Embed Size (px)
Citation preview

NAMI State Conference
November 16, 2013
Carole Specktor, M.P.A.1
Presentation Overview
• About ClearWay MinnesotaSM
• Why tobacco is still a problem• Why it is important to address tobacco
use?• Smoking and persons with mental
illness• QUITPLAN® Services
2
About ClearWay Minnesota
• Mission: Reduce the harm tobacco causes the people of Minnesota
• Grant-making, QUITPLAN stop-smoking services and statewide outreach activities
3
ClearWay Minnesota’s Work
• Policy Changes
• Research
• Reducing Disparities
• Cessation Services
4
Media Campaigns and Outreach
5
Why is Tobacco Still a Problem?
#1 Reason:
The Tobacco Industry
6

Tobacco Industry Adapts
7

Masterful Consumer Marketing
8

Targeted Marketing
• Tobacco industry has targeted populations to increase usage and loyalty
• Examples:– African Americans– American Indians– Latinos– Persons with mental
illness– LGBT community– Low-SES– Youth
E-Cigarettes
10
• Untested and unregulated• Not proven as safe
alternative to smoking• Not an approved
cessation aid• Often candy-flavored
• CDC study: use of e-cigarettes among middle- and high-school students more than doubled between 2011 and 2012
Quitting is Hard
11
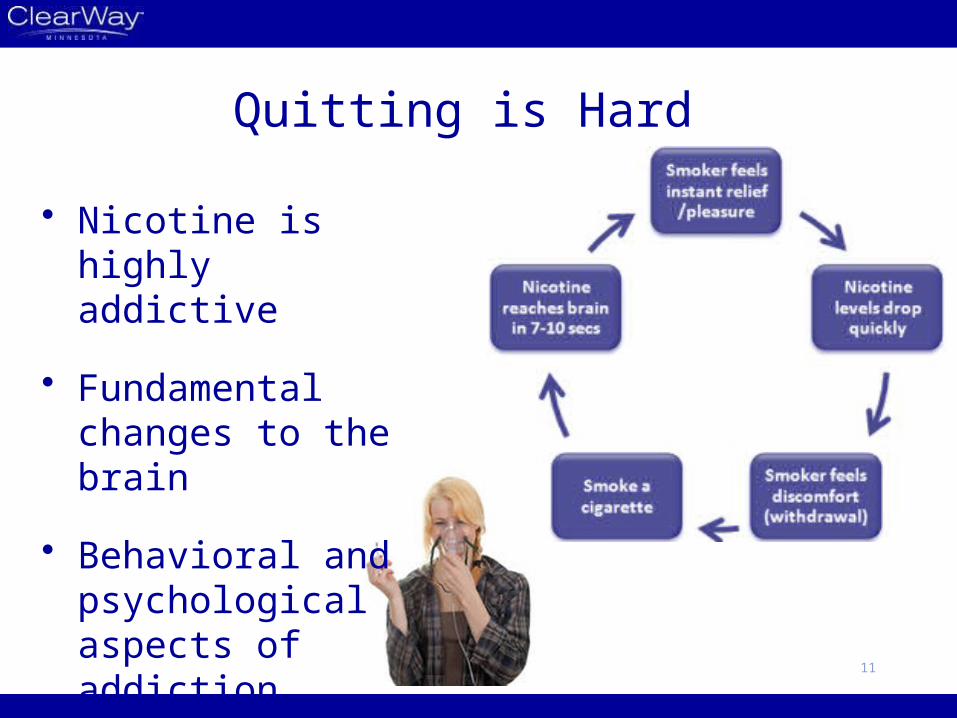
• Nicotine is highly addictive
• Fundamental changes to the brain
• Behavioral and psychological aspects of addiction
Why Address Tobacco?
12
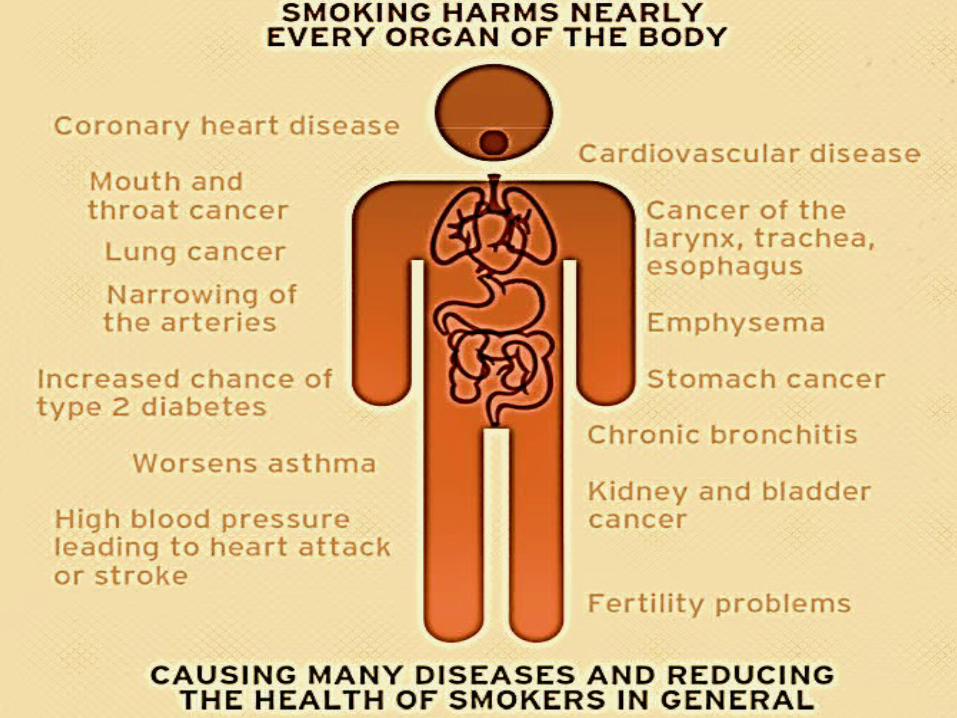
Tobacco is a Killer Problem
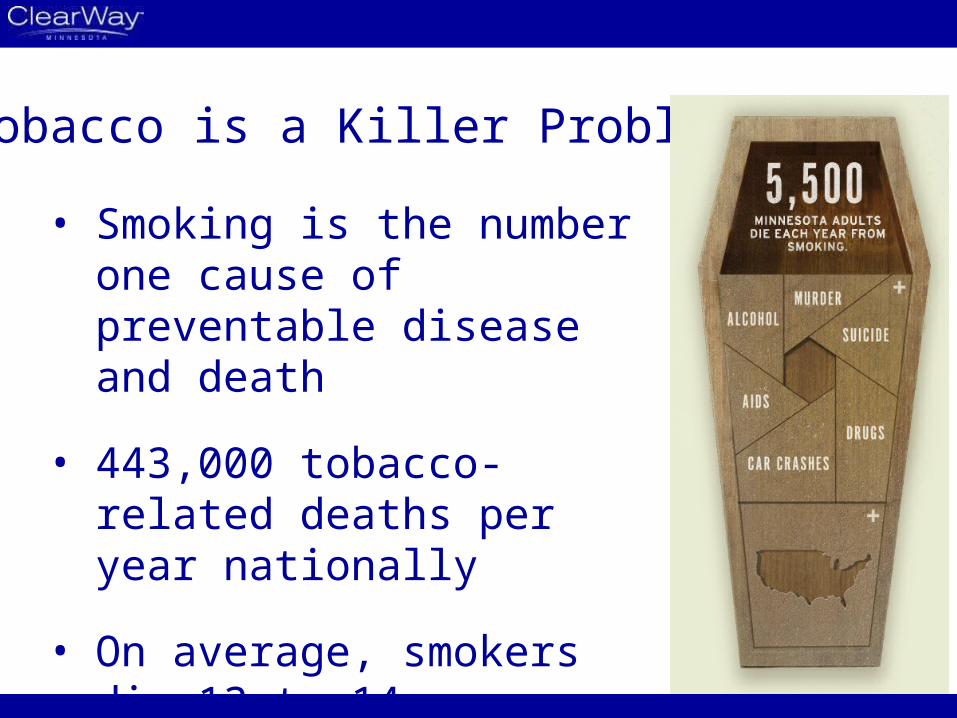
• Smoking is the number one cause of preventable disease and death
• 443,000 tobacco-related deaths per year nationally
• On average, smokers die 13 to 14 years earlier than nonsmokers
Smoking in Minnesota
• 625,000 Minnesota adults smoke (16%)
14
• Secondhand smoke exposure (2010):‒ Nearly 46% of adults exposed ‒ 282,000 Minnesota children exposed
• Majority of Minnesota smokers want to quitMinnesota Adult Tobacco Survey Tobacco Use in Minnesota: 1999-2010
4000 Chemicals in Cigarettes
Examples and where these chemicals are found:
– Acetone: nail polish remover – Acetic Acid: hair dye – Ammonia: household cleaner – Arsenic: rat poison – Butane: lighter fluid – Cadmium: battery acid – Carbon Monoxide: car exhaust– Nicotine: insecticide – Tar: pavement 15
16

Impact of Quitting
17
Smoking and Mental Illness
18
High Prevalence
• Higher prevalence imposes heavy morbidity and mortality burden
• Thirty-one percent of all cigarettes are smoked by adults with mental illness
19
• Why higher prevalence? − Targeted by tobacco industry− Biological, psychological and social factors− To date, not commonly addressed by providers
Vital Signs: Current Cigarette Smoking Among Adults Aged >18 Years with Mental Illness – United States, 2009-2011
Quitting and Persons with Mental Illness
• Can quit• Want to quit • Want information to help them quit• Some factors may make it harder to quit,
but . . . • Evidence shows cessation strategies work• Studies show that quitting smoking does
not worsen psychiatric symptoms20
Vital Signs: Current Cigarette Smoking Among Adults Aged >18 Years with Mental Illness – United States, 2009-2011; Tobacco Cessation for Persons with Mental Illness or Substance Use Disorders, Center for Tobacco Cessation
Understanding Higher Prevalence: Biological Factors
Persons with mental illness have unique neurobiological features that may:
– Increase tendency to use nicotine– Make it more difficult to quit; and– Complicate withdrawal symptoms
21Smoking Cessation for Persons with Mental Illnesses: A Toolkit for Mental Health Providers
Understanding Higher Prevalence: Psychological and Social Factors
• Psychological considerations:– Smoking relieves tension,
anxiety and stress– Daily routine
• Social considerations:– Smoke to relieve boredom– Smoke to feel part of a group
22Smoking Cessation for Persons with Mental Illnesses: A Toolkit for Mental Health Providers
Understanding Higher Prevalence: Myths and Barriers within Behavioral Health Care
Commonly stated reasons why mental health providers have not addressed smoking with clients:• They can’t or don’t want to quit• More pressing issues• Concerns about worsening symptoms• Lack of training • Don’t want to take away one of patients’ few pleasures• Shared smoke breaks build strong relationships
23
Triggering a Paradigm Shift in Treating Patients with Mental Health and Addictive Disorders, Wisconsin Nicotine Treatment Integration Project (presentation, July 28 2011); Vital Signs: Current Cigarette Smoking Among Adults Aged >18 Years with Mental Illness – United States, 2009-2011; Building the Case to support Tobacco Cessation, National Council for Behavior Health, June 28, 2013
Training • Recent study found psychiatrists:
– Address tobacco less frequently than other physicians
– Reported receiving no or inadequate training on tobacco-related interventions
• Survey of Wisconsin mental health providers: – The majority (72%) support adding nicotine
dependence treatment skills to credentials– With training, the majority (66%) are willing to
provide treatment
24Physician Behavior and Practice Patterns Related to Smoking Cessation, Association of American Medical Colleges ; Wisconsin Nicotine Treatment Integration Project
Strategies to Reduce Smoking for Persons with Mental Illness
• Reframe expectations of success
• Integrate tobacco as part of an approach to mental health treatment and overall wellness
25
• Provide mental health providers the training and tools they need to address tobacco with patients
• Utilize existing resources such as quitlines
26
QUITPLAN® Services
27

The Good News: Treatment Helps
• Evidence-based treatment can double or triple success
• Evidence-based treatment:– Counseling– FDA-approved medications– Both
• Best outcomes with both
28
QUITPLAN Helpline Basics
• Free Services• Serves:
– Uninsured– Underinsured, including Medicaid Fee-for-
Service– Live or work in Minnesota
• Phone Counseling in English and Spanish– Partner with Asian Smokers’ Quitline – Other languages through translation service
29
QUITPLAN Helpline Program
• Multi-call, one-on-one coaching program
• Integrated text messages• Print materials• Nicotine Replacement
Therapy • Two enrollments per year
30
QUITPLAN: Mental Health
• Training for coaches– Training for individualized services – Substantial mental health training– Ongoing
• Intake questions • Monitor field and adapt approach
as appropriate31

Nicotine Replacement Therapy
• Patches, gum or lozenge
• Uninsured and underinsured• Four weeks per enrollment*
(eight weeks per Medicaid enrollment)
• Medical screening
• Age 18 and older
• Live or work in Minnesota
32*twice every12-months
quitplan.com
• English and Spanish
• NRT not available through quitplan.com
• Available to all Minnesotans, regardless of insurance status
33
Materials• Order QUITPLAN Materials at:
www.clearwaymn.org (click “about”)– Brochures in English and Spanish– Smokeless tobacco brochure– Palm card
• Mailed to you free of charge• E-cigarette fact sheet available on
website
34

36
37