Embed Size (px)
Citation preview

Myeloma UpdatesASH 2011 Annual Meeting
Steve Smith
OHSU Knight Cancer Institute
Center for Hematologic Malignancies

What was new is now old…
long-term data on novel agent + chemo combinations
2nd generation immunomodulators, proteasome inhibitors
Will chemotherapy combinations be replaced by multitargeted therapies?

Overview: Progress in MM
Overall survival rates improving• in younger patients
Almost 800 ASH abstracts in multiple myeloma• about 10x more than a decade ago
understanding of pathbiology• of the malignant plasma cell and microenvironment
ASH 2011: • nontransplant (elderly) regimens: longer follow-up• second generation novel agents• “multitargeted” strategies

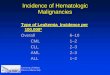
MM Survival Trends
1950 – 19591960 – 19691970 – 19791980 – 19891990 – 19992000 – 2005
0
0.2
0.4
0.6
0.8
1.0
Ove
rall
Su
r viv
al
(pro
po
r tio
n)
Ti me Si nce Di agnosi s (months)
0.1
0.3
0.5
0.7
0.9
12 24 36 48 60 72 84 96 108 120 132 144 156 168 1800
0.2
0.4
0.6
0.8
1.0
Ove
rall
Su
r viv
al
(pro
po
r tio
n)
Ti me Si nce Di agnosi s (months)
0.1
0.3
0.5
0.7
0.9
12 24 36 48 60 72 84 96 108 120 132 144 156 168 180
Patients < 65 years at Diagnosis* Patients > 65 years at Diagnosis*
Turesson I, et al. J Clin Oncol. 2009;28:830-834.
*Swedish Registry data.

MPT1
N = 129VMP2
N = 337MPR3
N = 153MPR-R4
N = 152VTP5
N = 130
CR 16% 30% 11% 16% 27%
> VGPR 29% Not reported 33% 32% 37%
> PR 69% 71% 68% 77% 81%
PFS 21.8 mo TTP: 24.0 mo 14 mo 31 mo 23 mo
Median follow-up 31.8 mo 36.7 mo 25 mo 25 mo 22 mo
1Palumbo A, et al. Blood. 2008;112:3107-3114; 2Mateos MV, et al. Blood. 2009;114(22). Abstract 3859;
3,4Palumbo A, et al. Blood. 2010;116(21). Abstract 622 and Abstract 566; 5Mateos MV, et al. Blood. 2009;114(22). Abstract 3.
MPT: melphalan, prednisone, thalidomide; VMP: bortezomib, melphalan, prednisone; MPR: melphalan, prednisone, lenalidomide; MPR-R: MPR with maintenance lenalidomide; VTP: bortezomib, thalidomide, prednisone.
Newly Diagnosed, Patients SCT Ineligible

VISTA Final Analysis
(Velcade) as Initial Standard Therapy in Multiple Myeloma= VISTA
updated OS analysis of VISTA after 5 years median follow-up
randomized, international, phase III clinical trial
Newly Diagnosed/SCT ineligible

VISTA Final Analysis
Newly Diagnosed/SCT ineligible

VISTA Final Analysis
5-year OS • VMP vs MP: 46.0% vs 34.4% • 13.3-month increase in OS
OS benefit in most subgroups • sex, race, geographic region, β2-microglobulin level, and
albumin level
OS benefit not observed for high-risk cytogenetics • OS benefit initially observed in VMP arm diminished when patients received
second-line therapy (included bortezomib in 60% of MP pts)
Newly Diagnosed/SCT ineligible

MPRR: Italian intergroup study MM-015 ASH 2011: 41 month f/u
MM-015: MPR with or without maintenance lenalidomide, vs MP in upfront SCT ineligible pts
Newly Diagnosed/SCT ineligible

Italian Intergroup MM-015
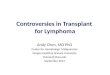
PFS benefit to lenalidomide maintenance
MPR-R vs MPR
Landmark Analysis: PFS After Cycle 9
Palumbo A, et al. Blood. 2009;114(22). Abstract 613;Palumbo A, et al. European Hematology Association 15th Congress. 2010. Abstract 566.
100
75
50
25
00 5 10 20 2515
Time (months)
Pat
ient
s(%
)
30
HR 0.314Log rank P< 0.001
Newly Diagnosed/SCT ineligible

MM-015: Outcomes in Overall Population
Continued lenalidomide significantly improves PFS vs placebo• PFS benefit extended through patient subgroups in landmark analysis
⁻ Age (65-75 vs > 75 yrs), response (PR vs ≥ VGPR), ISS stage (I/II vs III)
• No effect on OS or TTP with maintenance lenalidomide
Palumbo A, et al. ASH 2011. Abstract 475.
Outcome MPR-R(n = 152)
MPR(n = 153)
MP(n = 154)
Median PFS, mos HR vs MP P value vs MP
310.395< .001
140.796.135
13
4-yr OS, % HR vs MP P value vs MP
590.898.579
581.089.648
58
TTP HR vs MP 0.337 0.826

MM-015: Grade 4 Toxicities during induction and maintenance
1. é J et al. Br J Haematol. 1998;102:1115-1123. Palumbo A, et al. ASH 2011 Abstract 475
Adverse Events, %*Induction Therapy Maintenance
Therapy
MPR MP MPR-R MPR
Grade 4 hematologic events
•Neutropenia 32 7 2 0
•Thrombocytopenia 7 4 4 3
•Anemia 2 2 3 1
•Febrile neutropenia 0 0 0 0
Newly Diagnosed/SCT ineligible

MM-015: Second Malignancies
1. é J et al. Br J Haematol. 1998;102:1115-1123. Palumbo A, et al. ASH 2011 Abstract 475
Second Malignancies, Incidence Rate/100 Patients/Yr
MPR-R(n = 150)
MPR(n = 152)
MP(n = 153)
Total invasive second primary malignancies
3.04 2.57 0.98
Hematologic malignancies 1.75 1.54 0.24
Solid tumors 1.26 1.28 0.74
Nonmelanoma skin cancer 0.50 1.29 1.50
Newly Diagnosed/SCT ineligible

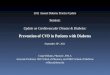
Kumar, et al. Haematologica. 2010;95(suppl 2). Abstract 376.
Patients Relapsing and Refractory to Bortezomib and Thalidomide or Lenalidomide
Relapsed / Refractory Disease
N Events (n) Median
Overall Survival 291 173 9 months
Event-Free Survival 291 222 5 months
0%
20%
40%
60%
80%
100%
0 12 24 36 48 60Months

The Next Generation…
2nd generation immunomodulatory agents
2nd generation proteasome inhibitors
HDAC Inhibitors
Monoclonal antibodies
Alkylating agents
Other proteasome inhibitors
Heat shock protein inhibitors
PI3K / AKT inhibitor
mTOR inhibitors

Carfilzomib: second-generation proteasome inhibitor
Administered IV• First 2 days of each week, for 3 weeks (repeated monthly)
Active in heavily pretreated MM patients
Mild neuropathy seen but uncommon (< 20%)• Severe neuropathy (grade 3-4): <2% • Toxicity
⁻ Myelosuppression, fatigue, URI/ PNA, infusion reactions ≈ 15% grade 3-4 anemia, thrombocytopenia, and neutropenia
PX-171-003-A1: Siegel DS, et al. Blood. 2010;116(2). Abstract 985;PX-171-004 Stewart K, et al. Hematologica. 2010;95(S2). Abstract 1099;
Wang ASH 2009 Abstract 302.
Niesvizky R, et al. Blood. 2010;116(2). Abstract 619.

Carfilzomib: Phase II Rel/Ref MM
ASH 2011: Single-Agent Carfilfzomib, rel/ref MM (PX-171-004): Final results from the bortezomib-naive group
n = 129 Treated for up to 12 cycles
Data from 2 cohorts presented
1- Carfilzomib 20 mg/m2 (n=59)
2- Carfilzomib 20 mg/m2 for cycle 1, then to 27 mg/m2 for cycles 2-12 (n=70)
Vij R, Kaufman JL, Jakubowiak AJ, et al. Abstract 813 Rel/Ref MM

Carfilzomib phase II PX-171-004: Baseline characteristics
Vij R, Kaufman JL, Jakubowiak AJ, et al. Abstract 813
CharacteristicCarfilzomib
20 mg/m2
(n = 59)
Carfilzomib 20/27 mg/m2
(n = 70)
Median age, yrs (range) 65 (38-82) 65.5 (45-85)
Median yrs from diagnosis (range) 3.5 (0.7-24.4) 3.6 (0.7-12.2)
Neuropathy, % 49 55
Median previous treatments, n (range)
2 (1-4) 2 (1-4)
Refractory to most recent therapy, %
66 64
Prior Stem cell transplantation (%)
80 67
Cyto or FISH = Unfavorable (%) 15 14
Rel/Ref MM

Carfilzomib phase II PX-171-004: Response Data
Vij R, Kaufman JL, Jakubowiak AJ, et al. Abstract 813
OutcomeCarfilzomib
20 mg/m2
(n = 59)
Carfilzomib 20/27 mg/m2
(n = 67)*
ORR, % 42 52 CR 3 2
VGPR 14 27
PR 25 24
Median time to response, mos
1.0 1.9
Median PFS, mos 8.2 NR
Median duration of f/u, mos
23.2 13.8
Rel/Ref MM

Carfilzomib phase II PX-171-004: Conclusions
In bortezomib-naïve rel/ref MM pts, combined ORR 48%• Potential dose-response relationship
No increase in neuropathy risk with carfilzomib in pts with history of, or pre-existing, neuropathy• PNP is
⁻ Mostly mild to moderate severity , not dose limiting
Grade 3/4 adverse events in 80% of patients- primarily hematologic
⁻ Generally reversible
AE’s led to treatment discontinuation in 16% of patients
Vij R, Kaufman JL, Jakubowiak AJ, et al. Abstract 813 Rel/Ref MM

ASH 2011: Phase 2 results
Carfilzomib + len + dex
Upfront, SCT-eligible

Upfront, SCT-eligible

Upfront, SCT-eligible

Upfront, SCT-eligible

Upfront, SCT-eligible

Upfront, SCT-eligible

MLN9708 Phase I Study: ASH 2011
MLN9708, PO proteasome inhibitor Phase I study relapsed/refractory MM (N = 56)
⁻ Dose-escalation phase (n = 26)⁻ Expansion phase (n = 36; 6 from dose-escalation cohort)⁻ 27% to 32% refractory to bortezomib on last previous therapy
MLN9708 dosing ⁻ Starting 0.24 mg/m2, increased to 2.23 mg/m2 on Days 1, 4, 8, 11 of a
21-day cycle for up to 12 cycles
• 46 patients evaluable for response
Richardson PG, et al. ASH 2011. Abstract 301.Rel/Ref MM

MLN9708 Phase I Study: Safety and Response
MTD 2.0 mg/m2
• 32% of patients required dose reductions due to adverse events⁻ Mainly thrombocytopenia, neutropenia, and rash⁻ 9% of patients discontinued treatment due to adverse events
Grade 3/4 adverse events: thrombocytopenia (34%), neutropenia (14%), fatigue (9%), rash (9%)• No grade 3 /4 neuropathy
15% (n = 7) patients achieved response• Durable disease control up to 15.9 mos• Majority (61%) of remaining patients reached SD, durable for up to 12.9
mos
Richardson PG, et al. ASH 2011. Abstract 301.Rel/Ref MM

MLN9708 + Len + Dex: Phase I/II Combination
Open-label, multicenter, dose-escalation phase I/II trial• Primary endpoints: safety, MTD, recommended phase II dose
⁻ Secondary endpoints: MLN2238 pharmacokinetics, treatment response
Previously untreated MM (n = 15 to date)
Treatment: 28-day cycles for up to 12 mos⁻ MLN9708: started at 1.68 mg/m2, increased in 33% increments based DLT
⁻ Dex: 40 mg/day on Days 1, 8, 15, 22
⁻ Lenalidomide: 25 mg/day on Days 1-21
Berdeja JG, et al. ASH 2011. Abstract 479.Upfront, SCT-eligible

MLN9708 + Len + Dex Phase I/II: outcomes
Responses observed in all patients (N =15), generally in cycle 1• CR (n = 4), VGPR (n = 5), and PR (n = 6)
No DLT observed up to 2.23 mg/m2 MLN9708• Recommended phase II dose: 2.23 mg/m2/wk
Well tolerated • Grade 1 peripheral neuropathy (n = 3)
• Grade 3: vomiting (n = 2), deep vein thrombosis (n = 2), anemia (n = 2),rash (n = 2)
• Grade 4: thrombocytopenia (n = 1)
Berdeja JG, et al. ASH 2011. Abstract 479.Upfront, SCT-eligible

Final topic…Relapsed/novel agents:
Multitargeted combinations

clinicaloptions.com/oncologyUpdate on Multiple Myeloma
VANTAGE 088: Study Design
International, multicenter, double-blind, randomized phase III trial[1]
– Vorinostat: HDAC inhibitor active when combined with bortezomib in phase I and II trials[2-4]
1. Dimopoulos MA, et al. ASH 2011. Abstract 811. 2. Weber D, et al. ASCO 2008. Abstract 871.3. Badros A, et al. Clin Cancer Res. 2009;15:5250-5257. 4. Siegel DS, et al. ASH 2011. Abstract 480.
Relapsed/refractory MM
patients with PD followingmost recent therapy
(N = 637)
1-3 previous therapies; bortezomib sensitive
PD or unacceptable
toxicity
Bortezomib 1.3 mg/m2
on Days 1, 4, 8, 11 +Vorinostat 400 mg/day
on Days 1-14(n = 317)
Bortezomib 1.3 mg/m2
on Days 1, 4, 8, 11 +Placebo(n = 320)
21-day cycles
Primary endpoint: PFSSecondary endpoints:OS, TTP, ORR, safety
Rel/Ref MM

clinicaloptions.com/oncologyUpdate on Multiple Myeloma
VANTAGE 088: PFS, OS, and Response
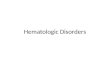
PFS significantly prolonged with addition of vorinostat to bortezomib
– No difference in median OS (data not yet mature)
Dimopoulos MA, et al. ASH 2011. Abstract 811.
0
10
20
30
40
50
60
70
ORR CR VGPR PRResponse Type
Res
pons
e R
ate
(%)
MR SD
Bortezomib + vorinostat (n = 315)Bortezomib + placebo (n = 320)
7.63 vs 6.83 mosHR: 0.774 (95% CI: 0.64-0.94; P = .01)
P < .0001
0
20
40
60
80
100
Pat
ient
s W
ith P
FS
(%
)
0 5 10 15 20 25Mos
PFS (IAC) Response (IAC)
Rel/Ref MM

clinicaloptions.com/oncologyUpdate on Multiple Myeloma
PANORAMA-2: Study Design
Panobinostat: potent, investigational HDAC inhibitor
– Combination with bortezomib active in relapsed/refractory MM
– ORR: 80% (overall population); 50% (bortezomib-refractory subset)[1]
Current study evaluated efficacy of panobinostat with bortezomib plus dexamethasone in relapsed bortezomib-refractory MM patients (N = 55)[2]
– Single-arm phase II trial
– Primary endpoint: ORR
1. San Miguel J, et al. 2011 EHA. Abstract 0314. 2. Richardson PG, et al. ASH 2011. Abstract 814.
Phase I: 8 x 3-wk cyclesPanobinostat 20 mg on Days 1, 3, 5, 8, 10, 12 +
Bortezomib 1.3 mg/m2 on Days 1, 4, 8, 11 +Dexamethasone 20 mg on Days 1, 2, 4, 5, 8, 9, 11, 12
Phase II (for patients with clinical benefit after phase I):6-wk cycles until PD
Panobinostat 20 mg on Days 1, 3, 5, 8, 10,12, 22, 24, 26, 29, 31, 33 +
Bortezomib 1.3 mg/m2 on Days 1, 8, 22, 29 +Dexamethasone 20 mg on Days 1, 2, 8, 9, 22, 23, 29, 30
Rel/Ref MM

clinicaloptions.com/oncologyUpdate on Multiple Myeloma
PANORAMA-2: Response and Safety
Responses were rapid, often within 1-2 cycles
Most frequent grade 3/4 events: thrombocytopenia (53%), anemia (16%), neutropenia (12%)
– Peripheral neuropathy (24%) was grade 3/4 in only 1 patient (2%)
– Fatigue (63%) was grade 3/4 in 16%; generally manageable with dose reduction
Response Rate, % Panobinostat + Bortezomib + Dexamethasone (n = 55)
ORR (CR + nCR + PR) 29
CR 0
nCR 4
PR 25
Clinical benefit (ORR + MR) 49
MR 20
VGPR 6
Richardson PG, et al. ASH 2011. Abstract 814.Rel/Ref MM

clinicaloptions.com/oncologyUpdate on Multiple Myeloma
PANORAMA-2: Conclusions
Combination of investigational HDAC inhibitor panobinostat with bortezomib active[1]
– Effective even in this heavily pretreated, bortezomib-refractory MM patient set
Treatment relatively well tolerated[1]
– Grade 3/4 myelosuppression manageable with dose reduction or interruption
– Infrequent grade 3/4 peripheral neuropathy
Lower toxicity with this dose schedule (1 wk rest period between cycles) vs previously observed in phase I trial[2]
1. Richardson PG, et al. ASH 2011. Abstract 814. 2. San Miguel J, et al. 2011 EHA. Abstract 0314.Rel/Ref MM

On the horizon
Improving outcomes for lenalidomide/bortezomib- refractory patients
maximizing clinical benefit • disease control using maintenance? drug holiday? Multitargeted combinations?
Active clinical trials: • Novel agents, orally administered• MLN+rev+dex upfront • optimal ASCT regimen? CTN 0702:
⁻ tandem len maintenance ⁻ single len+bort+dex consolidation len maintenance⁻ single len maintenance

Acknowledgements
Myeloma Program at OHSU: • Emma Scott, MD ([email protected])• Anne Kratz, RN• Richard Maziarz, MD ([email protected])• All other MD, RN, PA/NP, admin staff at OHSU
Slides• Rachid Baz, MD (Moffitt Cancer Center, Tampa, FL)• Clinical Care Options (clinicaloptions.com)• educational concepts group (www.educationalconcepts.net)

(Extra slides)

(Extra slides)Consolidation after ASCT- already presented in Paris 2011…
CALGB 100104 • OS benefit to len maintenance after ASCT (90 vs 83% OS
at 28 months, p=.02)• TTP benefit 48 mo vs 31 mo• second malignancies higher (n=15 vs 6)
IFM 2005- clear PFS benefit (42 vs 22 mo), second malignancies higher, study halted
both: higher cumulative grade 3-4 PMN with maintenance, more 2nd malignancies…

clinicaloptions.com/oncologyUpdate on Multiple Myeloma
QuiRedex: Study Design
Multicenter, open-label, randomized phase III trial
– Evaluated new treatment regimen for smoldering MM vs current standard of care
Mateos MV, et al. ASH 2011. Abstract 991.
Patients with high-risk
smoldering MM
(N = 126)
Lenalidomide 25 mg/day on Days 1-21 +
Dexamethasone 20 mg/day on Days 1-4, 12-15
No Treatment No Treatment
Lenalidomide10 mg/day on Days 1-21
(Low-dose dexamethasoneadded at time of
biologic progression)
Induction9 x 28-day cycles
Maintenance28-day cycles
2 yrs
Primary endpoint: TTP to symptomatic MMSecondary endpoints: response, duration of response, safety and tolerability, PFS, OS

clinicaloptions.com/oncologyUpdate on Multiple Myeloma
QuiRedex: TTP to Symptomatic MM and OS Significant increase in TTP with vs without treatment
Significantly prolonged OS with vs without treatment
– Median 3-yr OS (from study inclusion): 93% vs 76%; P = .04
– Median 5-yr OS (from diagnosis): 94% vs 79%; P = .03
Mateos MV, et al. ASH 2011. Abstract 991.
Median TTPLenalidomide/dexamethasone: NR
No treatment: 23 mosHR: 6.0 (95% CI: 2.9-12.6; P < .0001)
Median follow-up: 32 mos (range: 12-49)
1.0
0.8
0.6
0.4
0.2
0
Pro
port
ion
of
Pat
ient
s A
live
Mos From Inclusion0 455 10 15 20 25 30 35 40
Lenalidomide + dexamethasoneNo treatment

clinicaloptions.com/oncologyUpdate on Multiple Myeloma
QuiRedex: Safety
3 cases of second primary malignancies reported in treatment arm
Mateos MV, et al. ASH 2011. Abstract 991.
Adverse Event, % Lenalidomide + Dexamethasone(n = 57)
No Treatment(n = 62)
Grade 1/2 Grade 3 Grade 1/2
Anemia 28 2 --
Neutropenia 20 5 --
Thrombocytopenia 13 2 --
Asthenia 20 7 11
Constipation 18 -- 2
Diarrhea 24 2 4
Rash 33 4 --
Paresthesias 5 -- --
Tremor 13 -- 2
Infection 46 6 26
Deep vein thrombosis 5 --

Alternative Bortezomib Regimens
Reeder CB, et al. ASH Annual Meeting Abstracts. 2009;114(22):616; Palumbo A, et al. ASH Annual Meeting Abstracts. 2010;116(21):620.
Regimen N ORR CR Grade 1/2 PN
> Grade 3 PN
CyBorD Twice weekly btz Once weekly btz
3330
88%93%
39%40%
64%56%
6%0%
VMPT-VT Twice weekly btz Once weekly btz
63190
86%85%
35%30%
29%19%
14%2%
Btz: bortezomib; PN: peripheral neuropathy; CyBorD: cytarabine, bortezomib, dexamethasone; VMPT-VT: bortezomib, melphalan, prednisone, thalidomide followed by maintenance bortezomib and thalidomide.

Bort- Alternative Modes of Administration
Moreau P, et al. Blood. 2010;116(21). Abstract 312.
IV BortezomibN = 73
SC BortezomibN = 145
P
ORR after 8 cycles CR > VGPR
52%12%25%
52%10%25%
NSNSNS
Median TTP 9.4 months 10.4 months 0.39
1-year OS 77% 73% NR
Any grade 3/4 AE 70% 57% NR
PN Any grade > grade 3
53%16%
38%6%
0.040.03
IV: intravenous; SC: subcutaneous; CR: complete response; VGPR: very good partial response; TTP: time to progression; OS: overall survival; AE: adverse event; PN: peripheral neuropathy.