Embed Size (px)
Citation preview
Treat with confidence. Trusted answers from the American Academy of Pediatrics.Treat with confidence. Trusted answers from the American Academy of Pediatrics.
Neonatal Abstinence Syndrome
Jatinder Bhatia, MD, FAAPMedical College of GeorgiaAugusta UniversityAugusta, GA
Treat with confidence. Trusted answers from the American Academy of Pediatrics.Treat with confidence. Trusted answers from the American Academy of Pediatrics.
Disclosures & Disclaimers Consultant for Nestlé USA CME lectures for Mead Johnson Nutrition Grant support from Chiesi, Duke (NIH) Statements and opinions expressed are those of the author and not
necessarily those of the American Academy of Pediatrics. Mead Johnson sponsors programs such as this to give healthcare
professionals access to scientific and educational information provided by experts. The presenter has complete and independent control over the planning and content of the presentation, and is not receiving any compensation from Mead Johnson for this presentation. The presenter’s comments and opinions are not necessarily those of Mead Johnson. In the event that the presentation contains statements about uses of drugs that are not within the drugs' approved indications, Mead Johnson does not promote the use of any drug for indications outside the FDA-approved product label.
Treat with confidence. Trusted answers from the American Academy of Pediatrics.Treat with confidence. Trusted answers from the American Academy of Pediatrics.
Objectives Define Neonatal Abstinence Syndrome (NAS)
Incidence
Commonly used/abused drugs
Signs and symptoms
Complications
Testing
Prevention and treatment
Treat with confidence. Trusted answers from the American Academy of Pediatrics.Treat with confidence. Trusted answers from the American Academy of Pediatrics.
Treat with confidence. Trusted answers from the American Academy of Pediatrics.Treat with confidence. Trusted answers from the American Academy of Pediatrics.
Terminology NAS refers to a postnatal opioid withdrawal syndrome. 55%–94% of newborns are affected when mothers are
addicted to or treated with opioids during pregnancy. Other terms: Neonatal withdrawal syndrome; neonatal drug
withdrawal syndrome; neonatal withdrawal A more liberal definition includes exposure to non-opioid
substances; however, assessment tools for NAS were developed for infants exposed to opioids.
Polysubstance use is common among those who use opioids.
McQueen K, Murphy-Oikonen J. Neonatal abstinence syndrome. N Engl J Med. 2016;375(25):2468–2479; Finnegan LP, Connaughton JF Jr, Kron RE, Emich JP. Neonatal abstinence syndrome: assessment and management. Addict Dis. 1975;2(1–2):141–158; Hudak ML, Tan RC, American Academy of Pediatrics Committee on Drugs, Committee on Fetus and Newborn. Neonatal drug withdrawal. Pediatrics. 2012;129(2):e540–e560; Davies H, Gilbert R, Johnson K, et al. Neonatal drug withdrawal syndrome: cross-country comparison using hospital administrative data in England, the USA, Western Australia and Ontario, Canada. Arch Dis Child Fetal Neonatal Ed. 2016;101(1):F26–F30; Kaltenbach K, Jones HE. Neonatal abstinence syndrome: presentation and treatment considerations. J Addict Med. 2016;10(4):217–223; and Krans EE, Cochran G, Bogen DL. Caring for opioid-dependent pregnant women: prenatal and postpartum care considerations. Clin Obstet Gynecol. 2015;58(2):370–379
Treat with confidence. Trusted answers from the American Academy of Pediatrics.Treat with confidence. Trusted answers from the American Academy of Pediatrics.
Introduction to Opioids Chemical class: Opioid vs opiate
o Opiates are from poppy plantso Opioid means they act like an opiate
Functional class: Narcotic analgesic
Treat with confidence. Trusted answers from the American Academy of Pediatrics.Treat with confidence. Trusted answers from the American Academy of Pediatrics.
Opioid Receptors Found in the brain, spinal cord, gastrointestinal (GI)
tract, and other organso μ (mu) receptors – respiratory depressant + GIo Δ, δ (delta) receptors – development of toleranceo Κ (kappa) receptors – involved in sedation + GI
Activation of the receptors:o Supraspinal analgesiao Release of dopamine (brain’s reward system)
Treat with confidence. Trusted answers from the American Academy of Pediatrics.Treat with confidence. Trusted answers from the American Academy of Pediatrics.
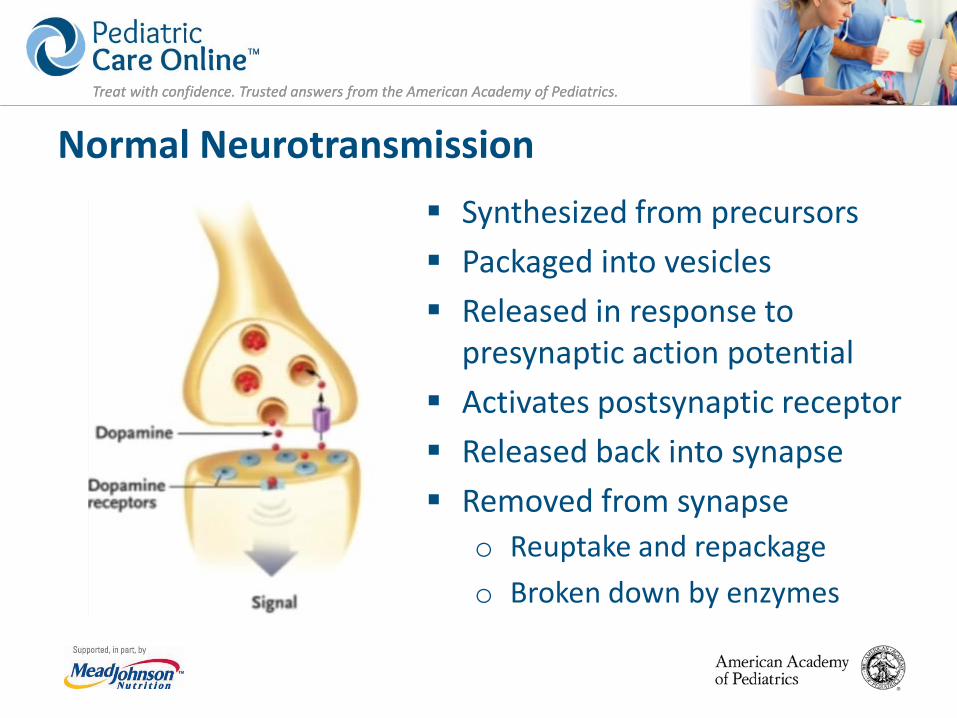
Normal Neurotransmission Synthesized from precursors Packaged into vesicles Released in response to
presynaptic action potential Activates postsynaptic receptor Released back into synapse Removed from synapse
o Reuptake and repackageo Broken down by enzymes
Treat with confidence. Trusted answers from the American Academy of Pediatrics.Treat with confidence. Trusted answers from the American Academy of Pediatrics.
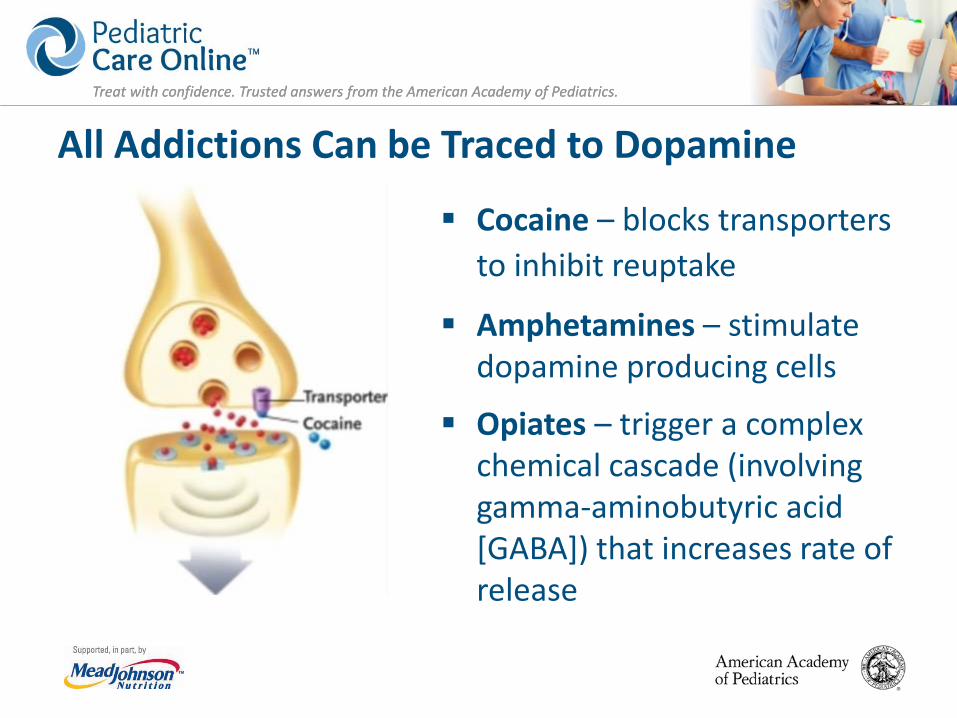
All Addictions Can be Traced to Dopamine
Cocaine – blocks transporters to inhibit reuptake
Amphetamines – stimulate dopamine producing cells
Opiates – trigger a complex chemical cascade (involving gamma-aminobutyric acid [GABA]) that increases rate of release
Treat with confidence. Trusted answers from the American Academy of Pediatrics.Treat with confidence. Trusted answers from the American Academy of Pediatrics.
Clinical Features Complex disorder
o Central and autonomic nervous systemso GI symptoms
• Clinical signs within the first few days after birth, but variable in timing and severity
• Mild tremors, irritability, fever• Excessive weight loss• Seizures• Type of opioid, dose, and timing of exposure alters risk
of withdrawalKocherlakota P. Neonatal abstinence syndrome. Pediatrics. 2014;134(2):e547–e561; and Wiles JR, Isemann B, Ward LP, Vinks AA, Akinbi H. Current management of neonatal abstinence syndrome secondary to intrauterine opioid exposure. J Pediatr. 2014;165(3):440–446
Treat with confidence. Trusted answers from the American Academy of Pediatrics.Treat with confidence. Trusted answers from the American Academy of Pediatrics.
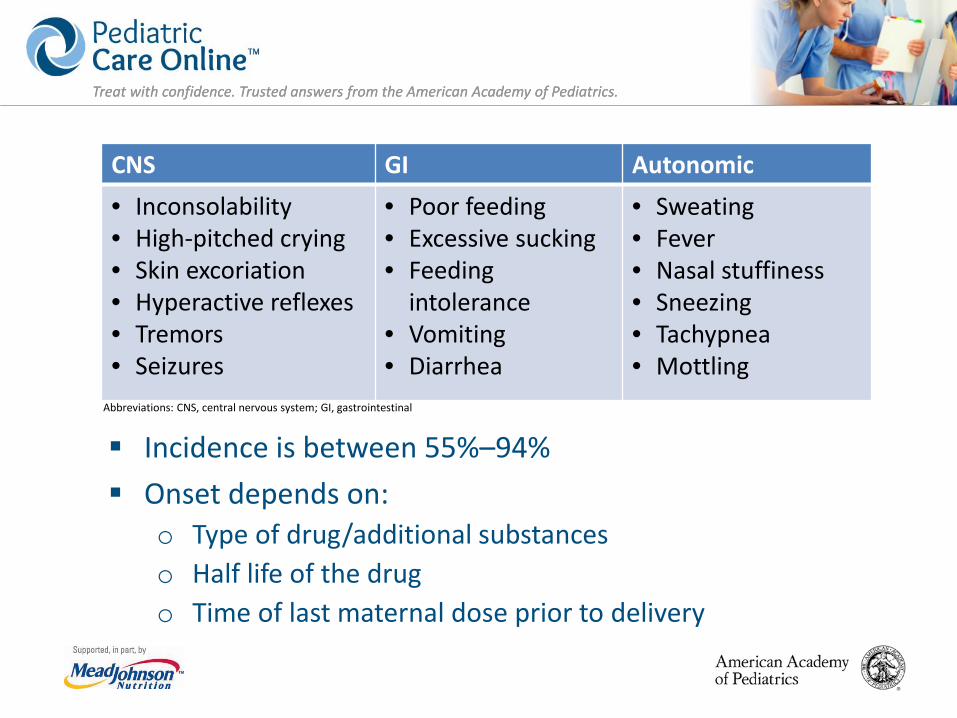
Incidence is between 55%–94% Onset depends on:
o Type of drug/additional substanceso Half life of the drugo Time of last maternal dose prior to delivery
CNS GI Autonomic• Inconsolability• High-pitched crying• Skin excoriation• Hyperactive reflexes• Tremors• Seizures
• Poor feeding• Excessive sucking• Feeding
intolerance• Vomiting• Diarrhea
• Sweating• Fever• Nasal stuffiness• Sneezing• Tachypnea• Mottling
Abbreviations: CNS, central nervous system; GI, gastrointestinal
Treat with confidence. Trusted answers from the American Academy of Pediatrics.Treat with confidence. Trusted answers from the American Academy of Pediatrics.
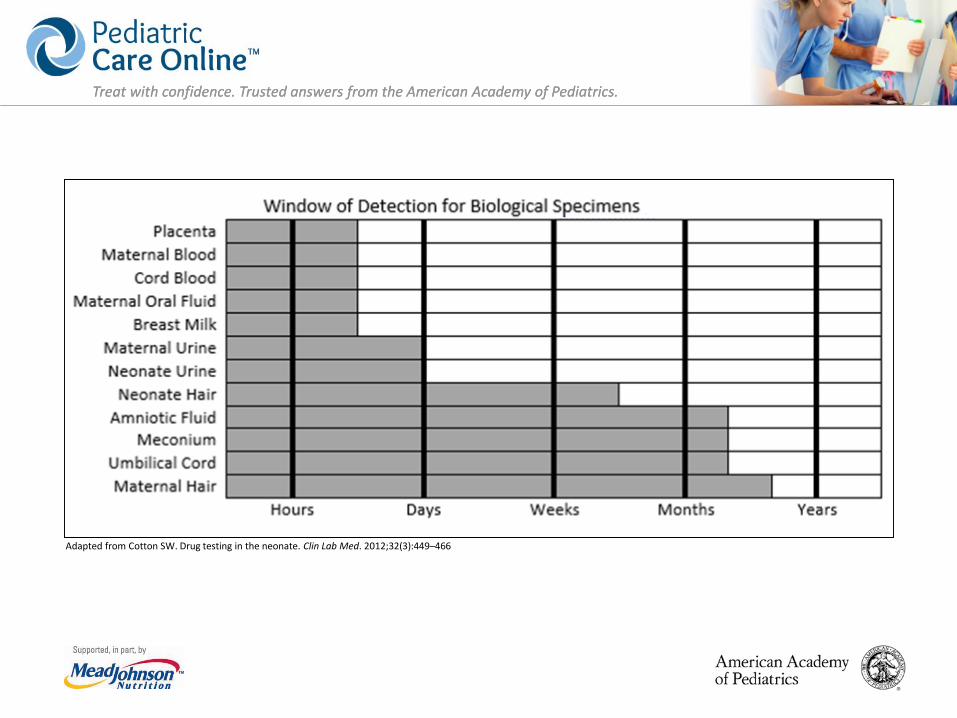
Adapted from Cotton SW. Drug testing in the neonate. Clin Lab Med. 2012;32(3):449–466
Treat with confidence. Trusted answers from the American Academy of Pediatrics.Treat with confidence. Trusted answers from the American Academy of Pediatrics.
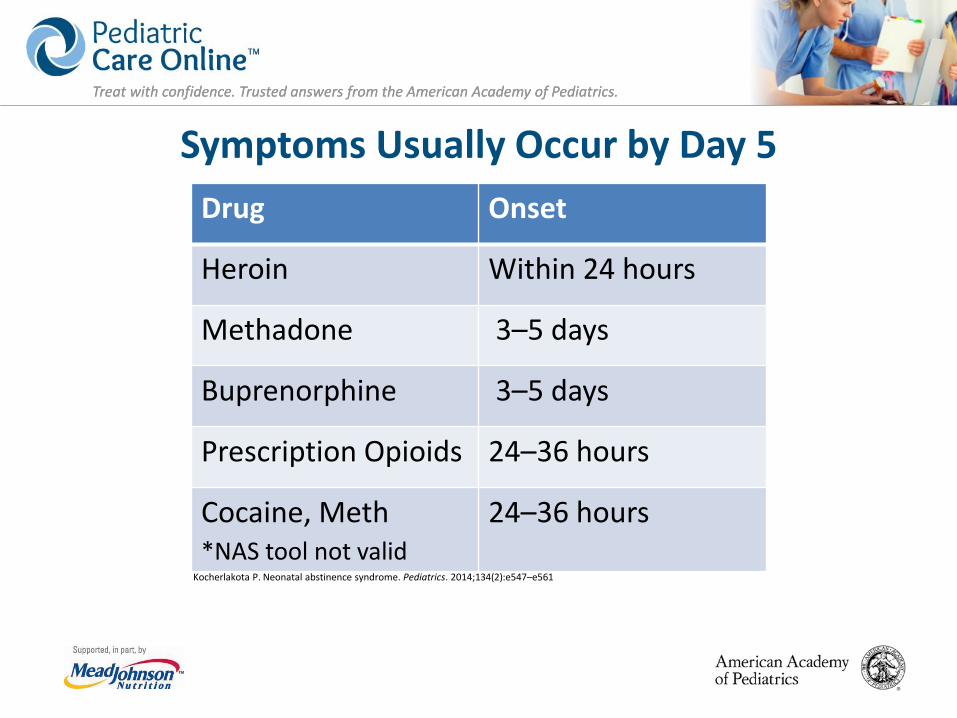
Symptoms Usually Occur by Day 5 Drug Onset
Heroin Within 24 hours
Methadone 3–5 days
Buprenorphine 3–5 days
Prescription Opioids 24–36 hours
Cocaine, Meth*NAS tool not valid
24–36 hours
Kocherlakota P. Neonatal abstinence syndrome. Pediatrics. 2014;134(2):e547–e561
Treat with confidence. Trusted answers from the American Academy of Pediatrics.Treat with confidence. Trusted answers from the American Academy of Pediatrics.
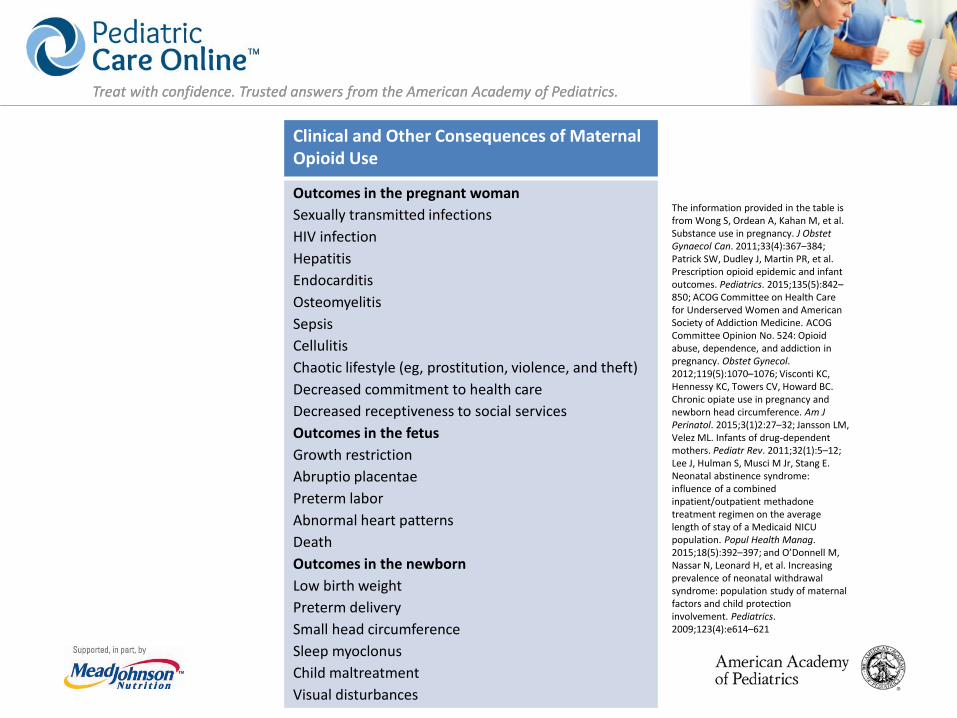
Clinical and Other Consequences of Maternal Opioid Use
Outcomes in the pregnant womanSexually transmitted infectionsHIV infectionHepatitisEndocarditisOsteomyelitisSepsisCellulitisChaotic lifestyle (eg, prostitution, violence, and theft)Decreased commitment to health careDecreased receptiveness to social servicesOutcomes in the fetusGrowth restrictionAbruptio placentaePreterm laborAbnormal heart patternsDeathOutcomes in the newbornLow birth weightPreterm deliverySmall head circumferenceSleep myoclonusChild maltreatmentVisual disturbances
The information provided in the table is from Wong S, Ordean A, Kahan M, et al. Substance use in pregnancy. J ObstetGynaecol Can. 2011;33(4):367–384; Patrick SW, Dudley J, Martin PR, et al. Prescription opioid epidemic and infant outcomes. Pediatrics. 2015;135(5):842–850; ACOG Committee on Health Care for Underserved Women and American Society of Addiction Medicine. ACOG Committee Opinion No. 524: Opioid abuse, dependence, and addiction in pregnancy. Obstet Gynecol. 2012;119(5):1070–1076; Visconti KC, Hennessy KC, Towers CV, Howard BC. Chronic opiate use in pregnancy and newborn head circumference. Am J Perinatol. 2015;3(1)2:27–32; Jansson LM, Velez ML. Infants of drug-dependent mothers. Pediatr Rev. 2011;32(1):5–12; Lee J, Hulman S, Musci M Jr, Stang E. Neonatal abstinence syndrome: influence of a combined inpatient/outpatient methadone treatment regimen on the average length of stay of a Medicaid NICU population. Popul Health Manag. 2015;18(5):392–397; and O’Donnell M, Nassar N, Leonard H, et al. Increasing prevalence of neonatal withdrawal syndrome: population study of maternal factors and child protection involvement. Pediatrics. 2009;123(4):e614–621
Treat with confidence. Trusted answers from the American Academy of Pediatrics.Treat with confidence. Trusted answers from the American Academy of Pediatrics.
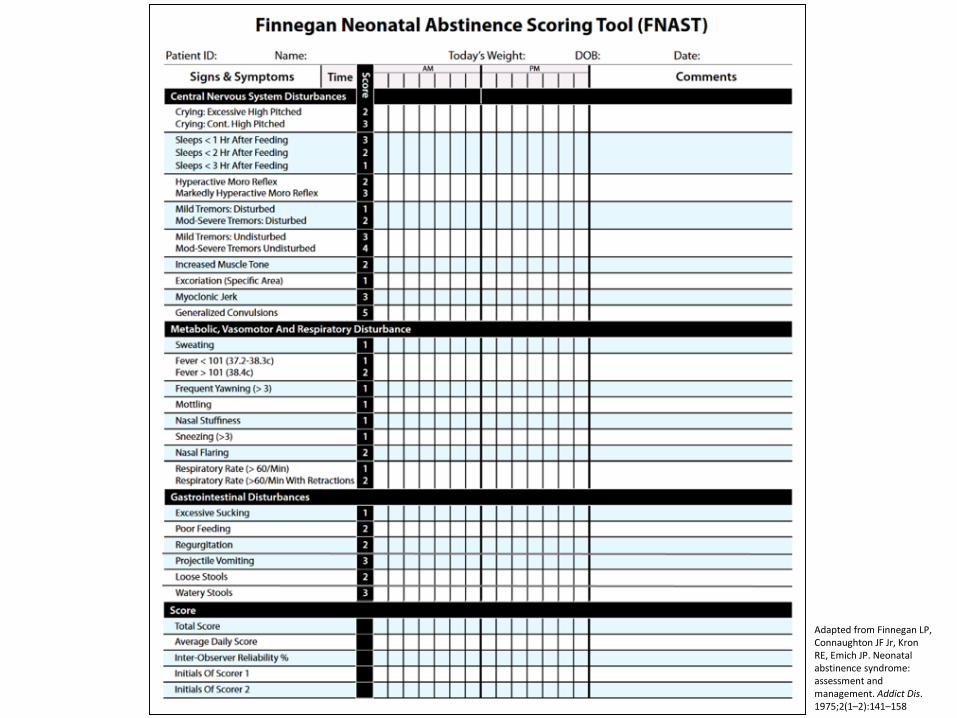
Adapted from Finnegan LP, Connaughton JF Jr, KronRE, Emich JP. Neonatal abstinence syndrome: assessment and management. Addict Dis. 1975;2(1–2):141–158
Treat with confidence. Trusted answers from the American Academy of Pediatrics.Treat with confidence. Trusted answers from the American Academy of Pediatrics.
Scoring Frequency Allow baby to transition before scoring begins
(generally within 2 hours)
Then score q 3–4 h
If total score >8, score q 2 h
Score before feeding
Consistent schedule
Treat with confidence. Trusted answers from the American Academy of Pediatrics.Treat with confidence. Trusted answers from the American Academy of Pediatrics.
What’s “Normal”? Healthy neonates with no opioid exposure On DOL 1–3, the median score = 2.0 Variability increased with age
o 95th percentile on DOL 1 = 5.5o 95th percentile on DOL 2 = 7.0
Circadian rhythm established by 5–6 weekso Median day score = 5.0o Median night score = 2.0
Scores >8 can be considered pathologicZimmermann-Baer U, Nötzli U, Rentsch K, Bucher HU. Finnegan neonatal abstinence scoring system: normal values for first 3 days and weeks 5-6 in non-addicted infants. Addiction. 2010;105(3):525–528
Treat with confidence. Trusted answers from the American Academy of Pediatrics.Treat with confidence. Trusted answers from the American Academy of Pediatrics.
Supportive Care
Scores <8 can generally be managed with non-pharmacologic, comfort care.
Treat with confidence. Trusted answers from the American Academy of Pediatrics.Treat with confidence. Trusted answers from the American Academy of Pediatrics.
Calm Environment Quiet, dim room with low activity
o Rooming-in: ↓Rx, ↓LOT, ↓LOS, ↓cost of NICU beds, promotes family-centered care
Away from high traffic areas (phone, sink, etc.) Prepare everything before disturbing and “cluster” care Limit visitors Avoid excessive handling Present one stimulus at a time (do not walk or sway
while feeding)
Treat with confidence. Trusted answers from the American Academy of Pediatrics.Treat with confidence. Trusted answers from the American Academy of Pediatrics.
Breastfeeding Encouraged:
o Promote bondingo Optimal nutritiono Passive immunityo ↓ severity of NAS
Contraindications:o HIV+o Not in treatmento Polydrugs?? (beware THC)
Cleveland LM. Breastfeeding recommendations for women who receive medication-assisted treatment for opioid use disorders: AWHONN Practice Brief Number 4. J Obstet Gynecol Neonatal Nurs. 2016;45(4):574–576; Pritham UA. Breastfeeding promotion for management of neonatal abstinence syndrome. J Obst Gynecol Neonatal Nurs. 2013;43(5):517–526; and Reece-Stremtan S, Marinelli KA. ABM clinical protocol #21: guidelines for breastfeeding and substance use or substance use disorder, revised 2015. Breastfeed Med. 2015;10(3):135–141
Miniscule amounts of drug in breastmilk:o Methadone = Hale category = L2o Buprenorphine transdermal = L2o Buprenorphine + Naloxone = L3
Treat with confidence. Trusted answers from the American Academy of Pediatrics.Treat with confidence. Trusted answers from the American Academy of Pediatrics.
Nursing Experience Parents may fear exposure as a “bad” person or losing
child to welfare systemo Parents may detach or distance from the infanto Nurse becomes surrogate mother
Nursing role conflicto Nurses have advanced training and specialized skillso Spend a considerable time soothing the affected infant,
and educating and consoling the familyo Perception that babies are less sick but very demanding
Murphy-Oikonen J, Montelpare WJ, Southon S, Bertoldo L, Persichino N. Identifying infants at risk for neonatal abstinence syndrome: a retrospective cohort comparison study of 3 screening approaches. J Perinat Neonatal Nurs. 2010;24(4):366–372 and Maguire D, Webb M, Passmore D, Cline G. NICU nurses’ lived experience: caring for infants with neonatal abstinence syndrome. Adv Neonatal Care. 2012;12(5):281–285
Treat with confidence. Trusted answers from the American Academy of Pediatrics.Treat with confidence. Trusted answers from the American Academy of Pediatrics.
AAP Guidelines
Drug therapy is indicated to relieve moderate to severe signs of NAS andto prevent complications such as fever, weight loss, and seizures if an infant does not respond to a committed program of non-pharmacologic support.
Treat with confidence. Trusted answers from the American Academy of Pediatrics.Treat with confidence. Trusted answers from the American Academy of Pediatrics.
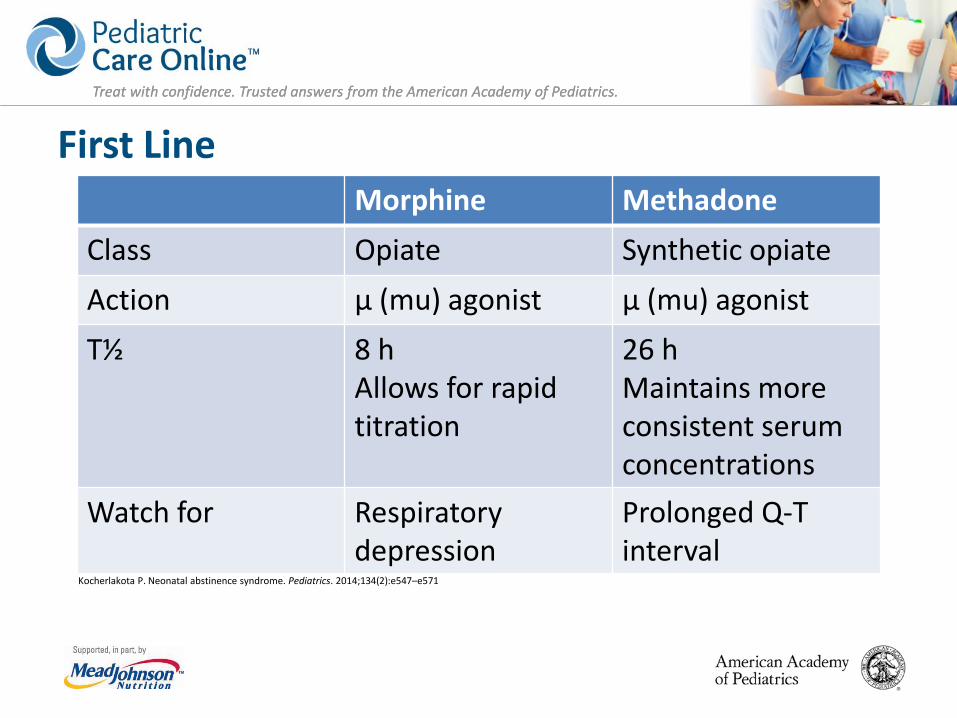
First Line
Kocherlakota P. Neonatal abstinence syndrome. Pediatrics. 2014;134(2):e547–e571
Morphine MethadoneClass Opiate Synthetic opiateAction μ (mu) agonist μ (mu) agonistT½ 8 h
Allows for rapid titration
26 hMaintains more consistent serum concentrations
Watch for Respiratory depression
Prolonged Q-T interval
Treat with confidence. Trusted answers from the American Academy of Pediatrics.Treat with confidence. Trusted answers from the American Academy of Pediatrics.
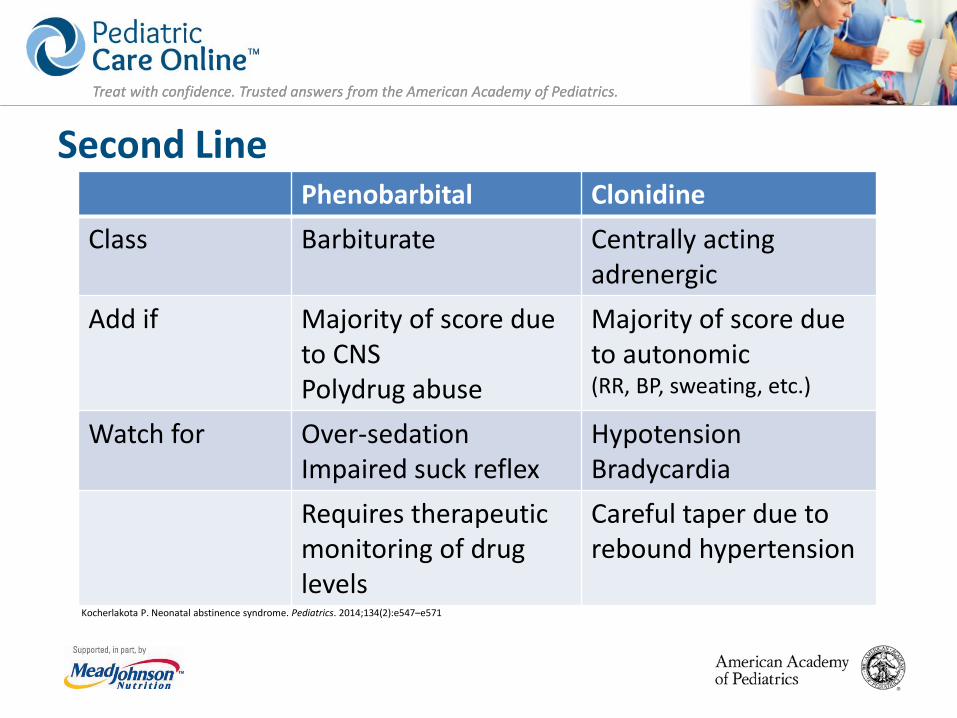
Second Line
Kocherlakota P. Neonatal abstinence syndrome. Pediatrics. 2014;134(2):e547–e571
Phenobarbital ClonidineClass Barbiturate Centrally acting
adrenergicAdd if Majority of score due
to CNSPolydrug abuse
Majority of score due to autonomic(RR, BP, sweating, etc.)
Watch for Over-sedationImpaired suck reflex
HypotensionBradycardia
Requires therapeutic monitoring of drug levels
Careful taper due to rebound hypertension
Treat with confidence. Trusted answers from the American Academy of Pediatrics.Treat with confidence. Trusted answers from the American Academy of Pediatrics.
If the infant is asleep when a dose is due, do not wake or skip the dose. Give dose in the inner cheek while offering a pacifier.
Treat with confidence. Trusted answers from the American Academy of Pediatrics.Treat with confidence. Trusted answers from the American Academy of Pediatrics.
Oral Sucrose Infants have a poorly functioning endogenous opioid
system.
Sucrose is ineffective in calming methadone exposed infants suffering from withdrawal signs and should not be used to treat abstinence.
May be helpful for minor procedural pain.
Marceau LD, Link CL, Smith LD, Carolan SJ, Jamison RN. In-clinic use of electronic pain diaries: barriers of implementation among pain physicians. J Pain Symptom Manage. 2010;40(3):391–404
Treat with confidence. Trusted answers from the American Academy of Pediatrics.Treat with confidence. Trusted answers from the American Academy of Pediatrics.
Remember, Narcan (naloxone) has been removed from NRP as a resuscitation medication.
Treat with confidence. Trusted answers from the American Academy of Pediatrics.Treat with confidence. Trusted answers from the American Academy of Pediatrics.
Weaning Stable NAS score (all scores <8 in the preceding
24–48 hours)
Allow 24–48 hours between medication weans
After discontinuing treatment, continue NAS scoring
Discharge when all scores are <8 for at least 24 hours
Treat with confidence. Trusted answers from the American Academy of Pediatrics.Treat with confidence. Trusted answers from the American Academy of Pediatrics.
Risk of Readmission
Infants diagnosed with NAS are nearly 2.5x as likely to be readmitted to the hospital in the first month after being discharged compared with full-term infants born without complications.
The most common cause is withdrawal.
Treat with confidence. Trusted answers from the American Academy of Pediatrics.Treat with confidence. Trusted answers from the American Academy of Pediatrics.
Discharge Education How to provide supportive care and soothing behaviors:
o Modify environment to ↓ sensory stimulationo Appropriate feedingo Good skin care
Infant and home safety Signs and symptoms of withdrawal How to handle stressful situations Appropriate babysitting arrangements Follow-up appointments and programs
Treat with confidence. Trusted answers from the American Academy of Pediatrics.Treat with confidence. Trusted answers from the American Academy of Pediatrics.
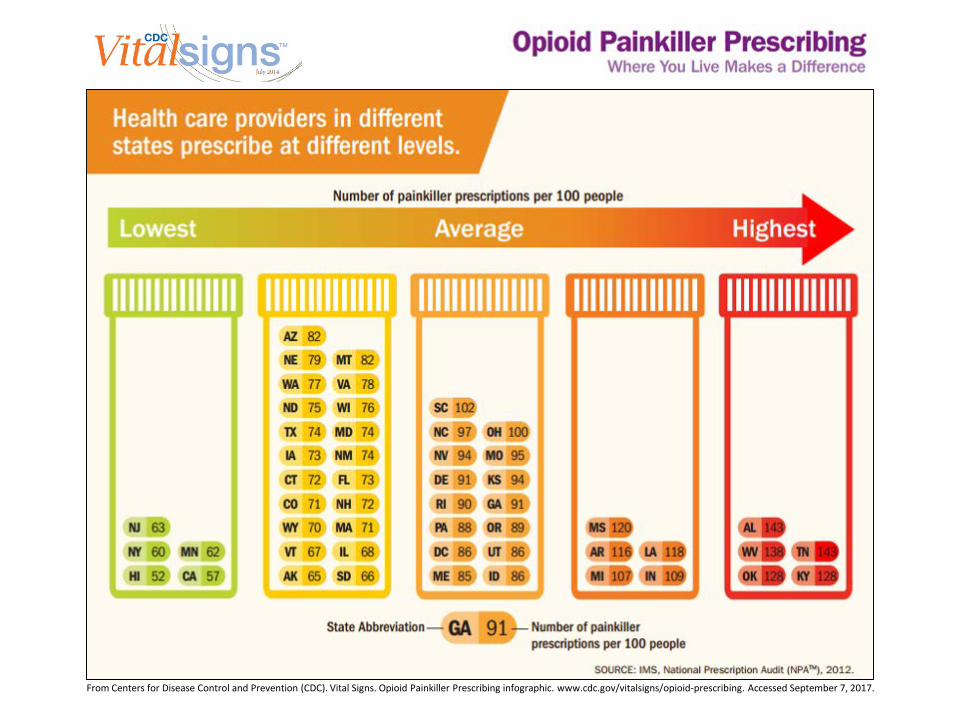
From Centers for Disease Control and Prevention (CDC). Vital Signs. Opioid Painkiller Prescribing infographic. www.cdc.gov/vitalsigns/opioid-prescribing. Accessed September 7, 2017.
Treat with confidence. Trusted answers from the American Academy of Pediatrics.Treat with confidence. Trusted answers from the American Academy of Pediatrics.
State Policies in Brief Substance abuse during pregnancy is considered:
o Criminal act (1 state) – allowed to “sunset” July 1, 2016o Child abuse (18 states)
When prenatal drug abuse is suspected:o Reporting is mandatory (18 states)
• Testing is mandatory (4 states)o Pregnant women given priority access to state-funded
treatment (13 states)
Guttmacher Institute. www.guttmacher.org
Treat with confidence. Trusted answers from the American Academy of Pediatrics.Treat with confidence. Trusted answers from the American Academy of Pediatrics.
Maternal Testing Requires Informed Consent Ferguson v City of Charleston, 532 US 67 (2001)
o Involuntary drug testing of pregnant women violates a person’s 4th amendment right(unreasonable search and seizure).
Linder v United States, 268 US 5 (1925) andRobinson v California, 370 US 660 (1962)o Addiction is an illness and criminalization is a
violation of the 8th amendment (cruel andunusual punishment).
Harris LH, Paltrow L. MSJAMA. The status of pregnant women and fetuses in US criminal law. JAMA. 2003;289(13):1697–1699
Treat with confidence. Trusted answers from the American Academy of Pediatrics.Treat with confidence. Trusted answers from the American Academy of Pediatrics.
Newborn Testing Does Not Require Maternal Consent
Individuals with Disabilities Education Act (IDEA)Part C: Early Intervention for Babies and Toddlers (1986)o Includes prenatal drug and alcohol exposure as a risk
factor for adverse developmental outcomes and therefore qualifies these children for evaluation and developmental services as needed.
Parents should be notified of the need for testing based on hospital policy and should be notified of the results.
Treat with confidence. Trusted answers from the American Academy of Pediatrics.Treat with confidence. Trusted answers from the American Academy of Pediatrics.
Conclusions A dramatic increase in prevalence, exposure substances,
and polypharmacy
Effective management strategies have been developed
Prevention strategies
Gaps exist: lack of clarity in definition and consistency
Treatment largely focused on isolation from mother/family
Follow-up of paramount importance
Treat with confidence. Trusted answers from the American Academy of Pediatrics.Treat with confidence. Trusted answers from the American Academy of Pediatrics.
Visit Pediatric Care Online today for additional information on this and other topics.
http://pediatriccare.solutions.aap.orgPediatric Care Online is a convenient electronic resource for immediate expert help with
virtually every pediatric clinical information need with must-have resources that are included in a comprehensive reference library and time-saving clinical tools.
Don’t have a subscription to PCO?Then take advantage of a free trial today!
Call Mead Johnson Nutrition at 888/363-2362 or,for more information, go to
http://pediatriccare.solutions.aap.org/SS/Free_Trial.aspx







![UC Davis Neonatal Abstinence Syndrome.pptx [Read-Only] Davis... · 19/4/2017 · Neonatal Abstinence Syndrome ... sensory neurons, intestinal tract ... and autonomic functioning)](https://img.pdfslide.net/doc/110x75/5ad501df7f8b9a48398d07fd/uc-davis-neonatal-abstinence-read-only-davis1942017neonatal-abstinence-syndrome.jpg)