Embed Size (px)
Citation preview

Mood, Alertness, and Performance in Response to Sleep Deprivation andRecovery Sleep in Experienced Shiftworkers Versus Non-Shiftworkers
Sophie M. T. Wehrens,1 Shelagh M. Hampton,1 Myriam Kerkhofs,2 and Debra J. Skene1
1Centre for Chronobiology, Faculty of Health and Medical Sciences, University of Surrey, Guildford, UK, 2Sleep Laboratory, CHUde Charleroi, Hôpital Vésale, Université Libre de Bruxelles, Montigny-le-Tilleul, Belgium
Previous studies have shown increased sleepiness and mood changes in shiftworkers, which may be due to sleepdeprivation or circadian disruption. Few studies, however, have compared responses of experienced shiftworkersand non-shiftworkers to sleep deprivation in an identical laboratory setting. The aim of this laboratory study,therefore, was to compare long-term shiftworkers and non-shiftworkers and to investigate the effects of one nightof total sleep deprivation (30.5 h of continuous wakefulness) and recovery sleep on psychomotor vigilance, self-rated alertness, and mood. Eleven experienced male shiftworkers (shiftwork ≥5 yrs) were matched with 14 non-shiftworkers for age (mean ± SD: 35.7 ± 7.2 and 32.5 ± 6.2 yrs, respectively) and body mass index (BMI) (28.7 ± 3.8and 26.6 ± 3.4 kg/m2, respectively). After keeping a 7-d self-selected sleep/wake cycle (7.5/8 h nocturnal sleep), bothgroups entered a laboratory session consisting of a night of adaptation sleep and a baseline sleep (each 7.5/8 h), asleep deprivation night, and recovery sleep (4-h nap plus 7.5/8 h nighttime sleep). Subjective alertness and moodwere assessed with the Karolinska Sleepiness Scale (KSS) and 9-digit rating scales, and vigilance was measured bythe visual psychomotor vigilance test (PVT). A mixed-model regression analysis was carried out on data collectedevery hour during the sleep deprivation night and on all days (except for the adaptation day), at .25, 4.25, 5.25, 11.5,12.5, and 13.5 h after habitual wake-up time. Despite similar circadian phase (melatonin onset), demographics, foodintake, body posture, and environmental light, shiftworkers felt significantly more alert, more cheerful, more elated,and calmer than non-shiftworkers throughout the laboratory study. In addition, shiftworkers showed a faster medianreaction time (RT) compared to non-shiftworkers, although four other PVT parameters did not differ between thegroups. As expected, both groups showed a decrease in subjective alertness and PVT performance during andfollowing the sleep deprivation night. Subjective sleepiness and most aspects of PVT performance returned tobaseline levels after a nap and recovery sleep. The mechanisms underlying the observed differences betweenshiftworkers and non-shiftworkers require further study, but may be related to the absence of shiftwork the weekprior to and during the laboratory study as well as selection into and out of shiftwork. (Author correspondence:[email protected])
Keywords: Alertness, Mood, Psychomotor vigilance test, Recovery sleep, Shiftwork, Sleepiness, Vigilance
INTRODUCTION
Although sleep deprivation results in decreased levels ofalertness, a recent meta-analysis showed that the largesteffects of 24- to 48-h total sleep deprivation (TSD)were ob-served on simple attention, such as lapses and reactiontime (Lim & Dinges, 2010). Sleep deprivation has alsobeen shown to impact mood (Pilcher & Huffcutt, 1996),but which aspects of mood are affected is less clear-cut.Evidence for these statements comes from laboratorystudies showing that reaction times, lapse frequency, andsubjective sleepiness increased, and some, but not all,negative aspects of mood worsened after one night ofTSD (Dinges et al., 1994; Doran et al., 2001; Franzen
et al., 2008; Jay et al., 2007; Pagani et al., 2009; Zhonget al., 2005), multiple nights of TSD (Gould et al., 2009;Kahn-Greene et al., 2007; Lamond et al., 2007), or partialsleep deprivation (PSD) (Axelsson et al., 2008; Buxtonet al., 2010; Dinges et al., 1997; Faraut et al., 2010; Haack& Mullington, 2005; Sallinen et al., 2008; Spiegel et al.,1999; Van Dongen et al., 2003; Vgontzas et al., 2004).These studieshave also indicated that the length anddistri-bution of recovery sleep and the type of mood, alertness,and performance assessed influence to what extent theeffects of sleep deprivation can return to baseline levels.
Both acute and chronic sleep deprivation, as well asthe need to work during the circadian trough of the
This paper was presented at the 20th International Symposium on Shift Work andWorking Time, Stockholm, Sweden, 28 June to 1 July 2011.
Address correspondence to Sophie M. T. Wehrens, PhD, Centre for Chronobiology, Faculty of Health and Medical Sciences, University ofSurrey, Guildford, Surrey GU2 7XH, UK. Tel.: +44 (0) 1483 689705; E-mail: [email protected]
Chronobiology International, 29(5): 537–548, (2012)Copyright © Informa Healthcare USA, Inc.ISSN 0742-0528 print/1525-6073 onlineDOI: 10.3109/07420528.2012.675258
Chr
onob
iol I
nt D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y Fr
anci
s A
Cou
ntw
ay L
ibra
ry o
f M
edic
ine
on 0
9/04
/13
For
pers
onal
use
onl
y.

alertness rhythm, are major causes of increased sleepi-ness in shiftworkers (Åkerstedt, 1998, 2003; Åkerstedt &Wright, 2009; Costa, 2003). Research has mainlyfocused on subjective alertness, vigilance, and generalwell-being of shiftworkers on different shift schedules(Härmä et al., 1998, 2006; Sallinen et al., 2005) and lesson differences between shiftworkers and non-shiftwor-kers. Reports on laboratory findings or specific aspectsof mood, such as depression, cheerfulness, and calm-ness, are rarer than information on sleepiness andgeneral health, but some studies have compared specifictypes of mood in different shifts systems (Cavallo et al.,2002; Folkard et al., 1990) or in simulated shift schedules(Kirkpatrick et al., 2009; Smith et al., 2009). There are alsoonly a few reports describing vigilance and mood differ-ences between shift- and non-shiftworkers, justifyingthe current study. A meta-analysis indicated, however,that shiftworkers have a higher odds ratio for depressionthan dayworkers (Driesen et al., 2010), and these authorsand others (Costa et al., 2006) have suggested that thisassociation may be related to high job demand, lowcontrol over shiftwork schedules, and inflexible workinghours. In addition, individual differences may play arole in coping strategies, and the strain of shiftworkmay be modified by factors such as morningness/even-ingness, age, flexibility of sleeping habits (Adan et al.,2010; Härmä, 1993; Kitamura et al., 2010; Nachreiner,1998), and genetics (Saksvik et al., 2011). These factorsas well as social conditions can, in turn, affect circadianadjustment and sleep, although their validity to predictshiftwork tolerance is not yet proven. Prediction and as-sessment of shiftwork tolerance is likely to impact on se-lection into and out of shiftwork, which, in turn, mayinfluence research outcomes on differences betweenshift- and non-shiftworkers (Knutsson, 2004).
To the authors’ knowledge, no previous studies haveassessed the effects of sleep deprivation and recoverysleep on mood, alertness, and vigilance in shiftworkerswhen tested in a controlled laboratory setting. Inaddition, shift- and non-shiftworkers have not been com-pared directly when both are subjected to the same sleepdeprivation and recovery conditions. The aim of thisstudy, therefore, was to investigate whether shiftworkersare more tolerant to sleep deprivation than non-shiftwor-kers with respect to alertness, mood, and psychomotorvigilance test (PVT) performance. In addition, the studyaimed to investigate whether shiftworkers recoverfaster from sleep deprivation than non-shiftworkers. Itwas hypothesized that group differences in theseresponses (alertness, mood, PVT performance) wouldbe observed.
METHODS
Details of the study protocol have been previously pub-lished (Wehrens et al., 2010, 2011). Procedures specificfor the assessment of wakefulness, subjective mood,alertness, and PVT performance are presented briefly.
Participants and ScreeningAll study procedures were conducted in accordance withthe guidelines by Portaluppi et al. (2010) and approvedby The University of Surrey Ethics Committee. Volunteerinformation was coded and held securely in compliancewith the Data Protection Act (1998). All participants gavewritten informed consent.
Screening and the laboratory study were carried out inthe Clinical Investigation Unit (CIU) at the University ofSurrey, the latter occurring between July and February.Male shiftworkers and non-shiftworkers (age range 25–45 yrs) were recruited, and the two groups werematched for age, body mass index (BMI), and cholesterolduring the screening. Demographics of both groups areshown in Table 1. Shiftworkers were required to have acumulative shiftwork history of ≥5 yrs (preferably con-tinuous), working either permanent nights or rotatingshifts with at least three night shifts/mo. All applicantscompleted a general health questionnaire and four vali-dated questionnaires (Wehrens et al., 2010). Buccalswabs (Epicentre Biotechnologies, supplied by Cambio,Cambridge, UK) were collected from all participantsprior to the laboratory study and were genotyped forPER3 according to an established protocol (Archeret al., 2003), with some modifications by Vandewalleet al. (2009). Volunteers were free of any medical con-ditions and medication (including over-the-countermedication) known to affect sleep, alertness, andmood. They did not consume >15 units of alcohol/wkand were nonsmokers. Past smoking behavior wassimilar in both groups (Table 1). Habitual caffeine con-sumption (mean ± SD) was also not significantly differentin shiftworkers (3 ± 2.3 cups/d) and non-shiftworkers(1.7 ± 1.5 cups/d). All subjects were negative for drugsof abuse at the time of recruitment and during thestudy, as confirmed by a urine screen.
Pre-Laboratory SessionIn order to establish entrained circadian rhythms, volun-teers kept a standard self-selected regular sleep/wakecycle (nocturnal sleep duration of 7.5 or 8 h) for 8 dprior to the laboratory study, as confirmed by voicemailmessages, actigraphy, and sleep diaries (Wehrens et al.,2010). Two days prior to the laboratory study, participantswere required to abstain from heavy exercise and sub-stances that affect sleep, alertness, and mood, such asalcohol and caffeine.
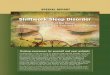
Laboratory SessionVolunteers spent four nights in the CIU (Figure 1). After anight of adaptation sleep and a night of baseline sleep,equal to the self-selected sleep/wake cycle during theweek prior to the laboratory study (sleep duration of 7.5or 8 h), subjects were required to stay awake for 30.5 huntil their 4-h recovery nap. The nap was included inthe protocol as a proxy for a real night shift and subsequentsleep taken by shiftworkers. This nap was followed by noc-turnal recovery sleep. During wake time, subjects were
S. M. T. Wehrens et al.
Chronobiology International
Chr
onob
iol I
nt D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y Fr
anci
s A
Cou
ntw
ay L
ibra
ry o
f M
edic
ine
on 0
9/04
/13
For
pers
onal
use
onl
y.

continuallymonitored by staff. In order to control for inter-individual differences in circadian phase, all interventionsand measurements were scheduled relative to each par-ticipant’s self-selected wake-up time, used as a proxy forcircadian phase (Burgess et al., 2003). Post-hoc determi-nation of dim-light salivary melatonin onsets (DLMOs)and phase angles between melatonin onset and bedtimeconfirmed that circadian phase and entrainment werenot significantly different between shift- and non-shiftwor-kers (Wehrens et al., 2011).
Body posture was controlled throughout the study.During the sleep periods, sleep deprivation, and the 4-h
periods each afternoon, subjects were asked to remain ina semirecumbent position in bed. All subjects onlyreceived the same standard meals and were allowedwater ad libitum throughout the study. The entire studywas conducted in constant temperature (20°C) and dimlight (<8 lux in the direction of gaze apart from the sleepperiods, 0 lux). Light levels were regularly checked witha calibrated lux meter (Edmund Optics, York, UK).
Assessment of WakefulnessContinuous polysomnographic (PSG) recordings wereperformed from 20:00 h on d 1 until after the last PVT
FIGURE 1. Laboratory study protocol. The diagram shows the five study days for an individual with sleep from 23:00 to 07:00 h. All inter-ventions (see key) were relative to each subject’s self-selected wake-up time.
TABLE 1. Characteristics of non-shiftworkers and shiftworkers prior to the start of the laboratory study
Non-shiftworkers (n = 14) Shiftworkers (n = 11)
Mean ± SD Range Mean ± SD Range
Shiftwork (yrs) .03 ±.11 0–.42 8.7 ± 5.2*** 5–18.5Time since last shift (mo) 60 1.6 ± 5.4 0–18Age (yrs) 32.5 ± 6.2 25–42 35.7 ± 7.2 25–45Weight (kg) 83.7 ± 13.5 67.8–109 91.6 ± 10.3 82–117Height (m) 1.77 ± .06 1.66–1.85 1.79 ± .07 1.71–1.91BMI (kg/m2) 26.6 ± 3.4 21.5–34.0 28.7 ± 3.8 23–35.7Waist circumference (cm) 91.2 ± 9.4 76–107 98.0 ± 6.7 90–110Hip circumference (cm) 100 ± 7.4 88–114 106 ± 6.2 95–114WHR .91 ± .04 .84–.96 .93 ± .03 .86–.98Cholesterol (mmol/L) 4.7 ± .5 3.9–5.5 4.9 ± 1.1 3–6.5HDL (mmol/L) 1.3 ± .2 .8–1.6 1.4 ± .4 .9–2.4PER34/4 (n) 10 5PER34/5 (n) 3 5PER35/5 (n) 1 1HÖ 60.2 ± 6.0 51–72 55.5 ± 13.0 34–60.2PSQI 3.9 ± 1.9 1–7 5.1 ± 2.2 2–3.9BDI 3.3 ± 3.0 0–9 4.7 ± 4.9 0–3.3ESS 4.9 ± 3.2 1–11 6.2 ± 3.3 2–4.9Past smoked (units/d) 3.6 ± 5.8 0–15.5 4.5 ± 5.7 0–15Smoking duration (yrs) 2.6 ± 4.4 0–14 4.4 ± 6.3 0–20Time since last smoked (mo) 17.9 ± 24.1 .5–60 38.4 ± 54.1 0–132Bedtime (decimal h) 23.3 ± .4 22.5–24 23.4 ± .6 22–24Wake-up time (decimal h) 7.2 ± .5 6–8 7.2 ± .6 5.5–8Time-in-bed (decimal h) 7.9 ± .2 7.5–8 7.9 ± .2 7.5–8
***p < .001 compared to non-shiftworkers by independent two-tailed t test. Bed- and wake-up times refer to the self-selected times the weekprior to the laboratory study.BDI = Beck’s Depression Inventory; BMI = body mass index; ESS = Epworth Sleepiness Scale; HÖ =Horne-Östberg questionnaire; PER3 =PERIOD3 gene; PSQI = Pittsburgh Sleep Quality Index.
Shiftworkers and Sleep Deprivation
© Informa Healthcare USA, Inc.
Chr
onob
iol I
nt D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y Fr
anci
s A
Cou
ntw
ay L
ibra
ry o
f M
edic
ine
on 0
9/04
/13
For
pers
onal
use
onl
y.

on d 5 in order to assess vigilance states according to therecommended guidelines of the American Academyof Sleep Medicine (AASM) (Iber et al., 2007). Therecommended derivations were applied for the electro-encephalogram (EEG) (occipital O1 and O2, central C3and C4, and frontal F3 and F4 referenced to mastoid A1and A2) and electrooculogram (EOG). The electromyo-gram (EMG) involved two electrodes placed 2 cm belowthe inferior edge of the mandible. All electrodes wereconnected to an ambulatory system (Siesta EEG/PSGrecorder; Compumedics, Abbotsford, Victoria, Australia),and signals were continuously recorded at 256 Hz withProFusion PSG 2 (version 2.1 build 134; Compumedics).The acquired data were converted into EuropeanData Format (EDF) and imported into SomnologicaStudio (version 5.0.1 build 1662; Embla, suppliedby Stowood Scientific Instruments, Oxford, UK) forfurther analysis.
PSG recordings were visually analyzed from habitualbedtime on the baseline day, throughout the sleep depri-vation night, until the start of the nap after TSD (compris-ing a period of 14.4 ± .3 h [mean ± SD], n = 25, apart from3.5% ± 2.8% data loss due to logistic or technical issues).To determine the extent of sleep/wakefulness duringTSD, recordings were scored for wake and unintentionalnon-rapid eyemovement sleep (NREM) stage 1, NREM 2,NREM 3, and rapid eye movement sleep (REM) accord-ing to AASM criteria. Subsequently, total sleep time(TST), time until the first unintentional sleep episode de-termined from the conventionally used sleep onsetlatency (SOL; time until the first occurrence of 60 s ofconsecutive sleep stages), number of awakenings fromthese sleep episodes (>30 s of wakefulness), andaverage sleep bout length (TST divided by the numberof awakenings + 1 for the final awakening) were calcu-lated. TST, time spent in NREM 1, NREM 2, NREM 3,and REM were also calculated as a percentage of thetotal scoring time.
Alertness and MoodSubjective alertness and mood were assessed at .25, 4.25,5.25, 7, 8, 9, 11.5, 12.5, and 13.5 h following adaptationsleep, baseline sleep, the TSD night, and recovery sleep(Figure 1). During the TSD night, alertness and moodassessments were carried out every hour, starting 16 hafter habitual wake time. Alertness, mood, and vigilance(PVT) were not assessed 7, 8, and 9 h after habitual waketime on the TSD day due to the scheduled nap. Subjectivealertness and mood were assessed by the KarolinskaSleepiness Scale (KSS) (Åkerstedt & Gillberg, 1990) aswell as 9-digit rating scales with only descriptions forthe extreme values (1 = “very alert” to 9 = “very sleepy”;1 = “very cheerful” to 9 = “very miserable”; 1 = “verycalm” to 9 = “very tense”; and 1 = “very depressed” to 9= “very elated”) (Lockley et al., 2008).
Vigilant attention was assessed by visual PVT (Ambu-latory Monitoring, Ardsley, NY, USA) after the subjectivealertness and mood ratings (Dinges & Powell, 1985) in 10
non-shiftworkers and 9 shiftworkers. The first six partici-pants having completed both the auditory and visual PVTwere not included in the PVT analysis (n = 19). Althoughthe PVT is assumed to have only a small learning effect(Kribbs & Dinges, 1994), all subjects performed a “prac-tice trial” to familiarize themselves with the test. Datawere downloaded using PVTcommW (Version 2.10.1.1)and analyzed using REACT (Version 1.1.05). For each10-min epoch, the following performance indices werecalculated: reciprocal reaction time/10-min epoch (1/RT or RRT), median RT, slowest 10% RTs/10-min epoch(SRT), fastest 10% RTs/10-min epoch (FRT), and thenumber of lapses (i.e., RT ≥500 ms). All settings for PVTtesting and analysis were done according to themanufacturer’s settings.
Statistical AnalysisAlertness, mood, and vigilance assessments during theTSD night and during the daytime were analyzed bymixed-model regression analysis (SAS 9.1, TS level1M3; SAS Institute, Chicago, IL, USA). The data of assess-ments done during the daytime were analyzed separatelyfrom those of the TSD night (16.5–23.6 h after waking).The model determined main effects (“group” and“time,” and “day”) and interactions between these maineffects. To locate post-hoc differences between daysand time points, least squares means were calculatedand t-type confidence limits were constructed for eachof the least squares means (Bonferroni-corrected formultiple comparisons). All data were analyzed omittingthe adaptation day and the afternoon measurements (i.e., those 7, 8, and 9 h after wake-up time), as the imbal-ance in these measurements after TSD, baseline, and re-covery sleep did not make post-hoc tests for the maineffects and day × group interactions possible.
RESULTS
Assessment of WakefulnessPolysomnography (PSG) confirmed that subjects wereawake, on average, >95% of the sleep deprivation (TSD)period. The amount and architecture of theunintentional sleep is shown in Table 2. No significantdifferences were observed between shift- and non-shiftworkers in any of the PSG parameters. There were,however, large interindividual differences in the subjects’ability to stay awake (TST [mean ± SEM, range] was 35 ±8 min, 7–83 min versus 29 ± 7 min, 0–74 min in shift- andnon-shiftworkers, respectively). The average sleep boutlength was ≈2 min, showing that subjects who had alonger TST did not necessarily sleep longer but fell inand out of sleep more often.
Subjective Alertness and Mood
Comparison of Shiftworkers and Non-ShiftworkersSubjective alertness and mood are shown in Figure 2.There was a significant effect of group for both the KSS
S. M. T. Wehrens et al.
Chronobiology International
Chr
onob
iol I
nt D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y Fr
anci
s A
Cou
ntw
ay L
ibra
ry o
f M
edic
ine
on 0
9/04
/13
For
pers
onal
use
onl
y.

and 9-digit scale for alertness (F1,408 = 10.9, p < .01 andF1,408 = 6.4, p < .05, respectively), (Table 3A) revealingthat shiftworkers felt more alert than non-shiftworkersthroughout the laboratory study. Shiftworkers were alsosignificantly more cheerful (F1,408 = 14.8, p < .001), moreelated (F1,408 = 28.4, p < .001), and calmer (F1,408 = 14.4,p < .001) than the non-shiftworkers (Table 3A).
Effect of Sleep DeprivationAssessment of subjective alertness and mood during thesleep deprivation night (analyzed separately from thedaytime measurements) also showed that all subjectiveparameters were significantly different between shift-and non-shiftworkers, with the former feeling lesssleepy according to the KSS (F1,178 = 5.5, p < .05) and
FIGURE 2. Subjective alertness and mood. (A) KSS and 9-digit scale scores for (B) alertness, (C) cheerfulness, (D) calmness, and (E)depression (mean ± SEM) in non-shiftworkers (•) (n = 14) and shiftworkers (○) (n = 11) .25, 4.25, 5.25, 11.5, 12.5, and 13.5 h after habitualwake time following baseline sleep, sleep deprivation, and recovery sleep. Clock times are for an individual with sleep from 23:00 to 07:00 h.Gray bars indicate the sleep deprivation night, black bars the baseline and recovery night. Note y-axis scales differ between graphs.
TABLE 2. Sleep parameters during the sleep deprivation night in non-shiftworkersand shiftworkers
Non-shiftworkers(n = 14) mean ± SEM
Shiftworkers (n = 11)mean ± SEM
TST (min) 29 ± 7 35 ± 8SOL (min) 370 ± 41 263 ± 51Number of awakenings 18 ± 4 19 ± 5Average sleep bout length (min) 1.6 ± .3 2.2 ± .5TST (%) 3.7 ± .8 4.5 ± .9NREM 1 (%) 2.4 ± .5 2.9 ± .7NREM 2 (%) 1.3 ± .4 1.1 ± .2NREM 3 (%) .1 ± 0 .5 ± .2REM (%) 0 .04 ± .04
Percentages are relative to total scoring time.NREM= unintentional non–rapid eye movement sleep; REM = rapid eye movement sleep; SOL =time until the first occurrence of 60 s of consecutive sleep stages; TST = total sleep time.
Shiftworkers and Sleep Deprivation
© Informa Healthcare USA, Inc.
Chr
onob
iol I
nt D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y Fr
anci
s A
Cou
ntw
ay L
ibra
ry o
f M
edic
ine
on 0
9/04
/13
For
pers
onal
use
onl
y.

9-digit scale (F1,178 = 5.8, p < .05), and more cheerful(F1,178 = 12.5, p < .001), elated (F1,178 = 10.2, p < .01), andcalm (F1,178 = 9.0, p < .01) (Figure 2, Table 3B).
In both shift- and non-shiftworkers, mood did notchange throughout the TSD night (Table 3B). However,a significant effect of time on the KSS score (F7,178 = 6.3,p < .001) and the 9-digit score for alertness (F7,178 = 7.4,p < .001) was observed during the TSD night (Figure 2,Table 3B), caused by the expected increase in sleepinessthroughout the night. Moreover, the KSS and alertnessratings showed significant effects of day (F2,408 = 49.5,p < .001 and F2,408 = 47.2, p < .001, respectively), time(F5,408 = 4.7, p < .001 and F5,408 = 8.5, p < .001, respectively),and day × time interactions (F10,408 = 5.7, p < .001 andF10,408 = 8.1, p < .001, Table 3A respectively) throughoutthe laboratory study (Figure 2, Table 3A). Post-hoc ana-lyses of these day × time interactions showed subjects’daytime sleepiness was highest (both KSS and alertnessratings) the morning following TSD (.25, 4.25, and 5.25 hafter habitual wake time) than at any other time pointduring the day. Cheerfulness, calmness, and depressionratings did not worsen significantly after sleep deprivation.
Speed of RecoveryThe nap and recovery sleep enabled recuperation ofalertness levels in both groups, as there were no signifi-cant differences in the KSS score and 9-digit score for
alertness after either the nap or recovery sleep comparedto after baseline sleep when the same time points werecompared. Furthermore, there was a trend for an effectof day (F2,408 = 2.8, p = .06) on depression ratings withsubjects feeling less depressed after recovery sleep thanafter TSD and baseline sleep ( p = .07). There was also asignificant effect of day (F2,408 = 13.8, p < .001) and aday × time interaction (F10,408 = 1.9, p < .05) for cheerful-ness. Subjects felt significantly more cheerful at almostany time after recovery sleep compared to after TSD (at.25, 4.25, and 5.25 h) and at the last time point (13.5 h)after recovery sleep compared to all but one (5.25 hafter recovery sleep, p = .07) other time point. Except forthe last time point (13.5 h) after recovery sleep, therewere no significant differences between the assessmentsafter either the nap or recovery sleep and baseline sleep.
PVT Performance
Comparison of Shiftworkers and Non-ShiftworkersAll PVT parameters at all time points are shown Figure 3.Comparison of the daytime measurements showed a sig-nificant group effect for median RT (F1,303 = 7.5, p < .01),with a faster median RT in shift- compared to non-shift-workers. The four other PVT parameters (RRT, lapses,SRT, and FRT) did not differ between the two groups(Table 3A).
FIGURE 3. Psychomotor vigilance performance. (A) RRT, (B) median RT, (C) number of lapses, (D) SRT, and (E) FRT (mean ± SEM) in non-shiftworkers (•) (n = 10) and shiftworkers (○) (n = 9) .35, 4.35, 5.35, 11.6, 12.6, and 13.6 h after habitual wake time following baseline sleep,sleep deprivation, and recovery sleep. Clock times are for an individual with sleep from 23:00 to 07:00 h. Gray bars indicate the sleep depri-vation night, black bars the baseline and recovery night.
S. M. T. Wehrens et al.
Chronobiology International
Chr
onob
iol I
nt D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y Fr
anci
s A
Cou
ntw
ay L
ibra
ry o
f M
edic
ine
on 0
9/04
/13
For
pers
onal
use
onl
y.

Effect of Sleep DeprivationDuring the sleep deprivation night, none of the PVT par-ameters showed a significant group effect nor time ×group interaction (Table 3B).
Throughout the TSD night, significant increases wereobserved for median RT (F7,134 = 2.6, p < .05), mean SRT(F7,134 = 3.2, p < .01), and number of lapses (F7,134 = 3.4,p < .01) in both groups. A decrease in mean RRT
(F7,134 = 4.0, p < .001) was observed, but FRT did notchange throughout the TSD night (Table 3B). Through-out the laboratory study, FRT showed a significant effectof day (F2,303 = 9.7, p < .001) and time (F5,303 = 2.3, p< .05) (Figure 3, Table 3A). FRTs were significantlylonger after TSD compared to after baseline sleep. Inaddition, a significant effect of day was observed formedian RT (F2,303 = 15.6, p < .001) (Table 3A), with
TABLE 3 A. F and p values for main effects and interactions for all mood, alertness, and vigilance parameters at six time points/d across thethree study days
Mood and alertness
Degrees offreedom for allparameters KSS Alert Cheerful Calm Depressed
Effect Num df Den df F p F p F p F p F p
Day 2 408 49.5 < .0001 47.2 < .0001 13.8 < .0001 .9 .3994 2.8 .0635Time 5 408 4.7 .0003 8.5 < .0001 1.8 .1054 .1 .9899 .8 .5668Group 1 408 10.9 .0011 6.4 .0118 14.8 .0001 14.4 .0002 28.4 < .0001Day × Time 10 408 5.7 < .0001 8.1 < .0001 1.9 .0445 .6 .8065 .5 .8837Day × Group 2 408 .8 .4458 0 .9977 1.2 .2965 .8 .4583 .2 .7832Time × Group 5 408 .9 .4861 .3 .8966 .1 .9932 .3 .9222 .2 .9732Day × Time × Group 10 408 .3 .9849 .3 .9708 1.2 .2747 .6 .7884 .3 .9786
Vigilance
Degrees offreedom for allparameters RRT Median RT Lapses SRT FRT
Effect Num df Den df F p F p F p F p F p
Day 2 303 28.5 < .0001 15.6 < .0001 28.6 < .0001 20.0 < .0001 9.7 < .0001Time 5 303 3.1 .0091 1.7 .1242 3.7 .0028 3.7 .0029 2.3 .0416Group 1 303 1.9 .1655 7.5 .0067 1.5 .2267 .6 .4417 1.9 .1644Day × Time 10 303 3.3 .0004 1.7 .0885 5.0 < .0001 4.7 < .0001 .8 .6369Day × Group 2 303 1.9 .1574 2.9 .0563 2.0 .1369 .6 .5689 1.3 .2646Time × Group 5 303 .1 .9972 .2 .9670 .3 .8866 .3 .9018 .3 .9022Day × Time × Group 10 303 .4 .9548 .4 .9430 .4 .9424 .1 .9994 .5 .8733
Lapses were defined as reaction time ≥500 ms.Den = denominator; Num = numerator; df = degrees of freedom; FRT = fastest 10% RTs/10-min epoch; KSS = Karolinska Sleepiness Scale;median RT =median reaction time; RRT = reciprocal reaction time; SRT = slowest 10% RTs.
TABLE 3 B. F and p values for main effects and interactions for all mood, alertness, and vigilance parameters throughout the sleepdeprivation night
Mood and alertness
Degrees offreedom for allparameters KSS Alert Cheerful Calm Depressed
Effect Num df Den df F p F p F p F p F p
Time 7 178 6.3 < .0001 7.4 < .0001 .3 .9476 .1 .9956 .2 .9890Group 1 178 5.5 .0197 5.8 .0174 12.5 .0005 9.0 .0030 10.2 .0017Time × Group 7 178 .6 .7324 .7 .6372 1.0 .4702 .2 .9810 .2 .9793
Vigilance
Degrees offreedom for allparameters RRT Median RT Lapses SRT FRT
Effect Num df Den df F p F p F p F p F p
Time 7 134 4.0 .0006 2.6 .0140 3.4 .0024 3.2 .0038 1.8 .0953Group 1 134 .5 .4779 1.8 .1876 .0 .9224 1.8 .1809 .9 .3481Time × Group 7 134 .3 .9432 .2 .9831 .4 .9216 .8 .6037 .3 .9456
Lapses were defined as reaction time ≥500 ms.Den = denominator; Num = numerator; df = degrees of freedom; FRT = fastest 10% RTs/10-min epoch; KSS = Karolinska Sleepiness Scale;median RT =median reaction time; RRT = reciprocal reaction time; SRT = slowest 10% RTs.
Shiftworkers and Sleep Deprivation
© Informa Healthcare USA, Inc.
Chr
onob
iol I
nt D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y Fr
anci
s A
Cou
ntw
ay L
ibra
ry o
f M
edic
ine
on 0
9/04
/13
For
pers
onal
use
onl
y.

significantly slower median RTs after TSD compared toafter baseline sleep. Furthermore, significant effects ofday, time, and day × time interactions were found forRRT (F2,303 = 28.5, p < .001; F5,303 = 3.1, p < .01; andF10,303 = 3.3, p < .001, respectively), mean SRT (F2,303 =20, p < .001; F5,303 = 3.7, p < .01; and F10,303 = 4.7, p< .001, respectively), and lapses (F2,303 = 28.6, p < .001;F5,303 = 3.7, p < .01; and F10,303 = 5.0, p < .001, respect-ively) (Table 3A). Post-hoc tests revealed a significant in-crease in the SRT and lapses and a decrease in RRT inthe morning (.35, 4.35, and 5.35 h) after a night of TSDcompared to all but a few other time points (seebelow). No additional significant differences werefound post hoc when the same time pointswere compared.
Speed of RecoveryThe absence of a day × time interaction for median RTand FRT indicated that these RT variables remainedslower after the nap than after the baseline sleep. Theeffects of day, however, revealed a significantly fastermedian RT and FRT after recovery sleep compared toafter TSD, and no significant differences after recoverysleep compared to after baseline sleep. Post-hoc testsshowed that SRT and lapse values at 5.35 h after recoverysleep were not significantly different from such values at5.35 h after TSD or from ones 5.35 h after baseline sleep.
Correlation Between Subjective Alertness and PVTPerformanceTherewere no significant correlations between subjectivesleepiness (KSS) and objective vigilance (median RT)across the study period, except at two points during thesleep deprivation night, namely 21 h after waking innon-shiftworkers ( p < .05) and 16.6 h after waking inshiftworkers ( p < .05) (data not shown).
DISCUSSION
Comparison of Shiftworkers and Non-ShiftworkersThroughout the sleep deprivation night and during thedaytime measurements, shiftworkers felt more alertaccording to the KSS and alertness ratings compared tothe non-shiftworkers. PVT parameters, however, showedno significant differences between the groups during theTSD night, but shiftworkers had significantly fastermedian RTs than non-shiftworkers throughout the study.During the study, shiftworkers were also more cheerful,moreelated, andcalmercompared to thenon-shiftworkers.
Since there were no significant group differences incircadian phase, as assessed by the DLMO (Wehrenset al., 2011), or in the sleep parameters during TSD, theobserved group differences in alertness and mood areunlikely to be a result of circadian and sleep changes.The fact that the current study did not investigate theacute effects of being in a shift but rather comparedmatched shift- and non-shiftworkers when subjected tosleep deprivation in the laboratory (where other
circumstances such as job demand and effects onsocial life were not present) may explain why the in-creased sleepiness and negative mood previously ob-served within groups of shiftworkers or in comparisonwith dayworkers (Åkerstedt & Wright, 2009; Driesenet al., 2010; Kaliterna et al., 2004) were not found in thecurrent study. Our findings, however, are in agreementwith previous studies that have suggested that it may bethe lack of flexibility aspect of shiftwork that affects irrit-ability, anxiety, and depression (Ahlberg et al., 2004;Costa et al., 2006), rather than circadian disruption orsleep deprivation, itself. The findings may also indicatethat keeping a regular sleep/wake cycle the week beforethe laboratory study could have improved the shiftwor-kers’ mood and alertness, for example, by minimizingcumulative sleep disruption. Furthermore, it could bethat when rating their sleepiness and mood comparedto previously experienced work situations, the shiftwor-kers were relatively more positive. Their shiftwork experi-ence may also have taught them how to deal with lack ofsleep. Another plausible explanation for the observeddifferences between the shift- and non-shiftworkersmay be selection into and out of shiftwork, rather thanthe long-term consequences of shiftwork, themself.Primary selection into shiftwork of those who rate them-selves as being more tolerant to shiftwork can influencethe outcome of studies (Boggild, 2009) and may explainthe present findings. Along the same lines, it may bethose individuals who are least affected by shiftworkand sleep deprivation, which is determined by factorssuch as age, sex, and various personality characteristics(Saksvik et al., 2011), who continue in shiftwork(Knutsson, 2004). Interestingly, dissatisfied shiftworkerswith a higher habitual sleep need and lower sleep flexi-bility have been reported to feel sleepier than satisfiedshiftworkers on work days (especially during morningand afternoon shifts), but not after recovery sleep, indi-cating that dissatisfied workers may be more sensitiveto restricted sleep and less able to cope with shiftwork(Axelsson et al., 2004). Reaction times or lapses,however, were not significantly affected by job satisfac-tion in this study (Axelsson et al., 2004). Shiftworkers ofthe current studymay thus be thosewho feel they can tol-erate sleep deprivation fairly well. Van Dongen (2006),however, noted that there was still interindividual vari-ation in flight-simulator performance in a self-selectedgroup of F-117 pilots.
These differences between groups and individualscould also be related to genotype; for example, poly-morphisms in the human clock genes, such asPERIOD3, and in genes involved in the adenosinergicsystem, such as adenosine deaminase, have beensuggested to be associated with the vulnerability to sleepdeprivation (King et al., 2009; Retey et al., 2005; Violaet al., 2007). In the current study, the traditional compari-son between PER34/4 and PER35/5 genotypes (Archeret al., 2003; Viola et al., 2007) was not possible becauseof the low number of PER35/5 genotypes detected.
S. M. T. Wehrens et al.
Chronobiology International
Chr
onob
iol I
nt D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y Fr
anci
s A
Cou
ntw
ay L
ibra
ry o
f M
edic
ine
on 0
9/04
/13
For
pers
onal
use
onl
y.

Relationship Between Subjective Sleepiness and VigilanceGroup differences in alertness and mood parametersoccurred throughout the laboratory study, whereasgroup differences in PVT performance were onlyobserved in the median RT and mainly after sleep depri-vation and recovery sleep. The explorative analysis of thecorrelation between subjective alertness (KSS) and objec-tive vigilance (median RT) failed to show any significantcorrelations in the majority of time points. The data,therefore, suggest that sleep deprivation does not resultin the loss of capability to judge one’s own alertness.The current findings, rather, indicate that there is nopattern in the correlation between an individual’ssubjective alertness and objective vigilance. This is inagreement with previous studies that have shown discre-pancies between vigilance or neurobehavioral perform-ance and subjective alertness (Franzen et al., 2008; Freyet al., 2004; Galliaud et al., 2008; Van Dongen et al.,2004a, 2004b), the only exception being when the KSSwas administered during the PVT and the within-PVT cor-relation was determined (Horne & Burley, 2010). It is notclear as to why there would be a poor correlationbetween subjective sleepiness and PVT performance.One possible reason could be that different brain areasor downstream pathways are involved in each of thesebehaviors. A second explanation could be that the corre-lation is dependent on the specific parameters comparedas well as the study conditions (Yang et al., 2004).
Effect of Sleep DeprivationNot surprisingly, an increase in sleepiness (KSS and 9-digit alertness scale), median RT, mean SRT, and lapsefrequency and a decrease in mean RRT were observedacross the night of sleep deprivation. This increase inRT, lapse frequency, and sleepiness may be part of therising phase of the circadian rhythms observed in subjec-tive and objective alertness that has been shown todisplay a maximum deterioration around the body temp-erature minimum (Cajochen et al., 1999, 2001; Dijk et al.,1992; Graw et al., 2004; Kline et al., 2010; Lee et al., 2009;Wyatt et al., 1999). However, there were no significantchanges in the mood parameters during the TSD night,although previous studies have demonstrated a circadianrhythm in mood with a trough around the temperatureminimum (Boivin et al., 1997; Kline et al., 2010).
When the daytime measurements (.25/.35 to 13.5/13.6 h after habitual wake time following TSD) were ana-lyzed, the KSS, alertness, SRT, lapses, and RRT demon-strated that subjects felt less alert and were less vigilantin the morning after sleep deprivation than at any othertime point. Both median RT and FRT were slower afterTSD compared to after baseline sleep and recoverysleep. These observations were not surprising and arein agreement with previous studies showing that alert-ness and vigilance are decreased after TSD (Gouldet al., 2009; Jay et al., 2007; Kahn-Greene et al., 2007)and PSD (Axelsson et al., 2008; Cohen et al., 2010;Dinges et al., 1997; Faraut et al., 2010; Mollicone, et al.,
2010; Sallinen et al., 2008; Vgontzas et al., 2004). Thetime course of changes in PVT parameters across thebaseline day and the sleep deprivation night was alsosimilar to that observed in other studies, with a fairlystable performance up to 16 h after habitual wake timeand deterioration beyond this point (Cajochen et al.,1999; Dijk et al., 1992; Urrila et al., 2007).
The current study also showed that mood was largelyunaffected by sleep deprivation. Most studies have alsoshown deteriorations in some aspects of mood andinconsistent results within a subtype of mood (e.g.,depression) after TSD (Kahn-Greene et al., 2007) andPSD (Dinges et al., 1997; Haack & Mullington, 2005),and in sleep-deprived compared to non-sleep-deprivedsubjects (Franzen et al., 2008).
Effect of the NapThe first recovery period after the TSD night was the sched-uled 4-h nap. The data indicated that the nap was able topartly reverse the increased sleepiness after TSD, as therewere no significant differences in evening alertness andvigilance after the nap compared to the evening of thebaseline day. This finding is in agreement with reportsthat a nap is beneficial (Dinges et al., 1987; Gillberg et al.,1996). FRT and median RT, however, showed a maineffect of day, with an increase after TSD compared withafter baseline sleep. Therefore, recuperation by the napcannot be assumed for these parameters. Alternatively, asignificant increase in sleepiness in the morning afterTSD, but not after the nap, could also be due to circadianmodulation of the effects of sleep deprivation (Cohenet al., 2010; Lee et al., 2009; Mollicone et al., 2010).
Effect of Recovery SleepThe recuperative effect of the nap, however, may be tem-porary, and, therefore, it was of interest to assess theeffect of recovery sleep. The effectiveness of recoverysleep also appeared to depend on the parametermeasured. For example, subjective sleepiness andmedian RT and FRT showed full recuperation after recov-ery sleep. Other PVT parameters (SRT and lapses) werealso not significantly different from baseline scores norfrom TSD at time point 5.35 h, suggesting a slower recov-ery process for SRT and lapses. Previous studies have alsoindicated that the length and distribution of recoverysleep and the aspect of mood, alertness, and perform-ance assessed influence the return of those levels to base-line. For one night to be sufficient to recover subjectivealertness and PVT performance levels to those prior toa night of (partial) sleep deprivation, at least 9-h timein bed (Faraut et al., 2010; Jay et al., 2007), but not 8 h(Sallinen et al., 2008), was needed. However, a 10-hnight was insufficient to recover from five nights ofpartial sleep restriction (4-h time in bed) (Banks et al.,2010), whereas two recovery nights were sufficient(Dinges et al., 1997). Moreover, different aspects of alert-ness and performance may not recover at the same rate(Lamond et al., 2007).
Shiftworkers and Sleep Deprivation
© Informa Healthcare USA, Inc.
Chr
onob
iol I
nt D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y Fr
anci
s A
Cou
ntw
ay L
ibra
ry o
f M
edic
ine
on 0
9/04
/13
For
pers
onal
use
onl
y.

Study LimitationsThe fact that several PVTparameterswere derived from thesame assessment tool may increase the risk for false posi-tives. The observation that the PVT findings pointed in thesame direction, however, supports the validity of the find-ings. Furthermore, group differences (mainly in the moodscales) thatmay have existed at baselinemake it difficult todrawconclusions about the effects of sleepdeprivationandrecovery sleep per se. Another point to note is that despiteintensivemonitoringbystaff, subjects fell asleepduring theTSD night. Unintentional sleep has also occurred in pre-vious studies that aimed to achieve TSD to assess moodand alertness (Cajochen et al., 1999; Urrila et al., 2007).Except for a few studies (Faraut et al., 2010; Kerkhofset al., 2007; Stenuit & Kerkhofs, 2005), however, moststudies on sleep deprivation do not report polysomno-graphic sleep (or only report sleep during the plannedsleep episode) (Dinges et al., 1997; Vgontzas et al., 2004).Most importantly, in the current study subjects were re-quired to lie very still for at least 20 min in the morningduring ultrasound recordings (Wehrens et al., 2011), andthe entire study was conducted in dim light (<8 lux),which would exacerbate sleepiness, in contrast to otherstudies (Faraut et al., 2010; Urrila et al., 2007; Vgontzaset al., 2004). The absence of significant group differencesin sleep architecture during the sleep deprivation night,however, suggests that the unintentional sleep episodesdo not account for the differences found between thedays and between both groups. Finally, the current studyonly examined the effect of a single night of sleep depri-vation. The effect of sleep deprivation and the recoveryprocess is likely to be different when sleep deprivation isprolonged and/or partial sleep deprivation is studied.
CONCLUSION
In conclusion, when experienced shiftworkers were com-pared to non-shiftworkers in identical settings (e.g., withsimilar circadian phase, physical activity, food intake, andlight exposure), shiftworkers were more alert and hadhigher mood scores throughout the laboratory protocol.Shiftworkers also had faster median reaction times com-pared to the non-shiftworkers. The present analyses,however, were not able to distinguish the shiftworkers’better tolerance to sleep deprivation from an overallmore positive attitude and increased alertness. The ob-served group differences could be due in part to the elim-ination of shiftwork the week prior to and during thelaboratory study as well as shiftwork selection, leavingmostly individuals who can tolerate shiftwork and sleepdeprivation. These group differences and the relation-ships between different alertness and vigilance par-ameters require further investigation.
ACKNOWLEDGMENTS
This work was supported by an EU Marie Curie ResearchTraining Network grant (CT-2004-512362), 6th
Framework project EUCLOCK (018741), and StockgrandLtd., University of Surrey, Guildford, UK. The authorswould like to thank researchers and staff at the Universityof Surrey for their help, especially Dr. Simon Archer forassistance with the PER3 genotyping, and Mr. Peter Wil-liams for statistical advice.
Declaration of Interest: The authors report no conflictsof interest. The authors alone are responsible for thecontent and writing of the paper.
REFERENCES
Adan A, Natale V, Caci H, Prat G. (2010). Relationship betweencircadian typology and functional impulsivity. Chronobiol. Int.27:606–619.
Ahlberg J, Nikkila H, Kononen M, Partinen M, Lindholm H, Sarna S,Savolainen A. (2004). Associations of perceived pain and painlessTMD-related symptoms with alexithymia and depressive mood inmedia personnel with or without irregular shift work. ActaOdontol. Scand. 62:119–123.
Åkerstedt T. (1998). Shift work and disturbed sleep/wakefulness. SleepMed. Rev. 2:117–128.
Åkerstedt T. (2003). Shift work and disturbed sleep/wakefulness.Occup. Med (Lond.) 53:89–94.
Åkerstedt T, Gillberg M. (1990). Subjective and objective sleepiness inthe active individual. Int. J. Neurosci. 52:29–37.
Åkerstedt T, Wright KP. (2009). Sleep loss and fatigue in shift work andshift work disorder. Sleep Med. Clin. 4:257–271.
Archer SN, Robilliard DL, Skene DJ, Smits M, Williams A, Arendt J, vonSchantz M. (2003). A length polymorphism in the circadian clockgene Per3 is linked to delayed sleep phase syndrome and extremediurnal preference. Sleep 26:413–415.
Axelsson J, Åkerstedt T, Kecklund G, Lowden A. (2004). Tolerance toshift work-how does it relate to sleep and wakefulness? Int. Arch.Occup. Environ. Health 77:121–129.
Axelsson J, Kecklund G, Åkerstedt T, Donofrio P, Lekander M, Ingre M.(2008). Sleepiness and performance in response to repeated sleeprestriction and subsequent recovery during semi-laboratory con-ditions. Chronobiol. Int. 25:297–308.
Banks S, Van Dongen HP, Maislin G, Dinges DF. (2010). Neurobeha-vioral dynamics following chronic sleep restriction: dose-responseeffects of one night for recovery. Sleep 33:1013–1026.
Boggild H. (2009). Settling the question—the next review on shift workand heart disease in 2019. Scand. J. Work Environ. Health35:157–161.
Boivin DB, Czeisler CA, Dijk DJ, Duffy JF, Folkard S, Minors DS,Totterdell P, Waterhouse JM. (1997). Complex interaction of thesleep-wake cycle and circadian phase modulates mood in healthysubjects. Arch. Gen. Psychiatry 54:145–152.
Burgess HJ, Savic N, Sletten T, Roach G, Gilbert SS, Dawson D. (2003).The relationship between the dim light melatonin onset and sleepon a regular schedule in young healthy adults. Behav. Sleep Med.1:102–114.
Buxton OM, Pavlova M, Reid EW, Wang W, Simonson DC, Adler GK.(2010). Sleep restriction for one week reduces insulin sensitivityin healthy men. Diabetes 59:2126–2133.
Cajochen C, Khalsa SBS, Wyatt JK, Czeisler CA, Dijk D-J. (1999). EEGand ocular correlates of circadian melatonin phase and humanperformance decrements during sleep loss. Scand J Work EnvironHealth. 2012; 38(2):171–181, doi:10.5271/sjweh.3197. The sitationoccurs in lines 172, 288, 864, 1066, 1354.
Cajochen C, Knoblauch V, Krauchi K, Renz C, Wirz-Justice A. (2001).Dynamics of frontal EEG activity, sleepiness and bodytemperature under high and low sleep pressure. Neuroreport12:2277–2281.
S. M. T. Wehrens et al.
Chronobiology International
Chr
onob
iol I
nt D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y Fr
anci
s A
Cou
ntw
ay L
ibra
ry o
f M
edic
ine
on 0
9/04
/13
For
pers
onal
use
onl
y.

Cavallo A, Jaskiewicz J, Ris MD. (2002). Impact of night-float rotationon sleep, mood, and alertness: the resident’s perception. Chrono-biol. Int. 19:893–902.
Cohen DA, Wang W, Wyatt JK, Kronauer RE, Dijk DJ, Czeisler CA,Klerman EB. (2010). Uncovering residual effects of chronic sleeploss on human performance. Sci. Transl. Med. 2:14ra13.
Costa G. (2003). Shift work and occupational medicine: an overview.Occup. Med. (Lond.) 53:83–88.
Costa G, Sartori S, Åkerstedt T. (2006). Influence of flexibility and varia-bility of working hours on health and well-being. Chronobiol. Int.23:1125–1137.
Dijk DJ, Duffy JF, Czeisler CA. (1992). Circadian and sleep/wakedependent aspects of subjective alertness and cognitive perform-ance. J. Sleep Res. 1:112–117.
Dinges DF, Powell JW. (1985). Microcomputer analyses of performanceon a portable, simple visual RT task during sustained operations.Behav. Res. Methods Instr. Comp. 17:652–655.
Dinges DF, Orne MT, Whitehouse WG, Orne EC. (1987). Temporalplacement of a nap for alertness: contributions of circadianphase and prior wakefulness. Sleep 10:313–329.
Dinges DF, Douglas SD, Zaugg L, Campbell DE, McMann JM,Whitehouse WG, Orne EC, Kapoor SC, Icaza E, Orne MT. (1994).Leukocytosis and natural killer cell function parallel neurobeha-vioral fatigue induced by 64 hours of sleep deprivation. J. Clin.Invest. 93:1930–1939.
Dinges DF, Pack F, Williams K, Gillen KA, Powell JW, Ott GE, AptowiczC, Pack AI. (1997). Cumulative sleepiness, mood disturbance, andpsychomotor vigilance performance decrements during a week ofsleep restricted to 4–5 hours per night. Sleep 20:267–277.
Doran SM, Van Dongen HP, Dinges DF. (2001). Sustained attentionperformance during sleep deprivation: evidence of state instability.Arch. Ital. Biol. 139:253–267.
Driesen K, Jansen NW, Kant I, Mohren DC, van Amelsvoort LG. (2010).Depressedmood in theworking population: associations with workschedules and working hours. Chronobiol. Int. 27:1062–1079.
Faraut B, Boudjeltia KZ, Dyzma M, Rousseau A, David E, Stenuit P,Franck T, Antwerpen PV, Vanhaeverbeek M, Kerkhofs M. (2011).Benefits of napping and an extended duration of recovery sleepon alertness and immune cells after acute sleep restriction. BrainBehav. Immun. 25:16–24.
Folkard S, Arendt J, Clark M. (1990). Sleep and mood on a “weekly”rotating (7-7-7) shift system: some preliminary results. Frankfurtam Main: Peter Lang.
Franzen PL, Siegle GJ, Buysse DJ. (2008). Relationships between affect,vigilance, and sleepiness following sleep deprivation. J. Sleep Res.17:34–41.
Frey DJ, Badia P, Wright KP Jr. (2004). Inter- and intra-individualvariability in performance near the circadian nadir during sleepdeprivation. J. Sleep Res. 13:305–315.
Galliaud E, Taillard J, Sagaspe P, Valtat C, Bioulac B, Philip P. (2008).Sharp and sleepy: evidence for dissociation between sleep pressureand nocturnal performance. J. Sleep Res. 17:11–15.
GillbergM, Kecklund G, Axelsson J, Åkerstedt T. (1996). The effects of ashort daytime nap after restricted night sleep. Sleep 19:570–575.
Gould KS, Hirvonen K, Koefoed VF, Roed BK, Sallinen M, Holm A,Bridger RS,MoenBE. (2009). Effects of 60 hours of total sleep depri-vation on two methods of high-speed ship navigation. Ergonomics52:1469–1486.
Graw P, Kräuchi K, Knoblauch V, Wirz-Justice A, Cajochen C. (2004).Circadian and wake-dependent modulation of fastest and slowestreaction times during the psychomotor vigilance task. Physiol.Behav. 80:695–701.
Haack M, Mullington JM. (2005). Sustained sleep restriction reducesemotional and physical well-being. Pain 119:56–64.
Härmä M. (1993). Individual differences in tolerance to shiftwork: areview. Ergonomics 36:101–109.
Härmä M, Tenkanen L, Sjoblom T, Alikoski T, Heinsalmi P. (1998). Com-bined effects of shiftwork and life-style on the prevalence of insomnia,
sleep deprivation and daytime sleepiness. Scand. J. Work Environ.Health 24:300–307.
Härmä M, Tarja H, Irja K, Mikael S, Jussi V, Anne B, Pertti M. (2006). Acontrolled intervention study on the effects of a very rapidly forwardrotating shift system on sleep-wakefulness and well-being amongyoung and elderly shift workers. Int. J. Psychophysiol. 59:70–79.
Horne JA, Burley CV. (2010). We know when we are sleepy: subjectiveversus objective measurements of moderate sleepiness in healthyadults. Biol. Psychol. 83:266–268.
Iber C, Ancoli-Israel S, Chesson A, Quan SF. (2007). The AASMmanualfor the scoring of sleep and associated events: rules, terminology andtechnical specifications.Westchester, IL: The American Academy ofSleep Medicine.
Jay SM, Lamond N, Ferguson SA, Dorrian J, Jones CB, Dawson D.(2007). The characteristics of recovery sleep when recovery oppor-tunity is restricted. Sleep 30:353–360.
Kahn-Greene ET, Killgore DB, Kamimori GH, Balkin TJ, Killgore WD.(2007). The effects of sleep deprivation on symptoms of psycho-pathology in healthy adults. Sleep Med. 8:215–221.
Kaliterna LL, Prizmic LZ, Zganec N. (2004). Quality of life, life satisfac-tion and happiness in shift- and non-shiftworkers. Rev. SaúdePública 38:3–10.
KerkhofsM, Boudjeltia KZ, Stenuit P, BroheeD, Cauchie P, Vanhaever-beek M. (2007). Sleep restriction increases blood neutrophils, totalcholesterol and low density lipoprotein cholesterol in postmeno-pausal women: a preliminary study. Maturitas 56:212–215.
King AC, Belenky G, Van DongenHP. (2009). Performance impairmentconsequent to sleep loss: determinants of resistance and suscepti-bility. Curr. Opin. Pulm. Med. 15:559–564.
Kirkpatrick M, Haney M, Vosburg S, Comer S, Foltin R, Hart C. (2009).Methamphetamine self-administration by humans subjected toabrupt shift and sleep schedule changes. Psychopharmacology203:771–780.
Kitamura S, Hida A, Watanabe M, Enomoto M, Aritake-Okada S, Mor-iguchi Y, Kamei Y, Mishima K. (2010). Evening preference is relatedto the incidence of depressive states independent of sleep-wakeconditions. Chronobiol. Int. 27:1797–1812.
Kline CE, Durstine JL, Davis JM, Moore TA, Devlin TM, Youngstedt SD.(2010). Circadian rhythms of psychomotor vigilance, mood, andsleepiness in the ultra-short sleep/wake protocol. Chronobiol. Int.27:161–180.
Knutsson A. (2004). Methodological aspects of shift-work research.Chronobiol. Int. 21:1037–1047.
Kribbs NB, Dinges DF. (1994). Vigilance decrement and sleepiness.InHarsh J, Ogilvie R (eds.). Sleep onset mechanisms. Washington,DC: American Psychological Association, 113–125.
LamondN, Jay SM, Dorrian J, Ferguson SA, Jones C, DawsonD. (2007).The dynamics of neurobehavioural recovery following sleep loss.J. Sleep Res. 16:33–41.
Lee JH, Wang W, Silva EJ, Chang AM, Scheuermaier KD, Cain SW,Duffy JF. (2009). Neurobehavioral performance in young adultsliving on a 28-h day for 6 weeks. Sleep 32:905–913.
Lim J, Dinges DF. (2010). A meta-analysis of the impact of short-termsleep deprivation on cognitive variables. Psychol. Bull.136:375–389.
Lockley SW, Dijk DJ, Kosti O, Skene DJ, Arendt J. (2008). Alertness,mood and performance rhythmdisturbances associatedwith circa-dian sleep disorders in the blind. J. Sleep Res. 17:207–216.
Mollicone DJ, Van Dongen HP, Rogers NL, Banks S, Dinges DF. (2010).Time of day effects on neurobehavioral performance duringchronic sleep restriction. Aviat. Space Environ. Med. 81:735–744.
Nachreiner F. (1998). Individual and social determinants of shiftworktolerance. Scand. J. Work Environ. Health 24(Suppl 3):35–42.
Pagani M, Pizzinelli P, Traon AP, Ferreri C, Beltrami S, Bareille MP,Costes-Salon MC, Beroud S, Blin O, Lucini D, Philip P. (2009). He-modynamic, autonomic and baroreflex changes after one nightsleep deprivation in healthy volunteers. Auton. Neurosci.145:76–80.
Shiftworkers and Sleep Deprivation
© Informa Healthcare USA, Inc.
Chr
onob
iol I
nt D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y Fr
anci
s A
Cou
ntw
ay L
ibra
ry o
f M
edic
ine
on 0
9/04
/13
For
pers
onal
use
onl
y.

Pilcher JJ, Huffcutt AI. (1996). Effects of sleep deprivation on perform-ance: a meta-analysis. Sleep 19:318–326.
Portaluppi F, Smolensky MH, Touitou Y. (2010). Ethics and methodsfor biological rhythm research on animals and human beings.Chronobiol. Int. 27:1911–1929.
Retey JV, Adam M, Honegger E, Khatami R, Luhmann UF, Jung HH,BergerW, Landolt HP. (2005). A functional genetic variation of ade-nosine deaminase affects the duration and intensity of deep sleepin humans. Proc. Natl. Acad. Sci. U. S. A. 102:15676–15681.
Saksvik IB, Bjorvatn B, Hetland H, Sandal GM, Pallesen S. (2011). Indi-vidual differences in tolerance to shift work—a systematic review.Sleep Med. Rev. 15:221–235.
Sallinen M, Harma M, Mutanen P, Ranta R, Virkkala J, Muller K.(2005). Sleepiness in various shift combinations of irregular shiftsystems. Ind. Health 43:114–122.
Sallinen M, Holm A, Hiltunen J, Hirvonen K, Härmä M, Koskelo J,Letonsaari M, Luukkonen R, Virkkala J, Müller K. (2008). Recoveryof cognitive performance from sleep debt: do a short rest pause anda single recovery night help? Chronobiol. Int. 25:279–296.
SmithMR, Fogg LF, EastmanCI. (2009). A compromise circadian phaseposition for permanent night work improves mood, fatigue, andperformance. Sleep 32:1481–1489.
Spiegel K, Leproult R, Van Cauter E. (1999). Impact of sleep debt onmetabolic and endocrine function. Lancet 354:1435–1439.
Stenuit P, Kerkhofs M. (2005). Age modulates the effects of sleeprestriction in women. Sleep 28:1283–1288.
Urrila AS, Stenuit P, Huhdankoski O, KerkhofsM, Porkka-Heiskanen T.(2007). Psychomotor vigilance task performance during total sleepdeprivation in young and postmenopausal women. Behav. BrainRes. 180:42–47.
Van Dongen HP, Maislin G, Mullington JM, Dinges DF. (2003). Thecumulative cost of additional wakefulness: dose-response effectson neurobehavioral functions and sleep physiology from chronicsleep restriction and total sleep deprivation. Sleep 26:117–126.
Van Dongen HP, Baynard MD, Maislin G, Dinges DF. (2004a). Sys-tematic interindividual differences in neurobehavioral impairmentfrom sleep loss: evidence of trait-like differential vulnerability.Sleep 27:423–433.
Van Dongen HP, Maislin G, Dinges DF. (2004b). Dealing with inter-individual differences in the temporal dynamics of fatigue andperformance: importance and techniques. Aviat. Space Environ.Med. 75:A147–A154.
Van Dongen HP, Caldwell JA, Jr Caldwell JL. (2006). Investigating sys-tematic individual differences in sleep-deprived performance on ahigh-fidelity flight simulator. Behav. Res. Methods 38:333–343.
Vandewalle G, Archer SN,WuillaumeC, Balteau E, Degueldre C, LuxenA, Maquet P, Dijk DJ. (2009). Functional magnetic resonanceimaging-assessed brain responses during an executive taskdepend on interaction of sleep homeostasis, circadian phase, andPER3 genotype. J. Neurosci. 29:7948–7956.
Vgontzas AN, Zoumakis E, Bixler EO, Lin HM, Follett H, Kales A,Chrousos GP. (2004). Adverse effects of modest sleep restrictionon sleepiness, performance, and inflammatory cytokines. J. Clin.Endocrinol. Metab. 89:2119–2126.
Viola AU, Archer SN, James LM, Groeger JA, Lo JC, Skene DJ, vonSchantz M, Dijk DJ. (2007). PER3 polymorphism predicts sleepstructure and waking performance. Curr. Biol. 17:613–618.
Wehrens SM, Hampton SM, Finn RE, Skene DJ. (2010). Effect of totalsleep deprivation on postprandial metabolic and insulin responsesin shift workers and non-shift workers. J. Endocrinol. 206:205–215.
Wehrens SM, Hampton SM, SkeneDJ. (2011). Heart rate variability andendothelial function after sleep deprivation and recovery sleepamong male shift and non-shift workers. Scand. J. Work Environ.Health Sep 27. Epub ahead of print. doi: 10.5271
Wyatt JK, Ritz-De Cecco A, Czeisler CA, Dijk DJ. (1999). Circadiantemperature and melatonin rhythms, sleep, and neurobehavioralfunction in humans living on a 20-h day. Am. J. Physiol. Regul.Integr. Comp. Physiol. 277:R1152–R1163.
Yang CM, Lin FW, Spielman AJ. (2004). A standard procedure en-hances the correlation between subjective and objective measuresof sleepiness. Sleep 27:329–332.
Zhong X, Hilton HJ, Gates GJ, Jelic S, Stern Y, Bartels MN, Demeers-man RE, Basner RC. (2005). Increased sympathetic and decreasedparasympathetic cardiovascular modulation in normal humanswith acute sleep deprivation. J. Appl. Physiol. 98:2024–2032.
S. M. T. Wehrens et al.
Chronobiology International
Chr
onob
iol I
nt D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y Fr
anci
s A
Cou
ntw
ay L
ibra
ry o
f M
edic
ine
on 0
9/04
/13
For
pers
onal
use
onl
y.