Embed Size (px)
Citation preview
In this issue:
From the Chair…………..1
From the Editor…….…….3
NDEP Officers..................4
Clinical Nutrition
Management (CNM)
DPG……………………….4
The Impact of DPD Program
Admission Criteria on RDN
Exam Pass Rates…….....5
Rise: Preparing Dietetic Interns for the Age of Telehealth…………..…...9 Change in Implicit Weight Bias Scores following a Multi-Faceted Bias Education Session in Undergraduate Nutrition Students and Dietetic Interns………….………12 Simulation within Dietetics
Education: How Educators’
Familiarity and Needs Have
Changed with Increased
Simulation-Related
Efforts………………..…18
2016 Outstanding Preceptor
Awardees ………………26
NDEP-Line Winter 2016
From the Chair...
Robyn Osborn, PhD, RD Dietetic Internship Director VA San Diego Healthcare System [email protected]
Welcome to the Winter 2016 edition of NDEP-Line. As I sit and reflect on our many roles and responsibilities in dietetics education, I am reminded about how many students and interns depend on us for the outcomes of their education and their future in our diverse field. As we all know, we are on the threshold of very important changes in dietetics education, and we are tasked with helping shape that future, so our responsibilities, at the moment, are even bigger. During FNCE in October, the NDEP Council had the opportunity to meet with ACEND leaders to discuss the Future Education Model draft standards for the proposed Master, Bachelor, and Associate Degree programs. During the NDEP Council meeting, your NDEP chairs and Regional Directors shared their input and concerns, and the ACEND representatives provided much clarification and feedback. During the ACEND/CDR Educators’ Round Table, many NDEP members, educators, and preceptors had the opportunity to meet in small groups to share their perspectives and provide input. My overall take-away from those sessions is that, as NDEP members, we are in the position to influence the outcome of the Future Model Standards, and ACEND is very interested in our input. Here are some things to keep in mind as you formulate your feedback:
Provide substantive feedback and realistic alternatives with strong, supporting arguments. It isn’t enough to argue that a proposed standard or competency isn’t realistic or you disagree with it.
Provide examples of best practices and methods to meet the desired competencies and outcomes.
ACEND is very interested in feedback on the competencies. It is my understanding that the ACEND Standards Committee’s expectation is that all performance indicators, not just the competencies, would need to be met. (It is not intended to be like the PDP where performance indicators are suggested ways in which the competencies can be met.) If this seems unrealistic to you, be sure to address this in your comments.
2 | NDEP-Line | Winter 2016
ACEND is aware that “technician” is not be seen as an acceptable title for the Bachelor’s trained practitioner. They are interested in suggestions for other names/titles.
ACEND has not been receiving as much feedback on the Associate-level standards as the Bachelor’s and Master’s. Please provide feedback on these standards, as well.
There is some confusion between the 2017 Standards and the Future Model Standards. It is the Future Model Standards that are currently open for public comment. The 2017 Standards are the updates to the 2012 standards. These go into effect in January 2017.
There is some confusion between the 2024 master’s degree requirement for eligibility to take the RD exam and ACEND’s Future Model Standards. The 2024 requirement is a CDR (Commission on Dietetic Registration) requirement. It is not related to ACEND’s Future Model Standards.
In summary, ACEND assured NDEP members and educators that required adoption of the Future Model Standards is many years (20 or more) in the future. Initially, they are hoping that 60 programs (of all three types, master, bachelor, and associate) will apply to be voluntary Demonstration (pilot) Programs accredited under the future education model standards in a first round, with another 60 in a later round. They anticipate that it may take 2-3 years for these demonstration programs to get up and running. Then several years of program graduates will be monitored and tracked for pass-rate, employment, level or practice, etc., and data on program operations and needed resources will be collected. It is only after they evaluate the outcomes data that decisions will be made about how the standards will actually look. In other news, NDEP’s seven areas have been
realigned into six areas, or regions – West Coast, West Central, North Central, South Central, Northeast, and Southeast. One of the changes that you will see as a result is that for 2017, there will be three area (or regional) meetings instead of four:
Western -- Asilomar Conference Center, Pacific Grove, CA, March 12-14, 2017
Central – Hyatt Regency Hotel, Louisville, KY, March 30-31
Eastern – Embassy Suites by Hilton Inner Harbor, Baltimore, MD, April 2021
Feel free to attend any one of the three meetings. Our goal is to standardize the agendas so that all NDEP members will receive consistent information regardless of which meeting they attend. In addition, we hope to organize the meetings to allow for more roundtables and working sessions, rather than focusing on presentations. If you have any suggestions, please contact your Regional Director. Their names are listed on the NDEP website at http://www.ndepnet.org/. Registration and additional information will be available on the NDEP website in January. Lastly, nominations for the 2017 Outstanding Educator are due to your NDEP Regional Directors on January 13, 2017, and nominations for the 2017 Outstanding Preceptor Awards are due to the NDEP Preceptor Director on March 3, 2017. Submission information is available for both awards on the NDEP website. In closing, it was a pleasure to represent all of you at FNCE as your NDEP Chair this year. Please know that the NDEP Council and I are here to represent all of yours (educators and preceptors) and your students’ and interns’ interests in all matters related to dietetics education. As always, we are open to your suggestions or feedback. Best Wishes for a Wonderful New Year!
Robyn
3 | NDEP-Line | Winter 2016
From the Editor... Colleen McCrief, MS, RDN Director, Didactic Program in Dietetics The Sage Colleges Troy, NY [email protected]
The spring 2017 edition of the NDEP-Line will not be published this year. This is temporary and editions will resume in summer 2017. Submissions for the summer edition will be accepted anytime through May 1.
Guidelines for NDEP-Line Authors NDEP-Line features viewpoints, statements, and information on materials and products for the use of Nutrition and Dietetic Educators and Preceptors (NDEP) members. These viewpoints, statements and information do not imply endorsement by NDEP and the Academy of Nutrition and Dietetics. Articles may be reproduced for educational purposes only. NDEP-Line owns the copyright of all published articles, unless prior agreement was made. © Copyright 2012 by Nutrition and Dietetic Educators and Preceptors of the Academy of Nutrition and Dietetics. All rights reserved. No part of this publication may be reproduced, stored in a retrieval system or transmitted in any form by any means without permission of the publisher. Article length
Article length is negotiated with the editor for the issue in which it will appear. Lead articles are usually around 2,000 words. Other feature articles are 1,000-1,500 words, while book reviews and brief reports are 500 words.
Text format All articles, notices, and information should be in Times New Roman font, 12 point, single-spaced.
Tables and illustrations Tables should be self-explanatory. All diagrams, charts and figures should be camera-ready. Each illustration should be accompanied by a brief caption that makes the illustration intelligible by itself.
References References should be cited in the text in consecutive order using superscript numerals. At the end of the text, each reference should be listed in order of citation. The format should be the same as that of the Journal of the Academy of Nutrition and Dietetics.
Author(s) List author with first name, initial (if any) last name, professional suffix, and affiliation (all in italics) below the title of the article, i.e., For NDEP members or other dietetic educators: Anne A. Anderson, PhD, RD, LD, American University
For authors in other fields/disciplines: Anthony T. Vicente, PhD, Director, Nutrigenomics Laboratory, American Human Nutrition Research Center on Genetics at American University
Author’s Contact Information Before the article, give the primary author’s complete contact information including program affiliation, phone, fax and email address.
Submission All submissions for the publication should be submitted to the editor as an e-mail attachment as an MS Word file. Indicate the number of words after author’s contact information.
Submission Deadlines
Spring: February 1 Summer: May 1 Fall: August 1 Winter: November 1
A submission may be returned to the primary author for revision if it does not conform to the style requirements.
Editor
Colleen McCrief, MS, RD The Sage Colleges Phone: 518-244-2043 [email protected]
Reprint permissions request or back issues:
Contact Colleen McCrief @ [email protected]
4| NDEP-Line | Winter 2016
Chair: Robyn Osborn [email protected]
Chair Elect: Patricia Knisley
Past Chair: Sylvia Escott-Stump
HOD Delegate: Kendra Kattelmann
Preceptor Director: Stephanie
Stockslager
Graduate Student Representative:
Emily Riddle [email protected]
Communications Director: Mary-Jon
Ludy [email protected]
Newsletter Editor: Colleen McCrief
Board of Directors Liaison: Aida Miles
ACEND Liaison: Maxine McElligott
Public Member: Sandra Gill
CDR Liaison: Rebecca Brody
Regional Directors
Area 1: Susan E. Helm – [email protected] and Wendy Buchan - [email protected]
Area 2: Kim Matwiejow – [email protected]
Area 3: Karen Smith – [email protected]
Area 4: Peggy Turner – [email protected] Area 5: Adam Burda - [email protected]
Area 6: Malinda Cecil – [email protected]
Area 7: Kathy Border – [email protected]
Clinical Nutrition Management (CNM) DPG Kerry Scott, RDN, CD Clinical Nutrition Management DPG Membership Chair [email protected] 509-474-7415
Do you come across students in your courses and programs that stand out, and you know they will one day make a good leader? There are those students who have a plan and know they will one day work towards a management position, but there are others who perhaps are quiet leaders that peers respect and gravitate towards. As you come across these students potential leaders for our profession, please keep in mind the Clinical Nutrition Management (CNM) DPG within the Academy. The word “manager” in the title can be misleading, as the DPG both fosters and encourages leadership development in non-traditional ways, as well. With several sub-groups within the DPG including Informatics, Quality Process Improvement and new this year Pediatric Management, members can learn about and specialize in areas other than more traditional management topics. Through membership in the CNM DPG, a dietitian or student could be become familiar with topics related to the business of dietetics, such as budgeting, staffing, communication styles and regulatory processes, before stepping into a role for which they are responsible for these tasks. In addition, wouldn’t it be wonderful to develop a silent leader who might not have a management title, but has a role with positive influence on employees and peers! The CNM DPG offers many member benefits including a quarterly newsletter that offers a CEU article, webinars on timely topics, an electronic mailing list with valuable sharing, a resource library, and an annual symposium for education and networking. This year the annual symposium will be in St. Petersburg, FL March 18th – 21st, 2017. Please encourage students to visit our web site and find out more about this practice group at www.cnmdpg.org.
5| NDEP-Line | Winter 2016
The Impact of DPD Program Admission Criteria on RDN Exam Pass Rates Heather Payne-Emerson, PhD, RDN, LD Director, Didactic Program in Dietetics Department of Family and Consumer Sciences Western Kentucky University [email protected] 270-745-6356 Karen G. Mason, PhD, RDN, LD, Western Kentucky University
The pass rate on the registration examination for dietitians is one of the primary means by which didactic programs and dietetic internships are evaluated by the Accreditation Council for Education in Nutrition and Dietetics (ACEND). ACEND requires at least an 80% pass rate for both the five year first time and one year pass rates according to the 2012 accreditation standards.1 Although the 2017 standards will no longer require monitoring of the first time pass rate, programs must still maintain a one year pass rate of 80%.2 Those programs not meeting this benchmark must submit a pass rate improvement plan and are subject to monitoring or withdrawal of accreditation.1 Consequently, monitoring and improving pass rates are major areas of program director focus.
In addition to the pass rate guidelines, the 2012 and 2017 accreditation standards further require programs to develop admission criteria as a means of assessing the ability of program applicants to succeed in the program.1,2 Although obtaining an internship is a competitive process, as evidenced by the most recent national match rate of 51%,3 we have observed within our didactic program that students who are not as strong academically do become matched to internship programs. These students often struggle to pass the RDN exam. Thus, not only are program admission criteria necessary for ensuring student success within didactic programs, but also for maintaining and improving RDN exam pass rates.
Our didactic program revised admission criteria in 2009 in an effort to improve the program pass rate. After review of curricular and other factors, the most likely contributing factor to
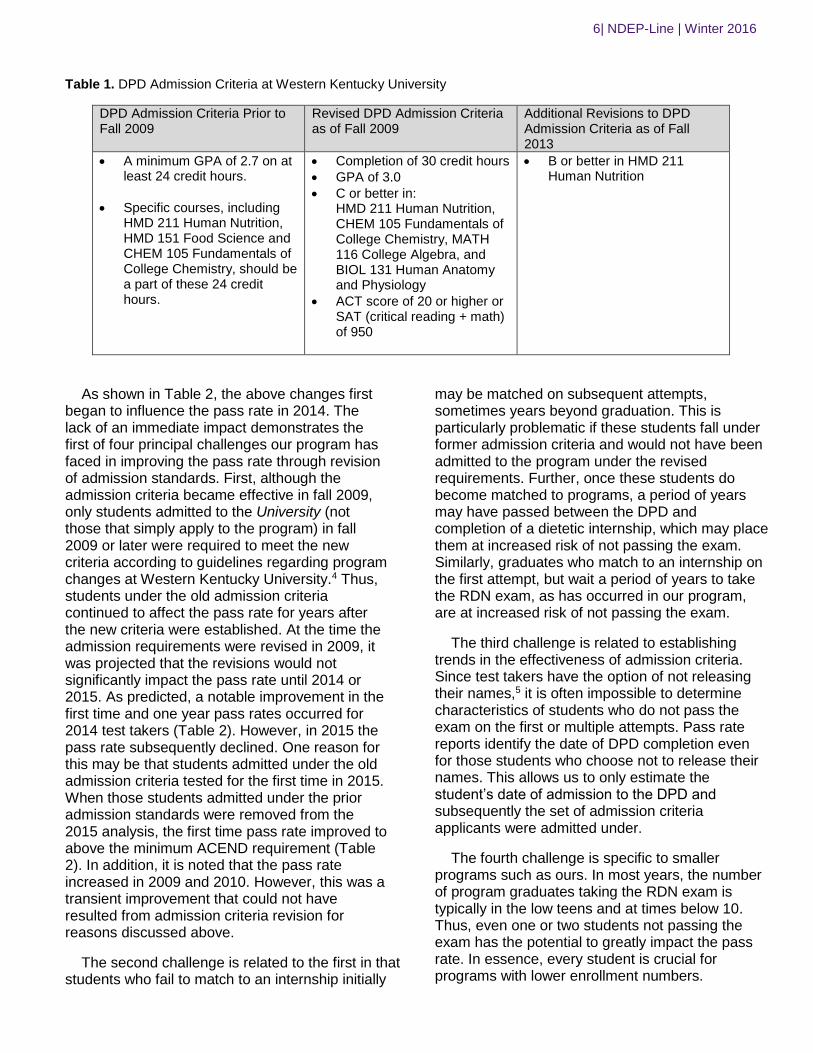
the pass rate was determined to be insufficient admission criteria. It was anticipated that more rigorous requirements would improve the pass rate by improving the qualifications of students that entered the dietetics program. Revisions were made based on characteristics that the DP director and program faculty observed to be associated with passing the RDN exam on the first attempt. Of particular note is the establishment of a minimum ACT score of 20. To establish this criterion, ACT and RDN exam scores for those students who released their names on pass rate reports were tracked for approximately 5 years. A score of 20 or higher tended to predict successful completion of the RDN exam, although a formal statistical analysis was not performed. In addition, foundational nutrition, science and math courses were included in admission requirements to ensure adequate scientific reasoning skills. In 2013 the admission criteria were further revised such that a grade of B, rather than a C, or better was required in HMD 211 Human Nutrition. This change was made 1) to ensure program applicants had sufficient knowledge and aptitude in human nutrition and 2) because those students who made a C in this introductory course typically did not meet GPA admission requirements. Even though such students did not factor into the pass rate, this criterion helped students and advisors to determine earlier if the student could eventually be admitted to the program. The admission criteria prior to and after fall 2009 are outlined in Table 1.
6| NDEP-Line | Winter 2016
Table 1. DPD Admission Criteria at Western Kentucky University
DPD Admission Criteria Prior to Fall 2009
Revised DPD Admission Criteria as of Fall 2009
Additional Revisions to DPD Admission Criteria as of Fall 2013
A minimum GPA of 2.7 on at least 24 credit hours.
Specific courses, including HMD 211 Human Nutrition, HMD 151 Food Science and CHEM 105 Fundamentals of College Chemistry, should be a part of these 24 credit hours.
Completion of 30 credit hours
GPA of 3.0
C or better in: HMD 211 Human Nutrition, CHEM 105 Fundamentals of College Chemistry, MATH 116 College Algebra, and BIOL 131 Human Anatomy and Physiology
ACT score of 20 or higher or SAT (critical reading + math) of 950
B or better in HMD 211 Human Nutrition
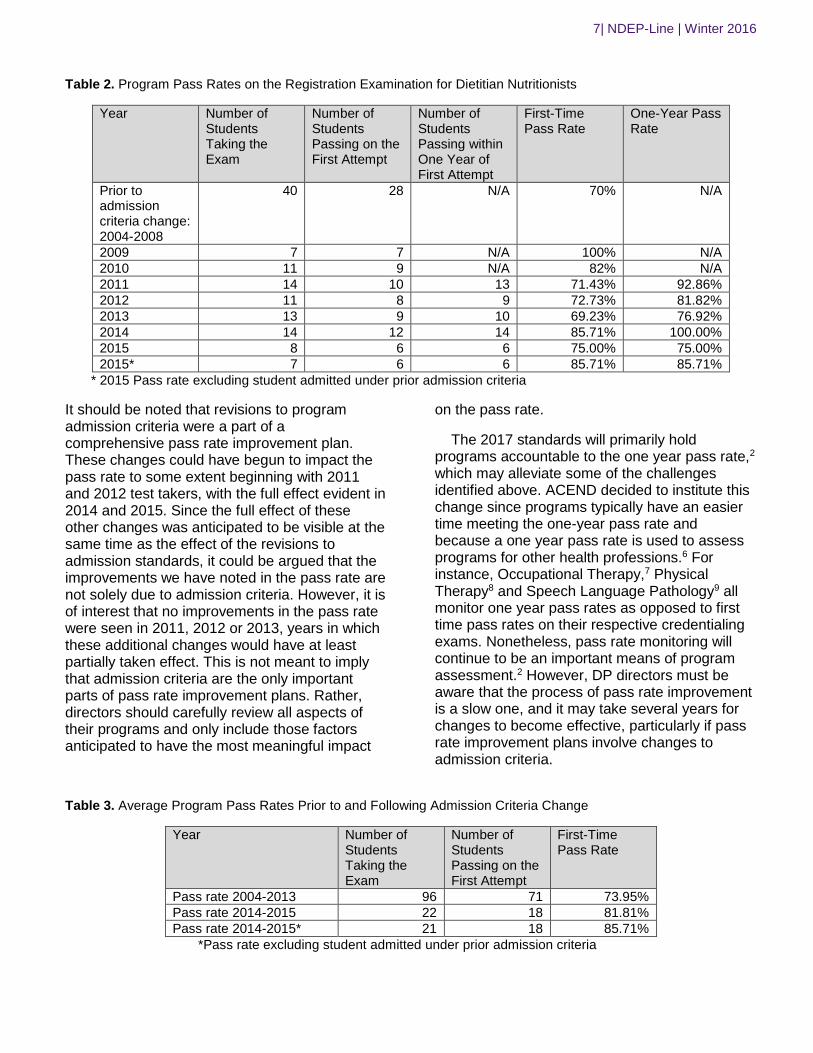
As shown in Table 2, the above changes first began to influence the pass rate in 2014. The lack of an immediate impact demonstrates the first of four principal challenges our program has faced in improving the pass rate through revision of admission standards. First, although the admission criteria became effective in fall 2009, only students admitted to the University (not those that simply apply to the program) in fall 2009 or later were required to meet the new criteria according to guidelines regarding program changes at Western Kentucky University.4 Thus, students under the old admission criteria continued to affect the pass rate for years after the new criteria were established. At the time the admission requirements were revised in 2009, it was projected that the revisions would not significantly impact the pass rate until 2014 or 2015. As predicted, a notable improvement in the first time and one year pass rates occurred for 2014 test takers (Table 2). However, in 2015 the pass rate subsequently declined. One reason for this may be that students admitted under the old admission criteria tested for the first time in 2015. When those students admitted under the prior admission standards were removed from the 2015 analysis, the first time pass rate improved to above the minimum ACEND requirement (Table 2). In addition, it is noted that the pass rate increased in 2009 and 2010. However, this was a transient improvement that could not have resulted from admission criteria revision for reasons discussed above.
The second challenge is related to the first in that students who fail to match to an internship initially
may be matched on subsequent attempts, sometimes years beyond graduation. This is particularly problematic if these students fall under former admission criteria and would not have been admitted to the program under the revised requirements. Further, once these students do become matched to programs, a period of years may have passed between the DPD and completion of a dietetic internship, which may place them at increased risk of not passing the exam. Similarly, graduates who match to an internship on the first attempt, but wait a period of years to take the RDN exam, as has occurred in our program, are at increased risk of not passing the exam.
The third challenge is related to establishing trends in the effectiveness of admission criteria. Since test takers have the option of not releasing their names,5 it is often impossible to determine characteristics of students who do not pass the exam on the first or multiple attempts. Pass rate reports identify the date of DPD completion even for those students who choose not to release their names. This allows us to only estimate the student’s date of admission to the DPD and subsequently the set of admission criteria applicants were admitted under.
The fourth challenge is specific to smaller programs such as ours. In most years, the number of program graduates taking the RDN exam is typically in the low teens and at times below 10. Thus, even one or two students not passing the exam has the potential to greatly impact the pass rate. In essence, every student is crucial for programs with lower enrollment numbers.
7| NDEP-Line | Winter 2016
Table 2. Program Pass Rates on the Registration Examination for Dietitian Nutritionists
Year Number of Students Taking the Exam
Number of Students Passing on the First Attempt
Number of Students Passing within One Year of First Attempt
First-Time Pass Rate
One-Year Pass Rate
Prior to admission criteria change: 2004-2008
40 28 N/A 70% N/A
2009 7 7 N/A 100% N/A
2010 11 9 N/A 82% N/A
2011 14 10 13 71.43% 92.86%
2012 11 8 9 72.73% 81.82%
2013 13 9 10 69.23% 76.92%
2014 14 12 14 85.71% 100.00%
2015 8 6 6 75.00% 75.00%
2015* 7 6 6 85.71% 85.71%
* 2015 Pass rate excluding student admitted under prior admission criteria
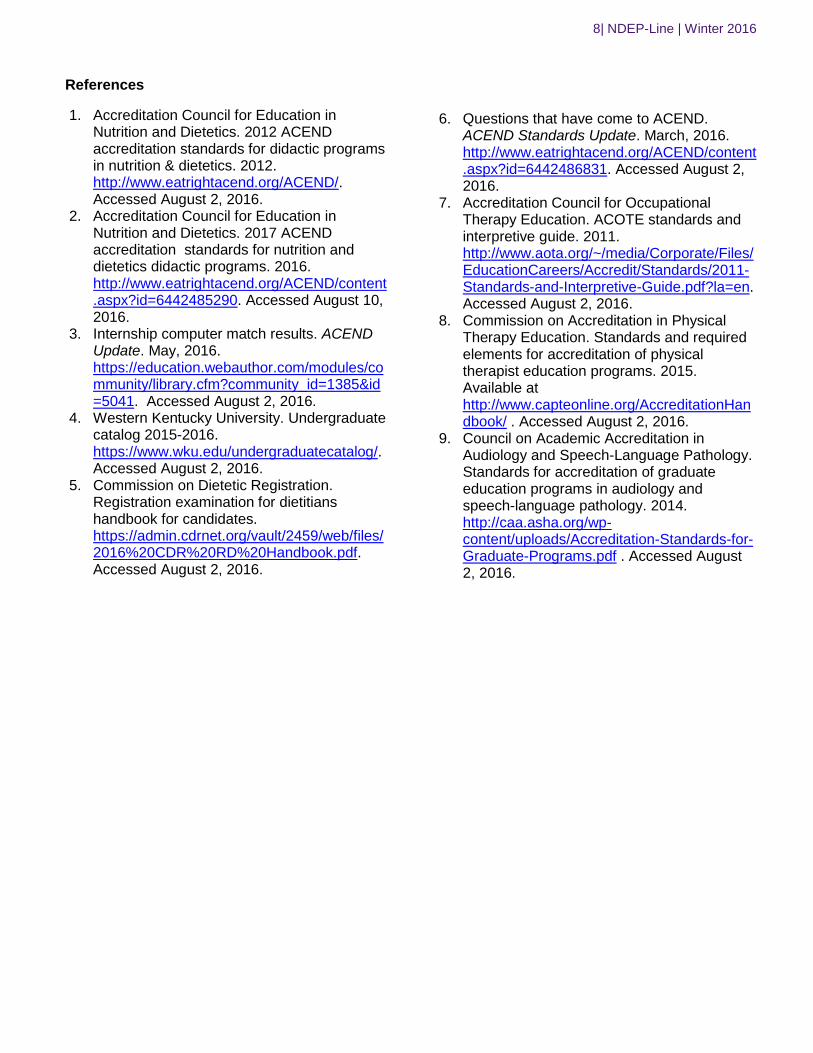
It should be noted that revisions to program admission criteria were a part of a comprehensive pass rate improvement plan. These changes could have begun to impact the pass rate to some extent beginning with 2011 and 2012 test takers, with the full effect evident in 2014 and 2015. Since the full effect of these other changes was anticipated to be visible at the same time as the effect of the revisions to admission standards, it could be argued that the improvements we have noted in the pass rate are not solely due to admission criteria. However, it is of interest that no improvements in the pass rate were seen in 2011, 2012 or 2013, years in which these additional changes would have at least partially taken effect. This is not meant to imply that admission criteria are the only important parts of pass rate improvement plans. Rather, directors should carefully review all aspects of their programs and only include those factors anticipated to have the most meaningful impact
on the pass rate.
The 2017 standards will primarily hold programs accountable to the one year pass rate,2 which may alleviate some of the challenges identified above. ACEND decided to institute this change since programs typically have an easier time meeting the one-year pass rate and because a one year pass rate is used to assess programs for other health professions.6 For instance, Occupational Therapy,7 Physical Therapy8 and Speech Language Pathology9 all monitor one year pass rates as opposed to first time pass rates on their respective credentialing exams. Nonetheless, pass rate monitoring will continue to be an important means of program assessment.2 However, DP directors must be aware that the process of pass rate improvement is a slow one, and it may take several years for changes to become effective, particularly if pass rate improvement plans involve changes to admission criteria.
Table 3. Average Program Pass Rates Prior to and Following Admission Criteria Change
Year Number of Students Taking the Exam
Number of Students Passing on the First Attempt
First-Time Pass Rate
Pass rate 2004-2013 96 71 73.95%
Pass rate 2014-2015 22 18 81.81%
Pass rate 2014-2015* 21 18 85.71%
*Pass rate excluding student admitted under prior admission criteria
8| NDEP-Line | Winter 2016
References
1. Accreditation Council for Education in Nutrition and Dietetics. 2012 ACEND accreditation standards for didactic programs in nutrition & dietetics. 2012. http://www.eatrightacend.org/ACEND/. Accessed August 2, 2016.
2. Accreditation Council for Education in Nutrition and Dietetics. 2017 ACEND accreditation standards for nutrition and dietetics didactic programs. 2016. http://www.eatrightacend.org/ACEND/content.aspx?id=6442485290. Accessed August 10, 2016.
3. Internship computer match results. ACEND Update. May, 2016. https://education.webauthor.com/modules/community/library.cfm?community_id=1385&id=5041. Accessed August 2, 2016.
4. Western Kentucky University. Undergraduate catalog 2015-2016. https://www.wku.edu/undergraduatecatalog/. Accessed August 2, 2016.
5. Commission on Dietetic Registration. Registration examination for dietitians handbook for candidates. https://admin.cdrnet.org/vault/2459/web/files/2016%20CDR%20RD%20Handbook.pdf. Accessed August 2, 2016.
6. Questions that have come to ACEND. ACEND Standards Update. March, 2016. http://www.eatrightacend.org/ACEND/content.aspx?id=6442486831. Accessed August 2, 2016.
7. Accreditation Council for Occupational Therapy Education. ACOTE standards and interpretive guide. 2011. http://www.aota.org/~/media/Corporate/Files/EducationCareers/Accredit/Standards/2011-Standards-and-Interpretive-Guide.pdf?la=en. Accessed August 2, 2016.
8. Commission on Accreditation in Physical Therapy Education. Standards and required elements for accreditation of physical therapist education programs. 2015. Available at http://www.capteonline.org/AccreditationHandbook/ . Accessed August 2, 2016.
9. Council on Academic Accreditation in Audiology and Speech-Language Pathology. Standards for accreditation of graduate education programs in audiology and speech-language pathology. 2014. http://caa.asha.org/wp-content/uploads/Accreditation-Standards-for-Graduate-Programs.pdf . Accessed August 2, 2016.

9| NDEP-Line | Winter 2016
Rise: Preparing Dietetic Interns for the Age of Telehealth
Samantha K. Jones, RDN, LDN
Graduate Research Assistant, Iowa State University
515-294-7316
Jill Schechinger, Dietetic Intern, Iowa State University
Emily Wisecup, Dietetic Intern, Iowa State University
Nina Streauslin, Dietetic Intern, Iowa State University
Kaitlyn Milligan, Dietetic Intern, Iowa State University
Janet S. Johnson, MS, RDN, LD, Iowa State University
Laurie Kruzich, MS, RDN, LD, Iowa State University
Jean Anderson, MS, RDN, LDN, Iowa State University
As 90% of hospital leaders interviewed by
the 2014 Telemedicine Survey are currently
developing or implementing a telemedicine
program1, it is no surprise that nutrition care is
following suit. In fact, the Academy of Nutrition and
Dietetics identified a shift towards technology based
nutrition services as a driving force impacting the
dietetics workforce in their future scan of the years
2012-20222. With the rising prevalence and patient
interest in telehealth, it is important that dietetic
interns be competent in utilizing technology in their
future practice. The Iowa State University Dietetics
Internship, in conjunction with One Medical Group
and the Partnership for a Healthier America, is
providing interns with a first of its kind experience to
coach low-income families via the Rise smartphone
app3.
To prepare for the coaching experience,
nine interns completed 12 weeks of training with
One Medical Group. During this time, interns
learned how to effectively coach using the app,
practiced communication over various digital
platforms, and applied motivational interviewing
techniques. The following 12 weeks were dedicated
to coaching clients with daily feedback on their
meals and exercise and answering clients’
questions. After completing several weeks of
coaching, interns were surveyed using a likert scale
(with 0 being the lowest and 5 being the highest
possible score) and free comment fields to evaluate
the effectiveness of the Rise training in the
following areas: application of motivational
interviewing, navigation of the app to provide
nutrition coaching, and ease of communication.
Motivational interviewing (MI) is a technique
that has been found to be effective at improving
health behavior change and health outcomes. It is
described as a client-centered method to increase
internal motivation by exploring and resolving
ambivalence4. Interns completing the Rise training
independently studied Molly Kellogg’s Dietetic
Intern’s “Step by Step” program and applied
counseling skills from each lesson in weekly video
conferences. A survey of the interns revealed that
86% found the Molly Kellogg trainings to be at least
moderately helpful at advancing their understanding
and application of MI strategies. Interns found the
segments focusing on “rolling with resistance” and
“engaging the client” most helpful, while the topics
of “open ended questioning” and “reflection” were
least helpful. Comments suggested interns learned
about open ended questioning and reflection during
their undergraduate studies, and they found these
segments of the Molly Kellogg trainings to be
repetitive. Several of those surveyed felt they
gained the most from the weekly video conferences
during which they were able to practice MI
concepts. Interns also commented that during the
video conferences, discussions that were more
structured and focused on applying MI within the
Rise app would be helpful to future interns.
Training on app navigation from both a
client and coach standpoint was also an important
component of the first 12 weeks of training. Interns

10| NDEP-Line | Winter 2016
were paired and adopted both the role of the client
and the coach to give each intern the opportunity to
become comfortable with operating the app and its
features. To evaluate functionally, interns were then
asked to rate user friendliness from the coaching
and client standpoint. Results indicated the app
was more user friendly from the client side, but
interns still felt well prepared to coach after the app
navigation training was complete. Interns offered
suggestions to improve the coaching interface
including navigational changes when looking at
clients’ meals and alterations in the meal
notification feature.
Effective communication among the interns
and Rise personnel was an essential component of
the Rise training. It was a unique challenge due to
the varying geographical locations of those
involved. The communication tools used included
Zoom, Slack, and Google Docs. Zoom is a video
conference platform used for online meetings that
allowed the interns, a Registered Dietitian
Nutritionist, and Rise representatives to
communicate through audio and video. The survey
indicated interns found Zoom was “easy to use” and
it was “beneficial to be able to communicate one-to-
one with everybody”. One negative comment
related to zoom was that “typing could be heard
over the speaker if the mic was not muted”. The
second communication tool used, Slack, is a
messaging app specifically designed for group
communication. The majority of interns rated Slack
as easy to use. Lastly, Google Docs was used for
online document sharing. The survey revealed that
interns felt it was hard to keep track of the multitude
of Google Docs that were created. An additional
communication tool that could be introduced to
future Rise coaches and interns is youcanbook.me.
Youcanbook.me is an online scheduling assistant
that could be used to plan phone conversations
with clients. Overall, the interns were pleased with
the tools used to communicate among themselves,
the Registered Dietitian Nutritionist, and the Rise
representatives.
The 12 week training led interns to feel
exceptionally prepared to provide clients with
positive and constructive feedback. By providing
comments and tips to clients, Rise interns gained
confidence in their coaching abilities and developed
positive relationships with their clients. According to
the survey 86% of interns reported the 12 weeks of
training prepared them to be successful coaches.
One respondent noted that practicing with another
intern was helpful to become familiar with a client’s
perspective of Rise. By practicing with each other,
interns felt better equipped to navigate real client
situations in the future. When asked about how the
training prepared coaches to respond to cultural
and ethnic foods, 71% of interns felt this area was
lacking. Interns commented they wished the
training would have included more ethnic foods and
addressed resources for evaluating the nutrition of
these foods.
This training opportunity provided interns
with a first of its kind experience to coach clients via
the Rise smartphone app3. The training included
application of motivational interviewing, navigation
of the app to provide nutrition coaching, and
communicating over various digital platforms. While
potential areas of improvement exist, there were
many positive aspects of the training. Interns
reported improvement in motivational interviewing
ability and increased confidence in utilizing
technology in health promotion. Current and future
Rise interns will be exceptionally prepared for the
emerging trend of telehealth in the dietetic field.
Acknowledgements: Thank you to following
interns, Jessica DaSilva, Helen Bernadt, Sonja
Ouimet, Kaitlyn Scheuermann, and Emmaline
Wright, who participated with Rise clients. Thank
you to dietetic internship faculty for their support
with this project, Erin Bergquist, MPH, RD, CNSC,
LD; Alison St. Germain, MS, RD, LD; and Tonya
Krueger, MA, RDN, LD. Special thanks to One
Medical Group and Partnership for a Healthier
America for collaboration on this project.
References
1. Foley & Lardner LLP. (2014). 2014
Telemedicine Survey [PDF]. Chicago, IL.
Foley & Lardner LLP. 2014.
2. Rhea, M., Bettles, C. (2012). Future
changes driving dietetics workforce supply
and demand: Future Scan 2012-2022. J
Acad Nutr Diet, 112 (1), S10-S24.
11| NDEP-Line | Winter 2016
3. University Relations. (2016). Iowa State
dietetic interns to work virtually with low-
income families to improve nutrition. Iowa
State University News Service. Published
July 20, 2016. Accessed October 4, 2016.
4. Gayes, L., Steele, R. (2014). A Meta-
Analysis of Motivational Interviewing
Interventions for Pediatric Heatlh Behavior
Change. J Consult Clin Psychol, 82 (3),
521-535.
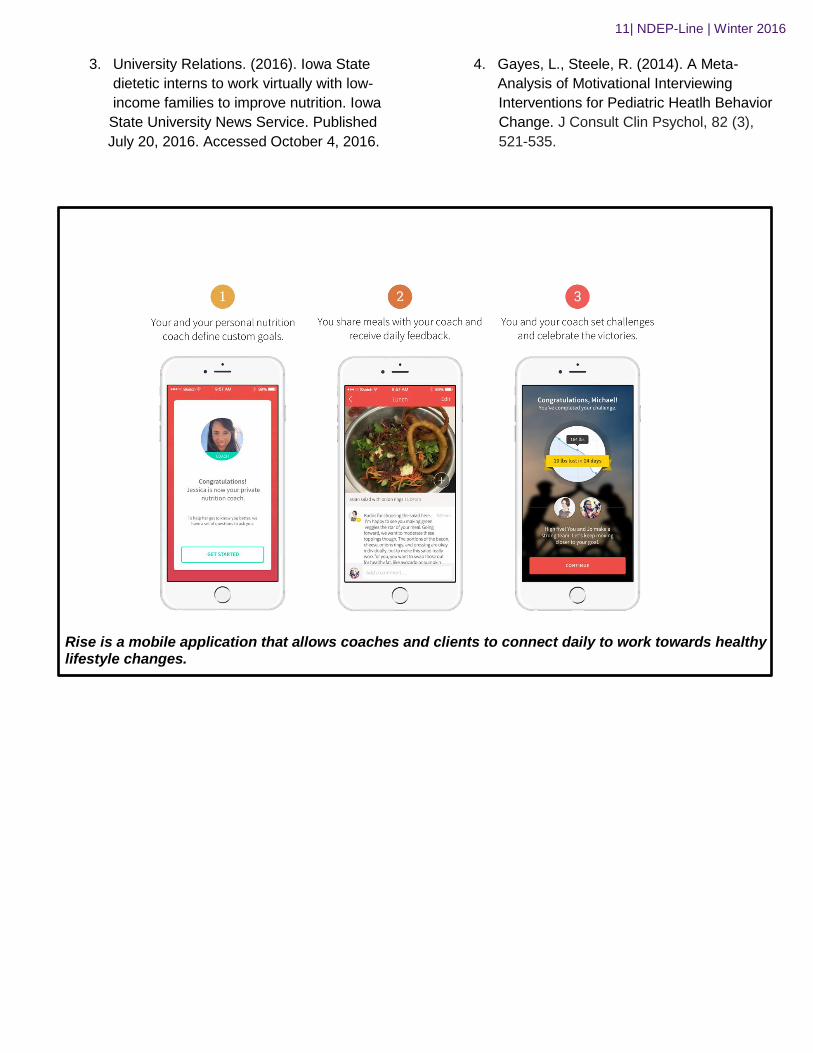
Rise is a mobile application that allows coaches and clients to connect daily to work towards healthy lifestyle changes.
12| NDEP-Line | Winter 2016
Change in Implicit Weight Bias Scores following a Multi-Faceted Bias Education Session in Undergraduate Nutrition Students and Dietetic Interns Elizabeth Tenison, MS, RDN, CSP, CNSC Riva Touger-Decker, PhD, RDN, FADA, CDN Rutgers, State University of New Jersey, School of Health Professions, Department of Nutritional Sciences [email protected] 860-231-5254
INTRODUCTION Obesity is reaching epidemic levels in the U.S. According to the 2011-2012 National Health and Examination Survey, approximately 35% of adults and 17% of youths are clinically obese. 1 Individuals who are obese are more likely to develop cardiometabolic diseases when compared to individuals with normal weight, including type 2 diabetes mellitus, hypertension, cardiovascular disease and atherosclerosis.2-5 Weight loss is a part of comprehensive lifestyle changes to reduce cardiometabolic risk factors.2-6 Successful achievement of weight reduction among individuals may require intervention by a health professional. Bleich et al studied non-physician health professionals to identify which discipline was most qualified to provide weight management counseling and found that nutrition professionals (RDNs) were determined as best suited. 7 However, health professionals including RDNs, need training for appropriate management of weight loss interventions in the individual with obesity. Research regarding weight stigma in healthcare suggests that health professionals perpetuate stereotypes regarding patients who are overweight and obese. Puhl8-11,Swift 12 Digiancinto13, Berryman 14, Welborn 15, Schwartz 16 O’Brien 17 and Peterson 18found physicians, physician assistants, RDNs, nurses, mental health workers and physical education professionals, as well as students in these professions, experience weight bias. Puhl 11, Swift 12 Berryman 14, Welborn 15 and Schwartz 16 studied weight bias among practicing RDNs and dietetics students; their scores reflected the same obesity stereotypes as other health care professionals.11, 14, 15, 16 Prior research has demonstrated that across the health professions there are beliefs that individuals who are obese are lazy, less attractive, less compliant and more depressed. 11-21 Schwartz16 and Tomiyana22
explored the relationship between age and BMI and expression of weight bias among physicians, dietitians, psychologists and pharmacologists who specialized in the treatment of persons with obesity. The results indicated that the strongest implicit bias was held by younger participants. Participants who self-reported their weight as “normal” expressed more negative attitudes toward individuals who were obese than participants who self-reported their weight as “overweight”. 16, 22 Puhl et al9 examined attitudes and beliefs of graduate students in physician assistant, psychology, medicine and psychiatry programs regarding the medical management of a patient who is overweight or obese. The researchers found student trainees viewed this patient population as difficult to counsel, lacking motivation and demonstrating non-compliance. Students who held the strongest weight bias expressed the greatest frustrations in the care and treatment of individuals with obesity. 9 Swift et al12 used the Fat Phobia 23 and Beliefs about Obese People (BAOP)24 scales to explore weight bias among dietetic, medical and nursing students. They reported that similar negative attitudes toward obesity existed among these student groups. Puhl’s and Swift’s studies 9,
11, 12 suggest that bias awareness training with nutrition and dietetic students is warranted.
Weight bias education is needed for students at all levels of the health professions curricula. The present study aimed to expand the work of Swift, Poustchi and O’Brien by assessing weight bias with three different scales among undergraduate nutrition students and dietetic interns. 12, 17, 26 In an effort to explore attitudes about weight bias among undergraduate nutrition students and dietetic interns, this study sought to determine implicit bias before and after a multifaceted education intervention in the classroom. The primary aims of this retrospective study were to assess the changes in implicit weight bias scores on the BAOP24 (Beliefs
13| NDEP-Line | Winter 2016
About Obese Persons Scale), ATOP24 (Attitude Toward Obese Persons Scale) and DBS26 (Dieting Belief Scale) among undergraduate nutrition students and dietetic interns from before to after a session on weight bias among health professionals. The BAOP24 measures the extent of belief that obesity is caused by lack of personal control, the ATOP24 measures attitudes and perceptions toward persons with obesity and the DBS26 measures locus of control. METHODS Study Design and Participants This study was a retrospective analysis of data collected at the University of Saint Joseph. The research protocol was approved by the Institutional Review Boards (IRB) of the University of St Joseph (original study protocol) and Rutgers University (current study protocol). Participants were students enrolled in an undergraduate medical nutrition therapy course (n=20) and a dietetic internship course (n=28) taught by the Principal Investigator (PI). All participants completed a demographic questionnaire which included questions about age, student group, height and weight and the three implicit weight bias scales (BAOP Scale24, ATOP Scale24 and DBS26) to determine beliefs toward individuals with obesity. All instruments were coded with unique identifiers for the purpose of matched pairs analyses. The week after the students completed the scales, both groups of students participated in a multi-faceted weight bias education session taught by the PI. The education session included professionally prepared weight bias awareness training videos entitled:” Weight Prejudice: Myths and Facts” and “Weight Bias in Health Care”27 as well as a group discussion led by the PI exploring questions provided by the Rudd Center for Food Policy and Obesity. 27 Participants engaged in a dialogue that included personal experiences of bias and observation of bias expressed by family members, co-workers, instructors and other health professionals. At the conclusion of the session, the same three scales (BAOP Scale24, ATOP Scale24 and DBS26) were completed by participants and placed in envelopes labeled with their unique identifiers and sealed. Outcome Measures The BAOP24 uses eight Likert scale questions
which assess beliefs about the underlying causes of obesity.25 BAOP scores range from 0 to 48 with a higher score indicating a stronger belief that obesity is driven by genetic factors as opposed to lack of self-control in the individual.25 The ATOP24includes 20 Likert Scale questions that measure perceptions and attitudes about individuals with obesity. ATOP scores range from 0 to 120 with a higher ATOP score reflecting more positive attitudes about individuals with obesity.24, 25, 28 The DBS26 has 16 Likert Scale questions focused on the locus of control. On the DBS instrument, higher scores indicate a belief that weight is controlled by one’s own behaviors and the locus of weight control is internal. Scores for DBS use a reference range of 45 to 86. 26 No score parameters were defined for the degree of positive or negative association by the authors of the BAOP, ATOP or DBS scales.
Data Analysis The data were entered into SPSS v22.0 (2014 IBM Corporation, Armonk, New York) and analyzed by the PI. Assumptions of normality for parametric tests were met. Descriptive statistics were calculated for the demographic characteristics, age and self-reported BMI. Total scores were calculated for the pre- and post- BAOP, ATOP and DBS scales. Paired t-tests were used to analyze changes in implicit bias scale scores from pre to post education intervention. Based on prior research by Schwartz16 and Tomiyana22 which supported relationships between age, weight and scale scores, Pearson’s product moment correlations were used to analyze relationships between pretest bias scale scores and age and BMI. The a priori alpha was set at p≤ 0.05 for all statistical analyses. The hypotheses tested were that there would be significant increases on the BAOP24 scale scores from pre- to post- intervention (higher score indicates obesity is not under one’s control) and significant increases in the ATOP24 scale scores from pre- to post- intervention (higher score indicates a more positive attitude toward persons with obesity). The third hypotheses was that there would be a significant decrease in the DBS26 scale score from pre- to post- intervention (higher scores indicate the locus of control is internal). RESULTS All three scales were completed at both time points by all 48 participants. Demographic characteristics
14| NDEP-Line | Winter 2016
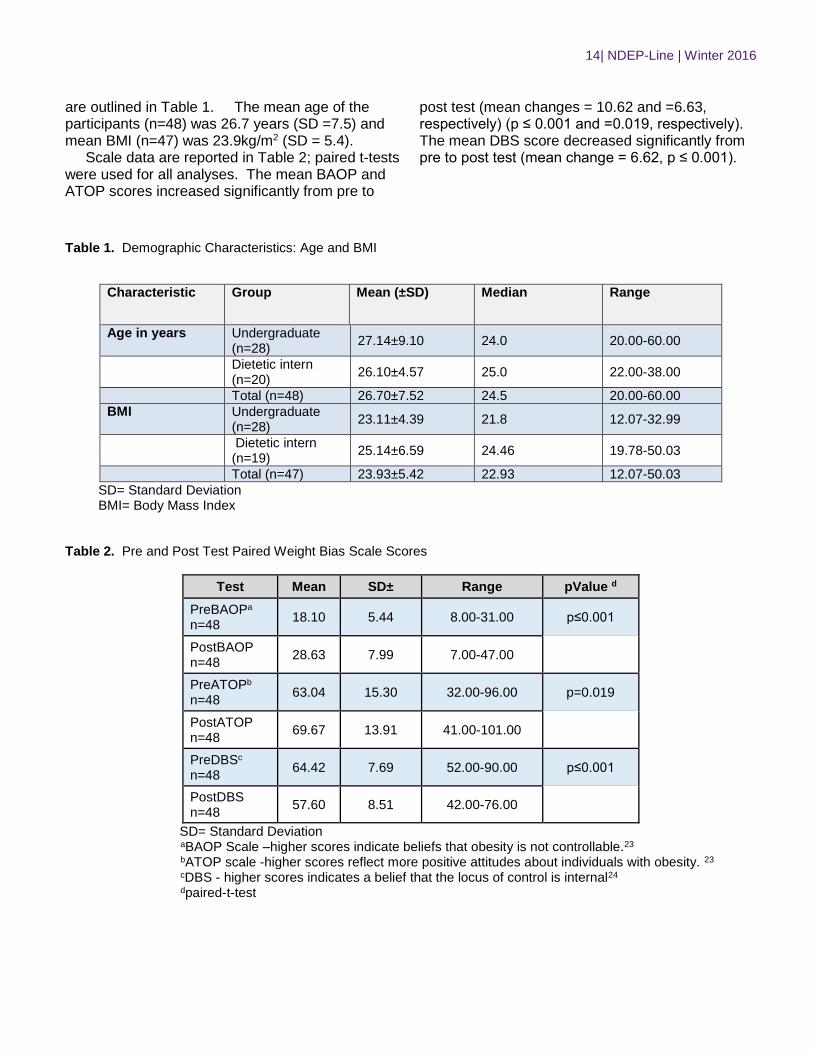
are outlined in Table 1. The mean age of the participants (n=48) was 26.7 years (SD =7.5) and mean BMI (n=47) was 23.9kg/m2 (SD = 5.4). Scale data are reported in Table 2; paired t-tests were used for all analyses. The mean BAOP and ATOP scores increased significantly from pre to
post test (mean changes = 10.62 and =6.63, respectively) (p ≤ 0.001 and =0.019, respectively). The mean DBS score decreased significantly from pre to post test (mean change = 6.62, p ≤ 0.001).
Table 1. Demographic Characteristics: Age and BMI
Characteristic Group Mean (±SD) Median Range
Age in years Undergraduate (n=28)
27.14±9.10 24.0 20.00-60.00
Dietetic intern (n=20)
26.10±4.57 25.0 22.00-38.00
Total (n=48) 26.70±7.52 24.5 20.00-60.00
BMI Undergraduate (n=28)
23.11±4.39 21.8 12.07-32.99
Dietetic intern (n=19)
25.14±6.59 24.46 19.78-50.03
Total (n=47) 23.93±5.42 22.93 12.07-50.03
SD= Standard Deviation BMI= Body Mass Index
Table 2. Pre and Post Test Paired Weight Bias Scale Scores
Test Mean SD± Range pValue d
PreBAOPa n=48
18.10 5.44 8.00-31.00 p≤0.001
PostBAOP n=48
28.63 7.99 7.00-47.00
PreATOPb
n=48 63.04 15.30 32.00-96.00 p=0.019
PostATOP n=48
69.67 13.91 41.00-101.00
PreDBSc
n=48 64.42 7.69 52.00-90.00 p≤0.001
PostDBS n=48
57.60 8.51 42.00-76.00
SD= Standard Deviation
aBAOP Scale –higher scores indicate beliefs that obesity is not controllable.23
bATOP scale -higher scores reflect more positive attitudes about individuals with obesity. 23
cDBS - higher scores indicates a belief that the locus of control is internal24
dpaired-t-test

15| NDEP-Line | Winter 2016
DISCUSSION The hypotheses explored that there would be significant increases in the BAOP and ATOP scores and significant decreases in the DBS implicit weight bias scores would change significantly from pre to post intervention in the sample of undergraduate nutrition students and dietetic interns were supported. The findings of this study are consistent with findings reported by others.17, 27,30 Poustchi et al 27 and Swift et al30 utilized bias awareness videos from the Rudd Center for Food Policy and Obesity27 in pretest posttest education intervention studies with graduate dietetic students and second and third year medical students, respectively. Both found significant increases in the mean implicit BAOP bias scores from pre to post intervention. In a randomized controlled trial, O’Brien et al17conducted a 1 hour per week, 12 week education intervention with three study arms (alcohol in youth, diet and physical activity in obesity and genes and the environment in obesity) among students enrolled in an undergraduate public health program. Implicit bias was measured using the BAOP and DBS scales pre and post intervention. The results revealed a significant increase in BAOP bias scores in the treatment group “diet and physical activity in obesity”, but no significant differences in the other treatment groups. A significant decrease in mean DBS scores was reported for the three treatment groups.17 The pretest BAOP scale answers among participants in the present study supported beliefs that obese people have a lack of willpower, simply eating more than non-obese people without a biological component to obesity. Following the intervention, posttest BAOP scale scores increased significantly. Higher mean BAOP scores post intervention suggest that participants believe that obesity is not under an individual’s control.24 Pretest ATOP scale answers reflected negative attributes such as obese people are not as happy or not as successful as those who are not obese. Higher mean ATOP scores indicate participants held more positive attitudes toward individuals with obesity. 24 The pretest DBS answers reflected attributes of internal locus of control. The significant decrease at posttest reflects attributes of external locus of control. The lower mean DBS score post intervention suggests that participants were less likely to believe a person’s behaviors control weight and more likely to believe obesity is caused by outside factors such as genetics or environment.26
The bias awareness intervention used in this pilot study represents one approach to weight stigma education. Weight bias reduction interventions may be classified as interventions that focus on obesity causality and controllability, empathy or social consensus techniques to reduce weight bias expression.32, 33 The pedagogy includes lectures, videos and written materials to address the complex etiology of obesity and increase the students’ understanding that obesity may be outside of an individual’s control, considering genetic and biological factors.12, 17 The limitations of this study include the lack of a control group and the use of a small convenience sample from a single institution. The small sample size limits generalizability as well. The strengths of the study include the use of three validated implicit bias scales to determine change in bias. Student engagement using a combination of videos, written material and verbal discussion was high. They were able to engage in a dialogue about weight bias in health professionals. Participants in this study, who served as their own controls, experienced a change in implicit bias expression as measured by the scores on three different scales. CONCLUSIONS The primary aims of this study, to determine the changes in implicit weight bias scores (BAOP, ATOP and DBS) among undergraduate nutrition students and dietetic interns following a multifaceted education session on weight bias were achieved. The results revealed significant changes in mean scores from pre to post intervention among undergraduate nutrition students and dietetic interns who participated in a bias awareness intervention. These changes reflected a reduction in the implicit weight bias expressed among this sample of undergraduate and graduate students. IMPLICATIONS The results of this study support the need for further research regarding weight bias education among dietetics students. Future studies may benefit from inclusion of a control group in a randomized controlled trial with a larger sample size from multiple colleges and universities. Addressing weight bias in dietetics education can help prepare future practitioners to provide appropriate nutrition intervention and treatment for persons with obesity. Exploring effective pedagogy on expression of weight bias among
16| NDEP-Line | Winter 2016
undergraduate nutrition students and dietetic interns is indicated. References
1. Ogden, C., Carroll, M., Kit, BK., Flegal, K. Prevalence of obesity in the United States, 2011-2012. JAMA. 2014; 311(8): 806-814.
2. Wadden, T., Volger, S., Sarwer, D., Vetter, M., Tsai, A., et al. A Two Year Randomized Trial of Obesity Treatment in Primary Care Practice. N Engl J Med. 2011; 365:1969-79.
3. Parker, A., Byham-Gray, L., Denmark, R., & Winkle, P. The effect of Medical Nutrition Therapy by a Registered Dietitian Nutritionist in Patients with Prediabetes Participating in a Randomized Controlled Research Trial. J Acad Nutr Diet. 2014; 114: 1739-1748.
4. Wing, R., Leng, W., Wadden, T., Safford, M., Knowler, W., Bertoni, A. et al. Benefits of Modest Weight Loss in Improving Cardiovascular Risk Factors in Overweight and Obese Individuals with Type 2 Diabetes. Diabetes Care. 2011; 34: 1481-1486.
5. Gelber R., Gaziano J., Orav E., Manson J., Buring J., Kurth T. Measures of Obesity and Cardiovascular Risk among Men and Women. Journal of the American College of Cardiology. 2008;52(8):605-615. doi:10.1016/j.jacc.2008.03.066.
6. Share, B., Naughton, G., Obert, P., Peat, J., Aumand, E. & Kemp, J. Effect of a Multidisciplinary Lifestyle Intervention on Cardiometabolic Risk Factors in Young Women with Abdominal Obesity: A Randomised Controlled Trial. Plos One. 10(6): e130270. Doi.1371/journal.pone.0130270.
7. Bleich, S., Bandara, S., Bennett, W., Cooper, L., and Gudzune, K. Enhancing the Role of Nutrition Professionals in Weight Management: A Cross-Sectional Survey. Obesity. 2015; 23: 464-460.
8. Puhl, R., Latner, J., King, K., Luedicke, J. Weight Bias among Professionals Treating Eating Disorders: Attitudes about Treatment and Perceived Patient Outcomes. International Journal of Eating Disorders. 2014; 47: 65-75.
9. Puhl, R., Luedicke, J., Grilo, C. Obesity Bias in Training: Attitudes, Beliefs, and Observations among advanced trainees in Professional Health Disciplines. Obesity. 2014; 22:1008-1015.
10. Puhl, R., Heuer, C., The Stigma of Obesity: A Review and Update. Obesity. 2009. DOI:10.1038/oby.2008.636.
11. Puhl, R., Wharton, C., Heuer, C. Weight Bias among Dietetic Students. Implications for Treatment Practices. J Am Diet Assoc. 2009; 109:438-444.
12. Swift, J., Hanlon, S., El-Redy, L., Puhl, R., Glazebrook, C. Weight bias among UK trainee dietitians, doctors, nurses and nutritionists. J Hum Nutr Diet.2013; 26: 395-402.
13. DiGiancinto, D., Gildon, B., Stamile, E., Aubrey, J. Weight-Biased Health Professionals and the Effects on Overweight Patients. Journal of Diagnostic Medical Sonography. 2015; 31: 132-135.
14. Berryman, D., Dubale, B., Manchester, D., Mittelstaedt, R. Dietetic Students Possess Negative Attitudes toward Obesity Similar to Nondietetics Students. J Am Diet Assoc. 2006; 106: 1678-1682.
15. Welborn. S., Comparison of Obesity Bias, Attitudes and Beliefs among undergraduate Dietetic students, Dietetic interns and Practicing dietitians. Electronic Theses and Dissertations. 2013 Paper 1104. http://dc.etsu.edu/etd/1104
16. Schwartz, M., Chambliss, H., Brownell, K., Blair, S., Billlington, C. Weight Bias among Health Professionals Specializing in Obesity. Obesity Research. 2003; 9: 1033-1039.
17. O’Brien, K., Puhl, R., Latner, D., Mir, A., Hunter, J. Reducing Anti-Fat Prejudice in Pre-service Health Students: A randomized Trial. Obesity. 2010; DOI:10.0338/oby.2010.79.
18. Peterson, J., Puhl, R., and Leudicke, J. An experimental assessment of physical educator’s expectations and attitudes: The importance of student weight and gender. Journal of School Health. 2012; 82:432-440.
19. Amy, N., Aalborg, A., Lyons, P., & Keranen, L. Barriers to routine gynecological cancer screening for White and African-American obese women. Int. J Obes. 2006; 30: 147-155.
20. Ferrante, J., Ohman-Strickland, P., Hudson, S. et al. Colorectal cancer screening among obese and non-obese patients in primary care practices. Cancer Detect Prev.2006; 30: 459-465.
21. Teachman, B., Brownell, K. Implicit Anti-Fat Bias among Health Professionals: Is Anyone Immune? Int J of Obesity. 2001; 25: 1525-1531.
17| NDEP-Line | Winter 2016
22. Tomiyama, A., Finch, L., Belsky, A., Buss, J., Finley, C., Schwartz, M., & Daubenmier, J. Weight bias in 2001 versus 2013: Contradictory Attitudes among Obesity Researchers and Health Professionals. Obesity. 2015; 23: 46-53.
23. Robinson, B., Bacon, J., O’Reilly, J. Fat Phobia: Measuring, Understanding, and Changing Anti-fat Attitudes. International Journal of Eating Disorders. 1993; 14: 467-480.
24. Allison, D., Basile, V. and Yuker, H. The measurement of attitudes toward and beliefs about obese persons. International Journal of Eating Disorders. 1991; 10: 599-607.
25. Poutstchi, Y., Saks, N., Piasecki, A., Hahn, K., & Ferrante, J., Brief Intervention Effective in Reducing Weight Bias in Medical Students. Family Medicine. 2013;45(5):345-348.
26. Stotland, S, Zuroff, D. A New Measure of Weight Locus of Control: The Dieting Beliefs Scale. Journal of Personality Assessment. 1990; 54: 191-203.
27. Weight Bias and Stigma. UCONN Rudd Center for Food Policy and Obesity website. Retrieved from http://biastoolkit.uconnruddcenter.org/module1.html. January 3, 2016.
28. Puhl, R. & Brownell, K. Confronting and Coping with Weight Stigma: An investigation of Overweight and Obese Adults. Obesity.2006; 14:1802-1807.
29. Swift, JA, Tischler, V, Markham, S, Gunning, I, Glazebrook, C, .Beer, C, Puhl, R. Are Anti-Stigma Films a Useful Strategy for Reducing Weight Bias among Trainee Healthcare Professionals? Results of a Pilot Randomized Control Trial. Obes Facts 2013; 6:91-102. DOI: 10.1159/000348714.
30. Persky, S., Eccleston, C. Medical students bias and care recommendations for an obese versus non-obese virtual patient. Int J Obes.2011; 35: 728-735.
31. Sabin, J., Marini, M., Nosek, B., Implicit and Explicit anti-fat bias among a large sample of medical doctors by BMI, race/ethnicity and gender. PLos One. 2012; 7(11):e48448.
32. Lee, M., Ata, R., Brannick, M. Malleability of weight-biased attitudes and beliefs: A meta-analysis of weight bias reduction interventions. Body Image. 2014;11: 251-259.
33. Danielsdottir, S., O’Brien, KS., and Ciao, A. Anti-fat Prejudice Reduction: A Review of Published Studies. Obes Facts. 2010; 3: 47-58.
18| NDEP-Line | Winter 2016
Simulation within Dietetics Education: How
Educators’ Familiarity and Needs Have
Changed with Increased Simulation-Related
Efforts Brittney Patterson, MS, RD Department of Nutrition, Food Science & Packaging San José State University Kasuen Mauldin, PhD, RD, Assistant Professor, Department of Nutrition, Food Science & Packaging San José State University [email protected] (408) 924-3109
INTRODUCTION Simulation is an educational method in which students learn by doing in an environment that is set up to mimic various aspects of the real world. One advantage of the hands-on learning in simulated environments is mistakes will not cause harm.1 Prior to going through the simulation experience, students receive objectives and goals to accomplish during the scenario. Technology within simulation environments can range from low- (eg, peer-to-peer), medium- (eg, computer-based), and high-fidelity (eg, realistic hospital room with life-size instructor-manipulated mannequin).2 The overall goal is to “suspend disbelief”3 to promote realism within the experience to solidify learning. Afterward, a debriefing session is held with the students, teachers, and observers to analyze the experience.
The history of simulation is far-reaching, with substantial adoption in military, space, aviation, and nuclear power industries. Medical simulation started with the use of anatomical models centuries ago, and since the 1960’s there has been an increase in use within various healthcare fields.4 Research among nursing,5 pharmacy,6 and dentistry7 students have found simulation to be an effective learning tool. Even with sound research backing up the ideology, the implementation of a new teaching modality can present challenges in the forms of cost, time, and lack of support from department heads.8
Over the past few years, there has appeared to be a surge in interest and support for using simulation within dietetics education. One such example is the seminal article by Thompson and Gutschall9 which provided a step-by-step framework for dietetic educators to start developing
and using simulation. The primary purpose of this study was to determine if and how simulation needs of dietetic educators have changed in accordance with the simulation-related efforts between academic year (AY) 2012-2013 and AY 2015-2016. The secondary purpose was to assess if dietetics educators would be interested in online simulation resources.
MATERIALS AND METHODS To assess dietetic educator demographics, barriers, needs, and desires for online resources, an anonymous 8-question “simulation needs assessment” survey was created. The survey was first distributed among educators at a 2013 Food and Nutrition Conference and Expo (FNCE) talk regarding simulation. All attendees were eligible to participate in the voluntary survey. The same survey was distributed via listserv email to the Nutrition and Dietetics Educators and Preceptors (NDEP) practice group in January 2016. NDEP participants were directed to the survey online that was hosted through Qualtrics.
Three methods were employed to quantify simulation-related efforts within dietetics. First, publications on ScienceDirect between AY 2012-2013 (ie, June 1, 2012 - May 31, 2013), AY 2013-2014, AY 2014-2015, and AY 2015-2016, were searched for the terms “dietetics” and “simulation”. Second, the 2012-2015 FNCE programs were audited for simulation-related presentation and posters. Third, the Academy of Nutrition and Dietetics (AND) webpages regarding simulation were reviewed for grants, funding, and standards.
Since the survey was distributed to two different groups, averages, frequencies, and percentages were completed in order to compare
19| NDEP-Line | Winter 2016
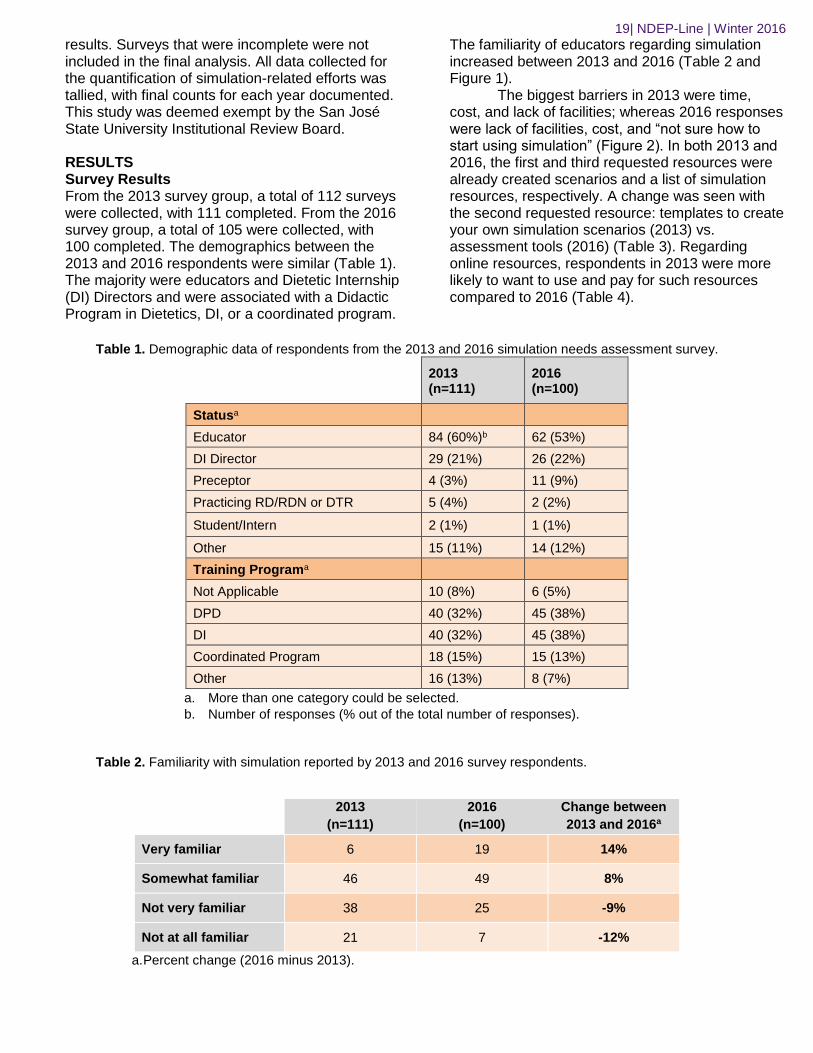
results. Surveys that were incomplete were not included in the final analysis. All data collected for the quantification of simulation-related efforts was tallied, with final counts for each year documented. This study was deemed exempt by the San José State University Institutional Review Board. RESULTS Survey Results From the 2013 survey group, a total of 112 surveys were collected, with 111 completed. From the 2016 survey group, a total of 105 were collected, with 100 completed. The demographics between the 2013 and 2016 respondents were similar (Table 1). The majority were educators and Dietetic Internship (DI) Directors and were associated with a Didactic Program in Dietetics, DI, or a coordinated program.
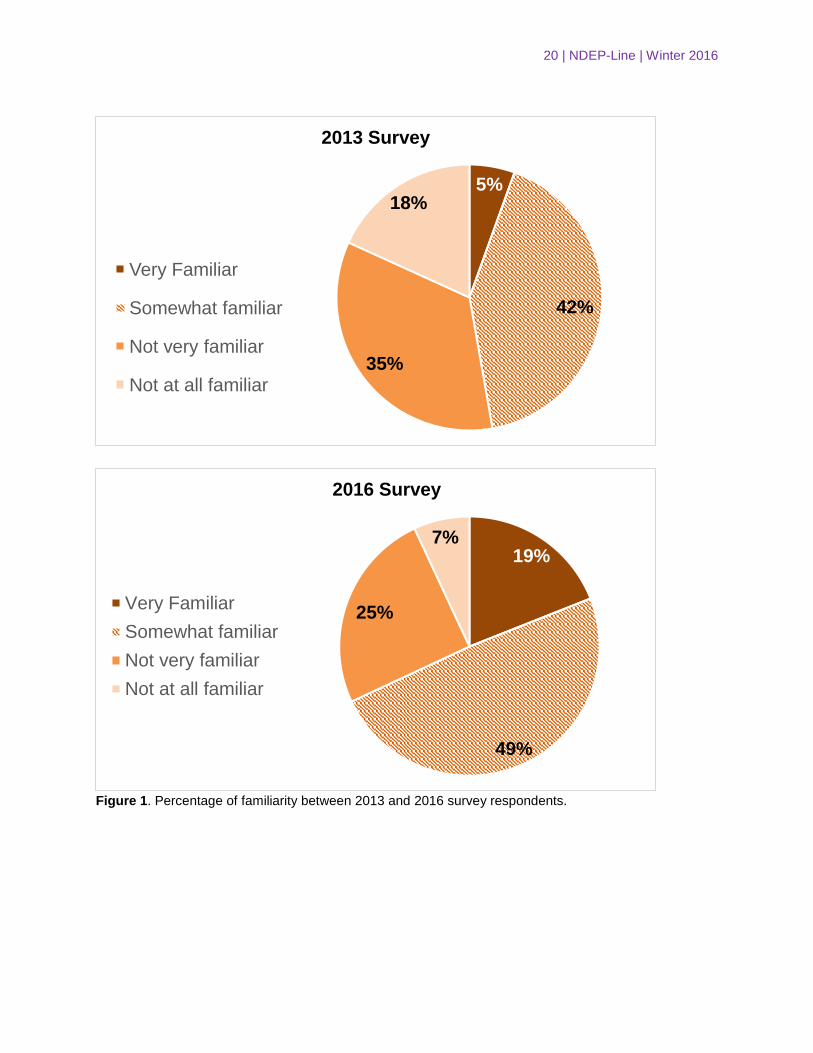
The familiarity of educators regarding simulation increased between 2013 and 2016 (Table 2 and Figure 1).
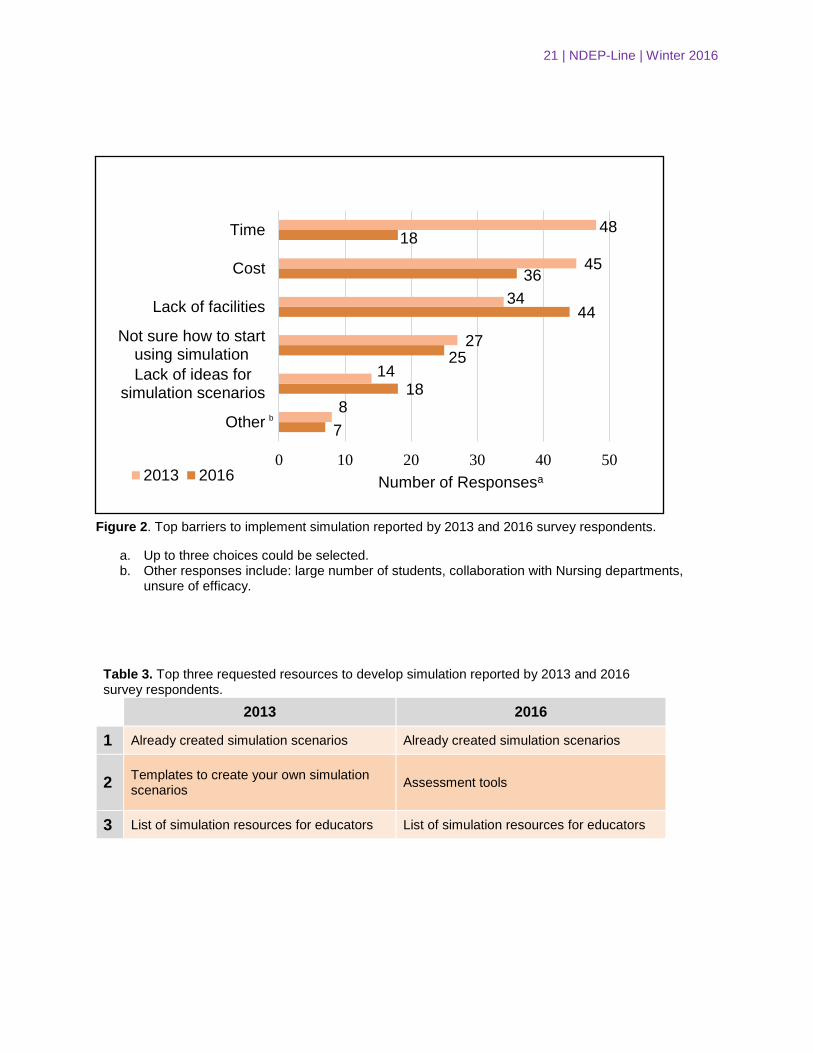
The biggest barriers in 2013 were time, cost, and lack of facilities; whereas 2016 responses were lack of facilities, cost, and “not sure how to start using simulation” (Figure 2). In both 2013 and 2016, the first and third requested resources were already created scenarios and a list of simulation resources, respectively. A change was seen with the second requested resource: templates to create your own simulation scenarios (2013) vs. assessment tools (2016) (Table 3). Regarding online resources, respondents in 2013 were more likely to want to use and pay for such resources compared to 2016 (Table 4).
Table 1. Demographic data of respondents from the 2013 and 2016 simulation needs assessment survey.
2013 (n=111)
2016 (n=100)
Statusa
Educator 84 (60%)b 62 (53%)
DI Director 29 (21%) 26 (22%)
Preceptor 4 (3%) 11 (9%)
Practicing RD/RDN or DTR 5 (4%) 2 (2%)
Student/Intern 2 (1%) 1 (1%)
Other 15 (11%) 14 (12%)
Training Programa
Not Applicable 10 (8%) 6 (5%)
DPD 40 (32%) 45 (38%)
DI 40 (32%) 45 (38%)
Coordinated Program 18 (15%) 15 (13%)
Other 16 (13%) 8 (7%)
a. More than one category could be selected.
b. Number of responses (% out of the total number of responses).
Table 2. Familiarity with simulation reported by 2013 and 2016 survey respondents.
2013
(n=111)
2016
(n=100)
Change between
2013 and 2016a
Very familiar 6 19 14%
Somewhat familiar 46 49 8%
Not very familiar 38 25 -9%
Not at all familiar 21 7 -12%
a. Percent change (2016 minus 2013).
20 | NDEP-Line | Winter 2016
Figure 1. Percentage of familiarity between 2013 and 2016 survey respondents.
5%
42%
35%
18%
2013 Survey
Very Familiar
Somewhat familiar
Not very familiar
Not at all familiar
19%
49%
25%
7%
2016 Survey
Very Familiar
Somewhat familiar
Not very familiar
Not at all familiar
21 | NDEP-Line | Winter 2016
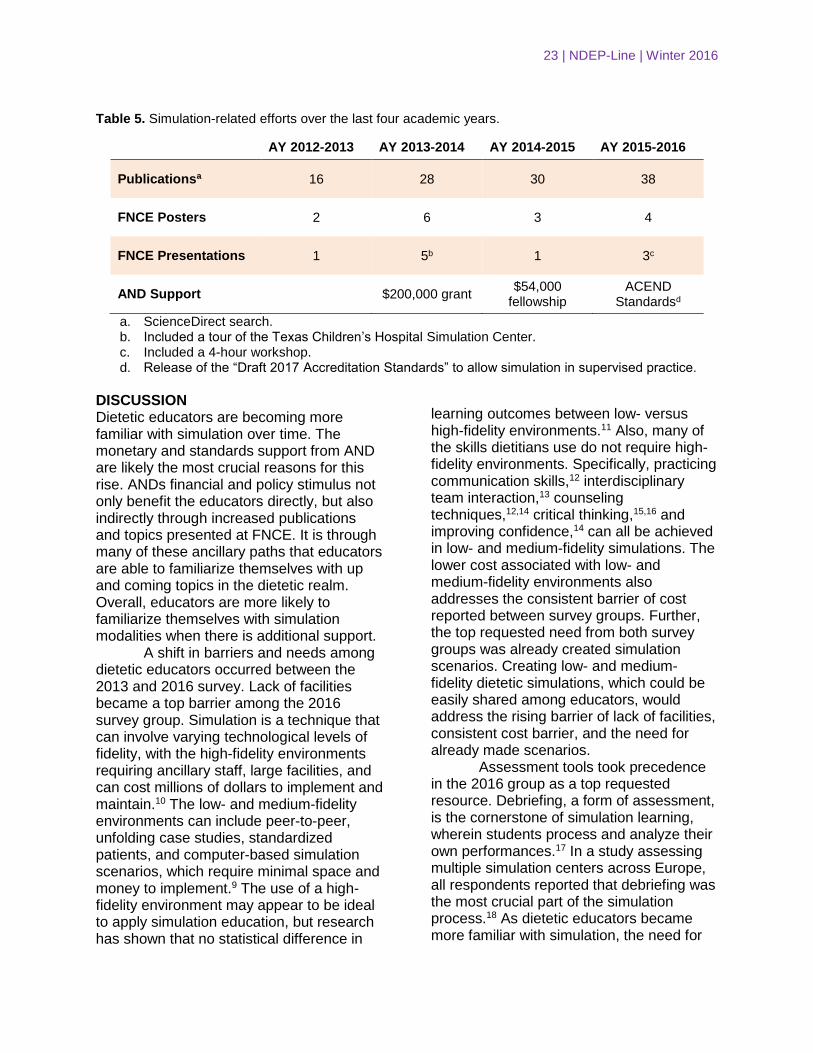
Figure 2. Top barriers to implement simulation reported by 2013 and 2016 survey respondents.
a. Up to three choices could be selected. b. Other responses include: large number of students, collaboration with Nursing departments,
unsure of efficacy.
Table 3. Top three requested resources to develop simulation reported by 2013 and 2016 survey respondents.
2013 2016
1 Already created simulation scenarios Already created simulation scenarios
2 Templates to create your own simulation scenarios
Assessment tools
3 List of simulation resources for educators List of simulation resources for educators
7
18
25
44
36
18
8
14
27
34
45
48
0 10 20 30 40 50
Other
Lack of ideas forsimulation scenarios
Not sure how to startusing simulation
Lack of facilities
Cost
Time
Number of Responsesa2013 2016
b
22 | NDEP-Line | Winter 2016
Table 4. Change in likelihood to use and pay for an online simulation resource between 2013 and 2016
survey respondents.
Use an online resource
Pay for an online resource
Very likely -12% -19%
Somewhat likely 7% 8%
Not very likely 4% 5%
Not at all likely 1% 6%
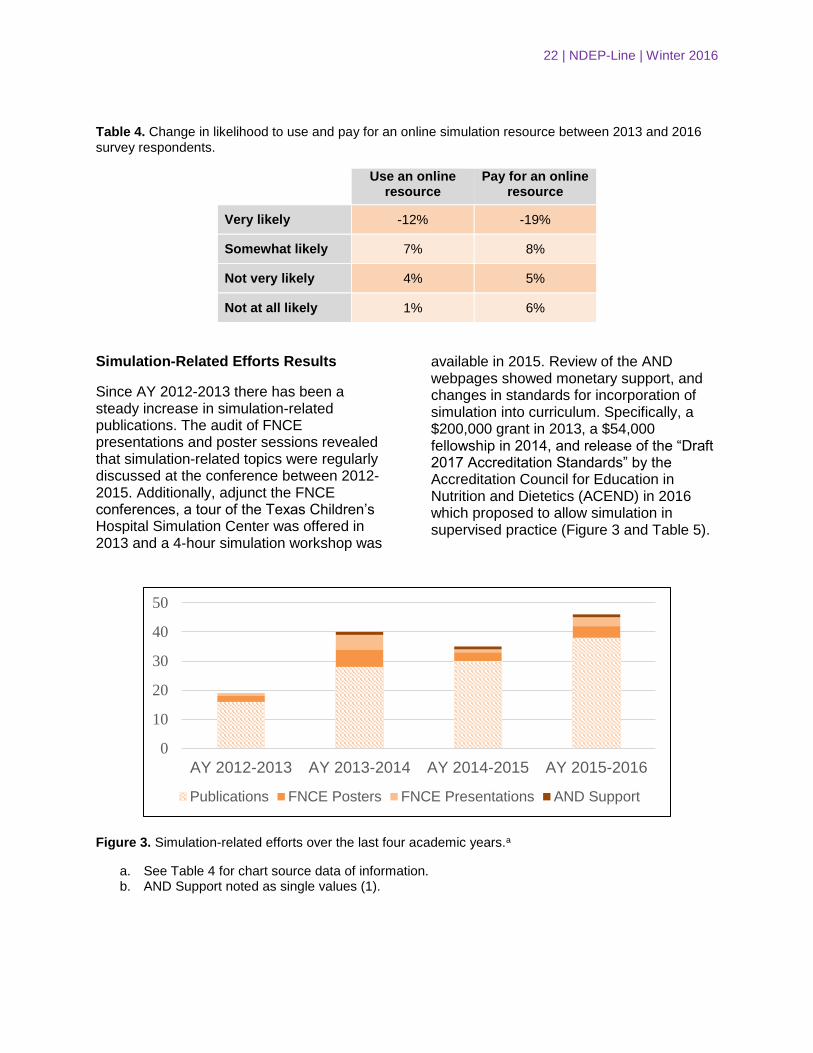
Simulation-Related Efforts Results
Since AY 2012-2013 there has been a steady increase in simulation-related publications. The audit of FNCE presentations and poster sessions revealed that simulation-related topics were regularly discussed at the conference between 2012-2015. Additionally, adjunct the FNCE conferences, a tour of the Texas Children’s Hospital Simulation Center was offered in 2013 and a 4-hour simulation workshop was
available in 2015. Review of the AND webpages showed monetary support, and changes in standards for incorporation of simulation into curriculum. Specifically, a $200,000 grant in 2013, a $54,000 fellowship in 2014, and release of the “Draft 2017 Accreditation Standards” by the Accreditation Council for Education in Nutrition and Dietetics (ACEND) in 2016 which proposed to allow simulation in supervised practice (Figure 3 and Table 5).
Figure 3. Simulation-related efforts over the last four academic years.a
a. See Table 4 for chart source data of information. b. AND Support noted as single values (1).
0
10
20
30
40
50
AY 2012-2013 AY 2013-2014 AY 2014-2015 AY 2015-2016
Publications FNCE Posters FNCE Presentations AND Support
23 | NDEP-Line | Winter 2016
Table 5. Simulation-related efforts over the last four academic years.
AY 2012-2013 AY 2013-2014 AY 2014-2015 AY 2015-2016
Publicationsa 16 28 30 38
FNCE Posters 2 6 3 4
FNCE Presentations 1 5b 1 3c
AND Support $200,000 grant $54,000
fellowship ACEND
Standardsd
a. ScienceDirect search. b. Included a tour of the Texas Children’s Hospital Simulation Center. c. Included a 4-hour workshop. d. Release of the “Draft 2017 Accreditation Standards” to allow simulation in supervised practice.
DISCUSSION Dietetic educators are becoming more familiar with simulation over time. The monetary and standards support from AND are likely the most crucial reasons for this rise. ANDs financial and policy stimulus not only benefit the educators directly, but also indirectly through increased publications and topics presented at FNCE. It is through many of these ancillary paths that educators are able to familiarize themselves with up and coming topics in the dietetic realm. Overall, educators are more likely to familiarize themselves with simulation modalities when there is additional support.
A shift in barriers and needs among dietetic educators occurred between the 2013 and 2016 survey. Lack of facilities became a top barrier among the 2016 survey group. Simulation is a technique that can involve varying technological levels of fidelity, with the high-fidelity environments requiring ancillary staff, large facilities, and can cost millions of dollars to implement and maintain.10 The low- and medium-fidelity environments can include peer-to-peer, unfolding case studies, standardized patients, and computer-based simulation scenarios, which require minimal space and money to implement.9 The use of a high-fidelity environment may appear to be ideal to apply simulation education, but research has shown that no statistical difference in
learning outcomes between low- versus high-fidelity environments.11 Also, many of the skills dietitians use do not require high-fidelity environments. Specifically, practicing communication skills,12 interdisciplinary team interaction,13 counseling techniques,12,14 critical thinking,15,16 and improving confidence,14 can all be achieved in low- and medium-fidelity simulations. The lower cost associated with low- and medium-fidelity environments also addresses the consistent barrier of cost reported between survey groups. Further, the top requested need from both survey groups was already created simulation scenarios. Creating low- and medium-fidelity dietetic simulations, which could be easily shared among educators, would address the rising barrier of lack of facilities, consistent cost barrier, and the need for already made scenarios.
Assessment tools took precedence in the 2016 group as a top requested resource. Debriefing, a form of assessment, is the cornerstone of simulation learning, wherein students process and analyze their own performances.17 In a study assessing multiple simulation centers across Europe, all respondents reported that debriefing was the most crucial part of the simulation process.18 As dietetic educators became more familiar with simulation, the need for
24 | NDEP-Line | Winter 2016
assessment tools understandably became a priority.
As reported by ACEND,19 demand for dietetic internships is increasing despite the lack of additional internship sites. In April 2009 matching, there were double the applications as there were sites available to take dietetic interns. This competitiveness is not unique to the dietetics field and has been seen in various other healthcare fields, specifically nursing.20 According to Jeffries,21 nursing research has shown the possibility that the majority of clinical learning will be done through simulation training. Given the updated standards support by AND, it is possible to see how simulation could aid in alleviating the pressure of a lack of internship sites.
The desire to use and pay for online resources decreased over time despite the reported need for a list of simulation resources as a top request among both groups. This decrease could have been associated with the different methods of survey disbursement. The 2013 group received a paper copy of the survey whereas the 2016 group took the survey online. The online survey method could have inadvertently targeted educators who may have been more familiar with searching for information online. Regardless of the change in desire for online resources, there still appears to be a need for dissemination of simulation resources to dietetic educators.
Limitations of the research included the decreased generalizability of the data, given the different survey methods and study groups used. Also, it was not asked within the survey how educators became familiar with simulation and if they were currently using this teaching modality. This information could have furthered our understanding if familiarization with simulation was resulting in actual implementation.
The core strength to the research is that currently, no other study has looked at change over time of dietetic educators’ simulation familiarity and needs. Additionally, both survey groups had large
sample sizes. Overall, this study provides a snapshot of the barriers and needs regarding simulation within the dietetic educator community. CONCLUSION Between AY 2012-2013 and AY 2015-2016, dietetic educators’ familiarity has increased and needs are changing with the rise in simulation-related efforts. Future research and support by AND needs to address these reported needs to allow for cohesive incorporation of simulation within curriculum to meet 2017 ACEND standards.
ACKNOWLEDGEMENTS The authors would like to thank the Circle of Friends Research Scholarship Award from the Department of Nutrition, Food Science, and Packaging at San José State University for partially funding this research. References
1. Lateef F. Simulation-based learning: Just like the real thing. J Emerg Trauma Shock. 2010; 3:348-352.
2. Motola I, Devine LA, Chung HS, Sullivan JE, Issenberg SB. Simulation in healthcare education: A best evidence practical guide. AMEE guide no. 82. Med Teach. 2013; 35(10):e1511-e1530. doi: 10.3109/0142159X.2013.818632.
3. Seropian MA. General concepts in full scale simulation: Getting started. Anesth Analg. 2003; 97:1695-1705.
4. Bradley P. The history of simulation in medical education and possible future directions. Med Educ. 2006; 40:254-262.
5. Alinier G, Hunt B, Gordon R, Harwood C. Effectiveness of intermediate‐fidelity simulation training technology in undergraduate nursing education. J Adv Nurs. 2006; 54:359-369.
6. Seybert AL, Smithburger PL, Kobulinsky LR, Kane-Gill SL. Simulation-based learning versus problem-based learning in an acute
25 | NDEP-Line | Winter 2016
care pharmacotherapy course. Simul Healthc. 2012; 7:162-165.
7. Urbankova A. Impact of computerized dental simulation training on preclinical operative dentistry examination scores. J Dent Educ. 2010; 74:402-409.
8. Adamson K. Integrating human patient simulation into associate degree nursing curricula: Faculty experiences, barriers, and facilitators. Clin Simul Nurs. 2010; 6:e75-e81. doi:10.1016/j.ecns.2009.06.002
9. Thompson KL, Gutschall MD. The time is now: A blueprint for simulation in dietetics education. J Acad Nutr Diet. 2015; 115:183-194.
10. Tuoriniemi P, Schott-Baer D. Implementing a high-fidelity simulation program in a community college setting. Nurs Educ Perspect. 2008; 29:105-109.
11. Hoadley TA. Learning advanced cardiac life support: A comparison study of the effects of low-and high-fidelity simulation. Nurs Educ Perspect. 2009; 30:91-95.
12. Puri R, Bell C, Evers WD. Dietetics students' ability to choose appropriate communication and counseling methods is improved by teaching behavior-change strategies in computer-assisted instruction. J Am Diet Assoc. 2010; 110:892-897.
13. Gibbs H, George K, Barkley R, Meyer M. Using multiple-patient simulations to facilitate interprofessional communication between dietetic and nursing students and improve nutrition care process skills. Top Clin Nutr 2015; 30:230-238.
14. Henry BW, Duellman MC, Smith TJ.
Nutrition‐based standardized patient sessions increased counseling awareness and confidence among dietetic interns. Top Clin Nutr. 2009; 24:25-34.
15. Harman T, Bertrand B, Greer A, et al. Case-based learning facilitates critical thinking in undergraduate nutrition education: Students describe the big
picture. J Acad Nutr Diet. 2015; 115:378-388.
16. Raidl MA, Wood OB, Lehman JD, Evers WD. Computer-assisted instruction improves clinical reasoning skills of dietetics students. J Am Diet Assoc. 1995; 95:868-873.
17. Fanning RM, Gaba DM. The role of debriefing in simulation-based learning. Simul Healthc. 2007; 2:115-125.
18. Rall M, Manser T, Howard S. Key elements of debriefing for simulator training. Eur J Anaesthesiol. 2000; 17:516-517.
19. Accreditation Council for Education in Nutrition and Dietetics. Availability of dietetic internship positions. http://www.eatrightacend.org/ACEND/content.aspx?id=6442485435. Accessed January 2, 2016.
20. Rutherford-Hemming T. Simulation methodology in nursing education and adult learning theory. Adult Learning. 2012; 23:129-137.
21. Jeffries PR. Dreams for the future for clinical simulation: Research and development in this hot topic area will lead to more sophisticated manikins and robots possessing even more realistic features and functionality. What is known as the high-fidelity simulator today will look simplistic when compared to the next generation of simulators in the years to come. Nurs Educ Perspect. 2009; 30:71-72.
26 | NDEP-Line | Winter 2016
2016 Outstanding Preceptor Awardees
At the NDEP Member Breakfast at FNCE in Boston, seven Outstanding Preceptors were recognized by NDEP with a 2016 Outstanding Preceptor Award. Sylvia Escott-Stump, NDEP Past-Chair, had the pleasure of presenting six of the seven awardees with a certificate. In addition to their certificate, each received $1000 from the Academy Foundation to attend FNCE.
Area 1: Anne Goetze, RD, LD, FAND, Senior Director of Nutrition Affairs, Oregon Dairy and Nutrition Council, Portland, OR, was nominated by Sara Wilson Wolfe, MS, RD.
27 | NDEP-Line | Winter 2016
Area 2: Kristin Cunningham, RD, LD, dietitian with BJC School Outreach and Youth Development, Saint Louis MO, was nominated by Camille Smith, RD, LD, dietitian with BJC School Outreach and Youth Development.
Area 3: Lynn Thomas, RD, LD, CSG, Director of Dietary Services, NHC Healthcare Lexington, West Columbia, SC, was nominated by Courtney, Lee, MS, RDN, LD, CFCS, dietitian with NHC Healthcare Lexington
28 | NDEP-Line | Winter 2016
Area 4: Katie Braun, MS, RD, LD, CNSC, Clinical Nutrition Specialist, Michael E. DeBakey VA Medical Center, Houston, TX, nominated by Kristy Becker, MS, RD, LD, CNSC, Director, Michael E. DeBakey VA Medical Center Dietetic Internship.
Area 5: Patricia Prince-Griffin, MS, RDN, LDN, Clinical Dietitian, Memphis VA Medical Center, Memphis, TN, nominated by Jacqueline Roos, MS, RDN, LDN, CDE, Memphis VA Medical Center Dietetic Internship Director.
29 | NDEP-Line | Winter 2016
Area 6: Kelly Ratteree, MPH, RD, Clinical Research Dietitian, National Institutes of Health, Bethesda, MD, nominated by Merel Kozlosky, MS, RD, Dietetic Internship Director, National Institutes of Health.
Area 7: Colette Murphy Cole, MS, RD, Community Nutritionist/Dietitian, Trinitas Regional Medical Center, Women’s Health Center, Elizabeth, NJ, nominated by M. Geraldine McKay, RD, Ed.M, Program Director, Rutgers University Medical Center.





























