Embed Size (px)
Citation preview
3National Rural Health Mission
(2005-2012)
Appendix
PREAMBLE
Recognizing the importance of Health in the process ofeconomic and social development and improving the qualityof life of our citizens, the Government of India has resolvedto launch the National Rural Health Mission to carry outnecessary architectural correction in the basic health caredelivery system. The Mission adopts a synergistic approachby relating health to determinants of good health viz. segmentsof nutrition, sanitation, hygiene and safe drinking water. Italso aims at mainstreaming the Indian systems of medicineto facilitate health care. The Plan of Action includes increasingpublic expenditure on health, reducing regional imbalance inhealth infrastructure, pooling resources, integration oforganizational structures, optimization of health manpower,decentralization and district management of health programes,community participation and ownership of assets, inductionof management and financial personnel into district healthsystem, and operationalizing community health centers intofunctional hospitals meeting Indian Public Health Standardsin each Block of the Country.
The Goal of the Mission is to improve the availability ofand access to quality health care by people, especially forthose residing in rural areas, the poor, women and children.
STATE OF PUBLIC HEALTH
• Public health expenditure in India has declined from 1.3percent of GDP in 1990 to 0.9 percent of GDP in 1999.The Union Budgetary allocation for health is 1.3 percentwhile the State’s Budgetary allocation is 5.5 percent.
• Union Government contribution to public healthexpenditure is 15 percent while States contribution about85 percent
• Vertical Health and Family Welfare Programs have limitedsynergization at operational levels.
• Lack of community ownership of public health programsimpacts levels of efficiency, accountability andeffectiveness.
• Lack of integration of sanitation, hygiene, nutrition anddrinking water issues.
• There are striking regional inequalities.• Population stabilization is still a challenge, especially in
States with weak demographic indicators.• Curative services favour the non-poor: for every Re.1 spent
on the poorest 20 percent population, Rs.3 is spent onthe richest quintile.
• Only 10 percent Indians have some form of healthinsurance, mostly inadequate
• Hospitalized Indians spend on an average 58 percent oftheir total annual expenditure
• Over 40 percent of hospitalized Indians borrow heavily orsell assets to cover expenses
• Over 25 percent of hospitalized Indians fall below povertyline because of hospital expenses
NATIONAL RURAL HEALTH MISSION–THE VISION
• The National Rural Health Mission (2005-12) seeks toprovide effective health care to rural population throughout
Appendices 9
the country with special focus on 18 states, which haveweak public health indicators and/or weak infrastructure.
• These 18 States are Arunachal Pradesh, Assam, Bihar,Chhattisgarh, Himachal Pradesh, Jharkhand, Jammu andKashmir, Manipur, Mizoram, Meghalaya, MadhyaPradesh, Nagaland, Orissa, Rajasthan, Sikkim, Tripura,Uttaranchal and Uttar Pradesh.
• The Mission is an articulation of the commitment of theGovernment to raise public spending on Health from 0.9percent of GDP to 2 to 3 percent of GDP.
• It aims to undertake architectural correction of the healthsystem to enable it to effectively handle increasedallocations as promised under the National CommonMinimum Program and promote policies that strengthenpublic health management and service delivery in thecountry.
• It has as its key components provision of a female healthactivist in each village; a village health plan preparedthrough a local team headed by the Health and SanitationCommittee of the Panchayat; strengthening of the ruralhospital for effective curative care and made measurableand accountable to the community through Indian PublicHealth Standards (IPHS); and integration of verticalHealth and Family Welfare Programs and Funds foroptimal utilization of funds and infrastructure andstrengthening delivery of primary health care.
• It seeks to revitalize local health traditions and mainstreamAYUSH into the public health system.
• It aims at effective integration of health concerns withdeterminants of health like sanitation and hygiene,nutrition, and safe drinking water through a District Planfor Health.
• It seeks decentralization of programs for districtmanagement of health.
• It seeks to address the inter-state and inter-districtdisparities, especially among the 18 high focus States,including unmet needs for public health infrastructure.
• It shall define time-bound goals and report publicly ontheir progress.
• It seeks to improve access of rural people, especially poorwomen and children, to equitable, affordable, accountableand effective primary health care.
GOALS
• Reduction in Infant Mortality Rate (IMR) and MaternalMortality Ratio (MMR).
• Universal access to public health services such as Women’shealth, child health, water, sanitation and hygiene,immunization, and nutrition.
• Prevention and control of communicable and non-communicable diseases, including locally-endemicdiseases.
• Access to integrated comprehensive primary health care.• Population stabilization, gender and demographic balance.• Revitalize local health traditions and mainstream AYUSH• Promotion of healthy life styles.
STRATEGIES
Core Strategies
• Train and enhance capacity of Panchayati Raj Institutions(PRIs) to own, control and manage public health services.
• Promote access to improved healthcare at household levelthrough the female health activist (ASHA).
• Health Plan for each village through Village HealthCommittee of the Panchayat.
• Strengthening sub-center through an untied fund to enablelocal planning and action and more Multi-purpose Workers(MPWs).
• Strengthening existing PHCs and CHCs, and provision of30 to 50 bedded CHC per lakh population for improvedcurative care to a normative standard (Indian Public HealthStandards defining personnel, equipment and managementstandards).
• Preparation and implementation of an intersectoral DistrictHealth Plan prepared by the District Health Mission,including drinking water, sanitation and hygiene andnutrition.
• Integrating Vertical Health and Family Welfare programsat National, State, Block, and District levels.
• Technical Support to National, State and District HealthMissions, for Public Health Management.
• Strengthening capacities for data collection, assessmentand review for evidence-based planning, monitoring andsupervision.
• Formulation of transparent policies for deployment andcareer development of Human Resources for health.
• Developing capacities for preventive health care at all levelsfor promoting healthy life styles, reduction in consumptionof tobacco and alcohol, etc.
• Promoting non-profit sector particularly in under servedareas.
Supplementary Strategies
• Regulation of Private Sector including the informal ruralpractitioners to ensure availability of quality service tocitizens at reasonable cost.
• Promotion of Public Private Partnerships for achievingpublic health goals.
10 Practical Approach in Tuberculosis Management
• Mainstreaming AYUSH—revitalizing local healthtraditions.
• Reorienting medical education to support rural healthissues including regulation of Medical care and MedicalEthics.
• Effective and viable risk pooling and social health insuranceto provide health security to the poor by ensuringaccessible, affordable, accountable and good qualityhospital care.
PLAN OF ACTION
Component (A): Accredited Social Health Activists
• Every village/large habitat will have a female AccreditedSocial Health Activist (ASHA)—chosen by andaccountable to the panchayat—to act as the interfacebetween the community and the public health system.States to choose State specific models.
• ASHA would act as a bridge between the ANM and thevillage and be accountable to the Panchayat.
• She will be an honorary volunteer, receiving performance-based compensation for promoting universalimmunization, referral and escort services for RCH,construction of household toilets, and other health caredelivery programs.
• She will be trained on a pedagogy of public healthdeveloped and mentored through a Standing MentoringGroup at National level incorporating best practices andimplemented through active involvement of communityhealth resource organizations.
• She will facilitate preparation and implementation of theVillage Health Plan along with Anganwadi worker, ANM,functionaries of other Departments, and Self-Help Groupmembers, under the leadership of the Village HealthCommittee of the Panchayat.
• She will be promoted all over the country, with specialemphasis on the 18 high focus States. The Governmentof India will bear the cost of training, incentives andmedical kits. The remaining components will be fundedunder Financial Envelope given to the States under theprograme.
• She will be given a Drug Kit containing generic AYUSHand allopathic formulations for common ailments. Thedrug kit would be replenished from time to time.
• Induction training of ASHA to be of 23 days in all, spreadover 12 months. On the job training would continuethroughout the year.
• Prototype training material to be developed at Nationallevel subject to State level modifications.
• Cascade model of training proposed through Training ofTrainers including contract plus distance learning model
• Training would require partnership with NGOs/ICDSTraining Centers and State Health Institutes.
Component (B): Strengthning Sub-centers
• Each sub-center will have an Untied Fund for local action@ Rs. 10,000 per annum. This Fund will be deposited ina joint Bank Account of the ANM and Sarpanch andoperated by the ANM, in consultation with the VillageHealth Committee.
• Supply of essential drugs, both allopathic and AYUSH,to the Sub-centers.
• In case of additional Outlays, Multipurpose Workers(Male)/Additional ANMs wherever needed, sanction of newSub-centers as per 2001 population norm, and upgradingexisting Sub-centers, including buildings for Sub-centersfunctioning in rented premises will be considered.
Component (C): StrengtheningPrimary Health Centers
Mission aims at Strengthening PHC for quality preventive,promotive, curative, supervisory and Outreach services,through:• Adequate and regular supply of essential quality drugs
and equipment (including Supply of Auto Disabled Syringesfor immunization) to PHCs
• Provision of 24 hour service in 50 percent PHCs byaddressing shortage of doctors, especially in high focusStates, through mainstreaming AYUSH manpower.
• Observance of Standard treatment guidelines andprotocols.
• In case of additional Outlays, intensification of ongoingcommunicable disease control programes, new programesfor control of noncommunicable diseases, upgradationof 100 percent PHCs for 24 hours referral service, andprovision of 2nd doctor at PHC level (I male, 1 female)would be undertaken on the basis of felt need.
Component (D): Strengthening CHCs forFirst Referral Care
A key strategy of the Mission is:• Operationalizing 3222 existing Community Health Centers
(30-50 beds) as 24 Hour First Referral Units, includingposting of anesthetists.
• Codification of new Indian Public Health Standards,setting norms for infrastructure, staff, equipment,management etc. for CHCs.
Appendices 11
• Promotion of Stakeholder Committees (Rogi KalyanSamitis) for hospital management.
• Developing standards of services and costs in hospitalcare.
• Develop, display and ensure compliance to Citizen’sCharter at CHC/PHC level.
• In case of additional Outlays, creation of new CommunityHealth Centers (30-50 beds) to meet the population normas per Census 2001, and bearing their recurring costs forthe Mission period could be considered.
Component (E): District Health Plan
• District Health Plan would be an amalgamation of fieldresponses through Village Health Plans, State andNational Priorities for Health, Water Supply, Sanitationand Nutrition.
• Health Plans would form the core unit of action proposedin areas like water supply, sanitation, hygiene and nutrition.Implementing Departments would integrate into DistrictHealth Mission for monitoring.
• District becomes core unit of planning, budgeting andimplementation.
• Centrally-Sponsored Schemes could be rationalized/modified accordingly in consultation with States.
• Concept of “funneling” funds to district for effectiveintegration of programs
• All vertical Health and Family Welfare Programs at Districtand state level merge into one common “District HealthMission” at the District level and the “State Health Mission”at the state level
• Provision of Project Management Unit for all districts,through contractual engagement of MBA, Inter Charter/Inter-cost and Data Entry Operator, for improved programmanagement.
Component (F): Converging Sanitation andHygiene Under NRHM
• Total Sanitation Campaign (TSC) is presentlyimplemented in 350 districts, and is proposed to cover alldistricts in 10th Plan.
• Components of TSC include IEC activities, rural sanitarymarts, individual household toilets, women sanitarycomplex, and School Sanitation Program.
• Similar to the DHM, the TSC is also implemented throughPanchayati Raj Institutions (PRIs).
• The District Health Mission would therefore guide activitiesof sanitation at district level, and promote joint IEC forpublic health, sanitation and hygiene, through Village
Health and Sanitation Committee, and promotehousehold toilets and School Sanitation Programe. ASHAwould be incentivized for promoting household toilets bythe Mission.
Component (G): Strengthening DiseaseControl Programs
• National Disease Control Programs for Malari a, TB, KalaAzar, Filaria, Blindness and Iodine Deficiency andIntegrated Disease Surveillance Program shall be integratedunder the Mission, for improved program delivery.
• New Initiatives would be launched for control of NonCommunicable Diseases.
• Disease surveillance system at village level would bestrengthened.
• Supply of generic drugs (both AYUSH and Allopathic)for common ailments at village, SC, PHC/CHC level.
• Provision of a mobile medical unit at District level forimproved Outreach services.
Component (H): Public-Private Partnership forPublic Health Goals, Including Regulation ofPrivate Sector
• Since almost 75 percent of health services are beingcurrently provided by the private sector, there is a need torefine regulation
• Regulation to be transparent and accountable• Reform of regulatory bodies/creation where necessary• District Institutional Mechanism for Mission must have
representation of private sector• Need to develop guidelines for Public-Private Partnership
(PPP) in health sector. Identifying areas of partnership,which are need based, thematic and geographic.
• Public sector to play the lead role in defining the frameworkand sustaining the partnership
• Management plan for PPP initiatives: at District/State andNational levels
Component (I): New Health Financing Mechanisms
A Task Group to examine new health financing mechanisms,including Risk Pooling for Hospital Care as follows:• Progressively the District Health Missions to move towards
paying hospitals for services by way of reimbursement,on the principle of “money follows the patient.”
• Standardization of services—outpatient, in-patient,laboratory, surgical interventions- and costs will be doneperiodically by a committee of experts in each state.
12 Practical Approach in Tuberculosis Management
• A National Expert Group to monitor these standards andgive suitable advice and guidance on protocols and costcomparisons.
• All existing CHCs to have wage component paid onmonthly basis. Other recurrent costs may be reimbursedfor services rendered from District Health Fund. Over theMission period, the CHC may move towards all costs,including wages reimbursed for services rendered.
• A district health accounting system, and an ombudsmanto be created to monitor the District Health FundManagement , and take corrective action.
• Adequate technical managerial and accounting supportto be provided to DHM in managing risk-pooling andhealth security.
• Where credible Community-Based Health InsuranceSchemes (CBHI) exist/are launched, they will beencouraged as part of the Mission.
• The Central Government will provide subsidies to cover apart of the premiums for the poor, and monitor theschemes.
• The IRDA will be approached to promote such CBHIs,which will be periodically-evaluated for effective delivery.
Component (J): Reorienting Health/MedicalEducation to Support Rural Health Issues
• While district and tertiary hospitals are necessarily locatedin urban centers, they form an integral part of the referralcare chain serving the needs of the rural people.
• Medical and para-medical education facilities need to becreated in states, based on need assessment.
• Suggestion for Commission for Excellence in Health Care(Medical Grants Commission), National Institution forPublic Health Management etc.
• Task Group to improve guidelines/details.
INSTITUTIONAL MECHANISMS
• Village Health and Sanitation Samiti (at village levelconsisting of Panchayat Representative/s, ANM/MPW,Anganwadi worker, teacher, ASHA, community healthvolunteers.
• Rogi Kalyan Samiti (or equivalent) for communitymanagement of public hospitals.
• District Health Mission, under the leadership of ZilaParishad with District Health Head as Convener and allrelevant departments, NGOs, private professionals etcrepresented on it.
• State Health Mission, Chaired by Chief Minister and co-chaired by Health Minister and with the State Health
Secretary as Convener—representation of relateddepartments, NGOs, private professionals etc.
• Integration of Departments of Health and Family Welfare,at National and State level.
• National Mission Steering Group chaired by Union Ministerfor Health and Family Welfare with Deputy ChairmanPlanning Commission, Ministers of Panchayat Raj, RuralDevelopment and Human Resource Development andpublic health professionals as members, to provide policysupport and guidance to the Mission.
• Empowered Programs Committee chaired by SecretaryHFW, to be the Executive Body of the Mission.
• Standing Mentoring Group shall guide and oversee theimplementation of ASHA initiative.
• Task Groups for Selected Tasks (time-bound).
TECHNICAL SUPPORT
• To be effective the Mission needs a strong component ofTechnical Support.
• This would include reorientation into public healthmanagement.
• Reposition existing health resource institutions, likePopulation Research Center (PRC), Regional ResourceCenter (RRC), State Institute of Health and Family Welfare(SIHFW).
• Involve NGOs as resource organiszations.• Improved Health Information System.• Support required at all levels: National, State, District
and sub-district.• Mission would require two distinct support mechanisms –
Programe Management Support Center and Health Trustof India.
Programe Management Support Center
• For Strengthening Management Systems-basic programemanagement, financial systems, infrastructuremaintenance, procurement and logistics systems,Monitoring and Information System (MIS), non-lapsablehealth pool etc.
• For Developing Manpower Systems—recruitment(induction of MBAs/CAs /MCAs), training and curriculumdevelopment (revitalization of existing institutions andpartnerships with NGO and private sector. Sectorinstitutions), motivation and performance appraisal etc.
• For Improved Governance—decentralization andempowerment of communities, induction of IT basedsystems like e-banking, social audit and right toinformation.
Appendices 13
Health Trust of India
• Proposed as a knowledge institution, to be the repositoryof innovation—research and documentation, healthinformation system, planning, monitoring and evaluationetc.
• For establishing Public Accountability Systems—externalevaluations, community based feedback mechanisms,participation of PRIs /NGOs etc.
• For developing a Framework for pro-poor Innovations• For reviewing Health Legislations.• A base for encouraging experimentation and action
research.• For Inter-and Intra-Sector Networking with National and
International Organizations.• Think Tank for developing a long-term vision of the Sector
and for building planning capacities of PRIs, Districts etc.
ROLE OF STATE GOVERNMENTS
Under NRHM
• The Mission covers the entire country. The 18 high focusStates are Uttar Pradesh, Bihar, Rajasthan, MadhyaPradesh, Orissa, Uttaranchal, Jharkhand, Chhattisgarh,Assam, Sikkim, Arunachal Pradesh, Manipur, Meghalaya,Tripura, Nagaland, Mizoram Himachal Pradesh andJammu and Kashmir. GoI would provide funding for keycomponents in these 18 high focus States. Other Stateswould fund interventions like ASHA, ProgrameManagement Unit (PMU), and upgradation of SC/PHC/CHC through Integrated Financial Envelope.
• NRHM provides broad conceptual framework. Stateswould project operational modalities in their State ActionPlans, to be decided in consultation with the MissionSteering Group.
• NRHM would prioritize funding for addressing inter-stateand intradistrict disparities in terms of health infrastructureand indicators.
• States would sign Memorandum of Understanding withGovernment of India, indicating their commitment toincrease contribution to Public Health Budget (preferablyby 10% each year), increased devolution to PanchayatiRaj Institutions as per 73rd Constitution (Amendment)Act, and performance benchmarks for release of funds.
FOCUS ON THE NORTH-EASTERN STATES
• All 8 North-East States, including Assam, ArunachalPradesh, Manipur, Meghalaya, Mizoram, Nagaland,
Sikkim and Tripura, are among the States selected underthe Mission, for special focus.
• Empowerment to the Mission would mean greaterflexibilities for the 10 percent committed Outlay of theMinistry of Health and Family Welfare, for North-EastStates.
• States shall be supported for creation/upgradation of healthinfrastructure, increased mobility, contractual engagement,and technical support under the Mission.
• Regional Resource Center is being supported under NRHMfor the North-Eastern States.
• Funding would be available to address local health issuesin a comprehensive manner, through State specificschemes and initiatives.
ROLE OF PANCHAYATI RAJ INSTITUTIONS
The Mission envisages the following roles for PRIs:• States to indicate in their MoUs the commitment for
devolution of funds, functionaries and programes forhealth, to PRIs.
• The District Health Mission to be led by the Zila Parishad.The DHM will control, guide and manage all public healthinstitutions in the district, Sub-centers, PHCs and CHCs.
• ASHAs would be selected by and be accountable to theVillage Panchayat.
• The Village Health Committee of the Panchayat wouldprepare the Village Health Plan, and promote intersectoralintegration
• Each sub-center will have an Untied Fund for local action@ Rs. 10,000 per annum. This Fund will be deposited ina joint Bank Account of the ANM and Sarpanch andoperated by the ANM, in consultation with the VillageHealth Committee.
• PRI involvement in Rogi Kalyan Samitis for good hospitalmanagement.
• Provision of training to members of PRIs.• Making available health related databases to all
stakeholders, including Panchayats at all levels.
ROLE OF NGOS IN THE MISSION
• Included in institutional arrangement at National, Stateand District levels, including Standing Mentoring Groupfor ASHA
• Member of Task Groups• Provision of Training, BCC and Technical Support for
ASHAs/DHM• Health Resource Organizations
14 Practical Approach in Tuberculosis Management
• Service delivery for identified population groups on selectthemes
• For monitoring, evaluation and social audit
MAINSTREAMING AYUSH
• The Mission seeks to revitalize local health traditions andmainstream AYUSH infrastructure, including manpower,and drugs, to strengthen the public health system at alllevels.
• AYUSH medications shall be included in the Drug Kitprovided at village levels to ASHA.
• The additional supply of generic drugs for commonailments at Subcenter/ PHC/CHC levels under the Missionshall also include AYUSH formulations.
• At the CHC level, two rooms shall be provided for AYUSHpractitioner and pharmacist under the Indian PublicHealth System (IPHS) model.
• Single doctor PHCs shall be upgraded to two doctor PHCsby mainstreaming AYUSH practitioner at that level.
FUNDING ARRANGEMENTS
• The Mission is conceived as an umbrella programesubsuming the existing programes of health and familywelfare, including the RCHII, National Disease ControlProgrames for Malaria, TB, Kala Azar, Filaria, Blindnessand Iodine Deficiency and Integrated Disease SurveillancePrograme.
• The Budget Head For NRHM shall be created in B.E.2006-07 at National and State levels. Initially, the verticalhealth and family welfare programes shall retain their Sub-Budget Head under the NRHM.
• The Outlay of the NRHM for 2005-06 is in the range ofRs.6700 crores.
• The Mission envisages an additionality of 30 percent overexisting Annual Budgetary Outlays, every year, to fulfillthe mandate of the National Common MinimumPrograme to raise the Outlays for Public Health from 0.9percent of GDP to 2 to 3 percent of GDP
• The Outlay for NRHM shall accordingly be determined inthe Annual Budgetary exercise.
• The States are expected to raise their contributions toPublic Health Budget by minimum 10 percent p.a. tosupport the Mission activities.
• Funds shall be released to States through SCOVA, largelyin the form of Financial Envelopes, with weightage to 18high focus States.
TIMELINES (FOR MAJOR COMPONENTS)
Merger of Multiple Societies June 2005Constitution of District/State MissionProvision of additional generic drugs December 2005at SC/PHC/CHC levelOperational Programe Management 2005-2006UnitsPreparation of Village Health Plans 2006ASHA at village level (with Drug Kit) 2005-2008Upgrading of Rural Hospitals 2005-2007Operationalizing District Planning 2005-2007Mobile Medical Unit at district level 2005-08
OUTCOMES
National Level
• Infant Mortality Rate reduced to 30/1,000 live-births• Maternal Mortality Ratio reduced to 100/100,000• Total Fertility Rate reduced to 2.1• Malaria mortality reduction rate: 50 percent upto 2010,
additional 10 percent by 2012• Kala Azar mortality reduction rate: 100 percent by 2010
and sustaining elimination until 2012• Filaria/Microfilaria reduction rate: 70 percent by 2010,
80 percent by 2012 and elimination by 2015• Dengue mortality reduction rate: 50 percent by 2010 and
sustaining at that level until 2012• Japanese Encephalitis mortality reduction rate: 50 percent
by 2010 and sustaining at that level until 2012• Cataract Operation: increasing to 46 lakhs per year until
2012.• Leprosy prevalence rate: reduce from 1.8/10,000 in 2005
to less than 1/10,000 thereafter• Tuberculosis DOTS services: Maintain 85 percent cure
rate through entire Mission period.• Upgrading Community Health Centers to Indian Public
Health Standards• Increase utilization of First Referral Units from less than
20 percent to 75 percent• Engaging 250,000 female Accredited Social Health
Activists (ASHAs) in 10 States.
Community Level
• Availability of trained community level worker at villagelevel, with a drug kit for generic ailments
• Health Day at Anganwadi level on a fixed day/month forprovision of immunization, ante/post natal checkups and
Appendices 15
services related to mother and child healthcare, includingnutrition.
• Availability of generic drugs for common ailments at Sub-center and hospital level.
• Good hospital care through assured availability of doctors,drugs and quality services at PHC/CHC level.
• Improved access to Universal Immunization throughinduction of Auto Disabled Syringes, alternate vaccinedelivery and improved mobilization services under theprogram.
• Improved facilities for institutional delivery throughprovision of referral, transport, escort and improvedhospital care subsidized under the Janani Suraksha Yojana(JSY) for the Below Poverty Line families.
• Availability of assured healthcare at reduced financial riskthrough pilots of Community Health Insurance under theMission.
• Provision of household toilets.
• Improved Outreach services through mobile medical unitat districtlevel.
MONITORING AND EVALUATION
• Health MIS to be developed upto CHC level, and web-enabled for citizen scrutiny.
• Sub-centers to report on performance to Panchayats,Hospitals to Rogi Kalyan Samitis and District HealthMission to Zila Parishad.
• The District Health Mission to monitor compliance toCitizen’s Charter at CHC level.
• Annual District Reports on People’s Health (to be preparedby Govt/NGO collaboration).
• State and National Reports on People’s Health to be tabledin Assemblies, Parliament.
• External evaluation/social audit through professionalbodies/NGOs.
• Mid Course reviews and appropriate correction.
International Standards for Tuberculosis CareSeventh Draft 7 September, 2005
INTRODUCTION
Purpose
The purpose of the International Standards for TuberculosisCare is to describe a widely accepted level of care, defined interms of specific actions, that all practitioners, public andprivate, should follow in dealing with patients who have, orare suspected of having, tuberculosis. The Standards areintended to facilitate the engagement of all care providers indelivering high quality care for patients of all ages, includingthose with smear-positive, smear-negative, and extra-pulmonary tuberculosis, tuberculosis caused by drug-resistantorganisms, and tuberculosis combined with HIV infection. Ahigh standard of care is essential to restore the health ofindividuals with tuberculosis, to prevent the disease in theirfamilies and others with whom they come into contact, andto protect the health of communities.1 Substandard care willresult in poor patient outcomes, continued infectiousness withtransmission of the infection to family and other communitymembers, and, perhaps, generation and propagation of drugresistance. Care that does not reach the defined level wouldbe considered substandard and not acceptable.
A standard differs from a guideline in that it does notprovide specific guidance on disease management but, rather,presents a principle or set of principles and actions based onthe principles that can be applied in nearly all situations.These principles and actions provide a platform on whichcare can be founded. In addition, a standard can be used asan indicator of the overall adequacy of disease managementagainst which individual or collective practices can bemeasured, whereas, guidelines are intended to assist providersin making informed decisions about appropriate healthinterventions.2
The basic principles of care for persons with, or suspectedof having, tuberculosis are the same worldwide: a diagnosisshould be established promptly and accurately; standardizedtreatment regimens of proven efficacy should be used togetherwith appropriate treatment support and supervision; theresponse to treatment should be monitored; and the essentialpublic health responsibilities must be carried out. Prompt,accurate diagnosis and effective treatment are not onlyessential for good patient care, they are the key elements inthe public health response to tuberculosis and are thecornerstone of tuberculosis control. Thus, all providers who

16 Practical Approach in Tuberculosis Management
undertake evaluation and treatment of patients withtuberculosis must recognize that, not only are they deliveringcare to an individual, they are assuming an important publichealth function that also entails a high level of responsibilityto the community, as well as to the individual patient.Adherence to these Standards will enable these responsibilitiesto be fulfilled.
Audience
The Standards are addressed to all health care providers,private and public, who care for persons with proventuberculosis or with symptoms and signs suggestive oftuberculosis. In general, providers in national tuberculosisprograms that follow existing international guidelines are incompliance with the Standards. However, in many instances(as described under Rationale) non-program clinicians (bothprivate and other state sector) do not have the guidance andsystematic evaluation of outcomes provided by controlprograms and, commonly, would not be in compliance withthe Standards. Thus, although program providers are notexempt from adherence to the Standards, the emphasis is onthe non-program providers as the target audience.
In addition to health care providers, both patients andcommunities are part of the intended audience. Patients areincreasingly aware of and expect that their care will measureup to a high standard. Having generally agreed uponstandards will empower patients to evaluate the quality ofcare they are being provided. Good care for individuals withtuberculosis is also in the best interest of the community.Community contributions to tuberculosis care and controlare increasingly important in raising public awareness of thedisease, providing treatment support, reducing the stigmaassociated with having tuberculosis, and demanding thathealth care providers in the community adhere to a highstandard of tuberculosis care.3 The community should expectthat standards of care will be provided and that, within thecommunity, care for tuberculosis will be up to the acceptedstandard.
Scope
Three categories of activities are addressed by the Standards:diagnosis, treatment, and public health responsibilities of allproviders. Specific prevention approaches, laboratoryperformance, and personnel standards are not addressed.The Standards are intended to be consistent with, andcomplementary to, local and national tuberculosis controlpolicies that are consistent with World Health Organizationrecommendations: they are not intended to replace local
guidelines and were written to accommodate local differencesin practice. They focus on the contribution that good clinicalcare of individual patients with or suspected of havingtuberculosis makes to population-based tuberculosis control.In reducing the suffering and economic losses fromtuberculosis, a balanced approach emphasizing both individualpatient care and public health principles of disease control isessential.
To meet the requirements of the Standards, approachesand strategies, determined by local circumstances and practicesand developed in collaboration with local and national publichealth authorities, will be necessary. Moreover, there are manysituations in which the level of care can, and should, gobeyond what is specified in these standards. Local conditions,practices, and resources also will determine the degree towhich this is the case.
The Standards do not address the extremely importantconcern with overall access to care. Obviously, if there is nocare available, the quality of care is not relevant. Additionally,there are many factors that impede access even when care isavailable: poverty, gender, and geography are prominentamong the factors that interfere with persons availingthemselves to care. Also, however, if the residents of a givenarea perceive that the quality of care provided by the localfacility(ies) is substandard, they will not seek care there. Thisperception of quality is a component of access that adherenceto these standards will address.1
Also not addressed by the Standards is the necessity ofhaving a sound, effective government tuberculosis controlprogram. The requirements of such programs are describedin a number of international recommendations from the WorldHealth Organization (WHO) and the International UnionAgainst Tuberculosis and Lung Disease (IUATLD). Havingan effective control program at the national or local levelwith linkages to non-program providers enables bidirectionalcommunication of information including case notification,consultation, patient referral, and in some instances, provisionof drugs or services such as treatment supervision/support forprivate patients. In addition the program may be the onlyprovider of laboratory services that enables the diagnosticstandards to me met.
Rationale
Although in the past decade there has been substantialprogress in the development and implementation of thestrategies necessary for effective global tuberculosis control,the disease remains an enormous and growing global healthproblem.4-7 One-third of the world's population is infected

Appendices 17
with Mycobacterium tuberculosis, mostly in developingcountries where 95 percent of cases occur.5 In 2003, therewere an estimated 8.8 million new cases of tuberculosis, ofwhich 3.9 million were sputum smear-positive and, thus,highly infectious.6 Alarmingly, the number of tuberculosis casesthat occur in the world each year is still growing, although therate of increase is slowing.6 In the African region of the WorldHealth Organization (WHO) the tuberculosis case ratecontinues to increase, both because of the epidemic of HIVinfection in sub-Saharan countries and the poor or absentprimary care services throughout the region.4,6 In EasternEurope after a decade of increases, case rates have onlyrecently reached a plateau, the increases being attributed tothe collapse of the public health infrastructure, increasedpoverty, and other socioeconomic factors complicated furtherby the high prevalence of drug resistant tuberculosis.4,7 Inmany other countries tuberculosis case rates are either stagnantor decreasing more slowly than should be expected becauseof incomplete application of effective care and controlmeasures. At least in part, the failure to bring about a morerapid reduction in tuberculosis incidence relates to a failureto fully engage non-tuberculosis control program providers inthe provision of high quality care that would contribute totuberculosis control.
It is now widely recognized that many providers areinvolved in the diagnosis and treatment of tuberculosis.8-11
Traditional healers, general practitioners, specialist physicians,nurses, clinical officers, academic physicians, unqualifiedpractitioners, physicians in private practice, practitioners ofalternative medicine, and community organizations, amongothers, all play roles in tuberculosis care and, therefore, intuberculosis control. In addition, other public providers suchas those working in prisons, army hospitals, or in generalpublic hospitals and facilities regularly evaluate personssuspected of having tuberculosis and treat patients who havethe disease.
Little is known about the quality of care delivered by non-program providers, but evidence from studies conducted inmany different parts of the world show great variability in thequality of tuberculosis care and poor quality care continuesto plague global tuberculosis control efforts.1 Findings of arecent global situation assessment by the WHO suggestedthat delays in diagnosis were common.10 The delay was moreoften in receiving a diagnosis rather than in seeking care,although both elements are important.12 This survey and otherstudies also show that clinicians, in particular those who workin the private health care sector, often deviate from standard,internationally recommended, tuberculosis management
practices.9,10 These deviations include under-use of sputummicroscopy for diagnosis, generally associated with over-reliance on radiography, and use of inappropriate drugregimens with incorrect combinations of drugs and mistakesin both drug dosage and duration of treatment, and failure tosupervise and assure adherence to treatment.9,10,13-19 Anecdotalevidence also suggests that there is over-reliance on poorlyvalidated or inappropriate diagnostic tests such as serologicassays, often in preference to conventional bacteriologicalevaluations.
Together, these findings highlight flaws in the health caresystem that lead to substandard tuberculosis care forpopulations that, often, are most vulnerable to the diseaseand are least able to bear the consequences of such systemicfailures. Any person anywhere in the world who is unable toaccess quality health care should be considered vulnerable totuberculosis and its consequences.1 Likewise, any communitywith no or inadequate access to appropriate diagnostic andtreatment services for tuberculosis is a vulnerable community.1
The initiative aimed at developing International Standardsfor Tuberculosis Care i is an attempt to reduce vulnerabilityof individuals and communities to tuberculosis by promotinghigh quality care for persons with, or suspected of having,tuberculosis.
Companion and Reference Documents
The standards in this document should be seen as beingcomplimentary to two other important companion documents.The first, Patients Charter of the Tuberculosis Communitythat specifies the rights and responsibilities of patients, is beingdeveloped in tandem with this document. Second, theInternational Council of Nurses has developed a set ofstandards, TB/MDR-TB Nursing Standards (www.icn.ch/tb/standards.htm) that define in detail the critical roles andresponsibilities of nurses in the care and control of tuberculosis.
As a single-source reference for many of the practices fortuberculosis care, we would refer the reader to "Toman'sTuberculosis: Case Detection, Treatment, and Monitoring.(second edition).20
There are many sets of guidelines and recommendationson various aspects of tuberculosis care and control (see http:// w w w . g f m e r . c h / P r e s e n t a t i o n s _ E n / P d f / T Bpercent20Guidelines_Statements_Ver8_Feb2005.pdf). Thecurrent document draws from many of these documents toprovide the evidence upon which these standards are based.In particular we have used guidelines that have gained generalacceptance by virtue of the process by which they weredeveloped and by their broad use. However, the existing

18 Practical Approach in Tuberculosis Management
documents do not present standards that define the acceptablelevel of care in such a way as to enable assessment of theadequacy of care by patients themselves, by communities,and by public health authorities.
In providing the evidence base for the Standards, ingeneral, we have cited summaries, meta-analyses, andsystematic reviews of evidence that have examined andsynthesized primary data. Throughout the document we haveused the terminology recommended in the "RevisedInternational Definitions in Tuberculosis Control."21
STANDARDS FOR DIAGNOSIS
Standard 1
All persons with otherwise unexplained productive cough lastingtwo-three weeks or more should be evaluated for tuberculosis.
Rationale and Evidence Summary
The most common symptom of pulmonary tuberculosis ispersistent productive cough, often accompanied by systemicsymptoms, such as fever, night sweats, and weight loss. Inaddition, findings, such as lymphadenopathy, consistent withconcurrent extra-pulmonary tuberculosis, may be noted,especially in patients with HIV infection.
Although most patients with pulmonary tuberculosis havecough, the symptom is not specific to tuberculosis; it canoccur in a wide range of respiratory conditions, including acuterespiratory tract infections, asthma and chronic obstructivepulmonary disease. In general, acute respiratory tract infectionsresolve within a 2 to 3 week period, whereas, cough causedby tuberculosis and by chronic respiratory conditions persists.Although the presence of cough for 2 to 3 weeks is verynonspecific, traditionally, having cough of this duration hasserved as the criterion for defining suspected tuberculosis andis used in most national and international guidelines,particularly in areas of moderate to high prevalence oftuberculosis.20-23
In a recent survey conducted in primary health care servicesof 9 low and middle-income countries, respiratory complaints,including cough constituted on average 18.4 percent ofsymptoms that prompted a visit to a health center for personsolder than 5 years of age. Of this group 5 percent of patients,overall, were categorized as possibly having tuberculosisbecause of the presence of an unexplained cough for morethan 2 to 3 weeks.24 Other studies have shown that 4 to 10percent of adults attending out-patient health facilities indeveloping countries may have a persistent cough of morethan 2 to 3 weeks' duration.25 This percentage varies somewhat
depending on whether there is active questioning concerningthe presence of cough. Respiratory conditions, therefore,constitute a substantial proportion of the burden of diseasesin patients presenting to primary health care services.24,25
Data from India, Algeria and Chile generally show thatthe percentage of patients with positive sputum smearsincreases with increasing duration of cough from 1 to 2 weeks,increasing to 3 to 4, and >4 weeks.26 However, even patientswith shorter duration of cough in these studies had anappreciable prevalence of tuberculosis. A more recentassessment from India demonstrated that by using a thresholdof >2 weeks to prompt collection of sputum specimens thenumber of patients with suspected tuberculosis increased by61 percent but, more importantly, the number of tuberculosiscases identified increased by 46 percent compared with athreshold of >3 weeks.27 The results also suggested thatactively inquiring as to the presence of cough in all adultclinic attendees may increase the yield of cases; 7 percent ofpatients who on questioning had cough ≥ 2 weeks had positivesmears, compared with 15 percent who, without prompting,volunteered that they had cough.27
Choosing a threshold of 2 to 3 weeks is an obviouscompromise, and it should be recognized that, while usingthis threshold reduces the clinic and laboratory workload,some cases would be missed. In patients presenting withchronic cough, the proportion of cases attributable totuberculosis will depend on the prevalence of tuberculosis inthe community.25 In countries with a low prevalence oftuberculosis, it is likely that chronic cough will be due toconditions other than tuberculosis. On the other hand, inhigh prevalence countries, tuberculosis will be one of theleading diagnoses to consider together with other conditions,such as asthma, bronchitis and bronchiectasis that arecommon in many areas.
Overall, by focusing on adults and children presentingwith chronic cough, the chances of identifying patients withpulmonary tuberculosis are maximized. Unfortunately, studiessuggest that not all patients with respiratory symptoms receivean adequate evaluation for tuberculosis.10,13,15-18,28 Thesediagnostic delays that miss opportunities for earlier detectionof tuberculosis lead to increased disease severity for the patientsand a greater likelihood of transmission of the infection in thecommunity.
Standard 2
For all patients (adults, adolescents, and children who arecapable of producing sputum) suspected of having pulmonarytuberculosis, at least two and, preferably, three sputumspecimens should be obtained for microscopic examination.

Appendices 19
Rationale and Evidence Summary
Because tuberculosis is caused by a bacterial pathogen, toprove the diagnosis every effort must be made to identify thecausative agent. Ideally, this includes isolation ofMycobacterium tuberculosis complex from specimens fromany suspected site of disease. A microbiological diagnosiscan only be confirmed by culturing M. tuberculosis or M.bovis (or under appropriate circumstances, identifying specificnucleic acid sequences in a clinical specimen). In practice,however, there are many settings in which culture is not feasiblecurrently. Fortunately, microscopic examination of stainedsputum is feasible in nearly all settings, and the diagnosis oftuberculosis can be strongly inferred by finding acid-fast bacilliby microscopic examination. In nearly all clinicalcircumstances in high prevalence areas, finding acid-fast bacilliin stained sputum is highly specific and, thus, is the equivalentof a confirmed diagnosis. In addition to being highly specificfor M. tuberculosis, identification of acid-fast bacilli bymicroscopic examination is particularly important for threereasons: it is the most rapid method for determining if a personhas tuberculosis; it identifies persons who are at greatest riskof dying from the disease*; and it identifies the most potenttransmitters of infection.
Failure to perform a proper diagnostic evaluation beforeinitiating treatment potentially exposes the patient to the risksof unnecessary or wrong treatment with no benefit. Moreover,such an approach may delay accurate diagnosis and propertreatment. This standard applies to adults, adolescents andchildren. With proper instruction and supervision many childrenfive years of age and older can generate a specimen.Adolescents, although often classified as children, at leastuntil the age of 15 years, can generally produce sputum.Thus, age alone should not be a reason for not attempting toobtain a sputum specimen from a child or adolescent.
The information summarized below describes the resultsof various approaches to sputum collection, processing andexamination. The application of the information to actualpractices and policies should be guided by local considerations.
The optimum number of sputum specimens to establisha diagnosis has been examined in a number of studies. In arecent review of data from a number of sourcesit was statedthat, on average, the initial specimen was positive in about83 to 87 percent of all patients ultimately found to haveacid-fast bacilli detected, in 10 to 12 percent with the secondspecimen, and 3 to 5 percent on the third specimen.32 Anotherongoing systematic review (Mase et al, unpublished data) of>20 studies on this topic showed that, on average, the firstsmear detected about 82 percent of smear-positive cases,and the second detected 14 percent of all cases. The thirdsmear identified about 4 percent of all smear-positive TBcases.
A recent reanalysis of data from a study involving 42laboratories in four high burden countries showed that theincremental yield from a third serial smear ranged from 0.7percent to 7.2 percent.33 Thus, it appears that in a diagnosticevaluation for tuberculosis, at least two specimens should beobtained. In some settings, because of practicality andlogistics, a third specimen may be useful, but examination ofmore than three specimens adds minimally to the number ofpositive specimens obtained. In addition, a third specimen isuseful as confirmatory evidence if only one of the first twosmears is positive. Ideally, the results of sputum microscopyshould be returned to the clinician within no more than oneworking day from submission of the specimen. The timing ofspecimens is also important. The yield is greatest from earlymorning (overnight) specimens.34-36 Thus, although it is notpractical to collect only early morning specimens, at leastone specimen should be from an early morning collection.A variety of methods have been used to improve theperformance of sputum smear microscopy. Angeby andcolleagues reviewed the evidence on the use of bleach toliquefy mucus followed by centrifugation to concentratesputum.37 They found that this method was associated witha statistically significant increase in proportion of positive testsor sensitivity of microscopy in 15 of 19 studies reviewed.37
Another systematic review of 21 studies reporting results ofvarious methods of concentration showed that, on average,
* It should be noted that in persons with HIV infection, mortality rates are greater in patients with clinically-diagnosed tubercu-losis who have negative sputum smears than among HIV-infected patients who have positive sputum smears.29. Harries AD, Hargreaves NJ, Kemp J, et al. Deaths from tuberculosis in sub-Saharan African countries with a high prevalenceof HIV-1. Lancet 2001;357(9267):1519-23,30. Maher D, Harries A, Getahun H. Tuberculosis and HIV interaction in sub-Saharan Africa: impact on patients and programmes;implications for policies. Trop Med Int Health 2005;10(8):734-42,31. Mukadi YD, Maher D, Harries A. Tuberculosis case fatality rates in high HIV prevalence populations in sub-Saharan Africa.Aids 2001;15(2):143-52.

20 Practical Approach in Tuberculosis Management
the sensitivity of microscopy (as compared to culture) washigher with concentration by centrifugation and/orsedimentation (usually after pre-treatment with chemicals suchas bleach, NAOH, and NaLC), as compared to direct smearmicroscopy.38 Fifteen of 21 studies demonstrated that,compared with direct smear, concentration increased thesensitivity by more than 20 percent. This review also evaluateddata from 38 studies that reported information enablinganalysis of the positivity rate (proportion of positive smears)for both the direct and concentrated smears and, thus,incremental yield. The average increase in positivity rate was5 percent, with 11 of 38 studies (29%) demonstrating anincrease in positivity rate of the concentrated smear of morethan 15 percent over direct smear.38
The results of this review have been verified in a morecomprehensive systematic review of 83 studies on the effectof various physical and/or chemical methods of concentratingsputum prior to microscopy.39 The results, althoughheterogeneous and difficult to summarize, indicate that in amajority of the studies, concentration resulted in a highersensitivity and smear-positivity rate, when compared to direct(unconcentrated) smears. Sedimentation with Ziehl-Neelsen(ZN) stain plus a chemical (N = 5 studies) demonstrated thegreatest effect, average increase in sensitivity about 25 percent(range, +2 to +36%) with all studies showing an increaseafter concentration. Studies using ZN stain and centrifugationwith a chemical (N = 16 studies) showed an average increasein sensitivity of approximately 10 percent (range, -59% to+39%), with about 80 percent of studies noting an increase.For studies using ZN stain and bleach (N = 9 studies), with orwithout a physical method, there was about a 10 percentincrease in sensitivity (range, 0 to 38%), with about 80 percentof studies noting an increase. An improvement was also foundusing bleach, with or without a physical method, in 22 studiesin which the outcome measure was incremental yield, averageincrease 7 percent (range, -4% to +21%), with over 90 percentof studies showing an increase. Studies utilizing bleach andcentrifugation together (N = 5 studies) demonstrated anaverage increase in sensitivity of about 15 percent (range,+1% to 38%), with all studies showing an increase insensitivity following concentration. However, a limitation ofthis review was the inability to clearly distinguish the impactof chemical and physical processes on concentration.39
Fluorescence microscopy, in which auramine-basedstaining causes the acid-fast bacilli to fluoresce against a darkbackground, is widely used in many parts of the world. Asystematic review, in which the performance of direct sputumsmear microscopy using fluorescence staining was comparedwith Ziehl-Neelsen staining using culture as the gold standard,
suggests that fluorescence microscopy is the more sensitivemethod.40 Both methods have a high degree of specificity.The combination of increased sensitivity with no loss ofspecificity makes fluorescence microscopy a more accuratetest, although the increased cost and complexity might makeit less applicable in many areas. For this reason fluorescencestaining is best used in centers with specifically trainedmicroscopists, in which a large number of specimens areprocessed daily.
Standard 3
For all patients (adults, adolescents, and children) suspectedof having extra-pulmonary tuberculosis, appropriate specimensfrom the suspected sites of involvement should be obtainedfor microscopy and, where facilities and resources areavailable, for culture and histopathological examination.
Rationale and Evidence Summary
Extra-pulmonary tuberculosis accounts for 15 to 20 percentof tuberculosis in populations with a low prevalence of HIVinfection. In populations with a high prevalence of HIVinfection, the proportion with extra-pulmonary tuberculosis ishigher. Because appropriate specimens may be difficult toobtain from some of these sites, bacteriological confirmationof extrapulmonary tuberculosis is often more difficult thanpulmonary tuberculosis. In spite of the difficulties, however,the basic principle that bacteriological confirmation of thediagnosis should be sought still holds. Generally, there arefewer M. tuberculosis organisms present in extra-pulmonarysites so identification of acid-fast bacilli in specimens fromthese sites is less frequent and culture is more important. Forexample, microscopic examination of pleural fluid intuberculous pleuritis detects acid-fast bacilli in only about 5to 10 percent of cases, and the diagnostic yield is similarlylow in tuberculous meningitis. Given the low yield ofmicroscopy, both culture and histopathological examinationof tissue specimens, such as are obtained by needle biopsy oflymph nodes, are important diagnostic tests. In addition tothe collection of specimens from the sites of suspectedtuberculosis, examination of sputum may also be useful,especially in patients with HIV infection, in whom there is anappreciable frequency of subclinical pulmonary tuberculosis.41
Standard 4
All persons with chest radiographic findings suggestive oftuberculosis should have sputum specimens submitted formicrobiological examination.

Appendices 21
Rationale and Evidence Summary
Chest radiography is a sensitive but nonspecific test to detecttuberculosis.42 Radiographic examination (film or fluoroscopy)of the thorax or other suspected sites of involvement may beuseful to identify persons for further evaluation. However, adiagnosis of tuberculosis cannot be established by radiographyalone. Reliance on the chest radiograph as the only diagnostictest for tuberculosis will result in both over- diagnosis oftuberculosis and missed diagnoses of tuberculosis and otherdiseases. As summarized,43 in a study from India44 in which2,229 outpatients were examined by photofluorography, 227were classified as having tuberculosis. Of the 227, 81 (36%)had negative sputum cultures, whereas, of the remaining 2002patients 31 (1.5%) had positive cultures. Looking at theseresults in terms of the sensitivity of chest radiography 32 (20%)of 162 culture positive cases would have been missed byradiography. Given these and other data, it is clear that theuse of radiographic examinations alone to "diagnose"tuberculosis is not an acceptable practice.
Chest radiography is useful to evaluate persons who havenegative sputum smears to attempt to find evidence forpulmonary tuberculosis and to identify other diseases thatmay be responsible for the symptoms. Its diagnostic utility isbest when applied as part of a diagnostic algorithm in theinvestigation of possible sputum smear-negative tuberculosis.(see standard 5).
Standard 5
The diagnosis of sputum smear-negative pulmonarytuberculosis should be based on the following criteria: at leastthree negative sputum smears (including at least one earlymorning specimen); chest radiography findings consistent withtuberculosis; and lack of response to a trial of broad-spectrumantimicrobial agents (NOTE: Because the fluoroquinolonesare active against Mycobacterium tuberculosis and, thus, maycause transient improvement, they should be avoided.). Forsuch patients if facilities for culture are available, sputumcultures should be obtained. In persons with known or suspectedHIV infection the diagnostic evaluation should be expedited.
Rationale and Evidence Summary
The designation of "sputum smear-negative tuberculosis"presents a difficult diagnostic dilemma. As noted above, onaverage sputum microscopy is only about 50-60 percentsensitive when compared with culture. Nevertheless, giventhe nonspecific nature of the symptoms of tuberculosis andthe multiplicity of other diseases that could be the cause of
the patient's illness, it is important that a rigorous approachbe taken in diagnosing tuberculosis in a patient in whom atleast three adequate sputum smears are negative. Becausepatients with HIV infection and tuberculosis frequently havenegative sputum smears, and because of the broad differentialdiagnosis for the respiratory symptoms in this group, such asystematic approach is crucial. It is important, however, tobalance the need for a systematic approach in order to avoidboth over-and under-diagnosis of tuberculosis with the needfor prompt treatment in a patient with an illness that isprogressing rapidly. Over-diagnosis of tuberculosis when theillness has another cause will delay proper diagnosis andtreatment, whereas, under-diagnosis will lead to more severeconsequences of tuberculosis, including disability and possiblydeath, as well as ongoing transmission of the infection.
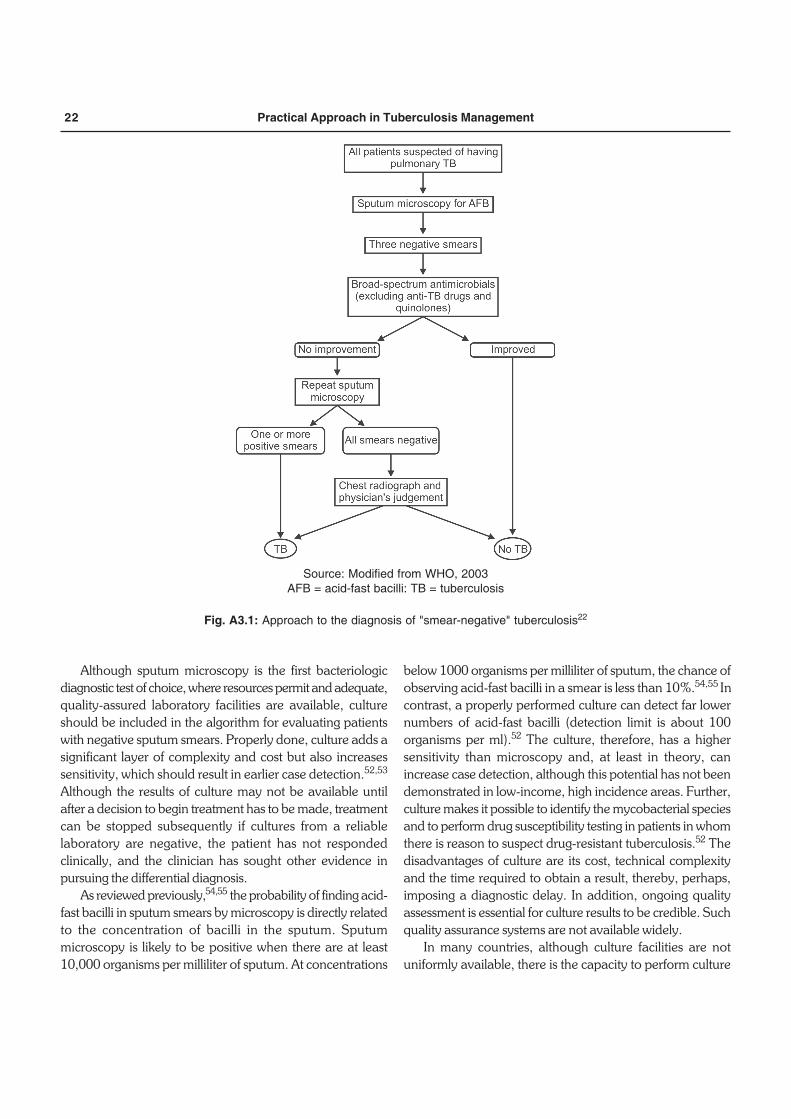
A number of algorithms have been developed as a meansof systematizing the diagnosis of smear-negative tuberculosis,although none has been adequately validated under fieldconditions.45,46 In particular there is little information orexperience on which to base approaches to the diagnosis ofsmear-negative tuberculosis in persons with HIV infection.Figure A3.1 is modified from an algorithm developed by WHOand is included, as an example of a systematic approach.22 Itshould be recognized that, commonly, the steps in thealgorithm are not followed in a sequential fashion by a singleprovider. The algorithm should be viewed as presenting anidealized approach to diagnosis.
There are several points of caution regarding the algorithm.First, completion of all of the steps in the algorithm requires asubstantial amount of time; thus, it should not be used forpatients with rapidly progressive illness. This is especially truein patients with HIV infection in whom tuberculosis may berapidly progressive. Second, several studies have shown thatpatients with tuberculosis may respond, at least transiently,to broad spectrum antimicrobial treatment.47-50 Obviously,such a response will lead one to delay a diagnosis oftuberculosis. Fluoroquinolones, in particular, have abactericidal activity against M. tuberculosis. Empiricfluoroquinolone monotherapy has been associated with delaysin initiation of appropriate antituberculosis therapy and alsoacquired resistance to the fluoroquinolones.51 Third, theapproach outlined in the algorithm may be quite costly to thepatient and deter her/him from continuing with the diagnosticevaluation. Given all these concerns, application of such analgorithm in patients with at least three negative sputum smearexaminations must be done in a flexible manner. Ideally, theevaluation of "smear-negative tuberculosis" should be guidedby locally-validated approaches, suited to local conditions.
22 Practical Approach in Tuberculosis Management
Although sputum microscopy is the first bacteriologicdiagnostic test of choice, where resources permit and adequate,quality-assured laboratory facilities are available, cultureshould be included in the algorithm for evaluating patientswith negative sputum smears. Properly done, culture adds asignificant layer of complexity and cost but also increasessensitivity, which should result in earlier case detection.52,53
Although the results of culture may not be available untilafter a decision to begin treatment has to be made, treatmentcan be stopped subsequently if cultures from a reliablelaboratory are negative, the patient has not respondedclinically, and the clinician has sought other evidence inpursuing the differential diagnosis.
As reviewed previously,54,55 the probability of finding acid-fast bacilli in sputum smears by microscopy is directly relatedto the concentration of bacilli in the sputum. Sputummicroscopy is likely to be positive when there are at least10,000 organisms per milliliter of sputum. At concentrations
below 1000 organisms per milliliter of sputum, the chance ofobserving acid-fast bacilli in a smear is less than 10%.54,55 Incontrast, a properly performed culture can detect far lowernumbers of acid-fast bacilli (detection limit is about 100organisms per ml).52 The culture, therefore, has a highersensitivity than microscopy and, at least in theory, canincrease case detection, although this potential has not beendemonstrated in low-income, high incidence areas. Further,culture makes it possible to identify the mycobacterial speciesand to perform drug susceptibility testing in patients in whomthere is reason to suspect drug-resistant tuberculosis.52 Thedisadvantages of culture are its cost, technical complexityand the time required to obtain a result, thereby, perhaps,imposing a diagnostic delay. In addition, ongoing qualityassessment is essential for culture results to be credible. Suchquality assurance systems are not available widely.
In many countries, although culture facilities are notuniformly available, there is the capacity to perform culture
Source: Modified from WHO, 2003AFB = acid-fast bacilli: TB = tuberculosis
Fig. A3.1: Approach to the diagnosis of "smear-negative" tuberculosis22

Appendices 23
in some areas. Providers should be aware of the local capacityand use the resources appropriately, especially for theevaluation of persons suspected of having tuberculosis whohave negative sputum smears and for persons suspected ofhaving tuberculosis caused by drug resistant organisms.
Traditional culture methods use solid media such asLowenstein-Jensen and Ogawa. Cultures on solid media areless technology-intensive and the media can be made locally.However, the time to identify growth is significantly longerthan in liquid media. Liquid media systems such as BACTEC®
utilize the release of radioactive CO2 from C-14 labeledpalmitic acid in the media to identify growth. The MGIT®
system, also using liquid medium, has the advantage of havinggrowth detected by the appearance of color in the growthmedium, thereby avoiding radioactivity. Decisions to provideculture facilities for diagnosing tuberculosis depend on financialresources, trained personnel, and the ready availability ofreagents and equipment service.
Nucleic acid amplification tests (NAATs), although widelydistributed, do not offer major advantages over culture atthis time. Although a positive result can be obtained morequickly than with any of the culture methods, the NAATs arenot sufficiently sensitive for a negative result to excludetuberculosis.56-59 In addition, they are not sufficiently sensitiveto be useful in identifying M. tuberculosis in specimens fromextra pulmonary sites of disease.57-59 Moreover, cultures mustbe available if drug susceptibility testing is to be performed.
Other approaches to establishing a diagnosis oftuberculosis, such as serological tests, are not of proven valueand should not be used in routine practice.56
Standard 6
The diagnosis of intrathoracic (i.e. pulmonary, pleural, andlymph node [mediastinal and/or hilar]) tuberculosis insymptomatic children with negative sputum smears is basedon the finding of chest radiographic abnormalities consistentwith tuberculosis, and either a history of exposure to aninfectious case or evidence of tuberculosis infection (positivetuberculin skin test or interferon gamma release assay). Forsuch patients, if facilities for culture are available, sputumspecimens should be obtained (by expectoration, gastricwashings, or induced sputum) for culture.
Rationale and Evidence Summary
Children with tuberculosis commonly have paucibacillarydisease without evident lung cavitation but with involvementof intrathoracic lymph nodes. Consequently, sputum smears
are more likely to be negative and cultures of sputum or otherspecimens, radiographic examination of the chest and teststo detect tuberculous infection are of relatively greaterimportance. Because many children less than five years ofage generally do not cough and produce sputum effectively,culture of gastric washings obtained by naso-gastric tubelavage has a higher yield than sputum.60
Several recent reviews have examined the effectiveness ofvarious diagnostic tools, scoring systems and algorithms todiagnose tuberculosis in children.60-63 Many of theseapproaches are poorly standardized, not well validated, and,thus, of limited applicability. Table A3.1 presents the approachrecommended by the Integrated Management of ChildhoodIllness (IMCI) program of WHO which is widely used in first-level facilities in low and middle-income countries.64
STANDARDS FOR TREATMENT
Standard 7
Any care provider treating a patient for tuberculosis is assuminga public health function that includes not only prescribing anappropriate regimen but also ensuring adherence to theregimen until treatment is completed.
Table A3.1: An approach to the diagnosis of tuberculosisin children64
The risk of tuberculosis is increased when there is an active case(infectious, smear-positive tuberculosis) in the same house, orwhen the child is malnourished, has HIV/AIDS, or has had measlesin the past few months. Consider tuberculosis in any child with:• A history of:
– unexplained weight loss or failure to grow normally;– unexplained fever, especially when it continues for more
than 2 weeks;– chronic cough;– exposure to an adult with probable or definite pulmonary
infectious tuberculosis.• On examination:
– fluid on one side of the chest (reduced air entry, stonydullness to percussion);
– enlarged non-tender lymph nodes or a lymph node abscess,especially in the neck;
– signs of meningitis, especially when these develop overseveral days and the spinal fluid contains mostlylymphocytes and elevated protein;
– abdominal swelling, with or without palpable lumps;– progressive swelling or deformity in the bone or a joint,
including the spine.
Source: Reproduced from WHO/FCH/CAH/00.1

24 Practical Approach in Tuberculosis Management
Rationale and Evidence Summary
As described in the Introduction, the main interventions toprevent the spread of tuberculosis in the community are thedetection of patients with infectious tuberculosis and providingthem with effective treatment to ensure a rapid and lastingcure. Consequently, treatment for tuberculosis is not only amatter of individual health, such as is provided by, for example,treatment of hypertension or diabetes mellitus, it is a matterof public health. Thus, all providers, public and private, whoundertake to treat a patient with tuberculosis, must have theknowledge to prescribe an appropriate treatment regimen andthe means to ensure adherence to the regimen until treatmentis completed.65 Communities and patients deserve to beassured that providers treating tuberculosis are doing so inaccordance with this principle and are, thereby, meeting thisstandard.
Standard 8
All patients (including those with HIV infection) who havenot been treated previously should receive an internationallyaccepted first line treatment regimen using drugs of knownbioavailability. The initial phase should consist of two monthsof isoniazid, rifampicin, pyrazinamide and ethambutol.* Thepreferred continuation phase consists of isoniazid andrifampicin given for 4 months. Isoniazid and ethambutol givenfor 6 months is an alternative continuation phase regimenbut is associated with a higher rate of failure and relapse,especially in patients with HIV infection.
The doses of antituberculosis drugs used should conformto international recommendations.
Rationale and Evidence Summary
A large number of well-designed clinical trials have providedthe evidence base for this standard and several sets oftreatment recommendations based on these studies have beenwritten in the past few years.22,23,65 These data will not be re-reviewed in this document. All of the data indicate that arifampicin-containing regimen is the backbone ofantituberculosis chemotherapy and is highly effective in treatingtuberculosis caused by drug-susceptible M. tuberculosis. It isalso clear from the studies that the minimum duration oftreatment for smear and/or culture-positive tuberculosis is sixmonths. For the six-month duration to be maximally effective,
the regimen must include pyrazinamide during the initial two-month phase and rifampicin must be included throughoutthe full six months. There are several variations of the regimens,especially in the frequency of drug administration, that havebeen shown to produce acceptable results.22,23,65
Although regimens of less than six months have beenevaluated in clinical trials, a Cochrane systematic review onthis topic,66 and amore recent review 67 found that regimensless than six months have an unacceptably high rate of relapse.The current worldwide standard, therefore, is a six-monthregimen.22,65 Although the six-month regimen is preferable,an alternative continuation phase regimen is isoniazid andethambutol given for six months (the total duration oftreatment, therefore, is eight months); however, this regimenis associated with a higher rate of failure and relapse, especiallyin patients with HIV infection.68,69 Nevertheless the eight-month regimen may be used when adherence to treatmentthroughout the continuation phase cannot be assured.22 Therationale for this approach is that if the patient is non-adherent,at least sensitivity to rifampicin will be preserved. A review ofthe outcomes of treatment of tuberculosis in patients withHIV infection clearly shows that tuberculosis relapse isminimized by the use of a regimen containing rifampicinthroughout a six-month course.68 Thus, the six month regimencontaining rifampin throughout the entire course is preferablein patients with HIV infection to minimize the risk of relapse;however, the patient's HIV stage, the need for, and availabilityof, antiretroviral drugs, and the quality of treatment supervision/support must be considered in choosing an appropriatecontinuation phase of therapy.
Intermittent administration of antituberculosis drugsenables supervision to be provided more efficiently andeconomically with no reduction in efficacy. The evidence oneffectiveness of intermittent regimens has been reviewedrecently.70,71 These reviews, based on several trials,72-77 suggestthat anti-tuberculosis treatment may be given intermittentlyeither three times or twice weekly without apparent loss ofeffectiveness. However, the WHO and The International UnionAgainst Tuberculosis and Lung Disease (Union) do notrecommend the use of twice-weekly intermittent regimensbecause missing one of the two doses results in insufficienttreatment.22,23,78 A simplified version of the current WHOrecommendations for treating persons who have not beentreated previously is shown in Table A3.2.22
* Ethambutol may be omitted in the initial phase of treatment for adults and children who have negative sputum smears, do nothave extensive pulmonary tuberculosis or severe forms of extrapulmonary disease and who are known to be HIV-negative.
Appendices 25
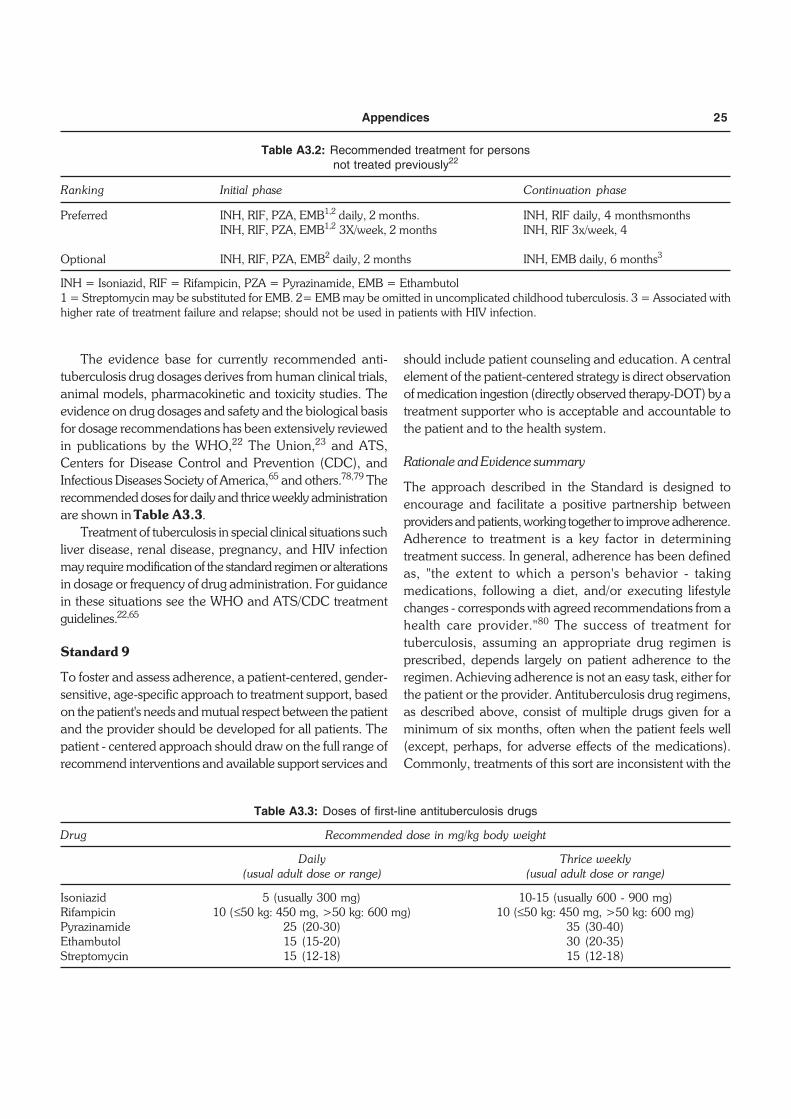
The evidence base for currently recommended anti-tuberculosis drug dosages derives from human clinical trials,animal models, pharmacokinetic and toxicity studies. Theevidence on drug dosages and safety and the biological basisfor dosage recommendations has been extensively reviewedin publications by the WHO,22 The Union,23 and ATS,Centers for Disease Control and Prevention (CDC), andInfectious Diseases Society of America,65 and others.78,79 Therecommended doses for daily and thrice weekly administrationare shown in Table A3.3.
Treatment of tuberculosis in special clinical situations suchliver disease, renal disease, pregnancy, and HIV infectionmay require modification of the standard regimen or alterationsin dosage or frequency of drug administration. For guidancein these situations see the WHO and ATS/CDC treatmentguidelines.22,65
Standard 9
To foster and assess adherence, a patient-centered, gender-sensitive, age-specific approach to treatment support, basedon the patient's needs and mutual respect between the patientand the provider should be developed for all patients. Thepatient - centered approach should draw on the full range ofrecommend interventions and available support services and
should include patient counseling and education. A centralelement of the patient-centered strategy is direct observationof medication ingestion (directly observed therapy-DOT) by atreatment supporter who is acceptable and accountable tothe patient and to the health system.
Rationale and Evidence summary
The approach described in the Standard is designed toencourage and facilitate a positive partnership betweenproviders and patients, working together to improve adherence.Adherence to treatment is a key factor in determiningtreatment success. In general, adherence has been definedas, "the extent to which a person's behavior - takingmedications, following a diet, and/or executing lifestylechanges - corresponds with agreed recommendations from ahealth care provider."80 The success of treatment fortuberculosis, assuming an appropriate drug regimen isprescribed, depends largely on patient adherence to theregimen. Achieving adherence is not an easy task, either forthe patient or the provider. Antituberculosis drug regimens,as described above, consist of multiple drugs given for aminimum of six months, often when the patient feels well(except, perhaps, for adverse effects of the medications).Commonly, treatments of this sort are inconsistent with the
Table A3.2: Recommended treatment for personsnot treated previously22
Ranking Initial phase Continuation phase
Preferred INH, RIF, PZA, EMB1,2 daily, 2 months. INH, RIF daily, 4 monthsmonthsINH, RIF, PZA, EMB1,2 3X/week, 2 months INH, RIF 3x/week, 4
Optional INH, RIF, PZA, EMB2 daily, 2 months INH, EMB daily, 6 months3
INH = Isoniazid, RIF = Rifampicin, PZA = Pyrazinamide, EMB = Ethambutol1 = Streptomycin may be substituted for EMB. 2= EMB may be omitted in uncomplicated childhood tuberculosis. 3 = Associated withhigher rate of treatment failure and relapse; should not be used in patients with HIV infection.
Table A3.3: Doses of first-line antituberculosis drugs
Drug Recommended dose in mg/kg body weight
Daily Thrice weekly(usual adult dose or range) (usual adult dose or range)
Isoniazid 5 (usually 300 mg) 10-15 (usually 600 - 900 mg)Rifampicin 10 (≤50 kg: 450 mg, >50 kg: 600 mg) 10 (≤50 kg: 450 mg, >50 kg: 600 mg)Pyrazinamide 25 (20-30) 35 (30-40)Ethambutol 15 (15-20) 30 (20-35)Streptomycin 15 (12-18) 15 (12-18)
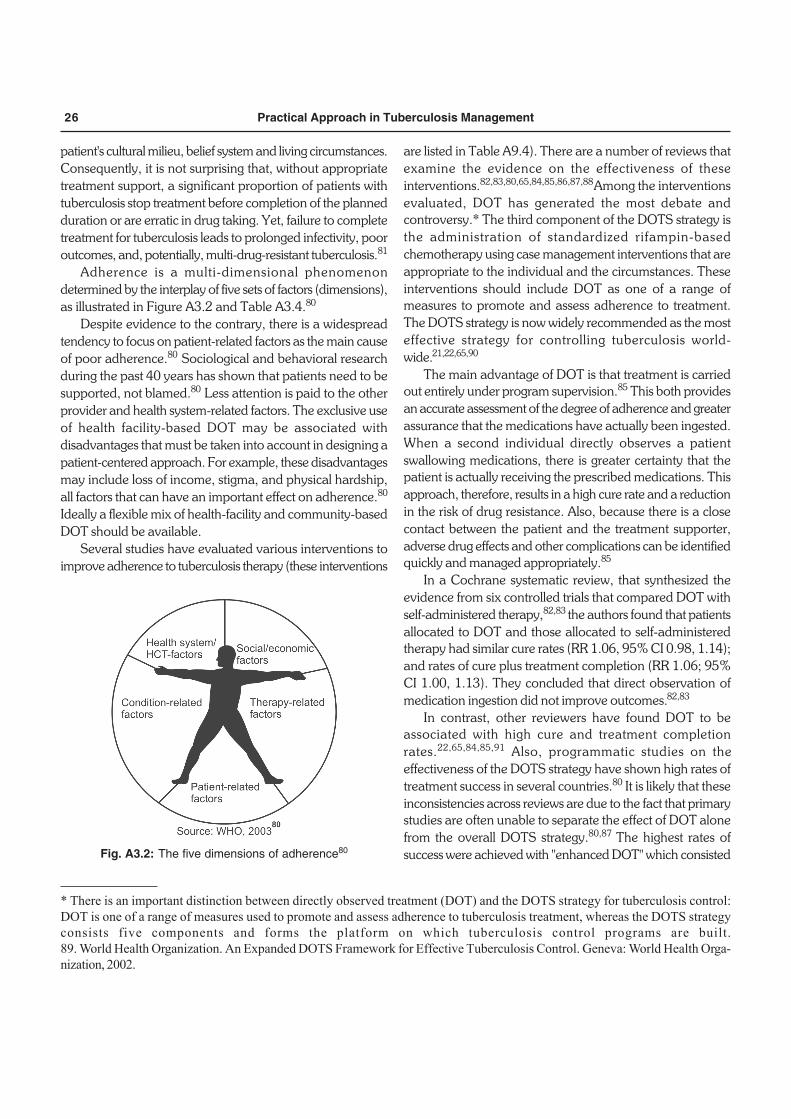
26 Practical Approach in Tuberculosis Management
patient's cultural milieu, belief system and living circumstances.Consequently, it is not surprising that, without appropriatetreatment support, a significant proportion of patients withtuberculosis stop treatment before completion of the plannedduration or are erratic in drug taking. Yet, failure to completetreatment for tuberculosis leads to prolonged infectivity, pooroutcomes, and, potentially, multi-drug-resistant tuberculosis.81
Adherence is a multi-dimensional phenomenondetermined by the interplay of five sets of factors (dimensions),as illustrated in Figure A3.2 and Table A3.4.80
Despite evidence to the contrary, there is a widespreadtendency to focus on patient-related factors as the main causeof poor adherence.80 Sociological and behavioral researchduring the past 40 years has shown that patients need to besupported, not blamed.80 Less attention is paid to the otherprovider and health system-related factors. The exclusive useof health facility-based DOT may be associated withdisadvantages that must be taken into account in designing apatient-centered approach. For example, these disadvantagesmay include loss of income, stigma, and physical hardship,all factors that can have an important effect on adherence.80
Ideally a flexible mix of health-facility and community-basedDOT should be available.
Several studies have evaluated various interventions toimprove adherence to tuberculosis therapy (these interventions
are listed in Table A9.4). There are a number of reviews thatexamine the evidence on the effectiveness of theseinterventions.82,83,80,65,84,85,86,87,88 Among the interventionsevaluated, DOT has generated the most debate andcontroversy.* The third component of the DOTS strategy isthe administration of standardized rifampin-basedchemotherapy using case management interventions that areappropriate to the individual and the circumstances. Theseinterventions should include DOT as one of a range ofmeasures to promote and assess adherence to treatment.The DOTS strategy is now widely recommended as the mosteffective strategy for controlling tuberculosis world-wide.21,22,65,90
The main advantage of DOT is that treatment is carriedout entirely under program supervision.85 This both providesan accurate assessment of the degree of adherence and greaterassurance that the medications have actually been ingested.When a second individual directly observes a patientswallowing medications, there is greater certainty that thepatient is actually receiving the prescribed medications. Thisapproach, therefore, results in a high cure rate and a reductionin the risk of drug resistance. Also, because there is a closecontact between the patient and the treatment supporter,adverse drug effects and other complications can be identifiedquickly and managed appropriately.85
In a Cochrane systematic review, that synthesized theevidence from six controlled trials that compared DOT withself-administered therapy,82,83 the authors found that patientsallocated to DOT and those allocated to self-administeredtherapy had similar cure rates (RR 1.06, 95% CI 0.98, 1.14);and rates of cure plus treatment completion (RR 1.06; 95%CI 1.00, 1.13). They concluded that direct observation ofmedication ingestion did not improve outcomes.82,83
In contrast, other reviewers have found DOT to beassociated with high cure and treatment completionrates.22,65,84,85,91 Also, programmatic studies on theeffectiveness of the DOTS strategy have shown high rates oftreatment success in several countries.80 It is likely that theseinconsistencies across reviews are due to the fact that primarystudies are often unable to separate the effect of DOT alonefrom the overall DOTS strategy.80,87 The highest rates ofsuccess were achieved with "enhanced DOT" which consistedFig. A3.2: The five dimensions of adherence80
* There is an important distinction between directly observed treatment (DOT) and the DOTS strategy for tuberculosis control:DOT is one of a range of measures used to promote and assess adherence to tuberculosis treatment, whereas the DOTS strategyconsists five components and forms the platform on which tuberculosis control programs are built.89. World Health Organization. An Expanded DOTS Framework for Effective Tuberculosis Control. Geneva: World Health Orga-nization, 2002.
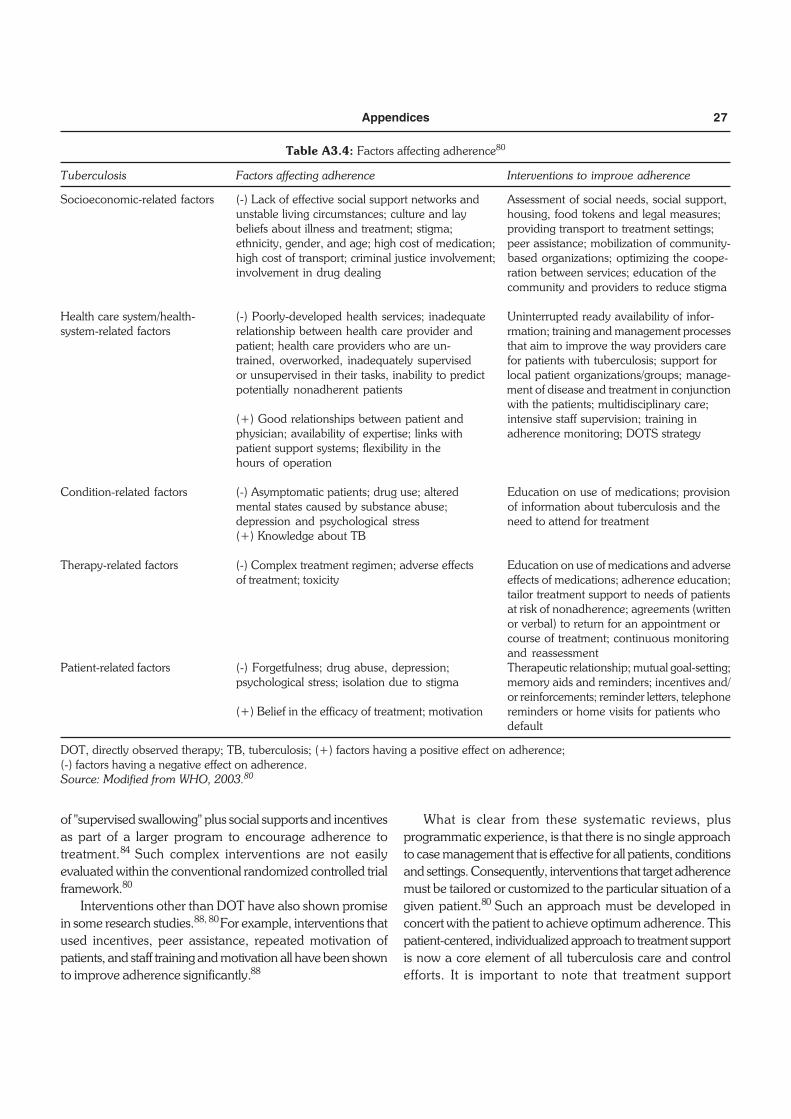
Appendices 27
of "supervised swallowing" plus social supports and incentivesas part of a larger program to encourage adherence totreatment.84 Such complex interventions are not easilyevaluated within the conventional randomized controlled trialframework.80
Interventions other than DOT have also shown promisein some research studies.88, 80 For example, interventions thatused incentives, peer assistance, repeated motivation ofpatients, and staff training and motivation all have been shownto improve adherence significantly.88
What is clear from these systematic reviews, plusprogrammatic experience, is that there is no single approachto case management that is effective for all patients, conditionsand settings. Consequently, interventions that target adherencemust be tailored or customized to the particular situation of agiven patient.80 Such an approach must be developed inconcert with the patient to achieve optimum adherence. Thispatient-centered, individualized approach to treatment supportis now a core element of all tuberculosis care and controlefforts. It is important to note that treatment support
Table A3.4: Factors affecting adherence80
Tuberculosis Factors affecting adherence Interventions to improve adherence
Socioeconomic-related factors (-) Lack of effective social support networks and Assessment of social needs, social support,unstable living circumstances; culture and lay housing, food tokens and legal measures;beliefs about illness and treatment; stigma; providing transport to treatment settings;ethnicity, gender, and age; high cost of medication; peer assistance; mobilization of community-high cost of transport; criminal justice involvement; based organizations; optimizing the coope-involvement in drug dealing ration between services; education of the
community and providers to reduce stigma
Health care system/health- (-) Poorly-developed health services; inadequate Uninterrupted ready availability of infor-system-related factors relationship between health care provider and rmation; training and management processes
patient; health care providers who are un- that aim to improve the way providers caretrained, overworked, inadequately supervised for patients with tuberculosis; support foror unsupervised in their tasks, inability to predict local patient organizations/groups; manage-potentially nonadherent patients ment of disease and treatment in conjunction
with the patients; multidisciplinary care;(+) Good relationships between patient and intensive staff supervision; training inphysician; availability of expertise; links with adherence monitoring; DOTS strategypatient support systems; flexibility in thehours of operation
Condition-related factors (-) Asymptomatic patients; drug use; altered Education on use of medications; provisionmental states caused by substance abuse; of information about tuberculosis and thedepression and psychological stress need to attend for treatment(+) Knowledge about TB
Therapy-related factors (-) Complex treatment regimen; adverse effects Education on use of medications and adverseof treatment; toxicity effects of medications; adherence education;
tailor treatment support to needs of patientsat risk of nonadherence; agreements (writtenor verbal) to return for an appointment orcourse of treatment; continuous monitoringand reassessment
Patient-related factors (-) Forgetfulness; drug abuse, depression; Therapeutic relationship; mutual goal-setting;psychological stress; isolation due to stigma memory aids and reminders; incentives and/
or reinforcements; reminder letters, telephone(+) Belief in the efficacy of treatment; motivation reminders or home visits for patients who
default
DOT, directly observed therapy; TB, tuberculosis; (+) factors having a positive effect on adherence;(-) factors having a negative effect on adherence.Source: Modified from WHO, 2003.80

28 Practical Approach in Tuberculosis Management
measures, and not the treatment regimen itself, must beindividualized to suit the unique needs of the patient.
In addition to one-on-one support for patients beingtreated for tuberculosis, community support is also ofimportance in creating a therapeutic milieu and reducingstigma.3 Not only should the community, as noted above,expect that optimum treatment for tuberculosis is beingprovided, but, also, the community should expect that thepatient will adhere to the prescribed regimen and recognizethat they have a role in ensuring adherence.
Standard 10
All patients should be monitored for response to therapy,best judged in patients with pulmonary tuberculosis by follow-up sputum microscopy (two specimens) at least at the timeof completion of the initial phase of treatment (two - threemonths), at five months, and at the end of treatment. Patientswho have positive smears during the 5th month of treatmentshould be considered as treatment failures and have therapymodified appropriately (see standards 14 and 15). In patientswith extra-pulmonary tuberculosis and in children, the responseto treatment is best assessed clinically. Follow-up radiographicexaminations are usually unnecessary and may be misleading.
Rationale and Evidence Summary
Patient monitoring and treatment supervision are two separatefunctions. Patient monitoring is necessary to evaluate theresponse of the disease to treatment and to identify adversedrug reactions. For the latter function contact between thepatient and a provider is necessary. To judge response ofpulmonary tuberculosis to treatment, the most expeditiousmethod is sputum smear microscopy. Ideally, where quality-assured laboratories are available, sputum cultures, as wellas smears, should be performed for monitoring.
Having a positive sputum smear at completion of fivemonths of treatment defines treatment failure, indicating theneed for determination of drug susceptibility and initiation ofa re-treatment regimen.21 Radiographic assessment, althoughused commonly, have been shown to be unreliable forevaluating response to treatment.92 Similarly, clinicalassessment can be unreliable and misleading in the monitoringof patients with pulmonary tuberculosis.92 In patients withextra-pulmonary tuberculosis and in children, clinicalevaluations may be the only available means of assessing theresponse to treatment.
Standard 11
A written record of all medications given, bacteriologicresponse, and adverse reactions should be maintained for allpatients.
Rationale and Evidence Summary
There is a sound rationale and clear benefits of a recordkeeping system.93 It is common for individual physicians tobelieve sincerely that a majority of the patients they initiateon anti-TB therapy are cured. However, when systematicallyevaluated, it is often seen that only a minority of patientshave successfully completed the full treatment.93 The recordingand reporting system enables targeted, individualized follow-up to identify patients who are failing therapy.93 It also helpsin facilitating continuity of care, particularly in settings (e.g.large hospitals) where the same clinician might not be seeingthe patient during every visit. A good record of medicationsgiven, results of investigations such as smears, cultures, andchest radiographs, and progress notes on clinical improvement,adverse events, and adherence will provide for more uniformmonitoring and ensure a high standard of care.
Records are important to provide continuity when patientsmove from one care provider to another and enable tracingof patients who miss appointments. In patients who defaultand then return for treatment, and patients who relapse aftertreatment completion, it is critical to review previous recordsin order to assess the likelihood of drug resistance. Lastly,management of complicated cases (e.g. multi-drug-resistanttuberculosis) is not possible without an adequate record ofprevious treatment, adverse events, and drug susceptibilityresults.
Standard 12
In areas with a high prevalence rate of HIV in the generalpopulation where tuberculosis and HIV are likely to co-exist,HIV counseling and testing is indicated for all tuberculosispatients as part of their routine management. In areas withlower prevalence rates of HIV, HIV counseling and testing isindicated for tuberculosis patients with symptoms and/or signsof HIV-related conditions, and in tuberculosis patients havinga history suggestive of high risk of HIV exposure.
Rationale and Evidence summary
Infection with HIV both increases the likelihood of progressionfrom infection with M. tuberculosis to active disease and

Appendices 29
changes the clinical manifestations of tuberculosis. A numberof studies have suggested that, in comparison with non-HIVinfected patients, patients with HIV infection who havepulmonary tuberculosis have a lower likelihood of having acid-fast bacilli detected by sputum smear microscopy. Moreover,data consistently show that the chest radiographic featuresare atypical and the proportion of extra pulmonary tuberculosisis greater in patients with advanced HIV infection comparedwith those who do not have HIV infection. Consequently,knowledge of a person's HIV status would influence theapproach to a diagnostic evaluation for tuberculosis. For thisreason it is important, particularly in areas in which there is ahigh prevalence of HIV infection, that the history and physicalexamination include a search for indicators that suggest thepresence of HIV infection. Table A3.5 presents clinical featuresthat are suggestive of HIV infection.94 A comprehensive listof clinical criteria/algorithms for HIV/AIDS diagnosis isavailable at: http://www.who.int/hiv/strategic/surveillance/definitions/en/
Tuberculosis is tightly linked to HIV infection worldwide.4Although the prevalence of HIV infection varies very widelyfrom country to country and within countries, among personswith HIV infection there is always an increased risk oftuberculosis. The variation in HIV prevalence means that avariable percentage of patients with tuberculosis will have
HIV infection as well. This ranges from well less than 1 percentin low HIV prevalence countries to 50-70 percent in countrieswith a high HIV prevalence, mostly sub-Saharan Africancountries.4 Even though in low HIV prevalence countries fewtuberculosis patients will be HIV infected, the connection issufficiently strong and the impact on the patient sufficientlygreat that the test should always be considered in managingindividual patients. In high HIV prevalence countries the yieldof positive results will be high and again, the impact of apositive result on the patient will be great. Thus, the indicationfor HIV testing is strong; co-infected patients may benefitthrough access to antiretroviral therapy as programs expandor through administration of co-trimoxazole for prevention ofopportunistic infections, even when antiretroviral drugs arenot available locally.94,95
Standard 13
Patients with tuberculosis and HIV infection who are notreceiving antiretroviral therapy should receive the sametuberculosis treatment regimen as those who do not haveHIV infection. All patients with tuberculosis and HIV infectionshould be evaluated to determine when they should receiveantiretroviral therapy. Appropriate arrangements for accessto antiretroviral drugs should be made for patients who meetindications for treatment. Given the complexity of co-administration of antituberculosis treatment and antiretroviraltherapy, consultation with a physician who is expert in thisarea is recommended before initiation of concurrent treatmentfor tuberculosis and HIV infection, regardless of which diseaseappeared first. However, initiation of treatment for tuberculosisshould not be delayed.
Rationale and Evidence Summary
The evidence on effectiveness of treatment for tuberculosis inpatients with HIV co-infection versus those who do not haveHIV infection has been reviewed extensively.22,65,68,94,96-99
These reviews suggest that, in general, the outcome oftreatment for tuberculosis is the same in HIV-infected andnon-HIV-infected patients with the notable exception thatdeath rates are greater among patients with HIV infection,presumably due in large part to complications of HIV infection.Thus, with two exceptions tuberculosis treatment regimensare the same for HIV-infected and non HIV-infected patients.The first exception is that thioacetazone is contraindicated inpatients with HIV infection. Thioacetazone is associated witha high risk of severe skin reactions in HIV-infected individualsand should not be used.22,94 Second, the results of treatment
Table A3.5: Clinical features suggestive of HIV infection inpatients with tuberculosis94
Past history • Sexually transmitted infections (STI)• Herpes zoster (shingles)• Recent or recurrent pneumonia• Severe bacterial infections• Recent treated tuberculosis
Symptoms • Weight loss (>10 kg or >20% of original weight)• Diarrhea (>1 month)• Retrosternal pain on swallowing (suggestive of
esophageal candidiasis)• Burning sensation of feet (peripheral sensory
neuropathy)Signs • Scar of herpes zoster
• Itchy popular skin rash• Kaposi sarcoma• Symmetrical generalized lymphadenopathy• Oral candidiasis• Angular cheilitis• Oral hairy leukoplakia• Necrotizing gingivitis• Giant aphthous ulceration• Persistent painful genital ulceration
Source: Modified from WHO, 200494

30 Practical Approach in Tuberculosis Management
are better if a rifampicin-containing regimen is used throughoutthe six-month course of treatment.68 Thus, the six monthregimen containing rifampin throughout the entire course ispreferable in patients with HIV infection to minimize the riskof relapse; however, the patient's HIV stage, the need for,and availability of, antiretroviral drugs, and the quality oftreatment supervision/support must be considered in choosingan appropriate continuation phase of therapy."
All patients with tuberculosis and HIV infection eithercurrently are or will at a point in the future be candidates forantiretroviral therapy. Antiretroviral therapy results in dramaticreductions in morbidity and mortality in HIV-infected personsand may improve the outcomes of treatment for tuberculosis.Highly active antiretroviral therapy (HAART) is the globalstandard of care.
In patients with HIV-related tuberculosis, treatingtuberculosis is the first priority. In the setting of advancedHIV infection, untreated tuberculosis can progress rapidly todeath. As noted above, however, antiretroviral treatment maybe lifesaving for patients with advanced HIV infection.Consequently, concurrent treatment may be necessary inpatients with advanced HIV disease (e.g. circulating CD4lymphocyte count <200/mm3). It should be emphasized,however, that treatment for tuberculosis should not beinterrupted in order to initiate antiretroviral therapy, and, inpatients with early stage HIV infection, it may be safer todefer antiretroviral treatment until at least the completion ofthe initial phase of tuberculosis treatment.94
There are a number of problems associated withconcomitant therapy for tuberculosis and HIV infection. Theseinclude overlapping toxicity profiles for the drugs used, drug-drug interactions (especially with rifamycins and proteaseinhibitors), and immune reconstitution reactions.65,94
Consequently, consultation with an expert in HIV managementis needed in deciding when to start antiretroviral drugs, theagents to use, and plan for monitoring for adverse reactionsand response to both therapies. (For a single-source referenceon the management of tuberculosis in patients with HIVinfection see the WHO manual TB/HIV: A Clinical Manual).94
Standard 14
An assessment of the likelihood of drug resistance, based onhistory of prior treatment, exposure to a possible source casehaving drug resistant organisms, and the communityprevalence of drug resistance, should be obtained for allpatients. Patients who fail treatment and chronic cases shouldalways be assessed for possible drug resistance. For patientsin whom drug resistance is considered to be likely, culture
and drug susceptibility testing for isoniazid, rifampin, andethambutol should be performed promptly.
Rationale and Evidence Summary
Drug resistance is largely man-made. Clinical errors thatcommonly lead to the emergence of drug resistance include:failure to provide effective treatment support and assuranceof adherence; failure to recognize and address patient non-adherence; inadequate drug regimens; adding a single newdrug to a failing regimen; and failure to recognize existingdrug resistance.100 In addition, co-morbid conditionsassociated with malabsorption or reduced serum levels ofanti-tuberculosis drugs (eg. rapid transit diarrhea, HIVpositivity, use of antifungal agents) may also lead to theacquisition of drug-resistance.100
Programmatic causes of drug resistance include drugshortages, poor-quality drugs and lack of policies andprocedures to prevent erratic drug intake.100 Patients with drug-resistant tuberculosis can spread the disease to their contacts.Transmission of drug resistant M. tuberculosis strains hasbeen well described in congregate settings and in susceptiblepopulations, notably HIV-infected persons.101-104 However,multiple drug resistant (MDR) tuberculosis (tuberculosis causedby organisms that are resistant to at least isoniazid andrifampin) may spread in the population at large as was shownin China, the Baltic States, and countries of the former SovietUnion.
The strongest risk factor for drug resistance is previousanti-tuberculosis treatment, as shown by the WHO/IUATLDGlobal Project on Anti-TB Drug Resistance Surveillance,started in 1994.105 In previously treated patients, the odds ofany resistance are at least 4-fold higher and that of MDR atleast 10-fold higher than in new (untreated) patients.105
Patients with chronic tuberculosis (sputum positive after re-treatment) and those who fail treatment (sputum-positive after5 months of treatment) are at highest risk of having MDR,especially if rifampicin was used throughout the course oftreatment.105 Persons who are in close contact with confirmedMDR tuberculosis patients, especially children and HIV-positiveindividuals, also are at high risk of being infected with MDRorganisms. In some closed settings prisoners, persons stayingin homeless shelters and certain categories of immigrants andmigrants are at increased risk of MDR-tuberculosis.100-105
Drug susceptibility testing (DST) to the first lineantituberculosis drugs should be performed only in specializedreference laboratories that participate in an ongoing, rigorousquality assurance program. First-line DST is currentlyrecommended for all patients with a history of previous anti-

Appendices 31
tuberculosis treatment: patients who have failed treatment,especially those who have failed a standardized retreatmentregimen, and chronic cases are the first priority.100 Patientswith tuberculosis who have been in close contact with knownMDR patients should also have routine DST. Although HIVhas not been conclusively shown as an independent risk factorfor drug resistance, MDR tuberculosis outbreaks in HIV settingsand well-described drug interactions leading to reduced serumlevels of rifampicin in the presence of several antiretroviraldrugs, warrant routine DST in all HIV-positive tuberculosispatients, resources permitting.100
Standard 15
Patients with MDR tuberculosis should be treated withspecialized regimens containing second-line anti-tuberculosisdrugs. At least four drugs to which the organisms are knownor presumed to be susceptible should be used and treatmentshould be given for at least 18 months. Patient centeredmeasures are required to ensure adherence. Consultation witha provider experienced in treatment of patients with MDRtuberculosis should be obtained.
Rationale and Evidence Summary
Definitive randomized controlled trials are nearly impossibleto conduct in MDR tuberculosis; consequently none have beenconducted. Current recommendations are therefore based onobservational studies, general microbiological and therapeuticprinciples, extrapolation from available evidence from pilotMDR tuberculosis treatment projects, and expert opinion.106,107
Three strategic options for treatment of MDR tuberculosis arecurrently recommended by WHO: these are standardizedregimens, empiric treatment and individualized treatmentregimens, based on local drug resistance patterns, the historyof use of second-line drugs and the availability of DST forfirst- and second-line anti-tuberculosis drugs.100 Basicprinciples involved in the design of any regimen include theuse of at least four drugs with either certain or highly likelyeffectiveness, drug administration at least six days a week,drug dosage determined by patient weight, the use of aninjectable agent (an aminoglycoside or capreomycin) for atleast six months, treatment duration of 18-24 months, anddirectly observed treatment throughout the treatment course.
Standardized treatment regimens are based onrepresentative drug-resistance surveillance data for specificpatient categories, with all patients in the same category gettingthe same regimen. Advantages include less dependency on
highly technical laboratories, less clinical expertise requiredto interpret DST results, simplified drug ordering and easieroperational implementation. A standardized approach isuseful in settings where second-line drugs have not been usedextensively and where resistance levels to these drugs areconsequently low or absent.
Empiric treatment regimens are commonly used in specificgroups of patients while the DST results are pending. Empiricregimens are strongly recommended to avoid clinicaldeterioration and prevent transmission of MDR tuberculosisto secondary cases,100 since most DST methods have aturnaround time of several months. However, once the resultsof DST are known, an empiric regimen may be changed toan individualized regimen.
Individualized treatment regimens (based on DST profilesand previous drug history of individual patients, or on thehistory of local patterns of drug utilization) have the advantageof avoiding toxic and expensive drugs to which the MDR strainis resistant. However, an individualized approach requiressubstantial human, financial and technical (laboratory)capacity. DST for second-line drugs are notoriously difficultto perform, largely because of drug instability and the factthat critical concentrations for defining drug resistance arevery close to the minimal inhibitory concentration (MIC) ofindividual drugs.108 Laboratory proficiency testing results arenot (yet) available for second-line drugs; as a result little canbe said about the reliability of DST for these drugs.105,108
Clinicians treating MDR tuberculosis patients must be awareof these limitations and interpret DST results with this in mind.
Current WHO recommendations for treatment of MDRtuberculosis can be found at (http://www.who.int/tb/en/).100
MDR tuberculosis treatment is a complex health interventionand medical practitioners are strongly advised to consultcolleagues experienced in the management of these patients.
STANDARDS FOR PUBLIC HEALTHRESPONSIBILITIES
Standard 16
All providers of care for patients with tuberculosis should ensurethat close contacts (especially children under 5 years of ageand persons with HIV infection) to patients with infectioustuberculosis are evaluated and managed in line withinternational recommendations. Children under 5 years ofage and persons with HIV infection who have been in contactwith an infectious case should be evaluated for both latentinfection with M. tuberculosis and for active tuberculosis.

32 Practical Approach in Tuberculosis Management
Rationale and Evidence Summary
The risk of acquiring infection with M. tuberculosis correlateswith intensity and duration of exposure to a patient withinfectious tuberculosis. Close contacts of patients withtuberculosis, therefore, are at high risk for acquiring theinfection. Contact investigation is considered an importantactivity, both to find persons with previously undetectedtuberculosis and persons who are candidates for treatment oflatent tuberculosis infection.109,110
The potential yield of contact investigation in high andlow incidence settings has been reviewed previously.109,110 Inlow incidence settings (e.g. USA), it has been found that, onaverage, 5-10 contacts are identified for each incidenttuberculosis case. Of these, about 30 percent are found tohave latent tuberculosis infection, and another 1 to 4 percentwill have active truberculosis.109,111,112 Much higher rates ofboth latent infection and active disease have been reportedin high incidence countries, where about 50 percent ofhousehold contacts have latent infection, and about 10-20percent have active tuberculosis at the time of initialinvestigation.110 A recent systematic review of more than 50studies on household contact investigations in high incidencesettings showed that, on average, about 6 percent (range0.5% to 29%; N= 40 studies) of the contacts were found tohave active tuberculosis.113 The median number of householdcontacts needed to screen to find one case of activetuberculosis was 19 (range 14-300).113 The median proportionof contacts found to have latent infection was 49 percent(range: 7.3 to 90%; N= 34 studies).113 The median numberof contacts needed to be screened to find one case of latentinfection was 2 (range 1-14).113 Evidence from this reviewsuggests that contact investigation in high incidence settingsmay be a high yield strategy for case finding.
Among close contacts, there are certain subgroups thatare particularly at high risk for acquiring the infection andprogressing rapidly to active disease - children and personswith HIV infection. Children (particularly those under the ageof five years) are a vulnerable group because of the highlikelihood of progressing from latent infection to active disease.Children are also more likely to develop disseminated andserious forms of tuberculosis (e.g. TB meningitis). The Union,therefore, recommends that children under the age of fiveyears living in the same household as a sputum smear-positivetuberculosis patient should be targeted for preventive therapy(after evaluation shows no evidence of active disease).110
Similarly, contacts with HIV infection are at substantiallygreater risk for progressing to active tuberculosis.
Unfortunately, lack of adequate staff and resources in manyareas makes contact investigation impractical orimpossible.61,110 This results in missed opportunities to preventadditional cases of tuberculosis, especially among children.Thus, in many areas more energetic efforts are necessary toovercome these barriers.
Standard 17
All providers must report both new and retreatment tuberculosiscases and their treatment outcomes to local public healthauthorities, in conformance with applicable legal requirementsand policies.
Rationale and Evidence Summary
Reporting of tuberculosis cases to the tuberculosis controlprogram is an essential public health function, and in manycountries is legally mandated. This enables a determinationof the overall effectiveness of tuberculosis control programs,of resource needs, and of the distribution and dynamics ofthe disease within the population as a whole. In most countries,tuberculosis is a reportable disease. A system of recordingand reporting information on tuberculosis cases and theirtreatment outcomes is one of the key elements of the DOTSstrategy.93 Such a system is useful not only to monitor progressand treatment outcomes of individual patients, but also toevaluate the overall performance of the tuberculosis controlprograms, at the local, national, and global levels.93
The recording and reporting system allows for targeted,individualized follow-up to help patients who are not makingadequate progress (i.e. failing therapy).93 The system alsoallows for evaluation of the performance of the clinician, thehospital or institution, local health system, and the countryas a whole. Finally, a system of recording and reportingensures accountability.
RESEARCH AND REVIEW NEEDS
As part of the process of developing the InternationalStandards for Tuberculosis Care, several key areas that requireadditional research and further evaluation were identified(Table A3.6). Systematic reviews and research studies ( someof which are underway currently) in these areas are critical togenerate evidence to support rational and evidence-based careand control of tuberculosis. Research in these operationaland clinical areas serves to complement the ongoing effortsthat are focused on developing new tools for tuberculosiscontrol - new diagnostics,114 drugs,115 and vaccines.116
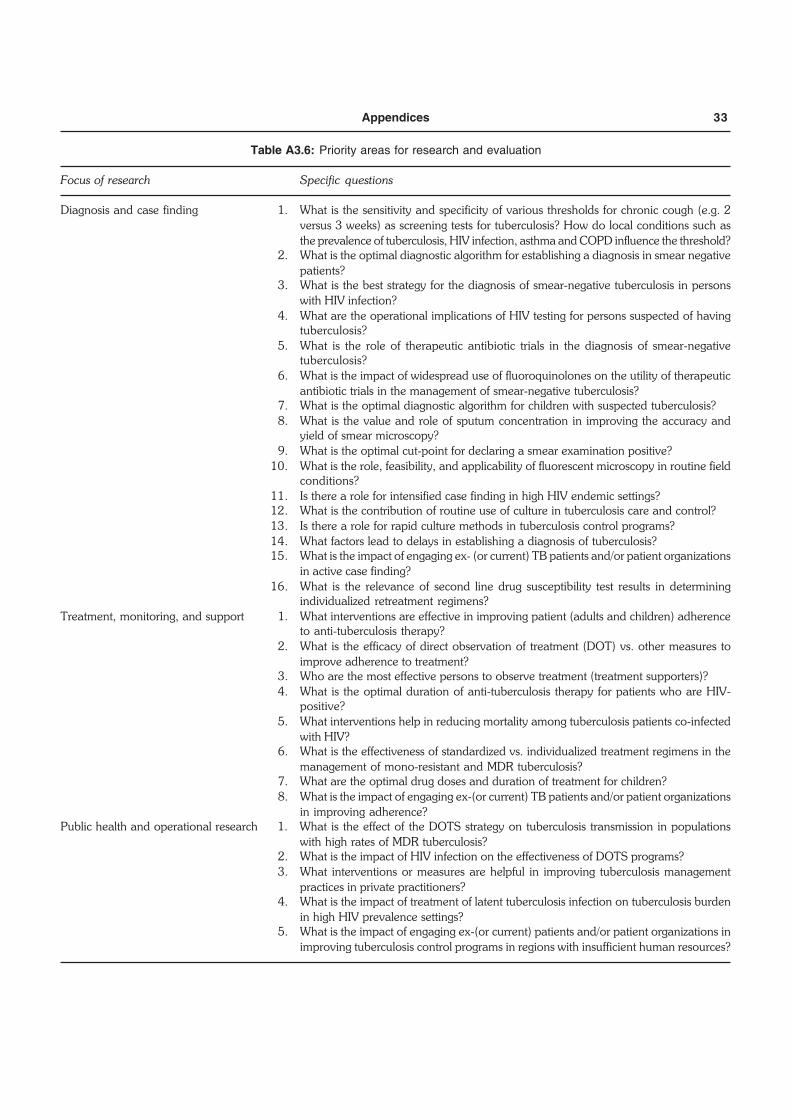
Appendices 33
Table A3.6: Priority areas for research and evaluation
Focus of research Specific questions
Diagnosis and case finding 1. What is the sensitivity and specificity of various thresholds for chronic cough (e.g. 2versus 3 weeks) as screening tests for tuberculosis? How do local conditions such asthe prevalence of tuberculosis, HIV infection, asthma and COPD influence the threshold?
2. What is the optimal diagnostic algorithm for establishing a diagnosis in smear negativepatients?
3. What is the best strategy for the diagnosis of smear-negative tuberculosis in personswith HIV infection?
4. What are the operational implications of HIV testing for persons suspected of havingtuberculosis?
5. What is the role of therapeutic antibiotic trials in the diagnosis of smear-negativetuberculosis?
6. What is the impact of widespread use of fluoroquinolones on the utility of therapeuticantibiotic trials in the management of smear-negative tuberculosis?
7. What is the optimal diagnostic algorithm for children with suspected tuberculosis?8. What is the value and role of sputum concentration in improving the accuracy and
yield of smear microscopy?9. What is the optimal cut-point for declaring a smear examination positive?
10. What is the role, feasibility, and applicability of fluorescent microscopy in routine fieldconditions?
11. Is there a role for intensified case finding in high HIV endemic settings?12. What is the contribution of routine use of culture in tuberculosis care and control?13. Is there a role for rapid culture methods in tuberculosis control programs?14. What factors lead to delays in establishing a diagnosis of tuberculosis?15. What is the impact of engaging ex- (or current) TB patients and/or patient organizations
in active case finding?16. What is the relevance of second line drug susceptibility test results in determining
individualized retreatment regimens?Treatment, monitoring, and support 1. What interventions are effective in improving patient (adults and children) adherence
to anti-tuberculosis therapy?2. What is the efficacy of direct observation of treatment (DOT) vs. other measures to
improve adherence to treatment?3. Who are the most effective persons to observe treatment (treatment supporters)?4. What is the optimal duration of anti-tuberculosis therapy for patients who are HIV-
positive?5. What interventions help in reducing mortality among tuberculosis patients co-infected
with HIV?6. What is the effectiveness of standardized vs. individualized treatment regimens in the
management of mono-resistant and MDR tuberculosis?7. What are the optimal drug doses and duration of treatment for children?8. What is the impact of engaging ex-(or current) TB patients and/or patient organizations
in improving adherence?Public health and operational research 1. What is the effect of the DOTS strategy on tuberculosis transmission in populations
with high rates of MDR tuberculosis?2. What is the impact of HIV infection on the effectiveness of DOTS programs?3. What interventions or measures are helpful in improving tuberculosis management
practices in private practitioners?4. What is the impact of treatment of latent tuberculosis infection on tuberculosis burden
in high HIV prevalence settings?5. What is the impact of engaging ex-(or current) patients and/or patient organizations in
improving tuberculosis control programs in regions with insufficient human resources?
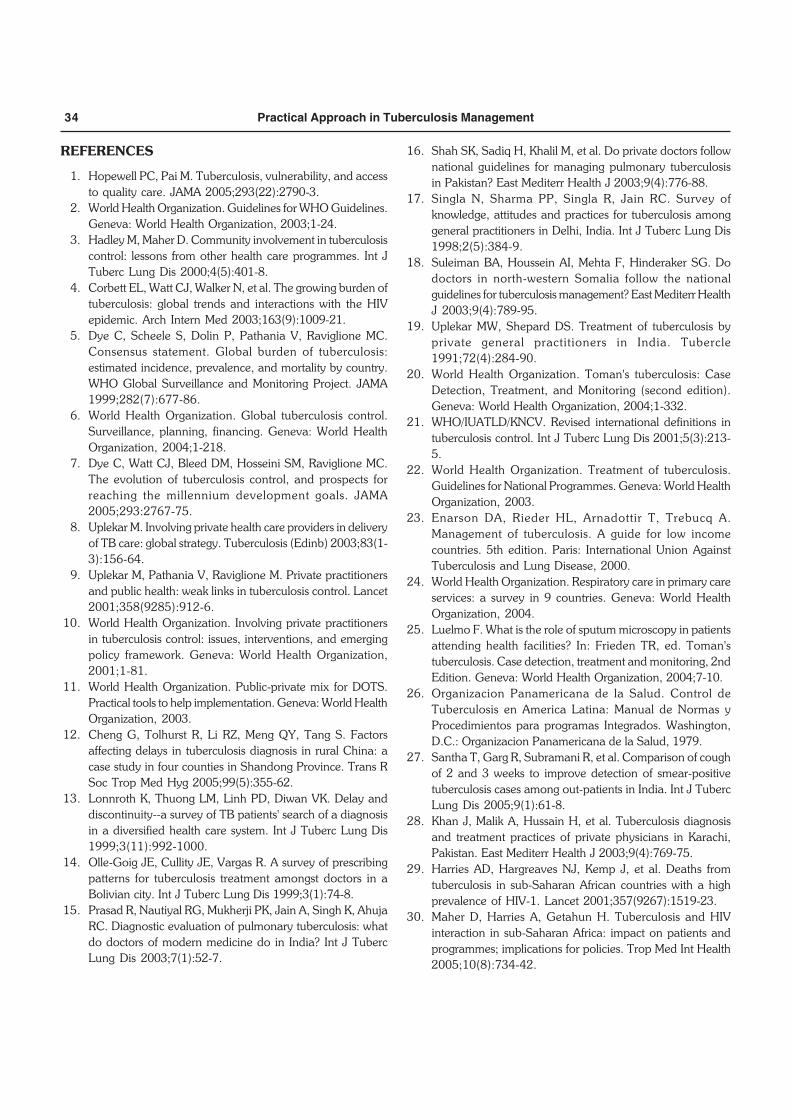
34 Practical Approach in Tuberculosis Management
REFERENCES
1. Hopewell PC, Pai M. Tuberculosis, vulnerability, and accessto quality care. JAMA 2005;293(22):2790-3.
2. World Health Organization. Guidelines for WHO Guidelines.Geneva: World Health Organization, 2003;1-24.
3. Hadley M, Maher D. Community involvement in tuberculosiscontrol: lessons from other health care programmes. Int JTuberc Lung Dis 2000;4(5):401-8.
4. Corbett EL, Watt CJ, Walker N, et al. The growing burden oftuberculosis: global trends and interactions with the HIVepidemic. Arch Intern Med 2003;163(9):1009-21.
5. Dye C, Scheele S, Dolin P, Pathania V, Raviglione MC.Consensus statement. Global burden of tuberculosis:estimated incidence, prevalence, and mortality by country.WHO Global Surveillance and Monitoring Project. JAMA1999;282(7):677-86.
6. World Health Organization. Global tuberculosis control.Surveillance, planning, financing. Geneva: World HealthOrganization, 2004;1-218.
7. Dye C, Watt CJ, Bleed DM, Hosseini SM, Raviglione MC.The evolution of tuberculosis control, and prospects forreaching the millennium development goals. JAMA2005;293:2767-75.
8. Uplekar M. Involving private health care providers in deliveryof TB care: global strategy. Tuberculosis (Edinb) 2003;83(1-3):156-64.
9. Uplekar M, Pathania V, Raviglione M. Private practitionersand public health: weak links in tuberculosis control. Lancet2001;358(9285):912-6.
10. World Health Organization. Involving private practitionersin tuberculosis control: issues, interventions, and emergingpolicy framework. Geneva: World Health Organization,2001;1-81.
11. World Health Organization. Public-private mix for DOTS.Practical tools to help implementation. Geneva: World HealthOrganization, 2003.
12. Cheng G, Tolhurst R, Li RZ, Meng QY, Tang S. Factorsaffecting delays in tuberculosis diagnosis in rural China: acase study in four counties in Shandong Province. Trans RSoc Trop Med Hyg 2005;99(5):355-62.
13. Lonnroth K, Thuong LM, Linh PD, Diwan VK. Delay anddiscontinuity--a survey of TB patients' search of a diagnosisin a diversified health care system. Int J Tuberc Lung Dis1999;3(11):992-1000.
14. Olle-Goig JE, Cullity JE, Vargas R. A survey of prescribingpatterns for tuberculosis treatment amongst doctors in aBolivian city. Int J Tuberc Lung Dis 1999;3(1):74-8.
15. Prasad R, Nautiyal RG, Mukherji PK, Jain A, Singh K, AhujaRC. Diagnostic evaluation of pulmonary tuberculosis: whatdo doctors of modern medicine do in India? Int J TubercLung Dis 2003;7(1):52-7.
16. Shah SK, Sadiq H, Khalil M, et al. Do private doctors follownational guidelines for managing pulmonary tuberculosisin Pakistan? East Mediterr Health J 2003;9(4):776-88.
17. Singla N, Sharma PP, Singla R, Jain RC. Survey ofknowledge, attitudes and practices for tuberculosis amonggeneral practitioners in Delhi, India. Int J Tuberc Lung Dis1998;2(5):384-9.
18. Suleiman BA, Houssein AI, Mehta F, Hinderaker SG. Dodoctors in north-western Somalia follow the nationalguidelines for tuberculosis management? East Mediterr HealthJ 2003;9(4):789-95.
19. Uplekar MW, Shepard DS. Treatment of tuberculosis byprivate general practitioners in India. Tubercle1991;72(4):284-90.
20. World Health Organization. Toman's tuberculosis: CaseDetection, Treatment, and Monitoring (second edition).Geneva: World Health Organization, 2004;1-332.
21. WHO/IUATLD/KNCV. Revised international definitions intuberculosis control. Int J Tuberc Lung Dis 2001;5(3):213-5.
22. World Health Organization. Treatment of tuberculosis.Guidelines for National Programmes. Geneva: World HealthOrganization, 2003.
23. Enarson DA, Rieder HL, Arnadottir T, Trebucq A.Management of tuberculosis. A guide for low incomecountries. 5th edition. Paris: International Union AgainstTuberculosis and Lung Disease, 2000.
24. World Health Organization. Respiratory care in primary careservices: a survey in 9 countries. Geneva: World HealthOrganization, 2004.
25. Luelmo F. What is the role of sputum microscopy in patientsattending health facilities? In: Frieden TR, ed. Toman'stuberculosis. Case detection, treatment and monitoring, 2ndEdition. Geneva: World Health Organization, 2004;7-10.
26. Organizacion Panamericana de la Salud. Control deTuberculosis en America Latina: Manual de Normas yProcedimientos para programas Integrados. Washington,D.C.: Organizacion Panamericana de la Salud, 1979.
27. Santha T, Garg R, Subramani R, et al. Comparison of coughof 2 and 3 weeks to improve detection of smear-positivetuberculosis cases among out-patients in India. Int J TubercLung Dis 2005;9(1):61-8.
28. Khan J, Malik A, Hussain H, et al. Tuberculosis diagnosisand treatment practices of private physicians in Karachi,Pakistan. East Mediterr Health J 2003;9(4):769-75.
29. Harries AD, Hargreaves NJ, Kemp J, et al. Deaths fromtuberculosis in sub-Saharan African countries with a highprevalence of HIV-1. Lancet 2001;357(9267):1519-23.
30. Maher D, Harries A, Getahun H. Tuberculosis and HIVinteraction in sub-Saharan Africa: impact on patients andprogrammes; implications for policies. Trop Med Int Health2005;10(8):734-42.
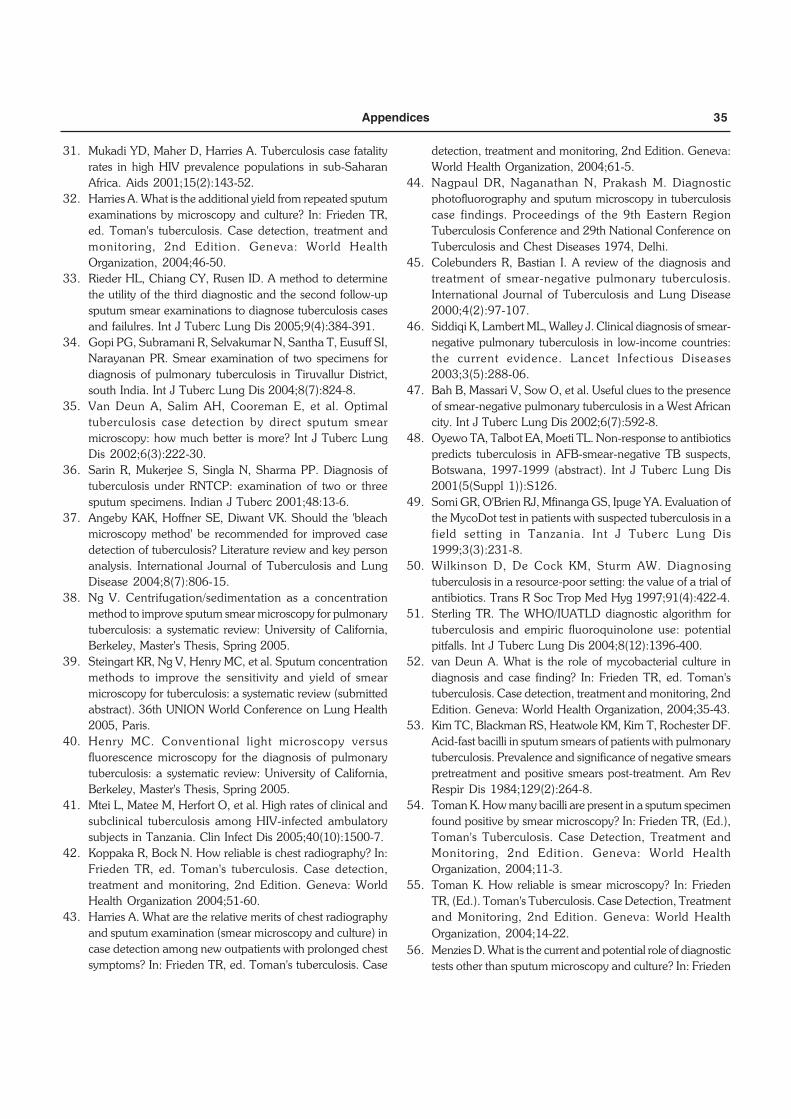
Appendices 35
31. Mukadi YD, Maher D, Harries A. Tuberculosis case fatalityrates in high HIV prevalence populations in sub-SaharanAfrica. Aids 2001;15(2):143-52.
32. Harries A. What is the additional yield from repeated sputumexaminations by microscopy and culture? In: Frieden TR,ed. Toman's tuberculosis. Case detection, treatment andmonitoring, 2nd Edition. Geneva: World HealthOrganization, 2004;46-50.
33. Rieder HL, Chiang CY, Rusen ID. A method to determinethe utility of the third diagnostic and the second follow-upsputum smear examinations to diagnose tuberculosis casesand failulres. Int J Tuberc Lung Dis 2005;9(4):384-391.
34. Gopi PG, Subramani R, Selvakumar N, Santha T, Eusuff SI,Narayanan PR. Smear examination of two specimens fordiagnosis of pulmonary tuberculosis in Tiruvallur District,south India. Int J Tuberc Lung Dis 2004;8(7):824-8.
35. Van Deun A, Salim AH, Cooreman E, et al. Optimaltuberculosis case detection by direct sputum smearmicroscopy: how much better is more? Int J Tuberc LungDis 2002;6(3):222-30.
36. Sarin R, Mukerjee S, Singla N, Sharma PP. Diagnosis oftuberculosis under RNTCP: examination of two or threesputum specimens. Indian J Tuberc 2001;48:13-6.
37. Angeby KAK, Hoffner SE, Diwant VK. Should the 'bleachmicroscopy method' be recommended for improved casedetection of tuberculosis? Literature review and key personanalysis. International Journal of Tuberculosis and LungDisease 2004;8(7):806-15.
38. Ng V. Centrifugation/sedimentation as a concentrationmethod to improve sputum smear microscopy for pulmonarytuberculosis: a systematic review: University of California,Berkeley, Master's Thesis, Spring 2005.
39. Steingart KR, Ng V, Henry MC, et al. Sputum concentrationmethods to improve the sensitivity and yield of smearmicroscopy for tuberculosis: a systematic review (submittedabstract). 36th UNION World Conference on Lung Health2005, Paris.
40. Henry MC. Conventional light microscopy versusfluorescence microscopy for the diagnosis of pulmonarytuberculosis: a systematic review: University of California,Berkeley, Master's Thesis, Spring 2005.
41. Mtei L, Matee M, Herfort O, et al. High rates of clinical andsubclinical tuberculosis among HIV-infected ambulatorysubjects in Tanzania. Clin Infect Dis 2005;40(10):1500-7.
42. Koppaka R, Bock N. How reliable is chest radiography? In:Frieden TR, ed. Toman's tuberculosis. Case detection,treatment and monitoring, 2nd Edition. Geneva: WorldHealth Organization 2004;51-60.
43. Harries A. What are the relative merits of chest radiographyand sputum examination (smear microscopy and culture) incase detection among new outpatients with prolonged chestsymptoms? In: Frieden TR, ed. Toman's tuberculosis. Case
detection, treatment and monitoring, 2nd Edition. Geneva:World Health Organization, 2004;61-5.
44. Nagpaul DR, Naganathan N, Prakash M. Diagnosticphotofluorography and sputum microscopy in tuberculosiscase findings. Proceedings of the 9th Eastern RegionTuberculosis Conference and 29th National Conference onTuberculosis and Chest Diseases 1974, Delhi.
45. Colebunders R, Bastian I. A review of the diagnosis andtreatment of smear-negative pulmonary tuberculosis.International Journal of Tuberculosis and Lung Disease2000;4(2):97-107.
46. Siddiqi K, Lambert ML, Walley J. Clinical diagnosis of smear-negative pulmonary tuberculosis in low-income countries:the current evidence. Lancet Infectious Diseases2003;3(5):288-06.
47. Bah B, Massari V, Sow O, et al. Useful clues to the presenceof smear-negative pulmonary tuberculosis in a West Africancity. Int J Tuberc Lung Dis 2002;6(7):592-8.
48. Oyewo TA, Talbot EA, Moeti TL. Non-response to antibioticspredicts tuberculosis in AFB-smear-negative TB suspects,Botswana, 1997-1999 (abstract). Int J Tuberc Lung Dis2001(5(Suppl 1)):S126.
49. Somi GR, O'Brien RJ, Mfinanga GS, Ipuge YA. Evaluation ofthe MycoDot test in patients with suspected tuberculosis in afield setting in Tanzania. Int J Tuberc Lung Dis1999;3(3):231-8.
50. Wilkinson D, De Cock KM, Sturm AW. Diagnosingtuberculosis in a resource-poor setting: the value of a trial ofantibiotics. Trans R Soc Trop Med Hyg 1997;91(4):422-4.
51. Sterling TR. The WHO/IUATLD diagnostic algorithm fortuberculosis and empiric fluoroquinolone use: potentialpitfalls. Int J Tuberc Lung Dis 2004;8(12):1396-400.
52. van Deun A. What is the role of mycobacterial culture indiagnosis and case finding? In: Frieden TR, ed. Toman'stuberculosis. Case detection, treatment and monitoring, 2ndEdition. Geneva: World Health Organization, 2004;35-43.
53. Kim TC, Blackman RS, Heatwole KM, Kim T, Rochester DF.Acid-fast bacilli in sputum smears of patients with pulmonarytuberculosis. Prevalence and significance of negative smearspretreatment and positive smears post-treatment. Am RevRespir Dis 1984;129(2):264-8.
54. Toman K. How many bacilli are present in a sputum specimenfound positive by smear microscopy? In: Frieden TR, (Ed.),Toman's Tuberculosis. Case Detection, Treatment andMonitoring, 2nd Edition. Geneva: World HealthOrganization, 2004;11-3.
55. Toman K. How reliable is smear microscopy? In: FriedenTR, (Ed.). Toman's Tuberculosis. Case Detection, Treatmentand Monitoring, 2nd Edition. Geneva: World HealthOrganization, 2004;14-22.
56. Menzies D. What is the current and potential role of diagnostictests other than sputum microscopy and culture? In: Frieden
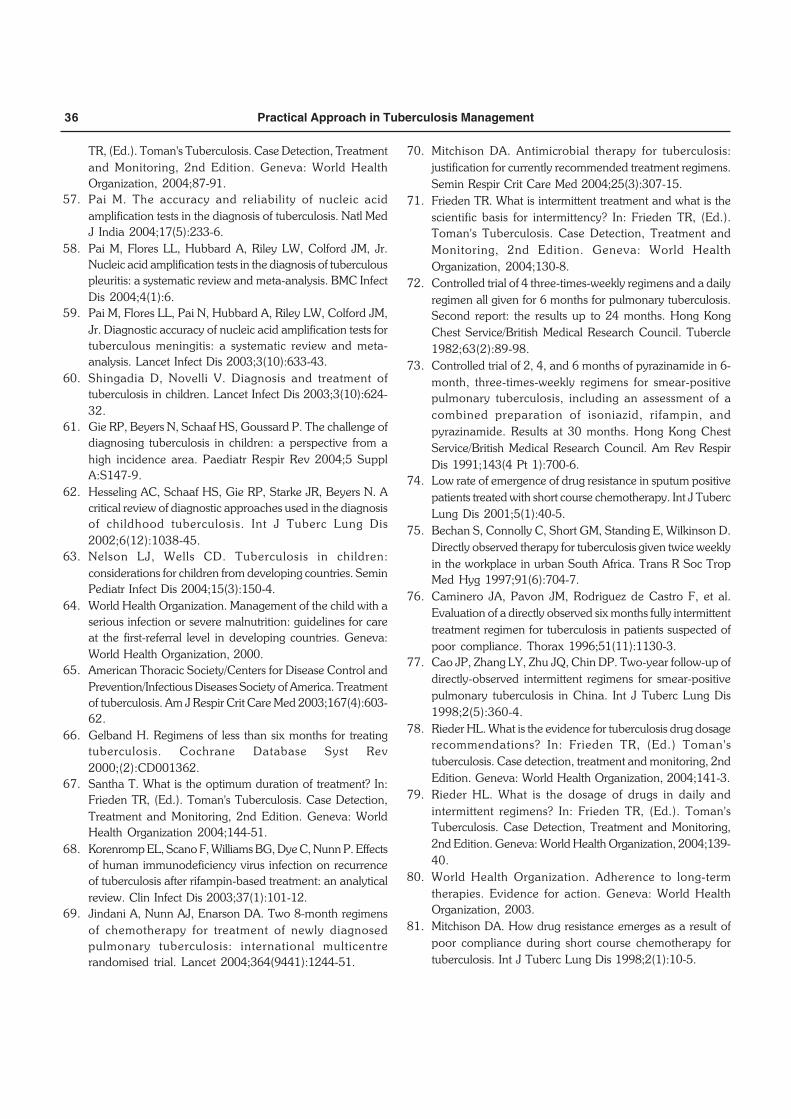
36 Practical Approach in Tuberculosis Management
TR, (Ed.). Toman's Tuberculosis. Case Detection, Treatmentand Monitoring, 2nd Edition. Geneva: World HealthOrganization, 2004;87-91.
57. Pai M. The accuracy and reliability of nucleic acidamplification tests in the diagnosis of tuberculosis. Natl MedJ India 2004;17(5):233-6.
58. Pai M, Flores LL, Hubbard A, Riley LW, Colford JM, Jr.Nucleic acid amplification tests in the diagnosis of tuberculouspleuritis: a systematic review and meta-analysis. BMC InfectDis 2004;4(1):6.
59. Pai M, Flores LL, Pai N, Hubbard A, Riley LW, Colford JM,Jr. Diagnostic accuracy of nucleic acid amplification tests fortuberculous meningitis: a systematic review and meta-analysis. Lancet Infect Dis 2003;3(10):633-43.
60. Shingadia D, Novelli V. Diagnosis and treatment oftuberculosis in children. Lancet Infect Dis 2003;3(10):624-32.
61. Gie RP, Beyers N, Schaaf HS, Goussard P. The challenge ofdiagnosing tuberculosis in children: a perspective from ahigh incidence area. Paediatr Respir Rev 2004;5 SupplA:S147-9.
62. Hesseling AC, Schaaf HS, Gie RP, Starke JR, Beyers N. Acritical review of diagnostic approaches used in the diagnosisof childhood tuberculosis. Int J Tuberc Lung Dis2002;6(12):1038-45.
63. Nelson LJ, Wells CD. Tuberculosis in children:considerations for children from developing countries. SeminPediatr Infect Dis 2004;15(3):150-4.
64. World Health Organization. Management of the child with aserious infection or severe malnutrition: guidelines for careat the first-referral level in developing countries. Geneva:World Health Organization, 2000.
65. American Thoracic Society/Centers for Disease Control andPrevention/Infectious Diseases Society of America. Treatmentof tuberculosis. Am J Respir Crit Care Med 2003;167(4):603-62.
66. Gelband H. Regimens of less than six months for treatingtuberculosis. Cochrane Database Syst Rev2000;(2):CD001362.
67. Santha T. What is the optimum duration of treatment? In:Frieden TR, (Ed.). Toman's Tuberculosis. Case Detection,Treatment and Monitoring, 2nd Edition. Geneva: WorldHealth Organization 2004;144-51.
68. Korenromp EL, Scano F, Williams BG, Dye C, Nunn P. Effectsof human immunodeficiency virus infection on recurrenceof tuberculosis after rifampin-based treatment: an analyticalreview. Clin Infect Dis 2003;37(1):101-12.
69. Jindani A, Nunn AJ, Enarson DA. Two 8-month regimensof chemotherapy for treatment of newly diagnosedpulmonary tuberculosis: international multicentrerandomised trial. Lancet 2004;364(9441):1244-51.
70. Mitchison DA. Antimicrobial therapy for tuberculosis:justification for currently recommended treatment regimens.Semin Respir Crit Care Med 2004;25(3):307-15.
71. Frieden TR. What is intermittent treatment and what is thescientific basis for intermittency? In: Frieden TR, (Ed.).Toman's Tuberculosis. Case Detection, Treatment andMonitoring, 2nd Edition. Geneva: World HealthOrganization, 2004;130-8.
72. Controlled trial of 4 three-times-weekly regimens and a dailyregimen all given for 6 months for pulmonary tuberculosis.Second report: the results up to 24 months. Hong KongChest Service/British Medical Research Council. Tubercle1982;63(2):89-98.
73. Controlled trial of 2, 4, and 6 months of pyrazinamide in 6-month, three-times-weekly regimens for smear-positivepulmonary tuberculosis, including an assessment of acombined preparation of isoniazid, rifampin, andpyrazinamide. Results at 30 months. Hong Kong ChestService/British Medical Research Council. Am Rev RespirDis 1991;143(4 Pt 1):700-6.
74. Low rate of emergence of drug resistance in sputum positivepatients treated with short course chemotherapy. Int J TubercLung Dis 2001;5(1):40-5.
75. Bechan S, Connolly C, Short GM, Standing E, Wilkinson D.Directly observed therapy for tuberculosis given twice weeklyin the workplace in urban South Africa. Trans R Soc TropMed Hyg 1997;91(6):704-7.
76. Caminero JA, Pavon JM, Rodriguez de Castro F, et al.Evaluation of a directly observed six months fully intermittenttreatment regimen for tuberculosis in patients suspected ofpoor compliance. Thorax 1996;51(11):1130-3.
77. Cao JP, Zhang LY, Zhu JQ, Chin DP. Two-year follow-up ofdirectly-observed intermittent regimens for smear-positivepulmonary tuberculosis in China. Int J Tuberc Lung Dis1998;2(5):360-4.
78. Rieder HL. What is the evidence for tuberculosis drug dosagerecommendations? In: Frieden TR, (Ed.) Toman'stuberculosis. Case detection, treatment and monitoring, 2ndEdition. Geneva: World Health Organization, 2004;141-3.
79. Rieder HL. What is the dosage of drugs in daily andintermittent regimens? In: Frieden TR, (Ed.). Toman'sTuberculosis. Case Detection, Treatment and Monitoring,2nd Edition. Geneva: World Health Organization, 2004;139-40.
80. World Health Organization. Adherence to long-termtherapies. Evidence for action. Geneva: World HealthOrganization, 2003.
81. Mitchison DA. How drug resistance emerges as a result ofpoor compliance during short course chemotherapy fortuberculosis. Int J Tuberc Lung Dis 1998;2(1):10-5.
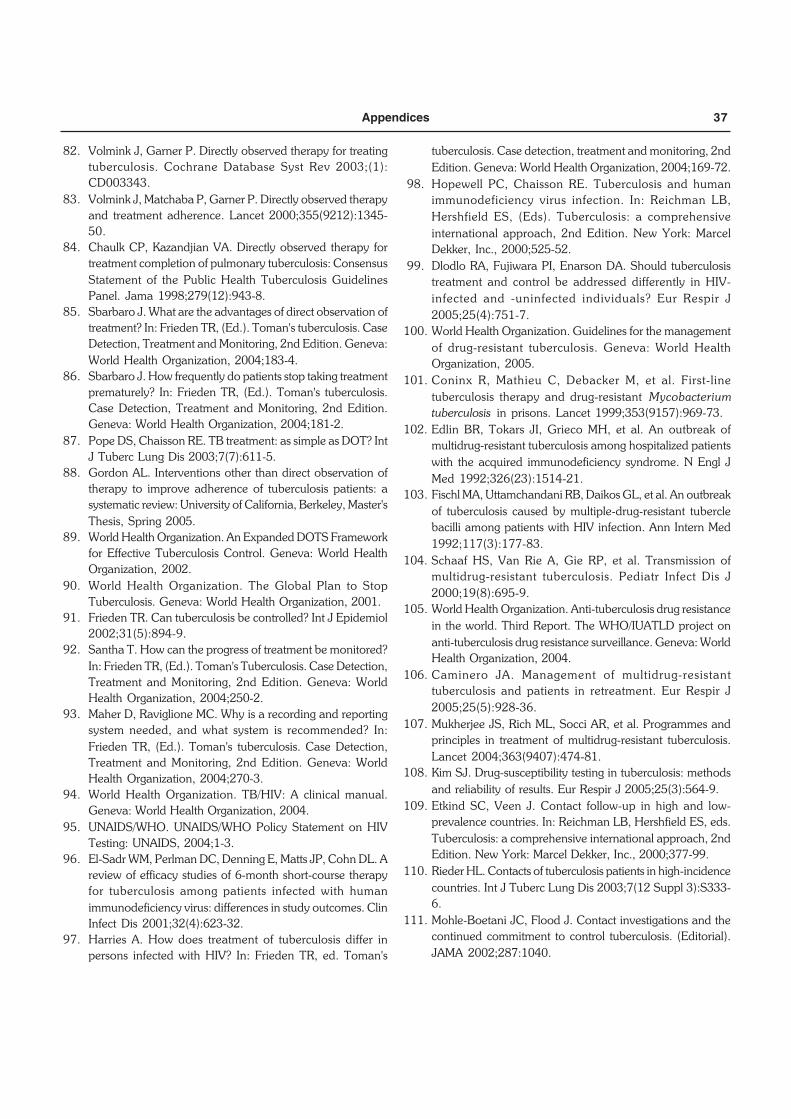
Appendices 37
82. Volmink J, Garner P. Directly observed therapy for treatingtuberculosis. Cochrane Database Syst Rev 2003;(1):CD003343.
83. Volmink J, Matchaba P, Garner P. Directly observed therapyand treatment adherence. Lancet 2000;355(9212):1345-50.
84. Chaulk CP, Kazandjian VA. Directly observed therapy fortreatment completion of pulmonary tuberculosis: ConsensusStatement of the Public Health Tuberculosis GuidelinesPanel. Jama 1998;279(12):943-8.
85. Sbarbaro J. What are the advantages of direct observation oftreatment? In: Frieden TR, (Ed.). Toman's tuberculosis. CaseDetection, Treatment and Monitoring, 2nd Edition. Geneva:World Health Organization, 2004;183-4.
86. Sbarbaro J. How frequently do patients stop taking treatmentprematurely? In: Frieden TR, (Ed.). Toman's tuberculosis.Case Detection, Treatment and Monitoring, 2nd Edition.Geneva: World Health Organization, 2004;181-2.
87. Pope DS, Chaisson RE. TB treatment: as simple as DOT? IntJ Tuberc Lung Dis 2003;7(7):611-5.
88. Gordon AL. Interventions other than direct observation oftherapy to improve adherence of tuberculosis patients: asystematic review: University of California, Berkeley, Master'sThesis, Spring 2005.
89. World Health Organization. An Expanded DOTS Frameworkfor Effective Tuberculosis Control. Geneva: World HealthOrganization, 2002.
90. World Health Organization. The Global Plan to StopTuberculosis. Geneva: World Health Organization, 2001.
91. Frieden TR. Can tuberculosis be controlled? Int J Epidemiol2002;31(5):894-9.
92. Santha T. How can the progress of treatment be monitored?In: Frieden TR, (Ed.). Toman's Tuberculosis. Case Detection,Treatment and Monitoring, 2nd Edition. Geneva: WorldHealth Organization, 2004;250-2.
93. Maher D, Raviglione MC. Why is a recording and reportingsystem needed, and what system is recommended? In:Frieden TR, (Ed.). Toman's tuberculosis. Case Detection,Treatment and Monitoring, 2nd Edition. Geneva: WorldHealth Organization, 2004;270-3.
94. World Health Organization. TB/HIV: A clinical manual.Geneva: World Health Organization, 2004.
95. UNAIDS/WHO. UNAIDS/WHO Policy Statement on HIVTesting: UNAIDS, 2004;1-3.
96. El-Sadr WM, Perlman DC, Denning E, Matts JP, Cohn DL. Areview of efficacy studies of 6-month short-course therapyfor tuberculosis among patients infected with humanimmunodeficiency virus: differences in study outcomes. ClinInfect Dis 2001;32(4):623-32.
97. Harries A. How does treatment of tuberculosis differ inpersons infected with HIV? In: Frieden TR, ed. Toman's
tuberculosis. Case detection, treatment and monitoring, 2ndEdition. Geneva: World Health Organization, 2004;169-72.
98. Hopewell PC, Chaisson RE. Tuberculosis and humanimmunodeficiency virus infection. In: Reichman LB,Hershfield ES, (Eds). Tuberculosis: a comprehensiveinternational approach, 2nd Edition. New York: MarcelDekker, Inc., 2000;525-52.
99. Dlodlo RA, Fujiwara PI, Enarson DA. Should tuberculosistreatment and control be addressed differently in HIV-infected and -uninfected individuals? Eur Respir J2005;25(4):751-7.
100. World Health Organization. Guidelines for the managementof drug-resistant tuberculosis. Geneva: World HealthOrganization, 2005.
101. Coninx R, Mathieu C, Debacker M, et al. First-linetuberculosis therapy and drug-resistant Mycobacteriumtuberculosis in prisons. Lancet 1999;353(9157):969-73.
102. Edlin BR, Tokars JI, Grieco MH, et al. An outbreak ofmultidrug-resistant tuberculosis among hospitalized patientswith the acquired immunodeficiency syndrome. N Engl JMed 1992;326(23):1514-21.
103. Fischl MA, Uttamchandani RB, Daikos GL, et al. An outbreakof tuberculosis caused by multiple-drug-resistant tuberclebacilli among patients with HIV infection. Ann Intern Med1992;117(3):177-83.
104. Schaaf HS, Van Rie A, Gie RP, et al. Transmission ofmultidrug-resistant tuberculosis. Pediatr Infect Dis J2000;19(8):695-9.
105. World Health Organization. Anti-tuberculosis drug resistancein the world. Third Report. The WHO/IUATLD project onanti-tuberculosis drug resistance surveillance. Geneva: WorldHealth Organization, 2004.
106. Caminero JA. Management of multidrug-resistanttuberculosis and patients in retreatment. Eur Respir J2005;25(5):928-36.
107. Mukherjee JS, Rich ML, Socci AR, et al. Programmes andprinciples in treatment of multidrug-resistant tuberculosis.Lancet 2004;363(9407):474-81.
108. Kim SJ. Drug-susceptibility testing in tuberculosis: methodsand reliability of results. Eur Respir J 2005;25(3):564-9.
109. Etkind SC, Veen J. Contact follow-up in high and low-prevalence countries. In: Reichman LB, Hershfield ES, eds.Tuberculosis: a comprehensive international approach, 2ndEdition. New York: Marcel Dekker, Inc., 2000;377-99.
110. Rieder HL. Contacts of tuberculosis patients in high-incidencecountries. Int J Tuberc Lung Dis 2003;7(12 Suppl 3):S333-6.
111. Mohle-Boetani JC, Flood J. Contact investigations and thecontinued commitment to control tuberculosis. (Editorial).JAMA 2002;287:1040.

38 Practical Approach in Tuberculosis Management
112. Reichler MR, Reves R, Bur S, et al. Evaluation of investi-gations conducted to detect and prevent transmission oftuberculosis. Jama 2002;287(8):991-5.
113. Morrison J, Pai M, Hopewell PC. Yield of tuberculosis contactinvestigations within households in high incidence countries:a systematic review (submitted abstract). Infectious DiseasesSociety of America (IDSA) 43rd Annual Meeting 2005, SanFrancisco.
114. Perkins MD. New diagnostic tools for tuberculosis. Int JTuberc Lung Dis 2000;4(12 Suppl 2):S182-8.
115. O'Brien RJ, Spigelman M. New drugs for tuberculosis: currentstatus and future prospects. Clin Chest Med 2005;26(2):327-40, vii.
116. Brennan MJ. The tuberculosis vaccine challenge.Tuberculosis (Edinb) 2005;85(1-2):7-12.