Embed Size (px)
Citation preview
This document is downloaded at: 2018-05-06T10:19:36Z
Title Dietary Zinc Supplementation to the Donor Improves Insulin SecretionAfter Islet Transplantation in Chemically Induced Diabetic Rats
Author(s)Mishima, Takehiro; Kuroki, Tamotsu; Tajima, Yoshitsugu; Adachi,Tomohiko; Hirabaru, Masataka; Tanaka, Takayuki; Kitasato, Amane;Takatsuki, Mitsuhisa; Eguchi, Susumu
Citation Pancreas, 43(2), pp.236-239; 2014
Issue Date 2014-03
URL http://hdl.handle.net/10069/34340
Right © 2014 by Lippincott Williams and Wilkins.; This is a non-final version ofan article published in final form in Pancreas, 43(2), pp.236-239; 2014
NAOSITE: Nagasaki University's Academic Output SITE
http://naosite.lb.nagasaki-u.ac.jp
Mishima T, et al.
Dietary zinc supplementation to the donor improves insulin secretion after 1
islet transplantation in chemically induced diabetic rats 2
3
Takehiro Mishima1, MD, PhD, Tamotsu Kuroki1, MD, PhD, Yoshitsugu 4
Tajima2, MD, PhD, Tomohiko Adachi1, MD, PhD, Masataka Hirabaru1, MD, 5
Takayuki Tanaka1, MD, Amane Kitasato1, MD, PhD, Mitsuhisa Takatsuki1, 6
MD, PhD, and Susumu Eguchi1, MD, PhD. 7
8
1Department of Surgery, Nagasaki University Graduate School of Biomedical 9
Sciences, Nagasaki, Japan. 10
2Department of Digestive and General Surgery, Shimane University, Shimane, 11
Japan. 12
13
Key words: type 1 diabetes, zinc, dietary supplementation, islet 14
transplantation, graft function 15
16
Running title: The effect of zinc on islet transplantation 17
18
1
Mishima T, et al.
1
2
To whom correspondence should be addressed: Takehiro Mishima, 3
Department of Surgery, Nagasaki University Graduate School of Biomedical 4
Sciences, 1-7-1 Sakamoto, Nagasaki 852-8102, Japan. 5
TEL 81-95819-7316 6
FAX 81-95819-7319 7
E-mail: [email protected] 8
9
All the authors have not received any funding for this work from any 10
organizations, and have no conflict of interest to declare. 11
12
2
Mishima T, et al.
1
Abstract 2
Objectives: Zinc (Zn) is related to insulin synthesis, storage and secretion. 3
This study demonstrates the effects of zinc supplementation in donor rats on 4
the outcomes of islet transplantation. 5
Methods: Donor rats received three different regimens of dietary zinc 6
supplementation for two weeks prior to undergoing pancreas donation: a 7
standard diet containing zinc at 50 ppm (control), 1 ppm (Low-Zn group) or 8
1,000 ppm (High-Zn group), respectively. Diabetic recipient rats underwent 9
islet transplantation, and the blood glucose levels and insulin secretion were 10
monitored for seven days after transplantation. 11
Results: The serum and pancreatic zinc levels at the time of donation were 12
significantly lower in the Low-Zn group (48.8±25.5 μg/dl and 11.3±1.9 μg/g) 13
and higher in the High-Zn group (147.3±17.6 μg/dl and 18.7±2.2 μg/g) when 14
compared with those observed in the controls (118.7±7.9 μg/dl and 14.6±2.0 15
μg/g) (p<0.05). The blood glucose levels became re-elevated two days after 16
transplantation in rats receiving islet grafts from the controls and the Low-Zn 17
groups. In contrast, in the rats that received islets from the High-Zn groups, 18
3
Mishima T, et al.
these were maintained within a normal range (p<0.01). 1
Conclusions: These data indicate that a zinc-rich diet for donor rats improves 2
the function of islet grafts in chemically induced diabetic rats. 3
4
4
Mishima T, et al.
Introduction 1
Type 1 diabetes is characterized by the profound destruction of the 2
insulin-producing β cells of the islets of the pancreas, thus requiring lifetime 3
endogenous insulin replenishment. Despite recent advances in diabetes care, 4
various life-threatening complications, including cardiovascular disease, 5
neuropathy and renal failure, can result in affected patients. 6
Pancreatic islet transplantation is now a promising treatment for type 1 7
diabetic patients. However, it still has some issues to overcome. For example, 8
an individual diabetic patient usually requires islets from multiple donors to 9
achieve normoglycemia. Xenotransplantation has thus been used to address 10
the insufficiency in the number of donors (1,2), and many studies have been 11
performed to refine the method for resolving the hypofunction of transplanted 12
grafts (3-11). 13
It is well known that a deficiency of zinc affects the onset and exacerbation of 14
diabetes (12) because zinc plays important roles in the synthesis, storage and 15
secretion of insulin, as well as β cell death leading to the occurrence of type 1 16
diabetes. Several studies have demonstrated that increasing the level of 17
dietary zinc can prevent the development of diabetes in animal models (13-15). 18
5
Mishima T, et al.
Our previous study indicated that a zinc-rich environment is advantageous for 1
the recipient in intraportal islet transplantation (16). Meanwhile, the effects 2
of zinc supplementation on the donor in regard to the graft function following 3
pancreatic islet transplantation have not yet been elucidated. 4
This study was designed to investigate whether dietary zinc supplementation 5
to the donor can improve the results of islet transplantation in chemically 6
induced diabetic rats. 7
8
6
Mishima T, et al.
1
Materials and Methods 2
Animals 3
Male Wistar rats (SLC, Shizuoka, Japan) weighing 250-300 g were used in 4
this study. They were housed one per plastic cage on sawdust bedding and 5
kept at 24±2℃ and 50±20% humidity with a 12-hour light-dark cycle. The 6
rats were fed a CE-2 pelleted diet (Clea Japan, Tokyo, Japan) and provided 7
drinking water ad libitum. The animals were checked daily throughout the 8
experiments. All experiments were conducted according to the Guidelines for 9
Animal Experimentation of Nagasaki University. 10
Zinc supplementation 11
The donor rats were divided into three groups according to the regimen of 12
dietary zinc supplementation, i.e., a standard pelleted diet containing zinc at 13
50 ppm (control group, n=10), a zinc-poor diet containing zinc at 1 ppm 14
(Low-Zn group, n=10) or zinc-rich diet containing zinc at 1,000 ppm (High-Zn 15
group, n=10). The animals received the dietary zinc supplementation for two 16
weeks prior to extirpation of the pancreas. 17
At the time of pancreas donation, blood samples were collected from inferior 18
vena cava for the measurement of the serum zinc levels and serum insulin 19
7
Mishima T, et al.
values, and pancreatic tissue samples were taken from splenic lobe for the 1
measurement of the pancreatic zinc levels. Pancreatic homogenate was 2
digested in 2N hydrochloric acid for 24 hours at room temperature. The 3
samples were then centrifuged at 7,000 g for 25 minutes, and the supernatant 4
was then used for direct measurements. Serum and pancreatic zinc levels 5
were measured by Atomic Absorption Spectrometry. 6
Isolation of pancreatic islets 7
Pancreatic islets were isolated using a modified method of ductal collagenase 8
distention (17) and iodixanol isolation (17,18). Briefly, laparotomy was 9
performed under general anesthesia, and the distal end of the common bile 10
duct was ligated at the entrance of the duodenum with a fine nylon suture. 11
The proximal common bile duct was cannulated with a 24-gauge polyethylene 12
catheter and injected with 10 ml of Hank’s balanced salt solution (HBSS) 13
containing 1,200 U/ml collagenase type XI (Sigma Chemical Co., St Louis, 14
MO) to distend the pancreas. The distended pancreas was removed and 15
incubated in a 50-ml conical tube with an additional 5 ml of collagenase 16
solution and then placed in a water bath at 37℃ for 20 minutes. The digestion 17
was stopped by the addition of 40 ml of cold HBSS. The pancreatic tissue was 18
8
Mishima T, et al.
filtered over 400-μm mesh and then washed twice. Islet purification was 1
performed using a continuous iodixanol (Optiprep (Axis-Shield PoC, Oslo, 2
Norway)) density gradient. The tissue pellets were resuspended in 10 ml of 3
1.095 g/ml density iodixanol solution. To form a continuous density gradient, 6 4
ml of 1.087 g/ml density iodixanol solution and 4 ml of Roswell Park Memorial 5
Institute (RPMI) medium were softly added above the tissue layer. Following 6
centrifugation, isolated islets were harvested from the interface between the 7
topmost layers with a pipette. The isolated islets were stained with dithizone 8
(140 mmol/L) and counted. The number of islets was determined using an 9
optical graticule attached to the eyepiece of a dissecting microscope and then 10
was converted to the standard islet equivalent. 11
Recipient rats 12
Diabetes was induced in the recipient rats via the intravenous injection of 13
streptozotocin (STZ). Two or three days before islet transplantation, STZ (60 14
mg/kg) was injected into the superficial dorsal vein of the penis of the 15
recipient rats. After 48 hours, the non-fasting blood glucose levels were 16
measured. Diabetes in rats was defined when the glucose level was greater 17
than 350 mg/dl with severe polyuria, and diabetic rats were prepared for islet 18
9
Mishima T, et al.
transplantation. 1
Under general anesthesia, islet transplantation was randomly performed 2
from a single donor to a single recipient with the injection of the harvested 3
islets into the portal vein in which the islets were collected in 0.1 ml of RPMI 4
medium. The amount of transplanted islets was 10 islet equivalents per one 5
gram of body weight of the recipient rat. 6
Assessment of the islet graft function 7
The non-fasting blood glucose levels of the recipient rats were measured daily 8
to monitor the function of the islet grafts for seven days after transplantation. 9
The recipient rats were then sacrificed, and the serum insulin values and the 10
serum zinc levels were measured. 11
Statistics 12
Unpaired Student’s t-test was used for the statistical analyses of the 13
differences in the serum and pancreatic zinc levels, the blood glucose levels 14
and the serum insulin levels among the groups. A P value of less than 0.05 15
was regarded as being statistically significant. 16
17
10
Mishima T, et al.
1
Results 2
Serum and pancreatic zinc levels, and serum insulin values of the donor rats 3
The zinc levels in the serum and pancreatic tissues of the donor rats were 4
significantly different among the three groups (Table 1). The serum and 5
pancreatic zinc levels of the donor rats in the Low-Zn group were significantly 6
lower than those observed in the controls (p<0.05). Conversely, the serum and 7
pancreatic zinc levels in the High-Zn group were significantly higher than 8
those observed in the controls (p<0.05). In addition, significantly lower serum 9
insulin values were observed in the Low-Zn group (p<0.05) and higher serum 10
insulin value were observed in the High-Zn group (p<0.05) compared to those 11
observed in the control group. 12
Islet graft function 13
The blood glucose levels of the recipient rats measured before and after islet 14
transplantation are shown in Figure 1. Elevated blood glucose levels greater 15
than 350 mg/dl in the recipient rats following the STZ treatment decreased to 16
less than 150 mg/dl immediately after islet transplantation. However, the 17
blood glucose levels re-elevated two days after islet transplantation in the rats 18
that received islet grafts from the controls or the Low-Zn diet donors. 19
11
Mishima T, et al.
Especially in the rats receiving islets from Low-Zn diet donor rats, the blood 1
glucose levels were extremely high, ranging from 350 to 400 mg/dl. In contrast, 2
in the rats receiving islets from High-Zn diet donors, the blood glucose levels 3
were well maintained within a normal range between 150 and 200 mg/dl 4
throughout the experiment. The blood glucose levels of the rats receiving 5
islets from High-Zn donors were maintained at significantly low levels seven 6
days after islet transplantation compared to those observed in the rats 7
receiving islets from Low-Zn donors (p<0.01). 8
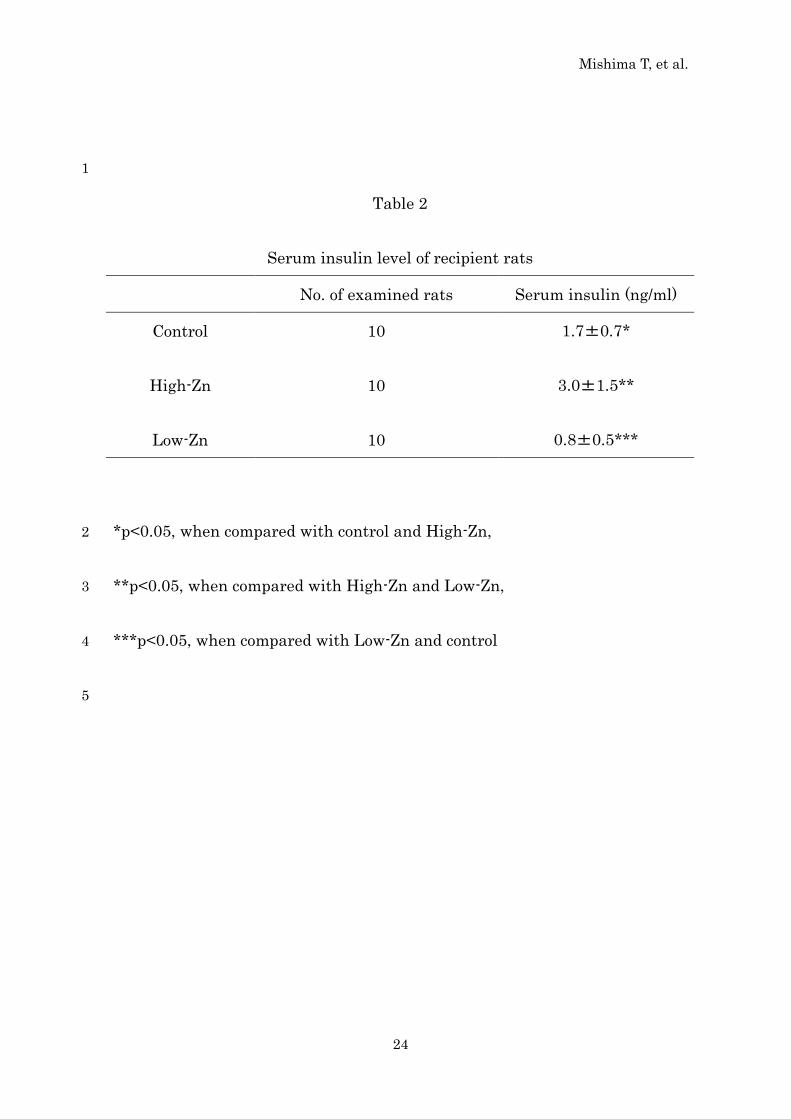
The serum insulin levels in the recipient rats seven days after islet 9
transplantation are shown in Table 2. The rats that received islets from 10
High-Zn diet donors demonstrated significantly high levels of serum insulin 11
(3.0±1.5 ng/ml) in contrast to those observed in the rats receiving islet 12
transplantation from the controls (1.7±0.7 ng/ml) or low-Zn diet donors 13
(0.8±0.5 ng/ml) (p<0.05). Meanwhile, the serum zinc levels of recipients at the 14
time were approximately 90 μg/g and were not significantly different among 15
three groups. 16
17
18
12
Mishima T, et al.
Discussion 1
Zinc is known to be important for numerous functions in the pancreas, 2
including insulin synthesis, secretion and signaling, glucagon secretion and 3
pancreatic digestive enzyme secretion and activity (19). It has been reported 4
that islets are the most zinc-rich cells in the body (20). Most intracellular zinc 5
is stored with insulin in the insulin secretory vesicles in pancreatic β-cells as a 6
zinc-insulin complex. The concentration of zinc in these vesicles is quite high 7
at approximately 20 mM (21). Zinc is released together with insulin into the 8
extracellular islet space when insulin is secreted. In addition, zinc is taken up 9
by neighboring cells (22). Zinc forms hexameric crystals with insulin, each of 10
which contains two zinc ions within β-cell insulin granules (23). Zinc-deficient 11
rats are known to exhibit lower insulin secretin and glucose uptake than 12
normal rats (24). It has also been reported that nutritional zinc 13
supplementation improves both fasting insulinemia and glycemia in rodents 14
(15). The mechanism of action of zinc remains unclear, i.e. whether it acts 15
directly on insulin receptors and glucose transporters or indirectly via 16
intracellular pathways of insulin (15). 17
This study demonstrated the effects of zinc on rat islet transplantation using 18
13
Mishima T, et al.
dietary zinc supplementation to donor rats for two weeks prior to donation. 1
The serum and pancreatic zinc levels and the serum insulin levels of the donor 2
rats were increased according to the degree of zinc supplementation. 3
Furthermore, the results of the islet function of islet transplantation were also 4
improved. The blood glucose levels were lower in the High-Zn group than 5
those observed in the control and Low-Zn groups, and the serum insulin levels 6
were also higher in the High-Zn group than those observed in the control and 7
Low-Zn groups. 8
It is also known that islet β cells are vulnerable to oxidative stress (13). It is 9
suspected that excess free radical production may contribute to the death of β 10
cells and lead to the onset of type 1 diabetes (25-28). Pancreatic islets also lack 11
antioxidant protection (29,30), rendering them especially susceptible to 12
damage by free radicals produced during inflammatory and immune processes. 13
In addition, instant blood mediated inflammatory reaction (IBMIR) is a major 14
factor contributing to poor initial engraftment of islets in clinical islet 15
transplantation (3). This reaction is expressed by transplanted pancreatic 16
islets when the islets come in contact with blood in the portal vein (3). IBMIR 17
involves the activation of coagulation and complement systems, which in turn 18
14
Mishima T, et al.
leads to local ischemia, injury of the endothelium and the upregulation of 1
pro-inflammatory mediators such as ICAM-1 (Intercellular Adhesion 2
Molecule-1) and MCP-1 (Monocyte Chemoattractant Protein-1) (31,32). The 3
mechanisms underlying the effects of zinc supplementation remain unclear, 4
although zinc may be involved in scavenging of free radicals (33,34) or 5
prevention of apoptosis (35,36). Zinc is an essential trace element possessing a 6
wide range of functions and antioxidant properties (37). IBMIR is initiated 7
upon intraportal infusion of islets (38). The present study indicated that the 8
blood glucose levels re-elevate two days after islet transplantation. These 9
findings suggest that IBMIR is a barrier to engraftment in our models of 10
intraportal islet transplantation. Therefore, zinc supplementation is thought 11
to have the potential to improve the results of clinical islet transplantation by 12
reinforcing the islet function and preventing graft loss through IBMIR. 13
The High-Zn diet donors ate more and grew more compared with the controls. 14
However, food consumption and transitions in body weight did not differ 15
significantly among the groups (data not shown). We thus did not think that 16
any side effects of the High-Zn diet were apparent throughout the experiment. 17
Zinc is considered to be relatively non-toxic to humans (39). 18
15
Mishima T, et al.
Xenotransplantation has been utilized to resolve donor insufficiency in clinical 1
islet transplantation (1,2). In the setting of xenotransplantation, zinc 2
supplementation may be useful for improving the patient outcomes. In 3
addition, in clinical islet transplantation (allotransplantation), the serum zinc 4
level is a potential indicator of the donor islet function. These data therefore 5
suggest the potential beneficial effects of zinc supplementation in donors for 6
islet transplantation and the applicability of zinc in clinical islet 7
transplantation. Further studies are needed to prove the effects of zinc 8
supplementation on islet transplantation, especially over a much longer 9
period and with respect to aspects of both histology and molecular biology. 10
11
12
16
Mishima T, et al.
1
References 2
1. Goto M, Tjernberg J, Dufrane D, et al. Dissecting the instant 3
blood-mediated inflammatory reaction in islet xenotransplantation. 4
Xenotransplantation. 2008; 15:225-34. 5
2. Cozzi E, Bosio E. Islet xenotransplantation: current status of preclinical 6
studies in the pig-to-nonhuman primate model. Curr Opin Organ 7
Transplant. 2008; 13:155-8. 8
3. Cabric S, Sanchez J, Lundgrenm T, et al. Islet surface heparinization 9
prevents the instant blood-mediated inflammatory reaction in islet 10
transplantation. Diabetes. 2007; 56:2008–2015. 11
4. Ryan EA, Lakey JR, Rajotte RV, et al. Clinical outcomes and insulin 12
secretion after islet transplantation with the Edmonton protocol. Diabetes. 13
2001; 50:710 –719. 14
5. Shapiro AM, Lakey JR, Ryan EA, et al. Islet transplantation in seven 15
patients with type 1 diabetes mellitus using a glucocorticoid-free 16
immunosuppressive regimen. N Engl J Med. 2000; 343:230 –238. 17
6. Johansson H, Lukinius A, Moberg L, et al. Tissue factor produced by the 18
endocrine cells of the islets of Langerhans is associated with a negative 19
outcome of clinical islet transplantation. Diabetes. 2005; 54:1755–1762. 20
7. Moberg L, Johansson H, Lukinius A, et al. Production of tissue factor by 21
pancreatic islet cells as a trigger of detrimental thrombotic reactions in 22
clinical islet transplantation. Lancet. 2002; 360:2039 –2045. 23
17
Mishima T, et al.
8. Moberg L, Korsgren O, Nilsson B. Neutrophilic granulocytes are the 1
predominant cell type infiltrating pancreatic islets in contact with ABO 2
compatible blood. Clin Exp Immunol. 2005; 142:125–131. 3
9. Piemonti L, Leone BE, Nano R, et al. Human pancreatic islets produce 4
and secrete MCP-1/CCL2: relevance in human islet transplantation. 5
Diabetes. 2002; 51:55– 65. 6
10. Johansson U, Olsson A, Gabrielsson S, et al. Inflammatory mediators 7
expressed in human islets of Langerhans: implications for islet 8
transplantation. Biochem Biophys Res Commun. 2003; 308:474–479. 9
11. Titus TT, Horton PJ, Badet L, et al. Adverse outcome of human 10
islet-allogeneic blood interaction. Transplantation. 2003; 75:1317–1322. 11
12. B. Chausmer, Zinc, Insulin, and Diabetes. J Am Col Nutrit. 1998; 17: 12
109-115. 13
13. Emily Ho, Ning Quan, Yu-Hwai Tsai, et al. Dietary zinc supplementation 14
inhibits NFκB activation and protects against chemically induced diabetes 15
in CD1 mice. Exp Biol Med. 2001; 226:103-111. 16
14. Liu J, Bao W, Jiang M, et al. Chromium, Selenium, and Zinc multimineral 17
enriched yeast supplementation ameliorates diabetes symptom in 18
streptozocin-induced mice. Biol Trace Elem Res. 2012; 146:236-245. 19
15. Chen MD, Liou SJ, Lin PY, et al. Effects of zinc supplementation on the 20
plasma glucose level and insulin activity in genetically obese (ob/ob) mice. 21
Biol Trace Elem Res. 1998; 61:303-11. 22
18
Mishima T, et al.
16. Okamoto T, Kuroki T, Kanematsu T, et al. Effect of zinc on early graft 1
failure following intraportal islet transplantation in rat recipients. Ann 2
Transpl. 2011; 16:114-120. 3
17. Yamasaki T, Onodera H, Takahashi R, et al. Islet films cures diabetes. J 4
Artif Organs. 2004; 7:37-40 5
18. van der Burg M.P.M, Basir I, and Bouwman E. No Porcine Islet Loss 6
During Density Gradient Purification in a Novel Iodixanol in University of 7
Wisconsin Solution. Transplantation Proceedings. 1998; 30, 362–363. 8
19. Bosco MD, Mohanasundaram DM, Drogemuller CJ, et al. Zinc and zinc 9
transporter regulation in pancreatic islets and the potential role of zinc in 10
islet transplantation. Rev Diabet Stud. 2010; 7:263-74. 11
20. Lemaire K, Ravier MA, Schraenen A, et al. Insulin crystallization 12
depends on zinc transporter ZnT8 expression, but is not required for 13
normal glucose homeostasis in mice. Proc Natl Acad Sci USA. 2009; 14
1;106:14872-7. 15
21. Chimienti F, Devergnas S, Favier A, et al. Identification and cloning of a 16
beta-cell-specific zinc transporter, ZnT-8, localized into insulin secretory 17
granules. Diabetes. 2004; 53:2330-7. 18
22. Gyulkhandanyan AV, Lu H, Lee SC, et al. Investigation of transport 19
mechanisms and regulation of intracellular Zn2+ in pancreatic alpha-cells. 20
J Biol Chem. 2008; 11;283:10184-97. 21
23. Dunn MF. Zinc-ligand interactions modulate assembly and stability of 22
the insulin hexamer - a review. Biometals. 2005; 18:295-303. 23
19
Mishima T, et al.
24. Faure P, Roussel AM, Martinie M, et al. Insulin sensitivity in 1
zinc-depleted rats: assessment with the euglycaemic hyperinsulinic clamp 2
technique. Diabete Metab. 1991; 17:325-31. 3
25. Oberley LW. Free radicals and diabetes. Free Radical Biol Med. 1988; 4
5:113–124. 5
26. Rabinovitch A, Suarez-Pinzon WL, Strynadka K, et al. Human pancreatic 6
islet beta-cell destruction by cytokines involves oxygen free radicals and 7
aldehyde production. J Clin Endocrinol Metab. 1996; 81:3197–3202. 8
27. Rabinovitch A. Free radicals as mediators of pancreatic islet β cell injury 9
in autoimmune diabetes [editorial; comment]. J Lab Clin Med. 1992; 10
119:455–456. 11
28. Corbett JA, McDaniel ML. Does nitric oxide mediate autoimmune 12
destruction of β cells? Possible therapeutic interventions in IDDM. 13
Diabetes. 1992; 41:897–903. 14
29. Lenzen S, Drinkgern J, Tiedge M. Low antioxidant enzyme gene 15
expression in pancreatic islets compared with various other mouse tissues. 16
Free Radical Biol Med. 1996; 20:463–466. 17
30. Tiedge M, Lortz S, Drinkgern J, et al. Relation between antioxidant 18
enzyme gene expression and antioxidative defense status of 19
insulin-producing cells. Diabetes. 1997; 46:1733–1742. 20
31. Cantaluppi V, Biancone L, Romanazzi GM, et al. Antiangiogenic and 21
immunomodulatory effects of rapamycin on islet endothelium: relevance 22
for islet transplantation. Am J Transplant. 2006; 6:2601-11. 23
20
Mishima T, et al.
32. Schröppel B, Zhang N, Chen P, et al. Role of donor-derived monocyte 1
chemoattractant protein-1 in murine islet transplantation. J Am Soc 2
Nephrol. 2005;16:444-51. 3
33. Zago MP, Oteiza PI. The antioxidant properties of zinc: interactions with 4
iron and antioxidants. Free Radic Biol Med. 2001; 15;31:266-74. 5
34. Bolkent S, Yanardag R, Bolkent S, et al. The influence of zinc 6
supplementation on the pancreas of streptozotocin-diabetic rats. Dig Dis 7
Sci. 2009; 54:2583-7. 8
35. Zhou Z, Liu J, Song Z, et al. Zinc supplementation inhibits hepatic 9
apoptosis in mice subjected to a long-term ethanol exposure. Exp Biol Med 10
(Maywood). 2008; 233:540-8. 11
36. Chai F, Truong-Tran AQ, Ho LH, et al. Regulation of caspase activation 12
and apoptosis by cellular zinc fluxes and zinc deprivation: A review. 13
Immunol Cell Biol. 1999; 77:272-8. 14
37. Powell SR. The antioxidant properties of zinc. J Nutr. 2000; 130(5S 15
Suppl):1447S-54S. 16
38. Fosmire GJ. Zinc toxicity. Am J Clin Nutr. 1990; 51:225-7. 17
18
21
Mishima T, et al.
1
Figure legends 2
Figure 1. The blood glucose levels of the recipient rats after islet 3
transplantation were consistently high in the Low-Zn group compared with 4
those observed in the control group and were consistently low in the High-Zn 5
group. The levels observed in the High-Zn group were significantly low 6
compared to those observed in the Low-Zn group and were maintained within 7
a normal range throughout the observation. 8
9
22
Mishima T, et al.
1
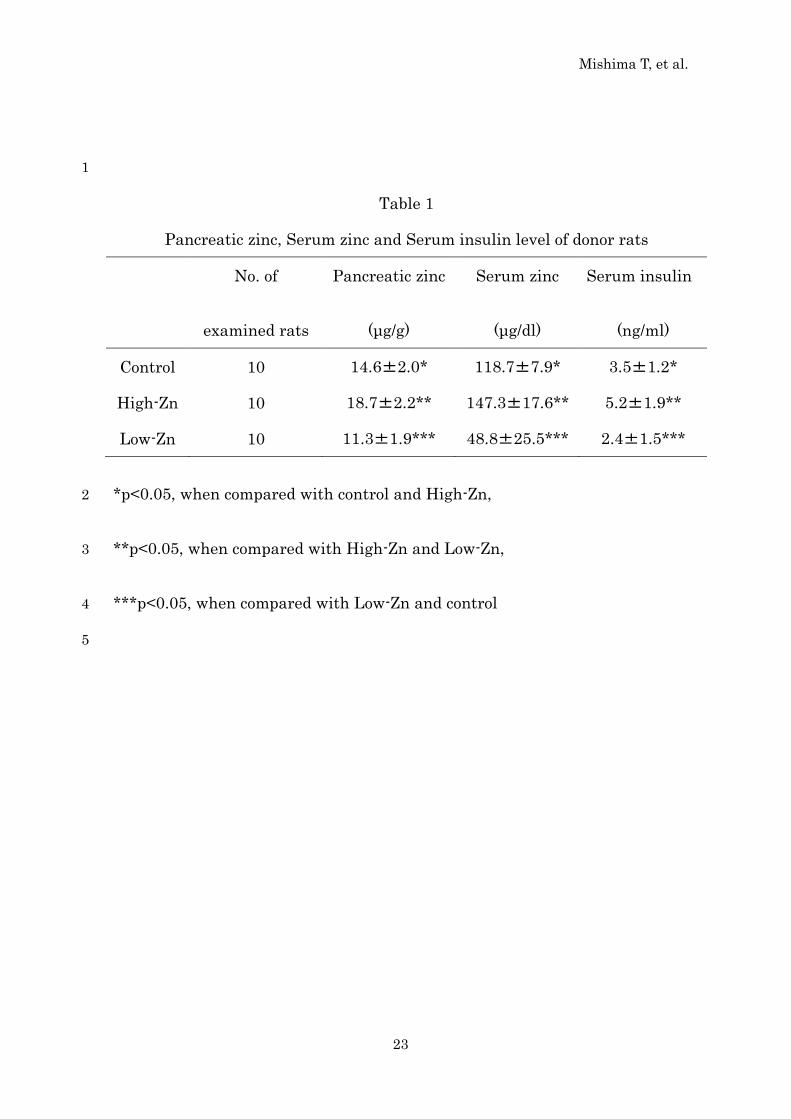
Table 1
Pancreatic zinc, Serum zinc and Serum insulin level of donor rats
No. of
examined rats
Pancreatic zinc
(μg/g)
Serum zinc
(μg/dl)
Serum insulin
(ng/ml)
Control 10 14.6±2.0* 118.7±7.9* 3.5±1.2*
High-Zn 10 18.7±2.2** 147.3±17.6** 5.2±1.9**
Low-Zn 10 11.3±1.9*** 48.8±25.5*** 2.4±1.5***
*p<0.05, when compared with control and High-Zn, 2
**p<0.05, when compared with High-Zn and Low-Zn, 3
***p<0.05, when compared with Low-Zn and control 4
5
23
Mishima T, et al.
1
Table 2
Serum insulin level of recipient rats
No. of examined rats Serum insulin (ng/ml)
Control
High-Zn
Low-Zn
10
10
10
1.7±0.7*
3.0±1.5**
0.8±0.5***
*p<0.05, when compared with control and High-Zn, 2
**p<0.05, when compared with High-Zn and Low-Zn, 3
***p<0.05, when compared with Low-Zn and control 4
5
24
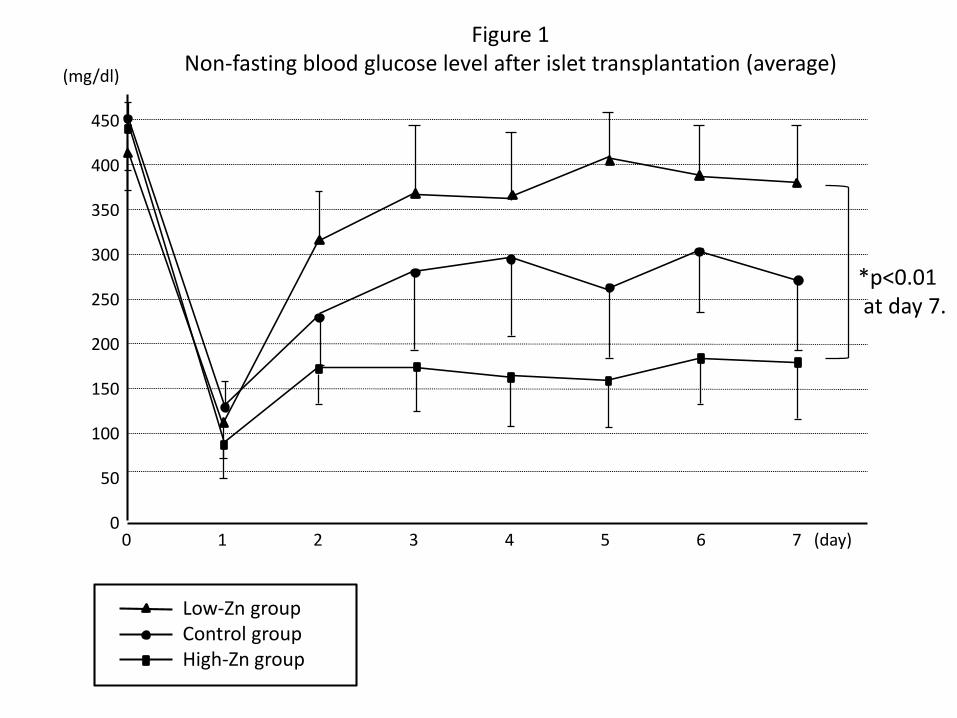
Figure 1Non-fasting blood glucose level after islet transplantation (average)(mg/dl)
450
400
350
300
250
200
150
100
50
00 1 2 3 4 5 6 7 (day)
Low-Zn groupControl groupHigh-Zn group
*p<0.01at day 7.





























![[OS 202C] 20120102 Pancreatic Islet Physiology (Insulin)](https://img.pdfslide.net/doc/110x75/577cd5451a28ab9e789a55e6/os-202c-20120102-pancreatic-islet-physiology-insulin.jpg)