Embed Size (px)
Citation preview

Needle exchange and difficulty with needle access during an ongoingHIV epidemic
Evan Wood a,b, Mark W. Tyndall a,b, Patricia M. Spittal a,b, Kathy Li a, RobertS. Hogg a,b, Michael V. O’Shaughnessy a,c, Martin T. Schechter a,b,*
a British Columbia Centre for Excellence in HIV/AIDS, St. Paul’s Hospital, Vancouver, BC, Canadab Department of Health Care and Epidemiology, University of British Columbia, 5804 Fairview Ave., Vancouver, BC, Canada V6T 1Z3
c Department of Pathology and Laboratory Medicine; University of British Columbia, Vancouver, BC, Canada
Abstract
During the mid to late 1990s, Vancouver, Canada experienced a rapid injection drug use-related HIV epidemic, despite the
presence of a well-established, high-volume, needle exchange program (NEP). The NEP presently exchanges needles through several
fixed sites, the largest of which operates in the city’s Downtown Eastside where injection drug users (IDU) are concentrated, and
through mobile exchange vans which exchange needles throughout neighboring areas. The program’s inability to prevent the
epidemic has led to persistent questions about the efficacy of needle exchange as a public health intervention. We recently sought
possible explanations for persistent needle sharing through an evaluation of the Vancouver Injection Drug Users Study (VIDUS), an
ongoing cohort study of IDU that began in 1996. In these analyses, the strongest predictor of needle sharing was difficulty accessing
needles; those who reported difficulty accessing needles were 3.5 times more likely to report sharing than those who did not have
difficulty with access. In the present study, we sought to identify reasons why IDU continued to have difficulty accessing needles
despite the efforts of the NEP. Overall, 761 active injectors were interviewed during the period June 2000�/May 2001. Of these 172
(22.6%) reported having difficulty accessing sterile needles. In a multivariate analysis, frequent cocaine injection and bingeing were
associated with difficulty accessing needles, whereas residing in the Downtown Eastside was negatively associated with difficulty.
When we evaluated IDU’s reasons for difficulty with access, the most common reasons given were the operating hours of the NEP,
difficulty meeting the needle exchange van, being away from the area where needles are exchanged, and being refused sterile needles
at pharmacies. These findings suggest that programmatic deficiencies related to the operation of the needle exchange and refusal of
pharmacists to sell needles may be primary factors related to difficulty accessing needles. # 2002 Elsevier Science B.V. All rights
reserved.
Keywords: HIV; AIDS; Needle exchange; Injection drug users; Harm reduction; Vancouver
Introduction
Studies have shown that providing injection drug
users (IDUs) access to clean needles through needle
exchange programs (NEP) substantially reduces the
transmission of HIV as well as HIV risk behaviors
(Bluthenthal, Kral, Gee, Erringer & Edlin, 2000; Des
Jarlais et al., 1996). Furthermore, needle exchange has
been shown to afford a crucial opportunity to reach
drug users and provide them with additional resources
such as HIV testing and counseling and referrals to drug
treatment (Heimer, 1998; Lurie, Reingold & Bowser,
1993; Strathdee et al., 1999).
However, NEPs remain a controversial intervention
in many countries. Opponents argue that NEPs enable
drug use, are not effective at reducing HIV transmission,
and may even promote its spread (American Journal of
Public Health, 2000Bellm, 1999; Bennett, 1998). Debate
over the efficacy of NEPs has been partially fueled by
the experience of Vancouver, Canada (Bellm, 1999;
Schechter et al., 1999). Although the city had in place
a NEP that had been ranked among the top three in
North America in terms of the proportion of drug users
ever reached and needles exchanged (Lurie et al., 1993),
in 1997 an explosive HIV epidemic characterized by an
18% annual incidence rate was observed among IDU
* Corresponding author. Tel.: �/1-604-822-3081; fax: �/1-604-806-
9044.
E-mail address: [email protected] (M.T. Schechter).
International Journal of Drug Policy 13 (2002) 95�/102
www.elsevier.com/locate/drugpo
0955-3959/02/$ - see front matter # 2002 Elsevier Science B.V. All rights reserved.
PII: S 0 9 5 5 - 3 9 5 9 ( 0 2 ) 0 0 0 0 8 - 7

residing in the city’s Downtown Eastside (Strathdee et
al., 1997b). We also observed that the prevalence of
HIV-1 among those who frequently attended the NEP
was higher than among those who attended lessfrequently (Strathdee et al., 1997b). These observations
were interpreted by some to suggest that NEPs may
exacerbate the spread of HIV (Bellm, 1999; Office of
National Drug Control Policy, 1998). Subsequently, we
demonstrated that the association between frequent
NEP attendance and HIV-1 was due to the selection
by NEPs of higher risk drug users (Schechter et al.,
1999). Furthermore, we and others have refuted thehypothesis that NEPs promote the formation of needle
sharing networks (Junge, Valente, Latkin, Riley &
Vlahov, 2000; Schechter et al., 1999).
Since the overwhelming majority of studies have
found a benefit of making sterile needles accessible to
IDU, a critical question surrounds the safest and most
effective means of providing this service (Coffin, 2000).
Prescription of syringes, legal pharmacy sales, andneedle exchange have all been evaluated as modes of
making sterile needles accessible to IDU (Cotten-Old-
enburg, Carr, DeBoer, Collison & Novotny, 2001; Rich,
Macalino, McKenzie, Taylor & Burris, 2001; Singer et
al., 2000). While in some settings, legal barriers have
limited the accessibility of syringes to IDU, in other
settings operational or structural barriers such as
geographic accessibility must also be explored (Case,Meehan & Jones, 1998; Rockwell, Des Jarlais, Fried-
man, Perlis & Paone, 1999).
Over the last few years, further efforts have been
made to expand access to clean needles in Vancouver.
The number of needles exchanged was over 3 million in
the year 2000 (City of Vancouver, 2000). The exchange
program serves the city’s approximately 5000�/10 000
IDU, and augments the pharmacy sale of needles, whichis legal in Canada (Health Canada, 1998; Royal
Canadian Mounted Police, 2000). The NEP operates
through a number of fixed site needle exchanges in the
Downtown Eastside, several of which are within the
neighborhood’s low-income hotels, as well as through
mobile exchange vans, which exchange needles through-
out the night (Schechter et al., 1998; City of Vancouver,
2000). The exchange vans also exchange syringes inneighboring areas where syringe exchanges do not exist,
and several small syringe exchange programs operate in
municipalities surrounding Vancouver. IDU are in-
formed about the locations of needle exchanges and
the exchange vans through advertisements and flyers at
the fixed sites and at other services for IDU, as well as
through word of mouth. Despite these efforts, the
continuing transmission of HIV and HCV suggeststhat high numbers of IDUs continue to share needles
(Patrick et al., 2000).
Most recently, we have shown that persons who
obtain needles exclusively from needle exchange were
half as likely to share needles than persons who acquired
their needles from other sources (Wood, Tyndall,
Spittal, Li, O’Shaughnessy & Schechter, 2001a). How-
ever, these analyses also identified several risk factorsthat may explain persistent high-risk needle sharing in
Vancouver. The risk factor most strongly associated
with needle sharing was reporting having difficulty
accessing needles. Those who reported difficulty with
accessing sterile needles were 3.5 times more likely to
report needle sharing than persons who did not report
having difficulty with access (Wood et al., 2001a). This
observation raises several questions about why IDUs inVancouver continue to have difficulty accessing sterile
injecting equipment despite the high volume of needles
exchanged through the large exchange program. There-
fore, the present study was conducted to evaluate
reasons for difficulty accessing needles among Vancou-
ver IDUs.
Methods
Beginning in May 1996, persons who had injected
illicit drugs in the previous month were recruited into
the Vancouver Injection Drug User Study (VIDUS).
Data collection for the project is conducted in a
storefront office. The study site is not connected to,
and operates independently of, the NEP. Over 1400study subjects were recruited through self-referral and
street outreach. Persons were eligible if they had injected
illicit drugs at least once in the previous month, resided
in the greater Vancouver region, and provided written
informed consent. Ethical approval for the project was
provided by the University of British Columbia. Evi-
dence of recent injection drug use was required by
inspection of needle tracks. At baseline and semi-annually, subjects provided blood samples and com-
pleted an interviewer-administered questionnaire. The
questionnaire elicits demographic data including age,
gender, and place of residence, as well as drug use, risk
behaviors, and attendance at drug treatment and needle
exchanges. Participants are provided a nominal mone-
tary stipend at each study visit.
For the purposes of this study, we restricted ouranalyses to persons who returned for follow-up during
the period June 1, 2000�/May 31, 2001. Persons who had
not injected drugs in the previous 6 months were
excluded from all analyses since we sought to evaluate
reasons for difficulty accessing needles among persons
who were actively injecting drugs.
In order to identify IDU that are having difficulty
accessing syringes, the following question was asked ofall current injectors at their most recent follow-up:
‘‘Right now, do you currently find it hard to get new
rigs [needles ] when you need them?’’.
E. Wood et al. / International Journal of Drug Policy 13 (2002) 95�/10296

Participants were then offered to answer either Yes,
No, or Sometimes. We defined a person as ‘having
difficulty accessing needles’ if they answered yes or
sometimes to this question.We then sought to derive a socio-demographic and
drug using profile of persons who had difficulty acces-
sing syringes. Demographic characteristics such as age,
gender, and ethnic background were derived from the
baseline questionnaire. In order to evaluate current
activities, behavioral characteristics such as drug use,
and health-related characteristics such as HIV infection
were derived from the participant’s most recent follow-up questionnaire during the study period. Drug using
variables considered included frequency of cocaine and
heroin injection, and bingeing. Persons who reported
injecting cocaine or heroin once or more per day were
defined as frequent cocaine and frequent heroin users,
respectively. Bingeing was defined as binges or runs
where drugs were injected more frequently than usual.
Statistical analyses were applied to compare personswho had difficulty with access to participants who did
not have difficulty with access in the last 6 months.
Categorical explanatory variables were analyzed using
Pearson’s x2-test and continuous variables were ana-
lyzed using the Wilcoxon rank sum test. All variables
that were statistically significant at the 0.05 cut-off were
considered in logistic regression analyses.
For all persons who reported having difficulty acces-sing needles, the following question was then asked: ‘‘If
yes or sometimes, why do you find it hard to get new
[unused ] rigs?’’.
The interviewer did not read out a list of possible
explanations, but had a list of nine possible responses,
which were developed through prior piloting of this
question, as well as space to note answers that did not fit
with one of the nine categories. Participants were able toprovide more than one explanation.
In order to evaluate participant responses to the latter
question, the answers of all participants who reported
difficulty with access were summarized. However, in
order to rule out the potential for confounding as a
result of needle exchange source, we stratified the data
so that participants were divided into those who
acquired most (]/75%) of their needles from the fixedsite needle exchanges, the exchange vans, or from
pharmacies. We then evaluated the reasons for difficulty
accessing needles in each of the three groups.
Results
Overall, 942 participants returned for follow-up
during the period June 1, 2000�/May 31, 2001. Sincethe study’s inception, 124 participants have died. A
linkage with the province’s Vital Statistics Agency
indicated that deaths were due to HIV/AIDS (23%),
overdoses (33%), and other causes such as hepatitis and
suicides (44%). In addition, there were 371 participants
who did not come in for the most recent follow-up. Of
the 942 participants who were followed during the studyperiod, 761 (81%) reported injecting drugs in the last 6
months and were, therefore, included in the present
study. Of the 761 participants who were identified as
active IDU, 589 (77%) did not report having difficulty
accessing needles in the last 6 months, whereas 172
(23%) reported difficulty.
Table 1 shows the socio-demographic and drug using
characteristics of the participants stratified by those thatdid and did not have difficulty accessing needles. As
shown here, younger age (P B/0.001), male gender (P�/
0.041), residing outside of the Downtown Eastside (P�/
0.027), having been incarcerated in the last 6 months
(P�/0.003), using cocaine frequently (P�/0.001), using
heroin frequently (P�/0.001), and bingeing (P�/0.003)
were associated with difficulty accessing needles. We
found no association between difficulty accessing nee-
Table 1
Univariate analyses comparing socio-demographic characteristics of
persons who did and did not report having difficulty accessing needles
Characteristic Difficulty assessing rigs?
No n (%) Yes n (%) P -value
Age
Median 39 34 B0.001
IQR 32�/45 28�/41
Gender
Female 366 (62.1) 92 (53.5) 0.041
Male 223 (37.9) 80 (46.5)
Ethnic background
Aboriginal 167 (28.4) 53 (30.8) 0.531
Other 422 (71.7) 119 (69.2)
HIV positive
No 393 (66.7) 119 (69.2) 0.545
Yes 196 (33.3) 53 (30.8)
Neighborhood residence
Other 222 (37.7) 81 (47.1) 0.027
Downtown Eastside 367 (62.3) 91 (52.9)
Unstable housing
No 278 (47.2) 72 (41.9) 0.217
Yes 311 (52.8) 100 (58.1)
Incarcerated in the last 6 months
No 471 (80.0) 119 (69.2) 0.003
Yes 118 (20.0) 53 (30.8)
Heroin use frequency
B1 per day 442 (75.0) 103 (59.9) 0.001
]1 per day 147 (25.0) 69 (40.1)
Cocaine use frequency
B1 per day 504 (85.6) 125 (72.7) 0.001
]1 per day 85 (14.4) 47 (27.3)
Bingeing
No 420 (71.3) 102 (59.3) 0.003
Yes 169 (28.7) 70 (40.7)
E. Wood et al. / International Journal of Drug Policy 13 (2002) 95�/102 97

dles and ethnic background, HIV sero-status, or hous-
ing. Overall, 142 (18.7%) participants injected approxi-
mately once per month, 338 (44.4%) injected less than
once per day, 114 (15.0%) injected one to three times per
day, 61 (8.0%) injected three to five times per day, 106
(13.9%) injected greater than five times per day.
Table 2 shows the logistic regression analysis of
factors associated with difficulty accessing needles. As
shown here, older age (adjusted odds ratio [AOR]�/0.95
per year) and Downtown Eastside residence (AOR�/
0.56) were associated with less difficulty, whereas
frequent cocaine injection (AOR�/2.20) and bingeing
(AOR�/1.63) were associated with greater difficulty
accessing syringes. When this analysis was stratified by
where persons acquired most of their sterile needles
(either fixed site, van, or pharmacy) we found similar
results. The only noteworthy difference between the
overall model and the stratified analyses was that living
in the Downtown Eastside was only significant for fixed
site users (AOR�/0.51), whereas this variable was not
significant for van users and pharmacy users in stratified
multivariate analyses.
Fig. 1. Frequency of responses to the question regarding why participants had difficulty accessing sterile needles among the 69 participants who
acquired most of their needles from the fixed site exchanges.
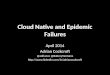
Fig. 2. Frequency of responses to the question regarding why participants had difficulty accessing sterile needles among the 33 participants who
acquired most of their needles from the exchange vans.
Table 2
Logistic regression analysisa of factors associated with difficulty
accessing sterile syringes
Variable Adjusted odds
ratio
95% Confidence
interval
Age (per year older) 0.95 (0.93�/0.97)
Downtown Eastside residence
(yes vs. no)
0.56 (0.39�/0.82)
Cocaine use frequency (]1
daily daily vs. B1)
2.20 (1.14�/3.43)
Bingeing (yes vs. no) 1.63 (1.11�/2.37)
a Variables that were statistically significant at the 0.05 cut-off were
considered in the model.
E. Wood et al. / International Journal of Drug Policy 13 (2002) 95�/10298

Overall, 351 (46.1%) of participants acquired most of
their needles from the fixed site exchanges, 109 (14.3%)
from the exchange vans, 60 (7.9%) from pharmacies,
and 241 (31.7%) acquired needles from multiple sourcesand did not identify a primary source. Of the 351
participants who acquired most of their needles from a
fixed site needle exchange, 69 (19.7%) also reported
difficulty with needle access. Fig. 1 depicts the reasons
given for this difficulty restricted to these 69 subjects. As
shown here, 49 (71.0%) of these individuals cited the
NEP being closed, 25 (36.2%) cited missing the exchange
van, and 22 (31.9%) cited being out of the area whereNEP operate as the primary reasons for difficulty having
access to sterile needles.
Fig. 2 provides analogous information for the 33
participants who acquired most of their needles from the
exchange vans and also reported difficulty with access.
As shown here, 19 (57.6%) of participants cited missing
the exchange van, 17 (51.5%) cited the NEP being
closed, ten (30.3%) cited being incarcerated, and seven(21.2%) cited being out of the area where NEP operate
as the primary reasons for difficulty having access to
sterile needles.
Similarly, Fig. 3 shows the same information for those
16 participants who acquired most of their needles from
pharmacies and also reported difficulty with access. As
shown here, 11 (68.8%) cited being refused needles at
pharmacies, 11 (68.8%) cited being out of the area whereNEP operate, and eight (50.0%) cited the NEP being
closed as the primary reasons for difficulty having access
to sterile needles.
Discussion
Previously, we identified several risk factors for high-
risk syringe sharing in Vancouver (Wood et al., 2001a).These factors included: bingeing, frequent cocaine
injection, male gender, and difficulty accessing needles
as the primary risk factor for high-risk needle sharing in
Vancouver. While the demographic and drug use factors
carried a relative risk of syringe sharing on the order of
approximately 2.0, persons who reported difficulty with
access to sterile needles were approximately 3.5 times
more likely to report syringe sharing after adjustmentfor other measured confounders. In the present study,
we found that several demographic and drug use
characteristics such as younger age, frequent injection,
bingeing, and living farther away from where exchange
services are concentrated to be associated with difficulty
accessing needles. In addition, the present study pro-
vides additional insight into why IDUs may be having
difficulty accessing needles through an assessment ofIDU’s explanations. Although problems with needle
access varied by needle source, several common themes
emerged. Specifically, the primary reasons for difficulty
accessing needles reported were the NEP being closed,
difficulty meeting the exchange van, being refused
needles at pharmacies, and being incarcerated in the
last 6 months.In previous analyses we have shown that frequent
cocaine injection and bingeing are associated with
needle sharing (Wood et al., 2001a). It is, therefore,
not surprising that these factors were in turn associated
with difficulty accessing needles, given the strong
association between difficulty accessing needles and
needle sharing. It is noteworthy, however, that neither
‘being too high’ nor bingeing emerged as common self-reported explanations for difficulty accessing needles.
This would suggest that bingeing and frequent drug use
may be associated with higher needle requirements, but
that structural barriers to sterile needle acquisition
contribute sharing behavior rather than merely the
instability of high intensity drug users.
Needle exchange operators face numerous challenges
in providing services for IDUs. In many settings,including Vancouver, needle exchanges face community
opposition as well as funding constraints. One way to
appease community concerns has been to offer restricted
hours of service. The operating hours of the Downtown
Eastside’s large fixed site needle exchange were from
8:00am to 8:00pm during the study period. Although it
may be perceived that these hours help to prevent drug
users coming into the area of the exchange during theevening, the present study identified restricted operating
hours as a primary reason for difficulty accessing
needles among all groups, even when the exchange
vans continue to operate. Similarly, funding limitations
may also force exchanges to provide only limited hours
of operation. In Vancouver, during the emergence of the
HIV epidemic, budgetary restrictions resulted in limiting
the services of the mobile exchange vans (Schechter etal., 1998). Although the present study suggests that
needle access would be greatly improved if the operating
hours of the NEP were increased, it is unclear if this
should be done at the expense of the services provided
by the exchange vans. We and others have shown that
mobile exchange vans may provide needle access to a
high-risk population that may not be serviced by fixed
site exchanges alone (Miller et al., 2001; Riley et al.,2000). This would argue for significant extensions of the
operating hours of the fixed site, even at times when the
vans are operating.
It is noteworthy that ‘missing the van’ was cited by a
number of respondents as contributing to their difficulty
in accessing needles. While mobile exchange is known to
expand the reach of NEPs and to access higher risk sub-
populations (Miller et al., 2001), it must be pointed outthat vans only remain in each distant location for a
limited period of time. This could explain the signifi-
cance of ‘missing the van’ as a risk factor. On this basis,
one might argue that an additional mechanism for
E. Wood et al. / International Journal of Drug Policy 13 (2002) 95�/102 99

exchange could be permanent but disseminated sources
of needles throughout high-risk areas. Strategies applied
elsewhere, that should be considered for evaluation in
Vancouver include needle vending machines and perma-
nent safe disposal boxes (Coffin, 2000; Obadia, Feroni,
Perrin, Vlahov & Moatti, 1999).
Needle exchange in the Vancouver region has been
targeted in the Downtown Eastside where IDU are most
highly concentrated, although limited NEPs exist in
some neighboring municipalities and some neighboring
areas are serviced by the exchange vans. Given the
concentration of the NEP’s services, it is not surprising
that being away from locations where needle exchange is
available was associated with difficulty accessing nee-
dles. However, injection drug use is found throughout
urban and rural areas of Canada, and the present study
suggests that novel strategies aimed at making needles
accessible to drug users in areas of low injection drug
use prevalence are needed. One such strategy has been to
legalize the pharmacy sale of needles to IDU. Alar-
mingly, being refused needles at pharmacies was com-
mon among all groups involved in the present study
regardless of their primary source of needles (fixed site,
van, or pharmacy) and was the primary reasons
reported by persons who primarily used pharmacies to
obtain sterile needles. Our findings support previous
analyses that have suggested that an educational cam-
paign directed at pharmacies throughout the province of
British Columbia may be required to help address this
concern (Myers, Cockerill, Worthington, Millson &
Rankin, 1998). In addition, although the present study
suggests that difficulty meeting the exchange van poses
problems, we and others have shown that exchange vans
may be an effective means of providing services to IDUs
in areas of low injection drug use prevalence (Miller et
al., 2001; Riley et al., 2000).
Being incarcerated in the last 6 months was also
identified as a reason for difficulty accessing needles. Of
concern is that we have recently found incarceration to
be independently associated with HIV seroconversion in
our cohort (Tyndall et al., 2001), as has been reported
elsewhere (Taylor et al., 1995). Previous studies have
indicated that injection drugs are widely available in
Canadian prisons, as well as prisons in most other
jurisdictions (Dolan, 2001; Kent, 1996). The present
study adds support to the growing body of literature
which suggests that the potential of NEPs to prevent the
spread of HIV within prisons must be explored,
especially considering the high-risk nature of prison
populations (Rothon, Mathias & Schechter, 1994).
There was little consistency among the ‘other’ answers
where IDUs provided additional explanations for diffi-
culty accessing syringes. It is noteworthy, however, that
several users reported that ‘police presence around the
needle exchange’ made accessing needles difficult, and
an earlier study from our setting identified police
intervention as barrier to sterile needle acquisition
(Strathdee et al., 1997a). To our knowledge, there is
no evidence that either targeted police presence or
incarceration are effective at reducing drug use, and
we have recently argued that legally sanctioned and
supervized safer injecting sites, where addicts can inject
pre-obtained illicit drugs, should be considered for
evaluation in Vancouver (Wood et al., 2001b). Such
facilities could be kept open 24 h and could alleviate
community concerns about drug users being drawn to
public spaces in the evenings, as well as provide space
where drug users could inject safely without fear of
police. Although the present study suggests that im-
proving the operating hours of the NEP may substan-
tially improve needle access, we have previously shown
that bingeing and frequent cocaine injection remain
strongly associated with needle sharing after adjustment
Fig. 3. Frequency of responses to the question regarding why participants had difficulty accessing sterile needles among the 16 participants who
acquired most of their needles from pharmacies.
E. Wood et al. / International Journal of Drug Policy 13 (2002) 95�/102100

for difficulty accessing needles (Wood et al., 2001a).
This observation suggests that merely improving needle
access as an isolated intervention will not be sufficient to
prevent the HIV epidemic in our setting.It is noteworthy that having no needles to exchange
and the NEPs ‘one for one’ exchange policy did not
emerge as common reasons why participants had
difficulty accessing needles. These policies have resulted
in greater than 100% re-acquisition of used needles by
the program, and undoubtedly less contaminated nee-
dles being discarded in public spaces. However, previous
studies have suggested that such policies may beproblematic due to the frequent injection behavior and
instability of cocaine users who are common in Van-
couver (Schechter et al., 1999; Wood et al., 2001a). A
qualitative study of these policies and how they relate to
HIV risk is currently ongoing.
When drawing conclusions from prospective cohort
data, several cautions are warranted. First, while some
studies have shown self-reported HIV risk behavior tobe valid (De Irala, Bigelow, McCusker, Hindin &
Zheng, 1996), other investigations have suggested that
IDUs may under-report HIV risk behavior (Des Jarlais
et al., 1999). Since the questions evaluated in the present
study did not involve HIV risk or other stigmatized
behaviors, it is unlikely that socially desirable reporting
is a major concern in this study.
In summary, our analyses indicate that difficulty inaccessing needles, the primary risk factor for needle
sharing in our setting, is likely related to operational
deficiencies in the NEP. Specifically, the major factors
identified in this study were the restricted operating
hours of the needle exchange and difficulty accessing the
exchange van. In addition, of concern are the reports of
being denied the sale of needles at pharmacies. Purchase
of needles at pharmacies is legal in Canada, and sincebeing away from where a needle exchange operates was
also a common reason for difficulty with access, it is
imperative that IDU have access to needles in areas
where injection drug use may not be prevalent. Finally,
we also identified being incarcerated as an explanation
for difficulty with access. Injection drugs are widely
available in Canadian prisons, and this finding adds to
the widespread consensus that NEPs should be evalu-ated within prisons (Dolan, 2001; Rothon et al., 1994).
Acknowledgements
Evan Wood is supported by Canadian Institutes for
Health Research, and the BC Heath Research Founda-
tion. Dr Schechter holds a tier I Canada Research Chair
in HIV/AIDS and Urban Population Health. The studywas supported by the US National Institutes of Health
(grant no. RO1 DA11591). We thank Bonnie Devlin,
Caitlin Johnston, Robin Brooks, Suzy Coulter, Steve
Kain, Guillermo Fernandez, John Charette, Will Small,
and Nancy Laliberte for their research and adminis-
trative assistance, and all the participants in the VIDUS
study.
References
American Journal of Public Health (2000). Discussion, American
Journal of Public Health 90 , 1385�/1396.
Bellm, J. (1999). Needle-exchange programmes are not the answer.
Lancet 353 , 1657�/1661 (letter; comment).
Bennett, S. S. (1998). Needle-exchange programmes in the USA.
Lancet 351 , 839 (letter; comment see comments).
Bluthenthal, R. N., Kral, A. H., Gee, L., Erringer, E. A. & Edlin, B. R.
(2000). The effect of syringe exchange use on high-risk injection
drug users: a cohort study. AIDS 14 , 605�/611.
Case, P., Meehan, T. & Jones, T. S. (1998). Arrests and incarceration
of injection drug users for syringe possession in Massachusetts:
implications for HIV prevention. Journal of Acquired Immune
Deficiency Syndrome and Human Retrovirology 18 (Suppl. 1), S71�/
S75.
City of Vancouver. (2000). Needle Exchange Review . Summary of
Findings to Date.
Coffin, P. (2000). Syringe availability as HIV prevention: a review of
modalities. Journal of Urban Health 77 , 306�/310.
Cotten-Oldenburg, N. U., Carr, P., DeBoer, J. M., Collison, E. K. &
Novotny, G. (2001). Impact of pharmacy-based syringe access on
injection practices among injecting drug users in Minnesota, 1998�/
1999. Journal of Acquired Immune Deficiency Syndromes 27 , 183�/
192.
De Irala, J., Bigelow, C., McCusker, J., Hindin, R. & Zheng, L. (1996).
Reliability of self-reported human immunodeficiency virus risk
behaviors in a residential drug treatment population. American
Journal of Epidemiology 143 , 725�/732.
Des Jarlais, D. C., Marmor, M., Paone, D., Titus, S., Shi, Q., Perlis,
T., Jose, B. & Friedman, S. R. (1996). HIV incidence among
injecting drug users in New York City syringe-exchange pro-
grammes. Lancet 348 , 987�/991.
Des Jarlais, D. C., Paone, D., Milliken, J., Turner, C. F., Miller, H.,
Gribble, J., Shi, Q., Hagan, H. & Friedman, S. R. (1999). Audio-
computer interviewing to measure risk behaviour for HIV among
injecting drug users: a quasi-randomized trial. Lancet 353 , 1657�/
1661.
Dolan, K. A. (2001). Can hepatitis C transmission be reduced in
australian prisons. Medical Journal of Australia 174 , 378�/379.
Health Canada (1998). Consortium to Characterize Injection Drug
Users in Canada Montreal, Toronto, and Vancouver.
Heimer, R. (1998). Can syringe exchange serve as a conduit to
substance abuse treatment. Journal of Substance Abuse Treatment
15 , 183�/191.
Junge, B., Valente, T., Latkin, C., Riley, E. & Vlahov, D. (2000).
Syringe exchange not associated with social network formation:
results from Baltimore. AIDS 14 , 423�/426.
Kent, H. (1996). Should prisons ease drug prohibition to help reduce
disease spread. Canadian Medical Association Journal 155 , 1489�/
1491.
Lurie, P., Reingold, A., & Bowser, B. E. A. (1993). The Public Health
Impact of Needle Exchange Programs in the United States and
Abroad: Summary, Conclusions, and Recommendations . Berkeley/
San Francisco: School of Public Health, University of California,
San Francisco, October 1993.
Miller, C. L., Tyndall, M. W., Li, K., Spittal, P. M. & Schechter, M. T.
(2001). Needle exchange source and risk taking behaviors among
E. Wood et al. / International Journal of Drug Policy 13 (2002) 95�/102 101

injection drug users. Canadian Journal of Infectious Diseases 12 ,
70B.
Myers, T., Cockerill, R., Worthington, C., Millson, M. & Rankin, J.
(1998). Community pharmacist perspectives on HIV/AIDS and
interventions for injection drug users in Canada. AIDS Care 10 ,
689�/700.
Obadia, Y., Feroni, I., Perrin, V., Vlahov, D. & Moatti, J. P. (1999).
Syringe vending machines for injection drug users: an experiment
in Marseille, France. American Journal of Public Health 89 , 1852�/
1854.
Office of National Drug Control Policy (1998). Executive Office of the
President, Washington, DC. Task Force Report on a Site Visit to
Vancouver .
Patrick, D. M., Tyndall, M. W., Cornelisse, P. G., Li, K., Sherlock, C.
H., Rekart, M. L., Strathdee, S. A., Currie, S. L., Schechter, M. T.
& O’Shaughnessy, M. V. (2000). The incidence of hepatitis C virus
infection among injecting drug users during an outbreak of HIV
infection. Canadian Medical Association Journal 2 165 (7), 889�/
895.
Rich, J. D., Macalino, G. E., McKenzie, M., Taylor, L. E. & Burris, S.
(2001). Syringe prescription to prevent HIV infection in Rhode
Island: a case study. American Journal of Public Health 91 , 699�/
700.
Riley, E. D., Safaeian, M., Strathdee, S. A., Marx, M. A., Huettner, S.,
Beilenson, P. & Vlahov, D. (2000). Comparing new participants of
a mobile versus a pharmacy-based needle exchange program.
Journal of Acquired Immune Deficiency Syndromes 24 , 57�/61.
Rockwell, R., Des Jarlais, D. C., Friedman, S. R., Perlis, T. E. &
Paone, D. (1999). Geographic proximity, policy and utilization of
syringe exchange programmes. AIDS Care 11 , 437�/442.
Rothon, D. A., Mathias, R. G. & Schechter, M. T. (1994). Prevalence
of HIV infection in provincial prisons in British Columbia.
Canadian Medical Association Journal 151 , 781�/787.
Royal Canadian Mounted Police Criminal Intelligence Directorate
(2000). Drug situation in Canada , 1999 .
Schechter, M., Currie, S., Strathdee, S. A., O’Shaughnessy, M. V.,
Patrick, D. M., Rekart, M. L., Turvey, J. & Schechver, M. T.
(1998). Maximizing needle exchange coverage among injection
drug users (IDUs): do mobile programs attract those at highest
risk. International Conference on AIDS 12 , 631 (abstract no.
33196).
Schechter, M. T., Strathdee, S. A., Cornelisse, P. G., Currie, S.,
Patrick, D. M., Rekart, M. L. & O’Shaughnessy, M. V. (1999). Do
needle exchange programmes increase the spread of HIV among
injection drug users? An investigation of the Vancouver outbreak.
AIDS 13 , F45�/F51.
Singer, M., Stopka, T., Siano, C., Springer, K., Barton, G., Khosh-
nood, K., Gorry de Puga, A. & Heimer, R. (2000). The social
geography of AIDS and hepatitis risk: qualitative approaches for
assessing local differences in sterile-syringe access among injection
drug users. American Journal of Public Health 90 , 1049�/1056.
Strathdee, S. A., Patrick, D. M., Archibald, C. P., Ofner, M.,
Cornelisse, P. G., Rekart, M., Schechter, M. T. & O’Shaughnessy,
M. V. (1997a). Social determinants predict needle-sharing beha-
viour among injection drug users in Vancouver, Canada. Addiction
92 , 1339�/1347.
Strathdee, S. A., Patrick, D. M., Currie, S. L., Cornelisse, P. G.,
Rekart, M. L., Montaner, J. S., Schechter, M. T. & O’Shaughnessy,
M. V. (1997b). Needle exchange is not enough: lessons from the
Vancouver injecting drug use study. AIDS 11 , F59�/65.
Strathdee, S. A., Celentano, D. D., Shah, N., Lyles, C., Stambolis, V.
A., Macalino, G., Nelson, K. & Vlahov, D. (1999). Needle-
exchange attendance and health care utilization promote entry
into detoxification. Journal of Urban Health 76 , 448�/460.
Taylor, A., Goldberg, D., Emslie, J., Wrench, J., Gruer, L., Cameron,
S., Black, J., Davis, B., McGregor, J., Follett, E., et al. (1995).
Outbreak of HIV infection in a Scottish prison. British Medical
Journal 310 , 289�/292.
Tyndall, M. W., Spittal, P. M., Laliberte, N., Li, K., O’Shaughnessy,
M. V. & Schechter, M. T. (2001). Intensive injection cocaine use as
a primary risk factor of HIV seroconversion among polydrug users
in Vancouver. Canadian Journal of Infectious Diseases 12 , 70B.
Wood, E., Tyndall, M. W., Spittal, P., Li, K., R. S., H., O’Shaugh-
nessy, M., & Schechter, M. T. (2001a). Predictors of Persistent
High-Risk Syringe Sharing During an Ongoing HIV Epidemic.
Canadian Journal of Infectious Diseases 12 (Suppl. B).
Wood, E., Tyndall, M. W., Spittal, P. M., Li, K., Kerr, T., Hogg, R.
S., Montaner, J. S., O’Shaughnessy, M. V. & Schechter, M. T.
(2001b). Unsafe injection practices in a cohort of injection drug
users in Vancouver: could safer injecting rooms help. Canadian
Medical Association Journal 165 , 405�/410.
E. Wood et al. / International Journal of Drug Policy 13 (2002) 95�/102102