Embed Size (px)
Citation preview

Blood Reviews (1997) 11,46-55 0 1997 Pearson Professional Ltd
State of the art
Monosomy 7 and 7q- associated with myeloid malignancy
E. Johnson, F. E. Cotter
An association between the complete or partial loss of chromosome 7 and preleukaemic myelodysplasia or acute myeloid leukaemia has been recognized from the early days of tumour cytogenetic analysis. Detection of such abnormalities usually heralds a poor prognosis. The loss of DNA on chromosome 7 has led to speculation that tumour-suppressor genes may play a significant role in this form of leukaemogenesis, although it may be part of a multistep process. A further association with leukaemia secondary to carcinogen exposure including previous chemotherapy or a number of congenital anaemias has increased the interest in discovering the gene or genes on chromosome 7. Banded chromosome analysis has suggested that there are two broad critical regions on the long arm of chromosome 7 at bands 7q22 and 7q34-q36 that may contain the relevant genes. Initial molecular analysis has confirmed these to regions to be of significance. The advent of fluorescence in-situ hybridization techniques has facilitated some definition of the 7q22 region, with identification of candidate genes for further functional analysis. It is becoming clear that there will be more than one gene on chromosome 7 involved in the leukaemic process and with the definition of these genes it may be possible to look for associations with different phenotypes and prognosis. As for the reason for chromosome 7 showing a particular predisposition to total or partial loss we may speculate that the DNA sequence and structure may confer a ‘fragility’ on the chromosome. A greater understanding of the DNA structure of the long arm may provide real insight into the mechanisms of leukaemia. We would like to speculate in the long term that this could lead to the ability to screen for leukaemia susceptibility and avoidance of ‘inducers’ in those at risk.
Monosomy 7 is one of the most frequent clonal chromosomal abnormalities associated with myelodysplasia (MDS) and the second most fre- quent numerical abnormality in acute myeloid leukaemia (AML).lm5 The first reports of monosomy 7 in association with myeloid disease date back to 1964 with Freireich’s report of three cases of
E. Johnson MRCP, F. E. Cotter PhD FRCP FRCPath, Molecular Haematology Unit, Institute of Child Health, London, UK.
Correspondence to: Dr Finbarr E. Cotter, Molecular Haematology Unit, Institute of Child Health, 30 Guilford Street, London WClN lEH, UK (Tel: +44(0)171 813 8191; Fax: (+44)(0)171 813 8100; E-mail: [email protected]).
refractory anaemia, granulocytic hyperplasia and a missing C group chromosome in marrow cells6 In this era (prior to chromosome banding), it is almost certain that these represented a chromosome 7 dele- tion. It is now established that there is a clear associ- ation between chromosome 7 alterations, MDS and AML in children and adults. The less well-estab- lished association with lymphoid malignancies is currently emerging. These changes may consist of long arm deletion (7q-) or total loss of the whole chromosome (monosomy 7) from bone marrow cells.1,4,7-25 The abnormalities occur in de novo MDUAML, in secondary cases following exposure to drugs, radiotherapy and toxins as well as
46

Monosomy 7 and 7q- associated with MDS 47
constitutional disorders including Fanconi’s anaemia, congenital neutropenia and neurofibro- matosis type 1. In all groups, the presence of chro- mosome 7 abnormalities defines a poor prognostic group. The majority of patients with MDS trans- form to a form of acute leukaemia resistant to ther- apy, including bone marrow transplantation (BMT). Fluorescence in situ hybridization (FISH) has accel- erated the study of these disorders at the cytogenetic and molecular levels.“,26s27 The loss of DNA associ- ated with malignant progression suggests the pres- ence of a tumour-suppressor gene (or genes) at these loci.28,29 No gene has been clearly implicated, although candidates have been suggested. The char- acterization of candidate genes is required to under- stand the mechanism of malignant transformation in these patients as it is not known, for example, whether both alleles of the putative suppressor gene need to be lost or whether loss of only one, i.e. gene dosage (haploinsufficiency), is more important. However, the loss of chromosome 7 material is almost certainly not the sole molecular abnormality. It is probable that this is not an initiating event, but occurs in cells already altered by a genetic event, per- mitting progression to clonal malignancy mediated by a gene on chromosome 7 as a secondary event.
CLASSIFICATION AND MANAGEMENT
A useful classification suggested originally for child- hood monosomy by Luna-Fineman3’ although not entirely applicable to the adult disease, is an applicable classification for monosomy 7 and MDS in general. The division into three broad groups is suggested. These are:
De novo disorders: primary MDS, primary AML, infant monosomy 7 syndrome (IMo7) and juvenile chronic myeloid leukaemia (JCML). The latter is distinct in that, although a primary form of childhood myelodysplasia, it is rarely associated with monosomy 7. Secondary disorders following therapy for previous malignancy or exposure through occupation or otherwise to toxic substances. Aplastic anaemia is also included in this group. Constitutional disorders, including Fanconi’s anaemia, Kostmann’s syndrome (severe congenital neutropenia), Shwachman’s syndrome, neurofibromatosis type 1, familial monosomy 7 and, occasionally, Down’s syndrome.
The classification groups are discussed in more detail below.
De novo disorders
MDS arising spontaneously with no predisposing factors may be classified as primary or de novo dis- ease. Clonal chromosome abnormalities occur in up to 79% of patients.23a3’ Trisomy 8, 5q-, monosomy 5, 7q-, monosomy 7 and 2Oq- are the predominant abnormalities. Chromosome 7 deletions occur at 7q22 and 7q32-36.5.20,23,‘2,33 Translocations involving chromosome 7 are unusual, although they have been reported in association with chromosome 1, result- ing in trisomy for lq and monosomy for 7q.23.3M8 A recent study highlighted 7q32 deletions as associ- ated with a particularly poor prognosis.39 Patients with monosomy 7/7q- will always do badly, no mat- ter which French-American-British (FAB) group is present.3i~4a~4i
Patients with monosomy 7 may present as classical MDS with abnormal erythroid, megakaryocyte and myeloid differentiation.8,4Z Monosomy 7 in lymphoid malignancy is unusuaP3 and lymphoblastoid cell lines from adults with 7q-/monosomy 7 retain heterozygos- ity for polymorphic markers on the long arm of chromosome 7.44 However, there are a few reports of monosomy 7 in lymphoid or biphenotypic leukaemias.24.45A’
Monosomy 7 in association with primary haemato- logical malignancy occurs in 40% of MDS and 7% of AML in children, while in adults the prevalence is lower, occurring in 14% of adult MDS and 10% adult AML.10-‘2~30~48-j’ Monosomy 7 is usually a single-chro- mosome change in children but in adults is usually accompanied by other complex chromosomal rear- rangements. With progression from MDS to AML, additional chromosomal abnormalities often occur. The age distribution is biphasic, with peak ages at 2-5 years and 60 years.3o No association with FAB groups32 occurs, although this classification is less applicable to children, in whom refractory anaemia with ring sideroblasts (RARS) is exceptionally rare, chronic myelomonocytic leukaemia (CMML) is more common, and two distinct groups, IMo7 and JCML, must be recognized. In childhood, unlike adulthood, there is a distinct male predominance (70-80%) of monosomy 7-associated MDS and AML.
Two conditions specific to young children deserve particular attention. JCML usually presents in boys aged 24 years, with characteristic facial and body rash, lymphadenopathy, hepatosplenomegaly, wasting and weight loss and typically with leucocytosis, thrombocytopenia, raised Hb F concentration (greater than 10%) and on bone-marrow morphology, features of CMML.‘3,54 Only 6% of JCMLs are reported to present with monosomy 7, although monosomy 7 may develop in association with

48 Blood Reviews
progression to acute leukaemia. IMo7 typically pre- sents at an even younger age range of 6 months-2 years. Pallor and bleeding due to anaemia and throm- bocytopenia occur. Infections and leucocytosis are even more common than in JCML. Hepatos- plenomegaly occurs, but unlike in JCML, the rash is not seen and Hb F is not raised. All have monosomy 7 with refractory anaemia with excess of blasts (RAEB) or CMML morphology. A significant review of 68 cases of childhood MDS reported 19 with JCML (none with chromosome 7 abnormalities), 12 with IMo7 and 5 others with chromosome 7 affected (3 CMML, 2 RAEB).lS
Secondary monosomy 7
This group consists principally of adults. Occupational exposure to pesticides, organic solvents and petroleum derivatives are described in association with monosomy 7 in adults.20,55-57 However, no epi- demiological studies linking chromosome 7 abnor- malities to such toxins in children have been reported. In childhood, secondary MDS is associated with cancer therapy.
At least 90% patients with therapy-induced MDS and AML (t-MDS and t-AML) have an abnormal karyotype and almost all of these have clonal aberra- tions affecting chromosomes 5 and 7 (-5, 5q-, -7, 7q-) .w* As with de novo disorders, trilineage dys- plasia occurs with transformation to AML almost inevitably. The prognosis even with treatment is very poor. Monosomy 7 is particularly associated with use of alkylating agents and radiotherapy, with the risks increasing with age and the dose of drug. The risk peaks at 3-7 years after the treatment.1~22~59 As a greater proportion of patients survive a primary malignancy, an increase in the number of such t-MDS and t-AML cases is predicted. This is most relevant to patients in their teens and 20s who have survived childhood cancer. t-MDS and t-AML occur in l-2% of children treated for cancer”’ and chromosome 7 is involved in up to 60% of cases.61 Most of these patients were exposed to alkylating agents. Chromosome 5 abnor- malities are observed in childhood cases but consider- ably fewer than in adult t-MDS and t-AML.
Aplastic anaemia has also been included in this sec- ondary group. A follow-up of 38 patients with severe aplastic anaemia (SAA) showed that 5 developed MDS/AML, 3 with chromosome 7 abnormalities that were not detected at presentation.62 In addition, an association between SAA patients treated with granu- locyte-colony stimulating factor (G-CSF) and the development of monosomy 7 MDS/AML has led to speculation that the cytokine may precipitate the lat- ter.63,” However, prolonged survival brought about by
the cytokine may be unmasking a dysplasia as part of the course of the disease if the patient survives long enough.
Constitutional disorders
Congenital bone-marrow disorders predispose to leukaemia, usually via a myelodysplastic phase with a high incidence of clonal change involving chromo- some 7. Monosomy 7 and 7q deletions in young chil- dren in association with congenital disorders, or as a familial condition, are particularly interesting in terms of the underlying molecular mechanisms. It is understandable that adults in their 5th-6th decades acquire genetic mutations in several critical genes and finally develop dysplasia with monosomy 7 at a rela- tively late age, as part of the ageing process. The occurrence in very young children is harder to explain in the light of the clear association of monosomy 7 in secondary MDWAML, suggesting that fetal toxin exposure may be important. The suspicion falls on inherited factors.65
Congenital neutropenia
The severe congenital neutropenias include congeni- tal agranulocytosis or Kostmann’s syndrome, which presents in early infancy with extremely low granulo- cyte counts and infections.@ G-CSF is very effective, raising granulocyte counts and improving symp- toms.67s68 Mutations in the G-CSF receptor gene69 have been reported. However, there is an association between this therapy and the development of MDS or AML with monosomy 7, occurring with equal sex incidence.63~70~7’ A few cases of MDS and AML are reported in children who have not received growth factors,30,72 although chromosome 7 was not impli- cated in those. It is still not clear whether G-CSF really contributes to the development of MDS, AML and monosomy 7 or whether these developments are part of the natural history of the disease. It may be that G-CSF is enabling children to survive longer and experience the natural progression of this disorder to acute leukaemia, analogous to aplastic anaemia.
Shwachman’s syndrome
Shwachman’s syndrome is a rare autosomal recessive disorder of exocrine pancreatic dysfunction, skeletal abnormalities with short stature and haematological abnormalities, especially neutropenia or pancytope- nia.73 Progression to MDS and AML in association with monosomy 7 is widely recognized and occurs more commonly in boys.74

Monosomy 7 and lq- associated with MDS 49
NeuroJibromatosis type 1 JNFl)
Neurofibromatosis type 1 (NFI) is the commonest autosomal dominant genetic disease in humans. The gene, on chromosome 17, has been characterized and identified as a tumour suppressor whose loss of function appears to be associated with a variety of tumours of neural crest origin.75 The NFl gene also predisposes to the development of malignant myeloid disorders, which have a prevalence higher than expected in children with NF1.76,77 The risk of any malignant myeloid disorder, including JCML, in children with NFl is increased 200-500 fold.53,78 Children with NFl and MDS/AML may have loss of heterozygosity for an NFl allele, losing the nor- mal allele and retaining the allele from the affected parent.79 Patients with NFl lack neurofibromin, the protein product of the NFl gene, which has sequence homology with GTPase-activating pro- teins (GAPS) which bind to and negatively regulate RAS, resulting in deregulated RAS activation. However, children with NFl and MDS/AML have a significantly increased incidence of monosomy 778 and those with NF-1 and JCML may acquire mono- somy 7 during the course of their disease.*O The triad of NFl, monosomy 7 and MDS/AML tends to occur in boys and, although initial evidence sug- gested maternal inheritance of NF1,78 there is now evidence that NFl is not imprinted in haematopoi- etic cells.79 The association between NFl and leukaemia seems to occur only in young children and not in adults.8’ Activating RAS mutations occur in 30% of adult MDS and one study shows this to be specific to patients with monosomy 7.82 RAS muta- tions are also observed in childhood monosomy 7 cases.*3 The evidenceg4 supports the tumour-suppres- sor role for the NFl gene in haematopoietic cells, with neurofibromin being a regulator of RAS in early myelopoeisis.” The coexistence of RAS activa- tion and monosomy 7 in MDS and the occurrence in boys with maternal inheritance of NFl, indicates that all these events may cooperate in the multistep process of leukaemogenesis.
Fanconi’s anaemia Fanconi’s anaemia (FA) is an autosomal recessive disorder characterized by pancytopnia, congenital anomalies, increased incidence of malignancy and spontaneous chromosome breakage.85 Leukaemia occurs in about 10% of FA patients and, of those with MDS or AML, 25% have chromosome 7 abnormali- ties.86-88 FA can be successfully treated by BMT, with 90% cured by allogeneic BMT but only if this occurs prior to the development of chromosome 7 abnormal- ities or leukaemic change.
Down’s syndrome
Down’s syndrome is associated with transient abnor- mal myelopoiesis (TAM), occurring in early infancy, and usually undergoes spontaneous remission. Some develop AML and the natural history of TAM is still unclear. The association with monosomy 7 is less widely recognized, with some studies confirming89-9’ and some excluding9’ its presence. However, one case of AML was shown, by FISH, to have the monosomy 7 clone affecting megakaryoblasts and not granulo- cytic cells9’ It is unlikely that the incidence of mono- somy 7 in Down’s syndrome AML is higher than in the general population.
Familial monosomy 7 The familial occurrence of bone-marrow monosomy 7 has been reported,‘2.93-99 but only in one generation, with equal sex incidence, with a higher age at diagno- sis compared to de novo cases and with no cases asso- ciated with consanguinity, so that the inheritance pattern is unclear. These patients have normal consti- tutional karyotypes with no abnormal chromosome breakage. Shannon proposed that a tumour-suppres- sor gene may be involved so that an inherited predis- position to cancer results from functional inactivation of one chromosome 7 allele, which is unmasked by loss of the normal chromosome 7 homologue. Familial cases would occur when siblings inherit the same abnormal allele (abnormality at the molecular level) on one chromosome 7 and then spontaneously lose the remaining protective homologous allele, in a haematopoietic progenitor cell developing 7q-lmono- somy 7 and hence deregulated growth and clonal expansion. In young children with non-familial monosomy 7, the first hit may occur in a parental gamete, during embryogenesis or even later after birth, again at the molecular level. A second hit then occurs spontaneously at a later stage resulting in loss of the 7q allele by deletion or monosomy. In cases of secondary MDS/AML, the first hit occurs following the toxic exposure and the second as above at a later stage. However, for this theory to be correct in familial cases, all siblings with monosomy 7 would have to share an abnormal allele on their remaining chromo- some 7, inherited from the same parent (similar to familial retinoblastoma). With currently available probes, using restriction fragment length polymor- phism (RFLP) analysis, this is not substantiated. Thus, the predisposing locus for familial monosomy 7 is not on the long arm of chromosome 7’oo,101 and must involve other genes not necessarily on chromosome 7. It is not altogether unexpected considering that, in contrast to the situation in retinoblastoma, where familial cases present earlier than non-familial cases,

50 Blood Reviews
children with familial monosomy 7 tend to be older than those with de novo disease.
Genomic imprinting is a phenomenon whereby expression of a gene depends on the parental origin of the abnormal allele, which is inactive because it is imprinted. Several malignancies, e.g. Wilms’ tumour, have an inactivated copy of the tumour-suppressor gene through imprinting and thus preferential retention of alleles from the same parent. However, in unrelated and related patients, there is no consistent evidence to support genomic imprinting in monosomy 7.‘02,‘03
TREATMENT
In general, treatment for all patients with monosomy 7 or 7q- is inadequate. This cytogenetic abnormality identifies a group of MDS patients who always do badly, compared with 5q- and trisomy 8. Response to standard chemotherapy is poor, with a low remission rate. Allogeneic or unrelated donor BMT is usually the only chance of cure.‘7.40*54,1~1a7 Eighty per cent of chil- dren with monosomy 7 and MDS die within 5 years of diagnosis due to infection, transformation to resistant AML or myelofibrosis. Increase in the percentage monosomy 7 clone in the marrow, i.e. clonal evolution, is associated with disease progression in children and
p ::
14
FISH Analysis 13 12 11
q 11
RFLP Analysis Patients with Deletions
ELN
4 2 Patients COLl A2 DLX5+6 21 COLiA2
Breakpoints ASNS
)22,, 4 7 Patients
TACP 22.2 EPO 22.
E::
EPO
ACHE ACHE PKANHl PLANHl CUTLl 3, CUTLl
MET 32 -- 33 34
35
4 3 Patients TCFibeta
4 2 Patients
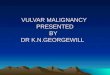
Fig. A schematic representation of chromosome 7 showing the current knowledge of molecular karyotype by RELP and FISH analysis. Sites of breakage and associated genes are indicated.
adultsI In contrast, rare cases in which complete disappearance of the monosomy 7 clone has been documented, suggest that cure is possible if the chro- mosome 7-bearing clone is eradicated.16 This highlights the importance of accurately following the cytogenetic characteristics of all MDS patients by bone marrow examination. Transformation to AML with monosomy 7 is almost always fatal as is de novo AML with mono- somy 7 at presentation.54 Some children and adults with apparent de novo AML have in fact experienced an undetected preleukaemic myelodysplastic phase with monosomy 7 developing during the progression to AML as retrospective studies have sometimes discov- ered.40 A prognostic scoring system for use in childhood MDS has been described. This is based on platelet count, HbF level and cytogenetic complexity (two or more clonal structural/numerical abnormalities), one point scored for each. A score of 0 gave 5-year survival of 61.6%, while a score of 2 or 3 resulted in 100% mortality by 5 years.”
MOLECULAR CYTOGENETICS OF CHROMOSOME 7 ALTERATIONS IN MDSlAML
Restriction fragment length polymorphism and karyotype analysis
Cytogenetic deletion mapping has shown that, in both AML and MDS, the chromosomes most commonly lost completely are 7 and Y, and that the region 7q22-36 is the extent of the deleted region in cases of partial loss on 7.5,20 7q22 and 7q32-34 represent the critical regions.4x22’44 Loss of heterozygosity (LOH) has been detected by RFLP analysis in 7 patients with 7q22 deletions (Fig.). The proximal breakpoints in these seven cases occurred between the genes for ery- thropoeitin (EPO), which was retained, and plasmino- gen activator inhibitor 1 (PLANHl), which was lost. More variability in the distal breakpoint at 7q34-35 is seen, which may or may not have involved the T-cell receptor beta (TCRB) gene. Another study using cos- mid probes has demonstrated two critical regions, a 2-3 Mb-deleted region in proximal band 7q22 in 2 CML patients and a second 20 Mb region encompass- ing the terminal 7q22 band and the entire 7q31 band, in MDS/AML.lo8 Deletions are usually interstitial with variability in both breakpoints.32,‘09-“’ Studies of patients with primary and therapy-related MDS/AML has shownthat those without a visible chromosome 7 abnormality do not have molecular LOH by RFLP analysis.“~“’ The absence of LOH for 7q22 alleles in JCML with normal cytogenetic karyotypes is notable.l12 A high proportion of secondary

MDS/AML have losses in the same regions as primary disorders suggesting that, in both, the same gene(s) may be involved in deregulated myeloid growth in association with chromosome 7 abnormalities. Loss of at least one normal copy of one of these genes may be a critical step. When homozygosity, as well as hemizy- gosity, of a specific chromosomal region is found for a particular type of cancer, the existence of a tumour- suppressor gene is suggested. In monosomy 7, it is still unclear whether simply loss of one whole gene with the other remaining normal, haploinsufficiency, is enough to cause disease or whether there needs to be an addi- tional mutation (or loss of function) on the remaining apparently healthy chromosome 7.
Fluorescence in situ hybidization
Most of the informative data are derived from adults. There are very few RFLP or FISH data from children because of the rarity of chromosome 7 deletions or other rearrangements as opposed to monosomy 7 in this group. However, it does support the involvement of the same critical regions as in adults. RFLP data and standard cytogenetic analysis generally agree in the detection of chromosome 7 abnormalities,“3 but these techniques have been boosted greatly by the introduction of FISH which, in patients with mono- somy 7, allows disease progression and response to treatment to be followed by estimating the proportion of interphase cells with only one chromosome 7. Interphase FISH can determine the percentage mono- somy 7 clone more accurately than metaphase analy- sis for several reasons. Far larger numbers of cells can be counted, many of which will be normal, but signif- icant monosomy 7 clones can be identified although missed by metaphase FISH, in which divisions may be of normal cells.““L17 However, patients without mono- somy 7 by standard or metaphase cytogenetics have not been shown to have a monosomy 7 clone by inter- phase FISH.“S Interphase FISH using chromosome 7- specific centromere probes would usually be performed in parallel with conventional cytogenetics, which is always the diagnostic gold standard. The ret- rospective study of fixed cell samples has shown the importance of karyotype evolution coincident with transformation to AML. FISH is useful to follow response to therapy, e.g. growth factors in MDS, and following BMT to detect relapse.
Newly available locus-specific cosmid and YAC probes have allowed more accurate definition of breakpoints in patients with MDS and chromosome 7 rearrangements.“’ A number of genes on chromo- some 7q may be important (Fig.), e.g. acetyl- cholinesterase (ACHE),l19 erythropoietin (EPO),12’ asparagine synthetase (ASNS),‘@ and NEDD2, an
Monosomy 7 and 7q- associated with MDS 51
apoptosis regulatory gene mapped to 7q34.12’ Others need to be identified and, with ‘chromosome walking’ techniques using new YAC, PAC (Pl artificial chro- mosome; a vector containing approx 100-150 kb of DNA and relatively easy to manipulate) and cosmid probes from this region, this should be possible.
Interphase FISH can also be combined with immunophenotyping using lineage-specific antibodies. Hence, CD-34 positive cells can be identified and sig- nals compared with those from normal lymphocytes. These experiments support previous data suggesting that the chromosome aberrations in MDS are usually restricted to myeloid lineage.‘2’,‘23 Whole chromosome paints allow the identification of the chromosome ori- gin of marker chromosomes, i.e. small fragments anonymous by standard cytogenetics. Not surpris- ingly, these are now widely reported in monosomy 7 patients.1’4s124 FISH will demonstrate the presence or absence of sequences incorporated within cosmid or YAC vectors and thus will help to define the minimum region of overlap in patients with deletions. Metaphase FISH is more accurate in this respect, although it is still difficult to obtain good-quality metaphase spreads from patient samples. Using whole chromosome paints, centromere probes and specific locus probes, translocations, inversions, ring chromosomes and dele- tions can be defined.27,‘25 The identification of probes that lie within a commonly deleted region on chromo- some 7 will also allow the identification of putative tumour-suppressor genes.26
It is to be hoped that recent developments will allow even more accurate assessment of tumour samples. Multiplex FISH involves the hybridization of up to 27 different DNA probes simultaneously, using a pool of chromosome paints each labelled with a different fluorochrome. This colour karyotyping can be readily applied to monosomy 7 and 7q- and perhaps used as a screening test on any new MDS or AML patient. If abnormalities are found, then conventional cytogenet- its and FISH can be used to define these further.lZ6
CONCLUSION
Summary
The role of chromosome 7 in abnormal haematopoei- sis is still far from clear. There is still a relative scarcity of published data on childhood MDS with mono- somy 7, making it difficult to compare with adult dis- ease. However, it appears that the same regions on chromosome 7 are involved. Constitutional and other genetic factors play an essential role in children, whereas toxic exposure is of greater importance in adults. The male predominance in de novo MDS in children, in cases associated with NFl and in

52 Blood Reviews
Shwachman’s syndrome but more equal sex incidence in Fanconi’s anaemia, Kostmann’s syndrome, familial monosomy 7 and in secondary cases suggest that the relationship with X-linked genes is complex.
Overall, submicroscopic loss of large segments of chromosome 7 DNA are uncommon in patients whose marrow does not show cytogenetically visible deletions. This still does not exclude small regions located between existing probes. All data suggest that chromosome 7 abnormalities are not the initiating event in MDS/AML. Additional genetic changes are certainly involved and ras-mediated signalling plays a significant role. It is likely that loss of function of a gene or genes on 7q contributes to leukaemic transfor- mation Although there is no direct evidence, the hap- loinsufficiency theory is perhaps more attractive, with loss of one whole gene resulting in half the amount of a critical protein and this resulting in the abnormal phenotype.12’ Possibly, both gene dosage and tumour- suppressor mechanisms can lead to the development of MDS and its transformation to AML. A multistep process in monosomy 7-associated disorders is con- ceivable. Our current knowledge of the molecular pathogenesis of MDS is. currently sketchy, but with the recent identification of candidate genes in chro- mosome 7 bands q22 and q32-34 should lead to a greater understanding.
REFERENCES
1. Rowley J, Golomb H, Vardiman J. Nonrandom chromosome abnormalities in acute leukemia and dysmyelopoietic syndromes in patients with previously treated malignant disease. Blood 1981, 58: 759-767.
2.Yunis JJ. Chromosomal defects are found in most patients with acute non-lymphocytic leukemia. Cancer Genet Cytogene 1984; 11: 1255137.
3. Fagan K, Gill A, Henry R, Wilkinson I, Carey B. A summary of 7q interstitial deletions and exclusion mapping of the gene for beta-glucuronidase. J Medical Genet 1989; 26: 619-625.
4. Fourth International Workshop on Chromosomes in Leukemia: Correlation of morphology and karyotype. Cancer Genet Cytogenet 1984; 11: 2499360.
5. Johansson B, Mertens F, Mitelman F. Cytogenetic deletion maps of hematologic neoplasms: circumstantial evidence for tumour suppressor loci. Genes Chromosomes Cancer 1993; 8: 2055218.
6. Freireich EJ, Whang J, Tjio JH, Levin RH, Brittin GM, Frei E. Refractory anemia, granulocytic hyperplasia of bone marrow and a missing chromosome in marrow cells. A new clinical syndrome? Cl& Res 1964; 12: 284.
7. Van Werine E. Kamus W. Vossen J. Van Der List-Nuver C. TheunissenP. Myelddysplastic syndromes in childhood: three case reports. Br J Haematol 1985; 60: 137-142.
8. Hogge D, Shannon K, Kalousek D et al. Juvenile monosomy 7 syndrome: evidence that the disease originates in a pluripotent hemopoietic stem cell. Leukem Res 1987; 11: 705-709.
9. Michiels J, Mallios-Zorbala H, Prins M, Hahlen K. Simple monosomy 7 and myelodysplastic syndrome in thirteen patients without previous cytostatic treatment. Br J Haematol 1986; 64: 425433.
10. Sieff C, Chessells J, Harvey A, Pickthall V, Lawler S. Monosomy 7 in childhood: a myeloproliferative disorder. Br J Haematol 1981; 49: 235-249.
11. Creutzig U, Cantu-Rajnoldi A, Ritter J et al. Myelodysplastic syndromes in childhood. Am J Pediatr Hematol Oncol 1987; 9: 324-330.
12. Brandwein J, Horsman D, Eaves A et al. Childhood myelodysplasia: suggested classification as myelodysplastic syndromes based on laboratory and clinical findings. Am J Pediatr Hematol Oncol 1990; 12: 63-70.
13. Hasle H, Jacobsen B, Pedersen N. Myelodysplastic syndromes in childhood: a population based study of nine cases. Br J Haematol 1992; 81: 495498.
14. Tuncer M, Pagliuca A, Hicsomnez G, Yetgin S, Ozsoylu S, Mufti G. Primary myelodysplastic syndrome in children: the clinical experience in 33 cases. Br J Haematol 1992; 82: 347-353.
15. Passmore SJ, Hann IM, Stiller CA et al. Pediatric myelodysplasia: a study of 68 children and a new prognostic scoring system. Blood 1995; 85: 1742-1750.
16. Weiss K, Stass S, Williams D et al. Childhood monosomy 7 syndrome: clinical and in vitro studies. Leukemia 1987; I:977104.
17. Guinan E, Tarbell N, Tantravahi R, Weinstein H. Bone marrow transplantation for children with myelosdsplastic svndromes. Br J Haematol 1989: 73: 619-622.
18. Baranger L, Baruchel A, Leverger G, Schaison G, Berger R. Monosomy-7 in childhood hemopoietic disorders. Leukemia 1990; 4: 3455349.
19. Daghistani D, Toledano S, Curless R. Monosomy 7 syndrome. Clinical heterogeneity in children and adolescents. Cancer Genet Cytogenet 1990; 44: 2633269.
20. Mitelman F, Nilsson PG, Brandt L, Alimena G, Gastaldi R, Dallapiccola B. Chromosome pattern, occupation and clinical features in patients with acute non-lymphocytic leukemia. Cancer Genet Cytogenet 1981; 4: 197-214.
21. Rowley JD. Chromosome changes in acute leukaemia. Br J Haematol 1980; 44: 339-346.
22. Le Beau M, Albain K, Larson R et al. Clinical and cytogenetic correlations in 63 patients with therapy-related myelodysplastic syndromes and acute nonlymphocytic leukemia: further evidence for characteristic abnormalities of chromosomes no 5 and 7. J Clin Oncoll986; 4: 325-345.
23.Yunis JJ, Rydell RE, Oken MM, Arnesen MA, Mayer MG, Lobe11 M. Refined chromosome analysis as an independent prognostic indicator in de novo myelodysplastic syndromes. Blood 1986; 67: 1721-1730.
24. Paietta E, Gucalp R, Wiernik P Monosomy 7 in multilineage and acute lymphoblastic leukaemia. Br J Haematol 1991; 79: 152-155.
25. Abrahamson G, Boultwood J, Madden J et al. Clonality of cell populations in refractory anaemia using combined approach, of gene loss and X-linked restriction fragment length polymorphism-methylation analyses. Br J Haematol 1991; 79: 550-555.
26. Le Beau MM, Espinosa III R, Neuman WL et al. Cytogenetic and molecular delineation of the smallest commonly deleted segment of chromosome 5 in malignant myeloid diseases. PNAS 1993; 90: 54845488.
27. Gibbons B, Lillington D, Monard S et al. Fluorescence in situ hybridisation studies to characterise complete and partial monosomy 7 in myeloid disorders. Genes, Chromosomes Cancer 1994; 10: 244249.
28. Seizinger BR, Klinger HP, Junien C et al. Report of the committee on chromosome and gene loss in human neoplasia. Cytogenet Cell Genet 1991; 58: 1080-1096.
29. Knudson AG. Hereditary cancer, oncogenes and antioncogenes. Cancer Res 1985; 45: 1437-1443.
30. Luna-Fineman S S K, Lange BJ. Childhood monosomy 7: epidemiology, biology, and mechanistic implications. Blood 1995; 85: 19851999.
31. Jacobs RH, Cornbleet MA, Vardiman JW, Larson RA, Le Beau MM, Rowley JD. Prognostic implications of morphology and karyotype in primary myelodysplastic syndromes. Blood 1986; 67: 1765-1772.
32. Kere J, Ruutu T, Davies K et al. Chromosome 7 long arm deletion in myeloid disorders: a narrow breakpoint region in 7q22 defined by molecular mapping. Blood 1989; 73: 230-234.

Monosomy 7 and 7q- associated with MDS 53
33. Kere J$ Donis-Keller H, Ruutu T. De la Chapelle A. Chromosome 7 long arm deletions in myeloid disorders: terminal DNA sequences are commonly conserved and breakpoints vary. Cytogenet Cell Genet 1989; 50: 226-229.
34. Scheres JMJC, Hustinx TWJ, Holdrinet RSG, Geraedts JPM, Hagemeijer A, van der Blij-Philipsen M. Translocation 1:7 in dyshaematopoiesis: possibly induced with a nonrandom geographic distribution. Cancer Genet Cytogenet 1984; 12: 283-294.
35. Scheres J, Hustinx T, Geraedts J, Leeksma C, Meltzer P Translocation 1;7 in hematologic disorders: a brief review of 22 cases. Cancer Genet Cytogenet 1985; 18: 207-213.
36. Stefanescu D, Colita D, Nicoara S, Calin G. t(1;7)(p36;q32): a new recurring abnormality in primary myelodysplastic syndrome. Cancer Genet Cytogenet 1994; 75: 103-105.
37.Pedersen B. Survival of patients with t(1;7)(pll;pll). Cancer Genet and Cytogenet 1992; 60: 53-59.
38. Smadja N, Krulik M, de Gramont A, Audebert AA, Debray J. Translocation 1;7 in preleukemic states, Cancer Genet Cytogenet 1985; 18: 189-192.
39. Velloso ERP, Michaux L, Ferrant A et al. Deletions of the long arm of chromosome 7 in myeloid disorders: loss of band 7q32 implies worst prognosis. Br J Haematol 1996; 92: 574581.
40. Yunis J, Lobe11 M, Arnesen M et al. Refined chromosome study helps define prognostic subgroups in most patients with primary myelodysplastic syndrome and acute myelogenous leukaemia. Br J Haematol 1988; 68: 1899194.
41. Parlier V, Van Melle G, et al. Beris P Hematologic, clinical and cytogenetic analysis in 109 patients with primary myelodysplastic syndrome. Cancer Genet Cytogenet 1994; 78: 219-231.
42. Kojima S, Mimaya J, Tonouchi T, Yokochi T, Kajitani S. Erythropoiesis during an erythrobmlastic phase of chronic myeloproliferative disorder associated with monosomy 7. Br J Haematol 1987; 65: 391-394.
43. Rowley JD. Chromosome abnormalities in acute lymphoblastic leukemia. Cancer Genet Cytogenet 1980; 1: 263-271.
44. Neuman W, Rubin C, Rios R et al. Chromosomal loss and deletion are the most common mechanisms for loss of heterozygosity from chromosomes 5 and 7 in malignant myeloid disorders. Blood 1992; 79: 1501-1510.
45.Chan L, Sheer D, Drysdale H, Bevan D, Greaves M. Monosomy 7 and multipotential stem cell transformation. Br J Haematol 1985; 61: 531-539.
46. Russo C, Carroll A, Kohler S et al. Philadelphia chromosome and monosomy 7 in childhood acute lymphoblastic leukemia: a pediatric oncology group study. Blood 1991; 77: 1050-1056.
47. van Lom K, Hagemeijer A, Smit EME, Hahlen K, Groeneveld K, Lowenberg B. Cytogenetic clonality analysis in myelodysplastic syndrome: monosomy 7 can be demonstrated in the myeloid and in the lymphoid lineage. Leukemia 1995; 9: 181881821.
48. Wegelius R. Bone marrow dysfunctions preceding acute leukemia in children: a clinical study. Leukemia Research 1992; 16: 71-76.
49. Blank J, Lange B. Preleukemia in children. J Pediatr 1981; 98:565-568.
50. Nowell P, Wilmoth D, Lange B. Cytogenetics of childhood preleukemia. Cancer Genet Cytogenet 1983; 261-266.
51. Mertens F, Johansson B, Mitelman F. Age- and gender-related heterogeneity of cancer chromosome abnormalities. Cancer Genet Cytogenet 1993; 70: 6-l 1.
52. Bennett J, Catovsky D, Daniel M et al. Group TF-A-BFc-0: proposals for the classification of the myelodysplastic svndromes. Br J Haematol 1982; 51: 1899199.
53. Castro-Malaspina H, Shaison G, Passe S et al. Subacute and chronic mvelomonocvtic leukemia in children (iuvenile CML). Cancer 1984; 54: 675:
54. Evans J, Czepulkowski B, Gibbons B; Swansbury G, Chessells J. Childhood monosomy 7 revisited. Br J Haematol 1988; 69: 41-45.
55. Cuneo A, Fagioli F, Pazzi I et al. Morphologic, immunologic and cytogenetic studies in acute myeloid leukemia following occupational exposure to pesticides and organic solvents. Leuk Res 1992; 16: 789.
56. Golomb HM, Alimena G, Rowley JD, Vardiman JW, Testa JR, Sovik C. Correlation of occupation and karyotype in adults with acute nonlymphocytic leukemia. Blood 1982; 60: 4041111.
57.Narod S, Dube I. Occupational history and involvement of chromosomes 5 and 7 in acute nonlymphocytic leukemia. Cancer Genet Cytogenet 1989; 38: 261-269.
58.PedersenBjergaard J, Philip P, Larsen S, Jensen G, Byrsting K. Chromosome aberrations and prognostic factors in therapy-related myelodysplasia and acute nonlymphocytic leukemia. Blood 1990: 76: 1083-1091.
59.Whang-Peng J. Young R, Lee E, Longo D, Schechter G, DeVita Jr V. Cytogenetic studies in patients with secondary leukemia/dysmyelopoietic syndrome after different treatment modalities. Blood 1988; 71: 4033414.
60. Pui C, Hancock M, Raimondi S et al. Myeloid neoplasia in children treated for solid tumours. Lancet 1990; 336: 417-421.
6 1. Rubin C, Arthur D, Woods W et al. Therapy-related myelodysplastic syndrome and acute myeloid leukemia in children: correlation between chromosomal abnormalities and prior therapy. Blood 1991; 78: 2982-2988.
62. De Planque MM, Kluin-Nelemans HC, van Krieken HJM et al. Evolution of acquired severe aplastic anaemia to myelodysplasia and subsequent leukaemia in adults. Br 3 Haematol 1988; 70: 55-62.
63. Imashuku S, Hibi S, Kataoka-Morimoto et al. Myelodysplasia and acute myeloid leukaemia in cases of aplastic anaemia and congenital neutropenia following G-CSF administration. Br J Haematol 1995; 89: 1888190.
64. Kojima S, Tsuchida M, Matsuyama T. Myelodysplasia and leukemia after treatment of aplastic anemia with G-CSF. NEJM 1992; 326: 1294.
65. Haber DA, Housman DE. Rate-limiting steps: the genetics of pediatric cancers. Cell 1991; 64: 5-8.
66. Kostmann R. Infantile genetic agranulocytosis. Acta Paediatr Stand 1975; 64: 362368.
67. Bonilla MA, Gillio AP, Ruggeiro M et al. Effects of recombinant human granulocyte colony-stimulating factor on neutropenia in patients with congenital agranulocytosis. N Engl J Med 1989; 320: 1574-1580.
68. Dale DC, Bonilla MA, Davis MW et al. A randomized controlled phase 111 trial of recombinant human granulocyte colony-stimulating factor (Filgrastim) for treatment of severe chronic neutropenia. Blood 1993; 81: 2496-2502.
69. Dong F, Brynes R, Tidow N, Welte K, Lowenberg B, Touw I. Mutations in the gene for the granulocyte colony-stimulating- factor receptor in patients with acute myeloid leukemia preceded by severe congenital neutropenia. NEJM 1995; 333: 487493.
70. Weinblatt ME, Scimeca P, James-Herry A, Sahdev I, Kochen J. Transformation of congenital neutropenia into monosomy 7 and acute nonlymphoblastic leukemia in a child treated with granulocyte colony-stimulating factor. J Pediatr 1995; 126: 263-265.
7 1. Zeidler C, Reiter A, Schafer 0, Urban C, Riehm H, Welte K. Is severe congenital neutropenia (SCN) a pre-leukemia condition? Med Pediatr Oncol 1992; 20: 445 (abstr).
72. Wong W, Williams D, Slovak ML. Terminal acute myelogenous leukemia in a patient with congenital apranulocvtosis. Am J Hematol 1993; 43: 133-138.
73. Svhwachman H, Diamond L, Oski F, Khaw K. The syndrome of pancreatic insufficiency and bone marrow dysfunction. J Pediatr 1964; 65: 645-663.
74. Woods W, Roloff J, Lukens J, Krivit W. The occurrence of leukemia in patients with the Shwachman syndrome. J Pediatr 1981; 99: 425428.
75. Seizinger BR. NFl: a prevalent cause of tumorigenesis in human cancers? Nature Genet 1993; 3: 97-99.
76. Bader JL, Miller RW. Neurofibromatosis and childhood leukemia. J Pediatr 1978; 92: 925-929.

54 Blood Reviews
77. Stiller CA, Chessells JM, Fitchett M. Neurofibromatosis and childhood leukaemia/lymphoma: a population-based UKCCSG study. Br .I Cancer 1994; 76: 9699972.
78. Shannon KM, Watterson J, Johnson P et al. Monosomy 7 myeloproliferative disease in children with neurofibromatosis, type 1: epidemiology and molecular analysis. Blood 1992; 79: 1311-1318.
79. Shannon KM, O’Connell P, Martin GA et al. Loss of the normal NFl allele from the bone marrow of children with type 1 neurofibromatosis and malignant myeloid disorders. NEJM 1994; 330: 5977601.
80. Kaneko Y, Maseki N, Sakurai M. Chromosome pattern in juvenile chronic myeloid leukaemia, myelodysplastic syndrome and acute leukaemia associated with neurofibromatosis. Leukemia 1989; 3 : 3641.
Sl.Riccardi VM, Eichner JE. Neurofibromatosis. Johns Hopkins: Baltimore, MD, 1986.
82. Stephenson .I, Lizhen H, Mufti GJ. Possible co-existence of Ras activation and monosomy 7 in the leukaemic transformation of myelodysplastic syndromes. Leukemia Res 1995; 19: 741-748.
83. Neubauer A, Shannon KM, Liu E. Mutations of the ras proto- oncogenes in childhood monosomy 7. Blood 1991; 77: 594598.
84. Bollag G, Clapp DW, Shih S et al. Loss of NFl results in activation of the Ras signaling pathway and leads to aberrant growth in haematopoietic cells. Nature Genet 1996; 12: 144-148.
85. Fanconi G. Familial constitutional panmyelocytopathy, Fanconi’s anemia (FA). I. Clinical aspects. Semin Hematol 1967; 4: 233-240.
86. Auerbach A, Allen R. Leukemia and preleukemia in Fanconi anemia patients. Cancer Genet Cytogenet 1991; 51: l-12.
87. Berger R, Le Coniat M, Schaison G. Chromosome abnormalities in bone marrow of Fanconi anemia patients. Cancer Genet Cytogenet 1993; 65: 47-50.
88. Stivrins T, Davis R, Sanger W, Fritz J, Purtilo D. Transformation of Fanconi’s anemia to acute nonlymphocytic leukemia associated with emergence of monosomy 7. Blood 1984; 64: 173-176.
89. Hecht F, Hecht B, Morgan R, Sandberg A, Link M. Chromosome clues to acute leukemia in Down’s syndrome. Cancer Genet Cytogenet 1986; 21: 93.
90. Bunin N, Nowell P, Belasco J et al. Chromosome 7 abnormalities in children with Down syndrome and preleukemia. Cancer Genet Cytogenet 1991; 54: 119-126.
91.Ziaurskv A. Thorner P. De Harven E. Christensen H. Dovle J. Mielodysplasia and acute megakaryoblastic leukemia in * Down’s syndrome. Leukemia Res 1994; 18: 163-17 1.
92. Kaneko Y, Rowley JD, Variakojis D, Chilcote RR, Moohr m, Pate1 D. Chromosome abnormalities in Down’s syndrome patients with acute leukemia. Blood 1981; 58: 459-466.
93. Carroll WL, Rodman Morgan MS, Glader BE. Childhood bone marrow monosomy 7: a familial disorder? J Pediatr 1985; 107: 578-580.
94. Gilchrist D, Friedman J, Rogers P, Creighton S. Myelodysplasia and leukemia syndrome with monosomy 7: a genetic perspective. Am J Med Genet 1990; 35: 437441.
95. Kamiyama R, Shibata T, Mori W. Two autopsy cases of atypical myeloproliferative disorder with group C monosomy occurring in siblings. Acta Path01 Jpn 1973; 23: 815. -
96. Larsen WE. Schimke RW. Familial acute mvelonenous leukemia with associated C-monosomy in two ageected members. Cancer 1976; 38: 841.
97. Li FP, Hecht F, Kaiser-McCaw B, Baranko PV, Potter NU. Ataxia-pacytopenia syndrome of cerebellar ataxia, hypoplastic anemia, monosomy 7, and acute myelogenous leukemia. Cancer Genet Cytogenet 1981; 4: 189.
98.Paul B, Reid MM, Davison EV, Abela M, Hamilton PJ. Familial myelodysplasia: progressive disease associated with emergence of monosomy 7. Br J of Haematol 1987; 65: 321-323.
99. Chitambar CR, Robinson WA, Glode LM. Familial leukemia and aplastic anemia associated with monosomy 7. Am J Med 1983; 75: 756-762.
100. Shannon KM, Turhan AG, Chang SSY et al. Familial bone marrow monosomy 7. J Clin Invest 1989; 84: 984989.
101. Shannon KM, Turhan AG, Rogers PCJ, Kan YW. Evidence implicating heterozygous deletion of chromosome 7 in the pathogenesis of familial leukaemia associated with monosomy 7. Genomics 1992; 14: 121-125.
102. Katz F, Webb D, Gibbons B et al. Possible evidence for genomic imprinting in childhood acute myeloblastic leukaemia associated with monosomy for chromosome 7. Br J Haematol 1992; 80: 332-336.
103. Savage P, Frenck R, Paderanga D, Emporer J, Shannon K. Parental origins of chromosome 7 loss in childhood monosomy 7. Leukemia 1994; 8: 485.
104. Appelbaum FR, Storb R, Ramberg RE et al. Allogeneic marrow transplantation in the treatment of preleukemia. Ann Intern Med 1984; 100: 689-693.
105. Borgstrom G, Teerenhovi L, Vuopio P et al. Clinical implications of monosomy 7 in acute nonlymphocytic leukemia. Cancer Genet Cytogenet 1980; 2: 115-126.
106. Sanders J, Buckner C, Thomas E et al. Allogeneic marrow transplantation for children with juvenile chronic myclogenous leukemia. Blood 1988; 71: 11441146.
107. Appelbaum F, Storb R, Ramberg R et al. Treatment of preleukemic syndromes with marrow transplantation. Blood 1987; 69: 92-96.
lOS.Fischer K, McAllister Brown J, Scherer SW et al. Molecular cytogenetic delineation of deletions and translocations involving chromosome band 7q22 in myeloid leukemias. Blood 1996; 88 (suppl 1): 65a.
109. Kere J. Chromosome 7 long arm deletion breakpoints in preleukemia: mapping by pulsed field gel electrophoresis. Nucleic Acids Res 1989; 17: 1511-1520.
110. Kere J, Ruutu T, Lahtinen R, de la Chapelle A. Molecular characterisation of chromosome 7 long arm deletions in myeloid disorders. Blood 1987; 70: 134991353.
111 .Lewis S, Abrahamson G, Boultwood J, Fidler C, Potter A, Wainscoat JS. Molecular characterization of the 7q deletion in myeloid disorders. Br J Haematol 1996; 96: 75-80.
112. Butcher M, Frenck R, Emperor J, Paderanga D, Maybee D, Shannon K. Molecular evidence that childhood monosomy 7 syndrome is distinct from juvenile chronic myelogenous leukemia and other childhood myeloproliferative disorders. Genes, Chromosomes Cancer 1995; 12: 50.
113. Abrahamson G, Rack K, Oscier D, Fitchett M, Buckle V, Wainscoat J. Comparison of cytogenetic and restriction fragment length polymorphism analses for the detection of loss of chromosomal material in clonal hemopoietic disorders. Am J Hematol 1993; 42: 171-176.
114. Zhao L, Van Oort J, Cork A, Liang J. Comparison between interphase and metaphase cytogenetics in detecting chromosome 7 defects in hematological neoplasias. Am J Hematol 1993; 43: 205-211.
115. Kibbelaar R, Mulder J, Dreef E et al. Detection of monosomy 7 and trisomy 8 in myeloid neoplasia: a comparison of banding and fluorescence in situ hybridization. Blood 1993; 82: 904-913.
116. Bentz M, Dohner H, Cabot G, Lichter P, Fluorescence in situ hybridization in leukemias: ‘The FISH are spawning!‘. Leukemia 1994; 8: 1447-1452.
117. Kolluri RV, Manuelidis L, Cremer T, Sait S, Gezer S, Raza A. Detection of monosomy 7 in interphase cells of patients with myeloid disorders. Am J Haematol 1990; 33: 117-122.
118. Johnson EJ, Scherer SW, Osborne L et al. Molecular definition of a narrow interval at 7q22.1 associated with myelodysplasia. Blood 1996; 87: 3579-3586.
119. Stephenson J, Czepulkowski B, Hirst W, Mufti GJ. Deletion of the acetylcholinesterase locus at 7q22 associated with myelodysplastic syndromes (MDS) and acute myeloid leukaemia (AML). Leukemia Res 1996; 20: 2355241.
120. Law ML, Cai G-Y, Lin F-K et al. Chromosomal assignment of the human erythropoietin gene and its DNA polymorphism. PNAS 1986; 83: 6920.

Monosomy 7 and 7q- associated with MDS .%
121.Kumar S, White D, Takai S, Turczynowicz S, Juttner C, Hughes T. Apoptosis regulatory gene NEDD2 maps to human chromosome segment 7q34-35, a region frequently affected in haematological neoplasms. Hum Genet 1995; 95: 641-644.
122,Kibbelaar R, Mulder J, Van Kamp H et al. Nonradioactive in situ hybridisation of the translocation t(1;7) in myeloid malignancies. Genes, Chromosomes Cancer 1992; 4: 128-134.
123. Gerritsen W, Donohue J, Bauman J et al. Clonal analysis of myelodysplastic syndrome: monosomy 7 is expressed in the myeloid but not in the lymphoid lineage as detected by fluorescent in situ hybridization. Blood 1992; 80: 217-224.
124. Baurmann H, Cherif D, Berger R. Interphase cytogenetics by fluorescent in situ hybridization (FISH) for characterization of monosomy-7 associated mycloid disorders. Leukemia 1993; 7: 384391.
125. Johansson B, Arheden K, Hoglund M et al. Fluorescence in situ hybridization analysis of whole-arm 7; 12 translocations in hematologic malignancies. Genes, Chromosomes Cancer 1995; 14: 56-62.
126. Le Beau MM. One FISH, two FISH, red FISH, blue FISH. Nat Genet 1996; 12: 341-344.
127. Fisher E, Scambler P. Human haploinsufficiency - one for sorrow, two for joy. Nat Genet 1994; 7: 5-7.