-
504 | july 2013 | volume 43 | number 7 |
journal of orthopaedic & sports physical therapy
[ research report ]
Visual observation of lower extremity movement patterns during
various tasks is a common way to assess dynamic function and
alignment in the clinical setting.7,19 Functional movements, such
as the lunge, step-up, step-down, single-
leg press, bilateral squat, and balance and reach, are
frequently used to assess movement quality of the lower
extremi-ties.2,5,19,20,22 Authors of previous studies have reported
moderate to good interrater reliability for visual assessment of
move-
ment quality during a single-limb mini-squat in healthy
individuals (κ = 0.92)1 and a lateral step-down in healthy
sub-jects (κ = 0.59)25 and in those with patel-lofemoral pain
syndrome (κ = 0.67).25 Thus, the interrater reliability of
these
observational lower extremity movement-pattern tests should be
adequate to sup-port their use in clinical practice.
The forward step-down (FSD) is a functional task requiring stair
descent, which involves weight-bearing stress at various knee
flexion angles as well as dynamic muscular control. Poor me-chanics
during an FSD task could place abnormal stresses on the knee at
both the tibiofemoral and patellofemoral joints.18 Accordingly, the
FSD task could be per-formed either as a screening tool18 or as an
exercise for knee rehabilitation.8,31,32 Loudon et al18 used the
FSD task as a screening tool to determine level of func-tion and
reported moderate to high in-trarater reliability (intraclass
correlation coefficient model 3,1 = 0.94) in individu-als with
patellofemoral pain syndrome. However, no studies have investigated
the interrater reliability of the FSD task in healthy individuals,
which is needed to determine how suitable the test is for clinical
practice and screening for risk of injuries.
An exaggerated dynamic knee valgus during weight-bearing tasks
can result from many factors, including a lack of muscular strength
and flexibility.23,24 Dur-ing weight-bearing tasks requiring knee
flexion, the hip abductors and external rotators act eccentrically
both to stabi-
TT STUDY DESIGN: Cross-sectional.TT OBJECTIVE: To investigate
the interrater reli-
ability of movement-quality ratings for the forward step-down
(FSD) test and to compare hip muscle strength and lower extremity
joint range of mo-tion and muscle flexibility among asymptomatic
women with different levels of movement quality.
TT BACKGROUND: The interrater reliability of the FSD test has
not yet been investigated. Ad-ditionally, it is not known whether
differences in musculoskeletal measures exist among individuals
with different levels of movement quality during the FSD test.
TT METHODS: Two physical therapists assessed movement quality
during the FSD test in 26 a symptomatic women (mean SD age, 22.7
0.9 years). Hip muscle strength and lower extrem-ity joint range of
motion and muscle flexibility were also assessed. The interrater
reliability of the FSD test was estimated by using the kappa
coefficient and percent agreement. Differences in musculo-skeletal
measures based on movement quality
were assessed by independent t tests.
TT RESULTS: The kappa coefficient and percent agreement for
rating the quality of movement on the FSD test were 0.80 (95%
confidence interval: 0.57, 1.00) and 85%, respectively. The
subjects with moderate movement quality had significantly less
strength of the hip abductors, less knee flexion range of motion
measured in prone (quadriceps flexibility), and less hip adduction
range of motion measured in sidelying (iliotibial band/tensor
fascia latae flexibility) compared to those with good movement
quality.
TT CONCLUSION: There was good agreement for the rating of
movement quality during the FSD test, and there were physical
attributes that distinguished those with moderate from those with
good quality of movement. J Orthop Sports Phys Ther
2013;43(7):504-510. Epub 11 June 2013.
doi:10.2519/jospt.2013.4073
TT KEY WORDS: abductors, hip, knee, reliability, strength
1Applied Kinesiology and Ergonomic Technology Laboratory,
Department of Physical Therapy, The Graduate School, Yonsei
University, Wonju, Gangwon-do, South Korea. 2Department of Physical
Therapy, The Graduate School, Yonsei University, Wonju, Gangwon-do,
South Korea. The protocol for this study was approved by the Yonsei
University Wonju Campus Human Studies Committee. The authors
certify that they have no affiliations with or financial
involvement in any organization or entity with a direct financial
interest in the subject matter or materials discussed in the
article. Address correspondence to Dr Heon-Seock Cynn, Department
of Physical Therapy, Yonsei University, 1 Yonseidae-gil, Wonju-si,
Gangwon-do, South Korea. E-mail: [email protected] T Copyright
©2013 Journal of Orthopaedic & Sports Physical Therapy®
KYUNG-MI PARK, PT, MS1 • HEON-SEOCK CYNN, PT, PhD1 • SUNG-DAE
CHOUNG, PT, BSc2
Musculoskeletal Predictors of Movement Quality for the Forward
Step-down Test
in Asymptomatic Women
43-07 Park.indd 504 6/19/2013 1:09:02 PM
Jour
nal o
f O
rtho
paed
ic &
Spo
rts
Phys
ical
The
rapy
®
Dow
nloa
ded
from
ww
w.jo
spt.o
rg a
t on
Oct
ober
5, 2
013.
For
per
sona
l use
onl
y. N
o ot
her
uses
with
out p
erm
issi
on.
Cop
yrig
ht ©
201
3 Jo
urna
l of
Ort
hopa
edic
& S
port
s Ph
ysic
al T
hera
py®
. All
righ
ts r
eser
ved.
mailto:[email protected]
-
journal of orthopaedic & sports physical therapy | volume 43
| number 7 | july 2013 | 505
lize the pelvis in the frontal plane and to control motion of
the femur in the fron-tal and transverse planes.16,24 Weakness of
these muscles can lead to excessive hip adduction and hip internal
rotation during weight-bearing activities12 and, consequently, to
excessive knee valgus alignment.13,24
Other potential factors can also lead to poor lower extremity
function during weight-bearing tasks. Limited quadriceps
flexibility may limit knee flexion and re-sult in greater
ipsilateral hip adduction, whereas limited iliotibial band/tensor
fascia latae (ITB/TFL) flexibility may lead to ipsilateral pelvic
rotation in the transverse plane, along with hip internal
rotation15,21 and tibial external rotation, inducing knee valgus
alignment.17 De-creased hamstring and gastrocnemius muscle
flexibility may contribute to ab-duction and external rotation of
the tib-ia, also facilitating dynamic knee valgus
alignment.3,17
The aims of this study were (1) to investigate the interrater
reliability of the movement-quality ratings for the FSD test and
(2) to compare hip muscle strength and lower extremity joint range
of motion and muscle flexibility among asymptomatic women with
different levels of movement quality on the FSD test. We
hypothesized that (1) interrater reliability of the
movement-quality rat-ings for the FSD would be high and (2) women
with lower levels of movement quality would have less hip abductor
and external rotator muscle strength, greater hip internal rotation
range of motion, and decreased flexibility of the ITB/TFL. Women
were selected for the study based on a higher incidence of
patellofemoral joint pain in this population.4
METHODS
Subjects
Twenty-six asymptomatic female subjects were recruited from the
Department of Physical Therapy at
Yonsei University. All subjects had not participated in regular
strength training
or in a stretching program for at least 3 months prior to the
study. The average SD age, height, and body mass of the subjects
were 22.7 0.9 years, 161.5 4.2 cm, and 54.0 3.9 kg, respectively.
Subjects were included if they were pain free and had no
musculoskeletal or neu-rological injuries in the lower extremities
or lumbar spine within the 6 months pri-or to the study. Subjects
were excluded if they had undergone surgery for the lower
extremities or lumbar spine during the 6 months preceding the
study, had any balance impairments secondary to a ves-tibular or
neurological disorder, or used medications that could cause
dizziness or loss of balance. All subjects read and signed an
informed-consent form prior to participation. The protocol for the
study was approved by the Yonsei Uni-versity Wonju Campus Human
Studies Committee.
The number of subjects in the study was determined by
calculating the ef-fect size, based on previously published data25
on the difference in ankle dorsiflex-ion range of motion measured
with knee extension between subjects with different levels of
movement quality during the lat-eral step-down test. With an effect
size of 1.26, power analysis indicated that a total sample size of
18 participants was required to achieve a significance level of .05
and a power of 0.8.
ProceduresTwo examiners participated in data col-lection. One
examiner had 2 years of clinical experience in the field of applied
kinesiology and musculoskeletal physi-cal therapy. The other
examiner had more than 6 years of clinical experience in
musculoskeletal physical therapy. Be-fore data collection, the 2
examiners had a 5-hour training session on the methods to be used
in the study. For reliability ex-amination of the FSD test, the
examin-ers discussed the operational definition and practiced
scoring and classifying subjects in 3 categories (good, moderate,
and poor), based on movement quality. For musculoskeletal
measurements (hip
muscle strength and lower extremity joint range of motion and
muscle flexibility), the 2 examiners determined the testing
position and methods to detect end range of movement, and
standardized all pro-cedures. Following this training session,
pilot testing was performed on 5 healthy volunteers and final
modifications of the testing procedures were made.
The 2 examiners assessed the move-ment quality of the FSD test
simulta-neously on each subject to establish interrater
reliability. Following the FSD test, each examiner completed the
musculoskeletal measurements of the subjects. The average value of
the 2 exam-iners was used for statistical analysis. The
data-collection session lasted approxi-mately 40 minutes for each
subject. The order of musculoskeletal measurements was randomly
determined by drawing a sealed envelope from a box, to account for
any potential effects of measurement order. All testing was
performed on the dominant limb of each subject, defined as the limb
used to kick a ball.10
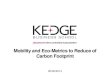
FSD TestThe FSD test used in this study was a modification of
the test used by Piva et al22 (FIGURE). Prior to performing the
test, the tibial tuberosity of the tested limb and the vertical
front edge of the step, just under the second toe of the tested
limb, were marked with a 1-cm red sticker to facilitate
visualization. Next, the height of the step was adjusted so that
each partici-pant achieved 60° of knee flexion during the test. If
the heel of the nontested limb did not contact the floor when the
knee of the tested limb was bent to 60°, wood blocks were placed on
the step to ensure that the knee of the tested limb reached 60° of
flexion when the heel of the non-tested limb touched the floor.
For testing, the subject stood on a 20-cm step, with the foot of
the tested limb close to the edge of the step and the nontested
limb positioned in front of the step, with the knee straight and
the ankle at maximum dorsiflexion. Subjects were asked to keep
their trunk straight, hands
43-07 Park.indd 505 6/19/2013 1:09:04 PM
Jour
nal o
f O
rtho
paed
ic &
Spo
rts
Phys
ical
The
rapy
®
Dow
nloa
ded
from
ww
w.jo
spt.o
rg a
t on
Oct
ober
5, 2
013.
For
per
sona
l use
onl
y. N
o ot
her
uses
with
out p
erm
issi
on.
Cop
yrig
ht ©
201
3 Jo
urna
l of
Ort
hopa
edic
& S
port
s Ph
ysic
al T
hera
py®
. All
righ
ts r
eser
ved.
-
506 | july 2013 | volume 43 | number 7 |
journal of orthopaedic & sports physical therapy
[ research report ]
on their waist, and to bend the knee on the tested side until
the heel of the non-tested limb touched the floor. The sub-jects
were asked not to apply any weight on the heel of the nontested
limb once it reached the floor and to immediately re-extend the
knee of the tested limb to re-turn to the starting position. The
subjects performed 5 consecutive FSD movements after 3 minutes of
familiarization. After the 5 consecutive trials were completed,
each examiner rated the performance of the subject across all 5
repetitions of the FSD. Standing 3 m directly in front of and
facing the subject, both examiners scored the test simultaneously,
based on the following 5 criteria:1. Arm strategy: if the subject
used an
arm strategy to recover balance, 1 point was given. Because
subjects were instructed to keep their hands on their waist,
removing their hands from their waist was interpreted as a strategy
to recover balance.
2. Trunk movement: if the subject leaned the trunk to either
side, interpreted as recovering balance, 1 point was given.
3. Pelvic plane: if 1 side of the pelvis was rotated in the
transverse plane or el-
evated in the frontal plane compared with the other side, 1
point was given.
4. Knee position: if the knee of the tested limb moved medially
in the frontal plane and the tibial tuberosity crossed an imaginary
vertical line positioned directly over the second toe of the tested
foot, 1 point was given. If the knee moved medially and the tibial
tu-berosity crossed an imaginary vertical line positioned directly
over the me-dial border of the tested foot, 2 points were
given.
5. Maintenance of a steady unilateral stance: if the subject had
to support body weight on the nontested limb, or the foot of the
tested limb moved dur-ing testing, 1 point was given.A total score
of 0 or 1 was classified as
good movement quality, a total score of 2 or 3 was classified as
moderate movement quality, and a total score of 4 or more was
classified as poor movement quality. Each examiner rated the
performance of the test individually for each subject. No
dis-cussion was allowed between the examin-ers during the
performance and scoring of the test. The raters’ scores of the FSD
test were used for the calculation of inter-
rater reliability.Immediately after testing, the 2 exam-
iners compared their ratings to determine if they agreed on the
good, moderate, or poor classification. Consensus was re-quired to
assign each subject to a single category for the analysis comparing
musculoskeletal measurements between groups of different movement
quality. If consensus was not present between the 2 raters, the
subjects were asked to repeat 5 additional FSD movements to
finalize the classification. Only 4 of 26 subjects were rated
differently between the 2 examiners and needed to repeat the
test.
Strength TestingStrength testing of the hip abductors and
external rotators was performed with a handheld dynamometer
(Lafay-ette Manual Muscle Testing System; La-fayette Instrument
Company, Lafayette, IN), as described by Piva et al,22 who
re-ported intraclass correlation coefficients of 0.85 and 0.79,
respectively, for inter-rater reliability. Muscle strength was
re-corded in kilograms and normalized by dividing the raw score by
the participant’s body mass. Each trial was performed for 3
seconds, with 1 minute of rest between trials. Each subject was
allowed 2 repeti-tions for practice, and the results of the 3
subsequent repetitions were averaged and recorded.Hip Abduction
Strength Hip abduction muscle strength was measured in the
sidelying position, with the subject ly-ing on the nontested side.
The subject’s tested hip was in approximately 30° of abduction and
5° of extension, and the iliac crest of the tested side was
manu-ally stabilized by the examiner. The sub-ject performed
isometric hip abduction against the resistance of the handheld
dynamometer, which was placed just proximal to the lateral
malleolus.Hip External Rotation Strength Hip external rotation
muscle strength was tested with the subject prone on the table, the
tested knee flexed to 90°, and the hip in neutral. The nontested
limb was positioned with the hip in the neu-
FIGURE. (A) Start and (B) end positions for the forward
step-down test.
43-07 Park.indd 506 6/19/2013 1:09:05 PM
Jour
nal o
f O
rtho
paed
ic &
Spo
rts
Phys
ical
The
rapy
®
Dow
nloa
ded
from
ww
w.jo
spt.o
rg a
t on
Oct
ober
5, 2
013.
For
per
sona
l use
onl
y. N
o ot
her
uses
with
out p
erm
issi
on.
Cop
yrig
ht ©
201
3 Jo
urna
l of
Ort
hopa
edic
& S
port
s Ph
ysic
al T
hera
py®
. All
righ
ts r
eser
ved.
-
journal of orthopaedic & sports physical therapy | volume 43
| number 7 | july 2013 | 507
tral position and full knee extension. The examiner manually
fixed the subject’s pelvis with 1 hand. The subject exerted an
isometric action of the hip external rotators against the
resistance of the handheld dynamometer, positioned just proximal to
the medial malleolus of the tested limb.
Range-of-Motion TestingHip external and internal rotation,
ad-duction, flexion, as well as knee flexion range of motion were
measured with a fluid-filled inclinometer (MIE Medi-cal Research
Ltd, Leeds, UK).29 Ankle dorsiflexion range of motion was mea-sured
with a universal goniometer in 1° increments. Intraclass
correlation coef-ficients for interrater reliability of these
range-of-motion measurements have been reported to be higher than
0.82.22,26 For this study, 1 examiner performed the measurements
while the other examiner read and recorded the values. The
incli-nometer was first zeroed on a fixed verti-cal reference prior
to the measurements. Two practice repetitions were performed to
ensure that the subject was relaxed and comfortable. Data are the
average of 3 measurements, taken with 5 seconds between trials.Hip
External Rotation Hip external ro-tation was measured with the
subject in a prone position. The knee of the tested limb was flexed
to 90°, and the nontested hip was abducted about 30°, so that the
hip motion on the tested side would not be obstructed. The starting
position for measuring hip rotation was determined by positioning
the tested tibia perpen-dicular to the support surface. The
in-clinometer was positioned on the distal third of the fibula. The
examiner manu-ally fixed the subject’s pelvis at neutral with 1
hand, then moved the tested limb through passive hip external
rotation. End range of motion was defined as the point at which the
lower shank could no longer be moved without pelvic rotation.Hip
Internal Rotation Hip internal ro-tation was determined in the same
way as the measurement of hip external rota-
tion, except that the tested hip was inter-nally rotated.Knee
Flexion in Prone (Quadriceps Flex-ibility) The examiner manually
fixed the subject’s pelvis in neutral with 1 hand to avoid anterior
tilting of the pelvis or extension of the lumbar spine. The
incli-nometer was placed over the distal half of the anterior
border of the tibia. The knee on the tested side was then
pas-sively flexed to end range of motion. The measurement was taken
when the lum-bar spine or pelvis first began to move or when the
end range of motion was achieved. The opposite limb remained flat
on the table.Hip Adduction in the Sidelying Posi-tion (ITB/TFL
Flexibility) Hip adduc-tion was examined using the Ober test.16 The
subject was positioned lying on the side, with the tested limb in
the superior position and the knee flexed at 90°. The nontested
limb was slightly flexed at the hip and knee to maintain stability
on the table. The examiner manually fixed the subject’s pelvis in
neutral with 1 hand and grasped just below the knee of the tested
side with the other hand. The inclinom-eter was placed over the
distal portion of the tested thigh. The examiner moved the tested
thigh first in flexion, then through abduction combined with
extension, un-til the hip was positioned in midrange hip abduction
with neutral flexion/extension. From this position, the thigh was
allowed to drop toward the table until the thigh stopped, at which
point the inclinometer value was recorded.Hip Flexion in the Supine
Position (Ham-string Flexibility) The subject was placed in the
supine position with the knee of the tested limb in full extension.
The nontested limb remained flat on the table to avoid posterior
pelvic tilt. The exam-iner lifted the tested limb in hip flexion,
while maintaining the knee in full exten-sion. The inclinometer was
placed on the distal half of the anterior border of the tibia. The
measurement was taken when no further motion occurred or when the
examiner noted any change in the posi-tion of the pelvis.
Ankle Dorsiflexion With the Knee Ex-tended (Gastrocnemius
Flexibility) The subject was positioned in the prone posi-tion,
feet over the edge of the table. The foot of the tested ankle was
maintained in subtalar joint neutral, with the examiner palpating
the medial and lateral aspects of the head of the talus.
Dorsiflexion was measured as the angle formed by the line from the
head of the fibula to the tip of the lateral malleolus and the
lateral mid-line of the foot, using the border of the
rearfoot/calcaneus.
Statistical AnalysisKappa coefficients and percent agree-ment
between examiners were used as estimates of interrater reliability
for the rating of the quality of movement on the FSD test. Kappa
values of 0.20 or less were considered poor, 0.21 to 0.40 fair,
0.41 to 0.60 moderate, and greater than 0.60 good.30 All of the
continuous vari-ables were found to approximate a nor-mal
distribution (Kolmogorov-Smirnov Z test, P>.05). Independent t
tests were used to identify differences in demo-graphic variables
(age, height, and body mass), as well as in the musculoskeletal
measurements between subjects with good and moderate movement
quality on the FSD test. The alpha level was set at .05. All
statistical analyses were per-formed using PASW Statistics 18 (SPSS
Inc, Chicago, IL).
RESULTS
The examiners rated the move-ment quality on the FSD test as
good for 11 subjects, moderate for 14
subjects, and poor for 1 subject. The kap-pa coefficient (95%
confidence interval) and percent agreement for the interrater
reliability of rating the quality of move-ment for the FSD test
were 0.80 (0.57, 1.00) and 85%, respectively. The results of the
independent t tests (excluding the subject with the poor rating)
assess-ing the differences in demographics and musculoskeletal
measurements between the good and moderate groups are sum-
43-07 Park.indd 507 6/19/2013 1:09:07 PM
Jour
nal o
f O
rtho
paed
ic &
Spo
rts
Phys
ical
The
rapy
®
Dow
nloa
ded
from
ww
w.jo
spt.o
rg a
t on
Oct
ober
5, 2
013.
For
per
sona
l use
onl
y. N
o ot
her
uses
with
out p
erm
issi
on.
Cop
yrig
ht ©
201
3 Jo
urna
l of
Ort
hopa
edic
& S
port
s Ph
ysic
al T
hera
py®
. All
righ
ts r
eser
ved.
-
508 | july 2013 | volume 43 | number 7 |
journal of orthopaedic & sports physical therapy
[ research report ]marized in TABLE 1. Significantly less hip
abductor strength, knee flexion range of motion in the prone
position, and hip ad-duction range of motion in the sidelying
position were found in the subjects with moderate movement quality
compared to those with good movement quality. The frequency of
movement deviations for each group, as rated by raters 1 and 2, is
summarized in TABLE 2.
DISCUSSION
The purposes of this study were to investigate the interrater
reliabil-ity of assessing movement quality
of the lower extremity during the FSD test and to compare the
musculoskeletal characteristics between asymptomatic women with
different levels of movement quality. The primary findings were
that the kappa coefficient and percent agree-ment of the FSD test
were high, and that the subjects with moderate movement quality had
significantly less hip abduc-tor strength and quadriceps and
ITB/TFL flexibility compared to those with good movement
quality.
The interrater reliability of the clas-sification system for
rating movement quality during the FSD test in our inves-tigation
(κ = 0.80; agreement, 85%) was similar to that previously reported
by Piva et al22 (κ = 0.67; agreement, 80%), who used the same
classification system during a lateral step-down test in patients
with patellofemoral pain syndrome. In contrast, previous studies
reported bet-ter interrater reliability for movement quality
assessed during functional tasks. Ageberg et al1 reported high
interrater reliability (κ>0.90; agreement, 96%) for the visual
assessment of mediolateral knee motion during a single-limb
mini-squat. Similarly, Ekegren et al11 reported high intrarater
reliability (κ = 0.75-0.85; agreement, 88%-90%) for visual ratings
of dynamic knee valgus during a drop jump performed by healthy
participants. These differences in interrater reliability can be
partially explained by the classi-fication criteria. These
authors1,11 used a
classification system solely based on the frontal plane position
of the knee relative to the foot. In contrast, the classification
system used in this study is more com-prehensive and requires the
simultaneous evaluation of arm strategy, trunk, pelvis, knee
alignment, and balance. This great-er number of scoring criteria
might have increased the probability of disagreement between
raters.
In this study, the examiners rated the movement quality on the
FSD test as good for 11 subjects and moderate for 14 subjects. In
addition, 1 subject (3.8%) was considered to have poor movement
quality during the FSD. Chmielewski et al5 reported that 11.5% of
uninjured sub-
jects who performed a lateral step-down task had a poor movement
rating. It is possible that the greater the number of deviations
during the FSD, the greater the potential risk of limited
performance and injury.
Previous studies have established an association between hip
abductor weakness and altered movement pat-tern during dynamic
activities.6,9,14,26,28 Our findings are consistent with these
studies, as we found that subjects with a moderate movement quality
during the FSD showed relatively lower hip ab-duction strength than
those with good movement quality. Hip abduction mus-culature
provides pelvis and stance limb
TABLE 1Subject Characteristics for Groups
Based on Quality of Movement*
Abbreviation: ROM, range of motion.*Values are mean
SD.†Significantly different between good and moderate groups (P
-
journal of orthopaedic & sports physical therapy | volume 43
| number 7 | july 2013 | 509
stability by eccentric control during weight-bearing
activities.12,16 Weakness of the hip abductors can lead to
excessive femoral adduction, a contralateral pelvic drop, or both
during weight-bearing ac-tivities.24 This, in turn, can alter hip
and knee joint mechanics.24 The 2 movement alterations more likely
to occur as a result of weaker hip abductors are changes in trunk
alignment and pelvic plane motion, which were the most frequent
movement deviations noted in our sample (TABLE 2). Leaning the
trunk laterally over the stance leg shifts the center of mass over
the hip joint center, thereby reducing the internal abduction
moment demand on the weak muscles.21 In addition, elevat-ing the
contralateral pelvis is a common compensation strategy for reducing
the demand on the hip abductors, as it moves the ground reaction
force vector closer to the hip joint center.23
In this study, strength of the hip ex-ternal rotators was not
reduced in those with moderate quality of movement, suggesting that
the trunk lean and pelvic rotation exhibited in the moderate group
during the FSD test were not caused by weak hip external
rotators.
Our findings showed that there was no significant difference in
hip external and internal rotation range of motion between the
groups with good and mod-erate quality of movement. Rabin and
Kozol25 investigated hip external and internal rotation range of
motion during the lateral step-down test in healthy fe-males and
reported no significant differ-ence between groups with different
levels of movement quality. In contrast to our findings, Sigward et
al27 demonstrated decreased hip external rotation range of motion
among subjects with greater me-dial displacement of the knee during
the drop-land task. The difference between our findings and those
of Sigward et al27 may be due to differences in the function-al
task used in the 2 studies (drop landing versus FSD).
The subjects with moderate move-ment quality had relatively
lower quad-riceps flexibility compared to those with
good movement quality. As the knee only needed to be flexed to
60° during the FSD test, it is not clear how reduced flexibility
could be associated with poor quality of movement. Our data also
indicated that individuals with moderate movement quality had less
ITB/TFL flexibility. De-creased muscle flexibility of the ITB/TFL
may lead to ipsilateral rotation of the pel-vis in the transverse
plane, internal rota-tion of the hip,15,21 and external rotation of
the tibia, thus facilitating dynamic knee valgus alignment.17
Finally, our study found no difference in hamstring and
gastrocnemius flexibility between sub-jects with good and moderate
quality of movement on the FSD, suggesting that hamstring and
gastrocnemius flexibility may not be responsible for the movement
deviation observed in a symptomatic women exhibiting moderate
quality of movement during the FSD test.
Our study has some limitations. First, the findings are limited
to asymptomatic women, which limits the generalizability of the
results to other populations, in-cluding asymptomatic males or
patients with a knee disorder. Second, because the subjects of this
study were recruited from the Department of Physical Therapy, we
cannot rule out subject bias, as these individuals could have had
knowledge of good and bad movement patterns. However, we provided
consistent verbal instruction to each subject to reduce this bias.
Third, because the functional move-ment test was performed first
and the musculoskeletal measurements second, the potential for
examiner bias during the musculoskeletal measurements can-not be
excluded. Fourth, we examined reliability using a categorical
distribution (good, moderate, and poor) and not each movement
deviation, which could have affected reliability ratings. Although
the frequency distribution was similar be-tween raters, it does not
guarantee that for each trial the raters observed the same movement
deviation. Fifth, a cause-and-effect relationship between movement
pattern and noted strength and flexibil-ity differences between
groups cannot be
assumed, given the cross-sectional de-sign of the study.
Finally, the validity of using movement quality on the FSD test to
predict those at greater risk of injuries is unknown.
CONCLUSION
Assessment of movement quality on the FSD test had good
interrater reliability. Asymptomatic women
with moderate movement quality during the FSD test exhibited
less hip abduction strength and decreased quadriceps and ITB/TFL
flexibility compared to those with good movement quality. t
KEY POINTSFINDINGS: Assessment of movement qual-ity on the FSD
test had good interrater reliability. Asymptomatic women with
moderate movement quality during the FSD test exhibited less hip
abduction strength and decreased quadriceps and ITB/TFL flexibility
compared to those with good movement quality.IMPLICATIONS:
Clinicians should consider assessment of hip abductor strength and
flexibility of the quadriceps and ITB/TFL when individuals
demonstrate poor quality of movement on the FSD test.CAUTION: The
results of this study are limited to asymptomatic women.
REFERENCES
1. Ageberg E, Bennell KL, Hunt MA, Simic M, Roos EM, Creaby MW.
Validity and inter-rater reli-ability of medio-lateral knee motion
observed during a single-limb mini squat. BMC Mus-culoskelet
Disord. 2010;11:265. http://dx.doi.org/10.1186/1471-2474-11-265
2. Austin AB, Souza RB, Meyer JL, Powers CM. Identification of
abnormal hip motion associ-ated with acetabular labral pathology. J
Orthop Sports Phys Ther. 2008;38:558-565.
http://dx.doi.org/10.2519/jospt.2008.2790
3. Bell DR, Padua DA, Clark MA. Muscle strength and flexibility
characteristics of people display-ing excessive medial knee
displacement. Arch Phys Med Rehabil. 2008;89:1323-1328.
http://dx.doi.org/10.1016/j.apmr.2007.11.048
4. Chinkulprasert C, Vachalathiti R, Powers CM. Patellofemoral
joint forces and stress during
43-07 Park.indd 509 6/19/2013 1:09:10 PM
Jour
nal o
f O
rtho
paed
ic &
Spo
rts
Phys
ical
The
rapy
®
Dow
nloa
ded
from
ww
w.jo
spt.o
rg a
t on
Oct
ober
5, 2
013.
For
per
sona
l use
onl
y. N
o ot
her
uses
with
out p
erm
issi
on.
Cop
yrig
ht ©
201
3 Jo
urna
l of
Ort
hopa
edic
& S
port
s Ph
ysic
al T
hera
py®
. All
righ
ts r
eser
ved.
http://dx.doi.org/10.1186/1471-2474-11-265http://dx.doi.org/10.1186/1471-2474-11-265http://dx.doi.org/10.2519/jospt.2008.2790http://dx.doi.org/10.2519/jospt.2008.2790http://dx.doi.org/10.1016/j.apmr.2007.11.048http://dx.doi.org/10.1016/j.apmr.2007.11.048
-
510 | july 2013 | volume 43 | number 7 |
journal of orthopaedic & sports physical therapy
[ research report ]
MORE INFORMATIONWWW.JOSPT.ORG@
forward step-up, lateral step-up, and forward step-down
exercises. J Orthop Sports Phys Ther. 2011;41:241-248.
http://dx.doi.org/10.2519/jospt.2011.3408
5. Chmielewski TL, Hodges MJ, Horodyski M, Bish-op MD, Conrad
BP, Tillman SM. Investigation of clinician agreement in evaluating
movement quality during unilateral lower extremity func-tional
tasks: a comparison of 2 rating methods. J Orthop Sports Phys Ther.
2007;37:122-129. http://dx.doi.org/10.2519/jospt.2007.2457
6. Cichanowski HR, Schmitt JS, Johnson RJ, Niemuth PE. Hip
strength in collegiate female athletes with patellofemoral pain.
Med Sci Sports Exerc. 2007;39:1227-1232.
http://dx.doi.org/10.1249/mss.0b013e3180601109
7. Costigan PA, Deluzio KJ, Wyss UP. Knee and hip kinetics
during normal stair climbing. Gait Pos-ture. 2002;16:31-37.
http://dx.doi.org/10.1016/S0966-6362(01)00201-6
8. Crossley K, Bennell K, Green S, Cowan S, McConnell J.
Physical therapy for patello-femoral pain: a randomized,
double-blinded, placebo-controlled trial. Am J Sports Med.
2002;30:857-865.
9. Dierks TA, Manal KT, Hamill J, Davis IS. Proximal and distal
influences on hip and knee kinemat-ics in runners with
patellofemoral pain during a prolonged run. J Orthop Sports Phys
Ther. 2008;38:448-456.
http://dx.doi.org/10.2519/jospt.2008.2490
10. Edwards L, Dixon J, Kent JR, Hodgson D, Whittaker VJ. Effect
of shoe heel height on vastus medialis and vastus lateralis
elec-tromyographic activity during sit to stand. J Orthop Surg Res.
2008;3:2. http://dx.doi.org/10.1186/1749-799X-3-2
11. Ekegren CL, Miller WC, Celebrini RG, Eng JJ, MacIntyre DL.
Reliability and validity of observational risk screening in
evaluating dy-namic knee valgus. J Orthop Sports Phys Ther.
2009;39:665-674. http://dx.doi.org/10.2519/jospt.2009.3004
12. Fulkerson JP. Disorders of the Patellofemoral Joint. 3rd ed.
Baltimore, MD: Williams & Wilkins; 1997.
13. Hewett TE, Myer GD, Ford KR, et al. Bio-mechanical measures
of neuromuscular control and valgus loading of the knee pre-
dict anterior cruciate ligament injury risk in female athletes:
a prospective study. Am J Sports Med. 2005;33:492-501.
http://dx.doi.org/10.1177/0363546504269591
14. Ireland ML, Willson JD, Ballantyne BT, Davis IM. Hip
strength in females with and without patellofemoral pain. J Orthop
Sports Phys Ther. 2003;33:671-676.
15. Jull GA, Janda V. Muscle and motor control in low back pain:
assessment and management. In: Twomey LT, Taylor JR, eds. Physical
Therapy of the Low Back. New York, NY: Churchill Living-stone;
1987:253-278.
16. Kendall FP, Provance P, McCreary EK. Muscles: Testing and
Function. 4th ed. Baltimore, MD: Williams & Wilkins; 1993.
17. Kwak SD, Ahmad CS, Gardner TR, et al. Ham-strings and
iliotibial band forces affect knee kinematics and contact pattern.
J Orthop Res. 2000;18:101-108.
http://dx.doi.org/10.1002/jor.1100180115
18. Loudon JK, Wiesner D, Goist-Foley HL, Asjes C, Loudon KL.
Intrarater reliability of func-tional performance tests for
subjects with patellofemoral pain syndrome. J Athl Train.
2002;37:256-261.
19. Lowry CD, Cleland JA, Dyke K. Management of patients with
patellofemoral pain syndrome using a multimodal approach: a case
series. J Orthop Sports Phys Ther. 2008;38:691-702.
http://dx.doi.org/10.2519/jospt.2008.2690
20. Mascal CL, Landel R, Powers C. Management of patellofemoral
pain targeting hip, pelvis, and trunk muscle function: 2 case
reports. J Orthop Sports Phys Ther. 2003;33:647-660.
21. Page P, Frank CC, Lardner R. Assessment and Treatment of
Muscle Imbalance: The Janda Ap-proach. Champaign, IL: Human
Kinetics; 2010.
22. Piva SR, Fitzgerald K, Irrgang JJ, et al. Reli-ability of
measures of impairments associated with patellofemoral pain
syndrome. BMC Musculoskelet Disord. 2006;7:33.
http://dx.doi.org/10.1186/1471-2474-7-33
23. Powers CM. The influence of abnormal hip mechanics on knee
injury: a biomechani-cal perspective. J Orthop Sports Phys Ther.
2010;40:42-51. http://dx.doi.org/10.2519/jospt.2010.3337
24. Powers CM. The influence of altered lower-
extremity kinematics on patellofemoral joint dysfunction: a
theoretical perspective. J Orthop Sports Phys Ther.
2003;33:639-646.
25. Rabin A, Kozol Z. Measures of range of motion and strength
among healthy women with differ-ing quality of lower extremity
movement during the lateral step-down test. J Orthop Sports Phys
Ther. 2010;40:792-800.
http://dx.doi.org/10.2519/jospt.2010.3424
26. Robinson RL, Nee RJ. Analysis of hip strength in females
seeking physical therapy treatment for unilateral patellofemoral
pain syndrome. J Or-thop Sports Phys Ther. 2007;37:232-238.
http://dx.doi.org/10.2519/jospt.2007.2439
27. Sigward SM, Ota S, Powers CM. Predictors of frontal plane
knee excursion during a drop land in young female soccer players. J
Orthop Sports Phys Ther. 2008;38:661-667.
http://dx.doi.org/10.2519/jospt.2008.2695
28. Souza RB, Powers CM. Differences in hip kine-matics, muscle
strength, and muscle activation between subjects with and without
patellofemo-ral pain. J Orthop Sports Phys Ther. 2009;39:12-19.
http://dx.doi.org/10.2519/jospt.2009.2885
29. Van Dillen LR, Bloom NJ, Gombatto SP, Susco TM. Hip rotation
range of motion in people with and without low back pain who
participate in rotation-related sports. Phys Ther Sport.
2008;9:72-81. http://dx.doi.org/10.1016/j.ptsp.2008.01.002
30. Viera AJ, Garrett JM. Understanding interob-server
agreement: the kappa statistic. Fam Med. 2005;37:360-363.
31. Witvrouw E, Danneels L, Van Tiggelen D, Wil-lems TM, Cambier
D. Open versus closed kinetic chain exercises in patellofemoral
pain: a 5-year prospective randomized study. Am J Sports Med.
2004;32:1122-1130. http://dx.doi.org/10.1177/0363546503262187
32. Witvrouw E, Lysens R, Bellemans J, Peers K, Vanderstraeten
G. Open versus closed kinetic chain exercises for patellofemoral
pain. A pro-spective, randomized study. Am J Sports Med.
2000;28:687-694.
NOTIFY JOSPT of Changes in AddressPlease remember to let JOSPT
know about changes in your mailing address. The US Postal Service
typically will not forward second-class periodical mail. Journals
are destroyed, and the USPS charges JOSPT for sending them to the
wrong address. You may change your address online at www.jospt.org.
Visit “INFORMATION FOR READERS”, click “Change of Address”, and
select and complete the online form. We appreciate your assistance
in keeping JOSPT’s mailing list up to date.
43-07 Park.indd 510 6/19/2013 1:09:11 PM
Jour
nal o
f O
rtho
paed
ic &
Spo
rts
Phys
ical
The
rapy
®
Dow
nloa
ded
from
ww
w.jo
spt.o
rg a
t on
Oct
ober
5, 2
013.
For
per
sona
l use
onl
y. N
o ot
her
uses
with
out p
erm
issi
on.
Cop
yrig
ht ©
201
3 Jo
urna
l of
Ort
hopa
edic
& S
port
s Ph
ysic
al T
hera
py®
. All
righ
ts r
eser
ved.
www.jospt.orghttp://dx.doi.org/10.2519/jospt.2011.3408http://dx.doi.org/10.2519/jospt.2011.3408http://dx.doi.org/10.2519/jospt.2007.2457http://dx.doi.org/10.1249/mss.0b013e3180601109http://dx.doi.org/10.1249/mss.0b013e3180601109http://dx.doi.org/10.1016/S0966-6362(01)00201-6http://dx.doi.org/10.1016/S0966-6362(01)00201-6http://dx.doi.org/10.2519/jospt.2008.2490http://dx.doi.org/10.2519/jospt.2008.2490http://dx.doi.org/10.1186/1749-799X-3-2http://dx.doi.org/10.1186/1749-799X-3-2http://dx.doi.org/10.2519/jospt.2009.3004http://dx.doi.org/10.2519/jospt.2009.3004http://dx.doi.org/10.1177/0363546504269591http://dx.doi.org/10.1177/0363546504269591http://dx.doi.org/10.1002/jor.1100180115http://dx.doi.org/10.1002/jor.1100180115http://dx.doi.org/10.2519/jospt.2008.2690http://dx.doi.org/10.1186/1471-2474-7-33http://dx.doi.org/10.1186/1471-2474-7-33http://dx.doi.org/10.2519/jospt.2010.3337http://dx.doi.org/10.2519/jospt.2010.3337http://dx.doi.org/10.2519/jospt.2010.3424http://dx.doi.org/10.2519/jospt.2010.3424http://dx.doi.org/10.2519/jospt.2007.2439http://dx.doi.org/10.2519/jospt.2007.2439http://dx.doi.org/10.2519/jospt.2008.2695http://dx.doi.org/10.2519/jospt.2008.2695http://dx.doi.org/10.2519/jospt.2009.2885http://dx.doi.org/10.1016/j.ptsp.2008.01.002http://dx.doi.org/10.1016/j.ptsp.2008.01.002http://dx.doi.org/10.1177/0363546503262187http://dx.doi.org/10.1177/0363546503262187
504JOSPTjul13505JOSPTjul13506JOSPTjul13507JOSPTjul13508JOSPTjul13509JOSPTjul13510JOSPTjul13





















![(Royton Sapporo [Royton Hall] 3F) 24 Cerebrovascular ... · Hiroki Abe Department of Neurology, National Center Hospital, ... development of mDA neurons in mice Du-seock Kang](https://img.pdfslide.net/doc/110x75/5be2ea9309d3f2f02d8c2ac3/royton-sapporo-royton-hall-3f-24-cerebrovascular-hiroki-abe-department.jpg)