Embed Size (px)
Citation preview

Multi- and Interdisciplinary Approach to Chronic Pain Management
Steven Stanos, DO

www.ric.orgwww.ric.org
Working Together- Critical for Success

www.ric.orgwww.ric.org
Criteria for Success
Society
Individual
Workers Comp
Return to Work
MCOHealth Care Utilization
Functional, Emotional improvements
Health Care Provider
Satisfaction, Low Adverse events
Pain Relief
Gatchel and Okifuji, J Pain 2006:7(11)

www.ric.orgwww.ric.org
Chronic Pain Interrupts
• Behavior• Function• Identity• Cognition
(Harris et al., Pain: 105, 2003)

www.ric.orgwww.ric.org
The PAIN Patient
• Demoralized by continued quest for relief
• Cascade of ongoing stressors• In a state of “medical limbo”• Inactivity leads to preoccupation
with “the body in pain”• Change from active to more
passive coping with the pain

www.ric.orgwww.ric.orgPincus T. Morley S. Psychological Bulletin. 2001;127(5)
Enmeshment and Pain
Pain Illness
Self
Healthy-normal enmeshment

www.ric.orgwww.ric.orgPincus T. Morley S. Psychological Bulletin. 2001;127(5)
Enmeshment and Pain
Pain Illness
Self
Enmeshment resulting in distress

www.ric.orgwww.ric.org
Symptom Magnifiers (Matheson)
“refugee”
“game player”
“identified patient”
Matheson LN. Symptom Magnification Syndrome. Aspen Publ. 1988.

www.ric.orgwww.ric.org
Gate Control Theory
Melzack R. Neural Blockade in Clinical Anesthesia & Management of Pain, 1998.

www.ric.orgwww.ric.org
Gatchel’s 3-Stage Model
• Stage I: Normal emotional reaction during acute phase• Stage II: Behavioral and psychological reactions and problems• Stage III: Acceptance or habituation to “sick role”
Gatchel RJ, 1991

www.ric.orgwww.ric.orgCassano eta l, J of Psychosom Research, 2002
Depression: Behavioral & Physical Symptoms
Behavioral• Interpersonal friction• Anger• Avoidance• Reduced productivity• Substance use/abuse• Victimization• Social withdrawal
Physical• Fatigue• Insomnia/hypersomnia• Appetite changes• Pains and aches• Muscle tension• Gastrointestinal upset

www.ric.org
Predictors of Depression in Chronic Pain
• Pain intensity• Frequency severe pain experienced• Number of painful areas• Psychosocial factors
– low self efficacy– poor coping– poor problem solving
• Functional disability

www.ric.org
Pain Symptoms More Resistant
EmotionalDepressive Symptoms
Positive Well-being
PhysicalNon-Pain Somatic
Pain Somatic
Months1 63 9
Greco T, et al. J Gen Intern Med. 2004;19:813-18.

www.ric.orgwww.ric.org
Interference
Life Control
Pain Depression.07
.47** .27*
-.28* -.44**
Cognitive-Behavioral Mediation Model
Turk et al. Pain, 61, 1995

www.ric.org16
Psychological Aspects of Persistent Pain

www.ric.orgwww.ric.org
Anger1
1. Okifuji Turk Curran 19982. Sullivan M, 2008.
Perceived Injustice2

www.ric.orgwww.ric.org
ANGER: Agent and Action
Injury/IllnessHealth care providersLegal systemInsurance companies/Social security systemEmployerSignificant othersGodSelfThe world
Chronic painDx ambiguity, failureAdversarial disputeInadequate compensationLose job, job retrainingLack of supportIll fateDisablementAlienation

www.ric.orgwww.ric.org
ACCEPTANCE“Living with pain without reaction, disapproval, or attempts to reduce or avoid it . . .
A disengagement from struggling with pain.”
McCracken LM, Pain; 1998.
McCracken LM, J Back Musculoskel Rehab; 1999.

www.ric.org
Typical Patient Referral Characteristics
• Preoccupation with pain• Strong needs for dependency
and nurturance• Feelings of loneliness and
isolation• Self-defeating behavior patterns• Anger and hostility

www.ric.org
Facilitators Obstacles
Motivational factors Motivational factors
Adheres to program Motivated to return to work
Does not believe in program Has other plans than RTW
Capacities Capacities
Good cognitive capacities Good coping strategies Good interpersonal skills
Low cognitive capacities Coping difficulties Poor interpersonal skills
Personality-related factors Personality-related factors
Positive realistic attitude Proactive, extroverted Genuine
Pessimistic, “victim” Demanding, introverted Opposed to physical activation Lack of sincerityLoisel P, et al. J Occ Rehab 2005;15:581-
90
Worker Factors to Consider

www.ric.org
Insurer’s Actions/ Attitudes
Facilitators ObstaclesTowards Team Towards Team
Refers appropriate workers Authorizes requests Understands program Trusts the team Reacts promptly Flexible
Does not understand program Delays communications Withholds information Poor knowledge of case Impatient Doubts team’s competence
Towards Worker Towards Worker
Informs worker of rights Knowledge of case
Does not inform worker Easily influenced by worker Splitting team and worker Too much bureaucracy
Liosel P, et al. J Occ Rehab 2005;15:581-90

www.ric.orgwww.ric.orgDersh, Polatin, Leeman. J Occ Rehab 2004;14.
Secondary Gain
Internal• Gratification pre-existing unresolved dependency
& revengeful strivings• Attempt to elicit care-giving• Ability withdraw from unpleasant or unsatisfactory
life roles• Adoption of “sick role”• Convert socially unacceptable disability to a
socially acceptable one

www.ric.orgwww.ric.org
Secondary Gain
External• Financial awards
– Wage replacement– Settlement– Debt protection
• Protection from legal and other obligations
• Job manipulation• Vocational retraining and skill upgrade

www.ric.orgwww.ric.org
Tertiary gains and losses
Gains1. Gratification of altruistic
needs2. Change in role3. Decrease family tension4. Resolve marital difficulties
Losses1. Increased responsibilities2. Emotional effect3. Disturbance within the
relationship4. Guilt created by the ill
individual5. Financial hardship
Dersh, Polatin, Leeman. J Occ Rehab 2004;14.

www.ric.orgwww.ric.org
Psycho-
Neurophysiology, Physical Dysfunction,
Tissue Trauma ?
Illness Behavior, Beliefs, Coping, Emotions,
Distress
Culture, Social interactions, Sick role
Bio-
Social-
Impairments
Activity limitations,
Personal factors
Environmental, participation
Waddell, Burton, Best Practice Res Clin Rheum 2005;19(4).
Classifications of Pain

www.ric.orgwww.ric.org
Continuum of Team Models
Boon H, et al. BMC Health Services Research. 2004;4:15.
Coordinated Interdisciplinary
Collaborative Multidisciplinary Integrative
Parallel Practice
Continuum of Team Models

www.ric.org
Multidisciplinary Team Network
Psych
RN
Psychiatrist
OTPT
Family
Addiction Medicine
Vocational
Pain Physician

www.ric.org
Interdisciplinary Team Approach
Psych
RN Physician
OT
PT
RT
SW
Voc
PATIENT

www.ric.orgwww.ric.org
Pain Program Goals
• Decrease pain intensity• Increase physical activity• Improve pain medication regimen• Improve psychosocial functioning• Return to leisure pursuits and work• Reduce utilization of health care
services

www.ric.orgwww.ric.org
Commonalities of Treatment
• Re-conceptualize patients’ pain• Foster optimism and combat
demoralization• Active patient participation and
responsibility• Specific training in specific skills• Encourage feelings of success, self-
control and self-efficacy

www.ric.orgwww.ric.org
“Yellow Flags”
• Maladaptive beliefs• Expectations and pain behavior• Reinforcement of pain• Heightened emotional activity• Job dissatisfaction• Poor social support• Compensation
Cairns MC, Spine 2003; 28(9):953-59

www.ric.orgwww.ric.org
Interdisciplinary Team Approach
Loeser JD, Turk DC. Multidisciplinary pain management. In: Loeser JD, Butler SH, Chapman CR, Turk DC, eds. Bonica’s Management of Pain. Philadelphia, PA: Lippincott Williams & Wilkins; 2001:2069-2079.
John Bonica, MDBen Crue, MD

www.ric.org
RIC’S CPM Program Components
• Physical therapy• Occupational therapy• Recreation Therapy• Psychology (CBT)• Relaxation Training• Nurse Education• Vocational Therapy• Mind Body Treatment/
Feldenkrais

www.ric.org
Monday Tuesday Wednesday Thursday Friday
8aWeekend
reviewGym Gym Relax (G) Gym
9Nursing lecture
OT Tolerance Psych Biofeedback MD visit
10 PT OT tolerance MD visit Voc OT
11 MD visit Video Feldenkrais
12 Relax (G) Feldenkrais PT
1 OT (G) PT BiofeedbackTherapeuticrecreation
Psych (G)
2 Biofeedback OTTherapeutic recreation
Relax (G) Relax (G)
3 Nursing Psych
4 Pool Wii Group Pool Family meeting (G) Pool
Sample: Full Pain Program Schedule

www.ric.orgwww.ric.org
Phases of Treatment
• Educational• Skills training• Application and relapse
prevention

www.ric.orgwww.ric.org
Physical Therapy
• Comprehensive assessment
• “Active” vs “Passive”• Movement based• Strengthening• Aerobic conditioning• Home exercise plan
www.ric.org
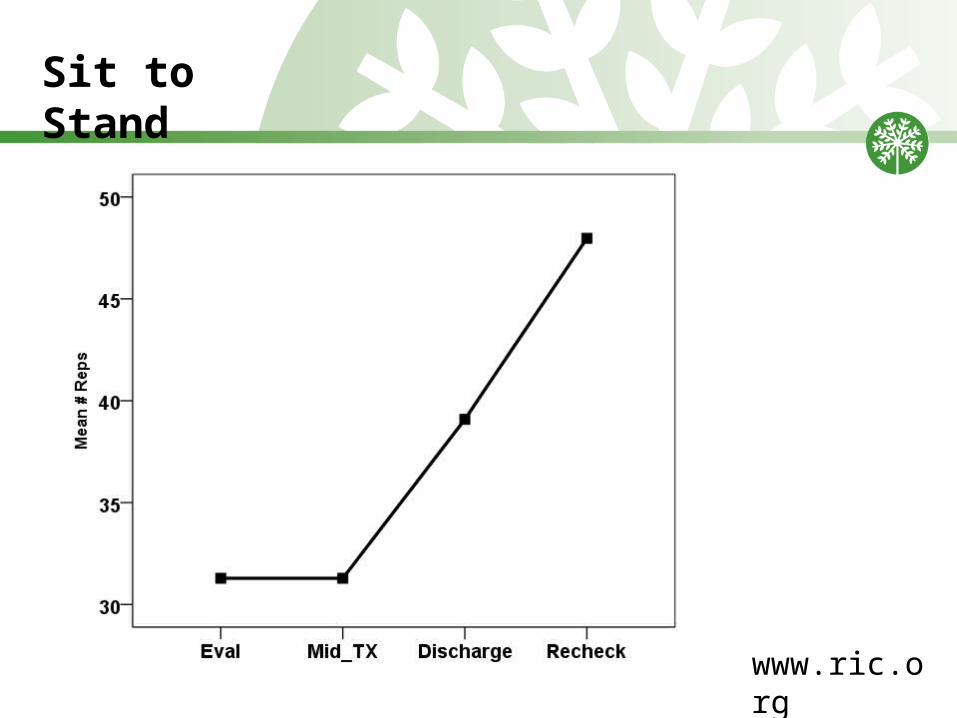
Sit to Stand
www.ric.org
Occupational Therapy
• Positioning • Pacing
Techniques/Implementation • Stress Loading Techniques • Strength/Endurance Training • Activity Tolerance
www.ric.orgwww.ric.org
Role of Pain Psychology
• WEEK I– Classes: Vicious cycles of chronic pain and Gate-control theory of pain– Individual: Acceptance of chronicity vs. continuing search for cure,
Rationale for techniques/tools to manage the pain Active self-management vs. passive medical treatment Focus on functional restoration as well as pain management
www.ric.orgwww.ric.org
Role of Pain Psychology
• WEEK II – Classes: Pain management tools (i.e. distraction, relaxation)
– Stress – Pain connection– Stress management– Identifying negative thoughts– Catastrophic pain thoughts (re-injury)– Depression thoughts (i.e.“Why bother?”)– Challenging negative thoughts
– Individual: Cognitive – behavioral intervention– Challenging negative and self-defeating thoughts– Encouraging re-activation (rather than “if it hurts, don’t do it”)– Encouraging behavioral flexibility (rather than “I’ve always done it this way”)

www.ric.orgwww.ric.org
Role of Pain Psychology
• WEEK III– Classes: Stress management– Skills Training
Communication Assertiveness Problem solving
– Individual: Cognitive – behavioral intervention Continued pain intervention Patient’s individual stressors Identifying stressful situations Developing attitudes & skills to cope more effectively

www.ric.orgwww.ric.org
Role of Pain Psychology
• WEEK IV– Classes:
Stress management tools Relapse prevention: Identifying high risk situations Developing a plan to prevent relapse
– Individual: Cognitive – behavioral intervention Anxiety management Return to work or vocational rehabilitation Identifying patient’s strengths and resources Increase confidence and self-efficacy

www.ric.org
Relaxation Training/ Biofeedback
• Deep Breathing• Imagery and Visualization• Progressive Muscle
Relaxation (PMR)• Biofeedback

www.ric.orgwww.ric.org
Vocational Rehabilitation
• Identify• Educate• Incorporate
• Return to Work• FCE• MMI• Closure

www.ric.orgwww.ric.org
The 12-C Approach
1. Communication2. Cooperation3. Cohesiveness4. Commitment5. Collaboration6. Confront problems
7. Coordination of efforts8. Conflict management9. Consensus10. Caring (patient-centered)11. Consistency12. Contribution
Heinemann GD, Zeiss. New York, 2002.

www.ric.org ©2003 Rehabilitation Institute of Chicago
47
Summary
• Multi- and Inter-disciplinary approach incorporates a biopsychosocial approach
• Depression, anxiety, anger, poor self efficacy, catastrophizing are important psychological factors that need to be identified and focused on for improved outcomes
• Pain management focuses on improving function, psychosocial well being, and making patients more active participants