Multi-centre trials in Orthopaedic Oncology: Dream or Reality?
Michelle Ghert, MD, FRCSC Associate Professor Department of Surgery
McMaster University
Slide 2
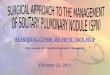
22 year-old male with sarcoma right femur
Slide 3
Slide 4
Slide 5
Slide 6
Slide 7
Slide 8
Slide 9
Slide 10
Slide 11
Slide 12
Slide 13
Slide 14
Slide 15
Slide 16
Slide 17
Deep infection in total joints Approximately 1% risk AAOS
guidelines: 24 hours of gram positive coverage with pre-operative
dosing
Slide 18
Tumour prosthesis: higher risk Patients are myelo-depleted due
to chemotherapy Surgeries are long and the wound is open for
several hours Large foreign body Large dead space Loss of
protective soft-tissue coverage
Slide 19
Slide 20
What is the magnitude of the problem?
Slide 21
Slide 22
Systematic Review Deep infection rate 9.5% (95% confidence
interval: 8.1% to 11%) Comparison to primary arthroplasty: 1%
Slide 23
Slide 24
Slide 25
Systematic Review Conclusions The risk for deep infection
following tumour prosthesis is high, X10 that of total joints
Antibiotic regimens vary from publication to publication There no
published guidelines to direct management
Slide 26
What antibiotic regimens do we use?
Slide 27
Slide 28
Duration of antibiotics Table 2: Length of Time Prophylactic
Antibiotics Prescribed Following Long-bone Reconstruction Type of
Reconstruction24 hrs48 hrs3-7 daysUntil Suction Drain Removed Tumor
prosthesis25 (35.7%)13 (18.6%)3 (4.3%)29 (41.4%) Allograft18
(26.5%)13 (19.1%)11 (16.2%)26 (38.2%) Allograft-prosthesis
composite17 (25.4%)12 (17.9%)9 (13.4%)29 (43.3%)
Slide 29
Results
Slide 30
PARITY Survey conclusions Practice patterns vary considerably
with respect to antibiotic regimen, dosages and duration Majority
of surgeons are willing to change practice Overwhelming support for
a multi-centre clinical trial
Slide 31
Hierarchy of Evidence Randomized Trials Prospective Cohort
Studies Retrospective Case Series Case Control Studies Opinion
Level 1 Level 2 Level 3 Level 4 Level 5 Less Bias More Bias
Slide 32
RCTs in Orthopaedic Oncology Orthopaedic Oncology multi-center
randomized controlled trials: Radiation Oncology: one trial, 150
patients Medical Oncology: 72, methodologically poor Surgical
Oncology: NONE There is a lot of talk about RCTs in Orthopaedic
Oncology, but no doing
Slide 33
Why do we need multi-centre trials?
Slide 34
Tibial Shaft Fractures (SPRINT)
Slide 35
Multicenter RCTs Advantages Level 1 Evidence more centers =
More Patients shorter study recruitment time increased
generalizability of results collaboration between centers,
countries and continents
Slide 36
Multicenter RCTs Disadvantages They are Hard to Do Complex
organization Very Expensive
Slide 37
But not impossible. Cardiology OASIS-6 RCT 13000 pts (JAMA,
2006) 447 hospitals 41 countries
Slide 38
But not impossible. Intensive Care Medicine PROTECT (DVT
prophylaxis) Canadian Critical Care Trials Group 4000 pts North
America/Australia
Slide 39
But not impossible Neonatal Medicine Trial of Indomethacin
Prophylaxis in Preterms (TIPP) Investigators. N=910 infants 32
centers NA, Austalia, NZ, China JAMA. 2003
Slide 40
Has it been done in Orthopaedic Surgery? SPRINT Trial (Tibial
Shaft Fractures) 1339 patients recruited, 95% F/U
Slide 41
Slide 42
Challenges in Surgical Trials
Slide 43
Can Surgeons be Blinded?
Slide 44
Who can be blinded? Patient and outcome assessors
Slide 45
Expertise Bias
Slide 46
Surgeons tend to stick to procedures that they are good at
Difficult to convince surgeons to develop new techniques Solution:
patients are allocated to provider, not procedure
Slide 47
But can it be done anyways?
Slide 48
Center for Evidence-Based Orthopaedics
Slide 49
SPRINT trial: 1339 patients, 95% follow-up FLOW trial: 2200
patients recruited, target 2200 FAITH trial: 900 patients, target
1000 TRUST trial: 600 patients, target 1000 HEALTH trial: 350
patients, target 1400 INORMUS and PRAISE prospective studies: 9000
patients All trials are funded by NIH/CIHR 150 centers around the
world
Slide 50
Slide 51
PARITY Objective: To evaluate the efficacy of short- vs.
long-term post-operative prophylactic antibiotic regimens on the
incidence of deep infection following endoprosthetic reconstruction
of lower extremity bone tumors
Slide 52
Study Design PARITY is a multi-center randomized controlled
trial using a parallel two- arm design
Slide 53
Patient screened and eligible and provides informed consent
Randomization Standard pre-op and intra-op antibiotics AND 24 hours
post op antibiotics Standard pre-op and intra-op antibiotics AND 5
days post op antibiotics Follow-up one year
Slide 54
Eligibility Criteria Lower extremity tumour prosthesis Skeletal
maturity Primary bone malignancy or benign aggressive tumor
Slide 55
Exclusion Criteria MRSA or VRE colonization Allergy to PCN or
Ancef [cefazolin] Previous local surgery (excluding biopsy)
Previous local infection Systemic infection
Slide 56
Randomization 24-hour computer randomization
(www.randomize.net) Pharmacist will randomize patient Stratified
based on center and tumor location (femur or tibia)
Slide 57
Slide 58
Slide 59
Slide 60
Blinding Patients, nurses, research staff, surgeons and central
adjudication committee (CAC) blinded Only pharmacist will be aware
of treatment allocation
Slide 61
Primary outcome and adjudication Deep infection as defined by
CDC 1992 Within one year of surgical implantation CAC: 2
Orthopaedic Surgeons and 1 Infectious Disease specialist Global
Adjudicator Platform
Slide 62
Secondary Outcomes MSTS-87 and -93 TESS Antibiotic-related
complications
Slide 63
Slide 64
Data Management
Slide 65
STEERING COMMITTEE Overall responsibility for the trial CENTRAL
ADJUDICATION COMMITTEE Review and classification of all clinical
events DATA MONITORING COMMITTEE Review of adverse events and
stopping rules based on benefit and harm METHODS AND COORDINATING
CENTRE Data management, daily conduct of the trial PARTICIPATING
CLINICAL CENTRES Patient recruitment and follow-up as per study
protocol PARITY Trial Organization Center for Evidence-Based
Orthopaedics
Slide 66
Steering Committee Dr. Michelle Ghert (McMaster University) Dr.
Ben Deheshi (McMaster University) Dr. Mohit Bhandari (McMaster
University) Dr. Tim OShea (McMaster University) Dr. Jay Wunder
(University of Toronto) Dr. Lor Randall (Huntsman Cancer Institute,
Utah) Dr. Lehana Thabane (McMaster University) Dr. Ginger Holt
(Vanderbilt University) Dr. Gordon Guyatt (McMaster
University)
Slide 67
STEERING COMMITTEE Overall responsibility for the trial CENTRAL
ADJUDICATION COMMITTEE Review and classification of all clinical
events DATA MONITORING COMMITTEE Review of adverse events and
stopping rules based on benefit and harm METHODS AND COORDINATING
CENTRE Data management, daily conduct of the trial PARTICIPATING
CLINICAL CENTRES Patient recruitment and follow-up as per study
protocol PARITY Trial Organization Center for Evidence-Based
Orthopaedics
Slide 68
Central Adjudication Committee Dr. Ben Deheshi (McMaster
University) Dr. Michelle Ghert (McMaster University) Dr. Tim OShea
(McMaster University) Dr. Lor Randall (Huntsman Cancer Institute,
Utah)
Slide 69
STEERING COMMITTEE Overall responsibility for the trial CENTRAL
ADJUDICATION COMMITTEE Review and classification of all clinical
events DATA MONITORING COMMITTEE Review of adverse events and
stopping rules based on benefit and harm METHODS AND COORDINATING
CENTRE Data management, daily conduct of the trial PARTICIPATING
CLINICAL CENTRES Patient recruitment and follow-up as per study
protocol PARITY Trial Organization Center for Evidence-Based
Orthopaedics
Slide 70
Data Safety Monitoring Board Dr. Peter Rose, Chair (Mayo
Clinic) Dr. Brian Brigman (Duke University Medical Center) Dr.
Vikram Venkateswaran (Georgetown, Ontario)
Slide 71
Power analysis Infection rate mean 9.5% Superiority of
long-term antibiotics: threshold of 5% for inferiority Alpha 5%,
Power 80% 431 patients per arm (862 total) Estimated sample size of
908 to account for 5% loss to follow-up, errors, drop-out etc
Slide 72
SPRINT trial: 1339 patients, 95% follow-up FLOW trial: 2200
patients recruited, target 2200 FAITH trial: 900 patients, target
1000 TRUST trial: 600 patients, target 1000 HEALTH trial: 350
patients, target 1400 INORMUS and PRAISE prospective studies: 9000
patients All trials are funded by NIH/CIHR 150 centers around the
world
Slide 73
Pilot: Feasibility Assess recruitment 10% of definite trial:
100 patients in 12 months Maintain follow-up (95%) and data quality
Assess ability to accurately use internet-based randomization
system Ensure compliance
Slide 74
Funding Orthopaedic Research & Education Foundation: PARITY
has been awarded an OREF/MSTS Clinical Research Grant in
Orthopaedic Oncology. PSI Foundation: PARITY has also received
funding from the Physicians Services Incorporated Foundation
Private Donation: Sarcoma Fund Canadian Cancer Society Research
Institute Innovation Grant
Slide 75
Active Sites (O7 Feb 2013) Canada *Juravinski Hospital &
Cancer Centre, Hamilton, Ontario, Canada *Mount Sinai Hospital,
Toronto, Ontario, Canada *Ottawa Hospital, Ottawa, Ontario, Canada
*McGill University Health Centre, Montreal, Quebec, Canada *Hopital
Maisonneuve Rosemont, Montreal, Quebec, Canada Franois dAssise et
LHotel-Dieu de Quebec, Quebec City, Quebec, Canada *Vancouver
General Hospital, Vancouver, British Columbia, Canada USA
*Vanderbilt Medical Centre, Nashville, Tennessee, USA Beth Israel
Deaconess Medical Centre, Boston, Massachusetts, USA Boston
Childrens Hospital, Boston, Massachusetts, USA *Huntsman Cancer
Institute, Salt Lake City, Utah, USA Memorial Sloan-Kettering
Cancer Centre, Cornell, New York, USA UK The Royal Orthopaedic
Hospital NHS Foundation Trust, Birmingham, UK The Royal National
Orthopaedic Hospital NHS Trust, Stanmore, UK The Robert Jones Agnes
Hunt Hospital NHS Foundation Trust, Oswestry, UK Oxford University
Hospital NHS Trust (Nuffield Orthopaedic Centre), Oxford UK The
Newcastle Upon Tyne Hospitals NHS Foundation Trust, Newcastle UK
Argentina Hospital Universitario Austral, Beuonos Aires, Argentina
*actively enrolling Interested sites Canada Halifax USA Albany
Medical College, Albany, New York, USA Menorah Medical Center and
Mid American Sarcoma Institute, Overland Park, Kansas, USA Marshall
University, Huntington, West Virginia University of Washington,
Washington, USA International University Hospital of Tampere,
Tampere, Finland Tel Aviv Medical Centre, Tel Aviv, Israel Nagoya
University, Chikusa-ku, Nagoya, Japan Cancer Institute Hospital
& the Japanese Foundation for Cancer Research, Toyko,
Japan
Slide 76
Launch Sept 28 th 2012 Toronto
Slide 77
Slide 78
Slide 79
PARITY International
Slide 80
To boldly go
Slide 81
Multi-centre trials in Orthopaedic Oncology: Dream or Reality?
Michelle Ghert, MD, FRCSC Associate Professor Department of Surgery
McMaster University