Embed Size (px)
Citation preview

Mood Disorders
A Closer Look at Psychological Disorders
Mood DisordersMood Disorders Mood disorders are disturbances of
emotions that are severe or prolonged enough to cause impairment of functioning. These conditions are magnifications of our
normal reactions.
The magnified states in mood disorders are mania and depression.
Mania – a period of abnormally high emotion and activity
Depression – a period of extreme sadness and helplessness
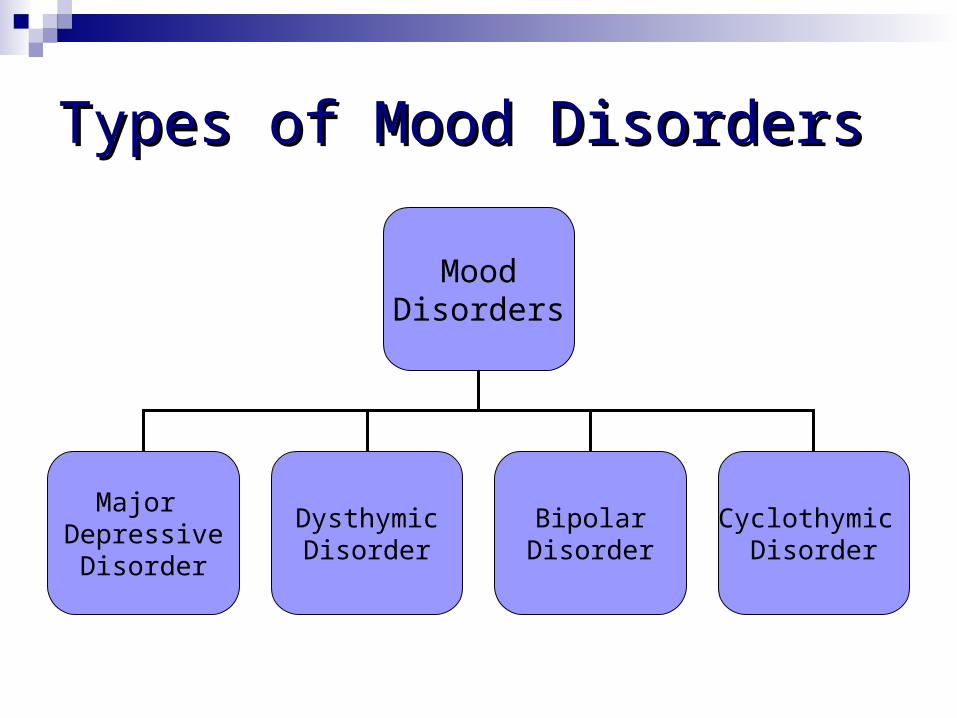
Types of Mood DisordersTypes of Mood Disorders
MoodDisorders
Major Depressive
Disorder
DysthymicDisorder
BipolarDisorder
Cyclothymic Disorder
Major Depressive Disorder (Unipolar Major Depressive Disorder (Unipolar Depression)Depression)
The most common mood disorder, and one of the more common psychological disorders in general.
Everyone gets depressed, so how do we know when normal depression crosses the line into major depressive disorder?
Major Depressive Disorder (cont.)Major Depressive Disorder (cont.) A person may be suffering from major
depressive disorder when five of the following nine symptoms have been present for two or more weeks:
Depressed mood most of the day, nearly every day Little interest or pleasure in almost all activities Significant changes in weight or appetite Sleeping more or less than usual Agitated or decreased level of activity Fatigue or loss of energy Feelings of worthlessness or inappropriate guilt Diminished ability to think or concentrate Recurrent thoughts of death or suicide
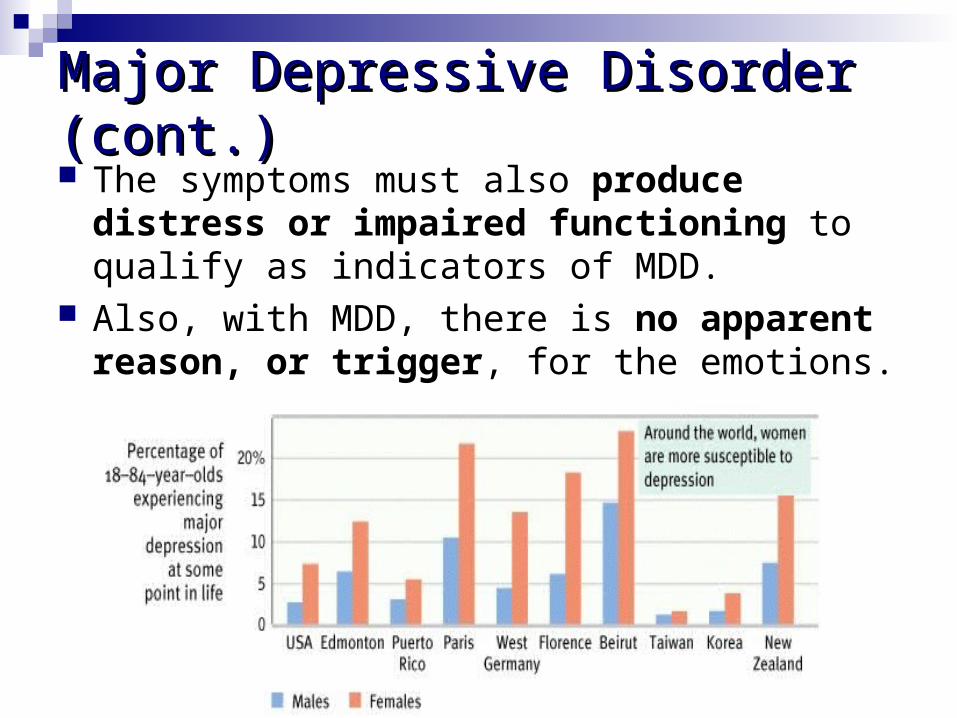
Major Depressive Disorder (cont.)Major Depressive Disorder (cont.) The symptoms must also produce distress or
impaired functioning to qualify as indicators of MDD.
Also, with MDD, there is no apparent reason, or trigger, for the emotions.
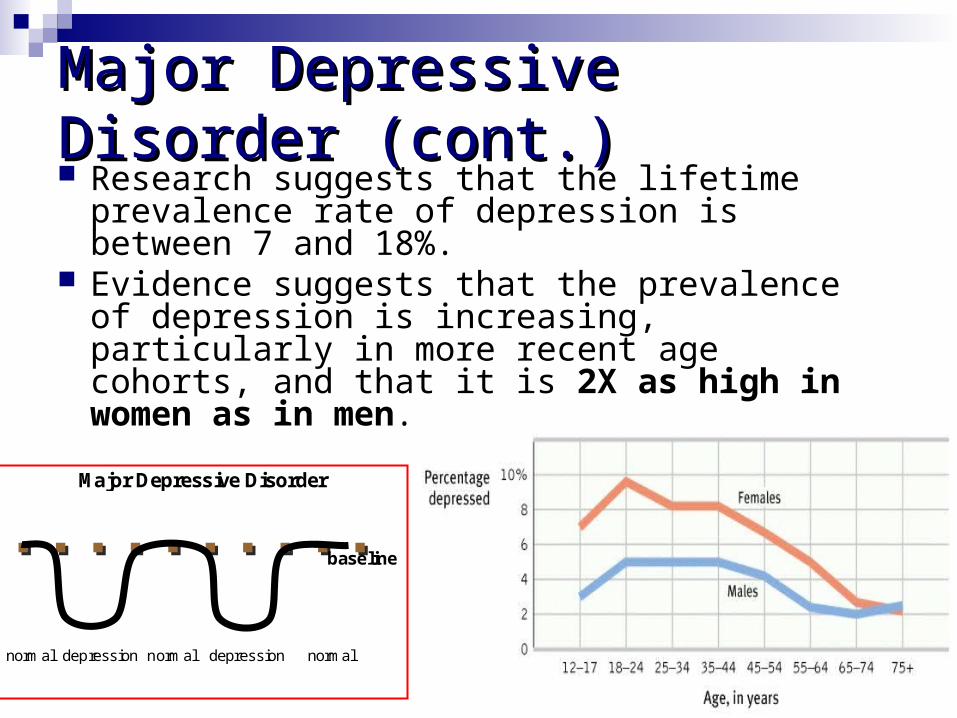
Major Depressive Disorder (cont.)Major Depressive Disorder (cont.) Research suggests that the lifetime prevalence
rate of depression is between 7 and 18%. Evidence suggests that the prevalence of
depression is increasing, particularly in more recent age cohorts, and that it is 2X as high in women as in men.
baseline
normal depression normal depression normal
Major Depressive Disorder
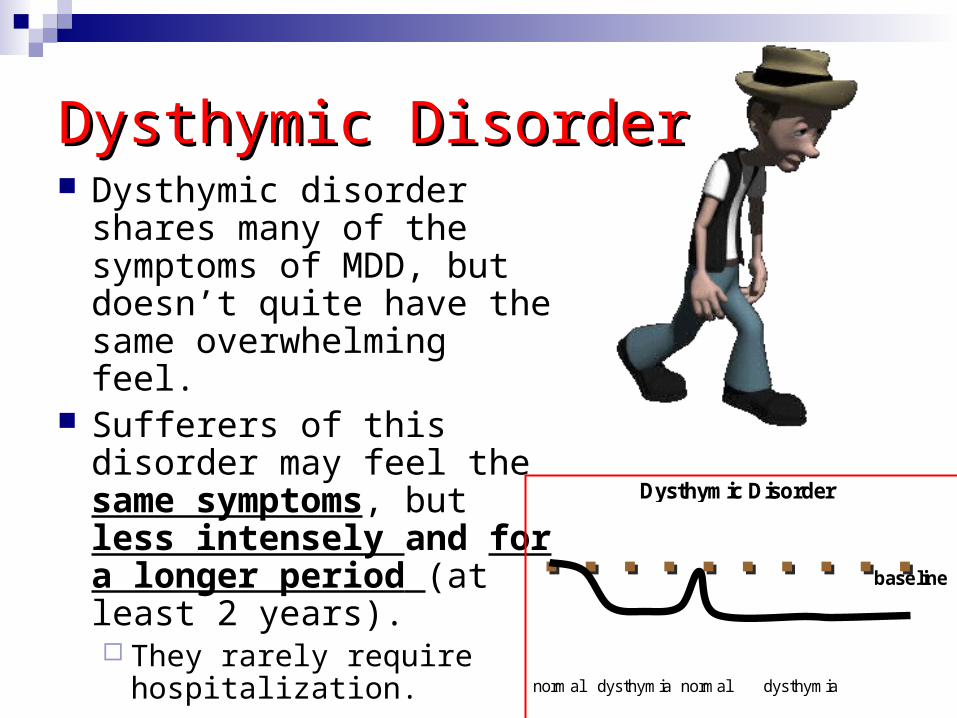
Dysthymic DisorderDysthymic Disorder Dysthymic disorder shares
many of the symptoms of MDD, but doesn’t quite have the same overwhelming feel.
Sufferers of this disorder may feel the same symptoms, but less intensely and for a longer period (at least 2 years). They rarely require
hospitalization.
baseline
normal dysthymia normal dysthymia
Dysthymic Disorder
Bipolar DisorderBipolar Disorder People with bipolar disorder also
experience the oppressive down periods of MDD; however, these periods alternate with manic episodes in which the person is unrealistically optimistic and displays wildly hyper behavior.
During mania, a person may go long periods without sleeping, experience changeable, racing thoughts, be easily distracted, and set impossible goals. Mania is sometimes also associated with
bouts of creative energy. Bipolar disorder affects a little over
1%-2% of the population and is equally as common in males and females.
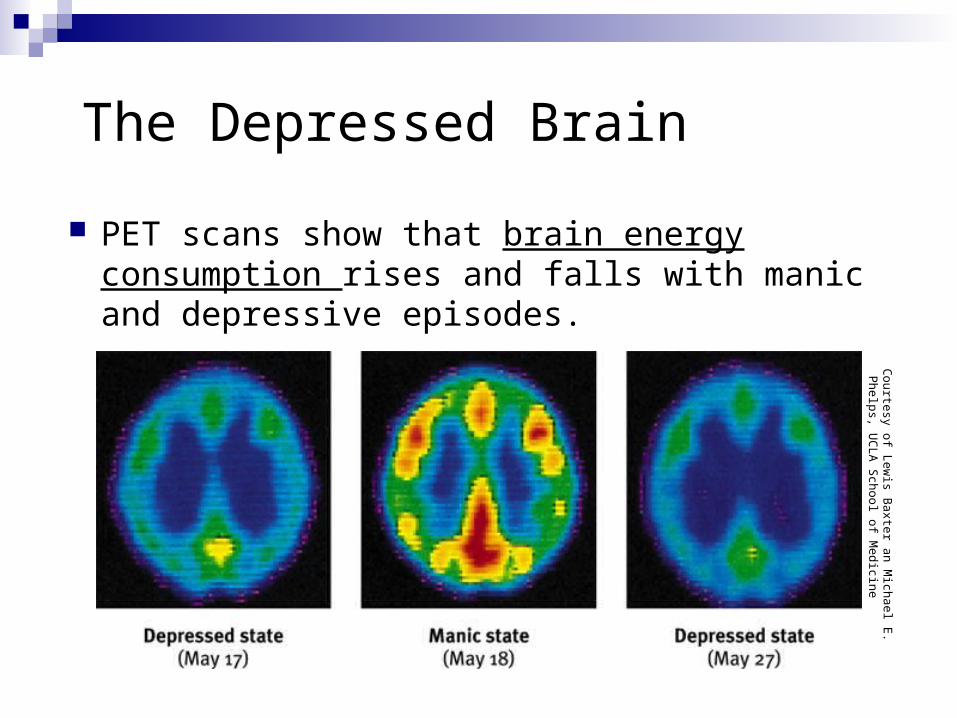
The Depressed Brain
PET scans show that brain energy consumption rises and falls with manic and depressive episodes.
Courtesy of L
ewis B
axter an Michael E
. P
helps, UC
LA
School of M
edicine
Victims of Bipolar Disorder? Victims of Bipolar Disorder? No one knows for sure, but some people
suspect that Vincent van Gogh was bipolar. His life alternated between periods of blazing
creativity – sometimes he finished more than a painting a day – and periods of deep depression. He committed suicide in 1890.
The world's most famous nurse, Florence Nightingale, is believed to have suffered from a bipolar disorder that caused long periods of depression and remarkable bursts of productivity.
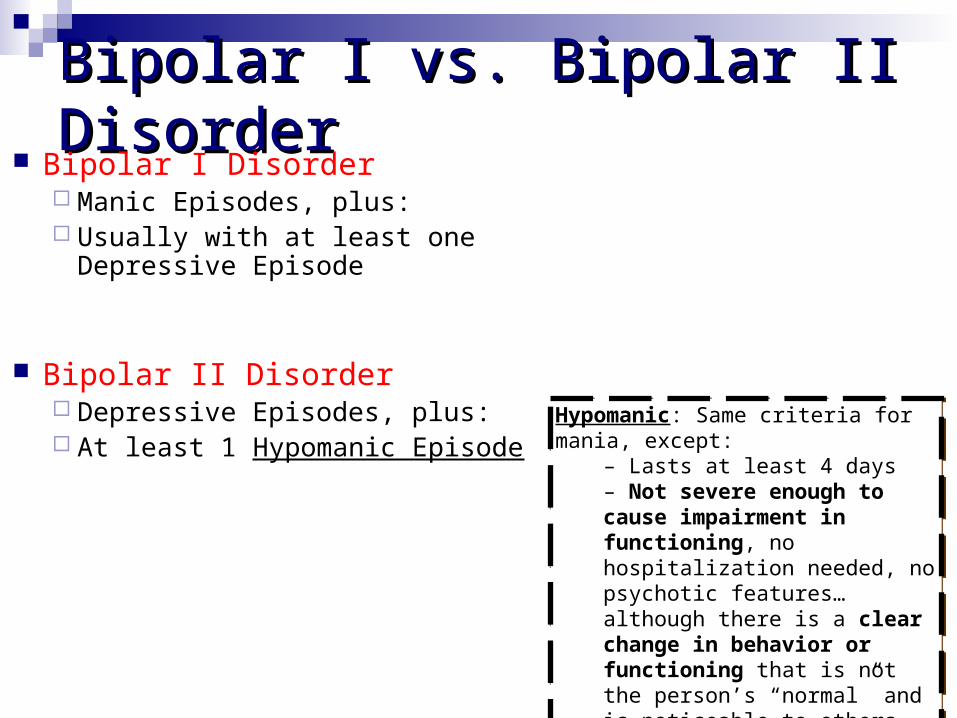
Bipolar I vs. Bipolar II DisorderBipolar I vs. Bipolar II Disorder Bipolar I Disorder
Manic Episodes, plus: Usually with at least one Depressive
Episode
Bipolar II Disorder Depressive Episodes, plus: At least 1 Hypomanic Episode
Hypomanic: Same criteria for mania, except:
– Lasts at least 4 days– Not severe enough to cause impairment in functioning, no hospitalization needed, no psychotic features… although there is a clear change in behavior or functioning that is not the person’s “normal” and is noticeable to others
Hypomanic: Same criteria for mania, except:
– Lasts at least 4 days– Not severe enough to cause impairment in functioning, no hospitalization needed, no psychotic features… although there is a clear change in behavior or functioning that is not the person’s “normal” and is noticeable to others

Cyclothymic DisorderCyclothymic Disorder Cyclothymia is
basically borderline bipolar disorder (milder than bipolar)
Includes Hypomanic symptoms
(not full mania), plus: Depressive symptoms
(not full depression) Lasts for at least 2
years
Hypomanic: Same criteria for mania, except:– Lasts at least 4 days– Not severe enough to cause impairment in functioning, no hospitalization needed, no psychotic features… although there is a clear change in behavior or functioning that is not the person’s “normal” and is noticeable to others
Hypomanic: Same criteria for mania, except:– Lasts at least 4 days– Not severe enough to cause impairment in functioning, no hospitalization needed, no psychotic features… although there is a clear change in behavior or functioning that is not the person’s “normal” and is noticeable to others
baseline
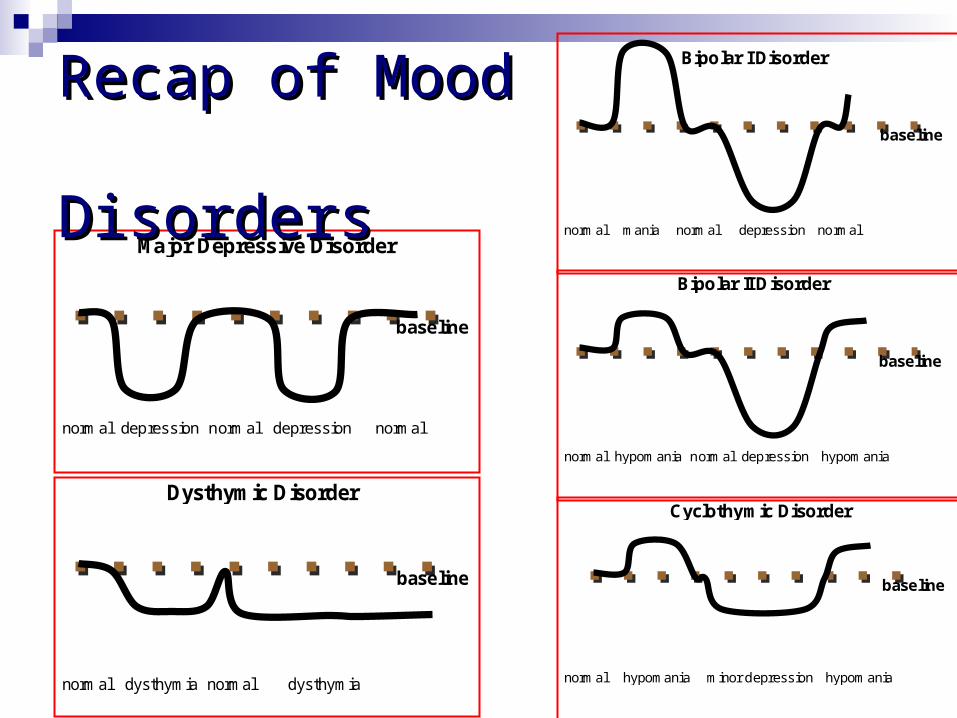
normal hypomania normal depression hypomania
Bipolar II Disorder
baseline
normal mania normal depression normal
Bipolar I Disorder
baseline
normal dysthymia normal dysthymia
Dysthymic Disorder
baseline
normal depression normal depression normal
Major Depressive Disorder
baseline
normal hypomania minor depression hypomania
Cyclothymic Disorder
Recap of Mood Recap of Mood DisordersDisorders
Other Types of “Depressions”Other Types of “Depressions” Seasonal Affective Disorder Double Depression (Dysthymia + Major
Depression) Post-partum depression
Etiology of Mood Disorders
Possible Causes
What causes mood disorders?What causes mood disorders?
Again, biology and environment interact as possible contributors to mood disorders.
Stress also seems to play a role, providing a trigger that sparks mood disorders when other factors are present.
Biomedical ApproachBiomedical Approach
Heredity – twin studies show that many mood disorders run in families. The rate of depression is higher in identical (50%) than fraternal twins (20%).
Brain function – Depressed people have depressed brains. Brain scans indicate that the brain is less active during major depression.
Also, certain neurotransmitters (serotonin and norepinephrine) are lacking during times of depression. Prozac and other antidepressant medications help
restore proper levels of these neurotransmitters.
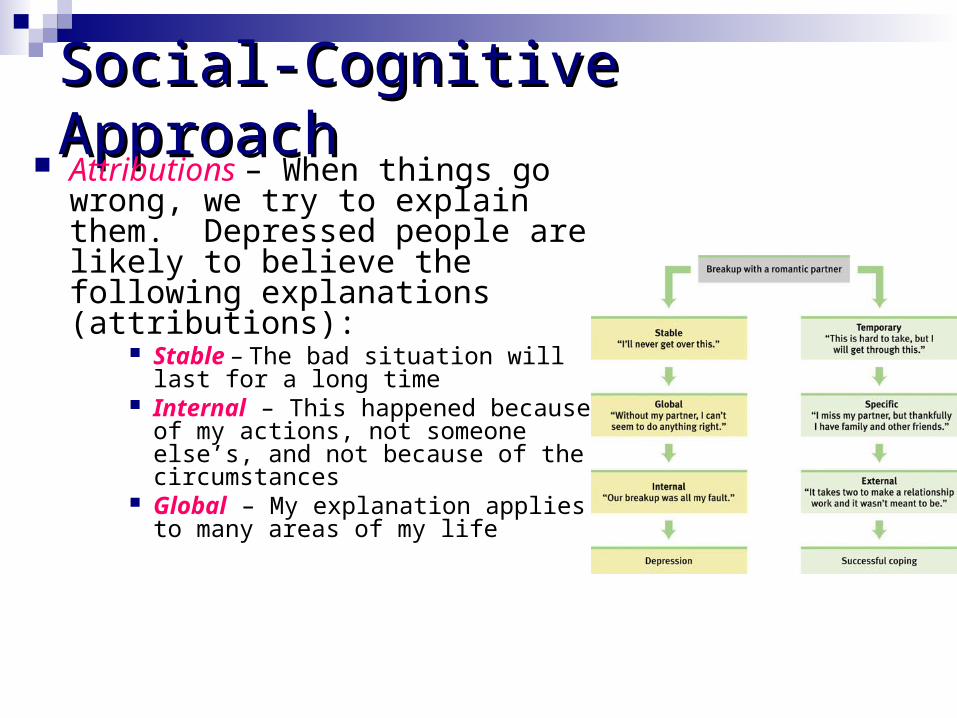
Social-Cognitive ApproachSocial-Cognitive Approach Attributions – When things go wrong,
we try to explain them. Depressed people are likely to believe the following explanations (attributions):
Stable – The bad situation will last for a long time
Internal – This happened because of my actions, not someone else’s, and not because of the circumstances
Global – My explanation applies to many areas of my life
Social-Cognitive Factors (cont.)Social-Cognitive Factors (cont.) Learned helplessness – People develop a
sense of helplessness when subjected to events over which they have little or no control. As they acquire this feeling of helplessness, they give up and no longer try to improve their situation, because they learned in the past that efforts to improve the situation will not work. This, by itself, can produce depression.
Learned helplessness may also explain why women suffer higher rates of depression than men do. Women are more likely to be abused and twice as likely to feel overwhelmed. This may explain women’s higher levels of learned helplessness and depression.
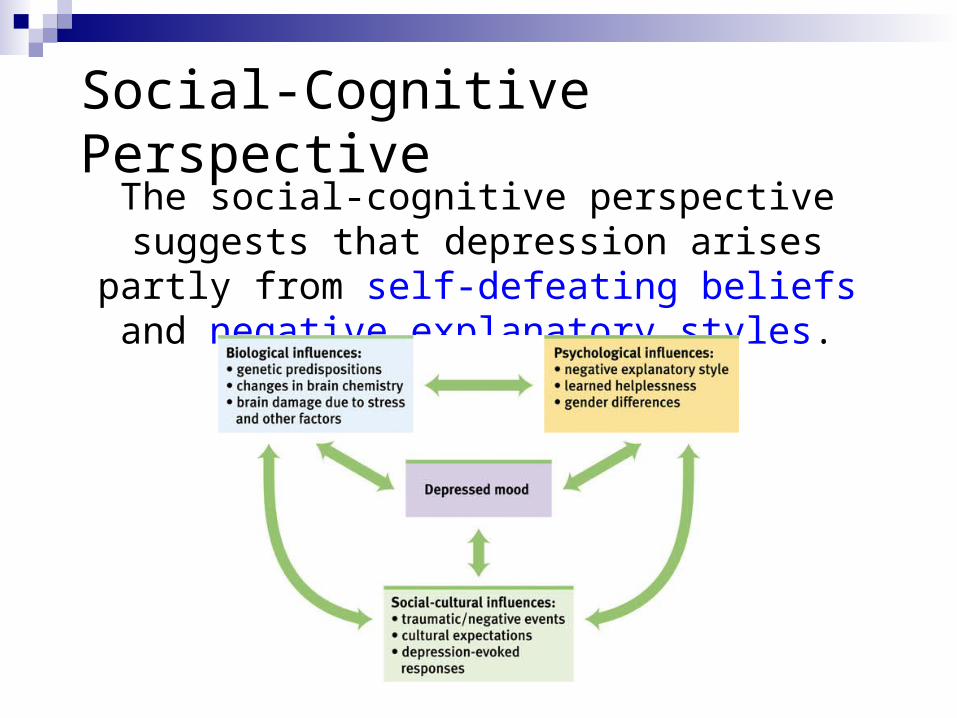
Social-Cognitive PerspectiveThe social-cognitive perspective suggests
that depression arises partly from self-defeating beliefs and negative
explanatory styles.
Humanistic ApproachHumanistic Approach Not enough life meaning Not enough authentic choices that lead to
self-fulfillment Connection of personal identity to others’
evaluation of ourselves, or to certain events (e.g., role at work), so that when these persons or events leave, there is loss and depression
Obstacles to self-actualization path
Behavioral ApproachBehavioral Approach Few rewards in life, many punishments Interactional theory (James Coyne)
Person acts depressed, which makes others annoyed or stressed by person, which makes others less likely to provide positive reinforcement and rewards to person, which makes person depressed…
Interpersonal inadequacies and poor social skills may lead to a scarceness of life’s reinforcers and frequent rejection.
Sociocultural ApproachSociocultural Approach
Cultural differences in symptom expression Different rates among different groups Higher rates among women Higher rates among single, divorced people Lower rates with social support Higher rates for younger adults Higher rates for lower socioeconomic status
Psychodynamic ApproachPsychodynamic Approach Parents fail to nurture person or they provide excessive
gratification of needs Actual or symbolic loss of the parent or loved one Regression to oral stage Introjection of loved one (Introjection – The process of
incorporating the characteristics of a person or object unconsciously into one's psyche, often as a defense mechanism)
Angry feelings towards loved one guilt + self-hatred Shifting dominance between superego (guilt and
worthlessness) and ego (asserts its strength and is elated and self-confident).