Embed Size (px)
Citation preview
8873
September 18, 1993 691
EDITORIAL
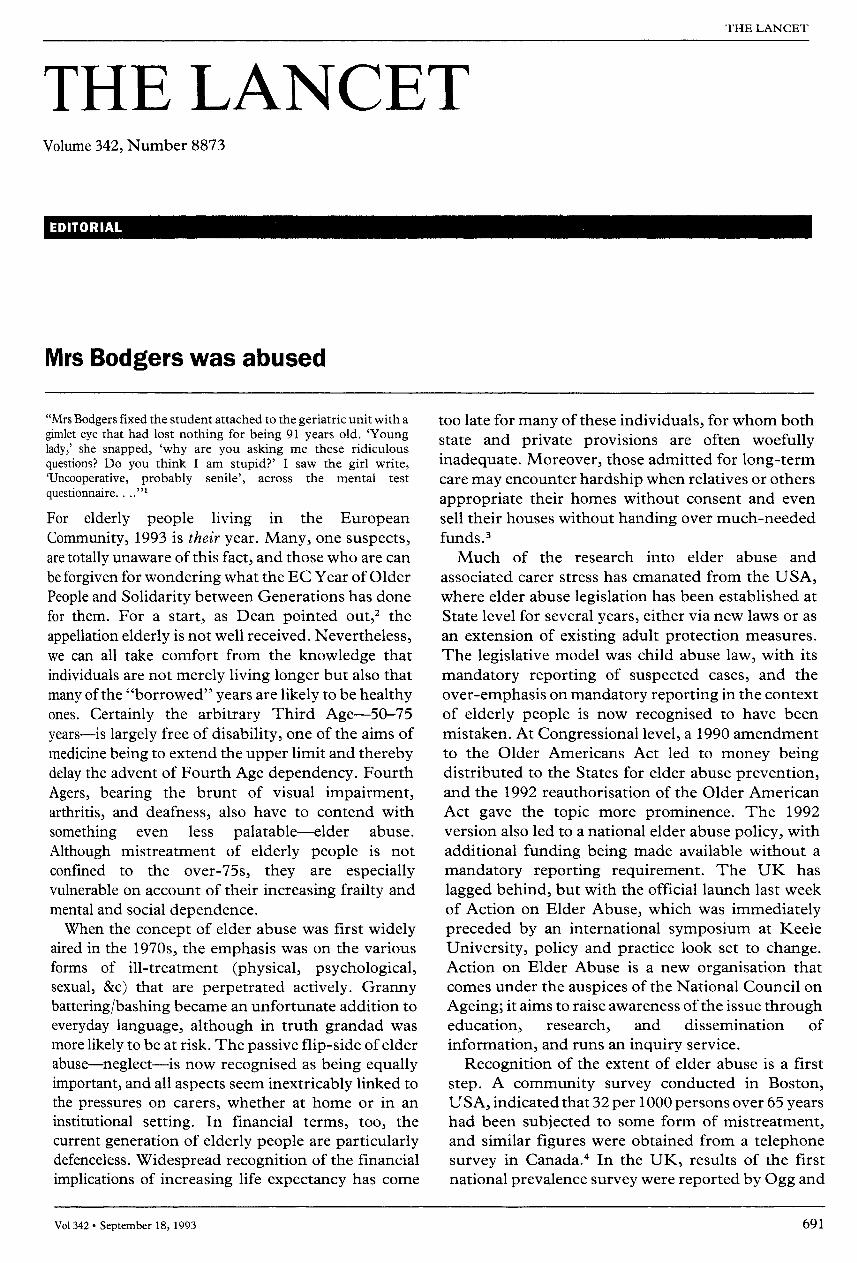
Mrs Bodgers was abused
"Mrs Bodgers fixed the student attached to the geriatric unit with agimlet eye that had lost nothing for being 91 years old. ’Younglady,’ she snapped, ’why are you asking me these ridiculousquestions? Do you think I am stupid?’ I saw the girl write,’Uncooperative, probably senile’, across the mental test
questionnaire...."1
For elderly people living in the EuropeanCommunity, 1993 is their year. Many, one suspects,are totally unaware of this fact, and those who are canbe forgiven for wondering what the EC Year of OlderPeople and Solidarity between Generations has donefor them. For a start, as Dean pointed out,2 theappellation elderly is not well received. Nevertheless,we can all take comfort from the knowledge thatindividuals are not merely living longer but also thatmany of the "borrowed" years are likely to be healthyones. Certainly the arbitrary Third Age-50-75years-is largely free of disability, one of the aims ofmedicine being to extend the upper limit and therebydelay the advent of Fourth Age dependency. FourthAgers, bearing the brunt of visual impairment,arthritis, and deafness, also have to contend withsomething even less palatable-elder abuse.
Although mistreatment of elderly people is not
confined to the over-75s, they are especiallyvulnerable on account of their increasing frailty andmental and social dependence.When the concept of elder abuse was first widely
aired in the 1970s, the emphasis was on the variousforms of ill-treatment (physical, psychological,sexual, &c) that are perpetrated actively. Grannybattering/bashing became an unfortunate addition toeveryday language, although in truth grandad wasmore likely to be at risk. The passive flip-side of elderabuse-neglect-is now recognised as being equallyimportant, and all aspects seem inextricably linked tothe pressures on carers, whether at home or in aninstitutional setting. In financial terms, too, thecurrent generation of elderly people are particularlydefenceless. Widespread recognition of the financialimplications of increasing life expectancy has come
too late for many of these individuals, for whom bothstate and private provisions are often woefullyinadequate. Moreover, those admitted for long-termcare may encounter hardship when relatives or othersappropriate their homes without consent and evensell their houses without handing over much-neededfunds.3
Much of the research into elder abuse and
associated carer stress has emanated from the USA,where elder abuse legislation has been established atState level for several years, either via new laws or as
an extension of existing adult protection measures.The legislative model was child abuse law, with itsmandatory reporting of suspected cases, and the
over-emphasis on mandatory reporting in the contextof elderly people is now recognised to have beenmistaken. At Congressional level, a 1990 amendmentto the Older Americans Act led to money beingdistributed to the States for elder abuse prevention,and the 1992 reauthorisation of the Older AmericanAct gave the topic more prominence. The 1992version also led to a national elder abuse policy, withadditional funding being made available without amandatory reporting requirement. The UK haslagged behind, but with the official launch last weekof Action on Elder Abuse, which was immediatelypreceded by an international symposium at KeeleUniversity, policy and practice look set to change.Action on Elder Abuse is a new organisation thatcomes under the auspices of the National Council onAgeing; it aims to raise awareness of the issue througheducation, research, and dissemination of
information, and runs an inquiry service.Recognition of the extent of elder abuse is a first
step. A community survey conducted in Boston,USA, indicated that 32 per 1000 persons over 65 yearshad been subjected to some form of mistreatment,and similar figures were obtained from a telephonesurvey in Canada.4 In the UK, results of the firstnational prevalence survey were reported by Ogg and

692
BennettS in 1992; these researchers worked in
conjunction with the Office of Population Censusesand Surveys omnibus survey team to investigate abuseof elderly people at home by family members or closerelatives. The questions they used were based on USand Canadian techniques, and the sample consisted ofa nationally representative assemblage of nearly 600people aged 60 or more. For the over-65s (439), 7%reported some kind of abuse (verbal, physical, orfinancial) and 1 % reported physical abuse.
In a book published last week, Bennett and
Kingston6 6 highlight the dearth of systematicEuropean research initiatives.’ 7 They further
comment on the complexity introduced by two-wayabuse-eg, when confused elderly people hit out attheir carers. So far, research on elder abuse hastended to adopt one of two methods: (a) studiesfocusing on identified cases via interviews with socialand health care workers (the child abuse model) or (b)interviews with people directly about their
experience of abuse. Many elderly people and theirfamilies find it immensely difficult to acknowledgethe existence of abuse, and researchers face the addeddifficulty that access to cases has to be via a
"gatekeeper" such as a general practitioner. Andshould the researcher discover evidence of abuse,what obligations are there to pass on this information?
Bennett and Kingston propose that future researchmight profit from looking at the characteristics ofthose abused older people and their family situationsas they are already known to social and health careservices and from focusing on older people who arevulnerable on account of disability, poverty, poorhousing, &c-ie, vulnerability-directed research.
Elder abuse begins with an attitude of mind, andthe medical profession has much to learn. The
psychiatrist who told Mrs Bodgers’ tale recognisedthe issues, describing the student’s approach as
"downright insulting" and an example of "wantoncruelty". One can only hope that the formerlyuncaring student has now become a qualifiedpractitioner with insight to match her academicachievements.
The Lancet
1 Anon. Old people. In: Binnie GAC, Sadler RL, Thomson WO, WhiteDMD, Sharp DW, eds. In England Now. London: The Lancet/Hodder & Stoughton, 1989: 104.
2 Dean M. The third age debate begins. Lancet 1993; 341: 1140-41’3 Homer A. Abuse of elderly people. BMJ 1992; 305: 1363.4 Anon. Elder abuse. Lancet 1991; 337: 1155-56.5 Ogg J, Bennett G. Elder abuse in Britain. BMJ 1992; 305: 998-99.6 Bennett G, Kingston P. Elder abuse: concepts, theories and
interventions. London: Chapman and Hall, 1993.ISBN 0-412435310X. £14.95.
7 Council of Europe. Violence against elderly people. Brussels: Councilof Europe, 1992.
COMMENTARY
Sight and insight: "visualisation" ofauditory hallucinations in schizophrenia?See page 703
Application of brain imaging techniques to schizophreniahas greatly facilitated our understanding of this enigmaticdisease. Magnetic resonance imaging (MRI) has revealed(left) temporal lobe abnormalities, particularly of thehippocampus, parahippocampal gyrus, and superiortemporal gyrus, together with other specific and non-specific subcortical and cortical abnormalities.1 How arethese structural changes related to the specific symptomsthat characterise the disorder? Positron emission
tomography (PET) and single photon emission
tomography (SPET) are functional imaging techniquesthat go some way to addressing these issues.! This week,McGuire and colleagues, using SPET, report an
association between auditory hallucinations and increasedcerebral blood flow in the left inferior frontal cortex
(Broca’s area). The finding is both striking and heuristic,because it seems to relate this cardinal symptom of thedisorder to hyperfunction in a major language centre of thebrain. How firm a basis is this observation for subsequenttheorising?
In recent PET studies, schizophrenic patients withpersistent psychotic symptoms that included hallucinationshave been reported as showing either increased perfusion inregions such as the parahippocampal gyrus, with decreasedperfusion in inferior frontal cortex related to other,
non-hallucinatory symptoms,2 or decreased cerebralmetabolic rate in the hippocampus and in the cingulate butnot the inferior frontal cortex.3 However, anatomicalcorrelates of hallucinations were not specificallyinvestigated. On studying patients who reportedexperiencing auditory hallucinations during the period offunctional imaging, Cleghorn et al4 found that the cerebralmetabolic rate determined by PET was reduced in superiortemporal gyrus/primary auditory cortex (Wernicke’s area)and increased in the right hemisphere homologue of Broca’sarea but not in Broca’s area itself. Increased perfusionshown by SPET was confined to the left superior temporalgyrus and returned to normal with amelioration of auditoryhallucinations during continuing neuroleptic therapy.sAlthough these studies seem to indicate different correlatesof auditory hallucinations in functional terms (ie, decreasedmetabolic rate vs increased perfusion), they are more
consistent anatomically in associating such hallucinationswith (left) temporal lobe dysfunction. Are there anyprocedural factors that might account for the ratherdifferent anatomical findings in McGuire’s study?McGuire and colleagues define more rigorously their
patients’ experiences of auditory hallucinations in relationto a SPET technique that provides, as they describe, a"freeze-frame" snapshot of the pattern of cerebral
perfusion during such experiences. Moreover, they re-examined each patient during a subsequent hallucination-free period as his own control. However, these importantadvantages must be set against the inability of theresearchers’ protocol, as they acknowledge, to exclude an





![[ FINAL ] - Case Report Kasus Drugs Abused](https://img.pdfslide.net/doc/110x75/5695d42d1a28ab9b02a092e0/-final-case-report-kasus-drugs-abused.jpg)