Embed Size (px)
Citation preview
1
National Audit of Small Bowel Obstruction
(NASBO)
Protocol V10 Date 02/08/2016 MJL
Email: [email protected]
Twitter: @nasbo2017
Steering group South Yorkshire Surgical Research Group Matthew Lee, Adele Sayers, Tom Drake, Jonathan Wild, Tim Wilson West Midlands Research Collaborative Paul Marriott, Pritam Singh, Marianne Hollyman Association of Coloproctology of Great Britain and Ireland: Austin Acheson, Iain Anderson, Simon Bach, Michael Davies, Malcolm McFall, Nicola Fearnhead, John Hartley, Hugh Paterson, Ciaran Walsh

2
Please see www.nasbo.org.uk for most up-to date documentation.
Lay Summary
Bowel obstruction is a common problem. People with a blockage in their bowel have symptoms
including vomiting, abdominal bloating and inability to open their bowels. For the time that they
have this problem, they are unable to eat or drink and require a drip to support them. Patients
are sometimes treated by putting a tube through the nose into the stomach to drain fluid and
sometimes with an operation. This national audit will look at how we assess nutrition in these
patients to see if we can improve this.
Background:
Bowel obstruction is a common condition presenting to the emergency surgery take. Symptoms
include abdominal pain, distension, vomiting and obstipation. This interruption of bowel function
causes a state of starvation that may be prolonged for treatment considerations. Blockage can
occur in either the small bowel or large bowel.
3
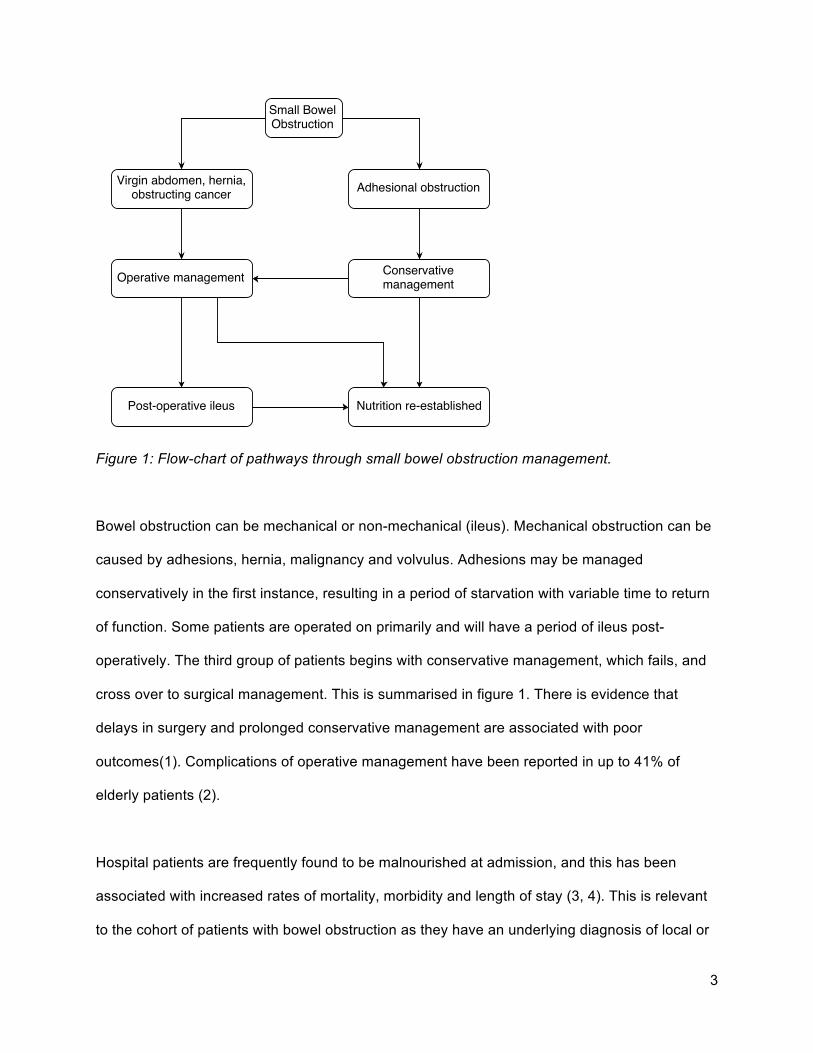
Figure 1: Flow-chart of pathways through small bowel obstruction management.
Bowel obstruction can be mechanical or non-mechanical (ileus). Mechanical obstruction can be
caused by adhesions, hernia, malignancy and volvulus. Adhesions may be managed
conservatively in the first instance, resulting in a period of starvation with variable time to return
of function. Some patients are operated on primarily and will have a period of ileus post-
operatively. The third group of patients begins with conservative management, which fails, and
cross over to surgical management. This is summarised in figure 1. There is evidence that
delays in surgery and prolonged conservative management are associated with poor
outcomes(1). Complications of operative management have been reported in up to 41% of
elderly patients (2).
Hospital patients are frequently found to be malnourished at admission, and this has been
associated with increased rates of mortality, morbidity and length of stay (3, 4). This is relevant
to the cohort of patients with bowel obstruction as they have an underlying diagnosis of local or
4
disseminated malignancy causing a chronic malnourished state. They then undergo a further
insult with the addition of acute gastrointestinal dysfunction.
Recommendations for the management of malnutrition in patients have been set out in NICE
clinical guideline 32 (CG32) and the British Association for Parenteral and Enteral Nutrition
(BAPEN) document ‘Perioperative Nutrition’ (5, 6). Patients with bowel obstruction may not be
managed in line with these recommendations.
Aim:
To assess outcomes and impact of guidelines for malnourished patients in small bowel
obstruction
Objectives
1. To audit use of malnutrition tools in patients with bowel obstruction
2. To audit outcomes in patients with small bowel obstruction and feed-back findings at unit
level.
3. To audit whether patients at a high risk of malnutrition receive appropriate management
in line with national guidelines.
5
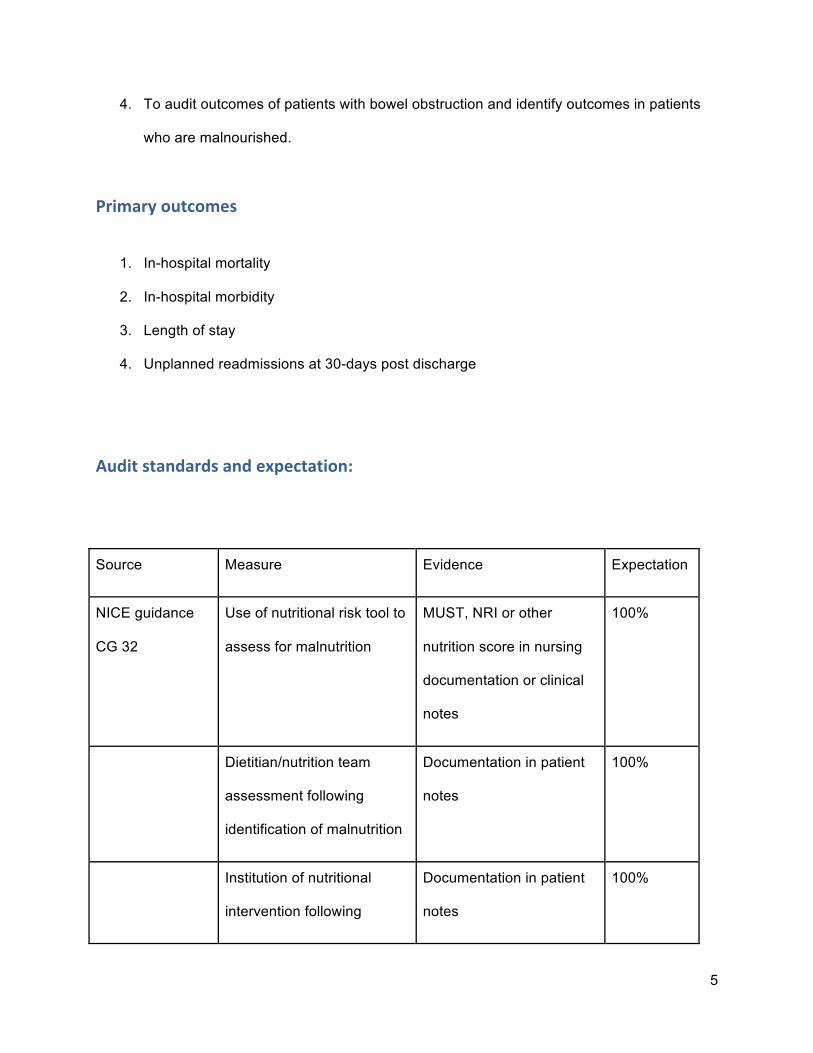
4. To audit outcomes of patients with bowel obstruction and identify outcomes in patients
who are malnourished.
Primary outcomes
1. In-hospital mortality
2. In-hospital morbidity
3. Length of stay
4. Unplanned readmissions at 30-days post discharge
Audit standards and expectation:
Source Measure Evidence Expectation
NICE guidance
CG 32
Use of nutritional risk tool to
assess for malnutrition
MUST, NRI or other
nutrition score in nursing
documentation or clinical
notes
100%
Dietitian/nutrition team
assessment following
identification of malnutrition
Documentation in patient
notes
100%
Institution of nutritional
intervention following
Documentation in patient
notes
100%
6
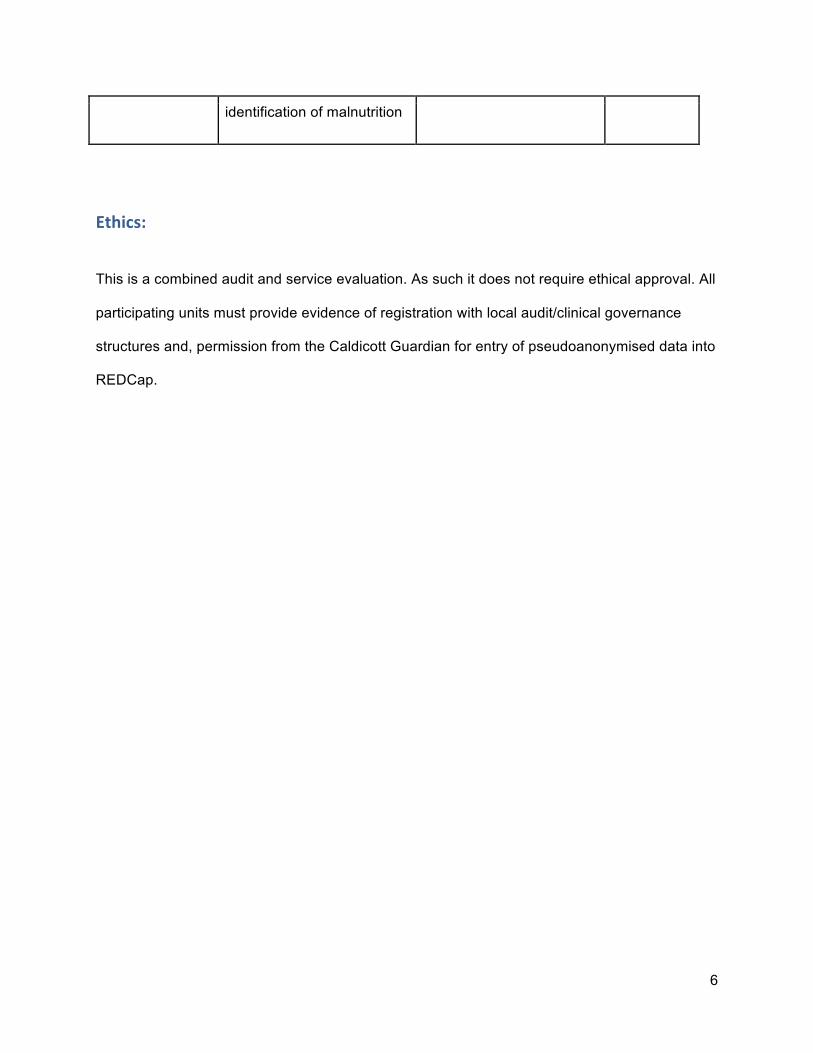
identification of malnutrition
Ethics:
This is a combined audit and service evaluation. As such it does not require ethical approval. All
participating units must provide evidence of registration with local audit/clinical governance
structures and, permission from the Caldicott Guardian for entry of pseudoanonymised data into
REDCap.
7
Method: Prior to undertaking the prospective assessment of practice, it is important to describe the
settings and processes that underpin the care of patients with SBO.
Establishing Practice As there are no formal guidelines for the management of SBO in the UK, there is likely to be
variation in the pathway of care for these patients. A questionnaire has been designed to assess
areas of perceived variation in care, including use of gastrograffin, timing of and indicators for
surgery, and surgical approaches.
This will be undertaken as a pilot during June 2016, and a full roll-out undertaken with
collaborative groups across the UK between July and August 2016. The questionnaire is
presented in Appendix A.
Profile of Centre In order to describe local processes and resources, each site will be asked to complete a site
profile questionnaire (Appendix B) when they register. This assesses availability of imaging,
theatres, emergency rota set-up, care for increased dependency patients and access to
nutritional support services.
8
Identification of patients
Patients referred to emergency surgical take with a working diagnosis made by the admitting
surgical team of small bowel obstruction will be screened for inclusion at the point of clinical
handover (typically 0800).
For the purpose of this study, small bowel obstruction will be defined as a clinical diagnosis of
small bowel obstruction as determined by specialist trainee (ST3+) or consultant surgeon during
that admission.
Inclusion and exclusion criteria
Inclusion criteria:
● Patients who are admitted direct to the emergency surgery service (via A&E or GP)
OR
● Patients who are referred to the emergency surgical team from another inpatient team
(e.g. medicine)
AND
● With a diagnosis of small bowel obstruction by ST3 or above
Exclusion criteria:
● Patients who have had abdominal surgery within the same hospital admission prior to
first symptoms of small bowel obstruction
● Pregnant women
● <16 years old
9
● Patients with large bowel obstruction (even when signs of small bowel obstruction are
present)
● Patients with total length of stay <24 hours
Patients who are initially included but later excluded should be recorded on the REDCap
system, with reason for exclusion documented.
Data collection period
Prospective patient identification will be undertaken over a two-month period.
Snapshot data will be collected at days 1, 3, 5 and 7 of hospital stay.
Identification of outcomes of management whilst an inpatient will be recorded
Patient disposition at 30-days post admission will be recorded.
For patients discharged within 30-days of admission, 30-day readmissions post-discharge will
be identified.
Data collection procedure
At registration, the Centre lead will complete a site profile form and return this to the steering
committee, along with audit and Caldicott approvals. This form is presented in Appendix B.
Data collection will be using the form presented in Appendix C. Hospital or NHS number will not
be entered onto this form, but will be kept separately with a key sheet. Data should be collected
prospectively for maximum accuracy. As there is variation in use of nutritional assessment tools
across hospitals, the tool asks only if the patient is defined as malnourished by the local
definition.
10
Patients will be screened for inclusion, and data collected where appropriate. Basic
demographics and comorbidities (in the form of Charlson Comorbidity Index) will be recorded.
This allows standardisation of comparisons between any groups. Documentation will be
assessed for time period since they last tolerated food, as well as recording of local malnutrition
scoring tool and any resulting actions. Data on aetiology will be recorded as will initial
management strategy (i.e. first 24 hours). This is split into operative e.g. early operation for
congenital band in virgin abdomen, conservative management, or e.g. trial of nasogastric tube
and catheter. Treatment intent is also captured. This includes curative i.e. treatment intended to
resolve obstruction such as adhesiolysis, temporising i.e. procedure offering temporary relief
prior to definitive procedure e.g. stoma, or palliative management which may be conservative
only. Timing and nature of any intervention will be recorded.
Recognition and intervention in malnutrition will be assessed. Interventions have been simplified
to oral supplements, enteral feeding and parenteral feeding.
At 30-days following discharge, hospital systems should be interrogated for evidence of
unplanned readmission.
Completed datasheets will be entered onto the secure REDcap system, hosted by the
University of Sheffield (https://redfox.shef.ac.uk/). Access to data-entry will be via issued
accounts. The REDcap data form matches the pro forma, but has an additional field capturing
the collaborator ID number to allow attribution.
11
Case Ascertainment
Case ascertainment will be estimated using local screening and recruitment data, with reference
to national numbers.
National Emergency Laparotomy Audit (NELA) data
Data from the NELA audit on surgical management in the corresponding period will be
assessed. This will act as an additional denominator for number of people undergoing surgery
for SBO or LBO. Proportions undergoing adhesiolysis, small bowel resection and hernia repair
will be recorded. Outcome data for 30-day mortality and 30-day readmission will be recorded for
comparison with our dataset.
Training Materials
As with previous multicentre studies, we will deliver online training to ensure standardisation.
This will be delivered through online presentation of project rationale, how to complete the
pro forma, and how to use the REDCap system for return of forms.
Pilot Study Period There will be an initial two-week study period from October 11th-October 25th 2016. This will
permit a trial of the data-collection pro forma and IT systems supporting the project.
Process results from the pilot will be reviewed at a steering group meeting in November 2016. If
no or minor modifications only are required, these will be made and the project will proceed as
planned. Updated documents will be available from the study website. If a major issue is
12
identified, which requires significant modification of the project, the main data collection window
will be delayed to allow this to be addressed.
Full Study Period
The steering group will provide documents to facilitate local audit registration at least three
months prior to commencement of data collection.
The study period is:
Period Date
Case Identification period 15/01/2017-13/03/17
Data collection period
(readmissions) ends 30/04/2017
During data collection, day 1 is defined as the first 24-hour period following admission/referral to
the general surgery team. Day two is the next 24-hour period.

13
Analysis plan
Statistical support will be obtained from Sheffield Clinical Trials Unit. A formal statistical analysis
plan will be developed with this group following the pilot study.
Descriptive analysis:
Description of demographics of captured patients including gender, median age, aetiology of
SBO and management pathway will be performed. Data on complications of management will
be described.
14
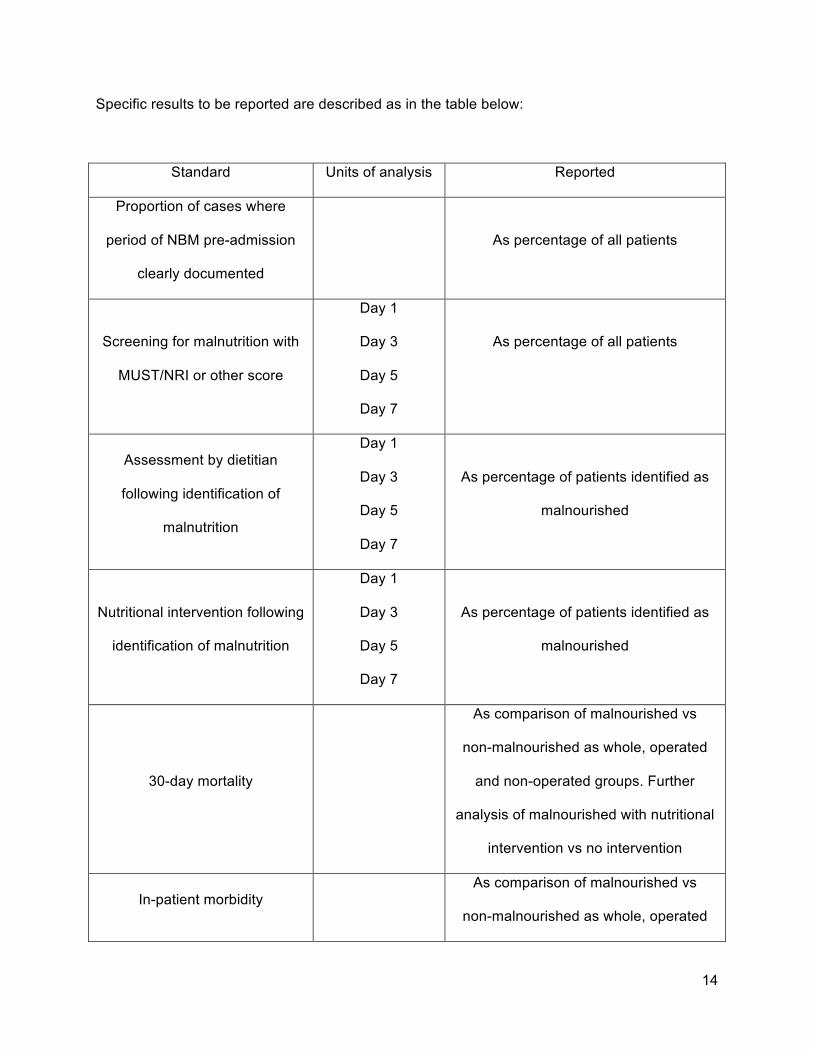
Specific results to be reported are described as in the table below:
Standard Units of analysis Reported
Proportion of cases where
period of NBM pre-admission
clearly documented
As percentage of all patients
Screening for malnutrition with
MUST/NRI or other score
Day 1
Day 3
Day 5
Day 7
As percentage of all patients
Assessment by dietitian
following identification of
malnutrition
Day 1
Day 3
Day 5
Day 7
As percentage of patients identified as
malnourished
Nutritional intervention following
identification of malnutrition
Day 1
Day 3
Day 5
Day 7
As percentage of patients identified as
malnourished
30-day mortality
As comparison of malnourished vs
non-malnourished as whole, operated
and non-operated groups. Further
analysis of malnourished with nutritional
intervention vs no intervention
In-patient morbidity As comparison of malnourished vs
non-malnourished as whole, operated
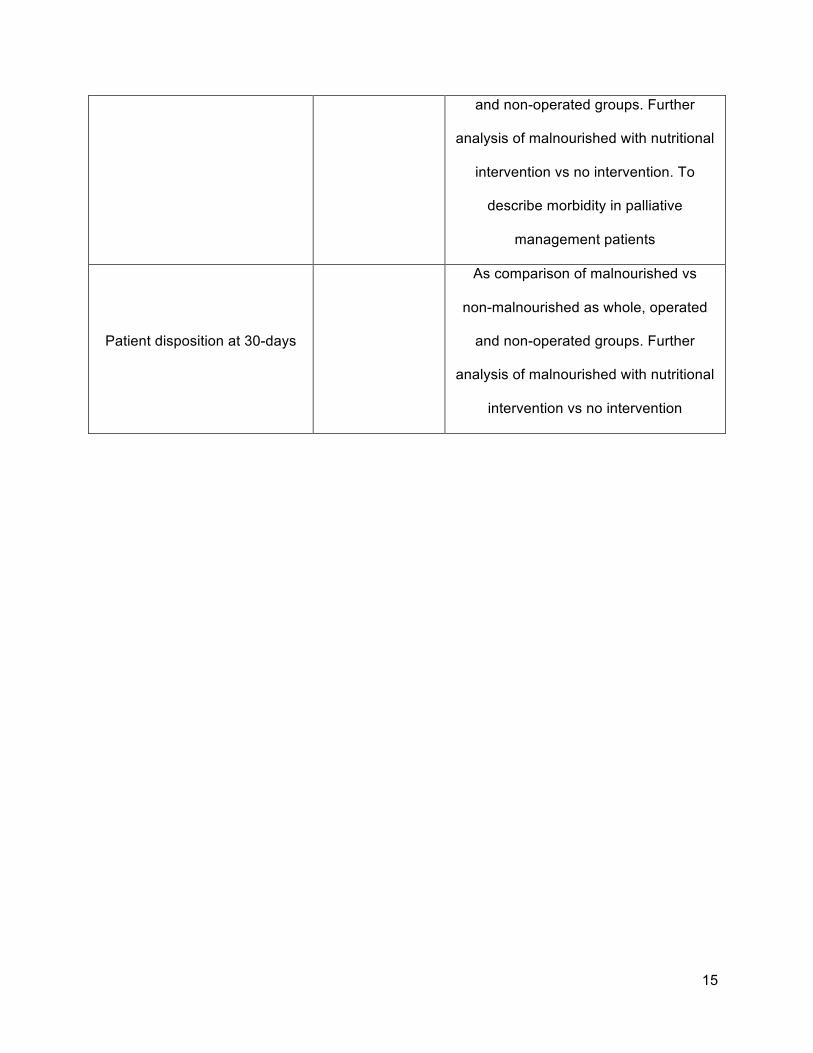
15
and non-operated groups. Further
analysis of malnourished with nutritional
intervention vs no intervention. To
describe morbidity in palliative
management patients
Patient disposition at 30-days
As comparison of malnourished vs
non-malnourished as whole, operated
and non-operated groups. Further
analysis of malnourished with nutritional
intervention vs no intervention
16
Collaboration criteria
The centre lead should be a substantive consultant with a practice in General Surgery, and will
be supported by collaborators, who are likely to be surgical trainees. It is expected that a team
of three collaborators will be required for each centre.
Collaborators will be issued with a confirmatory certificate after close of project as evidence for
their portfolio. In line with previous projects will be eligible for collaborative authorship which is
Pubmed citable on all published outputs. It is anticipated that there will be two levels of
corporate authorship – one for centre leads and one for team members.
Expected Outputs:
All data will be reported as a whole cohort. Unit level data for comparison will be fedback to
collaborators to support local service improvement.
This project will be submitted for presentation at a national or international surgical conference.
Manuscript(s) will be prepared following close of the project.
17
Further steps
With results from the audit, we will identify an intervention and repeat the audit post-intervention.
Examples of intervention may include:
• Dietitian assessment upon admission
• Accelerated management pathway
Appendix A: See Separate Document
Appendix B: See Separate Document
18
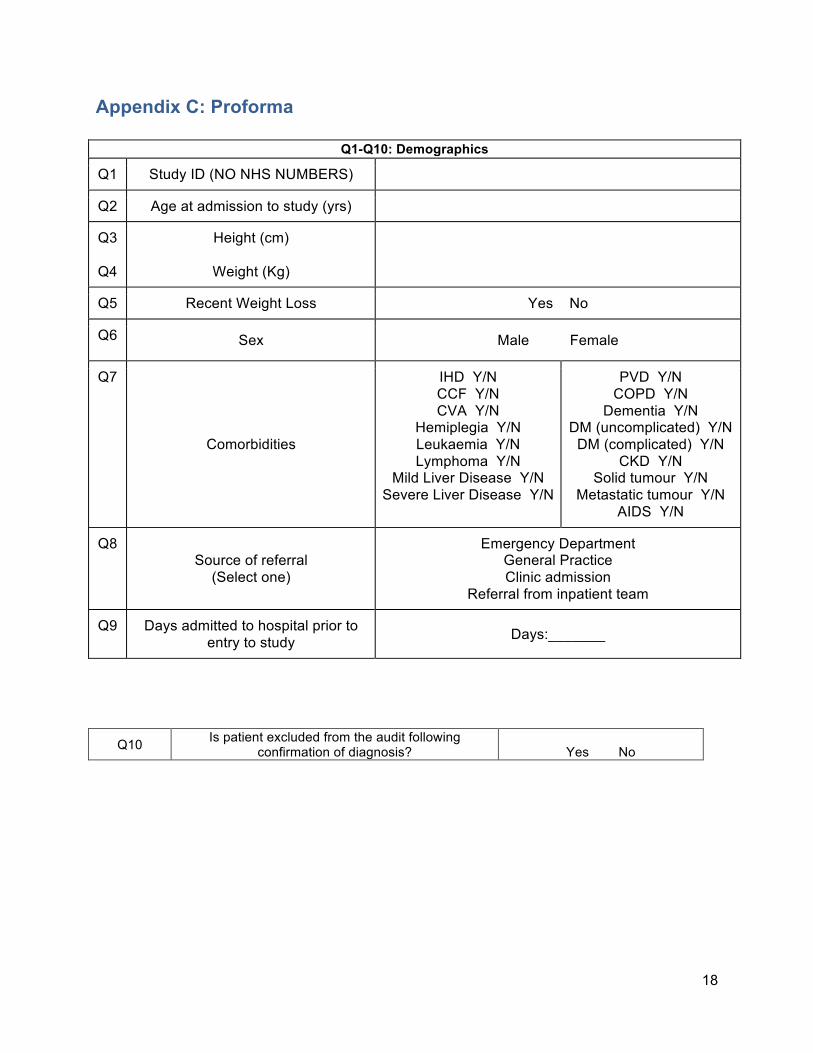
Appendix C: Proforma
Q1-Q10: Demographics
Q1 Study ID (NO NHS NUMBERS)
Q2 Age at admission to study (yrs)
Q3
Q4
Height (cm)
Weight (Kg)
Q5 Recent Weight Loss Yes No
Q6 Sex Male Female
Q7
Comorbidities
IHD Y/N CCF Y/N CVA Y/N
Hemiplegia Y/N Leukaemia Y/N Lymphoma Y/N
Mild Liver Disease Y/N Severe Liver Disease Y/N
PVD Y/N COPD Y/N
Dementia Y/N DM (uncomplicated) Y/N
DM (complicated) Y/N CKD Y/N
Solid tumour Y/N Metastatic tumour Y/N
AIDS Y/N
Q8 Source of referral
(Select one)
Emergency Department General Practice Clinic admission
Referral from inpatient team
Q9 Days admitted to hospital prior to entry to study Days:_______
Q10 Is patient excluded from the audit following confirmation of diagnosis?
Yes No
19
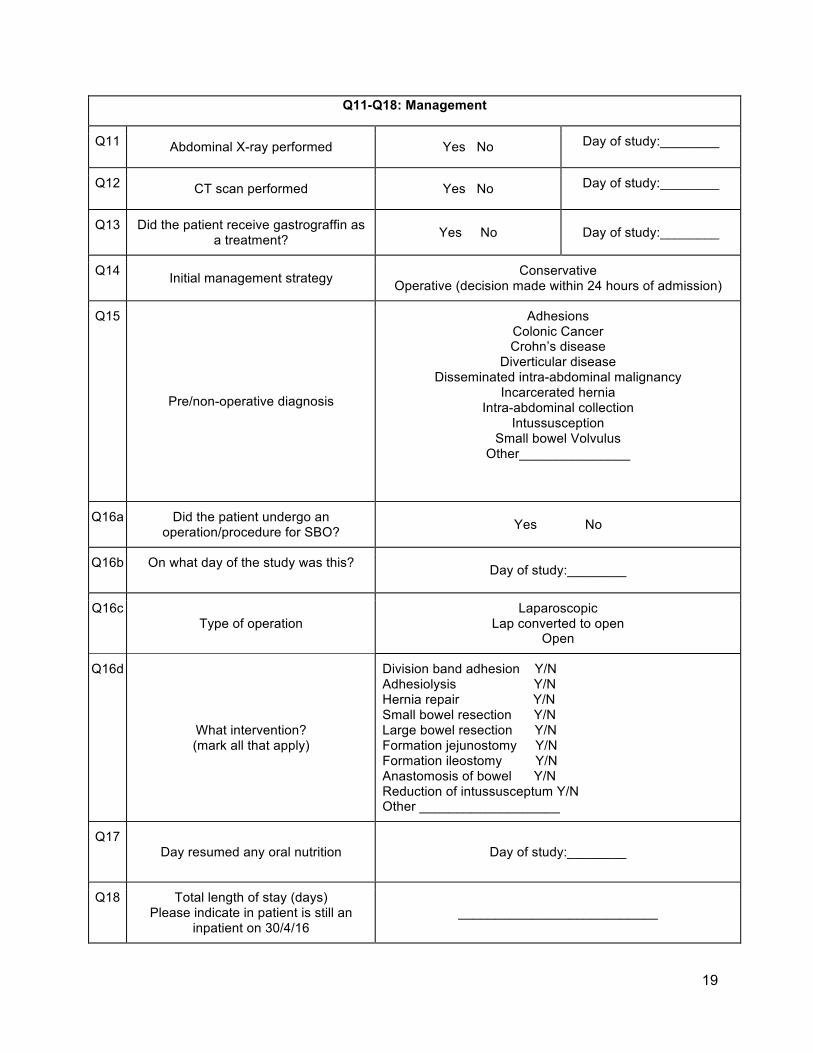
Q11-Q18: Management
Q11 Abdominal X-ray performed Yes No Day of study:________
Q12 CT scan performed Yes No Day of study:________
Q13 Did the patient receive gastrograffin as a treatment? Yes No Day of study:________
Q14 Initial management strategy Conservative Operative (decision made within 24 hours of admission)
Q15
Pre/non-operative diagnosis
Adhesions Colonic Cancer Crohn’s disease
Diverticular disease Disseminated intra-abdominal malignancy
Incarcerated hernia Intra-abdominal collection
Intussusception Small bowel Volvulus
Other_______________
Q16a Did the patient undergo an operation/procedure for SBO? Yes No
Q16b On what day of the study was this? Day of study:________
Q16c Type of operation
Laparoscopic Lap converted to open
Open
Q16d
What intervention? (mark all that apply)
Division band adhesion Y/N Adhesiolysis Y/N Hernia repair Y/N Small bowel resection Y/N Large bowel resection Y/N Formation jejunostomy Y/N Formation ileostomy Y/N Anastomosis of bowel Y/N Reduction of intussusceptum Y/N Other ___________________
Q17 Day resumed any oral nutrition Day of study:________
Q18 Total length of stay (days) Please indicate in patient is still an
inpatient on 30/4/16 ___________________________
20
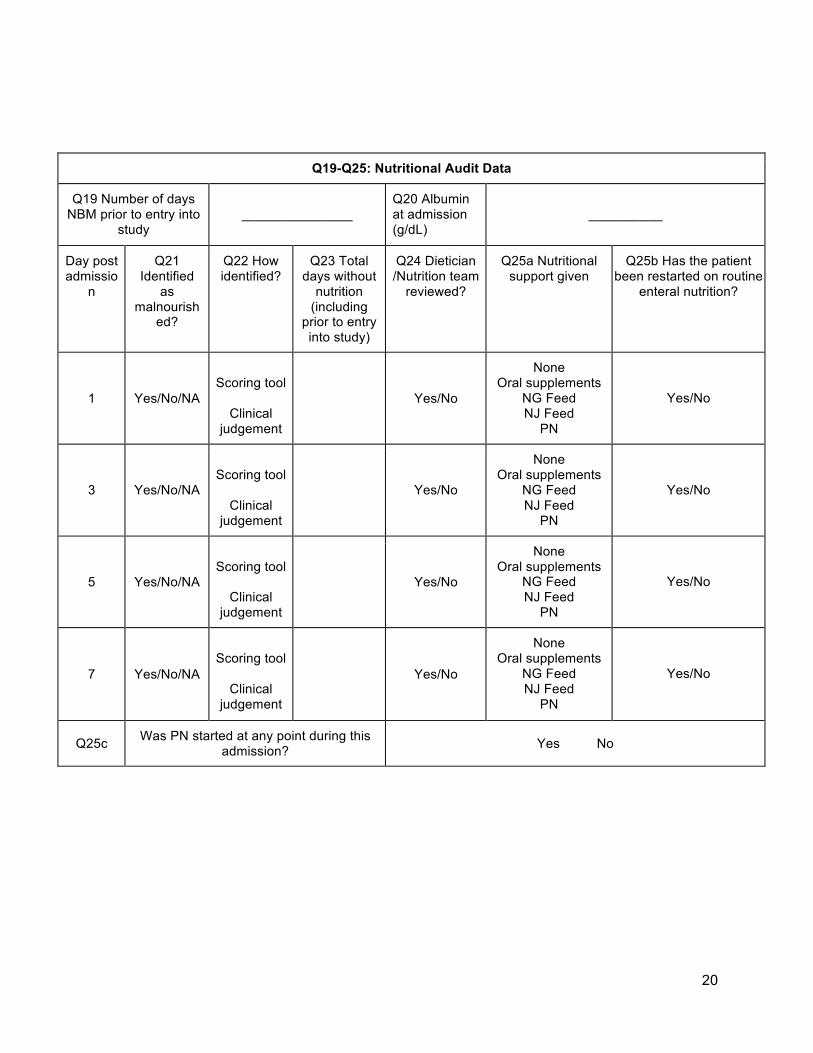
Q19-Q25: Nutritional Audit Data
Q19 Number of days NBM prior to entry into
study
_______________
Q20 Albumin at admission (g/dL)
__________
Day post admissio
n
Q21 Identified
as malnourish
ed?
Q22 How identified?
Q23 Total days without
nutrition (including
prior to entry into study)
Q24 Dietician /Nutrition team
reviewed?
Q25a Nutritional support given
Q25b Has the patient been restarted on routine
enteral nutrition?
1 Yes/No/NA
Scoring tool
Clinical
judgement
Yes/No
None Oral supplements
NG Feed NJ Feed
PN
Yes/No
3 Yes/No/NA
Scoring tool
Clinical
judgement
Yes/No
None Oral supplements
NG Feed NJ Feed
PN
Yes/No
5 Yes/No/NA
Scoring tool
Clinical
judgement
Yes/No
None Oral supplements
NG Feed NJ Feed
PN
Yes/No
7 Yes/No/NA
Scoring tool
Clinical
judgement
Yes/No
None Oral supplements
NG Feed NJ Feed
PN
Yes/No
Q25c Was PN started at any point during this admission? Yes No

21
Q26: Line complications
Q26a Was intravenous access established for nutrition? Yes No
Q26b What type of line was initially used?
Peripheral cannula
Peripherally inserted central catheter (PICC)
Central venous catheter (CVC/Central line)
Hickmann line
Q26c What day of the study was this inserted? Day of study:________
Q26d Did the patient develop line sepsis related to this line? Yes, confirmed Presumed No
Q26e Day line sepsis diagnosed Day of study:________
22
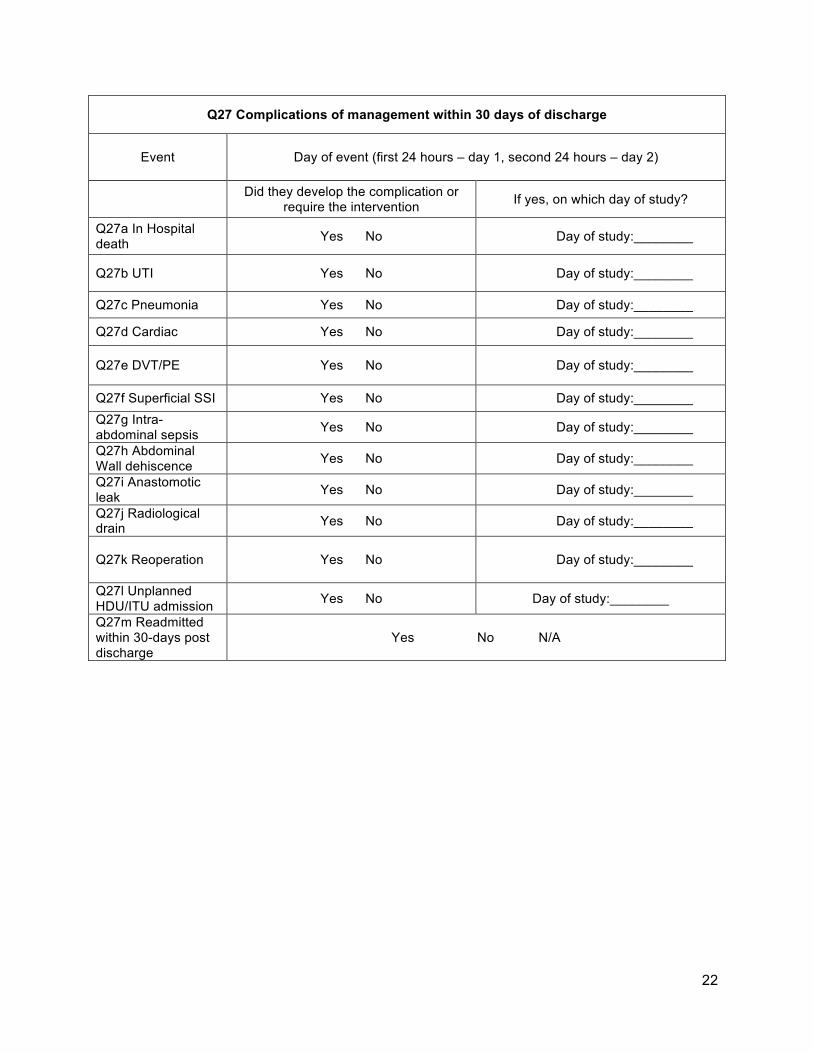
Q27 Complications of management within 30 days of discharge
Event Day of event (first 24 hours – day 1, second 24 hours – day 2)
Did they develop the complication or require the intervention If yes, on which day of study?
Q27a In Hospital death Yes No Day of study:________
Q27b UTI Yes No Day of study:________
Q27c Pneumonia Yes No Day of study:________
Q27d Cardiac Yes No Day of study:________
Q27e DVT/PE Yes No Day of study:________
Q27f Superficial SSI Yes No Day of study:________ Q27g Intra-abdominal sepsis Yes No Day of study:________
Q27h Abdominal Wall dehiscence Yes No Day of study:________
Q27i Anastomotic leak Yes No Day of study:________
Q27j Radiological drain Yes No Day of study:________
Q27k Reoperation Yes No
Day of study:________
Q27l Unplanned HDU/ITU admission Yes No Day of study:________
Q27m Readmitted within 30-days post discharge
Yes No N/A
23
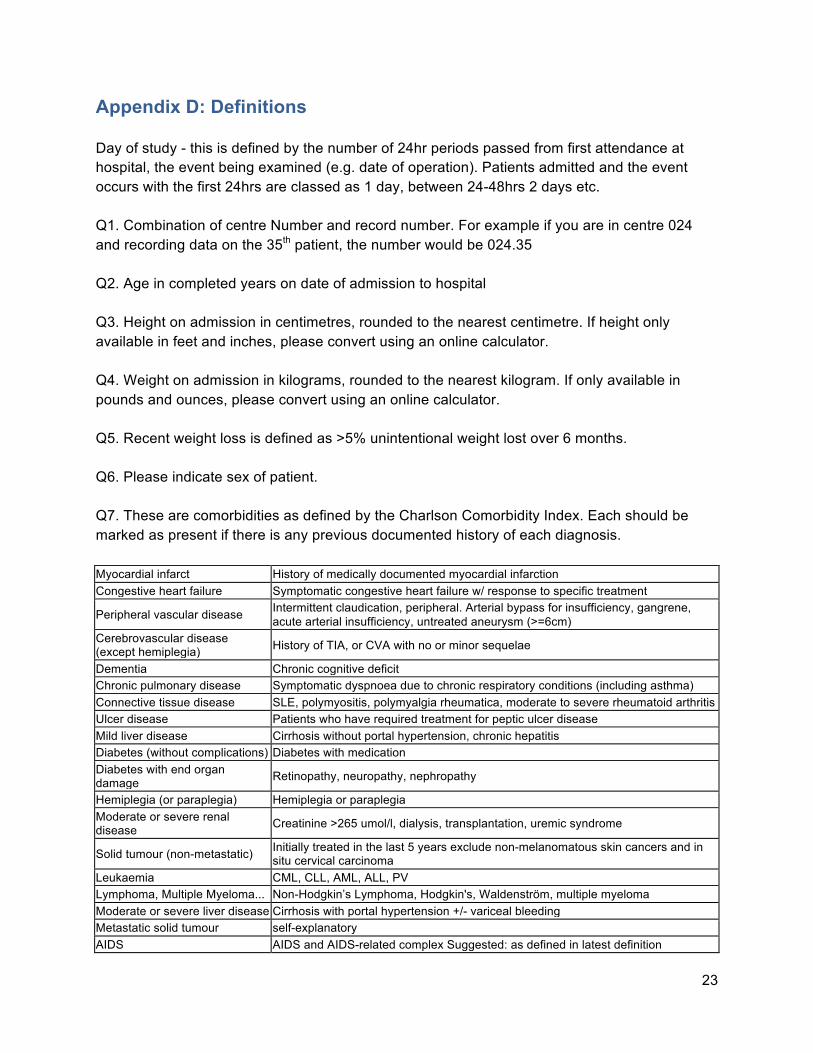
Appendix D: Definitions Day of study - this is defined by the number of 24hr periods passed from first attendance at hospital, the event being examined (e.g. date of operation). Patients admitted and the event occurs with the first 24hrs are classed as 1 day, between 24-48hrs 2 days etc. Q1. Combination of centre Number and record number. For example if you are in centre 024 and recording data on the 35th patient, the number would be 024.35 Q2. Age in completed years on date of admission to hospital Q3. Height on admission in centimetres, rounded to the nearest centimetre. If height only available in feet and inches, please convert using an online calculator. Q4. Weight on admission in kilograms, rounded to the nearest kilogram. If only available in pounds and ounces, please convert using an online calculator. Q5. Recent weight loss is defined as >5% unintentional weight lost over 6 months. Q6. Please indicate sex of patient. Q7. These are comorbidities as defined by the Charlson Comorbidity Index. Each should be marked as present if there is any previous documented history of each diagnosis. Myocardial infarct History of medically documented myocardial infarction Congestive heart failure Symptomatic congestive heart failure w/ response to specific treatment
Peripheral vascular disease Intermittent claudication, peripheral. Arterial bypass for insufficiency, gangrene, acute arterial insufficiency, untreated aneurysm (>=6cm)
Cerebrovascular disease (except hemiplegia) History of TIA, or CVA with no or minor sequelae
Dementia Chronic cognitive deficit Chronic pulmonary disease Symptomatic dyspnoea due to chronic respiratory conditions (including asthma) Connective tissue disease SLE, polymyositis, polymyalgia rheumatica, moderate to severe rheumatoid arthritis Ulcer disease Patients who have required treatment for peptic ulcer disease Mild liver disease Cirrhosis without portal hypertension, chronic hepatitis Diabetes (without complications) Diabetes with medication Diabetes with end organ damage Retinopathy, neuropathy, nephropathy
Hemiplegia (or paraplegia) Hemiplegia or paraplegia Moderate or severe renal disease Creatinine >265 umol/l, dialysis, transplantation, uremic syndrome
Solid tumour (non-metastatic) Initially treated in the last 5 years exclude non-melanomatous skin cancers and in situ cervical carcinoma
Leukaemia CML, CLL, AML, ALL, PV Lymphoma, Multiple Myeloma... Non-Hodgkin’s Lymphoma, Hodgkin's, Waldenström, multiple myeloma Moderate or severe liver disease Cirrhosis with portal hypertension +/- variceal bleeding Metastatic solid tumour self-explanatory AIDS AIDS and AIDS-related complex Suggested: as defined in latest definition
24
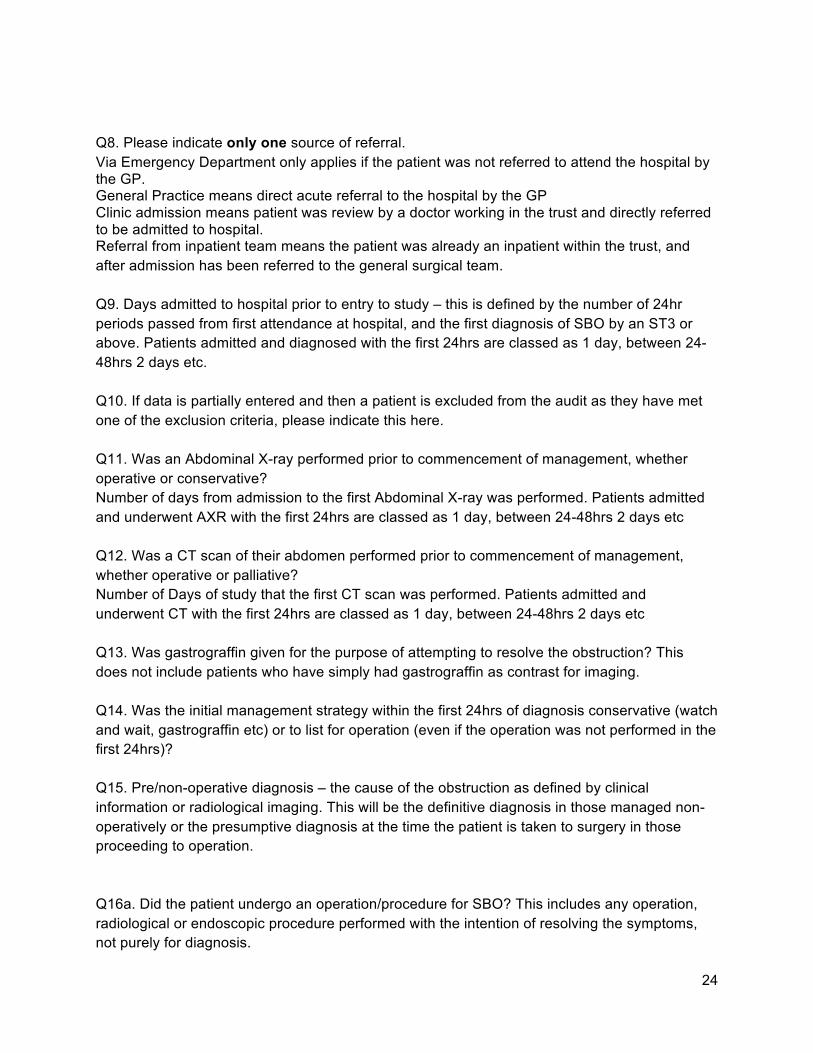
Q8. Please indicate only one source of referral. Via Emergency Department only applies if the patient was not referred to attend the hospital by the GP. General Practice means direct acute referral to the hospital by the GP Clinic admission means patient was review by a doctor working in the trust and directly referred to be admitted to hospital. Referral from inpatient team means the patient was already an inpatient within the trust, and after admission has been referred to the general surgical team. Q9. Days admitted to hospital prior to entry to study – this is defined by the number of 24hr periods passed from first attendance at hospital, and the first diagnosis of SBO by an ST3 or above. Patients admitted and diagnosed with the first 24hrs are classed as 1 day, between 24-48hrs 2 days etc. Q10. If data is partially entered and then a patient is excluded from the audit as they have met one of the exclusion criteria, please indicate this here. Q11. Was an Abdominal X-ray performed prior to commencement of management, whether operative or conservative? Number of days from admission to the first Abdominal X-ray was performed. Patients admitted and underwent AXR with the first 24hrs are classed as 1 day, between 24-48hrs 2 days etc Q12. Was a CT scan of their abdomen performed prior to commencement of management, whether operative or palliative? Number of Days of study that the first CT scan was performed. Patients admitted and underwent CT with the first 24hrs are classed as 1 day, between 24-48hrs 2 days etc Q13. Was gastrograffin given for the purpose of attempting to resolve the obstruction? This does not include patients who have simply had gastrograffin as contrast for imaging. Q14. Was the initial management strategy within the first 24hrs of diagnosis conservative (watch and wait, gastrograffin etc) or to list for operation (even if the operation was not performed in the first 24hrs)? Q15. Pre/non-operative diagnosis – the cause of the obstruction as defined by clinical information or radiological imaging. This will be the definitive diagnosis in those managed non-operatively or the presumptive diagnosis at the time the patient is taken to surgery in those proceeding to operation. Q16a. Did the patient undergo an operation/procedure for SBO? This includes any operation, radiological or endoscopic procedure performed with the intention of resolving the symptoms, not purely for diagnosis.
25
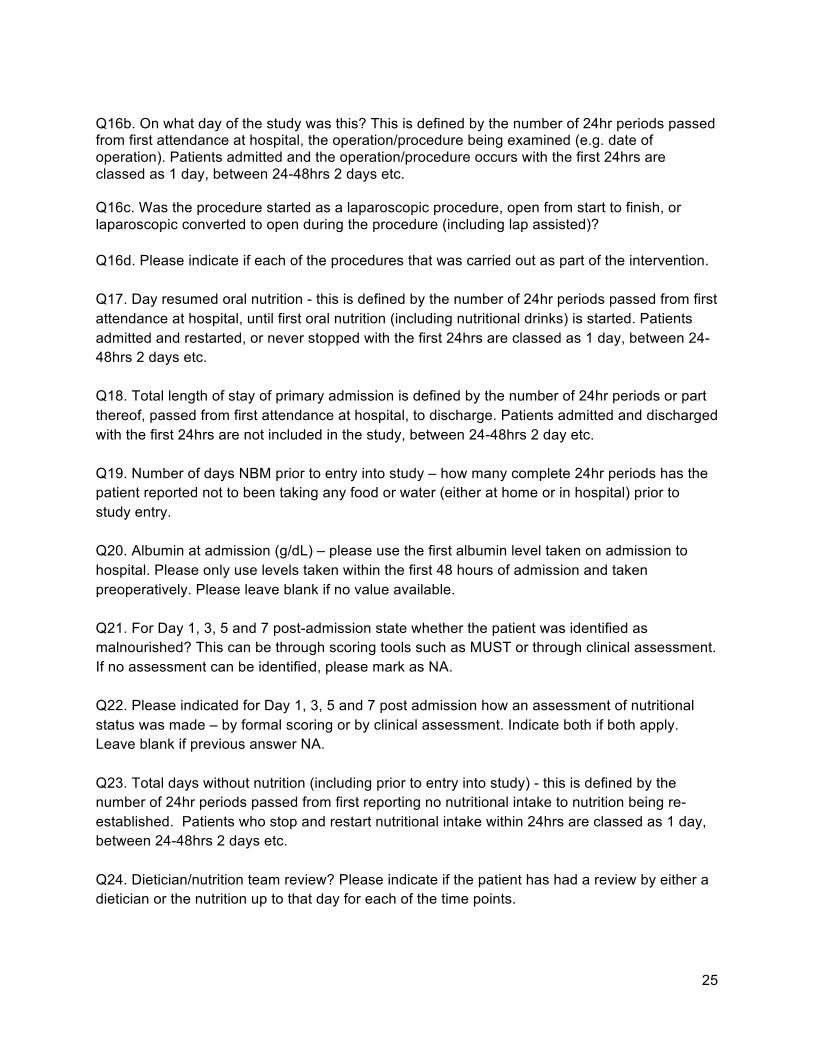
Q16b. On what day of the study was this? This is defined by the number of 24hr periods passed from first attendance at hospital, the operation/procedure being examined (e.g. date of operation). Patients admitted and the operation/procedure occurs with the first 24hrs are classed as 1 day, between 24-48hrs 2 days etc. Q16c. Was the procedure started as a laparoscopic procedure, open from start to finish, or laparoscopic converted to open during the procedure (including lap assisted)? Q16d. Please indicate if each of the procedures that was carried out as part of the intervention. Q17. Day resumed oral nutrition - this is defined by the number of 24hr periods passed from first attendance at hospital, until first oral nutrition (including nutritional drinks) is started. Patients admitted and restarted, or never stopped with the first 24hrs are classed as 1 day, between 24-48hrs 2 days etc. Q18. Total length of stay of primary admission is defined by the number of 24hr periods or part thereof, passed from first attendance at hospital, to discharge. Patients admitted and discharged with the first 24hrs are not included in the study, between 24-48hrs 2 day etc. Q19. Number of days NBM prior to entry into study – how many complete 24hr periods has the patient reported not to been taking any food or water (either at home or in hospital) prior to study entry. Q20. Albumin at admission (g/dL) – please use the first albumin level taken on admission to hospital. Please only use levels taken within the first 48 hours of admission and taken preoperatively. Please leave blank if no value available. Q21. For Day 1, 3, 5 and 7 post-admission state whether the patient was identified as malnourished? This can be through scoring tools such as MUST or through clinical assessment. If no assessment can be identified, please mark as NA. Q22. Please indicated for Day 1, 3, 5 and 7 post admission how an assessment of nutritional status was made – by formal scoring or by clinical assessment. Indicate both if both apply. Leave blank if previous answer NA. Q23. Total days without nutrition (including prior to entry into study) - this is defined by the number of 24hr periods passed from first reporting no nutritional intake to nutrition being re-established. Patients who stop and restart nutritional intake within 24hrs are classed as 1 day, between 24-48hrs 2 days etc. Q24. Dietician/nutrition team review? Please indicate if the patient has had a review by either a dietician or the nutrition up to that day for each of the time points.
26
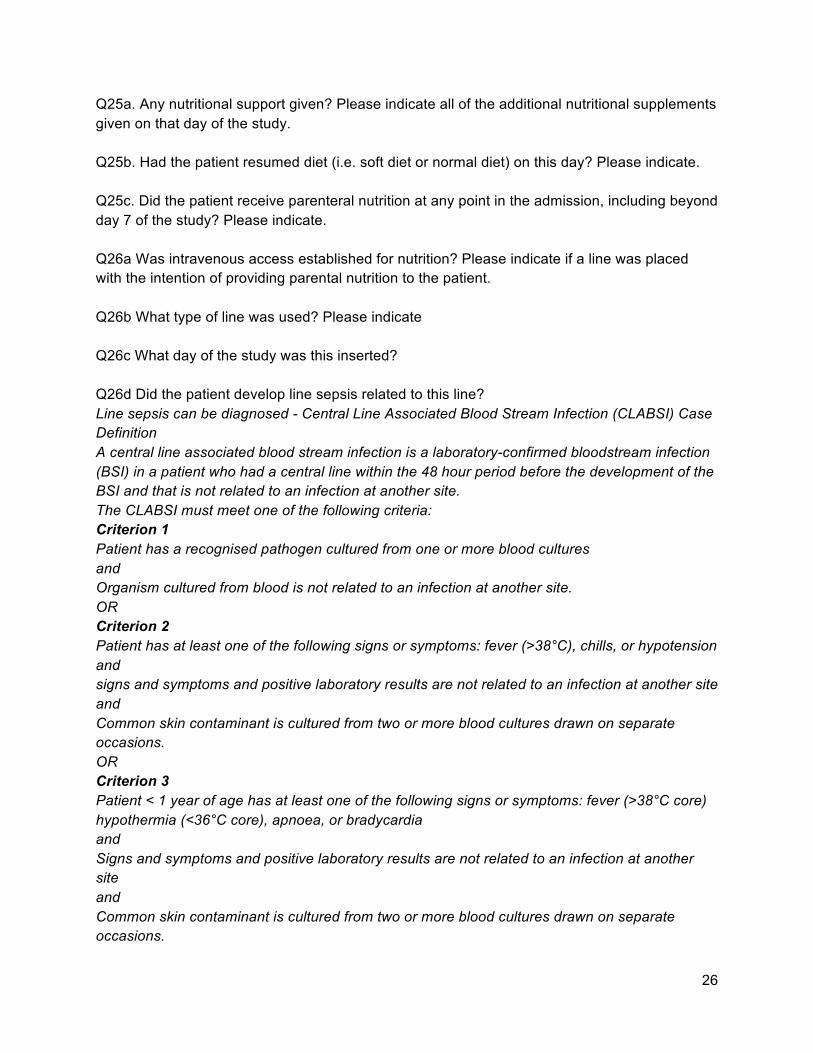
Q25a. Any nutritional support given? Please indicate all of the additional nutritional supplements given on that day of the study. Q25b. Had the patient resumed diet (i.e. soft diet or normal diet) on this day? Please indicate. Q25c. Did the patient receive parenteral nutrition at any point in the admission, including beyond day 7 of the study? Please indicate. Q26a Was intravenous access established for nutrition? Please indicate if a line was placed with the intention of providing parental nutrition to the patient. Q26b What type of line was used? Please indicate Q26c What day of the study was this inserted? Q26d Did the patient develop line sepsis related to this line? Line sepsis can be diagnosed - Central Line Associated Blood Stream Infection (CLABSI) Case Definition A central line associated blood stream infection is a laboratory-confirmed bloodstream infection (BSI) in a patient who had a central line within the 48 hour period before the development of the BSI and that is not related to an infection at another site. The CLABSI must meet one of the following criteria: Criterion 1 Patient has a recognised pathogen cultured from one or more blood cultures and Organism cultured from blood is not related to an infection at another site. OR Criterion 2 Patient has at least one of the following signs or symptoms: fever (>38°C), chills, or hypotension and signs and symptoms and positive laboratory results are not related to an infection at another site and Common skin contaminant is cultured from two or more blood cultures drawn on separate occasions. OR Criterion 3 Patient < 1 year of age has at least one of the following signs or symptoms: fever (>38°C core) hypothermia (<36°C core), apnoea, or bradycardia and Signs and symptoms and positive laboratory results are not related to an infection at another site and Common skin contaminant is cultured from two or more blood cultures drawn on separate occasions.
27
Q26e Day line sepsis diagnosed Q27. Complications In hospital death – Patient dies prior to discharge from acute hospital. UTI – Patient need to meet the two following criteria Patient has at least one of the following signs or symptoms: fever (>38.0°C) suprapubic tenderness costovertebral angle pain or tenderness urinary urgency urinary frequency dysuria And Patient has a urine culture with no more than two species of organisms identified, at least one of which is a bacterium of ≥ /ml Pneumonia must meet one of the criteria 1. Rales or dullness to percussion on physical examination of chest and any of the following: new onset of purulent sputum or change in character of sputum; organism isolated from blood culture; isolation of pathogen from specimen obtained by transtracheal aspirate, bronchial brushing or biopsy. 2. Chest radiographic examination shows new or progressive infiltrate, consolidation, cavitation or pleural effusion and any of the following: new onset of purulent sputum or change in character of sputum; organism isolated from blood culture; isolation of pathogen from specimen obtained by transtracheal aspirate, bronchial brushing or biopsy; isolation of virus or detection of viral antigen in respiratory secretions; diagnostic single antibody titre (IgM) or four-fold increase in paired serum samples (IgG) for pathogen. Superficial SSI - 1) Purulent drainage from the incision; OR (2) At least two of: pain or tenderness; localised swelling; redness; heat; fever; AND The incision is opened deliberately to manage infection or the clinician diagnoses a surgical site infection; OR (3) Wound organisms AND pus cells from aspirate/ swab
28
Deep (intra-abdominal) SSI - Intra-abdominal abscess/collection: (1) A clinical diagnosis of wound infection with dehiscence of mass closure or any layer below fat/scarpa’s fascia; (2) A clinical diagnosis of intra-abdominal collection (fever/abdominal pain) with operative/radiological evidence of a collection Cardiac - all complications newly diagnosed within 30 days of discharge (e.g. AF, MI, etc), even if unrelated to primary admission. DVT/PE – Radiologically confirmed within 30 days of discharge Abdominal Wall Dehiscence – full thickness dehiscence of lapaorotomy wound within 30 days of discharge. Anastomotic leakage - A clinical diagnosis will require symptoms related to leakage (gas, pus or faecal discharge from the drainage site, peritonitis or discharge of pus from the rectum). In the event of a clinically suspicious leak (fever or abdominal pain) the diagnosis can be established by operative or radiological diagnosis. When an anastomosis is defunctioned the presence or absence of a leak will be established by contrast radiology. Radiological drain – any additional procedure after operation, including imaging guided aspiration of collection or placement of a drain. Reoperation – any return to theatre for a general surgical cause within 30 days of discharge to hospital. Unplanned HDU/ITU admission - any unplanned episodes, even if unrelated to primary presentation Readmitted within 30-days post discharge - Readmission is defined as any admission following discharge which requires an overnight stay
29
Appendix E: Abbreviations ACS - Acute Coronary Syndrome AIDS - Acquired Immuno-Deficiency Disorder BAPEN - British Association for Parenteral and Enteral Nutrition CCF - Congestive Cardiac Failure CKD - Chronic Kidney Disease COPD - Chronic Obstructive Pulmonary Disease CT – Computer Tomography CVA - Cerebrovascular Accident CVC - Central Venous Catheter DM - Diabetes Mellitus DVT – Deep Vein Thrombosis GA – General Anaesthetic GP – General Practitioner HDU – High Dependency Unit IHD - Ischaemic Heart Disease ITU – Intensive Therapy Unit LBO - Large Bowel Obstruction LRTI - Lower Respiratory Tract Infection MI - Myocardial Infarction MUST - Malnutrition Universal Screening Tool N – No
30
NA – Not Applicable NBM – Nil By Mouth NELA – National Emergency Laparotomy Audit NG - Nasogastric NICE – National Institute of Clinical Excellence NJ – Nasojejunal NRI – Nutritional Risk Index PE – Pulmonary Embolism PICC - Peripherally Inserted Central Catheter PN – Parenteral Nutrition PVD - Peripheral Vascular Disease REDCap – Research Electronic Data Capture (http://projectredcap.org) SBO - Small Bowel Obstruction SLE - Systemic lupus erythematosus SSI – Surgical Site Infection TIA – Transient Ischaemic Attack US – Ultrasound Scan UTI – Urinary Tract Infection Y - Yes

31
References 1. Fevang B, Fevang J, Stangeland L, Soreide O, Svanes K, Viste A. Complications and Death After Surgical Treatment of Small Bowel Obstruction A 35-Year Institutional Experience. Annals of Surgery. 2000;231(4):529-37. 2. Krause WR, Webb TP. Geriatric small bowel obstruction: an analysis of treatment and outcomes compared with a younger cohort. Am J Surg. 2015;209(2):347-51. 3. Hu WH, Cajas-Monson LC, Eisenstein S, Parry L, Cosman B, Ramamoorthy S. Preoperative malnutrition assessments as predictors of postoperative mortality and morbidity in colorectal cancer: an analysis of ACS-NSQIP. Nutr J. 2015;14:91. 4. Thomas MN, Kufeldt J, Kisser U, Hornung HM, Hoffmann J, Andraschko M, et al. Effects of malnutrition on complication rates, length of hospital stay, and revenue in elective surgical patients in the G-DRG-system. Nutrition. 2016;32(2):249-54. 5. Decision Tree - Perioperative Nutrition: British Association for Parenteral and Enteral Nutritoin; 2012 [Available from: http://www.bapen.org.uk/pdfs/decision-trees/perioperative-nutrition.pdf. 6. Nutrition support for adults: oral nutrition support, enteral tube feeding and parenteral nutrition: National Institute for Health and Care Excellence; 2006 [Available from: https://www.nice.org.uk/guidance/cg32.