Embed Size (px)
Citation preview
Ph.D. Thesis
Sunniva Engelbrecht
Motivation and Burnout in Human Service Work
The Case of Midwifery in Denmark
National Institute of Occupational Health Roskilde University
Faculty of Psychology, Philosophy and Science Studies

Ph.D. Thesis
Motivation and Burnout in Human Service Work The Case of Midwifery in Denmark
Sunniva Engelbrecht
Main supervisor: Professor Peter Olsén, Roskilde University
Project supervisor: Dr. Birgit Aust, National Institute of Occupational Health, Copenhagen
Painting on cover: Muriel Engelbrecht
Copenhagen, April 2006
To Muriel and Tali
3
Acknowledgements.............................................................................................. 7
Abstract ................................................................................................................ 9
Resumé ............................................................................................................... 13
Chapter 1: Introduction.................................................................................... 17 1.1 Research interest, research field and research question...................... 17 1.2 Research approach .................................................................................. 19 1.3 Relevance .................................................................................................. 21 1.4 Structure of the monograph ................................................................... 22
Chapter 2: Theory ............................................................................................. 25 2.1 Introduction and organisation of the chapter....................................... 25 2.2 Burnout research throughout the last 30 years .................................... 25
2.2.1 Historical development from phenomenon to syndrome.................... 26 2.2.2 Burnout: symptoms, definitions, and measurement............................ 28
2.3 Selected motivation concepts .................................................................. 46 2.3.1 Implicit and explicit motivation .......................................................... 47 2.3.2 Commitment ........................................................................................ 49 2.3.3 Flow..................................................................................................... 52 2.3.4 Motivational concepts developed from within burnout research........ 53 2.3.5 Relationship and overlap between motivational concepts introduced
above .................................................................................................... 56 2.3.6 The relationship between motivation and burnout.............................. 56 2.3.7 The existential model of burnout ........................................................ 57
2.4 Selected empirical studies on the relationship between motivation and burnout..................................................................................................... 59
2.5 Work Family Conflict (WFC)................................................................. 65 2.6 Emotions at work ..................................................................................... 68
2.6.1 Concepts of emotion work .................................................................. 68 2.7 Summary and conclusion ........................................................................ 73
Chapter 3: Epistemological reference frame and method ............................ 75 3.1 Introduction.............................................................................................. 75 3.2 Phenomenology as research paradigm .................................................. 77
3.2.1 The phenomenological method ........................................................... 79 3.2.2 Context dependency ............................................................................ 84 3.2.3 The use of theory throughout the monograph ..................................... 85
4
3.2.4 Dialogue as a guideline for research ................................................... 87 3.3 Formal and methodological frame of the Ph.D.-project ...................... 89
3.3.1 Formal basis of the Ph.D. project ........................................................ 89 3.3.2 Description of the PUMA investigation.............................................. 90 3.3.3 The role of the researcher.................................................................... 93 3.3.4 Ethical considerations........................................................................ 101 3.3.5 Case study as research approach ....................................................... 103 3.3.6 Entering the field ............................................................................... 105
3.4 Research methods .................................................................................. 108 3.4.1 Description of the research field ....................................................... 109 3.4.2 Participant observation ...................................................................... 117 3.4.3 Qualitative research interview (single interviews)............................ 121 3.4.4 Group interview................................................................................. 129
3.5 Quality criteria used in the present study ........................................... 133 3.5.1 Proximity to the object of study ........................................................ 133 3.5.2 Reflexivity ......................................................................................... 134 3.5.3 Triangulation ..................................................................................... 135 3.5.4 Validity .............................................................................................. 136 3.5.5 Transferability ................................................................................... 136
Part II: Introduction of the result chapters (4-7)......................................... 138
Chapter 4: Engagement and burnout in midwifery .................................... 140 4.1 Introduction............................................................................................ 140 4.2 Reactions to the results of the PUMA study........................................ 140 4.3. Subjective descriptions of burnout...................................................... 145
4.3.1 Work-related burnout ........................................................................ 145 4.3.2 Emotions related to burnout .............................................................. 147 4.3.3 Behavioural aspects of burnout ......................................................... 149
4.4 Subjective descriptions of engagement at work.................................. 152 4.4.1 Professional self as sign of engagement............................................ 152 4.4.2 Work spirit as a sign of engagement ................................................. 153 4.4.3 Care for others and one’s self as a sign of engagement .................... 155
4.5 The relationship between engagement and burnout .......................... 157 4.6 Summary of findings on engagement and burnout in midwifery ..... 161
Chapter 5: Person-related and work-related factors................................... 165 5.1 Introduction............................................................................................ 165 5.2 Person-related factors............................................................................ 165
5.2.1 Biological age.................................................................................... 165
5
5.2.2 Generation membership .................................................................... 167 5.3 Structure of working time..................................................................... 169
5.3.1 Working in shifts and shift planning ................................................. 169 5.3.2 Work at night..................................................................................... 172 5.3.3 Part time work ................................................................................... 174 5.3.4 Work-family balance......................................................................... 175 5.3.5 Job routine ......................................................................................... 176
5.4 Summary of findings ............................................................................. 177
Chapter 6: The significance of resources in midwifery ............................... 179 6.1 Introduction............................................................................................ 179 6.2 Amount of resources and resource allocation practice ...................... 179 6.3 Balance between resources and job demands ..................................... 181
6.3.1 Balance of resources and demand to serve 100 percent.................... 181 6.3.2 Expertise, resources and security ...................................................... 184 6.3.3 Resources for client education .......................................................... 187
6.4 Summary................................................................................................. 188
Chapter 7: The role of emotional demands and feelings in midwifery...... 191 7.1 Introduction............................................................................................ 191 7.2 Emotional demands ............................................................................... 191
7.2.1 Reactions to rising demands from clients ......................................... 191 7.2.2 Demand to always give 100 percent service – regardless own feelings
and condition...................................................................................... 194 7.3 Emotional reactions to traumatic birth incidences ............................ 198
7.3.1 Experience with the handling of traumatic birth processes .............. 198 7.3.2 Feeling of responsibility and guilt..................................................... 201 7.3.3 Support and healing after traumatic incidences ................................ 205
7.4 Summary of findings concerning the role of emotional demands and feelings in midwifery............................................................................. 211
Chapter 8: Discussion ..................................................................................... 215 8.1 Introduction............................................................................................ 215 8.2 The nature of the primary task in midwifery and the relevance for the
research question................................................................................... 216 8.2.1 Essential characteristics of the primary task ..................................... 217 8.2.2 Demands and resources related to the primary task.......................... 218
8.3 Person related factors with relevance for the research question ...... 225
6
8.4 Assumptions about client-related factors of relevance to the research question .................................................................................................. 229
8.5 Structural and situational demands and conditions of work in midwifery ............................................................................................... 231
8.5.1 Impact of political decisions in the health care system..................... 232 8.5.2 Organisation of working time ........................................................... 235 8.5.3 Midwifery as a master piece of the female work role....................... 237 8.5.4 Relevance of implicit knowledge...................................................... 239 8.5.5 The significance and impact of traumatic birth incidences............... 242
8.6 Summary and conclusion of the explorative case investigation ........ 246 8.6.1 Strengths and limitations ................................................................... 249 8.6.2 Transferability of findings and reach of the study ............................ 252 8.6.3 Assumptions about the research field, directions for further research
and recommendations for midwifery practice ................................... 253
List of Figures .................................................................................................. 269
List of Tables.................................................................................................... 270
Appendices ....................................................................................................... 271
7
Acknowledgements The present Ph.D. thesis was written at the National Institute of Occupational Health (NIOH) in Copenhagen, Denmark which in cooperation with the Danish Research Agency provided me with the financial resources to carry out this research. The NIOH has been my physical workplace for the time living in Copenhagen and many of my colleagues at the NIOH have supported me in the course of this Ph.D. project. I want to thank: Vilhelm Borg for encouraging me to apply for the Ph.D. scholarship; The colleagues at the former psycho-social department of NIOH Copenhagen for welcoming me as non-Danish research colleague, holding space at times when my Danish was far from perfect and not at least for inspiring me professionally in many ways; Elizabeth Bengtsen, Rikke Nilsson, Birgitte Helm Nør, Elisabeth Frederiksen from the institute library, for their knowledgeable and friendly support in searching and ordering literature for me; the technical support staff at NIOH for help with connecting me virtually; Sofie LaCour Mosegaard who transcribed the interviews; Ingrid B. Lauritsen for support with the design and drawing of figures; Anna Garleff, Pia Gotterup, Bodil Holst for helping me with the problem of handling three languages by translating and correcting in a thorough and clear way. Palle Ørbæk, Kim Winding and Elsa Bach for having trust in me and going unconventional ways in regard to physical presence at work after our move back to Germany in April 2003. A special thanks to Marianne Borritz for being an exceptional friend and colleague. Those midwives who gave insight into their experience of motivation and burnout at work I want to thank. I honour their extracurricular interest and engagement by supporting me with invaluable insight in their field of work. This may be the place to explain about the picture on the cover of this Ph.D. thesis. It was painted of my 4-year old daughter Muriel on one of the busy days during the fall of this year. She gave it to me as a present and I put it up on the wall of my office at home. While I was finishing this thesis it caught my eye often and
8
sometimes I had the feeling it was talking to me about the midwives I was writing about. The expressive eyes, wide open, looking at the recipient of her service. The mouth is smiling a big smile but in the next moment is freezing into a stressed face. Large hands and fingers reaching out to help giving birth and yet seeming to be separated from the core of her body. It is a perfect picture to express what I have learned about motivation and burnout in midwifery which is content of the present Ph.D. thesis. Grateful thanks I owe Birgit Aust for taking responsibility of being the project supervisor at NIOH at a critical point of the project. The constructive feedback and structural help on the Ph.D. thesis has been an invaluable support. Furthermore, I want to thank Peter Olsén for taking the responsibility to be my main supervisor and helping me through the administrative jungle of a Ph.D. process. In Hamburg I want to thank Maren Masberg for opening the door to the qualitative research group at the University of Hamburg and for being a sparring partner in a short but exciting period of the project. A warm remembrance goes to Uschi Brucks an outstanding model of an impeccable researcher who died too early and whose knowledge and ‘firm scepticism’ I immensely missed in the last phase of the project A Ph.D. thesis cannot be written without the support in private life. A special thanks to Anne Sluhan, my dear American friend, who opened her house for me whenever I needed to be in Copenhagen for work, and who supported me emotionally through periods of ‘having enough’. ‘My’ AuPair girl Anna Baghdasaryan from Armenia deserves a big thank you for helping with all the practical things in the house. A loving thank you goes to my emotional buddy, spiritual source, and dear husband Frank for being just as he is. I dedicate this work to Muriel and Tali, my too little girls, who cheered me up at points of ‘burnout’ and showed me that life goes far beyond writing a Ph.D. thesis. Sunniva Engelbrecht Hamburg, December 2005
9
Abstract This Ph.D thesis summarizes the findings from a qualitative case investigation on the relationship between motivation and burnout carried out in the field of midwifery in Denmark. Major interest of the study was to understand the high burnout score amongst midwives in an ongoing six-year prospective intervention study in the human services sector (PUMA, Kristensen et al., 2005a). At baseline (1999-2000), and also in the three-year follow up (2002-2003), midwives were at the top of 15 job groups from the human services regarding burnout score measured with the Copenhagen Burnout Inventory (CBI, Kristensen et al., 2005a). Combined with the interest to understand the high score of burnout stood the interest to understand the relationship between motivation (engagement) and burnout in a job group which otherwise has one of the most meaningful primary tasks defined as “helping to give birth”. Midwives are known as a job group highly engaged in fulfilling their primary task. Therefore, it was both surprising and expected that midwives showed such a high level of burnout on each of the three scales of the CBI (personal, work-related, and client-related burnout) at baseline and consistently over time in the three year follow up investigation of PUMA. It was a surprise as those who were investigated in PUMA are still at work but nevertheless showed a high level of burnout. The high burnout score in PUMA can also be interpreted as expectable in the sense that a strong initial motivation is thought to be necessary in order to develop burnout (Freudenberger & Richelson, 1980; Pines, 1993; Burisch, 1989; Büssing, 1992; Schaufeli & Enzmann, 1998; Maslach et al. 2001). Following from this the aim of this case investigation was:
1. To reach an understanding of the high score of burnout amongst midwives in the PUMA study.
2. To gain insights into the relationship between motivation and burnout in midwifery in Denmark.
10
This project consists of two parts: the methodological summary and the empirical study. In the first part, the project describes the author’s theoretical ‘fore-understanding’ (Gadamer, 1960/1990) and delineates the methodological approach. This is done in some depth to clarify the frame of reference and to exemplify the explicit explorative approach into an established research field such as burnout research. In the empirical part, the author investigates the relationship between motivation and burnout using participative observation, single interviews, and a group interview following a case study approach. Fully transcribed interviews were analysed using the phenomenological method (Giorgi, 1985; Malterud, 1996). By using a qualitative in-depth approach grounded on a subject theoretical perspective (Dreier, 1993 & 1994 in Pedersen, 2002), the author sheds light on how the relationship between motivation and burnout in the field of midwifery can be understood. The case study approach yielded the following findings: Firstly, midwifery was described by the case study participants as highly-demanding with regards to work time, work pace, responsibility, low decision latitude, client demands, and emotional demands. A high level of engagement in the job was described as necessary precondition and is expressed as exceptionally professional self, good work spirit and high care for others, frequently leading to over-dedication and high commitment as well as an exaggerated feeling of responsibility as typical characteristics of a midwife. Some person-related and work-related factors of burnout were described by the participating midwives. Biological age and generation membership (understood as membership to a group being educated at the same time, having the same job age) were described as playing a role in the development of burnout. Younger generation midwives were described as having a different occupational identity from older generation midwives in regard to the acceptance of high demands and low resources at work. As work-related issues, working time was discussed. Shift work was viewed to be a critical and in principal unchangeable condition
11
of the midwife’s job, having negative impact on work-life balance. However, it was suggested that being more involved in the planning of shifts would improve the situation somewhat. Resources at work in form of number of employees proved to be a central theme in the single interviews and in the group interview. Resources were described to be low. Low resources were described to be a critical element in regard to the level of responsibility they feel to secure a safe and successful birth and were - in combination with high demands - thought to lead to work-related burnout. Resources were further described as being a critical factor in regard to the service given to the client. Low resources were described as being a stress factor because one’s own standards of service quality - especially in regard to security and time spent with the client in order to establish a trusting relationship (‘rapport’) - cannot be ensured. Emotional demands and feelings in midwifery were described as having significant impact on the relationship between motivation and burnout. Imbalance between clients’ demands and the occupational ideology and belief of the midwife was described as frustrating and the own job role is experienced as being called in question. Modern clients in midwifery were described as well-informed and demanding in regard to the treatment they wish to receive even if this stands in contrast to the recommendation of the midwife. ‘Giving of yourself’ was used as expression for the intensity of emotional availability while helping to give birth which is described as being tiresome when time to recover is low. The feeling of responsibility and guilt, and (not always successful) coping with traumatic birth incidences was discussed in depth in respect to their negative impact on health and well-being. Midwives referred to traumatic incidents as a ‘natural’ part of the job but described problems of transmitting this ‘belief’ to the emotional realm. Established procedures of debriefing and collegial supervision after traumatic birth incidences were viewed as being insufficient. This insufficiency was accused of sometime leading to post-
12
traumatic stress symptoms, which might contribute to the development of burnout. In conclusion, the findings of the present explorative investigation of the relationship between motivation and burnout in midwifery point to the necessity to understand the relationship between these two phenomena in their ecological context: the cultural, organizational, situational, and personal background. The findings gathered in this explorative study shed light on the particularities in midwifery in a Danish community hospital with regard to burnout. The study therefore contributes to a better understanding of the particular conditions of work in midwifery that play a role in the relationship between motivation and burnout. Even though the case approach chosen in this project is focussed on one particular setting, transferability of findings to other comparable settings (e.g., other maternity wards) is regarded as high because of the description of findings in relation to the primary task. Moreover, many new paths of investigation in the field are found in this explorative case study. Accordingly, the present Ph.D. thesis closes with new assumptions about the field of research to be investigated in further research projects.
13
Resumé Afhandlingen sammenfatter resultaterne fra en kvalitativ case-undersøgelse, som omhandler forholdet mellem motivation og udbrændthed blandt jordemødre i Danmark. I afhandlingen er der lagt stor vægt på at forstå den høje hyppighed af udbrændthed blandt jordemødre i et igangværende 6-årigt prospektivt interventionsstudie i socialsektoren (PUMA, Kristensen et al., 2005a). Ifølge CBI (Copenhagen Burnout Inventory, Kristensen et al., 2005a) viste baselineundersøgelsen (1999-2000) og den efterfølgende 3-års follow-up undersøgelse (2002-2003), at jordemødre lå i toppen af 15 udvalgte jobgrupper i den sociale sektor, hvor udbrændthed var mest markant. Foruden at fokusere på at få belyst den høje hyppighed af udbrændthed fokuseres der også på at få belyst forholdet mellem motivation (engagement) og udbrændthed indenfor en faggruppe, som normalt er karakteriseret som at have en af de mest meningsfyldte og vigtigste opgaver defineret som ”fødselshjælper”. Jordemødre hører til en faggruppe, hvor et stort engagement er påkrævet for at opfylde deres vigtigste opgave. Det var derfor meget overraskende og uventet, at jordemødre udviste en høj hyppighed af udbrændthed på hver af de tre CBI-skalaer (personligt, arbejdsrelateret og patientrelateret udbrændthed) ved baseline og konsekvent over tid. Det var overraskende, at de personer som deltog i PUMA-undersøgelsen stadig er i arbejde men ikke desto mindre udviste en høj hyppighed af udbrændthed. Den høje hyppighed i udbrændthed i PUMA kan også tolkes som forventet, dvs. forstået således, at en stærk motivation i begyndelsen er nødvendig før man kan komme til at føle sig udbrændt (Freudenberger & Richelsen, 1980; Pines, 1993; Burisch, 1989; Büssing, 1992; Schaufeli & Enzmann, 1998; Maslach et al. 2001). På baggrund af dette er formålene med denne undersøgelse følgende:
1. At forstå hvad der ligger bag den høje hyppighed af udbrændthed blandt jordemødre i PUMA-undersøgelsen, og
14
2. At få indblik i forholdet mellem motivation og udbrændthed indenfor jordemoderfaget i Danmark.
Projektet består af to dele: et metodeafsnit og en empirisk undersøgelse. Den første del omhandler forfatterens teoretiske ’forforståelse’ (Gadamer, 1969/1990) og skildrer hele problemstillingen mht. metode. Dette uddybes til en vis grad for at belyse referencerammen og for at eksemplificere den eksplicitte problemstilling mht. forskningen indenfor et etableret forskningsområde, som f.eks. udbrændthed. I den empiriske del undersøges forholdet mellem motivation og udbrændthed ved hjælp af deltager observation, personlige interviews og gruppeinterview efterfulgt af en caseundersøgelse. Detaljerede transskriberede interviews blev analyseret ved brug af fænomenologisk metode (Giorgi, 1985; Malterud, 1996). Ved brug af en kvalitativ tilgang baseret på et subjektteoretisk perspektiv (Dreier, 1993 & 1994 i Pedersen, 2002) kunne forfatteren kaste lys over en bedre forståelse af forholdet mellem motivation og udbrændthed indenfor jordemoderfaget. Caseundersøgelsen viste følgende resultater: for det første beskrev deltagerne i caseundersøgelsen jordemoderfaget som et meget krævende arbejde mht. arbejdstider, arbejdstempo, ansvar, lav beslutningsråderum, krævende gravide kvinder og følelsesmæssige krav. De typiske karakteristika for en jordemoder er at arbejdet kræver et højt engagement som en forhåndsbetingelse for jordemoderfaget, hvilket kommer til udtryk i en exceptionel og professionel personlighed, et godt arbejdsklima og en stor omsorg for andre, som ofte fører til en overdreven pligt- og ansvarsfølelse samt et højt engagement. Person- og arbejdsrelaterede faktorer indenfor udbrændthed blev defineret af jordemødre, som deltog i undersøgelsen. Det viste sig, at alder og ’generationstilhørsforhold’ (=tilhørsforhold til en gruppe, hvis medlemmer er uddannet på samme tidspunkt og har den samme alder) spiller en betydningsfuld rolle mht. udvikling af udbrændthed. Den yngre generation af jordemødre har
15
ifølge undersøgelsen en anderledes arbejdsidentitet end den ældre generation mht. at acceptere de høje arbejdskrav og de lave ressourcer. Mht. arbejdsrelaterede emner, blev arbejdstiden diskuteret. Skifteholdsarbejde blev betragtet som et kritisk og i princippet et uforanderligt forhold i arbejdsvilkårene, som har en negativ indflydelse på arbejdslivets balance. Imidlertid blev det foreslået, at hvis jordemødrene havde en større medindflydelse mht. planlægningen af vagterne ville dette forbedre arbejdsvilkårene væsentligt. Arbejdsressourcer i forhold til antallet af ansatte var et vigtig emne i både de personlige interviews og gruppeinterviewet. Ressourcerne var lave. Lave ressourcer var et kritisk element mht. den ansvarsfølelse, som jordemødrene føler de skal have for at sikre, at en fødsel foregår sikkerhedsmæssigt forsvarligt og bliver vellykket, og blev - samme med høje krav – mistænkt for at kunne føre til arbejdsbetinget udbrændthed. Derudover blev ressourcer beskrevet som værende en kritisk faktor mht. den service, der ydes til den fødende. Lave ressourcer blev beskrevet som en stressfaktor da ens egne normer for servicekvalitet – særligt mht. sikkerhed og tid brugt på den fødende med henblik på at etablere et tillidsfuldt forhold – ikke kan sikres. Emotionelle krav og følelser indenfor jordemoderfaget havde en betydelig indvirkning på forholdet mellem motivation og udbrændthed. Ubalance mellem den fødendes krav og den arbejdsmæssige ideologi og troen på jordemoderen blev opfattet som frustrerende og der sættes spørgsmålstegn ved ens egen arbejdssituation. Moderne fødende kvinder indenfor jordemoderfaget blev betegnet som velinformerede og krævende mht. den behandling de ønsker at modtage også selv om dette står i kontrast til jordemoderens anbefaling. ’At give dig selv’ blev brugt som et udtryk for den følelsesmæssige intensitet, som jordemoderen skal udvise overfor den fødende, hvilket beskrives som værende trættende når der er for lidt tid til at restituere sig bagefter. Følelsen af ansvar og skyld, og (ikke altid lige succesfuldt) coping i forbindelse med traumatiske
16
fødselsforløb blev diskuteret indgående af hensyn til deres negative indvirkning på helbredet og velbefindende. Jordemødre refererer til traumatiske fødselsforløb som en ’naturlig’ del af jobbet, men beskrev problemerne i at overføre denne ’tro’ til den emotionelle kategori. Etablerede procedurer mht. debriefing og til at følge op på kollegaer, der havde oplevet et traumatisk fødselsforløb blev karakteriseret som utilstrækkeligt. Denne utilstrækkelighed blev beskyldt for at føre til post-traumatiske stress-symptomer, der muligvis kan være en medvirkende årsag til udvikling af udbrændthed. Det må herefter konkluderes, at resultaterne fra undersøgelserne af forholdet mellem motivation og udbrændthed indenfor jordemoderfaget påviser nødvendigheden af at forstå forholdet mellem disse to fænomener i deres økologiske kontekst: den kulturelle, den organisations- og situationsmæssige samt personlige baggrund. Resultaterne fra denne undersøgelse kaster lys over enkelthederne indenfor jordemoderfaget på et dansk kommunehospital mht. udbrændthed. Undersøgelsen bidrager hermed til en bedre forståelse af de særlige arbejdsforhold, der gør sig gældende i jordemoderfaget, og som spiller en rolle i forholdet mellem motivation og udbrændthed. Selv om problemstillingen i denne afhandling fokuserer på et bestemt hospitalsmiljø, må overførbarhed af resultaterne til andre sammenlignelige omgivelser (f.eks. andre fødeafdelinger) regnes for at være høj pga. beskrivelsen af resultaterne i forhold til hovedopgaven. Desuden har afhandlingen bidraget med mange nye måder at undersøge det pågældende område på. Tilsvarende har antagelserne i denne Ph.D.-afhandling åbnet muligheden for yderligere fremtidige forskningsprojekter indenfor bestemte områder.
17
Chapter 1: Introduction 1.1 Research interest, research field and research question Human service work is to a high degree dependent on the people who deliver the service. To be good in providing good human service is dependent on very different factors such as education, skills, competencies, abilities, motivation, goal-orientation, passion, joy, interest, resources and not at least health and well-being. Quality in the human services is especially vulnerable to an impairment of any kind, hindering a person to deliver 100% service. The organizational structure of work and the conditions under which work is done are more or less enabling or hindering for the personal condition to be brought in. Burnout is often described as metaphor for suffering from doing ‘people work’ (Schaufeli & Enzmann, 1998; Kristensen et al., 2005a). Burnout as explicit outcome of work related stress in human service work was first discussed in the seventies (Freudenberger, 1974; Maslach, 1976). These first empirical descriptions of burnout were based on observations made in the field of human service work. Today, more than 5,500 empirical studies exist with the key word burnout in the title (Schaufeli & Enzmann, 1998). Nevertheless, we still cannot get a hold onto what is responsible for burnout in human service work (Burisch, 2002). A recurring theme in burnout research is the assumption that people who experience burnout must have been very engaged and enthusiastic about their work (Pines et al., 1981; Schmitz, 1998, 1999). Besides methodological weaknesses has this assumption shown to lead to equivocal results (Rösing, 2003). Traditionally, people in human service occupations have been regarded as being more prone to burnout than other job groups because of high communicative and emotional demands connected to doing people work. (e.g. clients, patients, customers). At the same time, many people working in human
18
service professions seem to be highly engaged and motivated to do the work they have chosen. However, the relationship still remains somewhat unclear. Even though the theoretical body of work on motivation and burnout in human service work is large, not much empirical research on the relationship between these phenomena can be found (Rösing, 2003). In Denmark, burnout has not been investigated in depth until the start of the PUMA project (1999) (Danish acronym for Project on Burnout, Motivation and Job Satisfaction) an ongoing six-year prospective intervention study in the human services sector (Kristensen et al., 2005a). One of the job groups with the highest levels of personal, work related , and client related burnout and high sickness absence at baseline and also later at three year follow up measured with the Copenhagen Burnout Inventory (CBI, Kristensen et al., 2005) were midwives. This has been both expectation and surprise. Midwifery is a field of work with high work demands (e.g. shift work, time pressure, high uncertainty, high physical demands) and therefore it was expected that some of the negative consequences in midwifery would show in lower levels of health and well-being in this job group. Otherwise it has been a surprise that the burnout score is the highest among 15 job groups in Denmark investigated in the PUMA study. At the same time midwives are known as an engaged job group with a highly satisfying and meaningful primary task. The coincidence of having a highly engaged work group with at the same time alarming high levels of burnout was predestination for this group to be investigated in more depth in the present Ph.D. project. Following from that the research question of the Ph.D. project has been formulated as: ‘How to understand the relationship between motivation and burnout in human service work-midwifery as case’.
19
The aims of the present Ph.D. project are: 1. To reach an understanding of the high score of burnout amongst midwives
in the PUMA study. 2. To gain insights into the relationship between motivation and burnout in
midwifery in Denmark. 1.2 Research approach In order to investigate how the relationship between motivation and burnout in midwifery can be understood a qualitative in depth approach was chosen. The complex meaning between structural, organisational, work related, client related, and personal factors leading into motivation or burnout can first be understood when as many facets as possible are investigated. A case study approach as chosen in the present project sets the frame to structure the investigation along a defined case. The group of midwives at a maternity ward in a Danish community hospital on Zealand was defined as case. Knowledge was gathered with three different methods: participative observation, single interviews, and a group interview. The group interview serves the purpose of communicative validation (member check) as findings from the single interviews are supported, supplied or a “rebellious” position is outlined. Participant observation is used to supply observations from the work environment to the narratives of the midwives. The present investigation is explorative in the sense of opening up new perspectives to look upon the two phenomena (motivation and burnout) in the context of midwifery and the relationship between the two. One important goal of this approach is “to investigate into the unknown”. To honour this goal, a phenomenological approach to the material has been chosen. Phenomenological data analysis empowers the researcher to be open for new interpretations emerging from the data material. Already established theory is regarded and
20
formulated as being part of the author’s fore-understanding1 understood as the backpack of practical and theoretical knowledge with which is looked upon the case. It plays an important role in setting the frame for interpretations in the present project. Existing theory is valued as important knowledge but is also looked upon with “firm scepticism” (Brucks, 1998). Scientific knowledge is defined as truth in process, to be confirmed over and over again in different settings as well as in new developments of society. With the vast amount of already existing publications in the field of burnout and motivation and the even faster growing volumes of scientific work, a definition of the theoretical reference frame as explication of one part of the author’s initial understanding is needed. From the tremendous body of work on motivation, four different approaches to motivation are used for reflection: the personality oriented concept of implicit and explicit motives, the concept of commitment as introduced by Meyer & Allen (1997), the concept of flow (Csikszentmihalyi, 1990), and the three dimensional model of engagement as published by Schaufeli et al. (2000, 2001). The theoretical description of burnout is more unequivocal. Comprehensive work and reviews published on burnout (e.g., Schaufeli & Enzmann, 1998, Rösing, 2003; Kristensen & Borritz, 1998; Söderfeldt, 1997) are part of the material used to reflect the empirical knowledge gathered through observations, interviews and group interviews. Within an approach to investigate into the unknown there must be space for new, unforeseen insights. A meta-goal of the present project is to exemplify how an open, qualitative approach in an otherwise well-defined research field can lead to impeccable scientific results, which lead to new perspectives and assumptions to look upon the phenomenon in context.
1 In the literature, different expressions for the German Vorverständnis (Gadamer, 1990) are used: fore-meanings, fore-conception, fore-structure of understanding, or fore-understanding. For the sake of consistencey fore-understanding is used in the present monograph.
21
1.3 Relevance Gathering more knowledge about the relation between motivation and burnout is relevant in regard to three different aspects. First, the relation between motivation and burnout which would explain the onset, development, and indeed the whole process of burnout, has not been investigated sufficiently in occupational health research. Especially complex and dynamic, ecological models to explain these phenomena in context are missing. Context specific knowledge (local understanding and theory) is meant to be an invaluable resource in order to understand the onset and development of burnout. The present project aims to establish a dialogue between different research traditions, theoretical assumptions and findings from the field in order to answer the research question. Second, relevance of the research question is found in the present organization and structure of work. The shift from mainly industrial work settings to human service work and knowledge based work has not attained enough recognition in work psychology models, concepts, and theory (Skovstad, Einarsen, 1996; Brucks, 1998). The late recognition of emotion work in work psychological theorizing (Ashkanasy, Härtel & Zerbe, 2000) is one example of the need to reflect on the appropriateness of traditional work psychology approaches (e.g. action theory) in modern work life. Third, midwives in Denmark (and also in other countries) face a change of working conditions as result of societal, organisational, and structural changes (e.g., health care sector as profit oriented business organization). These changes have impact on the recipients of service as well as on the service providers. Along with these actual changes go unchangeable conditions of the midwife’s job which can be regarded as stressful from the start. As the PUMA study has shown have these conditions negative impact on health and well-being of the investigated job group. Accordingly, the case investigation is not only relevant out of theoretical interest but also in a practical sense of providing practical knowledge for those who work in this field of human service work.
22
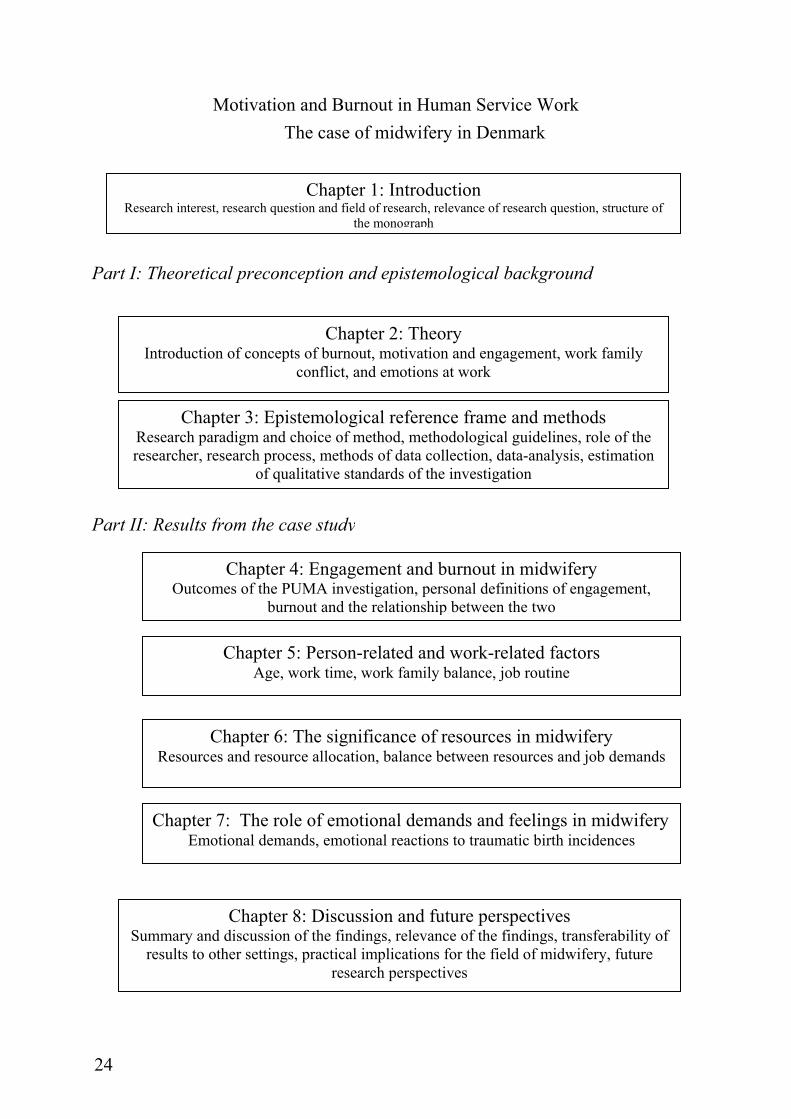
1.4 Structure of the monograph The present monograph is a combination of a traditional research report (introduction, theory, method, results, discussion) and a presentation of knowledge gathered within a dialogical, explorative case approach. Following the introduction, where the research interest, research field and research question along with reflections on relevance of the present investigation are introduced, the second chapter presents the theoretical reference frame as part of the author’s fore-understanding regarded as important for investigating the research question. Theory presented in Chapter 2 is understood as explicated fore-understanding which later is used as frame of reference for findings gathered in the present case investigation. Chapter 3 contains information about the epistemological reference frame and the research process. The methods used to investigate in the field and the form of data-analysis is described. Further, the quality of the study is estimated through reflecting on the qualitative standards of the investigation. Methodological guidelines (Malterud, 2001, Flick, 2002) are introduced as reflection of the research perspective. The third chapter also covers a reflection of the researcher’s role throughout the research process. The insights of the qualitative approach to understanding the relationship between motivation and burnout in human service work are presented throughout the following four chapters. In Chapters 4 to 7 the findings from the qualitative case investigation are presented in form of research themes illustrated by original citations. In Chapter 4, the subjective understanding and definition of the investigated concepts (burnout and motivation) as stated by the participants is summarized. In Chapter 5, background information is reported concerning work and person inherent factors, which are mentioned as having an impact on the relationship between motivation and burnout, as seen from the subjective perspective of the case study participants and from participative observation. In Chapter 6, the role of resources for being and feeling secure in the job is described. In Chapter 7, the role of emotional demands and feelings in midwifery is outlined. Especially the last two chapters open up unforeseen relations and new ways of thinking about the relationship between motivation
23
and burnout in human service work. In Chapter 8, the core statements and findings from Chapters 4 to 7 are summarized and reflected and related back to existing theoretical accounts in the field and explained along the primary task in midwifery. Challenges for further research are discussed and the practical implications of the findings for the field of midwifery are outlined.
24
Motivation and Burnout in Human Service Work The case of midwifery in Denmark
Chapter 3: Epistemological reference frame and methods Research paradigm and choice of method, methodological guidelines, role of the researcher, research process, methods of data collection, data-analysis, estimation
of qualitative standards of the investigation
Chapter 1: Introduction Research interest, research question and field of research, relevance of research question, structure of
the monograph
Chapter 4: Engagement and burnout in midwifery Outcomes of the PUMA investigation, personal definitions of engagement,
burnout and the relationship between the two
Chapter 5: Person-related and work-related factors Age, work time, work family balance, job routine
Chapter 6: The significance of resources in midwifery Resources and resource allocation, balance between resources and job demands
Chapter 7: The role of emotional demands and feelings in midwiferyEmotional demands, emotional reactions to traumatic birth incidences
Chapter 8: Discussion and future perspectives Summary and discussion of the findings, relevance of the findings, transferability of
results to other settings, practical implications for the field of midwifery, future research perspectives
Chapter 2: Theory Introduction of concepts of burnout, motivation and engagement, work family
conflict, and emotions at work
Part II: Results from the case study
Part I: Theoretical preconception and epistemological background
25
Chapter 2: Theory 2.1 Introduction and organisation of the chapter In the following chapter, a summary of the most relevant and most discussed issues in the field of burnout and motivation is given. The chapter is divided into five parts. After the introduction, main insights from the last 30 years of burnout research are summarized and reflected on (2.2). The historical development of burnout research, the theoretical and operational definitions of the phenomenon, the measurement of burnout, the challenges and shortcomings of recent burnout research and implications for the future are discussed. In the second section (2.3), five approaches to motivation are introduced. Motivation is an umbrella term for very different approaches. Therefore, the approaches to be introduced are thought to be the most relevant in regard to the research aim of the present Ph.D. project. In the third section (2.4) the one existing study on burnout in midwifery is summarized as well as a choice of the most relevant and recent empirical studies on the relationship between motivation and burnout in human service work. Fourth (2.5), recent research on work family balance is introduced. In section 2.6 different concepts and aspects of emotions at work are reflected on. Finally, in section 2.7 the theoretical reference frame representing the fore-understanding of the author of the present Ph.D. project is summarized. 2.2 Burnout research throughout the last 30 years The concept of burnout has undergone an impressive career from observational description to a scientifically defined term to an everyday description of mood state. In the context of the present work, it is regarded as important to take a look at the historical development of the concept and the public’s reception of the term.
26
2.2.1 Historical development from phenomenon to syndrome
Already in the 1950ies Isabel Menzies led a case study in nursing with the aim to facilitate desired social change (Menzies, 1975). Her psychodynamic approach using in-depth interviews, observations, and other informal contacts with the staff of the hospital brought her attention to a high level of tension, distress, and anxiety among the nurses. The symptoms she described following from her observation relate very much to what was 20 years later labelled burnout (Pedersen, 2002). This is one example that the phenomenon of burnout has been present long before the expression burnout was coined to describe the phenomenon. However, Herbert Freudenberger’s publication on staff burnout in 1974 is commonly referred to as the starting point for the broader recognition of burnout. Freudenberger made the observation that volunteers entering the field of social work usually walk through a phase of more or less severe wear out after approximately one year. Freudenberger began to use the term burnout to describe the experience of emotional depletion and loss of motivation and commitment. At almost the same time, Christina Maslach (1976) began to investigate how people in emotionally demanding jobs such as doctors, nurses, police officers cope in everyday work. Through interviews she found three themes that seemed to be important: emotional exhaustion, detached concern towards clients and a feeling of reduced personal accomplishment. This early work was dominated by qualitative descriptions of symptoms and the situational context. Interviews, case-studies and on-site observations were the way to approach the phenomenon in this phase (Maslach et al. 2001). These first cautious but impressive steps towards doing mostly qualitative burnout research are from a recent perspective (Schaufeli & Enzmann, 1998) often described as provisional form of doing burnout research. The empirical phase of burnout began in the 1980s with the publication of the Maslach Burnout Inventory (Maslach & Jackson, 1982). This quantitative approach to burnout has become the predominant burnout measure. Other instruments developed throughout the same time period, e.g. Burnout Measure
27
(Pines, Aronson & Kafry, 1981), OLBI, Oldenburg Burnout Inventory (Ebbinghaus, 1986, in Rösing, 2003) never reached the same popularity as the MBI. The MBI was first designed to measure burnout in human service work but with the growing interest from work and organizational psychologists, a more general view of burnout as a prolonged reaction to job stress in different occupations developed and raised the quest for a more general measurement tool. In 1996 the MBI-general Survey was published (MBI-GS; Schaufeli et al., 1996) which allows burnout to be studied independently from its specific job context. The MBI is translated into many different languages and is used as a global instrument to measure burnout. Burnout is, amongst others, one of the best-known concepts in modern psychology. The catchy nature of the phenomenon, the short and handy operational definition of burnout and a vast amount of publications has furthered and manifested the interest in burnout. The clinical and the empirical approach to burnout coexist ever since burnout was described. However, until recently most of the many burnout studies were cross-sectional and therefore did not allow causal inference (Kristensen & Borritz, 1998). Lately the methodological rigor of burnout research has improved (Schaufeli & Buunk, 2004). Especially since the late 1990s an increasing number of longitudinal studies have been conducted (Borritz, 2005). One of the newer developments in burnout research is the extension of the burnout concept by the positive antithesis job engagement, so that the full spectrum of workers well-being can be studied (Maslach et al., 2001; Schaufeli et al. 2002; Schaufeli & Buunk, 2004). Being developed from field observations rather than from theory, most burnout research has been rather atheoretical. Throughout the last years, the voices for a theoretical and empirical re-formulation of burnout became louder (Söderfeldt, 1997; Schaufeli & Enzmann, 1998; Kristensen & Borritz, 1998; Burisch, 2002; Rösing, 2003). According to Schaufeli & Buunk (2004) a growing number of
28
comprehensive conceptual approaches have proposed to link burnout to mainstream psychological theories. Nevertheless, there is a quest for more theory-driven approaches to burnout. With the introduction of a new tool to measure burnout (Kristensen et al., 2005a) the discussion about the main dimensions of the burnout concept has been taken up again and is currently ongoing (Schaufeli & Taris, 2005) (see also below).
2.2.2 Burnout: symptoms, definitions, and measurement
The following section gives an overview of the symptoms, definitions, and ways to measure burnout. After 30 years of burnout research has seen from sociology of science perspective reached the status of being an established field of research. However, burnout has neither reached the status of a disease (recognition in the classification systems for diseases (ICD-10 or DSM-IV) nor the status of an institutionalised field of research (Rösing, 2003). Söderfeldt (1997) refers to the Danish philosopher Uffe Juul Jensen in order to describe how burnout is recognized inside and outside the scientific community. Jensen uses the distinction between ideal and practice concepts of diseases. “The ideal concept refers to the situation where a concept exactly specifies those phenomena that are connoted by it. A practice concept refers to practical abilities, exertion of practical routines of some kind, never exactly delineated (Söderfeldt, 1997, p. 44)”. A disease is regarded as a historical phenomenon, starting as a classification of symptoms, leading into a syndrome, and eventually being called a disease. Historically, syndromes either disappear or become diseases. A practice concept of a disease is an ongoing, negotiable process of describing a phenomenon. This perspective helps to approach burnout as an open concept; a phenomenon in progress, and a “subjective” term. Nevertheless, many different approaches to describe burnout exist. In the following, a list of symptoms is introduced, the common definitions of burnout are summarized and approaches to measure burnout are discussed.
29
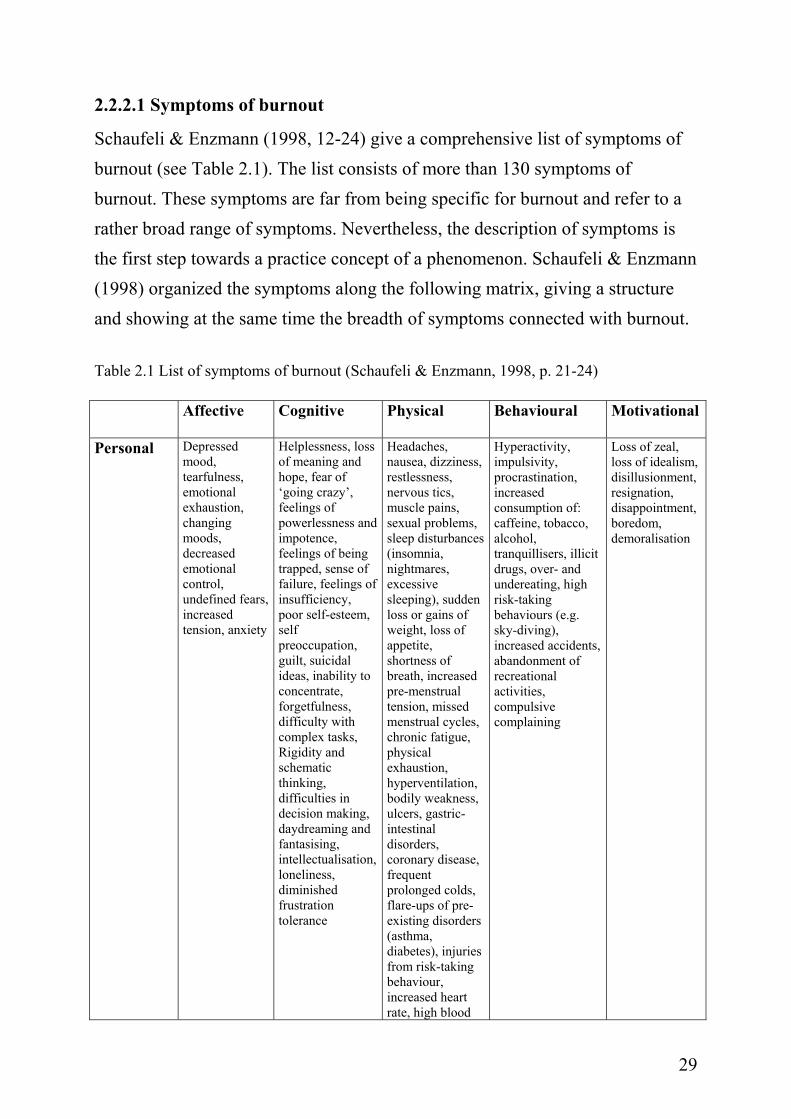
2.2.2.1 Symptoms of burnout
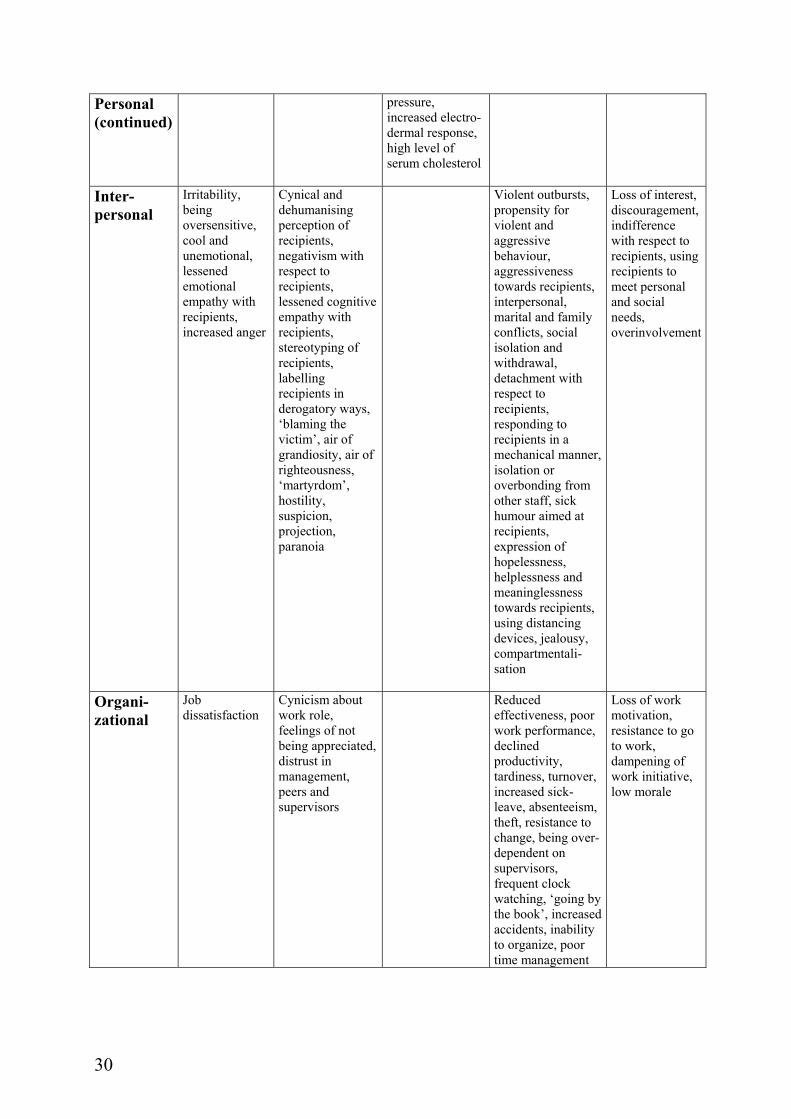
Schaufeli & Enzmann (1998, 12-24) give a comprehensive list of symptoms of burnout (see Table 2.1). The list consists of more than 130 symptoms of burnout. These symptoms are far from being specific for burnout and refer to a rather broad range of symptoms. Nevertheless, the description of symptoms is the first step towards a practice concept of a phenomenon. Schaufeli & Enzmann (1998) organized the symptoms along the following matrix, giving a structure and showing at the same time the breadth of symptoms connected with burnout. Table 2.1 List of symptoms of burnout (Schaufeli & Enzmann, 1998, p. 21-24) Affective Cognitive Physical Behavioural Motivational
Personal
Depressed mood, tearfulness, emotional exhaustion, changing moods, decreased emotional control, undefined fears, increased tension, anxiety
Helplessness, loss of meaning and hope, fear of ‘going crazy’, feelings of powerlessness and impotence, feelings of being trapped, sense of failure, feelings of insufficiency, poor self-esteem, self preoccupation, guilt, suicidal ideas, inability to concentrate, forgetfulness, difficulty with complex tasks, Rigidity and schematic thinking, difficulties in decision making, daydreaming and fantasising, intellectualisation, loneliness, diminished frustration tolerance
Headaches, nausea, dizziness, restlessness, nervous tics, muscle pains, sexual problems, sleep disturbances (insomnia, nightmares, excessive sleeping), sudden loss or gains of weight, loss of appetite, shortness of breath, increased pre-menstrual tension, missed menstrual cycles, chronic fatigue, physical exhaustion, hyperventilation, bodily weakness, ulcers, gastric-intestinal disorders, coronary disease, frequent prolonged colds, flare-ups of pre-existing disorders (asthma, diabetes), injuries from risk-taking behaviour, increased heart rate, high blood
Hyperactivity, impulsivity, procrastination, increased consumption of: caffeine, tobacco, alcohol, tranquillisers, illicit drugs, over- and undereating, high risk-taking behaviours (e.g. sky-diving), increased accidents, abandonment of recreational activities, compulsive complaining
Loss of zeal, loss of idealism, disillusionment, resignation, disappointment, boredom, demoralisation
30
Personal (continued)
pressure, increased electro-dermal response, high level of serum cholesterol
Inter- personal
Irritability, being oversensitive, cool and unemotional, lessened emotional empathy with recipients, increased anger
Cynical and dehumanising perception of recipients, negativism with respect to recipients, lessened cognitive empathy with recipients, stereotyping of recipients, labelling recipients in derogatory ways, ‘blaming the victim’, air of grandiosity, air of righteousness, ‘martyrdom’, hostility, suspicion, projection, paranoia
Violent outbursts, propensity for violent and aggressive behaviour, aggressiveness towards recipients, interpersonal, marital and family conflicts, social isolation and withdrawal, detachment with respect to recipients, responding to recipients in a mechanical manner, isolation or overbonding from other staff, sick humour aimed at recipients, expression of hopelessness, helplessness and meaninglessness towards recipients, using distancing devices, jealousy, compartmentali-sation
Loss of interest, discouragement, indifference with respect to recipients, using recipients to meet personal and social needs, overinvolvement
Organi-zational
Job dissatisfaction
Cynicism about work role, feelings of not being appreciated, distrust in management, peers and supervisors
Reduced effectiveness, poor work performance, declined productivity, tardiness, turnover, increased sick-leave, absenteeism, theft, resistance to change, being over-dependent on supervisors, frequent clock watching, ‘going by the book’, increased accidents, inability to organize, poor time management
Loss of work motivation, resistance to go to work, dampening of work initiative, low morale
31
Lists of symptoms are impressive for illustrating the broad character of the recent description of burnout, but they are also confusing, as they do not lead to differential insight and are not useful as basis for research. Schaufeli & Enzmann (1998, p. 30) summarize the following problems in regard to “laundry-lists” of symptoms:
1. Most symptoms result from uncontrolled observations rather than from empirical studies. Validity might be low.
2. Symptoms listed are rather indefinite. 3. Throughout the process of development of burnout symptoms may change
from one symptom into the opposite, e.g. over- or under-involvement 4. Different patterns of burnout are assumed, showing different groups of
symptoms. 5. Symptoms, precursors, and consequences of burnout are confused.
Schaufeli and Tarris (2005) point out that the strategy to include as many burnout characteristics as possible should be discouraged. Instead, they recommend looking for the smallest number of core symptoms that bear theoretical meaning and that are sufficient to characterize burnout.
2.2.2.2 Working definitions of burnout
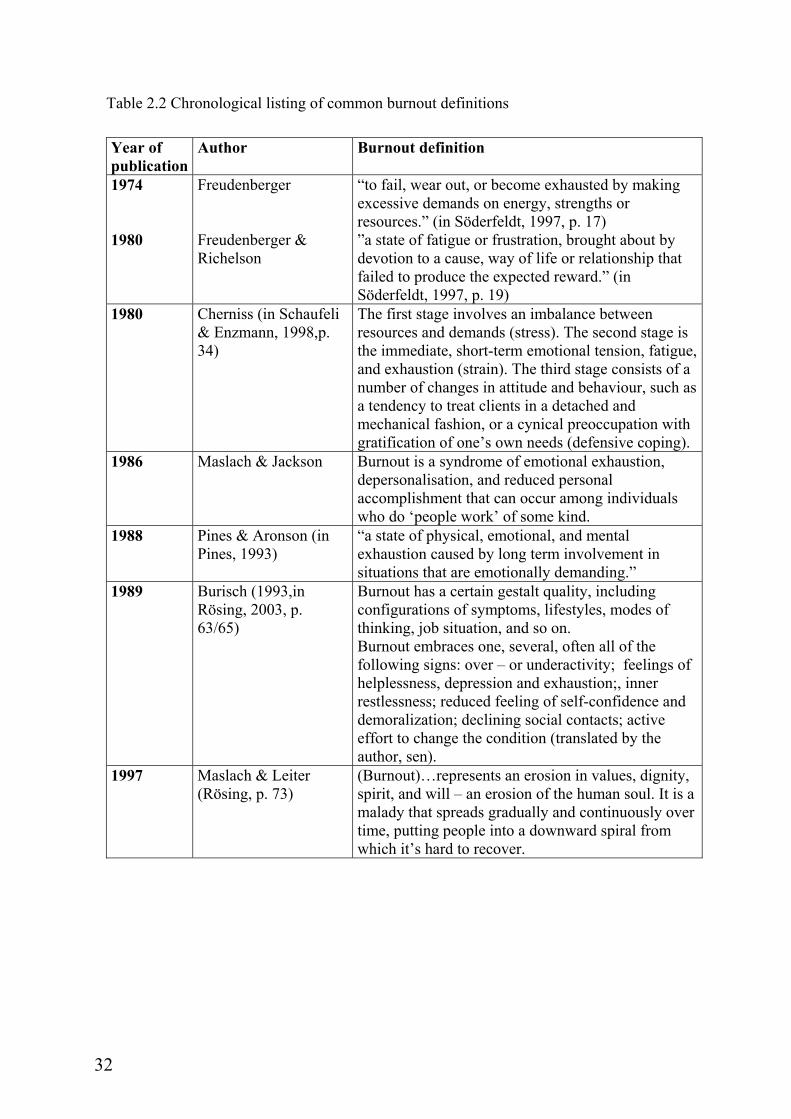
Definitions of burnout always focus on a certain facet of the phenomenon. State and process definitions of burnout can be distinguished. In the following table, selected definitions are listed chronologically regarding year of publication. The list of definitions is not comprehensive but it summarizes the most known and probably most often cited burnout definitions. Beyond that, a rather broad spectrum of international burnout definitions is gathered in the table below, referring to English, Scandinavian and German publications on burnout.
32
Table 2.2 Chronological listing of common burnout definitions
Year of publication
Author Burnout definition
1974 1980
Freudenberger Freudenberger & Richelson
“to fail, wear out, or become exhausted by making excessive demands on energy, strengths or resources.” (in Söderfeldt, 1997, p. 17) ”a state of fatigue or frustration, brought about by devotion to a cause, way of life or relationship that failed to produce the expected reward.” (in Söderfeldt, 1997, p. 19)
1980 Cherniss (in Schaufeli & Enzmann, 1998,p. 34)
The first stage involves an imbalance between resources and demands (stress). The second stage is the immediate, short-term emotional tension, fatigue, and exhaustion (strain). The third stage consists of a number of changes in attitude and behaviour, such as a tendency to treat clients in a detached and mechanical fashion, or a cynical preoccupation with gratification of one’s own needs (defensive coping).
1986 Maslach & Jackson Burnout is a syndrome of emotional exhaustion, depersonalisation, and reduced personal accomplishment that can occur among individuals who do ‘people work’ of some kind.
1988 Pines & Aronson (in Pines, 1993)
“a state of physical, emotional, and mental exhaustion caused by long term involvement in situations that are emotionally demanding.”
1989 Burisch (1993,in Rösing, 2003, p. 63/65)
Burnout has a certain gestalt quality, including configurations of symptoms, lifestyles, modes of thinking, job situation, and so on. Burnout embraces one, several, often all of the following signs: over – or underactivity; feelings of helplessness, depression and exhaustion;, inner restlessness; reduced feeling of self-confidence and demoralization; declining social contacts; active effort to change the condition (translated by the author, sen).
1997 Maslach & Leiter (Rösing, p. 73)
(Burnout)…represents an erosion in values, dignity, spirit, and will – an erosion of the human soul. It is a malady that spreads gradually and continuously over time, putting people into a downward spiral from which it’s hard to recover.
33
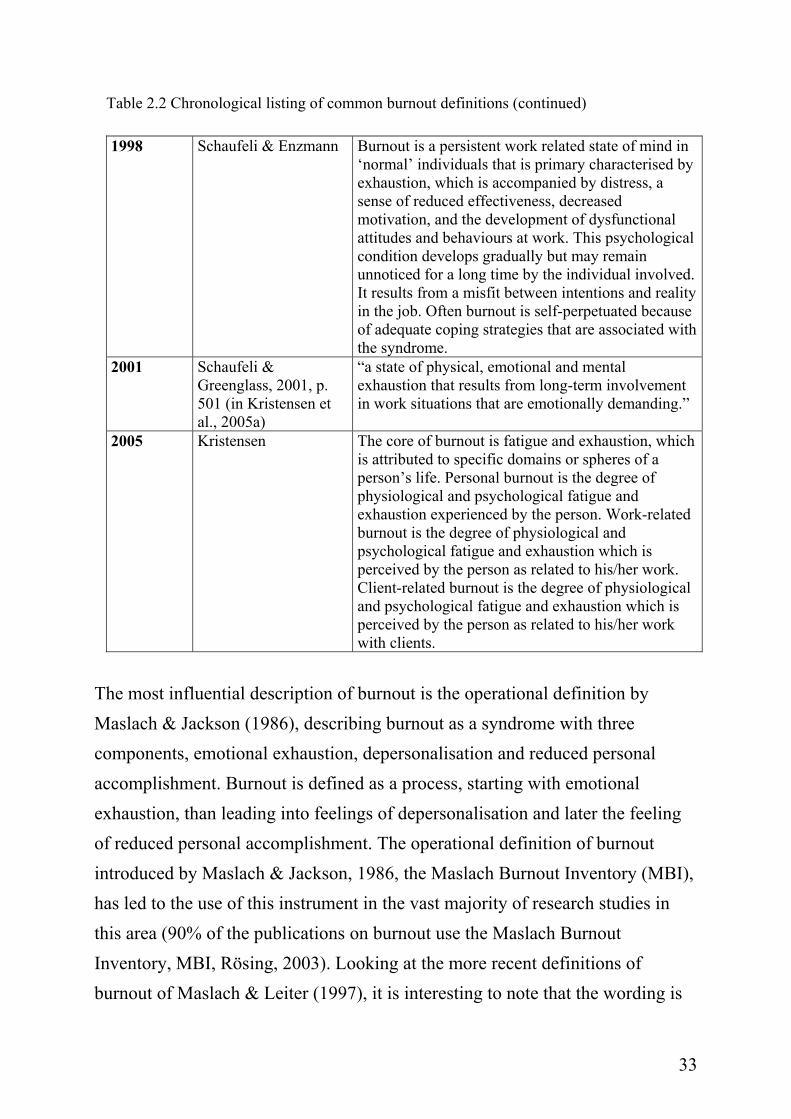
Table 2.2 Chronological listing of common burnout definitions (continued)
1998 Schaufeli & Enzmann Burnout is a persistent work related state of mind in ‘normal’ individuals that is primary characterised by exhaustion, which is accompanied by distress, a sense of reduced effectiveness, decreased motivation, and the development of dysfunctional attitudes and behaviours at work. This psychological condition develops gradually but may remain unnoticed for a long time by the individual involved. It results from a misfit between intentions and reality in the job. Often burnout is self-perpetuated because of adequate coping strategies that are associated with the syndrome.
2001 Schaufeli & Greenglass, 2001, p. 501 (in Kristensen et al., 2005a)
“a state of physical, emotional and mental exhaustion that results from long-term involvement in work situations that are emotionally demanding.”
2005 Kristensen The core of burnout is fatigue and exhaustion, which is attributed to specific domains or spheres of a person’s life. Personal burnout is the degree of physiological and psychological fatigue and exhaustion experienced by the person. Work-related burnout is the degree of physiological and psychological fatigue and exhaustion which is perceived by the person as related to his/her work. Client-related burnout is the degree of physiological and psychological fatigue and exhaustion which is perceived by the person as related to his/her work with clients.
The most influential description of burnout is the operational definition by Maslach & Jackson (1986), describing burnout as a syndrome with three components, emotional exhaustion, depersonalisation and reduced personal accomplishment. Burnout is defined as a process, starting with emotional exhaustion, than leading into feelings of depersonalisation and later the feeling of reduced personal accomplishment. The operational definition of burnout introduced by Maslach & Jackson, 1986, the Maslach Burnout Inventory (MBI), has led to the use of this instrument in the vast majority of research studies in this area (90% of the publications on burnout use the Maslach Burnout Inventory, MBI, Rösing, 2003). Looking at the more recent definitions of burnout of Maslach & Leiter (1997), it is interesting to note that the wording is
34
different. Here, burnout is described as “an erosion of the soul”, using complex words such as “values”, “dignity”, and “spirit”. This is an example of a softer, less distinct definition of burnout. This form of describing burnout sounds a bit like a homecoming to the “pioneer phase” of burnout research. One of the most recent definitions of burnout, described as working definition of burnout, is formulated by Schaufeli & Enzmann (1998) (see Table 2.2). This rather long and comprehensive definition is a compilation of different burnout definitions, all sharing common basic assumptions: (1) the three dimensional syndrome as defined by Maslach, burnout as a state of emotional exhaustion, depersonalisation and resulting in a reduced feeling of personal accomplishment. (2) Burnout as work related without defining what is meant by work. (3) Burnout is further defined, as a process, often undiscovered for a long period in time, not stopped by effective coping mechanisms. Last but not least (4) one cause for the development of burnout is seen in the misfit between expectations and realities on the job. This definition is useful in the sense that it summarizes some of the unequivocal findings in burnout research. The chronological listing shows further that: (1) Similar definitions of burnout appear in a short time interval to each other and are persistent over time. In all definitions, emotional exhaustion is regarded as the core of burnout. Burnout is also defined as developing over time. (2) In mainstream burnout research the reception and definition of burnout has not evolved much in the last 30 years of research, even though societal changes have been tremendous. There is a clear parallel between Pines & Aronson’s definition of burnout from 1988 and Schaufeli’s & Enzmann’s definition from 1998 (Kristensen et al., 2005a). Referring back to the idea of a practice concept of diseases, developing over time, changing, or disappearing, the concept of burnout has been rather steady. Besides the mainstream of burnout research, there are voices calling for a different understanding of burnout (Kristensen et al., 2005a; Pedersen, 2002). (3) In more recent definitions of burnout, there is no restriction to the sphere of “people work”. This was one of the core assets of the operational definition of
35
burnout from Maslach & Jackson (1986). Burnout is, in most publications, defined as restricted to the sphere of work but spill-over effects to private life are discussed (Burke & Greenglass, 2001).
2.2.2.3 Measurement of burnout
Most scientific research work in the field of burnout is based on the Maslach Burnout Inventory (MBI, Maslach & Jackson, 1986). The MBI is a self-report paper and pencil test, asking about the three facets of the burnout syndrome as defined by Maslach & Jackson (1986). The MBI measures burnout in regard to the three independent key dimensions: emotional exhaustion (depletion or draining of emotional resources caused by interpersonal demands), depersonalisation (development of negative, callous and cynical attitudes toward the recipients of one’s services) and reduced personal accomplishment (the tendency to evaluate one’s work with recipients negatively). Originally, the burnout concept was thought to be restricted to professionals who deal directly with recipients, but in 1996 the concept of burnout was broadened and defined as a crisis in one’s relationship with people at work. The three original dimensions of the MBI were broadened to encompass not just problems with regard to people work: Exhaustion now refers to fatigue irrespective of its cause. Cynicism reflects an indifferent or distant attitude towards work instead of other people and lack of professional efficacy encompasses both social and non-social aspects of occupational accomplishment (Schaufeli & Buunk, 2004). The career of the MBI is impressive. Translations into many languages are existent and the MBI is used in different countries around the globe. In regard to using the MBI for diagnostic purposes, it should be noted that there does not exist a cut-off point indicating where serious burnout starts. However, In the Netherlands clinically validated cut-off scores have bee developed recently that allow discrimination of ‘burnout cases’ from ‘non-cases’ (Schaufeli et al., 2001, in Schaufeli & Taris, 2005). The MBI must be seen as an instrument for research purposes and not suitable for making individual diagnoses.
36
Recently, Kristensen et al. (2005a) introduced a new tool to measure burnout: The Copenhagen Burnout Inventory (CBI). The instrument was developed in the course of the PUMA Study, a longitudinal study of burnout in human service workers in Denmark, which also gave the incentive to this PhD thesis. Although in the starting phase of the PUMA study, the MBI was considered as the main measurement tool for burnout, after careful consideration and testing, it was decided to not use the MBI but to develop a new measurement tool instead. The authors (ibid) name the following reasons for this decision: (1) The MBI is based on a circular argument by stating that burnout is restricted to persons in human service job. Even though extended versions exist, the main feature of the test stayed the same. (2) The relationship of the MBI to the concept of burnout is unclear. Burnout research has been engaged in a lively discussion about burnout being constituted of three independent dimensions (as proposed by the measurement with the MBI) or of burnout being a phenomenon with the exhaustion, depersonalisation, and diminished personal accomplishment as characteristics. (3) The understanding of burnout being a syndrome with the three constituting characteristics is neglecting the possible interpretation of depersonalisation being a coping strategy and diminished personal accomplishment being an effect. The last argument to be named is (4) the wording of the MBI was not accepted by the Danish participants, causing negative reactions and even anger. Many good reasons to develop an instrument that takes some of the criticism mentioned into account. With the Copenhagen Burnout Inventory, Kristensen et al. (2005a) introduce an interesting and different operational approach to burnout based on a comprehensive review of theoretical and empirical material. After a detailed testing of three instruments (Burnout Measure (BM), Pines et al., 1981; MBI and MBI-GS, Maslach et al. 1981, 1986.) and a review of research work in the field, it was decided to develop a new instrument but remaining in the general frame of reference of burnout research (Kristensen et al., 2005a). The CBI is
37
designed after careful investigation of existing instruments to measure burnout on the background of theoretical assumptions. The authors of the CBI claim in accordance with many other burnout researchers that exhaustion is the core of burnout (ibid). However, Kristensen et al. (2005) point out that burnout is not the same as the already existing concepts of fatigue and exhaustion. They write “In our understanding of the concept the additional key feature is the attribution of fatigue and exhaustion to specific domains or spheres in the person’s life.” (ibid, p.197). The three main domains most important in this respect are defined by the authors as the personal domain, the work domain and more specific the work with client domain. The CBI is therefore designed with three different scales: (1) a scale measuring general exhaustion, called personal burnout, (2) a scale on work-related burnout, and (3) a scale on client-related burnout. The questions of the personal burnout scale are inspired by the Burnout Measure questionnaire, the question of work-related burnout are inspired by the subscale on emotional exhaustion of the MBI/MBI-GS questionnaires. The questions on client-related burnout are newly formulated. The burnout scales of the CBI correlate with each other but the correlation is only partial, supporting the idea of three independent burnout scales (Borritz et al., 2005). The already existing studies have shown, that the various occupational groups revealed different patterns on the three scales, indicating that the measurement of burnout in different domains is possible using the CBI. Especially the dimensions work- and client related burnout refer to the concept of schemata and causal attributions people use to explain the experience of symptoms, such as headaches, nausea, coughs, chest pain , prolonged fatigue, etc. (Kristensen et al., 2005a). Symptoms are explained in the light of already existing schemata (Bishop, 1991; Eysenck & Keane, 1990; in Kristensen et al., 2005a). The way by which people build schemata is through causal attribution to internal or external factors. The same symptom can therefore be interpreted in different ways. Already now the CBI has been translated into a number of languages and studies are on the way to elucidate the acceptability and validity of the CBI. An
38
investigation of burnout amongst dentists in Australia (Winwood & Winefield, 2004) compared outcomes measured with the MBI and the CBI. The authors report that the basic psychometric properties for the CBI appear to be equivalent to those of the MBI. The results of the MBI were not found to be in line with the suggested concept of burnout, i.e. that high scores on the MBI Exhaustion subscale would be associated with high scores on the Depersonalization subscale and low scores on the Personal Accomplishment subscale. Therefore the authors conclude that the value of these two MBI subscales is called into question. Furthermore Winwood and Winefield propose that the CBI, with its simpler conceptualization of burnout as fundamentally a fatigue phenomenon, should be investigated further. However, the discussion of advantages and disadvantages of the CBI and the MBI and their respective theoretical and conceptional foundations has only just started. Several articles in the July-September 2005 issue of the Work & Stress journal comment the introduction of the CBI and the reasons for its development. The recent discussion shows that the long hold basis of the burnout concept is currently being debated from within the scientific community of burnout research. For many of the open questions it is helpful to draw to the many studies conducted in the past, other issues need to be studied further with new investigations using different approaches. This PhD thesis does not directly contribute to the ongoing discussion about how many dimensions should be used to measure burnout, as it was not the goal of this study. However, this in-depth study of the understanding of burnout and its manifestation in Danish midwives does shed some light on the subjective perception of burnout in human service work as concluded in Chapter 8. Furthermore, is with reference to the subject theoretical approach to burnout research (Pedersen, 2002) a different perspective introduced in the present thesis (see below).
39
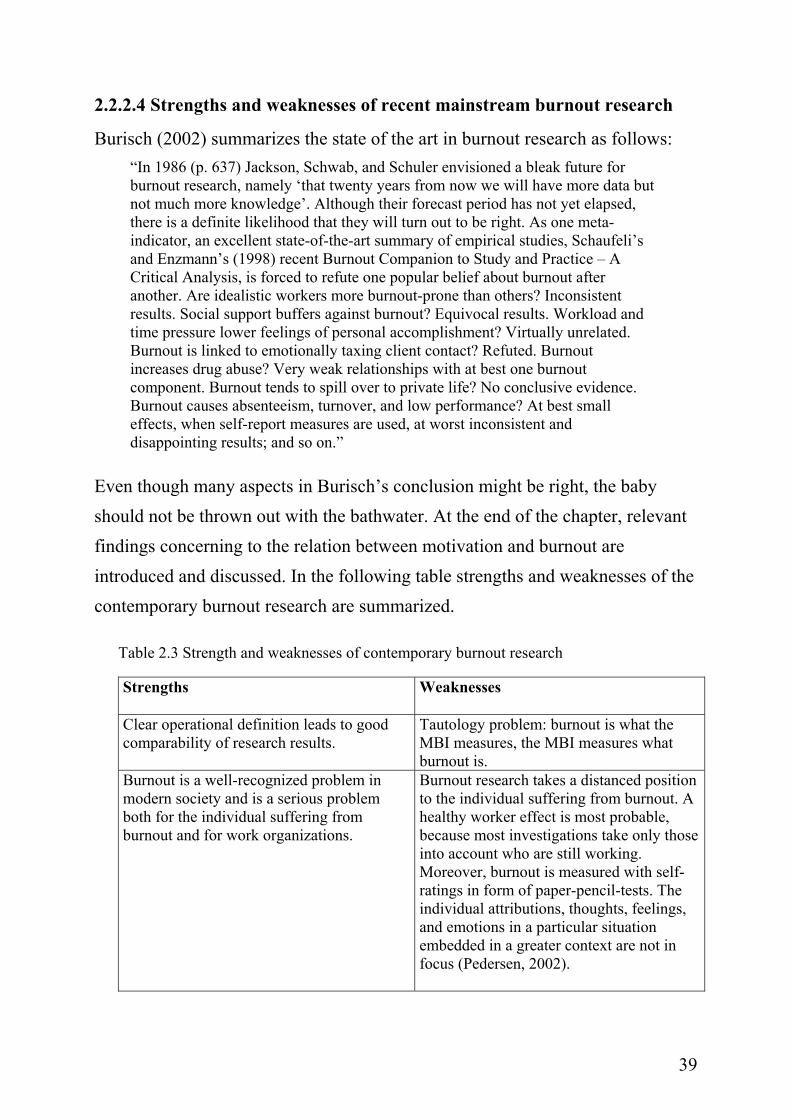
2.2.2.4 Strengths and weaknesses of recent mainstream burnout research
Burisch (2002) summarizes the state of the art in burnout research as follows: “In 1986 (p. 637) Jackson, Schwab, and Schuler envisioned a bleak future for burnout research, namely ‘that twenty years from now we will have more data but not much more knowledge’. Although their forecast period has not yet elapsed, there is a definite likelihood that they will turn out to be right. As one meta-indicator, an excellent state-of-the-art summary of empirical studies, Schaufeli’s and Enzmann’s (1998) recent Burnout Companion to Study and Practice – A Critical Analysis, is forced to refute one popular belief about burnout after another. Are idealistic workers more burnout-prone than others? Inconsistent results. Social support buffers against burnout? Equivocal results. Workload and time pressure lower feelings of personal accomplishment? Virtually unrelated. Burnout is linked to emotionally taxing client contact? Refuted. Burnout increases drug abuse? Very weak relationships with at best one burnout component. Burnout tends to spill over to private life? No conclusive evidence. Burnout causes absenteeism, turnover, and low performance? At best small effects, when self-report measures are used, at worst inconsistent and disappointing results; and so on.”
Even though many aspects in Burisch’s conclusion might be right, the baby should not be thrown out with the bathwater. At the end of the chapter, relevant findings concerning to the relation between motivation and burnout are introduced and discussed. In the following table strengths and weaknesses of the contemporary burnout research are summarized.
Table 2.3 Strength and weaknesses of contemporary burnout research
Strengths
Weaknesses
Clear operational definition leads to good comparability of research results.
Tautology problem: burnout is what the MBI measures, the MBI measures what burnout is.
Burnout is a well-recognized problem in modern society and is a serious problem both for the individual suffering from burnout and for work organizations.
Burnout research takes a distanced position to the individual suffering from burnout. A healthy worker effect is most probable, because most investigations take only those into account who are still working. Moreover, burnout is measured with self-ratings in form of paper-pencil-tests. The individual attributions, thoughts, feelings, and emotions in a particular situation embedded in a greater context are not in focus (Pedersen, 2002).
40
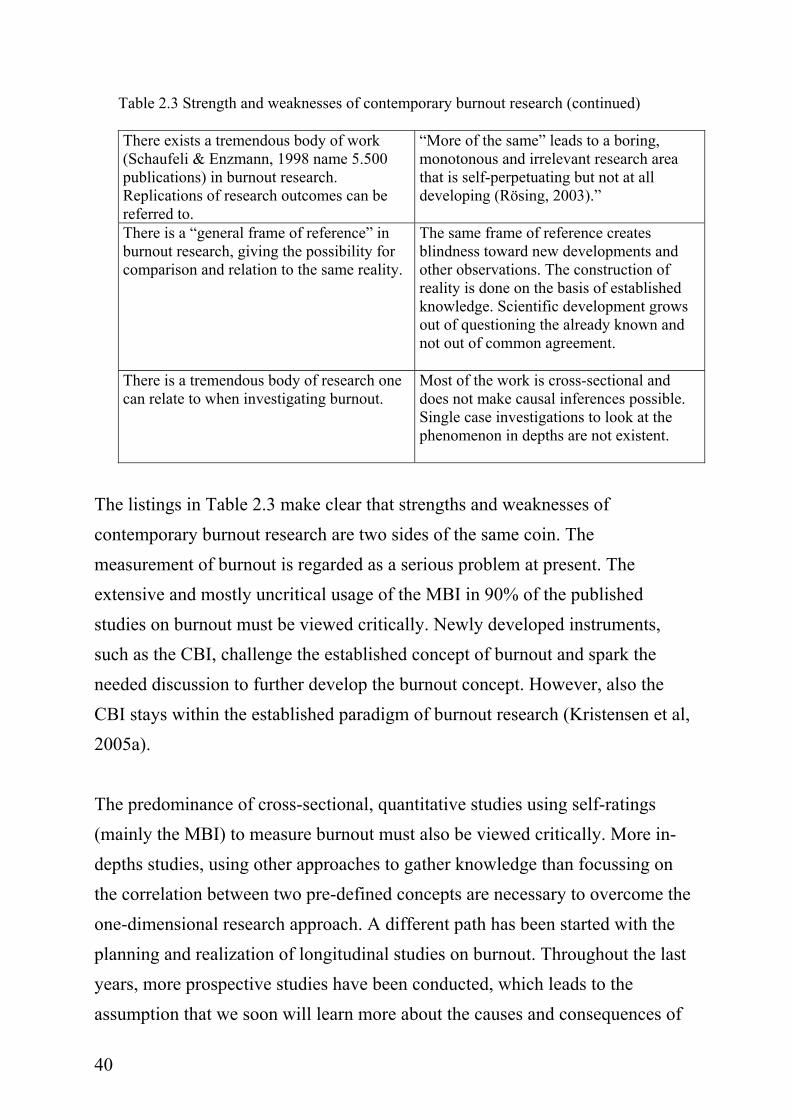
Table 2.3 Strength and weaknesses of contemporary burnout research (continued)
There exists a tremendous body of work (Schaufeli & Enzmann, 1998 name 5.500 publications) in burnout research. Replications of research outcomes can be referred to.
“More of the same” leads to a boring, monotonous and irrelevant research area that is self-perpetuating but not at all developing (Rösing, 2003).”
There is a “general frame of reference” in burnout research, giving the possibility for comparison and relation to the same reality.
The same frame of reference creates blindness toward new developments and other observations. The construction of reality is done on the basis of established knowledge. Scientific development grows out of questioning the already known and not out of common agreement.
There is a tremendous body of research one can relate to when investigating burnout.
Most of the work is cross-sectional and does not make causal inferences possible. Single case investigations to look at the phenomenon in depths are not existent.
The listings in Table 2.3 make clear that strengths and weaknesses of contemporary burnout research are two sides of the same coin. The measurement of burnout is regarded as a serious problem at present. The extensive and mostly uncritical usage of the MBI in 90% of the published studies on burnout must be viewed critically. Newly developed instruments, such as the CBI, challenge the established concept of burnout and spark the needed discussion to further develop the burnout concept. However, also the CBI stays within the established paradigm of burnout research (Kristensen et al, 2005a). The predominance of cross-sectional, quantitative studies using self-ratings (mainly the MBI) to measure burnout must also be viewed critically. More in-depths studies, using other approaches to gather knowledge than focussing on the correlation between two pre-defined concepts are necessary to overcome the one-dimensional research approach. A different path has been started with the planning and realization of longitudinal studies on burnout. Throughout the last years, more prospective studies have been conducted, which leads to the assumption that we soon will learn more about the causes and consequences of
41
burnout. Schaufeli & Enzmann (1998) report an interesting observation that cross-sectional findings with respect to job-demands on burnout could not be replicated in longitudinal studies. They assume that this might also be due to methodological problems (using regression approaches instead of simple change scores from time one to time two). A general frame of reference is positive when relating to the same phenomenon. However, especially with phenomena changing over time and situation it is also regarded as important to discuss different approaches to burnout which do not refer to a mainstream approach of burnout research. Pedersen (2002) makes a pledge for a subject theoretical approach, investigating forms of practice as historical, concrete, and situated by taking the first person’s perspective. In a subject theoretical approach relations between situational conditions, a person’s concrete actions, and the reasoning behind these actions is investigated. Instead of questions of cause and effect of single characteristics in relation to burnout (e.g., personality, work conditions, or subjective expectations) complex, dynamic relations are in the center of attention. In doing this, the researcher as person is involved in a different way then being involved in sending out a burnout questionnaire to an unknown person. This is in fact one fundamental difference between quantitative and qualitative research: the researcher as person suddenly has a face and needs to be referred to. A subject-theoretical approach always includes the relationship of societal conditions and the concrete situation and action of the person investigated and the interpretation and reasoning behind this action. In a subject theoretical approach the context gives meaning to a phenomenon. Therefore, the context stands in the center of investigation. In the case of burnout it is for example interesting to compare different job groups in regard to their primary task, what kind of actions need to be taken to fulfil the task and how does the person perceive the fulfilment of the task. By comparing different jobs and contexts this way it becomes obvious where the differences between jobs of the same categories are, e.g. human service jobs. Pedersen is criticising burnout research as one example for research
42
using categories as diagnosis for a single person or a job group without looking at the specific constellation of context. By doing this the category burnout becomes a label and a self-perpetuating process. This is also referred to by Kristensen et al. (2005a) pointing to the fact that burnout can be seen as a self-perpetuating process: at the moment that results about investigations of burnout are communicated to recipients, burnout is regarded as an unavoidable consequence of their specific work setting. A subject theoretical proposal to overcome some of the problems named by Pedersen (2002, p. 74) is to “investigate burnout as a development of manifold and different subjective interpretations of action strategies in regard to different historical and local aspects of the development and organisation of work.” Even though many burnout researchers (e.g., Schaufeli & Enzmann, 1998; Kristensen & Borritz, 1998; Söderfeldt, 1997; Burisch, 2002; Rösing, 2003) think that a qualitative approach to investigating the phenomenon could be helpful to understanding some of the open questions in the field, not much has happened (Rösing, 2003). It is a striking fact that qualitative, in depth studies which take the subjective, the individual and the specific into account are hardly known. Although burnout research originates in the description of subjective states (Freudenberger, 1974; Maslach, 1976), the scientific development of the phenomenon has forgotten about the quality of the qualitative. This is mainly due to the rules of the main scientific community emphasizing big, statistically sophisticated, and objective study of the phenomenon (Rösing, 2003). So far, burnout research has undergone a metamorphosis from being a promising new field of psychological research to developing into an image of its own conditions. The distance between researcher and person participating in a research study is huge and has parallels to the state of burnout described as depersonalised (Rösing, 2003). Kirkcaldy, Athanasou & Trimpop (2000) introduced a new and promising qualitative approach in the field of stress research. The focus of the approach is the subjective understanding of the work context and the idiosyncratic
43
perception of stress and diverse situational determinants. The authors summarize that nomothetic methods are useful for thinking generally about occupational health and stress whereas single case approaches help to detect parameters important to understanding the phenomenon in this specific context. In somewhat the same direction Söderfeldt (1997) argues in regard to understanding burnout. She claims that burnout should not be understood as an ideal concept but rather as a “social construction”, as a concept with reference in real life. With regard to this Ph.D. thesis burnout as social construction points to an understanding of the phenomenon as being bounded in a specific context (here: the job practices of the midwives), understood with a certain connotation (here: challenges and demands of the ‘helping to give birth’), and valued in a specific way (here: the organizational and situational problems at the ward which lead to frustrations and feelings of being burned out) (see discussion in Chapter 8). Definitively, the theoretical foundation of burnout needs to be developed further. There is some agreement about the weak theoretical foundation of burnout research (Schaufeli & Enzmann, 1998; Rösing, 2003; Pedersen, 2002). Schaufeli & Enzmann (1998, p. 101) distinguish four sets of theoretical approaches to burnout: individual, interpersonal, organisational, and societal. In conclusion, they propose an integrative and descriptive model of burnout as a “heuristic model that schematically summarizes common issues that are included in the previous approaches (ibid, p. 140).” As three recurrent themes, Schaufeli and Enzmann (1998) propose: (1) a strong initial motivation as a necessary precondition for the development of burnout; (2) the relation of burnout to an unfavourable job environment; and (3) burnout as self-perpetuating process because of inadequate coping strategies. A heuristic model is one way to react to the theoretical vacuum or fuzziness in burnout theory. An open framework of burnout could be another way out of the dilemma. A complex but comprehensive framework of burnout would help on a meta-theoretical level to organize research as well as the observation and cure of burnout. On a
44
theoretical level it would help to re-think burnout by understanding burnout as a phenomenon, which leaves space for idiosyncratic perceptions, subjective interpretation and causal attributions.
2.2.2.5 Prevention and cure of burnout
Another important aspect neglected in burnout research so far is the question of a cure for burnout. As blurry and fuzzy as the description of burnout is, the recommendation of what to do to prevent or cure burnout is far reaching. The catalogue reaches from meditation to medication, from activation to vacation, from running to yoga, and so forth. As in many other forms of psychological distress, cure is often accompanied by a long search for the right therapy. To test the reality of burnout in practice, Söderfeldt (1997) left the ivory tower of scientific research and went to the marketplace for burnout cures (e.g., convenience sample of acupuncturist, homeopaths, psychotherapists, and two health stores). Her conclusion is that many people know what to do about burnout and much is earned in curing it. If these approaches in practice are goal directed or trial and error led is left to one’s own appraisal. Kalimo et al. (2003) investigated work characteristics and personal resources that are associated with the burnout symptoms in the long term. They conclude that the paths to burnout and to well-being are drastically different. According to them, the development of burnout is furthered by weaknesses in the organizational climate and by unrewarding work as well as in the person’s lack of feelings of self-worth and competence. Well-being, on the other hand, is based on strong internal personal resources and challenging work. Therefore, “the prevention of burnout should include both enhancement of the possibilities for developing the employees’ personal resources and improvement of the social processes at work (ibid, p. 120).” Thinking about prevention and cure of burnout always brings the question of complexity of the issue into sight. It should be kept in mind that a complex phenomenon such as burnout is not curable with simple recommendations. Rather, a thorough investigation of causes and resources in a
45
certain setting can bring about a meaningful strategy to prevent and cure burnout. This PhD study, with its in-depth qualitative approach is one example of such an investigation which is needed to understand the specific circumstances for burnout in a particular job group.
2.2.2.6 Summary
Burnout is regarded as a complex phenomenon in context, with emotional exhaustion as core property. Further, it is regarded as a process, developing (and re-developing) in stages with differential properties. In this sense, burnout is understood as reversible. Personality is thought to have an influence on the onset (proneness), development, and the coping with burnout. Taking the context into account, new and important aspects for burnout research come into focus, e.g. the cure for burnout and the prevention of it. Burnout can develop in very different contexts, not only in human service work. One might want to differentiate the sources of burnout. From the individual’s point of view, burnout causes can originate in personal as well as social problems. Last but not least, burnout causes tremendous suffering, which needs some form of serious recognition beyond the recommendation of “Go, take a break!” Beyond that, is burnout understood as a slowly developing process throughout which a person and his/her social field need to be attentive to early changes of a person’s attitude, behaviour, and decline in emotional well-being. This is to a certain point paradoxical because burnout processes are slowly developing, most of the times first recognized when serious limitations have occurred. By any means this is a huge challenge for most modern work places where resources are cut-down to a minimum. Burnout research has a poor theoretical foundation. This is due to the complexity of the phenomenon and the in some parts existing overlap to other concepts. An approach taking the subjective into account will open up new perspectives in the field. The recommendation to investigate single cases in order to understand the subjective causes and consequences of burnout better
46
(Schaufeli, 1998; Burisch, 2002; Rösing, 2003) is put into practice with the present case study of motivation and burnout in midwifery. 2.3 Selected motivation concepts Motivation is an umbrella term for a wide array of very different concepts in psychology, ranging from attitude, belief, idealism, involvement, commitment, goals, expectancies, intentions, aspirations and meaning, to emotions. The interest in motivational concepts in work and organizational psychology lies in their ability to explain why people put effort and energy into the things they are engaged in. Motivation in the work setting is best described by referring to what a person does (direction), how hard a person works (intensity), and how long a person works (persistence) (Kanfer, 1990). In order to organize motivational constructs, Kanfer (1990) groups them in three related paradigms: (a) need-motive-value, (b) cognitive choice, and (c) self-regulation-metacognition. Theories in the need-motive-value paradigm look at the role of personality, stable dispositions, and values as a basis for behavioural variability. Theories in the cognitive choice paradigm focus on cognitive processes involved in decision-making and choice. The description of motivation in the third paradigm focuses on self-governing cognitive mechanisms that determine the transformation of motivational force into behaviour and performance. Further, motivation theories can be posed on a continuum of proximal and distal constructs. The impact of distal constructs on behaviour and performance is often indirect. At this end, needs, personality and interests might be found. Proximal constructs, on the other hand, focus on motivational constructs at the level of purposive action, e.g. goal setting theory (Locke & Latham, 1984). Distal and proximal theories of motivation generate complementary knowledge about the motivational system. In this following section, three relevant concepts of motivation in relation to work life are introduced, representing different motivational approaches on the continuum from proximal to distal and the three paradigms described above.
47
First, a functional approach to motivation (Kuhl, 2000) with roots in McClelland’s concept of power, achievement, and attachment motivation (1987), self-regulation theory and new developments in cognitive and personality psychology is introduced. Second, commitment research is introduced being defined as an applied form of cognitive choice models of motivation. Third, the concept of flow is presented as proximal concept of motivation. The concept of flow is regarded to be important because of the emergent quality of the experience and the possibility of describing an emotional experience in motivational terms. Along with the three constructs of motivation, two recently developed models of engagement from within burnout research are portrayed: the three dimensional concept of engagement from Schaufeli et al. (2001, 2002) and the rephrasing of burnout as an erosion of engagement with the job (Maslach & Leiter, 1997). To conclude, not the most prominent but, from the author’s point of view, the most promising concepts are introduced, representing different paradigms in motivation theory which can be related to concepts of health and well being at work, and more specific burnout.
2.3.1 Implicit and explicit motivation
The first concept to be introduced relates back to the beginnings of motive measurement in the early fifties of the last century. At that time, there was no “reliable measurement methodology for human motivation (Niitamo, 1999, p. 21)”. However, there was already a strong belief in two different motive systems: an implicit and an explicit system. The basic idea behind this thought is that personality is not totally accessible through consciousness but that to a certain degree, our personality functions on a conscious as well as subconscious (or nonconscious) level (here referred to as ‘in depth’). It was close at hand that this in depth personality is not to be measured through self-report because it is non-conscious and therefore not accessible through self-report measures. Two different traditions of motive measurement started to flourish side by side. The

48
first concentrates on self-reports to assess human motivation and the second relates to projective (fantasy) techniques in order to reach deeper levels of personality (e.g. Murray, 1933, in Niitamo, 1999). Motives measured in fantasy are called implicit motives and those measured through self-reports are called self-attributed motives (McClelland, 1989). ”Implicit motives seem to be better at predicting spontaneous, self-generated behaviors and behavioral trends over time and behavior in field settings. Explicit motives seem better at predicting specific responses in situations in which the incentives are explicit” (Niitamo, 1999, p. 27). Implicit and explicit motives seem to function in different motivational subsystems. Important in the context of the present work is the consequence of this assumption. If, in fact, two different motivational subsystems exist, they should be measured with different instruments. McClelland, Koester & Weinberger (1989, p. 697) emphasize the importance of measuring implicit motives with operant measures, because implicit motives seem more likely to be built on affective experiences with natural incentives early in life, before the development of language. Self-attributed motives are developed later in life, after concepts of the self, others, and what is valuable have been acquired. In 2000, Kuhl introduced an integrative framework of cognition, motivation and emotion; the personality systems interactions theory- PSI. This integrative approach wants to step beyond the shortcomings of previous motivation theories by merging personality trait approaches with motivation and action theoretical constructs. On the basis of the belief that cognitive content is not sufficient to explain volitional action, a functional-design approach to motivation and self-regulation is introduced (Kuhl, 2000). The rather complex theory shall not be explained further and the introduction may stay on a surface level, because it would exceed the frame of the present project to take it in depth. Most important at this point is the understanding that the early trend in motivational research to differentiate between the implicit and explicit
49
dimensions has recently found more and more scientific recognition and proves to be a valuable motivational approach - also in applied research (Niitamo, 1999). The PSI theory provides an integrative framework by combining knowledge about personality traits with approaches to motivation, volition, and emotion. The concept of implicit and explicit motivation is valued as important perspective in the work context, as implicit motivational processes are thought to have important influence and consequences for well-being (Brunstein, Schultheiss, Grässmann, 1998). Moreover, the implicit component of motivation is a neglected side, especially in work motivational research. This is interesting as in research on knowledge transfer and transactional memory systems in organizations concepts of implicit knowledge are of exceptional importance for the understanding of information processing and knowledge development in modern organizations (Masberg, 2004). Furthermore, has implicit knowledge proved to have an influence on the emotional exchange of a person with his/her environment (Herbig, 2001).
2.3.2 Commitment
Organizational commitment can most concisely be described as “a psychological state linking employees to their organization” (Meyer & Allen, 1997, p. 23). There is some consensus among commitment researchers to understanding commitment as a multidimensional construct, but less consensus about what kind of dimensions there are to be described. The most prominent model of commitment at the workplace at the moment is the three dimensional model (ibid). According to this model, commitment can be described by (a) the employee’s relationship to the organization (affective commitment), (b) the awareness about the costs of leaving the organization or the need to remain there (continuance commitment), and (c) the felt obligation to continue employment in the organization (normative commitment). Commitment is commonly regarded as a win-win-situation for employer and employee: for the individual commitment is thought to lead to a feeling of social identity; for the
50
organization, commitment is assumed to lead to benefits ranging from better performance to lower absence. However, evidence from research shows that the picture is more complex. In a meta-analysis of 35 studies, Randall (1990, in Tan & Akhtar, 1998) could show that higher levels of commitment had stronger positive relationships with attendance, effort, and continuing employment with the organization than with actual job-performance. Moreover, several researchers started to question the overemphasis of positive consequences of organizational commitment, formulating possible negative consequences of commitment. Organizational commitment in these approaches is regarded as possible source of psychological strain. Keenoy (1992, in Tan & Akhtar, 1998) terms this dilemma a “motivation-control” equation, which asks for greater autonomy and generous rewards for employees in order to reach greater commitment. Another critical view of commitment as form of managerial control is inspired by Hochschilds’ work (1983). She uses the term emotional labour in order to describe employees who are trained to modify their behaviours in accordance with organizational expectations of their emotional responses to customers. This facet of organizational commitment, operating on the affective domain, is meant to have negative consequences for the health and well being of the employee. The body of research work on commitment is complex and for the purpose of this short theoretical introduction of the concept, it might be enough to conclude that affective commitment has the strongest effect on an employee’s performance. Findings on commitment and employee well-being summarized by Meyer & Allen (1997) show that there is rather weak evidence that affective and normative commitment enhance employee well-being. Nonetheless, there is some evidence that affective commitment might have positive consequences whereas continuance commitment has negative consequences for employee well being. Thus, there is a need to investigate these relations in depth. It should also be noted that positive and negative outcomes of commitment depend to a large extent on the perspective from which commitment is looked at. An overly committed employee might perform highly satisfactorily but at the same time

51
develop serious health problems, such as burnout, because he/she does not take the time to care for herself. Tan & Akhtar (1998) stress the point that organizational commitment has culturally-bound connotations. The influence of culture on the globally used construct of commitment might be a strong predictor when investigating the relation of commitment and health related outcome factors, such as burnout. Dlugos & Friedlander (2001) formulate a working definition of passionate commitment based on the concepts of optimal experience (‘Flow’, Csikszentmihalyi, 1990), burnout and burnout prevention (Cherniss, 1995; Grosch & Olsen, 1994) and commitment (Marks, 1976 in Dlugos & Friedlander, 2001). Passionate commitment is defined as (a) a sense of being energized and invigorated by one’s work, (b) the ability to continue to love and thrive on one’s work; (c) be in balance in other life areas; and (d) a sense of energizing and invigorating those with whom one works. On this conceptual background, twelve peer-nominated psychotherapists were interviewed to provide an understanding of their high levels of work-commitment by identifying behavioural, existential, interpersonal, and personality factors that they might have in common. For the purpose of testimonial validity (Stiles, 1994; in Dlugos & Friedlander, 2001), self-ratings were conducted as well. Interesting in the context of the present project is the result that all persons interviewed showed a high level of personal accomplishment, suggesting that participants viewed themselves as competent and successful in their work. The results for emotional exhaustion and depersonalisation reach from low to moderate (two scoring high on depersonalization) but remain uncommented on by the authors. In summary, the concept of commitment introduced above is thought to supply an interesting perspective when investigating the research question of how to understand the relationship between motivation and burnout throughout the following chapters. The inclusion of the commitment concept as one possible addition to understanding work motivation addresses explicitly the relationship
52
between the organization and its different levels and the person working in a particular setting. In reference to the three paradigms described by Kanfer (1990), commitment is regarded as a cognitive choice approach to motivation.
2.3.3 Flow
Mihaly Csikszentmihalyi first introduced the concept of ‘flow’ 30 years ago (Csikszentmihalyi, 1990). Flow describes a state of optimal experience; an optimal balance between opportunity and ability, according to its own requirements, without interruptions. This kind of experience is called autotelic, referring to the Greek words autos=self and telios=goal; self-rewarding. The state of optimal experience is described by the following characteristics: (1) Merging of action and awareness; distortion of time perspective; (2) undivided intentionality because of clear goals; knowledge about means to reach these goals; and last but not least clear feedback; (3) a loss of self-consciousness – in a positive way; attention is focussed on the demands of the activity and not the self as an object of awareness. Csikszentmihalyi calls this state emergent motivation, a motivation which comes from within the person and is “triggered by specific experiences which provide unique rewards never before encountered (ibid, p. 99)”. Flow experiences can occur in almost any situation in life, but work has shown to be the activity which is most often associated with flow experiences (Csikszentmihalyi & LeFevre, 1989). Intense concentration, involvement, and loss of self-consciousness occurs most frequently when working and not at leisure (Csikszentmihalyi, 1985, p. 105). The capacity to experience flow can be regarded as an important personal skill. At the same time, conditions that further the experience of flow “will affect the ease with which people may find optimal experiences (Csikszentmihalyi, 1985, p. 107).” Flow is defined as the optimal balance between challenge and skill. In situations where skill is greater than challenge, boredom is present. On the other side,
53
when challenge is greater than skill, anxiety is present. Flow is defined as the diagonal between challenge and skill. At the lower end of the diagonal, anxiety and boredom are most likely to occur. At the higher end, flow is more likely to occur. A necessary precondition for the continued experience of flow in a certain situation is the range of increasing challenges. If challenges are limited, flow will occur up to the point where routine is reached. Routine at work for example is often experienced as positive state because of the control and security reached. At the same time, routine might lead to boredom when challenges are no longer present. To describe it in Csikszentmihalyi’s words: “Higher up the diagonal, behaviour is more complex because more differentiated responses are required to meet the demands of the situation. Therefore, the experience might be described as being more ‘deep’, since the cognitive and affective skills involved require more psychic energy to acquire, and the attention is more concentrated” (Csikszentmihalyi, 1985, p. 109). This process leads to personal growth.
2.3.4 Motivational concepts developed from within burnout research
Just recently, the two internationally predominant research groups in burnout research have started to show interest in the positive side of burnout. Christina Maslach and her colleague Michael Leiter, as well as the group around Wilmar Schaufeli, have developed an antipode to burnout, called engagement.
2.3.4.1 Engagement as antipode of burnout
Maslach & Leiter were the first to step beyond the pathological model of burnout as a negative psychological state by enlarging the concept through the positive antithesis of burnout; job engagement. Burnout is rephrased as an erosion of engagement with the job (Maslach et al., 2001). This relation can be described between the two poles of burnout and engagement. Burnout is, as before, defined as the three-dimensional model of emotional exhaustion, cynicism, and ineffectiveness. Engagement, on the other hand, is defined by
54
energy, involvement, and efficacy; the direct opposites of the three burnout dimensions. In the process of burning out, “energy turns into exhaustion, involvement turns into cynicism, and efficacy turns into ineffectiveness” (Maslach et al. 2001, p. 416). According to the authors of the concept, engagement can be differentiated from other established constructs in organizational psychology, such as job satisfaction, organizational commitment, or job involvement. Engagement focuses on the relation to the work itself, unlike organizational commitment, where the employee’s allegiance to the organization is centre of attention. Job satisfaction is defined as the source of need fulfilment and contentment. Job involvement is similar to one component, involvement, but does not include energy and effectiveness. Engagement seems to be the broader concept, providing a complex and thorough perspective on an individual’s relationship with work.
2.3.4.2 Engagement as a persistent, positive affective-motivational state
The second, recent approach towards engagement from within burnout research comes from the Netherlands. The research team around Wilmar Schaufeli developed an instrument to measure engagement. The concept of engagement grew out of a theoretical analysis (Schaufeli &Bakker, 2001) where two underlying dimensions of work-related well-being could be identified: (1) activation of the poles exhaustion and vigour, and (2) identification, ranging from cynicism to dedication. The third concept, absorption, is included in engagement; whereas reduced professional efficacy is enclosed in burnout. Absorption and reduced professional efficacy are not poles of a continuum but conceptually rather distinct from each other. Engagement is understood as a positive antithesis of burnout but assessed in its own rights. Engagement is defined as: “a positive, fulfilling, work-related state of mind that is characterized by vigour, dedication, and absorption. Rather than a momentary and specific state, engagement refers to a more persistent and pervasive affective-cognitive state that is not focused on a particular object,
55
event, individual, or behaviour.” Vigour is characterized by high levels of energy and mental resilience while working, the willingness to invest effort in one’s work, and persistence even in the face of difficulties. Dedication is characterized by a sense of significance, enthusiasm, inspiration, pride, and challenge. Different from involvement, which is also defined in terms of psychological identification with one’s work or one’s job, dedication goes a step beyond. In a quantitative sense, dedication refers to a particularly strong involvement that goes one step further than the usual level of identification. In a qualitative sense, dedication has a wider scope by not only referring to a particular cognitive or belief state but including the affective dimension as well. The final dimension of engagement, absorption, is characterized by being fully concentrated and deeply engrossed in one’s work, whereby time passes quickly and one has difficulties detaching oneself from work (Schaufeli et al., 2002). This recently developed concept of engagement seems to be a promising approach to understanding positive aspects at work. The measurement of engagement is done with the Utrecht Work Engagement Scale (UWES, Schaufeli & Bakker, 2003). The UWES scale provides a well-defined and thoroughly developed instrument to measure engagement. If this new path of burnout research should lead to interesting, new developments in the field, it is dependent on the creativity and openness with which the research community will approach it. It will further be interesting how relations to other related concepts (flow, job involvement, affective and passionate commitment) will be drawn. Nevertheless, engagement as positive work related behaviour is defined and clears the way for new insights on how to understand the relationship between motivation and burnout.
56
2.3.5 Relationship and overlap between motivational concepts introduced above
The two concepts of engagement developed from within burnout research try to define this continuum from engagement to burnout. In doing this, they do not explicitly refer to motivation research. Nonetheless, they both refer to the aspects of intensity and persistence of motivation. Engagement is regarded as a popular synonym for motivation. In fact, the Danish language prefers the term engagement to describe motivational states. Motivation is perceived as a scientific term, not used in every day language. Both concepts of engagement use the term energy in order to describe the resilience and willingness to invest effort. Energy as an antipode to exhaustion refers to the physical and cognitive realm, not so much the emotional. Being fully absorbed in one’s work comes close to a state of ‘flow’. However, typically, flow is a more complex concept that includes many aspects and refers to a rather particular, short-term ‘peak’ experience instead of a more pervasive and persistent state of mind, as is the case with engagement. The five concepts of motivation introduced above represent different streams in motivation research and are regarded as relevant in the context of this case investigation.
2.3.6 The relationship between motivation and burnout
One of the core assumptions in burnout research is the notion that a strong initial motivation is necessary in order to develop burnout (Freudenberger & Richelson, 1980; Pines, 1993; Burisch, 1989; Büssing, 1992; Schaufeli & Enzmann, 1998; Maslach et al. 2001). In a recent article, Friedman (2000) explains the process of burning out in teaching with the professional efficacy discrepancy approach. Thereafter, teachers entering the field with high levels of idealism and commitment experience a discrepancy between expected and observed sense of professional self-efficacy. This leads to a feeling of low accomplishment and frustration, and developing exhaustion. The threat to self-
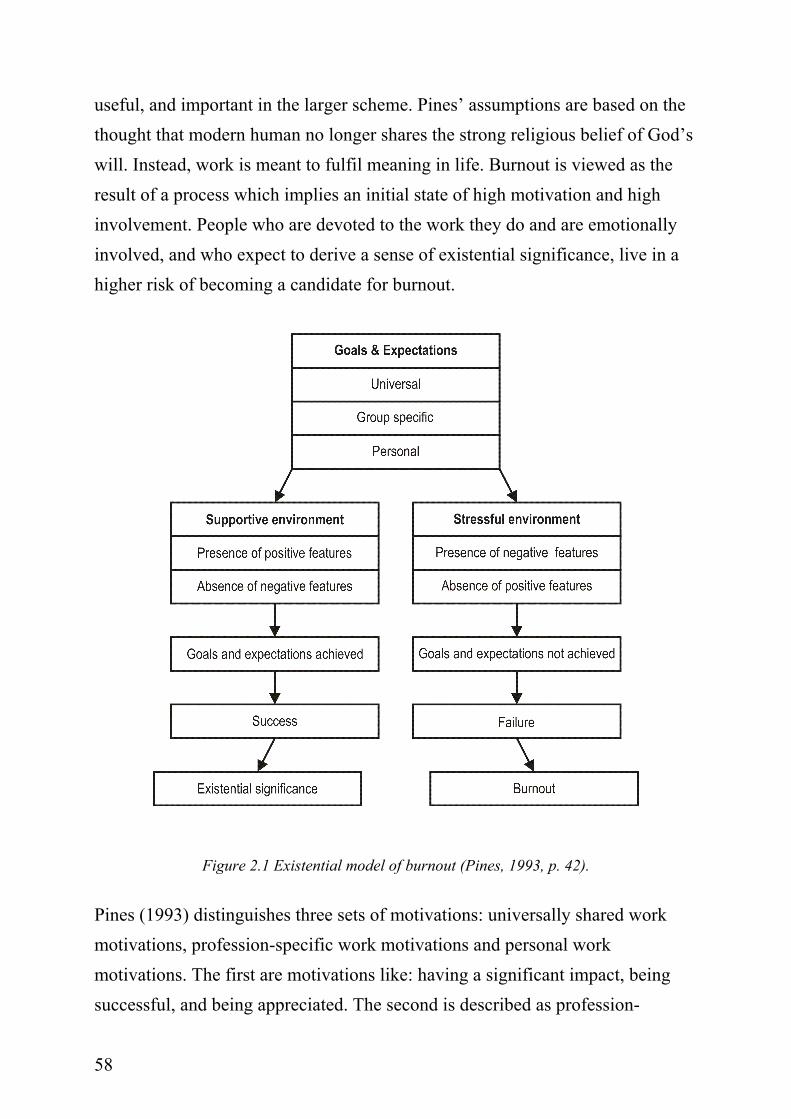
57
efficacy components, defined as tasks (teaching and school administrative organization) and relations (with students and with administration and colleagues) in a harsh reality of occupational life can lead to burnout. Although the assumption of motivation being a necessary pre-condition for the development of burnout is widely cited throughout the literature on burnout, empirical proof of the assumption is rare. In the following, the existential model of burnout (Pines, 1993), which describes the relationship between motivation and burnout based on experiential data, is introduced. Further, a selection of recent empirical studies is also introduced. All empirical work is recruited from a larger database search using the search terms ‘motivation and burnout’ and ‘commitment and burnout’, and from cross-citations. The author selected those studies which investigate explicitly the relationship between motivation and burnout.
2.3.7 The existential model of burnout
Alaya Pines is the one who described the core assumption of burnout research in rather powerful words (Pines, 1993, p. 41): “…in order to burn out, one has to first be ‘on fire’”. In the existential model of burnout, she formulates the assumption that a high motivation to succeed in one’s job is a necessary precondition in order to experience burnout. Only highly motivated individuals can burn out. Burnout is regarded to be a developmental process. This aspect is also included in many of the burnout concepts known from the literature, as for example, Golembiewski’s state model (Golembiewski & Munzenrider, 1988) or Maslach’s idea of different phases of burnout (Maslach et al. 2001). Pines (1993) argues that the loss of meaning in life causes burnout. She states that nowadays meaning in life often is approached through work instead of through religious beliefs as in the past. Work has become the religion of a secularised world. The existential significance of a person is measured by the meaning found in doing his/her job. The work we do ought to be significant,
58
useful, and important in the larger scheme. Pines’ assumptions are based on the thought that modern human no longer shares the strong religious belief of God’s will. Instead, work is meant to fulfil meaning in life. Burnout is viewed as the result of a process which implies an initial state of high motivation and high involvement. People who are devoted to the work they do and are emotionally involved, and who expect to derive a sense of existential significance, live in a higher risk of becoming a candidate for burnout.
Figure 2.1 Existential model of burnout (Pines, 1993, p. 42).
Pines (1993) distinguishes three sets of motivations: universally shared work motivations, profession-specific work motivations and personal work motivations. The first are motivations like: having a significant impact, being successful, and being appreciated. The second is described as profession-
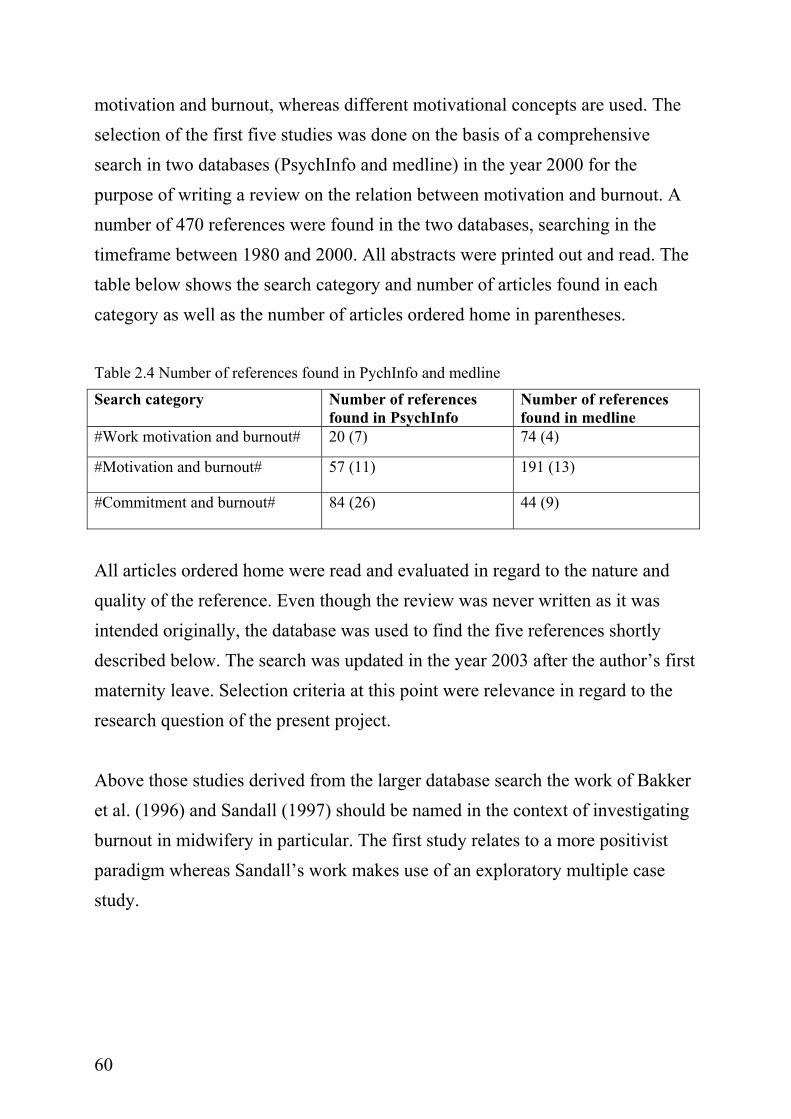
59
specific work motivation which results in interrelated processes: selection and professional socialization. The third are personal work motivations described as a “romantic image” of the work modelled after certain experiences, important persons, admired characters, etc.. A close relation to the three basic motives of power, achievement and affiliation (McClelland, 1983) can be drawn. Pines’ work is based on experience from some hundred burnout workshops. The experiential data is used as the basis for well-described research processes. The model is appealing in the sense that it is sound and easy to comprehend. The model leaves space for many assumptions about burnout research. For example, personality dispositions are not mentioned explicitly but can be thought of as having an influence in the process of setting goals and forming expectations. The recognition of subjective feelings and cognitions as being important for the appraisal of the situation is regarded as important aspect by the author of the present work. Another appealing aspect is seen in the clear assumption of an initial state of “being on fire” as a necessary prerequisite for burnout. The logic of the model works with the assumption that the environment has to be supportive with “a maximum of positive features that enable professionals to reach their goals by providing the needed autonomy, resources and support” (Pines, 1993, p. 43). Yet at the same time, Pines states that the appraisal of what is supportive or not is strongly dependent on the individual’s estimation of the situation. It can be concluded that the assumption of motivation as a necessary prerequisite for burnout has not been empirically proven by Pines’ work. Nevertheless, her observations are valuable as a reference frame for further research on the relationship between motivation and burnout. 2.4 Selected empirical studies on the relationship between motivation and burnout The following section comprehends short summaries of eight different empirical studies. The studies focus on the investigation of the relationship between
60
motivation and burnout, whereas different motivational concepts are used. The selection of the first five studies was done on the basis of a comprehensive search in two databases (PsychInfo and medline) in the year 2000 for the purpose of writing a review on the relation between motivation and burnout. A number of 470 references were found in the two databases, searching in the timeframe between 1980 and 2000. All abstracts were printed out and read. The table below shows the search category and number of articles found in each category as well as the number of articles ordered home in parentheses. Table 2.4 Number of references found in PychInfo and medline
Search category Number of references found in PsychInfo
Number of references found in medline
#Work motivation and burnout# 20 (7) 74 (4)
#Motivation and burnout# 57 (11) 191 (13)
#Commitment and burnout# 84 (26) 44 (9)
All articles ordered home were read and evaluated in regard to the nature and quality of the reference. Even though the review was never written as it was intended originally, the database was used to find the five references shortly described below. The search was updated in the year 2003 after the author’s first maternity leave. Selection criteria at this point were relevance in regard to the research question of the present project. Above those studies derived from the larger database search the work of Bakker et al. (1996) and Sandall (1997) should be named in the context of investigating burnout in midwifery in particular. The first study relates to a more positivist paradigm whereas Sandall’s work makes use of an exploratory multiple case study.
61
(1) “A Meta-Analytic Examination of the Correlates of the Three Dimensions of Job Burnout” (Lee & Ashforth, 1996) In a comprehensive meta-analysis, Lee & Ashforth (1996) assessed the associations between various correlates and the three burnout dimensions as operationalized in the MBI. The conservation of resources theory (Hobfall, 1989; Hobfall & Freedy, 1993) is used as framework for understanding how such correlates are related to the different dimensions of the burnout concept. The conservation of resources theory (COR) assumes that burnout occurs when certain valued resources are lost, fail to meet demands, or do not yield the anticipated returns. It is further suggested that certain outcomes occur as a result of resource loss and burnout, and one is the erosion of organizational commitment. The results of the meta-analysis support this assumption. Organizational commitment was negatively related to both emotional exhaustion and depersonalisation. (2) “Brennt wirklich aus, wer entflammt war? (Is really burning out who was enflamed?)” (Schmitz, 1998) Using a LISREL-analysis, Schmitz (1998) investigated the question “Do people really burn out who were once enflamed?” in a sample of 207 people in human service work. In reference to Hallsten (1993), burnout is thought to start with the counteraction of three factors: a certain vulnerability of the person, problematic conditions of the job, and specific expectations about the own role. The following original states for the development of burnout are defined and their roles in regard to burnout are investigated: basic beliefs and expectations towards the job, unrealistic aspirations, commitment, enthusiasm and involvement. Occupational disappointments are defined as mediating variables. The structural model included demographic information as exogenous and the original states of burnout (see above), the occupational disappointments (mediating) and burnout (endpoint) as endogenous variables. Results show that only the path from unrealistic aspirations towards the job through occupational
62
disappointments (mediating) is significant. The path from enthusiasm, involvement and commitment to burnout actually shows a slightly negative relation. The metaphor of “only those who have burnt can burn out” could not be tested with the structural analysis. Enthusiasm, commitment and involvement should not be defined as original states (Prodromalzustand, Prodromalmerkmal) to develop burnout. The author replicated the finding in a second investigation (Schmitz, 1999) using a sample of 103 teachers. (3) “Organizational commitment and experienced burnout: an exploratory study from a Chinese cultural perspective” (Tan & Akhtar, 1998) Tan & Akhtar (1998) investigated organizational commitment and the burnout experienced using a questionnaire survey of 147 employees of a Chinese-owned bank in Hong Kong. The assumption of the overemphasized beneficial effects of organizational commitment on health and well being of employees was questioned and investigated in depth. Moreover, a Confucian-based Chinese cultural perspective is included in the analysis. The authors refer to the three-dimensional concept of commitment proposed by Meyer & Allen (1997), differentiating normative, affective, and continuance commitment. Emotional exhaustion is measured, representing experienced burnout and is assumed to be the core constituent of burnout. Along with the commitment and burnout measures, work perceptions were measured using the Job Descriptive Index (Smith, Kendall & Hulin, 1969, in Tan & Akhtar, 1998). One proposition was that higher levels of normative commitment would lead to higher levels of emotional exhaustion. This proposition proved to be right, showing that normative commitment contributed five percent variance to emotional exhaustion in the predicted direction. Further, affective commitment showed no significant effect on emotional exhaustion. Both results are discussed on the background of cultural assumptions, differentiating between an Anglo-American culture and a Confucian-based Chinese culture. In a Confucian-based society, affective bonds are mainly tied to the family and not to the organization. Thus, affective commitment does not play an important role as a source of emotional
63
exhaustion. On the other hand, a strong appeal to normative commitment is reported. A normative orientation, expressed in loyalty towards the employer, respect for authority, filial submission and devotion to service, is core in a Confucian-based society. (4) Job Stages of Entry, Mastery, and Disengagement Among Nurses (McNeese-Smith, 2000) McNeese-Smith (2000) describes the relationship between different job stages and organizational commitment. Job stages are defined, following Graham’s model of entry, mastery and disengagement (1970, 1973; in McNeese-Smith, 2000). The study shows a strong relationship between organizational commitment, measured with The Organizational Commitment Scale (Porter et al., 1974), and the phase of mastery and preventing disengagement. Her study gives support to the notion that strong organizational commitment may prevent burnout. (5) The Measurement of Engagement and Burnout: A Two Sample Confirmatory Factor Analytic Approach (Schaufeli et al, 2002) Schaufeli et al. (2002) reformulated burnout as an erosion of engagement with the job. They compared and tested a model which suggested two second-order factors on which all three burnout scales load (exhaustion, cynicism, reduced efficacy) and the three engagement scales (vigour, dedication, absorption), with a model which suggested one general undifferentiated dimension of engagement. A test of the factor structure of the two concepts (burnout and engagement) yielded satisfactory results, proposing that the factor structure of burnout and engagement is reliable. Nevertheless, professional efficacy (being defined as a factor of burnout) loads onto the wrong factor, suggesting that the component of professional efficacy appears to be an element of engagement. This result is consistent with other findings (Leiter, 1993; Lee & Ashforth, 1996), suggesting that professional efficacy develops independently from exhaustion and cynicism. Further, the results of the analysis give to understand
64
that burnout and engagement are to a certain extent antipodes, sharing one-quarter to one-third of their variance. (6) ‘Burnout’ among Dutch midwives (Bakker et al., 1996) In a cross-sectional investigation of 200 community midwives in independent practice Bakker et al. (1996) tried to determine whether burnout amongst Dutch community midwives can be explained in terms of work load and work capacity. As indication of workload the average hours a midwife works per week, percentage of supervised home births, and level of urbanisation is used. Work capacity is operationalized as work experience (number of years a person has been working), practice type (number of midwives working in a practice), social support received (perceived support from significant others), and coping style (active and passive coping). Burnout is measured with the Dutch translation of the MBI. Response rate was with 74% fairly high. Some of the findings were contradictive, e.g. the more hours a midwife worked per week the higher was the sense of personal accomplishment (PA); a higher rate of home births leads to less emotional exhaustion (EE) and less depersonalisation (D). Accordingly number of hours worked was found to be a poor predictor of burnout and high percentage of home births is thought to reduce the risk of burnout. All three work capacity variables were significantly related to burnout: more social support leads to lower levels of EE and D and higher levels of PA. More passive coping style was related with higher levels of EE and D, no significant relationship with PA. The following three interaction terms showed significant correlates with burnout: More passive coping style showed in a significant correlation between percentage of home births and D. Combination of percentage of home births and practice type is significantly related to PA. The third interaction term found was the degree of urbanisation and practice type as being significantly related to D. Compared to a group of general practitioners the midwives showed same levels of EE, lower levels of D and higher levels of PA.
65
One conclusion drawn by the authors (ibid) is of particular interest in the context of the present thesis: “… for Dutch community midwives supervising births at the clients’ home instead of in a hospital maternity ward reduced their risk of burnout (ibid, p. 180).” (7) Midwives’ burnout and continuity of care (Sandall, 1997) Sandall (1997) investigated in a multiple site case study of community based maternity care the impact of continuity of care on midwives’ burnout. The data were gathered at three different sites being located on a continuum of complete one-to-one continuity of care to continuity within a team. From the interviews with 48 midwives and key informants three themes emerged from the data relating to sustainable practice, the avoidance of burnout, and the provision of flexible women-centred care: (1) occupational autonomy, (2) social support and (3) developing meaningful relationships with women. Control over own work organization, social support at work and at home, and being able to develop meaningful relationships with the women were associated with reduced burnout. Sandall concludes that models of care that recognize these factors are more likely to lead to sustainable work practice of the single midwife as well as to more personalized women-centred care. 2.5 Work Family Conflict (WFC) The introduced concepts of burnout and motivation research are short on explanations about the importance of context for a working person. The cross-over from work to family and the other way around is a focus in literature about work family conflict; also called work-home interference (Geurts & Demerouti, 2003). Work family conflict is defined as an incompatibility of work and family roles, leading to stress experienced by the individual (Geurts et all., 1999; Jansen et al., 2003). In the literature, the problem of work family balance is defined from two sides, work family conflict (WFC) and family-work conflict (FWC). Interestingly enough, the issue has, up to now, mainly been investigated
66
in males (Burke & Greenglass, 2001), even though women shoulder a greater responsibility for family issues than men (Hochschild, 1997). Midwifery is still a mainly women dominated work sphere. Frankenhaeuser (1991) could show that stress levels in men and women differ greatly after they returned home from work (declining for men and accelerating for women), showing the inability of women to unwind and relax after a demanding work day, whereas men are able to relax and recover directly after returning home from work. Therefore, it is reasonable that for women, the demand of one role interferes with participation and performance of the other role, causing WFC and consequently leading to health impairments. Jansen et al. (2003) investigated risk factors for the onset of work family conflict and could show that these differ for men and women. For women, physical demands, overtime work, commuting time, and having dependent children at home were found responsible for being risk factors for the onset of work family conflict. Burke & Greenglass (2001) could show that work-family concerns accounted for significant increments in explained variance on all three psychological burnout components (measured with the MBI). In a comprehensive review, Allen et al. (2000) report a number of studies focussing on the relation between WFC and job burnout. There is a significant mean correlation across studies (.42) for job burnout. Overall, the review stresses the importance of recognizing the serious consequences associated with WFC. Geurts et al. (1999) report a clear mediating role of work-home-interference between work characteristics (worktime schedule, quantitative workload, and dependency on supervisor) and home characteristics (overtime partners) and health outcomes (psychosomatic health complaints, sleep deprivation and burnout). Jansen et al. (2004) examined the effects of different worktime arrangements on work-home interference, controlling for other work-related factors, private situation, and health-status. They could show that worktime arrangements are clearly related to work-home interference. The outcomes are
67
of particular interest in the context of the present case study: (1) compared to daywork, baseline shiftwork was associated with higher work-home interference overtime. (2) baseline-overtime work and commuting time were especially critical for part-time workers. (3) Work-home interference at baseline was a good predictor for changing workhours over time. Altogether, they conclude that worktime arrangements are a good tool for reducing work-home interference. In a comprehensive review of existing theory and research in the field of work family conflict, Barnett (1998) proposes a systemic view onto the subject. A wide array of the literature on WFC is one-dimensional, focussing only on one single relationship. However, as Barnett (2000, p. 154) puts it: “Clearly people have multiple roles; they do not have multiple separate selves.” Barnett proposes a model taking an offset in the idea of the family adaptive strategy (Moen & Wethington, 1992 in Barnett, 1998). The idea is that workers adopt a certain work/social strategy to meet their various needs. The strategy takes proximal conditions (personal needs, values, and aspirations, the social system represented by family, friends, community as a whole and personal characteristics such as gender, age, race, health status, ability, education, marital and parental status) and distal conditions (macro economic, social-structural, and attitudinal factors, workplace policies and practices, as well as job conditions) into account. Fit describes the extent to which a worker is able to meet the various components of his/her work/family adaptive strategy. The complex model suggests a list of different outcomes, ranging from individual mental and physical health, to spouse’s needs, child/parent issues, friends, community, and finally, the workplace. Without going into depth into the interrelation of work and social spheres, it is safe to conclude that using a work/social system adaptive strategy will lead to a win-win situation. There is no doubt that there is considerable influence of one sphere onto the other: changes at the workplace will have impact on the social world of the employee as changes in the private social realm will lead to influences at work.
68
2.6 Emotions at work Emotions in the workplace first now are starting to get the same recognition that cognitive and behavioural aspects in the workplace have gotten for the last 40 years (Ashkanasy, Härtel & Zerbe, 2000). Fisher & Ashkanasy (2000) summarize that very little is actually known about emotions in the workplace, expressed in a special issue on the topic in the Journal of Organizational Behaviour. Nevertheless, emotions in the workplace are regarded as being a hot topic, as they are a fundamental part of human expression. Even though emotional exhaustion is regarded as the core dimension of burnout, emotional work demands have only rarely been considered as predictors of burnout (Zapf, 1999, 2001; Brotheridge & Grandey, 2002). Therefore, the observations and information gathered in the interviews are put in a broader frame of reference of emotions in the workplace. On the theoretical forefront stands Hochschild’s groundbreaking work on emotional labour. Further, Brucks’s reflections about action- and affect-psychological base of work psychology are introduced. Finally, Zapf’s theoretical and empirical work on emotion work and burnout is presented.
2.6.1 Concepts of emotion work
In 1983, Hochschild published The Managed Heart: Commercialization of Human Feeling, a book describing her experiences and observations of flight attendants who need to act in accordance to feeling rules of the corporation they work for. Since publication of the book, the display of emotions and the acting out of feelings demanded in order to be an excellent human service worker has been investigated in different research contexts. Hochschild (1983, p. 7) defines emotional labour as the requirement “to induce or suppress feeling in order to sustain the outward countenance that produces the proper state of mind in others”. Hochschild differentiates between surface and deep acting. In surface acting, a person is pretending to feel something she/he is not feeling. Others are deceived about how a person really feels but the person herself is not. In deep acting, feigning is unnecessary; the person really feels how she acts. In active
69
deep acting, individuals alter how they feel in order to get closer to what is expected from them to feel, e.g. a midwife is putting herself into an emotional state of feeling empathy in order to be able to be empathetic in a birthing situation. To express positive feelings is not per se bad. It is the estrangement or alienation from one aspect of self, which has damaging effect on the individual. Kruml & Geddes (2000) differentiated emotional dissonance from emotional effort and investigated different acting types in relation to the experience of burnout. They found, among other outcomes, that the more dissonance between one’s own feelings and the demanded feelings that the workers experience, the more likely they will be emotionally exhausted. The findings also indicate that people who are more likely to express their true feelings are less likely to experience emotional exhaustion. Brotheridge and Grandey (2002, p. 33) could show that deep acting in service professions “contributed to a greater sense of personal efficacy at work”. In an earlier concept on emotions at work, Strauss et al. (1980, in Brucks, 1998) differentiate between sentimental work and emotional work. Sentimental work describes work which takes the wishes, comments and demands of the recipient into account and is understood always to relate to the primary task. Emotional work refers to the process of regulating one’s own emotions as reactions to the primary task. On this background, Brucks (1998) discusses a third type of emotional labour as a specific job demand: the manipulation of feeling of the other. She describes the relation between a nurse and a patient as being non-reciprocal. In contrast to other human service professions, the object/matter (health, giving birth) and its’ quality are not to be seen apart from the other (the client/patient). Brucks (1998) points to the shortcoming of many work psychological constructs focussing on autonomous planned behaviour only to explain human work behaviour. As one example from burnout theory, she names Burisch’s integrated
70
burnout model (1984, ibid). However, work roles, especially in human service work, cannot be understood by looking at the side of autonomous planned behaviour only. Work routine, in the context of the present case investigation, is understood as the part of work which can be planned ahead and valued after the criteria of autonomous planned behaviour (Hacker, 1986). Other parts of the midwife’s daily job are not accessible through this approach. Technical mastery and control are necessary but not sufficient. A birth is a process that goes beyond technical mastery and control. This other part touches the intimacy of the other. By doing this, social tensions and emotional entanglement are ready to occur. The action and reaction of the other is not calculable. In all human service professions, the recipient plays a particular role. In midwifery, the recipient of the midwife’s service is in an acute state. Even if the person is known beforehand, her behaviour and the behaviour of the husband and family are not foreseeable. This is part of the thrill but can also be a challenge for the midwife. The importance of the service provider-client relationship is further described in the following section when referring to the work of Zapf et al. (1999, 2001). Zapf et al. (1999, 2001) combine concepts from the literature on emotion work (=emotional labour) with action-theory based approaches in stress research. In action theory, the psychological component of work is defined as a psychic regulation of work actions. Regulation requirements (hierarchic-sequential organization of action), regulation possibilities (control) and regulation problems (stressors) are thought to be differentially related to health and well-being. Accordingly, emotion work understood in the framework of action theory is part of intentional and goal-directed behaviour. In the realm of regulation requirements, Zapf et al. differentiated between frequency and variety/intensity of emotion work. Further sensitivity requirements are described as “the necessity to be sensitive and consider the emotions of clients”. Emotion work control is operationalized as a specific form of job control. Emotion work control describes the extent to which an employee can decide whether and to what point to show a certain emotion. Emotional dissonance is considered to be
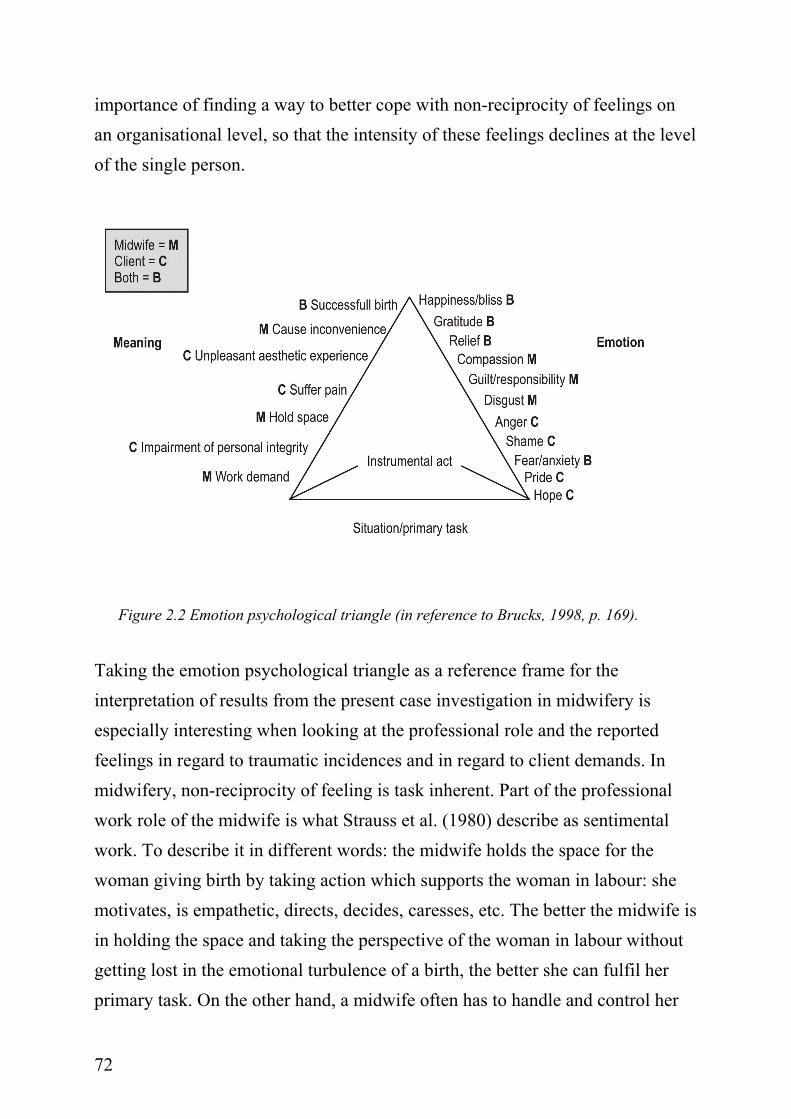
71
a regulation problem. Emotional dissonance is defined as an external demand according to display rules of an organisation or profession and not as a reaction; a discrepant feeling. Zapf et al. (1999) found that emotional dissonance was positively related to emotional exhaustion and depersonalization. The display of positive emotions and sensitivity requirements were positively related to personal accomplishment. These outcomes point to an understanding of emotion work as having positive as well as negative implications. In accordance with the theoretical work and the empirical findings, Zapf et al. (2001, p. 529) differentiate five aspects of emotion work: (1) the requirement to display positive emotions, (2) the requirement to display and handle negative emotions and at the same time a high variety of emotions to handle and to display, (3) the requirement to sense the emotion of the interaction partner, (4) the influence on the social interaction, and (5) the dissonance between felt and displayed emotions. Among many other findings Zapf et al. (2001) report that client-related stressors are important in the development of burnout. The qualitative aspects of the service provider-client relationship had some predictive power for the development of burnout. This seems to be of particular interest in regard to the present case study in midwifery. Referring to early research work from Dembo (1931, in Brucks, 1998) and Menzies (1975) and more recent work from Richard and Bernice Lazarus (1994), Brucks (1998) describes the emotion psychological triangle. The triangle describes the interdependence of an instrumental action (e.g. the dramaturgical plot of a work task); an emotion following from this action, and the significance of the situation for a person and the action following from it in order to cope with the situation. Both client and human service worker react in accordance with their own dramaturgical plot. At this point, non-reciprocity of feeling is experienced. Brucks (1998, p. 170) points to the two patterns of emotional labour which have been described by Strauss et al. (1980), as sentimental and emotional work. Emotional labour is described as work related to the handling of meaning and feelings of non-reciprocity. Brucks (1998) discusses the
72
importance of finding a way to better cope with non-reciprocity of feelings on an organisational level, so that the intensity of these feelings declines at the level of the single person.
Figure 2.2 Emotion psychological triangle (in reference to Brucks, 1998, p. 169).
Taking the emotion psychological triangle as a reference frame for the interpretation of results from the present case investigation in midwifery is especially interesting when looking at the professional role and the reported feelings in regard to traumatic incidences and in regard to client demands. In midwifery, non-reciprocity of feeling is task inherent. Part of the professional work role of the midwife is what Strauss et al. (1980) describe as sentimental work. To describe it in different words: the midwife holds the space for the woman giving birth by taking action which supports the woman in labour: she motivates, is empathetic, directs, decides, caresses, etc. The better the midwife is in holding the space and taking the perspective of the woman in labour without getting lost in the emotional turbulence of a birth, the better she can fulfil her primary task. On the other hand, a midwife often has to handle and control her
73
own feelings. A client might evoke certain feelings (e.g., compassion) which go beyond the personal capacity to control this feeling. In burnout research, it became obvious that the hope of gratitude from the client, or the motivation through feeling compassion are not regarded as professional (and in second line healthy) ways of taking action (Brucks, ibid). Another aspect which seems to be important in regard to emotional labour in midwifery is the cooperation between the human service worker and the recipient of service. The extent to which the human service worker and the recipient (here: client and midwife) can find ways to cooperate, the better to lower the feeling of non-reciprocity. Brucks’s conclusion reaches so far that emotional labour stands in second line to the primary task in human service work. At points, emotional labour is even more important than the primary task. Openness and transcendence of personal borders are important in order to be open for the feelings of the other. Yet, the fulfilment of the primary task still needs to be possible. If emotions are experienced as too overwhelming by the individual, performance of the primary task is impossible (Brucks, 1998). 2.7 Summary and conclusion In the previous chapter, the most prominent theories in burnout research were introduced; some selected approaches to motivation were outlined and an introduction to research to the fields of work family conflict (WFC) and emotion work was given. Burnout research has shown to be dominated by the usage of the Maslach Burnout Inventory (MBI, Maslach & Jackson, 1986), leading to a vast amount of research studies on burnout but not much knowledge about complex causes and consequences. Research on work motivation presented here is also diverse but not nearly as comprehensive. On a broader level of reflection, it can be concluded that most theorizing in work psychological research lacks a clear commitment to a specific setting under investigation. In Table 2.3 (p. 39), strengths and weaknesses of contemporary burnout research are summarized. The remaining question seems to be how
74
research focussing on isolated aspects of a person’s psychosocial wellbeing at work can be brought together into a broader perspective so that a more thorough understanding of processes which lead to either motivation or burnout in midwifery is possible, both on a collective as well as individual level. The present project is regarded as a step in between two research traditions. A strong reference to existing theory and research in the field is established with the purpose of staying connected to what I call a mainstream position in contemporary work psychological research which is dominated by a quantitative research approach. In a way, this is a pragmatic choice of being able to interconnect with colleagues, thinking, doing research, and writing about it from a positivist stand. I personally share the propositions of a post-modern approach of doing research in believing in the value of investigating the subjective lifeworld perspective as well as in the necessity of constantly questioning the own fore-understanding in order to come to a better understanding. Both traditions, the quantitative and the qualitative, seem to have advantages and disadvantages and are not to be seen independently from the epistemological paradigm they refer to. A quantitative approach inherits the beauty of being able to make assumptions about the world as it is whereas a qualitative approach is more hesitant and refers to a world as it seems to be. In the next chapter, the qualitative paradigm of doing research as understood in the present project is introduced in more depth. Further, the chosen research approach, strategy, and design of the present project are outlined. Whereas the previous chapter clearly represented knowledge gathered within the quantitative paradigm, the forthcoming chapter describes a way of understanding the relationship between motivation and burnout in midwifery from a different epistemological stand.
75
Chapter 3: Epistemological reference frame and method 3.1 Introduction The epistemological paradigm a researcher refers to is the expression of a basic belief system regarding the process of how to reach understanding. Thomas Kuhn (1970) introduced the term ‘paradigm’ in order to describe the process of gathering scientific knowledge. A paradigm is a certain belief system or mindset, which enables the scientist to relate to new knowledge in a certain way. At the same time, a paradigm is an entrance ticket to a scientific community. The knowledge about which paradigm one refers to enables the recipient of scientific insights to understand the outcome on a deeper level of understanding. Guba & Lincoln (1994, p. 105 in Christians, 2000, p. 149) emphasize the importance of the research paradigm, stating that “questions of method are secondary to questions of paradigm”, because the paradigm is the “basic belief system or worldview that guides the investigator, not only in choices of method but in ontologically and epistemologically fundamental ways”.
From the analysis of existing theory and research approaches in the field of motivation and burnout (Chapter 2), it became obvious that there is a strong need for an in-depth research approach to investigate the relationship between motivation and burnout. The statistically rather sophisticated approaches of quantitative research leave some important questions unanswered. This is partly due to the complex nature of the phenomena in context as well as the diversity of subcultures and lifestyles in modern society, as well as in organizations. Research approaches and methods need to take the diversification of modern ways of living with different contexts and perspectives into account (Flick, 2002; Pedersen 2002). Knowledge needs to be understood as local and transient. The investigation of a phenomenon is bound up in a specific context; the life world of the person. Qualitative research has the methodology to investigate
76
complex phenomena on a different level than quantitative research (Gordon et al., 2005). The present project refers to the qualitative research paradigm. The qualitative paradigm is characterized by different approaches to reach understanding about a phenomenon. Qualitative research approaches are well documented (e.g., Lamnek, 2005; Creswell, 2003; Flick, 2002, 2000; Denzin & Lincoln, 2000; Malterud, 1996, 2001; Strauss, 1998; Kvale, 1994; Moustakas, 1994; Lincoln & Guba, 1985; Kleining, 1985). Lamnek (2005, p. 33) summarizes the following attributes of qualitative research:
• Interpretative: Social reality is constructed through interpretation and meaning, it is not objective.
• Naturalistic: The field for research is the real world. Methods to investigate the natural world are naturalistic.
• Communicative: Rules for every day communication are also true for methodological rules in qualitative research.
• Reflexive: Qualitative research needs to be self-reflective in different ways.
• Qualitative: Qualitative research is different from standardized quantitative approaches. Not standardized methods are used in order to approach the field openly and adequately in regard to the research matter.
The interpretative nature of qualitative research is its strength and challenge at the same time. It is strength as the understanding of meaning is looked upon with imperturbability. Findings, results, knowledge interpretations and meaning are dependent on the context and must be understood as interpretations of reality. This does not imply that outcomes from qualitative investigations are arbitrary; they are just not normative. The challenging part is to transform, integrate and translate interpretive knowledge into new contexts. Concerning the naturalistic nature of methodology and the investigation in the real world the

77
following must be said: Most of all, natural settings are complex systems with a variety of influencing factors. The understanding about phenomena in a complex system cannot be more than an approach to reality. Moreover, the reality of complex systems is defined as being dependent from the observer and the observed (Ludewig, 1992). The quality and variety of communicative action between the two sets the ground for a good fit of findings and phenomena in the natural setting. The communicative nature of qualitative research takes into account that understanding and misunderstanding happen in the same way as in everyday communication. The difference is the reflexive nature of communicative action. The researcher in the qualitative setting is committed to reflect on his/her understanding critically on her own (e.g. in a log book, research diary) and together with others (e.g. colleagues, participants) for the aim of communicative validation. Last but not least, qualitative research implies the usage of not-standardized methods. Again, this must not lead to arbitrary procedures in qualitative research projects. Instead, thorough documentation of the approach, the chosen procedure of data collection and data analysis, and the way of interpreting meaning are ways of showing how knowledge is constructed. The purpose of the following chapter is to document and describe the research process from first epistemological assumptions to concrete methodological steps. Phenomenology as an epistemological paradigm is outlined; the frame for the research project is described as set by outer conditions and as decisions of the author; research methods are introduced and described on a practical level in regard to their realization in the present project; and, at the end of the chapter, quality criteria for the present investigation of the case are introduced and discussed. 3.2 Phenomenology as research paradigm Lamnek (2005, p. 48) describes the different levels of theory within social research as follows: Epistemological assumptions lead to a paradigm, which
78
refers to a corresponding methodology, which then is followed by exemplified methods and techniques. The particular choice of procedure is greatly connected to the research question and underlying assumptions about the phenomenon. Throughout this following section, phenomenology as a research paradigm is introduced. The phenomenological paradigm serves as the background for the choice of method and the implementation of techniques for data analysis in the present project. Phenomenology has the goal of investigating a phenomenon as it is, independent from pre-existing knowledge, prejudices, and theories (Lamnek, 2005). There is a difference between the thing as it is and the experience of a phenomenon. Intentionality is the central concept in Husserl’s transcendental phenomenology. “Intentionality refers to consciousness, to the internal experience of being conscious of something; thus the act of consciousness and the object of consciousness are intentionally related (Moustakas, 1994, p. 28).” The object exists (noetic) independent of the perception of the object (noema). The appearance can differ from one situation to the other, which does not change the essence of the phenomenon as such. The phenomenological approach tries to describe the phenomenon as objectively as possible, independent of subjective, theoretical and traditional elements. The essence of the phenomenon is reached through reduction. Lamnek (2005,p. 59) describes the process of reduction in four steps. First, all elements of the phenomenon are gathered. Second, the relevance for the research question is questioned. The irrelevant aspects are set aside. In phenomenological terms this process is called bracketing (Moustakas, 1994). Third, only those elements remain that are
Box 3.1 Bracketing Bracketing is a step in phenomenological reduction, ”…in which the focus of the research is placed in brackets (Moustakas, 1994, p. 97)”. Bracketing is a form of contemplation on the essence of the phenomenon. An object is considered “precisely as it is intended by an intentionality in the natural attitude (Sokolowski, 2000, p. 49).” The form of manifestation an object has for the subject in the natural attitude is maintained.
79
necessary and invariant for the object of investigation. Fourth, the remaining objects give a structure; they are the essence of the phenomenon.
3.2.1 The phenomenological method
In the present project, data from single interviews and the group interview are analysed using the phenomenological method, a well-described, codified method to analyse qualitative data in social and medical science (Giorgi, 1975, 1985; Malterud, 1996). This form of data-analysis focuses on the condensation of meaning. The procedure is summarized in the following four steps of analysis (Malterud, 1996):
1. Reading all the material to get an overall impression and formulation of general themes
2. Identifying meaning units and coding 3. Condensing and abstracting the meaning within each coded group 4. Summarizing the content of the analysis as a whole.
In the following sections, each of these steps is described in more depth. Ad 1) Reading and formulation of general themes The first out of four steps to analysing data, is, according to Giorgi (1975), the determination of “natural meaning units”. This procedure furthers the understanding on the interviewers’ side from one interview to the other and gives the opportunity to listen more closely when new meaning is established. This procedure makes the accumulation of knowledge more explicit. A period of transcribing data and interpreting meaning on a first rough level follows each interview. This stepwise acquisition of new information is treated as a growing base from which further interviews are conducted. First of all, the whole material is read in transcribed form to get a holistic impression of it. In this first
80
part of data analysis, it is important to put one’s fore-understanding and theoretical background aside and to try to be open for new insights and impulses coming from the material. This is a challenging and risky process, because the already existent theoretical background and knowledge is the foundation on which security of judgement is experienced. Yet judgement and quick interpretation is exactly what should be left aside at this point of the analysis. The first step of analysis is dominated by pure observation, keeping all senses open to perceive new insights. During this first step of analysis, the writing of notes can be helpful. Interesting things can be marked but should not be analysed in order to retain the impression of the whole. General themes2, themes grounded in the material, are the result of this first step of the analysis. In the present project, the entire interview material is read in one piece to get an impression of the whole before getting into a more thorough analysis of the material. General themes are noted in a logbook throughout the reading of the data material. Ad 2) Description of natural meaning units The second step is to code “natural meaning unit”. The material is analysed line by line in order to find natural meaning units. Each general theme from the first analysis step represents a preliminary idea, which is now systematized by finding natural meaning units in the material. Van Maanen (1990) uses the term “theme” to describe more closely what is meant by the description of meaning unit. According to this, themes are “like knots in the webs of our experiences, around which certain lived experiences are spun and thus lived through as meaningful wholes” (van Maanen, 1990, p. 90). Themes are those aspects of a phenomenon which stand out from the amount of observations made to describe the phenomenon in depth.
2 Van Manen (1990) describes a theme as an experience in the process of phenomenological reflection. In this sense it is described as an experience of focus, of meaning, of point, a simplification, a form of capturing the phenomenon one tries to understand.
81
This step of analysis relates strongly to the text. Natural meaning units are a more systematized classification of themes from the first step of analysis. This practical procedure is called coding. In the further process, only those themes are more closely investigated which seem to be interesting for further analysis. Malterud (1996) describes a variety of practical advice while coding which are used as guideline throughout the coding process of the present project:
• A double or triple coding of the same meaning unit is not regarded as a problem, but the code should be checked for precision.
• Coding is a systematic decontextualization because parts of the material are taken out of their former context to relate them to other parts (text elements) with the same meaning. A matrix can be helpful to get an overview of the different codes and their origin (interviewee). This table can be used to validate one’s findings at the end.
• On the way from raw-data to themes to codes, it is recommended to take a look back at the logbook (also understood as research diary) once in a while and reflect on hidden rules used to establish codes and the rules about inclusion and exclusion.
• Through the coding work, principles for decontextualisation are developed. The analysis can be described as ‘work in progress’.
Throughout the process of decontextualisation, meaning units across the whole material are used in comparison to other text elements which concern a similar issue. In the present project, coding is done in the logic of emic coding (Seeberg, 2001), which is described as an inductive coding process based on principles of grounded theory, e.g. focus for coding are not the questions asked but the answers given.
82
Ad 3) Condensation into abstract meaning units The third step in phenomenological data analysis is to find abstract categories to condensate the meaning units. Only those parts of the text coded as a meaning unit are further processed. Throughout this third step of data analysis, all coded meaning units are checked for redundancies. Redundant meaning units are either merged or deleted when not regarded as important for the research question. The material (textbites) is re-written into more abstract meaning using language different from the participants’ language. Codes with only a very small amount of coded text-bites are excluded or summarized under some other code. This step includes the researcher’s own professional perspective, fore-understanding, and experience. The process is both interpretative and associative. The content of each subgroup is condensed and reformulated in a more general form but it still contains the concrete content of the original meaning unit. The leading question throughout this process is: “How to understand the content of the material on the background of existing theoretical knowledge, one’s own experience, and in relation to the research question”.
Ad 4) Recontextualisation The fourth step in phenomenological data-analysis is recontextualisation. Recontextualisation assures that the patterns found throughout the process of decontextualisation still resemble the original holistic material and account for the informants’ reality (Malterud, 2001). Throughout the first three steps of the phenomenological analysis, the original material is taken apart in smaller bites and transferred into abstract language. Then these constructed units are collected and used to shape and to describe new concepts. To describe the structure of the phenomenon in more abstract terms, little comments (also called memos) are written. Each subgroup is put down in a section on its own. To describe these sections, expressions from the natural meaning units are used. This description of content is done for each coding group. This is a way of
83
showing and making public how the interpretation is related back to concrete raw material. A headline for the content description is to be formulated. In the present project, the coded material was structured around four themes: the description of engagement and burnout, the description of work context, the role of resources, and emotional demands and feelings at work. In all of these four sections old knowledge was confirmed as well as new understanding to the existing concepts of motivation and burnout was added. Reflection of own procedure using the phenomenological method The decision to use the phenomenological method is based upon the focus of the present project. Whereas the grounded theory approach (Strauss, 1998) is directed towards the inductive process of formulating new theory, the phenomenological method points at the description of the essence of the phenomenon. Formulation of new theory is regarded as a by-product. In the present project, the essence of the phenomenon has different aspects. First of all, context is regarded as important and as not to be neglected. How to deal with contextuality when focussing on the essence of the phenomenon in the practical phase of data-analysis was not clear. The problem was solved by recognizing the importance of always regarding a phenomenon as a phenomenon in context (see next section). Second, the two phenomena are each described in relation to one another. This is different from focussing on one phenomenon in its own right. Even though the relationship between the two phenomena is focus of the present project, the two phenomena are described individually. The (assumed) relationship is not explicitly formulated as a question in the interview guide, but is mentioned in the introduction of the interview to the participant. This was decided intentionally in order to keep the focus as open as possible. At the same time, it could be regarded as a weakness of the design of the single interviews. For practical reasons, transcribed data was analysed using a computer program based upon the principles of grounded theory. It has to be recognized critically
84
that any computerized logic is a reduction of the whole. Therefore, the fourth step of the phenomenological analysis is regarded as very important, where the whole material is re-read in order to make sure that nothing important was lost in the process of reduction.
3.2.2 Context dependency
The present project refers to two phenomena in psychology which have been widely studied: motivation and burnout. A tremendous amount of knowledge exists about these phenomena, but still open questions remain (Schaufeli & Enzmann, 1998; Burisch, 2002). The choice to use the phenomenological paradigm is based upon the assumption that there is an essence to these phenomena which needs some further explication. At the same time, it is assumed that the phenomenon as it is is dependent on the context in which it appears. The approach chosen in the context of this work tries to combine the idea of being able to capture the essence of a phenomenon with the idea of context. This second aspect is explained throughout the following section. The experienced truth of a phenomenon is found in subjective theories about a phenomenon of the lifeworld of an individual or group. “Individuals develop, similar to researchers, theories about the functioning of the world and their actions. They use these theories when taking actions, they test them and if necessary, they revise them (Flick, 2002, p. 37; according to Blumer, 1973).” The subjective theories inherit important knowledge about the investigated phenomenon, as they are basis for approaching the world in a certain way, using schemata and causal attributions to organize and find meaning in a complex world. The investigation of subjective theories opens up for new meaning about the phenomenon. Subjective theories can be based upon experience, culture, traditions, values, feelings and emotions, as well as spiritual beliefs. They can best be approached through proximal methods of investigation, such as field research, participant observation, qualitative research interviews, and focus
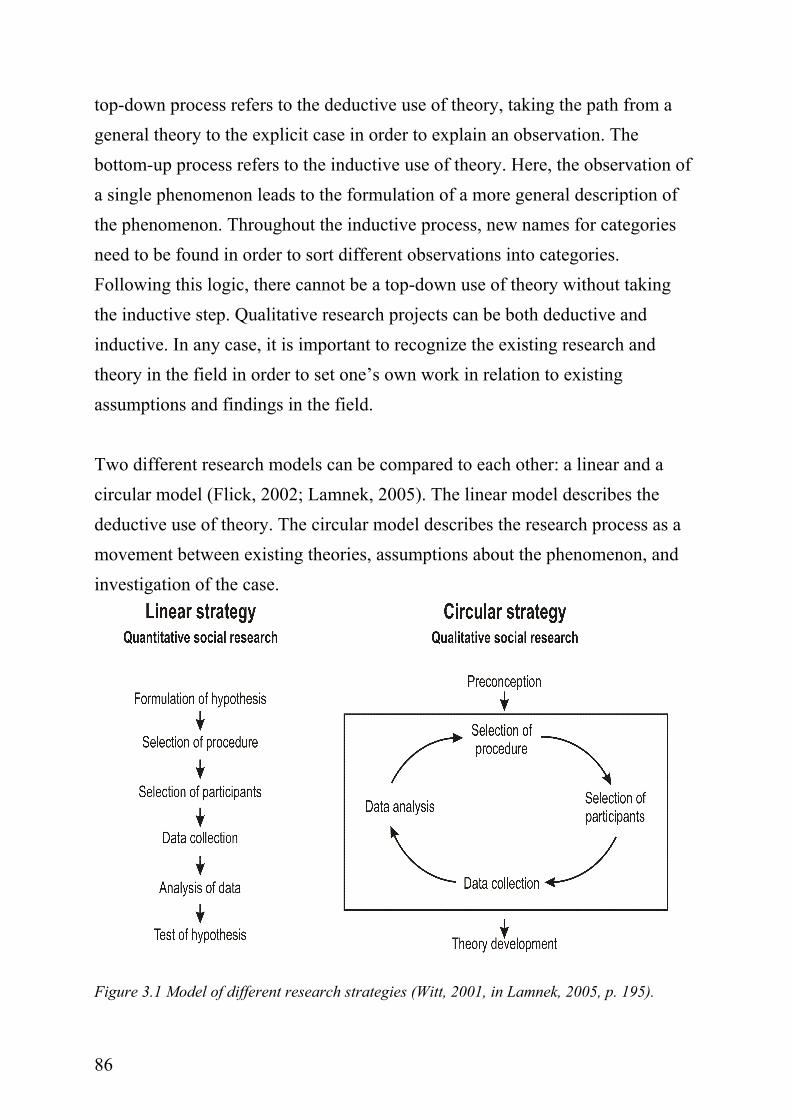
85
groups. According to these assumptions, the lifeworld of the person plays a fundamental role in understanding the phenomenon. Lifeworld refers to a concept of Habermas (in Hyde & Roche-Reid, 2004) and can be described as “the world viewed from a participant perspective, and it is structured through meaningful symbols, communicated through verbal action that is oriented toward understanding”. Reflection of context in the present case investigation Subjective theories can be both personal and collective. In the present case study, individual midwives are interviewed about their personal understanding of motivation and burnout. Each midwife has her own personal background which is different from all the others. This personal background has importance for the schemata, attributions, and subjective theories she uses to describe the phenomena. At the same time, each midwife belongs to the job group “midwife”. In the present project, shared subjective theories are in the foreground. The phenomena under investigation are related to the context of work, not private life. Even though personal experiences are shared throughout the interviews, most of these experiences can be related back to the primary task of a midwife, understood as helping to give birth. In conclusion, the work in midwifery is regarded as the context in which the data of the present case study need to be understood.
3.2.3 The use of theory throughout the monograph
A theory is a way of understanding the world in a certain way. It is a description of the world that is continuously revised, tested and reconstructed. In the best sense, theory can be used as a ‘tool for thinking’ (Greif, 1993, 2004). Theory can be used in different ways throughout a research process. Depending on the research question, theory is used top-down or bottom-up. The
“Far more interesting than the testing of existing ideas (…) is the generation of new ideas as they lead to more appropriate theories.” (Hermanns et al., 1984, S. 149, in Lamnek, 2005, p. 318, translated by A. Garleff).
86
top-down process refers to the deductive use of theory, taking the path from a general theory to the explicit case in order to explain an observation. The bottom-up process refers to the inductive use of theory. Here, the observation of a single phenomenon leads to the formulation of a more general description of the phenomenon. Throughout the inductive process, new names for categories need to be found in order to sort different observations into categories. Following this logic, there cannot be a top-down use of theory without taking the inductive step. Qualitative research projects can be both deductive and inductive. In any case, it is important to recognize the existing research and theory in the field in order to set one’s own work in relation to existing assumptions and findings in the field. Two different research models can be compared to each other: a linear and a circular model (Flick, 2002; Lamnek, 2005). The linear model describes the deductive use of theory. The circular model describes the research process as a movement between existing theories, assumptions about the phenomenon, and investigation of the case.
Figure 3.1 Model of different research strategies (Witt, 2001, in Lamnek, 2005, p. 195).
87
Critical reflection of using theory in the present case study In the present project, the relationship between motivation and burnout is re-investigated using a qualitative, in-depth approach. Using an abductive approach of reasoning (Reichertz, 2000a in Lamnek, 2005; Kirkeby, 1994) the participants were asked to give descriptions of the phenomena of motivation and burnout in their own language, referring to narratives from their life world. Theory is used in two different ways. First, theory is used as a reference frame. The reference frame explains the state of the art of research in the field. It is the theoretical knowledge base a researcher refers to (Lamnek, 2005). It should be noted that the reference frame is not an objective entity but, to a certain degree, a product of choice. The reference frame consists of the most prominent and most promising theoretical issues in the fields of burnout and motivation. Second, theory is used as a lens or perspective in order to interpret the observations made in the field. A bottom-up approach to investigating the phenomenon with open-ended questions is meant to lead to further insights concerning the research question. This led to affirmation of already existent knowledge in the field and to new descriptions of the investigated phenomena. Motivation as well as burnout is reflected in the light of new themes which emerged in the research process and that are meant to have impact on the relationship between motivation and burnout.
3.2.4 Dialogue as a guideline for research
In a qualitative approach, communication with another person (the field, the research participant) leads to a growing understanding. It is the other through whom we see the world as it is (Buber, 1965, in Moustakas, 1994). Communication is the path to reach a negotiated understanding of the world. Communication is context-bound and therefore understanding is something established in context, referring to a specific setting, a specific time and place. Within these communications, meaning is constructed. The construction of meaning is understood as an ongoing process. One necessary pre-condition for
88
understanding is putting one’s fore-understanding, mindsets, and beliefs aside and taking the risk of reformulation into account. During the process of understanding, the quality of the dialogue between the researcher and the participant is crucial. The researcher faces a lot of challenges. She has to be open enough to be perceptive on different levels. She needs to be focussed in order not to be overwhelmed by the amount of information she gets in the course of her investigation. She needs to be rational in order not to be swept away in sympathy for the person she is talking to. She has to be able to take someone else’s perspective in order to react in a responsible manner. Further, she needs to be reflective enough to give favourite assumptions up and look for new meanings. To fulfil these challenges, meta-positions (see Section 3.4.6) are used. In qualitative interview research, flexibility of the dialogue is another key issue. Fog (1994) stresses the point that the interview questions to be asked should be known by heart to be able to concentrate fully during the phase of contact to the participant (e.g., interview). Instead of working through a checklist of questions, answers are found on the way through talking about the phenomenon under investigation. This procedure of guided construction of meaning is an open but guided search for understanding the phenomenon in context. Kleining (1986, p. 734, in Lamnek, 2005) describes the dialogical process as follows: “A qualitative dialogue is not authoritarian-critical but rather egalitarian. As a rule, an answer creates a new question (and probably a new approach); and this in turn a new answer and so on, until the structure of the object is explained.”3 Another aspect of understanding is how to handle conflicting information and awkward interview partners. To really understand what an interview partner is talking about takes time and patience and the courage to reconfirm and ask again
3 Translation from German: „Ein qualitativer Dialog ist nicht autoritär-kritizistisch, sondern egalitär. Eine Antwort erzeugt in der Regel eine neue Frage (und möglicherweise eine neue Versuchsanordnung), diese wieder eine neue Antwort usw., bis die Struktur des Gegenstandes aufgeklärt ist (Kleining, 1986, p. 734).“
89
and again. It is a challenge to keep ones mind and heart open for any new aspects in the course of a research project. It is a challenge to stay rational at points where one’s heart is engaged in sympathy for the situation of the informant. Indeed, it can be annoying to be confronted suddenly with an interviewee who is stepping out of an already established pattern of meaning. Yet one should be thankful for any new insights gathered during the course of the investigation. Conflicting information gives a new dimension of insight into a social system. 3.3 Formal and methodological frame of the Ph.D.-project In the following section, the formal and the methodological frame of the Ph.D. project is described. First, the project’s development in the process of working with the subject is outlined. Second, the PUMA investigation (Danish acronym for Project on Burnout, Motivation, and Job Satisfaction) is described, being the basis for the choice of field for the investigation. Third, the role of the researcher in the project is described. Fourth, the case study approach as an approach to investigating the relationship between motivation and burnout is introduced. Finally, the process of entering the field of midwifery is described.
3.3.1 Formal basis of the Ph.D. project
The Ph.D.-project started on the first of July, 2000 after the formal application for a scholarship at the National Institute of Occupational Health in Copenhagen was successful. The flow of the Ph.D. work was interrupted at two points, being on maternity leave for a year each time. In the announcement, the following description of the research focus was given (translation by the author, sen).
Work motivation The goal of the Ph.D.-project is to analyse motivation in relation to work, understood as flow at work, engagement, joy at work or other
90
factors, which can both be inhibitory as well as supporting in regard to the preservation of work motivation throughout a whole work lifecycle. The project is both practical as well as theoretical. The theoretical part of the project contains a clarification and discussion of different work motivational theories. The empirical part can contain a combination of: qualitative analysis of motivation on an individual or workplace-level, and an analysis of motivation in regard to work climate and health-effects.
In the first proposal, a combination of qualitative as well as quantitative research methods was outlined. The main focus was work motivation and in a second step, the impact upon health and well being. An underlying goal of the project was the usage of relatively new methods to assess motivation (Experience Sampling Method to measure flow, Ciskszentmihalyi, 1987; Operanter Motiv Test to measure implicit motivation, Scheffer & Kuhl, 2000) as well as the qualitative approach to investigate the relationship between motivation and health. Some paths planned in a first step proved irrelevant, impractical or did not fit into the research scope of the National Institute of Occupational Health, Copenhagen (NIOH) and therefore were excluded. Altogether the first proposal was very far reaching and beyond the scope of a three-year Ph.D.-project. What remained is a coherent, consequent qualitative case study in the field of midwifery, investigating the question of how to understand the relationship between motivation and burnout in human service work. The research process throughout the project has been a great opportunity to learn and to develop my own research profile.
3.3.2 Description of the PUMA investigation
The present study of the case on motivation and burnout in human service work was initiated as reaction to the partly devastating results of a comprehensive,
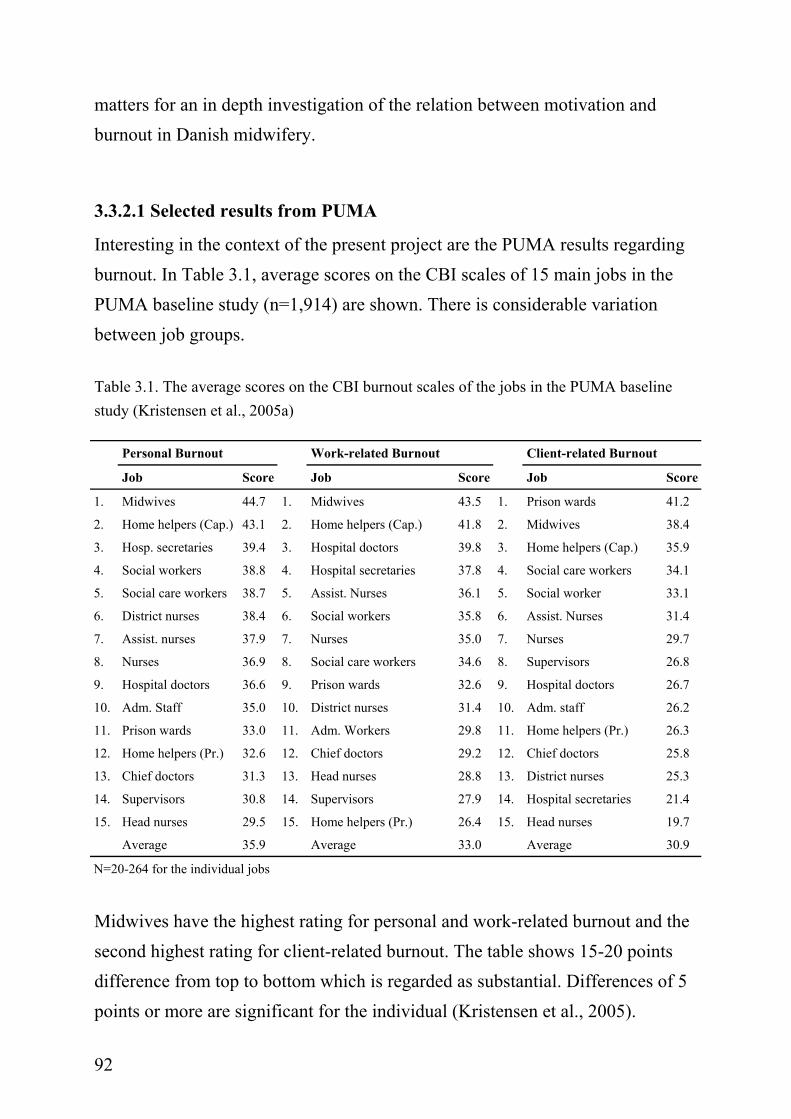
91
prospective study of burnout and psychosocial well-being at work in different job groups in Denmark (PUMA). The three main goals for the PUMA investigation were formulated as following: (1) to write a critical appraisal of international research on burnout with the focus on the conceptualization and measurement of burnout as well as intervention research in the field (Kristensen & Borritz, 1998; Thomsen, 2002); (2) to translate and validate the relevant instruments to measure burnout to the Danish language; (3) to carry out a prospective investigation in the field in order to be able to make assumptions about the extent, causes, and consequences of burnout in different job groups on the Danish labour market. Over a period of six years, 1,914 participants from the field of human service work are asked at three different points in time (baseline: 1999-2000, first follow-up 2002-2003; second follow-up 2005) to answer a questionnaire containing questions from the Copenhagen Psycho Social Questionnaire (COPSOQ, Kristensen et al., 2005b) and the Copenhagen Burnout Inventory (CBI, Kristensen et al., 2005; see Appendix A). The following seven organisations, representing different parts of the human service sector in Denmark participated in the PUMA investigation: home care services (countryside and capital), a somatic hospital, a state psychiatric prison, institutions for severely disabled adults in a county, and a social security service in the urban area. PUMA is designed as an intervention study with interventions not under control of the research team but to decide in the different workplaces. Interventions at the different workplaces can take place but do not necessarily take place. Through follow-up meetings with group delegates from the participating groups, the process of interventions at the sites is reflected on. Hence, the knowledge about interventions is not formally assessed. In the first round (and also in the follow-up investigation) of PUMA midwives showed the most severe levels of burnout in comparison to the other job groups and compared to an average through the Danish working population. This settled
92
matters for an in depth investigation of the relation between motivation and burnout in Danish midwifery.
3.3.2.1 Selected results from PUMA
Interesting in the context of the present project are the PUMA results regarding burnout. In Table 3.1, average scores on the CBI scales of 15 main jobs in the PUMA baseline study (n=1,914) are shown. There is considerable variation between job groups. Table 3.1. The average scores on the CBI burnout scales of the jobs in the PUMA baseline study (Kristensen et al., 2005a) Personal Burnout Work-related Burnout Client-related Burnout
Job Score Job Score Job Score
1. Midwives 44.7 1. Midwives 43.5 1. Prison wards 41.2
2. Home helpers (Cap.) 43.1 2. Home helpers (Cap.) 41.8 2. Midwives 38.4
3. Hosp. secretaries 39.4 3. Hospital doctors 39.8 3. Home helpers (Cap.) 35.9
4. Social workers 38.8 4. Hospital secretaries 37.8 4. Social care workers 34.1
5. Social care workers 38.7 5. Assist. Nurses 36.1 5. Social worker 33.1
6. District nurses 38.4 6. Social workers 35.8 6. Assist. Nurses 31.4
7. Assist. nurses 37.9 7. Nurses 35.0 7. Nurses 29.7
8. Nurses 36.9 8. Social care workers 34.6 8. Supervisors 26.8
9. Hospital doctors 36.6 9. Prison wards 32.6 9. Hospital doctors 26.7
10. Adm. Staff 35.0 10. District nurses 31.4 10. Adm. staff 26.2
11. Prison wards 33.0 11. Adm. Workers 29.8 11. Home helpers (Pr.) 26.3
12. Home helpers (Pr.) 32.6 12. Chief doctors 29.2 12. Chief doctors 25.8
13. Chief doctors 31.3 13. Head nurses 28.8 13. District nurses 25.3
14. Supervisors 30.8 14. Supervisors 27.9 14. Hospital secretaries 21.4
15. Head nurses 29.5 15. Home helpers (Pr.) 26.4 15. Head nurses 19.7
Average 35.9 Average 33.0 Average 30.9
N=20-264 for the individual jobs
Midwives have the highest rating for personal and work-related burnout and the second highest rating for client-related burnout. The table shows 15-20 points difference from top to bottom which is regarded as substantial. Differences of 5 points or more are significant for the individual (Kristensen et al., 2005).
93
Midwives are also one of the job groups with similar ranks on all three scales whereas other job groups have high ranks on one scale and middle to low on the other (e.g. hospital doctors, hospital secretaries). At the three year follow-up midwives still showed considerably high ratings on all three scales, as client-related and work-related burnout even went up some points and personal burnout was only slightly below the score measured in the first round of PUMA.
3.3.2.2 Role of PUMA within the present project
The PUMA investigation is the starting point as well as the frame of reference for the present case study. Chronologically, the present Ph.D. project started at the point where the first round of investigation was finished and the results were already given back to the sites. The high degree of burnout in midwifery was an alarming result and was met with high interest from the midwives who had participated. From a research perspective the results from the first round in PUMA suggested a qualitative approach to get more insight into causes and consequences of burnout in this job group which is otherwise known for high engagement at the job. Qualitative investigations (interviews) to help in the process of developing and validating an instrument to measure burnout and to find out about developmental processes of burnout had been planed for PUMA (Kristensen & Borritz, 1998) but had not taken place before the start of the quantitative investigation. Besides the present case study on the relationship between motivation and burnout in human service work in midwifery, two other job groups were chosen for further in-depth investigation: home care services in both the Danish capital and countryside (Thomsen, 2002) as well as in one county’s institutions for severely disabled adults (Christensen, 2003).
3.3.3 The role of the researcher
In psychological research referring to the quantitative paradigm, the importance of the researcher was long neglected. Moreover, the researcher has been defined as an objective agent whose influence needs to be controlled to a possible
94
minimum. This led to a distanced position of the researcher. With the re-introduction of interpretive methods as main source of gathering knowledge in a field of interest, the researcher’s role changes from the neutral observer to a catalyst in the process of creating meaning. Becker (1998, in Denzin & Lincoln 2000, p.4) describes the qualitative researcher as a bricoleur, “using the aesthetic and material tools of her craft, deploying whatever strategies, methods, or empirical material are at hand”. In the following, three different aspects of the researcher’s role in the post-positivist era are outlined: the researcher as catalyst for the production of knowledge, the researcher as traveller, and the researcher as observer. These metaphorical descriptions emphasize the research position chosen throughout the present project and therefore are introduced in the following.
3.3.3.1 The researcher as catalyst for knowledge production
All throughout the research process, the person of the researcher has influence on the emergent result. Malterud (1996) draws attention to the impossibility of defining the observer as an objective agent. The observer can have different forms of involvement (e.g., from sending out a survey to fieldwork over a longer period of time). Yet in the end, any observation is, to a certain degree, connected to the observer (Flick, 2002). The way of formulating the research question, the mode of data collection, the analysis and the communication of results is characteristic for the researcher as a person and mirrors her mindset and belief system. According to this, it is not a question whether the researcher has influence but rather how the researcher has influence on the production of knowledge (Malterud, 1996). To know one’s own role throughout the research process as well as one’s cultural background, explicated mindset and tradition is an important part of the investigation. Also of prominent importance is the explication of the author’s fore-understanding as well as the theoretical reference frame chosen as basis for further analysis. Fore-understanding (German: Vormeinung, Gadamer, 1990/1960) indicates the existence of a form
95
of pre-existing knowledge about a phenomenon. Malterud (2001) defines fore-understanding as “previous personal and professional experiences, pre-study beliefs about how things are and what is to be investigated, motivation and qualifications for exploration of the field, and perspectives and theoretical foundations related to education and interests.” It is the personal backpack of experience, knowledge, hypotheses, perspectives, ready to use as reference frame, mode for interpretation, and basis of reflection. The explication of one’s fore-understanding is important in order to reach a greater degree of freedom for interpretation of the empirical material. Within phenomenological research, this step is called Epoche (Moustakas, 1994). It is the process of setting one’s prejudgements aside and opening the research interview with an unbiased, receptive presence (Moustakas, 1994). Unbiased, receptive presence is understood as reflected subjectivity not neutrality. In other words: the better a researcher has explicated her own fore-understanding about the investigated phenomenon, the better she is able to differentiate between new insights and old knowledge about a phenomenon. A good example to illustrate this is therapeutical work. A psychotherapist is not immune against psychological disorder but in her work she uses conscious techniques to reflect her work with a client, e.g. in supervision. Later, in the process of writing about the findings of the empirical project, the formulation of fore-understanding can serve as point of reference. The “degree of surprise” stemming from the empirical data is a measure of how much new knowledge was found.
3.3.3.2 Researcher as traveller
The researcher as traveller is a metaphor used by Kvale (1994) in order to explain one approach to conducting a qualitative research interview. In contrast to a miner, whose prominent goal is to find buried treasure, the traveller “wanders along, asks questions that lead the subjects to tell their own stories of their lived world, and converses with them in the original Latin meaning of conversation as “wandering together with them” (Kvale, 1994, p. 18). The
96
researcher looks for the best possible form of understanding. Moreover, understanding is negotiated. It is a circular process changing both the observer as well as the observed. This is not only true for qualitative research approaches. Kristensen (2005a) mentions one important aspect when investigating health issues in practice: as soon as a person pays attention to a phenomenon, not known by name before, she will be even more attentive to it and her naïve perception about this phenomenon is gone forever. Her perception, her attitude, even her emotional relation to the phenomenon is different from before; her innocence in regard to the phenomenon is lost. The researcher’s role within a qualitative research paradigm is to lead through this explorative process without imprinting pre-formulated meaning about the phenomenon. The researcher has to be open to reformulate her understanding about the phenomenon at any time and risk a well-defined understanding about a phenomenon in order to reach to the essence of a phenomenon. Then again, this essence of the phenomenon is open for change, negotiable in context and defined in dialogue with the other.
3.3.3.3 The researcher as observer and constructor of meaning
The researcher sits with the expectation of constructing meaning on her own using the information provided by the participant and putting it into a new context (reconstructing or reframing). This process demands best knowledge about the field of investigation (theory, assumptions), good interpretative skills with high sensitivity for the data, the informant, and the context. Any phenomenon can be interpreted, put into another context, or seen from a different perspective, dependent from the observer, the creator of meaning. The description of any observation leads us back to the observer. It is her referential frame that is the ground for the observation described. The observed is so to say dependent on the observational skill of the observer. In qualitative research, the process of observation is reflected in-depth. The self-reflection is important in order to differentiate between the phenomenon as it is and the phenomenon as seen and described through the eyes of an observer. The influence of the
97
researcher as observer is taken into account and is a vital part of qualitative research. On the other hand, this does not imply that an observation is arbitrary (Fog, 1994). The observation is always bound up in context. Moreover, the observer has an obligation to stay connected to the context within which the observation is made. Meaning is created on the ground of the documented communication between the researcher and the field. Qualitative investigation is about finding a path or pattern of meaning in the chaos of perspectives on the phenomenon. The helping aid is active listening (understanding through asking and answering questions), thorough observing, and an open mind. The researcher’s body and mind is the lens through which the information is condensed. The characteristics of the lens are defined by the cultural and situational context the researcher is living and working in. The more experience she has gathered and deliberately integrated into her heart and mind, the more differentiated her interpretative skill. Especially with proximal methods of qualitative inquiry, it should be kept in mind that any interpretation of the information given can be threatening and hurtful for the participant. It can open new perspectives, which have been hidden behind a sound argumentative context for good reason. One important skill for any researcher engaged in qualitative research is the ability to look at the world from a different perspective. With any interpretation grounded on the data gathered, there is the responsibility to reflect on the respondents’ perspective (worldview) in the best way. Last but not least, there is no definite truth about social phenomena, because they are embedded in and grow out of the context, which is in flow. It can never be the same again; never be seen with the same pair of eyes, heard with the same ears, nor felt through the same body. The observer of the observed is unique and so is the observation, but this does not make the observation less relevant. Any qualitative research setting demands a direct contact to the participants in the field. Staying at the edge and observing from the outside will not lead to
98
reliable data, because the depth and richness of qualitative data depend on the trust and contact established between the researcher and her participants (Malterud, 1996; Fog, 1994). Understanding in the qualitative paradigm is like dancing an unknown dance with somebody just met. To be able to dance in harmony one has to be grounded as a person in context, trust the partner to follow or lead, be sensitive to any signal from the other, and be able to listen to the inner voice of intuition for movement to music.
3.3.3.4 Explicated fore-understanding and self-reflexivity
The explication of one’s fore-understanding and self-reflexivity are regarded as vital and important parts in a qualitative research approach. Therefore, different ways and methods of acknowledging this were used throughout the present project.
• An interview about the author’s fore-understanding was conducted: A colleague at the National Institute of Occupational Health (NIOH, Copenhagen) interviewed the author of the present monograph. The preparation for the interview was a written text, given to the interviewer before the interview took place. The informal paper served as first impression and focus throughout the interview. The interview was recorded to use as reminder. One important outcome of this reflection in dialogue was the cultural perspective onto the field of midwifery (see Chapter 8).
• Since October 2002, a logbook was used for documentation of the research process. All through the process of data analysis memos (Strauss, 1998) were written in this logbook. The logbook in the present study served different purposes. It had the purpose of documentation of the research process as a whole. It is a way of documenting choices and the influence of new insights during the process. More concrete in regards to the case study, the logbook serves the function of a diary. Present
99
Box 3.2 Memo writing Memos contain different aspects. They can be descriptions of categories used while coding certain passages of an interview. Memos are written about rules used throughout the coding process. They can be thoughts and ideas which come to the analysist’s mind while coding and/or which do not directly refer to the data analysis at the moment. It could be a question about the material which is not answered by the recent interview but might have some relevance in the further process of analysis. Memos also include comparisons or relations between people, situations, or single codes (Strauss, 1998).
thoughts, insights, feelings, surprising events, etc. were documented in an unstructured way. It kept the memory being an observer fresh during the course of the investigation. In the phase of participant observation, the journal was used to document the impressions and observations during and right after the observation period. Throughout the interviews, the logbook was used in a more structured way, documenting the course of each interview, recording important observation, awkward feelings and specific observations which were not communicated throughout the interview. Throughout the overall process of the project, the logbook serves as form of diary, in order to keep important thoughts alive. The unstructured documentation is not published as such, but serves as a way to ground interpreted meaning.
• Throughout the entire research process, the project was presented and discussed in different groups at different times: at the research meeting of the psycho-social department of NIOH, Copenhagen; at the Kvalinetværket of NIOH, Copenhagen; at the Doktorandenkolloquim at the University of Hamburg, led by Ursula Brucks; at the research meeting of the department production og ledelse of the DTU, Copenhagen. Further, project presentation at the following Ph.D.-courses: Fokusgrupper og gruppeinterview i almen medicinisk forskning (Kirsti Malterud, 2002); The meeting between the researcher and the field (Margaretha Järvinen, Nanna Mik-Meyer, 2002) Artikelskrivning fra kvalitative studier I almen medicinisk forskning (Kirsti Malterud, 2003). All these different locations, people, and situations have had more or less
100
influence throughout the process. Some of these situations were experienced as highly inspiring others as rather destructive. Nonetheless, taken together, all of them had influence on the development of the project as they added new perspectives onto the process of investigating the case.
• The cultural background of the author was a valuable platform for observation and reflection. Being brought up and being educated in Germany endows the author with a certain perspective onto the field which is meant to open up for further insights.4 Throughout the empirical phase, it gave a lot of freedom to ask questions, relating the participants’ narratives to the author’s cultural background. This was not done for the purpose of comparing Danish and German midwives but rather for stimulating thought. One specific example was the felt responsibility of Danish midwives; also in cases where they had already given the responsibility over to a doctor. Other observations were reflected in a rather informal manner, throughout collegial communication and with interested others (e.g., fellow Ph.D. students). The different cultural background also plays a role in choice of reference frame.
• During the course of the Ph.D. project, I went on maternity leave twice. This is of course a significant aspect to consider when investigating in the field of midwifery at the same time. In my diary (logbook), I reflected on my personal experience during the two pregnancies in regard to the focus and outcome of the case study. Twice, the need to consciously set the frame for observation beyond my personal experience made me change track. The first sequence was a planned period of participant observation during my first pregnancy. I was seven months’ pregnant and had a period of very scary dreams about birth. I decided that this period was not very good to expose myself to being witness of somebody else’s delivery. Not
4 One example is to be sensitive to differences between health care systems. Having a different frame of reference (German health care system) makes it easier to see particularities in the Danish health care system (e.g., less ‘technological’ check-ups such as ultrasound under pregnancy but higher workmanlike understanding of midwives (embodied knowledge).
101
only that this might have induced even more fear, it would in any case have “spoiled” my observation with the fear and negative anticipation which accompanied me through this phase. The second conscious bracketing happened in regard to the two natural and uncomplicated births I had. Both of the deliveries went well, strengthening my belief that natural birth is the best choice to make. This is very much in common with what I have heard from the midwives I interviewed. At some point my supervisor shared the concern of my being too much in coalition with the case study participants, seeing the world through their eyes. The need to bracket my own fore-understanding and experience at births in order to come to a better understanding of the phenomenon itself helped me to qualify my conclusion and understanding from the case investigation beyond my personal experience.
3.3.4 Ethical considerations
The qualitative research approach chosen in the present project is characterized by a proximal approach towards the participants. The single in-depth interviews conducted in the course of the project are an intimate approach into the understanding and perception of the lifeworld of a midwife’s work. There are several things to consider when investigating with such an open approach. The most important thing from the author’s perspective is the rapport with the interviewee and the establishing of an atmosphere of trust. In any case, the interviewee needs to be informed about the use and further analysis of information given in the interview. In the present case investigation, the anonymity of the individual is guaranteed by the author. Interviewees were given those parts of the interviews which were used to illustrate the findings for permission. Agreement was asked for regarding the general use of a statement but not for the understanding of the content of the interview.
102
At some points during the single interviews, the author decided not to investigate further into the subject, because the interviewee signalized clearly that she was not willing to reflect further on the subject. This might to be explained by the following outcome of the case study: the heroic description of an engaged midwife given by the interviewees and at the same time the problem of describing concrete experiences of burnout in the subjective work situation (see Chapter 4). From the author’s perspective, the interviewees made clear that they don’t want to boil the “problem” of burnout down to a personal problem and at the same time they exaggerated the positive feature of being engaged in the job to an unobtainable level. Looking at this observation through the lens of ethical consideration makes the acceptance of borders set by the interviewees evident. In work psychological research, the tension between person-related factors and work-related factors which are made responsible for causing a certain condition is a constant point of discussion. It is obvious that a person contributes to a condition in a particular way (by personality trait, habits, cultural descent, etc.), but the more important question while investigating health issues at work goes beyond the single condition. The present project is actually riding on the edge of this tension. By diving into the single condition, patterns are found to understand the phenomenon on a more general level. The investigator (interviewer, observer, field attendant) has the responsibility of holding the space and balance for a positive tension. Another ethical consideration was the renunciation of using material from the interviews which focussed on a particular person, e.g. the management of the maternity ward. The potential gain by using this information in order to gain a greater understanding in regard to the research question was estimated as being too low compared to the risk of offending the management which then could be traced back to a certain person. At the same time, the author believes that if a person definitively wants to know who delivered a certain statement, this is possible with the information given in the book even though the interviewee’s name is kept secret.
103
3.3.5 Case study as research approach
The case study is defined as research approach, an in-between of methodological paradigms and concrete techniques of data collection (Lamnek, 2005, p. 298). Throughout a case investigation, relatively few people are investigated in depth. The single person is regarded as an important knowledge agent for the interpretation of the life world. Case study approaches are open for the usage of very different techniques and methods. Case studies can refer to the qualitative as well as to the quantitative paradigm. Common is the combination of different methods in the sense of triangulation of methods (Denzin, 1989, in Flick 2002). The triangulation of methods furthers to the validity of the outcome of the case investigation (Lamnek, 2005), because bias of single methods is reduced.
The methods used within a case study approach refer to the criteria of qualitative research, as they are communicative, naturalistic, authentic, and open (Lamnek, 2005). A case study is conducted within a naturalistic setting, employing communicative methods, such as open or narrative interviews, group discussions, participant observations, and document analysis.
A case is defined by any kind of social unit, a person, a group, an institution, a culture, an organisation, a specific characteristic, etc.. The scientific approach to a case differs from an everyday understanding of a case in the sense that the scientific approach (also within the interpretative paradigm) reconstructs reality through controlled cross-understanding (German: Fremdverstehen) (Lamnek, 2005, p. 312). The goal is the identification of extreme, ideal or typical action patterns, not the observation of singular action, as for example is true for case analysis within the psychoanalytical setting. The research goal is to produce information that can be “shared and applied beyond the study setting” (Malterud, 2001, p. 485). In the qualitative research paradigm, cases are selected
104
after theoretical sampling procedures. The field of investigation and the single cases are systematically chosen, either representing an extreme or an ideal type.
The investigation of the present case is done in the natural setting of midwifery in Denmark. Within the research setting of the investigation of motivation and burnout in human service work, a maternity ward of a hospital on Zealand, Denmark is defined as case. More precisely, the group of midwives who already were involved in the PUMA investigation defines the field of research. Out of pragmatic considerations, it made sense to follow up with the group who already committed time and effort into a quantitative investigation of burnout and who were interested in following up with an in-depth approach. Moreover, a case investigation asks for some suggestive cases in order to be able to come to a greater understanding about a certain phenomenon. Two things define the borders of the case: job definition and voluntary participation. Regarding the former, only midwives were asked to participate even though there are other people working at the maternity ward, such as medical doctors, nurses, nurse assistants. This is taking the fact into account that midwifery has some specific job features, being important for the investigation of the relation between motivation and burnout. Through the investigation of motivation and burnout in single persons (midwives), insights into the relation between motivation and burnout in midwifery (and maybe even broader, in human service work) are thought to be possible. The aspect of voluntariness was regarded as important for an in-depth approach. Qualitative research uses proximal methods and techniques to approach the field and the single participant. Therefore, it is important to have the full commitment of a participant, letting her decide whether to take part or not. Critical in this respect might be a selection bias. It is possible that only those midwives participated who want to get their opinion about the issue through. Also the healthy worker effect (McMichael, 1976) should be discussed; meaning, to get commitment only from those who are healthy and still at the workplace. The triangulation of methods and the
105
investigation of subunits of the case diminish the selection bias. The healthy worker effect is not easy to control since only those midwives were asked to participate who are not absent from work. In the present project, this was deliberately taken into account because the case was defined accordingly. In the last chapter of this monograph, different options for further investigations are discussed. For the present work, both aspects of bias were recognized and reflected upon but not solved.
3.3.6 Entering the field
The access to the field; the opening up for the researcher; the step into the field - all are different descriptions of entering into the research field. To open up for a research investigation means taking time, investing effort, being willing to give answers, to risk losing control, etc. (Wolff, 2000). These aspects can also be described as costs or investments of the participant in a research project. In most cases, the initial contact to the group of participants is of core importance for the success of getting access to the field. Before being able to get in (physical entrance to the field) and to get on (social entrance to the participants), an initial contact has to be established. The decision to focus onto the field of midwifery was made after the author was asked by a research colleague at the National Institute of Occupational Health to use the research focus (relation between motivation and burnout) in order to shed some light on the devastating results from the investigation of burnout in different job groups in Denmark (see description of the PUMA investigation in section 3.3.2). Even though one underlying assumption of the PUMA study was the relationship between motivation and burnout, this relationship was not investigated in depth. For this reason it was decided to choose the scope of the case study of human motivation and burnout in human service work accordingly. The focus was defined as doing a case study within midwifery in Denmark, using one specific ward as case. The author decided to ask those
106
midwives who had already participated in the PUMA investigation to participate in an in-depth approach to investigate the relationship between motivation and burnout.
The research colleague responsible for PUMA at the National Institute of Occupational Health (NIOH) in Copenhagen made an initial contact introducing the author to the leading midwife at the ward. A first meeting took place in order to talk about the conditions and the procedure in the course of the research project. At that point the first round of the PUMA investigation had been published and first steps towards intervention had been started from the hospital’s side. The leading midwife has the role of a gatekeeper (Bortz & Döring, 1995, in Masberg, 2004), deciding about the access to a closed field. She signalled clear interest in getting to know causes for the relatively high levels of self-reported burnout at her ward. Besides this interest from the leading midwife’s side, it seemed to be of initial importance to get compliance from the group of midwives, being known as a rather active and critical job group. Therefore a short presentation of the project’s intention and scope was given to a group of midwives at one of their monthly central meetings. At this meeting, the project was introduced and outlined. Information included the methodological approach, confidential aspects, and how participants for interviews are to be selected for single interviews. In the course of the meeting, agreement for participation was asked from the participants. The midwives being present at the meeting (approximately 50% of the staff) decided positively about taking part in the case study.
In order to get an impression of the group and to give them a possibility to get acquainted with the mode of questioning throughout the project, they were asked to discuss positive aspects of the work of a midwife. This first session served as possibility to establish a first relationship (rapport) with the group. This happened to be successful: When the actual empirical phase of the project
107
began, participants did remember the author’s presentation at the ward even though almost two years had passed due to maternity leave. In the session the midwives were asked to discuss the question of: “What is positive about being a midwife?” in an open forum.
The following answers were documented by the author:
• To get insight into the whole range of life
• Get close to people, a great moment (almost religious)
• The atmosphere during the delivery, to study the parents
• The many sides of the job and the different people you meet
• The unpredictability
• To guide people through a crisis
• Responsibility
• To be the expert
• Independence
• Creativity, find new solutions
• Do something that makes people remember me (important to one’s self-esteem)
• To be appreciated
• To see people grow during the delivery
• When a team works well
• That nature is an incredible and uncomprehensable concept
• To get well through a difficult delivery
• Always good to talk about when you meet other people
• Professional pride A first interesting discussion about “getting well through a difficult delivery” started. Two of the midwives said it was OK that not all deliveries are according to the book, but that it is nice that they have the opportunity to guide the parents in a situation where the child is stillborn or in a poor condition. This comment provoked a hot-headed discussion. To the investigative question of which job
108
group they think they can be best compared with, the midwives were at one about being best comparable with nurses working in an intensive care unit. The list of positive characteristics of being a midwife contains some interesting details. Some of the points mentioned as positive are defined as problematic in other job settings, e.g. unforeseeability. The aspect of spirituality was rather surprising and is regarded as enlargement of the author’s fore-understanding about the research interest. The first hurdle to entering the field was passed when the presentation at the center meeting went well and the participating midwives signalled interest.
3.4 Research methods Following the principle of triangulation of methods, different methods were used to investigate the research question. In the following section, the research field is described in a first step. The description of the field is based upon insights into midwifery in Denmark through reading. This reading is defined as method rather than as acquisition of theoretical knowledge, because it focuses on one specific job group in a specific work setting in a defined cultural background. It is thought to give the interested reader an impression of the historical and practical developments in midwifery throughout the last years. Further, the reading serves as source for validation and reflection of outcomes from participant observation, qualitative research interviews and group interviews in the result section (Chapter 4-7). The description of the research field is followed by the description of the qualitative methods used to investigate the field:
• Participant observation, as means to understand the particularities of midwifery in situ.
• Single interviews, as core method to investigate the research question.
• Group interview, used as member check (see Box 3.5).
109
3.4.1 Description of the research field
Midwifery in Denmark was first legally recognized in 1537. In 1902, the Danish Midwife Organisation (Den Almindelige Danske Jordemoderforening) was founded. Throughout the last century, a lot has changed regarding the work situation of midwives in Denmark. On an organisational level midwifery changed from one-woman-businesses (private practice) into employee status (being employee at a midwife center and later hospital) in 1984 with the introduction of the midwife centers. Up until 2004 is maternity care in Denmark provided in 33 hospitals with a birth frequency ranging from 15 births per year on a small island up to 5.533 births per year in one of the large maternity centers in Copenhagen. Today, most of the midwives in Denmark are employed at a midwife center connected to a hospital, however, a small but growing number work in private practice. But still, 98,8 % of births in 2004 and 2005 took place in a hospital (Sundhedsstyrelsen, 2006). In recent years, economical press in the health sector increased and does not stop at the doors of the maternity wards. This has also serious consequences for the work in midwifery. These consequences are discussed in the result section in regard to the role of allocated resources. In the following, some of the historically important developments of midwifery in Denmark throughout the last 20-30 years are described. These latest developments in the field and the planned developments in the near future are those that have the greatest impact on the recent midwife generation. The job conditions in the public sector are also dependent on political developments in the Danish social welfare society. The following aspects of modern midwifery in Denmark are described in order to give some insight into the outer conditions of Danish midwifery today: (1) Midwifery as human service profession (2) From ‘pay per birth’ to regular monthly payment, challenges of becoming part of public human service (3) Job description for midwives in Denmark (4) Midwife education in modern Denmark (5) Working conditions of midwives in Denmark.
110
The section closes with a summary of selected results of a survey amongst active and passive members of the Danish Midwife Union (Jordemoderforeningens medlemundersøgelse, Resonans ApS, 2003).
3.4.1.1 Midwifery as a human service profession
Midwifery is a particular profession within human services. In reference to Hasenfeld (1983), human service work is classified by their goal (people processing, people sustaining, or people changing) as well as by the type of people they serve (customers, clients, patients, students, etc.). It is a challenge to classify midwifery according to this description. Midwifery is a little bit of all: people are processed, sustained, and changed. Women giving birth are today understood as clients but some midwives refer to them as customers. Hasenfeld’s classification is not distinctive enough to describe human service in midwifery. Another interesting approach pointing at the logic used to classify jobs is outlined by Kaross & Spindler (1994, in Brucks, 1998, p. 19). It was investigated if scientific categories of job classifications correspond to lay categories classifying the jobs. They asked medical doctors to classify five job groups in the human service sector in regard to different categories. The similarities they found between job groups were not based on the reputation of the job. Rather, a factor analysis showed that an inner relationship between the jobs exists that is thought to be grounded on content and functional criteria. This approach is regarded as interesting model of thought. Midwifery has, from the perspective of the author, certain characteristics which can also be found in other sectors, e.g. air traffic control. Although relationships are found between different job groups, it is important to recognize that human service work is characterized by specific demands. This is more than relevant today where the human service sector is the growing sector of labour in modern society with at the same time declining resources to pay for the services.
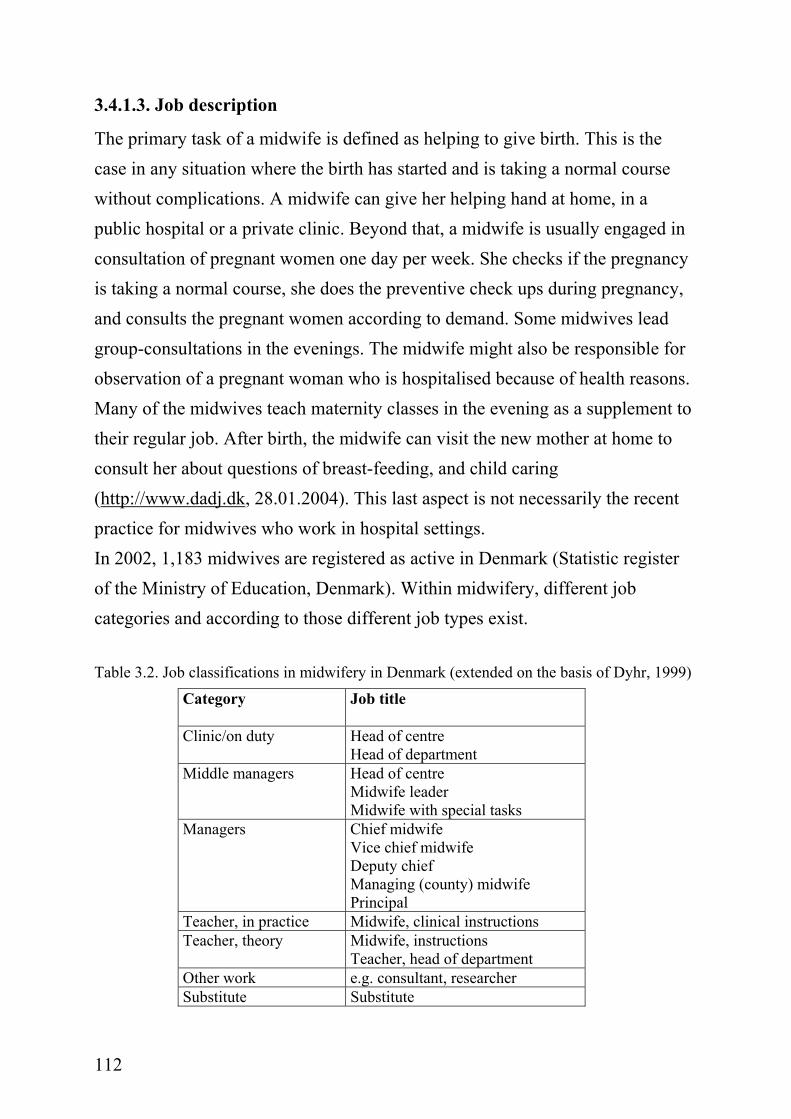
111
3.4.1.2. From “pay per birth” to regular monthly payment
The greatest change of working conditions in midwifery in Denmark throughout the last 30 years has been the change from free to public employment of midwives. Until 1984, most midwives worked in private practice, being in competition with other midwives in the same district. In 1984, the so-called center organization with public employment of midwives was introduced. Midwife centers are smaller or larger places where a group of midwife cooperates in the service provided to pregnant and birthing women. The midwives working in a center are public employees with regular pay. Today, midwife centers are most often connected to a hospital and resemble other wards in a hospital organization and have up to 30-40 midwives working together (Larsen, in Cliff, 2002). One of the biggest challenges was a change in perspective, not being competitors in helping to give birth any longer, but being colleagues with the responsibility of working together and cooperating. Another challenge related to the integration into public service was the change of the financial situation of midwives. There was some fear that the financial situation would change dramatically, because the midwives would change from “pay per birth” to a regular monthly pay. This change had, in fact, negative consequences for those midwives who had many births per year. Yet for many others it brought a regular monthly payment, security for times of illness and absence from work. Regarding work content, the center organization resulted in severe changes of the organization of work. Until then, midwives always had had their “own” pregnant women, consulting them through pregnancy and helping to give birth when the time had come, independent of where (at the hospital or at home) the woman in labour chose to give birth. With the organization of work in eight-hour shifts, this was no longer possible. Suddenly, midwives could not finish the work they had begun when the shift had ended. The holistic work experience simply vanished with the center organisation in midwifery. Today only a handful midwives work in private practice but with a growing tendency.
112
3.4.1.3. Job description
The primary task of a midwife is defined as helping to give birth. This is the case in any situation where the birth has started and is taking a normal course without complications. A midwife can give her helping hand at home, in a public hospital or a private clinic. Beyond that, a midwife is usually engaged in consultation of pregnant women one day per week. She checks if the pregnancy is taking a normal course, she does the preventive check ups during pregnancy, and consults the pregnant women according to demand. Some midwives lead group-consultations in the evenings. The midwife might also be responsible for observation of a pregnant woman who is hospitalised because of health reasons. Many of the midwives teach maternity classes in the evening as a supplement to their regular job. After birth, the midwife can visit the new mother at home to consult her about questions of breast-feeding, and child caring (http://www.dadj.dk, 28.01.2004). This last aspect is not necessarily the recent practice for midwives who work in hospital settings. In 2002, 1,183 midwives are registered as active in Denmark (Statistic register of the Ministry of Education, Denmark). Within midwifery, different job categories and according to those different job types exist. Table 3.2. Job classifications in midwifery in Denmark (extended on the basis of Dyhr, 1999)
Category Job title
Clinic/on duty Head of centre Head of department
Middle managers Head of centre Midwife leader Midwife with special tasks
Managers Chief midwife Vice chief midwife Deputy chief Managing (county) midwife Principal
Teacher, in practice Midwife, clinical instructions Teacher, theory Midwife, instructions
Teacher, head of department Other work e.g. consultant, researcher Substitute Substitute
113
The Table describes different positions in midwifery and the corresponding job title to exemplify the differences between the positions. In correspondence with category and title stand different functions of the midwife. It is close at hand that the difference in function makes also a difference in health status. Besides job type, two other features of the midwives’ job seem to be important and need to be discussed: job age - defined as years on the job, and work load - defined as birth per year. These two aspects are further reflected on in Chapter 4.
3.4.1.4. Midwife education and resources in modern Denmark
The education to become a midwife nowadays lasts three and a half years. Theory and practice each take 50% of the educational time. The midwife education is recognized as academic study, qualifying the students to do research and quality development at the worksite. The new professional bachelor degree enables the newly educated midwives to continue with further education. After having finished their education, midwives can apply for jobs at centers for midwifery, hospitals and at the midwife school. The conditions for entrance to the education are commonly recognized as high. It is not uncommon that those who are feel a call to become midwife but need to wait in order to get in. Resources in midwifery in Denmark always have been a problem. At the point of organizing midwifery in midwife-centers, there were not enough midwives to do the work. At the beginning of the 80s, birth rates went down dramatically so that the number of places in midwife education had to be reduced to 40 per year. Nonetheless, already in the 90s birth rates in Denmark went up and another dramatic shortage of midwives was experienced. At the end of 2003, there were 50 positions vacant throughout the country, which resulted in a lot of overwork for the remaining midwives. Therefore, the Danish ministry for education
114
decided to create more places to educate midwives. Throughout the coming years, 90 midwives per year will be educated in Denmark.
3.4.1.5 Working conditions of midwives in Denmark
Midwifery is a specific form of human service work, characterized by rather unique work demands and job characteristics. Dyhr (1999) summarizes some factors of the psychosocial work environment of midwives that might be relevant for work related health and well being: A midwife
• usually works in shifts,
• is regularly on 24 hour emergency call,
• works always with acute cases,
• works mostly alone,
• works with people in a crisis, and
• works in a field, in which a mistake can have serious or even fatal consequences.
Interesting with midwifery is that the core work task can be understood as universal. Yet at the same time there are cultural differences in this area of great importance. There are many differences in the perception of pregnancy, birth, and motherhood across different cultures. The role of and the way midwifery is organized differ from one country to the other. The job of a midwife in Denmark is characterized by low payment with at the same time high responsibility, dreadful ergonomic positions, challenging work hours (weekend work, work at times of holidays and vacation, work at night, working in short shifts with high qualitative and quantitative demand), and a high threat of stress related illness, e.g. burnout (Cliff, 2002). Working conditions of the midwives in the present project can be described by using the description of the psychosocial work environment of Dyhr above. The
115
participating midwives work in a three-shift-schedule (day, evening, night). The day shift lasts from 8.00 a.m. to 4.00.p.m.. Evening shift is from 4.00 p.m. to 12.00 p.m.. Night shift is accordingly from 12.00 p.m. to 8.00 a.m.. There are three midwives in each shift, supported by two nurses. There is one medical doctor responsible for each shift. All of them are present at shift change. Cases are shared at the beginning of each shift, when the leaving shift reports about the actual situation. The midwives work mostly alone with the women giving labour. In cases of insecurity or emergency other midwives are asked for support and professional help. The doctor is called in severe cases, e.g. sudden caesarean section and critical situation of mother or child. Some of the midwives at the ward work only day shift and evening shift. Others work only day shift being assigned to special duties not serving the primary task any longer.
3.4.1.6 Organisation of maternity care, desires of women and obstetrical figures
The organization of maternity care in Denmark is in my opinion best described as “being pragmatic”. The Danish health care system gives women access to a predetermined number of check-ups during pregnancy covered by the general practitioner and a midwife working in the hospital (maternity center) that the woman is assigned to give birth at. In case of complications during pregnancy, a woman has access to special treatment (ultrasound scanning, check ups done by a gynaecologist, acupuncture for pain relief, etc.). Pregnancy in Denmark is handled as a healthy state as long as everything is without complications. Danish midwives share the attitude of natural birth being the best option to vote for. Nevertheless, with further development of modern technologies, there is a growing tendency towards caesarean section, a good part of them being caesarean sections on maternal request. The rate of caesarean sections went from 12,4% of all deliveries in 1991 to 19,5% in 2003 (Sundhedsstyrelsen, 2005). Reasons for this growing number of caesarean sections have not yet been investigated in depth, but indicate that mainly multiparae (women who have
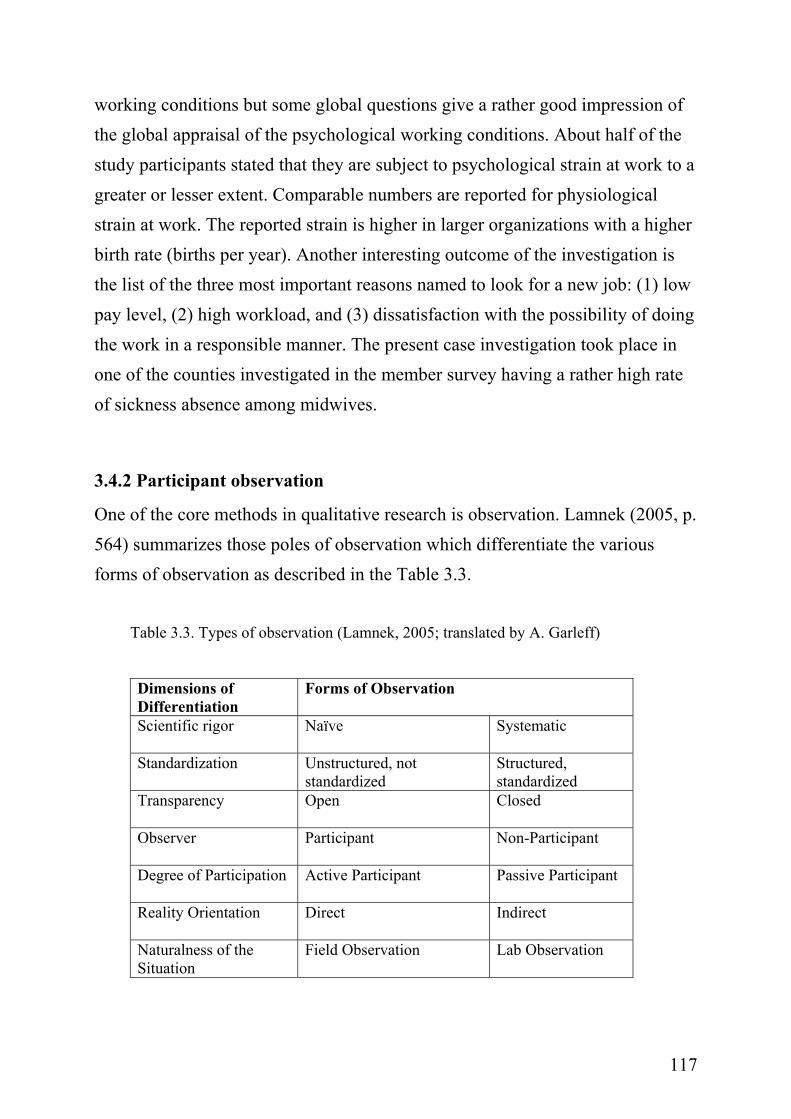
116
given birth before) who had a negative first birth experience more often request a caesarean section. It seems to be of great importance to assure a positive first birth experience not only for economical reasons but also for health reasons. At the moment there is an ongoing discussion in the media, the health professional circles and in the Danish parliamentary health committee about how to approach a growing number of maternally requested caesarean sections. Further research seems to be necessary to make a final conclusion but one aspect discussed in a recent report of the Danish Health Committee (Sundhedsstyrelsen, 2005) is the need for balanced information about the benefits and risks of a caesarean section for both mother and child. The percentage of stillborn children in Denmark went down unexpectedly by 0,1% from 0,5% in 2004 to 0,4% in 2005 even though the gestation age of the foetus went down from 28 weeks to 22 weeks counting a child as being stillborn.
3.4.1.7 Summary of member survey of the Danish Midwife Union
A recent questionnaire investigation amongst members of the Danish Midwife Union (Jordemoderforeningens medlemsundersøgelse, Resonans ApS, 2003) gives interesting background information for the present case study. In the late summer 2002, all active and passive members of the union were asked to answer a questionnaire. The main question of the investigation was about how the union should develop in the years to come. 1,142 members returned the questionnaire, which corresponds to a return rate of 57% (71% active members, 43% passive members, 44% students). Amongst other themes, 75% of the study participants wish that working conditions (psychological as well as physiological) got a higher recognition in the work of the union. Moreover, the participating midwives stress the fact that work organization is especially a problem in larger organizations. Especially the conditions of helping to give birth in a responsible manner were named. The investigation was not focused on psychological
117
working conditions but some global questions give a rather good impression of the global appraisal of the psychological working conditions. About half of the study participants stated that they are subject to psychological strain at work to a greater or lesser extent. Comparable numbers are reported for physiological strain at work. The reported strain is higher in larger organizations with a higher birth rate (births per year). Another interesting outcome of the investigation is the list of the three most important reasons named to look for a new job: (1) low pay level, (2) high workload, and (3) dissatisfaction with the possibility of doing the work in a responsible manner. The present case investigation took place in one of the counties investigated in the member survey having a rather high rate of sickness absence among midwives.
3.4.2 Participant observation
One of the core methods in qualitative research is observation. Lamnek (2005, p. 564) summarizes those poles of observation which differentiate the various forms of observation as described in the Table 3.3.
Table 3.3. Types of observation (Lamnek, 2005; translated by A. Garleff)
Dimensions of Differentiation
Forms of Observation
Scientific rigor
Naïve Systematic
Standardization Unstructured, not standardized
Structured, standardized
Transparency
Open Closed
Observer
Participant Non-Participant
Degree of Participation
Active Participant Passive Participant
Reality Orientation
Direct Indirect
Naturalness of the Situation
Field Observation Lab Observation
118
Forms of observation move between the poles of the seven dimensions. One main dispute in social research is the differentiation between cognitive-observation and emotional-participative experiences of reality. The former is observation in a limited and empirical form, also described as scientific-analytical. The latter is observation in the sense of understanding. Observation in the sense of understanding sets the precondition of “Adoption of an adequate mindset suiting the social system observed” (Lamnek, 2005, p. 551)5. This form of observation comes closer to a pragmatic, everyday form of observation. Good participant observation needs both aspects. Observation is the way to investigate behaviour in the real setting. The life world (natural setting) of the participant is the place for observation. Participant observation is a way to understand behaviour and routines, which might have become natural and self-explanatory for the observant.
3.4.2.1 Aims of participant observation
Because not much particular information about the specific work routine of midwives was accessible to the author, it was decided to do participant observation at the work place. The observation period served two different purposes: (1) get a profound insight into the field of midwifery in Denmark, the organizational work flow at the particular labour ward and to get an understanding of the overall climate at the ward, as well as (2) to observe a midwife being on duty throughout a whole shift in order to understand the particularities of the job, the daily organization of work life, and differences in fulfilling the job. The daily routines and core tasks were observed and questioned in order to understand the conditions which are an important part of the picture looking at motivation and burnout amongst midwives. Data from participant observation are used as supplement and confirmative asset while describing and interpreting data from the single interviews and the group interview.
5 German: Aneignung des dem beobachteten sozialen System angemessenen Sinnverständnis.
119
3.4.2.2 Procedure for participant observation
To offset the investigation and in between times, participant observation was planned during one of three shifts (morning, day and night shift). The days were chosen at random and were not communicated to the midwives on duty in advance. The decision whom to follow during the whole shift was made at the change of shifts. The three midwives being on duty during the shift decided amongst themselves who the researcher should follow during the shift. One midwife was followed for the whole course of a shift. Being the midwife’s shadow throughout the shift made a very smooth and silent observation possible, where not much talking was afforded while “running” from one room to the other. It was the most appropriate solution because it is very common that midwives are so busy delivering babies that they “disappear” for a longer period of time in the labour ward. Different from the original plan, the observation was done during two different shifts instead of three. (1) During a day shift in October 2002, 8.00 a.m. – 4.00 p.m., and (2) during an evening shift in November 2002, 4.00 p.m.-12.00 p.m.. Observations were documented in free form in the logbook during the observation period and were complemented right after returning from the observation. The rather unstructured observation was meant to further unexpected insights and to expand the tacit and explicit knowledge of the observer. A list with knowledge-based and experience-based questions was formulated before starting the observation to be used as red thread throughout the observation period.
Daily organization of work How many shifts per day? How many people per shift (midwives and other staff at the ward)? Who does what (work roles)? What kind of shared routines are there (e.g., meetings)? Content of work What particular tasks has a midwife? Are there obvious work routines? What kind of decision criteria can be observed?
120
Climate at the ward How do the midwives communicate with each other, with patients, and with people from other job groups (both, personal and professional)? How can the overall climate/atmosphere at the ward be described?
The list of criteria above is understood as a list of observational categories, helping to understand the work life of a midwife in this particular hospital. Insights from observation are used as basis to get a better understanding of the research field and in the sense of method triangulation. It is regarded as necessary to have some insights into the research field in order to be able to ask significant questions. In a second loop, observational insights are used to validate insights from interviews. The single interviews constitute the core method of investigating the relationship between motivation and burnout in human service work. The subjective nature of in-depth interviews is advantageous and challenging at the same time. By using insights from observation as validation, subjective information is “tested” against a second perspective onto the subject. Reflection of participant observation in the present project The way observation was done in the present study has the following limitations and shortcomings: (1) Two points of observation do not give a complete picture of the work situation of midwives. In regard to validation of insights of outcomes from the single interviews, a second observation period could have been helpful. This was not done because of organizational reasons. The organizational structure of the ward was changed throughout the research process and at the time the empirical phase came to an end, the process of restructuring was still in a “revolutionary” phase. This revolutionary phase was not regarded as particularly good point in time for observation of the regular work flow in midwifery. (2) As described in the foregoing section, observation was done by being the shadow of a single midwife. At the same time, it was not planned beforehand whom to shadow, it happened by chance. Those being present at the ward could volunteer to be shadowed. It should be noted that there
121
is a risk for selection bias. This risk is regarded as negligible because the focus of observation is the organization of work and not the behaviour of the particular person. A second hurdle to be described goes a step further. The leading midwife, being the gatekeeper in regard to getting access to the field, plays a particular role at this point. From her side came the permission for the researcher to step in at any day at any time. This made life very simple for the researcher because there was no need to plan long ahead. To approach the field in this rather surprising way had positive and negative effects. At least with two midwives being present at the two different shifts resistance could be felt when the researcher (author) arrived at the ward without having been announced beforehand. It was a little awkward to step in and demand how things would work best and be present throughout the whole shift without preliminary announcement. On the other hand, the “surprise factor” can be seen in a positive light. In fact, there was no time to build up assumptions about how it would be to have a researcher at the side to be one’s shadow.
3.4.3 Qualitative research interview (single interviews)
The core method throughout the case study is a set of in-depth, single, qualitative research interviews with approximately 10-12 midwives from the particular ward. A stepwise procedure of gathering, transcribing and analyzing information in regard to the research question gives the possibility of keeping the amount of interviews to be conducted open. As cut-off point of when to stop, the criterion of saturation of information and knowledge is formulated. In the following, the purpose and procedure of the phase of single interviews is described.
3.4.3.1 Purpose and methodological frame of the single interviews
The main purpose is to get a deeper understanding of the relationship between motivation and burnout in human service work based upon subjective interpretations of it. The acquisition of subjective definitions, cognitions,
122
emotions and feelings, and interpretations about the relationship between motivation and burnout is the focus throughout the interviews. Subjective, personal wording and description of the field is highly desirable wanted. It is assumed that the access to subjective understanding of the relationship between motivation and burnout brings about new perspectives. The particular, everyday understanding of scientific terms, which is determined by everyday experience, belief, and feelings are of interest. Understanding in the context of a qualitative interview is established through the process of professional interviewing. The research interview is different from a normal conversation of one-sided interest. The researcher approaches the interviewee in order to get information about the research topic. In fact, it is a rather uneven process, where the researcher is in a powerful position in relation to the interview person (Kvale, 2002; Hauge, 2005). The interviewer owns the role of being the one to ask questions, whereas the interviewee has the role of the one being “forced” to answer. Nevertheless, communication in the course of the single interviews is understood as a two-sided process, as dialogue (Kleining, 1982). Both interviewer and interviewee are able to direct the flow of the dialogue, even if the interviewer per definition has the power to interrupt and ask questions, which lead into a different direction than expected or even intended by the interviewee. In this sense, the interview can be understood as an interpersonal drama with a developing plot. Reality is negotiated between the parties of the communication (Holstein & Gubrium, 1995). In this post-modern understanding of the interview (Kvale, 1994; Fog, 1994), reality and truth are constructed in dialogue between the
Box 3.3 Post-modern understanding Post-modern thought can be traced back to Kuhn (1970) and Feyerabend (1976) who both questioned the modern understanding of explaining the world through systematic study (Gergen, 1992). Instead, truth is thought to be a matter of perspective. In a post-modern understanding the scientist is no longer the superior knower but understood as ‘traveller’ negotiating meaning on the way. Historical roots, cultural patterns, preferred discourse, and situational circumstances are accounted for in post-modern inquiry. The ability of critical self-reflection is essential for the post-modern scholar.
123
interviewer as knowledge and information seeker and the respondent as the one opening themselves up for the questions asked, interpreting and answering them in a specific and subjective way. An important aspect while interviewing another person is what is known as rapport in the therapeutic setting. Here, rapport is understood as the researcher’s ability to “take the role of the respondents and to attempt to see the situation from their viewpoint, rather than superimpose his or her world of academia and preconception upon them” (Fontana & Frey, 2000). Rapport is established through confidence and trust in the person who is conducting the interview. The more personal the theme of the interview, the more important it is to have established collaborative, reciprocal, trusting, and friendly relations with those studied.
3.4.3.2 Participants
Participants of this case study are midwives employed at a hospital on Zealand, Denmark. A number of wards of this particular hospital participated in the PUMA investigation (see section 3.3.2). All midwives (N=49) employed at the gynaecological ward in the month of October 2002 were asked in written form to participate in the present case study. A letter, a short form with demographic questions (Appendix B), and a free return envelope to the author’s workplace address was put into the personal post boxes at the ward. Midwife students were not invited. Out of 49 midwives employed at the ward at this point, 26 volunteered to participate in the single interview. Approximately 30% of the 49 midwives were working part-time. On average, 2,600 children per year are born at the ward. Altogether, the author got the impression that the interest in participating in the case study was quite strong. Different reasons were given for this interest. Some of the midwives felt that the PUMA study disclosed important shortcomings and challenges in the work life of midwives that need to be investigated in more depth. Others were rather discontent with the processing
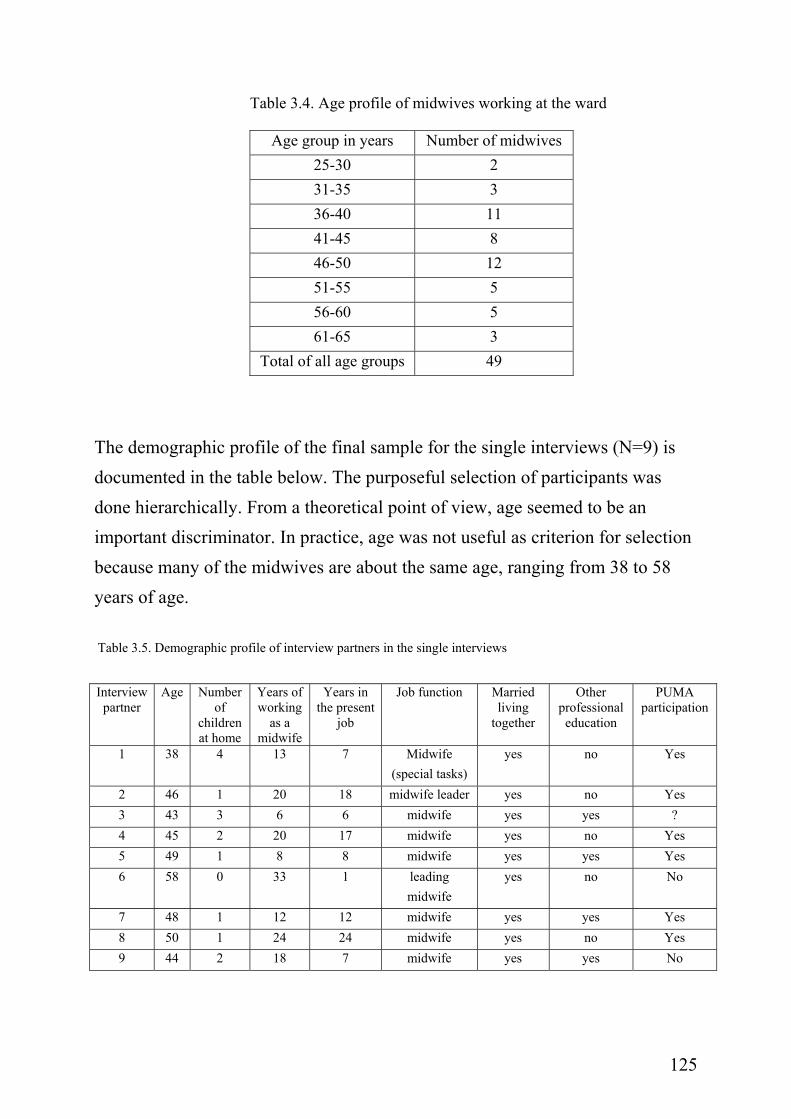
124
Box 3.4 Saturation of meaning Saturation is the criterion used to decide when data acquisition has reached a point of sufficiency in the sense that no more meaningful knowledge can be added to the already gathered material. Kvale (1994) mentions the rule that interviewing can be stopped at a point where further interviews do not add new insights.
of work group outcomes, focussing on change (e.g., making recommendations of how to plan shifts). 15 midwives were pre-selected after the principles of purposeful sampling (Denzin & Lincoln, 2000; Malterud, 2001). Purposeful sampling is done by pre-selecting settings, groups, and individual participants according to the most relevant criteria for the case to be studied. All possible participants (every midwife at the ward) of the interview investigation were asked to fill out a form with demographical questions (age, marital status, number of children, seniority, education, and job position, see Appendix B). Participants were selected according to the greatest possible diversity in regard to their demographical background, because it is assumed that such participants can contribute additional aspects to the research question. Interviews are done in stages. After each interview, the material is analysed before moving on to the next. This procedure enables the researcher to take information from one interview to the next, going into more depth with an issue of interest. Throughout the process of investigation stages, it became clear that saturation (Lincoln & Gobi, 1985) was reached after the first nine interviews.
The following Table (3.4) summarizes the age profile of midwives working at the ward. As can be seen in the age profile of the midwives employed at the ward, the middle age group (35-50 years old) is the largest group at the ward (31 out of 49 midwives belong to that group). In the group of midwives being younger than 35 years there were at total only five midwives.
125
Table 3.4. Age profile of midwives working at the ward
Age group in years Number of midwives 25-30 2 31-35 3 36-40 11 41-45 8 46-50 12 51-55 5 56-60 5 61-65 3
Total of all age groups 49
The demographic profile of the final sample for the single interviews (N=9) is documented in the table below. The purposeful selection of participants was done hierarchically. From a theoretical point of view, age seemed to be an important discriminator. In practice, age was not useful as criterion for selection because many of the midwives are about the same age, ranging from 38 to 58 years of age. Table 3.5. Demographic profile of interview partners in the single interviews
Interview partner
Age Number of
children at home
Years of working
as a midwife
Years in the present
job
Job function
Married living
together
Other professional education
PUMA participation
1 38 4 13 7 Midwife (special tasks)
yes no Yes
2 46 1 20 18 midwife leader yes no Yes 3 43 3 6 6 midwife yes yes ? 4 45 2 20 17 midwife yes no Yes 5 49 1 8 8 midwife yes yes Yes 6 58 0 33 1 leading
midwife yes no No
7 48 1 12 12 midwife yes yes Yes 8 50 1 24 24 midwife yes no Yes 9 44 2 18 7 midwife yes yes No
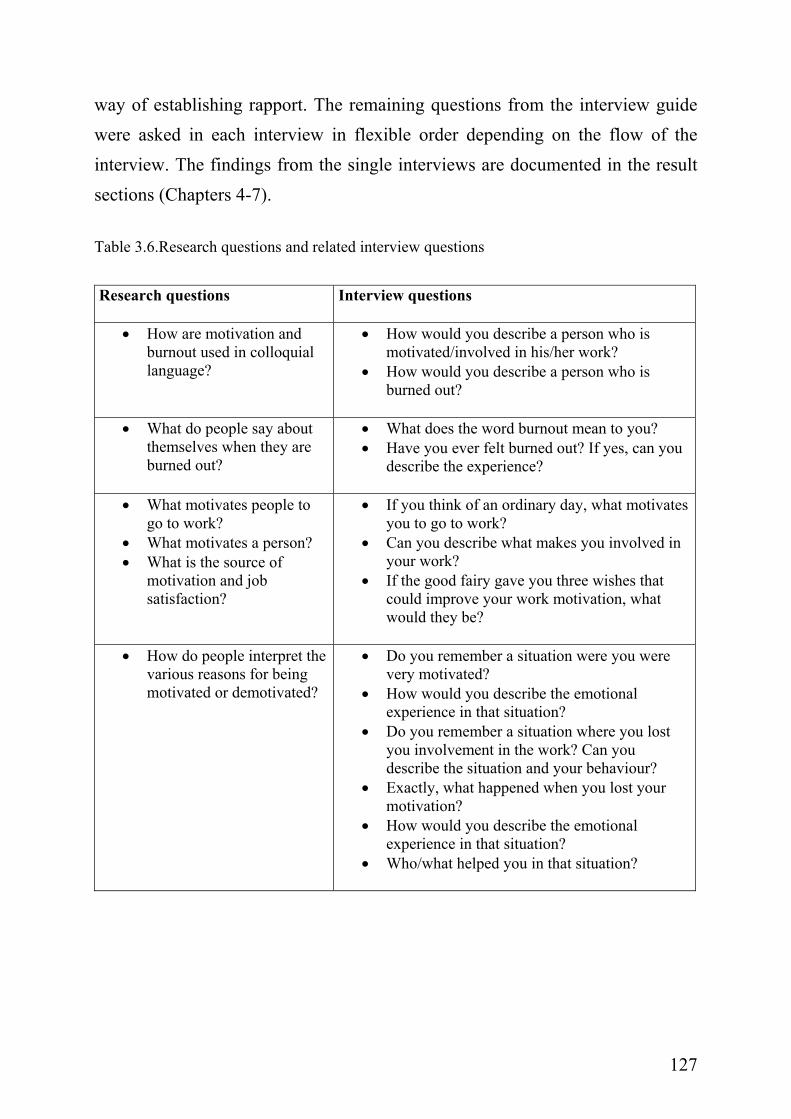
126
Unfortunately, it did not occur that someone from the group of younger midwives volunteered to take part in the round of single interviews. A second order factor was job age. Two groups of participating midwives could be interviewed, the one being in the middle job-age group (5-10 years old) and the other being part of the high job-age group (10-20 years old). Midwives who were only a short time on the job (less than five years) did not volunteer to participate in the interview. As third order factor, a second professional education was defined as being a discriminating factor. The group of midwives was split in half: four of them having had a former education before being educated as a midwife, five of them having started with midwife education right after high school. Family status was not a discriminating factor, because all of the midwives were married or living together with a partner. Of the nine midwives, three midwives worked with special assignments. Two of them were in a leading position.
3.4.3.3 Description of procedure
The interview itself is supposed to follow the natural flow of a dialogue. A preformulated interview guide (see next page) is used as a guideline for asking questions. Variations in order of questions in the course of a qualitative research interview are natural (Kvale, 1994; Fog, 1994). It is regarded as important to distinguish between research questions and interview questions, because a good research question must not necessarily be a good interview question (Kvale, 1994).
A complete version of the interview guide (including introductory and closing questions) can be found in Appendix C. The opening question is kept the same in each interview. It is a warm-up question about the history of the personal career development (beginning at the point of leaving school). It is thought of as an introduction into the interview situation as such and is meant to be a good
127
way of establishing rapport. The remaining questions from the interview guide were asked in each interview in flexible order depending on the flow of the interview. The findings from the single interviews are documented in the result sections (Chapters 4-7). Table 3.6.Research questions and related interview questions
Research questions Interview questions
• How are motivation and
burnout used in colloquial language?
• How would you describe a person who is motivated/involved in his/her work?
• How would you describe a person who is burned out?
• What do people say about
themselves when they are burned out?
• What does the word burnout mean to you? • Have you ever felt burned out? If yes, can you
describe the experience?
• What motivates people to go to work?
• What motivates a person? • What is the source of
motivation and job satisfaction?
• If you think of an ordinary day, what motivates you to go to work?
• Can you describe what makes you involved in your work?
• If the good fairy gave you three wishes that could improve your work motivation, what would they be?
• How do people interpret the various reasons for being motivated or demotivated?
• Do you remember a situation were you were very motivated?
• How would you describe the emotional experience in that situation?
• Do you remember a situation where you lost you involvement in the work? Can you describe the situation and your behaviour?
• Exactly, what happened when you lost your motivation?
• How would you describe the emotional experience in that situation?
• Who/what helped you in that situation?
128
3.4.3.4 Data processing
Interviews were recorded on a memory stick, a data device able to record sound files and transform them into the computer. From these files, a research assistant transcribed all interviews into full text. It was regarded as important to have some personal continuity throughout the transcription process. The transcription of the interviews was done after formulated rules for transcription (see Appendix D). For data analysis, the word document containing the full text of the interview was transformed into rich text format and coded with NVivo (Bazeley & Richards, 2000). NVivo is a data analysis program especially designed to code data from qualitative research projects. It is based on the principles of grounded theory (Glaser & Strauss, 1967) and is used in the present project as a help to organize data in the logic of phenomenological data analysis (Giorgi, 1985; Malterud, 1996; see description in Section 3.2.1). The program was used as structuring help and managing system for interview data (transcribed text). Reflection of the procedure of single research interviews Altogether, the interviews went well and brought various insights about the relationship between burnout and motivation in midwifery. Good contact (rapport) with the interview partners was established. A trusting atmosphere was established leading to openness in regard to the research question. In two interviews, the author had the impression that job position (leader) and union membership was responsible for a different perspective brought into the dialogue about the relationship between motivation and burnout. This is not understood as bias but rather as supplementing position. This observation makes obvious that role membership seems to have an important impact on the perspective to look upon the phenomena under investigation. All interviews had an explicitly subjective perspective regarding experiences, meanings, feelings, thoughts, and narratives were inquired about. The step-wise procedure of
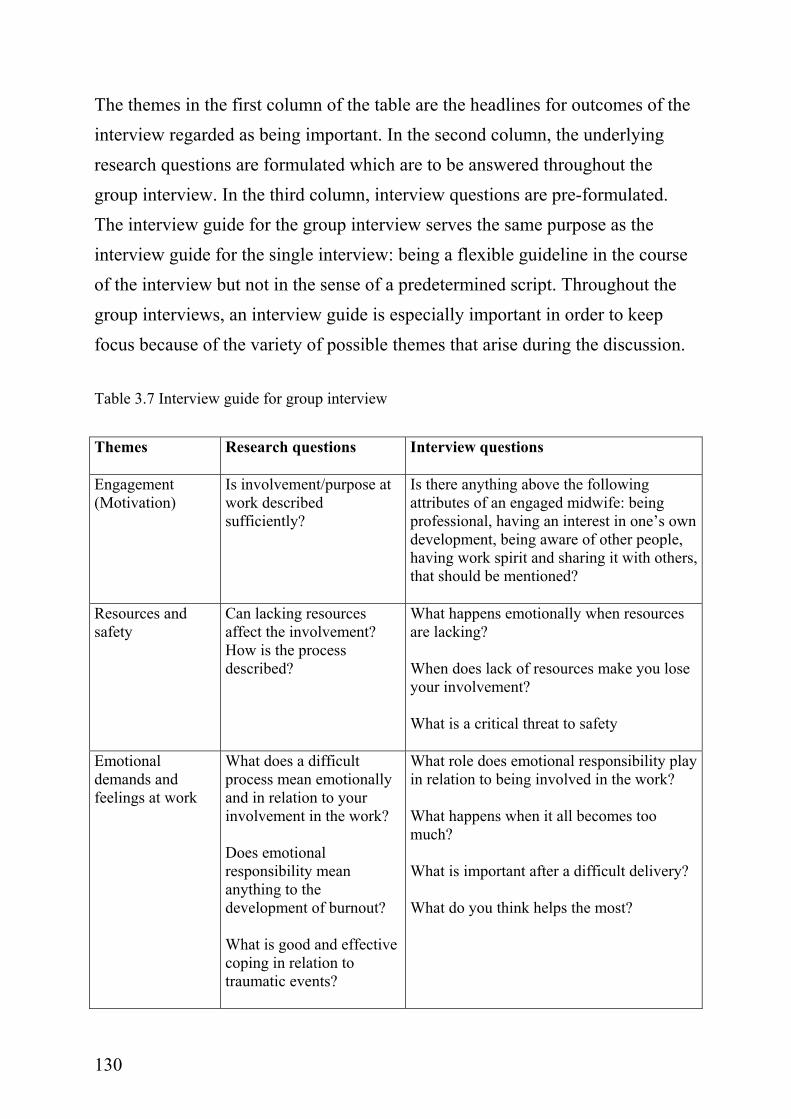
129
interviewing made reflection throughout the whole empirical process possible and led to enriched data in the course of the interviews.
3.4.4 Group interview
The third and last empirical part of the project was the group interview. The discussion during the group interview was recorded, transcribed, analysed, and reflected according to the same phenomenological procedure used for the single interviews. In Chapters 4-7, the results from the group interviews are used to validate findings from the single interviews.
3.4.4.1. Purpose
The purpose of the group interview is to check the results back with the members of the investigated group. Gobi & Lincoln (1985) refer to this procedure with the expression member check. The condensed information is taken back to the field and is discussed in the course of a group interview.
3.4.4.2. Description of procedure
All midwives at the ward were invited to take part in a group interview to discuss and interpret the findings from the single interviews. Aim of the group interview was to get affirmation or rejection of themes extracted from the single interviews was meant to play a role in explaining the relationship between motivation and burnout in midwifery. Further, new themes could be shared reaching beyond the aspects already mentioned in the single interviews.
Box 3.5 Member check For member check data, analytic categories, interpretations, and conclusions are ‘played back’ to the stake holding group from whom the data was collected. Member check is seen as the most crucial technique to establish credibility (Lincoln & Guba, 1985). Member check is also known as form of communicative validation of the material (Steinke, 2000).
130
The themes in the first column of the table are the headlines for outcomes of the interview regarded as being important. In the second column, the underlying research questions are formulated which are to be answered throughout the group interview. In the third column, interview questions are pre-formulated. The interview guide for the group interview serves the same purpose as the interview guide for the single interview: being a flexible guideline in the course of the interview but not in the sense of a predetermined script. Throughout the group interviews, an interview guide is especially important in order to keep focus because of the variety of possible themes that arise during the discussion. Table 3.7 Interview guide for group interview Themes Research questions Interview questions
Engagement (Motivation)
Is involvement/purpose at work described sufficiently?
Is there anything above the following attributes of an engaged midwife: being professional, having an interest in one’s own development, being aware of other people, having work spirit and sharing it with others, that should be mentioned?
Resources and safety
Can lacking resources affect the involvement? How is the process described?
What happens emotionally when resources are lacking? When does lack of resources make you lose your involvement? What is a critical threat to safety
Emotional demands and feelings at work
What does a difficult process mean emotionally and in relation to your involvement in the work? Does emotional responsibility mean anything to the development of burnout? What is good and effective coping in relation to traumatic events?
What role does emotional responsibility play in relation to being involved in the work? What happens when it all becomes too much? What is important after a difficult delivery? What do you think helps the most?
131
The group interview played the part of both giving and seeking information. Being designed as a way to member check the results from the single interviews, four pre-selected topics were discussed: definition of burnout, definition of engagement, the role of resources for the feeling of security on the job, and the work at the interface between life and death (traumatic birth incidences). The participants got first hand information about the outcome of the single interviews and were asked to supply new or supplementary information about the four topics. On the background of a recent restructuring of the ward other “burning” issues came up in the meantime which proved to be related to the role of resources in regard to felt security doing the job of a midwife. Besides the author, a research assistant was present for the course of the group discussion. She was instructed to make notes about the process and help with the technical aspects of recording. The same assistant transcribed the single interviews and was also responsible for the transcription of the group interview.
3.4.4.3 Participants
All midwives at the maternity ward who were contacted for the single interview were contacted again for the group interview. Both the midwives who already participated in a single interview and those who did not were welcome to participate in the group interview. A blending of new and old interview partners was wished for. A written invitation was sent to each of them with the possibility of choosing between two different days for participation. Selection criteria were not formulated in advance because it was expected that all who volunteered to participate would do so. On the answer sheet, the midwives were asked to give information about their age, job age, job position, and telephone number and address in order to be able to compose groups after the principle of most possible heterogeneity.
132
Description of the sample The interest in participating in a group discussion was disappointing. Eleven midwives showed interest in participating in a group interview. Five midwives could be scheduled on one of the two dates. Three of them had already participated in a single interview, two others had not. All came with a personal interest. The age range was between 41 and 51 years of age.
It is assumed that the low interest in participating in the group interview was due to a restructuring at the ward at the time when the group discussion was scheduled. Those who participated said that the motivation to participate was low, because many midwives felt that they were not being taken seriously enough throughout the re-structuring process at the ward and had given up being involved in extracurricular activities. They described themselves as being too tired to invest more time and effort into something not related to their daily work.
3.4.5.4 Data analysis
The group interview was read and analysed line by line using the programme NVivo. Interview parts were coded as free nodes. The third step of data analysis (condensation into abstract meaning units) was done on paper. Unlike the single interviews, the research questions formulated for the group interview were used as a filter for analysis. Free nodes were checked for redundancy and usability to answer the research question. Reflection on the group interview The goal of the group interview was fulfilled. Participants confirmed to a great extent the observations and greater meaning units extracted from the single interviews. The actual situation of organizational change (re-structuring of the ward) made it a challenge to keep focus throughout the interview. The midwives were thankful for a forum to exchange their opinions about these changes. Motivation and burnout were discussed again on the background of this

133
organizational change. The author kept the balance of letting conversation flow and keeping focus. A second group interview was not scheduled after the first because of saturation of knowledge. 3.5 Quality criteria used in the present study Quality standards for qualitative research are discussed in depth and with different positions (e.g. Malterud, 2001; Guba & Lincoln, 1985, 2000; Kvale, 1989, 1996; Seale, 1999; Steinke, 2000; Flick, 2002; Lamnek, 2005; see also Appendix E). In reference to quality standards published by Malterud (2001) and Mayring (2002, in Lamnek 2005), the quality of the present project was evaluated using the following quality criteria: (1) proximity to the subject matter, (2) reflexivity and metapositions, (3) triangulation, (4) validity, and (5) transferability. In the following sections, the five quality criteria are used to reflect on the research process of the present case study.
3.5.1 Proximity to the object of study
An essential difference between quantitative and qualitative methodology is the distance to the research participant. Qualitative methods are proximal methods, investigating a phenomenon in the natural setting. The aim is a relative high proximity to the object of study; here a midwife at work, fulfilling her primary task. It is taken into account that controllability in the natural setting is rather low. Instead, it is important to establish trustworthiness (Law et al., 1998) in order to ensure better quality of the study findings. In the present case investigation, proximity to the subject matter was realized through participant observation at the ward as well as in-depth interviews with both single midwives and a group of midwives. The proximity was furthered through an open interview format, letting the midwives guide the conversation within the framework given by the author. In regard to establishing trustworthiness, this is valued as essential and important. In fact, one of the
134
closing comments after the group interview referred to the trusting atmosphere established by the researcher, which made it possible to discuss critical aspects of work at the ward. Beyond that, the phase of participant observation as the first step within the case study had a very positive effect for the researcher’s overall understanding of midwifery in Denmark. This was useful knowledge in the single interviews and was positively recognized by the participants through single comments about the author’s knowledge of the subject matter (here midwifery) expressed in language.
3.5.2 Reflexivity
The second criterion focuses on the reflection of the position as a researcher in the research process. The researcher in qualitative studies plays an important role. In Section 3.3.3.4, the importance of reflecting on the fore-understanding before starting a research investigation is discussed. Malterud (2001, p. 484) refers to this term with the metaphor of the “knower’s mirror”, relating to the process of reflecting on each step in the research process in regard to the researchers own position; the preconceptions brought into the project, and the metapositions established in order to keep a balanced position as observer. This second aspect is the reflection of knowledge gathered through qualitative investigation from an archimedical point of view (Brucks, 1998, p. 12). Malterud (2001) describes this position as metaposition, creating an adequate distance from the study setting engaged in. The research has to be focussed and reflective about the course of the dialogue from a distanced perspective, being observer of the self and other. In summary, reflexivity refers to the thorough documentation of the whole research process from the researcher’s role to the clear documentation of the research process. This is even more important when procedures are used which have not been documented before. Steinke (2000) recommends the use of
135
codified methods in order to make the methodological choice more transparent and comparable to other investigations. In the present case study, different approaches to achieve reflexivity are chosen. First of all, the author’s fore-understanding was reflected on before entering the field and at different points in the process using a personal logbook. The logbook serves both as a diary where personal experience and unexpected issues are documented as well as in the real sense of a logbook, which is to document any step throughout the research process. Metapositions were established through discussion of study outcomes in three different research settings6 as well as in collegial exchange7.
3.5.3 Triangulation
In order to establish credibility of the investigation, methods of triangulation are recommended (Lincoln & Guba, 1985; Law et al., 1998; Denzin & Lincoln, 2000; Steinke, 2000). Triangulation furthers to the dependability of an investigation by using different methods, theories, or researchers in one investigation. Formerly thought of as establishing validity, triangulation now is regarded as a quality standard in its own right (Flick, 2002), heightening the depth, breadth, and consequences of the methodological procedure. In the context of the present case study, triangulation was applied by using different methods of investigating the phenomenon. The methods were applied
6 The research circle at the University of Hamburg (PD Ursula Brucks), the research circle at the National Institute of Occupational Health (NIOH) and the research circle at Technical University of Denmark (DTU), Copenhagen. 7 With my colleague Marianne Borritz (PUMA) and the members of the Qualitative Network at the NIOH (Danish: Kvalinetværk). Further, an unplanned reflection happened through discussion of the material with the scientific assistant Sofi LaCour Mosegaard who transcribed the interviews and was present throughout the group interview. Unintended as so far as it was not planned beforehand but it yielded interesting information, e.g. about the point of saturation.
136
in stages, starting with observation and followed by single interviews, which were member checked in a group interview as a last step. Triangulation of perspectives onto the research field was reached through discussion with colleagues, continuous literature work, and finally through writing. These different modes of reflection forced the author to adjust the frame of the present project at different points. Both forms of triangulation are meant to lead to a higher credibility of outcomes from the case study.
3.5.4 Validity
Communicative validation can be established through prolonged engagement and persistent observation, triangulation, peer debriefing, negative case analysis, and member check. In the present project, communicative validation was realized by designing the group interview in the form of a member check (Lincoln & Guba, 1985; Steinke, 2000; see Box 3.5). Interpretations made on the basis of single interviews were taken back to the participants for discussion in the group interview. The participants of the group interview were invited to make comments about the interpretation of results from the single interviews. The member check also served as a proof of authenticity of the findings.
3.5.5 Transferability
Transferability of results is important in regard to external validity. External validity refers to the question of what contexts the findings can be applied in (Malterud, 2001). A prominent aim of research is to reach insights which can be shared beyond the specific setting of the study. To what degree this might be possible should be reflected on thoroughly. An important aspect related to transferability is the way sampling is done. In qualitative research, it is common
137
to use purposeful or theoretical sampling. By taking this path, it is possible to further transferability. In the present study, one case (a maternity ward of a community hospital on Zealand, Denmark) was investigated in depth, using various methodological approaches. The results gathered by investigating the described case can be transferred to midwifery in general. In a personal conversation with a German midwife, it became clear to the author to what degree outcomes of the present case study are relevant for midwives with a culturally different background. Parts of the results are bound in context and as such specific, e.g. structure of the ward as a midwife center, role of the midwife (differences between countries). Other outcomes, e.g. primary task, demands from modern parents, security and uncontrollability and the role of traumatic birth incidences, can be transferred to other groups of midwives. The procedure of purposeful sampling led to heterogeneity within the group of participants. Nevertheless, the investigated group showed a small range of biological and job age. Altogether, transferability is valued as being high for all of the findings of the case study.

138
Part II: Introduction of the result chapters (4-7)
The aim of the present case study investigating the research question of “How to understand the relationship between motivation and burnout in human service work - midwifery as case” was (1) to reach an understanding of the high score of burnout amongst midwives in the PUMA study, and (2) to gain insights into the relationship between motivation and burnout in midwifery in Denmark. The pre-structured but open format of the interviews led to a web of knowledge spun around the research question. The explorative approach yielded valuable insights into the relationship between motivation and burnout in midwifery. In the course of data analysis using the phenomenological method as described in Chapter 3 different themes emerged. The following four chapters cover the presentation of findings referring to these themes. The information gathered stays foremost on a descriptive level. Original citations from the interviews are used to illustrate the insights found throughout the interviews. For better legibility the original citations were translated into English by two Danish colleagues and double checked by the author of this thesis. Four different themes represent the main findings from the single interviews and the group interview and are regarded as being of peculiar interest for understanding the relationship between motivation and burnout in human service work. The findings are separately outlined in the following four chapters (Chapters 4-7) of the result section. Chapter 4 summarizes the subjective definitions of motivation and burnout in midwifery in order to set up the frame of how the concepts of motivation and burnout and their relationship are understood by the participating midwives. In chapter 5 person-related and work-related factors named by the participating midwives as being important for the relationship between motivation and burnout are summarized. Chapter 6 discusses the role of resources in an insecure setting. The discussion about resources was given particular emphasis from the participating midwives’ side.
139
Finally, chapter 7 is outlining the reflections of the participating midwives about the role of emotional demands and feelings in midwifery. An integration of these findings with pre-existing knowledge and theory referred to as explicated fore-understanding of the author (see Chapter 2) follows in Chapter 8.
140
Chapter 4: Engagement and burnout in midwifery 4.1 Introduction The present project aims to investigate the relationship between two single phenomena: motivation and burnout. In the light of a phenomenological understanding, the interviewees were asked about their subjective understanding of each single phenomenon, relating to their personal experience in job situations. The interpretive nature of the chosen approach aims to understand the essence of the phenomena. Accordingly, statements about cause and effect cannot be made on the basis of the narratives from the interviews because participants do not distinguish between the two.
4.2 Reactions to the results of the PUMA study At the beginning of each interview, participants were asked about their first reaction to the high burnout score found in the baseline investigation of the PUMA study. Overall, a wide range of different explanations were given which reached from understanding, to doubt, astonishment, and disbelief. Altogether, participants were eager to find examples and external reasons for the devastating results.
Interview 2: 46 years old, 20 years work experience as midwife The PUMA report was made right after the electronic journal system had been introduced. ……. Yes, and when an entire ward introduces such a new product at the same time, it is something that is really hard. The preparations were fine, they had provided good training, but they had not given us enough support during the implementation of the system. There was money for new computers but there wasn’t any money for computer work stations. And we also have a couple of employees on long-term sick leave. That has made a great impression on me that an apparently healthy, young woman among us suddenly got it as bad as she did.
As learned from the preceding quote, some of the explanations given were quite simple and at the same time astonishing: e.g., the first round of the PUMA investigation took place at the same time as the electronic journal was
141
introduced at the ward. The introduction of the electronic journal was accompanied with a number of problems such as computer systems that did not run which led to some frustration among the midwives. Following along with these structural changes, the ward was affected by some serious long term sickness absences. Altogether the work morale at the time the baseline investigation took place was rather low. As another aspect, bad working conditions were named which were made responsible for the high burnout score.
Interview 1: 38 years old, 14 years work experience as midwife Well, I think the same. I believe I think the same. But it does not surprise me. It does not surprise me. This is of course because I do the job every day and I think it is an unbelievably demanding job for unbelievably low pay under unbelievably bad working conditions. Interview 3: 43 years old, 6 years work experience as midwife And then I thought it was a shame if many people thought it was a phenomenon in our field. But then I turned it around and said that it is a trade where you give much. You give yourself all the time. You can not come to work and say you have a bad day. Interview 8: 50 years old, 24 years work experience as midwife But I think the PUMA report must be published as we have some managerial problems.
The conditions described refer to the whole range of dimensions to estimate the quality of work: job demands, reward and recognition, job conditions, emotional demands, leadership quality. The three statements above show the variety of reasons given by the participating midwives. Taking a single condition as cause of burnout in midwifery is exaggerating the meaning of the single condition named. Nevertheless, the variety of reasons named is interesting to note. In the first interview excerpt, high work demands, paired with low financial reward and at the same time bad working conditions are made responsible for the high burnout score in the PUMA baseline study. The second statement refers to one aspect in midwifery which is referred to as a cause of burnout: the demand to
142
give something of one self. In the last interview quote, leadership problems are meant to be the reason for high burnout.
Interview 4: 45 years old, 20 years work experience as midwife No- I was also alarmed to hear that our field did so badly. This I have to say, I was very alarmed about it.
Some of the participating midwives stated they were surprised at the results from the PUMA study. They stated that they were alarmed and startled about the devastating outcome.
Interview 7: 48 years old, 12 years work experience as midwife I was a little surprised that it was so extreme, but I can certainly understand why you burn out. It is partly the nightshift and the irregular shifts, and I understand that you get very involved in your work. You familiarize yourself with the work in another way than I did at the time I was working in a kindergarten. You work with children, it is an important job, of course it is. But I have never, and that is why I keep my job, I think it is exciting, and it is not a shallow job where you just go home from work and that was that. You keep working and you think about if it was right or wrong. It is wonderful, but I can also understand those who burn out as they are so involved. You can’t just go home and say that was it. I really understand. If you are not good at working with things afterwards and get through it, become scared, then I can absolutely understand that you burn out. Interview 9: 44 years old, 18 years work experience as midwife Yes, in a way I was surprised, as you always use yourself as reference, and I could feel that some things became more and more difficult. You can still handle it, but I didn’t think that they were so burned out. No, that surprised me. Another thing which surprised me was that the night shifts – well you can feel on your own body – is so hard on you. But that it is so dangerous ….
The midwives who said they were surprised at the outcome try to make sense of the findings by looking for suitable explanations. Again, the participating midwives name clearly the different conditions in the job which are meant to cause burnout. The reaction of surprise and striving to find meaning in the results of the PUMA investigation can also be interpreted in the light of a healthy worker effect: only those midwives who are still on the job are asked about their understanding in regard to the phenomena of motivation and burnout. It is reasonable that these midwives have not necessarily experienced burnout or even just a decline in motivation themselves and therefore are surprised about
143
the devastating result from PUMA baseline study. There are also other reasons one can imagine which could be made responsible for this: maybe they are the most successful suppressing any sign of burnout and the symptoms of it, or they are those with the most support at home. Besides the total understanding and the surprise mentioned by the midwives in regard to the outcome of the PUMA study, one midwife analysed the outcome of the PUMA study from the perspective of disbelief.
Interview 6: 58 years old, 33 years work experience as midwife Well, first I was a little surprised, that I must say, but if you scrutinize the questions given to the midwives and the answers they gave, then there are some notes and differences which show it may not be that bad if you analyse it. I think that the things presented and focused on in the newspapers give a very crude picture but there are differences. There really are. So when I close-read the text and the questions again I’m not surprised at all – I’m really not surprised. … No, I don’t think they are burned out. I don’t. Much of it is just talk; we call it washroom talk – right? Oh yes, she is right etc, etc. We have tried to do something about it. We have thought, we listen and focus on it and when you start a debate it is not that bad. … Given up. You will not find that here. The midwives are willing to fight for things, e.g. a minor procedural thing. No, hell no, we shall not, we should work for things to become as we want them to be because that is what we think is the best. Maybe we’re not always right and then we must surrender at some point but we will fight. So in that way we are not burned out, we do not give up and mess about. We really fight. And again, I think we have had some successes in our lives which make us prepared to fight. So what has been written is not true, I think, that we are not burned out.
The reaction of this particular midwife can be interpreted as methodological critique from a lay perspective. From her understanding of the cause, the questions asked in PUMA and the interpretation drawn from these questions do not stand in any relation to each other. She also points out the fact that all the positive aspects of job engagement and motivation to do the hard work of a midwife are not shown in the PUMA study.
144
One interview participant referred to the public discussion of the PUMA results.
Interview 1: 38 years old, 14 years work experience as midwife You said something about how I thought the results from the PUMA report had led to some changes or how it had been received…..on the other hand, I think that the report has been poorly recognised by society. Not from the researcher’s side but by the general population and the press. Midwives always complain and they are not willing to make an effort in relation to the woman in labour. Midwives only want the women to suffer and be in pain so why is it that you have to feel sorry for the midwives. That is why I think the report has been received negatively in public.
The devastating outcome of PUMA was discussed in the media. In this discussion, midwives were accused of being self-centred in the sense of following a job ideology which is not beneficial for the ones giving birth. The public reputation of midwives emerged as having a negative connotation. From the midwives perspective, this discussion was experienced as not fair and also unexpected. Such a picture stands in deep contrast to the common vision of ideal practice (Hunter, 2005) shared by the midwives themselves. Two comments referred to the activities and initiatives started after the PUMA baseline study to improve the situation. There was, for example, an externally moderated meeting with all midwives to discuss the implications of the PUMA investigation. Workgroups were established to make plans for improvement, e.g. the shift planning.
Interview 6: 58 years old, 33 years work experience as midwife We have the results and we have discussed them, right. But we have also held many meetings about the psychological work environment, what we can do better etc. And …. no , it has not become better.
Interview 8: 50 years old, 24 years work experience as midwife We have spent so much money on this PUMA project and got no results.
The results of the PUMA study were not directly addressed by these interviewees. Frustration was given voice concerning the intervention process after the results of the PUMA baseline study had been published. Even though there had been some effort put into investigating the psycho-social work environment, according to these midwives, no change had happened.
145
4.3. Subjective descriptions of burnout Participants were asked about their personal understanding and meaning of burnout and if they could report any personal experience of burnout. The participants, describing states of physical, emotional and behavioural indisposition, use the expression burnout in a rather broad sense. Most of the descriptions refer to examples of everyday behaviour, like complaining a lot, choosing the easy work tasks, and being slow in reacting to clients’ needs. Burnout is often used as everyday description of “being fed up”. There are hardly any descriptions about own experiences with burnout which might be interpreted as a sign for either high social desirability or a healthy worker effect again. It is plausible that those midwives committed to take part in an interview are not at the edge to burnout but alert about and interested in it. In the following three sections, the results of the responses to subjective understanding of burnout are structured along the following themes found in the interviews: work related burnout, emotions related to burnout, and behavioural aspects of burnout.
4.3.1 Work-related burnout
Work-related burnout is understood as burnout caused by the work related conditions as for example high demands and low resources. Work-related burnout is referred to when an imbalance occurs between resources, work demands, reward and responsibility.
Interview 4: 45 years old, 20 years work experience as midwife That it what makes the work so great, you can’t get it any better. We work too many hours, the wage is poor, our families suffer but it is still a great job. I think it is these three things which are the reasons for the negative evaluation. You slog away; you totally involve yourself every day, 8 hours, 10 hours, 24 hours per day. You work Christmas Eve, you work during the Easter holiday and you work during the summer holiday. Maybe you have two weeks holiday with your children even though they have 8 weeks and you get lousy pay. Many of the young midwives won’t put up with it. They find other jobs.
146
Interview 5: 49 years old, 8 years work experience as midwife If you ask me…. No I’m not burned out, but I know the reason why. Working 8 hours per day and getting a good night’s sleep are extremely important. I remember how it was to be on a night shift. Just the thought of it makes me sick, really.
First, the work conditions are accused of causing burnout. The job of the midwife is described as fantastic in regard to the primary task but at the same time, the conditions under which the job has to be accomplished are described as problematic. Hence, there is a felt imbalance between the pleasure connected to carrying out the primary task and the problems faced while fulfilling the primary task. The primary task is regarded as the energizing factor, but the conditions are experienced as being draining. Especially work-family balance and working conditions in regard to time (shift work and work at night) are named as critical factors. These aspects are further referred to in Chapter 5. Another work-related aspect of burnout is seen in missing recognition (being heard) from the leadership.
Interview 1: 38 years old, 14 years work experience as midwife Not being heard when you complain to the management. Not being heard, not being taken seriously, nobody takes care of you. Showing care for the employees - if it is not part of one’s everyday then you burn out. …. And then there is the work conditions and also the wage. It is sad to say, but it is of some kind of importance (laughing).
Recognition from the leadership is expressed as being important. The responsibility of the leaders is seen in taking care of the problems and daily hassles of the job. In the case of missing care for the personnel, burnout is named as possible outcome. Reward is referred to as financial reward; as getting adequate pay for the responsibility taken when doing the core job. The participating midwives experience an imbalance between their own effort put into fulfilling the task and the reward they get out of it. Reward and recognition, resources, job demands, and responsibility are understood as being connected with each other. Keeping equilibrium between
147
them is regarded as important for staying motivated while doing the demanding job of a midwife.
4.3.2 Emotions related to burnout
In the following section, emotions which are related to burnout are described by the participating midwives: loss of work spirit, loss of volitional control over emotions, and fear as reaction to traumatic birth incidences.
Interview 6: 58 years old, 33 years work experience as midwife But if you have trouble getting dressed and going to work, meeting your colleagues, meeting the women you assisted during delivery the day before, then you are burned out. When you don’t feel like going to work. Interview 1: 38 years old, 13 years work experience as midwife Maybe you have lost interest in providing service, which in this case, is helping women during delivery. … Lost strength of mind in using yourself in the way you use yourself during a delivery. You really don’t feel like doing it. Maybe you think there have been too few wonderful experiences and you just feel more and more used.
The interviewees referred to the loss of spirit, interest, and pleasure in carrying out the primary task of a midwife. This state of feeling demotivated finds expression on a behavioural level in low energy to get started. It is explained by the fact that midwives give a lot and are used by their clients continuously and in different ways. The state of having lost the readiness to give something of one’s self is associated with burnout because this readiness to give is seen as part of the primary task (job inherent demand) in midwifery.
The second sign for emotional burnout is described as the loss of volitional control over emotions.
Interview 2: 46 years old, 20 years work experience as midwife And then ….. I have felt that way, and I know of others who have worked here and felt the same way – that you are instable. Cry easily, become distressed and can’t handle the fast shifts which we usually handle quite well. It is like you finish a delivery and then there are two more so what do we do now. Normally, we would all be able to say that the paper work should wait but you become
148
very pertinacious and say that you must finish the paper work before you can take on a new assignment, you can’t have it all in your head.
In regard to volitional control over emotions, overly high emotional sensitivity and instability is described as signs of burnout. When the borderline to emotional overcharge is lower than it used to be and emotional expressions (especially tears) are no longer under control, emotional burnout is seen by the midwives to be close at hand. Being able to react to job demands flexibly is described as declining alongside diminishing job stress tolerance because of ebbing resources. As soon as a state of overstrain is reached, extra demands cannot be accomplished as they once had been before. Losing the control over one’s own emotionality is seen as a sign of weakness. It is not seen as normal to break down because the work situation is busy. The usual readiness to go on with the work that needs to be done first is described as having disappeared. The ability to handle a busy job situation has changed into a more restricted behaviour pattern, which is no longer flexible. A last aspect described which might be a reason for emotional burnout is the inevitable condition of being confronted with uncontrollable exposure to traumatic incidences.
Interview 7: 48 years old, 12 years work experience as midwife to the question of reactions to traumatic incidences And I can see that some of my colleagues are tired out because of such processes where they have really been there and felt so sorry afterwards that they have reported sick. It is difficult to get on with other deliveries, being scared. Clearly afraid that it could happen again and what could then happen.
An emotionally demanding job situation is described as being a possible reason for absence from work. Not being able to cope with the emotionally straining situation is thought to lead to job related fear and further to the inability to carry out the primary task. Fear is described as the emotion related to traumatic incidences which could not be handled in a different way.
149
The emotions and emotional reactions described in the foregoing section are interpreted by the interviewees as signs of burnout. They are described as reactions to work conditions and unchangeable conditions (such as the possible exposure to traumatic incidences) in midwifery, which are experienced as demanding. Emotional demands in midwifery appeared to be a main theme in the single interviews, which was also confirmed in the group interview. Therefore, emotional demands in midwifery are discussed in depth in Chapter 7.
4.3.3 Behavioural aspects of burnout
As mentioned above, burnout is used as a broad reference category for different descriptions of work behaviour. Low client service, risk avoidance, and constant complaints are referred to by the midwives as behavioural aspects of burnout.
Interview 1: 38 years old, 14 years work experience as midwife I was tired and not very easy to get on with. Yes, you are not really easy to get on with, neither the one place nor the other. And you also partly lose your feeling of responsibility to be part of a greater system, and that things shall work together, don’t you?! … you distance yourself from everything and you don’t care to participate. … you serve on a minimal level. … but we have some who are a little slow to rise from their seat (laughing), as we say. It could also be a different style of working. It could be all kinds of things, that is difficult to know.
Low client service finds its expression in different aspects described by the participating midwives: tiredness, losing the sense of responsibility, serving at a minimum level. The behavioural metaphor used to describe this state is the promptness of getting off the chair when a client asks for help or a new client needs to be greeted.
Interview 4: 45 years old, 20 years work experience as midwife When a person who is burned out comes through the door it’s like ahhhhh. Sits down, looks at the whiteboard and says “God there is so much to do today, I’m tired, I’m exhausted, can’t I get something easy to do?”.
150
A burned out person is described as someone for whom any demand seems to be too much. Easy tasks are chosen and a distanced position to one’s work and the clients is taken. There is no sign of community and team spirit left. A burned out midwife cares for herself, not for others. This last aspect is also described in the following section:
Interview 5: 49 years old, 8 years work experience as midwife But a person who is burned out can behave in many different ways, but an example could be when we report to each other and you can see there is an easy delivery then there is another delivery which you can see can take all evening and it is pathologic and so many other things then the colleague will always choose the easy one. Or she starts with saying she is so tired and doesn’t have the strength to do it. That must be being burned out. And it can actually pass on to the colleagues as you may be a bit irritated if a colleague always avoids the difficult tasks and takes the easy way. It is okay for a while, but if it lasts for a long period then it affects the colleagues, I think. Personally I get irritated, it also affects others.
In the citation above, risk avoidance behaviour as sign of burnout is described. Colleagues, who show signs of burnout, are described as having the tendency to avoid any risk related to the core job. They always choose the easy tasks. At any possible time, excuses are found for not being able to take one of the more complicated cases. Another similar behaviour is the tendency to close the door to the delivery room and stay there no matter how busy everybody else at the ward is. Colleagues who behave like that are not much appreciated at the ward. The strong focus on the self describes the opposite of one reported aspect of engagement: the care for others (see Section 4.4.3). The following citation refers to constant complaints as sign for burnout.
Interview 3: 43 years old, 6 years work experience as midwife I would say that it is a colleague who comes in and is a bit sad and isn’t motivated, and while we sit and patients are handed over at shift change, so it is her to always complain about how exhausted she is. Some complain more than others. Some always complain. There are always some who complain. Then there is something wrong with the planning of who is on duty, and then they haven’t done enough to please us. Do you know the type, who must complain all the time?
151
Further, constant complaints were named as another behavioural sign of burnout. Colleagues contaminating the atmosphere by complaining about everything and everybody without taking the initiative to change things are experienced as irritating by the remaining midwives. Colleagues who constantly complain build a negative atmosphere and this kind of behaviour is experienced as being destructive for a good and equal relationship. An exaggerated feeling of responsibility is described as cause for burnout. Here it is assumed that a person who is overly committed at work will end up in an overly exaggerated work behaviour which later will end in a feeling of exhaustion.
Interview 2: 46 years old, 20 years work experience as midwife My experience is that those who break down easily are often those who feel a high degree of responsibility. They take on more than they should. They sometimes take on the responsibility for what others have done in the delivery room. Like if I had done something different my colleagues would also have done it differently. It is the colleagues with the highest sense of responsibility who break down.
The person meant to be prone to burn out is the one who feels responsible not only for things she has done herself but also for the actions of others. The rumination about what could have been done to make a difference can lead to a breakdown because some of the aspects are beyond one’s own control.
Group interview IP2: I think it affects the basic burnout if you resign totally if you put on blinkers and only concentrate on your own little square and withdraw from everything. Maybe the burnout isn’t so obvious for the others, but you mind your own things and go home as soon as possible. I think this frustration makes you less committed. The thing that is lacking is so massive that you just give up. That is how I see it on the outside IP4: No, it should be a right, as we talked about before, to be the one who is burned out. To be she who withdraws and says she will only have the normal situations afterwards. And I’m a little afraid that we are exposed to such situations at the moment, and then you know that you will be very busy on the next day’s shift, you must be there, and be busy for 8 or 12 hours depending on your shift. It is unfair and impossible.
152
The findings from the group interview support the results from the single interviews. In the group discussion, burnout was associated with resignation and seclusion on the one side. Beyond this negative behavioural aspect and supplementary to what was found in the single interviews, burnout is further described as an adaptive behaviour, understood as a coping mechanism when demands go too far.
Group interview IP 3: That is the reason why they frown on a midwife who always cries off and the other midwives can see that the patient is not cared for properly. In general, that is not accepted in the group. This lack of acceptance comes out in many ways, it is deeply rooted in us that we can’t accept that.
Further, the participating midwives discussed work behaviour described as “only taking the easy things”. Colleagues who do not take on their share at the ward are not accepted. As soon as a client has to bear the negative consequences of a midwife not being engaged enough to do her job in a responsible manner, the remaining group expresses displeasure about that kind of behaviour. 4.4 Subjective descriptions of engagement at work Participants in the present case study were first asked to describe a colleague who is highly engaged. Second, they were asked to describe a job situation where they remember having been engaged in a particular way. At this point it is interesting to note when participants refer to being engaged in the job, they refer to engagement which is not related to the primary task but to activities to organize work (e.g. union activities, education of young colleagues). The descriptions of work-related engagement are summarized in a triad of: professional self, work spirit, and care for others.
4.4.1 Professional self as sign of engagement
The first aspect of engagement, called ‘professional self’, describes the professional knowledge and the professional role a person brings to the field and
153
carries out. In other words: the midwives described a person being engaged as one who knows what to do and likes to share her knowledge with others.
Interview 3: 43 years old, 6 years work experience as midwife One you can look up to and use as a confidante. You can say you feel you can go to her if you have something to ask about. It shouldn’t be that you think: oh no I can’t ask her either because she probably doesn’t know and some people are more insecure than others, or because you think she thinks badly about you if there is something you don’t know.
A person who is engaged at work was described as one who has a lot of professional knowledge and a high professional work ethic. It is one who can be asked in cases of insecurity and questions. She can be trusted since she signals openness and is ready to hand her knowledge on to others. In this sense, she is described as one you can have confidence in. She is active in the acquisition of knowledge and shares this knowledge eagerly. It is a person of respect, one you can look up to.
Interview 1: 38 years old, 13 years work experience as midwife And at the same time she is full of initiative in relation to that there…that way there is development all the time, so you don’t stagnate.
She is interested in all kinds of developmental activities in order to learn more about best practice in the job. She invests time and effort into extracurricular activities in order to stay updated in her profession. An engaged midwife is described as proactive in seeking new information.
4.4.2 Work spirit as a sign of engagement
Work spirit is the second aspect named as part of a person’s engagement. Work spirit refers to the climate experienced which is created by a person.
Interview 5: 49 years old, 8 years work experience as midwife She is positive, she is dynamic and she radiates energy. She never complains (laughs). Well yes, she can do that. No, well it depends…. No she never complains, she gives constructive criticism and a lot of criticism but it is different from complaining.
154
A person who is engaged is described as one who has a positive work spirit expressed through being the pacemaker for others, especially in situations where work morale is low and frustration spreads. She radiates energy and keeps the spirit up at the ward. She is ready to do whatever needs to be done. She is not a complainer as described in Section 4.3.3. She expresses negative critique, but at the same time also constructive critique. In this respect, she is regarded as critical but positive, handing energy on to others by giving feedback in a polite and helpful way.
Interview 7: 48 years old, 12 years work experience as midwife But she is that type who wants to do it all when you come with the report in the morning. What shall I do and I’ll do it now. Sometimes she leaves the meeting before it is finished just to go and relieve one of the other midwives. She is also involved in many other activities at the maternity ward. She is what I call really involved; positive in her work. Always speaks positively about her work and colleagues. She lives for her work.
She is seen as a source of inspiration for herself and others. She has a positive attitude towards her work and is happy for the things she is doing. The love of the job she is doing is expressed through the passion with which she fulfils her daily tasks. In addition to the normal tasks of a midwife, she is also engaged in other job-related but voluntary activities at the ward.
Interview 2: 46 years old, 20 years work experience as midwife When you are involved …. then …… you radiate joy of being in a work situation. You take on the tasks that appear, you don’t refuse any of them. Such persons are happy and have energy when they leave their work. They …. When it has been a busy shift and there seem to be more clients than we can handle then such girls smile and say we must make the best of it. Other colleagues sit down and ask what to do. It can be an unorganised as well as a much organised person. It has nothing to do with that. They are good at involving the others. They spot when their colleagues are having a bad day and help them. They immediately stand up to receive and say hello to a new client, whereas the others remain sitting when they say hello. It is important to me that you stand up and say hello when they arrive at the ward.
A midwife who is engaged in her job is described as being the motor for colleagues, triggering good spirit and active engagement. She is cheerful even when the work piles up and looks for good solutions with restricted resources instead of complaining and mourning about it. Any task is good enough to be
155
done. The pleasure of doing the work stands in the centre of the description above: pleasure to serve, pleasure to give, pleasure to make the impossible possible. It puts some emphasis on the fact that this kind of behaviour is independent of being a neat or a disorderly person.
Interview 6: 58 years old, 33 years work experience as midwife An engaged midwife is one who has the spirit to lead the pregnant women through a long process. The short process is nothing. But in the morning she knows that this special delivery will be tough. But she does it with an open mind, and she says “I’ll do it, I’ll go into that woman and I’ll handle it”. She will also deal with all the other things to follow up upon. At the same time there are offers to participate in various obstetric groups, shift planning etc. and she signs up for what she finds interesting. She has the energy to do that. She has four kids at home and a husband who travels etc.. That is what I call being involved and enthusiastic. That is a midwife who enjoys it, and she has the ability to accomplish it. There are many of such midwives, especially here.
Spirit and pleasure are also at the centre of the last citation. Pleasure in fulfilling the job no matter how demanding or challenging a birthing situation might be is named as a sign of engagement. Further, an engaged midwife is described as a superwoman, being able to handle the primary task, extracurricular engagement in work groups, family and home. Moreover, enthusiasm about the work one is doing is named as sign for engagement.
4.4.3 Care for others and one’s self as a sign of engagement
The third aspect of engagement relates to proactive work behaviour and a form of intrinsic motivation. The descriptions of an engaged person in regard to especially this aspect are read as painting an ideal picture of a colleague.
Interview 9: 44 years old, 18 years work experience as midwife But engaged in a way which means to be happy also; so you do something for the good fellowship. At 4 am you say we need a quarters break, make some coffee or tea and toast so we can relax. Then you get new energy to think about other people.
A person who is engaged is described as one taking care of others. This is not only true for clients but also for colleagues. She has an eye on everybody being on the shift that needs to be taken care of. Even if things are running fast, a
156
person who is engaged finds the resources to take care of the group spirit. She promotes a sense of community in order to get over hard periods during a workday.
Interview 2: 46 years old, 20 years work experience as midwife It is those who answer telephone calls very calmly. Take the time to listen to what the caller says. She finishes the call in a proper manner. The engaged colleagues also see to it that their tasks are accomplished; nothing is left in a mess.
She is service-minded and client-oriented in her work, which can be noticed in her quick, calm and patient reaction towards clients. Last but not least, she is seen as one who brings her things to a close. Nothing is left to others to clean up after her. In summary, a midwife who is engaged is sensitive to the needs of others and herself.
Interview 8: 50 years old, 24 years work experience as midwife She is not the one to remain seated for the report. She is the one who says: she’ll take that one and who will you take. She is very aware of the woman in labour. She doesn’t necessarily spend all her time in the delivery room as such a colleague who closes the door and only cares for the woman while the rest of us run around - can be a problem. It is a person who finds the golden middle, who helps you with the paper work, replaces you if you haven’t had time for lunch or asks if she should fill in if you have a woman in labour to be with.
Further, an engaged midwife is described as being fast, standing up from the chair when a client is at the door. The opposite behaviour – not getting off the chair - was addressed when describing a person with signs of burnout. The immediacy of reaction to client demands is reflected as a sign of engagement and the absence of it as sign of burnout. In relation to the aspect of to what extent a person is service-minded; burnout and engagement are described by the midwives to be the ends of the same continuum. In the case of burnout, service-mindedness is meant to be secondary to self-centred focus of attention (e.g. complaining about low resources, only caring about the most necessary things). The person being burned out is busy with dealing with the condition of being in a bad mood and has not much energy left to take care for others. Engagement, on the other end of the continuum, is described as the immediate reaction to client demands.
157
In the group interview, the aspect of professional self was mentioned in particular:
Group interview, IP 2 A midwife is not engaged unless she enjoys working with childbirths. So it lies implicitly in her job that her engagement is the primary thing in the job. It is obvious that the clients are welcome and nice to work with and of course she enjoys working with them if she is engaged in her job. The first to feel if she is engaged is the customer. If she is not engaged, then she can’t work with childbirths. She can’t do the work if she doesn’t enjoy being with people in the delivery room. It is the prospect of a successful delivery that motivates her. To use some talents and get a good result.
Engagement was defined as a necessary precondition of the profession. Without being engaged it would not be possible to bear the hassles of the job and be a good help to the pregnant women throughout giving birth. The citation from the group interview, above, is a good example of the understanding midwives have of their defining engagement as an external demand in order to be able to fulfil the job sufficiently. In the context of the present project, engagement is also defined as part of the professional work ethic of this particular job group. The core task of helping to give birth is described as the source of being engaged. From a midwife’s perspective, the invariable conditions of the work are seen as part of the core job and experienced as a positive challenge and are seen as reasons for burnout at the same time. How these two aspects are seen to be related to each other is discussed in the next section. 4.5 The relationship between engagement and burnout In this last section of the chapter, the question of at what point engagement at work is lost is reflected on the background of selected statements from both the single interviews and the group interview. In the single interviews, the participants were asked about incidents and experiences of losing engagement at work. Out of the many comments on this question, two longer statements have been selected. These two statements illustrate in a comprehensive way the variety of reasons which purportedly cause declining engagement and support the development of burnout. The statements are regarded as being representative
158
of how the relationship between engagement and burnout is interpreted by the participating midwives.
Interview 2: 46 years old, 20 years work experience as midwife …. It could be something job-related that makes you lose the motivation. But it can also be personal. It could be something at home. We have seen colleagues in menopause, where the body changes, become a different person from what she usually is. The children leave home and what you usually lived and breathed for is suddenly gone. That also means something when you go to work. Too much and too hard work for some time; the fact that the clients have different characters. When I became a midwife everybody thought that I was only there for their good. That is not how the clients are today. I can enter a delivery room and the clients shows distrust even before I have said hello. If I meet many such clients I feel unsure of myself, what is it I do that make them feel I don’t want their good when I enter the room. If you are used to be the one who takes on everything, even the most difficult things, and then have had too many difficult things for a time then you can feel drained of energy. Then we must be aware of it and give such a person some of the easy tasks. You should have maternity rooms where things go easily and where people remember that you are there for doing something good. You must not compare your working life with the women who scream or women who have a bad birth experience or those who always end in something problematic as it has been a difficult process. It has nothing to do with me entering the maternity room. It has something to do with me choosing them, things which are difficult and that I think I can usually handle it so why not today. But that makes it hard.
In the foregoing interview statement, different reasons for burnout and diminishing engagement are named: job related, client related and person related (private) reasons. Declining engagement is described as losing the pleasure of doing the work of a midwife. Main theme in the interview quote above is the relation between engagement at work and quality of client contact. The participating midwives not only differentiated between easy and hard birth processes but also easy and hard clients. Complicated and unrighteous client behaviour is regarded as a reason for losing engagement to do the work of a midwife. The combination of high work demands and missing reward from the client and her family is thought as destructive for the feeling of being engaged. A good contact between client and midwife is regarded as important. The degree of trust and security a client has and feels in the relationship to her midwife is thought to give energy back to the midwife to do her job in a balanced way. If
159
the contact is out of balance, the midwife finds herself in a situation of giving without getting something in return. A feeling of being responsible for always taking the hard chores is also named as a cause of losing engagement and developing burnout. A person who feels responsible for tackling the difficult tasks is regarded as being prone to slide into negative experiences by being overcommitted. The balance between responsibility and commitment on the one hand and the concern for one’s own well-being and pleasure in doing the work on the other hand is named as being important in a demanding field such as midwifery. Interesting to note at this point, is the description of midwifery as being to a high degree nurtured by the positive birth experiences and drained by negative experiences. The absence of positive birth experiences is like cutting out the heart of the job, leaving behind an empty shell. This aspect needs some discussion in regard to work organisation in midwifery and the structure of modern maternity wards with increasing division of labour.
Interview 3: 43 years old, 6 years job experience as midwife Professionally at work, it could be the managerial problems which are the reasons why you don’t feel they listen to you. Maybe you feel a need for … .I don’t know …… not having so many night shifts or weekend shifts or time off for a period and then you feel they don’t listen. I have seen colleagues become distressed, and they feel used or abandoned by the management. There is not an understanding of people’s needs. The management doesn’t understand that it really is a rather hard job. It is physically hard, very hard physically. And if you feel back pain or in another way feel physically exhausted then you can feel the engagement as being up here or totally down. If people lie down and say they can’t or won’t but go to work anyhow. And then there is the psychological side of it as it is quite tough sometimes, and some feel let down by the working conditions which are existent. An example could be that there is too much to do compared to the amount of people to do it. And then you are in a situation where you feel that what you do is not enough. It is not because you are not good enough, it is simply because you are sold out, there are no more hands. It is extremely frustrating and some break down and become afraid, and yes, also frustrated, unhappy. Then there is the situation where the child is dead or the mother is close to dying, or the entire process is so terrible that you feel extremely affected psychologically and maybe even guilty even though it’s not your fault. But that is how we are, we make ourselves responsible for many things. It is typical of midwives, they take the responsibility. Everything has to be perfect, everything has to be so right, and it is real people we deal with so
160
nothing must go wrong. I have been through it and you become so distressed. But it hasn’t affected my ….. it hasn’t been so bad, I have had … good support from my surrounding and I have some fantastic colleagues. But I think you can feel abandoned by the management. They sit up there and are not aware of us having a need to deal with a specific experience. A birth or ……
A leading theme throughout the second comment about losing engagement to do the job is the feeling of being let down by the management. The feeling of being let down is experienced in regard to very different aspects of the job, reaching from help with the physical demanding job situation, to individual solutions regarding shift planning, to professional help with the coping with traumatic birth experiences. It is assumed that it is the incident as such combined with the missing support from leadership that causes a loss in job engagement. Especially the handling of traumatic incidences, causing stress and feelings of guilt on the midwife’s side is named as one example for need of support from leadership in the form of an institutionalized support system. Further the aspect of taking on (shouldering something) as midwife is named as a critical factor by the participating midwives. This aspect is named in the following statement as being responsible for the sudden turn of well-being at work:
Interview 2: 46 years old, 20 years work experience as midwife Something happens with midwives. Midwives are generally good at coping with many things. We receive live-born as well as stillborn children and many of us think that we must cope with it all alone. And suddenly you break down and end up being on long-term sick leave. As I see it, you haven’t been good at taking care of yourself, or too good at handling too much.
Part of the professional understanding of a midwife is the demand towards one’s self to be able to take on and on, no matter how hard the situation has been. This demand can hinder a healthy appreciation of one’s self, borders, and limitations. Engagement, formerly regarded as a positive work attitude and behaviour, turns into having a negative impact. The presumed positive effect turns into a serious impairment of health and well-being of the helping midwife.
161
In the group interview, the relationship between engagement and burnout was not addressed directly but the issue of why midwives stay at work despite the high demands and the challenging work conditions they face was touched. The two statements below name the central reason: helping to give birth.
Group interview
IP 5: No, that is why we come to work, to receive the children.
Group interview IP 2: A good and successful delivery restores your faith in your occupation.
It was discussed that engagement is maintained by doing a good and successful job at fulfilling the core task, helping to give birth. A birth of a child re-establishes the ‘broken’ belief of doing something important. 4.6 Summary of findings on engagement and burnout in midwifery In the foregoing chapter, four different fields of findings from the single interviews and the group interview were presented. First, reactions to the results from the PUMA baseline study were investigated. The variety of reactions was broad. One group of midwives expressed undivided understanding and supported the outcome of the PUMA baseline study with their own estimations about burnout relevant aspects in midwifery. They named a variety of reasons for the high level of burnout in midwifery, reaching from low reward and recognition from clients and leaders to emotional demand to ergonomically challenging job conditions. Another group of midwives expressed astonishment about the results and gave explanations how this high burnout score came about, e.g., the PUMA baseline investigation took place at the same time as major organizational change, the implementation of the electronic journal. One midwife simply stated her disbelief in the results of the PUMA investigation. For her, the high burnout score came about because the questions asked hit some important points in midwifery but should not be interpreted as burnout. It can be concluded that comprehension of the results from PUMA is far from being unequivocal.
162
In order to investigate the relationship between motivation and burnout, the participants were asked to describe their understanding of each of these phenomena. With regard to burnout, three main themes were found: work-related burnout, emotions related to burnout and behavioural aspects of burnout. Work-related burnout is referred to when outer conditions of the job were felt to be the reasons for the development of burnout. The aspects named by the participating midwives refer to established categories of work psychological research. High job demands paired with low reward and low recognition and at the same time low resources are thought to cause burnout. The positive energy connected with the primary task is spoiled by bad working conditions. Moreover, an imbalance is felt between the individual effort put into the fulfilment of the primary task and the reward gotten out of it. As emotions related to burnout, the following three were named: a feeling of being dispirited and having lost the core drive to carry out the primary task, high emotional sensitivity and instability leading to uncontrollable emotional outbreaks (especially tears), and fear as reaction to emotionally demanding situations (e.g., traumatic birth incidences). A feeling of being dispirited is, according to the midwives, seen in a low energy to serve clients. A consequence described in the context of losing control over one’s own emotional expression is a lower flexibility to react to high work demands and a higher rigidity in holding on to single tasks. Not being able to cope with the emotionally straining situation such as traumatic birth incidences is thought to lead to job-related fear and further, to the inability to carry out the primary task. As such, emotions related to burnout are described as having far reaching consequences for the fulfilment of the primary task. As behavioural signs for burnout, low client service, risk avoidance, constant complaints, and an exaggerated feeling of responsibility are named. The described signs of behavioural burnout give expression for the loss of readiness to carry out the primary task, which is understood as the core drive in midwifery. Low client service is described as finding expression in being tired,
163
losing the sense of responsibility and serving on a minimum level without taking the needs of others (clients or colleagues) into account. Risk avoidance is referred to as always choosing the easy tasks, which has a negative impact on colleagues because it leaves them with the difficult cases. Constant complaints were discussed in regard to their contaminating effect on others at the ward. An exaggerated feeling of responsibility is described as responsibility felt for actions of others which the person cannot directly influence. An exaggerated feeling of responsibility puts the person in a state of constantly ruminating about possible, negative outcomes. Findings from both the single interviews and the group interview on engagement in midwifery refer to three different facets of the phenomenon: the professional self, work spirit, and the care for others. Engagement as being a professional self is the description of a midwife who is a model in terms of professional knowledge and sharing this knowledge. A professional midwife is one to look up to and one who is engaged in all kinds of developmental activities to reach an even higher standard. An engaged midwife is described as having a high work spirit, reflected in being the pacemaker for others especially in times when work morale is low. Work spirit shows in a positive attitude towards the job, being happy for the tasks, and expressing passion while fulfilling the primary task. A person with high work spirit was further described as one who is an inspirational source for others, triggering good spirit and engagement in them. In regard to the description of caring for others, an engaged midwife is the one who is sensitive towards her colleagues and the clients she cares for. An engaged midwife is described as being truly empathetic, realizing and reacting to the needs and demands of others. The description about engagement given by the midwives is rich and diverse. The picture of an engaged person is painted as an ideal model of the perfect colleague. This almost unrealistic description might be expression for the high professional demand midwives feel and claim upon themselves. In the group interview, the aspect of professional self was
164
mentioned in particular. Furthermore engagement was defined as the necessary precondition to do the job. The last and fourth area discussed in this chapter summarizes the comments made by the participating midwives about the relationship between engagement and burnout. The way the participating midwives interpret it incorporates many of the other findings of the subjective description of the single phenomena. Job-related, client-related and person-related aspects are named as possible reasons for declining engagement. Midwifery is described as a highly demanding job in terms of work time, responsibility, clients’ demands, physical demands with at the same time low reward and low recognition from the management. It is assumed that facing a traumatic incident combined with missing support from leadership can lead to loss of engagement and even burnout. Further, midwifery is described as a field of work which incorporates many of the commonly known disadvantageous working conditions (e.g., high demand, low control, high effort, low reward etc.). Being overcommitted in terms of responsibility and demand towards one’s self and the exposure to too many negative birth experiences with a low recognition of one’s own limitations and borders are named as further reasons for losing engagement and being on the route to burnout. In contrast, positive birth experiences where everything goes well are described as highly rewarding situations. These positive experiences are seen as being the motor for the midwives’ engagement. The acute and significant nature of the primary task is described as being specific for this field of work.

165
Chapter 5: Person-related and work-related factors
5.1 Introduction In the following chapter, person-related and work-related factors that are important for the understanding of the relationship between motivation and burnout in midwifery are discussed. As person-related factors, biological age and generation membership are discussed. Work time, work family balance, and job routine are the work-related conditions described at this point. 5.2 Person-related factors Biological age has been shown to have an impact on being able to handle the outer conditions of the job and on the congruence of work and family demands. Generation membership is defined as a commitment to certain values and perspectives in regard to the primary task, leading to different ideologies and identities in midwifery practice.
5.2.1 Biological age
All midwives who volunteered to take part in the single interview part of the study are above 35 years of age. This is a reflection of the general age profile at the ward and in Danish midwifery in general (Danmarks Statistik, Indenrigs- og Socialministeriet, 2002) with a peak in the middle age group (35-45 years). 44 out of 49 midwives employed at the ward are 35 years old and above (see Table 3.5). For those who are 35 years old and above, the number of years on the job is at least eight years. The group of midwives investigated in this case study can be described as experienced. One midwife described differences between younger and older midwives in regard to recovery time and special needs for different age groups (e.g., seniority agreements).
166
Interview 7: 48 years old, 12 years work experience. It is primarily the older midwives who have a problem embracing the situation. I can feel that the younger midwives can embrace it more. The busy shifts become tough on you and it takes more time to recover.
The participating midwives described biological age as being important in regard to recovering from demanding shifts. Higher age is seen as being responsible for a longer recovery time after work-related stress (e.g. very busy shift). Also ergonomically challenging positions leading to backaches and problems of body posture over time (with higher job age) were mentioned in the interviews.
Interview 8: 50 years old, 24 years work experience. We have no seniority agreements have no …. As they go into labour at night and that is their right. We can’t make such an arrangement as if you make senior arrangements a group of other midwives must cover the extra night shifts and the extra 24-hour shifts. They will then burn out much earlier. Midwives who are 30 today and have the energy also have children, and they will also burnout at the age of 50, right. It is a vicious circle. We should have more work which includes fewer night shifts, among other things.
There are no seniority agreements at this ward. Such agreements would be difficult to realize because of the rather homogenous age profile of midwives at the ward. Biological age, job demands, and age-related stresses (e.g. having small children at home, longer recovery time for older midwives) are described as problems that are not easy to solve.
Interview 8: 50 years old, 24 years work experience. Yes, it can set you into a state of worrying, that you do it good enough, it is a high responsibility you face; and I could see some of us, maybe it was like that …. There is not only one example, I have this particular example now, but I have also seen this before, that this insecurity comes at last. I have experienced this a lot during the eighties and at the beginning of the nineties where we really developed the monitoring of the unborn child. The step from working with the wooden pipe (Danish: trærør) to the electronic monitoring, it such things, you know. At the point you have a certain age, it gets back on you; thereafter you have to say to yourself: I may find out about this also. It was the same thing when we implemented the electronic patient journal. There we could see many different types; we had two who took their hat because of the electronic journal. …
167
It worries me a little bit that relatively few midwifes have a job after they get older which is probably because they feel uncertain about the new technology and the like …
Biological age is further named as being relevant when talking about technical changes in regard to the primary task. The increasing computerization has cost some drop outs of older midwives who were thought to be unable to learn how to handle the technical challenges related to working with the computer and electronic monitoring devices. The midwives accuse a combination of high responsibility in midwifery and low security when handling new techniques for causing a feeling of incompetence and uncontrollability of events. With increasing age, midwives report an observation of colleagues being inverse flexible in learning new techniques and missing the openness to be able to adjust one’s own work routines.
5.2.2 Generation membership
The participating midwives described a change in work attitudes and expectations between different generations of midwives. There seems to be an “older generation of midwives” who got their education 20 or more years ago and a “younger generation of midwives” who were educated more recently.
Interview 2: 46 years old, 20 years work experience as midwife They are different than those who come now. They want something different. They will not work fulltime. They find out that the wage is too low compared to what want to be offered. It doesn’t add up and they want to be rewarded in another way. I feel that I’m rewarded by all the happy pregnant women I have met and the joy I have seen, but also by the families who come back and say they are expecting their fourth child and then ask me if I will help them again. That is an experience they will be without when they come to such an enormous hospital like this. They never become a part of their…… I work in my immediate environment. They see me on the street and the children say hello. They will not experience that as they are not in the system long enough as I have been.
The main differences are seen in how the job is approached and valued in regard to the effort put into the job and as well as the expected rewards. The young generation of midwives are described as not having patience enough to handle
168
the demanding aspects of the job and to stay committed to it regardless of the imbalance between effort and reward, whereas the older midwives stick to their profession. The new generation seems to act very differently than the former: They do not want to work full time, they put more emphasis on being engaged in research projects and further personal development and they want to have a financial reward for the job they do instead of being content with the non-financial recognition they get from the clients. From the perspective of a midwife with long job experience, this sounds like the wrong choice. For her, the non-material recognition is valued as an important part of the job, which “pays” for the other inconveniences. Another aspect of generational differences is the preferred work form; either team work or working alone.
Interview 2: 46 years old, 20 years work experience as midwife The members of the older generation of midwives want to work alone whereas the young ones like to work together. They like to be two in a maternity room and learn from each other. I think the older generation of midwives have a feeling of what if I mess it up, then I don’t want my colleagues to see it. I try to say that we can learn from each other, let me go with you or you can go with me. Look at me, see what I do, and then ask me afterwards why I did as I did. We must start a dialogue.
The younger generation (understood as more recently educated) is more used to working in teams and is actually looking for possibilities to do so. Working in teams is valued as positive, because of the aspect of learning and widening of horizon. For the older generation of midwives, teamwork is often experienced as challenging and threatening. To share knowledge and let somebody else take a look at one’s professional self is experienced as risky. According to one midwife, the focus of education seems to have shifted somewhat between the different generations of midwives.
Interview 8: 50 years old, 24 years work experience. I think that midwives who have ended their education recently and it is clear among our midwife students ……. I won’t say that the basic studies programme is different but they concentrate on other things. They are good at researching
169
and analyzing things, and they are, of course, nice to be with, but acute, basic obstetrics is missing in some areas, and I fear that they some day will run into an acute problem. It is very important that a recently educated midwife is included in a good group which supports her. Otherwise she is left high and dry. She really is.
Newly educated midwives are thought of as not being educated well enough to react to acute problems when helping to give birth. This might be understood as the standpoint of a single, older-generation midwife but is discussed further in Chapter 8 with regard to the importance of implicit knowledge in midwifery and other future challenges in midwifery from the perspective of the findings of the present case study. 5.3 Structure of working time One core issue in the single interviews was the structure of working time. Work time issues are a constant point of discussion even though the outer conditions of the primary task, which lead to these work time demands, are accepted as given. Different facets of work time are discussed: working shifts and shift planning, night work, part time work, the balance between work, family, and personal time, and job routine.
5.3.1 Working in shifts and shift planning
Due to the nature of giving birth, midwives need to be available at all times. For most midwives, this means that their work is organized in a rotating shift work system including day, evening, and night shifts. Under certain conditions, however, for example health impairments or other personal reason (e.g. family demands), midwives can be assigned to day work (day- and evening-shifts) only. Three of the participating midwives had such specific job assignments and work a normal eight hour day work schedule. Another three complained particularly about work at night and the related strain. The weekly change of schedule was not mentioned as either a positive or negative aspect of the job.
170
One of them described what it meant for her to go from the regular three shift system to day work.
Interview 2: 46 years old, 20 years work experience as midwife I’m a person who really needs to be alone sometimes. And I miss that time alone. I miss my mornings where I could do things at my own pace and then take the night shift. I miss the periods with quiet shifts. We have 24-hour shifts where we only have three hours but we are listed to have 14 hours. That is a surplus. If I have been on home duty I have never done any work at home. I know that many midwives do that. Clean the windows and …as they feel they are paid for working at home. I have always felt that I should be good to myself when I had a 24-hour shift. I have slept as long as I could, I have read some books, and I have enjoyed my needlework and just pottered about as it didn’t matter if I was there when I had finished something. Do some laundry. It doesn’t matter if you take out the clothes when it is done or three hours later. I didn’t find the 24-hour shifts hard. I didn’t. I really enjoy the unpredictability. Of course, I’m like the others; we are tired when we are being used too much for longer periods of time. But you also get time off in lieu of wages and the like. And that I never get anymore.
Although one would expect that working day shifts only is regarded as a relief to the demanding three shift system, this midwife describes the negative aspects of this change for her. Compared to the three shift system in the day shift only system, she feels that she does not have as much recreational time on her own as she used to have before. She describes that she actually does not have the time any more when nobody is at home. It is kind of a double-bind situation: in order to have more “quality time” for family and friends, the midwife has to sacrifice the time being alone without any demands from her children or husband. Daytime work is compared to the three-shift-system as more inflexible but also easier to plan. Another negative aspect of daytime work is the loss of unexpected extra time “earned” when not called in for emergency duty. These days are counted irrespective of being called in or not. Being on a day schedule, these unforeseen “free” days do not happen anymore. For those midwives who work the regular three shift system, the planning of the shifts is an important topic.
171
Interview 5: 49 years old, 8 years work experience as midwife But we can try to make smaller units. We have talked about it. Smaller units where we have influence on how the shifts are planned. I think it is right that the feeling of having no influence leads to burnout. I really think that.
Shift planning done centrally causes speculations about being unfairly dealt with. The wish to have influence on the planning of shifts has been discussed in depth and especially in regard to re-organizing the ward into smaller work groups which then are responsible for organizing their shift schedules themselves. However, not all interviewed midwives believe that having more influence on planning the shifts is the most important topic.
Interview 8: 50 years old, 24 years work experience as midwife A working group had, among other thing, worked with shift planning. We had expected a lot of that as many of my colleagues think that shift planning is our largest problem. I think not.
According to this midwife, shift planning might be a problem, but it might in the long run not solve the “real” problems at the ward. One problem she refers to is the use of a lot of the precious time which should be used for educating younger midwives in how to react in acute situations in practice instead. From her perspective, it would be for example better to think about how changing client demands (e.g. to be informed about each little step while giving birth) can be put together with decisive demands in an acute situation. She sees a need for younger midwives to be better prepared for making quick decisions when the situation demands it. The interview section below illustrates her critique of “wrong choice of priority” which she interprets as a fundamental problem at the ward in the future.
Interview 8: 50 years old, 24 years work experience as midwife And there I suddenly was with a trainee who ….. she was nice and everybody liked her. And then the woman starts bleeding and she turns to the woman and says she bleeds too much and it is a bit dangerous and that we must set up a drop. That is just a thing which is very dangerous. One thing is that you have to
172
be very didactic when you tell a patient what you are doing but you must also say that it has to be that way and we do it now.
5.3.2 Work at night
Among the different shifts most midwives have to cover, working at night is by far the most demanding. Work at night is described as being different in regard to the quality of service given to a client. In midwifery, the demands from clients being in labour during the day and at night are not different from each other. Children are born 24 hours a day and the same service a midwife gives to a client at daytime ought to be given to a woman in labour at night. Nevertheless, the participating midwives describe a difference in service they are able to give at day and at night. They are very frank and at the same time uncomfortable about their inability to serve during the night. They state that there is a difference in service readiness between night and day shift. At the same time, there is agreement about the necessity to cover the hours during the night, because childbirth cannot and should not be planned according to the working hours at the ward.
Interview 1: 38 years old, 14 years work experience as midwife I have to admit I am not good at working at night. I cannot at all provide the same quality of service as during the day. … I am simply too tired. I don’t function well. Interview 3: 43 years old, 6 years work experience as midwife Sometimes I think about what the women in labour ……… well you are different, I’m another person when I’m on night shift than if I have a day shift. But they don’t know. Then they would have to come a second time and see that there is a difference (laughs)
Interview 7: 48 years old, 12 years work experience as midwife Sitting in a delivery room makes me very sleepy and I have trouble not falling asleep. Sometimes I don’t dare to sit down as I’m afraid of falling asleep. And I don’t think I’m being nice, I’m not as patient as I usually am in the daytime. A midwife must be patient and I’m not at five o’clock in the morning, then I’m not patient anymore. I feel that I’m not good enough and I feel that I’m not a good midwife during the last hours of a night shift. I’m really not.
173
The midwives are quite open about their reduced capacities while working at night, especially if they have to work several night shifts in a row (which on paper is not the regular situation anymore).
Interview 1: 38 years old, 14 years work experience as midwife I don’t think that I provide optimal care or engagement at night. Well, yes …. Generally, fatigue makes you uncommitted, or generally not committed during the entire working day
Interview 3: 43 years old, 6 years work experience as midwife Who is not tired and burned out during the night, or what! … If I had three night shifts in a row I would probably also burn out. I can only handle one at a time (laughs).
Interview 7: 48 years old, 12 years work experience as midwife My biggest problem, the thing which burns me out the most, are the night shifts. This is actually something critical for me, these night shifts.
All three midwives report how demanding it is for them to work at night especially to overcome their tiredness in order to do their work and be as alert as during a day shift. It is interesting to note that two of these midwives mention burnout in this context. Here, the term burnout is used to describe physical exhaustion as a result of the night shift. However, it seems as if this exhaustion is an immediate reaction to the night shift and can be overcome rather quickly if followed by an adequate recovery time. These can be days off and consultancy days with a regular day working time.
Interview 8: 50 years old, 24 years work experience as midwife If you could only be sure about two days a week, where you just need to work from 8 am to 4 pm. The possibility to withdraw, it would be easier for midwives with children, those who are pregnant … we don’t have any; we don’t have an out-patient clinic where you can do some day work, for instance.
The consultation days (consulting women during pregnancy) are described as time to relax from the primary task of serving when helping to give birth. Unforeseeability, uncontrollability, and time pressure being present during a regular work day at the ward are not present when consulting pregnant woman. Instead, consulting days can be described as structured, planned ahead, and with
174
a rather strict time frame. These days are attractive for a greater number of “needy” groups (older midwives, midwives with small children and pregnant midwives) and are not a picture of the usual condition of the rest of a midwife’s work week (usually a midwife who works full time has one consultation day per week).
5.3.3 Part time work
About one third of the midwives in this ward work part time. For some midwives, part time work is regarded as the only solution to be able to coordinate a family, a home and the demanding job of a midwife. In their view, working part time gives some extra flexibility to recover between shifts. This is time which is not available as a full-time midwife.
Interview 1: 38 years old, 14 years work experience as midwife No. I believe that I instead would … My working hours have been reduced since I took this job. And maybe I want to work half-time later on. I believe that a half-time job which includes shift work means that you are not very much away from home and you have better time to recover between duties thus allowing you to spend more time with your family. To work full-time as a midwife would be impossible for me. I have never worked as a full-time midwife but “only” been employed 32 hours per week. Interview 7: 48 years old, 12 years work experience. I worked full time the first years, but it was tough. It was very tough as you have a tight schedule.
However, also part time work can be demanding as the part-timers are often assigned to the most straining or family-unfriendly shifts.
Interview 4: 45 years old, 20 years work experience as midwife When you are a midwife working part-time you also get many inconvenient shifts, meaning evening, night, weekend and 24-hour shifts. I don’t know if we have relatively more of such shifts. …… but it doesn’t help my family much that I’m home Monday, Tuesday, Wednesday and Thursday when they are away. That is not what they need.
The disadvantage of part time work is seen in the fact that part time workers are often put into the regular three shift schedule at those points where there is a
175
shortage of full time workers. One participant mentioned a feeling of injustice because part time work is used to cover the uncomfortable shifts. In doing so, the advantage of part time work fades away. Short work weeks stand in competition with inconvenient working hours, often to the disadvantage of the part time worker.
5.3.4 Work-family balance
Interview 2: 46 years old, 20 years work experience as midwife When I applied for the job, my family was quite happy about it as it was nice that I was home all the time. That is how they see it if you are home at dinner time and when you tuck them in and so on. Then you are always home if you ask a child. After some years, I had to find out if I wanted to stay in this job. We talked about it at home …. It was only our youngest who lived at home, he turned 15 …. And I went home and talked with him …. He must have been about 12 years old. I told him I could go back to the shifts as I think I am more at work in this function than in the other I had before. Then he asked if I had to work in the evening and on weekends. And yes that would be the consequence of that, but there would then be other positive things about it. He and my husband then said it would be nice if I could work day-time.
The foregoing interview quote illustrates the consequences of shift work at a maternity ward from the perspective of a midwife with special duties, working day shift only. The statement is an illustration of the ambivalence behind the effect that working hours have on work-family-balance in midwifery. For the family, the day shift is experienced as a tremendous relief. Even if the mother actually spends less day time at home, the perception is that the mother is spending much more time at home than before, because she is at home at the same time as the rest of the family. Shift work takes time away from the family, which cannot be paid back by time spent at home during hours of the day where the rest of the family is absent.
Interview 7: 48 years old, 12 years work experience as midwife Because it is so hard on our everyday lives, and it taxes our family once in a while, you work when the rest of the family has time off, sometimes you go to work at inconvenient hours, mother comes home and is a bit grumpy, and oh something is wrong again, right. And you can’t take a three-week holiday with your children. That is hard, I think.
176
For those working in the regular three-shift-system, it is not easy to accept that the family has to carry the burden of the job demands. One example mentioned is the demand to work through the main parts of summer vacation without having the opportunity to spend more than two weeks together with family
5.3.5 Job routine
At first sight, midwifery seems to be a field of work without any kind of work routine. Instead, high unforeseeability and uncontrollability of events seem to be the key characteristics of this job. However, during participant observation, it became obvious that even here some routine task exist.
Interview 4: 45 years old, 20 years work experience as midwife I have consultation hours as a midwife; One day every second week; I share them with a colleague, she has the other part. That is a lot, I think. Then, when it is only every second week, it doesn’t become as intensive as if it was once or even twice a week. But it makes up a large part of being a midwife ….. working with pregnant women. I wish I could do more. I would like to have consultation hours every week. Of course it takes a lot of time. And there are so many other things to do on a maternity ward. Not only births. Check-ups and observations and ……
One form of natural job routine is the regular consultation of pregnant women. These consultation days are very important for the midwives. The consultation days are predictable regarding work flow and work time. Maybe even more important than predictability, the consultation of the pregnant women is essential for the holistic understanding of the work of a midwife (leading a pregnant woman through her pregnancy and finally helping to give birth). There is also a lot of monitoring and controlling functions in the course of a regular work day at the ward. This became very obvious while being a participant observer at the ward. For activities directly related to the primary task of a midwife (e.g. helping to give birth), routine tasks are harder to perceive but not absent: every birth is followed by a number of routine check ups even though each birth is unique.
177
5.4 Summary of findings The foregoing chapter reported person and work related factors found in the interviews, which are meant to have relevance for the understanding of the relationship between motivation and burnout in midwifery. Biological age was interpreted as having an impact on the way stressful work episodes are handled by the single midwives. Older midwives are described as needing a longer time to recover from stressful work episodes. Moreover, biological age was put in contrast to flexibility to adjust to technical changes (e.g., new techniques, computerization). Differing occupational ideologies and identities are described for different midwife generations, leading to a difference in fulfilment of the primary task. In conclusion, younger generation midwives (understood as more recently educated) are described as being less committed to the primary task but more interested in developing other skills (e.g. doing research, look for different job opportunities) and less willing to accept high work demands with low recognition (financially, etc.). Younger midwives are described as being less competent in acute situations and at the same time more willing to learn from each other and more eager to work in teams. The organization of work time and time at the ward was reflected as a sensitive issue in regard to work motivation. Some midwives regard the system of shift planning as insufficient and dissatisfactory, because the central planning does not give them enough influence. However, at least one other midwife does not regard the missing influence in planning the shifts as the most important reason for work-related strain. Working at night is described as being very demanding and is thought to be a reason for burnout. The term burnout as defined and used by the participating midwives refers to an acute state of exhaustion which can be overcome if followed by an adequate recovery period typically known from minor states of physical exhaustion. Consultation days, which are more clearly structured and more foreseeable, are experienced as a welcomed break in the otherwise demanding work routine.
178
Part-time work is described as being common at the ward (approximately one third of the midwives work part time). An advantage of working part time is seen in a higher flexibility in the personal work schedule. A disadvantage is seen in getting fit into the schedule after shifts have been given to full timers, leading to unattractive shifts for those working part time. Work-family balance is also named as an important issue for the midwives. The acute nature of the work often leads to not being able to balance work and family sufficiently, family often standing in second line. This leads to strain for the family, especially for full timers. On the other hand, some disadvantages of day work were named by those three midwives on a day schedule. One interesting aspect they report is that time at home alone during the day used to recover from the demanding work is no longer available. Finally, job routine was discussed. Even though the job of a midwife is characterized by a high degree of unforeseeability, there are also aspects of a daily job routine. Job routine in this sense is described as recurrent tasks in the course of a work day (e.g., journaling after a birth has taken place) and in the course of helping to give birth (regular check ups).
179
Chapter 6: The significance of resources in midwifery 6.1 Introduction Resources and resource allocation emerged as an important subject to talk about in the course of the single interviews. Inadequate resources in terms of insufficient manpower at the ward are thought of as having immediate consequences for the quality of work which is highly valued by the single midwife. In the following, the availability of resources and allocation practice are discussed. Further, the balance between resources and job demands is reflected on, as is the aspect of feeling secure in regard to these resources. 6.2 Amount of resources and resource allocation practice Midwifery, being part of the public health care system, is treated the same way as other parts of the health care system when it comes to resource allocation. To measure the resources in midwifery, the number of births per year is divided by the number of midwives at the ward. In 2002 and 2003, when parts of the data collection took place, resources at the ward were described by the participating midwives as being low. 49 midwives (without student midwives) were employed at the ward. Approximately 2,600 births per year had to be taken care of.
Interview 2: 46 years old, 20 years work experience as midwife I think it is a problem that we must coordinate with the others as we are compared on the basis of different parameters. We are not able to discuss nursing in the same way as they do at a ward for cancer patients or a ward for patients with heart diseases or intensive care. We should be compared on the basis of the way we take in the patients, with intensive care or the emergency room. I think that is where burnout and the motivation and job satisfaction can be seen among midwives. Just because we are part of a huge organisation they compare us economically with the other wards. They compare our figures with figures presented by the other wards, and if you ask a politician how he defines a birth then he will define it as the moment the child comes out. And if I have 2,600 such births then I can keep on talking about the many consultations, the out-patient visits where the pregnant woman thinks she is in labour and then she isn’t, and she comes in to an examination. And then there is all the rest. No, we talk about births, such and such a number. It can be estimated as an average,
180
how long it takes as they don’t need help all the time, but the woman think they have that need, and then we are caught in the middle. But that is the reason why you don’t have the same time with the family as you had in the old days.
The interview quote above refers to the problem of being compared on the basis of incomparable parameters. Looking at the way how clients are admitted, midwifery comes closest to the way an emergency ward or an intensive ward functions. It is experienced as problematic when resources are calculated on the basis of birth rates, because many of the time consuming tasks of a midwife do not terminate with the birth of a child. The calculation of resources is done on the basis of fulfilment of the primary task (here helping to give birth), not taking into account that many cases in midwifery are of observational nature (e.g. acute problems during pregnancy such as no signs of life, bleeding, or nausea) or for consulting reasons. For the midwives, this leads to a dilemma between an own professional standard, the wishes of the client, and the allocated resources to do the work. In the course of participant observation, it became obvious that these sideline or secondary activities, not accounted for when resources are calculated, take a lot of the daily work time of a midwife. Moreover, a lot of former administrative work nowadays is done by the midwives themselves, e.g. journaling of births, answering telephones at the ward, ordering material. It is not unusual that these tasks can only be fulfilled by working overtime.
Interview 1: 38 years old, 14 years work experience as midwife It is a strange, strange job as it can’t be compared with other jobs. You keep comparing with nurses and other groups within the health care sector, but our job is a special area where you constantly work with people who experience a crisis. Not that a crisis has to be a bad thing. Giving birth to a child is some sort of life crisis – suddenly being a parent.
Besides the problems of comparing midwifery in terms of economical factors, midwifery is defined as special case in the public health care system because midwives work with people in a crisis. Although, fortunately, in most cases it is not a negative crisis, but one with a happy end, it is nevertheless a period were everyone involved is very anxious until the child is born and it is clear that mother and child are well off. The birth of a child, which is at the same time the
181
birth of a (larger) family, is in any case a form of fundamental experience, a significant life event. 6.3 Balance between resources and job demands The fit between resources and demands is rather sensitive, as it touches on a variety of issues. In the following, occupational standards and the ideology of serving 100% are discussed in the resource context. Moreover, the resource question is reflected on with regard to feelings of security while fulfilling the primary task. The meaning of resources for health and well-being is also discussed, as is the importance of resources for client education.
6.3.1 Balance of resources and demand to serve 100 percent
In the course of the interviews, it became clear to the author that midwifery is different from other occupations in regard to two aspects: first, service in midwifery often cannot be delayed. Second, there is no middle ground in regard to service, quality and commitment to the single birth process. Midwives need to be able to provide 100% service when fulfilling the primary task.
Interview 6: 58 years old, 33 years work experience as midwife At some point during a delivery you have to focus on the woman. And in our plans we say that a woman in the last phases of the delivery has a right to have a midwife present. However, the county doesn’t fully accept that. It still defines a delivery as something that at least takes 6-7 hours, so you have plenty of time to see other patients in between. But life is not always like that.
Most of the midwife’s work is work that has to be done immediately. There is no space for delay. On the job, the midwife must always be ready to provide the best possible service. The demand for resources experienced by the midwives differs to some extent from the official appraisal of resource demand. From the midwife’s perspective resource allocation is experienced as insufficient not only in amount but also flexibility. There are written standards about the use of resources which are described as being good in theory but do not actually function, given the recent allocation practice. Because of the spontaneous nature
182
of birth, some flexibility is needed in order to be able to secure 100% service in the critical phase of birth. The gap between official evaluation of standards and practical experience leads to an allocation practice which is far from being optimal seen with the eyes of a midwife.
Interview 3: 43 years old, 6 years work experience as midwife …… then you risk having to go from one room to another without being able to be there 100%. Then you feel you are on only 50% present in the two rooms. That is very frustrating.
Midwives react very strongly when resources are too low and the provision of 100% service is no longer secure. The participating midwives express frustration about not being able to meet their own occupational standard of 100% service.
Interview 9: 44 years old, 18 years work experience as midwife But that is part of it all. I think that we are often ill, and absence is not always covered. If you are so unfortunate to have a 24-hour shift such a day where you are called in and must cover some fixed shifts and you can see that if the shifts had been covered you wouldn’t have to work so hard. It is very tough. I feel that if the shifts are covered and you are called in then it is OK, not ………
Given the fact that the delivery of children is impossible to plan ahead in terms of time and complications, resources must be enough to stay flexible. There is an established system of emergency call, but unfortunately due to low resource availability (positions vacant) and high absence rates, regular shifts are frequently covered with those midwives being on call. The demand of having a person in the background being on call to take care of the extra demand is therefore not often fulfilled because the one who is supposed to be on call is already substituting on the regular shift. According to the interview participants, it is common practice to use the midwife on call as a substitute for a midwife who is on sick leave because there are no extra resources available. Consequently, the flexibility needed to deliver 100% service is not always given.
Interview 2: 46 years old, 20 years work experience as midwife You don’t have the chance to finish it properly. You leave them when you have congratulated them and the child has been weighed and measured, and then another person comes in and takes over. You don’t have your own group of
183
pregnant women as you would have if you chose to see the process instead of the financial side of it. If you asked yourself how things could become more rational, then the pregnant woman should follow a group of midwives, and one of these midwives would be with her during the delivery. That would make it much easier for both parties as many problems would be solved in advance. There are so many things a woman in labour should not think about and one is if she can trust me. That has been revealed during the pregnancy and it is OK as she can say that she wants another midwife. All the things that we say we can’t afford in Denmark today. Everything has to be rational, it is a huge impediment. A woman in labour comes by and a midwife comes by and helps her. That is the way it is. You don’t know the patients as you did before when you had small delivery wards.
Another aspect standing against the professional understanding of giving 100% service to the women in labour is the organisation of shifts in a centrally structured organization. The original meaning of midwife goes back to the Old English word med wife which, translated, means being with wife (Molnar, 2004). In the original sense, this is a description of the function a midwife is meant to serve while assisting to give birth. In the interview, the midwife mentioned that this original understanding of midwifery is not met in modern, large hospital organizations. Large organizations need to have a functional structure to organize work. On the contrary, natural birth, which still is the preferred birthing practice in modern midwifery, follows the rules of natural time. The eight-hour shift introduced with the centre organization of the maternity wards in Denmark led to a fragmentation of midwifery. This fragmentation is experienced as the second best way to work as a midwife. The work of the midwives nowadays is organized according to economical figures and not so much according to the natural birth process, which would, for example, require staying with the woman giving birth until the child is born. Instead, time and effort needs to be invested in order to build up confidence and rapport with the women coming to the ward and again throughout a birth process when shifts change. This effort costs resources (time and emotion), both for the midwife and the woman in labour. Therefore, this practice is not regarded as optimal birthing practice because it also leads to insecurity in the woman in labour. The organization of birth according to 8-hour shifts leads to a higher anonymity between midwife and
184
client. This is seen as a tremendous difference between small places to give birth and larger hospital organisations.
6.3.2 Expertise, resources and security
The aspect of job routine, understood as acquired expertise to do the job of a midwife with a feeling of high security about one’s own decisions, seems to be of importance in regard to resources and security. During the observation, one midwife said that it takes at least seven years to reach a feeling of professionalism on the job, which the other midwives confirmed. These first years on the job are like gathering invaluable experience and collecting precious and important moments and incidents.
Interview 6: 58 years old, 33 years work experience as midwife When you have worked here for so many years, things just happen. Things don’t become total routine, but you work up some kind of routine. And there are no two similar births, Ms. Hansen and Pedersen etc. How shall I put it – you can be more relaxed about it, in a positive way.
Each birth process is regarded as a new challenge not to be compared to previous birth processes. Expertise is associated with a greater security to make clear decisions in a highly uncontrollable setting. Uncontrollability is common in midwifery because of unforeseeable birth processes and emergencies of different kinds (e.g. premature contractions, bleeding, no signs of life, nausea, etc.) which can happen at any time. This kind of uncontrollability is taken into account and is also regarded as part of the challenge of midwifery. One point where this positive challenge can turn into a feeling of insecurity and even anxiety is when resources are low. The relation between feelings of security and resource availability was one aspect which emerged as important in the course of the single interviews. In the group interview, the issue was discussed in more depth. Findings from the single interviews were confirmed and emphasized.
185
Interview 6: 58 years old, 33 years work experience as midwife The limit is reached when you are forced to provide poor service as you have two of them. It becomes too much when you have to provide poor service.
Midwives are forced to deliver bad service at the point when resources are not sufficient. This point is described as being at the border a midwife is willing to accept. Not only is providing 100% service an important aspect of their occupational identity and fulfilling the personal wishes of a woman in labour, but it is seen as a guarantee of a high standard of security for mother and child. In the group interviews, the question of at what point low resources are experienced as critical was discussed in order to investigate in more depth the relation between resources and feelings of security. The intensity and directness of the following statements is an expression of the importance of the subject. Shortness of resources is discussed as one important reason for feeling uncomfortable with the service one can give and for growing frustration.
Group interview (to the question what is threatening for feeling secure about doing the job) IP 3: It is a critical situation where …… well, I would call it critical if I didn’t feel secure about what happened in the various delivery rooms. I would be very sad if I forgot to do something. I know that we all forget things sometimes, but if I did it often I would feel very insecure. I have been in situations with dead or sick children. It is something profound in me. The output should be healthy children - that is what it is all about, no matter if the resources are scarce. I also think it is the reason why we have so many extra shifts. It is my impression that when we could get help from temp agencies nobody had any energy left. It is so confusing that you take on extra shifts and it helps, but doesn’t help sufficiently. So I think that many midwives say that it is not worth it, and you are always here anyway…..
A feeling of security is named as being essential in the course of helping to give birth. A critical incidence starts at the point where the midwife is starting to feel insecure because she is not able to monitor what is going on in each birthing room. It is regarded as natural that death can happen in the course of birth, but it is stated as unacceptable if this happens because of low resources. One strategy to avoid this uncomfortable feeling of insecurity is described as staying voluntarily at the ward at busy times to help those colleagues on duty.
186
Group interview IP 2: A critical threat against safety is that you are suddenly alone on the shift, and you don’t know what comes next …. of course there are doctors but you are the first to deal with the problems. …. It is not always the most severe problems. They also come unannounced as they are the most acute problems as they bleed. These problems you must evaluate on your own, you have two telephone calls at the same time and maybe you also have two women in labour. And it takes time before the colleague called in arrives, and maybe you don’t even have time to call her. That is my nightmare and that makes me feel insecure as I wouldn’t know what to do in such a situation. I would wonder if I did the right thing.
Another threatening aspect is described as the imagination of being alone at the ward (which corresponds to the actual situation at the ward at the time of the group interview) without knowing what to expect. The possibility that something overwhelming and maybe uncontrollable will happen is stressful and described as ‘lurking’. Being alone with the possible situation of too much work and not knowing where to run to first is described as a real threat to established work routines.
Group interview IP 2: I feel that I would end up in a situation where I faced a catastrophe. In a state of total preparedness, with a rapid pulse, and extremely focused on all the things that can go wrong and what to react on. It can be compared with an animal ready to attack. It is a situation where the adrenaline is pumping. It is a rather stressing situation. And the thought of such shifts with regular intervals and that it can happen on my shift. It is not as it is planned but it can happen in the future. And in the phase before, where I know that I have a shift where I will be alone. Well, I really think about the situation and try to decide if I can handle it. In such a situation, I can easily imagine that if you feel just a little bit ill you could come up with an excuse for not taking that shift. The pain develops into a real headache. I think we could all be tempted to think like that.
The bodily reaction to such a situation is described as fight or flight and as a situation no one wishes to experience again soon. Trying to avoid this feeling can lead to absenteeism; here described as faking or the imagination of illness. To be forced to regularly work under conditions where the feeling of security is threatened because of short resources is experienced as stressful and frustrating.
187
6.3.3 Resources for client education
Client education was valued as an important field of work, which is increasingly reduced because of declining resources. Some of the midwives see client education as an important part of actively preparing women for the birth experience or to inform parents about the health impairments for the child connected to smoking, drug abuse, and alcohol during pregnancy and while breast feeding.
Interview 8: 50 years old, 24 years work experience as midwife And we think we do a good job, and we think we have much to offer within the health promotion area as we meet the women and their families at a perfect time in their lives. We meet them when they are young, when they a going to have a baby, when they are motivated and maybe then it is possible to change some habits etc. We can present health promotion to them but resources are cut down.
Frustrations about low resources were mentioned when talking about important steps for client information, e.g. smoking cessation programs. These preventive actions for pregnant women and their families are cut down because resources are not available. The midwives regard their preventive work as very important because they can approach families at a sensitive point in their life, having high impact upon them. During pregnancy, certain preventive steps can be taken which diminish the chance of complications during the birth process and also of sudden child death during the first months of life. Not being able to put further effort and resources into the instruction of clients who need more supervision further diminishes the sense of doing a holistic job. A success story about how to use limited resources to educate pregnant women in form of group consultations is told in one of the interviews. To be able to decide within a given frame about how to use the own work capacity is a degree of freedom and participation. The story sheds light on the engagement midwives at the ward put into the job. This kind of engagement is often extracurricular engagement, time not paid for.
Interview 8: 50 years old, 24 years work experience as midwife …. a teamwork concerning our group consultations. We have those who started it after the county had decided that it should be an offer in our county. So I
188
thought we must do it as good as we can with the few resources available and it was a huge success. I have invested all my energy in that project and I will keep on doing it.
In the group interview, the stressful aspects of the midwife’s job because of low resources were confirmed.
Group interview IP 1: Yes, it is tough. I think that you at many workplaces where the employees are stressed and burned out, can let go of it all, walk away and say you can’t take it anymore. We are in another situation, we can’t let go and go away if it all becomes too much. We must be able to handle the situation as a midwife, keep a stiff upper lip and then move on. There is no other option. Afterwards, it is rather stressful. When you go home, it all becomes too much and that taxes you. When you are in the middle of it, you cannot break down; there is no room for that.
Midwifery was described as work without space for personal weaknesses and feelings while active. When time is busy at the ward, there is no time to reflect on a particular situation; this must take place when the situation is over and the midwife is already at home. In regard to resource allocation, this aspect is important to keep in mind. The health and well-being of a midwife are described as being seriously threatened when resources are cut down to a point that stressful situations like the one described above are the rule and no longer the exception. 6.4 Summary The question of resources in midwifery emerged as a central theme in both the single interviews and the group interview. Resource allocation practice is described as being insufficient. It is regarded as problematic to be compared with other wards on the basis of incomparable parameters, e.g. birth rate being the numeric factor of resource calculation, not cases. In the course of participant observation, it became obvious that secondary activities such as journaling after birth, consultation of pregnant women coming to the ward, answering the telephone etc. which are not accounted for when resources are calculated, take a lot of the daily work time of a midwife. Another important difference between

189
midwifery and other wards in a hospital is seen in the acute nature of the task and the working with clients in a crisis; the transformation into a (larger) family. The fit of resources and demands was brought up referring to different aspects. First, resources are meant to be one decisive factor regarding the quality of service which can be given to the client. For the participating midwives, the provision of 100% service is described as being of great importance. Not being able to do the work in a responsible and sufficient manner because of low resources is regarded as not acceptable, causing frustration for the midwives. The low flexibility of resources was also addressed, pointing to the fact that midwives on emergency call are frequently called in to cover the regular shifts. One last aspect discussed in regard to the demand to deliver 100% service is the impact of the structure of modern maternity wards onto the primary task. The participating midwives expressed at different points that the 8-hour schedule leads to a segmentation of the task with negative impacts for both clients and the midwives themselves. The demand to provide 100% service is more difficult to fulfil when shifts change in the middle of a birth process. Second, low resources are made responsible for a diminished feeling of security. Security is established through expertise won while fulfilling the primary task. The expertise is sabotaged when resources are too low to be able to do the work in a responsible manner. Knowing they are not able to serve100% is described as a negative impact, leading to stress reactions known as fight (expressed in working over own limits), flight (expressed as staying absent from work or as ‘taking’ a leave of absence), and freeze (as described as staying in the delivery room no matter how busy the rest of the ward is). Not being able to ensure high security while helping to give birth is experienced as threatening. Similarly, not being able to be with a woman giving birth because two others are in the same state of needing the midwife’s service who is alone at the ward, not knowing what to expect and with an ever-present ‘lurking’ threat are named as highly unbearable work conditions. Last but not least, resources for client education are valued as important for the holistic job experience and as supporting factors for
190
fulfilling the primary task successfully; in terms of “bringing healthy babies to Earth”. Low resources and the connected consequences are seen as leading to serious health impairments.
191
Chapter 7: The role of emotional demands and feelings in midwifery
7.1 Introduction In the following chapter, emotional demands and feelings in midwifery are described. The interview partners talked about emotional demands connected to the primary task in midwifery and feelings as reactions to traumatic birth incidences. In regards to emotional job demands, three aspects are discussed: (1) reactions to differences between professional conviction and client demands, (2) the demand to serve the best way regardless of own feelings and condition, and (3) to give as a core demand when helping to give birth. Feelings as reactions to traumatic birth incidences have a different connotation. This second aspect focuses on the midwife’s immediate (in the sense of not controlled) feelings when confronted with traumatic birth incidences. Here, her reactions, both as a professional and as a person are described. The support from colleagues and family as well as formal psychological help after traumatic incidences is presented. Last but not least, the aspect of formal versus felt responsibility is discussed. 7.2 Emotional demands Emotional demands are those job demands which require emotional involvement of the midwife regardless of her momentary feelings and condition. It is emotion work, following from the nature of the job.
7.2.1 Reactions to rising demands from clients
In the interviews, the midwives report about rising demands and expectations from their clients in recent years. There are more women now who express their own ideas about how the birth process should be arranged. There is a higher demand for techniques and medicine to avoid pain in the birth process and
192
especially planned caesarean sections are requested more frequently by the younger generation.
Interview 2: 46 years old, 20 years work experience as midwife Another factor which has appeared in the past years is the medical aspect where the clients are becoming very demanding with respect to how they approach birthing. Take someone like me, who has always felt convinced that women are born to give birth to children and that it is a natural process which they need help and support to go through … however, they do not need all kinds of technicalities. But if you ask me today, I think it is all right to ease their pain when they are in labor, though I still find it difficult to see completely healthy, pregnant women telling me that they are so scared of giving birth that they want a caesarean section. They prefer an operation which I know will have a serious impact on their body instead of the completely normal and natural process a birth is, and which their body is made to go through. It causes some complications which make us and our clients confused. They often come from homes where they have learned that if there is anything you need from the health service - you should just insist on having it! And if the authorities are not willing to give you what you want, you have the right to complain. Nobody would have complained about me 20 years ago because I did my very best. However, to do your very best today just isn’t enough anymore!
The quote above is an example of the self-image the participating midwives refer to when they talk about their clients. This image is as being a facilitator and pacemaker throughout the birth process, guiding the woman in labour and her family. This self-image stands in contrast to the clients’ demands experienced by the midwives. The midwives describe the recent birthing generation as a generation with high demands, being less willing to go through pain and discomfort during the birth process. Women giving birth are described as being well informed, often knowing exactly what they want, and who confront the midwives with their wishes and demands. The fact that women are informed is not seen as critical but the decline of recognition of the professional knowledge of a midwife is experienced as problematic, especially in combination with the accelerating demands towards the midwife. Modern women are seen as expecting to receive best service according to their own conditions. The opinion of the midwife is heard but not necessarily accepted as the last word. The participants of the case study describe a feeling of being bewildered, especially when a pregnant woman is making choices against the good knowledge, experience, and advice of the midwife. Moreover, a midwife
193
nowadays has a greater risk of being made legally responsible for actions connected to the birth process. This last aspect is further discussed in relation to felt responsibility (Section 7.3.2).
Interview 3: 43 years old, 6 years work experience as midwife … I believe that I would much rather change the women. I think there is a huge difference between women today as compared to when I started as a midwife 6-7 years ago. … They have started to become women whom you can’t get close to. They are all façade and whimpering, whimpering, whimpering …! They tell you that they want things done in this and that way. They feel that we are down here and they want us to do exactly what they tell us to do. The situation has become more or less out of scale, don’t you think? About 220 years ago, the midwife was standing up here looking down on the woman while she was guiding her through the birth. Before, the scale was more or less in equilibrium but now I believe there is some imbalance.
There is a gap between the self-understanding of a midwife and the appreciation from the women’s side. The birthing generation is often described as self-centred and commanding. In contrast to former times, the respect and appreciation brought to a midwife seem to have diminished. The comment above goes as far as to speak of imbalance of the present situation whereas ‘to look down’ on the woman is described as the opposite of the situation today.
Interview 9: 44 years old, 18 years work experience as midwife To the question: What is it that is so difficult about doing the work of a midwife nowadays? What has become difficult or more difficult is that we are not only there helping to give birth but in some situation even if you can not generalize this they expect us to deliver the child, and this I think is a little tough. Well, I have delivered my children and I really want to help others to deliver theirs but I cannot deliver for them. Especially in situations which are a little bit difficult, where the process is maybe a little tiring and slow and quiet, she does of course get tired and her husband cannot bear to look at his wife in such a condition where she is in pain, and still it is not happening much; in these situations you can experience that they turn their frustrations against us. And this I think is a little difficult to handle; you are there to help them but each time you try to say something about what the woman shall try to get some relief you get the eyes of the partner on you as if he says, ‘hello!, don’t you understand, have you not understood anything?’; and than you might think ah, I do not say this to make it worse, I say this because I try to help.
194
Interview 1: 38 years old, 14 years work experience as midwife And if they make demands which are in opposition to the rules ... you can say that normal practice means wide limits. But sometimes they can make impossible demands, e.g. they want an epidural or a caesarean because they don’t want to be in labor anymore or … and suddenly you see a whole family “blow themselves out” at the birth where nothing indicates that things are meant to turn out that way.
Besides the bewilderment felt about the behaviour of some birthing women nowadays, the participating midwives talked about their frustration when helping to give birth. The group of midwives describe a generation shift when looking at their clients and the way the clients approach birthing. There is a perceived trend to demanding more and more service from the midwives and at the same time not accepting her leading position throughout the birth process. Especially the aspect of epidural anaesthesia and planned caesarean sections was discussed in the interviews. The participating midwives expressed acceptance but not understanding for this sort of client demand. The group of midwives taking part in the interviews represent a with nature approach of midwifery, believing in the natural strength and ability of women to give birth the natural way. This belief stands in contrast to a perception of a changing attitude in younger generation women who do not want to trust this natural birthing process. The client and her family are in this respect experienced as demanding and frustration is the feeling connected to this experience.
7.2.2 Demand to always give 100 percent service – regardless own feelings and condition
As discussed already in Chapter 6, midwifery is a human service profession where delay of service is not acceptable. A woman in labour and her family are in transition to a new phase in life, in the middle of a critical life incident. Naturally, she is self-centred, not having in mind that there might be some others also in expectancy to give birth.
Interview 6: 58 years old, 33 years work experience as midwife The midwife must smile and welcome even the third pregnant woman although she deep inside herself was hoping that the next woman giving birth could wait
195
two hours so she could “recover” from the last birth. It is in a situation like this where things get difficult; however, I think that they are doing a great job! None of our clients has made any complaints about midwives being in a bad mood or too busy to offer any service. It is not my impression at all.
Interview 8: 50 years old, 24 years work experience as midwife ... when you have been at work for 16 hours, and another pregnant woman shows up, you must show the same degree of commitment which you showed to the first two women giving birth.
The midwife’s role is described as committed to serve even after long work hours. It is the own work ethic and the expectation from the outside to serve even when it is beyond the available strength and power. The same professional service and empathetic engagement should be given to each woman. A further aspect described in the interviews is to ‘give something of yourself’. Connected to the understanding that midwifery functions on the basis of giving 100% and not less, it is thought that true 100% giving is not possible without being involved as a person.
Interview 3: 43 years old, 6 years work experience as midwife But you are forced to raise yourself up and say ahhh. And all the time being cheerful, sweet, and caring. And this might be what others mean by getting burnout quickly. The reason might be that you are in high gear all the time anyhow, and maybe you are not always the type. You cannot be like this all the time.
To deliver the same standard of service regardless of one’s own feelings and energies is an unchangeable demand in midwifery. There is not much space for having a bad day. Needing to be happy, understanding, and caring is considered as a probable reason for burnout. A difference between the demanded and the actual emotional condition is thought to lead to emotional turmoil after some time.
Interview 5: 49 years old, 8 years work experience as midwife A midwife is not allowed to have a bad day at work. You cannot say ‘ok’, I will just “take a backseat” today. You are on and you are being evaluated every time and forced to give everything you can. You give a part of yourself every time which cannot be done half. You can’t walk into the maternity room and tell your client that you are having a really bad day. Such remarks are useless. So just forget everything about that.
196
The demand to give something of one’s self is related to the demand to serve 100% in the sense that it is not asked if the midwife is ready to give or not, it is described as part of her professional work role. The interview participants refer to the aspect of giving as an implicit, but at the same time, very demanding part of their job. The picture of giving something of oneself is strong, expressing the emotional quality with which this situation is connected.
Interview 1: 38 years old, 14 years work experience as midwife To the question: As I understand, is there a possibility both of getting energy because of the primary task or to lose energy; can it go both ways? Is this something you can relate to? I would answer yes to that. It works both ways. I believe that … I really believe that you can have a positive birth process with couples having children where everything fits together. And they are having a wonderful birth and a lovely child, and their way of coping is just fantastic. It can really make you “high”. But generally speaking, I believe that your involvement in the birth is so deep that it drains you of energy which can make it difficult for you to have a private life with children because you pay so much attention the whole day that it makes it difficult for you to face family demands. You also need someone to care for you. After all, your involvement is much deeper than it really should be; and when you get home, you are completely drained of energy. However, it is difficult to say whether it is the job or the way we are working. If it is the work shifts and irregular working hours day and night and a family life at the same time, or if it is because you use all your attentiveness and empathy to facilitate the birth is difficult to say. I believe that things are connected though it drains you of energy. You are very tired when you have been standing for 8 hours trying to help a woman giving birth to a child. You are completely physically and mentally exhausted when you get home.
In positive birth processes - and even more so in difficult situations - the midwives need to give their full attention, empathy, and make use of their professional knowledge as well as intuition. In each birth process, midwives need to get physically and emotionally involved as well as be alert and highly concentrated. These high demands are experienced as tiring, especially when there are no possibilities for recovery. Moreover, facing family demands upon coming home and not being able to satisfy them in a sufficient way because the job has been too demanding is experienced as frustrating.
197
As way out of the spiral of giving 100% and at the same time working on the edge in regard to low recovery time, the draw back from clients is named. Not being in the mood to serve women in labour anymore is described as serious reaction to the extensive demand experienced over time.
Interview 9: 44 years old, 18 years work experience as midwife Sometimes I feel that I can’t stand these women anymore. They suck everything out of me and give me nothing in return. Then I simply don’t want to help them anymore.
The topic of treating all women with the same eagerness and concentration, while not showing any signs of exhaustion was also discussed in the group interview. Here the midwives confirmed that working in midwifery demands that they play a certain role where they need to display strength and power in order to lead through the critical life event.
Group interview IP 1: ….but we are in a different situation, we can not let go and go our way and let them stay alone, because we think we have had enough. There is nothing like this. As midwife you have to tackle a situation like this and you grit your teeth. There is no other possibility. … IP2: You must be nice and kind and always speak politely to the clients even if you are facing a breakdown. You must not show your emotion to the clients. A midwife “hides” herself in the white hospital coat and acts normally so she is able to deliver a decent product when the clients show up.
The interview participants describe the midwife as the one who is supposed to give the best service she can give. The personal demands of the midwife need to stay behind. It is the client who has the whole attention. The midwives describe and accept that the professional role at times demands that they keep going even when their own resources are low. In the second interview quote the midwife talks with some distance about the direct (woman in labour) and indirect (child to be born) recipient of her service. The delivery of a child is described as to deliver a decent ‘product’. The aspect of resignation and distance felt towards clients was not discussed further in the group interview.
198
7.3 Emotional reactions to traumatic birth incidences Traumatic birth incidences are a natural part of the job of a midwife. Giving birth is a natural process with a certain chance of failure. Even though modern times demand the control of nature in the best possible way, giving birth is maybe one of the archaic incidences to which there is no access to total control. In the interviews, it became obvious that traumatic birth incidences lead to emotional reactions (entanglements) which might have influence on the relationship between motivation and burnout. In the following three sections, the different challenges a midwife faces in regard to traumatic birth incidences are discussed. First, how the midwives experience the handling of traumatic incidences is presented. Second, the feeling of being responsible is described. Third, the aspect of healing and support after traumatic birth incidences is discussed.
7.3.1 Experience with the handling of traumatic birth processes
In the course of the interviews, the experience of and the dealing with traumatic birth incidences was reflected.
Interview 6: 58 years old, 33 years work experience as midwife I believe that pregnant women today really demand that nothing must fail or happen to them or their child. Moreover, they want the best service they can get. They want full “security” through the whole process.
This first statement from one of the interviews reflects a modern attitude of the birthing generation towards the birth process. Today, in the western world, most children are born without any major complications and even when they arise, a lot of help is available. Although this is a very positive development, it might have given rise to very high expectations, not giving room to the possibility that sometimes difficulties and even fatal outcomes are unavoidable. The midwives are therefore sometimes confronted with women who expect that all kinds of negative developments or outcomes during the birth process can be avoided. The midwives, however, know that things can go wrong and that they not always have a chance to avoid that happening.
199
At the same time, the midwives describe their own work ethic as a demand to provide perfect service even though they do not think that they necessarily have influence on the process to the end.
Interview 4: 45 years old, 20 years work experience as midwife ….This is also typical midwife, you take it upon yourself. Everything must be perfect, everything must be fantastically right, and it is living people we work with, nothing may go wrong. I have myself experienced that you get very sad when something happens.
Interview 2: 46 years old, 20 years work experience as midwife And I’m not only being evaluated on my skills. I’m also evaluated on my humanity. Moreover, I’m being evaluated on something which I don’t have a chance of influencing.
The foregoing statement refers to a feeling of humility and belief in some higher order. The midwives themselves use expressions like “there is more between heaven and earth” (see below) or “not having an earthly chance to make a difference in the process” in order to express their belief in something above their own capacity. In a secularized world with a longing for human control over nature, it is hard to transmit that every birth is a little miracle hitting the edge between life and death. It might not be by chance that the book about the 100th anniversary of the Danisch Midwife Association (Den Almindelige Dansk Jordemoderforening, DADJ) has the title “Fast ansat ved mysteriet” (“Employed in the miracle of life”, free translation by the author). Also in the group interview, the topic of dealing with traumatic birth incidents was addressed. Here the midwives discussed the difficult situation of not having the possibility to talk openly about mistakes that might have happened during the birth process. They refer to air traffic controllers who can talk about “near misses” without having to face any negative consequences, but instead can use the open talk about these incidences to learn and prevent similar situations.
Group interview IP 1: However, what really is the taboo is the usual problem that you refuse to acknowledge any faults at all. It is the serious discussion going on and on
200
forever about her fault-localization. The air line business offer all their employees’ openness which means that you can report everything, and they don’t blame you for anything afterwards, whereas the health care sector doesn’t offer their employees the same kind of openness, though it is getting better now. It is still something they want to remain in the delivery room with respect to traumatic incidences because the hospital fears it may ruin its reputation.
The participating midwives know that there are situations in midwifery that are not possible to control from every side and there are also critical situations that happen because somebody was too late to react. The situation in midwifery today, as described by the participating midwives, is as follows: In competition to be the safest place to give birth, near misses (to use the technical term from air traffic control) are kept under the seal of secrecy. Midwives, being part of a traumatic birth process, face a double burden. They have to emotionally deal with the incident and they are not allowed to talk openly about what has or could have happened.
Group interview IP 1: Some of us have tried to receive a letter where someone is complaining about you. Sometimes you are so lucky that things couldn’t have been done any differently, or it may be that things could have been done differently. I find it all right that we are held responsible, but the fact that you risk someone taking legal action against you, or you risk a fine, is scary. We are not talking about gross negligence but about situations that cannot always be controlled. Your whole world can break down under such circumstances! … Things are becoming more and more “Americanized” which is becoming more and more obvious, and I find that very difficult to tackle. … however, it is just as if it doesn’t get into their heads which I believe is dangerous because it can knock them off their feet!
The midwives feel that they are faced more and more with an accusation culture. The midwives discussed this aspect as an Americanized way of looking for somebody who is not only responsible but also convictable. This leads to a climate of not talking about incidents which are inherent to the job and which need openness in order to be able to react in a good manner the next time something similar happens.
Group interview IP 1: And that’s a very difficult situation! I believe that there is a tradition among midwives to tackle difficult situations. We know that there are more
201
things in heaven and on earth that are beyond our control and responsibility, and more than we can tackle. So it is not our fault! Sometimes when you walk home from the hospital, you can ask yourself about what you could have done differently; but after a while, you realize that it wasn’t your fault. Fortunately, we come out as healthy8 individuals on the other side, but I believe that when someone is complaining about you because they believe that you have made a mistake, it can sometimes make you break down. But if we get some time where we have the possibility to talk about it, it might be possible to get through some things without the big professional help.
The interview participant describes the fact that midwives know that there is more between heaven and earth and this knowledge enables to stay whole as a person even after having been part of a traumatic birth situation. Moreover, openness is needed to stay whole as a person and to be able to get over such an incident. When traumatic incidences are condemned to be kept in silence, it is the midwife who is left with the burden of tackling the question of responsibility and guilt alone. It is regarded as important by the participating midwives to talk about the traumatic incident as part of the “therapeutic” process, to learn from it, and to share grief and sorrow about the outcome.
7.3.2 Feeling of responsibility and guilt
Responsibility is often the immediate feeling described in connection to difficult or even fatal birth processes. Especially in unforeseen fatal incidences, feelings of responsibility or even guilt can arise. The midwives also report feeling responsible even without having the formal responsibility. Finally, there is the feeling of being responsible for supervising clients and their families who have experienced a traumatic birth process.
Interview 4: 45 years old, 20 years work experience as midwife Of course you experience traumatic birth incidences where either the child is dead or the mother almost dies, and the whole birth process becomes so terrible that it affects you mentally afterwards and sometimes makes you feel guilty though it isn’t necessarily your fault, Midwives are like that – we feel guilty! We want everything to be perfect and correct – it is living human beings we are dealing with. Nothing must go wrong. I have also felt terribly sad sometimes.
8 Healthy is here used in the sense of being emotionally in one piece.
202
The citation above reflects in a comprehensive way the emotional entanglement when thinking about responsibility in traumatic birth situations. Emotionally, the midwife goes through a variety of feelings, which reach from being puzzled to feeling guilty. Traumatic birth situations are often not clear in respect to who is to be made responsible. The feeling of being responsible or even guilty is described as the immediate and most consistent feeling connected to an incomprehensible birth process with a negative outcome. Midwives are described as taking this responsibility upon themselves, also with the consequence of emotional strain.
Interview 3: 43 years old, 6 years work experience as midwife Another thing is when I have assisted women in delivering a stillborn child where they already knew the child was dead. In a situation like that you must act professionally. You feel terribly sorry for the parents and you must of course … it is so terrible, particularly when the child is perfect and it is dead. However, you can’t walk around with this sense of guilt that you have done something wrong. You feel guilty when you are carrying a dead child in your arms and have to tell its parents or the father (who sometimes hasn’t participated in the birth) that their child is dead. Interview 9: 44 years old, 18 years work experience as midwife It is extremely difficult to assist a woman in delivering a stillborn child. The worst situation for a midwife is when a pregnant woman is carrying a live child in her stomach when she arrives and delivers a stillborn child. It is the worst thing that can happen to me!
The midwives refer to two different situations facing traumatic birth processes: foreseen and unforeseen. The foreseen situation, for example when the child has died before the birth process started, is easier for the midwives to handle with a professional approach without being strained by feelings of responsibility or guilt. In contrast, this professional mind-set is much harder to hold on to in unforeseen traumatic situations. As one midwife described it, the worst case is when a woman delivers a stillborn child even though she and her unborn child were apparently in good condition when they came into the hospital. Here, a feeling of uncertainty can arise and the midwives might start asking themselves if they could have done something different in order to avoid the fatal outcome.
203
Another difficult situation can develop in those cases where a doctor is called in and the midwife passes on the responsibility to him/her. According to the role definition, she is at that point no longer responsible. Instead, she takes the role of the woman’s advocate in communication with the medical doctor, telling him/her how the process has gone so far and what her recommendation would be. She can discuss further steps but cannot make decisions contrary to the doctor. This is regarded as a difficult position, because the midwife is involved but does not have the power to make the final decision. The ambivalence of giving responsibility away by calling the doctor but at the same time still feeling emotionally responsible for the birth process, can be unsatisfactory and might lead to insecurity about one’s own action. In any case, when a child dies or gets seriously hurt in the process of delivery, it is experienced as worst case, as catastrophe.
Interview 1: 38 years old, 12 years work experience as midwife Some years ago, I assisted a woman in a twin birth at a time where I was pregnant myself, and where everything went wrong with child B. Despite that the woman was open by 4 cm, I recommended a caesarean section. However, the doctor was not of the same opinion as me. The woman opened quickly and child A was taken with a ventouse; however, child B didn’t come down which made it impossible for the mother to deliver him. When he finally came down, it was with the bottom first and we took a scan which showed that his heart rate was fine but the amniotic fluid was green. After we had tried to get him out for half an hour, the doctor finally recommended a caesarean section and the woman was given an epidural which she never should have had. And she had a child in a very poor condition. He suffered from brain damage and was almost dying but survived. It was a terrible story. But to be in a situation where you disagree with the doctor and where you don’t have the authority to make a difference is terrible. I later realized that I could have called for one of the chief physicians at home but it takes a lot of courage to say to a doctor that you completely disagree with him, and that you are going to call one of the chief physicians. Today, I would have done it, but at that time, I wasn’t so sure because I was in doubt. The rule is that when the birth process is normal, the midwife is responsible. And when the birth process isn’t normal, the midwife calls for a doctor and the birth situation is no longer her responsibility. In a situation like that, it is difficult to be the woman’s advocate in a process you had to let go of.
The interview section above refers to the conflict of being torn between formal and felt responsibility. Formally, the midwife was not responsible for the outcome of the case. She had called for a doctor early in the process and it was
204
the doctor’s decision to wait with the c-section against the recommendation of the midwife. Nevertheless, the midwife still feels responsible for the process and asks herself what she could have done differently to prevent this traumatic outcome. It is said by the midwives that some of the traumatic incidents with unresolved feelings of responsibility can develop their own psychological power, inducing insecurity and fear. They can accompany a midwife all through her professional life, being something like critical life incidences. In situations with high emotional impact, it might not really matter who was responsible. The feeling of having lost control over the birth process stays the same. Another aspect of felt responsibility is the ambivalence over how much involvement and care needs to be given to a mother or a couple who has been through a traumatic birth process, at the end losing the child or ending up with a handicapped child.
Interview 7: 48 years old, 12 years work experience as midwife You may back out saying that you’ve had enough and want to stop. However, I must admit that there are certain incidences which I find it difficult to let go of. There are incidences where I have given them my telephone number and asked them to call me if they need to talk. Some of our clients really have a need for talking very often. Sometimes I have called the clients after a couple of months just to hear how they were doing. You always have a talk with them after a month. That’s the least you can do. You also pay them a visit after a month to hear how they are doing. Anyway, it can last for years. The last incidence I had lasted for 1.5 years. At last I just called to hear how they were doing. She always sounded so happy every time I called her, and she really needed it. They are so grateful to you because it has been such a traumatic and difficult situation in their life.
There is a mandatory follow up call or visit from the midwives’ side a month after the traumatic birth incident. There also is a felt responsibility to follow up with those families who seem to need more support over a longer period of time. A formal demand (call one month after the incident) becomes an informal obligation to follow up and care for those who seem to need it. The regular working time usually does not cover the invested resources (emotionally,
205
mentally and time). So the midwife is torn between wanting to give more support to those who she feels need it and investing her own time and resources in order to do so.
7.3.3 Support and healing after traumatic incidences
In the following, different ways of handling and coping with traumatic incidences and the related consequences, as referred to by the midwives, are presented.
Interview 1: 38 years old, 12 years work experience as midwife Maybe it is something that makes you feel burned out after a certain number of years. You have been involved in so many traumatic incidences and you have never had a chance to discuss them with anyone. Sometimes you discuss it with someone in your private life or with your colleagues after work but it never really get paid much attention to; and it is expected that you keep on working just as if nothing has happened. Of course they feel sorry for you for about three days but then you have to move on. We have all tried that. It is expected to be like that. … No, I’m more of the opinion that it is about what can be tolerated or not … working as a midwife is a job and you have to act professionally. Of course it is both traumatic and terrible when a child dies, and it can make you sad for about a week. But then it is expected that you start all over again and help other women with their delivery. The first time you’re involved in a traumatic incidence, your colleagues may show up a short time after and ask you if you’re all right and if things went well and so on. However, after some time, they forget that you have had a traumatic incident where you either lost the child or watched it die. It has also something to do with the fact that it is not the same people you’re working together with all the time. If you are at work on the same day one of your colleagues is involved in a traumatic incident, it is brought to our attention of course. But you haven’t been part of the whole birth process and the experience, which can be a problem when you have to discuss a traumatic incidence you have just heard about through your colleagues a whole week later. And all of a sudden you are on duty with the one who had the traumatic incident! After three weeks or so … , the whole incident is over and done with. However, the traumatic incident is not over for the one who went through it. It keeps haunting her for a long time after.
The interview participant talks about the difference in time it takes to heal from the inside in relation to the time given to heal as a professional. One problem with traumatic incidents is seen in the difference between one’s own feeling
206
after a traumatic incident has happened and the organizational expectation of how to react to it. There is actually not much time given to cope with traumatic incidences because of busy shifts and changing personnel working together. There is an expectation from the working environment to be back on track after a relatively short period if time. The emotional body, on the other hand, is described as being slow in getting over a severe incident. In consequence, traumatic incidences are banned to stay unresolved. This can in accord to the participating midwives lead to serious problems as more and more such incidences need to be stored in a “subconscious” state. In the end, in this midwife’s view, these unresolved experiences can lead to burnout.
Interview 7: 48 years old, 12 years work experience as midwife It takes up a lot of your time, and you keep asking yourself whether it is right or wrong. It is nice, but I also understand those colleagues who break down because you are so much involved, and you can’t just walk home and say - well, that was that!
The job of the midwife demands a very intense way of being involved in the job. The high load of emotionality is experienced both as gift and as challenge. Being a midwife keeps you emotionally attached beyond the regular work time. The midwife takes emotionally strong experiences (positive and negative) home with her, which than can cost a lot of personal resources and resources of the personal network (husband, children, friends, and relatives).
Interview 4: 45 years old, 20 years work experience as midwife With respect to “out-of-control” and terrible deliveries, I also believe that your colleagues feel and know that something is wrong. They have either heard about it or even participated, or it may simply be the case that they feel that something is wrong. I think that we are very good at observing when something goes wrong and giving each other social support and a hug when it is needed. I really believe we are good at that. To observe when something goes wrong and to be there so that the person involved really feels that you are physically present. Another important aspect is the discussion about what did you do, and tell us what happened next, and who did this and who did that, and he (the doctor, sen) didn’t have to do it like that etc. To try and have a discussion about how well your colleague coped with the situation! If it’s possible at all, try to be there and offer your colleague social support when she comes out from the delivery room after a terrible incident. There is always somebody there to offer you social support, and if you don’t feel like talking, the person will just remain silent and be there for you. I think that’s very important. Going home sometimes makes
207
things much worse. It’s not everybody, who has someone to offer them social support. I just have to say this and that, and then my husband knows what to ask and how to ask; but not everybody has that opportunity. It’s not everybody who has a husband or a husband who can give their wife social support and is good at listening! Some midwifes just walk home and sit there alone! They don’t get any feed-back until they return to work again, and then you risk that your colleagues have forgotten about your experience, or maybe your colleagues at work that day haven’t heard about it! That’s no good at all!
It is described as important to work things through, talk about the traumatic incident and take the time to recover. This is not always possible and the overall structure of a person’s life can be supporting, challenging, or hindering in this respect. Midwives react very differently to such incidences. One group is described as thinking that it is a sad part of the job, which has to be taken into account with some professionalism. Others are described as getting deliberately personally involved in the history of parents and families who had to go through a traumatic birth event. A third position is described as acquiring a strong professionalism in order to be able to handle these traumatic incidences in a more distanced way. Altogether, it is regarded as a job demand to be able to handle traumatic incidences and to develop the capacity to digest them. The form of social support on the job is described as being existent ‘in the moment’. The midwives try to support each other when having been through a traumatic incident. Yet there is some implicit expectation to be back on track after a short period of time. The support is described as physical, as “being there”, as supportive in the sense of short term relief from questioning one’s own professionalism. However, as soon as the shift is over, it is hard to keep track on those who have had a traumatic experience. The formation of teams changes from shift to shift and it is not easy to maintain continuity. There exists a form of peer debriefing after a traumatic incident, but there is no formal offer of professional psychological help yet. However, during the study period, a psychologist was employed at the ward for a limited period of time in order to give quick professional support to those who have been impacted by a traumatic birth incident. The midwives were positive about the psychologist’s work and
208
hope it will continue after the pilot phase. Collegial support happens on a different level than professional psychological support. Collegial support as described by the participants has an affirming character. Affirmation is given about the actions and steps that have been taken throughout the traumatic birth process. This mainly has a relieving and supporting function. Healing from traumatic incidences takes a longer time and more effort in working things through and maybe accepting one’s own fallibility. Social support in this sense is not described as a sustainable form of support throughout mourning and healing. Healing processes take time and need professional support. Both forms of support have an important role in the processing of traumatic incidences.
Interview 4: 45 years old, 20 years work experience as midwife The kind of supervision where a midwife is called directly by the supervisor and which our supervisor tries to manage, is missing as a formal structure. But sometimes she is not present or she has no time for offering social support or maybe she hasn’t heard about the traumatic incident. She calls you and asks if you need to talk, if you want her to come home to you, or if you want to come to her instead, or if you need a psychologist. We want to do something extra. However, it doesn’t always work
Supervision as a step in between social support and professional psychological help has, until recently, not been used as a form of support in the case of traumatic incidences. After the first round of the PUMA investigation, two colleagues were professionally trained to give collegial supervision. This form of supervision is thought to be first help at hand after a traumatic incident has happened. However, experience so far has shown that this form of collegial support is not asked for. This is frustrating for those who went through the education to become a supervisor. At the same time, it is interpreted as a sign that collegial support is not the right way to approach the issue.
Interview 1: 38 years old, 12 years work experience as midwife Debriefing in connection with traumatic birth processes, specifically traumatic birth processes, is new. But they don’t use psychological help, which I believe is missing. You are missing in relation to … the fact that you feel a heavy responsibility being a midwife? And you do. Though a doctor comes in and performs an operation, you still feel more or less responsible for what he or she is doing. You need some kind of follow-up in a difficult situation like that.
209
In relation to the responsibility a midwife has and feels - the support she gets when something happens during a birth - is experienced as insufficient. Collegial support is there in the moment and is experienced as helpful. Debriefing is experienced as a first step of getting over a traumatic incident but is not viewed as particularly helpful on a deeper level of emotional trauma. Psychological help offered to the single midwife is being tested at the moment at the case site by a psychologist employed at the ward and might be an important step in finding a sufficient way to support midwives after a traumatic birth incident. Besides the difficulties and shortcomings related to the support and healing after traumatic incidents reflected in the statement below, it should be mentioned that one midwife described a growth in coping capacity over the years. She describes a feeling of ‘getting used’ to and being more able to handle traumatic incidences with growing experience on the job.
Interview 5: 49 years old, 8 years work experience as midwife I really believe that your mental resources increase concurrently with your education. The first time you experience a stillborn child, you feel terrible several days after. I’m sorry to admit it, but after you have helped delivering the tenth stillborn child; your attitude has become more professional. It still affects you emotionally, but you don’t break down so easily anymore. I believe that you grow concurrently with your independence, and I also believe that it takes a lot to upset a midwife! People don’t expect that, because they believe that giving birth is always a happy event! Giving birth is a happy event in most of the cases; however, there are many situations where the adrenaline pumps in your veins and you have to be very alert all the time, and that’s not always a happy event! But you get used to that as time goes by.
In the group interview, the midwives describe themselves as being good at giving support to each other because giving support and holding onto somebody in a crisis is the core action when fulfilling the primary task as midwife.
Group interview: IP: What is it what we do every single day, 8, 10, 12, 14, 24 hours in a row? We stand at the labour ward and we bear, and we lift up and we support and we hold onto. This is what we do, this is our job. And this is also what we do as soon as we get home from work, maybe not directly at home because home is the place where you have the space to break down sobbing. But in all other contexts you
210
do, it is typical midwife to say: because of this, I will do it and come on; we can get over it together. This is what we do.
The collegial support is reflected by the midwife on the background of the competencies connected to the fulfilment of the primary task. Besides the capacity to give support to each other, it was confirmed in the group interview that emotional trauma is common in midwifery even if it is not an issue to be talk about. The aspect of healing was brought up as being important in case of emotional trauma. Healing can happen in different ways. The most direct and cleansing way to heal from the inside is described as crying.
Group interview IP 2: We cry. Well, I feel to really cry through something is a real cleansing process. It does not happen that often, but when you have been totally down and out and have cried through the whole process, than you are washed from the inside, almost, and than you are ready again. So, I think, this is really good when it is too much. In any case for me it is a good thing to cry through these phases. And I also think there is the aspect of time, and than you also have a lot of security nets you can establish for your own sake, so that the probability to come into a traumatic situation another time is low. In these situations you check over and over again with all kinds of technical devices, and the doctor is called 117 times – you establish all kinds of security checks in order to heighten the security you can at all establish.
Being able to shed tears about a disturbing emotional experience is described as relief and a healing path. Beyond that, it is important to have time to get some distance from work at the ward, find time for meditation, and time for healing in order to built up new confidence in one’s own competence and knowledge again.
Group interview IP 2: If you have been involved in a traumatic incident, you need time to recover. You feel deeply involved in the crises, and you need time for healing and find your confidence, competence and professional way to tackle problems again. You believe that you can do things in a safe and competent way. You need time to find out if the help you offered the pregnant woman (and her husband) really was the best help she (they) could get. You need time to find out how they are getting along with their lives after a traumatic incident. And you need time to return to your workplace and talk with your colleagues and find your own self again, and slowly get back to work. A traumatic incident is a major drawback for your career where you don’t feel certain about many things.
211
Your faith and way of doing things are shaken during such emotional crises. You need to start all over again.
The aspect of healing and how healing can best be achieved added a new perspective to the discussion about how to handle traumatic birth incidences. Healing adds a second dimension to the question of how to deal traumatic birth incidences in a healthy way. Being able to express sorrow and having time to do so is experienced as important step towards “becoming whole again”. 7.4 Summary of findings concerning the role of emotional demands and feelings in midwifery In the course of the interviews, emotions were mentioned in relation to emotional demands connected to the primary task in midwifery and as feelings as reactions to traumatic birth incidences. The first aspect discussed in regard to emotional demands in midwifery is the difference between one’s own professional image in regard to service given to the clients and the clients’ appreciation of the service. The midwives report a rising trend among the current birthing generation of coming with their own ideas about the birthing process which can often stand in contrast to the midwives beliefs, professional knowledge and experience. Emotions related to this aspect range from bewilderment to frustration. Frustration is also expressed about the recent birthing generation not giving recognition to the service they get from the midwives. At the same time, the participating midwives refer to their job as demanding 100% service for the clients. Connected to this demand is emotion work in situations where one’s own feelings and conditions stand against the explicit job demand of treating each woman in labour with the same eagerness, concentration, and not at least empathy. The midwives refer to the demand of giving 100% service as ‘giving something of yourself’, which is used as a metaphor for using intuition, empathy and feelings whilst fulfilling the primary task. This demand is experienced as tiring, especially in situations when time to recover is not available. As reaction to this demand, the midwives described a
212
reaction of drawing back from clients as way out of the vicious cycle of re-action instead of action. Experiences with the handling of traumatic birth incidences were discussed as partly incompatible understandings by client and midwife. The participating midwives felt humility towards something beyond human influence when at the same time clients nowadays were described as often demanding high level of security throughout the birth process. The midwives also report often feeling left alone after having experienced a traumatic birth incident. The demand to return to “work as usual” as quickly as possible and a missing support system for coping with these experiences were discussed. References to air traffic controllers were made, who have the option to talk about “near misses” in order to learn from mistakes and prevent them in the future. The midwives instead experience an atmosphere which does not allow them to talk openly about “near misses” or even mistakes. They therefore feel a double burden of feeling left alone with their coping and an atmosphere of denial. As a theme in its own right, emotional reactions to traumatic incidences were discussed. First, the feeling of responsibility for one’s own actions in the birthing process as well as for those of others was addressed. Feelings of responsibility and guilt were drawn out by the participating midwives. A difference was made between foreseen and unforeseen traumatic birth incidences. Unforeseen incidences were seen as being tragic and more traumatic for the midwife in regard to her professional ego. The midwives also reported difficult situations in which they feel torn between formal and felt responsibility. Although, formally, they are no longer responsible once they have called a physician to take over a difficult case, the feeling of responsibility towards the woman giving birth often remains. Another aspect of felt responsibility discussed was the question of how much support and consultation needs to be

213
given to a woman and her family who have lost a child in the course of birth after they leave the hospital. The mandatory support – one phone call one month after the incident – is regarded as not being sufficient by some midwives. Some therefore choose to invest a lot more time for follow-up, which often is not covered by their regular working time. These midwives feel a discrepancy of formal rules and feelings of responsibility. The third point of discussion in respect to traumatic birth incidences was the support given to midwives and the healing process after having been part of a traumatic incident. The midwives stated clearly that the support they receive to recover from traumatic incidences is insufficient, especially when looking at the responsibility they have while helping to give birth. Some midwives mention that they can understand how these unresolved experiences over time can lead to burnout for some of them. Moreover, the interview participants reported a gap between time given to heal and the actual time of a healing process after severe trauma. The organizational demand is to be back on track after a short period of time (2-3 days) whereas personal time to heal often exceeds the rather short break a midwife is allowed to be absent from normal duty. The high emotional involvement of the midwife doing her duty can lead to spill-over effects to other life spheres (especially home and family). The personal social structures available to a midwife are seen as either possible sources of support or hindrance in respect to coping with traumatic birth incidences. Support given from the worksite is deemed insufficient. Although the informal collegial support is experienced as helpful, many report that it is not enough. The supervision by colleagues who went through special training for these purposes did not have the expected effects because there seems to be a need for more consistent and more professional supervision and collegial supervision is also discussed by the midwives as critical in regard to be open about own fallibilities towards a colleague you daily work with. Nevertheless, some midwives also report having been able to develop coping skills in dealing with these situations by retreating to the skills and abilities of the professional role and not the
214
emotional competencies as part of this professional role and therefore emotionally distance themselves from the immediate experience. In summary, emotion work showed to be a core theme in the single interviews and this finding was supported in the group interview. Implications of the different emotional demands and feelings related to the primary task in midwifery are discussed in Chapter 8.
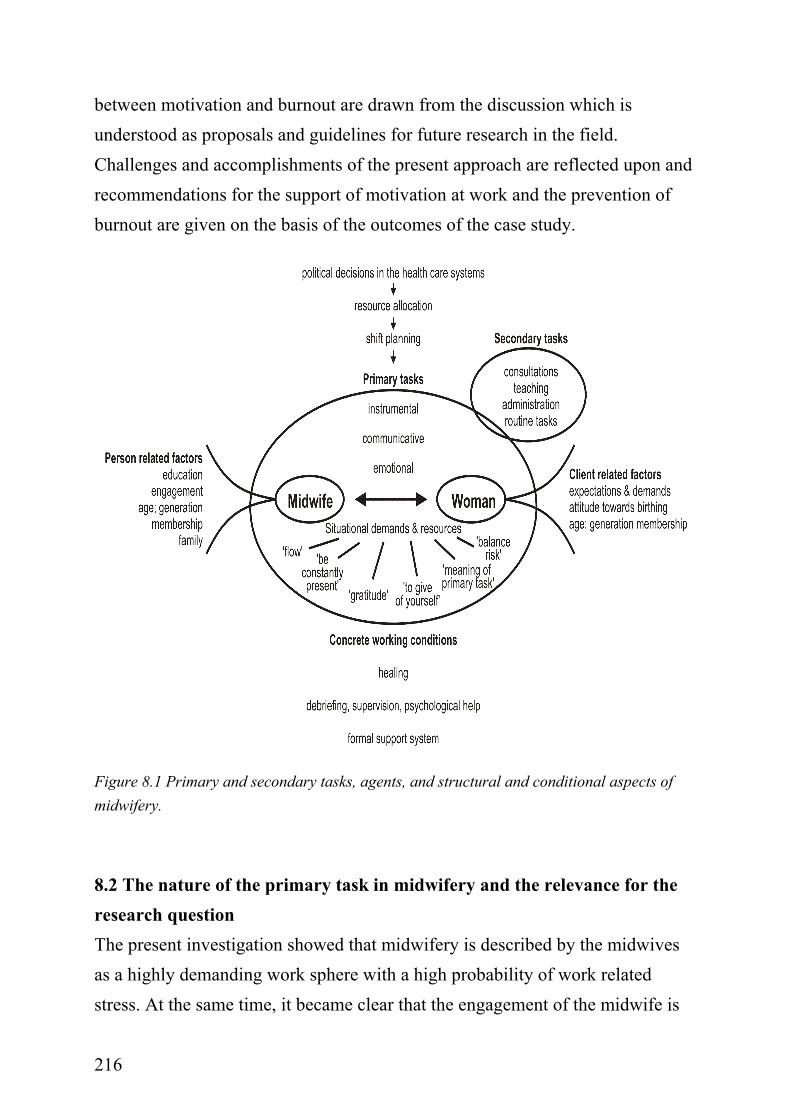
215
Chapter 8: Discussion 8.1 Introduction Findings from the present case study using participant observation, single interviews and a group interview as method are numerous. Due to the qualitative approach, a thick description of the research field has been reached, giving access to a complex understanding of the multifaceted relationship between motivation (engagement) and burnout in midwifery. Thinking out of the box of traditional research in both fields yielded expected and new insights. Burisch (2002, p.16) concludes his description of a longitudinal study of burnout in nursing with the following sentence: “It seems entirely possible, however, that major breakthroughs can only be expected from much more in-depth studies of individual cases” (italics set by the author, sen). This conclusion is also shared in two other theoretical reviews of burnout research (Schaufeli & Enzmann, 1998; Rösing, 2003) and putting this into research practice was taken seriously in the present case investigation. The in-depth investigation of the relationship between motivation and burnout in one particular field of human service work can be described as an explorative approach to a research field (burnout research) which has been studied over the last 30 years. The case approach opens the door to a more thorough understanding of the relationship between motivation and burnout in a specific context and new ideas have indeed emerged as a result of the present case investigation. The results introduced in Chapters 4 to 7 are discussed in the following. Figure 8.1 summarizes the different findings and sets the primary task in midwifery, described as helping to give birth, in the center of discussion. On the horizontal axis, midwifery in Denmark is described along the demands and resources inherent in the primary task. Furthermore, person and client related factors influencing the fulfilment of the primary task are discussed. On the vertical axis, the structural and organizational setting is represented in regard to the research question. Assumptions about how to understand the relationship
216
between motivation and burnout are drawn from the discussion which is understood as proposals and guidelines for future research in the field. Challenges and accomplishments of the present approach are reflected upon and recommendations for the support of motivation at work and the prevention of burnout are given on the basis of the outcomes of the case study.
Figure 8.1 Primary and secondary tasks, agents, and structural and conditional aspects of midwifery.
8.2 The nature of the primary task in midwifery and the relevance for the research question The present investigation showed that midwifery is described by the midwives as a highly demanding work sphere with a high probability of work related stress. At the same time, it became clear that the engagement of the midwife is
217
nurtured by the positive experience connected to the primary task. The primary task is described as the core drive and the only reason to accept the unfavourable conditions of the job. Putting the primary task into the center of the discussion links the variety of findings of the present case investigation in a significant way. The following discusses essential characteristics of the primary task, task related demands and resources as described by the midwives. It refers to related research, pointing to the aspects in common and to the uniqueness of the present approach.
8.2.1 Essential characteristics of the primary task
The primary task in midwifery is specific in comparison to other tasks in the human service work. The list of aspects in midwives’ psychosocial work environment as proposed by Dyhr (1999, see Chapter 3) are used as a guideline to describe the relevance of the primary task. The acute nature of birthing might be comparable to cases in an emergency ward. The same is true for the necessity of working in shifts, 24-hours, and all days of the year. Clients in midwifery are in a life crisis. This crisis is different from an accident crisis as it is basically a positive crisis with a rather small probability of a negative outcome. At the same time, the possibility of a negative outcome is a constant threat, and has an impact on the way midwives establish nets of security. Those partaking in birth processes (most often the husband, partner, and family) are involved just as in other acute life situations. In the case of birth, the involvement happens to be planned, as today most men explicitly want to take part in the birth process. In contrast to other settings, the involvement is proximate. This both supports as well as hinders the work of the midwife in the sense that she needs to communicate not only with the woman in labour in this acute situation but also with the surrounding network present at the ward. Midwifery traditionally is also characterized as work done alone. On the other hand, it was observed in the present case investigation that midwives use their colleagues for discussion about birth processes when meeting in the staff room. There is a constant
218
rumination about how to proceed, using each other to confirm actions taken and to give support for decisions made. In the center of the primary task stands the relationship between midwife and client. In contrast to other human service settings, this relationship is described as being intimate and at the same time of rather short duration. Due to modern hospital organisation in Denmark, midwife and client see each other for the first time at the labour ward even though midwives have an active role in prenatal care as they see the pregnant women several times throughout pregnancies. The midwife, being the facilitator in the process of birthing, needs some outstanding communicative skills in order to establish a trusting relationship (‘rapport’), described as essential for a good birth. As soon as the child is born, the contact between midwife and client formally ends. In relation to the intimacy shared between client and midwife, this abrupt cut seems to be inappropriate and stands in contrast to the emotional involvement demanded. Midwives share the idea of giving best service when their task of helping to give birth is embedded in a system which provides continuity of care deVries et al. (2001). Midwifery practice in Denmark today is forced to make compromises in regard to this principle. This is mainly due to the organization of birth in larger birthing units as part of or connected to a hospital.
8.2.2 Demands and resources related to the primary task
The nature of the primary task leads to the following unchangeable work demands reported by the midwives: constant, 100% attention when on duty, shift work which includes nights and emergencies, the need to utilize the own body as an instrument while helping to give birth, giving something of one’s self as one form of emotional demand, the ability to handle traumatic birth incidences, and the skills to balance uncertainty and security. Demands related to the primary task in midwifery are specific to the way birth is recently organized in Denmark. The present case investigation made explicit that the
219
work demands which are thought to cause burnout need to be discussed in relation to the resources inherent in the primary task. Resources named in the present case are the meaningfulness of the primary task and the positive energy drawn from good birth experiences. Recognition from clients was named as a further resource. Resources interpreted in this sense, are the source of motivation to stay present and serve 100% even under demanding work conditions. For the well-being of the participating midwives the balance between resources and demands shows to be of particular importance. Imbalance occurs when resources are diminished. Two widely known theoretical models of work place stress are the demand-control model (Karasek, 1979; Karasek & Theorell, 1990) and the effort-reward-imbalance model (Siegrist, 1996). Both models are used in the following to exemplify the demands and resources related to the primary task in midwifery as found in the present case study. The demand-control model (ibid) identifies the relation between job demands and job control as the main aspects causing work related stress with negative effects on health. High work demands and at the same time low control (so called high-strain jobs), is thought to have negative consequences for health and well-being. Dyhr (1999) used the demand-control model as a research frame to investigate the psycho-social demands in midwifery in Denmark. The investigated midwives showed to be in the high-strain quartile. In the present investigation, high demands with corresponding high as well as low resources were reported by the participating midwives. In accordance with the demand-control model, this leads to the conclusion that being a midwife as described by the participating midwives is a high strain, active job, being both stressful and a positive challenge at the same time. Negative as well as positive aspects are described as essential characteristics of the primary task. Besides the description of the demanding aspects of midwifery, the findings of the present case study point to the importance of the positive aspects of the primary task which give energy back to the midwife.
220
The importance of these kinds of work resources is formulated in the job demands-resources-model introduced by Demerouti et al. (2001), enlarging the perspective of the demand-control model. Demerouti et al. (2001) could show that the development of burnout is determined by a specific constellation of working conditions. According to the model, exhaustion increases when job demands are high, whereas disengagement is higher with low resources. At the same time, disengagement is not an outcome of exhaustion but is related to the shortage of resources. Taking the job-demands resources model as a perspective from which to interpret the findings of the present study, it can be stated that the model fits the subjective descriptions that the midwives gave in both the single interviews and the group interview. Exhaustion was referred to when specific job demands were discussed. It was described as a short-term state of low energy, which can be regained through sufficient time to unwind from stress at work. The primary task was described as the main source of positive energy in a highly demanding work environment. Low resources are experienced as threatening to this positive work experience, because service quality, which is highly valued by the participating midwives, becomes the buffer between low resources and high demands. In other words, midwifery practice in Denmark is characterized by high demands with at the same time task inherent resources being present. Some of the task inherent demands can be interpreted as resources and resources can also turn into demands. Most important resource in midwifery is with no doubt the meaning of work done by a midwife when fulfilling the primary task. A further point in regard to resources is the intimate contact to the client and the gratitude the midwife gets as reward for her engagement. Especially for the older generation of midwives interviewed here, recognition from clients is seen as a valuable resource. However, this resource is diminished by the attitude towards giving birth shown by the recent birthing generation (see further discussion in Section 8.4). As another job related resource, secondary tasks in midwifery were named. Consultations with pregnant women, teaching maternity
221
classes, and even otherwise disliked administrative duties were described as welcomed time-out from the need to be constantly present while helping to give birth. The importance of the secondary tasks reported by the midwives emphasizes the necessity to unwind from stress at work. The importance of unwinding in order to be able to cope with job-related stress is found elsewhere in the literature (Hobfall, 1989; Frankenhaeuser, 1991; Mejman & Mulder, 1998; Sonnentag, 2001). Finally, some of the characteristics known from flow experiences (see Chapter 2, Section 2.3.3) are described as resource inherent in the primary task in midwifery. Yet in contrast to other activities which elicit flow states, midwifery is also characterized by the structure and organization of the primary task: the high workload and related to this the need to be present at different places at the same time as well as the presence of a partner in dialogue. These two conditions are seen as hindering for states defined as flow experience. High workload leads to short intervals of task fulfilment before rushing to the next client. Moreover, the intensity of client contact is different from tasks which can be done in meditative contemplation. At the one side can client contact evoke states of ‘feeling high’, comparable to flow states when a feeling of reciprocity between client and midwife is present and the rapport to the client is good. On the other side hinders the presence of the client a state of deep concentration because the midwife needs to react to signals of her client. Furthermore, helping to give birth is described as an engaging task with clear goals and a high focus of attention. The effort-reward imbalance model (Siegrist, 1996, 2004) describes humans’ strive for balance between demands (efforts) and rewards. Siegrist defines three different types of reward which together form the reward category of the model: income, job security and rewards from colleagues and supervisors. A prolonged imbalance between high efforts and low rewards is thought to lead to negative health consequences. Important in the relation to the present case seems to be that midwifery is a highly demanding job with at the same time seemingly low
222
reward and recognition. The three reward categories defined by Siegrist can be described as following with regard to the midwives studied: (1) income which is seen by the midwives as too low; (2) work security, which is objectively high at the moment (many positions are vacant) but is viewed as somewhat lower by the midwives themselves. The discrepancy between the objective state and the subjective appreciation might be due to the role unclarity felt by the participating midwives. Due to frequent, recent changes in the maternity ward at the particular case site, the participating midwives expressed some confusion about the definition of their own work role. Confusion here refers to one’s own state of mind in the sense of ‘willingness to do the job under these conditions’ not as confusion in regard to the role while fulfilling the primary task. (3) The third category is the recognition from leaders or colleagues which was not explicitly discussed in the present case investigation. Nevertheless, support from leaders was mentioned by some midwives as being good; others felt low support from the leading side. Furthermore, the midwives mentioned the importance of recognition from clients as being very important for them. Especially the older generation of midwives described it as highly rewarding to get recognition from the client. A further, important aspect which might be seen as a category of reward in midwifery is the meaningfulness of the task. Helping to give birth is essentially meaningful as it facilitates the child’s first entry into life. It is a challenging, and at the same time, fulfilling task. Even though the participating midwives reported a form of getting used to being present “at the mystery of birth”, the meaning drawn from this task has shown to have great importance for the participating midwives. To be present at birth outweighs many of the unfavourable work conditions in midwifery. This strong emphasis on the meaningfulness of work would explain a contradictive finding in the PUMA study where high levels of meaning of work and high quality of leadership were associated with higher levels of burnout in the 3-year follow-up survey (Borritz et al., 2005): Good leadership quality and meaningful work might keep people with a high level of personal burnout on the job (which was the case for the group of midwives participating in the present case investigation, see Table 3.1).
223
A different explanation is that high quality of leadership and a meaningful work task keeps a group who has shown to be overly dedicated and to have an exaggerated feeling of responsibility longer in the job because of a feeling of ‘owing good performance’. Both assumptions must stay on surface as the present case investigation did not investigate the theme leadership in depth. In conclusion, an imbalance between demands and resources has a negative impact on health and well-being. From the findings of the present study, it seems safe to assume that the recent changes in midwifery have impact on the balance between demands and resources. These include: reduced professional and personal recognition of the midwife helping to give birth as well as mothers’ increasing dependency on external help while giving birth, such as epidurals (described by the midwives as “Prinsesse Alexandra-Effect” because the rate of epidurals went up after the princess had given birth to her first son with the help of an epidural) or caesarean sections (see section 3.4.1.6). One demand in particular which should be mentioned is the increased demand for security and controllability of the birth process from the birthing women’s side. The recent birthing generation was described as a generation who is less willing to accept any insecurity or pain while birthing. This development is recently discussed in public and governmental circles under the headline “Caesarean section on maternal request” (Sundhedsstyrelsen, 2005, 7(4)). This demand has two consequences for the midwife: she has to spend more time in preparing and convincing the woman of natural childbirth, which is in her opinion still the best way to birth a child. This is time she does not have because of resource reduction in all parts of the hospital sector. Further, she has to train herself in the use of new technical devices against her own convictions. This aspect was probably very meaningful for those midwives participating in the case investigation. All of them had been in the job for more than five years, most of them much longer. They had have experience with other conditions in midwifery than the ones they work under now. Actually, there was a slight tendency to glorify the ‘good old days’, when helping to give birth was a holistic
224
task organized in smaller sections, reaching from prenatal care to postnatal visits and when midwives were recognized personalities in their community. Today, the midwife’s job is under redefinition. In the United States, where the medicalization of birth is much stronger than in most European countries (DeVries et al., 2001), a new job group, the ‘doula9’, was established to serve as with-women advocates in the birthing process. A doula is “a person trained and experienced in childbirth who provides continuous physical, emotional and informational support to the mother before, during and just after childbirth (http://www.dona.com).” From the author’s perspective, a doula does what midwives like to declare as their core job of supporting a mother while giving birth. Instead, the greater focus nowadays on medical care (e.g. more check ups in the process of giving birth) takes away awareness and time to be spent on the support of the woman in labour. The technological development in midwifery is making more and more sophisticated check ups throughout pregnancy possible. In regard to technological development there is an ongoing discussion about what comes first. Is the technological development reason for a changing perception of birth practice or is it the other way around? A more profound discussion of the issue is found in the book Birth by Design (DeVries et al., 2001). From a midwife’s perspective so much can be said: the time that needs to be spent to use the machines as instrument is higher than the time needed to use the own body as instrument. One example is the use of ultrasound to check the weight and height of the unborn child compared to the use of the own hands. In fact holds the group of midwives investigated in the present case an ongoing competition about how closed they come to estimate the birth weight of the unborn. The form of contact to the client is also different when using more distant methods. The bodily awareness of a midwife is assumingly lower when she is mainly using technical devices. In Denmark, the country of the present study, midwifery still defines helping to give birth as the primary task but the
9 The word “doula” comes from ancient Greek, meaning “Woman’s servant.” (www.dona.com).
225
way this is done in modern hospital settings matches the occupational ideology of those midwives who participated in the present study only to a certain extent. The midwife is forced to be more flexible in jumping in and out of a birthing situation and to rely on technical devices monitoring the process. This kind of work profile has been typical for a medical doctor, who steps in and out of a situation and leaves the remaining monitoring and caring to the nurses. Seen from this perspective, there is a high probability for a felt ambiguity in role definition in the recent midwife generation. The recent generation of midwives is caught in the modern dilemma of being able to provide high technology medicine at childbirth but not willing to step back from the low-technology tradition of natural childbirth. How this dilemma is to be solved is interesting to follow up upon. De Vries (1993) suggests that today an occupational group gains power to the extent that it can reduce risk and uncertainty for clients. A loss in status happens where other practitioners offer seemingly superior means of risk reduction or where birth is redefined as a less risky event. The recognition of a profession can be summarized as a problem of risk, knowledge, and power. Even if this has not been discussed as pointed in the present case, it has become clear that there is a need to renounce some of the traditional convictions in order to keep primary status as birth attendant. This is further discussed in the next section also in regard to different midwife generations.
8.3 Person related factors with relevance for the research question Even if the chosen approach to investigate the relationship between motivation and burnout in human service work makes use of a subjective approach, personal characteristics (such as motive dispositions, personality factors, coping style; etc.) of the interviewees were of minor interest. Nevertheless, individual characteristics were referred to in the course of the interviews which can be related back to research concepts from burnout research, e.g. Freudenberger & Richeslon’s concept of idealised self-image (1980). The description of engagement given by the midwives is similar to what Freudenberger and Richelson describe as an idealised self-image, seeing one’s self as a person who
226
is “charismatic, dynamic, inexhaustible, and super-competent" (Schaufeli & Enzmann, 1998, p. 102). In the course of the interviews, signs of over-dedication, an exaggerated feeling of responsibility and high demands towards one-self were named by the midwives as being somewhat typical for an engaged midwife. Hockey (1993) describes in the control model of demand management how individuals use a performance protection strategy und the influence of stressors in the environment. Through mobilization of sympathetic activation (autonomic and endocrine), performance protection is achieved. As a long-term effect of greater activation and effort, the draining of an individual’s energy and a state of breakdown or exhaustion are named. In midwifery, performance protection is a sensitive issue. The participating midwives were very clear about the importance of providing outstanding service when helping to give birth. With the decline of resources, extra effort has to be put in, in order to make sure that a high level of performance can be assured. In a positive sense, this work behaviour can be described as engaged. However, it can also lead to over-dedication and exaggerated demands towards oneself: This form of extreme engagement can lead to serious health impairments for the midwife (Engelbrecht, 2001). Over-dedication is also expressed in the fact that the formal job-role is not accepted as ideal practice but rather high demands are thought to be the ideal, which are at the same time not explicitly formulated by the work environment but implicitly agreed upon by the midwives as part of their occupational ideology. These findings from the present case support Freudenberger & Richeslon’s concept of idealised self-image (1980) as a reason for burnout. Age is one of the demographic factors assessed in the present study which is meant to have influence on the relationship between motivation and burnout. As can be seen in the age profile of the midwives employed at the ward (see Table 3.5, Chapter 3), the middle age group (35-50 years old) is the largest group at the ward (31 out of 49 midwives belong to that group). Biological age is thought to be responsible for playing a significant role in the development of burnout in
227
the group of midwives, taking the fact that burnout develops over a longer period of time and that older midwives might be more prone to develop health impairments in a highly demanding work environment due to increased recovery time and reduced flexibility in reacting to change. Generation differences were discussed by the midwives as being meaningful for the development of burnout. Older generation midwives are described as being more prone to burnout because they have a different style of approaching work than younger generation midwives. The more recently educated are described as being more pragmatic about the fulfilment of the primary task. They might also start with lower expectations towards the primary task, knowing the modern hospital organization functions in a certain way and not knowing the difference to older times in midwifery. The glorification of former times was obvious at different points. This might be due to the fact that the midwives who volunteered to take part in the present investigation of the case mostly belong to the older generation of midwives, all of them having been in the job for at least eight years. Some of them have experienced different forms of birthing and experience the recent structure of their work sphere as disillusion from the occupational ideology they started with. In regard to biological age, recovery time and declining flexibility to handle change was discussed. Different occupational ideologies and identities do not necessarily correspond with biological age but rather with time at the job. These different ideologies are meant to make a difference when talking about the relationship between engagement and burnout. The findings from the case study in midwifery propose that older generation midwives are better able to balance high job demands with the energy they get out of the fulfilment of the primary task. Younger generation midwives were described as being more sensitive to negative working conditions, i.e. being more critical and at the same time drawing less from the positive experiences in their work as a source for balancing otherwise unsatisfactory working conditions. The reaction of younger generation midwives to the high work demands can also be interpreted as
228
adaptive coping behaviour. Younger generation midwives were described as not willing to accept high demands and at the same time low recognition of the work they do. Research on effort-reward-imbalance has shown that short term imbalances between effort put into the job and reward from it might be acceptable to the individual and do not have negative consequences for health and well-being (Siegrist et al., 2004). However, midwifery in this study was characterized as being a high strain job with high effort-reward-imbalance. For a younger generation midwife, it can be regarded as highly adaptive and at the same time protective to not put too much effort into the fulfilment of the primary task but rather prioritize parts of the job where personal effort might lead to adequate reward, e.g. research work. In the context of the present case investigation, the difference in age and attitude towards the job is not stated as a problem by the midwives themselves. The reason might be the small number of younger generation midwives at the ward. Yet the more critical attitude of the younger, upcoming generation of midwives might influence traditional job beliefs in the future. In fact, a recent study by Hunter (2004) has shown that not only client contact can be a reason for emotion work but instead, conflicting ideologies of midwifery practice amongst midwives. The first ideology mostly found in hospital settings functions by necessity, and was termed ‘with institution’. The other ideology found in community-based midwifery favoured a so called ‘with-women’ ideology, standing for an individualised, natural model of childbirth. Particularly evident were these conflicting ideologies in the accounts of novice midwives and integrated team midwives in a hospital setting, both committed to a ‘with women’ ideology (Hunter, 2004). Midwifery in Denmark today is mostly taking place in growing birthing units which are most of the times part of the gynaecological ward of a hospital. This fact has influence on the education and socialization of younger generation midwives. In the present case study, midwives gave expression to favouring a ‘with-women’ ideology but named the structure and organization of work as a hindrance in this respect. The
229
professional identity of midwives is under constant redefinition dependant from the setting in which education, socialization and work of the midwives takes place (Benoit et al., 2001). In the future, the generational differences discussed above might therefore be followed by a change in ideology in regard to midwifery practice. A different scenario could be the reestablishment of smaller birthing units or a growing tendency towards private practice in midwifery. A comparison of the developmental history of midwifery practice in different countries (deVries et al., 2001) has shown that changes in midwifery practice often times were brought about by the dissatisfaction of the midwives themselves either opposed by or supported by organisational structure, political initiative, as well as the clients themselves. Sandall et al. (2001) recommend three questions to be asked while creating new models of care:
1. Does the new way of organizing care empower my profession? 2. Does it allow me to live a fulfilling professional and personal life? 3. Does it provide the best service to my clients?
The three questions above reflect the three life-spheres the midwives in the case study mentioned to be important for a balanced work-life: the profession, private life, and the relation to her client. Imbalance in one life-sphere will after some time cause problems in tone of the other. 8.4 Assumptions about client-related factors of relevance to the research question In the center of the fulfilment of the primary task stands the relationship between the midwife and her client. This relationship is described as intimate, intense, and yet of short duration. In the present case study, expectations and demands from clients as well as the recent generation’s attitude towards birthing were discussed. The participating midwives reported incongruence felt between their own professional image of service given to the clients and the appreciation of service from the clients’ side. Brucks (1998) describes emotional labour as the work related handling of meaning and feelings of non-reciprocity. Midwives in the present case described precisely this non-reciprocity in regard to
230
fulfilment of the primary task and the appreciation of this service from the clients. In part, non-reciprocity is close at hand because the birthing situation is unique (in the sense of happening one or two maybe three times in life) for the client but is an everyday chore for the midwife. The emotional triangle (Figure 2.2, Chapter 2) illustrates the non-reciprocal situation of client and midwife. Giving birth for most women is connected to a variety of different emotions: fear and anxiety, shame, hope, pride, gratitude, relief. For the midwife, positive as well as negative feelings are connected to the fulfilment of the primary task, reaching from bliss to fear, from compassion to anger, or from relief to guilt (Figure 2.2). The participants in the present case study also mentioned that each birthing situation is unique for them as well, demanding particular reactions from their side. The frustration felt in relation to the demands from clients and the missing appreciation of service given by the midwives stands against high expectations and demands towards one’s self. The participating midwives used the expression ‘to give something of yourself’ when they referred to the kind of service they give helping a woman giving birth. This high demand towards one’s self, expressed as an occupational ethic, stands in contrast to the recognition received from the recent birthing generation. Zapf et al. (2001) relate the importance of recognizing client-related stressors in the development of burnout. Furthermore, Brucks (1998) points to the shortcoming of work psychological research, focussing mainly on the instrumental part of the primary task, whereas emotional labour (as often caused in the relation between client and human service provider) remains implicit. In the medical field in general, professional expertise is in the focus of attention even though emotional labour describes an important part of the successful fulfilment of the task (Hahn, 1988, in Brucks, 1998). Also in the present case, the participants reported how important emotional labour is for the fulfilment of the midwife’s job. Yet this part of the work is implicit in the sense of not being officially defined as part of the primary task and therefore not recognized in organisational structures; as for example, in sufficient time given to recover from demanding work situations or
231
from traumatic birth incidences. Midwives stated very clearly client-related stress as being related to feelings of being burned out. In regard to these conflicting demands and beliefs between client and midwife, the aspect of emotional dissonance as the requirement to display emotions which are not felt, needs to be discussed. Emotional dissonance has been shown as the most stressful aspect of emotion work (Zapf et al., 2001). The primary task in midwifery demands a clear position of one’s own work role, a high feeling of responsibility, and high sensitivity towards the clients’ needs. At the same time, the midwife is confronted with unrealistic wishes and beliefs from the clients. Whereas midwives in former times had both the necessary reputation but also respect from clients to decide in the birth process what needs to be decided, the modern ‘with-women’ attitude in midwifery has led to emancipated clients who demand what they think is right. In principle, this is valued as positive by the midwives of the present case investigation, but at the same time, they reported greater friction between them and the recent birthing generation in the case of non-reciprocity of belief about what needs to be done. Finally, it should be mentioned that there was a rather high consistency when the participating midwives referred to friction with clients. The recent birthing generation’s attitude and behaviour was repeatedly described as being in conflict with the experience and belief of the participating midwives. This leads to two contradictive assumptions: Either the clients are really very different from former birthing generations or the midwives are short tempered because of the high workload they face and a ‘blaming the victim attitude’ is a first sign of depersonalisation. 8.5 Structural and situational demands and conditions of work in midwifery The vertical axis of the descriptive model (Figure 8.1) illustrates structural as well as situational demands in midwifery which are variable and therefore ought to be named in regard to their recent influence on the fulfilment of the primary
232
task and the potential to change it in addition to the influence on the relationship between motivation and burnout.
8.5.1 Impact of political decisions in the health care system
The assessment of structural and organisational particularities in midwifery was not done in the sense of a document analysis but ‘happened on the way’ of investigating the case using participant observation, single interviews, and the group interview. Even if this kind of data is not structured in the same way as the rest of the data is, the following assumptions are drawn: Resources and resource allocation practice are influenced by the mindset and ideology of the present health care system. This mindset and ideology can be described most briefly as following market principles in the sense of applying cost-benefit-analyses to human factors. In the case of midwifery this leads to a resource allocation practice which is far from optimal in the eyes of the midwives and to the segmentation of the primary task contradicting the effort to provide continuity of care. Resources in midwifery are described as being a core issue. This is due first of all to the importance of sufficient resources to fulfil the primary task in a responsible manner. In the present case study, resources were described by the participating midwives as being a significant aspect regarding the relationship between motivation and burnout. The delivery of 100% service is described as being of great importance for the participating midwives. Low resources lead to a decline in service quality in fulfilling the primary task. Related to this, negative feelings such as frustration, fear, anxiety, and the need to be alert are experienced by the midwife. On the contrary, the primary task was described as the main source of positive energy in a highly demanding work environment. Low resources are experienced as threatening to this positive work experience, because service quality, which is highly valued by the participating midwives, becomes the buffer between low resources and high demands. A stress theory
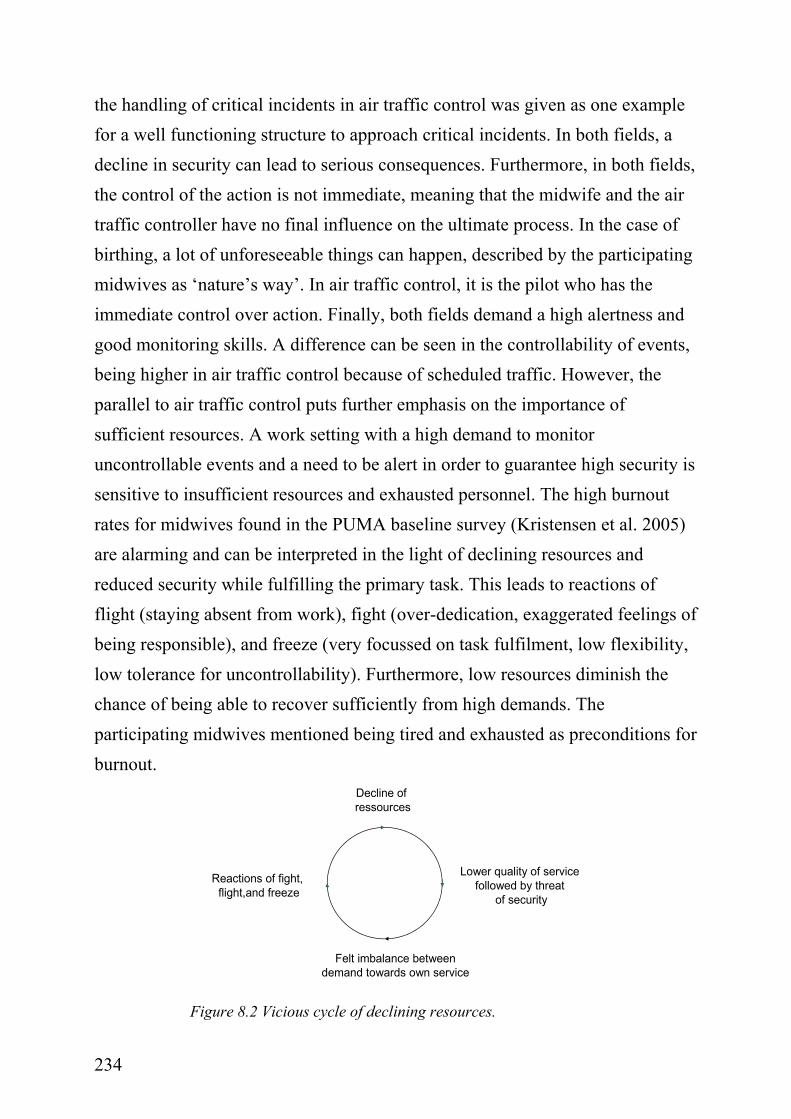
233
focussing on the meaning of resource protection and enhancement is introduced by Hobfall (1989). In the conservation of resources theory, resources are defined as “those objects and personal characteristics, conditions, or energies that are valued by the individual or that serve as a means for attainment of these objects, personal characteristics, conditions, or energies" (Hobfall, 1998, in Sonnentag, 2001, p. 197). According to the theory, stress is caused by a threat of resource loss. In midwifery, one energy resource is the successful fulfilment of the primary task, described as “getting healthy children to earth”. If this is perceived as being threatened to an extent where a midwife gets uncomfortable with the service she is able to give, the capacity threshold for work related demands is lowered to a point of imbalance, leading to negative consequences of health and well-being, here described as burnout. This phenomenon is also described in capacity theories as an overflow when multiple stressors develop a joint effect and then exceed certain capacity thresholds (Schönpflug, 1982, Wieland-Eckelmann, 1992; in Zapf et al. 2001). The idea of a capacity threshold is appealing and explains why a person’s breakdown often comes rather unexpectedly as was also described in the present case investigation. The following basic theoretical assumption from PUMA confirms this finding: “…exposure to adverse psychosocial work characteristics lead to unfavourable psychophysiological arousal (distress), which in the long run will lead to a state of exhaustion, which we label burnout” (Borritz et al, 2005, p. 1016). The demand to guarantee highest security while helping to give birth was also discussed in connection with resource availability. It was described by the participating midwives that midwifery is a field where resources are not easy to calculate because unforeseeability of events is high. Not being able to deliver high security because of low resources is experienced as stressful and not acceptable. Reactions of flight, fight and freeze, commonly known as stress reactions, were described by the participating midwives. It is interesting to note that there is a parallel in regard to the security issue between midwifery and air traffic control mentioned by the midwives themselves. In the group interview
234
the handling of critical incidents in air traffic control was given as one example for a well functioning structure to approach critical incidents. In both fields, a decline in security can lead to serious consequences. Furthermore, in both fields, the control of the action is not immediate, meaning that the midwife and the air traffic controller have no final influence on the ultimate process. In the case of birthing, a lot of unforeseeable things can happen, described by the participating midwives as ‘nature’s way’. In air traffic control, it is the pilot who has the immediate control over action. Finally, both fields demand a high alertness and good monitoring skills. A difference can be seen in the controllability of events, being higher in air traffic control because of scheduled traffic. However, the parallel to air traffic control puts further emphasis on the importance of sufficient resources. A work setting with a high demand to monitor uncontrollable events and a need to be alert in order to guarantee high security is sensitive to insufficient resources and exhausted personnel. The high burnout rates for midwives found in the PUMA baseline survey (Kristensen et al. 2005) are alarming and can be interpreted in the light of declining resources and reduced security while fulfilling the primary task. This leads to reactions of flight (staying absent from work), fight (over-dedication, exaggerated feelings of being responsible), and freeze (very focussed on task fulfilment, low flexibility, low tolerance for uncontrollability). Furthermore, low resources diminish the chance of being able to recover sufficiently from high demands. The participating midwives mentioned being tired and exhausted as preconditions for burnout.
Decline ofressources
Lower quality of service followed by threat
of security
Reactions of fight, flight,and freeze
Felt imbalance betweendemand towards own service
Figure 8.2 Vicious cycle of declining resources.
235
8.5.2 Organisation of working time
Working time issues were discussed by the participating midwives as work related factors which cause burnout. In regard to work time issues, work family balance is a constant point of discussion. Time at work, time for the family, and time to be alone are competing issues, needing to be balanced in one way or the other. The midwife is often not able to satisfy her personal needs to recover and relax, stepping from one active and demanding environment into the other. This might not be an uncommon experience for working women but it might be particularly tough when doing a job which demands a lot of physical, mental, and emotional availability, as is the case in midwifery. Furthermore, the planning of shifts was mentioned as critical factor. Given the fact that midwives spent a lot of time (regular working hours plus overtime) at the ward, the influence they have on planning the shift is seen as too low. Particularly part timers mentioned a feeling of injustice when talking about shift planning. They feel neglected in the allocation of desired shifts (day shift during the normal work week). Part time work is described as one possibility to balance work and family demands. At the same time, part timers feel they are fit into the schedule at unattractive points in time. No matter if this is the subjective perception or a fact, it leads to a feeling of injustice and finally to frustration. Kivimäki et al. (2003) investigated the potential impact of organisational justice on employee health in a longitudinal study in the Finnish hospital sector. Organisational justice is defined as “the extent to which employees are treated with justice at their workplace" (ibid, p. 27). They found that the extent to which employees are treated with justice has predictive power on health outcomes. Especially the discussion in the group interview pointed to a feeling of injustice in the group of midwives regarding work time and the recent re-structuring. Tausig & Fenwick (2001) investigated the time-bind known as the inability to combine work time and family time in a manner which causes less work-life
236
imbalance by looking at the relationship between different work time schedules and perceived work-life balance. The result of most interest in this body of work is that alternate schedules do not unbind time, although perceived balance was increased with higher control over one’s schedule. Work family balance was named as a serious problem by the participating midwives. Many midwives work reduced hours in order to be able to follow commitments in the family and at work. According to results from Tausig & Fenwick (2001), low control over the work schedule was named as a source of frustration and burnout. Sandall (1997) also reports a relationship between occupational autonomy expressed in control over worktime and midwives’ burnout (see p. 63). The anticipated positive impact of reduced work hours is absent when work schedules do not take the individual needs into account. Consequently, giving control over work schedules back to the midwives is assumed to have the most direct impact on perceived work-family balance and in second line on the motivation of the midwife. One further aspect discussed by the participating midwives is the issue of working at night. This also is an unchangeable condition in midwifery. Yet it is not only an inconvenience but a real physical and psychological strain. The participating midwives reported not being able to give the same quality of service at night as during the day. From the perspective of professional belief and the high expectation midwives have towards themselves, this reduced service is not seen as being good enough. Besides the physical strain, it is the psychological side of having a bad conscience when not being able to serve optimally during the night. In connection with work at night, extreme exhaustion is mentioned, which midwives feel after having been on a night shift. This phenomenon is widely investigated and negative aspects of shift work are known. A recent study on job-related stress and shift work in a three-shift system revealed an increase of job-related stress and low control for workers in a three-shift system (Harada et al. 2005). The problems reported by the midwives in the case study are sleeping problems, exhaustion, circadian rhythm
237
being upside- down, and a feeling of numbness for more than 24 hours after having been on a night shift schedule. For some of the interview participants, work at night was such a serious problem that the thought of quitting the job was described as appealing. A sufficient recovery time after having been on night shift is valued as essential. One midwife mentioned the importance of being good to one’s self when being at home after an exhausting shift, not feeling obliged to care for all the things in the house which need to be done. However, midwives described themselves as being used to care for others. It might cost them some extra energy to relax at home after a night shift (see also Section 8.2.1). One last aspect mentioned in the course of the interviews and a particular point for observation, was job routine in midwifery. Even though midwifery is described as a work sphere with high uncontrollability, there are at least some reasonable parts of recurrent routines. Routine work is described as being both annoying and relaxing. The weekly consultation day is described as being a welcome break in the weekly shift schedule. The consultation days have two positive points to offer: they are accountable in terms of time and effort and not less important they nurture the desire to be part of a holistic birth experience, where prenatal information and contact is thought to be an important part. The annoying part of routine is described as recurrent tasks that need to be done but are of more administrative character, e.g. writing of birth journals. In relation to the primary task the singularity of each birth process is much more in focus than the fact that many of the tasks the midwife needs to do while helping to give birth are to a certain extent routine tasks.
8.5.3 Midwifery as a master piece of the female work role
In the present study, one aspect of engagement was described as ‘the care for others’. The care for others is traditionally a primarily female role in society (Brucks, 1998). Ostner and Beck-Gernsheim (1979, in Brucks, 1998)
238
investigated the female work capability (German: weibliches Arbeitsvermögen) as being characterized by three arguments: (1) the female work capability refers to skills and competencies already present before entering the job as being part of the female family role; (2) work within the dilemma of content orientation and exchange orientation, “two faces of work” (Ulich, 1991; Schmale, 1995, in Brucks, 1998, p. 40). Professional work forces different from house-work into a dilemma between setting the priority in favour of the subject matter (content orientation) or in favour of getting adequate gratification and recognitions (exchange orientation). Women tend to prioritizing content and not exchange and (3) the care for others is not easy to fit into the description of a modern job role as described by Parsons (1952, in Brucks, 1998, p. 37) in the following citation: “The role of the medical practitioner belongs to the general class of professional roles, a sub-class of the larger group of occupational roles…In common with the predominant patterns of occupational roles generally in our society it is therefore in addition to its incorporation of achievement values, universalistic, functionally specific, and affectively neutral. Unlike the role of the business man however, it is collectivity-oriented, not self-oriented.” The three aspects of the work capability are partly represented in the midwife’s role. Traditionally, midwifery is a mainly female work environment relating to some degree (communicative skills, emotional ability) to the female family role. The form of engagement described by the participating midwives as to give something of one’s self, to show empathy, to take responsibility at points where it is not one’s own responsibility are characteristics of the female family role and not so much in accordance with the work role described by Parsons. The relatedness of female work role in midwifery and female family role can be challenging, especially in the case of high work demands. Borders between work and home are less clear and make an unwinding after a busy day at the ward difficult. The participating midwives working on a day schedule reported the disadvantage of working during the day as having less time on their own at home. Their families enjoy having them at home yet at the same time they sometimes miss the quietness to have a day alone. Engagement as the care for
239
others therefore is regarded as to be especially vulnerable to work related stress. Caring for the other as central component of the primary task is demanding in the same way as is the care for members in the family. Because of this similarity, unwinding from stress at work when being at home is not easy to achieve for a midwife and is dependent on the family situation. Capacity thresholds might be further strained when being at home instead it being a place where batteries can be filled up. In regard to the second aspect of the female work capability, the difference between content- and exchange-orientation, the high importance of recognition from the client needs to be discussed. As mentioned by the midwives, the recent birthing generation does not express gratitude for the midwife’s service to the same extent as former generations. For the older generation midwives, exchange of personal recognition seems to be more important then the exchange of financial value. This attitude is close to the housewife’s attitude of hoping for recognition of the work she has done for the family and might not be a good estimate of reward for professional service given to a client.
8.5.4 Relevance of implicit knowledge
The instrumental (or professional) knowledge needed to do the job of a midwife can be discussed from two perspectives: the knowledge acquired in the course of primary and further education and experiential knowledge, often stored as tacit or implicit knowledge10. The midwives referred to the latter as important in regard to felt security on the job. Professional knowledge is, like in many other fields of work, under constant development. New developments first are approached explicitly. Explicit knowledge can become implicit through job routine. The acute nature of the primary task sets the hurdle of accepting new 10 Both terms (tacit and implicit) are used in the present monograph in order to describe knowledge not accessible through conscious processes. Tacit knowledge relates back to Polanyi who published his groundbreaking work on Tacit Knowledge already in 1966. In psychological research the terms implicit and explicit are recently used as referring to the different modes of storing information in memory (Kuhl, 2000; Rothschild, 2000).
240
routines at a high point. Old job routines are not easy to give up in a field of work with high uncertainty, high demand for security, and a high relevance of implicit knowledge. Implicit knowledge in midwifery is described as embodied knowledge. Embodied knowledge is knowledge stored in the body, using the body as an instrument and as a knowledgeable agent. This kind of knowledge can be observed in simple daily routines like bike riding which one first has to learn before it becomes a routine of self-acting movement. In midwifery embodied knowledge is for example seen in the way a midwife uses her fingers to measure and estimate the dilation of the uterus, it is an embodied measure. The change of job routine following from technological development has consequences for the implicit and explicit competence of a midwife. Change in job routine is often accompanied with insecurity and anxiety, especially in a field in which mistakes can have serious and even fatal consequences. Therefore, a natural and most of all very human reaction to change is rejection. Change is not the most comfortable situation to be in. Change in an already uncontrollable setting leads to a feeling of even higher uncontrollability. Menzies (1975) elaborated the avoidance of change in nursing and observed that nurses were clinging to the familiar even if this was not the most appropriate option. In the present study, staying with the familiar gets an extra connotation because the primary task is described as not routine-based but is rather based on individual cases (e.g., each birth representing a single case). Furthermore, experienced midwives rely to a certain degree on their implicit knowledge in the sense of ‘feeling’ the decision to take. This form of tacit knowledge is a valuable competency in order to sustain the uncontrollability and uncertainty which is a fundamental character of birthing. Implicit knowledge is thought to have high importance in a work environment with a high frequency of acute situations, which cannot be handled on the basis of one single job routine. On the other hand, the meaning of implicit knowledge in midwifery has serious consequences for actions following from implicit decision making. Often the implicit dimension is described in a positive light and it is forgotten that the implicit
241
dimension has, because of its pre-lingual nature, a tendency to remain in a state which may no longer be adaptive with a representation of knowledge which is inflexible to change (Herbig, 2001). One participating midwife described that the acceptance of using implicit knowledge grows with the years of experience in the job and the reputation the midwife has at the ward. The more a midwife is recognized as highly professional, the more it is accepted that she refers to the implicit knowledge base. This might not always be justified. Unfortunately, it is inherent in the implicit dimension that change is not easy to establish. Functional approaches have shown that the implicit and explicit dimensions work with different memory systems (Kuhl, 2000; Rothschild, 2000). Explicit memory is also called declarative memory as it stores facts, concepts, and ideas. Language is a necessary mean to store explicit memory. Yet, explicit memory also contains complex step-by-step operations like baking a cake that can be recalled in a cohesive narrative. The counterpart, implicit memory, involves procedures and internal states that are automatic. Here learned routines and behaviours are stored and can be recalled. Implicit memory therefore is also called procedural or nondeclarative memory. It is laborious and sometimes even impossible to transform implicit memory back into language. In the present case one midwife shared the experience of not being able to put her embodied knowledge (as being stored in implicit memory) down on paper when wanting to write an article about the competencies in midwifery. Part of the female work mystique might be exactly based on this form of tacit knowledge stored as implicit memory used with an instinct of knowing what needs to be done. Among other interesting outcomes to the meaning of implicit and explicit knowledge in nursery Herbig (2001) could show that implicit knowledge embraces the emotional exchange of a person with her environment to a greater extent than the explicit knowledge base does. This would be an explanation for the frequent use of tacit ‘embodied’ knowledge in midwifery, which is regarded as highly emotional work sphere. The methodology applied to investigate the research question is not valued as being the right approach to investigate implicit processes. Implicit processes cannot simply be explicated through language.
242
Herbig (2001) solved the problem with simulating a critical situation in nursery and let the study participants react to this situation as if it was a real case. In the present case it was initially planned to use a recently developed test to investigate implicit motivation in midwives (Operant Motive Test, Kuhl & Scheffer, 2001). The final research aim suggested a different approach first. In a next step it is valued as highly interesting to look for forms of in-depth investigation of implicit processes at work. Nevertheless, the findings of the present study have revealed the importance of tacit knowledge in midwifery and the bodily expression of this knowledge form on a surface level. One example is the reported increase in felt security with years of experience which goes beyond better mastery of the task because of experience. The feeling of security was described by the midwives as being based on embodied knowledge, the feeling of what is right and what needs to be done. This base of knowledge is meant to have the character of an implicit knowledge base. In motivation research, first steps towards implicit processes have been made and promise useful insights (Brunstein et al., 1995; Niitamo, 1999; Kuhl, 2000; Scheffer, 2001). Findings from this research point to the importance of congruence between implicit motives often established in early phases of human life (beyond language) and explicit motives established in relation to the concrete context of life. A person can for example have a high implicit motive of attachment to others and has explicitly chosen to work in a context where this attachment motive comes to its right, e.g. human service work. Higher incongruence between the two showed to be related to reduced well-being (Brunstein et al., 1995). This path of research is thought to be interesting in a work environment which relies considerably on implicit processes.
8.5.5 The significance and impact of traumatic birth incidences
One aspect of emotions in midwifery was described as feelings in reaction to traumatic birth incidences. The first point to discuss in this regard is the different comprehension of traumatic incidences from a midwife’s perspective and from
243
the perspective of a modern client. Client and midwife start with different presuppositions. The clients’ longing for control over the process of giving birth has reached a different quality with modern birthing practice. At the same time, there is a longing amongst some older generation midwives to reach back in time and reactivate birthing practices that have become buried in the organization of childbirth in greater, modern birthing units. The gap between midwife ideology of natural birth and client demand for controllability was discussed in the single interviews. The participating midwives reported bewilderment and frustration about the attitude of some women of the recent birthing generation towards natural childbirth. The demand of total control from the women’s side stands in contrast to the experience and beliefs of the midwife. The attitude of a midwife is nurtured by the belief of not being able to solve the paradox of total control in an uncontrollable process. The knowledge of the importance of letting go and the belief in something bigger than their own competence is questioned by the demand from the client and the growing technical control throughout pregnancy and in the process of giving birth. This is in fact a question of belief which often leads to frustration when not solved to the satisfaction of both sides. In the case of midwifery, a re-thinking of occupational ideology and identity might be one way to reduce friction between midwives and clients. Another way could be to enable midwives to convince the recent birthing generation with their arguments being based on experience of best practice. A woman in labour might not be listening to a midwife she has not met before. In the crisis of giving birth she might be more trusting on and listening to her own feelings of pain and fear. Being able to instantly establish rapport is a high skill but seems to be important in the way midwifery is organized today. The foregoing discussion might also be interpreted as a strong argument for re-thinking the way labour wards are organized (e.g. segmentation of primary task by shift schedule). Even if the midwives have a more accepting attitude towards the uncontrollability of the birth process, the impact of traumatic incidences is
244
reported to be massive. The participating midwives reported a feeling of being left alone with the burden of coping with traumatic birth incidences. Trauma experienced at work is a singular issue. As in other medical fields, trauma can happen to the provider of service as part of the primary task. However, midwifery is regarded as particular case because death is on one side close at hand but on the other side fortunately not the most probable thing to expect. In contrast to an intensive care unit, the probability of clients’ deaths is rather low in midwifery. It can and does, however, happen to each midwife in the course of her professional career. Therefore, all kinds of check ups are implemented in the process. During participant observation, it became obvious that there is a form of rumination about outcomes, a constant discussion about cases, often with detailed descriptions about what was done and what is planned to do. There is a paradoxical feeling connected to traumatic incidences described by the midwives. The possible exposure to traumatic incidences is on the one hand seen as an inevitable part of the primary task; furthermore, responsibilities are clear cut on paper. Nevertheless, midwives described the feeling of having been exposed to a traumatic incident as highly negative, leading to feelings of guilt and low confidence in the own professional competence. When a traumatic incident happens, midwives in the present case study reported reacting to it on the basis of ‘intuition’, because midwifery training does not include the preparation for the worst case. According to them, the reaction to traumatic incidences becomes more skilled after the first couple of years in the job. Yet, each time a traumatic incident happens to a midwife or one of her colleagues is described as being appalling. The reported burnout as a reaction to traumatic incidents has a more severe character than the work related burnout based on high work demands and low resources. From the perspective of trauma research, this is not at all surprising. Traumatic incidences find their manifestation in bodily reactions which again have influence on the way to react to the next incident of the same nature (Rothschild, 2000). If trauma is not sufficiently dealt with, it could happen that –
245
as one midwife described it - a person who actually was known for being able to cope with all the obstacles of the job in a professional way has a sudden breakdown. Furthermore, knowledge about the tacit dimension proposes a different procedure then established at present for intervention procedures offered to midwives after being part of a traumatic birth incident. The procedure of psychological debriefing makes use of a process of narrative healing. The re-telling of the traumatic incident is thought to have healing effect (Rothschild, 2000). This might be true for the explicit dimension but the implicit dimension probably needs some other form of healing as the implicit dimension is not accessible to language; it uses emotional, bodily, sensory information types, all being speechless (ibid). One approach to understanding the implicit processes after trauma is formulated in the SIBAM model (Levine, 1992, in Rothschild, 2000). SIBAM is the acronym for: Sensation, Image, Behaviour, Affect, and Meaning. The model proposes that during or after a distressing/traumatic incident, experiences become disconnected, e.g. image and affect of a traumatic incident are disconnected and cause in consequence visual flashbacks. In the context of the present study, traumatic incidences are referred to as having the power to cause long term effects, such as burnout. Even though the occurrence of traumatic birth incidences is seen as being a natural part of midwifery, there is not much information about how they can react when confronted with the situation. One participating midwife described her reaction as experiential learning; as a process of getting used to the fact that traumatic birth incidences happen. It is assumed that the addition of an implicit perspective to the handling of traumatic birth incidences will lead to better ways of coping with them. In the field of German air traffic control, a Critical Incident Stress Management program (CISM) was established to help employees to cope with stress reactions related to critical incidences (Vogt et al., 2004). Even though burnout is not named amongst the stress reactions, the procedure seems to be of interest to
246
discuss in regard to the impact of traumatic incidences in midwifery. The probability of fatal outcome in Air Traffic Control is comparable to birth processes, as fortunately having a rather low probability. Yet, a fatal or even just critical outcome in both fields is experienced as highly traumatic for everybody involved. The CISM program has two aims: (1) to reduce the impact of the stressful event by facilitating an employee’s return to work and (2) by educating the employees about signs and symptoms of traumatic stress and mechanisms to manage stress. Moreover, additional support or professional referrals to recover fully are established. The effects of CISM were estimated as successful. Those who took part in a CISM program mentioned the enlargement of communication possibilities after critical incidents in the form of supervision, whereas peers emphasized the avoidance of long-term emotional consequences with substantial losses of performance capability. The impact of traumatic incidences in midwifery is, from the author’s perspective, largely underestimated. Critical incidences in air traffic control have a higher impact because more people are involved and the loss is greater than losing a single child under birth. However, the impact on the employee stays the same regardless if one person is lost or many. Vogt’s study points to the importance of establishing formal support systems for traumatic incidences in order to support the employee instantly and professionally. The economical evaluation of the CISM program showed a financial gain for the company. The same is estimated by the author to be true for formal support programs in midwifery once fully established. Yet, in midwifery it is on the background of what was said about the importance of implicit knowledge in the natural process of giving birth regarded as important to establish support in regaining trust and confidence in implicit knowledge processes proposing something beyond a cognitive stress management technique. 8.6 Summary and conclusion of the explorative case investigation The findings of the present investigation point to the importance of the primary task as a source of positive work experiences, which in turn balance the negative
247
influences. In this sense, positive work experiences - being frequent in midwifery - are regarded as an important resource and a buffer against high demands and otherwise low resources (financial reward, recognition from supervisors, colleagues and clients, etc.). This resource is threatened by segmentation of the task and by growing demands of clients in regard to security and controllability of the birthing process. A midwife’s core competency is helping to give birth the natural way. However, there is a trend in birthing to rely more and more on technical devices and other medical support when birthing a child. Furthermore, modern hospital organisation is modelled after economical market principles. In the field of midwifery, it becomes obvious that this approach has definite disadvantages, leading, for example, to a form of resource allocation practice which does not take the task specific demands into account. In the present investigation, it was shown that structural conditions surrounding the organization of the primary task have an influence on the vigour and well-being with which the task is and can be accomplished. Personal factors were not investigated in depth though it was found that the group of midwives is characterised by an idealistic self-image which is hard to live up to. Non-reciprocity of idealized-self and real-self, combined with the structural limitations (low resources), leads to frustration about the conditions at work (Freudenberger & Richelson, 1980). The present study has further shown the impact of emotional demands and feelings in midwifery. On the whole, emotions in contemporary work settings receive higher recognition as being important for health and well-being than even ten years ago (Ashkanasy et al., 2000). Zapf (1999) pointed to the necessity of including emotional demands in burnout research in the field of human service work. However, until now, emotional labour has not been a defined part of the primary task of a midwife. Hence, emotional labour is done in ad hoc action by a single person (in best case supported by her supervisor) and not as an explicit strategy implemented at the workplace. Of particular interest is that emotional labour in a field of work which obviously deals with the whole range
248
of emotions possible to imagine is not explicitly addressed and cared for. The narratives from the participating midwives expressed the great importance of taking the impact of traumatic incidences on the single midwife seriously. Generation differences or even gaps have been discussed; also in the recent work of Hunter (2004). One shortcoming of the present investigation is that only ‘older’ generation midwives were interviewed. Future research needs to look at whether the occupational ideology of younger and older generation midwives is distinct from each other in a way that it has impact on the basic understanding of the primary task. However, looking at the findings from the present case investigation, role ambiguity (here understood as a difference between own occupational understanding and formal job role) leads to frustrations, and probably under certain circumstances, to burnout. As soon as the positive experience related to the primary task of supporting a woman in labour physically, mentally, and emotionally is reduced to a minimum due to rapid technological development and the need to use it - with at the same time unchanged conditions in regard to job demands - imbalance occurs. Greater technical help or even caesarean operations diminish the midwife’s part, degrading her to be assistant in an otherwise ‘automatic’ process. Clarity about this entangled understanding of the primary task is thought to be helpful in redefining the primary task and related to this, establish new job routines. Nevertheless, in combination with the interviews’ finding that pregnant women’s views have changed throughout the last years, one could interpret the difference in behaviour of younger midwives (mentioned by older generation midwives) as an evolutionary fit to the unchangeable, recent challenges of the job. It is reasonable that those who give birth and those who help to give birth from the same generation have certain mindsets and tracks in common. Following from that, there might not be the same emotional upset for a younger generation midwife in accepting a clients’ wish for an alternative to a natural birth. Following from that younger generation midwives do not experience the
249
same kind of friction with the client described by the older generation midwives as being frustrating and as leading to a distanced attitude towards the client.
8.6.1 Strengths and limitations
As reported at the beginning of this Ph.D. thesis, most research on the relationship between motivation and burnout is of quantitative nature, neglecting the importance of defining the phenomena of motivation and burnout in context. The investigation of midwifery as being a singular case in human service work has shown that the interpretation of outcome is, to a high degree, dependent on context variables. The understanding of burnout and engagement as a practice concept of disease/motivation, taking conditional factors in midwifery into account, emerged as being of high importance for the discussion of the relationship of motivation and burnout. A comparison between data from PUMA and data from the present case is helpful in order to highlight one positive aspect of the explorative in-depth investigation of the relationship between motivation and burnout. In PUMA, a newly established questionnaire to measure forms of emotional exhaustion in regard to clients, to work, and personal exhaustion was applied to measure burnout (Kristensen et al., 2005). The open nature of the interviews in the present case investigation encouraged interpretations beyond the variables used in the PUMA study. Further, the findings from the interviews indicate that research results do not necessarily get communicative validation by those who were investigated. Some of the participating midwives mentioned doubt and even disbelief in the findings of the PUMA study (see Chapter 4). This is interpreted by the author as being an outcome of the research method used in PUMA. This is further regarded as a serious but accepted shortcoming of distal methods of investigation in applied research. Participants who volunteer to take part in a research study invest time and effort to answer questions. At the same time, they expect to get something back. If this expectation is not met, the
250
degree of acceptance and the belief in the outcome is low. This does not mean that the findings are invalid, but it diminishes the reach of a project in practice. Accordingly, methods to investigate context variables at the same time as the phenomena of interest need to be developed further. A combination of distal methods of investigation, using, for example, questionnaires combined with a more proximal method (e.g., interview), might be a way to open the way for a larger number of participants than possible in singular qualitative approaches. Mixed method approaches (Creswell, 2003) are thought to overcome many of the shortcomings connected with either method. The combination of quantitative as well as qualitative data sources in a single study are meant to lead to a thorough level of investigation. The present investigation was launched on the basis of outcomes from a longitudinal investigation of burnout (PUMA). Combining these two approaches in one investigation in the future will lead to even more specific insights and understanding of the relationship between motivation and burnout in human service work. The investigated group of midwives is rather homogenous in terms of demographic factors. Unfortunately, none of the younger midwives employed at the ward volunteered to take part in the single interviews or the group interview. The only contact with a newly educated and young midwife happened during the work place observation part of the study, as she was the only one on that particular shift who volunteered to be shadowed by the author. Two assumptions can be made in regard to this. First, younger midwives might not have been at the ward long enough to experience feelings of burnout and therefore think that they cannot contribute valuable insights. Moreover, due to the short time on the job they may not be confident about the positive side investigated in the present case, engagement in the job, because engagement is described as an ideal state which is first reached with a certain level of expertise. Second, younger midwives might be more open for proximal methods, giving insight into their daily activity at the ward whereas not being interested in or being too shy for an in-depth approach such as a single interview. The discussion with the midwives
251
about at what point trust in the own performance while fulfilling the primary task is established, made clear that younger generation midwives are not regarded as being fully competent to tackle critical situations until they have reached up to seven years of work experience. This might be the reason for that the little group of midwives with a job experience of less than 5 years do not feel confident about sharing their knowledge. Two other forms of selection bias were already mentioned in Chapter 3 (see Section 3.3.4). Firstly, the explicit voluntary nature of participation in the interviews maybe led to only those partaking who want to transport personal issues in regard to the subject. Since the present study both provokes yet overlooks these tendencies through its in-depth approach, this bias would seem to be an important consideration for future studies. Secondly, a healthy worker effect is reasonable to expect as only those who are still at work were asked to participate. A different but very fruitful approach would be to explore the perspectives of those who are absent from work because of work-related stress/burnout and put those findings into perspective with the findings of the present case investigation. In regard to the research methods applied in the present case study, the following needs to be mentioned critically: two points of participant observation are the minimum for getting a somewhat comprehensive understanding of a work task. Even if data from the participant observation were only used as source of confirmation of findings of the single and group interviews, it would have been of extra value to have more days of participant observation at the ward and to have another period of observation after the interviews were finished. An extended period of initial observation would have given more insight into personal style of different midwives. A second round of observations after the single interviews were carried out would have been a valuable source of information to be used in the sense of a more focused reality check of outcomes of the single interviews.
252
8.6.2 Transferability of findings and reach of the study
The primary task in midwifery, due to the natural process of giving birth, is universal. However, differences can be found in the structure, organisation and even appreciation of giving birth in different cultures. Being pregnant and giving birth is the most natural and yet also culturally defined process. Differences between the way midwives work in urban and rural areas are close at hand. As other parts of the health care system, midwifery is dependent on the values, mindsets, and not least financial possibilities of the participating actors on the local level. However, the strong emphasis on the primary task, the changing demands of modern clients (recent birthing generation), the possibility of experiencing trauma in relation to the work task, and the reduced resources in modern health care systems is perceived as a general problem in modern midwifery. Therefore, the findings from the present study are interpreted as being transferable to other settings. Beyond these findings, it is important to note that the case study also revealed a tendency in birthing which points to the fundamental sell-out of ideological and ethical convictions in midwifery. The findings about generational differences between midwives and between birthing generations propose a shift in midwifery towards a medicalised and planned process. From the perspective of the midwives, the organisational structure of birthing in modern maternity wards (like the one investigated here) is not only counterproductive but also takes the pinch of mystery away which is inherent in the primary task of helping to give birth. The more and more sophisticated prenatal diagnostics further a tendency towards the totally controlled, explicitly designed, and expectably received child. Maybe, also on the background of this, the findings indicate insecurity in the present job role, being more and more set aside or even replaced by a medical doctor. Midwives in Denmark are increasingly forced to engage in secondary tasks, such as consultations during pregnancy, teaching of younger midwives, administration and routine tasks in order to stay motivated in an otherwise less satisfying job.
253
8.6.3 Assumptions about the research field, directions for further research and recommendations for midwifery practice
From the discussion of findings, the following assumptions and perspectives for further research can be drawn.
1. The relationship between motivation and burnout in midwifery in Denmark has shown to be influenced by:
• the balance between demands and resources,
• the attention given to the emotional demands of the primary task,
• the relationship to clients and their demands, and
• the tacit/implicit dimension of knowledge and feeling.
In further studies of the relationship between motivation and burnout, it would be of great value to include these dimensions explicitly.
2. Besides already existent measures of the tacit dimension (e.g. Operant
Motive Test, Kuhl & Scheffer, 2001; Repertory Grid, Kelly, 1955; Herbig, 2001), new paths of investigation need to be found, especially in the field of occupational psychology, in order to investigate the implicit dimension and get access to this base of knowledge, emotion, and experience.
3. Emotional demands related to the fulfilment of the primary task need the same attention as other factors in contemporary occupational psychology.
4. Trauma at work has a far-reaching impact on the professional confidence and well-being of doing the midwife’s job. Insufficient handling of trauma leads to states of impaired well-being (not necessarily burnout) and higher absence rates.
5. Sufficient time is crucial for quick and full recovery (unwind, cope, and heal) after demanding days at the ward as well as after traumatic
254
incidences. Low (time) resources lead to the accumulation of negative feelings and might end in sudden breakdowns.
With the perspective of reaching highest impact (enhanced motivation and less burnout), the following recommendations for the practice of midwifery are drawn from the findings of the investigation. (1) Recent structural and value changes in midwifery have led to a re-definition of the core actions of the primary task. With reference to Visholm (2004), it is regarded as important by the author of this Ph.D. thesis to re-define the primary task, the traditional beliefs, and the borders to other systems in recent Danish midwifery in order to give back the strong occupational identity which has been commonly found in midwifery. Assurance about the occupational identity strengthens the position of the midwife and leads to a more realistic self. The frictions with clients reported by the participating group of midwives might also be understood as one example and image of an entangled and distracted self-understanding in midwifery being provoked by distressing conditions which define the borders of the recent system of midwifery. (2) A formal procedure to support and follow those being confronted with trauma at work is regarded as being an essential method to minimize the traumatic stress related to these incidents. (2) Re-think resource allocation practice and base a new model of resource allocation on cases at the ward and not number of births per midwife. (3) As Tausig & Fenwick (2001) proposed, the easiest way to solve the feeling of work-family imbalance is by giving control over working time back to those who bind time in the organization. Giving control over shift planning back to the midwives would have an educating and healing effect for the leadership as well as for the staff.
255
(4) Offer flexible solutions of work organization in order to take generation differences and specific needs into account. (5) Compare different forms of midwifery practice (e.g., the Dutch community midwife, the British model of maternity care) in regard to the impact they have on the relationship between motivation and burnout. From the findings of the present investigation and related research done by others (Bakker et al., 1996; Hunter, 2004; Hyde & Roche-Reid, 2004), it can be concluded that a different form of work organization in midwifery in Denmark will have a positive influence on the serious health status of Danish midwives found in the PUMA study. The conclusions drawn from the present case need to be interpreted on the background of the specific context investigated. New understanding about burnout and motivation in midwifery in Denmark has grown and at the same time new questions came about, as new knowledge sets everything known before into new perspective. The wisdom from this case is regarded as being creative source for new projects, especially those which put high priority on understanding well researched phenomena in a specific context.
256
References Allen, T.D., Herst, D.E.L., Bruck, C.S. & Sutton, M. (2000). Consequences Associated With Work-Family Conflict: A Review and Agenda for Future Research. Journal of Occupational Health Psychology, 5(2), 278-308. Ashkanasy, N.M., Härtel, C.E.J., & Zerbe, W.J. (2000). Emotions in the workplace. Research, Theory, and Practice. London: Quorum Books. Bakker, R.H.C., Groenewegen, P.P., Jabaaij, L., Meijer, W., Sixma, H. & de Veer, A. (1996). ‘Burnout’ among Dutch midwives. Midwifery, 12, 174-181. Barnett, R. (1998). Toward a Review and Reconceptualization of the Work/Family Leisure. Genetic, Social, and General Psychology Monographs, 124(2), 125-182. Bazeley, P. & Richards, L. (2000). The NVivo Qualitative Project Book. London: Sage. Benoit, C., Davis-Floyd, R., van Teijlingen, E.R., Sandall, J. & Miller, J.F. (2001). Designing Midwives. In R. Devries, C. Benoit, E.R. van Teijlingen & S. Wrede, (Eds.), Birth by Design, p. 139-165. London: Routledge. Borritz, M. (2005). Burnout in human service work – causes and consequences. Ph.D. thesis, NIOH, Copenhagen. Borritz, M., Bültmann, U., Rugulies, R., Christensen, K.B., Villadsen, E. & Kristensen, T.S. (2005). Psychosocial Work Characteristics as Predictors for Burnout: Findings From 3-Year Follow Up of the PUMA Study. Journal of Occupational and Environmental Medicine, 47, 1015-1025. Brotheridge, C.M. & Grandey, A.A. (2002). Emotional Labour and Burnout: Comparing Two Perspectives of “People Work”. Journal of Vocational Behaviour, 60, 17-39. Brucks, U. (1998). Arbeitspsychologie personenbezogener Dienstleistungen. (Schriften zur Arbeitspsychologie, Nr. 56, herausgegeben von E. Ulich). Bern: Hans Huber. Brunstein, J. C., Lautenschlager, U., Nawroth, B., Pöhlmann, K. & Schultheiss, O. (1995). Persönliche Anliegen, soziale Motive und emotionales
257
Wohlbefinden. Zeitschrift für Differentielle und Diagnostische Psychologie, 16 (1), 1-10. Brunstein, J.C., Schultheiss, O.C., & Grässmann, R. (1998). Personal goals and emotional well-being: the moderating role of motive dispositions. Journal of Personality and Social Psychology, 75(2), 494-508. Büssing, A. (1992). Ausbrennen und Ausgebranntsein. Psychosozial, 15(IV/52), 42-50. Burisch, M. (1989). Das Burnout-Syndrom: Theorie der inneren Erschöpfung. Springer Verlag: Berlin. Burisch, M. (2002). A longitudinal study of burnout: the relative importance of dispositions and experiences. Work & Stress, 16(1), 1-17. Burke, R.J. & Greenglass, E.R. (2001). Hospital restructuring, work family conflict and psychological burnout among nursing staff. Psychology & Health, 16(5), 583-594. Cherniss, C. (1995). Beyond burnout. New York: Routledge. Christians, C.G. (2000). Ethics and Politics in Qualitative Research. In N.K. Denzin & Lincoln, Y.S. (Eds.), Handbook of Qualitative Research, p. 133-155. London: Sage. Christensen, S. (2003). hvad går jeg her og fløjter for. en antropologisk analyse af arbejde med mennesker. Institut for Antropologi, København. Cliff, H. (2002). Fast Ansat Ved Mysteriet. Den Almindelige Danske Jordemoderforening (DADJ). Creswell, J.W. (2003). Research Design. Qualitative, Quantitative, and Mixed Methods Approaches 2nd edition. London: Sage. Csikszentmihalyi, M. (1985). Emergent motivation and the evolution of the self. Advances in Motivation Achievement, 4, 93-119. Csikszentmihalyi, M. (1990). Flow – Das Geheimnis des Glücks. Stuttgart: Klett-Cotta. Csikszentmihalyi, M., LeFevre, J. (1989). Optimal Experience in Work and Leisure. Journal of Personality and Social Psychology, Vol. 56, No. 5, 815-822.
258
Demerouti, E., Bakker, A.B., Nachreiner, F., Schaufeli, W.B. (2001). The Job Demands-Resources Model of Burnout. Journal of Applied Psychology, 86(3), 400-512. Denzin, N.K. & Lincoln, Y.S. (2000). Handbook of Qualitative Research. London: Sage. De Vries, R.G. (1993) A cross-national view of the status of midwives. In E. Riska & Wegar, K. (Eds.), Gender, Work and Medicine: Women and the Medical Division of Labour, pp. 131-146, London: Sage. DeVries, R., Benoit, C., Van Tejlingen, E.R. & Wrede, S. (2001). Birth by Design. Pregnancy, Maternity Care, and Midwifery in North America and Europe. London: Routledge. Dlugos, R.F. & Friedlander, M.L. (2001). Passionately Committed Psychotherapists: A Qualitative Study of Their Experiences. Professional Psychology: Research and Practice, 32(3), 298-304. Dyhr, M. (1999). Karakteristiske psykosociale belastninger i jordemødres arbejdsmiljø. Master of Public Health Afhandling, Institut for Folkesundhedsvidenskab, Københavns Universitet. Engelbrecht, S. (2001). Hinsides arbejdsengagement. In H.H. Larsen (red.). Noget for Noget? Rekruttering og fastholdelse af unge højtuddannede. København: Berlinske Annoncecenter. Feyerabend, P. (1976). Wider den Methodenzwang. Frankfurt am Main: Suhrkamp. Flick, U. (2000). Triangulation in der qualitativen Forschung. In U. Flick, von Kardorff, E. & Steinke, I. (Hrsg.). Qualitative Forschung, S. 309-318. Reinbek: Rowohlt Taschenbuch Verlag. Flick, U. (2002). Qualitative Sozialforschung. Eine Einführung. Reinbek: Rowohlt Taschenbuch Verlag. Fisher, C.D. & Ashkanasy, N.M (2000). The emerging role of emotions in work life: an introduction. Journal of Organizational Behaviour, 21, 123-129. Fog, J. (1994). Med samtalen som udgangspunkt. Det kvalitative forskningsinterview. Akademisk Forlag.
259
Fontana, A. & Frey, J.H. (2000). The Interview. From Structured Questions to Negotiated Text. In N.K. Denzin & Lincoln, Y.S. (2000). Handbook of Qualitative Research, pp. 645-672. London: Sage. Frankenhaeuser, M. (1991). The Psychology of Workload, Stress, and Health: Comparison between the Sexes. Workload, Stress and Health, 13(4), 197-204. Freudenberger, H.J. (1974). Staff burn-out. Journal of Social Issues, 30(1), 159-165. Freudenberger, H. & G. Richelson (1980). Burnout: The high cost of high achievement. Garden City, NY: Anchor Press. Friedman, I.A. (2000). Burnout in Teachers: Shattered Dreams of Impeccable Professional Performance. Psychotherapy in Practice, 56(5), 595-606. Gadamer, H.-G. (1960/1990). Hermeneutik I. Wahrheit und Methode. Grundzüge einer philosophischen Hermeneutik. Tübingen: J.C.B. Mohr. Gergen, K.J. (1992). Toward a Postmodern Psychology. In S. Kvale, Psychology and Postmodernism, pp. 17-30. London: Sage. Geurts, S., Rutte, C. & Peeters, M. (1999). Antecedents and consequences of work-home interference among medical residents. Social Science & Medicine, 48, 1135-1148. Geurts, S. & Demerouti, E. (2003). Work/Non-Work Interface: A Review of Theories and Findings. In M.J. Schabracq, Winnubst, J.A.M. & Cooper, C.L., The Handbook of Work and Health Psychology, 279-312. Giorgi, A. (1975). An Application of Phenomenological Method in Psychology. In: A. Giorgi, C. Fisher & E. Murray (eds.): Duquesne Studies in Phenomenological Psychology, II. Pittsburgh: Duquesne University, 82-103. Giorgi, A. (1985). Sketch of a phenomenological method. In A. Giorgi, (ed.). Phenomenological and psychological research. Pittsburgh: Duquesne University Press, 8-22. Golembiewsky, R.T. & Munzenrider, R.F. (1988). Phases of burnout: Developments, and Concepts and Applications. New York:Praeger.
260
Gordon, D.R., Ames, G.M., Yen, I.H., Gillen, M., Aust, B., Rugulies, R., Frank, J.W. & Blanc, P.D. (2005). Integrating Qualitative Research into Occupational Health: A Case Study Among Hospital Workers. Journal of Occupational Environmental Medicine, 47(4), 399-409. Greif, S. (1993). Mensch-Computer Interaktion, psychologische Theorien und innovatives Problemlösen. In T. Herrmann & Bungard, W. (Hrsg.), Arbeits- und Organisationspsychologie im Spannungsfeld zwischen Grundlagenorientierung und Anwendung, pp. 145-166. Bern: Huber. Greif, S., Runde, B. & Seeberg, I. (2004). Erfolge und Misserfolge beim Change Management. Göttingen: Hogrefe. Grosch, W.N. & Olsen, D.C. (1994). When helping starts to hurt: A new look at burnout among psychotherapists. New York: Norton. Guba, E.E. & Y. Lincoln (1985). Naturalistic Inquiry. London: Sage. Hacker, W. (1986). Arbeitspsychologie. Psychische Regulation von Arbeitstätigkeiten. Berlin: VEB Deutscher Verlag der Wissenschaften. Hallsten, L. (1993). Burning out: A framework. In W.B. Schaufeli, Maslach, C. & Marek, T. (Eds.), Professional Burnout: Recent developments in theory and research, pp. 95-113, Washington DC: Taylor & Francis. Harada, H., Y. Suwazono, K. Sakata, Y. Okubo, M. Oishi, M. Uetani, E. Kobayashi & E. Nogawa (2005). Three-shift system increases job-related stress in Japanese workers. Journal of Occupational Health, 47(5), 536-541. Hasenfeld, Y. (1983). Human Service Organisations. Engelwood Cliffs: Prentice Hall. Hauge, B. (2005). Følelsesfælleskabet. Det kvalitative interview i emotionelle felter. In C. Baarts & Fredslund, H. (eds.). Perspektivet – kvalitative forskning i arbejdsmiljø og arbejdsliv, s. 76-99. København: Arbejdsmiljøinstituttet. Herbig, B. (2001). Vergleichende Untersuchung von Struktur und Inhalt expliziten und impliziten Wissens. Aachen: Shaker. Hobfall, S.E. (1989). Conservation of resources: A new attempt of conceptualizing stress. American Psychologist, 44, 513-524.
261
Hobfall, S.E. & Freedy, J. (1993). Conservation of resources: A general stress theory applied to burnout. In W.B. Schaufeli, Maslach, C. & Marek, T. (Eds.), Professional Burnout: Recent developments in theory and research, pp. 115-129, Washington DC: Taylor & Francis. Hochschild, A.R. (1983). The Managed Heart. Berkeley: University of California Press. Holstein, J.A. & Gubrium, J.F. (1995). The active interview. Thousands Oaks, CA: Sage. Hunter, B. (2004). Conflicting ideologies as a source of emotion work in midwifery. Midwifery, 20, 261-272. Hunter, B. (2005). Emotion work and boundary maintenance in hospital-based midwifery. Midwifery, 21(3), 253-266. Hyde, A. & Roche-Reid, B. (2004). Midwifery practice and the crisis of modernity: implications for the role of the midwife. Social Science and Medicine, 58, 2613-2623. Jansen, N.W.H, Kant, I.J., Kristensen, T.S. & Nijhuis, F.J.N. (2003). Antecedents and Consequences of Work-Family Conflict: A Prospective Cohort Study. JOEM, 45(5), 479-491. Jansen, N.W.H, Kant, I.J., Nijhuis, F.J.N., Swaen, G.M.H., Kristensen, T.S. (2004). Impact of worktime arrangements on work-home interference among Dutch employees. Scandinavian Journal of Environmental Health, 30(2), 139-148. Jordemoderforeningens Medlemsundersøgelse. Resonans Aps. (2003). http://www.jordemoderforeningen.dk/multimedia/Medlemsundersøgelse_-_hovedrapporten.pdf Kalimo, R., Pahkin, K., Mutanen, P. & Toppinen-Tanner, S. (2003). Staying well or burning out at work: work characteristics and personal resources as long-term predictors. Work & Stress, 17(2), 109-122. Kanfer, R. (1990). Motivation Theory and Industrial and Organizational Psychology. In M.D. Dunette & Hough, L.M. (Eds.) Handbook of Industrial and Organizational Psychology. Palo Alto: Consulting Psychologists Press, Inc.
262
Karasek, R. (1979). Job demands, job decision latitude, and mental strain: Implications for job redesign. Administrative Science Quarterly, 24, 285-307. Karasek, R. & Theorell, T. (1990). Healthy Work. Stress, Productivity, and the Reconstruction of Working Life. Basic Books. Kelly, G.A. (1955). The psychology of personal constructs. New York: Norton. Kirkcaldy, B.D., Athanasou, J.A. & Trimpop, R. (2000). The idiosyncratic construction of stress: examples from medical work settings. Stress Medicine, 16, 315-326. Kirkeby, O.F. (1994). Abduktion. In: H. Andersen (ed.), Videnskabsteori og metodelære. Bind 1. Introduktion. København: Samfundslitteratur, 122-153. Kivimäki, M., Elovainio, M., Vahtera, J., Ferrie, J.E. (2003). Organisational justice and health of employees: prospective cohort study. Occupational Environmental Medicine, 60, 27-34. Kleining, G. (1982). Umriss zu einer Methodologie Qualitativer Sozialforschung. Kölner Zeitschrift für Soziologie und Sozialpsychologie, 34, 224-253. Kristensen, T.S. & Borritz, M. (1998). Forbyggelse af udbrændthed. En forundersøgelses-rapport. København: Arbejdsmiljøfondet. Kristensen, T.S. & Borritz, M., Villadsen, E. & Christensen, K.B. (2005a). The Copenhagen Burnout Inventory: A new tool for the assessment of burnout. Work & Stress, 19(3), 192-207. Kristensen T.S., Hannerz, H., Høgh, A. & Borg, V. (2005b). The Copenhagen Psychosocial Questionnaire (COPSOQ). A tool for the assessment and improvement of the psychosocial work environment. Scandinavian Journal of Work and Environmental Health (In press). Kruml, S.M. & Geddes, D. (2000). Catching fire without burning out: Is there an ideal way to perform emotional labour? In N.M. Ashkanasy, Härtel, C.E.J., & Zerbe, W.J. (2000). Emotions in the workplace. Research, Theory, and Practice, pp. 177-188. London: Quorum Books. Kuhl, J. (2000). A Functional-Design Approach to Motivation and Self-regulation. In M. Boekarts, Pintrich, P.R. & Zeidner, M., Self-regulation: Direction and challenges for further research, pp. 111-169. Academic Press.
263
Kuhl, J. & Scheffer, D. (2001). The Operant Motive Test (OMT). Scoring manual, test characteristics and empirical validation. Universität Osnabrück. Kuhn, T. (1970). The structure of scientific revolutions, 3rd ed. Chicago: University of Chicago Press. Kvale, S. (1989). Issues of Validity in Qualitative Research. Lund: Studentlitteratur. Kvale, S. (1994). Interview. Copenhagen: Hans Reitzel. Kvale, S. (2002). Dialogue as oppression and interview research. Center for kvalitative metodeudvikling, nyhedsbrev nr. 32, maj 2002. Lamnek, S. (2005). Qualitative Sozialforschung. Weinheim: Beltz. Law, M., Stewart, D., Letts, L., Pollock, N., Bosch, J., & Westmorland, M. (1998). Guidelines for Critical Review Form – Qualitative Studies. http://www-fhs.mcmaster.ca/rehab/ebp/pdf/ qualguidelines.pdf Lazarus, R.S. & Lazarus, B.N. (1994). Passion & Reason. Making sense of our emotions. New York: Oxford University Press. Lee, R.T. & Ashforth, B.E. (1996). A Meta-Analytic Examination of the Correlates of the Three Dimensions of Job Burnout. Journal of Applied Psychology, 81 (2), 123-133. Leiter, M.P, (1993). ‘Burnout as developmental process: Consideration of models’. In W.B. Schaufeli, Maslach, C. & Marek, T. (Eds.), Professional Burnout: Recent developments in theory and research, pp. 237-250, Washington DC: Taylor & Francis. Lincoln, Y.S. & Guba, E.G. (1985). Naturalistic Inquiry. London: Sage. Locke, E.A. & Latham, G.P. (1984). Goal setting: A motivational technique that works. Englewood Cliffs, NJ: Prentice Hall. Ludewig, K. (1992). Systemische Therapie. Stuttgart: Klett Cotta. Malterud, K. (1996). Kvalitative metoder i medisinsk forskning. Tano Aschehoug.
264
Malterud, K. (2001). Qualitative research: standards, challenges and guidelines. The Lancet, Vol. 358, 483-488. Masberg, M. (2004). Wissensmanagement bei geplantem Führungswechsel – Entwicklung eines Modells. Dissertation an der Universität Hamburg. http://www.sub.uni-hamburg.d/ opus/volltexte/2004/2273. Maslach, C. (1976). Burned-out. Human Behavior, 5, 16-22. Maslach, C. & Leiter, M.P. (1997). The truth about burnout. San Francisco: Jossey-Bass. Maslach, C. & Jackson, S. (1981). The measurement of experienced burnout. Journal of Occupational Behaviour, 2, 99-113. Maslach, C. & Jackson, S. (1982). Maslach Burnout Inventory Manual. 2nd ed. Palo Alto, CA: Consulting Psychologists Press. Maslach, C. & Jackson, S. (1986). The measurement of experienced burnout. Journal of Occupational Behavior, 2, 99-113. Maslach, C., Schaufeli, W.B. & Leiter, M.P. (2001). Job Burnout. Annual Review of Psychology, 52, 397-422. McClelland, D.C. (1987). Human Motivation. Cambridge: University Press. McClelland, D.C., Koester, R. & Weinberger, J. (1989). How Do Self-Attributed Motives Differ? Psychological Review, 96(4), 690-702. McNeese-Smith, D.K. (2000). Job Stages of Entry, Mastery, and Disengagement among Nurses. JONA, 30 (3), 140-147. McMichael A.J. (1976). Standardized mortality ratios and the “healthy worker effect”: Scratching beneath the surface. Journal of Occupational Medicine, 18, 165-168. Menzies, I.E.P. (1975). A case-study in the functioning of social systems as defense against anxiety. In A.D. Colman & Bexton, W.H. (ed.). Group Relations 1. Washington: A.K. Rice Institute. Meyer, J.P. & Allen, N.J. (1997). Commitment in the Workplace. Theory, research, and Application. Thousands Oaks, California: Sage.
265
Molnar, C. (2004) Woman’s Work. Midwifery Today. Spring 2004. Moustakas, C. (1994). Phenomenological Research Methods. London: Sage. Niitamo, P. (1999). “Surface” and “Depth” in Human Personality: Relations Between Explicit and Implicit Motives. Helsinki: Institute of Occupational Health Pedersen, B. (2002). Udbrændthed. Nordiske Udkast, 2, 55-76. Polanyi, M. (1985). Implizites Wissen. Frankfurt am Main: Suhrkamp. (American Original first published in 1966 with the title “The tacit dimension”). Porter, L.W., Steers, R.M., Mowday, R. & Boulian, P.V. (1974). Organizational Commitment, job satisfaction, and turnover among psychiatric technicians. Journal for Applied Psychology, 59, 603-609. Pines, A.M. (1993). Burnout: An existential perspective. In W.B. Schaufeli, Maslach, C. & Marek, T. (Eds.) Professional Burnout: Recent Developments in Theory and Research, pp. 33-51, Washington, DC: Taylor & Francis. Pines, A., Aronsson, E. & Kafry, D. (1981). Burnout: from tedium to personal growth. New York: The Free Press. Rösing, I. (2003). Ist die Burnout-Forschung ausgebrannt? Heidelberg: Asanger. Rothschild, B. (2000). The Body Remembers. The Psychophysiology of Trauma and Trauma Treatment. London: W.W. Norton & Company. Sandall, J. (1997). Midwives’ burnout and continuity of care. British Journal of Midwifery, 5(2), 106-111. Schaufeli, W.B. & Bakker, A.B. (2003). Utrecht Work Engagement Scale. Preliminary manual, Version 1, November, 2003. Utrecht University: Occupational Health Psychology Unit. Schaufeli, W.B. & Bakker, A.B. (2004). Job demands, job resources and their relationship with burnout and engagement: A multi-sample study. Journal of Organizational Behavior, 25, 293-315.
266
Schaufeli W B & Buunk B.P. (2003). Burnout: An Overview of 25 Years of Research and Theorizing. In: M. Schabracq, Winnubst, J.A.M. and Cooper, C.L. (eds.). The Handbook of Work and Health Psychology. John Wiley & Sons, Ltd. Schaufeli, W. & Enzmann, D. (1998). The burnout companion to study and practice. A critical analysis. London: Taylor & Francis. Schaufeli, W.B., Leiter, M.P., Maslach, C. & Jackson, S.E. (1996). The MBI-General Survey. In C. Maslach & S.E. Jackson (eds.). Maslach Burnout Inventory (3rd edn.), pp. 19-26. Palo Alto, CA: Consulting Psychologists Press. Schaufeli, W.B., Salanova, M., González-Romá, V. & Bakker, A. (2002). The Measurement of Engagement and Burnout: A Two Sample Confirmatory Factor Analytic Approach. Journal of Happiness Studies, 3, 71-92. Schaufeli, W.B., Taris, T., LeBlanc, P., Peeters, M., Bakker, A. & de Jonge, J. (2001). Maakt arbeid gezond? De Psycholoog, p. 422-428. Schaufeli, W. B. & Taris, T.W. (2005). The conceptualization and measurement of burnout: Common grounds and worlds apart. Work & Stress, 19 (3), 256 -262. Scheffer, D. (2001). Entwicklungsbedingungen impliziter Motive. Bindung, Leistung & Macht. Dissertation an der Universität Osnabrück. http://elib.ub.uni-osnabrueck.de/ publications/diss/E-Diss150_thesis.pdf. Schmitz, E. (1998). Brennt wirklich aus, wer entflammt war? Eine LISREL-Analyse zum Burnout-Prozess bei Sozialberufen. Psychologie, Erziehung, Unterricht, 45, 129-142. Schmitz, E. & Leidl, J. (1999). Brennt wirklich aus, wer entflammt war? Studie 2: Eine LISREL-Analyse zum Burnout-Prozess bei Lehrpersonen. Psychologie, Erziehung, Unterricht, 46, 302-310. Seale, C. (1999). Quality in Qualitative Research. Qualitative Inquiry, 5(4), 465-478. Seeberg, J. (2001). Nvivo 2.0 træningsmanual: Nvivo hands-on workshop. HRA Consult. Siegrist, J. (1996). Adverse Health Effects of High-Effort/Low-Reward Conditions. Journal of Occupational Health Psychology, 1(1), 27-41.

267
Siegrist, J., Starke, D., Chandola, T., Godin, I., Marmot, M., Niedhammer, I. & Peter, R. (2004). The measurement of effort-reward imbalance at work: European comparisons. Social Science & Medicine, 58, 1483-1499. Singh, S. N., Mishra, S. & Kim, D. (1998). Research-related burnout among faculty in higher education. Psychological Reports, 83, 463-473. Skostad, A. & S. Einarsen (1996). Perspektiver på begrepet psykosocialt arbeidsmiljø. En analyse av en motivasjonspsykologisk og en stressteoretisk modell. Nordisk Psykologi, 48(3), 200-213). Smith, P.C., Kendall, L.M. & Hulin, C.L. (1969). The measurement of satisfaction in work and retirement. Chicago: Rand-McNally. Söderfeldt, M. (1997). Burnout? Lund University: School of Social Work Sokolowski, R. (2000). Introduction to Phenomenology. Cambridge: University Press. Sonnentag, S. (2001). Work, Recovery Activities, and Individual Well-Being: A Diary Study. Journal of Occupational Health Psychology, 6(3), 196-210. Steinke, I. (2000). Gütekriterien qualitativer Forschung. In U. Flick, von Kardorff , E. & Steinke, I. (Hg.). Qualitative Forschung, S. 39-331. Reinbek: Rowohlt Taschenbuch Verlag. Strauss, A. (1998). Grundlagen qualitativer Sozialforschung: Datenanalyse und Theoriebildung in der empirischen und soziologischen Forschung. 2nd Edition. München: Fink. Strauss, A., Farahaugh, S., Suczek, B. & Wiener, C. (1980). Gefühlsarbeit. Ein Beitrag zur Arbeits- und Berufssoziologie. Kölner Zeitschrift für Soziologie und Sozialpsychologie, 32, 629-651. Sundhedsstyrelsen. Center for Evaluering og Medicinisk Teknologivurdering (2005). Kejsersnit På Moders Ønske. www.cemtv.dk. Tan, D.S.K. & Akhtar, S. (1998). Organizational commitment and experienced burnout: an exploratory study from a Chinese cultural perspective. The International Journal of Organizational Analysis, 6 (4), 310-333.
268
Tausig, M. & Fenwick, R. (2001). Unbinding Time: Alternate Work Schedules and Work-Life Balance. Journal of Family and Economic Issues, 22(2), 101-119. Thomsen, L. (2002). Undersøgelse af psykosocialt arbejdsmiljø – overvejelser omkring et sammenlignende casestudie i hjemmeplejen. Institut for Psykologi, Københavns Universitet. Van Manen, M. (1990). Hermeneutic Phenomenological Reflection, In M. Van Manen. Researching lived experience. Human Science for an action sensitive pedagogy. New York: State University of New York Press, p. 77-109. Visholm, S. (2004). Organisationspsykologi og psykodynamisk systemteori. In T. Heinskou & Visholm, S. Psykodynamisk Organisationspsykologi. På arbejde under overflåden, s. 23-48. København: Hans Reitzels Forlag. Vogt, J., Leonhardt, J. Köper, B. & Pennig, S. (2004). Economic evaluation of the Critical Incident Stress Management Programme. The International Journal of Emergency Mental Health, 6(4), 185-196. Winwood, P.C. & Winefield, A.H. (2004). Comparing two Measures of Burnout Among Dentists in Australia. International Journal of Stress Management, 11(3), 282-289. Wolff, S. (2000). Wege ins Feld und ihre Varianten. In Flick, U., von Kardorff, E. & Steinke, I. (Eds.). Qualitative Forschung, S. 334-348. Reinbek: Rowohlt Taschenbuch Verlag. Zapf, D., Seifert, C., Schmutte, B., Mertini, H. & Holz, M. (2001). Emotion work and job stressors and their effects on burnout. Psychology and Health, 16, 527-545. Zapf, D., Vogt, C., Seifert, C., Mertini, H. & Isic, A. (1999). Emotion Work as Source of Stress: The Concept and Development of an Instrument. European Journal of Work and Organizational Psychology, 8(3), 371-400.
269
List of Figures Figure 2.1 Existential model of burnout. Figure 2.2 Emotion psychological triangle. Figure 3.1 Model of different research strategies. Figure 3.2 Stages of the project investigating the relationship between
motivation and burnout in human service work. Figure 8.1 Primary and secondary tasks, agents, and structural and conditional
aspects of midwifery. Figure 8.2 Vicious cycle of declining resources.
270
List of Tables Table 2.1 List of symptoms of burnout Table 2.2 Chronological listing of common burnout definitions Table 2.3 Strength and weaknesses of contemporary burnout research Table 3.1. The average scores on the CBI burnout scales of the jobs in the
PUMA baseline study Table 3.2. Job classifications in midwifery in Denmark Table 3.3. Types of observation Table 3.4. Age profile of midwives working at the ward Table 3.5. Demographic profile of interview partners in the single interviews Table 3.6. Research questions and related interview questions Table 3.7 Interview guide for group interview
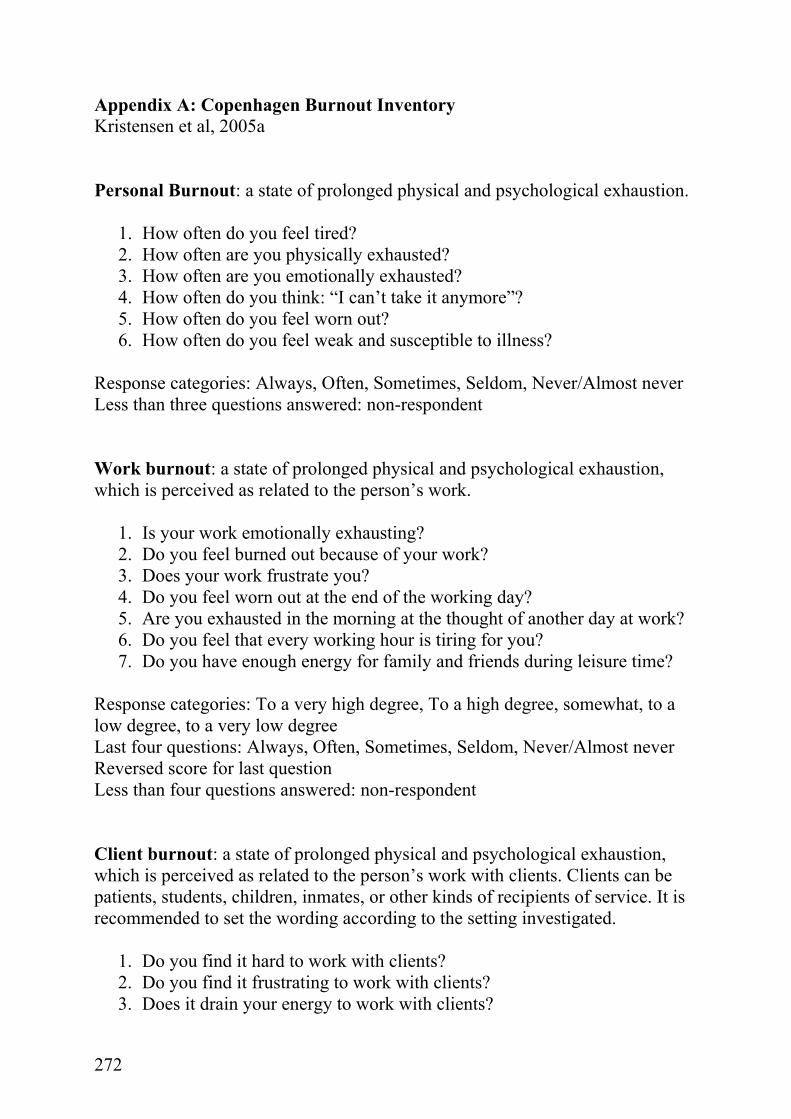
271
Appendices A: Copenhagen Burnout Inventory (CBI, Kristensen et al. 2005a) B: Demographic Questions C: Interview guide for single interviews D: Rules for Transcription E: Comprehensive list of quality criteria for qualitative research
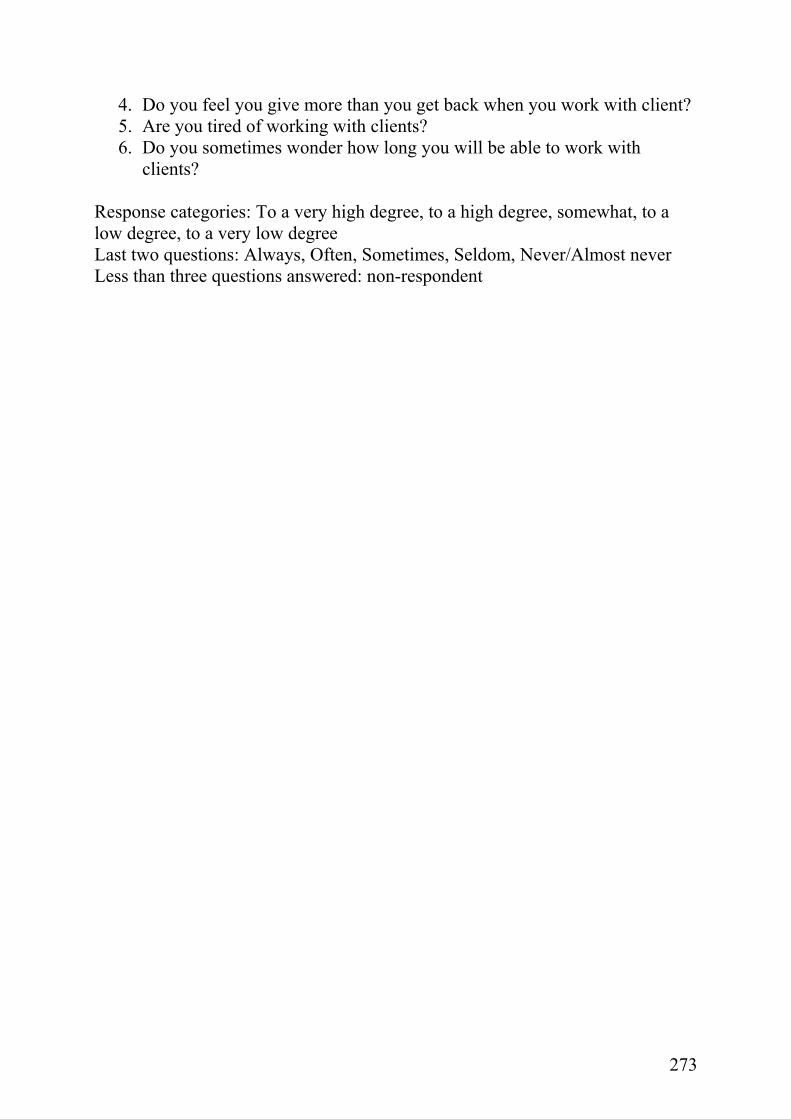
272
Appendix A: Copenhagen Burnout Inventory Kristensen et al, 2005a Personal Burnout: a state of prolonged physical and psychological exhaustion.
1. How often do you feel tired? 2. How often are you physically exhausted? 3. How often are you emotionally exhausted? 4. How often do you think: “I can’t take it anymore”? 5. How often do you feel worn out? 6. How often do you feel weak and susceptible to illness?
Response categories: Always, Often, Sometimes, Seldom, Never/Almost never Less than three questions answered: non-respondent Work burnout: a state of prolonged physical and psychological exhaustion, which is perceived as related to the person’s work.
1. Is your work emotionally exhausting? 2. Do you feel burned out because of your work? 3. Does your work frustrate you? 4. Do you feel worn out at the end of the working day? 5. Are you exhausted in the morning at the thought of another day at work? 6. Do you feel that every working hour is tiring for you? 7. Do you have enough energy for family and friends during leisure time?
Response categories: To a very high degree, To a high degree, somewhat, to a low degree, to a very low degree Last four questions: Always, Often, Sometimes, Seldom, Never/Almost never Reversed score for last question Less than four questions answered: non-respondent Client burnout: a state of prolonged physical and psychological exhaustion, which is perceived as related to the person’s work with clients. Clients can be patients, students, children, inmates, or other kinds of recipients of service. It is recommended to set the wording according to the setting investigated.
1. Do you find it hard to work with clients? 2. Do you find it frustrating to work with clients? 3. Does it drain your energy to work with clients?
273
4. Do you feel you give more than you get back when you work with client? 5. Are you tired of working with clients? 6. Do you sometimes wonder how long you will be able to work with
clients? Response categories: To a very high degree, to a high degree, somewhat, to a low degree, to a very low degree Last two questions: Always, Often, Sometimes, Seldom, Never/Almost never Less than three questions answered: non-respondent
274
Appendix B: Demographic questions Tilmelding til interview (Send venligst tilbage senest den 1. november 2002. Jeg kan desværre ikke garantere at alle tilmeldte vil blive interviewet.) Navn ___________________________________________
Adresse _________________________________________
Telefon/evt. træffetid ______________________________
Hvad er din jobfunktion? Ledende jordemoder Afdelingsjordemoder Jordemoder Hvor længe har du været ansat på denne afdeling? Cirka: ____ år og ____ måneder Hvor længe har du sammenlagt arbejdet som jordemoder? Cirka: ____ år og ____ måneder Har du en anden erhvervsuddannelse og hvis ja, hvilken? Ja, ______________________________________________ Nej Hvor gammel er du? ____ år Er du gift/samboende? Ja Nej Hvor mange hjemmeboende børn har du? Antal: _____ Hvor mange af disse er under 7 år? Antal: _____ Har du deltaget i PUMA-undersøgelsen? Ja, i første runde Ja, i anden runde Ja, i begge runde Nej Tak for oplysningerne. Jeg kontakter dig så snart jeg har valgt interviewpersonerne ud fra de blanketter jeg har fået tilbage. Venlig hilsen Sunniva Engelbrecht
275
Appendix C: Interviewguide for single interviews Aim / agreements
• Focus is on personal emotions and understanding; there is no right or wrong; the interest is personal experience
• Agreements: Use of memory stick to safe data; secrecy/anonymity; authorization for use of citations will be asked before publication; permission to discuss outcomes of single interviews in group interview sessions
• Interview has different themes. The researcher is responsible to hold the focus.
• Ask, if there are any questions. 1. Introductory Questions
• Career (kind of education, reason to become midwife, way to get in, time being midwife, time being in the present job)
• Participation in PUMA (How have you been involved?) • Positive and negative experiences in relation to PUMA study? • If you think of an ordinary day, what motivates you to go to work?
2. Practice concept of motivation and burnout
• How would you describe a person who is engaged in her/his work? • How would you describe a person who is burned out?
3. Personal meaning of burnout
• What does burnout mean to you? • Have you ever felt burned out? If yes, can you describe the experience?? • What did you do?
4. Personal motivation and aim
• Can you describe what makes you involved in your work? • If the good fairy gave you three wishes that could improve your work
motivation, what would they be?
276
5. Emotions in relation to motivation
• Do you remember a situation were you were very motivated? • How would you describe the emotional experience in that situation? • Do you remember a situation where you lost you involvement in the
work? Can you describe the situation and your behaviour? • Exactly, what happened when you lost your motivation? • How would you describe the emotional experience in that situation? • Who/what helped you in that situation?
6. Question about the future
• If you imagine you could look ahead in time, where do you stand in relation to your work one year from today?
7. Closure
• Is there something you want to supply? • Thank you! • Ask for permission to contact the interview partner again if necessary.
277
Appendix D: Rules for transcription All participants get an identification number at the beginning of the investigation. No names are connected to the transcribed form of the interviews in order to assure anonymity of the participant. In case the name of the participant is said in the course of the interview it is exchanged by IP plus the number of the interview person. The text is transcribed as heard from the recording. Pauses are marked (pause), “øh’er” or other small remarks are also written down in order to be able to take a look at the flow of the conversation (e.g., hesitation). The text is formatted in Times New Roman style, 12 point. Not finished sentences should be finished with …. . Any sound from the tape e.g. latter, which is not spoken is noted in [] brackets. Spoken words, which are not to understand, are written down as [utydelig tale] The interviewer is marked as S: (return), the interview person is marked as IP: (return). With change of subject should there be double space. As soon as I have received the transcribed text, the file should be deleted from your computer (wait until I have affirmed the delivery of the file).
Home address Sunniva Engelbrecht Katharinenkirchhof 1 20457 Hamburg Tyskland 0049-40-33395092
Work address Sunniva Engelbrecht Lersø Parkallé 105 2100 København Ø [email protected]
278
Appendix E: Guidelines for qualitative research Malterud, 2001; Steinke, 2000 Aim
• Is the research question a relevant issue? • Is the aim sufficiently focused, and stated clearly? • Does the title of the article give a clear account of the aim?
Reflexivity
• Are the researcher’s motives, background, perspectives, and preliminary hypotheses presented, and is the effect of theses issues sufficiently dealt with?
Method and design
• Are qualitative research methods suitable for exploration of the research question?
• Has the best method been chosen with respect to the research question? Data collection and sampling
• Is the strategy for data collection clearly stated (usually purposive or theoretical, usually not random or representative)?
• Are the reasons for this choice stated? • Has the best approach been chosen; in view of the research question? • Are the consequences of the chosen strategy discussed and compared with
other options? • Are the characteristics of the sample presented in enough depth to
understand the study site and context? Theoretical framework
• Are the perspectives and ideas used for data interpretation presented? • Is the framework adequate, in view of the aim of the study? • Does the author account for the role given to the theoretical framework
during analysis?
279
Analysis • Are the principles and procedures for data organisation and analysis fully
described, allowing the reader to understand what happened to the raw material to arrive at the results?
• Were the various categories identified from theory or preconceptions in advance, or were they developed from the data?
• Which principles were followed to organise the presentation of the findings?
• Are strategies used to validate results presented, such as cross-check for rivalling explanations, member checks, or triangulation? (If such strategies are not described in this section, they should appear as validity discussions later in the report.)
Findings
• Are the findings relevant with respect to the aim of the study? • Do they provide new insight? • Is the presentation of the findings well organised and best suited to ensure
that findings are drawn from systematic analysis of material, rather than from preconceptions?
• Are quotes used adequately to support and enrich the researcher’s synopsis of the patterns identified by systematic analysis?
Discussion
• Are questions about internal validity (what the study is actually about); external validity (to what other settings the findings or notions can be applied), and reflexivity (the effects of the researcher on processes, interpretations, findings, and conclusions) addressed?
• Has the design been scrutinised? • Are the shortcomings accounted for and discussed, without denying the
responsibility of choices taken? • Have the findings been compared with appropriate theoretical and
empirical references? • Are a few clear consequences of the study proposed?

280
Presentation
• Is the report easy to understand and clearly contextualised? • Is it possible to distinguish between the voices of the informants and those
of the researcher? References
• Are important and specific sources in the field covered, and have they been appropriately presented and applied in the text?





























