Embed Size (px)
Citation preview

ORIGINAL ARTICLES I I
Indian J Pediatr 1994; 61 : 341-346
Morning Steroid Profile in Children with Congenital Adrenal Hyperplasia Under Different Hydrocortisone Schedules
I.N. Silva, D.F. Oliveira-Junior, C.J.R. Simal*, M.B. Viana and A.J. Chagas
Pediatric Department of Medical School, and *Department of Nuclear Medicine, Medical School, Federal University of Minas Gerais, Brasil
Abstract. We studied 13 children with 21-hydroxyalse deficiency to explore the immediate po(ential suppressive effect of hydrocortisone dose schedule on the adrenal codex. They were given 20 mg/m 2 daily in a controlled trial. After random administration of a greater dose in the morning (7 patients) or at night (6 patients), we measured plasma levels of 17- hydroxyprogesterone, testosterone, and androstenedione at times-24, 0, 2, 4, and 6h. Considerable fluctuation of the steroid levels, unrelated to the drug intake, was observed. There was no statistically significant differences between the "morn|ng dose" and "night dose" groups for any steroid. We conclude that; (i) the greater night dose didnot avoid the 17-hydroxyprogesterone morning peaks, and (ii) the ,variation in plasma steroid l e v ~ is so marked that a single morning sample is unreliable to reflect the degree of adrenal suppression. (Indian J Pedlatr 1994; 61 : 341-346)
Key words : Congenital adrenal hyperplasia; Hydrocortisone schedule; Adrenal steroids.
Congenital adrenal hyperplasia (CAH) due to 21-hydroxylase deficiency (21- OHD) accounts for most cases of ambiguous genitalia in the female newborn, and may be responsible for psychological problems and short stature in adult life. Greater improvement in the quality of life has been achieved since Willdns's first trails with hydrocortisone began in the 50's. 1 In spite of this, almost half a century later, we still don't know how to adequately manage these patients. There are still some co , troversies on what is the best hydrocortisone schedule and
l~eprint requests : Profa. Ivani Novato Silva, Departsmento de Pediatria, Faculdade de Medicina da UFbiG, Av. Alfredo Balena 190-4 ~ ~dar-Sta. Efigenia , Cep 30130-100, Belo Horizonte, Minas Gerais, Brasil.
which parameters should be used to evaluate the adequacy of treatment. The optimistic speech of Winter in 1980". today the infant with CAH can look forward. . , to the opportunity to become a healthy adult with normal children ''2 has not been completely proved yet and DiMartino-Nardi et aP showed, in a retrospective study, how frustrating can be the growth of children with CAH after two decades of surveillance.
Several trials were done to find out simple and accurate parameters to detect subtle changes in treatment that could be followed by harmful growth velocity fluctuations. Plasma levels of 17-hydroxyprogesterone (17-OHP), test- osterone (T), and its precursors were frequently used for this purpose. ~s We have determined 17-OHP, T, and

342 THE INDIAN JOURNAL OF PEDIATRICS 1994; VoL 61. No. 4
anclrostenedione (A) plasma profiles in a
group of CAH children to explore the immediate potential suppressive effect of hydrocortisone administration on the secretion of these steroids.
MATERIAL AND Mt-rxoDs
P a t i e n t p o p u l a t i o n a n d methods. W e
studied 13 previously diagnosed and clini- cally well-controlled children with 21- OHD (8 salt-losers and 5 with the simple virilizing form) aged 1 to 10 years. They had been followed up based on standard clinical criteria for controlling children with CAH. 3 24h following the discontinuation of their regular treatment fasting blood samples (basal) were drawn and hydrocortisone acetate treatment (20 mg /mZ/day qid) was begun. Children were randomly allocated to two groups : 6 received a greater night dose (40% of total) and 7 a.m. greater morning dose. The next morning a blood sample was collected at time 0, between 7 and 8 a.m., (12h after the last hydrocortisone dose and immediately before the morning dose) and after 2, 4, and 6h for 17-OHP, T, and A determina- tions. No food intake was allowed during the test, except for I year-old patients who received fat-free food and water. Mineralo- corticoid supplements were also halted un- !il the end of the test.
Serum samples were stored for up to two months frozen at-20~ for subsequent analysis by RIA techniques in the Central Laboratory of "Hospital das Clinicas", Federal University of ~linas Gerais. Com- mercial kits were employed for steroid de- terminations (Coat-A-Count, Diagnostic Products Corporation, Los Angeles, U.S.A., for 17-OHP and A and Serano, MAIA kit, Santiago del Estero, Argentina,
for T). Reference values had been previ- ously defined in the laboratory.
All parents gave written informed con- sent for the participation of their children in the study.
~tatietieal method~. The absolute basal values of each steroid from the two ran- domized groups ("morning dose" x "night dose") were compared by the Mann- Whitney test. The individual variability of the plasma values of steroids precluded an analysis based on absolute figures at 0, 2, 4, and 6h. Accordingly, a fraction (value at 0, 2, 4, or 6 h)/(basal value) was calculated for each patient and the two randomized groups were then compared at each hour by the Mann-Whitney test. These fractions were then summed up and the mean for each patient was obtained. This mean might represent the overall degree of ste- roid inhibition achieved by the treatment schedule. The two groups were again com- pared by the same test.
RESULT AND DISCUSSION
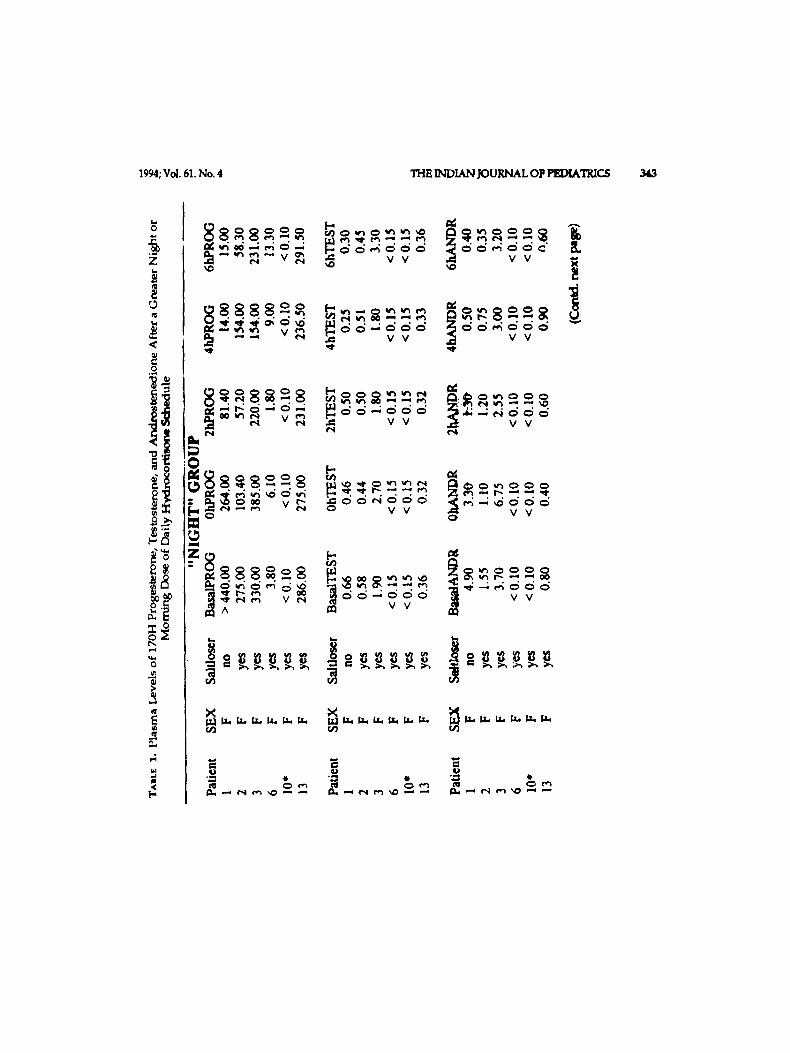
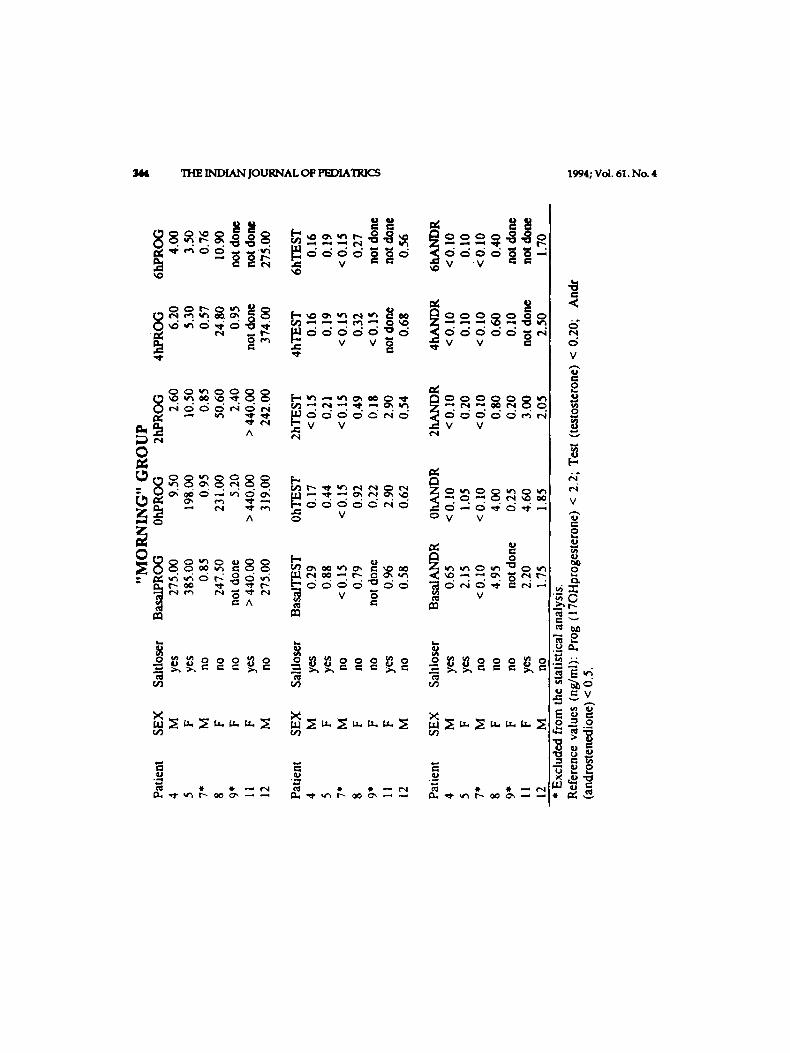
The plasma levels of 17-OHP, T, and A are stiown in Table 1. Remarkable fluctuation of values unrelated to the hydrocortisone administration is apparent.
At times minus 24h (basal) or Oh all but two children (patients 7 and 10) had elevated 17-OHP levels which are characteristic of 21-OHD. These two patients, however, had elevated levels recorded in other occasions and thus, had previous adrenal suppression. Both were excluded from the statistical analysis. Patient 9 was also excluded because his basal value was missing and the relative values at 0, 2, 4, and 6h could not be determined. The absolute basal values for
1994; Vol. 61. No. 4 TIIE INDIAN JOURNAL OP P~D[ATRICS 34,3
li 0 . I=
is
I-,
v ~ v v ~ v v
~ V ~ V V
~ ~ v v v ~ v v
~ ~ . ~ ~ - ~ ~ ~ - ~ _ o v v ~ v v
~ m d o - - o d d v v ~ V ~ A ~ V V
rJ3
THE INDIAN JOURNAL OF PEDIATRICS 1994; VOI. 61. No. 4
~oV " V
~ ~ ~ ~ . @ . ---~- �9 ~ ~
~ v v
e , i ~ ~ . . . . . . .
' ~ '~ "~ V V V V
0
A
A m ~
_o~ooor, o =o~r, oo~r,o _
x x x
~ E
V
o
111
v
" I . . . . . . . V
v v
e u
~ ~ d a ~
1994; Vol. 61. No. 4 THE INDIAN JOURNAL OF PEDIATRICS
"MIGHT" GROUP
1 ~ .
~ - - x - - $
(~ 11.1 24 @ - i ~ i i - - ~ , 3 TIME 0mum I
"MORNIMG" GROUP - - : = - - 4
t 111! .......4....__ ?
| . ~ l l
LI-i24 l 2 4 I ----o--- 11
TIME Okoum) ~ lZ
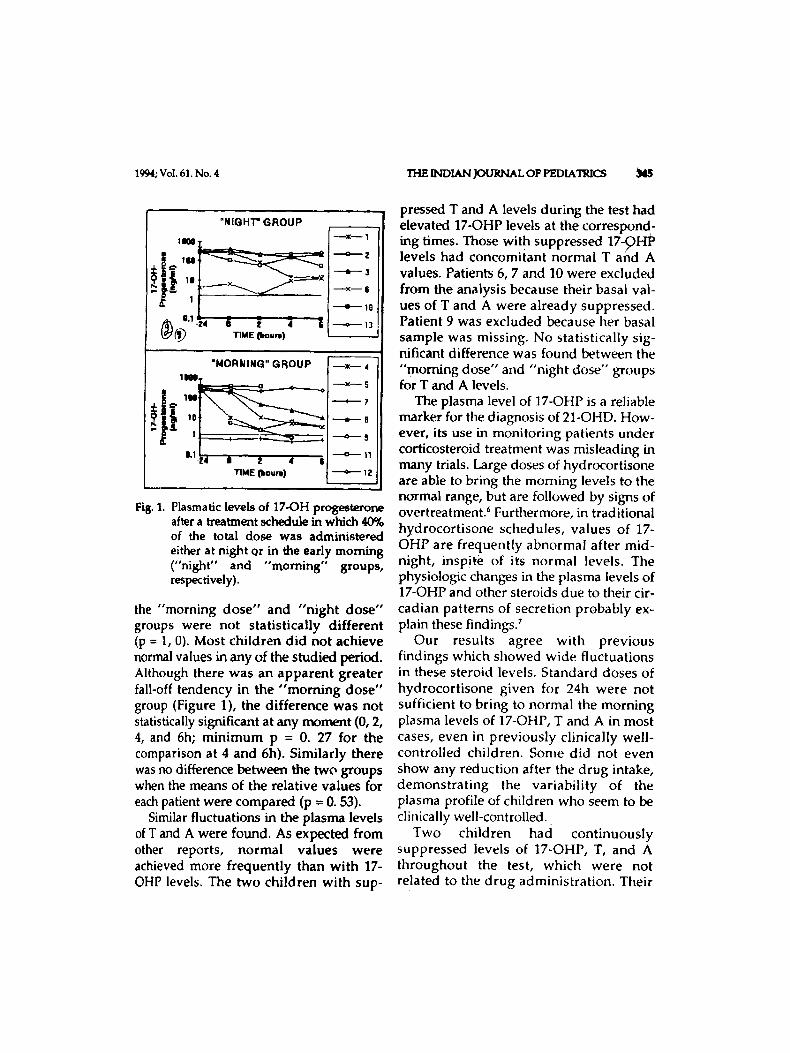
Fi 8.1. Plasmatic levels of 17-OH progesterone after a treatment schedule in which 40% of the total dose was administe,ed either at night or in the early morning ("night" and "morning" groups, respectively).
the "morning dose" and "night dose" groups were not statistically different (p = 1, 0). Most children did not a c h i e v e normal values in any of the studied period. Although there was an apparent greater fail-off tendency in the "morn ing dose" group (Figure 1), the difference was not statistically significant at any moment (0, 2, 4, and 6h; min imum p = 0. 27 for the comparison at 4 and 6h). Similarly there was no difference between the two groups when the means of the relative values for each patient were compared (p = 0. 53).
Similar fluctuations in the plasma levels of T and A were found. As expected from other reports, normal values were achieved more frequently than with 17- OHP levels. The two children with sup-
pressed T and A levels during the test had elevated 17-OHP levels at the correspond- hag times. Those with suppressed 17-QHP levels had concomRant normal T and A values. Patients 6, 7 and 10 were excluded from the analysis because their basal val- ues of T and A were already suppressed. Patient 9 was excluded because her basal sample was missing. No statistically sig- nificant difference was found between the "morning dose" and "night dose" groups for T and A levels.
The plasma level of 17-OHP is a reliable marker for the diagnosis of 21-OHD. How- ever, its use in monitoring patients under corticosteroid treatment was misleading in many trials. Large doses of hydrocortisone are able to bring the morning levels to the normal range, but are followed by signs of overtreatment. 6 Furthermore, in traditional hydrocort isone schedules, values of 17- OHP are frequently abnormal after mid- night, insp!te of its normal levels. The physiologic changes in the plasma levels of 17-OHP and other steroids due to their cir- cadian patterns of secretion probably ex- plain these findings/
Our results agree with previous findings which, showed wide fluctuations in these steroid levels. Standard doses of hydrocort isone given for 24h were not sufficient to bring to normal the morning plasma levels of 17-OHP, T and A in most cases, even in previously clinically well- controlled children. Some did not even show any reduction after the drug intake, demonstra t ing the variability of the plasma profile of children who seem to be clinically well-controlled..
Two children had continuously suppressed levels of 17-OHP, T, and A throughout the test, which were not related to the drug administration. Their

346 THE INDIAN JOURNAL OF PEDIATRICS 1994; VoL 61. No. 4
adrenal cortical function was probably suppressed by glucocorticoid over- treatment, although daily doses above 20 m g / m 2 had not been recorded previously, and clinical signs of hypercortisoljsm were never detected.
Although a steeper fall in 17-OHP levels was observed in some patieats after a larger morning dose, we could not confirm any significant differences between the two groups. A larger population is neces- sary to prove or discard this trend.
Fluctuations .in the plasma levels of T and A usually followed the same pattern of 17-OHP.
Thus, a single morning sample for 17- OHP, T or A seems unreliable for adequate information about the actual level of adre- nal suppression, considering ~ a t remark- able fluctuation of the plasma levels of these steroids do occur and that probably only large doses of hydrocortisone are able to decrease morning values to normal. Similarly, a larger bedtime hydrocortisone intake had no evident advantage since it did not avoid the morning 17-OHP peak levels. We reinforce that parameters other than simple clinical data are not yet avail- able to monitor CAH children under corti- costeroid treatment. Improved methods for detecting the dai lymetabol ic states of these children are sorely needed.
ACKNOWLEDGEMENTS
The authors thank Dr. Claudio Elias Kater for revising the manuscript. This work was
partially suppor ted by "Pro-Reitoria de Pesquisa", Federal Universi ty of Minas Gerais, Brasil.
REFERENCES
1. Wilkins L, Lewis RA, Klein R et al. The suppression of androgen secretion by cortisone in a case of congenital adrenal hyperpiasia - preliminary report. Bull Johns Hoph'ns Hasp 1950; 86 : 249-252.
2. Winter JSD. Marginal comment : Current approaches to the treatment of congenital adrenal hyperplasia. J Pediatr 1980; 97 : 81-82.
3. Dimartino-Nardi J, Stoner E, O'Connell A et al. The effect of treatment of final height in classical congenital adrenal hyperplasia (CAH). Acta Endocrinol Suppl (Copenh) 1986; 279 : 305-314.
4. Young MC, Hughes IA. Response to treatment of congenital adrenal hyperplasia in infancy. Arch Dis Child 1990; 65 : 441-444.
5. Lippe BM. LaFranchi SH, Lavin N e t al. Serum 17-alpha-hdroxyprogesterone, progesterone, estradiol, and testosterone in the diagnosis and management of congenital adrenal hyperplasia. J Pediatr 1974; 85 : 782-787.
6. Hughes IA, Winter JSD. The application of a serum' 17 OH-progesterone radioimmunoassay to the diagnosis and management of congenital adrenal hyperplasia. J Pediatr 1976; 88 : 766-773.
7. Frisch H, Parth K, Schober E et al. Circadian patterns of plasma contisol, 17- hydroxyprogesterone, and testosterone in congenital adrenal hyperplasia. Arch Dis Child 1981; 56 : 208-213.










![Endometrium presentation - Dr Wright[1] · Endometrial Hyperplasia Simple hyperplasia Complex hyperplasia (adenomatous) Simple atypical hyperplasia ... Progression of Hyperplasia](https://img.pdfslide.net/doc/110x75/5b8a421e7f8b9a50388bc13d/endometrium-presentation-dr-wright1-endometrial-hyperplasia-simple-hyperplasia.jpg)