cases
•298 deaths
•Case fatality rate 59%
•14 countries
• With 2009 H1N1, hospital labs with molecular capabilities
were able to implement new assays very rapidly, relieving
the potentially overwhelmed public health labs.
• These capabilities will likely be valuable for the next outbreak
of an emerging virus.

Summary
(1) Factors to consider when implementing molecular testing:
- Cost of instrument and reagents
- FDA approval and Reimbursement
- Data on assay performance from good studies
- Turn-around-time decisions
- Expertise required for some assays
- Rapidly changing technology (buy or lease)
- List of viral targets to be included
- Ability to run other assays on same instrument
- Computer interface for reporting results
- Ability to subtype viruses on same platform
- Likelihood that additional improvements or additional targets will be made to current platform
- Availability of validation panel

Summary
(1) Xx
(2) Molecular testing of respiratory viruses has
definitely been beneficial for patient care,
especially in immunocompromised hosts.
(3) Laboratories must be able to adapt to newly
identified viruses, changing resistance patterns,
and rapidly evolving technologies for
identification of respiratory pathogens.

Self Assessment Questions
1. Describe three molecular diagnostic methods
used for the identification of respiratory viruses.
2. List four critical factors to consider when
choosing a respiratory virus testing platform for
a specific laboratory / institution.
2. Discuss three issues that a clinician must
consider when interpreting the results of the
respiratory virus testing as a treatment plan is
created.