Embed Size (px)
Citation preview

SURGERY
Multiple Functional Neuroendocrine Tumors of Pancreasand Duodenum Managed by Robotic TotallyDuodenumpancreatectomy
A. G. Kriger1 & D. S. Gorin2& S. V. Berelavichus3 & R. S. Dugarova4 & O. V. Paklina5 & V. I. Panteleev6 & A. R. Kaldarov7
Accepted: 2 April 2020# Springer Nature Switzerland AG 2020
AbstractMultiple endocrine neoplasia (MEN) syndrome type I is a rare genetic syndrome characterized by the growth ofendocrine tumors in different organs, mostly endocrine glands. Zollinger-Ellison and organic hyperinsulinism can bea part of this syndrome but it is very rare when they can be observed together in one patient. Clinical case of MENI was described. Symptoms, presented by hypoglycemia and multiple ulcers, occurred in a 42-year-old woman. Shesuffered for 9 years, the diagnosis was multiple neuroendocrine tumors of the pancreas and duodenum, organichyperinsulinism, Zollinger-Ellison syndrome. Robotic total duodenumpancreatectomy, splenectomy, distal gastrectomywith D2 lymphadenectomy was performed. Postoperative recovery was uneventful; patient was discharged after lessthan 2 weeks. Long-term survival showed no recurrence of the disease. In reviewed literature, we found no othercases of synchronous hypoglycemic and Zol l inger-El l ison syndromes managed by tota l robot icduodenumpancreatectomy. Robotic technology can become a feasible and preferable method of treatment even insuch difficult cases.
Keywords Neuroendocrinetumor .Pancreatectomy .Duodenumpancreatectomy .Hyperinsulinism .Robotic-assisted .Robotic .
Wermer syndrome . Insulinoma . Gastrinoma
This article is part of the Topical Collection on Surgery
* A. R. [email protected]
A. G. [email protected]
D. S. [email protected]
S. V. [email protected]
R. S. [email protected]
O. V. [email protected]
V. I. [email protected]
1 Abdominal Surgery Department, A.V. Vishnevsky centre of Surgery,5 Universitetskiy prospect Street, 289, Moscow, Russian Federation119296
2 Researcher of Abdominal Surgery Department, A.V. VishnevskyCenter of Surgery, 40 Seslavinskaya Street 48, Moscow, RussianFederation 121309
3 Leading Researcher of Abdominal Surgery Department, A.V.Vishnevsky Center of Surgery, 16/1 Solov’iniy proezd street 139,Moscow, Russian Federation 117593
4 Abdominal Surgery Department, A.V. VishnevskyCenter of Surgery,40, Skobelevskaja street 70, Moscow, Russian Federation 117624
5 Research of Pathologic anatomy Department, A.V. VishnevskyCenter of Surgery, 27, B. Serpuhovskaja, Moscow, RussianFederation 117997
6 Abdominal Surgery Department, A.V. VishnevskyCenter of Surgery,3 Angelov pereylok 40, Moscow, Russian Federation 125368
7 Surgeon of Abdominal Surgery Department, A.V. VishnevskyCenterof Surgery, 9, Novoe shosse street 78, Drojjino, Moscowregion, Russian Federation 142718
SN Comprehensive Clinical Medicinehttps://doi.org/10.1007/s42399-020-00272-6

Introduction
Multiple endocrine neoplasia I (MEN I) syndrome is a rare ge-netic disease, which passes by autosomal dominant inheritance.Target organs of tumor growth when this syndrome occurs areparathyroid glands, pituitary gland, and pancreas. Rarely tumorlocation is adrenal glands, thyroid gland, duodenum, bronchi,and thymus [1]. Severity of clinical manifestation of the diseasedepends on tumors hormonal activity. Mostly MEN I patientsappear with organic hyperinsulinism associated with pancreaticinsulinoma or Zollinger-Ellison syndrome caused by pancreaticor duodenal gastrinoma. Synchronous insulin and gastrin hor-monal activity of tumor is a rare condition. In this paper, wedescribe MEN I patient with combination of severe organic hy-perinsulinism and Zollinger-Ellison syndromes.
Case Report
A42-year-old woman, suffering fromweakness, episodes of faint,migraine, convulsions, decrease of memory and concentration,was hospitalized into our department on November 22, 2016.
Disease started in 2007 with episodes of faint and difficultawaking in the morning. No medical examination on thesesymptoms was passed. At the same time, acute duodenal ulcerwas verified. The patient permanently received proton pumpinhibitors, without which duodenal ulcer recurred. In 2014, hy-poglycemia 2.8 mmol/l was detected during hospitalization foracute duodenal ulcer. On January 15, 2016, the patient underwenta lower left lobectomy for carcinoid tumor (T1N0M0). In
June 2016, the patient was hospitalized in the endocrinologydepartment with hypoglycemic coma. After diagnostic research,7-mm endocellar adenoma of pituitary gland was found byMRIof the head (without hormonal activity); adenomas of both para-thyroid glands and pancreatic head tumor were found by CTandtranscutaneal ultrasound. The patient did not suffer from primaryparathyroidism; her biochemical profile was normal. Whippletest was positive on the 6th hour of examination. Insulin andC-peptide levels were in reference range borders and composed10.23 mkE/ml (N 2.3–26.3) and 2.16 ng/ml (N 1.1–4.4), respec-tively; gastrin level was 10 times higher than normal range 1559MEd/ml (N 13–150). Her pituitary hormonal profile was withoutany deviations: adrenocorticotropic hormone, 17 pg/ml; prolac-tin, 257 mE/ml; luteinizing hormone, 1.3 mE/ml; follicle-stimulating hormone, 2.7 mE/ml; thyrotropin, 2.9 mE\l.
Preoperative Diagnostic
Permanent intravenous glucose infusions in the night timewere necessary, or patient could not awake by herself.Gastroscopy showed hypertrophy of gastric wall and ulcerousdeformation of duodenal bulbus.
Computed tomography (CT) showed hypervascular oval-shaped 19-mm mass in the head of the pancreas, which wasnearby the intrapancreatic part of the common bile duct.Similar masses, sized 9mm and 20mm, located in the ulcinateprocess and the distal part of the tail, respectively. Also, sev-eral hypervascular areas were detected in the tail of the gland.There were enlarged contrast-positive lymph nodes along pos-terior pancreaticoduodenal and splenic arteries (groups 10, 11,
Fig. 1 CT, arterial phase, axial scans. a Hypervascular tumor in the head of the pancreas 18 × 15 mm. b Heterogeneous tumor in the tail of the pancreas22 × 18 mm with hypercontrast margin (1); enlarged left adrenal gland (2)
Fig. 2 CT, arterial phase, axial scans. a Hypervascular tumors in duodenal wall. b Hypervascular metastasis in lymphatic node group 13a
SN Compr. Clin. Med.

13, and 17). CT revealed hypertrophic plications of gastricwall with increased vascularization (consequential sign ofZollinger-Ellison syndrome). In the anterior and posterior wallof the duodenal bulb, submucosal small hypervascular 5.5-mm and 10-mm tumors were presented. Similar masses werein the wall of the descending duodenum of 3 mm, 5 mm,5.5 mm, and 8 mm (located above the level of the papilla).
Arterial calcium stimulation with hepatic venous samplingwas performed on November 16, 2016, and confirmed highdegree insulin and C-peptide ejection after stimulation ofcommon hepatic artery (Figs. 1 and 2).
After studying of anamnesis, clinical presentation, laborato-ry, and instrumental methods, diagnosis was verified: clinicalMEN I syndrome, multiple neuroendocrine tumors of pancreas,organic hyperinsulinism, multiple neuroendocrine tumors ofduodenum, Zollinger-Ellison syndrome, lymphatic nodes me-tastasis, adenomas of right bottom and left top parathyroidglands, endocellar adenoma of pituitary gland, adenoma ofright adrenal gland, and carcinoid of left lung (left lobectomyJanuary 15, 2016). In this case, total duodenumpancreatectomy,spleenectomy, and distal gastric resection with lymphadenecto-my D2 were indicated. Patient received gastroprotective thera-py before and after surgery.
Intraoperative Data
Robotic procedure was performed on November 23, 2016. Ondiagnostic laparoscopy, no peritoneal metastases were detected.After cholecystectomy, common bile duct and common hepaticduct were mobilized, as so right and left propria and commonhepatic arteries, portal vein; lymphadenectomy of hepatoduodenalligament was done (group 12). Gastroduodenal artery and com-mon hepatic duct were clipped and transected. Diameter of com-mon hepatic duct was 3 mm. Tunnel under the pancreatic neckwas created. Stomach mobilization was made along the greatercurvature including gastric fundus and upper polar of the spleen.Parietal peritoneumwas transected along upper margin of pancre-as, splenic artery was mobilized and preventively clipped on theproximal 1/3 level. Transection of parietal peritoneum along lowermargin of pancreaswas performed and tunnelizationwas finished.Antrum and duodenum were mobilized; group 3 and 4 lymphaticnodes were deviated to the side of deleting specimen. Then thestomach was transected on the level of its angle by Endo GIAstapler. Superior mesenteric vein was circularly separated fromadipose tissue; Henle trunk was clipped and transected. Superiormesenteric artery was mobilized, mesopancreas was transected onthe right side of the artery, and lymphatic nodes of group 14 wereremoved, lower pancreaticoduodenal artery was clipped andtransected. Kocher maneuver was performed, Herot’s fascia wasremoved, and vena cava inferior and left renal vein were exposed.Jejunum was transferred to the right side through the hole undersuperior mesenteric vessels and was crossed at the level of itsvascular arcade by Endo GIA stapler. Pancreas was tractionedupper and forward, celiac trunk was mobilized, group 8 and 9lymphatic nodes were removed, and splenic artery was clippedtwice and transected. Body and tail of pancreas were mobilized incomplex with peripancreatic tissue, group 10 and 11 lymphaticnodes, and spleen and Herot’s fascia. Specimen was transferred tothe right side of abdominal cavity. Intracorporalhepaticoenteroanastomosis and gastroenteroanastomosis wereformed. Specimen was removed from the abdominal cavitythrough the minilaparotomy (4 cm) at the place of robotic portin hypogastrium. Two drainages were placed in the abdominal
Fig. 3 Specimen: distal part of the stomach, jejunum, pancreas, andspleen
Fig. 4 CT, arterial phase, frontal scans. a Hypertrophic gastric wall before procedure. b Normal gastric wall 9 days after procedure
SN Compr. Clin. Med.
cavity. Operation timewas 420min, estimated blood loss, 300ml.Glucose rate was 5.8 mmol/l at the end of procedure (Fig. 3).
Postoperative Recovery
For the period of 2 days after surgery, the patient was in ICunit. Glucose monitoring and correction were carried out.Dietary intake and insulin doses were established consideringspecific insulin insufficiency. There were no complicationsafter surgery. Abdominal drainages were removed on postop-erative days 1 and 3. Control CT was done on postoperativeday 10: there were no metastatic lymph nodes or lesions left;pathologic hypertrophy of gastric wall disappeared (Fig. 4).
Patient was discharged from our department on postopera-tive day 13. Medical observation of endocrinologist, oncolo-gist, and nutritionist was recommended. Postoperative geneticanalysis revealed heterozygous mutation in Menin gene andproved MEN I syndrome.
After discharging from the hospital, a specificantineureoendocrine tumor biotherapy was admitted to the pa-tient. In 9 months postoperative follow-up period, there were notumor, hypoglycemia, or Zollinger- Ellison syndrome signs(Table 1).
Pathological examination showed 5 tumors in duode-num and 7 tumors in pancreas. Histologically, tumors of
duodenum showed a trabecular growth pattern,hyalinized stroma, low atypical in absence of necrosis.Psammoma bodies were absent. Tumor’s growth waslimited by lamina submucosa without infiltration of lam-ina muscularis propria. All 5 duodenal tumors andlymph node metastases expressed synaptophysin,chromogranin A, and gastrin. Angioinvasion was notobserved. Highest Ki-67 proliferation rate was 7.9% inthe gastrinoma of duodenal bulbus 10 mm in diameterand 2.9% in the gastrinoma of descending part of duo-denum. A total of 33 lymph nodes were examined, 9 ofthem were positive. Ultrastructurally, cells of tumor andlymph node metastases contained “typical” G-cellgranules.
Duodenal tumors were categorized as gastrinomas, diffuse typeof growth (5 small tumors), grade 2, pT1, pN1 (LNR 0,3), cM0.
All pancreatic tumors showed trabecular-gyriform and sol-id patterns. Angioinvasion was not observed, no mitoses per10 HPF, Ki-67 rate was less than 2%.
Size of pancreatic tumors was bigger than duodenal but alltumors were G1 according WHO 2010. Pancreatic head tumorexpressed insulin; two others did not express insulin or gastrin. Inthe head of the pancreas, we observed 5 small tumors 1–2 mm,which expressed synaptophysin and chromogranin A. One ofthem expressed insulin; others did not expressed any hormones.
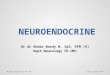
Table 1 Specimen examination. CT, microscopic, histochemical, and ultrastructural findings
CT Localization Gross Grade, WHO Ki-67%
Insulin Gastrin EM, granules
Pancreas 19 mm hypervascular Head 18 mm G1 < 1 + – Proinsulin/insulin
9 mm hypervascular Pr. Uncinatus 8 mm G1 < 1 + – –
20 mm hypervascular Tail 17 mm G1 < 2 – – Mixed proinsulin/gastrin
Duodenum 5.5 mm hypervascular Bulbus 6 mm G1 < 1 – + Gastrin
10 mm hypervascular Bulbus 6 mm G2 7.9 – + Gastrin
5 mm hypervascular Descending part 4 mm G1 < 1 – + Gastrin
5.5 mm hypervascular Descending part 6 mm G2 2.9 – + Gastrin
8 mm hypervascular Descending part 6 mm G1 < 1 – + Gastrin
Lymph node (metastases) 7 mm 13b group No data – – – + Gastrin
13.5 mm 13 No data – – + Gastrin
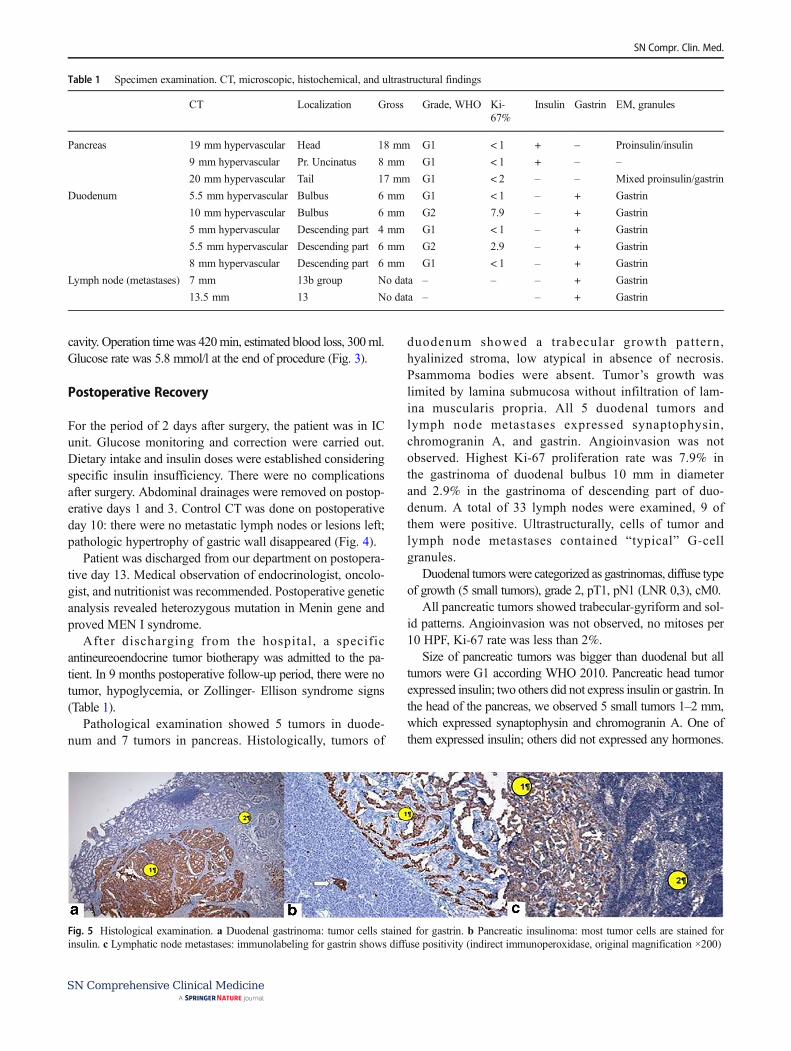
Fig. 5 Histological examination. a Duodenal gastrinoma: tumor cells stained for gastrin. b Pancreatic insulinoma: most tumor cells are stained forinsulin. c Lymphatic node metastases: immunolabeling for gastrin shows diffuse positivity (indirect immunoperoxidase, original magnification ×200)
SN Compr. Clin. Med.

Pancreatic tumors were categorized as insulinoma of pancre-atic head, 19 mm, grade 1, pT1, pN0, cM0, and non-functionalNETs of pancreatic tail and processus uncinatus, 20 mm and8 mm, WHO grade 1, pT1, pN0, and cM0 both (Figs. 5 and 6).
Discussion
MEN I syndrome was described by Paul Wermer in 1954 [2].Insulinomas are found in 23–29% of MEN I patients,gastrinomas in 40% [3]. Synchronous presentation of hypo-glycemic and Zollinger-Ellison syndromes is extremely rare.There are 8 cases of MEN I with such a course that we havefound in the literature.
The first case of insulin- and gastrin-producing tumor com-bination was described by Saburo Murakami in 1995 [4]. Itwas a 55-year-old patient with pituitary adenoma, hyperpara-thyroidism, pancreatic head gastrinoma and insulinoma andmultiple duodenal ulcers. At first step of treatment, parathy-roid glands resection was done. One month later, total gastrec-tomy for gastric ulcer was performed. There were no attemptsfor removing gastrin-producing tumor, neither pancreatic headinsulinoma. Postoperative hypoglycemia was managed bypermanent intravenous glucose infusion. Patient died 3monthsafter surgery.
Furthermore, 2 patients with MEN I, who had 3 and4 months interval between hypoglycemia and duodenalulcers, were described [5, 6]. It is also known the ob-servation of a 67-year-old patient with nonresectablepancreatic adenocarcinoma associated with insulinomasof body and tai l of pancreas and unlocal izedgastrinoma. Patient survived 7 years after diagnosis.Morphological and immunohistochemical investigationconfirmed the presence of adenocarcinoma, insulinoma,and gastrinoma [7]. The only clinical case of surgicaltreatment was an 18-year-old woman with hypoglycemicand Zollinger-Ellison syndromes. Pancreatic head tumor,producing simultaneously gastrin and insulin, was re-moved [8].
The patient, described in our observation, according tothe anamnesis and disease symptoms, has had clinically
active MEN I syndrome during 9 years before the diag-nosis was verified. She had severe hypoglycemia whileserum insulin level was within normal range and duode-nal ulcers while serum gastrin was 10 times higher thannormal range. These symptoms were absolute indicationsfor surgery, so we did not consider medical treatment.The presence of multiple hormone-producing tumorsand metastatic regional lymphatic nodes excluded thepossibility of organ-preserving surgery. Radical roboticsurgical t reatment of mult iple insul inomas andgastrinomas has not been described yet. Multiple charac-ters of tumors in endocrine glands and presence of met-astatic lymphatic nodes determine not so optimistic prog-nosis of disease.
Conclusion
We present the rare case of combination of two hormonalsyndromes caused by multiple neuroendocrine tumors of thehepatobiliary zone. Moreover, the surgery was performed byrobotic complex only: total pancreatectomy, splenectomy, andlymphadenectomy were performed. The treatment showedgood long-term survival result.
Authors’ Contributions AGK and DSG designed the surgical conceptand performed the surgery. SVB, ARK, RSD, and VIP carried out theacquisition of data and drafted the manuscript. OVP is responsible for themorphological part. AGK, DSG, SVB, ARK, and VIP revised the article.All authors read and approved the final manuscript.
Data Availability The data are not available for public access because ofpatient privacy concerns, but are available from the corresponding authoron reasonable request.
Compliance with Ethical Standards
Ethics Approval and Consent to Participate The present study was con-ducted in accordance with the ethical standards of our institution.
Consent for Publication Written informed consent was obtained fromthe patient for publication of this case report and any accompanyingimages.
Fig. 6 Histotologicalexamination. a Duodenalgastrinoma: typical vesicular G-cell granules. b Pancreaticinsulinoma: round haloed gran-ules of low density (×14000)
SN Compr. Clin. Med.

Competing Interests The authors declare that they have no competinginterests.
Abbreviations CT, computed tomography; IC unit, intensive care unit;HPF, high presentative field;MEN I,multiple endocrine neoplasia type I;NET, neuroendocrine tumor; WHO, World Health Organization
References
1. Mason TH, Keigher HA. Intramedullary spinal neurilemmoma: casereport. J Neurosurg. 1968;29(4):414–6. https://doi.org/10.3171/jns.1968.29.4.0414.
2. Yoshino T, Yoneda K. Laparoscopic resection of a retroperitonealancient schwannoma: a case report and review of the literature.Anticancer Res. 2008;28(5B):2889–91.
3. Propp JM, McCarthy BJ, Davis FG, Preston-Martin S. Descriptiveepidemiology of vestibular schwannomas. Neuro-Oncology.2006;8(1):1–11. https://doi.org/10.1215/S1522851704001097.
4. Jayaraj SM, Levine T, Frosh AC, Almeyda JS. Ancient schwannomamasquerading as parotid pleomorphic adenoma. J Laryngol Otol.1997;111(11):1088–90.
5. Conti P, Pansini G, Mouchaty H, Capuano C, Conti R. Spinalneurinomas: retrospective analysis and long-term outcome of 179consecutively operated cases and review of the literature. SurgNeurol. 2004;61(1):34–44. https://doi.org/10.1016/S0090-3019(03)00537-8.
6. Li Q, Gao C, Juzi JT, Hao X. Analysis of 82 cases of retroperitonealschwannoma. ANZ J Surg. 2007;77(4):237–40. https://doi.org/10.1111/j.1445-2197.2007.04025.x.
7. Chan PT, Tripathi S, Low SE, Robinson LQ. Case report–ancientschwannoma of the scrotum. BMC Urol. 2007;7:1. https://doi.org/10.1186/1471-2490-7-1.
8. Jindal T, Mukherjee S, Kamal MR, Sharma RK, Ghosh N, Mandal SN,et al. Cystic schwannoma of the pelvis. Ann R Coll Surg Engl.2013;95(1):1–2. https://doi.org/10.1308/003588413X13511609956697.
Publisher’s Note Springer Nature remains neutral with regard to jurisdic-tional claims in published maps and institutional affiliations.
SN Compr. Clin. Med.